/
\
PB96-910406
NTSB/AAR-96/06
DCA95MA054
NATIONAL
TRANSPORTATION
SAFETY
BOARD
WASHINGTON,
D.C.
20594
AIRCRAFT ACCIDENT REPORT
IN-FLIGHT LOSS OF PROPELLER BLADE
FORCED LANDING, AND COLLISION WITH TERRAIN
ATLANTIC SOUTHEAST AIRLINES, INC., FLIGHT 529
EMBRAER
EMB-120RT,
N256AS
CARROLLTON,
GEORGIA
AUGUST 21, 1995
6609B

The National Transportation Safety Board is an independent Federal agency dedicated to
promoting aviation, railroad, highway, marine, pipeline, and hazardous materials safety.
Established in 1967, the agency is mandated by Congress through the Independent Safety
Board Act of 1974 to investigate transportation accidents, determine the probable causes of
the accidents, issue safety recommendations, study transportation safety issues, and evaluate
the safety effectiveness of government agencies involved in transportation. The Safety
Board makes public its actions and decisions through accident reports, safety studies, special
investigation reports, safety recommendations, and statistical reviews.
Information about available publications may be obtained by contacting:
National Transportation Safety Board
Public Inquiries Section,
RE-51
490
L’Enfant
Plaza,
S.W.
Washington,
D.C.
20594
(202)382-6735
(800)877-6799
Safety Board publications may be purchased, by individual copy or by subscription, from:
National Technical Information Service
5285
Port
Royal
Road
Springfield, Virginia 22161
(703)487-4600

NTSB/AAR-96/06 PB96-910406
NATIONAL TRANSPORTATION
SAFETY BOARD
WASHINGTON, D.C. 20594
AIRCRAFT ACCIDENT REPORT
IN-FLIGHT LOSS OF PROPELLER BLADE
FORCED LANDING
AND COLLISION WITH TERRAIN
ATLANTIC SOUTHEAST AIRLINES, INC., FLIGHT 529
EMBRAER EMB-120RT, N256AS
CARROLLTON, GEORGIA
AUGUST 21, 1995
Adopted: November 26, 1996
Notation 6609B
Abstract:
This report explains the accident involving Atlantic Southeast Airlines flight
529, an EMB-120RT airplane, which experienced the loss of a propeller blade and
crashed during an emergency landing near Carrollton, Georgia, on August 21, 1995.
Safety issues in the report focused on manufacturer engineering practices, propeller
blade maintenance repair, propeller testing and inspection procedures, the relaying of
emergency information by air traffic controllers, crew resource management training, and
the design of crash axes carried in aircraft. Recommendations concerning these issues
were made to the Federal Aviation Administration.

this page intentionally left blank

iii
CONTENTS
EXECUTIVE SUMMARY .................................................................. v
1. FACTUAL INFORMATION
1.1 History of Flight ..................................................................................... 1
1.2 Injuries to Persons .................................................................................. 5
1.3 Damage to Airplane................................................................................ 5
1.4 Other Damage......................................................................................... 6
1.5 Personnel Information ............................................................................ 6
1.6 Airplane Information.............................................................................. 7
1.6.1 General.................................................................................................... 7
1.6.2 Weight and Balance................................................................................ 8
1.6.3 Propeller Design ..................................................................................... 8
1.6.4 Airplane and Propeller Design Requirements on Released Blades....... 10
1.6.5 Airworthiness Standards for Engines and Propellers............................. 12
1.7 Meteorological Information ................................................................... 13
1.8 Aids to Navigation.................................................................................. 15
1.9 Communications..................................................................................... 15
1.10 Airport Information ................................................................................ 16
1.11 Flight Recorders ..................................................................................... 16
1.12 Wreckage and Impact Information......................................................... 17
1.12.1 Fuselage .................................................................................................. 18
1.12.2 Wings...................................................................................................... 19
1.12.3 No. 1 (Left) Engine Nacelle ................................................................... 19
1.12.4 No. 2 (Right) Engine Nacelle................................................................. 20
1.13 Medical and Pathological Information................................................... 20
1.14 Fire.......................................................................................................... 21
1.15 Survival Aspects..................................................................................... 21
1.16 Tests and Research ................................................................................. 23
1.16.1 Laboratory Examination of the Fractured Propeller Blade.................... 23
1.16.2 Previous Failures of Similar Model Propellers...................................... 26
1.16.3 Blade Inspection and Repair - Actions Taken by
Hamilton Standard and the FAA........................................................... 28
1.16.4 The Failed Propeller, Information, and Service History........................ 36
1.16.5 Results of 14RF-9/EMB-120 Stress Survey .......................................... 39
1.17 Organizational and Management Information....................................... 44
1.17.1 Hamilton Standard Division, United Technologies Corporation .......... 44
1.17.2 Hamilton Standard Propeller Customer Service Center ........................ 45
1.17.2.1 Employee Training at Hamilton Standard Customer Service Center.... 45

iv
1.17.3 Designated Engineering Representative ................................................ 46
1.17.4 FAA Certification Engineer ................................................................... 47
1.18 Additional Information........................................................................... 48
1.18.1 Safety Board Recommendations ............................................................ 48
1.18.2 Postaccident Hamilton Standard and FAA Actions............................... 50
2. ANALYSIS
2.1 General.................................................................................................... 53
2.2 Analysis of the Propeller Blade Failure ................................................. 53
2.2.1 The Accident Blade’s June 1994 Inspection, Repair,
and Return to Service ........................................................................... 54
2.2.1.1 Inappropriate Use of PS960A Blending Repair .................................... 54
2.2.1.2 Sanding (Blending) of the Accident Blade ............................................ 56
2.2.2 Adequacy of Hamilton Standard Procedures for Detecting Corrosion . 59
2.2.2.1 Borescope Inspection.............................................................................. 59
2.2.2.2 Technician Training and Supervision .................................................... 60
2.2.2.3 Adequacy of Improvements to Inspection Procedures .......................... 61
2.3 Effect of Blade Resonance ..................................................................... 62
2.4 Adequacy of Vibration Testing.............................................................. 65
2.5 Effect of Blade Failure and Analysis of Terminating Action................ 66
2.6 FAA Oversight........................................................................................ 68
2.6.1 Role of Designated Engineer Representative and FAA
Certifying Engineer ............................................................................... 68
2.7 Weather................................................................................................... 69
2.8 Air Traffic Control Services................................................................... 70
2.9 Survival Factors Aspects........................................................................ 72
2.9.1 Time Management During Emergencies................................................ 72
2.9.2 Crash Axes.............................................................................................. 74
3. CONCLUSIONS
3.1 Findings .................................................................................................. 75
3.2 Probable Cause ....................................................................................... 79
4. RECOMMENDATIONS ..................................................................... 80
5. APPENDIXES
Appendix A--Investigation and Hearing................................................ 83
Appendix B--Cockpit Voice Recorder Transcript ................................. 84
Appendix C--Fracture Summary............................................................ 110
Appendix D--EMB-120/14RF-9 Stress Resurvey
................................. 111

v
EXECUTIVE SUMMARY
On August 21, 1995, about 1253 eastern daylight time, an
Empresa Brasileira de Aeronautica S. A. (Embraer) EMB-120RT, N256AS,
airplane operated by Atlantic Southeast Airlines Inc., (ASA) as ASE flight
529, experienced the loss of a propeller blade from the left engine propeller
while climbing through 18,100 feet. The airplane then crashed during an
emergency landing near Carrollton, Georgia, about 31 minutes after
departing the Atlanta Hartsfield International Airport, Atlanta, Georgia.
The flight was a scheduled passenger flight from Atlanta to Gulfport,
Mississippi, carrying 26 passengers and a crew of 3, operating according to
instrument flight rules, under the provisions of Title 14 Code of Federal
Regulations Part 135. The flightcrew declared an emergency and initially
attempted to return to Atlanta. The flightcrew then advised that they were
unable to maintain altitude and were vectored by air traffic control toward
the West Georgia Regional Airport, Carrollton, Georgia, for an emergency
landing. The airplane continued its descent and was destroyed by ground
impact forces and postcrash fire. The captain and four passengers sustained
fatal injuries. Three other passengers died of injuries in the following 30
days. The first officer, the flight attendant, and 11 passengers sustained
serious injuries, and the remaining 8 passengers sustained minor injuries.
The National Transportation Safety Board determines that the
probable cause of this accident was the in-flight fatigue fracture and
separation of a propeller blade resulting in distortion of the left engine
nacelle, causing excessive drag, loss of wing lift, and reduced directional
control of the airplane. The fracture was caused by a fatigue crack from
multiple corrosion pits that were not discovered by Hamilton Standard
because of inadequate and ineffective corporate inspection and repair
techniques, training, documentation, and communications.
Contributing to the accident was Hamilton Standard’s and the
Federal Aviation Administration’s failure to require recurrent on-wing
ultrasonic inspections for the affected propellers.
Contributing to the severity of the accident was the overcast
cloud ceiling at the accident site.

vi
Safety issues in the report focused on manufacturer engineering
practices, propeller blade maintenance repair, propeller testing and
inspection procedures, the relaying of emergency information by air traffic
controllers, crew resource management training, and the design of crash
axes carried in aircraft. Recommendations concerning these issues were
made to the Federal Aviation Administration.

NATIONAL TRANSPORTATION SAFETY BOARD
WASHINGTON, D.C. 20594
AIRCRAFT ACCIDENT REPORT
IN-FLIGHT LOSS OF PROPELLER BLADE
FORCED LANDING
AND COLLISION WITH TERRAIN
ATLANTIC SOUTHEAST AIRLINES, INC., FLIGHT 529
EMBRAER EMB-120RT, N256AS,
CARROLLTON, GEORGIA
AUGUST 21, 1995
1. FACTUAL INFORMATION
1.1 History of Flight
On August 21, 1995, about 1253
1
eastern daylight time, an Empresa
Brasileira de Aeronautica S.A. (Embraer) EMB-120RT, N256AS, airplane
operated by Atlantic Southeast Airlines Inc., (ASA
2
) as ASE
3
flight 529,
4
experienced the loss of a propeller blade from the left engine propeller while
climbing through 18,100 feet. The airplane then crashed during an emergency
landing near Carrollton, Georgia, about 31 minutes after departing the Atlanta
Hartsfield International Airport (ATL), Atlanta, Georgia. The flight was a
scheduled passenger flight from ATL to Gulfport, Mississippi (GPT), carrying 26
passengers and a crew of 3, operating according to instrument flight rules (IFR),
under the provisions of Title 14 Code of Federal Regulations (CFR) Part 135. The
flightcrew declared an emergency and initially attempted to return to Atlanta. The
flightcrew then advised air traffic control (ATC) that they were unable to maintain
altitude and were vectored toward the West Georgia Regional Airport (CTJ),
Carrollton, Georgia, for an emergency landing. The airplane continued its
1
All times are reported in eastern daylight time unless noted.
2
The Atlantic Southeast Airlines Inc., corporate logo and airplane paint scheme are
represented by the letters ASA.
3
The air traffic control system call sign for flights of Atlantic Southeast Airlines is ASE.
4
Because a code sharing agreement existed between ASA and Delta Air Lines, passenger
flight schedules also identified the airplane as Delta flight 7529.

2
descent, passed through some trees, and was destroyed by impact forces with the
ground and postcrash fire. The captain and four passengers sustained fatal
injuries. Three other passengers died of injuries in the following 30 days. The
first officer, the flight attendant, and 11 passengers sustained serious injuries,
5
and
the remaining 8 passengers sustained minor injuries.
On August 21, 1995, the accident flightcrew began a 2-day trip at
Macon, Georgia (MCN). They operated the accident airplane, N256AS, as flight
ASE 211 from MCN to ATL. A jump seat rider, an ASA captain, reported that the
flight was uneventful and that the crew appeared to be rested and in a relaxed
mood during the flight.
In ATL, the captain remained in the airplane on the ground to receive
the ATC clearance; the first officer deplaned and remained in the immediate area.
The accident flight, ASE 529, was cleared IFR from ATL to GPT via the Atlanta 4
departure and flight planned route at flight level 240.
6
The estimated flight time
was 1 hour and 26 minutes. The ASA EMB-120 load manifest prepared by the
first officer recorded 26 passengers, 3 crewmembers, 724 pounds of cargo, and
2,700 pounds of fuel for departure.
ASE 529 taxied from the ramp area at 1210 and was airborne at 1223.
At 1236, the first officer reported to the west departure sector of the Atlanta air
route traffic control center (Atlanta Center) that they were climbing past 13,000
feet. About 1242, following several intermediate climb clearances, the controller
issued a clearance to climb and maintain flight level 240, which the flightcrew
acknowledged.
The flight data recorder (FDR) and the cockpit voice recorder (CVR)
data
7
indicated that at 1243:25, while climbing through 18,100 feet at 160 knots
indicated airspeed (KIAS), several thuds could be heard from the cockpit, and the
torque on the left engine decreased to zero. The airplane then rolled to the left,
pitched down, and subsequently started to descend. Immediately thereafter, the
FDR shows numerous flight control inputs consistent with an attempt to
counteract the flightpath deviations; however, the airplane attitude decreased to
5
Section 1.2 contains more details regarding serious injuries.
6
Flight level 240 represents a barometric altimeter indication of 24,000 feet.
7
Appendix B contains the transcript of the CVR. All relevant ATC communications with
ASE 529 are contained in the transcript.

3
about 9 degrees nose low, and the airplane began a descent rate that progressed to
about 5,500 feet per minute (fpm). The captain said, “I can’t hold this thing,” then
“help me hold it.” At 1244:26, the first officer declared an emergency with
Atlanta Center and stated, “we’ve had an engine failure.” Atlanta Center cleared
ASE 529 direct to the Atlanta airport.
According to data from the FDR and CVR, airspeed and descent rate
changes continued and were accompanied by abrupt excursions in vertical and
lateral acceleration values. At 1245:46, the CVR revealed that the first officer
informed the flight attendant that they had experienced an engine failure, had
declared an emergency and were returning to ATL, and he told her to brief the
passengers. At 1246:13, the first officer stated, “we’re going to need to keep
descending, we need an airport quick and uh, roll the trucks and everything for
us.” The controller provided the flightcrew with heading information to CTJ. The
flightcrew applied various combinations of flight control inputs and power on the
right engine, partially stabilizing the airplane descent rate to between 1,000 and
2,000 fpm and the airspeed to between 153 and 175 knots indicated airspeed
(KIAS).
The Atlanta Center controller lost ASE 529’s transponder code from
radar when the airplane descended through 4,500 feet. About 1250, he instructed
the flightcrew to contact Atlanta approach control. The flightcrew contacted
Atlanta approach and requested the localizer frequency and vectors for the West
Georgia Regional Airport. The controller issued the localizer frequency. The
flightcrew acknowledged and then requested vectors for a visual approach. The
controller verified the altitude of the airplane and that the flight was in visual
flight rules (VFR) conditions and said, “fly heading zero four zero...airport’s at
your about 10 o’clock six miles....” At 1251:47, ASE 529 acknowledged, “zero
four zero ASE 529.” This transmission was the last one received by the approach
controller from the accident flight. After 1251:30, airspeed steadily decreased
from 168 KIAS to about 120 KIAS. FDR and CVR information indicated that the
landing gear and flaps remained retracted. CVR sounds indicated that the first
ground impact occurred about 1252:45.
In postcrash interviews, survivors indicated that during the climbout,
they heard a loud sound and felt the airplane shudder. They also indicated that
two or three blades from the left propeller were wedged against the front of the

4
Figure 1.--Propeller installation - left wing.

5
wing. The flight attendant said that she looked out the left side of the aircraft and
observed, “a mangled piece of machinery where the propeller and the front part of
the cowling was.” Other passengers observed the propeller displaced outboard
from its original position on the engine (see Figure 1). The flight attendant stated
that after the first officer notified her of the flight’s emergency return to ATL (at
1245:46), she prepared the cabin for an emergency landing and evacuation. She
stated that she had no further dialogue with the flightcrew.
Investigators found the left engine propeller assembly early in the
ground debris path. The propeller hub contained three complete blades and about
1 foot of the inboard end of the fourth blade protruding from the hub. The
remainder of the fourth blade was not at the accident site. (See Section 1.12 for
more wreckage information.)
The accident took place in daylight visual conditions. The crash site
was located at 33 degrees, 34’, 50.5” north latitude and 85 degrees, 12’, 51.2” west
longitude. A topographical map indicated that the elevation of the site was 1,100
feet above sea level.
1.2 Injuries to Persons
Injuries
Flightcrew Cabincrew Passengers Other Total
Fatal 1 0 7 0 8
Serious 1 1 11
8
0 13
Minor 0 0 8 0 8
None 0
0 0 0 0
Total 2 1 26 0 29
1.3 Damage to Airplane
The airplane was destroyed by the impact and postcrash fire. Its
estimated value was $5,000,000.
8
One passenger died 4 months after the accident as a result of her injuries. She sustained
third-degree burns over 50 percent of her body, as well as inhalation injuries. In accordance with
49 CFR 830.2, which defines “fatal injury” as any injury that results in death within 30 days of
the accident, her injuries were classified as “serious.”
6
1.4 Other Damage
The crash site was located on 20 acres of unimproved farmland with
trees, adjacent to an open field. There was environmental damage from airplane
fuel and fire-fighting efforts along the wreckage path, and immediately adjacent to
the wreckage.
1.5 Personnel Information
The captain, age 45, held an airline transport pilot certificate for
airplane multiengine land, type rated in the EMB-120, with commercial privileges
for airplane single-engine land. He held a flight instructor certificate with ratings
for airplane, instrument, and multiengine. His most recent Federal Aviation
Administration (FAA) first-class medical certificate was issued on April 3, 1995,
with the limitation: “Holder shall wear correcting lenses for near vision while
exercising the privileges of his airman certificate.” The captain’s overnight bag,
found in the wreckage, contained an empty eyeglasses case.
The captain was employed by ASA in March 1988. Company records
indicate that at the time of the accident, he had accumulated 9,876.13 total hours
of flying experience, with 7,374.68 hours in the EMB-120 of which 2,186.94
hours was pilot in command. His last proficiency check was on March 3, 1995,
and his most recent training, on August 7, 1995, was Line Oriented Flight
Training (LOFT).
The first officer,
9
age 28, held a commercial pilot certificate with
ratings for airplane, single-engine land, airplane multiengine land, and instrument-
airplane. He held a flight instructor certificate with ratings for airplane,
multiengine, and instrument. His most recent FAA first-class medical certificate
was issued on June 15, 1995, without limitations.
The first officer was employed by ASA in April 1995. Company
records indicate that at the time of the accident, he had accumulated 1,193 total
hours of flying experience, with 363 hours in the EMB-120. He received his ASA
first officer training in April 1995, and completed his initial operating experience
on May 4, 1995.
9
Because of his severe injuries that included burns and inhalation damage, Safety Board
investigators were unable to interview the first officer.

7
The flight attendant, age 37, was employed by ASA on February 8,
1993. She completed her initial training, which included emergency procedures
training, on February 23, 1993. She had no prior experience as a flight attendant.
Her most recent recurrent training on the EMB-120 was on January 26, 1995.
Activities of the crew in the days before the accident were routine and
unremarkable. They appeared to have received normal rest.
1.6 Airplane Information
1.6.1 General
The airplane, N256AS, was an Embraer EMB-120RT “Brasilia,”
serial number 120122, manufactured and certificated in Brazil. The airplane was
certificated in the United States in accordance with a bilateral airworthiness
agreement between the FAA and the Brazilian certification authorities. The
airplane was delivered to ASA on March 3, 1989.
Prior to the day of the accident, the airplane had accumulated
17,151.3 flight hours and 18,171 flight cycles. Maintenance records indicate that
maintenance inspections were accomplished in accordance with ASA’s Standard
Practice No. 624, Airplane Maintenance Program, an FAA-approved maintenance
plan.
The airplane had been assigned to ASA’s Dallas-Fort Worth, Texas,
hub until 1 week prior to the accident when it was transferred to ASA’s Atlanta
hub in preparation for a “C” check (required at 3,300-hour intervals). The
inspection was scheduled to take place the coming week at the ASA maintenance
facility at MCN but the accident intervened. Safety Board investigators reviewed
the airplane records at MCN and found no remarkable discrepancies or minimum
equipment list (MEL) items carried forward in the records.
As part of the ASA maintenance program, a line check
10
is required at
75-hour intervals. A line check was accomplished by employees of ASA’s MCN
maintenance facility on the night of August 20, 1995, during an overnight stop.
According to ASA maintenance work cards, the line check included a specific
10
An ASA line check for the EMB-120 airplane consists of detailed visual inspections in
14 areas to detect leaks, damage, and ensure the continuing airworthiness of all systems.

8
visual inspection of the left and right propellers for any evidence of oil leaks or
damage; and none were noted. Maintenance records indicate that a maintenance
daily inspection
11
was performed at MCN on August 21, 1995, the date of the
accident, by ASA line mechanics prior to the first flight of the day. Maintenance
personnel indicated that a flightcrew walk around inspection was also
accomplished by the first officer prior to departing MCN. Neither of these
inspections noted anything remarkable.
1.6.2 Weight and Balance
ASA dispatch records indicate that the takeoff weight of N256AS at
ATL was 24,237 pounds. The maximum takeoff weight, as stated in the airplane
flight manual (AFM), is 25,353 pounds. The planned landing weight was 22,637
pounds; the AFM maximum landing weight is 24,802. The takeoff percent mean
aerodynamic chord (MAC) was 28.65; the AFM forward and aft center of gravity
limits are 21.0 and 42.0 percent MAC respectively. The airplane was within its
prescribed weight and center of gravity limitations at takeoff and at the time of the
accident.
1.6.3 Propeller Design
Hamilton Standard manufactures a family of composite propeller
blades, including the 14RF (the accident propeller blade), 14SF, and 6/5500/F,
that are intended for use on turbopropeller commuter airplanes. The solid, forged
7075-T73 aluminum alloy spar is the main load-carrying member. The airfoil
shape of the blade is formed by glass fiber-filled epoxy and foam adhesively
bonded to the spar (see Figure 2). A conical hole (taper bore) is bored in the
center of the spar from the inboard end to blade station 21,
12
for weight reduction
and balance weight installation. The taper bore on the 14RF blade can be one of
two different shaped designs: straight taper bore known as the “M” style
13
) and a
11
An ASA maintenance daily inspection is performed prior to the first flight of the day. It
consists of external and internal visual inspections, checks of system operating pressures and
fluid levels, and an operational check of radio and navigational equipment.
12
Blade stations on the 14RF model propeller are measured in inches from a reference
point 3.427 inches inboard of the blade pin platform on the inboard end of the blade.
13
Produced from February 1986 to February 1987 through serial number 85344.

9
63.00 STA
60.00 STA
LEADING EDGE
NICKEL SHEATH
+1
48.00 STA
36.00 STA
EROSION STRIP
DE-ICE HEATER
d
24.00 STA —
16.60 STA —
J
12.00 STA
;
00.00 STA
HAMILTON STANDARD
14RF-9
PROPELLER BLADE
UNTWISTED PLANFORM
WITH SECTION THRU
SHANK & TAPERBORE
OF THE ALUMINUM SPAR
ALUMINUM SPAR
SEPARATION
TAPER BORE
Figure 2.--Illustration of a
14RF-9
propeller blade.

10
bellmouth shape (known as the “N” style). Also, during very early production, the
taper bore was shotpeened.
14
However, early in the production run, Hamilton
Standard reviewed the production process, deemed shotpeening unnecessary, and,
with FAA approval, it was discontinued. The accident blade was originally an N
style blade, but it was rebalanced on customer request for ASA fleet
standardization to the M style and reidentified as an M blade. The accident blade
taper bore was not shotpeened during production.
The taper bore provides space for a measured amount of lead wool to
be inserted for blade balancing. Until April 1994, a cork was used to retain the
lead wool in the taper bore; however, it was later eliminated
15
because it was found
to be a source of chlorine (and potential corrosion) in the taper bore, as well as
unnecessary to retain the lead wool. The model 14RF, 14SF and 6/5500/F
propellers, which vary in length from 10.5 to 13 feet, operate at a maximum of
1,200 to 1,384 rpm. As of July 1996, the 14RF, 14SF and 6/5500/F propeller
assemblies were installed on 9 types of commuter aircraft, operated by 143
operators, on approximately 1,300 aircraft, for an industry total of about 15,000
blades worldwide.
According to information provided to the Safety Board in February,
1995, Hamilton Standard statistical data from field service experience indicate that
blades without shotpeened taper bores are susceptible to earlier corrosion and
cracking.
1.6.4 Airplane and Propeller Design Requirements on Released Blades
When the EMB-120 was certificated in the United States, the effect
on safe flight of a failed or released propeller blade was addressed in FAR
25.571(e)(2), “Damage tolerance (discrete source) evaluation,” which, at that time,
required that the airplane be capable of successfully completing a flight during
which likely structural damage occurs as a result of a propeller blade impact.
14
Shotpeening is a metallurgical surface treatment to improve resistance to cracking. The
surface to be treated is bombarded with air-propelled glass beads or steel shot. Only the first 431
production blades were shotpeened.
15
Use of cork was discontinued in the manufacturing process between April 1994 and
November 1995. Existing corks have been removed from all model 14RF blades, and will be
removed from other models pursuant to PS960A and later AD 95-05-03, which sets forth end
dates for each propeller model.
11
Embraer petitioned the FAA on January 11, 1983, to permit type certification of
the EMB-120 without compliance with that requirement. On March 22, 1983, the
FAA exempted the EMB-120 from compliance with FAR 25.571(e)(2) through
Grant of Exemption No. 3722, which also contained the statement that, “all
practical precautions must be taken in the design of the airplane taking into
account the design features of the propeller and its control system to reduce the
hazard which might arise from failure of a propeller hub or blade.”
In 1990, the (e)(2) requirement was eliminated from FAR 25.571.
The FAA noted at that time (in the preamble to this and other regulatory changes),
that service experience had shown compliance to be “impossible,” and that “[a]s a
result of the granting of exemptions for good cause, no manufacturer has, in fact,
been required to show compliance with the current requirement.” At the same
time, however, the FAA promulgated FAR 25.905(d), which requires that “design
precautions must be taken to minimize hazards to the airplane from a failed or
released blade, including damage to structure and vital systems due to impact of a
failed or released blade, and from the unbalance created by such failure.” (55 Fed.
Reg. 29756 at 29772, 29766, July 20, 1990.)
According to Embraer records, after initial certification of the
airplane, Embraer evaluated the effects on the wing, the nacelle, and the
empennage from a blade tip loss, a mid-blade loss, and a full blade loss.
16
Embraer’s analysis indicated that the nacelle would not withstand the loss of a
mid-blade or full blade segment.
After the accident, the FAA indicated that records from the original
certification of the 14RF propeller indicate that Hamilton Standard demonstrated
compliance, through testing, with the requirement of FAR 35.15 that the propeller,
“not have design features that experience has shown to be hazardous or
unreliable.” The FAA further stated that Hamilton Standard designed, tested and
demonstrated the 14RF-9 propeller blade to meet the FAR 35 requirements and it
was approved as having an unlimited life when maintained in accordance with
FAA-accepted Hamilton Standard maintenance instructions.
16
Embraer Report No. 120-DE-180, “Effect Analysis on Propeller Failures,” dated
September 3, 1984.

12
1.6.5 Airworthiness Standards for Engines and Propellers
To comply with the airworthiness requirements, the propeller
manufacturer must also consider during design and must subsequently
demonstrate the vibration characteristics of the propeller assembly to ensure that
resonant frequencies
17
that can produce critical vibration stresses do not occur
within the normal operating range of use. The applicable regulations are 14 CFR
23.907,
18
25.907,
19
35.37,
20
and 35.39.
21
Advisory Circular
22
(AC) 20-66 provided
17
The resonant frequency of any vibration is the naturally occurring frequency at which
the blade will vibrate when excited. To avoid excessive vibration and overstressing of the
propeller, propeller design practice requires that the propeller spend only a minimal amount of
time in an rpm range that corresponds to a resonant frequency.
18
Each propeller with metal blades or highly stressed metal components must be shown to
have vibration stresses, in normal operating conditions, that do not exceed values that have been
shown by the propeller manufacturer to be safe for continuous operation. This must be shown
by: Measurement of stresses through direct testing of the propeller; comparison with similar
installations for which these measurements have been made; or any other acceptable test method
or service experience that proves the safety of the installation. Proof of safe vibration
characteristics for any type of propeller, except for conventional, fixed pitch, wood propellers,
must be shown where necessary.
19
The magnitude of the propeller blade vibration stresses under any normal condition of
operation must be determined by actual measurement or by comparison with similar installations
from which these measurements have been made. The determined vibration stresses may not
exceed values that have been shown to be safe for continuous operation.
20
A fatigue evaluation must be made, and the fatigue limits must be determined for each
metallic hub and blade and each primary load-carrying metal component of nonmetallic blades.
The fatigue evaluation must include consideration of all reasonably foreseeable vibration load
patterns. The fatigue limits must account for the permissible service deterioration, such as nicks,
grooves, galling, bearing wear, and variations in material properties.
21
For variable-pitch propellers. Compliance with this paragraph must be shown for a
propeller of the greatest diameter for which certification is requested. Each variable-pitch
propeller (the pitch setting can be changed by the flightcrew or by automatic means while the
propeller is rotating) must be subjected to one of the following tests: A 100-hour test on a
representative engine with the same or higher power and rotational speed and the same or more
severe vibration characteristics as the engine with which the propeller is to be used. Each test
must be made at the maximum continuous rotational speed and power rating of the propeller. If
a takeoff rating greater than the maximum continuous rating is to be established, an additional
10-hour block test must be made at the maximum power and rotational speed for the takeoff
rating. Operation of the propeller throughout the engine endurance tests is prescribed in Part 33
of this subchapter.

13
the propeller manufacturer an acceptable means of compliance with the CFRs
relating to airplane propeller vibration.
In Chapter Two, Vibration Measurement Program, it is recommended
that for multiengine installations:
Propeller diameters to be used are tested in at least two percent or
two-inch intervals throughout the diameter range to be approved
and should include the maximum diameter and the minimum
diameter, including cutoff repair limit.
AC 20-66 also states:
For installations where the propeller diameter is greater than 13
feet or the engine nacelles are toed in or toed out, propeller
vibration testing include complete flight and ground crosswind
tests. Flight tests includes the effects of yaw, maximum and
minimum aircraft gross weight at maximum and minimum
airspeeds, flap settings during takeoff and landings, propeller
reversing, and any other condition that would create an
aerodynamic excitation of the propellers. On the ground, the
aircraft is headed at different angles to the prevailing wind to
determine the effects of crosswind excitation. Wind velocities
typical of conditions to be encountered in service are included.
1.7 Meteorological Information
The West Georgia Regional Airport (CTJ) at Carrollton, Georgia, is
about 4 miles northeast of the crash site. The airport authority owns and operates
an Automated Weather Observing System-3 (AWOS-3). The CTJ AWOS-3, and
similar independent systems at other airports that do not serve air carriers, are not
connected through long-line transmission to the National Weather Service (NWS)
or the FAA weather communication networks. The observations are available to
airport users on a dedicated radio frequency. The CTJ AWOS-3 observation just
after the accident was reported as follows:
22
An AC is an FAA document that sets forth an acceptable means to comply with
provisions of Federal Aviation Regulations (FAR). An AC is intended for guidance purposes
only and is not mandatory or regulatory in nature.

14
Type--AWOS-3; time--1301; clouds--800 feet overcast; visibility--
10 miles; temperature--76 degrees F; dew point--75 degrees F;
wind--150 degrees at 6 knots; altimeter--30.08 inches Hg;
Anniston Airport (ANB), Alabama is about 32 miles west of the crash
site. The reported ANB aviation weather observation just before the accident was
as follows:
Type--Record; time--1252; clouds--estimated ceiling 1,500 feet
broken; visibility--5 miles; weather--haze; temperature 87 degrees
F; dew point--73 degrees F; wind--050 degrees at 5 knots;
altimeter--30.02 inches Hg.
The departure airport, ATL, is about 40 miles east of the crash site.
The reported ATL aviation weather observation just before the accident was as
follows:
Type--Record special; time--1246; clouds--200 feet scattered
measured ceiling 1,600 feet broken 3,400 feet overcast; visibility--
2 miles; weather--light rain fog, temperature 73 degrees F; dew
point--73 degrees F; wind--140 degrees at 3 knots; altimeter--
30.08 inches Hg; remarks--surface visibility 5 miles.
The CVR transcript at 1250:15 (2 minutes and 30 seconds before
impact) contained a captain’s statement that, “we can get in on a visual.” The
FDR altitude at that time was about 3,760 feet. The CVR transcript at 1251:05 (1
minute and 40 seconds before impact) contained a captain’s statement, “we can get
in on a visual, just give us vectors.” The FDR altitude at that time was about
2,450 feet. The ATC and CVR transcripts indicate that the first officer reported at
1251:33 (1 minute and 12 seconds before impact) “out of nineteen hundred (feet)
at this time” and the captain added “we’re below the clouds, tell ‘m.” The first
officer then transmitted, “’K we’re uh, VFR at this time, give us a vector to the
airport.”
A helicopter pilot, who arrived at the accident site about 1400,
estimated scattered clouds at about 1,500 feet and a broken ceiling at around 2,500
feet. He estimated the visibility at 3.5 miles in haze.

15
1.8 Aids to Navigation
There were no reported or known difficulties with the navigational
aids.
1.9 Communications
There were no reported or known communications equipment
difficulties.
At the time of the propeller blade separation, ASE 529 was
communicating with an Atlanta Center air traffic controller. Although the base of
the Atlanta Center controller’s airspace is 11,000 feet, the center controller
continued to direct the airplane for about 7 minutes after the blade separation. At
that point (1250:45), with the airplane at about 4,500 feet in altitude, changeover
to Atlanta approach took place. Recorded radar information at that time indicated
that the airplane was about 7 miles from CTJ. The Atlanta approach controller
issued a vector toward the CTJ ILS localizer at 1250:49. Later the controller
provided the localizer frequency; however, neither the AWOS frequency nor the
CTJ weather conditions were provided.
Atlanta approach is responsible for flights inbound or outbound from
ATL and all airports within an approximate 40-mile radius, which includes CTJ.
However, the ATL approach control facility’s access to the CTJ AWOS weather
information is limited to commercial telephone sources. The Georgia Department
of Transportation, which (as the operator of the airport) would be responsible for
the costs of disseminating AWOS information via private communications
networks directly to ATC, determined that the amount of air traffic at CTJ did not
justify the cost of acquiring this service. This is because flightcrews destined for
the smaller airports receive their AWOS weather information on the airport
discrete AWOS frequency.
The closest weather report immediately available to the approach
controller was the ATL Airport observation, the flight’s departure point. No
controller was assigned to the “assist” position. Although the manager and
supervisor were nearby, they became occupied with coordinating and monitoring
activities supporting the flight and did not attempt to retrieve the CTJ AWOS
weather information by telephone. During the 90 seconds that the approach
controller was in radio communication with the flight, the controller issued a

16
vector toward the runway, stated the localizer frequency, confirmed the flight was
in visual conditions, and issued a vector for the visual approach.
FAA ATC procedures
23
state, in part, “If you are in communication
with an aircraft in distress, handle the emergency and coordinate and direct the
activities of assisting facilities. Transfer this responsibility to another facility only
when you feel better handling of the emergency will result.”
Following their declaration of an emergency with Atlanta Center, at
1246:13 the flightcrew indicated their need to land as soon as possible and
requested, “roll the trucks and everything for us.” The controller then advised the
flightcrew that CTJ was the closest airport and directed the aircraft to CTJ.
However, the request for emergency vehicles was not passed to the fire department
serving CTJ, (the Carroll County Fire Department) or to the Atlanta approach
controller. Following the accident, Atlanta approach did call the Carroll County
Sheriff’s Office and was informed that a private citizen had already reported the
airplane crash near CTJ.
1.10 Airport Information
CTJ has one asphalt surface runway, 5,001 feet by 100 feet, oriented
340/160 degrees, and the field elevation is 1,160 feet. There are two instrument
approaches, an instrument landing system (ILS) localizer only (LOC) RWY 34
and a nondirectional beacon (NDB) RWY 34. Atlanta approach control is the
feeder ATC agency on sector frequency 121.0 megahertz (MHz). Weather at the
airport is available directly through an AWOS-3 reporting system on 118.175
MHz. The airplane crashed about 4 miles from the airport.
1.11 Flight Recorders
The airplane was equipped with an operating cockpit voice recorder
(CVR) and flight data recorder (FDR). They were recovered from their installed
positions in the aft portion of the airframe and appeared in good condition with
only minor sooting on the cases. The CVR was a Fairchild Model A100A, S/N
57597. The recording was good and showed no evidence of loss of quality as a
result of the crash.
23
FAA Order 7110.65, Chapter 10, “Emergencies,” Section 1, “General,” paragraph 10-1-
4, “Responsibility,” applies.

17
The FDR was a Fairchild Digital Model F-800, S/N 04856, with 28
parameters of data. The recording was of good quality; however, the parameter
for rudder pedal position indicated only small changes that did not approach
normal travel. Postaccident investigation of the airframe wreckage revealed that
the rudder pedal potentiometer coupler was not securely connected to the shaft of
the rudder pedal potentiometer.
ASA maintenance records indicate that the rudder pedal
potentiometer was installed on the accident airplane in November 1990. The most
recent calibration check was performed in June 1994. At that time, no
discrepancies were noted during a 3-point calibration check (neutral, full left, and
full right). On June 27, 1996, the Safety Board issued two safety
recommendations to address this issue (see Section 1.18.1).
1.12 Wreckage and Impact Information
The main wreckage area consisted of the cockpit, fuselage, right wing
and engine, and the empennage. Portions of two of the right engine’s propeller
blades remained attached to the propeller hub and engine. The remaining two
blades of the right engine propeller assembly were located nearby. An area of the
grass leading up to and surrounding the main wreckage was burned out to a radius
of about 30 feet.
The airplane came to rest at the northwest end of an 850 foot
wreckage trail that was aligned on a heading of about 330 degrees magnetic.
Numerous trees were sheared off prior to ground contact, consistent with a descent
angle of about 20 degrees, and an increasing left-wing-down attitude of 15 to 40
degrees. Impact with the trees extended for about 360 feet, and, following the last
tree impact, a debris path continued for 490 feet through an open field on slightly
upsloping terrain to the main wreckage.
Prominent ground scars were observed at the beginning of the debris
field (about 40 feet from the last tree impact) that were consistent with the
dimensional measurement of the left wing to the fuselage. The first scars
contained several pieces of the left wing. Ground scars were consistent with
separation of the left wing at its root. Debris from the airplane was scattered along
the wreckage path in the field. The left engine’s propeller and reduction gear box
(RGB) assembly were located approximately 160 feet past the tree line. The

18
propeller hub and blade assembly contained three complete propeller blades with
the inboard piece of a fourth blade protruding about 1 foot from the hub.
The Safety Board’s Airplane Performance Group used its
WINDFALL computer program to calculate the trajectory of the missing blade
piece. The group devised a search area and alerted the local residents and
authorities about the missing piece. Three weeks after the accident, the outboard
piece of the blade was discovered by a farmer. It had been well hidden in some
tall grass within about 100 yards of the primary search area.
The fractured blade sections were sent to the Safety Board’s Materials
Laboratory for detailed examination (see Section 1.16.1 for details).
1.12.1 Fuselage
The aft portion of the fuselage had separated from the forward portion
in two places, near the trailing edge of the wing and also just behind the cockpit.
The forward fuselage section (including the cockpit) was upright. The aft portion
of the fuselage was resting on the right side and was supported by the right
horizontal stabilizer. The vertical stabilizer was intact and essentially undamaged.
Most of the passenger cabin that was not resting on the ground was destroyed by
fire.
The right side of the forward fuselage from the radome rearward to
the cockpit had very little damage. The left side of the forward fuselage below the
cockpit window from the radome to just forward of the passenger/crew entry door
was crushed in, aft, and up to the left side of the nose landing gear wheel well.
Inward deformation was less severe near the aft portion of the crushed area. The
external fuselage skin forward of the passenger/crew entry door was undamaged
by fire except for an area of sooting aft and above the captain’s side window.
Fire had destroyed the left side of the fuselage aft of the
passenger/crew entry door. The fire damage extended to just forward of the cargo
door and the entire right side of the fuselage from the leading edge of the wing to
two seat rows forward of the cargo section. The upper portion of the right
fuselage forward of the leading edge of the wing to the cockpit had also been
destroyed by fire.

19
1.12.2 Wings
The major portion of the left wing, with the nacelle and engine
partially attached, came to rest along the wreckage path about 125 feet in front of
the cockpit. The inboard portion of the left wing leading edge, from the fuselage
to the left engine nacelle, was intact. The leading edge outboard of the left engine
nacelle was recovered from the debris field but was broken into several pieces.
There were no cuts or gouges in the leading edge. The inboard and nacelle flaps
and the inboard flap track for the outboard flap were attached. Damage to the flap
tracks was consistent with the flaps being in the retracted position.
The entire right wing remained intact and attached to the fuselage.
The inboard section of wing between the engine and the fuselage was destroyed by
fire. There was no fire damage to the wing outboard of the engine. All flap
segments appeared to be in the retracted position.
1.12.3 No. 1 (Left) Engine Nacelle
The outboard member of the front frame of the No. 1 left engine
nacelle was deformed aft approximately 90 degrees and was twisted outboard
slightly. There was also a semicircular flattened area in the middle of the outboard
member of the front frame. The axis of the flattened area was oriented upward
approximately 20 degrees from the horizontal. The forward inboard engine mount
bolt had sheared in an upward and slightly outboard direction. The corresponding
metal surface area of the attachment fitting was smeared in the same direction.
The engine air inlet fairing and the forward portion of the forward
cowling remained attached to the propeller/RGB assembly, but they were
deformed outboard. Both steel tubes connected to the forward and aft engine
mounts were found separated from the terminal ends. The inboard tube was bent
slightly; the outboard tube was not bent.
Five of the six hinges that secure the inboard and outboard forward
cowling doors were attached, but they were bent in a direction consistent with up
and aft movement of the cowling doors. The area underneath several of the hinges
was damaged consistent with overtravel of the hinges. The forward, inboard hinge
had separated, and the area of the inboard door where the hinge was attached was
torn. The forward edge of both forward cowling doors was bent upward.

20
The forward inboard engine/RGB mount bolt, and forward, outboard
engine/RGB mount, upper and lower rod ends of the inboard and outboard torque
mount assemblies were removed and submitted to the Safety Board’s Materials
Laboratory for examination of all fracture surfaces. That examination revealed no
indications of fatigue or other preexisting defects. The inboard engine/RGB
mount and the outboard engine mount bolt were intact and remained attached to
the engine and the nacelle structure, respectively. No deformation was noted on
the inboard engine mount. The forward, outboard engine/RGB mount was
deformed aft near the fracture location. No definitive failure directions were
obtained from the upper rod ends, which had fractured near the first screw thread.
Examination of the fracture surfaces of the lower rod ends revealed characteristics
consistent with the fracture propagating inboard to outboard.
1.12.4 No. 2 (Right) Engine Nacelle
The No. 2 engine and RGB remained mounted to the wing. Although
a fire consumed the adjacent inboard wing-to-fuselage area, damage to the No. 2
engine nacelle was not remarkable. All cowlings and fairings were found in place
with little evidence of fire or soot.
1.13 Medical and Pathological Information
The Carroll County Medical Examiner determined that the seven
fatally injured passengers succumbed to thermal burns and smoke inhalation. The
cause of death for the captain was also reported to be thermal burns and smoke
inhalation. However, in his report, the Medical Examiner indicated that blunt
force trauma injuries to the face and head were “other significant conditions.”
This is consistent with impact-related damage on the forward left side of the
fuselage. The first officer survived with burns over 80 percent of his body.
Physicians indicated that as a result of his injuries, he would require extensive
therapy.
Urine samples obtained post-mortem from the captain, and blood and
urine samples obtained from the first officer after the accident, tested negative for
alcohol and other drugs of abuse.

21
1.14 Fire
Based on ASA flight dispatch records, investigators estimated that
about 350 gallons of fuel were on board at the time of the accident. Per normal
operating practice, the fuel would have been equally distributed between the left
and right side tanks. The two tanks in the left wing separated early during the
impact sequence, and there was evidence of fuel spilled on vegetation along the
wreckage path. The inboard tank in the right wing was found burned at the
accident site, but the outboard tank was intact. Passengers did not observe fire
until after the airplane came to a complete stop. They said that there was a period
of about 1 minute before the outbreak of fire. The passengers described black
smoke and flame consistent with what would be expected of a fuel-fed fire.
Passengers reported that the fire was immediately preceded by cracking sounds
and sparks from wires and cables and that the fire started in small patches and
spread quickly, fully engulfing the area aft of the cockpit entrance door.
Some passengers related that they found portions of their clothing
saturated with fuel, and one passenger saw “a couple of people on fire.” The flight
attendant and several passengers said that they had to run through flames to escape
from the cabin wreckage.
The flight attendant received second degree burns to her ankles and
legs. She was wearing a skirt, white blouse, hosiery, and an airline uniform vest.
1.15 Survival Aspects
The CVR revealed that the flightcrew advised the flight attendant of
the planned emergency return to ATL about 7 minutes prior to impact. There were
no further communications from the flightcrew to the flight attendant. The flight
attendant stated that while preparing the passengers for the emergency landing,
she saw tree tops, immediately returned to her seat, and shouted commands to
brace for landing.
According to passengers, immediately following the loss of the
propeller blade, the flight attendant checked with each passenger to make sure that
they understood how to assume the brace position, and she yelled instructions to
the passengers until the time of impact. Despite being seriously injured, she
continued to assist passengers after the accident by moving them away from the
airplane. She also extinguished flames on at least one passenger who was on fire.

22
The postcrash fire destroyed the passenger cabin. According to the
surviving passengers, the cabin breakup started at the initial ground impact.
Passengers stated that overhead storage bins in the cabin dislodged during the
initial ground impact and that passenger seat structures separated and/or became
deformed. According to one passenger, as the fuselage slid on its left side, several
large holes were created that allowed enough daylight to appear in the cabin that
provided the flight attendant and passengers visual escape cues. None of the
survivors reported escaping from the cabin through the main entrance door, the
overwing emergency exits, or the cabin emergency exit. They escaped through the
holes in the fuselage, which were immediately behind the cockpit and aft of the
wing. Passengers who were unable to escape from the wreckage succumbed to
smoke inhalation.
Shortly after the airplane came to rest, the first officer attempted
unsuccessfully to open the right side cockpit window, which was damaged during
the impact. Thereafter, he reached behind his crew seat and retrieved a small ax
with a wooden handle. He subsequently attempted to chop a hole in the side
window but was only successful in chopping a hole approximately 4 inches in
diameter in the center of the window through which he handed the small ax to a
passenger. The passenger attempted unsuccessfully to use the ax to extricate him
from the cockpit.
When a Carroll County Sheriff’s deputy arrived at the scene within
about 5 minutes, he saw a passenger striking the first officer’s side window with
the small ax,
24
which was aboard the airplane as FAA-required emergency
equipment. The wooden handle separated from the ax head early in the rescue
effort. About 2 minutes after the ax handle broke, the local fire department arrived
and tried, unsuccessfully to break the window using full size axes. The fire
department applied water to the cockpit side window. The deputy reported that
during the time of the rescue, a continuous roaring sound emanated from an area
behind the cockpit in which there was intense fire. In the following several
minutes, the fire aft of the cockpit was controlled sufficiently to allow firefighters
to enter the cabin and break through the cockpit door to rescue the first officer.
The Sheriff’s deputy did not observe any signs of life from the captain during the
rescue sequence.
24
The ax had a short wooden handle about 14 inches long and resembled a hatchet. It had
a single blade with a nail puller notch, and the opposite end of the blade had a shape that was
similar to a hammerhead.
23
Postaccident inspection of the cockpit area indicated that movement
of the right and left cockpit sliding windows was restricted by airframe damage
consistent with impact and deformation of the windows’ slide tracks. The first
officer’s cockpit sliding window was found to have jammed in its track in the
closed position. Investigators were able to open the sliding windows with the aid
of pry bars (tools not normally available to flightcrews ).
The flightcrew oxygen walkaround cylinder and smoke masks were
found stored, respectively, on the left and right sides of the cockpit. They did not
appear to have been used. Protective breathing equipment (PBE) required in 14
CFR Part 121 airplanes was not carried (nor was it required to be) because the
airplane was operated under 14 CFR Part 135.
1.16 Tests and Research
1.16.1 Laboratory Examination of the Fractured Propeller Blade
The inboard piece of the fractured blade, serial number 861398, was
retained in the left engine propeller hub, which was recovered at the accident
scene on August 21, 1995. The outboard piece of the blade was recovered on
September 15, 1995, after it was discovered by a farmer on property about 35
miles west of the accident site adjacent to an area that had previously been
searched by helicopter. Both portions of the blade were examined at the Safety
Board’s Materials Laboratory. The blade spar
25
was separated at blade station 16.6
(about 13.2 inches outboard of the blade pin platform). Initial visual examination
revealed that a portion of the spar fracture was on a flat transverse plane and
contained crack arrest positions, typical of fatigue cracking (see Figure 3). The
fatigue cracking appeared to initiate from at least two adjacent locations on the
taper bore surface. Below the taper bore surface, the individual cracks joined to
form a single crack that propagated toward the face side
26
of the blade and
progressed circumferentially around both sides of the taper bore. The extent of the
fatigue cracking progressed through about 75 percent of the spar cross section.
The fracture surface in areas beyond the terminus of the fatigue region contained
rough features with a matte appearance, typical of an overstress separation area.
25
The main load-carrying member of the blade.
26
The face side of the blade is aerodynamically similar to the bottom side of a wing.

24
Figure 3.--Photo of the blade fracture surface.

25
The origin areas on both the inboard and outboard faces of the
fracture were examined with a scanning electron microscope (SEM) before the
faces of the fracture were cleaned. The fracture surface near the origin area on
both faces of the fracture contained a layer of heavy oxide deposits that had a
mud-cracked appearance. These deposits extended to a maximum depth of 0.049
inch from the taper bore surface. Their maximum circumferential width was 0.130
inch, based on the examination of the damaged outboard fracture face. X-ray
energy dispersive spectroscopy (EDS) of the deposits of both faces generated
similar spectra with a major peak for aluminum, a substantial peak for oxygen, and
a minor peak for zinc.
27
EDS of the deposit area on the inboard fracture face also
revealed the presence of chlorine.
After the fracture surface had been cleaned, additional SEM
examination revealed that the fatigue cracking initiated from several corrosion pits
in a line of pits in the taper bore that extended over a distance of about 0.070 inch.
The maximum depth of the corrosion pitting at the fatigue origin area was
measured as slightly less than 0.006 inch below the taper bore surface.
The taper bore surface, including the area adjacent to the fatigue
initiation area, contained a series of nearly circumferential sanding marks. The
marks extended over about 180 degrees of the circumference of the taper bore and
to a maximum distance of about 1.5 inches inboard of the fracture surface.
Outboard of the fracture, the sanding marks extended about 2 inches from the
fracture surface.
The investigation revealed that sanding rework of the area had been
accomplished using the blending repair procedures contained in PS960A.
28
The
procedures required that the surface finish of the blended area should be restored
to the original surface finish. Postaccident surface profilometer measurements
conducted on the taper bore sanding marks indicated that the surface finish was
much rougher than the manufactured surface not disturbed by the rework
process.
29
Measurements also indicated that the nondisturbed surface met the
manufacturing specifications.
27
Zinc is an alloying element in the 7075 aluminum alloy specified for the blade spar.
28
PS960A is described in paragraph 1.16.3.
29
The surface roughness in the blended area was measured as Ra 125, whereas the surface
finish requirement of PS960A is 63 RMS, which converts to approximately Ra 50. (“Ra”
denotes arithmetically averaged roughness.)

26
The taper bore was measured to determine the minimum thickness of
the spar between the taper bore hole and the spar’s face side and was found to be
within the requirements of the manufacturing specifications. Measurements also
indicated that about 0.002 inch of material appeared to have been removed from
the taper bore surface during the sanding process.
Specimens of material cut from the fractured blade were tested for
tensile strength, hardness, conductivity, and composition. All the tests indicated
values that were consistent with the specified composition for 7075-T73 aluminum
alloy.
1.16.2 Previous Failures of Similar Model Propellers
Prior to this accident, there were two failures of Hamilton Standard
composite-type propeller blades that were found to have resulted from cracks that
originated from inside the taper bore. The first event took place on March 13,
1994, on an Inter-Canadien
30
Aerospatiale-Aeritalia ATR 42 equipped with a
model 14SF propeller blade. The second event occurred on March 30, 1994, on a
Nordeste
31
Embraer EMB 120 equipped with a model 14RF blade. (Appendix C
contains details of the fractures).
The Transportation Safety Board of Canada (TSB) conducted an
investigation
32
of the Inter-Canadien event. TSP analysis indicated that forces
induced from the rotation of the three remaining blades resulted in propeller
imbalance and loads on the forward engine mounts that exceeded the ultimate
limits. This resulted in separation of the propeller and the RGB assembly from the
airplane. The RGB with the propeller hub, three complete blades, and the retained
portion of the fourth blade fell onto an ice-covered lake and was recovered during
the investigation. Indications were that the separated blade passed through the
fuselage and caused depressurization of the cabin. There were no injuries, and the
flightcrew accomplished a safe landing.
30
Inter-Canadien is a regional air carrier based in Montreal, Canada.
31
Nordeste Linhas Aereas Regionals S.A. is a regional air carrier based in Salvador,
Bahia, Brazil.
32
The TSB released the results of its investigation as Aviation Occurrence Report No.
A94Q0037 on February 28, 1995.

27
The Aircraft Accident Prevention and Investigation Center of Brazil
(CENIPA) investigated the Nordeste occurrence. CENIPA did not publish a
formal report; however, it provided documentation contained in a technical report
by Embraer that affirmed causal findings similar to the Inter-Canadien blade
separation. Embraer’s report indicated that during the Nordeste event, the
imbalance forces from the rotation of the three remaining blades resulted in
damage to the RGB. The remaining three blades and fourth blade stub were found
moved toward the feathered position (resulting in minimum aerodynamic drag);
and the propeller and RGB assembly remained within the nacelle area and were
partially attached to the airframe. There were no injuries, and this flightcrew also
accomplished a safe landing.
Laboratory examination of the failed blades indicated the presence of
chlorine-based corrosion pits in both instances. The chlorine source was traced to
a bleached cork installed in the taper bore to retain the lead balance wool. These
findings were corroborated by Hamilton Standard engineers and the FAA.
In addition to the Inter-Canadien and Nordeste propeller blade
fractures that were related to taper bore corrosion, on August 3, 1995, about 3
weeks prior to the ASA accident, there was an in-flight loss of a Hamilton
Standard Model 14RF-9 propeller blade that was not related to taper bore
corrosion. The propeller was installed on a Luxair
33
EMB-120 airplane that was in
the final approach to landing when the right propeller and portions of the RGB
separated. Some of the separating components struck the airplane; the flightcrew
accomplished a safe landing, and there were no injuries. The Belgian Civil
Aviation Administration (CAA) conducted an investigation on behalf of the
Ministry of Transport of Luxembourg.
34
The investigation determined that one of
the four propeller blades had failed from a fatigue crack about 9 inches from the
butt end of the blade. It was found that the crack began on the outer surface of the
blade shank in an area of mechanical damage induced by a localized interference
condition between the blade spar and the foam mold, which occurred during the
manufacturing process.
33
Luxair is a regional air carrier based in Luxembourg City, Luxembourg.
34
The Belgian CAA released the “Final Report of Aircraft Accident” on July 5, 1996.

28
1.16.3 Blade Inspection and Repair - Actions Taken by Hamilton
Standard and the FAA
(See Table 1 for a timeline of significant events related to the 14RF-9
propeller.) Following the March 1994 blade failures, Hamilton Standard began an
immediate program to inspect ultrasonically all model 14RF, 14SF, and 6/5500F
propeller blades for evidence of cracks. Blades with rejectable ultrasonic
indications were returned to Hamilton Standard. Early in the process of inspecting
the returned blades, Hamilton Standard discovered that some ultrasonic
indications were caused by visible mechanical damage. Although no cracks were
found, the mechanical damage was in excess of what engineers thought was
acceptable. Hamilton Standard reviewed the shop practices and concluded that the
mechanical damage was a result of tools and techniques used during the
installation and removal of balance wool lead. As a result, Hamilton Standard
developed repair procedures to blend locally visible mechanical damage and
eliminate ultrasonic indications that had no associated cracks. This repair was
described in Hamilton Standard repair procedure PS960 (and was approved by the
FAA on April 8, 1994.) PS960 specified the following steps:
1) Visually inspect the blade taper bore for evidence of mechanical
damage. No unblended mechanical damage is allowed.
2) Locally blend mechanical damage to 50 times the repair depth.
Repair limits are 0.010” maximum stock removal for the face area, 0.020”
maximum stock removal for all other areas, including end of taper bore.
When the blending is complete, no evidence of damage may remain.
Reference Figure 1 (page 3) for definition of face area at any taper bore
location.
3) Inspect repairs using a borescope with a 1:1 magnification to
verify blending to the above requirements. Surface finish of repair area
must be 63 RMS.
4) Perform an ultrasonic inspection of the blade taper bore area.
5) WARNING; CONVERSION COATING IS POISONOUS TO
EYES, SKIN, AND RESPIRATORY TRACT. USE SKIN AND EYE
PROTECTION. MAKE SURE THE TIME YOU USE IT IS THE

29
MINIMUM NECESSARY. MAKE SURE THE AREA HAS A GOOD
FLOW OF AIR.
6) Apply “PS960” to the face and camber side of each blade with
white stenciling ink in accordance with stenciling procedures provided in
the applicable Component Maintenance Manual.
With a brush, touch up all areas repaired per the above procedure
with a coating that agrees with MIL-C-5541, Class 1A. Allow to cure 24
hours.
NOTE: Alodine 600 is recommended because it is without cyanide, but
Alodine 1200 or 1201, or any material which agrees with MIL-C-5541,
Class 1A is satisfactory.
Soon thereafter, it was determined that the cork in the taper bore
contained chlorine residue that could cause corrosion in the taper bore. As a
result, PS960 was amended by PS960A to include procedures to eliminate the
taper bore cork and to replace it with a sealant. PS960A was approved by the
FAA on April 18, 1994.
Concurrent with the development of the PS960A repair procedure,
Hamilton Standard was also developing a series of alert service bulletins (ASB) to
address the problem of cracks originating from inside the taper bore in the model
14RF, 14SF, and 6/5500F blade spars. The bulletins called for a one-time, on-
wing ultrasonic shear wave inspection to be performed by level II
35
Hamilton
Standard employees or contractor inspection teams to detect abnormalities in the
blade taper bore. Blades rejected for ultrasonic indications above specified limits
found during the on-wing inspection were to be removed from service and sent to
Hamilton Standard Customer Support Centers. Upon receipt of the blades,
35
Hamilton Standard inspectors were certified according to the American Society for
Nondestructive Testing (ASNT) or the Hamilton Standard, FAA-approved equivalent.
According to ASNT, an NDT Level II individual is qualified to set up and calibrate equipment,
and to interpret and evaluate results with respect to applicable codes, standards, and
specifications. The NDT Level II is thoroughly familiar with the scope and limitations of certain
NDT methods, and guides and performs on-the-job training of trainees and NDT Level I
personnel. The NDT level III individual is familiar with other NDT methods and is capable of
training and examining NDT Level I and II personnel for certification in those methods.

30
TABLE 1
SIGNIFICANT EVENTS RELATED TO
HAMILTON STANDARD 14RF/SF SERIES PROPELLERS
Previous Accident(s): Blade Separation
Date Company Airplane Type
3/13/94 Inter-Canadien ATR-42
3/30/94 Nordeste EMB-120
Inspection and Repair Action
Date Document Reason Action
4/8/94
4/18/94
Hamilton Standard
PS960, as revised by
PS960A. (FAA
approved procedure.)
Mechanical damage
and chlorine deposits
found in taper bores.
-Visual inspection for
mechanical damage.
-Blend mechanical
damage.
-Remove cork and
replace with sealant.
4/18/94 Hamilton Standard
ASB 14RF-9-61-A66
Inter-Canadien &
Nordeste blade failures
due to fatigue cracking
-One-time on-wing
ultrasonic inspection to
detect abnormalities in
taper bore
- If rejectable
indications are found,
remove from service
and return to Hamilton
Standard
4/27/94 Hamilton Standard
Internal Memorandum
To document decision
to use 960A repair to
eradicate UT
indications caused by
peaks of shotpeen
impressions
-Was interpreted as
expansion of PS960A
blending repair to
include blades without
mechanical damage.
5/2/94 AD 94-09-06 -Required one-time UT
inspection for cracks in
taper bore (within 45
days) in accordance
with ASB 14RF-9-61-
A66.
- If cracks are found,
replace propeller.

31
ASA Accident Blade History
5/19/94 ASA accident blade inspected on-wing per AD and removed from service.
6/7/94 ASA accident blade inspected at Hamilton Standard, no visible faults found,
blend repaired per PS960A.
Inspection and Repair Action (Continued)
Date Document Reason Action
8/29/94 Hamilton Standard ASB
14RF-9-61-A69
(Revised10/5/94)
Continuing
airworthiness
-Repeat ultrasonic insp.
every 1,250 cycles for
specified unpeened
blades, or do improved
visual inspection per
Safety Board 14RF-9-61-
A70, or return to
Hamilton Standard.
- In all cases, return
rejected blades to
Hamilton Standard
-Remove cork (if still
installed).
- ASA blade exempted.
8/29/94 Hamilton Standard SB
14RF-9-61-A70
Continuing
airworthiness
-(For unpeened blades
only) Improved taper
bore visual inspection
with borescope photo
and mold transfer.
- If pits found, remove
from service or return to
repair facility.
9/1/94 Component
Maintenance Manual
(CMM)
No. 61-13-04
Detect corrosion, if
none then repair.
Eliminates PS960A
-Improved taper bore
cleaning & visual
inspection (cracks, pits,
and mechanical damage)
and FPI.
- Shotpeen.
3/ 23/95 AD 95-05-03 -Required SB 14RF-9-
61-A69 Rev 1, and SB
14RF-9-61-70 (by
12/31/97) and provided
terminating action to
repetitive inspection.

32
Accident(s): Blade Separation
Date Company Airplane Type
8/3/95 Luxair EMB-120
8/21/95 ASA EMB-120
Further Inspection and Repair Action
Date Document Reason Action
8/25/95 NTSB
recommendations
ASA Accident Recommended re-
inspection of reworked
blades; vibration and
loads survey; review of
requirements for
shotpeened taper bores.
8/25/95 TAD 95-18-51 ASA Accident and
NTSB
recommendations
Required re-inspection
of reworked blades.
9/30/95 14RF-9-61-86, Rev
4,11/9/95
LUXAIR blade shank
failure due to fatigue
cracking
Shank on-wing
ultrasonic inspection,
for “N” blades
11/9/95 14RF-9-61-A90
ASB
same as above Shank off-wing
ultrasonic inspection,
for “M” blades
11/16/95 AD 95-24-09 -Require SB 14RF-9-
61-A86 Rev 4 or SB
14RF-9-61-A90.
12/15/95 14RF-9-61-A91
ASB
Revised fracture
mechanics info. and risk
assessment of blade and
shank fatigue cracks.
-New off-wing
ultrasonic insp., lead
removed, each 500
cycles.
12/18/95 14RF-9-61-A95
ASB
Rev 1, 12/18/95
same as above -New on-wing
ultrasonic insp., with
balance lead.
1/19/96 AD 96-01-01 -Require ASB 14RF-9-
61-A91 or ASB 14RF-
9-61-A95.

33
Terminating Action
Date Document Reason Action
3/6/96 14RF-9-61-A94
ASB
terminate recurrent
ultrasonic inspections.
-Repair taper bore,
rework to like new.
4/24/96 AD 96-08-02 -Require ASB 14RF-9-61-
A94 taper bore
repair by 8/31/96.

34
Hamilton Standard performed a borescope inspection and initiated the repair
process, if warranted. The FAA mandated the inspection described in the ASBs
by AD 94-09-06, effective on May 2, 1994. The AD required that blades with
ultrasonic indications above 50 percent be removed from service. A rejectable
ultrasonic indication was found on the accident blade, and it was removed from
service on May 19, 1994. The accident blade was one of 490 rejected blades that
were sent to Hamilton Standard for further evaluation and possible repair.
Hamilton Standard customized inspection and repair instructions set
forth in a shop traveler form (Rock Hill Flow Traveler - Form Number RH243)
36
were used to define the taper bore inspection and repair actions for blades rejected
as a result of the field on-wing ultrasonic inspections. The shop traveler form
required that the taper bores of the returned blades be ultrasonically inspected
again to verify the unacceptable rejectable indication. The taper bores of the
blades were then to be cleaned and borescope inspected for evidence of cracks,
corrosion, pits, and other flaws. None of the returned blades were discovered to
be cracked. Corrosion was identified in approximately 13 percent of the blades;
these blades were set aside for further analysis by Hamilton Standard engineering.
Some of these blades were subsequently cut up or were otherwise destructively
tested; others were used to develop further testing and repair processes. None of
the blades with confirmed corrosion were returned to service.
After PS960A and the alert service bulletins were issued, Hamilton
Standard discovered that a small percentage of the returned blades with ultrasonic
indications did not have observable corrosion, mechanical damage, or cracks in
the taper bore. All such blades identified at that time had shotpeened taper bores.
Hamilton Standard determined that the roughness inherent in shotpeened surfaces
could in some cases also generate a rejectable ultrasonic indication. According to
Hamilton Standard engineering managers, as a measure to further reduce the
number of apparently unsubstantiated ultrasonic indications and to return these
blades to service, Hamilton Standard engineering personnel decided that the
procedures set forth in PS960A for blending areas of mechanical damage could
also be used to blend the area surrounding the ultrasonic indication inside the taper
bore of shotpeened blades, even though there was no associated mechanical
damage. This decision to extend the applicability of PS960A was discussed and
36
The shop traveler form that was in use at the time the accident blade was inspected and
approved by the engineering manager at Rock Hill on May 13, 1994 (approximately 1 month
before the accident blade was received there).

35
authorized in conference calls that included engineering managers of the three
Customer Service Centers and Hamilton Standard engineering. It was
implemented without the knowledge or approval of the FAA or the DER.
According to Hamilton Standard management, the authorization to
use PS960A in this manner was confirmed through an internal memorandum,
dated April 27, 1994, from the Manager of Operations Engineering to the three
Customer Service Center engineering managers, stating:
Subject: Blade U. T. [ultrasonic] Inspection
Per direction from [the head of Project Engineering] you should
handle blades returned from the field as a result of U.T. inspection
as follows:
1) Perform a U. T. inspection. Record results on the ASB form
except that this form should have the [applicable location]
written at the top of the form. Forward the form to HSD
Service via FAX.
2) Rework blade per PS960A. Perform a U.T. inspection and
record the results on the modified form as described in para. (1).
3) Ship acceptable blades. Hold rejected blades until further
notice.
In a letter to the Safety Board dated March 5, 1996, Hamilton
Standard indicated that the intent of this memo was to document the decision to
use PS960A “to eradicate false ultrasonic positives being caused only by
superficial irregularities,” specifically, to “remove tool marks or the peaks of shot
peen impressions.”
On August 29, 1994, Hamilton Standard issued an additional series of
ASBs and SBs for unshotpeened blades in the 14RF, 14SF, and 6/5500/F series
with procedures for repeating the on-wing ultrasonic inspection every 1,250 cycles
or, in the alternative, accomplishing a borescope inspection for pits. Rejected
blades were to be returned to Hamilton Standard for inspection (including FPI)

36
and repair according to the new maintenance procedure
37
in the Component
Maintenance Manual
38
(CMM), which superseded the procedures in PS960A. The
1,250 cycle interval was based on the minimum detectable flaw using the
ultrasonic inspection technique and the operating time to failure of the Nordeste
and Inter-Canadien blades.
Shortly after these ASBs were issued, the FAA issued AD 95-05-03,
effective on March 23, 1995, referencing the Hamilton Standard SBs and ASBs
and requiring that blades be ultrasonically inspected at an interval of 1,250 cycles
or, alternatively, that a borescope inspection of the taper bore be performed. The
AD provided appropriate ASB/SB references. If the borescope inspection found
no corrosion pits in the taper bore, the blade could be returned to service. AD 95-
05-03 also contained a provision that a return to service following the results of a
satisfactory borescope inspection constituted terminating action to the requirement
for recurrent ultrasonic inspections every 1,250 cycles.
Following this accident, the Safety Board made several urgent
recommendations resulting in additional ADs. (See Sections 1.18.1) Other
postaccident actions taken by Hamilton Standard and the FAA are discussed in
Section 1.18.2.
1.16.4 The Failed Propeller, Information, and Service History
The fractured propeller blade from N256AS was model 14RF-9, part
number RFC11M1-6A, serial number 861398, manufactured with an
unshotpeened taper bore in 1989 by the Hamilton Standard Division, United
Technologies Corporation, Windsor Locks, Connecticut. The 14RF-9 model blade
is certificated only for the EMB-120 airplane.
37
Repair 4-25 in the CMM required the removal of the bore plug, cork (if installed), and
lead wool, followed by a cleaning, white light borescope and FPI inspections. For unpeened
blades: If a blade had damage less than 0.005 inch, with no previous blending per PS960A, then
the blade was shotpeened, balanced and marked +A. If the blade had damage less than 0.005
inch, but it was previously blended per PS960A, then the blade was shotpeened, balanced and
marked +B. If the damage was greater than 0.005 inch, but less than 0.020 inch (0.010 inch on
the blade face), then the blade was reamed, shotpeened, balanced and also marked +B. If the
damage was greater than 0.020 inch (0.010 on the blade face), then the blade was reamed,
balanced and marked +C. The process was similar for shotpeened blades.
38
The CMM is the FAA-approved maintenance manual that contains instructions for
continued airworthiness of Hamilton Standard propellers.

37
The fractured blade had accumulated a total of 14,728 operating
hours and 5,182 hours since overhaul. The overhaul was accomplished by
Hamilton Standard customer service technicians at East Windsor on April 7, 1993.
At that time, the blade had accumulated 9,546 hours.
39
Records indicated that only
routine maintenance actions were necessary at the time of overhaul.
On April 20, 1993, upon return to ASA from overhaul, the blade was
installed on an airplane (not the accident airplane) where it remained until May 19,
1994. On that day, the blade received an on-wing ultrasonic inspection of the
taper bore by a Hamilton Standard contract inspector in accordance with AD 94-
09-06. The blade was rejected for a 60-percent, full-scale height
40
ultrasonic
indication.
The blade was removed from service and returned to Hamilton
Standard facilities at East Windsor, Connecticut. It was subsequently shipped to
Hamilton Standard’s Customer Support Center at Rock Hill, South Carolina, for
inspection and repair.
According to the shop traveler form for the accident blade, an
ultrasonic inspection of the accident blade on June 7, 1994, confirmed the
rejectable indication, with a reading of 52 percent full-scale height. Following this
ultrasonic inspection, the lead wool was mechanically removed from the taper
bore and the hole was examined with a white-light borescope for evidence of
corrosion, pits, or cracks. In the space provided on the shop traveler form for the
“results” of this inspection, the technician recorded, “No visible fa[u]lts found,
blend rejected area.”
The shop traveler form reflects that he then blend-repaired
41
the taper
bore “damage” with aluminum oxide sanding tools, using the procedures of
PS960A. The technician, who was not an FAA-certificated mechanic, stated that
39
The inspection limit for 14RF-9 propeller blades is 9,500 hours. ASA had FAA
approval to fly in excess of the required inspection time by as many as 500 hours.
40
Pursuant to criteria set forth in Hamilton Standard ASB 14RF-9-A66 (incorporated by
reference in AD 94-09-06), indications of 50 percent full-scale height and above, as viewed on a
cathode ray tube screen, were rejectable. Indications of 40 to 50 percent were “reportable” on the
inspection record but were not cause to reject the blade.
41
Blending in this context means grinding or sanding the surface to remove a small
amount of material containing an imperfection and then restoring the surface finish to a condition
equal to the surrounding area.

38
he was permitted to perform and sign off the work that he was qualified to
perform. The technician, as an employee of Hamilton Standard’s Rock Hill blade
repair facility, which is an FAA-certificated repair station under 14 CFR Part 145,
is not required to be a certificated mechanic to work on the propeller blades. In
the shop traveler form for the accident blade, the instructions to blend the taper
bore also specify that the surface finish should be 63 RMS. The block on the form
was initialed and dated by the technician, but an adjacent block that would have
signified a second inspection by a repairman
42
was blank. Although the shop
traveler form for the ultrasonic inspection after the blending on the accident blade
showed that there were no reportable or rejectable indications, the shop traveler
form did not show that the blade had received a final inspection after the work was
completed. However, Hamilton Standard provided ASA with an FAA Form 8130-
3, Airworthiness Approval Tag, indicating that the PS960A repair had been
completed.
Subsequent examination by the Safety Board indicated that about
0.002 inch of material was removed from the taper bore. The shop traveler form
indicates that the blade passed a postrepair ultrasonic inspection.
43
Because no
defects were found during the June 7, 1994, borescope inspection, and the blade
was marked with “PS960A” (indicating accomplishment of the repair), the blade
was exempt from the requirements of AD 95-05-03 (effective on March 23, 1995)
for recurrent taper bore ultrasonic inspections and enhanced borescope inspection.
Investigators attempted to establish how the decision was made to
blend the area of the unacceptable indication in the taper bore of the accident
blade, even though there was no visible mechanical damage and PS960A did not
explicitly require or authorize blending of a blade taper bore that was free of
visible mechanical damage. During an interview with the technician who
performed the taper bore repair, he stated that he had been told that the
shotpeening of the taper bore could cause “false” ultrasonic indications. Further,
he stated that he understood, based on his training in the repair by the Rock Hill
42
A repairman, as defined in 14 CFR, Parts 65.101 and 65.103, is recommended for
certification by the repair station and is then certificated by the FAA. He must have at least 18
months of experience on the specific task, have completed specialized training, and may
supervise maintenance of aircraft components by the repair station.
43
The shop traveler form indicated that a blade that “failed” the postrepair, ultrasonic
inspection could be reblended. If the blade “failed” the ultrasonic inspection after the second
attempt to blend the rejected area, it was to be sent to Hamilton Standard’s Windsor Locks
facility.

39
facility Engineering Manager, that it was acceptable to use the PS960A process to
blend out unexplained ultrasonic indications for blades with unshotpeened taper
bores, as well as those with shotpeened taper bores. He said that he recognized the
difference in surface finish between shotpeened and unshotpeened blades. He also
stated that if he came across something that he did not understand or recognize, he
would not hesitate to seek assistance from the facility Engineering Manager. The
technician further stated that he had blended about 10 propeller blades without
shotpeened taper bores that had ultrasonic indications but no visible damage.
During an interview on October 19, 1995, the Rock Hill Engineering Manager
stated that the April 27, 1994, memorandum covered both shotpeened and
unshotpeened blades. However (as already noted in Section 1.16.3), in a letter to
the Safety Board dated March 5, 1996, Hamilton Standard indicated that the
memorandum was intended to document the authorization to use the PS960A
blend repair to “remove tool marks or the peaks of shot peen impressions.” The
letter further stated that “there was no discussion of how to handle blades that had
not been shot peened.”
After the PS960A blending repair, the accident blade was rebalanced
and the taper bore was sealed with protective material. It was also determined that
some additional repair was necessary to the composite surface features of the
blade. The blade was returned to Hamilton Standard’s East Windsor, Connecticut,
facility to complete that work. The blade was shipped back to ASA on August 30,
1994, and was reinstalled on the left propeller assembly of the accident airplane on
September 30, 1994. It remained there until the accident. At the time of the
accident, the blade had accumulated 2,398.5 hours and 2,425 cycles since the
Hamilton Standard repair at Rock Hill.
1.16.5 Results of 14RF-9/EMB-120 Stress Survey
To reduce cabin noise during ground operation, the EMB-120 aircraft
was certificated with model 14RF-9 propeller assembly designed to rotate at a
relatively low ground idle revolutions per minute (rpm), between 50 and 65
percent. To operate successfully in the 50 to 65 percent rpm range without
overstressing the propeller, the design had to avoid the coincidence of any blade
resonant frequencies
44
with any excitation frequencies.
45
To accomplish this, the
44
The resonant frequency of any vibration is the naturally occurring frequency at which
the blade will vibrate when excited. To avoid excessive vibration and overstressing of the

40
upper rpm limit of 65 percent for ground operation was set below the resonant
frequency of the first flat-wise mode of vibration
46
of the 14RF-9 blade of
approximately 70 percent rpm. Although all 14RF blades have a resonant
frequency at approximately 70 percent rpm, because of small differences in blade
construction, there is some variation in the exact resonant frequency from blade to
blade.
47
The exact resonant frequency of the accident blade could not be
determined because it had separated and was damaged.
The Hamilton Standard 14RF-9 blade for the EMB-120 was designed
so that its first flat-wise resonant frequency would not coincide with the 2P
48
excitation frequency during ground operation. However, the coincidence or close
proximity of the ground rotational speed and the first flat-wise resonant frequency
can place the propeller in a resonant condition and results in undesirable vibratory
stress. (See Figure 4 for an illustration of the vibratory modes of the 14RF-9
propeller.)
propeller, propeller design practice requires that the propeller spend only a minimal amount of
time in an rpm range that corresponds to a resonant frequency.
45
Excitation frequencies are created by aerodynamic loads that act on a propeller. Some
aerodynamic loads on a propeller are cyclical. The frequency of these cyclical loads are
multiples of propeller rpm. The frequency of the first cyclical aerodynamic load (1P) is equal to
propeller rpm; that is, one cycle per revolution.
46
The first flat-wise mode of vibration is the lowest frequency vibration. (There are
multiple orders of vibration, and each has an associated frequency called a resonant or natural
frequency.)
47
A resonant frequency of a propeller blade is a function of the blade’s rigidity, mass
distribution and, to some extent, retention stiffness.
48
The frequency of the second aerodynamic load (2P) acts on all propeller blades twice
per revolution because the blade senses the wing leading edge as it rotates past it. The 2P
excitation frequency is always present but is most pronounced during ground operation in a
tailwind or quartering tailwind condition.

41
w
TECHNOLOGIES
wLm
‘W-
CAMPBELL DIAGRAM FOR
EMB120
4P
JAV-9-1 2-95
HAMILTON STANDARD
14RF-9
PROPELLER
n
80
70-
2
II
Ill
I
60
>
Q
u
z
g
g
50
u
A
Ill
APPROXIMATE
u
RESONANT RPM
L
40
1-
BAND FOR Ist MODE
z
("REACTIONLESS")
*
u
g
30
in
=-
&
u
20
-
‘~
/
10
Y
.
*
,Allowable’
Range for
Static
OD
v
o
10
20
70
Pi”OPELL:#
PERC:~T
SPEE:O(l 00%
=
1300
RPh~
90 1
00
|
0
100
200
300 400 500 600
700
800
900
1000
1100
1200
1300
PROPELLER RPM
Figure 4.--Vibratory modes of the
14RF-9
propeller.

42
When the first flat-wise vibration frequency and the 2P excitation
frequency coincide, a four-bladed propeller, such as the 14RF-9, vibrates in the
reactionless
49
mode. The reactionless mode of vibration is characterized as when
two blades of a four-bladed, rotating propeller, 180 degrees apart, reach a negative
stress peak at the same time that the other two blades reach their positive stress
peak. This type of propeller vibration is called reactionless because the bending
loads of the four blades are canceled at the propeller hub which consequently
transmits little or no vibratory loading to the propeller mounting structure.
As originally certificated, the EMB-120 Airplane Flight Manual,
Maintenance Manual, and a cockpit placard stated that propeller rpm (Np)
50
above
65 percent should be avoided during ground operations with the aircraft stationary,
and with rear quartering winds in excess of 10 knots, except for short duration
transitions.
The 1983 and 1985 certification testing of the EMB 120 with the
model 14RF propeller was accomplished using an instrumented, new propeller
blade. The original stress surveys, which included flight and ground
51
tests, and an
additional ground test following the ASA accident, revealed that the resonant
frequency of the first flat-wise mode varied from approximately 70 percent to 76
percent. Because the actual resonant frequency of a propeller must be determined
during ground testing, and because propeller assemblies are not measured
49
The Safety Board investigated another accident on April 19, 1993, in Zwingle, Iowa, in
which a Mitsubishi MU-2B-60 airplane experienced an in-flight loss of a propeller blade and
collided with terrain (NTSB/AAR-93-08). All of the occupants were killed, and the airplane was
destroyed. The Safety Board attributed the loss of the propeller to a reduction in the fatigue
strength of the hub material, combined with exposure to higher-than-normal cyclic loads during
ground operations when the propeller vibrated in the reactionless mode. The investigation
revealed that during certification testing of the Hartzell HC-B4 propeller on the MU-2B airplane,
a reactionless mode of vibration was identified with the peak stress occurring at a propeller speed
of 1,079 rpm. As a result, the propeller was prohibited from continuous operation on the ground
below 1,145 rpm. The Safety Board did not find evidence that the test was repeated using
propeller blades altered to conform to the minimum dimensions specified in the repair limit
criteria of Hartzell’s HC-B4 propeller maintenance manual.
50
Propeller rpm expressed as a percentage of the maximum operational limitation.
51
The test airplane was subjected to the propeller wash of a second airplane to simulate
normal ground operations in a quartering tailwind. This was accomplished to determine the high
stress peaks of the propeller blade associated with the 2P excitation frequency within the normal
propeller rpm range.

43
separately, the actual resonant frequency of the accident blade could have been
slightly different than the frequencies measured in these tests.
Following the accident, Hamilton Standard conducted an independent
blade stress survey in the latter part of 1995 and presented its report as part of a
technical presentation to Safety Board investigators on February 2, 1996 (see
Appendix D for Summary of Results, Conclusions and Recommendations). The
1995 stress survey also consisted of a flight and ground test, using four
instrumented blades on both engines with two taper bore configurations. Of the
four blades, one blade had zero service time, and the other three blades had
approximately 12,000 service hours. The survey concluded that only small
differences
52
from previous stress level surveys were observed, including those
from the original certification and the postaccident test referenced above. The
highest vibratory stress measured in flight was reported to be about 6,000 pounds
per square inch (psi). The highest ground running peak stress was reported to be
about 18,000 psi. This occurred with quartering tailwinds when the propeller
passed through the range corresponding to vibration of the blade twice per
revolution in the first flat-wise mode (2P/1f).
After the ground tests were completed, Hamilton Standard initiated
actions to modify the EMB-120 Airplane Flight Manual and Maintenance Manual
Limitations Sections with revised language to reduce the maximum propeller Np
limit during ground operation from 65 to 60 percent. On December 20, 1995,
airworthiness authorities in Brazil and the FAA approved temporary revisions to
the language as follows:
Airplane Flight Manual: Condition Levers must be in MIN RPM
position during all ground operations, except when cleared for
takeoff or during landing roll. Power Levers must remain at or
below Flight Idle during all ground operations, except for brief
(approximately 5 seconds) excursions as needed to maneuver the
airplane.
52
The vibration and loads survey was conducted by Hamilton Standard on the 14RF
propeller on an Embraer EMB-120 airplane. A possible small downward shift was discovered in
the 2P resonant frequency relative to the 1985 certification test data. The downward shift was
attributed by Hamilton Standard to normal wear and mass properties in the propeller blade from
normal operation.

44
CAUTION: GROUND OPERATION ABOVE FLIGHT IDLE
SIGNIFICANTLY INCREASES PROPELLER STRESS UNDER
CERTAIN ADVERSE WIND CONDITIONS (E.G., TAILWINDS
OR REAR CROSSWINDS). OPERATION IN THIS RPM
RANGE MUST BE AVOIDED TO THE MAXIMUM EXTENT
PRACTICABLE.
Maintenance Manual: Propeller System Operating Limitations, To
prevent excessive propeller stress, do not operate above 60% Np
unless the wind is less than 18.5 Km/h (10 Knots) or the airplane
is headed into the wind + or - 45 degrees. Wind direction must be
monitored locally at the run-up site.
1.17 Organizational and Management Information
1.17.1 Hamilton Standard Division, United Technologies Corporation
Hamilton Standard Division, Windsor Locks, Connecticut, has
produced aluminum blade propellers with taper bores since 1958. More than
10,000 such blades are in use on C-130 and P-3 military airplanes. Composite
blade propellers were introduced for military airplanes in 1974. Their use was
expanded to regional (commuter) airplanes in 1978. Since that time, regional
airplane propellers equipped with more than 15,000 blades that are fabricated with
an aluminum spar and an aerodynamic shell of composite materials have
accumulated in excess of 17 million flight hours.
A customer support facility for regional propeller inspection and
repair was opened in East Windsor, Connecticut, in 1989. Hamilton Standard’s
engineering support continued to reside with the manufacturing facilities at
Windsor Locks.
From 1989 through 1990, regional propeller inspection and repair
expanded to facilities in Long Beach, California, and Maastricht, the Netherlands.
In 1993, the regional propeller customer support center was moved from East
Windsor, Connecticut, to a facility in Rock Hill, South Carolina.

45
1.17.2 Hamilton Standard Propeller Customer Service Center
Selected engineering and management personnel from the Hamilton
Standard Division, Windsor Locks, were transferred in 1993 to the new regional
propeller Customer Support Center in Rock Hill. Management at the Rock Hill
facility hired technicians from a large pool of local area applicants and trained
them to perform various propeller blade repairs. The facility was certificated by
the FAA to begin repairing propeller blades in February 1994.
As a result of the two propeller blade failures in March 1994,
53
and
the resulting ultrasonic inspections of the taper bore mandated by the FAA
54
in
May 1994, there was a sudden increase in the number of propeller blades requiring
inspection and repair in May and June 1994. The accident propeller blade was one
of the blades returned to Hamilton Standard as a result of the inspection. The
taper bore inspection and repair of the accident blade was performed at Hamilton
Standard’s Customer Support Center in Rock Hill between June 7, and June 9,
1994.
According to Hamilton Standard work records from May and June
1994, the technician who performed the taper bore inspection and repair of the
accident blade worked between 8 and 26 hours of overtime each week, in addition
to his normal work week.
1.17.2.1 Employee Training at Hamilton Standard
Customer Service Center
According to the Engineering Manager in Rock Hill, new technicians
at the facility received approximately 250 hours of training on a specific propeller
blade repair before they are permitted to make repairs without direct supervision.
However, the technician who made the taper bore repair to the accident blade was
transferred from the nickel sheath and fiberglass repair area of the shop and had
received 250 hours of training in connection with that position. In addition, he
received approximately 90 hours of additional on-the-job training (OJT) on the
taper bore repair. This technician had a background in automotive repair. His
additional OJT training on the taper bore repair procedure was administered by the
53
Details of the two previous failures are contained in Section 1.16.2.
54
AD 94-09-06 required an ultrasonic inspection of the taper bore. (See Section 1.16.3
for details on the AD.)

46
facility Engineering Manager, who had other responsibilities in addition to
employee training.
The investigation revealed that during the time the accident blade was
being repaired, the technicians at the service centers had not been provided a
photograph or model illustrating the appearance of corrosion or cracking in a taper
bore. Neither the Engineering Manager nor the technician who performed the
inspection and repair of the accident blade had ever seen a crack in the taper bore
of a blade. Several months after the accident blade was inspected and repaired, all
the service center technicians were provided with an enlarged color photograph of
taper bore corrosion, a model and an instructional video.
1.17.3 Designated Engineering Representative
The FAA annually appointed several Hamilton Standard engineering
employees based in Windsor Locks to serve as Designated Engineering
Representatives (DER) in propeller systems to approve certain engineering
information.
55
Those DER duties normally represented about 20 to 30 percent of
his or her workload. There were nine DERs certificated to support propeller
systems at the time of the accident. Under an agreement with the FAA, Engine
and Propeller Directorate, DERs have authority to approve certain engineering
changes, repairs, service bulletins and maintenance manuals. However, the
requirement for direct FAA approval was retained for changes affecting critical
parts or single point failure components.
After the two blade failures in March 1994,
56
a Hamilton Standard
DER
57
was in contact with the FAA, Engine and Propeller Directorate, several
times a week during the development of the ultrasonic inspection requirements
that were set forth in the ASB subsequently mandated by AD 94-09-06, and the
taper bore repair procedures contained in PS960 and PS960A. The DER was
55
In accordance with 14 CFR 183.29(f), a propeller engineering representative may
approve engineering information relating to propeller design, operation, and maintenance, within
limits prescribed by the Administrator of the FAA, whenever the representative determines that
information complies with applicable FARs.
56
See Section 1.16.2 for details.
57
The DER who was the central figure in the activity related to this accident was initially
appointed in October 1992. He had 16 years of experience at the Windsor Locks propeller
facility. He holds a Bachelor of Science degree in astronomy and a Master’s Degree in business
administration. He also attended a university-level course in aircraft accident investigation.
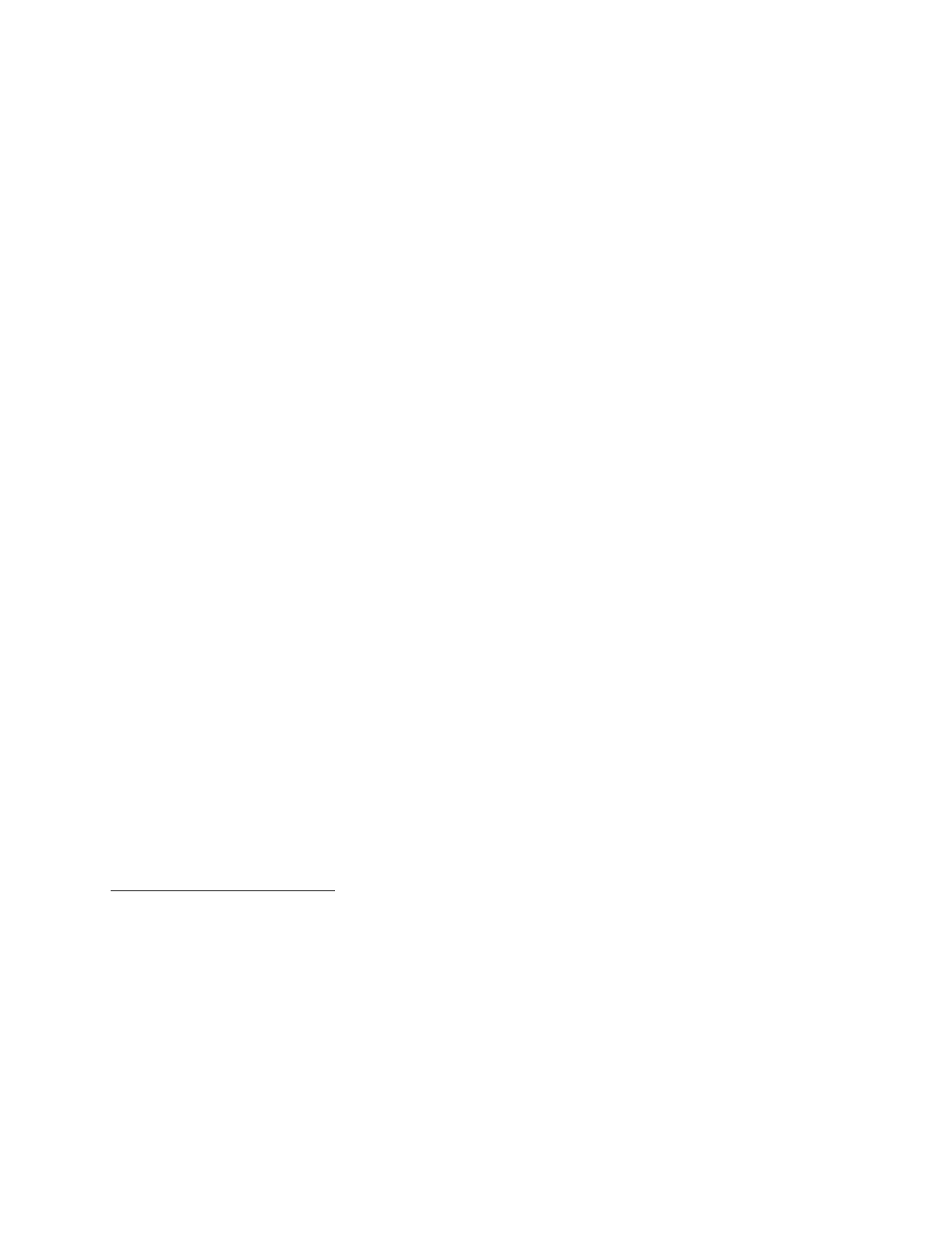
47
involved in developing the ASB and PS960/960A. The DER was familiar with the
issue of taper bore corrosion, the formation and functions of the Rock Hill
Customer Service Center, and the white light borescope inspection technique used
to search for evidence of cracks and corrosion, and to reject blades for engineering
evaluation. After the accident, he told investigators that based on his knowledge
of the March 1994 accidents, he believed the white light borescope inspection
would be adequate to enable technicians to detect corrosion pits in the taper bore
of the size that led to the cracks that caused the two previous failures.
The DER stated that he was not aware of the discussions between
engineering managers at Windsor Locks and the Customer Service Centers in
which it was decided to extend the taper bore repair procedures outlined in
PS960A beyond their intended use (to blend visible mechanical damage in taper
bores) to blend ultrasonic indications that were not related to visible mechanical
damage. He said that this lack of coordination from the engineering department
was atypical.
1.17.4 FAA Certification Engineer
The FAA certification engineer
58
responsible for Hamilton Standard
regional propellers reviewed the fracture analysis of the two blade fractures in
March 1994. He determined that the FAA should retain direct approval authority
for the data and the inspection and repair techniques used for PS960/PS960A
because, based on the two blade failures that resulted from taper bore corrosion, he
considered the taper bore to be a critical part.
59
The Certification Engineer also
required that the repair for mechanical damage in the taper bore be accomplished
only at Hamilton Standard repair facilities.
58
The FAA certification engineer had been with the FAA Engine and Propeller
Directorate for 9 years at the time of the accident. He holds a Bachelor of Science degree in
mechanical engineering. He has 30 years of government experience, primarily with U.S. Navy
programs. His experience includes propellers for surface ships and submarines.
59
FAA Order 8110.37A (DER Guidance Handbook), Paragraph 14.h.(1)states that “The
DER must obtain specific authorization from the appointing ACO [Aircraft Certification Office]
prior to initiating approvals for repairs or alterations. An authorized DER may approve technical
data for major repairs and alterations without first notifying the project ACO, except when the
part is critical or life limited. For critical or life limited parts, the DER must contact the project
ACO for guidance.”

48
The Certification Engineer (like the DER) stated that he was not
aware that blending procedures outlined in PS960A (originally approved as a
repair for areas with visible mechanical damage) had been extended by Hamilton
Standard engineers as an authorized repair to areas in which ultrasonic indications
were present without visual evidence of mechanical damage.
1.18 Additional Information
1.18.1 Safety Board Recommendations
The Safety Board issued the following three Safety Recommendations
to the FAA on August 25, 1995, which was 4 days after the accident:
A-95-81 (Class I, Urgent Action)
Immediately implement the ultrasonic inspection program on
Hamilton Standard propeller blades cited in paragraph (a)(2) of
airworthiness directive (AD) 95-05-03, irrespective of prior
compliance with paragraph (d) of the AD. Require the initial
inspection before further flight on any propeller blades that have
accumulated 1,250 cycles since the last ultrasonic inspection or
since the visual and borescope inspection required by paragraph
(d) of the AD.
A-95-82 (Class II, Priority Action)
Conduct a vibration and loads survey and analysis of the propeller
installation on the Embraer EMB-120 airplanes with applicable
Hamilton Standard propellers throughout the ground and flight
operating range of the engine with specific consideration for the
effects [that] propeller in-service wear, maintenance, or other
changes may have on the resonant frequencies. Based on the
findings, broaden the survey and analysis to other installations as
appropriate.
A-95-83 (Class II, Priority Action)
Review the current overhaul and inspection requirements for all
Hamilton Standard 14 series propeller blades for which the taper
bore hole has been shotpeened to determine whether additional
inspections or maintenance should be required.

49
Regarding Safety Recommendation A-95-81, on August 25, 1995, the
FAA issued a telegraphic AD (T95-18-51) requiring that certain blades installed
on EMB-120 aircraft that had ultrasonic crack indications discovered as a result of
inspections required by AD 94-09-06 or AD 95-05-03, been reworked, and had
been returned to service, be removed from service within the next 10 flight cycles
and be replaced with serviceable parts. The telegraphic AD also required that
propeller blades installed on aircraft other than the EMB-120 meeting the same
criteria (ultrasonic crack indications reworked and blade returned to service) be
inspected ultrasonically for cracks within the next 10 flight hours and every 1,250
cycles thereafter. Any blades removed from service as a result of the AD could
not be returned to service. On January 16, 1996, the Safety Board classified
Safety Recommendation A-95-81 “Closed--Acceptable Alternate Action.”
Regarding A-95-82, on July 24, 1996, the FAA informed the Safety
Board that it conducted the requested vibration and loads survey. The FAA
reported that the survey substantiated the results of past stress surveys indicating
that no new high stress conditions were uncovered, and that it did not show that
further evaluations were needed on other installations. However, to limit propeller
exposure to known high vibratory stresses during ground operation, on December
27, 1995, the FAA issued AD 95-25-11, which requires installation of a placard
reading “Avoid Np Above 60% During Ground Operations,” and also requires
revising the EMB-120 Airplane Flight Manual and maintenance program to limit
the rotational speed of the propeller during ground operation. In its Final Rule,
published in the Federal Register, the FAA stated that the AD is considered “an
interim action until final action is identified, at which time the FAA may consider
further rulemaking.” Based on the FAA’s interim actions and the statement
contained in its announcement of the Final Rule, on November 15, 1996, the
Safety Board classified Safety Recommendation A-95-82 “Open--Acceptable
Response.”
Regarding A-95-83, on July 24, 1996, the FAA informed the Safety
Board that its review of the overhaul and inspection requirements for all Hamilton
Standard 14RF, 14SF and 6/5500/F blade designs for which the taper bore hole
has been shotpeened showed that additional action should be taken. On April 24,
1996, it issued AD 96-08-02, requiring repetitive ultrasonic inspection of the
blades until they are repaired and restored to their certificated strength. The repair
of EMB-120 blades was required to be accomplished by August 1996, and all
other blades will be repaired by February 1997. Since the actions of the FAA are

50
responsive to the intent of the recommendation, on November 15, 1996, the Safety
Board classified Safety Recommendation A-95-83 “Closed--Acceptable Action.”
On June 27, 1996, the Safety Board issued the following additional
safety recommendations to the FAA:
A-96-33
Conduct a design review of the Embraer EMB-120 flight data
recorder system, with emphasis on potentiometer failures, and
mandate design, installation, and/or maintenance changes, as
necessary, to ensure that reliable flight control data are available
for accident/incident investigation.
A-96-34
Require Embraer EMB-120 operators to perform a flight data
recorder (FDR) readout or a potentiometer calibration test per
section 31-31-00 of the EMB-120 Maintenance Manual every 6
months until FDR sensor design, installation, and/or maintenance
improvements are incorporated.
On September 5, 1996, the FAA responded that it had initiated a
design review focusing on the potentiometers and associated attaching hardware,
and would determine a course of action when the review is complete. The FAA
also stated that it would contact the manufacturer and coordinate the necessary
maintenance instructions with an appropriate inspection interval. Therefore, on
October 15, 1996, the Safety Board classified both A-96-33 and A-96-34 “Open--
Acceptable Response,” pending final action.
1.18.2 Postaccident Hamilton Standard and FAA Actions
As a result of the accident and Safety Board recommendations, on
August 25 and 28, 1995, the FAA issued AD T95-18-51 and AD 95-18-06,
respectively, which required that all blades installed on EMB-120 aircraft that, like
the accident blade, had been removed from service in accordance with AD 94-09-
06 (or 95-05-03) and been reworked and returned to service be immediately
removed from service, and it required an ultrasonic reinspection of all other 14RF,
14SF, and 6/5500/F blades (a total of approximately 15,000 blades) on a 1,250
cycle interval.

51
As a result of the Luxair accident, Hamilton Standard developed an
additional series of service bulletins that were mandated by the FAA in
Airworthiness Directive (AD) 95-24-09, issued on November 16, 1995. This AD
required an ultrasonic shear wave inspection on the propeller shank for cracks or
indentations. Four blades were removed from service as a result of this AD.
As the inspections mandated by AD 95-18-06 began to take place,
Hamilton Standard recognized a need for a detailed reevaluation of the
adequacy/appropriateness of this inspection procedure because the ultrasonic
inspections continued to reject blades with no apparent discrepancies on the taper
bore. This reevaluation showed that the minimum detectable size of a taper bore
crack varied widely. That is, it could be much greater (and, in some cases,
smaller) than previously believed. Hamilton Standard found that there were
differences in the calibration blocks
60
distributed for the inspection, and that
differences in the thickness of the surface composite layers and in the
transmitability of the ultrasonic beam through the aluminum spar could
substantially affect the inspection results.
Coincidentally, Hamilton Standard performed a risk analysis of the
failed blades to resolve inconsistencies in the crack growth data from the Inter-
Canadien, Nordeste, and ASA blade separations. Results from a NASA-developed
fracture mechanics FASTRAN program were integrated into the risk analysis.
Hamilton Standard concluded that for some blades of each model, the 1,250 cycle
inspection interval using the original ultrasonic technique provided insufficient
safety margins for the detection of taper bore cracks. Thereafter, Hamilton
Standard issued another series of ASBs for the 14RF, 14SF, and 6/5500/F blades,
containing a newly-developed ultrasonic inspection technique with a customized
calibration procedure for each blade and a reduced inspection interval. For the
14RF blades used on the EMB-120 airplanes, the inspection interval was reduced
to 500 cycles. The FAA issued AD 96-01-01, effective on January 19, 1996,
requiring the improved ultrasonic inspection technique and mandating the reduced
cyclic inspection interval.
In March 1996, Hamilton Standard issued ASB 14RF-9-61-A94 to
repair and restore the taper bore surface to its original surface finish (with
shotpeening) on all model 14RF-9 propeller blades installed on EMB 120
60
Test specimens manufactured with defects of known sizes used to adjust the threshold
of pass/fail for ultrasonic inspection equipment.

52
airplanes and on similar model blades installed on other commuter-type airplanes.
On April 24, 1996, the FAA issued AD 96-08-02, which required that all blades of
the affected propellers be repaired by specific end dates. The end date for the
14RF-9 model blade was August 31, 1996, and for other affected models is
February 28, 1997. The repair procedure included removal of a layer of spar
material from the taper bore, followed by an eddy current inspection, fluorescent
penetrant inspection (FPI), removal of an additional layer of material, a wall
thickness check, shotpeening, and the application of a corrosion-protective
coating. Hamilton Standard also conducted fatigue tests on a set of blades with
the minimum allowable remaining wall thickness between the taper bore and the
outside of the spar, thereby verifying the fatigue characteristics of blades repaired
in this manner. Once a blade is repaired, the requirements for ultrasonic
inspection are eliminated, and further visual inspections of the taper bore will take
place only as part of the major inspection that is required every 9,500 flight hours.
There are no calendar-based inspection requirements.
Hamilton Standard informed the Safety Board that all 14RF-9 blade
repairs were accomplished within the time limit established in the AD. The Safety
Board also notes that the Component Maintenance Manual (CMM) for all
Hamilton Standard model 14FR, 14SF, and 6/5500F airplane propellers (which
includes all propellers used in commuter operations), has been amended to include
a recurring inspection of the taper bore.

53
2. ANALYSIS
2.1 General
The flightcrew was trained, certificated and qualified to conduct the
flight, and the flight was conducted in accordance with applicable FARs and
company requirements. The flight attendant also was appropriately trained and
qualified. The flightcrew was in good health and held the proper FAA medical
certificates. There was no evidence that the performance of any crew member was
impaired by alcohol, drugs, or fatigue.
The airplane was maintained in accordance with applicable FARs and
company Operations Specifications. A review of the airplane’s maintenance
records and operating history did not reveal any maintenance discrepancies or
mechanical anomaly that would have either caused or contributed to the accident.
Evidence from the CVR, FDR, and examination of the powerplants,
reduction gear boxes, and propellers indicated that the engines were operating
normally during the flight until the loss of a major portion of one propeller blade
on the left engine. After the propeller blade separation, the combination of the
resulting loss of left engine thrust, increased drag from a deformed engine nacelle
and the three blades retained in the propeller hub, and added frontal drag from
external sheet metal damage, degraded airplane performance, preventing the
flightcrew from arresting the airplane’s descent or making rapid changes in its
direction of flight making a forced landing necessary. The Safety Board concludes
that because of the severely degraded aircraft performance, the flightcrew’s
actions were reasonable and appropriate during their attempts to control and
maneuver the airplane throughout the accident sequence and were not a factor in
this accident.
2.2 Analysis of the Propeller Blade Failure
The Safety Board concludes that one of the four blades from the left
engine propeller separated in flight because a fatigue crack that originated from
multiple corrosion pits in the taper bore surface of the blade spar propagated
toward the outside of the blade, around both sides of the taper bore, then reached
critical size. (See Section 1.16.1.)

54
Results of investigations conducted in two previous propeller blade
failures in 1994, one in Brazil with this model blade and the other in Canada with
a similar model blade, indicated that corrosion was produced when entrapped
moisture reacted with residual chlorine in a bleached cork used to retain the lead
wool in the taper bore hole of the propeller. The accident blade exhibited a nearly
continuous layer of oxide deposits on the initial 0.049 inch of the crack depth.
These deposits contained a substantial amount of chlorine. The Safety Board
found that the ASA propeller blade contained corrosion damage (pitting) in the
taper bore and the oxide layer in the origin area of the fatigue crack in the
separated ASA propeller blade, as did the two previous failed propellers. Because
the oxidizing condition and the cork containing chlorine were eliminated from the
accident blade per PS960A during the June 1994 repair at the Hamilton Standard
Customer Support Center in Rock Hill, oxide deposits would not be expected to
have formed during further crack propagation after the PS960A repairs.
Therefore, the extent of the oxide layer on the fracture (to a depth of 0.049 inch
below the surface) was indicative of the size of the crack at the time of the Rock
Hill repair activities.
2.2.1 The Accident Blade’s June 1994 Inspection, Repair, and Return
to Service
2.2.1.1 Inappropriate Use of PS960A Blending Repair
As discussed in Section 1.16.4, the technician who inspected and
repaired the accident blade first confirmed the rejectable ultrasonic indication, and
then visually examined the taper bore for evidence of corrosion, pits or cracks
using a white light borescope. He wrote on the shop traveler, “No visible fa[u]lts
found, blend rejected area,” and used the blending repair procedure set forth in
PS960A to remove the ultrasonic indication. The blended area was later found to
be the site of a crack originating in corrosion pits.
Apparently, Hamilton Standard engineering originally intended
PS960A only to remove possible sources of stress concentration by blend-
repairing mechanical damage (visible tool marks) within the taper bore of any
blade, without regard for whether the surface was shotpeened or not shotpeened.
The instructions in PS960A with regard to the surface finish of the taper bore
specifically stated, “No unblended mechanical damage is allowed.” The FAA
reviewed and approved the repair for this purpose. However, the use of PS960A
blending repair was expanded by Hamilton Standard engineering to blend the area

55
of ultrasonic indications even when there was no apparent mechanical reason
(visible tool mark) associated with the ultrasonic indication.
The Safety Board considered whether it was appropriate, from an
engineering perspective, for Hamilton Standard to extend the applicability of
PS960A beyond its original purpose (blending of mechanical damage), and to
authorize its use for removing ultrasonic indications caused by shotpeen
impressions. Surface irregularities created by shotpeening are, in effect, a form of
mechanical surface alteration, and the concept of blending mechanical damage is
not per se objectionable, so long as there are no cracks or other defects in the area
being blended.
61
Based on the prior blade separations (both of which involved
cracks originating from corrosion), Hamilton Standard had no reason to believe
that mechanical damage in taper bores was causing cracks. Therefore, the Safety
Board concludes that Hamilton Standard’s engineering decision to use the
PS960A blending repair to remove ultrasonic indications caused by a shotpeened
taper bore surface was technically reasonable.
Although the decision by Hamilton Standard engineers to extend the
applicability of PS960A to impressions in shotpeened taper bores was technically
reasonable, the procedure by which that decision was communicated to others
within Hamilton Standard was deficient. The decision was communicated during
a conference call involving top engineering managers, but it was not discussed
with the DER or the FAA. It was then documented in a memorandum that
contained no indication that it represented an extension of PS960A, and made no
reference to shotpeened taper bores. The memorandum stated only that blades
returned as a result of an ultrasonic inspection should be reworked “per
PS960A.”
62
The substance of the decision was then verbally transmitted by the
engineering manager of the Rock Hill facility to his staff but, as evidenced by the
technician’s belief that he was authorized to use the PS960A blend repair to
remove ultrasonic indications on both shotpeened and unshotpeened blades, it was
either misstated or misunderstood.
61
The blending process could mask the existence of a crack if done improperly (see
Section 2.2.1.2, discussing effects of failing to restore the original surface finish) or if enough of
the crack is removed by the blending so that the ultrasonic indication is reduced to a
nonrejectable height.
62
See Section 1.16.3 for more information about the circumstances surrounding the
decision to extend PS960A.

56
Although Hamilton Standard management asserted that this
expansion of the use of the PS960A blending repair procedure applied only to
ultrasonic indications in shotpeened taper bores, it was understood, at least by the
technician who worked on the accident blade, as being applicable to unexplained
ultrasonic indications in unshotpeened taper bores as well. Given that
unexplained ultrasonic indications in the taper bore area represent an unknown
condition suggestive of cracking and, further, that (according to statistical data
provided by Hamilton Standard) blades without shotpeened taper bores are
susceptible to earlier corrosion and to cracking once corrosion begins, Hamilton
Standard management (both in Windsor Locks and in Rock Hill) should have
made certain that the technicians performing the repair clearly understood that the
extension of PS960A was intended for shotpeened taper bores only.
If the technician had clearly understood that he was not authorized to
blend unexplained ultrasonic indications in unshotpeened taper bores, he would
have rejected the accident blade, or at least sought additional guidance from his
engineering manager as to how to handle the unexplained ultrasonic indication. In
either case, the accident blade would not have been subjected to the PS960A blend
repair, which masked the existence of the crack (see Section 2.2.1.2), and would
not likely have been returned to service. The Safety Board concludes that the
manner in which the unapproved extension of PS960A was documented and
communicated within Hamilton Standard, and the lack of training on the
extension, created confusion and led to misapplication of the blending repair to
unshotpeened blades with unexplained ultrasonic indications, allowing the
accident blade to be placed back into service with an existing crack, thus
contributing to this accident. The Safety Board is concerned about the adequacy
of Hamilton Standard’s internal communication and documentation. This issue is
further addressed in Section 2.6.1.
2.2.1.2 Sanding (Blending) of the Accident Blade
As noted in Section 1.16.1, although PS960A required that the
blended area be restored to its original surface finish, the sanding marks in the
blended area of the accident blade were much rougher than the original surface
finish. The sanding marks left by the blending appeared to have smeared some of
the corroded surface, suggesting that the sanding took place after the corrosion
had formed. Although some of the fatigue initiation area was along the sanding
marks, the fatigue cracking initiated from corrosion pitting damage that extended
below the taper bore surface to a depth much greater than the sanding marks.

57
Therefore, the Safety Board concludes that the sanding marks left by the PS960A
blending repair did not contribute to the initiation of the fatigue crack in the
accident blade. However, as discussed below, the sanding marks may well have
allowed the cracked blade to pass the ultrasonic inspection following the PS960A
blending repair.
Following the PS960A blending repair, the accident blade was again
ultrasonically inspected, and this time, neither a rejectable
63
nor a reportable
64
indication was generated. This allowed the blade to be returned to service, and it
was installed on the accident airplane. Safety Board laboratory measurements
indicated that only a minimal amount of material (less than about 0.002 inch) was
removed from the taper bore surface during the PS960A blending repair process.
Although removal of this amount of material would have slightly decreased the
size of the crack, it is unlikely that such a small decrease, by itself, would have
reduced the ultrasonic indication from 60 or 52 percent (the magnitude of the
indications recorded in the previous on-wing inspection and upon receipt at Rock
Hill, respectively) to below 40 percent (the minimum level that must be recorded
on the inspection form).
The ultrasonic inspection beam must reflect off both the defect and
the taper bore surface to bounce back to the transducer and be detected. However,
the surface finish in the taper bore was much rougher than the original finish, and
the sanding scratches that remained in the taper bore surface would have caused
the ultrasonic beam to scatter or become diffused as the beam reflected from the
taper bore surface. It is likely that this was the major reason for the decrease in the
size of the ultrasonic indication. Therefore, the Safety Board concludes that the
failure to restore the taper bore surface to the original surface finish during the
blend repair, as required by PS960A, was a factor that caused the reduction of the
ultrasonic indication that allowed the blade to pass the final ultrasonic inspection
and to be returned to service, and thus contributed to the accident.
In trying to determine why the technician did not properly perform
the blend repair, the Safety Board noted that PS960A did not describe or refer to
procedures that would ensure that the blended area was restored to its original
surface finish but simply stated this as a requirement. The technicians were
provided with examples of the required surface finish, which were designed to
63
50 percent or over of full-scale height.
64
40 percent or over of full-scale height.

58
assist them in determining whether the blended surface finish was appropriate.
However, Safety Board investigators found that it was difficult to distinguish
whether a particular surface finish varied from the examples. Investigators also
considered the possibility that the technician’s improper performance of the blend
repair was related to inadequate training in the repair,
65
his automotive
background, or the long hours he was working at the time.
66
However, after
extensive records examination and questioning of the technician, his supervisor
and others at Hamilton Standard, it was not possible to determine whether, or to
what extent, these factors contributed to the technician’s failure to properly restore
the blended area to its original surface finish.
Although the PS960A blend repair is no longer being used, Hamilton
Standard uses blending (sanding) in a variety of other propeller repair procedures.
In view of the potential for improperly performed blend repairs to mask existing
corrosion and cracks, the Safety Board believes that the FAA should require
Hamilton Standard to review and evaluate the adequacy of its tools, training and
procedures for performing propeller blend repairs, and ensure that those blend
repairs are being performed properly.
The technician who performed the blend repair on the accident blade
was neither an FAA-certificated mechanic nor, as an employee of a 14 CFR Part
145 repair station, was he required to be certificated. The technician stated that he
was permitted to sign off the work that he was qualified to perform. The shop
traveler form, which listed the requirement for the 63 RMS surface finish, showed
that the technician had signed off that he had accomplished the taper bore blend
repair. However, except for the subsequent ultrasonic inspection that was to
determine if the rejectable indication had been eliminated, there were no other
inspections of the accident blade. 14 CFR Part 65.87 states, in part, that a
certificated mechanic may return a propeller blade to service after he has repaired
and inspected, or supervised the repair and inspection of, that part. 14 CFR Part
145.45 specifies that a repair station must have an inspection system with qualified
personnel to determine the airworthiness of the parts being altered or maintained.
Therefore, the Safety Board believes that the FAA should review the need to
require inspection (“buy back”) after the completion of work that is performed by
65
He received 90 hours of on-the-job training from the engineering manager, whose
primary duties did not relate to training.
66
His work records indicate that during May and June of 1994, he worked between 8 and
26 hours of overtime each week.

59
uncertificated mechanics at Part 145 repair stations to ensure the satisfactory
completion of the assigned tasks.
2.2.2 Adequacy of Hamilton Standard Procedures for Detecting
Corrosion
2.2.2.1 Borescope Inspection
From an engineering and airworthiness perspective, the
appropriateness of the PS960A blending repair procedure rests on the premise that
there are no cracks or corrosion in the area being blended. However the
investigation revealed that during the initial stages of inspecting and repairing the
490 returned blades, although great emphasis was given to the development and
implementation of the PS960A repair procedure, little consideration was given to
the adequacy of the procedures being used to detect cracks and corrosion.
The inside of the taper bore is less than 1 inch in diameter. Visual
inspection of the interior of the taper bores was accomplished using a borescope
that did not provide low angle (indirect) illumination, which would have
highlighted changes in the surface depth, such as those related to subtle corrosion.
Instead, the borescope inspection used direct illumination, which produced a glare
and made visual detection of corrosion difficult. Using this direct-light borescope
resulted in a view of the taper bore interior that would reveal gross discoloration
or widespread corrosion but that would not readily reveal minor corrosion or small
cracks. In addition, the glare could have caused eye strain over time. For these
reasons, the probability of detection of cracks or corrosion decreased over the
course of a work period.
Corrosion in earlier blade failures, such as the Inter-Canadien
accident, was widespread and deep, and most likely would have been readily
detected by a visual inspection, even with a direct light source. However, the
corrosion involved in the accident blade was shallow, diffused and more difficult
to recognize as corrosion. In fact, the ultrasonic inspection performed prior to the
PS960A repair directed the technician to the location of the corrosion pits, but
upon visual examination of that area, the technician reported that he did not see
“visible faults.” Safety Board investigators, and other experts who have examined
the accident blade, agreed that inspection with a direct light source might not have
adequately highlighted the corrosion and cracking that had already developed.

60
(An FPI inspection technique was later introduced, using a black light borescope,
which would more readily reveal cracks and corrosion.)
In addition, at the time the accident blade was inspected, the
movement of the borescope into the taper bore hole and circumferentially around
the hole was controlled by hand, and there was no procedure to ensure that the
entire inner surface was inspected. Therefore, it is possible that the visual
inspection of some blades, possibly even the accident blade, might have been
incomplete. (Mechanical assistance to control the location of the borescope was
introduced later.)
Therefore, the Safety Board concludes that the borescope inspection
procedure developed and used by Hamilton Standard in June 1994 to inspect
returned blades that had rejectable ultrasonic indications for evidence of cracks,
pits, and corrosion was inadequate and ineffective.
2.2.2.2 Technician Training and Supervision
Investigators were informed that technicians at Hamilton Standard,
Rock Hill, normally received approximately 250 hours of general training before
they began working on propellers being returned to airworthy condition. Because
the technician who accomplished the taper bore repair to the accident blade
transferred from another shop area (fiberglass and nickel sheath replacement and
repair), he received his 250 hours of training in that area. After transferring to the
taper bore area, he received about 90 hours of on-the-job training (OJT) for taper
bore repair. However, that training was deficient because he was not provided a
photograph or model of what corrosion or cracking looked like inside a taper bore.
It was not until the fall of 1994 that such material was provided (in the form of a
photographic example of corrosion and an instructional video), as part of a group
of inspection improvements covered in a Component Maintenance Manual
revision and Service Bulletin 14RF-9-61-70A. Compliance with that Service
Bulletin was not required until March 23, 1995, with AD-95-05-03.
In the absence of a photograph or model of different types of potential
corrosion, the technician might have expected the type of gross corrosion or
cracking more familiar to his automotive background and, thus, failed to realize
the significance of corrosion with a more subtle appearance, such as that present in
the accident blade. This problem was most likely compounded by the poor
borescope inspection techniques discussed above. Further, technician training in

61
how to perform the taper bore repair procedure was provided by the Rock Hill
facility engineering manager, who had numerous additional responsibilities at the
time. Moreover, because the other inspectors were also recently hired and trained
and were relatively inexperienced in finding corrosion in the taper bore of
aluminum aircraft propellers, they were unable to provide guidance or help to each
other.
The Safety Board concludes that although the introductory technical
training to prepare the new, inexperienced workforce at Hamilton Standard’s Rock
Hill Customer Service Center may have been adequate, the specific training
initially given to technicians who inspected blades returned to Rock Hill as a
result of the on-wing ultrasonic inspections, including the accident blade, was not
adequate to ensure that they were proficient in the detection of taper bore
corrosion or associated cracks. (Hamilton Standard eventually improved its
training by providing photographs and an instructional video.)
2.2.2.3 Adequacy of Improvements to Inspection Procedures
The Safety Board is concerned that Hamilton Standard and the FAA
determined that repetitive ultrasonic inspections (per AD 95-05-03) could be
terminated by a one-time visual borescope inspection to detect corrosion or by a
previous PS960A repair, even though the probability of detection (POD
67
) for the
visual borescope method would be less than 100 percent. As a result of this
determination, when the ASA accident blade was visually inspected, repaired, and
marked with “PS960A” (which incorporated a borescope inspection of the taper
bore), the blade was exempt from further ultrasonic or visual inspections.
Hamilton Standard’s and FAA’s expectations for a visual inspection were
unrealistic, particularly when using hand-held borescopes with a direct light
source, and when the technician did not have explicit examples of what was a
rejectable visual condition.
In the months following the first two failures in March 1994,
Hamilton Standard identified inadequacies in the inspection process and generated
improvements to address these inadequacies. Specifically, Hamilton Standard
provided a photographic example of corrosion, a training video, a borescope feed
adapter, and a process upgrade to FPI. However, when these improvements in the
67
The probability of detection (POD) for a visual inspection is dependent upon many
variables including the flaw size, environment, ocular assistance devices, training and operator
experience and fatigue.

62
inspection methods were made, Hamilton Standard either did not recognize or was
not concerned that taper bore flaws, such as the crack in the ASA blade, might
have gone undetected during the previous inspection and repair process before the
improvements were made because Hamilton Standard did not implement
retroactive inspection of those blades that had been inspected previously and
returned to service under inspection standards and processes that were no longer
considered adequate.
Because the accident blade had been rejected once for an ultrasonic
indication caused by the crack that ultimately propagated to cause separation, it is
very likely that the existing crack would have been redetected if the accident blade
had been subjected to additional ultrasonic inspections (at the required 1,250 cycle
intervals, per AD 95-05-03) after it was returned to service following the Rock
Hill maintenance activities. If the accident blade had been subjected to the
recurrent on-wing ultrasonic inspections required by AD-95-05-03, it would have
received one inspection, and possibly a second, before the crack reached critical
size and the blade separated. Therefore, the Safety Board concludes that Hamilton
Standard’s failure to recommend, and the FAA’s failure to require, repetitive
ultrasonic inspections for all propellers (particularly those already inspected when
there were recognized shortcomings in the inspection process) contributed to the
accident because the crack in the accident blade would likely have been detected
in a recurrent ultrasonic inspection.
2.3 Effect of Blade Resonance
When Hamilton Standard attempted to model the growth of a taper
bore fatigue crack in the fall of 1995, the results of the initial fracture mechanics
analysis of the fracture of the Inter-Canadien (ATR-42) blade were consistent with
the initiation and propagation of the crack from the corrosion pits in that blade.
However, the analysis indicated that cracking should not have developed from the
smaller corrosion pits that were found at the origin area of the ASA blade and the
Nordeste blade (both from EMB 120 airplanes).
To more fully understand the ASA taper bore fracture mechanics,
Hamilton Standard then used a NASA-developed program called FASTRAN,
which addressed the magnitudes and numbers of stress cycles required for
corrosion pits to form cracks and for the cracks to propagate to critical size. Using
the measured flaw sizes from the accident blade and the two previous fractures,
the FASTRAN program was able to predict the stress cycles needed for the crack

63
in each of the blades, including the ASA blade, to propagate from the initial flaw
size to fracture. Hamilton Standard indicated to the Safety Board that for a
corrosion pit to initiate a crack, especially for small pit sizes, such as in the ASA
blade, a blade would have to have been subjected to a very high number of stress
cycles of the most severe type that the blade would normally encounter in routine
operations. Since a ground-air-ground (GAG) cycle
68
imparts severe stress to the
blade only once per flight, Hamilton Standard engineers believed that 2P
resonance (which occurs twice per revolution of the propeller) in adverse winds,
perhaps during a maintenance ground run, contributed to the initiation of the crack
from corrosion pitting and propagation of the crack while it was small. The
FASTRAN program calculated that for a crack the size of the ASA crack at the
time the blade was at Rock Hill (0.050 by 0.060 inch) to propagate to failure, an
average of 50 maximum level 2P stress cycles would have to be accumulated each
flight. This number of cycles could be accumulated in about 1.6 seconds of
operation at the rpm range associated with 2P resonance during ground operation
in adverse winds (quartering tailwinds).
69
Through independent testing using a corporate-owned EMB-120
airplane, Hamilton Standard confirmed previous test results that the most severe
stress cycles were the GAG cycles, and the vibratory stresses encountered during
2P resonance (which are about the same magnitude as the GAG stresses) in
adverse winds during ground operations.
It should be noted that during the propeller ground tests conducted by
Hamilton Standard (where stress levels up to 18,000 psi were measured), the test
lasted for only 30 seconds. The 30-second interval might not have been of
sufficient duration, with the given test conditions, to produce maximum possible
stress. Additionally, the quartering tailwinds were generated by the propeller
wash of a small executive turbopropeller aircraft. It is possible that stress levels in
excess of 18,000 psi could be attained if the propeller were allowed to remain in
the resonant condition in excess of 30 seconds or if the propeller was subjected to
natural quartering tailwind conditions of higher velocity.
68
A GAG cycle included engine power application for takeoff, climb, cruise, descent and
reverse thrust after landing.
69
Ground operation in a tailwind or quartering tailwind causes the airplane to shake and
buffet, which hampers the mechanic’s ability to read instruments and perform any meaningful
tests.

64
The Safety Board noted that ASA’s operational procedures prohibited
single-engine taxi. Because single-engine taxi increases the potential for ground
operation in the resonant range, by requiring higher engine rpm to initiate and
continue movements, it might be expected that other operators of EMB-120
airplanes that allow single-engine ground operation would have a higher incidence
of cracks. That is, if a 2P resonant condition could be generated during normal
ground operations and could initiate and propagate a fatigue crack, it would be
more likely that cracking would occur on blades used by operators that allow
single engine operation on the ground. However, this did not occur.
It is also possible that a 2P resonant condition was generated during
some type of ground maintenance activity and that these stresses contributed to the
initiation and propagation of the crack. However, ground operation in a tailwind
or quartering tailwind is contrary to all standard maintenance practice and is
prohibited in the EMB-120 maintenance manual. The Safety Board could find no
documented evidence, and was not provided any information by Hamilton
Standard, Embraer, Pratt and Whitney of Canada, or the operator, that the
propeller was operated in a 2P resonant condition. Additionally, the EMB-120
cockpit was placarded, and there were cautions set forth in the airplane flight
manual and engine maintenance manual to avoid engine operation above 65
percent Np range in adverse wind conditions. Safety Board investigators had a
number of opportunities to observe whether there was compliance with these
limitations, and they did not observe noncompliance.
Although ground operation in a tailwind causes the airplane to shake,
the shaking is a result of disturbed airflow across the wings and fuselage and is not
damaging. However, under such conditions, an increase of the propeller rpm into
the resonant range would generate a reactionless vibratory mode in the propellers.
This would be undetectable, especially during crosswind-induced airframe buffet.
Such circumstances could arise at any time during ground operation in a strong
quartering tailwind, such as while operating in the vicinity of jet wash from a large
transport aircraft. With a population of more than 2,450 14RF-9 model blades in
service on EMB-120 airplanes throughout the world, there have probably been
many occasions when blades were operated in quartering tailwinds in excess of the
10 knots cautioned about in the flight manual and placards.
The Safety Board concludes that a combination of 2P resonance and
GAG cycle stresses initiated the crack from the corrosion pits in the ASA blade
and caused the crack to propagate to failure under normal operating conditions.

65
2.4 Adequacy of Vibration Testing
Hamilton Standard’s 1983 and 1985 certification stress surveys were
conducted using one instrumented blade with a second instrumented blade as a
backup. None of the tests were conducted using blades that had previously been
used in service. The 1995 stress survey conducted as a consequence of this
accident included three instrumented blades that had approximately 12,000 service
hours. The 1995 stress survey revealed a small but important difference from the
1983 and 1985 certification tests. Although no new high stress conditions were
discovered, a small downward shift in the first flat-wise natural frequency was
detected. This downward shift was attributed to normal wear and mass properties
in the propeller blade from normal operation.
On April 19, 1993, the Safety Board investigated a propeller in-flight
separation on an MU-2B-60 in Zwingle, Iowa. As indicated in the accident report,
the Safety Board discovered that during certification testing of the Hartzell HC-B4
propeller on the MU-2B airplane, a reactionless mode of vibration was identified
with the peak stress occurring at a propeller speed of 1,079 rpm. As a result, the
propeller was prohibited from continuous operation on the ground below 1,145
rpm. The Safety Board did not find evidence that the test was repeated using
propeller blades altered to conform to the minimum dimensions specified in the
repair limit criteria contained in the Hartzell HC-B4 propeller maintenance
manual.
The FAA recommends in Advisory Circular (AC) 20-66, Vibration
Evaluation of Aircraft Propellers, in the chapter on vibration measurement
programs, that propeller diameters should be tested at various lengths throughout
the diameter range, to include the maximum and minimum diameters, and the
cutoff repair limit. Although it is not explained in AC 20-66, testing a propeller
blade at its cutoff repair limit is conducted presumably to ensure that the decrease
in blade length does not alter the natural frequency to the extent that a resonant
vibration condition could be entered while operating within the normal rpm range.
AC 20-66 considers the expected loss of mass of a metal propeller blade following
blend repair; however, the AC does not consider the expected mass gain with age
of a composite propeller blade. Composite blades may gain mass with age with
the addition of layers of paint, introduction of moisture, and patch repairs.
A review of AC 20-66, which includes a detailed discussion of the
propeller vibratory phenomenon, does not explain that a propeller blade’s natural

66
vibratory response varies with varying conditions (i.e. mass gain, mass loss,
variations in airfoil shape, etc.) and that adequate margin from a potentially
coincident excitation frequency should be maintained. Consequently, the Safety
Board concludes that the AC does not provide guidelines for adequate margin
between a propeller blade’s natural frequencies and its potentially coincident
excitation frequencies over the life of the blade.
Therefore, the Safety Board believes that the FAA should revise AC
20-66 to include the vibratory testing of composite propeller blades that have been
previously operated for a substantial number of service hours, and composite
blades that have been altered to the limits set forth in FAA-approved repair
manuals to determine the expected effects of age on propeller vibration and
provide guidelines for rpm margin between a propeller blade’s natural frequencies
and the excitation frequencies associated with propeller operation.
2.5 Effect of Blade Failure and Analysis of Terminating Action
The forward half of the fractured front inlet case, found along the
wreckage path, was attached to the reduction gear box (RGB) of the left engine.
The RGB case was also fractured, empty of oil, and some internal gearbox
components were missing. The in-flight fracture of the RGB case most likely
resulted in the loss of the gearbox components and the venting liquid reportedly
seen by the passengers.
Damage to the forward engine mounts and the front frame of the left
engine nacelle indicated that the propeller RGB first separated upward at the
inboard mount location, followed by the aft and outboard failure at the outboard
mount location. Failure of the engine mounts were the result of overload stresses.
The imbalance loads associated with the separated blade on the
accident airplane apparently exceeded the design strength of the RGB attachment
points. In this instance, it appears that the RGB was retained on the airplane in an
outboard displaced position, as observed by the passengers, from the time of
propeller blade separation until the beginning of the initial ground impact.
Embraer’s postcertification (September 1984) testing determined that
the nacelle would not withstand a mid-blade or full-blade segment loss. To date,
there have been four blade separations--three from fatigue cracks that initiated in
the taper bore. The first blade separation (Inter-Canadien) resulted in RGB and

67
propeller separation, and the assembly fell to earth. During the second blade
separation (Nordeste), the RGB and propeller assembly remained in place. During
the third separation (the Luxair accident), in which a fracture occurred in the blade
shank area, the RGB and propeller assembly again fell from the airplane. During
the fourth blade failure (this accident), the RGB rotated out of position, and
resulted in degraded aerodynamic performance and a fatal accident.
Although in two of the occurrences, the RGB and propeller fell clear
and did not seriously compromise the airplane or degrade its performance, all of
the occurrences clearly placed the airplane and its occupants at potential serious
risk. On four occasions, stresses on blades with flaws (corrosion pits or
mechanical damage) have produced a blade separation even though the propeller
was certificated based on the assumption of an unlimited life. Because the current
regulations do not require that an airframe survive if a blade breaks, and because
Embraer has determined that the EMB-120 cannot survive the loss of a mid-blade
or full-blade segment, minimizing the possibility of a propeller blade separation is
imperative. To prevent future failures, it is essential that stress risers in the form
of corrosion or mechanical damage are not permitted to occur on any propeller
blade.
The Safety Board concurs that the taper bore repair procedure
specified in the March 1996 Service Bulletins (and required by ADs) should have
restored the surface of the taper bore of all existing propellers to a nearly new
condition. Also, because Hamilton Standard has prohibited the use of the
mechanical lead-removal tools during routine blade balancing, the likelihood of
future inadvertent mechanical damage has been greatly reduced.
However, while the terminating taper bore repair procedure should
detect and eliminate any chlorine-induced corrosion or mechanical damage, the
Safety Board is concerned that exposure to small amounts of moisture or other
atmospheric elements during routine maintenance, the recurring inspection
procedure set forth in the CMM, periods of low utilization, or long-term storage
may allow atmospheric-induced corrosion to begin in the taper bore. The Safety
Board is aware of reports of corrosion and cracking in the taper bores of P-3 and
C-130 propellers associated with long-term storage. Because of this, the Safety
Board concludes that despite all the actions taken by Hamilton Standard and the
FAA to date, there is a continuing potential for corrosion to develop in taper bores
of the affected Hamilton Standard propeller blades. Therefore, the Safety Board
believes that the FAA should require that Hamilton Standard consider long-term,

68
atmospheric-induced corrosion effects and amend the CMM inspection procedure
to reflect an appropriate interval that will detect any corrosion within the taper
bore.
2.6 FAA Oversight
2.6.1 Role of Designated Engineering Representative and FAA
Certifying Engineer
As discussed in Section 1.16.3, Hamilton Standard extended the
applicability of the PS960A blending repair beyond its original purpose (blending
of mechanical damage) to also allow blending of shotpeen impressions to remove
ultrasonic indications without informing or involving its DER or the FAA
(through its Certifying Engineer in the Engine and Propeller Directorate).
Hamilton Standard was aware that the FAA Certifying Engineer had earlier
determined that repair procedures to the taper bore would require direct FAA
approval. Consistent with this determination, both the DER (who served as a
liaison to the FAA) and the Certifying Engineer were involved in developing the
initial ultrasonic inspection procedures later set forth in ASB 14RF-0-61-A66 and
the PS960A repair procedure. If Hamilton Standard had consulted with the DER
and the FAA about the proposed extension and the reason for it (ultrasonic
indications in blades without any visible damage), it might have prompted the
FAA to reconsider whether the inspection and repair processes then being used
were adequate to identify blades at risk for cracking.
Even though the extension of PS960A to allow blending of shotpeen
impressions might have been approved by the FAA, if approval had been
requested, Hamilton Standard’s failure to seek such approval nonetheless played a
role in creating the confusion that led to the misapplication of PS960A. The
FAA’s approval would likely have been documented in a fashion similar to its
approval of PS960 and PS960A, clearly specifying the limits of the approved
extension. In contrast, as discussed in Section 2.2.1.1, Hamilton Standard’s
attempt to internally document the extension was confusing and led to the
misapplication of the repair to unshotpeened taper bores with unexplained
ultrasonic indications.
Accordingly, the Safety Board concludes that Hamilton Standard’s
failure to seek FAA approval of the extension of PS960A blending repair hindered
the FAA’s ability to oversee Hamilton Standard’s handling of the taper bore crack

69
and corrosion problem, and led to an inadequate documentation of the extension
that caused confusion and misapplication of the repair. Although the DER stated
that this lapse in communication was atypical, the Safety Board is concerned--
especially in light of the inadequate manner in which Hamilton Standard
communicated the information to its managers and technicians--that it may
represent a deficiency in Hamilton Standard’s corporate communication.
Specifically, it suggests that Hamilton Standard placed insufficient emphasis on
proper communication of vital safety information. Accordingly, the Safety Board
believes that the FAA should require Hamilton Standard to review and, if
necessary, revise its policies and procedures regarding 1) internal communication
and documentation of engineering decisions, and 2) involvement of the DER and
FAA, and to ensure that there is proper communication, both internally and with
the FAA, regarding all significant engineering decisions.
2.7 Weather
The flight was operating in accordance with an IFR flight plan and
was climbing above overcast clouds at the initiation of the accident sequence. A
weather observation taken at CTJ, approximately 4 miles from the crash site,
reported an 800-foot overcast cloud ceiling just after the accident. However,
weather conditions appropriate for visual flight below the clouds were reported at
several airports near the accident site.
From the flightcrew’s requests to ATC for vectors to the airfield, it is
apparent that the cloud ceiling affected the flightcrew’s ability to visually acquire
a suitable landing site during the descent for a forced landing. In the latter portion
of the descent, after descending below the overcast cloud ceiling, the airplane’s
height above the terrain would have limited the view of the flightcrew to just the
immediate area. The airplane impacted the ground in a left-wing-down attitude,
probably because the flightcrew was attempting to complete a turn to properly
align themselves for the forced landing. If the overcast cloud ceiling had been
higher, the crew would have had more time to align the airplane and level the
wings before the impact. Consequently, the Safety Board concludes that the cloud
ceiling precluded the flightcrew from being able to see the ground and thus to
make a more successful forced landing, a situation that contributed to the severity
of the accident.

70
2.8 Air Traffic Control Services
All FAA ATC personnel were trained, certificated, and qualified for
their duties. There were no apparent physiological or behavioral impairments or
disabilities that would have detracted from their ability to provide the expected air
traffic services. Following the declaration of the emergency by the flightcrew and
their continuing description of their difficulties, the controllers provided
appropriate assistance to the crew.
The Atlanta Center controller did not issue the CTJ AWOS
frequency. Although FAA ATC procedures
70
require that “both center and
approach controllers shall provide current approach information to aircraft
destined to airports for which they provide approach control services,” in this case,
the Atlanta Center controller was not responsible for approaches into CTJ and was
not in the best position to have provided this information.
The closest weather report immediately available to the approach
controller was the ATL Airport observation, the flight’s departure point. There
was no controller assigned to the “assist” position and although the manager and
supervisor were nearby, they became occupied with coordinating and monitoring
activities supporting the flight and did not attempt to retrieve the CTJ AWOS
weather information by telephone. During the 90 seconds that the approach
controller was in radio communication with the flight, the controller issued a
vector toward the runway, the localizer frequency, confirmed the flight was in
visual conditions and issued a vector for the visual approach. Therefore, the
Safety Board concludes that, although the Atlanta approach controller did not
issue the AWOS frequency or provide weather information, the controller
performed higher priority tasks and, because the flight had to land at the nearest
airport regardless of the weather, the failure to provide the CTJ weather
information to the flightcrew was not a factor in this accident.
The Safety Board examined the performance of both the center and
the approach controllers in assisting the accident flight. Once the flightcrew
declared the emergency, Atlanta Center immediately issued instructions to permit
the flight to return to ATL. Because of the location of the aircraft within the
sector, the radar controller and manual assist controller coordinated with
70
FAA Order 7110.65, “Air Traffic Control,” Chapter 4, “IFR,” Section 7, “Arrival
Procedures,” paragraph 4-7-13, “Approach Information,” applies.

71
surrounding sectors; the center controller attempted to assist the accident
flightcrew by providing vectors and airport information. However, because of the
degraded flight performance of the aircraft, the flightcrew was not able to effect a
timely response to the controller’s instructions. When the flightcrew requested
information normally available from the approach controller, such as runway
heading and airport surface condition, the center controller instructed the
flightcrew to contact the approach control facility. FAA ATC procedures
71
state in
part, “If you are in communication with an aircraft in distress, handle the
emergency and coordinate and direct the activities of assisting facilities. Transfer
this responsibility to another facility only when you feel better handling of the
emergency will result.”
The flightcrew would have been able to advise the center controller
that they preferred to remain on the current frequency because of the emergency,
and the center controller may have been able to coordinate alternate procedures.
Also, in retrospect, the Atlanta Center controller could have made an earlier
handoff if he had been informed by the flightcrew of, or if he had perceived the
full extent of, the performance degradation to the accident airplane. However, the
Safety Board concludes that the timing of the handoff to Atlanta approach control
by the Atlanta Center controller was not a factor in the accident.
The Safety Board is concerned, however, about the failure of ATC
controllers to notify CFR services once the controllers were aware of the
emergency situation. At 1644:25, the flightcrew of ASE 529 notified the Atlanta
Center air traffic controllers that they had experienced an engine failure and
declared an emergency. Two minutes later, the flightcrew advised that they
needed to “land quick” and requested the controller to “roll the trucks and
everything for us.” The controller then advised the flightcrew that CTJ was the
closest airport and directed the aircraft to CTJ. Although ATC was aware of the
emergency situation and destination airport, ATC did not notify the fire and
emergency services covering CTJ, the Carroll County Fire Department, of the
incoming aircraft.
Atlanta Center should have immediately advised the appropriate CFR
service or instructed Atlanta approach of the pilot’s request so that they could have
made timely airport emergency services notification. The accident had already
71
FAA Order 7110.65, Chapter 10, “Emergencies,” Section 1, “General,” paragraph 10-1-
4, “Responsibility,” applies.

72
occurred when the Atlanta approach controller made the call to the Carroll County
Sheriff, and it had already been reported by a citizen on 911. The Safety Board
concludes that if the Atlanta Center had placed a call for emergency services as
soon as the pilot requested, which was 10 minutes before the accident, personnel
would have responded sooner, and the rescue efforts might have been more timely
and effective. Therefore, the Safety Board believes that the FAA should include
an article in the Air Traffic Bulletin and provide a mandatory formal briefing to all
air traffic controllers regarding the necessity and importance of notifying crash,
fire and rescue personnel upon a pilot’s request for emergency assistance. Ensure
that air route traffic control center (ARTCC) controllers are aware that such a
request may require them to notify local emergency personnel.
2.9 Survival Factors Aspects
The Safety Board commends the exemplary manner in which the
flight attendant briefed the passengers and handled the emergency. According to
passengers, immediately following the loss of the propeller blade, the flight
attendant checked with each passenger individually to make sure that they all
understood how to assume the brace position, and she yelled instructions to the
passengers up until the time of impact. After the crash, although she was seriously
injured, she continued to assist the passengers by moving them away from the
airplane and extinguishing flames on at least one passenger who was on fire.
2.9.1 Time Management During Emergencies
The Safety Board recognizes that the flightcrew in this accident was
attempting to control the aircraft. However, the Safety Board is concerned that the
flight attendant neither received nor sought information about the time remaining
to prepare the cabin or to brace for impact. The CVR transcript revealed that the
flightcrew informed her 7 minutes before impact that they had experienced an
engine failure, that they had declared an emergency for return to ATL, and that
they had advised her to brief the passengers. There were no further
communications to the flight attendant. Specifically, the flight attendant was
never told that the airplane would not be able to make ATL, and would instead be
making an off-airport crash landing. The flight attendant stated that while
preparing the cabin and passengers, she saw the tree tops from a cabin window.
She immediately returned to her jump seat and shouted her commands. A
passenger commented that the flight attendant was barely in the brace position
when the impact occurred.

73
The Safety Board is concerned that the flight attendant and the
flightcrew did not discuss a brace signal and the time available to prepare the
cabin, and that the flightcrew did not announce a brace command on the public
address system. Further, if the flight attendant had not had sufficient time to
fasten her safety belt and shoulder harness, she might have received more serious
or fatal injuries, and she might have been incapable of directing an evacuation.
The FAA has recognized that communication and coordination
between cockpit crewmembers and flight attendants continue to challenge air
carriers and the FAA. Advisory Circular (AC) 120-51B, “Crew Resource
Management Training,” suggests several methods of addressing this problem.
Paragraph 15, Evolving Concepts of CRM: Extending Training Beyond the
Cockpit, addresses specific subjects for joint training but does not specifically deal
with the communication of critical information during an emergency.
The Safety Board’s special investigation report on flight attendant
training
72
describes another accident on page 28:
The lead flight attendant in the DC-10 stated that she knew
emergency procedures required her to determine the amount of
time available to prepare the passengers and the cabin. However,
she chose not to ask the flightcrew about the time. Additionally,
the second item on the flight attendant checklist was “Determine
Time,” but none of the flight attendants followed this checklist
procedure.
Although the FAA issued Air Carrier Operations Bulletin 1-91-11 in
response to Safety Board Safety Recommendation A-90-173, which called for
inspectors to reiterate the importance of time management in the preparation of the
cabin in a planned emergency, the Safety Board concludes that this accident also
illustrates that critical information regarding time available to prepare the aircraft
for an emergency landing or impact is not being considered and communicated
among flight and cabin crewmembers. Therefore, to improve the interactions
between the cockpit and cabin crews, the Safety Board believes that the FAA
should amend AC 120-51B to include guidance regarding the communication of
72
See Special Investigation Report—“Flight Attendant Training and Performance During
Emergency Situations” (NTSB/SIR-92/02)

74
time management information among flight and cabin crewmembers during an
emergency.
2.9.2 Crash Axes
The captain and first officer were trapped in the cockpit by fire that
had ignited on the cabin side of the cockpit door. When the first officer found it
impossible to open his cockpit sliding window, he unsuccessfully attempted to
chop a hole in the hardened Plexiglas side window using the airplane crash ax. It
was apparently intended for use as a woodworking tool because it consisted of a
blade and nail puller attached to a wooden handle. Given the resilient composition
of the cockpit window material, it was difficult to make a hole in the window
panel; however, if the ax had been equipped with a pry bar rather than a nail
puller, the first officer might have been successful in wedging the pry bar between
the window and the track or frame and prying or forcing the window open.
Although regulations exist that require most passenger-carrying aircraft to be
equipped with a crash ax,
73
there is no FAA or other civil technical standard
regarding the design and use of crash axes. This accident demonstrates the
importance of an adequate crash ax design.
The crash ax carried aboard military transport aircraft conforms to a
special design. Large commercial transport airplanes manufactured in the United
States are equipped with crash axes of similar design. Additionally, firefighter
axes that have a wedge and pry bar tool features are in use by airport rescue and
fire fighting personnel and municipal emergency medical technicians. The Safety
Board concludes that there should be standards governing the design of crash axes
required to be carried aboard passenger-carrying aircraft. Therefore, the Safety
Board believes that the FAA should evaluate the necessary functions of the
aircraft crash ax, and provide a technical standard order or other specification for a
device that serves the functional requirements of such tools carried aboard aircraft.
73
See 14 CFR 91.513(e), 135.177(a)(2), and 121.309(e).

75
3. CONCLUSIONS
3.1 Findings
1. The flightcrew was trained, certificated and qualified to
conduct the flight, and the flight was conducted in accordance
with applicable Federal Aviation Regulations and company
requirements.
2. The flightcrew was in good health and held the proper FAA
medical certificates. There was no evidence that the
performance of any crewmember was impaired by alcohol,
drugs, or fatigue.
3. ASA maintained the airplane in accordance with applicable
Federal Aviation Regulations and company Operations
Specifications.
4. After the propeller blade separation, the combination of the
resulting loss of left engine thrust, increased drag from a
deformed engine nacelle and the three blades retained in the
propeller hub and added frontal drag from external sheet
metal damage degraded airplane performance preventing the
flightcrew from arresting the airplane’s descent or making
rapid changes in its direction of flight making a forced
landing necessary.
5. One of the four blades from the left engine propeller
separated in flight because a fatigue crack that originated
from multiple corrosion pits in the taper bore surface of the
blade spar propagated toward the outside of the blade, around
both sides of the taper bore, then reached critical size.
6. Because of the severely degraded aircraft performance
following the propeller blade separation, the flightcrew’s
actions were reasonable and appropriate during their attempts
to control and maneuver the airplane throughout the accident
sequence, and they were not a factor in this accident.

76
7. Hamilton Standard’s engineering decision to use the PS960A
blending repair to remove ultrasonic indications caused by a
shotpeened taper bore surface was technically reasonable.
8. The manner in which the unapproved extension of PS960A
was documented and communicated within Hamilton
Standard, and the lack of training on the extension, created
confusion and led to misapplication of the blending repair to
unshotpeened blades with unexplained ultrasonic indications,
allowing the accident blade to be placed back into service
with an existing crack.
9. The sanding marks left by the PS960A blending repair did not
contribute to the initiation of the fatigue crack in the accident
blade.
10. The failure to restore the taper bore surface to the original
surface finish, as required by PS960A, was a factor that
caused the reduction of the ultrasonic indication that allowed
the blade to pass the final ultrasonic inspection and to be
returned to service.
11. The borescope inspection procedure developed and used by
Hamilton Standard in June 1994 to inspect returned blades
that had rejectable ultrasonic indications for evidence of
cracks, pits, and corrosion was inadequate and ineffective.
12. The introductory technical training to prepare the new,
inexperienced workforce at Hamilton Standard’s Rock Hill
Customer Service Center might have been adequate; but the
training initially given to technicians, who inspected blades
that were returned to Rock Hill as a result of on-wing
ultrasonic inspections, including the accident blade, was
inadequate to ensure proficiency in the detection of taper bore
corrosion or associated cracks.
13. If Hamilton Standard had recommended, and the FAA had
required, repetitive ultrasonic inspections for all propellers
after shortcomings were recognized and improvements were

77
made in the inspection process (particularly those that had
already been inspected), the crack in the accident blade would
most likely have been detected.
14. A combination of 2P resonance and GAG cycle stresses
initiated the crack from the corrosion pits in the ASA blade
and caused the crack to propagate to failure under normal
operating conditions.
15. Advisory Circular AC 20-66 does not provide guidelines for
adequate margin between a propeller blade’s natural
frequencies and its potentially coincident excitation
frequencies over the life of the blade.
16. There is a potential for corrosion to develop in taper bores of
the affected Hamilton Standard propeller blades.
17. The cloud ceiling precluded the flightcrew from being able to
see the ground and thus to make a more successful forced
landing.
18. Hamilton Standard’s failure to seek FAA approval of the
extension of PS960A blending repair hindered the FAA’s
ability to oversee Hamilton Standard’s handling of the taper
bore crack and corrosion problem, and led to an inadequate
documentation of the extension that caused confusion and
misapplication of the repair.
19. The timing of the handoff to Atlanta approach control by the
Atlanta Center controller was not a factor in the accident.
20. Although the Atlanta approach controller did not issue the
AWOS frequency or provide weather information, the
controller performed higher priority tasks; and because the
flight had to land at the nearest airport regardless of the
weather, the failure to provide the CTJ weather information to
the flightcrew was not a factor in this accident.

78
21. If the Atlanta Center had placed a call for emergency services
as soon as the pilot requested, which was 10 minutes before
the accident, personnel would have responded sooner, and the
rescue efforts might have been more timely and therefore
more effective.
22. This accident illustrates that critical information regarding
time available to prepare the aircraft for an emergency
landing or impact is not being considered and communicated
among flight and cabin crewmembers.
23. There should be standards governing the design of crash axes
required to be carried aboard passenger-carrying aircraft.

79
3.2 Probable Cause
The National Transportation Safety Board determines that the
probable cause of this accident was the in-flight fatigue fracture and separation of
a propeller blade resulting in distortion of the left engine nacelle, causing
excessive drag, loss of wing lift, and reduced directional control of the airplane.
The fracture was caused by a fatigue crack from multiple corrosion pits that were
not discovered by Hamilton Standard because of inadequate and ineffective
corporate inspection and repair techniques, training, documentation, and
communications.
Contributing to the accident was Hamilton Standard’s and FAA’s
failure to require recurrent on-wing ultrasonic inspections for the affected
propellers.
Contributing to the severity of the accident was the overcast cloud
ceiling at the accident site.

80
4. RECOMMENDATIONS
As a result of the investigation of this accident, the National
Transportation Safety Board makes the following recommendations:
--to the Federal Aviation Administration:
Require Hamilton Standard to review and evaluate the adequacy of
its tools, training, and procedures for performing propeller blend
repairs, and ensure that those blend repairs are being performed
properly. (A-96-142)
Review the need to require inspection (“buy back”) after the
completion of work that is performed by uncertificated mechanics
at Part 145 repair stations to ensure the satisfactory completion of
the assigned tasks. (A-96-143)
Revise Advisory Circular 20-66 to include the vibratory testing of
composite propeller blades that have been previously operated for
a substantial number of service hours, and composite blades that
have been altered to the limits set forth in FAA-approved repair
manuals to determine the expected effects of age on propeller
vibration and provide guidelines for rpm margin between a
propeller blade’s natural frequencies and the excitation
frequencies associated with propeller operation. (A-96-144)
Require that Hamilton Standard consider long-term, atmospheric-
induced corrosion effects and amend the Component Maintenance
Manual (CMM) inspection procedure to reflect an appropriate
interval that will detect any corrosion within the taper bore. (A-
96-145)
Require Hamilton Standard to review and, if necessary, revise its
policies and procedures regarding 1) internal communication and
documentation of engineering decisions, and 2) involvement of the
Designated Engineering Representative (DER) and FAA, and to
ensure that there is proper communication, both internally and
with the FAA, regarding all significant engineering decisions. (A-
96-146)
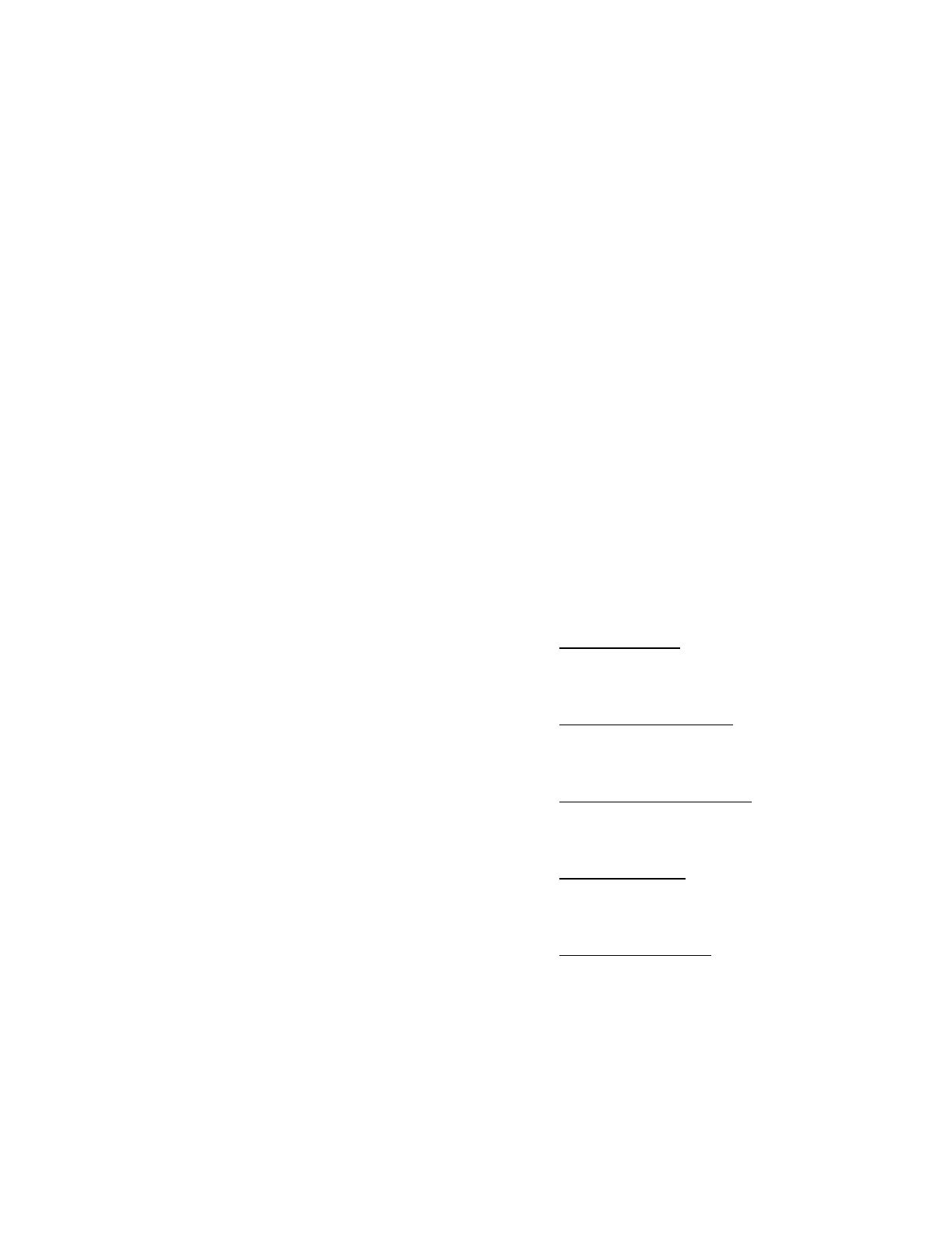
81
Include an article in the Air Traffic Bulletin and provide a
mandatory formal briefing to all air traffic controllers regarding
the necessity and importance of notifying crash, fire and rescue
personnel upon a pilot’s request for emergency assistance. Ensure
that air route traffic control center (ARTCC) controllers are aware
that such a request may require them to notify local emergency
personnel. (A-96-147)
Amend Advisory Circular 120-51B (Crew Resource Management
Training) to include guidance regarding the communication of
time management information among flight and cabin
crewmembers during an emergency. (A-96-148)
Evaluate the necessary functions of the aircraft crash ax, and
provide a technical standard order or other specification for a
device that serves the functional requirements of such tools carried
aboard aircraft. (A-96-149)
BY THE NATIONAL TRANSPORTATION SAFETY BOARD
James E. Hall
Chairman
Robert T. Francis II
Vice Chairman
John Hammerschmidt
Member
John J. Goglia
Member
George W. Black
Member
November 26, 1996

this page intentionally left blank

83
5. APPENDIXES
APPENDIX A
INVESTIGATION AND HEARING
1. Investigation
The Safety Board was notified of the accident by the FAA
Communication Center about 1330 on August 21, 1995. An investigator was
immediately dispatched to the crash site from the Southeast Field Office in
Atlanta, and a full go-team was sent from Safety Board Headquarters in
Washington, D.C. The following investigative groups were formed: Operations,
Structures, Systems, Powerplants, Maintenance Records, Air Traffic Control,
Weather, Aircraft Performance, Survival Factors, Cockpit Voice Recorder, and
Flight Data Recorder. Member John Hammerschmidt accompanied the team to
Carrollton, Georgia. A Metallurgy Group was later formed at the Safety Board’s
Materials Laboratory to study evidence of the failed propeller.
In accordance with the provisions of the International Civil Aviation
Organization’s International Standards and Recommended Practices, Annex 13,
Aircraft Accident and Incident Investigation, the Center for the Investigation and
Prevention of Accidents, Brazil, (state of manufacture of the airplane) and the
Transportation Safety Board of Canada, (state of manufacture of the engines) were
notified of the accident, and each state sent an Accredited Representative, with
advisers to participate in the investigation. A draft of the final accident report was
provided to each Accredited Representative for comment. Their comments have
been incorporated into the final report.
Parties to the investigation included the Federal Aviation
Administration, Atlantic Southeast Airlines, Empresa Brasileira de Aeronautica S.
A. (Embraer Aircraft Corporation), the Pratt and Whitney, Canada, Division of
United Technologies Corporation, the Hamilton Standard Division of United
Technologies Corporation, the Air Line Pilots Association, the Association of
Flight Attendants, and the National Air Traffic Controller’s Association.
2. Public Hearing
No public hearing was conducted for this investigation.

84
APPENDIX B
COCKPIT VOICE RECORDER TRANSCRIPT
LEGEND
HOT
Crewmember hot microphone voice or sound source
HOT-M
Aircraft mechanical voice heard on all channels
RDO
Radio transmission from accident aircraft
CAM
Cockpit area microphone voice or sound source
INT
Transmissions over aircraft interphone system
TWRA
Radio transmission from Atlanta control tower
ATLD
Radio transmission from Atlanta departure control
CTR
Radio transmission from Atlanta center
ATLA
Radio transmission from Atlanta approach control
UNK
Radio transmission received from unidentified aircraft
PA
Transmission made over aircraft public address system
-B
Sounds heard through both pilot’s hot microphone systems
-1
Voice identified as Pilot-in-Command (PIC)
-2
Voice identified as Co-Pilot
-3
Voice identified as female flight attendant
-?
Voice unidentified
*
Unintelligible word
@
Non pertinent word
#
Expletive
%
Break in continuity
( )
Questionable insertion
[ ]
Editorial insertion
....
Pause
Note: Times are expressed in eastern daylight time (EDT).
Times shown in brackets { } are computer reference times measured from the beginning of the recording.

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
START of RECORDING
START of TRANSCRIPT
1222:39 {00:22}
TWRA
AC five twenty nine, turn left heading zero six zero runway eight
right. cleared for takeoff.
1222:45 {00:28}
RDO-2
zero six zero eight right, cleared for takeoff, AC five twenty
nine.
1222:48 {00:31}
HOT-1
takeoff check, below the line, I got your lights.
1222:52 {00:35}
HOT-2
condition levers? max.
1222:52 {00:35}
HOT-2
bleeds and packs? standard.
1222:53 {00:36}
HOT-2
external lights? on.
1222:54 {00:37}
HOT-2
below the line's complete.
1222:55 {00:38}
HOT-1
alright.
1223:00 {00:43}
CAM
[sound of increase in rpm similar to takeoff power being applied]
85

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1223:19 {01:02}
HOT-2
power set, auto-feather's armed, panel's clear, airspeed’s alive.
1223:24 {01:07}
HOT-2
V 1.
1223:25 {01:08}
HOT-2
V r.
1223:29 {01:12}
HOT-2
pos' rate.
1223:30 {01:13}
HOT-1
gear up.
1223:37 {01:20}
HOT-1
wipers off.
1223:46 {01:29}
TWRA
AC five twenty nine, contact departure. fly heading zero six
zero now. we'll see ya.
1223:49 {01:32}
RDO-2
zero six zero switching, see ya.
1223:51 {01:34}
HOT-B
[single beep similar to radio frequency change]
1224:00 {01:43}
RDO-2
Atlanta departure, AC five twenty nine's with you, leaving one
point eight for four, heading sixty.
1224:07 {01:50}
ATLD
AC five twenty nine, Atlanta departure roger, radar contact.
maintain one zero thousand.
1224:13 {01:56}
RDO-2
one zero thousand, AC five twenty nine.
86

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1224:17 {02:00}
HOT-2
**.
1224:17 {02:00}
HOT-1
ten.
1224:31 {02:14}
HOT-1
climb power, * takeoff.
1225:04 {02:47}
HOT-2
gear's up, flaps are up, pressure's checked, climb power set, bleeds
and packs auto, APU's off, auto-feather off, flight attendant notified
****.
1225:11 {02:54}
HOT-1
thank you.
1225:26 {03:09}
RDO-2
five twenty nine's up, at twenty four.
1225:27 {03:10}
HOT-B
[single beep similar to radio frequency change]
1225:41 {03:24}
HOT-1
is this the s*, this the ## that uh, kept doin' that to us? on takeoff?
1225:54 {03:37}
HOT-2
yeah this is the one, that these were loose.
1225:57 {03:40}
ATLD
AC five twenty nine turn left heading three six zero.
1225:59 {03:42}
RDO-2
left three sixty, AC five twenty nine.
87

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1226:03 {03:46}
HOT-1
no he didn't, didn't know whether, the high pack was causing the
problem or.
1227:29 {05:12}
ATLD
AC five twenty nine turn left heading two seven zero.
1227:33 {05:16}
RDO-2
left * two seven zero, AC five twenty nine.
1227:41 {05:24}
HOT-1
let's look at the radar there.
1227:44 {05:27}
HOT-2
just a bunch of scattered stuff *.
1228:37 {06:20}
ATLD
AC five twenty nine, maintain one one thousand.
1228:40 {06:23}
RDO-2
one one thousand, AC five twenty nine.
1228:42 {06:25}
HOT-2
eleven.
1228:43 {06:26}
HOT-1
*.
1228:59 {06:42}
HOT-1
stick it back in auto and see if it'll, work again.
1229:35 {07:18}
HOT-2
one more. (feels) alright.
1230:05 {07:48}
CAM
[sound of three beeps similar to altitude alert signal]
88
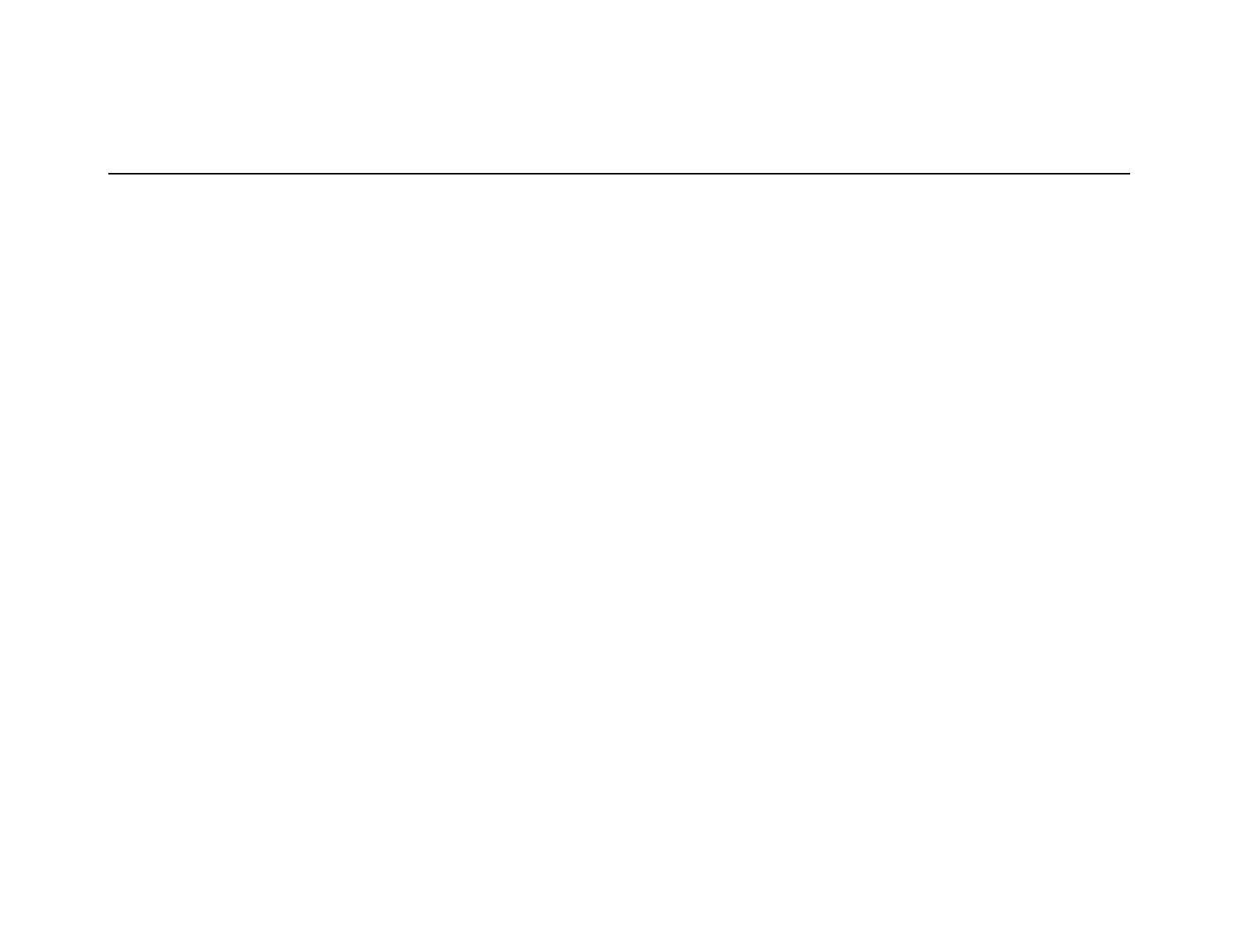
INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1231:33 {09:16}
ATLD
AC five twenty nine, turn left heading two five zero.
1231:35 {09:18}
RDO-2
two five zero, AC five twenty nine.
1232:02 {09:45}
ATLD
AC five twenty nine, climb and maintain one two thousand.
1232:06 {09:49}
RDO-2
one two thousand, AC five twenty nine.
1232:08 {09:51}
HOT-2
twelve.
1232:09 {09:52}
HOT-1
tell Robin it just be a couple of minutes it'll smooth out.
1232:18 {10:01}
CAM
[sound of two chimes similar to flight attendant call chime]
1232:19 {10:02}
INT-3
hello.
1232:20 {10:03}
INT-2
hey Robin.
1232:21 {10:04}
INT-3
hi.
1232:22 {10:05}
INT-2
it'll be a just a couple more minutes like this, it'll smooth out.
1232:24 {10:07}
INT-3
uuh, couple more minutes and then I can get up?
89

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1232:25 {10:08}
INT-2
yes ma'am.
1232:26 {10:09}
INT-3
alright, thank you.
1232:27 {10:10}
INT-2
see ya.
1232:40 {10:23}
HOT-2
four more.
1232:41 {10:24}
HOT-B
[three beeps similar to altitude alert signal]
1234:52 {12:35}
ATLD
AC five twenty nine, climb and maintain one three thousand.
1234:55 {12:38}
RDO-2
one three thousand, AC five twenty nine.
1234:57 {12:40}
HOT-1
thirteen.
1235:01 {12:44}
HOT-1
props ninety.
1235:02 {12:45}
HOT-?
***.
1235:07 {12:50}
HOT-1
[mechanical vibrating sound starts similar to boom microphone vi-
brating against cockpit surface]
1235:15 {12:58}
CAM
[sound similar to propellers decreasing in RPM]
90

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1235:31 {13:14}
HOT-B
[sound of three beeps similar to altitude alert]
1235:34 {13:17}
CAM-2
four more.
1235:42 {13:25}
CAM-1
** lights out *****.
1235:54 {13:37}
PA-2
ladies and gentlemen, good afternoon, welcome aboard Atlantic
Southeast Airlines flight seventy five twenty nine, service to Gulfport.
we're passing through thirteen thousand feet, captain has turned off
the fasten seat belt sign. you are free to move about the cabin as
you wish. however if you're in your seats, we ask you do so with your
belts fastened loosely around you, just in case we encounter any tur-
bulence enroute. Gulfport on the hour is calling for partly cloudy
skies, temperature of eighty degrees, and winds ten miles an hour
out of the northeast. there's anything we can do to make your flight
more enjoyable, please do not hesitate to call upon us. and thank
you for flying with ASA.
1235:58 {13:41}
ATLD
AC five twenty nine maintain one four thousand. contact At-
lanta center on one three four point niner five.
1236:05 {13:48}
RDO-1
one three four ninety five and fourteen thousand, AC uh, five
twenty nine.
1236:10 {13:53}
ATLD
good day sir, it's thirty four ninety five.
1236:13 {13:56}
RDO-1
thirty four ninety five.
91

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1236:20 {14:03}
HOT-B
[single beep similar to radio frequency change]
1236:25 {14:08}
RDO-1
center, AC five twenty nine is out of thirteen for fourteen.
1236:28 {14:11}
CTR
AC five twenty nine, Atlanta center roger. I'll have a higher al-
titude for you in just a moment.
1236:32 {14:15}
RDO-1
five twenty nine.
1236:35 {14:18}
CAM-2
I'm back.
1236:36 {14:19}
CAM-1
alright, up to fourteen and, talking to center, expectin' higher in a
while.
1236:42 {14:25}
CAM-2
OK.
1237:10 {14:53}
HOT-B
[sound of three beeps similar altitude alert signal]
1237:14 {14:57}
CAM-2
***.
1237:20 {15:03}
CAM-1
yeah, I guess. I'm not sure what the hell is this?
1237:32 {15:15}
CTR
AC five twenty nine, climb and maintain one five thousand.
1237:34 {15:17}
RDO-2
one five thousand, AC five twenty nine.
92
INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1237:38 {15:21}
CAM-2
*** fifteen ***.
1237:51 {15:34}
CAM-1
**** I can't get to.
1238:10 {15:53}
CAM-1
something underneath the #.
1238:17 {16:00}
CAM-2
it'll drive you nuts.
1238:18 {16:01}
CAM-1
it will drive you nuts.
1238:29 {16:12}
HOT-B
[three beeps similar to altitude alert]
1238:32 {16:15}
CAM-2
four more.
1239:24 {17:07}
CTR
AC five twenty nine, climb and maintain flight level one niner
zero.
1239:27 {17:10}
RDO-2
one niner zero, AC five twenty nine.
1239:30 {17:13}
CAM
[single beep similar to altitude alert]
1241:32 {19:15}
CAM-1
**long* duct tape ** around here *****.
1241:57 {19:40}
CTR
AC five twenty nine, climb and maintain flight level two zero
zero.
93

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1242:01 {19:44}
RDO-2
two zero zero, AC five twenty nine.
1242:04 {19:47}
CAM-2
twenty.
1242:40 {20:23}
CTR
AC five twenty nine, climb and maintain flight level two four
zero.
1242:44 {20:27}
RDO-2
two four zero, AC five twenty nine.
1242:46 {20:29}
CAM
[sound similar to dialing altitude alerter]
1242:50 {20:33}
CAM-2
twenty four.
1242:51 {20:34}
CAM-1
twenty four.
1243:25 {21:08}
CAM
[sound of several thuds]
1243:26 {21:09}
CAM-1
****.
1243:28 {21:11}
CAM
[three chimes similar master warning] auto-pilot, engine control, oil
[and continues to repeat]
1243:29 {21:12}
CAM-?
*.
1243:32 {21:15}
CAM-2
pack off.
94

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1243:34 {21:17}
CAM-1
*.
1243:38 {21:21}
CAM-1
we got a left engine out. left power lever. flight idle.
1243:45 {21:28}
CAM
[shaking sound starts and continues for thirty three seconds]
1243:46 {21:29}
CAM-1
left condition lever. left condition lever.
1243:48 {21:31}
CAM-2
yeah.
1243:49 {21:32}
CAM-1
feather.
1243:51 {21:34}
HOT-B
[series of rapid beeps for one second similar to engine fire warning]
1243:54 {21:37}
CAM-1
yeah we're feathered. left condition lever, fuel shut-off.
1243:59 {21:42}
CAM-1
I need some help here.
1244:02 {21:45}
CAM
[mechanical voice messages for engine control and oil cease.
chimes and auto-pilot warning continues]
1244:03 {21:46}
CAM-2
OK.
1244:03 {21:46}
CAM-1
I need some help on this.
95

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1244:05 {21:48}
CAM-?
(you said it's) feathered?
1244:06 {21:49}
CAM-1
uh,
1244:07 {21:50}
CAM-2
it did feather.
1244:07 {21:50}
CAM-1
it's feathered.
1244:09 {21:52}
CAM-2
OK.
1244:09 {21:52}
CAM
[master warning chimes and voice warning continues]
1244:10 {21:53}
CAM-1
what the hell's going on with this thing.
1244:13 {21:56}
CAM-2
I don't know... got this detector inop.
1244:16 {21:59}
CAM-1
OK ***.
1244:18 {22:01}
CAM-?
OK, let's put our head sets on.
1244:20 {22:03}
CAM-1
I can't hold this thing..
1244:23 {22:06}
CAM-1
help me hold it.
96

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1244:24 {22:07}
HOT-2
OK.
1244:26 {22:09}
CAM-1
alright comin' on headset.
1244:26 {22:09}
RDO-2
Atlanta center. AC five twenty nine, declaring an emergency.
we've had an engine failure. we're out of fourteen two at this
time.
1244:31 {22:14}
CTR
AC five twenty nine, roger, left turn direct Atlanta.
1244:33 {22:16}
HOT-1
# damn.
1244:34 {22:17}
RDO-2
left turn direct Atlanta, AC five twenty nine.
1244:36 {22:19}
HOT-?
[sound of heavy breathing]
1244:41 {22:24}
HOT-?
** back **.
1244:57 {22:40}
HOT-?
[sound of squeal]
1245:01 {22:44}
CAM
[tone similar to master caution cancel button being activated. all
warnings cease]
1245:03 {22:46}
HOT-1
alright turn your speaker off. oh, we got it. its.
1245:07 {22:50}
HOT-1
I pulled the power back.
97

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1245:10 {22:53}
CTR
AC five twenty nine, say altitude descending to.
1245:12 {22:55}
RDO-2
we're out of eleven six at this time. AC five twenty nine.
1245:17 {23:00}
HOT-1
alright, it's, it's getting more controllable here ... the engine ..... let's
watch our speed.
1245:32 {23:15}
HOT-1
alright, we're trimmed completely here.
1245:38 {23:21}
HOT-2
I'll tell Robin what's goin' on.
1245:39 {23:22}
HOT-1
yeh.
1245:44 {23:27}
HOT-B
[sound of two chimes similar to cabin call button being activated]
1245:45 {23:28}
INT-3
yes sir.
1245:46 {23:29}
INT-2
OK, we had an engine failure Robin. we declared an emergency,
we're diverting back into Atlanta. go ahead and uh, brief the passen-
gers. this will be an emergency landing back in.
1245:55 {23:38}
INT-3
alright. thank you.
1245:56 {23:39}
HOT-1
tell 'em we want ...
98

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1245:58 {23:41}
CTR
AC five twenty nine, say altitude leaving.
1246:01 {23:44}
RDO-2
AC five twenty nine's out of ten point three at this time.
1246:03 {23:46}
CTR
AC five twenty nine roger, can you level off or do you need to
keep descending?
1246:09 {23:52}
HOT-1
we ca.. we're gonna need to keep con.. descending. we need a air-
port quick.
1246:13 {23:56}
RDO-2
OK, we uh, we're going to need to keep descending. we need
an airport quick and uh, roll the trucks and everything for us.
1246:20 {24:03}
CTR
AC five twenty nine, West Georgia, the regional airport is at
your .. ten o'clock position and about ten miles.
1246:28 {24:11}
RDO-2
understand ten o'clock and ten miles, AC five twenty nine.
1246:30 {24:13}
CTR
's correct.
1246:36 {24:19}
HOT-1
(* give me) [whispered]
1246:38 {24:21}
HOT-1
let's get out the uh .... engine failure check list, please.
99

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1246:47 {24:30}
HOT-2
OK, I'll do it manually here.
1246:55 {24:38}
HOT-2
OK, engine failure in flight.
1246:57 {24:40}
CTR
AC five twenty nine, say heading.
1246:59 {24:42}
RDO-2
turnin' to about uh, three ten right now.
1247:01 {24:44}
HOT-2
power level's, flight idle.
1247:03 {24:46}
CTR
AC five twenty nine, roger. you need to be on about a zero
three zero heading for West Georgia Regional, sir.
1247:07 {24:50}
RDO-2
roger, we'll ("probly", or possibly,"try'ta") turn right. we're having
uh, difficulty controlling right now.
1247:11 {24:54}
HOT-2
OK, condition lever's, feather,
1247:13 {24:56}
HOT-1
alright.
1247:14 {24:57}
HOT-2
it did feather... Np's showing zero.
1247:18 {25:01}
HOT-1
'K.
1247:19 {25:02}
HOT-2
OK.
100
INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1247:20 {25:03}
CTR
AC five twenty nine, when you can, it's zero four zero.
1247:22 {25:05}
RDO-2
zero four zero, AC five twenty nine.
1247:25 {25:08}
HOT-2
'K, electric, yeah OK it did feather. there's no fire.
1247:27 {25:10}
HOT-1
alright.
1247:28 {25:11}
HOT-2
OK..
1247:32 {25:15}
HOT-2
main auxiliary generators of the failed engine off.
1247:35 {25:18}
HOT-1
'K. I got that.
1247:40 {25:23}
HOT-2
'K, APU .. if available, start. want me to start it?
1247:45 {25:28}
HOT-1
we gotta, bring this down, bring those. put the that off. bring the ice
off...
1247:54 {25:37}
HOT-B
[sound of chime similar to master caution starts and repeats at six
second intervals until the end of the recording]
1247:56 {25:39}
HOT-?
*.
1247:56 {25:39}
CTR
AC five twenty nine uh, say your altitude now sir.
101

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1247:59 {25:42}
RDO-2
out of seven thousand, AC five twenty nine.
1248:00 {25:43}
HOT-B
[sound of three chimes followed by voice message] trim fail. [warning
starts and continues]
1248:04 {25:47}
HOT-1
good start.
1248:04 {25:47}
CTR
AC five twenty nine, I missed that, I'm sorry.
1248:06 {25:49}
RDO-2
we're outta six point nine right now, AC five twenty nine.
1248:09 {25:52}
CTR
AC five twenty nine roger, West Georgia Regional, heading
zero seven zero.
1248:13 {25:56}
RDO-2
zero seven zero, AC five twenty nine.
1248:20 {26:03}
HOT-B
[sound of single beep]
1248:33 {26:16}
HOT-2
OK, it's up and running, Ed.
1248:34 {26:17}
HOT-1
alright, go ahead.
1248:35 {26:18}
CTR
AC five twenty nine, West Georgia Regional is your closest air-
port. the other one's uh, Anniston and that's about thirty miles
to your west, sir.
102

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1248:40 {26:23}
HOT-1
how long, how far West Georgia Reg ... what kind of a runway they
got?
1248:44 {26:27}
RDO-2
what kind of runway's West Georgia Regional got?
1248:54 {26:37}
HOT-1
go ahead and finish the check list.
1248:58 {26:41}
CTR
West Georgia Regional is uh, five say one six and three four
and it's five thousand feet ....
1249:01 {26:44}
HOT-2
OK, APU started. OK, prop sync, off. prop sync's comin' off.
1249:03 {26:46}
HOT-1
OK.
1249:04 {26:47}
HOT-2
fuel pumps failed engine. you want uh, max on this?
1249:07 {26:50}
HOT-1
go ahead, please.
1249:08 {26:51}
HOT-2
OK.
1249:09 {26:52}
CAM
[sound similar to propeller increasing in RPM]
1249:09 {26:52}
CTR
... and it is asphalt sir.
1249:11 {26:54}
HOT-2
hydraulic pump, failed engine? as required. put it to the on position?
103

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1249:15 {26:58}
HOT-1
correct.
1249:17 {27:00}
HOT-2
'K. engine bleed failed engine is closed and the pack is off.
1249:19 {27:02}
HOT-1
'K.
1249:26 {27:09}
HOT-2
'K, cross-bleed open.
1249:29 {27:12}
HOT-1
'K.
1249:32 {27:15}
HOT-2
electrical load, below four hundred amps.
1249:38 {27:21}
HOT-1
it is. put the ice ba ... (well you) don't need to do that just leave that
alone.
1249:45 {27:28}
HOT-1
alright, single engine check list please.
1249:48 {27:31}
CTR
AC five twenty nine, I've lost your transponder. say altitude.
1249:52 {27:35}
RDO-2
we're out of four point five at this time.
1249:54 {27:37}
CTR
AC five twenty nine, I've got you now and the airport's at your,
say say your heading now sir.
104

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1249:59 {27:42}
RDO-2
right now we're heading uh, zero eight zero.
1250:01 {27:44}
CTR
roger, you need about ten degrees left. should be twelve
o'clock and about eight miles.
1250:05 {27:48}
RDO-2
ten left, twelve 'n eight miles and uh, do we got a, ILS to this
runway?
1250:10 {27:53}
CTR
uh, I'll tell you what. let me put you on approach. he works that
airport and he will be able to give you more information. con-
tact Atlanta approach on one two one point zero, sir.
1250:15 {27:58}
HOT-1
we can get in on a visual.
1250:17 {28:00}
RDO-2
one more time on the freq..
1250:20 {28:03}
RDO-1
say again the frequency?
1250:22 {28:05}
CTR
Atlanta approach one two one point zero.
1250:24 {28:07}
RDO-2
twenty one zero, see ya.
1250:26 {28:09}
UNK-?
good luck guys.
1250:27 {28:10}
RDO-2
'preciate it.
105

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1250:28 {28:11}
HOT-B
[single beep similar to radio frequency change]
1250:29 {28:12}
RDO-2
Atlanta approach, AC five twenty nine's with you out of three
point four.
1250:36 {28:19}
HOT-1
engine's exploded. it's just hanging out there.
1250:43 {28:26}
RDO-2
Atlanta approach, AC five twenty nine.
1250:45 {28:28}
ATLA
AC five twenty nine, Atlanta approach.
1250:48 {28:31}
RDO-2
yes sir, we're with you declaring an emergency.
1250:49 {28:32}
ATLA
AC five twenty nine, roger. expect localizer runway three four
approach and uh, could you fly heading one eight zero uh no
sorry, one six zero?
1250:56 {28:39}
RDO-2
yeah we can do that. give me the loc freq ...
1250:59 {28:42}
ATLA
localizer frequency, runway three four localizer frequency is uh,
one one one point seven.
1251:05 {28:48}
HOT-1
we can get in on a visual. just give us vectors.
1251:07 {28:50}
RDO-2
one one one point seven ..... just give us vectors. we'll go the
visual.
106

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1251:17 {29:00}
HOT-1
sing, single, single engine check list, please.
1251:28 {29:11}
HOT-2
where the # is it?
1251:29 {29:12}
ATLA
AC five twenty nine, say altitude leaving.
1251:31 {29:14}
RDO-2
we're out of nineteen hundred at this time.
1251:33 {29:16}
HOT-1
we're below the clouds. tell 'm ...
1251:35 {29:18}
ATLA
you're out of nineteen hundred now?
1251:36 {29:19}
RDO-2
'K we're uh, VFR at this time. give us a vector to the airport.
1251:39 {29:22}
ATLA
AC five twenty nine. turn left uh, fly heading zero four zero.
bear, the uh, airport's at your about ten o'clock and six miles sir.
radar contact lost this time.
1251:47 {29:30}
RDO-2
zero four zero, AC five twenty nine.
1252:07 {29:50}
HOT-M
five hundred.
1252:10 {29:53}
HOT-M
too low gear. [starts and repeats]
107

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1252:11 {29:54}
ATLA
AC five twenty nine, if able, change to my frequency, one one
eight point seven. the airport uh, in the vicinity of your ten
o'clock at twelve o'clock and about four miles or so.
1252:20 {30:03}
HOT-1
help me, help me hold it, help me hold, help me hold it.
1252:26 {30:09}
ATLA
AC five twenty nine, change frequency, one one eight point
seven if able.
1252:32 {30:15}
HOT-B
too low gear [warning stops]
1252:32 {30:15}
HOT-B
[series of rapid beeps similar to aural stall warning]
1252:32 {30:15}
CAM
[vibrating sound similar to aircraft stick shaker starts and continues
for four seconds]
1252:36 {30:19}
CAM
[vibrating sound similar to aircraft stick shaker starts again and con-
tinues to impact]
1252:37 {30:20}
HOT-2
Amy, I love you.
1252:40 {30:23}
HOT-B
landing gear.
1252:41 {30:24}
CAM-?
[sound of grunting]
1252:45 {30:28}
CAM
[sound of impact]
108

INTRA-COCKPIT COMMUNICATION AIR-GROUND COMMUNICATION
TIME & TIME &
SOURCE CONTENT SOURCE CONTENT
1252:46 {30:29}
HOT-B
landing gear
1252:46 {30:29}
CAM
[sound of impact]
1252:46 {30:29}
END of RECORDING
END of TRANSCRIPT
109

110
APPENDIX C
Aircraft/
Blade
Model
ATR42/
14SF-5
EMB120/
14RF-9
FRACTURE SUMMARY *
Fracture
Operator
Location
Initiating
Defect
InterCanadian
Taperbore
0.031" deep pit
x
0.058"
wide
Nordeste
Taperbore
Band
of
pits .011 -.015"
deep x 0.160" wide
EMB120/
ASA
14RF-9
Taperbore
Pit (initial size
unknown);
.005"deep x 0.037"
wide
(at
surface)
0.011 wide (subsurface)
TT
TO
&
12,038
4,748
4,210
N/A
14,664
*
*
2,399
Blade
Observations
S/N
—
Coarse
banding
856922
10,000-15,000
Oxidized beach mark;
865093
0.032"deep x
0.160" wide
Oxidized beach mark;
861398
0.0487
"
deep x
0.0542"
wide
(at
surface)
0.066"
wide [subsurface)
All dimensions after rework
*Information provided by Hamilton Standard for
a
February 2, 1996, briefing to the Safety Board.
**The Safety Board’s investigation revealed that the total time
was
14,728
operating hours and 5,182
hours since overhaul.
1.
2
.
3.
4.
5.
6.
7.
8.
9.
10.
111
APPENDIX D
EMB-120/14RF-9
STRESS RESURVEY *
Summary
of
Flight Test Results
The
highest
vibratory stress
measured in flight was
±6000 psi and
occurred at the
20-inch and the
26-inch
stations during maneuvers
outside the normal flight envelope.
Vibratory stresses measured on the left propeller were about 2%
higher than those seen in the 1985 survey.
Vibratory stresses measured on the right propeller were about
8%
higher than those seen in the 1985
survey.
The right propeller stresses were about 6% higher than the left.
Some small differences in stressing amongst the blades were
observed. Generally, blade number four was the highest.
Average
relative levels for the other blades were: Blade no.
1- 97%
Blade
no. 2 - 95%, Blade no. 3-
96%, Blade no. 5-
100%. Also, there
was a standard deviation of
±3%
on these relationships.
The frequency of vibratory stressing for
all
the strain gages excep
t
the shank leading edge was primarily 1P. The shank leading edge
gage was primarily 2P with
1P
also present during high-stress
operation. This is consistent with historical data.
The Vee
gage was
always low in magnitude indicating no
significant torsional response. This was as expected.
The distribution of stress along the blade was seen to be slightly
different than theoretical. The 20-inch station was sometimes
higher than the 26-inch station. Analysis indicates that the
26-inch
station should be the highest. Also, the reduction in stress going
inboard from the peak is less than theoretical, see plot.
The trend of stress versus
aircraft
c.g.
vertical
acceleration
compares favorably with previous data, see plots.
The stresses experienced at the extremes of yaw maneuvers were
considerably
lower than those seen in the previous tests.
*Information provided by Hamilton Standard for a February 2, 1996, briefing to the
Safety
Board.

112
Summary of Ground Test Results
1.
2.
3.
4.
5.
6.
7.
8.
The highest vibratory stresses of the entire test
occurred
during
ground
running
in an adverse wind when the propeller speed
passed through the 2P/1f critical. The peak stress reached
±18,600 psi at the 26-inch station of blade number four. The wind
was from the rear quarter at approximately 28 knots.
The 2P/1f critical speed was found to exist at approximately 935
rpm, which is between the locations observed in the previous
two
tests (1983 and 1985), see plots.
The
vibratory stressing that occurs under these conditions is
almost completely 2P in frequency. Adjacent blades are out of
phase such that the reactions of the four blades cancel within the
hub. This is
consistent
with previous data.
Frequency analysis of the strain gage data showed poorly defined
peaks in the vicinity of the expected natural frequency. This could
be due to mis-tunning or other unknown reasons.
The Vee gage was always low in magnitude indicating no
significant torsional response. This was as expected.
The distribution of stress along the blade was seen to be slightly
different from previous experience, see plot.
The high stressing associated with the 2P/1f critical speed were
only observed during adverse wind operation. Tests in mild
headwinds showed very low levels of stress. Again this is as
expected.
In addition to the high stresses seen during operation in the region
of the 2P/1f critical speed, additional stress peaks were
observed
during transient conditions at speeds other than the critical. These
peaks appear to happen immediately after a power lever
movement, independent of the operating speed. They look exactly
like a rapid excursion through the critical speed, 2P in frequency
with adiacent blades out of
phase,
see
examples.
113
Conclusions & Recommendations
The
results
of this stress
survey
are consistent with past experience.
Small differences from previous stress levels were
observed.
Also,
differences were seen among the blades and between
the left
and
right
nacelles. These differences are not considered significant
The highest
vibratory
stressing occurred during
ground
operation in
adverse winds when the
prope!ler
speed was at
or
near 935 rpm
(72%
of
take-off).
This is due to the presence of a critical speed caused by
the coincidence of the
first
flatwise
blade mode and excitation due to
the second harmonic of the rotational
speed.
During the worst of
these conditions the vibratory stresses
were more
than
triple the
highest values measured
in
flight, including
maneuvers.
Operation
in
this
speed range must be kept to an absolute minimum to avoid
fatigue damage to the blades.
