
PRIVATE HEALTH
INSURANCE
Limited Data Hinders
Understanding of
Short-Term Plans’
Role and Value during
the COVID-19
Pandemic
Report to Congressional Committees
May 2022
GAO-22-104683
United States Government Accountability Office

United States Government Accountability Office
Highlights of GAO-22-104683, a report to
c
ongressional committees
May 2022
PRIVATE HEALTH INSURANCE
Limited Data
Hinders Understanding of Short-Term
Plans’ Role and Value
during the COVID-19 Pandemic
What GAO Found
One option that may be available to those who lose jobs with employer-
sponsored insurance (ESI) during the COVID-19 pandemic is short-term plans,
which can cover certain health expenses. These plans are generally not subject
to federal requirements for individual health insurance coverage established by
the Patient Protection and Affordable Care Act (PPACA), such as restrictions on
basing premiums on pre-existing health conditions and the requirement to cover
10 essential health benefits. Federal requirements for short-term plans are
primarily limited to defining their duration—the length of time a consumer can be
covered by them. States have broad authority and discretion in regulating short-
term plans, and regulation of short-term plans varies across states. For example,
some states have prohibited their sale and some have imposed restrictions in
addition to federal requirements.
GAO found that limited and inconsistent data hinder understanding of the role
short-term plans played during the COVID-19 pandemic for those who lost ESI,
such as whether they were used by consumers as temporary coverage or as a
longer-term alternative to PPACA-compliant plans. Policy researchers and
representatives of national organizations that GAO interviewed said there was a
lack of comprehensive data and information on short-term plans, including data
on how many people enroll in them and for how long. In addition, data collected
on short-term plans varied across the six states that GAO reviewed.
• Two states did not have data on short-term plan enrollment.
• Three states reported fewer than 10,000 enrollees in short-term plans and
trends varied as to whether enrollment increased or decreased.
• One state did not have short-term plans offered from 2019 through 2021.
State officials in the five states with plan sales were not able to report on the role
of short-term plans for consumers, as none of them collected data on the
duration of short-term plan coverage.
Views vary widely about the value of short-term plans to consumers. Officials
from two of the six states GAO reviewed and other stakeholders interviewed said
that short-term plans meet an important need for certain consumers who lost ESI
during the COVID-19 pandemic. They said short-term plans provide additional
options for certain consumers such as those needing temporary insurance until
they become employed again, and those who cannot afford insurance premiums
for PPACA-compliant plans. In contrast, officials in two other states and some
other policy researchers said that short-term plans did not provide good value to
consumers. While most of those GAO interviewed said that short-term plans
often had lower premiums than PPACA-compliant plans, some also emphasized
that short-term plans (1) provided fewer benefits, (2) were not available to those
with pre-existing conditions, and (3) could result in higher total out-of-pocket
costs for some consumers compared to PPACA-compliant plans. In addition,
unlike PPACA-compliant plans, short-term plans are not subject to federal
requirements to provide consumers with key information about their benefits that
would facilitate comparison with other options.
View GAO-22-104683. For more information,
contact
John E. Dicken at (202) 512-7114 or
DickenJ
@gao.gov.
Why GAO Did This Study
Millions of Americans who lost their
jobs during the COVID
-19 pandemic
also lost their ESI.
Short-term plan
insurance was one option for
these
consumers. However, these plans can
be significantly
different from other
health coverage
options for those
losin
g ESI. Therefore, it is important to
understand the role
they play in the
market and for individual consumers.
GAO was responsible
under the
Coronavirus Aid, Relief, and Economic
Security Act for
monitoring the federal
government's pandemic response.
In
th
is report, GAO describes what is
known about short
-term plans and the
role that they might play for individuals
who lost ESI during the pandemic
.
S
takeholder views of the value of
short
-term plans in meeting consumer
needs
are also discussed.
GAO conducted
a literature search and
review of studies on short
-term plans
and conducted interviews with national
organizations such as the National
Association of Insurance
Commissioners.
GAO
also interviewed
seven
policy researchers selected to
include diverse polic
y perspectives
and
stakeholders. This included
(1) officials
from
six state insurance departments
selected to represent
different levels
and type
s of regulation, and (2)
representatives from four organizations
that sell short
-term plans.

Page i GAO-22-104683 Private Health Insurance
Letter 1
Background 5
Data Limitations Hinder Understanding of the Role Short-Term
Plans Played during the COVID-19 Pandemic 9
Views Varied Widely about the Value of Short-Term Plans to
Consumers and as Compared to Individual Health Insurance
Coverage 15
Additional Data Would Enhance Understanding of the Role of
Short-Term Plans and Help States Oversee Insurer Market
Conduct 27
Agency Comments 28
Appendix I Publications on Short-Term Plans 32
Appendix II GAO Contact and Staff Acknowledgments 38
Tables
Table 1: Short-Term Plan Enrollment in Selected States, 2019 and
2020 13
Table 2: Regulation of Contract Period and Renewal for Short-
Term Plans Sold in Selected States, 2020-2021 14
Table 3: Examples of Data and Information about Short-Term
Plans Suggested for Collection from Insurers by
Stakeholders and Policy Researchers 27
Figure
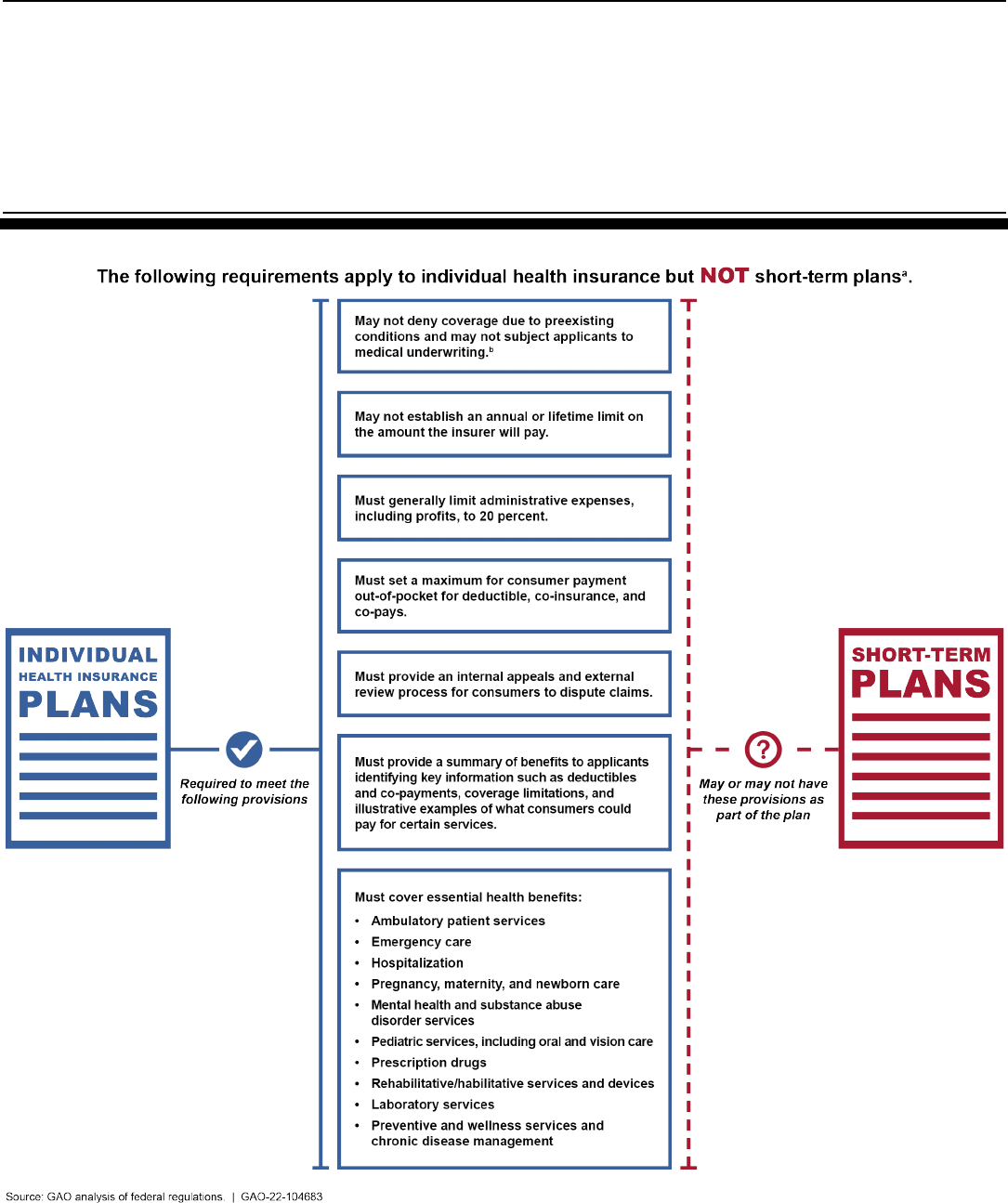
Figure 1: Selected Requirements in PPACA That Apply to
Individual Health Insurance Coverage but Not to Short-
Term Plans 6
Contents

Page ii GAO-22-104683 Private Health Insurance
Abbreviations
ESI Employer-sponsored insurance
NAIC National Association of Insurance Commissioners
PPACA Patient Protection and Affordable Care Act
This is a work of the U.S. government and is not subject to copyright protection in the
United States. The published product may be reproduced and distributed in its entirety
without further permission from GAO. However, because this work may contain
copyrighted images or other material, permission from the copyright holder may be
necessary if you wish to reproduce this material separately.

Page 1 GAO-22-104683 Private Health Insurance
441 G St. N.W.
Washington, DC 20548
May 31, 2022
Congressional Committees
It is estimated that millions of Americans experienced a disruption in
health insurance coverage during the COVID-19 pandemic due to loss of
jobs that provided employer-sponsored insurance (ESI).
1
Those who lost
ESI had several options for obtaining an alternative source of health care
coverage, including short-term, limited-duration insurance, referred to
hereafter as short-term plans.
2
A short-term plan is health insurance
traditionally designed to fill temporary gaps in coverage that may occur
when an individual is transitioning from one source of long-term,
comprehensive coverage to another.
3
States are the primary regulators of private health insurance, which is
also subject to certain federal standards and minimum requirements.
Federal requirements for short-term plans are primarily limited to defining
their duration—the length of time a consumer can be covered by a short-
term plan and the ability of the consumer to renew the plan—and in 2018
1
In prior work, we reported on estimates of employer-sponsored insurance that suggested
that more than 3.1 million non-elderly adults lost their insurance during the COVID-19
pandemic; some losing this insurance were able to obtain an alternative source of
coverage. GAO, COVID-19: Additional Actions Needed to Improve Accountability and
Program Effectiveness of Federal Response, GAO-22-105051 (Washington, DC, Oct. 27,
2021), 72.
2
Under current regulations, short-term, limited-duration insurance is generally defined as
health insurance that expires less than 12 months after the effective date of the coverage
and, taking into account renewals or extensions, has a duration of no longer than 36
months in total. See 45 C.F.R. § 144.103 (2021). For purposes of this report, we refer to
this insurance as short-term plans.
As GAO has reported elsewhere, other health coverage options subject to federal
regulation include: coverage through a federal or state health insurance exchange
established under the Patient Protection and Affordable Care Act (PPACA); Medicaid, a
joint federal-state health financing program for certain low-income and medically needy
individuals; and benefits under the Consolidated Omnibus Budget Reconciliation Act
(COBRA) of 1985, which provides certain individuals who lose their employer-sponsored
health coverage with temporary access to continue their coverage for limited periods of
time under certain circumstances. GAO-22-105051.
3
Coverage is long-term if it can be annually renewed without limitation, and it is
comprehensive if it covers a broad array of health care services. Examples of renewable,
comprehensive coverage are ESI, Medicare, and Medicaid, which are renewable each
year for eligible individuals, and cover a broad array of health care services.
Letter

Page 2 GAO-22-104683 Private Health Insurance
the limit was extended from less than 3 months of coverage to up to 3
years of coverage.
4
Short-term plans are excluded from the definition of
individual health insurance coverage under federal law and thus are not
subject to the Patient Protection and Affordable Care Act’s (PPACA)
requirements for health insurance coverage provided by plans in the
individual market (hereafter referred to as PPACA-compliant plans).
5
For
example, unlike PPACA-compliant plans, short-term plans are not
prohibited by federal law from varying premiums based on the individual
consumer’s health status or gender.
Because short-term plans can be significantly different than PPACA-
compliant plans, and because they can be purchased for longer periods
of coverage than previously allowed, it is important to understand the role
they play for consumers in the health insurance market—such as whether
the plans are purchased to fill a temporary need or as longer-term
coverage—as well as the extent to which these plans reduce or defray
consumers’ medical costs during periods of economic downturn—such as
during the COVID-19 pandemic. Understanding the role these short-term
plans play and the extent to which this provides value to consumers is
also important because consumers who buy short-term plans are not
included in PPACA individual market risk pools—the population that buys
individual health insurance coverage in each state—which influences the
4
Federal requirements for the maximum duration of short-term plans have varied over
time, with the latest change increasing the duration from 3 months to up to 1 year with the
option to renew for up to a total of 3 years.
5
See 42 U.S.C. § 300gg-91(b)(5); 45 C.F.R. § 144.103 (2021) (definition of individual
health insurance coverage). See also Pub. L. No. 111-148, 124 Stat. 119 (2010), as
amended by the Health Care and Education Reconciliation Act of 2010, Pub. L. No. 111-
152, 124 Stat. 1029 (2010) (hereafter “PPACA”).
For example, PPACA established new requirements for individual health insurance
coverage regarding what benefits must be covered, what costs consumers may be
responsible for, and what information insurers may use to determine the monthly
premiums they charge, but these requirements do not apply to short-term plans. See Pub.
L. No. 111-148, §§ 1001, 1201, 124 Stat. 119, 131, 161, 885 (codified as amended at 42
U.S.C. §§ 300gg-6, 300gg-13, 300gg-18).
In this report we use the phrase “PPACA-compliant plans” to mean plans that must meet
federal requirements for individual health insurance coverage. We did not evaluate the
legal compliance of any plans for purposes of this report. PPACA-compliant plans may be
sold through federal or state PPACA exchanges that allow consumers to access possible
federal subsidies, or they may be sold by insurers directly to individuals outside of the
exchanges. Consumers may purchase PPACA-compliant plans during annual open
enrollment periods or at any time if they have a qualifying life event, such as having or
adopting a child or loss of insurance coverage.

Page 3 GAO-22-104683 Private Health Insurance
cost of premiums set by insurers and the amount of federal subsidies
available under PPACA.
6
For example, if relatively healthy individuals
choose short-term plans instead of PPACA-compliant plans, this could
result in higher premiums for PPACA-compliant plans and higher federal
subsidies.
The Coronavirus Aid, Relief, and Economic Security Act includes a
provision for GAO to conduct monitoring of, among other things, the effect
of the COVID-19 pandemic on the health, economy, and public and
private institutions of the United States.
7
In this report, we describe:
1. what is known about short-term plans, including the role they might
play for individuals who lost ESI during the COVID-19 pandemic;
2. how stakeholders and policy researchers view the value of short-term
plans in meeting consumer needs, including in comparison to PPACA-
compliant plans; and
3. what data about short-term plans would be useful for understanding
their role and value, according to stakeholders and policy researchers.
To address all of these objectives, we examined information from a
variety of sources, including a review of federal and state regulations, a
literature search and review of studies on short-term plans, and interviews
with selected national organizations, stakeholders and policy researchers.
We reviewed studies on short-term plans published from 2016 through
2021 to learn about (1) what has been reported on the role of short-term
plans in the insurance market generally, as well as related to people who
lost ESI during the COVID-19 pandemic from March 2020 through 2021,
and (2) views of the value of short-term plans compared to individual
health insurance coverage. (App. I provides more detail on our approach
6
Individuals purchasing coverage through the exchanges may be eligible, depending on
their incomes, to receive financial assistance to offset the costs of their coverage through
two types of subsidies. Premium tax credits reduce an eligible individual’s premium costs.
Some enrollees who qualify for premium tax credits may also be eligible to receive cost-
sharing reductions, which lower enrollees’ deductibles, coinsurance, and co-payments,
based on their income and the type of plan they select. The American Rescue Plan Act of
2021 expanded eligibility for subsidies to individuals with higher incomes and increased
subsidies for lower-income individuals for 2021 and 2022. . Pub L. No. 117-2, § 9661, 135
Stat. 4, 182 (codified as amended at 26 U.S.C. § 36B).
Premiums are set by insurers to cover the expected health care costs of the state’s
individual market and thus may vary based on whether the population is sicker or
healthier.
7
Pub. L. No. 116-136, § 19010(b), 134 Stat. 281, 580.
Page 4 GAO-22-104683 Private Health Insurance
to identify relevant literature.) We focused our research on short-term
plans sold by insurers to individuals. We did not review products sold as
group insurance.
8
Through our literature search we identified national associations that had
collected or analyzed information about short-term plans, and we
interviewed representatives from these organizations, including the
National Association of Insurance Commissioners (NAIC) and the
America’s Health Insurance Plans. We also interviewed officials from the
Congressional Budget Office, which has collected and analyzed
information about short-term plans.
In addition, we interviewed policy researchers as well as officials with
selected stakeholder organizations involved in the sale or oversight of
short term plans—including insurers that sell short-term plans and state
insurance departments.
• Through our literature search, we identified policy researchers who
had analyzed information on short-term plans from calendar years
2016 through 2021, and we interviewed seven of these individuals
selected to achieve variation across the group with respect to
organizational affiliation and policy perspective.
• We interviewed officials from six state insurance departments
selected to achieve variation in geographic region and the extent to
which the states regulate short-term plans.
9
• Finally, we interviewed four sellers of short-term plans, including three
insurers and one broker, selected to achieve variation in volume of
short-term plan sales, whether the company operated in one state or
multiple states, and to include one or more insurers that sold in our
selected states.
10
8
The private health insurance market includes individual and group coverage. The
individual market is where individuals and families buy health insurance on their own.
Health plans sold in the group market are offered through plan sponsors such as
employers.
9
The states selected for this study include Alabama, Colorado, Florida, Idaho, Michigan,
and Pennsylvania.
10
A broker is an individual who receives commissions from the sale and service of
insurance policies. These individuals work on behalf of the customer and are not restricted
to selling policies for a specific company but commissions are paid by the company with
which the sale was made.

Page 5 GAO-22-104683 Private Health Insurance
We conducted this performance audit from December 2020 to May 2022
in accordance with generally accepted government auditing standards.
Those standards require that we plan and perform the audit to obtain
sufficient, appropriate evidence to provide a reasonable basis for our
findings and conclusions based on our audit objectives. We believe that
the evidence obtained provides a reasonable basis for our findings and
conclusions based on our audit objectives.
Short-term plans were traditionally designed to fill temporary gaps that
may occur when an individual is transitioning from one coverage to
another; for example, when someone has left a job and is seeking other
employment. However, although sold by insurers directly to individuals,
short-term plans are exempted from the definition of individual health
insurance coverage under federal law and therefore are not required to
comply with PPACA’s requirements for individual health insurance
coverage.
11
For example, PPACA prohibits insurers that sell individual
health insurance coverage from denying coverage or charging higher
premiums because of a pre-existing condition—a condition that the
consumer had prior to applying for coverage, such as diabetes or heart
disease—and it requires such insurers to cover 10 essential health
benefits. (See fig. 1 for individual health insurance requirements under
federal regulation, including the 10 essential health benefits.) Unlike
PPACA-compliant plans, however, federal rules prohibiting the varying of
premiums based on a consumer’s health status or gender—a process
called medical underwriting—do not apply to short-term plans. Moreover,
these plans also are not subject to federal rules prohibiting denial of
coverage for pre-existing conditions, rules limiting the amount of
expenses the consumer must pay, or prohibitions on annual or lifetime
limits on how much money the insurer will pay.
12
11
See 42 U.S.C. § 300gg-91(b)(5); 45 C.F.R. § 144.103 (2021). Similarly, PPACA
requirements for group health plans and for insurance offered through an employer to a
group of its employees do not apply to short-term plans, which are sold to individuals.
12
For example, health status could include such things as physical and mental illnesses,
medical history, genetic information, and disability. While federal rules allow short-term
plans to vary premiums based on the individual consumer’s health status, gender, and
other factors, PPACA-compliant plans can only vary premiums based on four
characteristics associated with the consumer: geographic area within a state, tobacco use,
individual versus family plan, and age—plans may not charge an older adult more than
three times the premium that they charge a younger adult. See 42 U.S.C. § 300gg(a)(1).
Background
Short-Term Plans
Page 6 GAO-22-104683 Private Health Insurance
Figure 1: Selected Requirements in PPACA That Apply to Individual Health Insurance Coverage but Not to Short-Term Plans
a
For purposes of this report, we refer to short-term limited duration insurance as short-term plans.
Such plans are excluded from the federal definition of individual health insurance coverage and thus
are not subject to Patient Protection and Affordable Care Act (PPACA) requirements for such

Page 7 GAO-22-104683 Private Health Insurance
coverage. See 42 U.S.C. § 300gg-91(b)(5). See also Pub. L. No. 111-148, 124 Stat. 119 (2010), as
amended by the Health Care and Education Reconciliation Act of 2010, Pub. L. No. 111-152, 124
Stat. 1029 (2010).
b
Medical underwriting is a process whereby premiums may vary based on a consumer’s health status
or gender.
Although short-term plans do not have to meet these federal
requirements, some may use certain terminology and marketing
approaches that are similar to PPACA-compliant plans. For example,
short-term plans may set an annual deductible—a dollar amount for which
the consumer is responsible before the insurer makes any payments—as
well as an annual limit on the consumer’s out-of-pocket expenses for
covered services; they may establish co-payments for certain types of
services, such as $35 for each physician visit; and they may set co-
insurance rates, such as 30 percent of inpatient medical expenses.
13
They may also list the types of services that are covered. Short-term
plans may be marketed through certain brokers and on-line websites that
sell both short-term plans and PPACA-compliant plans.
In contrast to the body of federal regulations applicable to PPACA-
compliant plans, federal regulation of short-term plans is primarily
concerned with the plan’s duration of coverage and the ability of the
consumer to renew the plan. In addition, federal regulations require short-
term plans to prominently display certain information in the contract and in
any application materials including that, among other things, the coverage
is not required to comply with certain federal requirements.
14
Federal
regulations concerning short-term plan coverage duration and
renewability have changed over time, as noted below.
• Effective in June 1997, short-term plan contracts were restricted to a
maximum duration of 12 months of coverage.
15
13
Co-payments are fixed amounts that the consumer pays for a covered health service—
usually when they receive the service—and the amount can vary by the type of covered
health service. Co-insurance also requires the consumer to share in the cost of a covered
health service, but the share is calculated as a percentage of the allowed amount, which is
the maximum an insurance plan will pay for a covered service.
14
See 45 C.F.R. § 144.103 (2021).
15
62 Fed. Reg. 16,894, 16,942, 16,958 (April 8, 1997). See also 69 Fed. Reg. 78,720,
78,783 (Dec. 30, 2004).
Federal Regulation of
Short-Term Plans
Page 8 GAO-22-104683 Private Health Insurance
• Effective in January 2017, the Obama administration shortened the
maximum duration of a short-term plan contract to up to 3 months of
coverage.
16
• Effective in October 2018, the Trump administration increased the
maximum duration of a short-term plan contract to up to 12 months
and also provided that the plan could be renewed for a total of up to
36 months of coverage.
17
While states cannot allow short-term plans to have a duration longer than
federal limits, states have broad authority and discretion to regulate
health insurance, including short-term plans sold to individuals. A state
may regulate various aspects of the health insurance sold within the
state, including plan design, insurer compliance with consumer
protections, and information insurers must report to the states in which
they operate.
• Plan design. States vary in the extent to which they impose additional
restrictions on short-term plans beyond the federal requirements, for
example by:
• restricting the maximum contract duration of a single plan to 3 or 6
months, limiting the number of times a consumer can renew the
plan, or prohibiting renewal entirely;
• requiring short-term plans to offer certain benefits;
• prohibiting short-term plans from being medically underwritten,
meaning that insurers cannot vary premiums based on a
consumer’s health status;
• prohibiting the sale of short-term plans during the state’s PPACA
open enrollment period but permitting their sale outside of that
timeframe; or
• prohibiting short-term plan sales in the state.
• Consumer protections. States may have health insurance consumer
protections in place, typically known as “market conduct regulations.”
These regulations may require that consumers (1) are charged fair
and reasonable prices for short-term plans, (2) are dealing with plans
that comply with appropriate laws and regulations, and (3) are
16
81 Fed. Reg. 75,316, 75,326 (Oct. 31, 2016).
17
83 Fed. Reg. 38,212, 38,243 (Aug. 3, 2018).
State Regulation of Short-
Term Plans

Page 9 GAO-22-104683 Private Health Insurance
protected against insurers that fail to operate in ways that are legal
and fair to consumers.
• Insurer reporting. State departments of insurance may require
insurance companies licensed in the state to report a variety of
information, and this may include information about short-term plans.
States participate as members of the National Association of
Insurance Commissioners (NAIC) which collects certain data from
insurers on behalf of state members; for example, information about
different insurance products sold by the insurer and data on the
amount of premiums earned and the number of policies sold in a
state.
18
Policy researchers and representatives of national organizations we
interviewed told us that there was a lack of comprehensive data and
information on short-term plans generally, including during the COVID-19
pandemic in 2020 and 2021. This included data on enrollment in short-
term plans and the duration of policies sold—e.g., whether they were for
several months or a year and how often they were renewed. These data
would provide information about the role of short-term plans for
consumers in terms of how much consumers relied on them, and whether
they used them for temporary needs or as longer-term coverage.
• For example, one policy researcher said that most states’ insurance
departments did not collect data, and, when they did, they did not
18
NAIC is the standard-setting and regulatory support organization created and governed
by the chief insurance regulators from the 50 states, the District of Columbia and five U.S.
territories. Through the NAIC, state insurance regulators establish standards and best
practices, collect data from insurers, conduct peer review, and coordinate their regulatory
oversight. For example, NAIC collects data from insurers on behalf of states through its
Market Conduct Annual Statement.
Data Limitations
Hinder Understanding
of the Role Short-
Term Plans Played
during the COVID-19
Pandemic
Policy Researchers and
National Organizations
Cited a General Lack of
Data on Short-Term Plans

Page 10 GAO-22-104683 Private Health Insurance
collect it in comparable ways. This researcher also indicated that most
states did not review premium rates for short-term plans.
19
• Another policy researcher said that there is a lack of data sources for
short-term plans that are publicly available, and that this lack of data
limits the scope of what can be known about these plans.
• A third policy researcher said that claims about the role of short-term
plans cannot be proven or disproven without systematic data
collection.
Officials with the NAIC and the Congressional Budget Office told us that
there is a lack of accurate data and information on short-term plans,
including, but not limited to, enrollment data.
• Officials with NAIC, which collects data from insurers on behalf of
state departments of insurance, told us that data reported to them by
insurers on short-term plan enrollment and premiums in NAIC’s
annual Accident and Health Policy Experience Reports were not
complete or accurate, in part because insurers varied in how they
reported data and categorized both short-term plans and other
unregulated products in their reports. To address this issue, NAIC
issued a separate request to insurers in 2020 that sought to gather
enrollment information from insurers about short-term plans, but,
according to NAIC officials, some insurers did not respond and other
insurers did not provide complete information.
20
• Officials with the Congressional Budget Office, which studies trends in
the types of health insurance consumers have, told us that there is no
comprehensive tracking of short-term plans. In 2020, the Office
reported on the lack of data on short-term plans and cited the need for
19
Christina Lechner Goe, National Association of Insurance Commissioners, Non-ACA-
Compliant Plans and the Risk of Market Segmentation, Consideration for State Insurance
Regulators (National Association of Insurance Commissioners, March 2018).
20
Officials with NAIC told us that the association plans to implement a more
comprehensive and regular approach to data collection through a new Short-term Limited
Duration Insurance Market Conduct Annual Statement in 2022 to address state concerns
about the lack of information about short-term plans and other similar products. This
comprehensive data request was developed through a working group involving
representatives from state insurance departments and other stakeholders. It will include
data about short-term plans and association health plans—plans offered by business and
professional associations to their members—and will gather information about plan
duration, insurer denials of claims, and consumer complaints. However, as with certain
other NAIC products, most of the data will be made available only to member state
insurance departments.

Page 11 GAO-22-104683 Private Health Insurance
(1) enrollment data by state and year and (2) claims data for those
enrolled.
21
This report indicated that these data would provide a better
understanding of the effect of federal regulations for short-term plan
duration on consumer selection of these plans. In addition, according
to the report, these data could also provide information about what
types of health care spending enrollees incur and how payments to
providers compare to other individual insurance products. Officials
with the Congressional Budget Office said that they were aware of the
challenges faced by NAIC in collecting these data on behalf of state
regulators.
One policy researcher we interviewed noted that, in contrast to data
available on short-term plans, a wide range of data on PPACA-compliant
plan options is collected by the federal government and the states to
support oversight and policy-making. The Centers for Medicare &
Medicaid Services collects data through the federal and state exchanges,
including data on enrollment in different types of plans, premiums, and
demographic and income characteristics of consumers. NAIC collects
information about PPACA-compliant plans from insurers on behalf of
states through its Health Market Conduct Annual Statement, which
includes data for each state and insurer on the number of plan policies
sold and other information such as consumer cost-sharing, consumer
grievances and appeals, and insurers’ denials of claims. This information
can be used for a variety of purposes, such as monitoring consumer
preferences, tracking the cost of coverage to consumers—including both
premiums and out-of-pocket expenses—and developing policies to
improve access and affordability.
Just as comprehensive data on short-term plans is not collected
nationwide, the states we reviewed varied in the extent that they collected
data on short-term plans. None of the six states collected data on the
duration of short-term plans and the extent to which they are renewed.
22
• States that do not collect data. Two states—Pennsylvania and
Alabama—do not regularly collect data on short-term plans, including
data on the number of individuals enrolled in them. Specifically,
21
Congressional Budget Office, Letter from Director Phillip Swagel to Senator Tammy
Baldwin Re: CBO’s Estimates of Enrollment in Short-Term, Limited Duration Insurance
(Washington, DC: Congressional Budget Office, Sept. 25, 2020).
22
We interviewed officials within the departments of insurance in Alabama, Colorado,
Florida, Idaho, Michigan, and Pennsylvania. At the time of our interviews with these
states, 2021 data was not available.
Data Collection and
Enrollment Trends Varied
in Selected States, Making
It Difficult to Understand
the Role of Short-Term
Plans

Page 12 GAO-22-104683 Private Health Insurance
officials from Pennsylvania said they were not able to track short-term
plan enrollment very well in part because insurers often combined
these plans together with other products, such as fixed indemnity
products, but did not break down enrollment separately for each
product.
23
Officials in Alabama reported that they did not collect data
on short-term plans on a regular basis, saying this would involve
establishing new reporting requirements, and that their staff size was
relatively small and did not have the capacity to regularly monitor new
reporting.
• States that collect data. In the three states in our review that collected
enrollment data from insurers on short-term plans—Florida, Idaho,
and Michigan—the extent of data collected varied based on what
officials told us. According to officials, Michigan only collects
information on enrollment and premiums. Florida officials said that in
addition to enrollment and premium information, they collected data
on short-term plans including claims submitted and medical loss ratios
to the extent that insurers provided that information in rate filings.
24
Officials in Idaho told us that, In addition to enrollment and premium
information, the state collects information on the number of new
policies issued, the number of policies ended, claims billed, and
rescissions (policies cancelled retroactively by insurers).
• A state with no sales of short-term plans. Colorado limits short-term
plans to up to 6 months’ duration. According to officials, short-term
plans were not sold in Colorado from 2019 through 2021.
Among the three states in our review that do collect data, enrollment
trends from 2019 to 2020—the first year of the COVID-19 pandemic—
were inconsistent. These data show that Michigan and Florida
experienced a decrease in enrollment in short-term plans, while Idaho
experienced an increase. (See table 1.) Officials in each of these states
reported that short-term plans generally accounted for a relatively small
part of their individual insurance markets. Officials in Michigan said they
did not have an explanation for why enrollment declined in 2020, and that
there were no regulatory changes that occurred during this time period
that would explain the change. Officials in Idaho explained that the
enrollment increase in 2020 may have been related to the state’s
23
Fixed indemnity products pay the consumer a fixed dollar amount per a certain time
period, regardless of what services are provided; for example, a fixed dollar payment per
day that someone is hospitalized.
24
Medical loss ratios indicate the total amount the insurer paid for claims compared to the
total amount collected in premiums.

Page 13 GAO-22-104683 Private Health Insurance
establishment in 2019 of a new form of short-term plan—called an
“enhanced” short-term plan— that provided additional protections to
consumers compared to the traditional short-term plan available in the
state.
25
Table 1: Short-Term Plan Enrollment in Selected States, 2019 and 2020
State
Short-term plan
enrollment in 2019
Short-term plan
enrollment in 2020
a
Florida
5,923
5,841
Idaho
b
5,748
6,877
Michigan
8,847
7,778
Source: GAO interviews with selected states’ departments of insurance. | GAO-22-104683
Note: Enrollment includes all lives covered by the policies sold (e.g., spouses and children, if also
covered).
a
COVID-19 was declared a pandemic by the World Health Organization in March, 2020.
b
Idaho’s market includes two kinds of short-term plans—traditional and enhanced. Legislation
enacted in 2019 in Idaho established enhanced short-term plans, which must meet certain
requirements beyond traditional short-term plans; for example, meeting the state’s benchmark for
essential health benefits. According to officials, Idaho enrollment data for 2019 may include some
enrollment in enhanced short-term plans, which began to be sold in December 2019. Idaho
enrollment for 2020 included 3,298 in traditional short-term plans and 3,579 in enhanced short-term
plans.
State officials were not able to report on the role of short-term plans for
consumers—such as whether they are purchased to fill a temporary need
or as longer-term coverage—as none of the five states we examined in
which short-term plans were sold compiled data on the duration of short-
term plan coverage. Therefore, officials could not report whether
consumers purchased them as temporary coverage between having other
types of coverage, or for longer periods of time as an alternative to
individual or employer-based insurance. Officials in two of our selected
states believed that most consumers purchased them primarily as
temporary coverage, officials in two other states felt that some consumers
purchased them as temporary coverage while other consumers
25
Idaho’s market includes two kinds of short-term plans—traditional and enhanced.
Legislation enacted in Idaho in 2019 established enhanced short-term plans, which must
meet certain requirements beyond traditional short-term plans. Enhanced short-term plans
must meet the state’s benchmark for essential health benefits, must provide coverage for
longer than 6 months, and cannot vary premiums based on gender. Insurers offering
enhanced short-term plans in Idaho can consider medical history, including pre-existing
conditions, only if sold outside the PPACA open enrollment period. Insurers offering
enhanced short-term plans must set their premiums based on data for the same risk
pool—the population that buys individual health insurance in the state—as PPACA-
compliant plans.

Page 14 GAO-22-104683 Private Health Insurance
purchased them more as permanent coverage, and officials in the fifth
state did not know. Four of the six states in which we interviewed
officials—Alabama, Florida, Pennsylvania and Idaho (for enhanced short-
term plans)—allowed initial short-term plan contracts for up to 1 year with
renewals that could allow for a total duration of coverage of up to 36
months. (See table 2 for requirements regarding limits on the length of
coverage and renewability of short-term plans in the six states we
examined.)
Table 2: Regulation of Contract Period and Renewal for Short-Term Plans Sold in Selected States, 2020-2021
State Plan contract period
Contract renewal and total coverage duration
allowed
Alabama
Less than 12 months
May be renewed or extended for a total duration not
to exceed 36 months
Colorado
a
Up to 6 months
Not renewable
Florida
Less than 12 months
May be renewed or extended for a total duration not
to exceed 36 months
Idaho: traditional short-term plans
b
Up to 6 months
Not renewable
Idaho: Enhanced short-term plans
b
Longer than 6 months, up to 12
months
May be renewed or extended for a total duration not
to exceed 36 months
Michigan
Up to 185 days
c
Consumers are limited to 185 days of coverage in a
365 day period
Pennsylvania
Less than 12 months
May be renewed or extended for a total duration not
to exceed 36 months
Source: GAO interviews with state departments of insurance and review of state regulations. | GAO-22-104683
a
No insurers offered short-term plans in 2020 or 2021 in Colorado.
b
Idaho’s market included two kinds of short-term plans—traditional and enhanced. Legislation
enacted in Idaho in 2019 established enhanced short-term plans, which must meet certain
requirements beyond traditional short-term plans; for example, meeting the state’s benchmark for
essential health benefits.
c
Exceptions apply.

Page 15 GAO-22-104683 Private Health Insurance
Concerns about Association Health Plans and Health Care Sharing Ministries
In addition to short-term plans, certain other products, including those commonly
referred to as association health plans, are not subject to certain health insurance
coverage requirements established under the Patient Protection and Affordable Care
Act (PPACA). For example, under a 2018 Department of Labor regulation, association
health plans are not subject to the PPACA requirement to cover the 10 essential health
benefits. Historically, these sales were made by associations that had a primary
purpose other than selling insurance, but several individuals we spoke to expressed
concerns about short-term plans sold by associations, including in some cases by
associations created primarily for the purpose of selling association health plans.
Officials in several of the states we studied said they were concerned about the growth
of these plans.
• Florida officials said that enrollment in these plans had grown significantly since
2017, as fewer individuals were able to afford plans subject to PPACA
requirements. They said that a filing to the state by one large out-of-state insurer of
short-term plans indicated that it may have from 15,000 to 18,000 policies that
were similar to short-term plans sold through associations.
• Pennsylvania officials said that, among associations selling health coverage in the
state, one claimed to have 40,000 lives covered in Pennsylvania, while others had
as few as 2,500.
In addition, products sold by certain faith-based organizations, commonly referred to as
health care sharing ministries, may not comply with federal requirements of individual
health insurance coverage. Officials in Colorado and Idaho noted their concerns about
the recent growth of consumer purchases of coverage through health care sharing
ministries that share resources for medical needs among members who make a
periodic payment.
• Idaho officials estimated that there were 25,000 consumers in health care sharing
ministries in 2019 and 2020, compared to 102,000 and 82,000 consumers,
respectively, who purchased individual coverage on the PPACA exchanges in
those years.
• Colorado officials said that there was an increase in enrollment in health care
sharing ministries after insurers stopped selling short-term plans in the state, but
officials said they did not have specific data on their enrollment.
Source: GAO interviews with selected states’ departments of insurance. | GAO-22-104683
Our interviews with stakeholders and policy researchers, and our
literature search, found widely varying views of the overall value of short-
term plans to consumers, including for those who lost ESI during the
COVID-19 pandemic. In addition, we found disagreement about how
short-term plans compared to PPACA-compliant plans with respect to
cost, benefit coverage, and consumer information. Given that there are no
comprehensive data available on short-term plans, stakeholders based
their views on their observations of the insurance market and some
limited data; policy researchers based theirs on information collected in
specific research studies.
Views Varied Widely
about the Value of
Short-Term Plans to
Consumers and as
Compared to
Individual Health
Insurance Coverage

Page 16 GAO-22-104683 Private Health Insurance
Some interviewees said that short-term plans provide an important option
for consumers, in some cases to meet short-term needs and in other
cases for longer-term coverage.
• Some interviewees identified examples of consumers who they said
could benefit from short-term plans, including those who lost ESI
during the pandemic and were in need of coverage until they became
re-employed, consumers whose employment varies by season, and
consumers whose income is too high to be eligible for Medicaid but
too low to afford a PPACA-compliant plan.
26
Officials with the
Alabama Department of Insurance said that, in times of economic
downturns, it is critical to offer individuals as many options as possible
to allow them to guard against health-related risk. Officials with one
insurer said that short-term plans can help consumers who need
coverage until the next open enrollment period. One broker we spoke
to said that he had previously purchased a short-term plan to cover
himself until the PPACA open enrollment period.
• Some interviewees noted that short-term plans can be beneficial as
longer-term coverage, since current federal regulations allow short-
term plans to last for up to 1 year with the possibility of renewing for
up to 3 years. One insurer we spoke with said that their company
works with many consumers who seek to buy short-term plans and
renew them regularly to maintain coverage over time. Officials with
the Alabama Department of Insurance said that short-term plans
provide additional pricing levels for consumers who do not have
access to PPACA subsidies. Officials in Idaho said that PPACA-
compliant plans had become unaffordable for many residents, and
that short-term plans provided an option to them. One policy
researcher reported that his family was enrolled in a short-term plan,
noting that he is self-employed and does not have an offer of health
coverage through an employer.
In contrast, other interviewees said that short-term plans do not provide
good value to consumers. They said that short-term plans can be
financially risky for consumers and should be prohibited by the federal
government or more strongly regulated by states or the federal
government; for example, by limiting a plan’s total duration to less than 1
year with no renewability.
26
Medicaid is a federal-state program that finances health care for low-income and
medically needy individuals. Individuals who lose health coverage due to job loss may be
eligible to enroll in individual health insurance coverage and may be eligible for subsidies
for exchange coverage.
Some Stakeholders and
Policy Researchers Said
Short-Term Plans Serve
an Important Purpose,
While Others Expressed
Strong Reservations about
Their Value

Page 17 GAO-22-104683 Private Health Insurance
• Several policy researchers said that, ideally, short-term plans should
be prohibited, but, if they are not, they should be limited to 3 months
or less in duration, they should not be renewable, and they should be
required to comply with at least some PPACA consumer protections.
One policy researcher told us that, while short-term plans may serve a
legitimate purpose for some consumers, they should nevertheless not
be renewable and only allowed for short-term needs.
• The commissioner of Pennsylvania’s Insurance Department testified
to Congress regarding the problems with short-term plans their state
experienced, including numerous consumer complaints related to
denials of claims by insurers.
27
The commissioner recommended
limiting the duration of these plans to less than 1 year and not
allowing them to be renewed. The Department has issued periodic
notices to consumers alerting them about possible issues with short-
term plans.
• Officials with Colorado’s Department of Insurance said that, when
short-term plans were sold in the state, there were consumer
complaints about them, and consumers did not understand the plans’
pre-existing condition exclusions.
Stakeholders, policy researchers, and research studies also disagreed
about the extent to which short-term plans provide value compared to
PPACA-compliant plans, specifically with respect to cost, benefit
coverage, and consumer information. In addition, some state officials,
policy researchers and research studies identified strong concerns with
the marketing of short-term plans.
Most of the individuals we spoke to, and some research studies reported,
that short-term plans can have lower premiums than PPACA-compliant
plans. However, while some individuals said this indicated the positive
value of short-term plans to consumers, others said that it does not reflect
the full cost to the consumer, and that, in order to compare short-term
plans to other options such as PPACA-compliant plans, additional
information needs to be considered.
27
Strengthening Our Health Care System: Legislation to Reverse ACA Sabotage and
Ensure Pre-Existing Conditions Protections: Hearing Before the Subcommittee on Health
of the Committee on Energy and Commerce, 116
th
Cong. (2019) (statement of Jessica K.
Altman, Commissioner, Pennsylvania Insurance Department).
Views Differed on the
Value of Short-Term Plans
to Consumers with
Respect to Cost, Benefit
Coverage, and
Information, Compared to
PPACA-Compliant Plans
Cost of Coverage

Page 18 GAO-22-104683 Private Health Insurance
Individuals we spoke to and some studies indicate that short-term plan
premiums can be lower than premiums for PPACA-compliant plans. An
insurer we spoke with described an example of a 6-month short-term plan
for a 19-year-old individual with no pre-existing conditions that had a
monthly premium of $39. By comparison, the Centers for Medicare &
Medicaid Services reported that monthly premiums for a PPACA-
compliant plan for a 27-year old (the only individual premium rate
described) in 2020 ranged from $278 to $426, not including any subsidies
for which certain individuals might be eligible.
28
One study illustrated the
difference in premium amount by comparing the premiums for a popular
short-term plan and a popular low-cost PPACA-compliant plan in the
individual health insurance market in Atlanta, Georgia, in 2019, for a 27-
year old female nonsmoker. The monthly premium for the short-term plan
was $77 per month and $293 for the PPACA-compliant plan, not including
any subsidy.
29
Another study compared premiums for the lowest cost
bronze tier exchange plan to the lowest short-term plan premium posted
online in 10 urban areas, and found that the lowest cost short-term plan
premiums could be as much as 91 percent cheaper.
30
A third study
28
Centers for Medicare & Medicaid Services, Center for Consumer Information and
Insurance Oversight, Plan Year 2021 Qualified Health Plan Choice and Premiums in
HealthCare.gov States, (Nov. 23, 2020). Premium data reflects the average lowest cost
plan across different tiers of plans, with tiers defined by their actuarial value, or the
percentage of total average costs for covered benefits that a plan will cover. These data
do not include adjustments for premium tax credits that some low income individuals are
eligible for through the PPACA exchanges. Eighty-six percent of exchange enrollees
received premium tax credits on average each month in 2020. Center for Medicare &
Medicaid Services, Effectuated Enrollment: Early 2021 Snapshot and Full Year 2020
Average. (June 5, 2021).
29
Dane Hansen and Gabriela Dieguez, The Impact of Short-Term Limited-Duration Policy
Expansion on Patients and the ACA Individual Market (Seattle, WA; Milliman Research
Report, February 2020). The researchers chose a “bronze” tier plan for comparison to the
short-term plan, because it has among the lowest cost premiums among PPACA-
compliant plans. In general, as actuarial value—the percentage of total average costs for
covered benefits that a plan will cover—increases, consumer cost-sharing decreases. The
actuarial values of the metal tiers are: bronze (60 percent), silver (70 percent), gold (80
percent), and platinum (90 percent).
30
Monthly premiums for the PPACA plans did not reflect discounts for premium tax credits.
Monthly premiums for short-term plans reflected prices posted online, were not
guaranteed, and could be adjusted after medical underwriting. Karen Pollitz, Michelle
Long, Ashley Semanskee, and Rabah Kamal, Understanding Short-Term Limited Duration
Health Insurance (San Francisco, CA: Kaiser Family Foundation, April 2018).

Page 19 GAO-22-104683 Private Health Insurance
estimated that short-term plans premiums could be as much as 54
percent lower than PPACA-compliant exchange plans.
31
However, although short-term plan premiums may sometimes be lower
than those for PPACA-compliant plans, some interviewees and research
studies reported that, to compare the value of the two types of coverage,
additional information needs to be considered, and that it is misleading to
suggest that short-term plan coverage is similar to comprehensive
coverage under a PPACA-compliant plan.
• For example, the cost of PPACA coverage is reduced for individuals
who—based on their income—qualify for partial or complete premium
subsidies or reduced cost-sharing. According to one study, over 20
million individuals were estimated to be eligible for PPACA subsidies
in 2020.
32
According to the Centers for Medicaid & Medicare Services,
the average monthly premium for those receiving advance premium
tax credits through the PPACA exchanges in 2020 was $89.
33
• Most of the individuals we spoke to reported that some short-term
plans do not cover services for pre-existing health conditions, which
PPACA-compliant plans must cover. Some of those we spoke to told
us that some people would not be eligible to purchase a low cost
short-term plan due to pre-existing conditions or would be charged
higher premiums based on their health history. One research study
estimated that, in 2018, 27 percent of non-elderly adults in the United
States—about 54 million people—had a pre-existing condition that
would be declined for coverage under medically underwritten health
insurance.
34
31
Larry Levitt, Rachel Fehr, Gary Claxton, Cynthia Cox, and Karen Pollitz, Why do Short-
Term Health Insurance Plans Have Lower Premiums than Plans that Comply with the
ACA? (San Francisco, CA: Kaiser Family Foundation, October 2018).
32
Kaiser Family Foundation, Marketplace Enrollees Receiving Financial Assistance as a
Share of the Subsidy-Eligible Population (San Francisco, CA: Kaiser Family Foundation,
2022).
33
Centers for Medicare & Medicaid Services, Health Insurance Marketplaces 2021 Open
Enrollment Report, retrieved on 3/4/2022 from: https://www.cms.gov/research-statistics-
data-systems/marketplace-products/2021-marketplace-open-enrollment-period-public-
use-files.
34
Gary Claxton, Cynthia Cox, Larry Levitt, and Karen Pollitz, Pre-existing Condition
Prevalence for Individuals and Families (San Francisco, CA: Kaiser Family Foundation,
October 2019), accessed March 4, 2022, https://www.kff.org/health-reform/issue-brief/pre-
existing-condition-prevalence-for-individuals-and-families/#.

Page 20 GAO-22-104683 Private Health Insurance
• As another example, short-term plans can establish a higher limit for
what consumers must annually cover out-of-pocket, beyond premium
payments, than PPACA-compliant plans are allowed to do. These out-
of-pocket costs include deductibles, co-payments, and co-insurance.
One research study estimated the costs that consumers would pay for
premiums and out-of-pocket expenses if they were newly diagnosed
with one of several conditions—for example, diabetes, a heart attack,
or lung cancer—and found that the total cost to those covered by
short-term plans and diagnosed with one of these conditions was
significantly greater than their costs would have been under a
PPACA-compliant plan. The study estimated, for example, that a
consumer who had a heart attack would face a cost of $32,100 under
the short-term plan in the 6 months following diagnosis, compared to
$7,900 under a PPACA-compliant plan in the same time period.
35
Policy researchers and the research literature disagreed in their
characterization of the extent to which short term plans offer a
comprehensive array of health benefits compared to PPACA-compliant
plans.
One policy researcher we spoke to said that, in assessing short-term
plans’ coverage of benefits, it is most important that consumers have at
least one short-term plan option in their area that covers a broad array of
benefits. They discussed their research that found that short-term plans
covering all of PPACA’s essential health benefits—except maternity
benefits—are widely available.
36
This study looked at the number of short-
term plans that two online websites listed in the major urban area in each
state, and whether these plans included coverage for certain benefits:
prescription drugs, mental health, substance abuse and maternity care. It
found that in most states there were at least some short-term plans that
provided coverage for three of these services, specifically, prescription
drugs, mental health and substance abuse.
35
Dane Hansen and Gabriela Dieguez, The Impact of Short-Term Limited-Duration Policy
Expansion.
36
Chris Pope, Renewable Term Health Insurance: Better Coverage than Obamacare (New
York, NY: Manhattan Institute, May 2019).
Pollitz, Long, Semanskee, and Kamal, Understanding Short-Term Limited Duration
Insurance.
Benefits

Page 21 GAO-22-104683 Private Health Insurance
In contrast, other research studies and stakeholder interviews
emphasized that short-term plans often do not cover these benefits. For
example, one study looked at the same state-level data as in the study
noted above but calculated the percent, rather than the number, of short-
term plans that did not cover these benefits. The study concluded that 71
percent of short-term plans did not cover prescription drugs, 62 percent
did not cover substance abuse treatment, and 43 percent did not cover
mental health services.
37
The study further noted that, even when a plan
did cover one of these services, there were almost always limitations or
exclusions in the short-term plan that would not be permitted under
PPACA-compliant plans, such as a limit on the payment amount for
mental health services. Therefore, according to the study, it would be
misleading to suggest the short-term plan coverage is similar to
comprehensive coverage under a PPACA-compliant plan. One insurer we
spoke with said that their short-term plans cover fewer benefits than
PPACA-compliant plans. They said that their plans cover some essential
health benefits but not others, such as preventive care, so a consumer’s
visit to a physician would only be covered if the consumer was sick. In
addition, rather than providing prescription drug coverage, the short-term
plan provided a drug discount card.
38
Stakeholders, policy researchers, and research studies also disagreed
about the degree to which consumers seeking coverage may face
challenges in obtaining and understanding information about short-term
plans, particularly compared to PPACA-compliant plans.
Some of the interviewees we spoke to reported that insurers provided
consumers with information about short-term plan policies that consumers
needed.
37
Pollitz, Long, Semanskee, and Kamal, Understanding Short-Term Limited Duration
Insurance. Another study looked at 96 short-term plans offered via an online source in the
Atlanta, Georgia, market in 2019 and found that 67 percent did not include prescription
drug benefits, and 58 percent did not include mental health and substance abuse disorder
benefits. See Hansen and Dieguez, The Impact of Short-Term Limited-Duration Policy
Expansion. A third study reviewed 12 short-term plans being sold in three states, and
reported that 11 excluded nearly all coverage of prescription drugs, with some providing
limited coverage of inpatient prescriptions. Emily Curran, Kevin Lucia, JoAnn Volk, and
Dania Palanker. In the Age of COVID-19, Short-Term Plans Fall Short for Consumers
(New York, NY: The Commonwealth Fund, May 12, 2020).
38
Drug discount cards or coupons provide the consumer with a discount when purchasing
a prescription drug from a pharmacy; they are not considered insurance.
Consumer Information

Page 22 GAO-22-104683 Private Health Insurance
• The broker we spoke to, whose company markets short-term plans
directly to consumers online, said that consumers are given clear
disclosures that these plans are not PPACA-compliant, and that pre-
existing conditions are not covered.
• Similarly, officials with one insurer said they did not believe there were
risks to consumers buying its short-term plans, because the terms of
these plans were clearly laid out in their promotional materials.
• Officials with another insurer noted that they assumed that consumers
were satisfied with their short-term plans because they had fewer
consumer complaints for their short-term plans than for their Medicaid
and Medicare products.
• Officials from Alabama said their guidance requires insurers to clearly
state the terms of the short-term plan policy to avoid any
misinterpretations, their department has issued news briefings to the
general public about short-term plans, and they have a chart on their
website that provides a full synopsis of what short-term plans are
relative to PPACA-compliant plans.
In contrast, some policy researchers and stakeholders reported that
consumers may have less information about short-term plans than for
PPACA-compliant plans or may not understand certain aspects of short-
term plans. One researcher said that, because short-term plans are not
subject to PPACA requirements, they are difficult to compare to each
other, and that, while some insurers provide straightforward policy
descriptions, others’ policies are confusing, ambiguous, and include lots
of exceptions. Insurers offering short-term plans are not required to
provide consumers with a summary of benefits and coverage that
complies with PPACA guidelines for format and content, although they
may choose to do so. (See text box.) In one secret shopper study of sales
representatives selling non-PPACA-compliant products, including short-
term plans, most of the sales representatives refused to provide plan
documentation in advance to the consumer—even when asked for it
directly—and would only provide it after the consumer made an initial
payment.
39
Officials with the Michigan Department of Insurance said that
consumers may not understand that short-term plans provide limited
coverage, or that there are differences compared to PPACA-compliant
plans. Officials with the Pennsylvania Department of Insurance reported
many cases of consumers purchasing short-term plans without a full
39
Center on Health Insurance Reforms, Dania Palanker and JoAnn Volk, Misleading
Marketing of Non-ACA Health Plans Continued During COVID-19 Special Enrollment
Period (Washington, DC: Georgetown University Health Policy Institute, October 2021).

Page 23 GAO-22-104683 Private Health Insurance
understanding of the product’s limitations. In some of these cases,
officials said, consumers faced significant costs to pay for care that the
short-term plan would not pay for. Legislation was proposed in the
Pennsylvania House of Representatives in February 2021 to establish
requirements for insurers to disclose complete and accurate information
to consumers, among other things, but it had not been passed as of
February 2022.
Source: GAO analysis of federal regulations and requirements. | GAO 22 104683
Several individuals we interviewed told us that there are certain concepts
important to understanding short-term plans that can be challenging for
consumers to understand, such as “post-claims underwriting” and “pre-
existing condition.”
40
One researcher said that they had never seen post-
claims underwriting explained to consumers in short-term plan marketing
materials. Others said that the definition of pre-existing condition may not
40
Post-claims underwriting is a process whereby an insurer conducts an in-depth review of
a consumers’ medical records after the consumer has received the service, and after the
insurer has received an insurance claim, in order to ensure that the claim is for a benefit
that is covered and not, for example, for a pre-existing condition. Post-claims underwriting
may be used to deny claims to enrollees of short-term plans or rescind a short-term plan
policy, except where prohibited by state law.
Information Available to Consumers about PPACA-Compliant Plans
Plans compliant with the Patient Protection and Affordable Care Act (PPACA) must
meet certain federal requirements related to providing consumers with information
about plan characteristics and provisions. Specifically, issuers of PPACA-compliant
plans must provide a summary of benefits and coverage to applicants and enrollees.
This summary must provide a list of benefits and deductibles, co-payments, and co-
insurance rates, among other things. All plans must present this summary in the same
format to make it easy for consumers to compare plans. They must also provide
examples of what the plan will cover in common medical situations and must tell
consumers what is not covered under the specific plan.
In addition to a summary of benefits and coverage for individual plans, PPACA health
insurance exchange websites may offer side-by-side comparisons of multiple plans and
their key features such as premiums and deductibles. PPACA-compliant plans sold on
these federal and state websites may be grouped into categories based on plans’
relative “actuarial value,” which is the percentage of total average costs for covered
benefits that a plan will cover, which can help consumers assess the relative similarities
and differences among different plan options, and what the consumer’s expected costs
will be. For example, if a plan has an actuarial value of 70 percent, consumers, on
average, would be responsible for 30 percent of the costs of all covered benefits.
However, an individual consumer could be responsible for a higher or lower percentage
of the total costs of covered services for the year, depending on actual health care
needs and the terms of the insurance policy. They would also be protected by a
maximum out-of-pocket threshold for the year.

Page 24 GAO-22-104683 Private Health Insurance
be obvious or clear to many consumers; for example, a consumer may
not know that a reference to “chest cold” in their medical record may
suggest or be considered a pre-existing condition, and that therefore any
future treatment for a chest cold or other respiratory illness might not be
covered. Officials with an insurer agreed that it can be challenging to
educate consumers about the exclusion of pre-existing conditions. A joint
report by 30 national organizations that represent patients with serious
health conditions profiled examples of consumers who purchased short-
term plans and subsequently were faced with high costs because the
insurer found that their illness was a pre-existing condition.
41
A report by
the House Energy and Commerce Committee Democratic Staff profiled
cases of consumers who had purchased short-term plans and whose
claims were subsequently denied because the insurer found that the
medical services were for a pre-existing condition.
42
Finally, short-term plans are not subject to PPACA’s requirements for
maximum lifetime out-of-pocket costs limits for consumers, although
states could set such a maximum. Such a limit provides protection to
consumers who have, for example, long-term illnesses that result in
significant medical costs. According to one researcher, when looking at
short-term plans a consumer may only notice the total maximum dollar
amount that the insurer will cover under the plan and think that it will be
enough to meet their needs. However, they may not be aware of detailed
provisions within different parts of the policy that limit how much the
insurer would pay to cover a specific service, or that exclude coverage for
the service, for example outpatient chemotherapy, which can be
expensive.
Interviews with some state officials and policy researchers, and our
review of research studies, indicated strong concerns about the marketing
of short-term plans, including concerns about misleading and fraudulent
sales practices as well as about the financial incentives for insurers and
brokers selling short-term plans versus PPACA-compliant plans.
41
Partnership to Protect Coverage, Under-Covered: How “Insurance-Like Products Are
Leaving Patients Exposed. 2021 (Accessed March 21, 2022,
https://nami.org/About-NAMI/NAMI-News/2021/New-Report-Under-Covered-How-Insuran
ce-Like-Products-are-Leaving-Patients-Exposed).
42
U.S. House of Representatives Committee on Energy and Commerce, Democratic Staff,
Shortchanged: How the Trump Administration’s Expansion of Junk Short-Term Health
Insurance Plans is Putting Americans at Risk (June 2020).
Marketing
Page 25 GAO-22-104683 Private Health Insurance
• Officials with three of the state insurance departments we spoke with
expressed such concerns. For example, officials in Pennsylvania said
that some insurers and brokers told consumers that short-term plans
would cover the same benefits as a PPACA-compliant plan, when in
fact they did not. Officials in Florida said that the biggest risk of short-
term plans relates to brokers misrepresenting what the plans cover
during the sales process.
• Several policy researchers reported that their work had identified
marketing practices that directed consumers to short-term plans when
they might have been eligible for a subsidized PPACA-compliant plan.
For example, one study that looked at the results of web-based
searches for health insurance in eight states found that, regardless of
search terms used, companies selling short-term plans generally
dominated the results returned.
43
Another study, which surveyed
consumers about their experience in shopping for coverage, found
that 22 percent of consumers who were helped by a broker or
commercial health plan representative said they were offered an
alternative to a PPACA-compliant plan, such as short-term plans with
lower premiums but that excluded pre-existing conditions and other
benefits required of PPACA-compliant plans.
44
Another study,
conducted following the federal increase of PPACA premium
subsidies, found that most sales representatives contacted were more
likely to refer consumers to products that were not PPACA-compliant,
such as short-term plans, and most representatives did not suggest
PPACA-compliant coverage.
45
43
Sabrina Corlette, Kevin Lucia, Dania Palanker and Olivia Hoppe, The Marketing of
Short-Term Plans: An Assessment of Industry Practices and State Regulatory Responses
(Washington, DC: Robert Wood Johnson Foundation and Urban Institute, January 2019).
44
Karen Pollitz, Jennifer Tolbert, Liz Hamel, and Audrey Kearney, Consumer Assistance in
Health Insurance: Evidence of Impact and Unmet Need (San Francisco, CA: Kaiser
Family Foundation, Aug. 7, 2020).
45
Dania Palanker and JoAnn Volk, Misleading Marketing of Non-ACA Health Plans
Continued During COVID-19 Special Enrollment Period (Washington, DC: Georgetown
University Health Policy Institute, October 2021).
Initially, tax credits were available to consumers with income below 400 percent of the
federal poverty level if the applicable premiums were greater than a specified percent of
their income. The American Rescue Plan Act of 2021, signed into law in March 2021,
reduced the highest threshold to 8.5 percent of income and allowed consumers to obtain
the tax credit regardless of their income level through 2022 if they exceed that threshold.
Pub L. No. 117-2, § 9661, 135 Stat. 4, 182 (codified as amended at 26 U.S.C. § 36B).
Page 26 GAO-22-104683 Private Health Insurance
• Our prior work found that some sales of insurance plans included
problematic marketing practices. In eight of 31 covert shopping tests,
the sales representatives identified through a health insurance
consumer information website engaged in potentially deceptive
marketing practices about plans that were not PPACA-compliant,
including short-term plans, such as claiming that a consumer’s pre-
existing condition was covered when the health plan documents
received after purchase said otherwise.
46
• Several interviews and studies identified concerns that the
compensation paid by insurers to insurance brokers may lead to
incentives to sell short-term plans rather than PPACA-compliant
plans. Officials in one state noted that brokers receive significantly
higher compensation for sales of short-term plans—in the range of a
12 to 15 percent commission on the premium amount—compared to
PPACA-compliant plans, which pay between 1 and 2 percent in
commission.
47
The officials noted that a broker might not inform
consumers that they are eligible for subsidized exchange plans, since
they might receive a larger commission for the short-term plan. One
study that interviewed brokers in six states reported that, after PPACA
was enacted, many insurers reduced or eliminated the commissions
they paid to brokers.
48
A subsequent study that interviewed insurance
brokers across seven states reported that broker compensation for
short-term plans and other products that do not comply with PPACA
requirements, such as health care sharing ministries, involved
46
GAO, Private Health Coverage: Results of Covert Testing for Selected Offerings,
GAO-20-634R, (Washington, DC: Aug. 24, 2020). Another GAO study, conducted solely
among sales representatives listed on the federal government’s website, healthcare.gov,
found that none of the sales representatives we contacted engaged in potentially
deceptive marketing practices that misrepresented or omitted information about the
products they were selling. GAO, Private Health Coverage: Results of Covert Testing for
Selected Sales Representatives Listed on Healthcare.gov, GAO-21-568R (Washington,
DC: Aug. 10, 2021).
47
The amount a broker is paid reflects both the commission percentage and the premium
amount; therefore, for short-term plans with low premiums, the higher commission rate
may not result in higher total compensation for the sale.
48
Kevin Lucia, Sabrina Corlette, Dania Palanker, and Olivia Hoppe, Views from the
Market: Insurance Brokers’ Perspectives on Changes to Individual Health Insurance
(Washington, DC: Robert Wood Johnson Foundation and Urban Institute, Aug. 2018).

Page 27 GAO-22-104683 Private Health Insurance
commissions in the range of 15 to 28 percent of the monthly
premium.
49
Stakeholders and policy researchers we interviewed identified specific
short-term plan data, in addition to general enrollment and policy duration
data, that would be beneficial for understanding the role of short-term
plans in a pandemic, informing regulators about consumer coverage, and
ensuring effective oversight of consumer protections. The specific short-
term plan data our interviewees recommended fell into several general
categories, including enrollment, plan characteristics, marketing and
financial information. (See table 3 for examples of data stakeholders and
policy researchers recommended be collected about short-term plans.)
Table 3: Examples of Data and Information about Short-Term Plans Suggested for
Collection from Insurers by Stakeholders and Policy Researchers
Category
Data and information
Enrollment
• Enrollment numbers, including covered lives, based on a
uniform definition and approach to counting enrollment (e.g.,
enrollment at a point-in-time or the total number of consumers
ever enrolled during the year)
• Enrollment numbers by length of coverage duration of policies
• Rate of renewals and denials of coverage
• Average length of time policies are held
• Demographic characteristics of enrollees: age, prior insurance
coverage, employment status, health status, and residence
Plan
characteristics
•
Benefits that the plan covers or excludes
• Annual out-of-pocket maximum that the consumer would be
responsible for, for services covered by the plan
• Maximum amount insurer will pay
• Deductible amounts
• Co-payments and co-insurance rates by type of service
a
Marketing
•
How plans are marketed and what information is presented to
consumers
• Sources of plan sales (e.g., with an independent broker or an
insurer’s agent; whether the website where the plan is sold is a
federal or private website
b
)
• Broker commissions
• Consumer complaints, consumer satisfaction
49
Sabrina Corlette, Eric Wengle, Ian Hill, and Olivia Hoppe, Perspectives from Brokers:
The Individual Market Stabilizes While Short-Term and Other Alternative Products Pose
Risks (Washington, DC: Robert Wood Johnson Foundation and Urban Institute, April
2020).
Additional Data
Would Enhance
Understanding of the
Role of Short-Term
Plans and Help
States Oversee
Insurer Market
Conduct

Page 28 GAO-22-104683 Private Health Insurance
Category
Data and information
Financial factors
•
Range of monthly premiums charged, and what share of
enrollees pay different premium amounts
• The types of information used to set premiums, such as age or
health status
• Medical loss ratio: the total amount the insurer paid for claims
compared to the total amount collected in premiums
• Denials of claims; consumer appeals of denials
Source: GAO interviews with a selection of: seven policy researchers selected to achieve variation with respect to educational training,
organizational affiliation, and policy perspective; officials with six states selected to achieve variation in geographic region and the
extent of state regulation of short-term plans; four sellers of short-term plans including three insurers and one broker selected to include
companies that operated in one state and multiple states. | GAO-22-104683
a
Co-payments are fixed amounts that the consumer pays for a covered health service—usually when
they receive the service—and the amount can vary by the type of covered health service. Co-
insurance also requires the consumer to share in the cost of a covered health service, but the share
is calculated as a percentage of the allowed amount for the service.
b
A broker is an individual who receives commissions from the sale and service of insurance policies.
These individuals work on behalf of the customer and are not restricted to selling policies for a
specific company but commissions are paid by the company with which the sale was made.
Stakeholders and policy researchers and research studies indicated ways
in which additional data—such as data listed in table 3—could be
valuable to states. For example, additional data could clarify the role of
short-term plans during a pandemic or other economic downturn as well
as in the market generally, including whether the plans were used by
consumers as temporary coverage or as an alternative to PPACA-
compliant plans. Such data could also provide information about what
types of health care costs short-term plan enrollees incur and how
payments to providers compare to that of PPACA-compliant plans.
Finally, additional data could support state oversight of the market
conduct of insurers and consumer protections, for example protections
related to ensuring that prices are fair and that consumers’ claims are
being handled appropriately.
We provided a draft of this report to HHS for review and comment. HHS
provided technical comments, which we incorporated as appropriate.
Agency Comments

Page 29 GAO-22-104683 Private Health Insurance
If you or your staff have any questions about this report, please contact
me at (202) 512-7114 or [email protected]. Contact points for our Offices
of Congressional Relations and Public Affairs may be found on the last
page of this report. GAO staff who made key contributions to this report
are listed in appendix II.
Sincerely yours,
John E. Dicken
Director, Health Care

Page 30 GAO-22-104683 Private Health Insurance
List of Committees
The Honorable Patrick Leahy
Chairman
The Honorable Richard Shelby
Vice Chairman
Committee on Appropriations
United States Senate
The Honorable Ron Wyden
Chairman
The Honorable Mike Crapo
Ranking Member
Committee on Finance
United States Senate
The Honorable Patty Murray
Chair
The Honorable Richard Burr
Ranking Member
Committee on Health, Education, Labor, and Pensions
United States Senate
The Honorable Gary C. Peters
Chairman
The Honorable Rob Portman
Ranking Member
Committee on Homeland Security and Governmental Affairs
United States Senate
The Honorable Rosa L. DeLauro
Chair
The Honorable Kay Granger
Ranking Member
Committee on Appropriations
House of Representatives
The Honorable Frank Pallone, Jr.
Chairman
The Honorable Cathy McMorris Rodgers
Republican Leader
Committee on Energy and Commerce
House of Representatives

Page 31 GAO-22-104683 Private Health Insurance
The Honorable Bennie G. Thompson
Chairman
The Honorable John Katko
Ranking Member
Committee on Homeland Security
House of Representatives
The Honorable Carolyn B. Maloney
Chairwoman
The Honorable James Comer
Ranking Member
Committee on Oversight and Reform
House of Representatives
The Honorable Richard E. Neal
Chairman
The Honorable Kevin Brady
Republican Leader
Committee on Ways and Means
House of Representatives

Appendix I: Publications on Short-Term Plans
Page 32 GAO-22-104683 Private Health Insurance
We conducted a literature search on short-term plans for the period 2016
through 2021 and reviewed relevant publications to learn about what has
been reported on the role of short-term plans in the insurance market
generally in the past, as well as for employees who lost employer
sponsored insurance (ESI) during the COVID-19 pandemic in 2020 and
2021.
1
The literature search reviewed sources that included scholarly
publications, government reports, insurance industry sources, association
and think tank sources, and general news sources. In addition, we
conducted additional searching through citations in publications identified
in the literature search and periodic scanning of websites of organizations
that cover topics related to this objective and collected referrals of articles
from policy experts and stakeholders to whom we spoke.
From this overall search, we selected and reviewed 50 publications that
addressed one or more of the following topics: data on short-term plans,
views about why consumers might choose short-term plans compared to
other options, views about the benefits and risks of short-term plans, and
views about the role of short-term plans generally and during the COVID-
19 pandemic. We reviewed these publications to identify the views of
stakeholders and policy researchers on these topics, as well as to select
policy researchers to interview. We did not conduct an independent
review or assessment of data reported in these publications.
Badger, Doug and Whitney Jones. Five Steps Policy Makers Can Take to
Permit the Sale and Renewal of Affordable Alternatives to Obamacare
Policies, Backgrounder No. 3310. Washington, DC: The Heritage
Foundation, April 26, 2018.
Blase, Brian. Individual Health Insurance Markets Improving in States that
Fully Permit Short-Term Plans. Paeonian Springs, VA: Galen Institute,
February 2021.
Blase, Brian and Doug Badger. “The Value of Short-Term Health Plans:
Rebutting the Energy and Commerce Democratic Staff Report.” Health
Affairs Blog. August 17, 2020.
Blumberg, Linda J., Matthew Buettgens, and Robin Wang. Updated: The
Potential Impact of Short-Term Limited-Duration Policies on Insurance
1
Search terms included: short-term plans, short-term health insurance, short-term health
coverage, short-term health insurance coverage, short-term limited duration insurance,
and skimpy plans.
Appendix I: Publications on Short-Term
Plans

Appendix I: Publications on Short-Term Plans
Page 33 GAO-22-104683 Private Health Insurance
Coverage, Premiums and Federal Spending. Washington, DC: Urban
Institute, March 2018.
Center on Health Insurance Reforms, Goe, Christina L. Comparing Short-
Term Health Plans is Practically Impossible for Consumers. Washington,
DC: Georgetown University Health Policy Institute, July 27, 2020.
Center on Health Insurance Reforms, Palanker, Dania and JoAnn Volk.
Misleading Marketing of Non-ACA Health Plans Continued During
COVID-19 Special Enrollment Period. Washington, DC: Georgetown
University Health Policy Institute, October 2021.
Congressional Budget Office. Cost Estimate for H.R. 1010, a Bill to
Provide that the Rule Entitled “Short-term, Limited Duration Insurance”
Shall Have No Force or Effect. Washington DC: April 29, 2019.
Cox, Cynthia, Jennifer Kates, Karen Pollitz, Laurie Sobel, MaryBeth
Musumeci, Samantha Artiga, Alina Salganicoff, et al. Potential Health
Policy Administrative Actions under President Biden. San Francisco, CA:
Kaiser Family Foundation, December 8, 2020.
Corlette, Sabrina, Kevin Lucia, Dania Palanker and Olivia Hoppe. The
Marketing of Short-term Health Plans: An Assessment of Industry
Practices and State Regulatory Responses. Washington, DC: Robert
Wood Johnson Foundation and Urban Institute, January 2019.
Corlette, Sabrina, Erik Wengle, Ian Hill and Olivia Hoppe. Perspective
from Brokers: The Individual Market Stabilizes While Short-Term and
Other Alternative Products Pose Risks. Washington, DC: Robert Wood
Johnson Foundation and Urban Institute, April 2020.
Curran, Emily, Kevin Lucia, JoAnn Volk, and Dania Palanker. In the Age
of COVID-19, Short-Term Plans Fall Short for Consumers. New York, NY:
The Commonwealth Fund, May 12, 2020.
Fehr, Rachel, Cynthia Cox, and Larry Levitt. Data Note: Changes in
Enrollment in the Individual Health Insurance Market through Early 2019.
San Francisco, CA: Kaiser Family Foundation, August 21, 2019.
Gill, Lisa L. “The High Cost of Cheap Health Insurance.” Consumer
Reports (2021).

Appendix I: Publications on Short-Term Plans
Page 34 GAO-22-104683 Private Health Insurance
Giovanelli, Justin, Kevin Lucia, and Sabrina Corlette. New York, NY: The
Commonwealth Fund. Accessed on May 11, 2021.
https://www.commonwealthfund.org/publications/maps-and-interactives/2
021/oct/what-your-state-doing-affect-access-adequate-health
Goe, Christina L. Non-ACA-Compliant Plans and the Risk of Market
Segmentation, Considerations for State Insurance Regulators. Kansas
City, MO: National Association of Insurance Commissioners, March 2018.
Goe, Christina L. Short-Term Plans: No Provider Networks Lead to Large
Bills for Consumers. New York, NY: The Commonwealth Fund, April 30,
2019.
Goodman, John. “Donald Trump Takes a Big Step toward Personal and
Portable Health Insurance.” Forbes. Jersey City, NJ: Forbes Media
Group, June 18, 2019. Accessed on March 2, 2022.
https://www.forbes.com/sites/johngoodman/2019/06/18/donald-trump-tak
es-a-big-step-toward-personal-and-portable-health-insurance/?sh=9299fd
d71c1d
Haislmaier, Edmund F. and Abigail Slagle. Obamacare Has Doubled the
Cost of Individual Health Insurance. Washington, DC: The Heritage
Foundation, March 2021.
Hansen, Dane, and Gabriela Dieguez. The Impact of Short-term Limited-
Duration Policy Expansion on Patients and the ACA Individual Market.
Seattle, WA: Milliman Research Report, February 2020.
Kaiser Family Foundation. Fact Sheet for Consumers Considering Short-
Term Plans. San Francisco, CA: October 2019.
Kamal, Rabah, Cynthia Cox, Rachel Fehr, Marco Ramirez, Katherine
Horstman, and Larry Levitt. How Repeal of the Individual Mandate and
Expansion of Loosely Regulated Plans are Affecting 2019 Premiums. San
Francisco, CA: Kaiser Family Foundation, October 2018.
Keith, Katie. “CMS Actuary Finds Risk of Short-Term Plans to be Higher
than Estimates in Proposed Rule.” Health Affairs, (May 21, 2018).
Levitt, Larry, Rachel Fehr, Gary Claxton, Cynthia Cox, and Karen Pollitz.
Why Do Short-Term Health Insurance Plans Have Lower Premiums than
Plans that Comply with the ACA? San Francisco, CA: Kaiser Family
Foundation, October 2018.

Appendix I: Publications on Short-Term Plans
Page 35 GAO-22-104683 Private Health Insurance
Lotven, Amy. “Experts Offer Recommendations on Regulating Short-
Term Plans.” Health Exchange Alert, vol. 5, no.49 (2017).
Lotven, Amy. “16 Stakeholders to Becerra: Reverse Short-Term Plan
Rule.” Inside Health Reform, vol. 31, no. 32 (2021).
Lueck, Sarah. Commentary: Growing Evidence Shows Need for Stronger
Rules for Short-Term Health Plans. Washington, DC: Center on Budget
and Policy Priorities, October 23, 2020.
Lueck, Sarah and Tara Straw. Recovery Legislation Should Build on ACA
Successes to Expand Health Coverage, Improve Affordability.
Washington, DC: Center on Budget and Policy Priorities, April 8, 2021.
McGuire, Colleen. “Pivot Health Experiences Spike in Search Traffic after
Coronavirus Layoffs and Furloughs Surged in the U.S.” PR Newswire,
(July 7, 2020).
Palanker, Dania, JoAnn Volk, and Maanasa Kona. Seeing Fraud and
Misleading Marketing: States Warn Consumers about Alternative Health
Insurance Products. New York, NY: The Commonwealth Fund, October
30, 2019.
Palanker, Dania, Kevin Lucia, and Christina L Goe. Opportunities to
Better Protect Consumers and Markets from the Negative Impact of
Short-Term Plans. New York, NY: The Commonwealth Fund, January 14,
2021.
Palanker, Dania and Christina L Goe. States Don’t Know What’s
Happening in Their Short-Term Health Plan Markets and That’s a
Problem. New York, NY: The Commonwealth Fund, March, 27, 2020.
Palanker, Dania and Kevin Lucia. Limited Plans with Minimal Coverage
Are Being Sold as Primary Coverage, Leaving Consumers at Risk. New
York, NY: The Commonwealth Fund, September 10, 2021.
Palanker, Dania, Maanasa Kona, and Emily Curran. States Step up to
Protect Insurance Markets and Consumers from Short-Term Health
Plans. New York, NY: The Commonwealth Fund, May 2019.
Palanker, Dania, Emily Curran, and Arreyellen Salyards. Limitations of
Short-Term Plans Persist despite Predictions that They’d Evolve. New
York, NY: The Commonwealth Fund, July 22, 2020.

Appendix I: Publications on Short-Term Plans
Page 36 GAO-22-104683 Private Health Insurance
Partnership to Protect Coverage. Under-Covered: How “Insurance-Like”
Products Are Leaving Patients Exposed. Partnership to Protect
Coverage, 2021. Accessed March 21, 2022.
https://nami.org/About-NAMI/NAMI-News/2021/New-Report-Under-Cover
ed-How-Insurance-Like-Products-are-Leaving-Patients-Exposed.
Pollitz, Karen, Jennifer Tolbert, Liz Hamel, and Audrey Kearney.
Consumer Assistance in Health Insurance: Evidence of Impact and
Unmet Need. San Francisco, CA: Kaiser Family Foundation, August 7,
2020.
Pollitz, Karen and Michelle Long, Ashley Semanskee, and Rabah Kamal.
Understanding Short-Term Limited Duration Health Insurance. San
Francisco, CA: Kaiser Family Foundation, April 2018.
Pope, Chris. Maximizing Health Coverage Enrollment Amidst
Administrative Sabotage, testimony to U.S. House Committee on Ways
and Means, Oversight Subcommittee Hearing, 116th Cong., 2nd sess.,
October 20, 2020.
Pope, Chris. Renewable Term Health Insurance: Better Coverage than
Obamacare. New York, NY: Manhattan Institute, May 2019.
Pope, Chris. Renewability Protections are Key to Avoiding “Junk
Insurance”. New York, NY: Manhattan Institute, February 5, 2021.
Seervai, Shanoor, Munira Z. Gunja, and Sarah R. Collins. Health Plans
That Don’t Comply with the ACA Put Consumers at Risk. New York, NY:
The Commonwealth Fund, November 14, 2019.
Spitalnic, Paul. Estimated Financial Effects of the Short-Term, Limited
Duration Policy Proposed Rule. Washington, DC: Centers for Medicare &
Medicaid Services, April 6, 2018.
Swagel, Phillip. Letter to Honorable Tammy Baldwin Re: CBO’s Estimates
of Enrollment in Short-term Limited-Duration Insurance. Washington, DC:
September 25, 2020.
Tammy Baldwin, U.S. Senator, Wisconsin, and Chris Murphy, U.S.
Senator, Connecticut. Letter to the director of the Congressional Budget
Office. 116th Cong, 2nd Sess., August 13, 2020.

Appendix I: Publications on Short-Term Plans
Page 37 GAO-22-104683 Private Health Insurance
USC-Brookings Schaeffer Initiative for Health Policy. Young, Christen
Linke. Taking a Broader View of “Junk Insurance.” Washington, DC: The
Brookings Institution, July 2020.
USC-Brookings Schaeffer Initiative for Health Policy. Young, Christen
Linke, and Kathleen Hannick. Misleading Marketing of Short-Term Health
Plans amid COVID-19. Washington, DC: The Brookings Institution, March
24, 2020.
USC-Brookings Schaeffer Initiative for Health Policy. Hannick, Kathleen,
and Christen Linke Young. GAO Report Sheds Additional Light on
Misleading and Deceptive Marketing Practices among Non-Compliant
Health Plans. Washington, DC: The Brookings Institution, September 25,
2020.
U.S. House of Representatives Committee on Energy and Commerce,
Democratic Staff. Shortchanged: How the Trump Administration’s
Expansion of Junk Short-Term Health Insurance Plans is Putting
Americans at Risk. June, 2020.
Volk, JoAnn, Rachel Schwab, and Dania Palanker. Trump Administration
Promotes Coverage That Fails to Adequately Cover Women’s Key Health
Care Needs. New York, NY: The Commonwealth Fund, October 9, 2020.
Wakely Consulting Group, Cohen, Michael, Michelle Anderson, and Ross
Winkelman. Effects of Short-Term Limited Duration Plans on the ACA-
Compliant Individual Market. Washington, DC: Association for Community
Affiliated Health Plans. Accessed March 21, 2022.
communityplans.net/policy/effects-of-short-term-limited-duration-plans-on-
the-aca-compliant-individual-market/

Appendix II: GAO Contact and Staff
Acknowledgments
Page 38 GAO-22-104683 Private Health Insurance
In addition to the contact named above, Bob Copeland (Assistant
Director), Mary Giffin (Analyst-in-Charge), Helen Sauer, and Andrew
Nguyen made key contributions to this report. Also contributing were
Laurie Pachter, Jennifer Rudisill, Jeffrey Tamburello, and Emily Wilson
Schwark.
Appendix II: GAO Contact and Staff
Acknowledgments
GAO Contact
Staff
Acknowledgments
(104683)

The Government Accountability Office, the audit, evaluation, and investigative
arm of Congress, exists to support Congress in meeting its constitutional
responsibilities and to help improve the performance and accountability of the
federal government for the American people. GAO examines the use of public
funds; evaluates federal programs and policies; and provides analyses,
recommendations, and other assistance to help Congress make informed
oversight, policy, and funding decisions. GAO’s commitment to good government
is reflected in its core values of accountability, integrity, and reliability.
The fastest and easiest way to obtain copies of GAO documents at no cost is
through our website. Each weekday afternoon, GAO posts on its website newly
released reports, testimony, and correspondence. You can also subscribe to
GAO’s email updates to receive notification of newly posted products.
The price of each GAO publication reflects GAO’s actual cost of production and
distribution and depends on the number of pages in the publication and whether
the publication is printed in color or black and white. Pricing and ordering
information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077, or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard,
Visa, check, or money order. Call for additional information.
Connect with GAO on Facebook, Flickr, Twitter, and YouTube.
Subscribe to our RSS Feeds or Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
Contact FraudNet:
Website:
https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454 or (202) 512-7700
A. Nicole Clowers, Managing Director, [email protected], (202) 512-4400, U.S.
Government Accountability Office, 441 G Street NW, Room 7125, Washington,
DC 20548
Chuck Young, Managing Director, young[email protected], (202) 512-4800
U.S. Government Accountability Office, 441 G Street NW, Room 7149
Washington, DC 20548
Stephen J. Sanford, Managing Director, [email protected], (202) 512-4707
U.S. Government Accountability Office, 441 G Street NW, Room 7814,
Washington, DC 20548
GAO’s Mission
Obtaining Copies of
GAO Reports and
Testimony
Order by Phone
Connect with GAO
To Report Fraud,
Waste, and Abuse in
Federal Programs
Congressional
Relations
Public Affairs
Strategic Planning and
External Liaison
Please Print on Recycled Paper.
