
DOT/FAA/AM-18/5
Office of Aerospace Medicine
Washington, DC 20591
Literature Review and
Recommendations
Concerning Alcohol
Tolerance Under Part 67
Alejandro Caro-Nuñez
1
Thomas Chidester
2
1
Aerospace Medicine
National University of Colombia
Bogotá, Colombia
2
Civil Aerospace Medical Institute
Federal Aviation Administration
Oklahoma City, Oklahoma
July 2018
Final Report
NOTICE
This document is disseminated under the sponsorship of
the U.S. Department of Transportation in the interest of
information exchange. The United States Government
assumes no liability for the contents thereof.
___________
This publication and all Office of Aerospace Medicine
technical reports are available in full-text from the
Civil Aerospace Medical Institute’s publications website:
http://www.faa.gov/go/oamtechreports

i
Technical Report Documentation Page
1. Report No.
2. Government Accession No.
3. Recipient's Catalog No.
DOT/FAA/AM-18/5
4. Title and Subtitle
5. Report Date
Literature Review and Recommendations Concerning Alcohol Tolerance
Under Part 67
July 2018
6. Performing Organization Code
7. Author(s)
8. Performing Organization Report No.
Caro- Nuñez A,
1
Chidester T
2
9. Performing Organization Name and Address
10. Work Unit No. (TRAIS)
1
Aerospace Medicine, National University of Colombia, Bogotá,
Colombia
2
FAA Civil Aerospace Medical Institute, Oklahoma City, OK 73125
11. Contract or Grant No.
12. Sponsoring Agency name and Address
13. Type of Report and Period Covered
Office of Aerospace Medicine
Federal Aviation Administration
800 Independence Ave., S.W.
Washington, DC 20591
14. Sponsoring Agency Code
15. Supplemental Notes
16. Abstract
In the aviation industry, preventing misuse of alcohol among pilots has long been a concern for controlling
operational risk. Certification decisions in response to an airman’s report of an alcohol-related offense often
turn on evidence of tolerance. The Deputy Federal Air Surgeon consulted Aerospace Medical Research
management for guidance regarding appropriate standards referencing observed blood alcohol concentration
to determine tolerance. The authors were asked to complete a literature review and make recommendations.
In brief, there is good evidence, collected over more than seventy years, that a conscious and responsive
person with a BAC greater than or equal to 0.20% evidences alcohol tolerance. However, the literature
suggests a BAC greater than or equal to 0.15%, if accompanied by a report of minimal behavioral evidence
of intoxication, similarly evidences tolerance. And, current approaches to at-risk drinking would target
consumption of 5 or more drinks in one session of drinking (4 or more for females), even at lower BACs.
The latter would call attention to airmen of higher than average body weight when an arrest report indicates
a BAC less than 0.20%.
17. Key Words
18. Distribution Statement
Ethanol, Alcohol, Airmen Certification, Tolerance,
Dependence
Document is available to the public through the
Internet: www.faa.gov/go/oamtechreports/
19. Security Classif. (of this report)
20. Security Classif. (of this page)
21. No. of Pages
22. Price
Unclassified
Unclassified
11
Form DOT F 1700.7 (8-72) Reproduction of completed page authorized

1
LITERATURE REVIEW AND RECOMMENDATIONS CONCERNING
ALCOHOL TOLERANCE UNDER PART 67
In the aviation industry, preventing misuse of alcohol among pilots has long been a concern
for controlling operational risk. Between 1989 and 2013 in the United States, ethanol was detected
in 7% of civil aviation fatalities (1). Substance dependence and substance abuse are specified as
disqualifying medical conditions under 14 Code of Federal Regulations Part 67 (14 CFR 67),
Medical Standards and Certification. The FAA certifies airmen with alcohol-related incidents
under provisions of subparts 107 (First Class), 207 (Second Class), and 307 (Third Class). Under
mental health conditions, these subparts include:
(a) No established medical history or clinical diagnosis of any of the following:
(4) Substance dependence, except where there is established clinical evidence,
satisfactory to the Federal Air Surgeon, of recovery, including sustained total abstinence
from the substance(s) for not less than the preceding 2 years. As used in this section -
(i) “Substance” includes: Alcohol . . .; and
(ii) “Substance dependence” means a condition in which a person is dependent on a
substance, . . ., as evidenced by -
(A) Increased tolerance;
(B) Manifestation of withdrawal symptoms;
(C) Impaired control of use; or
(D) Continued use despite damage to physical health or impairment of social,
personal, or occupational functioning.
(b) No substance abuse within the preceding 2 years defined as:
(1) Use of a substance in a situation in which that use was physically hazardous, if there
has been at any other time an instance of the use of a substance also in a situation in which
that use was physically hazardous;
(2) A verified positive drug test result, an alcohol test result of 0.04 or greater alcohol
concentration, or a refusal to submit to a drug or alcohol test required by the U.S.
Department of Transportation or an agency of the U.S. Department of Transportation; or
(3) Misuse of a substance that the Federal Air Surgeon, based on case history and
appropriate, qualified medical judgment relating to the substance involved, finds -
(i) Makes the person unable to safely perform the duties or exercise the privileges of
the airman certificate applied for or held; or
(ii) May reasonably be expected, for the maximum duration of the airman medical
certificate applied for or held, to make the person unable to perform those duties or
exercise those privileges.
Certification decisions in response to an airman’s report of an alcohol-related offense often
turn on paragraph (4) and subparagraph (ii)(A), focusing on evidence of tolerance. This is typically

2
the most objective source for determining whether an airman is dependent upon alcohol. If the
examining AME determines that there is tolerance/dependence validated by an authoritative source
(Blood Alcohol Concentration, BAC, administered by Law Enforcement) or documentation
(medical records), the airman must be deferred for further review. If the Office of Aerospace
Medicine concurs with that evidence, they must then apply a 2-year waiting period that can be
waived only if the airman enters a valid treatment program, is monitored by a HIMS-trained
Designee, and qualifies for a special issuance medical certificate.
The Deputy Federal Air Surgeon consulted Aerospace Medical Research management for
guidance regarding appropriate standards referencing observed blood alcohol concentration to
determine tolerance. The perspectives of AMEs (including HIMS-trained) evaluating airmen are
variable depending upon their clinical experience and the academic/medical discipline in which
they were trained. Their application of non-regulator diagnostic criteria do not map consistently to
14 CFR 67. This situation could improve with reference to an objective measurement with a
defensible cut score. BAC greater than 0.20% was proposed as a cut point for stating conclusively
that tolerance exists. We were asked to review the literature to assess the validity of applying that
value.
In brief, there is good evidence, collected over more than seventy years, that a conscious and
responsive person with a BAC greater than or equal to 0.20% evidences alcohol tolerance.
However, the literature suggests a BAC greater than or equal to 0.15%, if accompanied by a report
of minimal behavioral evidence of intoxication, similarly evidences tolerance. And, current
approaches to at-risk drinking would target consumption of 5 or more drinks in one session of
drinking (4 or more for females), even at lower BACs. The latter would call attention to airmen of
higher than average body weight when an arrest report indicates a BAC less than 0.20%.
BACKGROUND
The use of alcoholic beverages is widespread in the United States. The National Institute on
Alcohol Abuse and Alcoholism (NIAAA) reports that 86 percent of adults have consumed alcohol
in their lifetime, 70% have done so in the last year, and 26% have engaged in binge drinking (five
or more drinks in one session) in the past month (2). Alcohol use disorder prevalence has been
estimated at 6.2% among adults through the National Survey on Drug Use and Health (3). In 2016,
more than one million drivers were arrested for driving under the influence of alcohol (4). In 2015,
there were 10,265 people killed in alcohol-impaired driving crashes. Among those, 67% (6,865)
were in crashes in which at least one driver in the crash had a BAC of 0.15 g/dL or higher (5).
Skaggs and Norris reported that as of 2016, there were 560,152 active medically certificated
airmen. Of these, 29,670 (5.3%) airmen have reported an alcohol related offense. Alcohol abuse
or dependence was identified in airmen records among 5,023 (0.90%) airmen (6).
Blood Alcohol Concentration is the result of a dynamic process, referred to as ethanol
pharmacokinetics (7). Ethanol absorption begins passively upon ingestion (7,8). Around 20
percent is absorbed in the stomach and the remaining 80 percent through the duodenum and
jejunum. Gastric emptying is a determining factor to the rate of rising and peak ethanol

3
concentration, which can vary depending on the presence or absence of food in the stomach (7,9).
There is a first-pass metabolism in the stomach by alcohol dehydrogenase (ADH). However, the
major enzyme systems responsible for the oxidation of ethanol are in the liver, with ADH and
cytochrome P450 oxidation of remaining ethanol. Since alcohol is not stored, the volume of
distribution tends to follow the distribution of total body water until eliminated (9). Elimination
follows the Michaelis-Menten model, which presents limitations when concentration approaches
zero and when it tends to infinity; when the concentration is very high, the rate of elimination is
independent of the plasma concentration and follows zero order kinetics (10). Despite a large
disparity in rates across persons, in a standard individual weighing154 lbs., the mean metabolic
capacity to remove ethanol is around 170 to 240 g per day or about 7 g per hour—roughly, one
standard drink (defined as any drink containing 14 grams of pure alcohol, equivalent to 12 ozs. of
beer at 5% alcohol, 5 ozs. wine at 12%, or 1.5 ozs. 80-proof liquor), per hour (11, 9). This
approximation allows the calculation of predicted BAC from number of drinks consumed, given
an individual’s body weight, and conversely the number of standard drinks consumed and yet to
be metabolized when BAC is reported following an arrest.
Tolerance to any drug may be described as acute or chronic. Acute tolerance is evidenced
during the descending phase of the blood alcohol curve where the behavioral effects of a certain
level of alcohol diminish compared to the same level in the ascending phase of the curve. The
individual appears and perceives him or herself to be less intoxicated at the same BAC after peak
concentration than before the peak. Chronic tolerance develops with repeated exposure, meaning
that consumption of a constant amount of alcohol produces a lesser effect or increasing amounts
of alcohol are necessary to produce the same effect (12). Chronic tolerance is the type referenced
in 14 CFR 67 and involves both metabolic and functional processes. Functional tolerance refers to
cell or tissue resistance to the effects of alcohol, requiring increasing doses to achieve the same
effect. Metabolic tolerance refers to the increase in alcohol absorption, distribution, degradation,
and excretion rate due to chronic administration (12,13). Research in blood alcohol concentrations
and metabolic or functional tolerance have been conducted for decades (13).
Evidence of tolerance with BAC between 0.15% and 0.20%
There is a consensus in the literature that BAC greater than 0.15 g/dl in a functional subject
can be related to some degree of tolerance (13–15). In 1938, Jetter collected blood and urine
samples from 1159 patients presenting with acute intoxication to Buffalo City Hospital. He
believed this sample to be biased towards chronic alcoholics and reported that intoxication could
be observed (by abnormal gait, abnormal speech, dilated pupils, and flushed face) in 10% of
patients at a BAC of 0.05%, 18% at 0.10%, 47% at 0.15%, 83% at 0.20%, 90% at 0.25%, and 95%
at 0.30% (16). In contrast, the American Medical Association Council on Scientific Affairs
reported in 1986 that intoxication at 0.05% BAC ranged from 0 to 10 %, at 0.10% from 14 to 68%,
at 0.15% from 47 to 93%, 90 to 100% above 0.20% BAC (17). Intoxication rate differences
between these reports between 0.10% and 0.20% BAC would support Jetter’s perception of a
sample biased towards chronic tolerance.

4
In 1943, Goldberg and colleagues studied single-event intoxication in abstainers, moderate
drinkers, and heavy drinkers. They provided alcohol in fixed doses to all three groups, then
assessed the blood alcohol curve and its consequences for vision, motor functions, and cognitive
performance. Perhaps most importantly, abstainers were unable to function with the dosage of
ethanol that created “measurable disorders of all functions tested” among moderate drinkers, but
“failed to produce any visible symptoms which could be used for quantitative measurement”
among heavy drinkers (p. 101-102). After adjusting dosage among the groups, habitual drinkers
maintained test performance at almost twice the dosage of alcohol given abstainers. Timing of
BAC rise and peak differed, with heavy drinkers reaching peak BAC sooner (18).
In 1964, Talland et al. conducted an experiment among male prisoners with a history of
alcoholism and found that reaction time with continuous manual performance was unaffected at
blood alcohol levels below 150mg/dL (0.15% BAC), and dexterity was unaffected below 200 mg
(0.20% BAC). These subjects tended to maintain cognitive and behavioral efficacy at high blood
alcohol levels, though decline in performance to non-responsiveness tended to result as BAC
approached 0.30% (19). A blood alcohol level of 51-100 mg/100 ml (0.05% to 0.10% BAC) was
most frequently associated with optimum efficiency in these chronic alcohol users. In the range of
150-200 mg/100ml their performance varied slightly (20). This finding is in stark contrast to tables
of BAC effects (21). At a BAC of 0.10%, non-tolerant individuals evidence significant
impairments of motor coordination, judgment, speech, balance, vision, reaction time, and hearing.
At a BAC of 0.15%, non-tolerant individuals suffer gross motor impairment and lack of physical
control; vomiting is expected. At a BAC of 0.20%, non-tolerant individuals are likely to black out,
suffer an inhibited gag reflex making nausea and vomiting dangerous, need help to stand or walk,
and may not experience pain when injured (22).
In 1975, Moskowitz, Daily, and Henderson conducted an experiment contrasting motor and
cognitive performance of moderate and heavy drinkers and reported that “frequency of drinking is
positively correlated with resistance to alcohol of both behavioral and physiological measures.”
Examination of performance charts in the paper reveals impairment levels to be different at all
measured BACs, with levels of impairment equivalent to moderate drinkers appearing among
heavy drinkers between 0.11 and 0.13%, depending upon the measure. On average, heavy drinker
impairment was 28% less across BAC levels up to 0.10%. Moderate drinkers were not exposed to
higher BACs (23).
There are ethical issues that make experiments like these unlikely to be replicated. For
example, the Talland study exposed a group of prisoners, probably sober solely due to their
incarceration, to high levels of intoxication (ramping up to 40 ounces per day of 86 proof whiskey
over the course of the study). The ability of prisoners to give fully informed consent is always
compromised by their incarceration and resulting motivation to improve their condition or reduce
their time in custody. Giving a drug to people in recovery (even when imposed by incarceration)
compromises their ability to return to full functionality. Goldberg worked in a time before World
War II-revelations of Nazi medical experiments resulted in a move to formalize the ethical

5
standards for experimentation with human subjects. Talland’s work also predates revelations of
the Tuskegee syphilis experiments that led to the Common Rule (see 45 CFR 46) now fundamental
to protection of human subjects (24). Subsequent research with alcohol has been more clinical and
observational, in the context of recovery, rather than experimental. Researchers have studied those
who drink to excess and sought help in recovery, rather than deliberately exposing abstainers and
experienced drinkers to high concentrations of alcohol.
In 1986, Perper et al. carried out a study with 110 patients who voluntarily requested admission
to a detoxification center. Patients’ speech, verbal comprehension, gait, pupil and vision, and
coordination were evaluated. Despite BACs above 200mg/100ml (0.20% BAC), 24 percent of the
subjects showed no signs of intoxication, and two subjects with BACs greater than 0.30%
exhibited sobriety at the time of examination (25).
The literature repeatedly references a BAC of 0.15% with minimal observable behavioral
effects, and 0.20% generally, as evidence of ethanol tolerance. Wallach states, “Blood ethanol
levels are also useful in the diagnosis of alcoholism because individuals who habitually use this
drug become tolerant. This diagnosis is suggested when a person can function in a relatively
normal capacity (without evidence of intoxication) with a blood ethanol level greater than 150
mg/dL.” (26). Mayo clinic publishes a similar statement on its website: “The blood ethanol level
is also useful in diagnosis of alcoholism. A patient who chronically consumes ethanol will develop
a tolerance to the drug, and requires higher levels than described above to achieve various states
of intoxication. An individual who can function in a relatively normal manner with a blood ethanol
level >150 mg/dL (>0.15%) is highly likely to have developed a tolerance to the drug achieved by
high levels of chronic intake.” (27)
This consensus is incorporated into the Diagnostic and Statistical Manual (DSM) of the
American Psychiatric Association. DSM-IV reads:
The blood level of a substance may be a useful clue in determining whether the
person has a high tolerance to a given group of substances (e.g., a person presenting
with a blood alcohol level of over 150 mg/dl without signs of Alcohol Intoxication
has a significant tolerance to alcohol and is likely to be a chronic user of either
alcohol or a sedative, hypnotic, or anxiolytic) (28).
DSM-5 reads:
An individual with a concentration of 150mg/dL of blood who does not show signs
of intoxication can be presumed to have acquired at least some degree of tolerance
to alcohol. At 200mg/dL, most nontolerant individuals demonstrate severe
intoxication (15).
In light of consensus incorporated into diagnostic and treatment standards, a decision rule
concerning regulatory interpretation of tolerance under Part 67 based upon an arrest BAC of 0.20%
is defensible and could be lowered to 0.15%, if referenced to behavioral evidence of intoxication
in the police report.
6
At-risk drinking implications for a BAC standard
On the other hand, there are reasons to be more conservative than this—to suspect evidence of
dependence at lower BAC levels under certain circumstances. Current thinking in alcohol use
disorder prevention and treatment focuses on at-risk drinking. The National Institute on Alcohol
Abuse and Alcoholism (NIAAA) argues that there are increased risks for alcohol-related problems
when men drink 5 or more standard drinks in a day (or more than 14 per week) and women drink
4 or more in a day (or more than 7 per week) (29). At-risk drinking is tied to multiple health and
behavioral outcomes in prospective studies, regardless of the peak BAC reached during drinking
episodes. Outcomes include subsequent diagnosis of dependence, development of liver disease,
initiation of illicit drug use, and social harm including relationship disruption and license
suspension (30, 31). A policy based upon drinks consumed could be developed from these
observations, requiring for example, alcohol use disorder evaluation for an arrest BAC
documenting consumption of 4 or more (for females) or 5 or more (for males) standard drinks
prior to the arrest. But at a minimum, it suggests some concern that tolerance or dependence may
have developed at lower observed BACs among airmen with higher body weight.
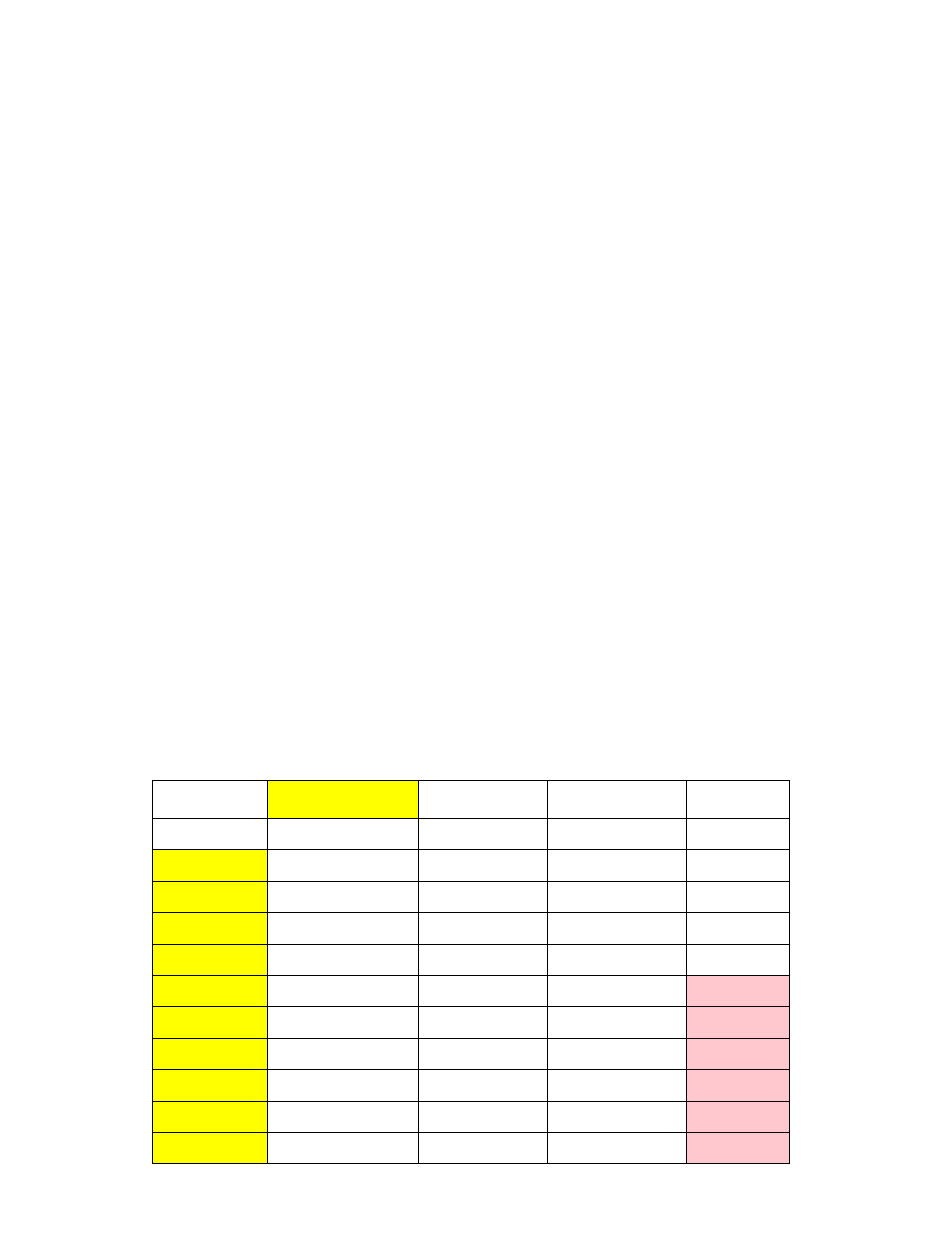
Taking into account toxicokinetics, Canfield (Canfield, DV 2017, oral communication, 8
th
September) constructed tables to estimate the number of drinks required to reach defined BACs,
given the body weight of male and female airmen, and highlighted where at-risk drinking is
reflected (See Table 1–2). Importantly, this is a calculation of standard drinks yet to be
metabolized. More drinks may have been consumed and metabolized over a multi-hour episode
preceding testing associated with an arrest.
Table 1. Converting concentrations into number of drinks for an average male airman (190lb/86kg (6)),
assuming post absorptive phase.
Weight
190
86
Vd
0.69
BAC
Dose (g)
Dose (oz)
Beer (oz)
Drinks
0.02
11.89
0.42
8.39
0.7
0.04
23.79
0.84
16.78
1.4
0.08
47.57
1.68
33.56
2.8
0.10
59.47
2.10
41.95
3.5
0.15
89.20
3.15
62.92
5.2
0.20
118.93
4.19
83.90
7.0
0.25
148.67
5.24
104.87
8.7
0.30
178.40
6.29
125.84
10.5
0.35
208.13
7.34
146.82
12.2
0.40
237.87
8.39
167.79
14.0
Dose=BAC(g)*VdxKg
Cells highlighted in pink represent at-risk drinking

7
Table 2. Converting concentrations into number of drinks for an average female airman (140lb/63kg (6)),
assuming post absorptive phase.
Weight
140
64
Vd
0.69
Conc.
Dose (g)
Dose (oz)
Beer (oz)
Drinks
0.02
8.00
0.28
5.64
0.5
0.04
16.00
0.56
11.29
0.9
0.08
32.01
1.13
22.58
1.9
0.10
40.01
1.41
28.22
2.4
0.15
60.01
2.12
42.33
3.5
0.20
80.02
2.82
56.44
4.7
0.25
100.02
3.53
70.55
5.9
0.30
120.02
4.23
84.66
7.1
0.35
140.03
4.94
98.77
8.2
0.40
160.03
5.64
112.89
9.4
Dose=BAC(g)*VdxKg
Cells highlighted in pink represent at-risk drinking
Use of a 0.20% BAC as evidence of tolerance under Part 67 is also consistent with concepts
of at-risk drinking for female airmen of average weight, 4.7 drinks. For male airmen of average
weight, a 0.20% BAC translates to 7 drinks; the at-risk drinking standard is reached at a BAC of
0.15%. For males, at-risk definition and 0.20% BAC are equivalent for airmen weighing
approximately 160 lbs. Recognizing that tolerance and at-risk drinking are not identical, the BAC
of 0.20% is probably a reasonable standard for males up to 190 lbs and females up to 170 lbs. The
risk of this approach is that this BAC represents 140% of at-risk drinking, but it does create some
regulatory slack for an arrest that might represent a once-in-a-lifetime binge.
However, for example, a male airman weighing 250 lbs at a 0.20% BAC would have consumed
9 drinks, 180% of at-risk drinking; a female of the same weight 8 drinks, 200% of at-risk drinking.
This suggests some concern that tolerance or dependence may have developed at lower observed
BACs among airmen with higher body weight.
SUMMARY AND RECOMMENDATIONS
Alcohol tolerance under 14 CFR 67 references chronic tolerance, which develops with repeated
exposure, meaning that consumption of a constant amount of alcohol produces a lesser effect or
increasing amounts of alcohol are necessary to produce the same effect.
Tolerant individuals evidence maintenance of cognitive function and motor skills at higher
levels of blood alcohol than observed in normal individuals, and less than optimal cognitive
function and motor skills when abstinent of alcohol.
The literature repeatedly references a BAC of 0.15% with minimal observable behavioral
effects, and 0.20% generally, as evidence of ethanol tolerance.

8
The National Institute on Alcohol Abuse and Alcoholism (NIAAA) argues that there are
increased risks for alcohol-related problems when men drink 5 or more standard drinks in a day
(or more than 14 per week) and women drink 4 or more in a day (or more than 7 per week). This
approach suggests some concern that tolerance or dependence may have developed at lower
observed BACs among airmen with higher body weight.
Canfield has constructed tables to estimate the number of standard unmetabolized drinks
required to reach defined BACs, given the body weight of male and female airmen, and highlighted
where at-risk drinking is reflected.
Based upon review of the literature, we recommend the Federal Air Surgeon identify a
documented BAC of 0.20% or greater to be presumptive evidence of ethanol tolerance under 14
CFR 67, and further a documented BAC between 0.15% and 0.20% to be potential evidence of
tolerance. In making decisions regarding the latter, the Federal Air Surgeon should consider the
airman’s weight, if greater than 190 lbs. for male or 170 lbs. for female, and evidence of degree of
behavioral impairment in an arrest report accompanying the alcohol test.
REFERENCES
1. Chaturvedi AK, Craft KJ, Hickerson JS, Rogers PB, Canfield D V. Ethanol and Drugs
Found in Civil Aviation Accident Pilot Fatalities, 1989–2013. Aerosp Med Hum Perform.
2016.
2. National Institute on Alcohol Abuse and Alcoholism. Alcohol Facts and Statistics
[Internet]. NIH Turning Discovery Into Health. 2017 [cited 2017 Oct 20]. Available from:
https://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/alcohol-facts-
and-statistics
3. Substance Abuse and Mental Health Services Administration. National Survey on Drug
Use and Health [Internet]. 2017 [cited 2017 Oct 20]. Available from:
https://nsduhweb.rti.org/respweb/homepage.cfm
4. Crime in the United States 2016: Uniform Crime Reports. Federal Bureau of
Investigation.
5. Highway Traffic Safety Administration N, Department of Transportation U. 2015 Data:
Alcohol-Impaired Driving. 2015.
6. Skaggs VJ, Norris AI. 2016 Aerospace Medical Certification Statistical Handbook. Off
Aerosp Med. 2017.
7. Pizon AF, Becker CE, Bikin D. The Clinical Significance of Variations in Ethanol
toxicokinetics. J Med Toxicol. 2007;3(2):63–72.
8. Dubowski KM. Absorption, distribution and elimination of alcohol: highway safety
aspects. J Stud Alcohol. 1985;10:98–108.
9. Cederbaum AI. Alcohol Metabolism. Clinics in Liver Disease. 2012.
10. Norberg Å, Jones WA, Hahn RG, Gabrielsson JL. Role of variability in explaining ethanol
pharmacokinetics: Research and forensic applications. Clinical Pharmacokinetics. 2003.
11. National Institute on Alcohol Abuse and Alcoholism. What is a standard drink? [Internet].
9
[cited 2017 Nov 8]. Available from:
https://pubs.niaaa.nih.gov/publications/Practitioner/pocketguide/pocket_guide2.htm
12. Tabakoff B, Cornell N, Hoffman PL. Alcohol Tolerance. Ann Emerg Med. 1986;15:1005–
12.
13. Caplan YH, Goldberger BA. Garriot’s medicolegal aspects of alcohol. Sixth edit.
Tucson,AZ: Lawyers & Judges Publishing Company. 2015.
14. Wallach J. Interpretation of Diagnostic Tests. Lippincott Williams & Wilkins. 2007.
15. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
Fifth Edit. Washington: American Psychiatric Publishing. 2013.
16. Jetter W. Studies in alcohol. I. the diagnosis of acute alcohol intoxication by a correlation
of clinical and chemical findings. Am J Med Sci. 1938;196:475–87.
17. Chesher G, Greeley J. Tolerance to the effects of alcohol. Alcohol, Drugs Driv.
1992;8(2):93–106.
18. Goldberg L. Quantitative studies on alcohol tolerance in man. Part III. The influence of
habituation on Alcohol Tolerance. Acta Physiol Scand. 1943;5(16):95–114.
19. Talland GA, Mendelson JH, Ryack P. Experimentally induced chronic intoxication and
withdrawal in alcoholics. Pt 4. Tests of motor skills. Q J Stud Alcohol. 1964;2:53–73.
20. Talland GA, Mendelson JH, Ryack P. Experimentally Induced Chronic Intoxication and
Withdrawal in Alcoholics. Pt5. Tests of Attention. Q J Stud Alcohol. 1964;2:74–86.
21. Centers for Disease Control and Prevention. What are the effects of blood alcohol
concentration (BAC)? [Internet]. Impaired Driving: Get the Facts. 2017 [cited 2017 Oct
18]. Available from: https://www.cdc.gov/motorvehiclesafety/impaired_driving/impaired-
drv_factsheet.html
22. Slick and Bubba’s. B.R.A.D. 21 Be responsible about drinking. Effects at specific B.A.C.
levels. 2017.
23. Moskowitz H, Daily J, Henderson R. Acute tolerance to behavioral impairment by alcohol
in moderate and heavy drinkers: Final report. Dep Transp Natl Highw Traffic Saf Adm.
1974;DOT HS-009(L).
24. Office for Human Research Protections. 45 CFR Part 46 Protection of Human Subjects
[Internet]. Regulations. 2009 [cited 2017 Oct 18]. Available from:
https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/index.html
25. Perper J, Twerski A, Wienand JW. Tolerance at high blood alcohol concentrations A
study of 110 cases and review of the literature. J Forensic Sci. 1986;1:212–21.
26. Wallach, J. Interpretation of Diagnostic Tests. Disorders due to Physical and Chemical
Agents. 8
th
ed. Lipincott Lilliams and Wilkins, 2007
27. Mayo Clinic Mayo Medical Laboratories. Test ID: ALC Ethanol, Blood [Internet].
Clinical and Interpretative. 2017 [cited 2017 Oct 20]. Available from:
https://www.mayomedicallaboratories.com/test-catalog/Clinical+and+Interpretive/8264
28. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
Fourth Edi. Washington, DC: the Association. 1994.
10
29. National Institute on Alcohol Abuse and Alcoholism. Helping Patients Who Drink Too
Much: A CLINICIAN’S GUIDE Updated 2005 Edition. Bethesda, MD. 2016.
30. D. A. Dawson, Grant BF, Li TK. Quantifying the risks associated with exceeding
recommended drinking limits. Alcohol Clin Exp Res. 2005;29(5):902–8.
31. Dawson DA. Defining Risk Drinking. Alcohol Res Heal. 2011;34(2):144–56.
