
U.S. DEPARTMENT OF THE TREASURY
Long-Term Care Insurance: Recommendations for Improvement of Regulation i
U.S. DEPARTMENT OF THE TREASURY
Long-Term Care Insurance:
Recommendations for Improvement
of Regulation
Report of the Federal Interagency Task Force
on Long-Term Care Insurance
AUGUST 2020

U.S. DEPARTMENT OF THE TREASURY
Long-Term Care Insurance:
Recommendations for Improvement of
Regulation
Report of the Federal Interagency Task Force on
Long-Term Care Insurance
Steven T. Mnuchin
Secretary
Michael Faulkender
Assistant Secretary for Economic Policy
Acknowledgments
The Federal Interagency Task Force on Long-Term Care Insurance consists of representatives
from the U.S. Department of the Treasury (Treasury), the U.S. Department of Health and Human
Services (HHS), the U.S. Department of Labor (DOL), and the Office of Management and
Budget (OMB). Secretary Mnuchin and Treasury Assistant Secretary Michael Faulkender would
like to thank the following individuals for their service as members of the Task Force and their
contributions to this report:
Treasury: Jason Brown, Diana Furchtgott-Roth, Anne Hall, Alex Hart, Eda Herzog-Vitto, Gillian
Hunter, Louisa Quittman, Shanthi Ramnath, Bruce Saul, Steven Seitz, Angela Walitt, and Harlan
Weller
HHS: William Marton and Mary Nugent
DOL: Jeanne Klinefelter Wilson
OMB: Amy Batchelor and Rebecca Spavins
Secretary Mnuchin and Assistant Secretary Michael Faulkender would also like to thank
Treasury staff members Bruce Saul and Elizabeth Sawyer for supporting the Task Force and
leading Treasury staff’s work on the report.
Long-Term Care Insurance: Recommendations for Improvement of Regulation iv
Table of Contents
Executive Summary ................................................................................................... 1
Introduction ......................................................................................................................... 1
Scope and Objectives of the Task Force ............................................................................. 2
Long-Term Care Insurance in the United States................................................................. 2
Review of the Process for this Report................................................................................. 3
Summary of Analysis and Recommendations .................................................................... 4
The Role of Insurance in Long-Term Care ..............................................................10
Prevalence of Need for LTSS ........................................................................................... 10
Projections of Demand for LTSS ...................................................................................... 12
Financing of LTSS ............................................................................................................ 14
Factors Impeding the Market for Private LTCI ................................................................ 19
Innovation and Product Development .....................................................................23
Combination Products ....................................................................................................... 23
Other New Product Designs.............................................................................................. 27
Regulatory Efficiency and Alignment .....................................................................34
Inflation Protection ........................................................................................................... 34
Other Consumer Protections ............................................................................................. 37
Review and Approval of Rate Increases ........................................................................... 37
Financial Literacy and Education ............................................................................40
Reviewing the Federal Role in Financial Education......................................................... 40
Stakeholder Recommendations Relating to Education ..................................................... 41
Best Practices for Financial Education ............................................................................. 42
Tax Incentives ..........................................................................................................44
Current Tax Rules Regarding LTCI ................................................................................. 44
Analysis of Tax Incentives Considered ............................................................................ 48
Alternative Financing Approaches ..........................................................................55
Front-End Benefit Options ................................................................................................ 55
Back-End (Catastrophic) Options ..................................................................................... 58
Comprehensive Options .................................................................................................... 59
Long-Term Care Insurance: Recommendations for Improvement of Regulation v
Appendices ...............................................................................................................60
Appendix A: Participants in the Engagement Process ...................................................... 60
Appendix B: Summary of Analysis and Recommendations............................................. 61

Long-Term Care Insurance: Recommendations for Improvement of Regulation v
Abbreviations
Acronym
Abbreviation
ACI
Annual Compound Inflation
ADLs
Activities of Daily Living
AGI
Adjusted Gross Income
CBO
Congressional Budget Office
CDC
Centers for Disease Control and Prevention
CMS
U.S. Department of Health and Human Services, Centers for
Medicare & Medicaid Services
Code
Internal Revenue Code
DOL
U.S. Department of Labor
DRA
Deficit Reduction Act of 2005
EBSA
U.S. Department of Labor, Employee Benefits Security
Administration
EPDV
Expected Present Discounted Value
ERISA
Employee Retirement Income Security Act of 1974
FIO
U.S. Department of the Treasury, Federal Insurance Office
FLEC
Financial Literacy Education Commission
FSA
Flexible Spending Arrangement
HDHP
High-Deductible Health Plan
HHS
U.S. Department of Health and Human Services
HIPAA
Health Insurance Portability and Accountability Act of 1996
HRS
Health and Retirement Study
HSA
Health Savings Account
IADLs
Instrumental Activities of Daily Living
IRA
Individual Retirement Account
LTC
Long-Term Care
LTCI
Long-Term Care Insurance

Long-Term Care Insurance: Recommendations for Improvement of Regulation vi
Acronym
Abbreviation
LTCI Model Act
NAIC Long-Term Care Insurance Model Act
LTCI Model Regulation
NAIC Long-Term Care Insurance Model Regulation
LTCSA
Long-Term Care Savings Account
LTSS
Long-Term Services and Supports
MA
Medicare Advantage
NAIC
National Association of Insurance Commissioners
NAIC 2017 List
Long-Term Care Federal Options Presented by the NAIC in April
2017
NHEA
National Health Expenditure Accounts
Partnership program
Partnerships for Long-Term Care Federal-State Program
SECURE Act
Setting Every Community Up for Retirement and Enhancement Act
of 2019
SOA
Society of Actuaries
SSA
U.S. Social Security Administration
Task Force
Federal Interagency Task Force on Long-Term Care Insurance
Treasury
U.S. Department of the Treasury

Long-Term Care Insurance: Recommendations for Improvement of Regulation 1
Executive Summary
Introduction
In July 2018, the U.S. Department of the Treasury (Treasury) convened a federal interagency
task force on long-term care insurance (Task Force) in response to recommendations in
Treasury’s October 2017 Report on Asset Management and Insurance (Insurance Report).
1
The
Insurance Report identified the challenges of financing long-term care (LTC) as a matter of
national interest requiring a coordinated response from the federal government, while affirming
the primary role of the U.S. states as insurance regulators in the United States. Accordingly, the
Insurance Report recommended that Treasury convene the Task Force to develop policies to
complement reforms at the state level relating to the regulation of long-term care insurance
(LTCI). The Insurance Report stated that the Task Force should coordinate its work with the
ongoing work of state insurance regulators and the National Association of Insurance
Commissioners (NAIC).
2
The Task Force consists of representatives from Treasury’s Office of Economic Policy
(including the Assistant Secretary for Economic Policy, who chairs the Task Force); other
Treasury offices (Tax Policy, Consumer Policy, and the Federal Insurance Office (FIO)); the
U.S. Department of Health and Human Services (HHS); the Centers for Medicare & Medicaid
Services (CMS); the U.S. Department of Labor (DOL); and the Office of Management and
Budget.
Since its inception in 2018, the Task Force has identified and analyzed proposed reforms to the
regulation of LTCI and consulted with a range of stakeholders. The Task Force concludes that
LTCI can play a role in providing financial protection against LTC risks and helping individuals
plan their financial future. To that end, this report describes the work conducted by the Task
Force and presents its recommendations to improve the regulation of LTCI in the United States.
In making these recommendations, the Task Force does not intend to either promote or
discourage LTCI over other solutions to the challenges of financing LTC. Implementation of the
recommendations will remove barriers to innovation and increase regulatory efficiency and
alignment, potentially making LTCI more affordable and accessible while allowing the market to
continue shaping the evolution of this product line.
1
U.S. Department of the Treasury, A Financial System That Creates Economic Opportunities: Asset Management
and Insurance (Treasury, October 2017), 163 [hereinafter Insurance Report], available at:
https://www.treasury.gov/press-center/press-releases/Documents/A-Financial-System-That-Creates-Economic-
Opportunities-Asset_Management-Insurance.pdf.
2
Treasury, Insurance Report, 144. The NAIC is the U.S. standard-setting and regulatory support organization
created and governed by the chief insurance regulators from the 50 states, District of Columbia, and five U.S.
territories.
Long-Term Care Insurance: Recommendations for Improvement of Regulation 2
Scope and Objectives of the Task Force
The Task Force determined that its primary objectives were to analyze, evaluate, and make
recommendations concerning:
• The LTC federal policy options presented to federal agencies and Congress by the NAIC
in April 2017 (NAIC 2017 List);
3
• Other potential new federal policies, or modifications of existing policies, to complement
state-based regulation of LTCI; and
• The manner and degree to which current laws and regulations appropriately recognize
and respond to newer product designs and features in the LTCI market.
In conducting its work, the Task Force focused on federal laws and regulations relating to the
private insurance market. The Task Force also examined certain state laws and regulations,
primarily those referenced in federal laws.
The Task Force substantially completed its analysis and recommendations prior to the onset of
the COVID-19 pandemic. The pandemic is likely to affect the provision of LTC and the market
for LTCI, but the full effects will continue to emerge over time.
4
For these reasons, this report
does not seek to assess the potential impacts of COVID-19 on LTC or LTCI.
Long-Term Care Insurance in the United States
The terms “long-term care” (LTC) and “long-term services and supports” (LTSS) cover a range
of services provided to people with long-term physical or cognitive limitations. The private
insurance industry typically uses LTC as a shorthand term, while academic and public policy
literature, as well as some governmental publications, typically use LTSS. With some
exceptions, this report generally adopts LTC.
5
Most LTC is not medical care, but rather assistance with the basic personal tasks of everyday
life, such as bathing, dressing, using the toilet, transferring (to or from bed or a chair), caring for
3
National Association of Insurance Commissioners, Long-Term Care Innovation (B) Subgroup: Federal Policy
Options to Present to Congress (Kansas City: NAIC, April 2017), 2, available at:
https://www.naic.org/documents/cmte_e_res_mech_wg_related_federal_policy_issues.pdf
.
4
Treasury will continue to monitor the effects of COVID-19 on insurance products and markets, including LTCI.
COVID-19 disproportionally affects older adults and individuals with chronic illnesses or other high-risk health
conditions, making the LTC population (particularly those in nursing homes or assisted living facilities) more
vulnerable to the virus than the general population. Relevant factors with respect to the pricing of LTCI include
mortality, policy lapses, the incidence of claims, utilization of benefits, and changes in interest rates. See Andrew
Dalton et al., “Pandemic Risk on LTC Insurance Reserves,” Milliman, April 2020, available at:
https://us.milliman.com/en/insight/pandemic-risk-on-ltc-insurance-reserves
.
5
The Role of Insurance in Long-Term Care and the Alternative Financing Approaches sections generally adopt
LTSS.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 3
incontinence, and eating.
6
Approximately half of Americans turning age 65 today will need
some type of LTC in their lives. The older a person is, the more likely it is that he or she will
need LTC at some point. The Congressional Budget Office (CBO) has projected that U.S.
spending on LTC for the elderly (age 65 and above) will increase from 1% of gross domestic
product in 2010 to 3% in 2050.
Based on data from the National Health Expenditure Accounts (NHEA), the Medicaid program
was the largest payer of LTSS expenses in 2018 (total payments of $159.1 billion), followed by
out-of-pocket spending by individuals ($55.0 billion). By contrast, based on industry data,
private LTCI paid $10.3 billion in claims in 2018.
Private insurers began offering LTCI in the 1970s in response to demand for financial protection
against the risk of having to enter a nursing home. Sales of new policies peaked in the early
2000s, but have since declined as numerous insurers decided to exit the market due to the poor
financial performance of the product line. The market remains in flux, with sales of traditional,
standalone LTCI continuing to drop while “combination” insurance products have become more
popular with consumers.
7
The role of the private insurance market in addressing the growing
need for LTC will largely depend on the four main subject areas examined in this report:
innovation in product design and delivery; the efficiency and effectiveness of regulation;
education and awareness with respect to LTC needs and planning; and federal income tax
treatment of LTCI.
Review of the Process for this Report
For this report, the Task Force consulted with a wide range of stakeholders, including consumer
and other advocacy groups, trade groups, insurance companies and insurance product
distributors, actuaries, academics, legal experts, state insurance regulators, the NAIC, and other
stakeholders with relevant knowledge. See Appendix A for a list of organizations and individuals
providing input to the Task Force. The Task Force also reviewed data, research, and
publications from both public and private sector sources.
On July 25, 2019, the Task Force held a public meeting at Treasury to obtain additional input for
this report. Topics discussed at the meeting included the social need for LTC; the individual
private LTCI market; employer, group, and worksite LTCI products; state regulation of LTCI;
the federal government and LTCI; and federal-state partnerships and other financing approaches.
6
“Long-Term Care – The Basics – What is Long-Term Care?” LongTermCare.gov, U.S. Department of Health and
Human Services, last modified October 2017, available at:
https://longtermcare.acl.gov/the-basics/what-is-long-
term-care.html.
7
In this report, “traditional” or “stand-alone” LTCI refers to policies that provide only LTCI coverage, as
distinguished from “combination” policies or other product designs that combine LTCI with other coverages, such
as life insurance or an annuity.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 4
Through a posting on Treasury’s website and an announcement at the public meeting, the Task
Force offered the public an opportunity to provide written comments. The Task Force received
comments from a total of 16 consumers and consumer advocacy groups, actuarial organizations,
and industry experts and consultants.
8
This report addresses several recommendations from the
comments, and incorporates certain data and other information provided by commenters.
Summary of Analysis and Recommendations
The Task Force organized its analysis and recommendations into four subject areas:
• Innovation and Product Development – product development and other innovation in
the private market, including policies that combine LTCI with other types of insurance
products or product features offering alternatives to traditional, stand-alone LTCI.
• Regulatory Efficiency and Alignment – improvements in regulatory efficiency and
alignment with respect to LTCI, including inflation protection requirements, harmony
between federal and state laws and regulations, and cross-state subsidization and other
issues relating to state regulatory review and approval of premium increases.
• Financial Literacy and Education – the appropriate federal role in financial literacy and
education relating to LTC needs and LTCI.
• Tax Incentives – current tax law treatment of LTCI and proposals to provide additional
tax incentives for the purchase and use of LTCI.
Although public programs providing LTC benefits were not in scope for specific
recommendations, the Task Force also reviewed several proposed public insurance options as
described in the Alternative Financing Approaches section of this report.
Appendix B presents the analysis and recommendations of the Task Force and identifies the
policymakers and other stakeholders the Task Force considers well positioned to implement each
recommendation. Following publication of this report, Treasury will continue to monitor
implementation of the recommendations.
Innovation and Product Development
In response to the decline in the market for traditional LTCI, insurers have introduced alternative
product designs and new features to both increase the consumer appeal of LTCI and improve the
financial returns on LTCI for insurers. These designs and features include combination products,
limited LTCI, group products, and incidental benefits.
Innovation and product development have the potential to significantly strengthen the private
LTCI market and better address the LTC needs of consumers. Accordingly, the Task Force
8
See “Public Comments Received by the Task Force,” U.S. Department of the Treasury, August 2019, available at:
https://home.treasury.gov/system/files/226/Public-Comments-Received-by-the-Task-Force.pdf
.
Long-Term Care Insurance: Recommendations for Improvement of Regulation 5
recommends that federal and state policymakers foster a regulatory environment that encourages
flexibility, experimentation, and innovation in product design to improve consumer choice and
access to benefits, while appropriately protecting the rights of consumers and the solvency of
insurers.
Combination Products
Insurers have introduced a variety of products that combine LTCI with different types of
insurance, primarily life insurance and annuities. These combination products offer potential
advantages to consumers and insurance distributors, but also present challenges for these groups
due to their complexity and the wide range of combinations available. Although claims
experience on these relatively new products is limited, companies report that the incidence of
claims and other actuarial results to date have been positive.
Policymakers could benefit from analysis of the impact of combination products on the market
for LTCI risk protection. The Task Force recommends that actuaries, academics, and other
stakeholders explore such an analysis, with coordination by FIO.
Limited LTCI Products
Compared to traditional LTCI, “short” or “limited” LTCI policies (i.e., policies that pay benefits
for less than 12 months) generally have lower benefits, but also typically have no deductible or
waiting period, as well as less stringent underwriting and lower premiums. Because limited
LTCI emerged later than traditional LTCI, regulation of this market is less mature than the
traditional market. In late 2018, the NAIC adopted a model act and model regulation for this
product. However, the states generally have not yet adopted either model.
The Task Force recommends that federal policymakers work with their state counterparts and
with private sector stakeholders to evaluate and monitor the market for limited LTCI, including
potential impacts on the risk pool for longer-term products and on Medicaid. The Task Force
further recommends that state legislators and insurance regulators take steps to better streamline
and standardize the regulation of this market.
Group Products
The Task Force considered two policy proposals for LTCI group products that were included
under the NAIC 2017 List, both involving the fiduciary provisions of the Employee Retirement
Income Security Act of 1974 (ERISA). The first proposal is to create a safe harbor to remove
potential exposure to ERISA fiduciary liability as a factor in employers’ decisions not to offer
LTCI to employees. The second proposal is to permit 401(k) and individual retirement account
(IRA) participants to purchase LTCI within their accounts. The objective of both proposals is to
promote a more viable group LTCI market by increasing employee participation, resulting in a
larger and more favorable risk pool for insurers and, potentially, lower premiums.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 6
Based on stakeholder input and an assessment of the market and legal landscapes for the
employer market, the Task Force does not recommend either option because it is uncertain
whether either proposal would have a meaningful impact on participation levels.
Incidental Benefits
Under most LTCI policies, the insured is not eligible to submit a claim for benefits until he or
she becomes “chronically ill” as defined under state insurance laws and the Internal Revenue
Code (Code). Some stakeholders proposed that Congress should amend the Code to permit
payment of incidental benefits (such as home assessments to identify safety hazards, home
modifications, or caregiver training for family members) from a LTCI policy prior to the onset of
chronic illness, without causing the policy to forfeit its tax-qualified status.
Supporting the ability of those needing LTC to remain in their homes could benefit both
consumers and insurers. Accordingly, the Task Force encourages industry, federal
policymakers, and other experts, in consultation with consumer representatives, to identify and
assess research-based evidence of cost-effective interventions. If cost-effective incidental
benefits are identified, Congress could consider amending the Code to permit payment of those
benefits under a tax-qualified LTCI contract prior to the insured becoming chronically ill, subject
to a monetary cap and other conditions set by regulation.
Regulatory Efficiency and Alignment
The Task Force considered various recommendations to improve the efficiency and effectiveness
of regulation of LTCI at the federal and state levels, including federal policies identified in the
NAIC 2017 List.
Inflation Protection Under the Health Insurance Portability and Accountability Act of 1996
(HIPAA)
Because LTCI policies often remain in force for many years, purchasers of LTCI face a
significant risk that inflation will erode the value of their benefits over time. Under current state
laws and regulations, insurers must offer policyholders the right to purchase a policy feature that
increases benefits at an annual compounded rate not less than 5%. In 2006, when it codified
requirements for tax-qualified LTCI as part of HIPAA, Congress incorporated the 5% compound
standard through reference to the 1993 version of the NAIC Long-Term Care Insurance Model
Regulation (LTCI Model Regulation).
9
The NAIC and Congress based the 5% compound inflation standard on inflation rates that
prevailed in the 1980s and 1990s. Since then, particularly following the financial crisis, this
standard has become a costly feature that increases premiums to levels most consumers will not
9
HIPAA amended the Code to add Section 7702B, which sets forth the requirements for a “qualified long-term care
insurance contract.” See 26 U.S.C. § 7702B(a)(1).

Long-Term Care Insurance: Recommendations for Improvement of Regulation 7
accept. The Task Force concludes that inflation protection requirements under HIPAA and state
insurance laws should be revised to increase the efficiency and effectiveness of regulation.
To both address outdated inflation protection requirements and provide flexibility to adapt
inflation protection to evolving economic conditions, the Task Force recommends that Congress
amend the Code to authorize Treasury to set inflation protections for tax-qualified LTCI.
Inflation Protection Under the DRA
In the early 1990s, four states (California, Connecticut, Indiana, and New York) implemented a
federal-state program known as “Partnerships for Long-Term Care” (Partnership program). As
part of the Deficit Reduction Act of 2005 (the DRA), Congress extended the Partnership
program nationwide, subject to specified conditions including inflation protection and other
consumer protections.
10
The states have adopted widely varying inflation protection
requirements for LTCI policies under the Partnership program, resulting in a regulatory
patchwork with uneven consumer protections and additional complexity that makes it more
difficult to write LTCI. Additionally, high inflation protection mandates in some states may
raise the costs and reduce the attractiveness of Partnership policies.
The Task Force recommends that state policymakers—legislators, state Medicaid directors,
insurance commissioners, and the NAIC—improve regulatory efficiency and effectiveness by
harmonizing and streamlining inflation protection requirements under the Partnership program.
Alternatively, Congress should consider delegating to HHS the authority to set Partnership
program inflation protection requirements.
Other Consumer Protections
Apart from inflation protection, both HIPAA and the DRA mandate compliance with certain
consumer protections contained in the NAIC Long-Term Care Insurance Model Act (LTCI
Model Act) and the LTCI Model Regulation. However, the DRA defines “model regulation”
and “model Act” by reference to the NAIC models adopted as of October 2000, while HIPAA
defines these terms by reference to the January 1993 versions. This cross-referencing in two
federal statutes of two outdated and conflicting versions of NAIC models creates confusion and
adds complexity to conducting LTCI business.
The Task Force recommends that Congress consider options to address this regulatory
inefficiency. For example, as one option, Congress could consider giving Treasury the authority,
in consultation with HHS, to set consumer protection standards using one version of the LTCI
Model Act and LTCI Model Regulation for purposes of both tax qualification under HIPAA and
Partnership eligibility under the DRA, with flexibility to update the standards periodically (e.g.,
every 10 years).
10
See 42 U.S.C. § 1396p.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 8
Review and Approval of Rate Increases
The authority of state insurance regulators to review and approve proposed rate increases for
LTCI before the insurer implements those changes is a critical factor in the LTCI marketplace.
Due to the non-uniform nature of the state-by-state rate increase process, policyholders in states
where regulators have approved rate increases may subsidize the cost of premiums for
policyholders in other states where regulators have either approved limited increases or rejected
rate increases in their entirety.
In 2019, the NAIC identified the regulation of LTCI as the organization’s top priority. The Task
Force recommends that the NAIC and the states maintain their focus on LTCI and continue
working together in 2020 to develop a consistent national approach to regulatory reviews of
LTCI rate increase requests. The Task Force also recommends that FIO continue to monitor and
report on this issue.
Financial Literacy and Education
The NAIC 2017 List included a federal education program around retirement security and the
importance of planning for potential LTC needs. In 2019, Treasury released a report (Financial
Literacy Report), laying out an appropriate federal role for financial education based on a
literature review and consultations with experts and stakeholders inside and outside of the
government.
11
In the Financial Literacy Report, Treasury recommended that the primary federal
role in this area should be to empower financial education providers, as opposed to attempting to
reach every American household directly.
The Task Force recommends that Treasury, HHS, DOL, and other agencies, working through the
Financial Literacy Education Commission (FLEC), assess federal education resources on LTC
needs and planning, and modify, update, and supplement these resources as needed.
Tax Incentives
The NAIC 2017 List included consideration of more generous tax incentives for the purchase of
LTCI. Multiple stakeholders encouraged the Task Force to consider a range of amendments to
tax laws or regulations aimed at increasing the take-up of private LTCI. The Task Force
analyzed several potential new tax incentives and other potential tax reforms.
In its analysis, the Task Force took into account that the Code already provides favorable income
tax treatment to LTCI. The Task Force concludes that the proposed incentives, in general, would
reduce tax revenues and primarily benefit higher-income taxpayers, and may not be fully
effective in targeting lower and middle-income individuals who need financial protection against
LTC risks. Finally, the proposals would increase the complexity of the Code and could, in some
11
U.S. Department of the Treasury, Federal Financial Literacy Reform: Coordinating and Improving Financial
Literacy Efforts (Treasury, July 2019) [hereinafter Financial Literacy Report], available at:
https://home.treasury.gov/system/files/136/FFLRCoordinatingImprovingFinancialLiteracyEfforts.pdf
.
Long-Term Care Insurance: Recommendations for Improvement of Regulation 9
cases, be difficult to implement, monitor, and enforce. For these reasons, the Task Force does
not recommend adoption of any of the proposed additional tax incentives, with the exception of
the proposal to eliminate the additional tax on early withdrawal of funds from an IRA, 401(k), or
403(b) account that are used to pay LTCI premiums.
Alternative Financing Approaches
Experts and policymakers have proposed a range of alternative approaches to the financing of
LTC, including public programs administered by the federal and state governments. Most of
these approaches have focused on either front-end insurance (providing limited coverage for
short, initial durations) or back-end or catastrophic insurance (coverage for longer durations
beyond a specified level of need or cost). The Task Force does not recommend pursuing any
particular alternative financing approach at this time. Policymakers and stakeholders should
continue to develop, monitor, and analyze LTC and LTCI reform proposals—including those
discussed in this report—to better understand the advantages and disadvantages of specific
options, tradeoffs, program costs, and distributional impacts.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 10
The Role of Insurance in Long-Term Care
As the elderly population continues to grow in both size and as a percentage of the overall
population, the need for LTSS becomes increasingly important for social welfare. This section
discusses the prevalence of need, projected future demand, and financing of LTSS, including the
roles of public programs and the private LTCI market. The section concludes with an overview
of supply and demand factors impeding the private market.
Prevalence of Need for LTSS
The terms “long-term care” or “long-term services and supports” encompass a wide variety of
services provided to individuals with long-term physical or cognitive limitations who need help
with certain daily activities. These activities include “activities of daily living” (ADLs) and
“instrumental activities of daily living” (IADLs).
HIPAA defines ADLs as six basic activities:
12
• Eating
• Toileting
• Transferring
• Bathing
• Dressing
• Continence
The IADLs include activities necessary for independent life such as paying bills and managing
money, medication management, meal preparation, shopping, and using the telephone.
LTSS, therefore, include services such as direct physical assistance with ADLs, meal provision,
housekeeping services, and transportation services, as well as medical services. These services
and supports can be provided in individuals’ homes or in institutional settings such as assisted
living facilities or nursing homes. Individuals’ needs for LTSS vary widely, ranging from round-
the-clock assistance with all six ADLs to assistance with one or two IADLs.
Table 1 provides summary statistics on the prevalence of difficulty with at least one IADL, the
prevalence of needing assistance with two or more ADLs, and the use of home health care in
approximately the previous two years among individuals age 60 and above in the Health and
Retirement Study (HRS) during 2016.
13
The prevalence of difficulty with IADLs and the need
12
26 U.S.C. § 7702B(c)(2)(B).
13
The HRS is conducted every two years and follows individuals over time, with new respondents added each round
to replace deceased respondents. Questions about medical utilization focus mainly on utilization since the previous

Long-Term Care Insurance: Recommendations for Improvement of Regulation 11
for assistance with ADLs rise sharply in both sexes above age 75. The share using home health
care in the previous two years rises in parallel with the need for assistance with daily activities.
Women above age 85 have the highest need for LTSS; around half in this group report having
difficulty with at least one IADL, and nearly a quarter need assistance with two or more ADLs.
A lower share (17%) used home health care in the past two years.
Table 1: Prevalence of Serious Disability and Use of Long-Term Services and
Supports Among Those Age 60 and Over
Share Having
Difficulty with at Least
One IADL (%)
Share Needing Help
with Two or More of
Five ADLs (%)
Share with Home
Health Care Use in
Past Two Years (%)
Whole
Sample
16 5 3
Female
60-69 11 3 0
70-84
18
5
3
85+ 50 24 17
Male
60-69
9
2
1
70-84 15 3 2
85+
39
16
10
Notes: The sample consists of respondents in the 2016 HRS age 60+. The sample size is 13,153. All means
are weighted using sample weights for the 2016 wave. For purposes of the HRS, IADLs include preparing
hot meals, shopping for groceries, using the telephone, managing medications, and managing money. ADLs
include dressing, bathing, eating, transferring into or out of a bed or chair, and using the toilet.
Table 2 shows statistics on nursing home use and estimated spending on stays in excess of 90
days in the previous two years among HRS respondents age 60 and over.
14
The table focuses on
stays longer than 90 days to illustrate exposure to financial risk for stays not covered by
insurance (private LTCI plans generally have an exclusion period of 90 days). As Table 2
shows, spending on nursing homes is estimated to be only about $2,900 on average over two
years across those age 60 and over. However, this average figure encompasses a wide range of
interview (approximately two years earlier) for continuing respondents and in the last two years for new
respondents. For more information about the HRS, see “The Health and Retirement Study – About,” available at:
https://hrs.isr.umich.edu/about
.
14
Because the HRS tracks only the total number of nights in a nursing home in the past two years, not whether any
particular stay is longer than 90 days, the table may slightly overstate the risk of long-term stays. The HRS assumes
$225 in spending for one night in a nursing home based on the average cost according to HHS. See
“LongTermCare.gov – Costs of Care,” available at:
https://longtermcare.acl.gov/costs-how-to-pay/costs-of-
care.html.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 12
spending. Among these individuals, the risk of having a long nursing home stay is low, but the
average cost of a long-term stay is approximately $112,000.
Table 2: Spending on Stays of More Than 90 Nights in a Nursing Home
Mean Number of
Nights in a Nursing
Home in Excess of
90 Nights in the
past Two Years
Estimated Mean
Spending on
Stays of More
Than 90 Nights
Across Whole
Sample ($)
Share with More
Than 90 Nights
in a Nursing
Home in past
Two Years (%)
Mean
Spending for
Those with
More Than 90
Nights ($)
Whole Sample
13
2,898
2.6
111,744
Female
60-69 2 407 0.3 136,629
70-84
11
2,545
2.7
94,150
85+ 105 23,651 18.8 125,957
Male
60-69
3
636
0.7
91,578
70-84 9 1,916 1.8 108,315
85+
51
11,584
11.4
102,047
Notes: The sample consists of respondents in the 2016 HRS age 60+. The sample size is 13,153. All means are
weighted using sample weights for the 2016 wave. Returning respondents were asked about nursing home
utilization since their previous interview approximately two years earlier; new respondents were asked about
utilization in the past two years.
Projections of Demand for LTSS
The share of the U.S. population who are elderly is expected to rise steadily throughout most of
the twenty-first century. In their 2019 report, the trustees for Social Security project that the
ratio of the number of people age 65 and over to the number of people age 15 through 64 (the
aged-dependency ratio) will rise from 0.268 in 2018 to 0.425 in 2075, an increase of nearly
60%.
15
Accordingly, the demand for LTSS is projected to rise in upcoming years. The CBO projected in
2013 that spending for LTSS for the elderly (age 65 and above) will rise from 1.3% of gross
domestic product in 2010 to 3% in 2050, if age- and sex-specific rates of impairment are held
15
Board of Trustees of the Federal Old-Age and Survivors Insurance and Federal Insurance Trust Fund, The 2019
Annual Report of the Board of Trustees of the Federal Old-Age and Survivors Insurance and Federal Disability
Insurance Trust Funds (Board of Trustees, April 2019), available at:
https://www.ssa.gov/OACT/TR/2019/tr2019.pdf
.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 13
constant over time and the increase is due solely to the aging of the population.
16
If increased
obesity results in higher age-specific impairment rates, spending for LTSS for the elderly will
rise to 3.3% of gross domestic product in 2050, according to the CBO. These estimates do not
include the value of informal care. The CBO also projected that the share of nonelderly adults
engaged in caregiving, either formally or informally, will increase from around 5% in 2010 to
10% in 2050, if impairment rates are held constant, and to 11% under the more pessimistic
scenario of increasing impairment rates.
Dementia, LTSS, and LTCI
Dementia is a general term for impairment in a person’s ability to remember, think, or make
decisions that interferes with performing everyday activities. Alzheimer’s disease is the most
common type of dementia. According to the Centers for Disease Control and Prevention (CDC),
5.8 million Americans have Alzheimer’s, and the number of individuals with dementia is
expected to triple over the next 40 years. Deaths from Alzheimer’s in the United States
increased by 145% from 2000 to 2017, making Alzheimer’s the sixth leading cause of death (and
the third leading cause when combined with other types of dementia). Part of the increase may
be due to a greater emphasis on reporting dementia and Alzheimer’s disease as a cause of death.
In any case, the burdens of dementia fall heavily on families and other caregivers—more than 16
million Americans provide unpaid care for people with Alzheimer’s or other dementias.
17
The CDC estimates that in 2016, the percentage of LTSS users diagnosed with Alzheimer’s
disease or other dementias was 41.9% for residential care community residents, 44.5% for
hospice patients, and 47.8% for nursing home residents.
18
Because a diagnosis of severe
cognitive impairment triggers coverage under most LTCI policies, many LTCI claims (roughly
half, according to some industry sources), are filed by policyholders with Alzheimer’s or other
dementias. Therefore, dementia already accounts for a large portion of LTCI claim payments.
While there is evidence that the prevalence of dementia is declining in the United States,
19
population aging is likely to increase demand for LTSS in the future, which may in turn increase
16
Congressional Budget Office, Rising Demand for Long-Term Services and Supports for Elderly People (CBO,
June 2013), available at: https://www.cbo.gov/publication/44363
.
17
See “Promoting Health for Older Adults,” Centers for Disease Control and Prevention, last modified September
2019, available at: https://www.cdc.gov/chronicdisease/resources/publications/factsheets/promoting-health-for-
older-adults.htm; “What Is Dementia?” Centers for Disease Control and Prevention, last modified April 2019,
available at: https://www.cdc.gov/aging/dementia/index.html; Alzheimer’s Association, 2019 Alzheimer’s Disease
Facts and Figures (Chicago: Alzheimer’s Association, 2019), 24-25, available at:
https://www.alz.org/media/Documents/alzheimers-facts-and-figures-2019-r.pdf; Ellen A. Kramarow and Betzaida
Tejada-Vera, “Dementia Mortality in the United States, 2000-2017,” National Vital Statistics Reports 68, no. 2
(March 2019), available at:
https://brainhealthinstitute.rutgers.edu/wp-content/uploads/2019/03/Dementia-
Report_March-2019.pdf; “Alzheimer's Disease and Healthy Aging,” Centers for Disease Control and Prevention,
last modified September 2019, available at: https://www.cdc.gov/aging/aginginfo/alzheimers.htm.
18
“National Center for Health Statistics: Alzheimer’s Disease,” Centers for Disease Control and Prevention, last
modified March 2016, available at: https://www.cdc.gov/nchs/fastats/alzheimers.htm
.
19
Kenneth M. Langa et al., “A Comparison of the Prevalence of Dementia in the United States in 2000 and 2012,”
JAMA Intern Med. 177, no. 1 (January 2017): 51-58, available at: https://www.ncbi.nlm.nih.gov/pubmed/27893041
.
Long-Term Care Insurance: Recommendations for Improvement of Regulation 14
demand for financial protection against LTSS risks. In addition, higher than expected claims,
together with other factors, have led many insurers to set aside more assets to cover future
liability and to increase premiums on both in-force and newly issued policies. Notwithstanding
these challenges, the social need for protection against the costs of LTSS for dementia is also a
major opportunity for insurers to develop new products and services to improve the quality of
life of a large and growing segment of the U.S. population.
Financing of LTSS
Payment Sources
Public financing of LTSS in the United States is provided largely through the Medicaid program.
To be eligible to receive LTSS through Medicaid, individuals generally must be 65 or over (or
found to be disabled by the Social Security Administration (SSA)), and must meet tests designed
to limit benefits to individuals with very low income and wealth. Because Medicaid is partly
financed by the states, eligibility and benefits vary, but rules follow broad federal guidelines.
Formulas for determining Medicaid eligibility are complex; in general, single individuals with
more than $2,000 in assets, other than their home and car, are not eligible.
20
All states must
cover nursing home care through Medicaid, and nearly all offer some level of home- and
community-based care through waivers provided by CMS.
21
Based on data from the NHEA, Medicaid was the largest payer of LTSS expenses in 2018 (total
payments of $159.1 billion), followed by out-of-pocket spending ($55.0 billion).
22
By contrast,
an industry association estimates that private LTCI paid $10.3 billion in claims in 2018.
23
20
Married couples with both spouses applying for nursing home coverage are allowed $3,000 in countable assets to
qualify for Medicaid. However, if only one spouse applies, the non-applicant is permitted to transfer a specified
amount of assets (from $25,728 to $128,640 in 2020) to the non-applicant spouse. See “2020 SSI and Spousal
Impoverishment Standards,” CMS, available at:
https://www.medicaid.gov/sites/default/files/2020-01/ssi-and-
spousal-impoverishment-standards_0.pdf. In addition, the value of the applicant’s primary home does not count
against the asset limit.
21
Section 915(c) of the Social Security Act, 42 U.S.C. §1396n, establishes standards for these waivers.
22
Amounts provided by CMS Office of the Actuary. For information about the NHEA, see “National Health
Expenditure Data: Historical,” CMS, available at:
https://www.cms.gov/Research-Statistics-Data-and-
Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NationalHealthAccountsHistorical. Although
the NHEA tracks Medicare spending, that program only covers home health and skilled nursing care for a relatively
short period (100 days) following an acute episode such as surgery. Out-of-pocket expenses are likely understated
in the NHEA because it does not include payments to independent home health care providers. One study using the
National Long-Term Care Survey suggests that nearly half of LTSS (as measured by hours of care) are paid for out
of pocket. John Ermisch and Alexander L. Janus, “Who pays for home care? A study of nationally representative
data on disabled older Americans,” BMC Health Services Research 15, no. 301 (July 2015), available at:
https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-015-0978-x.
23
“Long-Term Care Insurance Industry Paid $10.3 Billion in Claims in 2018,” American Association for Long-
Term Care Insurance, last modified January 2019, available at:
https://www.aaltci.org/news/long-term-care-
insurance-association-news/long-term-care-insurance-industry-paid-10-3-billion-in-claims-in-2018.
Long-Term Care Insurance: Recommendations for Improvement of Regulation 15
The Value of Informal Care
Notably, statistics on LTSS spending omit the value of informal (and unpaid) care. Estimates of
the value of this care range widely depending on the value attributed to the unpaid hours from
caregivers. A 2013 study estimated that the total value of informal care for those age 65 and
over in 2011 was $234 billion, while a 2015 study estimated that value to be $522 billion for the
same year.
24
The difference between the two analyses rested largely on whether to value the
caregivers’ hours at the wage of a home health aide or at the actual or imputed wage of the
caregiver, which gives a higher value for their time in most cases.
A later study, in 2018, noted that the method used by the 2013 and 2015 analyses to estimate the
value of informal care does not take into account the effects on caregivers from future foregone
wages from leaving employment, the value of foregone leisure time, or intrinsic benefits to
caregivers from caregiving.
25
Using methods designed to account for these other costs and
benefits, the 2018 study found that the value of informal care in 2011 was $277 billion. In all
three of these studies, the estimated total value of informal care in 2011 exceeded formal
spending on LTSS for the elderly (age 65 and above) in that year, which the CBO estimated to
be $192 billion.
Private LTCI
Since the 1970s, private insurers have offered LTCI to protect against the financial risk of high
LTSS expenditures. Unlike short-term medical insurance or publicly-funded Medicaid, the
structure of LTCI relies on the pre-funding of benefits. Typically, purchasers buy LTCI at
relatively younger ages, in their 50s or 60s, and then hold the insurance while paying premiums
for a lengthy period, often over twenty years.
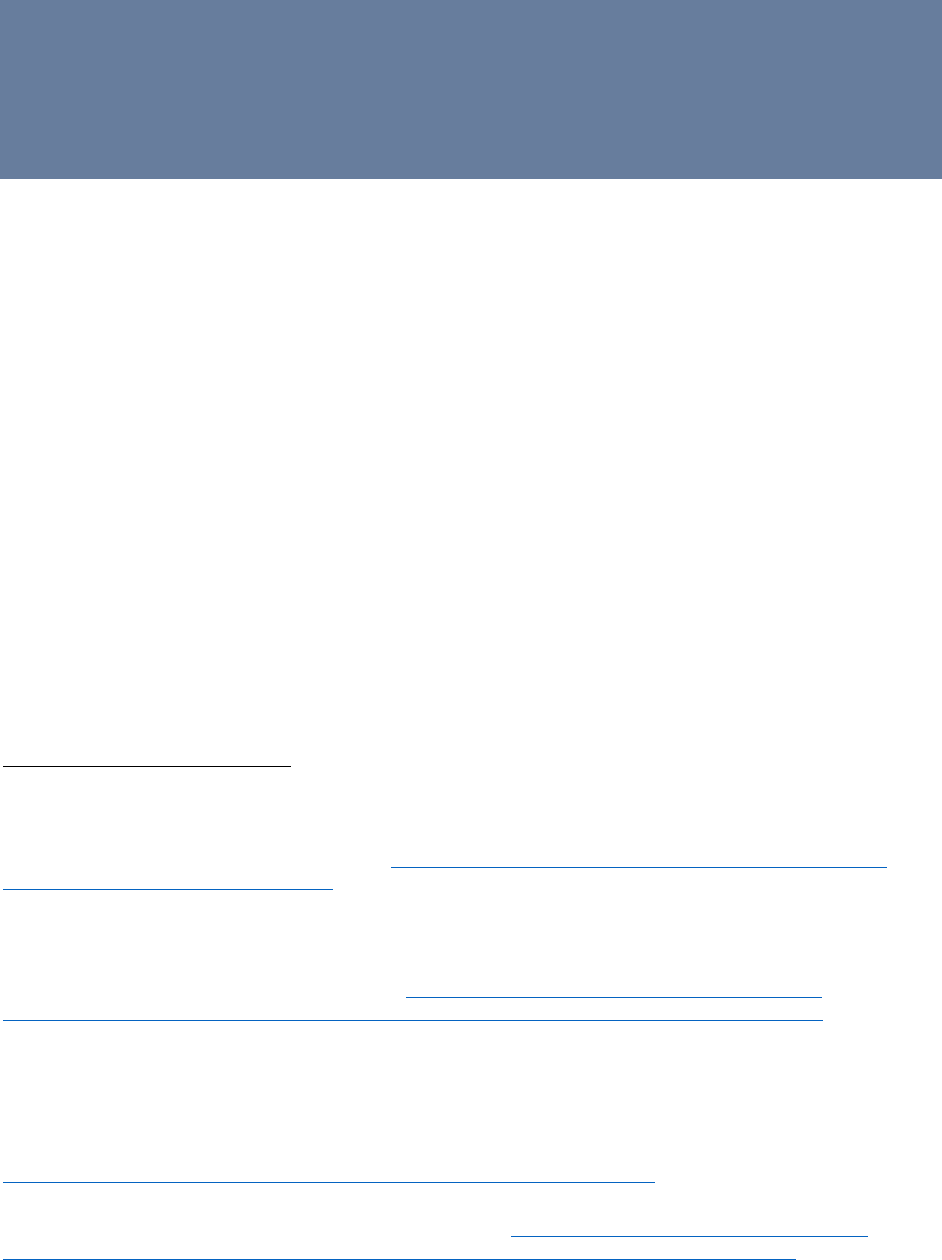
The private market for traditional individual LTCI is in steep decline. After rising from 380,000
in 1990 to a peak of 754,000 in 2002, the number of individual LTCI policies sold declined to
129,000 by 2014.
26
As shown in Figure 1, based on sales reports from the LIMRA
organization,
27
this downward trend accelerated over the five-year period from 2014 to 2018, as
24
CBO, Rising Demand, 2; Amalavoyal V. Chari et al., “The Opportunity Costs of Informal Elder‐Care in the
United States: New Estimates from the American Time Use Survey,” Health Services Research 50, no. 3 (June
2015): 871-882, available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4450934/
.
25
Norma B. Coe, Eric B. Larson, and Meghan M. Skira, “A Comprehensive Measure of the Costs of Caring for a
Parent: Differences According to Functional Status,” Journal of the American Geriatrics Society 66, no. 10
(September 2018): 2003-2008, available at: https://onlinelibrary.wiley.com/doi/full/10.1111/jgs.15552
.
26
Marc A. Cohen, “The State of the Long-Term Care Insurance Market,” in The State of Long-Term Care
Insurance: The Market, Challenges and Future Innovations, ed. by Eric C. Nordman (Kansas City: NAIC and the
Center for Insurance Policy and Research, May 2016), 7-29, available at:
https://www.naic.org/documents/cipr_current_study_160519_ltc_insurance.pdf
.
27
LIMRA is a worldwide research, consulting, and professional development trade association focused on the life
insurance industry. It is a recognized source for product data and other metrics in the U.S. life insurance, annuity,
and LTCI markets.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 16
the industry sold only 67,000 individual policies in 2017 and 57,000 in 2018.
28
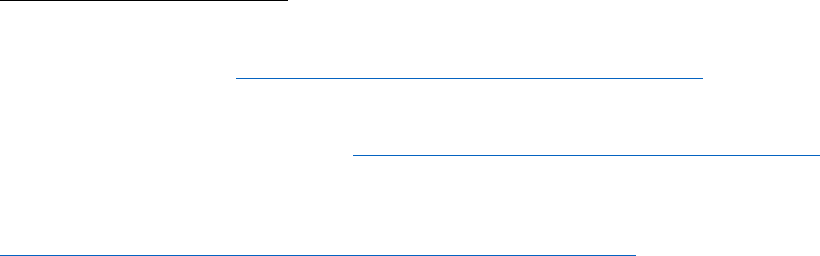
In addition, as
shown in Figure 2, individual new annualized premiums fell to record lows, below $200 million,
in 2017 and 2018. Meanwhile, Figure 3 shows that the level of combined premiums paid by in-
force policyholders has increased only modestly in recent years. Lower sales have occurred even
as the share of the population in the age group most likely to purchase private LTCI, those age
60 to 69, rose from 9.5% in 2010 to 11.4% in 2018, based on Census population estimates.
28
The market for employer-sponsored group LTCI has fallen even more precipitously, with annual new lives
insured reaching 140,000 in 2012 before declining to 22,000 by 2015. Currently, only one carrier continues to offer
employer-sponsored group LTCI. This discussion does not include LTCI products offered to employees through
employers at the worksite.
0
50,000
100,000
150,000
200,000
250,000
New Lives
Figure 1: Individual LTCI New Lives
Source: LIMRA.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 17
Table 3 shows ownership rates of private LTCI in the 2016 HRS for respondents age 60 and
above, by gender, marital status, age, and wealth quintile. Overall, 11.4% of those age 60 and
over own a private LTCI policy. Men own policies at a slightly higher rate than women, and
married people are more likely to own a policy than are unmarried individuals. Ownership rates
0
200
400
600
800
1,000
1,200
$ Millions
Figure 2: Individual LTCI Annualized Premiums
Source: LIMRA
.
0
2,000
4,000
6,000
8,000
10,000
12,000
$ Millions
Figure 3: Individual LTCI Premiums in Force
Source: LIMRA.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 18
rise by wealth quintile, with around one-fifth of the top quintile having bought policies compared
to only 6-7% of the bottom two quintiles. Ownership rates also rise with age, up to age 85.
Additionally, Table 3 updates a 2011 study that reported the same statistics for respondents in the
2008 HRS.
29
Compared with 2008, overall ownership rates declined slightly by 2016, from
13.8% in 2008 to 11.4%. The declines from 2008 to 2016 were driven by those age 60 to 69, the
group most likely to purchase new LTCI; ownership rates among those age 70 and over rose
between 2008 and 2016. This finding is consistent with reports from the industry, as shown in
Figures 1-3, that sales are in sharp decline and the number of in-force policies has plateaued.
In summary, older individuals are exposed to financial risk from the consequences of serious
disability. This exposure may be increasing over time, as sales of new policies decline and the
age 60 to 69 cohort appear to be less likely to purchase LTCI than previous cohorts. The
eligibility requirements for Medicaid and the limited and declining purchasing of private LTCI
imply that a large proportion of LTC costs are paid for out-of-pocket by individuals not covered
by Medicaid.
Table 3: Private Long-Term Care Insurance Ownership Rates Among the Elderly
Percentage by Wealth Quintile
Whole Sample
Top
Fourth
Third
Second
Bottom
Whole Sample
11.4 21.8 12.7 9.8 6.5 6.1
By Gender
Men
12.0
23.6
13.4
10.8
6.6
6.7
Women
10.8
20.0
12.0
8.7
6.5
5.3
By Marital Status
Married
12.7 21.8 12.8 9.3 7.3 6.1
Single
9.5 22.0 12.6 10.6 5.7 6.1
By Age Cohort
60-64
9.9
18.4
11.6
7.4
5.5
5.4
65-69
13.3
22.9
13.2
10.3
8.1
8.0
70-74
15.1 27.5 12.9 14.5 8.3 5.6
75-79
17.2 29.2 20.9 16.4 7.4 6.4
80-84
18.9 31.3 17.5 18.6 12.3 12.4
85+
16.0
30.2
21.3
10.1
9.0
8.3
Notes: The sample consists of respondents in the 2016 HRS age 60+. The sample size is 13,271. All means are
weighted using sample weights for the 2016 wave. Wealth is defined as total non-housing wealth.
29
Jeffrey R. Brown and Amy Finkelstein, “Insuring Long-Term Care in the United States,” Journal of Economic
Perspectives 25, no. 4 (Fall 2011): 119-42, available at: https://www.aeaweb.org/articles?id=10.1257/jep.25.4.119
.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 19
Factors Impeding the Market for Private LTCI
The utilization statistics in Table 2 show that individuals over age 60 face a risk of having to stay
a greater number of nights in nursing homes, thereby incurring significant expenses.
Furthermore, nursing homes represent only a part of spending on LTSS; as Table 1 shows, a
small but significant share of individuals also use paid home health care or require assistance
with two or more ADLs.
Standard economic models suggest that in the presence of potentially severe financial risk,
individuals should be willing to pay to insure themselves against that risk. However, private
LTCI appears to be underutilized relative to the potential demand and relative to the market for
short-term medical insurance. Factors impeding the development of the market can largely be
divided into the supply side and the demand side.
Supply-Side Factors
• Asymmetric information and adverse selection. Like other insurers, LTC insurers face
the challenge of managing their risk pool when individuals purchasing insurance know
more about their own risks than the insurer. This asymmetry of information between
seller and buyer likely leads to buyers purchasing insurance only when they believe the
benefits they will receive outweigh the premiums they will pay. This tilts the market
towards buyers with higher average costs, driving up premiums and further limiting the
pool of potential buyers.
o Underwriting. LTC insurers manage adverse selection with medical underwriting,
i.e., the practice of assessing applicants for policies for medical issues likely to result
in future use of LTSS. A 2016 study found that between 2000 and 2009,
underwriting standards tightened and the share of applications rejected for failing
underwriting rose.
30
Another 2016 study found that 20-25% of applicants for private
LTCI are ultimately rejected on medical grounds.
31
More recent data suggests that
firms may be starting to relax underwriting standards by reducing requirements for
medical testing in the past few years.
32
• Moral hazard. Beneficiaries of insurance incur a lower cost for services covered by
insurance and, as a result, may use those services more than they would if they did not
have insurance--a phenomenon is known as “moral hazard.” A 2019 study found
evidence of significant moral hazard in the use of home care (and, potentially, nursing
30
LifePlans, Inc., “Tolerating Risk: A Look at LTC Underwriting Strategies,” Behind the Data, January 2011.
31
Portia Y. Cornell et al., “Medical Underwriting in Long-Term Care Insurance: Market Conditions Limit Options
for Higher-Risk Consumers,” Health Affairs 35, no. 8 (August 2016): 1494-1503, available at:
https://www.healthaffairs.org/doi/10.1377/hlthaff.2015.1133
.
32
Chris Giese, Allen Schmitz, and Claude Thau, “2019 Milliman Long-Term Care Insurance Survey,” Broker World
Magazine, July 2019, available at: https://brokerworldmag.com/2019-milliman-long-term-care-insurance-survey/
.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 20
homes) among owners of private LTCI.
33
Another study, which surveyed private LTCI
claimants, found that the majority reported they would have used less paid care if they
had not had insurance.
34
Insurers must take moral hazard into account when pricing
plans, which may raise premiums above what some purchasers are willing to pay.
The issues of adverse selection and moral hazard are common to all insurance markets and not
unique to private LTCI. Other insurance markets, however, have features that address adverse
selection, such as a mandate for the purchase of insurance or a subsidy, both of which have the
effect of improving the risk pool. For example, automobile owners in all states are required to
purchase liability insurance, and employers usually subsidize health insurance they offer to
employees.
In addition, management of these supply-side factors can impose significant administrative costs
on private LTCI, resulting in low comprehensiveness (share of LTSS spending paid for by
private LTCI) and high “loads,” which is a measure of the difference between the expected
present discounted value (EPDV) of future benefits received and the EPDV of future premiums
paid over the life of the policy.
Demand-Side Factors
• Use of substitutes for private LTCI
o Medicaid. As discussed above, Medicaid covers LTSS for individuals with very low
income and assets. Therefore, Medicaid pays for some services that would be
covered by private LTCI, which reduces the incentive to purchase private LTCI.
According to studies conducted by the same authors in 2008 and 2011, for the lower
60% of the wealth distribution, it is rational not to purchase actuarially fair private
LTCI because of the availability of Medicaid.
35
For example, for a 65-year-old
woman at the median of the wealth distribution, 75% of the EPDV of the benefits of a
private LTCI policy would be paid for by Medicaid in the absence of the policy,
significantly reducing the policy’s net financial benefit. Other papers have
maintained that, in practice, the effect of Medicaid may not be as pronounced. A
2018 paper modeled the effects on private LTCI purchase, savings, and nursing home
33
R. Tamara Konetzka et al., “Moral Hazard and Long-Term Care Insurance,” The Geneva Papers on Risk and
Insurance: Issues and Practice 44, no. 2 (April 2019): 231-251, available at:
https://link.springer.com/article/10.1057%2Fs41288-018-00119-1
.
34
Marc A. Cohen, Jessica S. Miller, and Xiaomei Shi, “Following an Admissions Cohort: Care Management, Claim
Experience and Transitions among an Admissions Cohort of Privately Insured Disabled Elders over a 16 Month
Period,” Office of the Assistant Secretary for Planning and Evaluation, May 2007, available at:
https://aspe.hhs.gov/system/files/pdf/75086/16moclm.pdf
.
35
Jeffrey Brown and Amy Finkelstein, “The Interaction of Public and Private Insurance: Medicaid and the Long-
Term Care Insurance Market,” American Economic Review 98, no. 3 (June 2008): 1083-1102, available at:
https://www.aeaweb.org/articles?id=10.1257/aer.98.3.1083; Brown and Finkelstein, “Insuring Long-Term Care,”
119-42.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 21
entry by single elderly women if Medicaid is assumed to be unavailable. The study
found that the main effects were increased savings and reduced nursing home entry,
with only a small increase in private LTCI purchase.
36
o Unpaid care. As discussed earlier in this section of the report, the aggregate value of
unpaid care is likely higher than the value of paid care. A 2015 study found that the
presence of LTCI coverage leads to reduced reliance on informal care, fewer children
residing with parents, and a greater likelihood that children will be in the formal labor
force.
37
These results suggest that the ability to receive informal care from family
results in lower demand for private LTCI. Similarly, a 2012 survey found that
respondents who reported receiving care from family were less likely to buy private
LTCI.
38
• Bequest motives. Some sellers of private LTCI present the preservation of assets for
heirs as a reason to purchase the product. A 2018 study, however, suggested that a desire
to leave assets to heirs can suppress demand for private insurance because these motives
reduce the negative consequences of postponing consumption in order to save.
39
• Lack of information and awareness. Two surveys, one published in 2012 and the other
in 2015, have studied individuals’ awareness of LTC needs and financing.
40
In general,
respondents exhibited low knowledge of LTC costs, ways to finance those costs, and
private LTCI. For example, the 2015 survey found that only 20% of respondents
correctly estimated the average cost of a month in a nursing home and only 25% correctly
identified Medicaid as the government program that pays the most for LTSS. In the 2012
survey, 72% of respondents reported they knew only “a little” about private LTCI, while
29% believed incorrectly that Medicare covered LTSS.
• Lack of trust in insurers. The same surveys assessed respondents’ level of trust in LTC
insurers as low. In the 2015 survey, 32% of respondents agreed with the statement “I do
not trust private insurers.” In the 2012 survey, 46% of respondents agreed with the
statement “I am concerned that an insurance company might deny reasonable claims for
36
Geena Kim, “Medicaid Crowd-Out of Long-Term Care Insurance with Endogenous Medicaid
Enrollment,” Journal of Human Capital 12, no. 3 (Fall 2018): 431-474, available at: https://doi.org/10.1086/698134
.
37
Norma B. Coe, Gopi Shah Goda, and Courtney Harold Van Houtven, “Family Spillovers of Long-Term Care
Insurance,” National Bureau of Economic Research, Working Paper no. w21483 (August 2015), available at:
https://www.nber.org/papers/w21483
.
38
Jeffrey R. Brown, Gopi Shah Goda, and Kathleen McGarry, “Long-Term Care Insurance Demand Limited by
Beliefs about Needs, Concerns about Insurers, and Care Available from Family,” Health Affairs 31, no. 6 (June
2012): 1294-1302, available at: https://doi.org/10.1377/hlthaff.2011.1307
.
39
Lee M. Lockwood, “Incidental Bequests and the Choice to Self-Insure Late-Life Risks,” American Economic
Review 108, no. 9 (September 2018): 2513-50, available at:
https://www.aeaweb.org/articles?id=10.1257/aer.20141651
.
40
Brown, Goda, and McGarry, “Long-Term Care Insurance Demand,” 1294-1302; “Findings from the Survey of
Long-Term Care Awareness and Planning,” Office of the Assistant Secretary for Planning and Evaluation, July
2015, available at: https://aspe.hhs.gov/system/files/pdf/110366/SLTCAPrb.pdf
.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 22
long-term care,” while 58% of respondents expressed concern that their premiums would
increase. In addition, policyholders in recent years have experienced a number of
unexpected premium rate increases, and this history is likely an impediment to growing
the market for private LTCI.
• Premiums, costs and loads. Lower demand for LTCI is likely attributable in part to the
high level of premiums charged under new LTCI policies compared to older designs.
41
Premiums vary widely and are based on multiple factors, including the insured’s age,
gender, and health, the period of coverage selected, the elimination period, and the
premium for optional riders. The administrative costs and high loads of private LTCI
also play a role in limiting demand.
42
For additional information on LTCI pricing, see
the “Premium Increases on LTCI” box in the Regulatory Efficiency and Alignment
section of this report.
41
A recent report estimates that in 2019 the average individual LTCI policyholder paid $3,036 during the first year
of coverage, 2% more than in 2018. LIMRA, U.S. Individual Long-Term Care Insurance (Annual Review 2019), 3.
42
The 2012 survey reported that, in response to open-ended questions, the most common reason cited for not
purchasing private LTCI was the cost. The authors noted, however, that this answer does not distinguish among
potential inhibitors such as lack of actuarial fairness, administrative costs, and affordability of premiums.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 23
Innovation and Product Development
In response to the decline of LTCI in the traditional market, insurers have introduced alternative
product designs and new features to both increase the consumer appeal of LTCI and improve
financial returns on this product line for insurers. In addition, insurers and industry experts have
researched and proposed new designs and features that have not been introduced in the market
for several reasons, including regulatory considerations and uncertain demand from consumers
and insurance distributors. This section of the report describes several innovations that have
generated activity and attracted attention from insurers, consumers, regulators, and other
stakeholders.
Recommendation: Overall, the Task Force believes that innovation and product development
have the potential to significantly strengthen the private LTCI market and better address the LTC
needs of consumers.
43
Accordingly, the Task Force recommends that federal and state
policymakers and regulators foster a regulatory environment that encourages flexibility,
experimentation, and innovation in product design to improve consumer choice and access to
benefits, while appropriately protecting the rights of consumers and the solvency of insurers.
Combination Products
Insurers have introduced a variety of products that combine LTCI with other types of insurance.
One popular “combination” or “hybrid” product combines a life insurance policy with a rider
that accelerates payment of the death benefit for qualifying “chronic illness” (as defined under
federal tax law) needs.
44
Another common design features a life insurance policy that
accelerates the death benefit for qualifying LTC needs. These accelerated chronic illness or
accelerated LTC riders limit the payout to 100% of the death benefit amount. Insurers also offer
life insurance policies with extension of benefits riders that allow payouts higher than the death
benefit.
45
Finally, some insurers offer deferred annuity contracts with LTC riders that also allow
payouts exceeding the death benefit.
Figures 4-6 present data for combination products during the five years from 2014 to 2018. Life
combination products generated $4.3 billion in premiums in 2018, which is 2% lower than in
43
The NAIC has studied and commented on the important role of innovation in LTC financing. For example, a
2016 study by the NAIC’s research arm aimed to stimulate debate to support innovation and the future development
of LTC. See National Association of Insurance Commissioners and the Center for Insurance and Policy Research,
The State of Long-Term Care Insurance: The Market, Challenges and Future Innovations, ed. by Eric C. Nordman
(Kansas City: NAIC and the Center for Insurance Policy and Research), May 2016, available at:
https://www.naic.org/documents/cipr_current_study_160519_ltc_insurance.pdf. As another example, the NAIC
2017 List was produced by the NAIC’s Long Term Care Innovations (B) Subgroup.
44
Chronic illness riders may have triggers identical to traditional LTCI (i.e., severe cognitive impairment or inability
to perform two ADLs), but they are regulated differently for federal tax law and state law purposes, and cannot be
marketed as LTCI.
45
Stakeholders indicated that some EOB riders pay up to two or three times higher than the death benefit amount.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 24
2017 but almost 80% higher than $2.4 billion in premiums in 2014. New policy counts increased
2% year-over-year in 2018, with over 400,000 policies sold, a fourfold increase compared to the
number of new policies sold in 2014. Measured by new lives insured, life combination products
constituted more than 87% of the market for individual LTCI solutions in 2018.
46
Annuity
combination sales reached $575 million in 2018, 4.5% higher than the prior year, while the
number of contracts sold grew from 4,940 to 5,130, or 4%.
46
Source: LIMRA.
2,000
2,500
3,000
3,500
4,000
4,500
2014 2015 2016 2017 2018
$ Millions
Figure 4: Life Combination Premiums
Source: LIMRA.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 25
Combination products offer potential advantages from the consumer perspective, particularly for
those consumers who are deterred by the “use or lose” aspect of stand-alone LTCI policies. The
underlying life insurance policy builds cash value and provides a death benefit even if the
policyholder does not make a claim for LTCI expenses. The ability to combine different
coverages into a single policy, with one purchasing decision instead of two or more, appeals to
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
450,000
2014 2015 2016 2017 2018
New Lives
Figure 5: Life Combination New Lives
Source: LIMRA.
400
425
450
475
500
525
550
575
600
2014
2015 2016
2017 2018
$ Millions
Figure 6 : Annuity Combination Premiums
Source: LIMRA.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 26
some consumers. In addition, consumers may perceive that premiums for stand-alone LTCI, or
for both a life insurance policy and a stand-alone LTCI policy, are too expensive and that a
combination product is more affordable.
47
On the other hand, navigating the market for combination products can be challenging for both
consumers and distributors. Because these products differ from each other in their basic designs
(accelerated benefits, extension of benefits, and either a life insurance or an annuity chassis),
pricing, and features, selecting an appropriate solution to an individual’s particular needs can be
highly complex. For this reason, the quality of consumer information and education, the clarity
of marketing materials, and the training of insurance producers are important attributes in the
market.
From the insurers’ perspective, combination products are less risky than LTC stand-alone
products.
48
According to a 2017 survey of 11 insurers in the LTCI market, the incidence of
claims and other actuarial results with respect to combination products have been positive for
insurers.
49
Given their consumer appeal, lower risk profile, and favorable actuarial experience,
combination products are likely to continue growing in variety and volume (although cost may
limit their upside potential).
50
Recommendation: Policymakers could benefit from analysis of the impact of combination
products on the market for LTC risk protection. To the extent that combination products are
attracting purchasers who would otherwise buy stand-alone products, they are not necessarily
expanding overall LTCI coverage. However, if combination products are attracting consumers
who would not otherwise buy LTC protection, on balance they likely are increasing coverage.
The Task Force recommends that actuaries, academics, and other stakeholders explore such an
analysis, with coordination by FIO.
47
Comparative pricing between combination products and stand-alone LTCI is not straightforward because the
products provide different coverages with different features and payment structures. For a comparison of premiums
and benefits under life combination products, annuity combination products, and stand-alone LTCI at issue ages 50
and 65, see Carl Friedrich et al., “Unlocking Potential – New Combination Long-Term Care Insurance Solutions
Show Promise,” Contingencies Magazine, May/June 2019, Figures 2 and 3, available at:
http://contingencies.org/unlocking-potential-new-combination-long-term-care-insurance-solutions-show-promise/
.
48
See “Quantification of the Natural Hedge Characteristics of Combination Life or Annuity Products Linked to
Long Term-Care Insurance,” Milliman, March 2012, available at:
https://www.soa.org/globalassets/assets/files/research/projects/research-2012-03-quant-nat-hedge-report.pdf
.
49
Friedrich et al, “Unlocking Potential.”
50
Earlier versions of life combination products were largely funded by single premiums, requiring large up-front
payments compared to a recurring premium design. A 2018 LIMRA market overview found that in 2017, the
average single premium for a life combination product with an extension of benefits rider was $91,000, well beyond
the price range of the middle market (households with annual income of $35,000 to $99,999). However, the
overview noted that newer recurring premium policies offer more affordable premiums, and that life combination
products with chronic illness or LTC acceleration riders can be less expensive.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 27
Other New Product Designs
“Morphing” Policies
Innovation and experimentation in the LTCI market extend beyond combination products. The
NAIC 2017 List included allowing products that begin as life insurance (or other type of
coverage, such as disability or chronic illness) and later automatically convert (“morph”) into
LTCI at a pre-determined date, such as after the policyholder reaches a certain age. In addition,
the Society of Actuaries (SOA) has developed a product concept it refers to as “LifeStage
Protection,” an insurance policy that starts as term life insurance during prime income-earning
years and switches to LTCI in later years.
51
The Task Force is not aware of any insurers that have developed and launched a morphing
product such as LifeStage Protection. The level of potential demand from consumers and
insurance distributors is uncertain, and it is possible that insurers are hesitant to incur the expense
of fully developing this type of product due to uncertainty regarding its regulatory treatment
under state law.
52
At the same time, state regulators may be reluctant to define precisely how
they would treat the product if they do not have access to product specifications or a policy
form.
53
Limited LTCI
“Short” or “limited” LTCI policies have attracted attention from some insurers and consumers as
a lower-cost alternative to traditional products. This interest is reflected in the NAIC 2017 List,
which includes the option of “allowing shorter maximum benefit plans (<1 year) to be tax
qualified to incent market expansion through lower-price, shorter duration policies.” Unlike
traditional LTCI, which must provide coverage for a period of not less than 12 consecutive
months, limited LTCI typically stops providing coverage after one year from the commencement
of benefit payments.
54
51
“Society of Actuaries Drives Innovation in the Long-Term Care Market; Conceptualizes New, Low-Risk Products
That Could Help Ease Industry Challenges,” Society of Actuaries, July 2018, available at:
https://www.soa.org/globalassets/assets/files/resources/research-report/2018/ltc-market-fact-sheet.pdf
; see also
Treasury, “Public Comments,” Society of Actuaries.
52
State law uncertainty derives from the absence of product specifications and policy forms tailored to this new
product concept. At the federal level, the Task Force did not identify any federal income tax barriers to the
morphing product concept.
53
Several states have demonstrated openness to considering innovative product designs. For example, the state of
Minnesota has been directly involved in developing LifeStage Protection and has stated that “there appear to be
pathways available to overcome potential regulatory hurdles.” See “LifeStage Protection Product Final Report,”
Minnesota Department of Human Services, December 2018, available at:
https://mn.gov/dhs/assets/LifeStage-
protection-product%E2%80%93final-report_tcm1053-373463.pdf.
54
Under the NAIC’s LTCI Model Act, a policy does not meet the definition of “long-term care insurance” unless it
provides coverage for not less than 12 consecutive months for each person covered. National Association of
Insurance Commissioners, Long-Term Care Insurance Model Act (Kansas City: NAIC, Quarter 1 2017), Section
4.A, available at: https://www.naic.org/store/free/MDL-640.pdf?10
.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 28
Although metrics for this market are not widely published, one insurance association estimates
that:
• Almost half (49%) of traditional LTCI claims last one year or less;
• The typical limited LTCI policy provides coverage for one year or less;
• The majority of limited policies have no deductible or elimination period, while about
94% of traditional policies feature a 90-day waiting period before benefits can be paid;
• Most applications for limited policies have seven to ten health questions with no
additional underwriting requirements;
• The typical buyer of limited LTCI is between the ages of 65 and 74 and has a net worth
of less than $500,000;
• A typical premium at age 65 is $105 monthly; and
• Typical benefit amounts are $100, $150, or $200 per day.
55
Based on these estimates, limited LTCI may be an alternative to traditional policies for
individuals who cannot afford the higher premiums charged for traditional products. However,
consumer representatives note that limited LTCI policies may not pay for coverage outside of
nursing homes, such as assisted living or home care, and likely do not provide adequate
protection against a catastrophic LTCI event.
56
In addition, some insurers and insurance
regulators have expressed concerns that the labels “short long-term care” or “limited long-term
care” are counter-intuitive and inherently confusing for consumers, and that policies with shorter
benefit periods are susceptible to misunderstanding and inappropriate marketing practices.
57
In late 2018, the NAIC adopted the Limited Long-Term Care Insurance Model Act and the
Limited Long-Term Insurance Model Regulation.
58
In general, these models track those for
traditional LTCI, with adjustments to reflect a benefit period of less than twelve months. In
particular, the models contain substantially the same consumer protections as their traditional
55
“National Advisory Center for Short-Term Care Information,” American Association for Long-Term Care
Insurance, last accessed February 2020, available at: https://www.aaltci.org/short-term-care-insurance/
.
56
Ellen Stark, “Long-Term-Care Insurance Gets a Makeover,” Consumer Reports, August 2017, available at:
https://www.consumerreports.org/long-term-care-insurance/long-term-care-insurance-gets-a-makeover/
; Eleanor
Laise, “Short-Term-Care Insurance Policies on the Rise,” Kiplinger, October 2015, available at:
https://www.kiplinger.com/article/insurance/T027-C000-S004-short-term-care-insurance-policies-on-the-rise.html.
57
Allison Bell, “Short-Term Care Insurance Faces a Name Fight,” ThinkAdvisor, May 2018, available at:
https://www.thinkadvisor.com/2018/05/30/short-term-care-insurance-faces-a-name-fight/?kw=%27Short-
Term%20Care%20Insurance%27%20Faces%20a%20Name%20Fight&et=editorial&bu=TA&cn=20180530&src=E
MC-Email&pt=LifeHealthNewsFlash.
58
National Association of Insurance Commissioners, Limited Long-Term Care Insurance Model Act (Kansas City:
NAIC, Quarter 4 2018), available at: https://www.naic.org/store/free/MDL-642.pdf
; National Association of
Insurance Commissioners, Limited Long-Term Care Insurance Model Regulation (Kansas City: NAIC, Quarter 4
2018), available at:
https://www.naic.org/store/free/MDL-643.pdf.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 29
counterparts, except that insurers must offer inflation protection at a 3% annual compound rate
instead of a 5% annual compound rate. However, the states generally have not yet adopted either
model.
59
Recommendation: The Task Force recommends that federal policymakers work with their state
counterparts and with private sector stakeholders to evaluate and monitor the market for limited
LTCI, including potential impacts on the risk pool for longer-term products and on Medicaid.
The Task Force further recommends that state legislators and insurance regulators take steps to
better streamline and standardize the regulation of this market.
Group Products
The Task Force considered two policy proposals for LTCI group products that were included
under the NAIC 2017 List, both involving the fiduciary provisions of ERISA. ERISA safeguards
the participants and beneficiaries of employee benefit plans by imposing standards of care and
loyalty on plan fiduciaries, and by holding fiduciaries accountable when they breach those
obligations. ERISA does not require any employer to establish a plan, but does require those
who establish plans to meet certain standards.
One policy proposal is to create a safe harbor to remove potential exposure to ERISA fiduciary
liability as a factor in employers’ decisions not to offer LTCI to employees, including offering it
on an automatic enrollment or “opt-out” basis. A second policy proposal is to permit 401(k) and
IRA participants to purchase LTCI within their accounts (“Retirement Plus”). The objective of
both proposals is to promote a more viable group LTCI market by increasing employee
participation, resulting in a larger and more favorable risk pool for insurers and, potentially,
lower premiums.
Recommendation: Based on stakeholder input and an assessment of the market and legal
landscapes, the Task Force questions whether either proposal would have a meaningful impact
on participation levels. Accordingly, the Task Force does not recommend either proposal.
In general, while automatic enrollment has increased employees’ participation in 401(k) plans,
60
the effect may not be the same with respect to LTCI. Low take-up rates for LTCI appear to stem
at least in part from low demand for these products, as reflected in some stakeholders’ comments
to the Task Force. Currently, employees generally must affirmatively enroll or “opt-in” to LTCI
and shoulder the entire premium cost without favorable tax treatment. According to the U.S.
59
Utah adopted the Limited Long-Term Insurance Model Act in April 2020. Utah Code Ann. §§ 31A-22-2001-
2006.
60
See Brigitte C. Madrian and Dennis F. Shea, “The Power of Suggestion: Inertia in 401(k) Participation and
Savings Behavior,” The Quarterly Journal of Economics 116, no. 4 (November 2001): 1149-1187, available at:
https://www.ssc.wisc.edu/~scholz/Teaching_742/Madrian_Shea.pdf
.
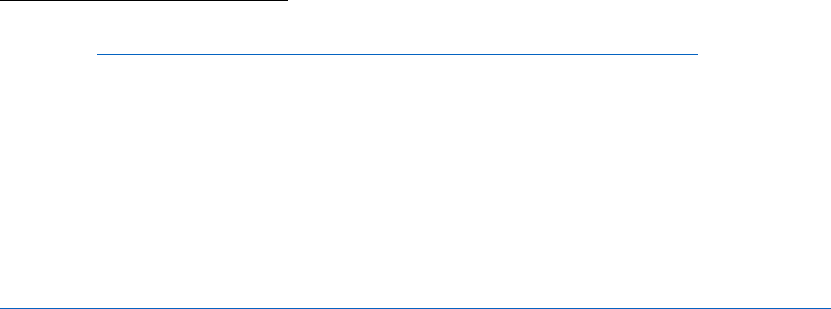
Long-Term Care Insurance: Recommendations for Improvement of Regulation 30
Bureau of Labor Statistics, 17% of civilian employees had access to LTCI in 2019.
61
Employee
take-up rates are typically between 5% and 7% based on a report from the NAIC and the Center
for Insurance Policy and Research in 2016.
62
Without higher demand for LTCI on the part of employees, the Task Force does not expect
employers to choose to provide LTCI as part of their compensation package. The Task Force
considers it unlikely that employers would default a percentage of their workers’ payroll towards
contributions for LTCI premiums, regardless of a fiduciary safe harbor. Similarly, with respect
to the purchase of LTCI as a 401(k) plan “investment” option, the Task Force questions whether
employers or workers would be willing to increase their contributions to the plan to fund LTCI
premiums or replace current contributions to retirement savings with LTCI premium payments.
In addition to considerations of employee demand, 401(k) plans and LTCI impose different
obligations on plan sponsors, as discussed below.
Fiduciary Safe Harbor
The NAIC 2017 List suggests “addressing concerns that may prevent an employer from
providing LTCI on an opt-out basis by providing a safe harbor to limit the employer’s fiduciary
liability.”
63
The Task Force recognizes both employers’ concerns and the power of automatic
enrollment to promote participation in many contexts, but generally considers it unlikely that this
proposal would promote a significant increase in demand for LTCI.
As an initial matter, the proposal is premised on the possibility that potential exposure to ERISA
fiduciary liability may be a significant factor in employers’ decisions not to offer LTCI,
especially with respect to opt-out arrangements where the employee is not making an affirmative
choice to participate. Similar concerns about long-term fiduciary liability exposure for selection
of the insurance provider have been cited as an obstacle to employers offering annuities in
401(k) plans, but efforts to address the issue in that context to date have not had a significant
effect on availability or use of annuity options in 401(k) plans.
64
61
“Table 41. “Health-related Benefits: Access, Civilian Workers, March 2019,” Bureau of Labor Statistics,
available at:https://www.bls.gov/ncs/ebs/benefits/2019/ownership/civilian/table41a.pdf
.
62
NAIC and CIPR, State of Long-Term Care Insurance, 10.
63
The NAIC 2017 list additionally proposes expanding “catch-up” contributions to retirement plans and allowing
LTCI purchases through a cafeteria plan. These are primarily tax-related rather than ERISA-related proposals, and
as such are addressed in the Tax Incentives section of this report.
64
In 2008, DOL issued a rule that provides plan fiduciaries with the steps they should take when selecting annuities
in such cases. In 2015, DOL publicly emphasized that, under this rule, a fiduciary decision is evaluated based on the
information available at the time the decision was made, and not on subsequent events (e.g., an insurer’s subsequent
failure, which was not foreseeable at the time of the decision). See 29 CFR § 2550.404a-4; “Field Assistance
Bulletin No. 2015-02,” Employee Benefits Security Administration, July 13, 2015, available at:
https://www.dol.gov/agencies/ebsa/employers-and-advisers/guidance/field-assistance-bulletins/2015-02
. This rule
and guidance, however, are generally perceived to have stopped short of fulfilling employers’ wishes for bright-line
safe harbor criteria. Congress responded to these concerns in the Setting Every Community Up for Retirement and

Long-Term Care Insurance: Recommendations for Improvement of Regulation 31
In circumstances where workplace LTCI is not covered by ERISA, a fiduciary safe harbor would
be of no consequence. ERISA includes a statutory enumeration of classes of benefits it covers,
including retirement, medical benefits, and benefits in the event of sickness or disability, but
does not explicitly include LTCI benefits.
65
Therefore, whether LTCI constitutes an ERISA-
covered benefit depends, in part, on whether particular LTCI benefits fall within the scope of one
of the listed classes of benefits. Further, the statutory definition covers enumerated benefits only
when they are offered as part of a covered “employee benefit plan,” which requires a certain
level of involvement by the employer. A DOL regulation provides conditions under which
voluntary arrangements funded entirely with employee contributions are not treated as ERISA-
covered employee benefit plans.
66
Potential conflicts with state wage payment laws pose a challenge to mandating auto-enrollment.
DOL has taken the position that ERISA generally preempts state laws that limit, prohibit, or
regulate an employer’s adoption of automatic enrollment arrangements in connection with an
ERISA-covered plan, or from making related deductions from employee wages for contributions
to such a plan.
67
Finally, the success of an existing statutory safe harbor for 401(k) default investments may not
provide evidence for the likely success of a safe harbor for LTCI.
68
As described below, there
are three important differences between this 401(k) precedent and a potential safe harbor for
LTCI.
First, the current 401(k) safe harbor for default investments is narrower than the contemplated
LTCI safe harbor insofar as it addresses only the selection of the broad types of investments
Enhancement Act of 2019 (SECURE Act). Section 204 of the SECURE Act amended ERISA to provide a statutory
safe harbor for complying with ERISA’s prudent person standard of care for the selection of an insurer to provide a
guaranteed retirement income contract. There is no data yet available on whether this statutory version of a
fiduciary safe harbor will materially affect employers’ decisions to offer annuity options in 401(k) plans or
employee use of such options.
65
See U.S. House, H.R.2 – Employee Retirement Income Security Act (Washington: 93rd Congress, 1974), Sections
3(1) and 3(2).
66
These types of voluntary group and group-type insurance programs are not treated as ERISA plans if the employer
merely offers such insurance for employee purchase by payroll deduction and neither endorses nor helps pay for the
insurance. See 29 CFR 2510.3-1(j).
67
While ERISA generally does not preempt state criminal laws of general application, it generally does preempt
state civil laws that otherwise would interfere with automatic enrollment in ERISA-covered welfare plans. For a
fuller discussion of this topic, see “Information Letter 12-4-2018,” Employee Benefits Security Administration,
December 2018, available at:
https://www.dol.gov/agencies/ebsa/employers-and-advisers/guidance/information-
letters/12-4-2018.
68
A 2006 federal pension law amended ERISA and the Code to add a fiduciary safe harbor and other provisions to
facilitate automatic enrollment in, and automatic payroll withholding contributions to, 401(k)-type plans. U.S.
House, H.R.4 – Pension Protection Act of 2006 (Washington: 109th Congress, 2006); U.S. House, ERISA, Section
514(e). That law addressed two obstacles to automatic 401(k) plans: fiduciary concern about the selection of default
investments and state wage payment laws. The 2006 law charged DOL with issuing a fiduciary safe harbor for
qualified default investments, and preempted state wage payment laws for plans that operate within the safe harbor.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 32
(generally, a diversified mix of stocks and bonds) available under the plan.
69
Default options are
also easier for plan sponsors to implement for 401(k) plans than for LTCI. Employers who offer
LTCI have to consider whether, or under what circumstances, automatic enrollment in LTCI
would be appropriate for their workforce in light of variation in employees’ circumstances and
needs.
Second, the current 401(k) safe harbor bears less weight than its potential LTCI counterpart
because 401(k) participants can more easily shift out of default investments, while LTCI
participants are more constrained.
Third, as noted above, it is unclear how many of these LTCI arrangements would be covered by
ERISA. For these reasons, while the 401(k) fiduciary safe harbor is generally regarded as a
success in increasing participation in 401(k) plans, an LTCI safe harbor would likely be less
effective.
In summary, even if Congress or DOL could craft an appropriate fiduciary safe harbor, there
remains substantial doubt regarding whether it would materially expand the demand for LTCI.
Demand is low in the marketplace and it is unclear whether concern for fiduciary liability is an
important driver in employers’ decisions on LTCI. The lack of employer and employee demand,
as reflected in some stakeholders’ comments to the Task Force, also would likely continue to
discourage employers from deciding to auto-enroll employees (and direct a portion of their pay)
into LTCI.
70
Retirement Plus
The SOA, in its comment letter to the Task Force, references its “Retirement Plus” proposal.
71
The proposal would make LTCI available as an option within a 401(k) or IRA, with premiums
deducted directly from the account balance. However, the Task Force notes that adding LTCI as
a 401(k) “investment” option would likely require changes to current law.
ERISA generally classifies plans as providing either retirement or welfare benefits, and includes
separate provisions tailored for each. ERISA’s fiduciary provisions applicable to 401(k)
accounts generally speak to the “investment” of “assets” in the account. If ERISA were
amended to facilitate LTCI within a 401(k) plan, employers still might be reluctant to offer this
feature, fearing fiduciary liability.
69
The current 401(k) safe harbor does not address the evaluation of insurers’ claims-paying capability, the amount
of premiums, or the appropriateness of alternative insurance policy provisions.
70
For example, some stakeholders expressed that employers are disinclined to offer LTCI benefits because they face
more pressing issues, such as compliance with health care laws. Stakeholders further cited wariness of financial
products stemming from the 2007-2009 recession as a factor in the low demand for LTCI.
71
Treasury, “Public Comments,” Society of Actuaries.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 33
Incidental Benefits
Under most LTCI policies, the insured is not eligible to submit a claim for benefits until he or
she becomes “chronically ill” as defined under state insurance laws and the Code. Policies
typically define chronic illness as severe cognitive impairment or the inability to perform without
substantial assistance at least two ADLs. In order for an LTCI policy to qualify for favorable tax
treatment under the Code, it must condition the payment of benefits upon certification by a
licensed health care practitioner that the insured is chronically ill.
72
Some stakeholders proposed that Congress should amend the Code to permit payment of
incidental benefits from a LTCI policy prior to the onset of chronic illness, without causing the
policy to forfeit its tax-qualified status. These benefits could include limited provision of
evidence-based, cost-effective incidental benefits that would reduce the likelihood of someone at
higher than average risk of becoming chronically ill. For example, a LTCI policy could pay for
home assessments or modifications to identify and mitigate fall risks or other safety hazards to
mobility- or vision-impaired individuals. In addition, incidental benefits might include caregiver
training for non-professional caregivers, including family, or sharing information regarding local
LTC providers to policyholders who need or anticipate needing assistance to remain in their
homes. The rationale for this proposal is that permitting these types of benefits would support
healthy, independent living and aging in place.
Recommendation: Supporting the ability of those potentially needing LTC to remain in their
homes could benefit both consumers and insurers. Accordingly, the Task Force encourages
industry, federal policymakers, and other experts, in consultation with consumer representatives,
to identify and assess evidence of cost-effective interventions. Depending on the results of the
analysis, Congress could consider amending the Code to permit payment of evidence-based,
cost-effective incidental benefits under a tax-qualified LTCI contract prior to the insured
becoming chronically ill, subject to a monetary cap and other conditions set by regulation.
72
26 U.S.C. §7702B(c)(2).

Long-Term Care Insurance: Recommendations for Improvement of Regulation 34
Regulatory Efficiency and Alignment
The Task Force considered various recommendations to improve the efficiency and effectiveness
of regulation of LTCI at the federal and state levels, including options under the NAIC 2017 List.
This section discusses proposed regulatory reforms in the areas of inflation protection, other
consumer protections, and the review and approval of premium increases on LTCI policies.
Inflation Protection
An LTCI policy is, by definition, a long-term financial obligation of the insurer that issues the
policy.
73
Although the period between issuance of the policy and a claim for benefits will vary
widely by policyholder, that period can exceed 20 years or more. Accordingly, consumers face a
significant risk that inflation will erode the value of their benefits over time.
Recognizing this risk, the NAIC included inflation protection as a core consumer safeguard when
it adopted the LTCI Model Regulation in 1988. Under the LTCI Model Regulation, insurers
must offer to each policyholder, at the time of purchase, the option to purchase a policy with an
inflation protection feature that increases benefit levels at an annual compounded rate not less
than 5%. Insurers must also provide a graphic comparison between the benefit levels of a policy
that increases benefits over a period of at least 20 years and a policy that does not increase
benefits. The LTCI Model Regulation further requires insurers to include inflation protection in
the policy unless the policyholder rejects it in writing.
74
Inflation protection is also required under two federal statutes addressing LTCI: HIPAA and the
DRA. These statutes address two different subjects—tax qualification under HIPAA, and a
federal-state partnership program under the DRA—and their inflation protections operate
differently. The Task Force concludes that the efficiency and effectiveness of both statutes can
be improved, as detailed below.
Inflation Protection for Tax-Qualified LTCI Policies Under HIPAA
As part of enacting HIPAA in 1996, Congress amended the Code to add Section 7702B, which
sets requirements that an LTCI policy must meet in order to be “qualified” LTCI for purposes of
the itemized expense deduction and certain other Code purposes. Among these requirements is
compliance with consumer protections contained in specified sections of the 1993 versions of the
73
Under the LTCI Model Act, a “long-term care insurance” policy must provide coverage for not less than 12
consecutive months for each person covered. NAIC, LTCI Model Act, Section 4.A. However, according to the
American Association for Long-Term Care Insurance, the average time elapsed between purchase of a LTCI policy
and eligibility for benefits is 13.4 years. “Long-Term Care Insurance Facts – Data – Statistics – 2019 Report,”
American Association for Long-Term Care Insurance, last modified October 2019, Figure 13, available at:
https://www.aaltci.org/long-term-care-insurance/learning-center/ltcfacts-2019.php#2019claims2
.
74
National Association of Insurance Commissioners, Long-Term Care Insurance Model Regulation (Kansas City:
NAIC, Quarter 1 2017), Section 13, available at: https://www.naic.org/store/free/MDL-641.pdf
.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 35
LTCI Model Act and LTCI Model Regulation, including the provision in the LTCI Model
Regulation requiring insurers to offer 5% annual compound inflation (ACI) protection.
75
Accordingly, although HIPAA does not directly impose a requirement to offer ACI protection, it
accomplishes the same result by reference to the LTCI Model Regulation.
Because almost all currently sold LTCI policies are tax-qualified under HIPAA, the requirement
to offer 5% ACI protection is effectively universal.
76
For every sale, the insurer or producer
must explain and graphically illustrate a benefit feature that is misaligned with actual economic
conditions and that very few consumers accept.
77
The benefit is costly, potentially increasing
premiums by four or five times over a policy with no inflation protection.
78
For these reasons,
the Task Force concludes that inflation protection requirements under HIPAA and state
insurance laws should be revised to increase the efficiency and effectiveness of regulation. At
the same time, the Task Force believes that inflation continues to represent a risk to consumers
and, accordingly, policymakers should revise the current 5% ACI standard rather than eliminate
the offer of inflation protection.
79
Unless Congress changes the existing statutory structure, with its intertwining of HIPAA and the
NAIC models, revising the inflation protection standard is dependent upon both (1) the NAIC
amending the LTCI Model Regulation to set a different standard, and (2) Congressional
legislation amending HIPAA to define the “model regulation” by reference to the updated
model.
80
Finally, even if Congress and the NAIC did so, the revised standard would itself likely
become outdated and uncorrelated with economic conditions.
Recommendation: To both address the outdated inflation requirement and to provide flexibility
to adapt inflation protection to evolving economic conditions, the Task Force recommends that
Congress amend the Code to authorize Treasury to set inflation protections for tax-qualified
75
For purposes of these consumer protections, the Code defines the LTCI Model Regulation and LTCI Model Act as
“the long-term care insurance model regulation, and the long-term care insurance model Act, respectively,
promulgated by the [NAIC] (as adopted as of January 1993).” 26 U.S.C. § 7702B(g)(2)(B)(i).
76
Giese, Schmitz, and Thau, “Milliman Survey,” 17.
77
Over time, and particularly in the prevailing interest rate environment following the financial crisis, this 5%
standard has become an anachronism, with inflation in recent years running significantly lower than 20 years ago
when the NAIC and (by reference) Congress set the ACI at 5%. See Treasury, “Public Comments,” American
Academy of Actuaries. Consumers have reacted to this change by increasingly rejecting the initial offer of 5% ACI
because of the higher premium costs associated with this level of protection. According to one survey, in 2018 only
2% of LTCI sales included 5% ACI protection, compared to 56% in 2003 and more than 47% each year from 2006
to 2008. Giese, Schmitz, and Thau, “Milliman Survey,” 11-13.
78
Treasury, “Public Comments,” American Academy of Actuaries.
79
Some stakeholders suggested that inflation in the cost of LTSS might be a more appropriate HIPAA benchmark
than a fixed percentage or the rate of inflation in the general economy. For estimates of increases in the cost of
various categories of LTSS from 2018 to 2019, see “Genworth Cost of Care Survey 2019: Summary and
Methodology,” Genworth Financial, Inc., last modified October 2019, available at:
https://pro.genworth.com/riiproweb/productinfo/pdf/131168.pdf
.
80
In addition, even if the NAIC and Congress took these two steps, state insurance laws and regulations would
continue to require the 5% ACI offer until the states conformed those laws and regulations to the revised model.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 36
LTCI. With this authority, Treasury and Congress could coordinate with the NAIC and the
states to implement changes in inflation protection through the regulatory process without the
necessity of additional Congressional legislation.
Inflation Protection for the Partnership Program Under the DRA
In the early 1990s, four states—California, Connecticut, Indiana, and New York—implemented
the Partnership program. The program aims to lower federal LTC costs by encouraging
individuals who might otherwise “spend down” their assets (in order to qualify for Medicaid) to
rely instead on a LTCI policy. For every dollar of coverage paid by a Partnership policy, the
policyholder may disregard one dollar of the asset amount necessary to become eligible for
Medicaid LTC benefits.
81
The DRA opened the Partnership program to all states, subject to specified conditions including
inflation protection and other consumer protections.
82
The DRA inflation protection rules differ
from those under HIPAA in three significant ways: (1) under the DRA, inflation protection must
be not only offered, but also included in the policy; (2) the DRA links inflation protection to
three age tiers;
83
and (3) the DRA does not specify the amount of inflation protection required,
leaving that issue to the states.
Based on Treasury staff research, states that have adopted the Partnership program vary widely
in their inflation protection requirements.
84
This lack of uniformity has created a regulatory
patchwork with uneven consumer protection standards and additional complexity that makes it
more difficult to write LTCI. Additionally, high inflation protection requirements may raise
costs and reduce the attractiveness of Partnership policies. For example, insurers sell almost no
Partnership policies in California, a populous state that requires 5% inflation protection.
Although multiple factors can affect sales volume in a given state, the effect of 5% compound
inflation on pricing is significant.
85
81
See generally “Long-Term Care Partnership Expansion: A New Opportunity for States,” Center for Health Care
Strategies, Inc., last modified May 2007, available at:
https://www.chcs.org/media/Long-
Term_Care_Partnership_Expansion.pdf; “Long Term Care Insurance Partnership Plans,” American Association for
Long-Term Care Insurance, last accessed February 2020, available at: https://www.aaltci.org/long-term-care-
insurance/learning-center/long-term-care-insurance-partnership-plans.php.
82
42 U.S.C. § 1396p.
83
The DRA requires the policy to provide ACI protection for individuals under age 61, “some level” of inflation
protection for individuals between ages 61 and 75, and no inflation protection for individuals age 76 and over
(although inflation protection may be included). 42 U.S.C. § 1396p(b)(1)(C)(iii)(IV).
84
Four require no less than 5%; 17 require no less than 3%; six require no less than 1%; three have other formulas;
and 17 do not specify a level of inflation protection. Approximately 25 states link the level of protection to either a
stated percentage or changes in the Consumer Price Index. As an example of additional variations, some states
specifically prohibit guaranteed purchase options as a means of meeting inflation protection requirements, others are
silent, and a smaller number specifically allow guaranteed purchase options.
85
According to one estimate, in early 2019 a typical Partnership policy for a 57-year-old couple in California costs
$15,099 per year with 5% compound protection compared to $7,312 per year with 3% compound. Louis H.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 37
Recommendation: The Task Force recommends that state policymakers—legislators, state
Medicaid directors, insurance commissioners, and the NAIC—improve regulatory efficiency and
effectiveness by harmonizing and streamlining inflation protection requirements under the
Partnership program. Alternatively, Congress could delegate to HHS the authority to set
Partnership program inflation protection requirements under the DRA.
86
Other Consumer Protections
Apart from inflation protection, both HIPAA and the DRA mandate compliance with certain
consumer protections contained in the NAIC’s LTCI Model Act and LTCI Model Regulation.
However, the DRA defines “model regulation” and “model Act” by reference to the NAIC
models adopted as of October 2000, while HIPAA does so by reference to the January 1993
versions. This federal cross-referencing in two separate statutes of two outdated and conflicting
versions of NAIC models creates confusion and adds complexity to writing LTCI business.
Recommendation: The Task Force recommends that Congress consider options to address this
regulatory inefficiency. For example, as one option, Congress could empower Treasury, in
consultation with HHS, to set consumer protection standards using one version of the LTCI
Model Act and LTCI Model Regulation for purposes of both tax qualification under HIPAA and
Partnership eligibility under the DRA, with flexibility to update the standards periodically (e.g.,
every 10 years). Under this approach, Treasury and HHS could coordinate with the NAIC and
the states to maintain consistency between federal and state laws with respect to consumer
protection, without the necessity of additional federal legislation.
Review and Approval of Rate Increases
In most states, the chief insurance regulator has the authority to approve fully, approve in part, or
reject premium rate increases proposed by an insurer. The regulator may also condition its
approval on actions or commitments by the insurer, such as agreeing to withhold requests for
future rate increases for a specified number of years. The authority of state regulators to review
and approve proposed rate increases before the insurer implements those changes is a critical
factor in the LTCI marketplace.
Historically, some state insurance regulators have been more receptive than others to proposed
rate increases. Policyholders in states where regulators have approved rate increases may
Brownstone, “The California Partnership for Long-Term Care Revives,” Broker World Magazine, February 2019,
available at: https://brokerworldmag.com/the-california-partnership-for-long-term-care-revives/
. In September
2016, California enacted Senate Bill 1384. This bill requires insurers to offer both 5% compound inflation and at
least one lower cost option. See California Welfare and Institutions Code § 22005.1(b)(3). To date, the California
Department of Health Care Services has not issued guidance or regulations identifying a lower cost option.
86
The DRA already allows the Secretary of HHS to incorporate revisions to consumer protections under the LTCI
Model Act and LTCI Model Regulation into Partnership requirements. See 42 U.S.C. § 1396p(b)(5)(C).

Long-Term Care Insurance: Recommendations for Improvement of Regulation 38
subsidize premiums in other states where regulators have limited or rejected rate increases.
87
Insurers’ uncertainty concerning regulatory treatment of requested rate increases limits their
ability to remain active in the LTCI market. In addition, the inability to obtain timely and
consistent approvals of actuarially justified rate increases may threaten the financial stability of
in-force blocks of LTCI policies and, in some cases, an insurer itself.
88
Premium Rate Increases for LTCI
Insurers set rates, or premiums, for their products based on actuarial assumptions about risk,
future policyholder behavior, and future economic conditions. The accuracy of these
assumptions is particularly important for products such as LTCI that remain in force for long
periods. Primary determinants of pricing for LTCI include morbidity (how many policyholders
need LTC, and for how long), lapse (how many policyholders voluntarily drop their coverage),
and interest rates (which determine the amount of income earned by insurers on assets supporting
their liabilities). Since 2000, all of these factors have gone in an unfavorable direction for
insurers: morbidity is somewhat worse than expected; voluntary lapse rates are lower than for
other insurance products; and interest rates are significantly lower than levels assumed in
pricing.
89
As the profitability of in-force LTCI policies has eroded over the past two decades, many
insurers have increased premiums on those policies, in some cases by a cumulative 100% or
more. Although regulators often require insurers to phase in these increases over a specified
timeframe, such as three years, the impact on affordability for policyholders can be severe. In
addition, repeated rate increases generate both adverse publicity for insurers and distrust among
consumers and insurance producers, lowering demand for LTCI.
The financial performance of in-force LTCI policies remains a key issue for the insurance
industry, investors, regulators, and policyholders. LTCI carriers continue to increase their
reserves (funds set aside to pay future claims), update their actuarial assumptions, and disclose
their reserving methodologies in more detail. One rating agency estimates that most insurers will
87
See, e.g., Jason Wobelen, “Regulator Rejects LTC Rate Hike, Says Request Biased against Utah Policyholders,”
S&P Global Market Intelligence, November 2019, available at:
https://platform.marketintelligence.spglobal.com/web/client?auth=inherit&ignoreIDMContext=1#news/article?id=5
5482328&KeyProductLinkType=2.
88
Insurers that focus mainly on the LTCI product line may be particularly vulnerable. For example, on February 3,
2020, the Pennsylvania Insurance Commissioner obtained a state court order placing Senior Health Insurance
Company of Pennsylvania into rehabilitation. As of December 31, 2019, the company had approximately 54,000
LTCI policyholders, $2.7 billion in liabilities, and a surplus deficit of $466 million. See Allison Bell, “Pennsylvania
Puts LTCI Issuer in Rehabilitation,” ThinkAdvisor, February 2020, available at:
https://www.thinkadvisor.com/2020/02/06/pennsylvania-puts-ltci-issuer-in-rehabilitation/
. When an insurer is
liquidated, state insurance guaranty associations pay certain covered claims and fund those payments by assessments
on solvent insurers in the states of residence of the policyholders.
89
Marc A. Cohen “The Current State of the Long-Term Care Insurance Market,” presentation to the Federal
Advisory Committee on Insurance, February 2018, available at:
https://home.treasury.gov/system/files/311/FACIFebruary2018_UMass.pdf
.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 39
not reach their peak reserves for in-force business for another 10 to 15 years.
90
Accordingly,
uncertainty about the profitability of in-force business will persist. This uncertainty, combined
with negative trends in claims experience as well as ongoing questions regarding the ability of
insurers to obtain regulatory approvals of rate increases, has led many insurers to exit the LTCI
market, creating a drain in capital.
91
Concerns over the financial solvency of insurers, and the
potential impact of insolvencies on state insurance guaranty associations, are also important
considerations for this market.
In 2019, the NAIC identified the regulation of LTCI as the organization’s top priority, noting
significant issues posed by the current LTCI environment to both consumers and the state-based
system of insurance regulation. The NAIC formed an Executive Task Force charged with
developing “a consistent national approach for reviewing LTCI rates that results in actuarially
appropriate increases being granted by the states in a timely manner and eliminates cross-state
rate subsidization.”
92
The Executive Task Force is also charged with identifying options to
provide choices for consumers regarding modifications to LTCI contract benefits where policies
are no longer affordable due to rate increases.
The primary work stream of the Executive Task Force is a multistate review of LTCI focusing on
different actuarial methodologies used by the states. In addition, the Executive Task Force has
organized five other work streams to:
• explore alternatives for protecting policyholders from caps on state guaranty association
coverage and potential inequities arising from the states’ inconsistent approaches to
premium rate increase requests;
• ensure policyholders understand their options when faced with a rate increase;
• evaluate the interaction between rate increase issues and reserving issues;
• address non-actuarial variances among the states when reviewing rate increases; and
• consider whether the task force needs additional data to support its work.
Recommendation: The Task Force recommends that the NAIC and the states maintain their
focus on LTCI and work together in 2020 to develop a consistent national approach to regulatory
reviews of LTCI rate increase requests. The Task Force also recommends that FIO continue to
monitor and report on this issue.
90
“Following the Trail of U.S. Insurers’ Long-Term Care Assumptions,” S&P Global Ratings, January 10, 2019,
available at:
https://www.spratings.com/documents/20184/908539/LifeINSHT_Jan2419_Article4.pdf/2f9c6736-
6f26-36ae-d32e-3f2d8c265818.
91
The number of insurers offering LTCI policies has dropped from more than 100 in 2000 to only a dozen or so in
2020.
92
“Long-Term Care Insurance (EX) Task Force,” National Association of Insurance Commissioners, last accessed
February 2020, available at: https://content.naic.org/cmte_ex_ltci_tf.htm
.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 40
Financial Literacy and Education
Reviewing the Federal Role in Financial Education
The NAIC 2017 List included a federal education program around retirement security and the
importance of planning for potential LTC needs. In July 2019, Treasury issued the Financial
Literacy Report, which laid out an appropriate federal role for financial education and considered
the roles of the private and non-profit sectors, and other government entities in this field.
93
The
issuance of the Financial Literacy Report followed a literature review and extensive
consultations with experts and stakeholders inside and outside of the government.
In the Financial Literacy Report, Treasury recommended that the primary federal role for
financial literacy and education should be to empower financial education providers as opposed
to attempting to reach every American household directly. This federal role could include
developing and implementing policy, encouraging research, and other activities, such as
conducting financial education programs and developing educational resources to advance best
practices and standards. The Financial Literacy Report further recommended that the federal
government should consider the impact of the lack of financial literacy on households and the
risk to the economy from negative externalities and market failures.
The Financial Literacy Report defined high-priority areas for financial education, including
retirement saving and investor education. Treasury noted the significant level and
interconnection among retirement planning concerns. For example, 25% of Americans have no
retirement savings, less than 40% of non-retired adults believe they are on track for a secure
retirement, and many working age Americans face difficult challenges in planning for their old
age.
94
The Financial Literacy Report also described current federal programs on retirement planning,
including programs and information provided by DOL’s Employee Benefits Security
Administration (EBSA) and by SSA. EBSA provides education materials and tools, conducts
outreach, and answers questions from employers and employees about all aspects of workplace
retirement savings plans; and SSA conducts outreach through websites, mass media, and in-
person events. Other federal agencies promote their retirement planning resources through
networks of relevant organizations and through social media. However, despite the number of
programs and resources available, in fiscal year 2017, retirement savings education was one of
the least-funded financial education priorities in the federal government, totaling less than 1% of
expenditures on financial education ($2.2 million out of $273 million).
95
93
Treasury, Financial Literacy Report.
94
Treasury, Financial Literacy Report, 32.
95
Treasury, Financial Literacy Report, 1, 53.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 41
From 2005 to 2010, HHS, along with 24 states and the District of Columbia, participated in the
Own Your Future Awareness Campaign, which was designed to raise awareness about the risks
of needing LTC and to encourage LTC financial awareness.
96
The National Clearinghouse for
Long-Term Care Information website was launched in 2006 to supplement the campaign by
helping Americans actively engage in planning for LTC.
97
Through this campaign,
approximately 20 million households were reached and 1.5 million LTC planning guides were
distributed.
98
A post-campaign survey found that people who received the planning guide were more likely to
take action (as compared to those who did not), such as reviewing existing coverage, talking to
an advisor about LTC needs, or buying LTCI.
99
Additionally, a 2004 survey of consumers aged
45 to 70 found that those who had heard about LTC were more likely to request additional
information, especially those who received direct mail.
100
However, there is evidence that those
who requested the guide would have been more likely to take those steps even without the
prompt.
101
Stakeholder Recommendations Relating to Education
A number of organizations have recommended education as an important way to improve
awareness of LTCI and LTC planning; however, these recommendations do not provide
evidence or specificity about how to implement education in ways that will have a measurable
impact.
In 2019, the NAIC organized a Retirement Security Working Group, which drafted a work plan
that includes researching and developing financial education curricula for each life stage from
high school through retirement (financial literacy and decision-making, the time value of money,
LTC, and debt and credit are subjects to be considered). Additionally, the plan includes
developing an education campaign targeting employers to provide retirement plans and assist
96
See “Empowering Consumers Through Education,” America’s Health Insurance Plans, last modified September
2018, available at: https://www.ahip.org/empowering-consumers-through-education/
.
97
Section 6021(d) of the DRA directed the Secretary of HHS to establish the Clearinghouse.
98
“Final Report on the “Own Your Future” Consumer Survey,” U.S. Department of Health and Human Services,
Office of the Assistant Secretary for Planning and Evaluation, last modified November 2006, available at:
https://aspe.hhs.gov/basic-report/final-report-own-your-future-consumer-survey
.
99
Eileen J. Tell, “The Own Your Future Long-Term Care Awareness Campaign: Implications for CLASS,” CLASS
Technical Assistance Brief Series, Spring 2011, available at:
http://www.thescanfoundation.org/sites/default/files/TSF_CLASS_TA_No_13_Own_Your_Future_FINAL.pdf
.
100
Tell, “Own Your Future.”
101
Office of the Assistant Secretary for Planning and Evaluation, “Final Report.”

Long-Term Care Insurance: Recommendations for Improvement of Regulation 42
employees with saving for retirement.
102
While these concepts are promising, additional work
will be needed to develop specifics about how to effectively attain goals through these strategies.
Insurance industry organizations favor more federally-funded education. For example,
America’s Health Insurance Plans and the American Council of Life Insurers recommended re-
starting the Own Your Future Awareness Campaign, and the National Association of Insurance
and Financial Advisors similarly pointed to the value of such a campaign.
103
In 2018, the Maryland Governor’s Task Force on Long-Term Care Planning recommended
methods to educate residents about LTC. The group concluded that current workers should be a
key target of outreach and education, especially through employers, and young people should be
introduced to LTC planning early.
104
Industry stakeholders similarly identified employers as a
venue for effectively providing education about LTCI at the July 25, 2019 public meeting of the
Task Force. However, these recommendations reflect a wide variety of strategies and are not
backed by clear evidence of effectiveness or plans for implementation.
Task Force consultations with consumer advocates pointed to the challenges of LTCI education.
One group noted that insurance products, including LTCI, can be complex, and emphasized the
need for understandable, plain language information, and the need to train insurance and
investment professionals on appropriate application of suitability standards.
105
Another
consumer organization commented that promotion of stand-alone LTCI is not consistent with
government efforts to help consumers understand lifetime insurance and retirement income
needs.
106
Finally, a health policy group pointed to the value of personalized assistance with
navigating the care delivery system at critical points, such as before or after retirement.
107
Best Practices for Financial Education
The Financial Literacy Report details best practices for financial education that are applicable to
educating consumers about LTC planning and LTCI. These include:
• Provide Actionable, Relevant, and Timely Information. Delivering financial
information in an actionable, relevant, and timely manner results in greater likelihood of
102
“Retirement Security Working Group,” National Association of Insurance Commissioners Retirement Security
(A) Working Group, last modified November 2019, available at:
https://content.naic.org/sites/default/files/inline-
files/Taylor%20Retirement%20Security%20Work%20Plan%20November%202019a.pdf.
103
Treasury, “Public Comments,” America’s Health Insurance Plans, American Council of Life Insurers, and
National Association of Insurance and Financial Advisors.
104
Maryland Governor’s Task Force on Long Term Care Planning, Report of the Maryland Governor’s Task Force
on Long Term Care Planning (Annapolis: October 2018), available at:
http://dlslibrary.state.md.us/publications/NonMd/SB696Ch212HB953Ch213(2017)_2018.pdf
.
105
Treasury, “Public Comments,” California Health Advocates.
106
Treasury, “Public Comments,” Center for Economic Justice.
107
Treasury, “Public Comments,” Healthsperien.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 43
retention and action. This practice underscores the need for information that is clear and
provides actionable steps for the consumer at appropriate times in their decision-making.
• Build on Motivation. Effective financial literacy and education programs capitalize on
people’s motivations. This may mean that financial education on LTC planning could be
effectively delivered by trusted sources, such as faith-based or community
organizations.
108
• Make It Easy to Make Good Decisions and Follow Through. The environment or
context can make it easier for people to carry out their intentions. For example, changing
the options presented, removing hassles and barriers, and adding supports can help people
bridge the gap between intentions and actions. Simplifying options is often key to
helping people make good choices.
109
Recommendations: There is a clear need for consumers to plan for retirement and later life,
including consideration of LTC costs and how to finance those costs. Yet, decisions about these
topics are complex, unpredictable, and often made more challenging by social and emotional
hurdles to planning for possible disability. In addition, LTCI can be difficult to understand and
easy to avoid. These factors likely detract from the effectiveness of financial education focused
solely on LTC and LTCI. Rather, planning for LTC costs and ways to pay for them should be
included as part of other financial education on planning, saving, and investing for retirement.
The Task Force recommends that Treasury, HHS, DOL, and other agencies working through the
FLEC, assess federal education resources on LTC needs and planning, and modify, update, and
supplement these resources as needed.
110
As part of its efforts to improve consumers’ capability
in retirement planning, the FLEC should clearly integrate LTC planning into retirement
education topics. These efforts should be consistent with the recommendations and best
practices set forth in the Financial Literacy Report. In particular, educational programs and
materials should be clear, simple, avoid jargon, and point people to concrete actions that they can
take or avoid. Interagency cooperation is necessary in modifying, updating, and supplementing
resources, alongside coordination with private sector entities, state government agencies, and
other appropriate parties.
108
Although multiple stakeholders recommend that consumers make LTC decisions in consultation with family
members, a 2014 survey found that barely one-quarter of adults had a detailed discussion about LTC preferences
with a partner or family member. Benjamin Allaire et al., “Long-Term Care Awareness and Planning: What Do
Americans Want?” Office of the Assistant Secretary for Planning and Evaluation, July 30, 2015, available at:
https://aspe.hhs.gov/system/files/pdf/111341/Awareness.pdf
.
109
For the full list of best practices, see Treasury, Financial Literacy Report, 54-58.
110
Congress established the FLEC under the Fair and Accurate Credit Transactions Act of 2003 for the purpose of
coordinating the federal government’s financial literacy efforts.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 44
Tax Incentives
The Code currently provides favorable federal income tax treatment for LTCI. Multiple
stakeholders encouraged the Task Force to consider a range of amendments to tax laws or
regulations aimed at increasing the take-up of private LTCI. This section of the report begins
with an overview of current tax rules regarding LTCI, and then presents an analysis of various
tax proposals considered by the Task Force.
Current Tax Rules Regarding LTCI
The Code currently treats a “qualified” LTCI contract as an accident and health insurance
contract and provides various tax preferences.
111
For example, the Code permits individuals to
deduct premiums paid for LTCI under limited circumstances. It also permits employers to
provide LTCI to their employees on a pre-tax basis. The requirements for a LTCI contract to be
tax qualified and the current tax treatment of qualified LTCI are summarized below.
Requirements for Qualified LTCI Contracts
The Code defines a qualified LTCI contract as any insurance contract if the only insurance
protection provided under the contract is coverage of qualified long-term care services.
112
A
qualified LTCI contract also may not provide for a cash surrender value in excess of premiums
paid under the contract or provide other money that can be paid, assigned, pledged as collateral
for a loan, or borrowed.
113
As discussed in more detail below, premiums paid for a qualified
LTCI contract are eligible to be deducted as medical expenses, subject to specified, age-based
dollar limits. In addition, amounts received under the contract generally are excludable from
gross income as amounts received for personal injuries or sickness.
The Code defines qualified LTC services as necessary diagnostic, preventive, therapeutic,
curing, treating, mitigating, and rehabilitative services, and maintenance or personal care
services, which are required by a chronically ill individual, and are provided pursuant to a plan of
care prescribed by a licensed health care practitioner.
114
A “chronically ill individual” means any individual who has been certified by a licensed health
care practitioner as:
111
26 U.S.C. §7702B(a)(1).
112
26 U.S.C. §7702B(b).
113
In this regard, 26 U.S.C. §7702B(b)(2)(C) permits a refund that does not exceed the aggregate premiums paid
under the contract upon: (i) the death of the insured or (ii) a complete surrender or cancellation of the LTCI contract.
Any such refund must be includible in gross income to the extent that any deduction or exclusion from income was
allowed with respect to the premiums paid. See also 26 U.S.C. §7702B(b)(1)(D) (additional requirements for
qualified LTCI contracts).
114
26 U.S.C. §7702B(c)(1).

Long-Term Care Insurance: Recommendations for Improvement of Regulation 45
i. Being unable to perform (without substantial assistance from another individual) at least
two of six ADLs (eating, toileting, transferring, bathing, dressing, and continence) for a
period of at least 90 days due to a loss of functional capacity;
ii. Having a level of disability similar (as determined under regulations) to the level of
disability described in i.; or
iii. Requiring substantial supervision to protect such individual from threats to health and
safety due to severe cognitive impairment.
115
Tax Treatment of LTCI Premium Payments by Individuals
Under current law, qualified LTCI premiums are eligible to be deducted as medical expenses
only to the extent that total medical expenses, including qualified LTC expenses, exceed the
threshold of adjusted gross income (AGI). Currently, the threshold is 7.5% of AGI.
116
The
annual amount of LTCI premiums that qualify as medical expenses is capped at an age-
dependent amount indexed for inflation. This cap on LTCI premiums (Age-Dependent Cap) is
applied before calculating whether total eligible medical expenses exceed 7.5% of AGI.
117
Table 4: 2020 Age-Dependent Caps
Age at End of Tax Year Maximum LTCI Premium Deduction
40 or less $430
41 to 50
$810
51 to 60 $1,630
61 to 70
$4,350
Over 70 $5,430
Further, an individual taxpayer may claim a medical expense deduction only if itemizing
deductions on Schedule A of Form 1040. The Tax Cuts and Jobs Act almost doubled the
standard deduction amount for tax years beginning after December 31, 2017.
118
Standard
deductions for 2020 are:
• $12,400 if the taxpayer is single or uses married filing separately status,
• $24,800 if the taxpayer is married and files a joint return with spouse, and
115
26 U.S.C. §7702B(c)(2).
116
For tax years beginning on or after January 1, 2021, the AGI threshold for deducting medical expenses will
increase to 10% unless Congress chooses to extend the 7.5% threshold. See 26 U.S.C. §213(a) and (f).
117
26 U.S.C. §213(d)(10).
118
U.S. House, H.R.1 – An Act to Provide for Reconciliation Pursuant to Titles II and V of the Concurrent
Resolution on the Budget for Fiscal Year 2018 (115th Congress, December 2017).

Long-Term Care Insurance: Recommendations for Improvement of Regulation 46
• $18,650 if the taxpayer is a head of household.
Thus, in order to deduct LTCI premium payments under the existing rules, a taxpayer must have
a proportionally large amount of medical expenses (to meet the 7.5% of AGI threshold) and have
sufficient additional itemized deductions for itemizing to be tax-advantageous. As an example, a
married couple filing jointly for the 2020 tax year that earns $100,000 in annual income may
include medical expenses in itemized deductions only to the extent that they exceed $7,500 in
2020. In addition, unless the couple’s total medical expenses were in the range of 32.5% of AGI,
or $32,500, they would need additional itemizable deductions in order for itemizing to be
economically advantageous. The increased standard deduction is more tax-advantageous than
itemizing for many taxpayers.
For the 2017 tax year (the latest year for which data is available), approximately 10 million tax
returns claimed an itemized medical deduction.
119
It is likely that this number will decrease for
the 2018 tax year, given the increase in the standard deduction. The extent to which LTCI
premiums are a component of the itemized medical deduction is not known, but it may be
relatively uncommon. Individuals in poor health are less likely to qualify for LTCI protection
due to medical underwriting for these policies, and individuals in good health may be unlikely to
incur enough out-of-pocket medical expenses to exceed the 7.5% of AGI threshold, particularly
if they have employer-provided health insurance and pay their own share of health insurance
premiums pre-tax.
Restrictions on Retirement Account Distributions
Distributions from qualified retirement plans (such as 401(k) and 403(b) plans and IRAs) prior to
age 59½ generally are subject to an additional 10% tax on the amount of the distribution,
although certain exceptions apply.
120
The exceptions include distributions to pay premiums for
LTCI under two circumstances:
i. Qualified LTCI premiums (up to the Age-Dependent Cap amount) can be paid with
401(k), 403(b), or IRA distributions with no additional early withdrawal tax to the extent
that, in combination with other out-of-pocket medical expenses, they exceed the
threshold for deductible medical expenses.
121
It is not necessary to itemize deductions for
tax return purposes to obtain this additional tax relief. However, taxpayers would still
need relatively high total medical expenses to take advantage of this exception.
ii. Qualified LTCI premiums (up to the Age-Dependent Cap amount), as well as other health
insurance premiums, can be paid with IRA (but not 401(k) or 403(b)) distributions with
no additional early withdrawal tax if the policyholder experiences a substantial period of
119
“Individual Income Tax Returns Complete Report 2017,” Internal Revenue Service, 91, available at:
https://www.irs.gov/pub/irs-pdf/p1304.pdf
.
120
26 U.S.C. §72(t)(1).
121
26 U.S.C. §72(t)(2)(B).

Long-Term Care Insurance: Recommendations for Improvement of Regulation 47
unemployment, regardless of whether the taxpayer’s total medical expenses exceed the
threshold for deductible medical expenses.
122
This provision can help taxpayers keep up
with LTCI premiums when the loss of a job interrupts disposable income.
In 2016, a majority of families at relevant ages held retirement accounts (IRAs, 401(k)s, and
403(b)s), including 57% of those headed by someone age 35-44, 60% age 45-54, and 59% age
55-64. Among those holding accounts, the median amounts held at these same ages were
$37,000, $83,000, and $120,000, respectively.
123
These amounts are quite low compared to
projected retirement income needs. For example, at the federal employee Thrift Savings Plan
annuity rate, $120,000 at age 65 would provide a level annuity of $7,488 each year for life.
124
Tax Treatment of LTCI Purchases in the Employment Context
The costs of employer-provided accident and health plans are excluded from employees’ gross
income and tax-qualified LTCI qualifies as an accident and health plan for this purpose (although
the employer’s deduction for premiums paid is limited to the Age-Dependent Cap).
125
Accordingly, employers can currently provide LTCI to employees tax-free. However, employers
cannot currently offer LTCI as part of a cafeteria plan, which is a common vehicle for providing
employees with benefits for which the employer does not incur additional costs.
Cafeteria plans (often incorporating a flexible spending arrangement (FSA), discussed below)
provide employees an opportunity to substitute a portion of their taxable cash compensation with
one or more qualified benefits on a pre-tax basis.
126
If an employee chooses to receive a
qualified benefit under a cafeteria plan, the fact that the employee could have received cash or a
taxable benefit instead will not make the qualified benefit taxable. Under current law, qualified
benefits include most accident and health insurance benefits, including insurance policy
purchases, adoption assistance, dependent care assistance, group term life insurance, and health
savings accounts (HSA) (including the ability to use HSA funds to pay for qualified LTC
services). However, cafeteria plans may not offer LTCI.
127
122
Generally, the relief from the additional early withdrawal tax applies if the individual receives unemployment
compensation for 12 consecutive weeks under a federal or state unemployment compensation law in the current year
(or received it in the preceding year) and the relief extends to distributions for up to 60 days after employment
resumes. A self-employed individual may be treated as meeting this requirement if the individual would have
received unemployment compensation under federal or state law but for the fact that the individual was self-
employed. See 26 U.S.C. §72(t)(2)(D).
123
“Survey of Consumer Finances – 2016 SCF Chartbook,” Board of Governors of the Federal Reserve System,
October 16, 2017, 442, available at: https://www.federalreserve.gov/econres/files/BulletinCharts.pdf. The Board of
Governors of the Federal Reserve System conducts the Survey of Consumer Finances every three years. The Board
has not yet published the 2019 survey.
124
Calculated at the current 1.75% interest rate assumption.
125
See 26 U.S.C. §106(a).
126
See 26 U.S.C. §125(f)(1).
127
See 26 U.S.C. §125(f)(2).

Long-Term Care Insurance: Recommendations for Improvement of Regulation 48
A Health FSA may be established under an employer’s cafeteria plan, either as one of several
components or as the sole component. Health FSAs are accounts funded each year with pre-tax
income (i.e., income that is not subject to federal income and payroll tax) that may be used to
pay for qualified medical expenses during the relevant year that are not reimbursable by health
insurance or otherwise. Most common uses are to cover health insurance policy deductibles and
co-pays, as well as qualified medical expenses that may not be covered by insurance, such as
vision care. The annual Health FSA funding cap is indexed for inflation, and the maximum
contribution for 2020 is $2,750. A Health FSA differs from an HSA (discussed below) in that
HSA balances carry over in full from year to year and can earn tax-free investment income,
whereas Health FSA annual contributions are generally “use or lose,” with the exception of a
permissible grace period or carryover limit. An employer may either choose to allow Health
FSAs a two and a half month grace period at the end of the plan year so that account holders can
use their remaining Health FSA balance to pay for expenses incurred during that extended
period, or choose to allow account holders to carry over an amount equal to 20 percent of the
maximum salary reduction contribution for any given plan year ($550 for the 2020 plan year).
Health FSA balances do not accrue interest. Under current law, insurance premium payments,
including LTCI premiums, are not eligible expenses for Health FSAs.
An HSA is a tax-advantaged medical savings account available to taxpayers who enroll in a
high-deductible health plan (HDHP). The funds contributed to an HSA are not subject to federal
income tax at the time of deposit. Annual contributions in 2020 are limited to $3,550 for an
individual and $7,100 for a family, with HSA holders age 55 and over being allowed to
contribute an additional $1,000 per year. Further, individuals eligible for Medicare cannot
contribute to HSAs. Around 22 million people held an HSA-qualified HDHP in 2017.
128
HSAs (in combination with an HDHP) are also available to persons who are self-employed or to
persons whose employer does not offer a health plan, but most often are offered in conjunction
with an employer-sponsored HDHP.
Analysis of Tax Incentives Considered
Based on the NAIC 2017 List (Options 1, 2, 4, and 8) and stakeholder feedback, the Task Force
considered the following additional tax incentives to encourage the purchase of LTCI:
• Allow a full federal tax deduction for LTCI premiums paid by individuals.
• Allow increased contributions to an HSA if the HSA is used to fund LTCI premiums.
• Create a new type of account modeled after HSAs (but without the requirement that the
account holder have an HDHP) that could be used to fund both direct LTC expenses and
LTCI premiums.
128
“Health Savings Accounts and Consumer-Directed Health Plans Grow as Valuable Financial Planning Tools,”
America’s Health Insurance Plans, April 2018, available at:
https://www.ahip.org/wp-
content/uploads/2018/04/HSA_Report_4.12.18-1.pdf.
Long-Term Care Insurance: Recommendations for Improvement of Regulation 49
• Allow purchase of LTCI through cafeteria plans offered by employers.
• Allow purchase of LTCI through Health FSAs.
• Allow cash value beyond a return of premium under qualified LTCI contracts.
• Allow retirement plan participants to receive a distribution from 401(k)s, 403(b)s, or
IRAs to purchase LTCI with no additional early withdrawal tax.
Recommendation: In its analysis of these proposed incentives, the Task Force took into account
that the Code already provides favorable income tax treatment to LTCI. The Task Force
recognizes that the proposed incentives could have the beneficial effect of motivating individuals
to plan their financial future and help protect their retirement savings against depletion by LTCI
expenses. However, the proposals would likely reduce tax revenues and the amount of the
reductions could be significant. In addition, the proposals would primarily benefit higher income
taxpayers with higher marginal tax rates, and may not be fully effective in targeting lower- and
middle-income families who need financial protection against LTC risks. Finally, the proposals
would increase the complexity of the Code and could, in some cases, be difficult to implement,
monitor, and enforce. Accordingly, the Task Force does not recommend adoption of any of the
proposed additional tax incentives, with the exception of the proposal to eliminate the early
withdrawal tax if funds from an IRA, 401(k), or 403(b) account are used to pay LTCI premiums.
Federal Income Tax Deduction for LTCI Premiums
The Code currently allows taxpayers to deduct a limited set of expenses “above the line” from
their gross income. These deductions, which reduce AGI, are available irrespective of whether a
taxpayer claims the standard deduction or itemizes deductions. The permitted above the line
expense deductions are mostly business expenses or other expenses incurred for the production
of income, but include other categories of expenses, such as IRA contributions, HSA
contributions, and student loan interest expense deductions. The Task Force considered a
proposal to add LTCI premiums (with or without Age-Dependent Caps) as an above the line
deduction category.
The argument in support of this proposal is that the current rules regarding LTCI premium
deductions do not provide an incentive to purchase LTCI for most individual taxpayers, because
(1) most taxpayers take the standard deduction rather than itemize, and (2) only medical
expenses in excess of the AGI threshold (7.5%) may be deducted as an itemized deduction—a
threshold not reached by most taxpayers who itemize deductions.
However, from a tax policy perspective, an above the line tax deduction is a very significant
subsidy that would decrease tax revenue. Although increasing the number of U.S. persons with
LTCI may be desirable, it is debatable whether LTCI premiums should have a privileged
deductibility status compared to other medical expenses (which are subject to the 7.5% AGI cap)
and other expense categories (such as the charitable contribution deduction) that cannot be
deducted unless the taxpayer itemizes. As previously discussed, the Tax Cuts and Jobs Act

Long-Term Care Insurance: Recommendations for Improvement of Regulation 50
almost doubled the standard deduction for individual taxpayers. The standard deduction
simplifies tax filing by not requiring taxpayers to track which of their expenses may be claimed
as itemized deductions. A separate deduction for LTCI premiums would increase complexity
and largely benefit higher-income taxpayers.
Increased Contributions to an HSA to Fund LTCI Premiums
The Task Force considered a proposal to allow increased contributions to an HSA if the HSA is
used to fund LTCI premiums. Because HSA funds may already be used to purchase LTCI (up to
the Age-Dependent Cap amounts), this proposal would increase the overall HSA contribution
allowed (currently capped at $3,550 for an individual and $7,100 for a family, plus an additional
$1,000 for HSA holders age 55 and over) if the HSA is used to purchase LTCI. This proposal
would make LTCI more affordable for persons with HSAs who are already maximizing their
HSA contributions and could stimulate demand for private purchases of LTCI.
However, HSA contribution limits are already high and the tax treatment for HSAs is currently
the most generous treatment for health care expenses because it is mathematically equivalent to
combining tax-free build-up on earnings with an above-the-line deduction for medical care. For
individuals who use their HSAs to fund medical care a few years in the future, the tax-free build-
up on earnings is relatively modest. For LTC, where the build-up can occur over decades, the
tax-free build-up on earnings combined with tax-free contributions and withdrawals for qualified
LTCI or LTC services already provide a substantial tax subsidy.
Furthermore, this proposed change would be likely to primarily benefit persons with relatively
high incomes who can afford larger HSA contributions, rather than lower- or middle-income
taxpayers, since this proposal would affect only individuals who already contribute the
maximum annual amount to HSAs (e.g., $7,100 yearly for a family). In addition, the proposal
would only help individuals with HSAs, which are limited to those with HDHPs.
129
Individuals
eligible for Medicare, who might be more likely to take advantage of this new rule, cannot
contribute to HSAs.
New Type of Account to Fund LTC Expenses and LTCI Premiums
The Task Force considered a proposal to create a new type of account modeled after HSAs,
without the requirement that the account holder have a HDHP, which could be used to fund
direct LTC expenses and LTCI premiums on a pre-tax basis (a LTC savings account (LTCSA)).
If the HSA model were followed, distributions from an LTCSA would receive more generous tax
treatment than distributions from other retirement savings accounts because a distribution from a
401(k), 403(b), or IRA is generally included in income at least in part; in addition, any deduction
for medical expenses (including qualified LTC expenses) would be subject to the 7.5% AGI
129
Approximately 22 million people held an HSA-qualified HDHP in 2017. America’s Health Insurance Plans,
“Health Savings Accounts,” available at:
https://www.ahip.org/wp-content/uploads/2018/04/HSA_Report_4.12.18-
1.pdf.
Long-Term Care Insurance: Recommendations for Improvement of Regulation 51
floor for medical expenses deductions and would not be available to taxpayers who itemize. By
contrast, a distribution from the LTCSA would be tax-free, provided it was used to pay LTC
premiums (up to the Age-Dependent Cap) or other LTC expenses.
This proposal could increase saving for LTC expenses generally, if the contribution limits for
LTCSAs did not affect the limits for retirement savings accounts. Because the benefit would not
be limited to persons with HDHPs, it could incentivize LTCI purchases by a larger number of
taxpayers than the proposal to increase HSA contribution limits.
However, because the new LTCSA would be available to all taxpayers, and not just taxpayers
with HDHPs, the tax revenue impact of this proposal would be correspondingly larger.
Availability of the LTCSA would potentially provide a large tax subsidy that likely would
benefit mainly higher income taxpayers because individuals with high marginal tax rates are
most likely to take advantage of this type of account.
With respect to the use of the LTCSA to pay LTC expenses (as opposed to insurance premiums),
there is not always a clear line between an LTC expense and post-retirement living expenses
generally, and people cannot know in advance whether they will need LTC. It may be
advantageous for most taxpayers to contribute more robustly to existing retirement accounts than
to isolate a stream of savings specifically for LTC expenses when there is no guarantee that a
particular taxpayer will incur expenses that clearly qualify as LTC expenses. In addition, if the
LTCSA were allowed, taxpayers would have an incentive to characterize a larger amount of
expenses as LTC expenses because LTCSA distributions would often receive more generous tax
treatment than distributions from retirement accounts. Federal tax authorities would need to
monitor appropriate use and develop rules regarding how to treat unused LTCSA balances, if a
taxpayer does not need LTC.
Purchase of LTCI Under Cafeteria Plans
The Task Force considered a proposal to allow employers to add tax-qualified LTCI to the group
of qualified benefits that employees may receive on a pre-tax basis under a cafeteria plan. Under
this proposal, LTCI premium exclusions from income could be limited based on the current Age-
Dependent Caps.
Under current law, employers can provide LTCI to employees outside of a cafeteria plan,
although not very many employers do so. If employers could provide LTCI through a cafeteria
plan, they might be more likely to offer it. Employees might be more likely to opt to purchase
LTCI offered on a pre-tax basis under a cafeteria plan. Employers also might be able to
negotiate more favorable product terms than an individual could obtain independently. Allowing
the offer of LTCI on a pre-tax basis within cafeteria plans would further encourage employers to
include information about LTC options in their employee benefits packages.
Like any tax incentive, this proposal would decrease tax revenue to the extent that additional
employees purchased LTCI through their cafeteria plan. Higher income taxpayers may be most
Long-Term Care Insurance: Recommendations for Improvement of Regulation 52
likely to take advantage of this new cafeteria plan option, as they can better afford to purchase
LTCI, whether on a pre- or post-tax basis.
Employers can already provide LTCI to their employees on a pre-tax basis outside of cafeteria
plans. It seems unlikely that a statutory change permitting employers to offer LTCI as a pre-tax
option within a cafeteria plan would also cause employers to make additional contributions to the
cafeteria plan to help fund the employees’ purchase. If so, the cost of the LTCI cafeteria plan
offering would still come out of employee pockets (although it would be on a pre-tax basis).
Purchase of LTCI Through Health FSAs
The Task Force considered a proposal to add tax-qualified LTCI to the group of expenses that an
employee can pay with Health FSA funds, subject to Age-Dependent Caps on LTCI premium
payments. Allowing the funding of LTCI on a pre-tax basis through Health FSAs could
encourage purchase of LTCI.
One purpose of Health FSAs is to help fund medical expenses not covered by insurance (e.g.,
deductibles and co-pays). The maximum annual contribution to Health FSAs is only $2,750 (for
2020), and allowing Health FSA contributions to cover premiums would reduce amounts
available to meet the types of costs that Health FSAs were intended to cover. Unless other types
of insurance premiums were also eligible for payment from a Health FSA, the proposal would
privilege LTCI over other types of insurance. In addition, higher income taxpayers may be most
likely to take advantage of the option to use Health FSA contributions to fund LTCI because they
can better afford it, even on a pre-tax basis.
Cash Value Under Qualified LTCI Contracts
Under current law, a qualified LTCI contract generally may not provide for a cash surrender
value or other money that can be paid, assigned, pledged as collateral for a loan, or borrowed.
As a limited exception, a qualified LTCI contract may provide for a refund that does not exceed
the aggregate premiums paid on the death of the insured, complete surrender, or cancellation of
the contract. Any such refund is includible in gross income to the extent that any deduction or
exclusion was allowable with respect to the premiums paid. In addition, premium refunds and
dividends credited while the contract is in force may be used to reduce future premiums or
increase future benefits, but may not be paid out to the policyholder.
The Task Force considered a proposal to allow cash value beyond a return of premium under
qualified LTCI contracts. Cash value or cash surrender value is the amount of money the
insurance company is obligated to pay a policyholder or beneficiary if a life insurance or annuity
contract is terminated. Policyholders also may be able to borrow against or otherwise benefit
from the cash value. If the Code permitted qualified LTCI to accumulate cash value, LTCI could
be more attractive because policyholders could receive a benefit (cash value withdrawal) even if
they did not become chronically ill.
Long-Term Care Insurance: Recommendations for Improvement of Regulation 53
However, if a qualified LTCI contract were permitted to have cash surrender value beyond the
limited return of premium currently allowed, it would to that extent be an investment vehicle and
more closely resemble a type of life insurance contract than an accident and health insurance
contract. While the Code permits earnings on life insurance and annuity contracts with cash
value generally to accumulate tax-free, it generally does not permit policyholders to deduct
premiums paid for life insurance or annuity contracts. Policyholders are also required to pay
taxes on the investment component of distributions made under life insurance and annuity
contracts (other than payment of death benefits under life insurance contracts). Congress
imposed the current cash value restrictions on qualified LTCI in exchange for permitting LTCI to
receive some of the more favored tax treatment provided to health insurance premium payments,
including deductions for premium payments under some circumstances and tax-free treatment of
policy benefits when received. Allowing qualified LTCI to have substantial cash value would
give it more of a life insurance character and undermine the rationale for the tax-favored
treatment currently accorded to qualified LTCI.
Receiving 401(k), 403(b), or IRA Distributions to Purchase LTCI
The Task Force considered a proposal to allow retirement plan participants to receive
distributions from 401(k)s, 403(b)s, or IRAs to purchase LTCI with no additional early
withdrawal tax. This could be accomplished by adding a new exception to the Code to fully
exempt distributions from 401(k)s, 403(b)s, and IRAs used to purchase LTCI from the 10%
additional income tax. The retirement account distributions in many cases would still be subject
to regular income tax (depending on whether the taxpayer’s retirement account contribution was
originally made pre-tax or post-tax), but the additional early withdrawal tax would not apply.
The proposal could lower an obstacle to LTCI affordability (or perceived affordability) for some
individuals with retirement savings but limited disposable income.
In some cases, the proposal may provide little or no true economic advantage over using current
income to pay LTCI premiums. For example, there would be no economic difference for active
401(k) or 403(b) participants who are contributing more than needed to receive the maximum
employer matching contributions (and to any active IRA contributor) between taking a
distribution and alternatively redirecting some contributions to LTCI premiums. On the other
hand, individuals who wish to contribute just enough to their 401(k) or 403(b) plan to receive the
maximum employer matching contribution, but who also have limited funds available to pay
LTCI premiums, might be more likely to purchase LTCI if they had the option of receiving an
early distribution of previously-contributed funds without the additional 10% early withdrawal
tax.
Arguments against the proposal include the concerns that too many Americans have insufficient
retirement savings, an individual who diverts funds otherwise earmarked for retirement income
to LTCI could erode retirement security, and the proposed exemption would not benefit the large
minority of families without retirement accounts.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 54
Given that the Code provides exceptions to the additional 10% early withdrawal tax for the
purchase of LTCI insurance in certain circumstances already (including as medical expenses
above the itemized medical deduction floor regardless of whether an itemized deduction is
claimed, as well as health insurance and LTCI premiums for unemployed individuals),
130
the
Task Force recommends that the Code be amended to allow retirement plan participants to
receive distributions from 401(k)s, 403(b)s, or IRAs to purchase LTCI with no early withdrawal
tax. This change may make it easier for some individuals with retirement savings, but limited
disposable income, to pay LTCI premiums, and the individuals most likely to take advantage of
the early distribution option may be individuals in their mid-to-late 50s when LTCI premiums
are becoming more expensive, but the individuals are not yet age-eligible to take ordinary
retirement account distributions. This recommendation will likely have a minimal effect on tax
revenues as taxpayers most likely to purchase long-term care insurance could avoid the penalty
by reducing contributions to these accounts, reducing other consumption, or borrowing.
130
26 U.S.C. §72(t)(2)(B) and (D).

Long-Term Care Insurance: Recommendations for Improvement of Regulation 55
Alternative Financing Approaches
This section briefly reviews proposals for public insurance approaches to reform in the United
States organized around the structure of the benefit and how it protects individuals from the
financial risk of needing LTC. Most of these approaches focus on either front-end insurance
(coverage of initial LTC costs for mostly short durations or limited scope) or back-end, or
catastrophic, insurance (coverage beyond a specified level of need or cost for longer durations).
Very few options provide comprehensive coverage of the entire spectrum of LTC risk. In
addition, this review is limited to proposals and approaches that include detailed descriptions of
major program features such as program eligibility, scope of coverage, and, most importantly,
financing and cost estimates. The Task Force has not attempted to review in detail conceptual
proposals and ideas that are not supported by specific financing and cost estimates.
Front-End Benefit Options
Options that address initial LTC costs are frequently referred to as front-end coverage
benefits.
131
These options are also typically limited in their duration of coverage. Option 9
under the NAIC 2017 List is a good example of a type of front-end benefit. Specifically, this
option recommends that policymakers:
Explore adding a home care benefit to Medicare or Medicare Supplement and/or
Medicare Advantage plans. Medicare provides extensive acute care coverage but more
limited post-acute coverage (home health and skilled nursing facility care). Medicare
Advantage and Medigap plans fill the gaps in Medicare coverage. But most LTC
services are not covered by Medicare, leaving a considerable gap in coverage for post-
acute care… There has been discussion of adding either something akin to a long-term
care benefit or, less extensive, new home and community-based benefits either to
Medicare (which would affect supplemental carriers) or to Medicare Advantage and/or
Medigap plans.
Establishing a home care benefit, a type of front-end insurance option that addresses initial needs
for LTC services, has been an objective of policymakers for decades. For example, the 1993
Health Security Act included a state-run home care program for persons with disabilities that
would be funded largely through federal grants. Rather than establishing a new, completely
independent program, a 2016 report
132
recommended adding a home-care benefit to Medicare or,
like Option 9, including it as part of Medicare Supplement Insurance (such as Medigap) policies
or Medicare Advantage (MA).
131
Melissa M. Favreault, Howard Gleckman, and Richard W. Johnson, “Financing Long-Term Services and
Supports: Options Reflect Trade-Offs for Older Americans and Federal Spending,” Health Affairs 34, no. 12
(December 2015): 2181–91, available at: https://www.healthaffairs.org/doi/full/10.1377/hlthaff.2015.1226
.
132
Karen Davis, Cathy Schoen, and Amber Willink, “Medicare Help At Home,” Health Affairs, April 2016,
available at: https://www.healthaffairs.org/do/10.1377/hblog20160413.054429/full/
.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 56
The home-care benefit proposal would pay for 20 hours per week of home care and other
services for Medicare beneficiaries with two or more limitations in ADL or severe cognitive
impairment, a benefit trigger similar to that for tax-qualified LTCI policies. Like Medicare
Supplement Insurance, people turning age 65 who are eligible for Medicare would have the
option to enroll in the program without medical underwriting. The home care benefit would be
financed through a combination of co-insurance varying by income, beneficiary premiums, and a
payroll tax. Beneficiaries would have a co-pay requirement ranging from 5% of the cost of
service for low-income beneficiaries to 50% for those with income greater than 400 percent of
the federal poverty level. The 2016 report estimated that a monthly premium of $35 and a
payroll tax of 0.35% paid by both employer and worker would cover the public costs of the
program under specific assumptions.
133
One of the policy options explored by the Bipartisan Policy Center in their 2017 report is the
provision of a limited home care benefit through Medigap or MA plans.
134
The basic structure
of the benefit is similar to the home-care benefit proposal with some significant differences. For
example, the amount of the daily benefit available to pay for services is much higher, $100 per
day, but is limited to one year. In addition, enrollees are not eligible to receive a benefit until 90
days after a documented need for LTC. Most importantly, private insurers rather than the
government provide the benefit and the program is financed exclusively through premiums paid
after voluntary enrollment in the program. Assuming a discount rate of 3% and a loss ratio of
85%, estimated monthly premium costs range from $55 if all eligible beneficiaries enroll at age
65 to approximately $200 if only 5% enroll at that age. Although the Bipartisan Policy Center
does not specify the participation rate, it estimates that reducing the benefit to $75 per day and
increasing the elimination period to 180 days could result in monthly premiums of $35 to $40.
Washington State’s Long-Term Services and Supports Trust Program
In 2019, Washington State passed a public LTCI program, the Long-Term Services and Supports
Trust Program.
135
Beginning in 2025, the program will pay, per individual, up to $36,500 of
LTSS received from approved providers. The list of services that can be reimbursed is quite
broad and includes services and equipment provided in the community (e.g., in-home personal
care, adaptive equipment and technology, home modifications, respite for family caregivers,
home delivered meals, transportation, etc.) as well as those provided in assisted living and
nursing facilities. The program will be funded through a mandatory payroll tax of 0.58% on
133
These estimates assume that home care services cost approximately $20 per hour ($15 per hour plus 33% for
fringe benefits) and that 75% of those eligible for the home care benefit who are not already on Medicaid would
participate each year. Benefits would, therefore, cost up to $400 per week or $20,800 per year.
134
“Financing Long-Term Services and Support: Seeking Bipartisan Solutions in Politically Challenging Times,”
Bipartisan Policy Center, July 2017, 22-24, available at:
https://bipartisanpolicy.org/wp-
content/uploads/2019/03/BPC-Health-Financing-Long-Term-Services-and-Supports.pdf.
135
Washington State Legislature, Title 50B Long-Term Care – Chapter 50B.04 RCW: Long-Term Services and
Supports Trust Program (Olympia: 2019).

Long-Term Care Insurance: Recommendations for Improvement of Regulation 57
employees. Self-employed workers may opt into the program, while persons with LTCI could
choose not to participate. Payroll tax withholding is scheduled to begin in 2022.
In order to be a qualified program participant, an individual must have paid the payroll tax for
ten years (without interruption for five consecutive years) or three years within the last six, and
worked at least 500 hours during each of those years. Once qualified, an individual is eligible to
receive a benefit if he or she is 18 years or older, was not disabled before the age of 18, is a
Washington State resident, and requires assistance with at least three ADLs. Because the
legislation did not identify specific ADLs, eligibility criteria could be more or less restrictive
than those for tax-qualified LTCI. The lack of consistency between the two sets of eligibility
criteria will likely create a barrier to the development of private insurance that supplements the
benefits of the new program.
In November 2019, a nonbinding advisory measure was included on the state’s general election
ballot and voters voted against the idea of paying a new tax on wages to fund the program. A
media representative for the Washington State Office of the Insurance Commissioner said the
vote was an advisory measure that would not affect the enacted legislation.
136
Medicare Advantage
The Bipartisan Budget Act of 2018 amended Section 1852(a) of the Social Security Act to
expand the types of supplemental benefits that may be offered by MA plans to chronically ill
enrollees.
137
These benefits, referred to as Special Supplemental Benefits for the Chronically Ill
(SSBCI), include supplemental benefits that are not primarily health-related and may be offered
non-uniformly to eligible chronically ill enrollees. The purpose of the new category of
supplemental benefits is to enable MA plans to better tailor benefit offerings, address gaps in
care, and improve health outcomes for the chronically ill population.
As a result of these changes, beginning in 2020 many MA plans are allowed to cover certain
“non-primarily health related” items or services as a supplemental benefit for certain
beneficiaries. This includes adult day health care, home based palliative care, caregiver support,
in-home support services, transportation, and general supports for living, food, and other
expenses.
138
In general, MA organizations have broad discretion in developing items and
services they may offer as SSBCI, if the item or service has a reasonable expectation of
improving or maintaining the overall health or overall function of the chronically ill enrollee.
136
Allison Bell, “Wash. State Continues Public LTCI Effort, in Spite of Ballot Measure Results,” ThinkAdvisor,
November 2019, available at:
https://www.thinkadvisor.com/2019/11/26/wash-state-continues-public-ltci-effort-in-
spite-of-ballot-measure-results/.
137
U.S. House, H.R. 1892 – Bipartisan Budget Act of 2018 (115th Congress, February 2018).
138
“Implementing Supplemental Benefits for Chronically Ill Enrollees,” Centers for Medicare & Medicaid Services,
April 24, 2019, available at:
https://www.cms.gov/Medicare/Health-
Plans/HealthPlansGenInfo/Downloads/Supplemental_Benefits_Chronically_Ill_HPMS_042419.pdf.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 58
Furthermore, MA organizations have broad discretion in determining what may be considered “a
reasonable expectation” when choosing to offer specific items and services as SSBCI.
While the 2018 legislation provides increased flexibility to MA plans, it does not change the
payment structure used to finance supplemental benefits. Medicare pays MA plans a capitated
amount to provide all Medicare Part A and B benefits. Plans submit bids every year in each
county of operation and each bid is compared to a payment area’s benchmark, which is the
maximum amount that Medicare will pay MA plans in that area. CMS also risk adjusts the
benchmark base rate payments for each enrollee to account for various demographic and health
status differences. If a plan bids below the benchmark, the plan and Medicare split the difference
(with the plan’s share known as the “rebate”) between the bid and the benchmark. The rebate
must be used to lower out-of-pocket costs, provide supplemental benefits, or both. If a plan bids
above the benchmark, enrollees pay the difference between the bid and the benchmark in the
form of a monthly premium in addition to the Part B premium.
139
Back-End (Catastrophic) Options
Back-end, or catastrophic, coverage options mitigate the risk of long durations of LTC and
associated high costs. This approach addresses the risk of an unlikely, but potentially very costly
and financially ruinous, event. An advantage to focusing on the tail of the risk distribution is that
the cost of the insurance should be lower than other more comprehensive approaches. Several
advocacy and non-partisan organizations have supported, at least in principle, the development
of a catastrophic coverage option, and a 2018 paper proposed and modeled a detailed
catastrophic insurance option.
140
The latter effort is notable because it is one of the few
catastrophic reform efforts to estimate the cost of the program and explore distributional impacts.
The authors of the 2018 paper maintained that a public catastrophic insurance option could
provide a platform for private insurers to offer supplemental policies that in combination would
provide more comprehensive coverage. Their proposed program is structured around a lifetime
$110 per day cash benefit that would be available once enrollees had a demonstrated need for
services beyond a specified duration. The 2018 paper referred to this duration as an “income-
139
“Medicare Advantage,” Kaiser Family Foundation, last modified June 2019, available at:
https://www.kff.org/medicare/fact-sheet/medicare-advantage/
.
140
See, e.g., Treasury, “Public Comments,” America’s Health Insurance Plans and American Council of Life
Insurers; Bipartisan Policy Center, “Financing Long-Term Services and Support;” Treasury, “Public Comments,”
California Health Advocates; Marc Cohen, Melissa Favreault, and Judith Feder, “A New Public-Private Partnership:
Catastrophic Public and Front-End Private LTC Insurance,” LeadingAge LTSS Center @UMass Boston, Urban
Institute, and Office of the Assistant Secretary for Planning and Evaluation, last modified January 2018, available at:
https://www.urban.org/research/publication/new-public-private-partnership-catastrophic-public-and-front-end-
private-ltc-insurance; “A Consensus Framework for Long-Term Care Financing Reform,” Convergence Center for
Policy Resolution, last modified February 2016, available at: https://www.convergencepolicy.org/wp-
content/uploads/2016/02/LTCFC-FINAL-REPORT-Feb-2016.pdf; U.S. Senate, Commission on Long-Term Care:
Report to Congress (September 2013), available at: https://www.govinfo.gov/content/pkg/GPO-
LTCCOMMISSION/pdf/GPO-LTCCOMMISSION.pdf.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 59
related waiting period” ranging from one to four years depending on an enrollee’s lifetime
income.
141
The waiting period would begin once an enrollee met the same criteria for LTC
needs found in tax-qualified LTCI policies, i.e., need for assistance with two or more ADLs or
severe cognitive impairment. A surcharge on the Medicare payroll tax paid by workers age 40
and older would finance the benefit. The program would be phased in over ten years and
enrollees would be eligible for benefit after having paid the requisite payroll tax for 40 quarters.
Assuming an average waiting period of 2.2 years, the 2018 paper estimated that the program
could be funded with a payroll tax surcharge of 1%. Approximately one-third of enrollees would
eventually receive benefits, and payouts would cover 31% of all LTC costs. Compared to the
current system, the new program would lead to an increase in overall LTC spending, but family
out-of-pocket costs would decline by 15% and spending for Medicaid would be 25% lower,
according to the authors.
Comprehensive Options
Recent LTC reform efforts have generally not focused on covering the full risk and cost of LTC
services. The few full risk options have largely been conceptual and lack critical program
details, such as specific financing mechanisms and cost estimates. For example, the 2013 Report
to Congress of the Commission on Long-Term Care outlined a comprehensive Medicare benefit
for LTSS as a model of what can achieved through social insurance.
142
Enrollees would be
eligible for benefits under roughly the same criteria as those for tax-qualified private LTCI, and
an increase in the Medicare payroll tax and premiums would finance the program. However, this
report discussed neither the scope of benefits nor the requisite tax rates and premium amounts.
In fact, the Commission did not agree on a financing mechanism for any of its proposals and thus
made no formal recommendation.
Recommendation: The Task Force does not recommend pursuing any particular alternative
financing approach at this time. Policymakers and stakeholders should continue to develop,
monitor, and analyze LTC and LTCI reform proposals—including those discussed in this
report—to better understand the advantages and disadvantages of specific options, tradeoffs,
program costs, and distributional impacts.
141
The specific waiting period schedule is one year for enrollees with lifetime income in the lowest two income
quintiles, two years if one’s lifetime income was in the third highest quintile, and three and four years if lifetime
income was in the two highest quintiles.
142
U.S. Senate, Commission on Long-Term Care.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 60
Appendices
Appendix A: Participants in the Engagement Process
Actuarial Organizations and Consultants
American Academy of Actuaries Oliver Wyman
Milliman Society of Actuaries
Consumer Advocates
AARP California Health Advocates
Alzheimer's Association Center for Economic Justice
Government-Related Entities
National Association of Insurance Commissioners
Industry and Trade Groups
America’s Health Insurance Plans Lincoln National
American Council of Life Insurers
National Association of Insurance and
Financial Advisors
Davis and Harmon New York Life Insurance Company
Genworth Financial O’Leary Marketing Associates, LLC
The Golleher Group, LLC Transamerica Life Insurance Co.
John Hancock
Regulators
Alaska Department of Commerce,
Community, and Economic Development
Division of Insurance
Maryland Insurance Administration
Colorado Department of Regulatory Agencies
Division of Insurance
Nebraska Department of Insurance
Connecticut Insurance Department Pennsylvania Insurance Department
Think Tanks
The LeadingAge LTSS Center @UMass
Boston
Urban Institute

Long-Term Care Insurance: Recommendations for Improvement of Regulation 61
Appendix B: Summary of Analysis and Recommendations
Analysis/Recommendation
Implementation
Federal State
Other
Stakeholders
Innovation and Product Development
Innovation and product development have the
potential to significantly strengthen the private
LTCI market and better address consumers’
needs for LTC. The Task Force recommends
that federal and state policymakers and
regulators foster a regulatory environment that
encourages flexibility, experimentation, and
innovation in policy design to improve
consumer choice and access to benefits, while
appropriately protecting the rights of consumers
and the solvency of insurers.
Treasury,
IRS, HHS,
DOL
Insurance
Regulators,
NAIC
Policymakers could benefit from analysis of the
impact of combination products on the market
for LTC risk protection. The Task Force
recommends that actuaries, academics, and
other stakeholders explore such an analysis with
coordination by FIO.
Treasury,
FIO
Actuaries,
Academics,
Policy Experts
The Task Force recommends that federal
policymakers work with their state counterparts
and with private sector stakeholders to evaluate
and monitor the market for limited LTCI,
including potential impacts on the risk pool for
longer-term products and on Medicaid.
Treasury,
IRS, HHS,
CMS
Insurance
Regulators,
NAIC
Industry,
Consumer
Groups, Policy
Experts
The Task Force recommends that state
legislators and insurance regulators take steps to
better streamline and standardize the regulation
of the limited LTCI market.
Legislators,
Insurance
Regulators
The Task Force considered two policy
proposals for LTCI group products, both
involving the fiduciary provisions of ERISA.
The Task Force does not recommend either
proposal.

Long-Term Care Insurance: Recommendations for Improvement of Regulation 62
Analysis/Recommendation
Implementation
Federal State
Other
Stakeholders
Supporting the ability of individuals who need
LTC to remain in their homes could benefit
both consumers and insurers. The Task Force
encourages industry, federal policymakers, and
other experts, in consultation with consumer
representatives, to identify and assess evidence
of cost-effective pre-claim interventions under
LTCI policies. Depending on the results of the
analysis, Congress could consider amending the
Code to permit payment of evidence-based,
cost-effective incidental benefits under a tax-
qualified LTCI contract prior to the insured
becoming chronically ill, subject to a monetary
cap and other conditions set by regulation.
Congress,
Treasury,
IRS
Industry,
Policy Experts,
Consumer
Groups
Regulatory Efficiency and Alignment
Inflation protection requirements under HIPAA
and state insurance laws should be revised to
improve the efficiency and effectiveness of
regulation. To both address outdated
requirements and provide flexibility to adapt
inflation protection to evolving economic
conditions, the Task Force recommends that
Congress amend the Code to authorize Treasury
to set inflation protections for tax-qualified
LTCI.
Congress,
Treasury,
IRS
Insurance
Regulators,
NAIC
The Task Force recommends that state
policymakers—legislators, Medicaid directors,
insurance regulators, and the NAIC—improve
regulatory efficiency and effectiveness by
harmonizing and streamlining inflation
protection requirements under the Partnership
program. Alternatively, Congress could
delegate to HHS the authority to set Partnership
program inflation protection requirements.
Congress,
HHS
Legislators,
Medicaid
Directors,
Insurance
Regulators,
NAIC

Long-Term Care Insurance: Recommendations for Improvement of Regulation 63
Analysis/Recommendation
Implementation
Federal State
Other
Stakeholders
HIPAA and the DRA create regulatory
inefficiency by incorporating two outdated and
conflicting versions of NAIC models with
respect to consumer protections for LTCI. The
Task Force recommends that Congress consider
options to address this regulatory inefficiency.
One option is to empower Treasury, in
consultation with HHS, to set consumer
protection standards using one version of the
LTCI Model Act and Model Regulation for
purposes of both tax qualification under HIPAA
and Partnership eligibility under the DRA, with
flexibility to update the standards periodically
(e.g., every ten years).
Congress,
Treasury,
HHS
The Task Force recommends that the NAIC and
the states maintain their focus on LTCI and
work together in 2020 to develop a consistent
national approach to regulatory reviews of
LTCI rate increase requests. The Task Force
also recommends that FIO continue to monitor
and report on this issue.
Treasury,
FIO
NAIC,
Insurance
Regulators
Industry,
Consumer
Groups
Financial Literacy and Education
The Task Force recommends that Treasury,
HHS, DOL, and other agencies, working
through the FLEC, assess federal education
resources on LTC needs and planning, and
modify, update, and supplement these resources
as needed. As part of its efforts to improve
consumers’ capability in retirement planning,
the FLEC should clearly integrate LTC
planning into retirement education topics.
Treasury,
HHS,
DOL,
FLEC

Long-Term Care Insurance: Recommendations for Improvement of Regulation 64
Analysis/Recommendation
Implementation
Federal State
Other
Stakeholders
Tax Incentives
The Task Force considered multiple proposals
to amend federal tax laws and regulations to
encourage the purchase of LTCI. The Task
Force does not recommend adoption of any of
the proposed additional tax incentives, with the
exception of the proposal to eliminate the
additional tax on early withdrawal of funds
from an IRA, 401(k), or 403(b) account that are
used to pay LTCI premiums.
Congress,
Treasury,
IRS
Alternative Financing Approaches
The Task Force conducted a high-level review
of select public insurance approaches to
financing LTC. The Task Force does not
recommend pursuing any particular alternative
financing approach at this time. Policymakers
and other stakeholders should continue to
develop, monitor, and analyze LTC and LTCI
reform proposals to better understand the
advantages and disadvantages of specific
options, tradeoffs, program costs, and
distributional impacts.
Treasury,
HHS,
CMS
Legislators,
Medicaid
Directors,
Insurance
Regulators
