
THE RELATIONSHIP BETWEEN FAM ILY TYPE
AND FERTILITY
KANTI PAKRASI
AND
CHITTARANJAN MALAKER
The large increase in the total population of India between 1951
and 1961 has been correctly described as “phenomenal.” 1 The prob
ability of success of any developmental measure initiated in India
must be appraised against the immediate background of staggering
population growth. The Planning Commission is anxious for a sub
stantial reduction in the population so that the Five Year Plans of
the country will have a genuine chance for success. Great effort and
enormous amounts of money are being expended to strike at the
root of problem of population increase.
In keeping with this situation, researchers are striving to sift out
the factors responsible for the conspicuous fertility differentials
among the general population. The fertility of Indian couples of
different social and economic strata have been subjected to meticu
lous investigation. Several studies have been carried out in different
parts of India to pinpoint the role of several cultural, economic and
demographic variables assumed to induce the high birth rate.2
The results of these studies serve to point out differences in fer
tility according to socioeconomic status and geographic location, the
major cultural and demographic factors associated with high or low
reproduction and the effect of deliberate limitation of reproduction.
The evidence now available, however, does not offer any clue to
451
understanding the persistent 2.2 per cent annual population growth
in India. The stage at which controlled fertility affects fertility dif
ferentials is yet to begin in the under-developed societies in the
country.3
During the past two decades population experts have focused their
attention on the rapid and massive population growth in India.
Davis4 attempted an exposition of fertility on the basis of rural-
urban, class and religious differentials to evaluate the prospects for
an early decline. Chandrasekhar5 pointed out various sociological
factors that were presumed to influence the population increase. He
commented that “the very low level of living, the absence of a pro
longed period of education or training, the existing social attitudes
that encourage a large family, the joint family, the want of nation
wide contraceptive clinical service, and above all, the psychological
reason that encourages every man to look to his wife and sex inti
macy as the only relaxation and recreation in an otherwise dull and
unexciting life of a relentless struggle to make both ends meet—all
these are contributing factors.” Thus the sociological factors asso
ciated with high fertility in Indian families have already been
highlighted, and this may provide a proper perspective for future
demographic research. Because reproduction is one of the primary
functions of the family, the organizational pattern of the family itself
is of special significance in the study of fertility, particularly within
the traditional establishment of Asian society.
Kiser and Whelpton6 have so well established the value of study
ing fertility patterns in terms of the socioeconomic status of the
couples concerned that this variable has become an essential ingre
dient in later fertility studies. In defining socioeconomic status, how
ever, the attribute of family orientation of the couples under investi
gation was given hardly any consideration. Factors such as annual
earnings, occupation, education, monthly rental value, food habits,
place of work, attitude on birth control and children’s future edu
cation have frequently been employed to measure the behavior to
ward reproduction. The crucial factor in the relationship between
fertility and the kind of family in which the couple lives, acts and
452
procreates, with all familial prerogatives and obligations, has yet
to receive the attention and utilization merited by its importance.
That the role of the family is immediately related to the repro
duction functions of couples living in nonindustrial and agrarian
societies has already been stressed.7 Lorimer8 was one of the few
pioneers to indicate the significance of that social truth when he
dwelt upon the relation of cultural conditions to fertility. According
to him, large, cohesive families in an Asiatic society serve not only
to protect prestige and collective economic security, but also to
provide the constituent members with a “source of deep emotional
security.” The cultural context of this society is such that the families
representing “group family life” are commonly “idealized” and,
according to Lorimer, are “likely to be conducive to high fertility.”
His explanation for high reproduction rates in large, cohesive fam
ilies, including traditional joint (extended) units, remains to be
substantiated by empirical findings from the contemporary rural
or urban societies of India.
The academic and professional interest shown by experts con
tinues in their search for the probable interrelations between various
social and demographic factors, including the factor of family struc
ture and human fertility.9
Following Lorimer, demographers extended their efforts to point
out various “cultural barriers” against fertility reduction, particularly
in underdeveloped societies.10 As to the nature of such a barrier in
India, “The relation of the family pattern to birth rate is obvious.
In large traditional families such as the joint family in India . . .
the normal economic deterrents against the arrival of that extra
baby do not operate.” 11 The primary contention of Chandrasekhar
appears to be that the large family units (extended or joint) in
India are culturally equipped to accommodate any “ extra baby”
of the young parents, and thus serve as “ an incentive to higher
birth rate.” In agreement with him are the views of Davis12 who
also had the occasion to correlate the pattern of joint family estab
lishment with the high rate of reproduction in the peasant-agricul
tural societies of the underdeveloped areas of the world.
453

Other recent studies13 have focused on the relationship between
the extended (joint) type of family pattern and high fertility. These
studies have been initiated in several different types of communities
in different states in India, and the data from the studies indicate
that the women living in joint families are less fertile than are those
in simple (nuclear) families. The connection between extended
(joint) families and high fertility is, thus, a controversial but exciting
issue.
A study has been made to determine “whether the joint families in
contemporary Indian setting have actually higher fertility than the
single families.” 14 The conclusion reached is that for each one of
three Hindu and three Muslim groups of rural West Bengal, “the
average number of children in joint families is less than that in sim
ple families when women of all ages are considered. This is also
true for the majority of age categories of women.” The author ad
mitted that the observed differences on the average are “quite small
and are not likely to be statistically significant.” Nevertheless, the
study deserves commendation since it attempts to cope with the
problem by utilizing empirical data on Bengali women of seven
villages of the state. Data accumulated in this paper have their own
importance to interested researchers, even though the method em
ployed to analyze the data is not strong enough to establish a sta
tistically sound conclusion about the problem in question. Standard
ized averages should have been calculated to indicate the nature of
actual differences in fertility of the women belonging to joint or
simple families. As Table 1 shows, the results of such calculations
indicate that fertility differentials of the women belonging to joint
and simple families within a social group do not appear to be widely
fluctuating.
The intrinsic fertility performance of women varies from age to
age. For that reason, simple averages, as are given in the Nag pa
per,14 do not indicate the true fertility performance of the group or
the fertility differentials between groups because of the difference in
the proportion of women in the different age groups. Comparison of
the standardized averages in Table 1 shows that the differentials
diminish to an appreciable extent. Fertility differentials should be
454
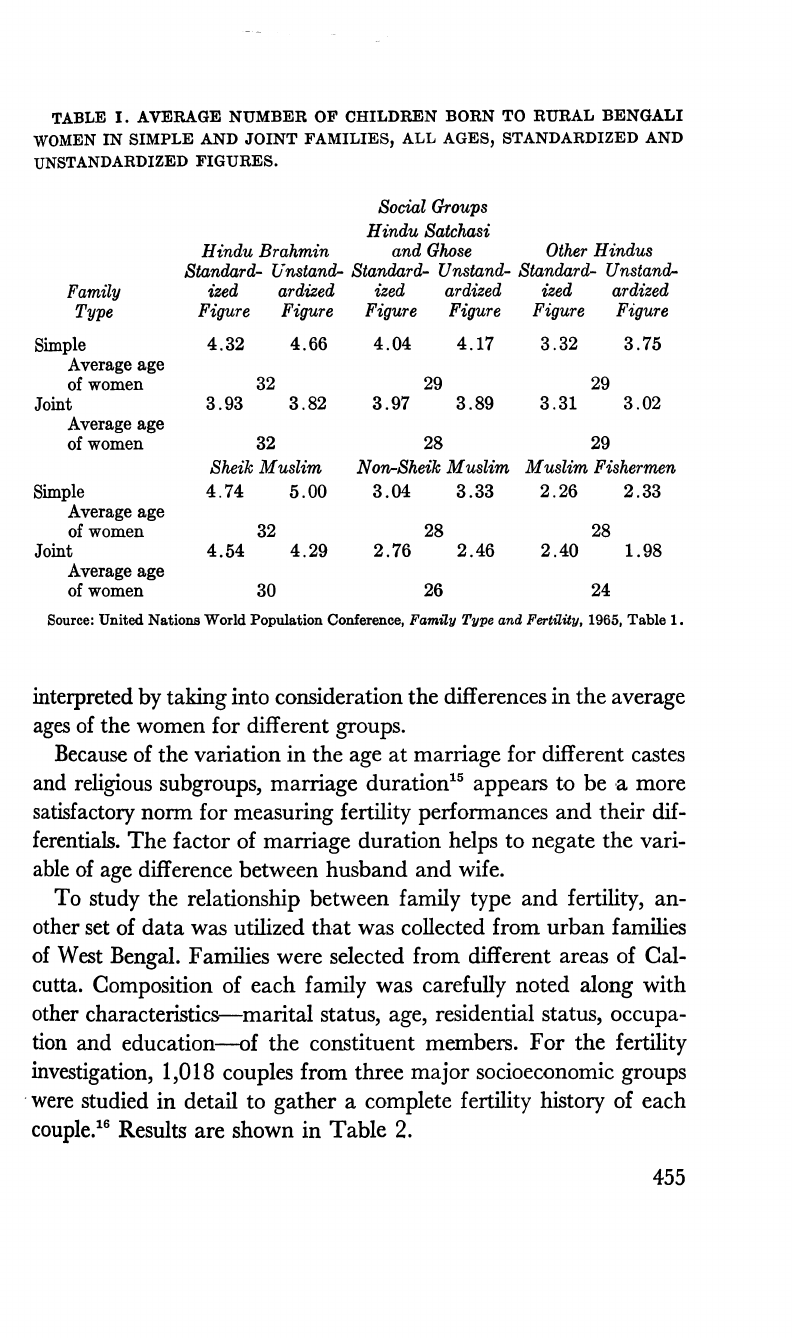
TABLE I. AVERAGE NUM BER OP CHILDREN BORN TO RU RAL BENGALI
WOMEN IN SIMPLE AND JOINT FAM ILIES, ALL AGES, STANDARDIZED AND
UNSTANDARDIZED FIGURES.
Social Groups
Hindu Satchasi
Hindu Brahmin and Ghose Other Hindus
Standard- Unstand- Standard- Unstand- Standard- Unstand-
Family
ized
ardized ized ardized ized ardized
Type
Figure Figure
Figure
Figure Figure Figure
Simple
4.32 4.66
4.04
4.17
3.32
3.75
Average age
of women
32
29 29
Joint
3.93
3.82 3.97 3.89 3.31
3.02
Average age
of women
32 28 29
Sheik Muslim
Non-Sheik Muslim
Muslim Fishermen
Simple
4.74
5.00
3.04
3.33
2.26
2.33
Average age
of women
32
28 28
Joint
4.54
4.29 2.76
2.46
2.40 1.98
Average age
of women
30 26
24
Source: United Nations World Population Conference, Family Type and Fertility, 1965, Table 1.
interpreted by taking into consideration the differences in the average
ages of the women for different groups.
Because of the variation in the age at marriage for different castes
and religious subgroups, marriage duration15 appears to be a more
satisfactory norm for measuring fertility performances and their dif
ferentials. The factor of marriage duration helps to negate the vari
able of age difference between husband and wife.
To study the relationship between family type and fertility, an
other set of data was utilized that was collected from urban families
of West Bengal. Families were selected from different areas of Cal
cutta. Composition of each family was carefully noted along with
other characteristics— marital status, age, residential status, occupa
tion and education— of the constituent members. For the fertility
investigation, 1,018 couples from three major socioeconomic groups
were studied in detail to gather a complete fertility history of each
couple.16 Results are shown in Table 2.
455

TABLE 2. DISTRIBUTION OP SIMPLE AND JOINT FAMILIES BY DURATION
OP MARRIAGE AND SOCIAL STRATA AMONG THE POPULATION OF CAL
CUTTA, WEST BENGAL, 1956- 57.
Social Class
and Family
0-4
Duration of Marriage
5-9 10-14
15 years
All
Type
years
years
years and above
Durations
Class I
Simple
29.4%
43.9%
47.2% 50.6%
42.8 %
Joint
70.6%
56.1% 52.8%
49.4%
57.2%
Number of
family units
34
66 53 85
238
Class II
Simple
17.4%
33.6% 35.1%
55.7%
35.5%
Joint
82.6%
66.4%
64.9% 44.3%
64.5%
Number of
family units
69
116
134 140
459
Class III
Simple 50.0% 47.5%
55.4% 58.1%
52.8%
Joint
50.0% 52.5%
44.6% 41.9%
47.2%
Number of
family units 20
82 128
91
321
The three socioeconomic groups, which were identified jointly on
the basis of the husband’s occupation and educational status, were:
I. Higher professions and services: physicians, engineers, office
executives, wholesale businessmen.
II. Clerks, supervisors, retail traders.
III. Manual laborers, skilled and unskilled.
Composition of the family unit of each couple under study was
first carefully examined to place the unit under one of two broad
types: 1. simple (nuclear) type composed of only the parents and
their unmarried children, and 2. extended or joint (non-nuclear)
type consisting of simple families plus one or more consanguineous
relatives or other genealogically determinable relatives. To avoid a
detailed discussion of typological classification17 these two broad
types of family organization have been adhered to primarily in con
sideration of the current controversy over the question of joint (ex
tended) family’s relationship to higher fertility.
The couples belonging to each of the three socioeconomic groups
456

were further classified by duration of marriage, and the average
number of children ever-born per couple in each marriage duration
class was analyzed. Family affiliation of each couple was also noted.
The proportional concentrations of simple and joint families under
each marriage-duration class are shown in Table 2.
Regarding the nature of variation in fertility rates within the
three occupationally oriented social classes, it has already been
pointed out that “fertility rates of couples belonging to higher
professions, higher services, etc. (social class I) are lower than those
pertaining to the social classes II and III, particularly in the higher
marriage duration classes.” 18
Variations in the average number of children ever-born per couple
in the different social classes have been further examined on the
TABLE 3. AVERAGE NUM BER OF CHILDREN BORN PE R COUPLE BY
SOCIAL CLASS, D URATION OF MARRIAGE AND FAM ILY TYPE AMONG THE
POPULATION OF CALCUTTA, W EST BENGAL, 1956- 57.
Average Number of
Children Ever Born
Duration of Number of Couples in per Couple in
Social Marriage
Simple
Joint
Simple
Joint
Class (years)
Family Family
Family*
Family'-
Class I 0-4
10
24
0.9 0.6
5-9 29
37
2.1
2.1
10-14
25
28
3.4
2.6
154- 43
42
3.8
3.4
all 107 131
2.9
2.3
All-standardized rate 2.9
2.5
Class II 0-4
12
57
1.2
1.0
5-9 39 77
2.6 2.1
10-14
47 87
3.8
3.4
154-
78
62
4.9
4.6
all 176 283 3.8 2.8
All standardized rate
3.4
3.1
Class III 0-4
10
10 1.0 0.7
5-9 39 43 2.0 2.6
10-14
71 57 3.5
4.1
15+
53
38
5.3 5.1
all 173 148 3.5 3.7
All standardized rate
3.5 3.8
* Averages are based on the number of couples falling under each family type and each marriage
duration—class.
457

basis of the structural characteristics of the family in which the
couples were components. Table 3 shows that for social classes I
and II the average number of children ever-born per couple in
extended or joint families is definitely less than that in simple (non-
extended) families, when women of all marriage duration classes
are considered. This is also true for nearly all women of any mar
riage-duration class, except the initial one (0-4 years). Standardized
rates have been computed and the trend in classes I and II indicates
that this development cannot be explained simply by chance.
In class III, the average number of children ever-born per couple
is more in extended or joint families. Couples in this group differ
from the couples in classes I and II in having less of a children load
within simple (non-joint) family units. In this group, however, any
trend in the averages cannot be proved.
The couples in class I not only had the lowest fertility rate of the
three classes, but also maintained the same trend with respect to
their family orientation toward simple or joint family types. The
lowest standardized rate of fertility for couples belonging to simple
or joint families is obtained in the highest socioeconomic group. The
highest standardized rates, of course, are obtained from couples in
the lowest socioeconomic class, with the couples in class II scoring
between the two extremes.
Some interesting conclusions may be based upon these findings:
1. Joint (extended) families are not an essential prerequisite for
abundant reproduction.
2. Urban population closely resembled the rural population of West
Bengal in the fertility differentials between women of joint and sim
ple families. The urban, class I population averaged the fewest num
ber of children per mother, especially in joint families.
3. Irrespective of their location, whether urban or rural, the women
of West Bengal averaged a greater number of children in simple
families than in joint families. This trend is evident in Nag’s study14
and in the present one. Under the circumstances, can this trend be
explained by chance factors alone?
4 5 3

4. A possible relationship between family type and fertility appears
to be a pertinent issue that cannot be ruled out of current social-
demographic research. A greater number of field investigations cover
ing wider areas to include more Indian communities are needed to
accumulate empirical data. What has been attempted so far has only
served to highlight the problem. The underlying basis of the rela
tionship between family type and fertility has yet to be established.
To this end, it is hoped that the findings in this paper, together with
those of Nag and others, may be the base of future investigations.
REFERENCES
1 Final Population Totals, in C e n su s of I ndia (1961), Government of
India, pp. x-xi.
2 Das Gupta, Ajit, et al., Couple Fertility, National Sample Survey Report
no. 7, Ministry of Finance, Government of India; Rele, J. R., Fertility Differ
entials in India: Evidence from a Rural Background, Milbank Memorial Fund
Quarterly, 41, 183-199, April, 1963; Chandrasekaran, G. and George, M. V.,
Mechanism Underlying the Differences in Fertility Patterns of Bengalee
Women from Three Socio-Economic Groups, Milbank Memorial Fund Quar
terly, 40, 59-89, January, 1962; Jain, S. P., R elatio n sh ip Between Fertility
and Economic and Social Statu s in th e Pu n jab, Lahore, Punjab Board of
Economic Inquiry, 1939; Sovani, N. V. and Dandekar, Kumudini, Fertility
Survey of Na sik, K olaba and Satara (N or t h ) D istricts, Poona Gokhale
Institute of Politics and Economics, 1955; Sinha, J. N., Differential Fertility and
Family Limitation in an Urban Community of Uttar Pradesh, Population Stud
ies, 11, 157-169, November, 1957.
3 Chandrasekaran, C., Fertility Trends in India, Proceedings of the World
Population Conference, 1, 827, August—September, 1954; Jain, S. P., Indian
Fertility: Trends and Patterns, Proceedings of the World Population Conference,
1, 901, August-September, 1954; Rele, J. R., loc. cit.
4 Davis, Kingsley, Human Fertility in India, The American Journal of
Sociology, 52, 243-254, November, 1946.
5 Chandrasekhar, Sripathi, I ndians Population : Fact and Policy, New
York, The John Day Company, Inc., 1946.
6 Kiser, Clyde V. and Whelpton, P. K., Number of Children in Relation to
Fertility in Planning and Socio-Economic Status, Eugenical News, 34, 33-43,
1949.
7 The Family Planning Association of India, Report of the Proceedings of
the Third International Conference on Planned Parenthood, Bombay, 1952, pp.
14-25 and 68-79.
8Lorimer, F., C ultu re and H um an Fertility, Paris, UNESCO, 1954.
459

9 Davis, Kingsley, T he Population of I ndia and Pa k istan, Princeton,
New Jersey, Princeton University Press, 1951; Driver, Edwin D., Fertility Dif
ferentials Among Economic Strata in Central India, Eugenics Quarterly, 7,
77-85, 1960; T he M ysore Population Study, New York, The United Na
tions, 1961; Samuel, T. J., Culture and Human Fertility in India, Journal of
Family Welfare, 9, 48, June, 1963; Stycos, J. M., Problems of Fertility Control
in Underdeveloped Areas, in Mudd, S. (Editor), T he Population Crisis
and th e U se of W orld R esources, Bloomington, Indiana, Indiana Univer
sity Press, 1964, p. 95; Bebarta, Prafulla C., Family Structure and Fertility, in
Proceedings (A b s t r act s) of t h e I ndian Science Congress, Part 3, 1965,
p. 503, Pakrasi, Kanti, On Some Aspects of Fertility and Family in India, Indian
Journal of Social Work, 17, 153-162, July, 1966.
10 International Planned Parenthood Federation, Report of the Proceedings
of the Fifth International Conference on Planned Parenthood, London, 1955.
11 Chandrasekhar, Sripathi, Cultural Barriers to Family Planning in Under
developed Countries, Proceedings of the Fifth International Conference on
Planned Parenthood, London, 1955, pp. 64-70.
12 Davis, Kingsley, Institutional Patterns Favoring High Fertility in Under
developed Areas, Eugenics Quarterly, 2, 33-39, March, 1955; and in Shanon,
L. W. (Editor), U nderdeveloped A reas, New York, Harper & Brothers, Pub
lishers, 1957.
13 Poti, Sankar J. and Dutta, Subodh, Pilot Study on Social Mobility and Its
Association with Fertility in West Bengal in 1956, Artha Vijnana, 2, 85-96,
June, 1960; Bebarta, Prafulla C., loc. cit., Mukherjee, Ramkrishna, T he Soci
ologist and Social C hanges in India T oday, New Delhi, Prentice-Hall of
India, Ltd., 1965, pp. 10-11; Mathen, K. K., Preliminary Lessons Learned from
the Rural Population Control Study of Singur,
in Kiser, Clyde V. (Editor),
R esearch in Fam ily Planning, Princeton, New Jersey, Princeton University
Press, 1962, pp. 33-50.
14 Nag, Moni, Family Type and Fertility, Paper submitted to the United
Nations World Population Conference, Belgrade, 1965.
15 Das Gupta, Ajit, et al., op. cit., pp. 7-8.
16 Poti, Sankar J., Malaker, Chittaranjan and Chakraborti, Bimal, An En
quiry into the Prevalence of Contraceptive Practices in Calcutta (1956-57), in
Studies in Fam ily Plannin g, Ministry of Health, Government of India, 1960,
pp. 63-89; Poti, Sankar J., Chakraborti, Bimal and Malaker, Chittaranjan,
Reliability of Data Relating to Contraceptive Practices, in Kiser, R esearch
in Fam ily Plannin g, op. cit., pp. 51-65.
17 Pakrasi, Kanti, A Study of Some Aspects of Household Types and Family
Organization in Rural Bengal, 1946—47, The Eastern Anthropologist, 15, 55—63,
September-December, 1962; and A Study of Some Aspects of Structural Varia
tions among Immigrants in Durgapur, West Bengal, Man In India, 42, 114-125,
April-June, 1962.
18 Poti, Malaker and Chakraborti, An Enquiry into the Prevalence of Con
traceptive Practices in Calcutta, op. cit., p. 3.
460

REVIEW ARTICLE
STUDIES IN EPIDEMIOLOGY
Selected Papers of Morris Greenberg, M.D.
FRED B. ROGERS, EDITOR
New York, G. P. Putnam’s Sons, 1965. 418 + xxviii pp. $8.50
This book, a collection of more than a score of previously pub
lished papers and documents, was conceived and published by the
friends and colleagues of Morris Greenberg as a tribute to the
late Director of the Bureau of Preventable Diseases for the New
York City Department of Health, who was also the Adjunct Pro
fessor of Epidemiology at Columbia University. The affection and
esteem in which Greenberg was held is apparent in the tributes by
Leona Baumgartner, Harry Mustard and Gurney Clark, which
preface the book.
The general purpose of this collection, as stated by Gurney Clark,
is to add a new volume to the growing “bookshelf of collected public
health papers by leading modem American workers.” The editor,
Fred B. Rogers, comments that the papers “ illustrate technical
competence in gathering and evaluating data, arriving at conclu
sions, and finally taking action.” It is by editorial action that papers
on diverse subjects have been integrated, and it is therefore this
editorial contribution which must be examined to see if the man and
his mind emerge from behind the memorial facade. In short, does
editor Rogers do justice to his subject?
To begin with, Greenberg and his department have already been
introduced to a generation of medical students and public by the
461
Boswellian accounts of Berton Roueche, which cover the same time
period and many of the same epidemiological adventures as in the
Rogers collection. But Roueche is better able to communicate the
drama, triumphs and hardships of field epidemiology than the crisp,
terse case reports included in this book.
Greenberg himself defined epidemiology from the vantage point
of one accustomed to dealing with the community: “a science con
cerned with the relationships of disease in the aggregate—what has
been called ‘crowd diseases.’ ” Perhaps because he was a practicing
pediatrician during the early period of his professional life, the sub
ject matter of his papers tends to retain a clinical orientation and to
specialize in the area of maternal and child health. Statistical and
research sophistications appear in his publications, but are not em
phasized in this collection; the viewpoint is eminently practical and
even the most theoretical considerations are translated into public
health action. Two examples illustrate both his style and the concern
arising out of his investigations:
Blanket advocacy of therapeutic abortion in pregnant women
who develop rubella during the early months of pregnancy is
medically unjustified. Exposure of susceptible young girls to cases
of rubella is medically justified and is a sound public-health
procedure.
What difference does it make if you give the patient a shot of
penicillin? Well, it does make a difference! It is time to call a
halt to the march back to Lister’s era and to remember that
cleanliness is still nearest to Godliness.
It is, however, becoming the practice to define epidemiology as
that which epidemiologists do. Therefore, any collection of the
life’s work of a great epidemiologist could be a formative document
which helps to delineate the methods of epidemiological enquiry. If
this is the aim of this memorial, the editorial work is not always
successful. Rogers has organized the reports into five groups—scope,
content and method of epidemiology; studies in community and in
stitutional settings; bacterial and viral diseases; immunoprophylaxis
and therapy; and congenital anomalies and defects. Rogers precedes
each paper with an introduction intended to put Greenberg’s con
462

tribution into the global scope of medical progress. The introduc
tions, however, tend to focus upon the disease state in question,
rather than upon Greenberg’s contribution to the growing list of
epidemiological skills and practices.
Sometimes the reason for the selection of a specific paper is un
certain. In fact, the editor is not always kind to his author: he in
cludes three early reports on the clinical use of gamma globulin for
“historical record” but omits the historical first four reports of
Rickettsialpox, substituting a summary prepared for a textbook. A
lengthy series of clinical and pathological case reports of congenital
cardiac anomalies in infants is included, though their focus is not
epidemiological. Two papers originally published in Nursing World
display Greenberg’s skills in communication about such topics as
Salk vaccine and viral diseases, though these treat epidemiological
considerations too superficially. Another technical paper on po
liomyelitis prepared for Hospitals is more successful, only because
it includes matters of organization and mobilization of medical ser
vices which were based upon sound epidemiological principles. In
the case of poliomyelitis and the embryopathic effects of rubella in
pregnancy, however, the order of scientific reports and the editorial
comment blend and successfully communicate the steps of epi
demiological investigation; in the case of others, even when the
original research protocol is included, the brevity of details will make
them less suitable as models for teaching methods of enquiry.
The reader may also find a number of minor editorial decisions
troublesome: publication citations are not given immediately in as
sociation with each paper; individual articles are not listed in the
table of contents or on the page headings, so that one has difficulty
in finding a paper quickly; photographs included with several of
the papers are not of sufficient quality to warrant reproduction.
Whether Rogers’ collection and editorial comments do justice
to the mind of his subject can best be answered by Morris Green
berg’s friends. This reviewer cannot help but feel that the unique
contribution which Greenberg made to epidemiological progress has
not, however, been given sufficient prominence by the editorial work.
In his prefatory tribute Harry Mustard points out that Morris Green
463
berg, the epidemiologist, was a product of both his native ability
and New York City: “The city’s own vast and mixed population,
its packed millions, its steady flood of visitors, its incoming mari
time commerce .. . made inevitable the endemic existence of a wide
gamut of communicable diseases and the threat of epidemics a
continuing menace.” Greenberg rose to the challenge which this
megapolis afforded. The epidemiological method is usually con
fined to the study of diseases of relatively high prevalence. But in a
population base the size of New York City, it is possible to study, by
both prospective and retrospective means, diseases of low incidence
rate. Possible, yes— but only with a superb epidemiological intelli
gence system that permeates the entire health care system. This or
ganization Morris Greenberg had, and developed so that he could
conceive and perform research studies impossible elsewhere. New
York City gave scope for Greenberg’s scientific curiosity.
In some cases, his studies were conducted specifically because of
the existence of this reporting system, as, for example, an evaluation
of different methods of prophylaxis for ophthalmia neonatorum and
the study of congenital defects of children bom to mothers who had
rubella in their first trimester of pregnancy. In another situation, this
large population produced enough persons for anti-rabies treatment,
so that it was possible for Greenberg to compare duck embryo and
Semple vaccines. The massive vaccination programs during the
1947 epidemic of smallpox in New York City permitted him to
undertake a definitive analysis of the complications, and report
on the effects of vaccination during pregnancy. It required this large
population to produce 13 infants whose acute diarrhea was identified
as being caused by Salmonella montevideo in canned egg yolk
powder, and 194 cases of pica from which 28 cases of proven and
20 of probable lead poisoning were found. An outbreak of 84 cases
of trichinosis led Greenberg to make a comparison of the intradermal
and precipitin tests for this disease. The periodic epidemics of
poliomyelitis provided him with sufficient numbers of cases to com
plete a most thorough examination of the relationship between
tonsillectomy and poliomyelitis. Yet, this combination of natural
and planned experiments was always carefully handled, and Green
464

berg assiduously avoided generalizing beyond his data or drawing
false conclusions. The limitations of natural experiments were
clearly always before this investigator.
The real value of this book, then, lies in the fact that the ma
jority of its papers comprise the first collection in the growing prac
tice of mass epidemiology, or to coin a term, epimegademiology—
the study of disease distribution and determinants in massive popu
lation groups. That this work was done by a man who had significant
administrative responsibilities is a tribute not only to his scientific
curiosity, but also to his organizational expertise. If this is not wholly
apparent in this book, the fault must be regarded as an editorial one.
Rogers has focused upon disease; the book would have been a more
useful and a greater tribute to its subject had it focused on the
epidemiological intelligence service Greenberg used so effectively.
In one sense, the collection portrays Greenberg in the same sense
as the novelist Ian Fleming portrayed James Bond— in a series of
spectacular confrontations with the criminal world. What was
needed was the viewpoint of Bond’s superior, M, and a description
of how he selected priorities and used his agents effectively. That,
I think, was the way Morris Greenberg advanced the discipline of
epidemiology.
DONALD O. ANDERSON
465
