Enferm
Intensiva.
2018;29(2):86---93
www.elsevier.es/ei
CASE
REPORT
Botulism
in
the
ICU:
Nursing
care
plan
夽
G.
Zariquiey-Esteva
(RN)
a,∗
,
D.
Galeote-Cózar
(RN)
a
,
P.
Santa-Candela
(RN)
b
,
A.
Castanera-Duro
(MSN)
c,d
a
UCI,
Hospital
Universitari
Dr.
Josep
Trueta
de
Girona,
Girona,
Spain
b
Servei
de
Cirurgia
i
Traumatologia,
Hospital
de
Figueres,
Figueres,
Girona,
Spain
c
Unitat
de
Reanimació,
Hospital
Universitari
Dr.
Josep
Trueta
de
Girona,
Girona,
Spain
d
Departament
d’Infermeria,
Universitat
de
Girona,
Girona,
Spain
KEYWORDS
Botulism;
Nerve
block;
Critical
care;
Nursing
care
Abstract
Introduction
and
case
evaluation:
Botulism
is
a
rare
disease
in
Europe,
caused
by
the
bacterium
Clostridium
botulinum,
notifiable,
non-transmissible
person-to-person
and
potentially
fatal
(between
5%
and
10%)
if
not
treated
quickly.
The
favorable
opinion
of
the
Clinical
Research
Ethics
Committee
was
obtained.
We
present
the
nursing
care
plan
of
a
49-year-old
man
with
a
diagnosis
of
bacterial
intoxication
caused
by
Clostridium
botulinum,
secondary
to
ingestion
of
beans
in
poor
condition,
who
was
admitted
to
the
ICU
for
a
total
of
35
days.
Diagnosis
and
planning: Holistic
nursing
evaluation
during
the
first
24
h,
with
prioritisation
of
the
systems
that
were
deteriorating
fastest:
neurological
and
respiratory.
Nine
diagnoses
were
prioritised
according
to
the
NANDA
taxonomy:
risk
for
allergy
response,
ineffective
breathing
pattern,
impaired
oral
mucous
membrane,
impaired
physical
mobility,
risk
for
disuse
syndrome,
risk
for
dysfunctional
gastrointestinal
motility,
impaired
urinary
elimination,
risk
for
acute
confusion
and
risk
for
caregiver
role
strain.
Discussion:
The
nursing
care
plan,
standardised
and
organised
with
the
NANDA
taxonomy
and
prioritised
with
the
outcome-present
state-test
(OPT)
model,
guaranteed
the
best
care
based
on
evidence,
as
the
NOC
scores
improvement
demonstrated.
It
was
impossible
to
compare
the
nursing
intervention
with
other
case
reports.
©
2017
Sociedad
Espa
˜
nola
de
Enfermer
´
ıa
Intensiva
y
Unidades
Coronarias
(SEEIUC).
Published
by
Elsevier
Espa
˜
na,
S.L.U.
All
rights
reserved.
DOI
of
original
article:
https://doi.org/10.1016/j.enfi.2017.07.003
夽
Please
cite
this
article
as:
Zariquiey-Esteva
G,
Galeote-Cózar
D,
Santa-Candela
P,
Castanera-Duro
A.
Botulismo
en
la
UCI:
proceso
de
cuidados.
Enferm
Intensiva.
2018;29:86---93.
∗
Corresponding
author.
E-mail
address:
gzariquiey[email protected]
(G.
Zariquiey-Esteva).
2529-9840/©
2017
Sociedad
Espa
˜
nola
de
Enfermer
´
ıa
Intensiva
y
Unidades
Coronarias
(SEEIUC).
Published
by
Elsevier
Espa
˜
na,
S.L.U.
All
rights
reserved.
Botulism
in
the
ICU:
Nursing
care
plan
87
PALABRAS
CLAVE
Botulismo;
Bloqueo
nervioso;
Cuidados
críticos;
Atención
de
Enfermería
Botulismo
en
la
UCI:
proceso
de
cuidados
Resumen
Introducción
y
valoración
del
caso:
El
botulismo
es
una
enfermedad
poco
frecuente
en
Europa,
causada
por
la
bacteria
Clostridium
botulinum,
de
declaración
obligatoria,
no
transmisible
de
persona
a
persona
y
potencialmente
mortal
(entre
un
5
y
10%)
si
no
se
trata
rápidamente.
Se
obtuvo
el
dictamen
favorable
del
Comité
de
Ética
de
Investigación
Clínica.
Se
presenta
el
proceso
de
cuidados
enfermero
de
un
varón
de
49
a
˜
nos
con
diagnóstico
de
intoxicación
bacteriana
por
Clostridium
botulinum,
secundario
a
la
ingesta
de
alubias
en
mal
estado,
que
estuvo
ingresado
en
la
UCI
un
total
de
35
días.
Diagnósticos
y
planificación: Valoración
enfermera
de
forma
holística
durante
las
primeras
24
h,
con
priorización
de
los
sistemas
que
presentaron
un
deterioro
más
rápido:
el
neurológico
y
el
respiratorio.
Se
priorizaron
9
diagnósticos
según
la
taxonomía
NANDA:
riesgo
de
respuesta
alérgica,
patrón
respiratorio
ineficaz,
deterioro
de
la
mucosa
oral,
deterioro
de
la
movilidad
física,
riesgo
de
síndrome
de
desuso,
riesgo
de
motilidad
gastrointestinal
disfuncional,
deterioro
de
la
eliminación
urinaria,
riesgo
de
confusión
aguda
y
riesgo
de
cansancio
del
rol
del
cuidador.
Discusión:
El
proceso
de
cuidados
enfermero,
estandarizado
y
organizado
con
la
taxonomía
NANDA
y
priorizado
con
el
método
sistemático
AREA,
garantizó
los
mejores
cuidados
basados
en
la
evidencia
y
prueba
de
ello
fue
la
mejoría
de
las
puntuaciones
de
los
indicadores
de
resultado
NOC.
Resultó
imposible
comparar
la
actuación
enfermera
con
la
de
otros
casos
documentados.
©
2017
Sociedad
Espa
˜
nola
de
Enfermer
´
ıa
Intensiva
y
Unidades
Coronarias
(SEEIUC).
Publicado
por
Elsevier
Espa
˜
na,
S.L.U.
Todos
los
derechos
reservados.
Introduction
Botulism
is
a
disease
caused
by
Clostridium
botulinum,
an
anaerobic
gram-positive
bacillus
formed
by
spores
that
produce
a
powerful
neurotoxin.
1
It
is
notifiable,
not
trans-
missible
person-to-person
and
potentially
fatal
(between
5%
and
10%)
if
it
is
not
treated
promptly.
2
The
spores
produced
by
the
C.
botulinum
bacteria,
which
have
been
found
in
green
beans,
spinach,
mush-
rooms,
ham,
sausages,
tinned
tuna
and
fish
(fermented,
salted
and
smoked
2
),
germinate
in
anaerobic
environments,
and
when
they
grow
in
certain
environmental
conditions
create
neurotoxins.
1,2
They
are
heat
resistant
(they
can
survive
at
more
than
100
◦
C
for
5
h
or
more,
but
if
they
are
exposed
to
120
◦
C
for
5
min
they
are
destroyed
1
).
They
do
not
develop
in
acid
media
(although
a
pH
<
4.6
will
not
degrade
an
already
existing
neurotoxin
1
)
and
a
low
temperature
and
salt
content
can
prevent
their
growth.
2
C.
botulinum
is
found
all
over
the
world
and
its
growth
depends
on
environmental
factors.
3
Van
Ermengem
isolated
the
bacteria
in
1897
from
a
badly-cured
ham.
Leuchs,
in
1910,
demonstrated
that
2
strains
of
C.
botulinum
would
produce
toxins
with
different
antigenicities
and
in
1919
Burke
named
them
as
type
A
and
B,
thus
establishing
their
current
alphabetical
designations.
Subsequently,
5
further
types
of
toxins
were
discovered
(C,
D,
E,
F
and
G),
some
with
dual
toxicities.
4
Types
A,
B,
E
and
occasionally
F
can
cause
human
botulism;
A
is
used
cosmetically.
1 --- 3
There
are
6
types
of
human
botulism
1,2
:
food-borne
(through
ingestion
of
foods
contaminated
during
their
prepa-
ration,
processing
or
packaging
1 --- 3
),
infant
(through
ingestion
of
the
spores
that
colonise
the
intestinal
tract
and
release
the
toxin
1 --- 3
),
wound
(generally
due
to
injection
of
black
tar
heroin
1 --- 3
),
adult
intestinal
colonisation
(the
toxin
is
produced
in
vivo
in
the
infected
intestinal
tract
1
),
inhala-
tion
(very
rare,
as
an
act
of
bioterrorism
1,2
)
and
iatrogenic
(through
incorrect
treatment
1
).
Between
2007
and
2015,
cases
of
food
botulism
were
notified
in
some
countries
in
Europe
and
North
America.
According
to
the
World
Health
Organisation,
approximately
35%
were
serious,
with
a
mortality
rate
of
15%,
and
the
disease
lasted
from
5
to
180
days.
The
age
mode
was
50
(min-
imum
age
of
4
and
maximum
of
88)
and
48%
were
males.
5
In
Spain,
according
to
the
Carlos
III
Health
Institute,
the
autonomous
communities
with
the
highest
incidence
of
food
botulism
were
Castile
and
Leon,
Andalusia
and
Madrid,
with
20,
15
and
10
cases,
respectively,
although
they
do
not
spec-
ify
the
severity.
6
In
food
botulism
the
neurotoxins,
created
by
the
diges-
tive
enzymes
after
C.
botulinum
has
been
ingested,
pass
into
the
blood
stream
and
interrupt
the
release
of
acetylcholine,
causing
a
nerve
block
1,2
and
descending
flaccid
paralysis
develops
in
the
motor
and
autonomic
nerves.
2
Symptoms
appear
between
12
and
36
h
after
ingestion
and
are
prin-
cipally
neurological
2
and
gastrointestinal
1,2
:
fatigue,
2
neck
muscle,
2
respiratory
muscle
1,2
and
lower
limb
weakness,
2
vertigo,
2
blurred
vision,
1,2
diplopia,
1
drooping
eyelids,
1
photophobia,
3
symmetric
cranial
neuropathy
2
(speech
and
swallowing
difficulty
and
dry
mouth),
vomiting,
diarrhoea,
constipation
and
abdominal
inflammation.
2
Diagnosis
is
based
on
clinical
history,
physical
examination
1
and
confirmed
by
samples
(faeces
or
wound,
blood
or
food
2,3
).
There
will
be
no
alterations
in
consciousness
1
or
haemodynamic
alterations,
fever
or
sensory
deficit.
2
Differential
diagnosis
will
consider
88
G.
Zariquiey-Esteva
et
al.
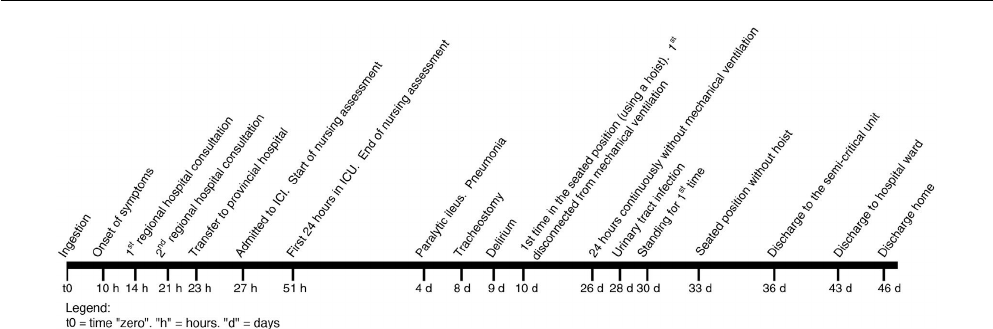
Figure
1
Time
frame
of
progress
from
ingestion
until
discharge
home.
Guillain-Barré
syndrome,
1,2
myasthenia
gravis
1,2
and
cerebral
vascular
accident.
2
Treatment
consists
of
administering
the
botulin
antitoxin
as
promptly
as
possible,
1 --- 3
monitoring
for
signs
of
hypersen-
sitivity
because
it
is
equine-derived,
1
and
overcoming
the
neuromuscular
complications
caused
by
the
poisoning
(respi-
ratory
failure
is
the
primary
cause
of
death
1
).
Antibiotherapy
is
only
indicated
for
wound
botulism.
1 --- 3
Description
of
the
case
A
49-year-old
male,
1.72
m
tall,
weighing
75.9
kg
(body
mass
index
25.66
kg/m
2
).
Allergic
to
pyrazolones,
active
smoker
(1
pack/day).
No
medical
history.
Self-employed
(Barthel
Index
100).
The
patient
attended
his
regional
hospital
with
dizziness,
blurred
vision,
unstable
gait
and
frontal
headache,
of
4-h
onset.
He
mentioned
having
eaten
an
uncertain
amount
of
beans
in
poor
condition
14
h
previously.
On
examination
his
blood
pressure
(BP)
was
160/100
mmHg.
After
3
h
he
was
discharged
diagnosed
with
bacterial
food
poisoning
(Interna-
tional
Classification
of
Disease
[ICD]
005.9).
Fig.
1
shows
the
time
frame
of
the
progression
of
the
disease
from
ingestion
to
discharge.
He
attended
the
emergency
apartment
again
with
droop-
ing
eyelids
in
addition
to
the
abovementioned
symptoms.
The
patient
had
a
dry
mouth,
mydriatic
pupils
with
slow
photomotor
reflex,
bilateral
drooping
eyelids,
and
full
loss
of
eye
motion.
BP
156/99
mmHg.
Arterial
blood
gases
(ABG):
SaO
2
96.6%,
pO
2
78.7
mmHg.
There
were
no
alterations
in
consciousness,
cutaneo-plantar
and
osteotendinous
reflexes
or
on
the
electrocardiogram.
The
patient
was
transferred
to
the
emergency
depart-
ment
of
the
provincial
hospital
with
suspected
C.
botulinum
food
poisoning
(ICD
005.1).
The
patient
now
had
mild
dysarthria
in
addition
to
his
previous
symptoms.
BP
139/98
mmHg.
ABG:
SaO
2
96.4%,
pCO
2
34
mmHg,
pO
2
82
mmHg.
Peak
expiratory
flow
(PEF,
indicator
of
lung
func-
tion,
measured
by
spirometer)
450
l/min
(expected
value
for
his
height,
age
and
sex:
601
±
48
l/min
7
).
Oxygen
ther-
apy
was
started
through
nasal
cannula
and
3
h
later
he
was
admitted
to
the
intensive
care
unit
(ICU).
He
was
given
a
first
dose
of
the
trivalent
botulin
antitoxin
(A,
B,
E)
by
continuous
infusion
through
a
single
line,
and
for
4
h.
Nursing
assessment
During
the
first
24
h
in
ICU
a
holistic
assessment
was
made
of
the
patient
that
highlighted
the
neurological
and
respiratory
system
alterations.
Bilateral
facial
paralysis
was
identified,
neck
muscle
alteration,
proximal
upper
limb
weakness
and
increased
dysarthria.
The
impact
of
the
neuromuscular
block
on
the
respiratory
system
required
orotracheal
intubation
and
mechanical
ventilation,
due
to
dyspnoea
and
increased
respiratory
effort.
The
PaO
2
/FiO
2
ratio,
indicator
of
pul-
monary
oxygen
diffusion
calculated
by
ABG,
considers
there
to
be
acute
lung
injury
below
300
mmHg
8
:
in
only
5
h
it
had
dropped
from
300
mmHg
to
220
mmHg
and
the
PEF
fell
from
220
l/min
to
130
l/min.
In
addition
to
the
neurological
and
respiratory
alter-
ations,
and
after
having
administered
a
total
of
2
doses
of
the
antidote,
the
patient
was
distressed
and
nauseous
(with
preserved
peristalsis).
A
nasogastric
tube
was
passed,
and
a
urinary
catheter
inserted
which
revealed
oliguria
(<400
ml/24
h)
and
a
central
jugular
venous
catheter
to
administer
vasoactive
drugs,
analgesia,
sedation
and
saline.
Over
the
subsequent
34
days,
the
patient
presented
complications
associated
with
intoxication
and
his
stay
in
ICU.
He
was
diagnosed
with
unspecified
hypotension
(ICD
458.9),
pneumonia
caused
by
other
gram-negative
bacte-
ria
(ICD
482.83),
urinary
tract
infection,
site
not
specified
(CIE
599.0)
and
paralytic
ileus
(ICD
560.1).
An
early
tra-
cheostomy
was
performed
after
7
days
to
enable
weaning
and
start
rehabilitation.
The
patient
was
in
ICU
for
a
total
of
35
days,
7
in
a
semi-
critical
unit
and
3
on
the
hospital
ward.
Diagnoses
and
care
planning
(NANDA-NOC-NIC)
The
main
problem
was
approached
by
employing
the
OPT
model
of
clinical
reasoning,
9
focussing
intervention
on
out-
comes
and
not
on
the
health
problems
identified.
The
nursing
objective
was
to
anticipate
the
problems
of
progres-
sion
of
the
patient’s
neuromuscular
paralysis
that
was
found
on
assessment.
Fig.
2
shows
the
nursing
clinical
reasoning
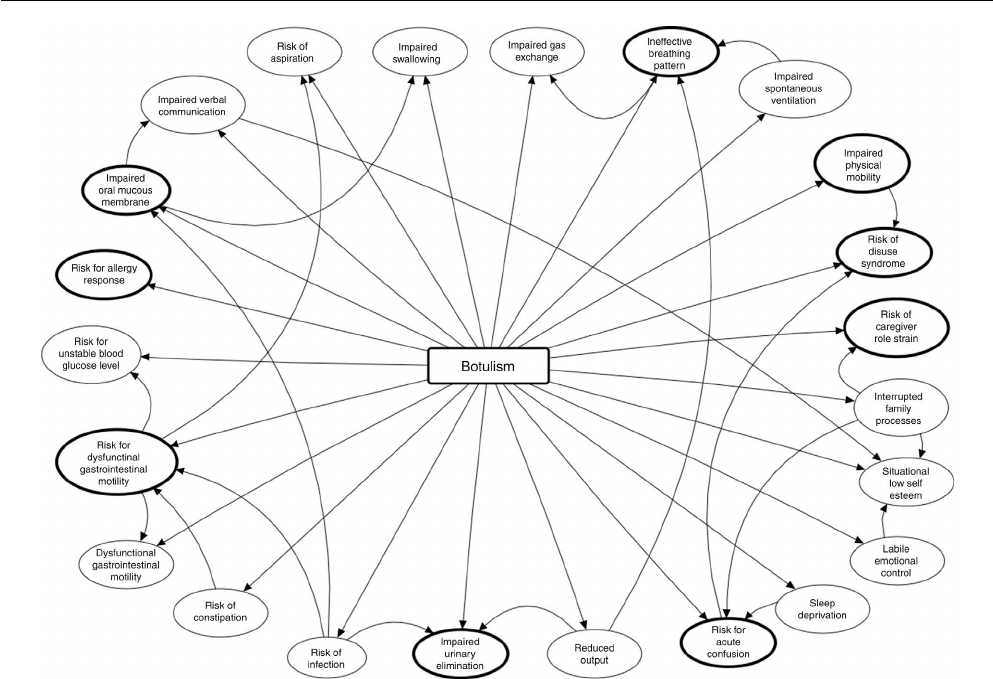
Botulism
in
the
ICU:
Nursing
care
plan
89
Figure
2
Nursing
clinical
reasoning
net,
according
to
the
OPT
model.
net,
as
created
by
Pesut
and
Herman
in
1999.
9
It
shows
the
main
problem,
the
nursing
diagnoses
(ND)
initially
identified
and
their
interrelations.
Note
that
9
of
them
are
those
that
eventually
formed
the
care
process
(Table
1):
these
are
the
most
important
because
if
not
resolved,
the
other
14
would
persist
(except
for
the
risk
of
allergy,
which
derived
directly
from
administration
of
the
antidote).
Table
1
combines
the
ND
(NANDA
10
),
outcomes
(NOC
10
)
and
nursing
interventions
(NIC
10
),
with
their
respective
out-
come
and
activity
indicators.
Table
2
shows
the
assessment
scales
of
the
different
outcome
indicators.
10
Assessment
of
outcomes
Bearing
in
mind
the
natural
course
of
the
disease,
out-
come
indicators
(NOC)
with
deficient
scores
were
inevitable.
The
thorough
neurological
monitoring,
the
deterioration
in
breathing
over
the
first
24
h,
the
early
tracheostomy
and
the
persistent
nursing
action
on
rehabilitation
were
noteworthy.
Discussion
The
case
we
present
confirms
the
need
for
good
coordination
between
practitioners,
in
terms
of
communication,
inter-
vention
and
recording,
since
the
patient
made
good
progress
thanks
to
the
rapid
action
of
the
multidisciplinary
team.
The
nursing
care
process
comprised
a
holistic
assessment
that
flagged
up
the
involvement
of
the
neurological
and
res-
piratory
systems,
and
action
based
on
strict
monitoring
of
the
course
of
the
disease
and
the
constant
moral
and
phys-
ical
support
of
the
patient.
The
use
of
standardised
language
(NANDA-NOC-NIC)
and
systematic
use
of
the
OPT
model
of
clinical
reasoning
enabled
the
nursing
intervention
to
be
organised
and
pri-
oritised,
ensuring
the
best
care
based
on
current
scientific
evidence.
We
found
no
literature
relating
to
the
nursing
care
of
patients
with
botulism
in
ICU;
therefore
it
is
impossible
to
compare
our
action
with
that
of
other
authors.
Ethical
responsibilities
Protection
of
people
and
animals.
The
authors
declare
that
the
research
was
carried
out
according
to
the
ethi-
cal
standards
set
by
the
responsible
human
experimentation
committee,
the
World
Medical
Association
and
the
Helsinki
Declaration.
Data
confidentiality.
The
authors
declare
that
they
have
followed
the
protocols
of
their
centre
of
work
regarding
the
publication
of
patient
data.
Right
to
privacy
and
informed
consent.
The
authors
have
obtained
the
informed
consent
of
the
patients
and/or
sub-
90
G.
Zariquiey-Esteva
et
al.
Table
1
Diagnosis,
outcome
objectives,
interventions
and
nursing
activities
according
to
NANDA-NOC-NIC.
Diagnosis
(NANDA)
Outcome
objectives
(NOC)
Nursing
interventions
(NIC)
00217
Risk
for
allergy
response,
associated
with
exposure
to
allergens
(equine-derived
botulism
antitoxin)
0707
Immune
hypersensitivity
response
6680
Vital
signs
monitoring
070703
allergic
reactions
(5,
scale
n)
Monitor
blood
pressure,
pulse,
temperature
and
respiratory
status,
as
appropriate
6410
allergy
management
Identify
known
allergies
(medication,
food,
insect,
environmental)
and
usual
reaction
Monitor
patient
for
reactions
to
new
medications,
formulas,
foods,
latex
and/or
test
dyes
Monitor
the
patient
after
exposure
to
agents
known
to
cause
allergic
responses
for
signs
of
generalised
flush,
angioedema,
urticaria,
paroxysmal
coughing,
severe
anxiety,
dyspnoea,
wheezing,
orthopnoea,
vomiting,
cyanosis
or
shock
3350
Respiratory
monitoring
Monitor
for
noisy
respirations
such
as
crowing
or
snoring
Monitor
rate,
rhythm,
depth
and
effort
of
respirations
00032
ineffective
breathing
pattern,
related
to
neuromuscular
impairment
and
respiratory
muscle
fatigue,
manifested
by
reduced
vital
capacity
0415
Respiratory
status
3350
Respiratory
monitoring
041503
Depth
of
inspiration
(2,
scale
b)
Monitor
oxygen
saturation
levels
continuously
in
sedated
patients
(SaO2)
per
agency
policy
and
as
indicated
041509
Pulmonary
function
tests
(1,
scale
b)
Monitor
results
of
pulmonary
function
tests,
particularly
vital
capacity,
maximal
inspiratory
force,
forced
expiratory
volume
in
1
s
(FEV1),
and
FEV
monitor
1/FVC,
as
available
Monitor
for
dyspnoea
and
events
that
improve
and
worsen
it
3320
Oxygen
therapy
Administer
supplemental
oxygen
as
ordered
Monitor
the
effectiveness
of
oxygen
therapy
(pulse
oximetry,
ABGs),
as
appropriate
0402
Respiratory
status:
gas
exchange
5820
Anxiety
reduction
040203
Dyspnoea
at
rest
(3,
scale
n)
Monitor
the
patient’s
anxiety
in
relation
for
the
need
for
oxygen
therapy
040205
Restlessness
(3,
scale
n)
040208
Partial
pressure
of
oxygen
in
arterial
blood
(PaO2)
(4,
scale
b)
0008
Fatigue:
Disruptive
Effects
3120
Airway
Insertion
and
Stabilisation
0803
Reduced
Energy
(2,
scale
n)
Assist
with
insertion
of
an
endotracheal
tube
by
gathering
necessary
intubation
and
emergency
equipment,
positioning
patient,
administering
medications
as
ordered,
and
monitoring
the
patient
for
complications
during
insertion
Instruct
patient
and
family
about
the
intubation
procedure
Monitor
mechanical
ventilator
readings,
noting
increases
in
inspiratory
pressures
and
decreases
in
tidal
volume,
as
appropriate
3180
Artificial
Airway
Management
Maintain
inflation
of
the
endotracheal/tracheostomy
cuff
at
15---25
mmHg
during
mechanical
ventilation
and
during
and
after
feeding
Institute
endotracheal
suctioning,
as
appropriate
Monitor
secretions
colour,
amount,
and
consistency
Institute
measures
to
prevent
spontaneous
decannulation:
secure
artificial
airway
with
tape
or
ties,
administer
sedation
and
muscle
paralysing
agent,
use
arm
restraints,
as
appropriate
00045
Impaired
oral
mucous
membrane,
related
to
reduced
salivation
and
manifested
by
dry
mouth
1100
Oral
hygiene
1730
Oral
Health
Restoration
110010
Moisture
of
oral
mucosa
and
tongue
(2,
scale
a)
Monitor
condition
of
the
patient’s
mouth
(tongue,
mucous
membranes),
including
character
of
abnormalities
Administer
mouthwash
(antibacterial
solution)
Apply
lubricant
to
moisten
lips
and
oral
mucosa,
as
needed
1720
Provide
oral
care
for
unconscious
patient
using
appropriate
precautions
Encourage
and
assist
patient
to
rinse
mouth
00085
Impaired
physical
mobility
related
to
neuromuscular
involvement,
as
manifested
by
limited
ability
to
perform
gross
and
fine
motor
skills
0208
Mobility
0226
Exercise
therapy:
muscle
control
020802
body
positioning
performance
(4,
scale
a)
Assist
patient
to
sitting/standing
position
for
exercise
protocol,
as
appropriate
020803
Muscle
movement
(4,
scale
a)
Encourage
the
patient
to
self-exercise
020809
Coordination
(4,
scale
a)
Monitor
the
emotional,
cardiovascular
and
functional
response
of
the
patient
to
the
exercise
protocol
Provide
positive
reinforcement
for
patient’s
efforts
in
exercise
and
physical
activity
Assist
patient
to
participate
in
stretching
exercises
when
lying,
sitting,
or
standing
Assist
patient
to
move
to
sitting
position,
stabilise
trunk
with
arms
placed
at
the
side
on
bed/chair,
and
rock
trunk
over
supporting
arm
0212
Coordinated
movement
0224
Exercise
therapy:
joint
mobility
021203
Speed
of
movement
(2,
scale
a)
Assist
patient
to
optimal
body
position
for
passive/active
joint
movement
021204
Smooth
movement
(2,
scale
a)
Perform
passive
or
assisted
range
of
movement
exercises
021205
Control
of
movement
(2,
scale
a)
Encourage
to
sit
in
bed,
on
side
of
bed,
or
in
chair
021207
Balanced
movement
(4,
scale
a)
Provide
positive
reinforcement
for
performing
joint
exercises
0210
Transfer
performance
1806
Self-care
assistance:
transfer
021001
Transfer
from
bed
to
chair
(1,
scale
a)
Determine
current
ability
of
patient
to
transfer
self
(e.g.,
mobility
level,
limitations
of
movement,
endurance,
ability
to
stand
and
bear
weight,
medical
or
orthopaedic
instability)
Botulism
in
the
ICU:
Nursing
care
plan
91
Table
1
(Continued)
Diagnosis
(NANDA) Outcome
objectives
(NOC) Nursing
interventions
(NIC)
Provide
encouragement
to
patient
as
he/she
learns
to
transfer
independently
Determine
amount
and
type
of
assistance
needed
Lift
and
move
patient
with
hoist
Evaluate
patient
at
end
of
transfer
for
proper
body
alignment,
nonocclusion
of
tubes,
wrinkled
linens,
unnecessarily
exposed
skin,
adequate
patient
level
of
comfort,
raised
side
rails,
and
call
bell
within
reach
0005
Activity
tolerance 0180
Energy
management
000502
Pulse
rate
with
activity
(5,
scale
a) Monitor
cardiorespiratory
response
to
activity
(e.g.,
tachycardia,
other
dysrhythmias,
dyspnoea,
diaphoresis,
pallor,
haemodynamic
pressures,
respiratory
rate)
000508
Respiratory
rate
with
activity
(4,
scale
a)
00040
Risk
for
disuse
syndrome,
related
to
paralysis
0204
Immobility
consequences:
physiological 5612
Teaching:
prescribe
exercise
020412
Muscle
tone
(1,
scale
a)
Inform
the
patient
of
the
purpose
for,
and
the
benefits
of,
the
prescribed
exercise
Teach
the
patient
how
to
do
the
prescribed
exercise
Reinforce
information
provided
by
other
health
care
team
members,
as
appropriate
0201
Exercise
promotion:
strength
training
Collaborate
with
family
and
other
health
professionals
(e.g.,
activity
therapist,
exercise
physiologist,
occupational
therapist,
recreational
therapist,
physiotherapist)
planning,
teaching,
and
monitoring
a
muscle
training
programme
0914
Neurological
status:
Spinal
Sensory/Motor
Function
2620
Neurological
monitoring
091401
Head
and
shoulder
movement
(2,
scale
a)
Monitor
pupillary
size,
shape,
symmetry,
and
reactivity
091405
Upper
body
strength
(2,
scale
a) Monitor
level
of
consciousness
091406
Flaccidity
(3,
scale
n) Monitor
level
of
orientation
0912
Neurological
status:
consciousness Monitor
trend
of
Glasgow
coma
scale
091201
Opens
eyes
to
external
stimuli
(1,
scale
a)
Monitor
cough
and
gag
reflex
91213
Delirium
(2,
scale
n)
Monitor
facial
symmetry
Monitor
EOMs
and
gaze
characteristics
Monitor
for
visual
disturbance:
diplopia,
nystagmus,
visual-field
cuts,
blurred
vision,
visual
acuity
00197
Risk
for
dysfunctional
gastrointestinal
motility,
related
to
ingestion
of
contaminated
foods
0501
Bowel
elimination 2300
Medication
administration
050101
Elimination
pattern
(1,
scale
a) Monitor
patient
for
the
therapeutic
effect
of
the
medication
050129
Bowel
sounds
(2,
scale
a)
Document
the
administration
of
medication
and
the
patient’s
response
capacity,
per
agency
protocol
2380
Medication
management
Monitor
patient
for
the
therapeutic
effect
of
the
medication
1015
Gastrointestinal
function
1570
Vomiting
management
101501
Food
tolerance
(1,
scale
a) Measure
or
estimate
emesis
volume
101510
Amount
of
residual
gastric
aspirates
(1,
scale
a)
Ensure
effective
antiemetic
drugs
are
given
to
prevent
vomiting,
when
possible
101530
Gastric
reflux
(1,
scale
n)
Monitor
fluid
and
electrolyte
balance
1874
Tube
care:
gastrointestinal
Check
that
the
tube
is
correctly
in
place
monitoring
for
signs
and
symptoms
of
tracheal
positioning,
checking
the
colour
and
and/or
pH
of
aspirate,
inspecting
the
oral
cavity
and/or
verify
placement
by
X-ray,
if
appropriate
Initiate
and
monitor
delivery
of
enteral
tube
feedings,
as
appropriate
per
agency
protocol
Monitor
amount,
colour,
and
consistency
of
nasogastric
output
Monitor
for
sensations
of
fullness,
nausea,
and
vomiting
Connect
tube
to
suction,
as
appropriate
1056
Enteral
tube
feeding
Check
residual
every
4 --- 6
h
for
the
first
24
h,
then
every
8
h
during
continuous
feedings
Check
residual
before
each
intermittent
feeding
Hold
tube
feedings
if
residual
is
greater
than
150
cc
or
more
than
110---120%
of
the
of
the
hourly
rate
in
adults
1200
Total
parenteral
nutrition
administration
Encourage
a
gradual
transition
from
parenteral
to
enteral
feeding,
if
indicated
2301
Medication
response 1080
Gastrointestinal
intubation
230101
Expected
therapeutic
effects
(3,
scale
a)
Administer
medication
to
increase
peristalsis,
if
indicated
00016
Impaired
urinary
elimination,
related
to
sensory-motor
impairment,
as
manifested
by
oliguria
0503
Urinary
elimination 4120
Fluid
management
050303
Urine
amount
(2,
scale
a)
Maintain
accurate
intake
and
output
record
0601
Fluid
balance Insert
urinary
catheter,
if
appropriate
060107
24-hour
intake
and
output
balance
(3,
scale
a)
Administer
prescribed
diuretic
drugs,
if
appropriate
Administer
prescribed
I.V.
therapy
92
G.
Zariquiey-Esteva
et
al.
Table
1
(Continued)
Diagnosis
(NANDA)
Outcome
objectives
(NOC)
Nursing
interventions
(NIC)
4130
Fluid
monitoring
Determine
possible
risk
factors
for
fluid
imbalance
(diuretic
therapy,
infection)
Examine
skin
turgor
by
pinching
the
skin
gently
holding
it
for
a
second
and
releasing
(skin
will
fall
back
quickly
if
patient
is
well
hydrated)
Monitor
serum
and
urine
electrolyte
values,
as
appropriate
Monitor
BP,
heart
rate,
and
respiratory
status
Keep
an
accurate
record
of
intake
and
output
(enteral
intake,
IV
intake,
antibiotics,
fluids
given
with
medications,
NG
tubes,
vomit)
Monitor
colour,
quantity,
and
specific
gravity
of
urine
00173
Risk
for
acute
confusion
aguda,
related
to:
0901
Cognitive
orientation
4820
Reality
orientation
---
pharmacological
agents
90101
Identifies
self
(5,
scale
a)
Address
patient
by
name
when
initiating
interaction
---
disorders
of
sleep-wake
cycle
90102
Identifies
significant
other
(5,
scale
a)
Speak
to
the
patient
in
a
distinct
manner
with
an
appropriate
pace,
volume,
and
tone
---
impaired
mobility
90103
Identifies
current
space
(5,
scale
a)
90105
Identifies
correct
month
(5,
scale
a)
Inform
patient
of
person,
place,
and
time,
as
needed
Engage
the
patient
in
concrete
‘‘here
and
now’’
activities
(ADL)
that
focus
on
something
outside
the
self
that
is
concrete
and
reality
oriented
5270
Emotional
support
Discuss
with
the
patient
the
emotional
experience
Make
supportive
or
empathetic
statements
6430
Chemical
restraint
Monitor
the
patient’s
response
to
the
medication
Monitor
level
of
consciousness
5820
Anxiety
reduction
Provide
factual
information
concerning
diagnosis,
treatment,
and
prognosis
Identify
when
level
of
anxiety
changes
Help
patient
identify
situations
that
precipitate
anxiety
Administer
medications
to
reduce
anxiety,
as
appropriate
7560
Visitation
facilitation
Determine
patient’s
preferences
for
visitation
and
release
of
information
Determine
the
need
to
promote
visits
by
family
and
friends
Encourage
the
family
member
to
use
touch,
as
well
as
verbal
communication,
as
appropriate
00062
Risk
for
caregiver
role
strain,
related
to
unpredictable
illness
course
(applied
to
the
family)
1803
Knowledge:
disease
process
7040
Caregiver
support
180302
Characteristics
of
specific
disease
(2,
scale
u)
Determine
caregiver’s
level
of
knowledge
180303
Cause
and
contributing
factors
(1,
scale
u)
Determine
caregiver’s
acceptance
of
role
180305
Physiological
effects
of
disease
(2,
scale
u)
Acknowledge
difficulties
of
caregiving
role
180307
Usual
course
of
disease
process
(2,
scale
u)
Acknowledge
dependency
of
patient
on
caregiver
(as
appropriate)
180309
Potential
complications
of
disease
(3,
scale
u)
Make
positive
statements
about
caregiver’s
effort
Provide
support
for
decisions
made
by
caregiver
Provide
information
about
patient’s
condition
in
accordance
with
patient
preferences
Identify
sources
of
respite
care
Support
caregiver
in
setting
limits
and
taking
care
of
self
Taken
from
NNNConsult.
10
Botulism
in
the
ICU:
Nursing
care
plan
93
Table
2
Likert
scales
to
assess
outcome
indicators.
Scale
a
Severely
compromised
Substantially
compromised
Moderately
compromised
Mildly
compromised
Not
compromised
Scale
b:
Severe
deviation
from
normal
range
Substantial
deviation
from
normal
range
Moderate
deviation
from
normal
range
Mild
deviation
from
normal
range
No
deviation
from
normal
range
Scale
n:
Severe
Substantial
Moderate
Mild
None
Scale
u
No
knowledge
Limited
knowledge
Moderate
knowledge
Substantial
knowledge
Extensive
knowledge
Taken
from
NNNConsult.
10
jects
referred
to
in
the
article.
This
document
is
held
by
the
corresponding
author.
Conflict
of
interest
The
authors
have
no
conflict
of
interest
to
declare.
Acknowledgements
We
would
like
to
thank
all
the
professionals
who
docu-
mented,
provided
and
contributed
towards
the
compilation
of
information.
References
1.
Pegram
PS,
Stone
SM.
Botulism;
2017.
Available
at:
http://www.
uptodate.com/contents/botulism
[updated
07.03.16;
accessed
10.11.16].
2.
OMS.
Botulismo.
OMS;
2014.
Available
at:
http://www.
who.int/mediacentre/factsheets/fs270/es/
[accessed
03.11.16].
3.
Botulism.
Ames,
Iowa:
The
Center
for
Food
Security
&
Public
Health;
2010.
Available
at:
http://www.cfsph.
iastate.edu/Factsheets/pdfs/botulism.pdf
[accessed
04.11.16].
4.
Barash
JR,
Arnon
SS.
A
novel
strain
of
Clostridium
botulinum
that
produces
type
B
and
type
H
botulinum
toxins.
J
Infect
Dis.
2014;209:183---91.
Available
at:
https://academic.
oup.com/jid/article/209/2/183/828053/A-Novel-Strain-of-
Clostridium-botulinum-That
[accessed
03.11.16].
5.
WHO.
WHO
estimates
of
the
global
burden
of
foodborne
diseases.
Foodborne
disease
burden
epidemiology
reference
group
2007---20015.
WHO;
2015.
Available
at:
http://apps.who.
int/iris/bitstream/10665/199350/1/9789241565165
eng.pdf
[accessed
08.11.16].
6.
Epidemiología.
Enfermedades
de
declaración
obligatoria-Series
temporales.
Instituto
de
Salud
Carlos
III;
2016.
Available
at:
http://www.isciii.es/ISCIII/es/contenidos/fd-servicios-
cientifico-tecnicos/fd-vigilancias-alertas/fd-enfermedades/
enfermedades-declaracion-obligatoria-series-temporales.shtml
[accessed
08.11.16].
7.
Miquel-Gomara
JP,
Román
MR.
Medidor
de
Peak-flow:
técnica
de
manejo
y
utilidad
en
Atención
Primaria.
Med-
ifam.
2002;12:206---13.
Available
at:
http://scielo.isciii.
es/pdf/medif/v12n3/tecnicas.pdf
[accessed
15.01.17].
8.
Ramos
L,
Benito
S.
Interpretación
de
los
gases
en
san-
gre.
In:
Serra
R,
editor.
Fundamentos
de
la
ventilación
mecánica.
1st
ed.
Barcelona:
Marge
Médica
Books;
2012.
p.
23---32.
9.
Pesut
DJ,
Herman
J.
The
OPT
model
of
clinical
rea-
soning.
In:
William
Brottmiller,
editor.
Clinical
reasoning.
The
art
&
science
of
critical
&
creative
thinking.
1st
ed.
Albany,
New
York:
Delmar
Publishers;
1999.
p.
31---45.
10.
NNNConsult.
Barcelona:
Elsevier
Espa
˜
na;
2016.
Available
at:
http://www.nnnconsult.com/
[updated
2016;
accessed
17.01.17].
