
Federal Aviation Administration
MedXPress
User Guide
Version 5.2
June 2024
MedXPress
User Guide
Version 5.2
April 2024
1
Contents
2 Table of Figures ................................................................................................................. 4
3.1 The Medical Certification Process at a Glance ......................................................................... 6
4 Request an Account ........................................................................................................... 6
4.1 Request an Account Form ................................................................................................... 7
4.2 Account Request Result ...................................................................................................... 8
4.3 Registration Confirmation ................................................................................................... 9
4.4 Privacy Act Statement ........................................................................................................ 9
4.5 Change Password ............................................................................................................ 10
5 Login ............................................................................................................................. 11
5.1 Privacy Act Statement ...................................................................................................... 12
5.2 Login Confirmation .......................................................................................................... 12
5.3 Home ............................................................................................................................. 13
5.4 Account .......................................................................................................................... 13
5.5 Help ............................................................................................................................. 14
6 Account Maintenance ....................................................................................................... 14
6.1 Update Account Information .............................................................................................. 14
6.1.1 Update your Personal Information ................................................................................... 12
6.1.2 Change your Password ................................................................................................... 12
6.1.3 Update your Security Question Answers ........................................................................... 12
6.2 Forgot Password .............................................................................................................. 13
6.3 Password Reset Notification .............................................................................................. 14
6.4 Session Timeout .............................................................................................................. 16
7 Accessing Form 8500-8 .................................................................................................... 16
8 Exam Type Selection ........................................................................................................ 16
9 Pilot’s Bill of Rights .......................................................................................................... 18
10 Step-by-Step Form 8500-8 ............................................................................................... 18
10.1 Navigation Breadcrumb ................................................................................................... 18
10.2 Navigation Buttons ......................................................................................................... 18
10.2.1 Save and Complete Later ............................................................................................. 19
10.2.2 Cancel My Application .................................................................................................. 20
10.2.3 Check for Errors .......................................................................................................... 20
10.3 Additional Instruction ..................................................................................................... 21
10.4 General Section (Items 1 and 2) ...................................................................................... 21
10.4.1 Item 1 Application For .................................................................................................. 22
10.4.2 Item 2 Class of Medical Certificate ................................................................................. 22
10.4.3 Applicant ID ............................................................................................................... 22
10.5 Demographics Section (Items 3 - 9) ................................................................................. 23
10.5.1 Item 3 Full Name ........................................................................................................ 24
10.5.2 Item 4 Social Security Number ...................................................................................... 24
10.5.3 Item 5 Address ........................................................................................................... 24
10.5.4 Item 6 Date of Birth .................................................................................................... 25
10.5.5 Item 7 Color of Hair ..................................................................................................... 25
10.5.6 Item 8 Color of Eyes .................................................................................................... 25
10.5.7 Item 9 Sex ................................................................................................................. 25
10.6 Prior Certification Section (Items 10 - 16) ......................................................................... 25
10.6.1 Item 10 Type of Airman Certificate(s) You Hold ............................................................... 26
10.6.2 Item 11 Occupation ..................................................................................................... 26
10.6.3 Item 12 Employer ....................................................................................................... 27
10.6.4 Item 13 Has Your FAA Airman Medical Certificate Ever Been Denied, Suspended, or Revoked?
MedXPress
User Guide
Version 5.2
April 2024
2
27
10.6.5 Item 14 Total Pilot Time (Civilian Only) To Date .............................................................. 27
10.6.6 Item 15 Total Pilot Time (Civilian Only) Past 6 Months ...................................................... 27
10.6.7 Item 16 Date of Last FAA Medical Application .................................................................. 27
10.7 Medication Section (Items 17a and 17b) ........................................................................... 28
10.7.1 Item 17a Do You Currently Use Any Medication (Prescription or Nonprescription)? ............... 28
10.7.1.1 Removing Medications ............................................................................................... 29
10.8 Medical History Section (Item 18) .................................................................................... 29
10.8.1 Item 18 Have you ever in your life been diagnosed with, had, or do you presently have any of
the following? ................................................................................................................. 31
10.8.1.2 Part 2 ...................................................................................................................... 31
10.8.1.3 Part 3 ...................................................................................................................... 31
10.9 Medical Visits Section (Item 19) ....................................................................................... 32
10.9.1 Item 19 Have you visited any health professionals within the last 3 years? .......................... 32
10.10 Declarations Section ..................................................................................................... 33
10.10.1 Item 20 Applicant's National Driver Register and Certifying Declarations: .......................... 34
11 Validate and Submit Application ........................................................................................ 34
12 Submit My Application ...................................................................................................... 34
13 Application Successfully Submitted .................................................................................... 35
14 Application Summary (Items 1 to 17b) ............................................................................... 36
15 Application Summary (Items 18 to 20) ............................................................................... 37
16 Application Summary (Continuation Page) .......................................................................... 37
17 Application Submission Confirmation Email ......................................................................... 38
18 Viewing Confirmation after Submission ............................................................................... 39
19 Creating a New Application After Submission ....................................................................... 40
20. Application Status ............................................................................................................ 40
20.1 No Application Submitted ................................................................................................ 40
20.2 Submitted ..................................................................................................................... 41
20.3 Imported ...................................................................................................................... 42
20.4 Transmitted .................................................................................................................. 43
20.5 In Review ..................................................................................................................... 44
20.6 Action Required ............................................................................................................. 48
20.7 Transmitted Status – No Activity for More Than 60 Days ...................................................... 51
20.8 Certificate Decision – Medical Certificate Issued ................................................................. 52
20.9 Certification Decision – Denial, Disqualification, Withdrawal ................................................. 54
20.10 Certificate Decision - Final Review ................................................................................. 56
Appendix A: Instructions for Completion of the Application for Airman Medical Certificate, FAA Form
8500-8 ........................................................................................................................... 57
Appendix B: Additional Instructions (available by expanding applicable 8500-8 Items) ................... 59
1.
Application For ................................................................................................................ 59
2.
Class of Medical Certificate Applied For ............................................................................... 59
3.
Full Name ....................................................................................................................... 59
4.
Social Security Number .................................................................................................... 59
5.
Address .......................................................................................................................... 59
6.
Date of Birth ................................................................................................................... 59
7.
Color of Hair ................................................................................................................... 59
8.
Color of Eyes................................................................................................................... 59
9.
Sex ................................................................................................................................ 59
10.
Type of Airman Certificate(s) You Hold ............................................................................... 60
11.
Occupation ..................................................................................................................... 60
12.
Employer ........................................................................................................................ 60
13.
Has Your FAA Airman Medical Certificate Ever Been Denied, Suspended, or Revoked? .............. 60
14.
Total Pilot Time (Civilian Only) to Date ............................................................................... 60
MedXPress
User Guide
Version 5.2
April 2024
3
15.
Total Pilot Time (Civilian Only) Past 6 Months ...................................................................... 60
16.
Date of Last FAA Medical Application .................................................................................. 60
17.a. Do You Currently Use Any Medication (Prescription or Nonprescription)? .............................. 60
17.b. Do You Ever Use Near Vision Contact Lens(es) While Flying? .............................................. 60
18.a. Frequent or severe headaches ........................................................................................ 60
18.b. Dizziness or fainting spell ............................................................................................... 61
18.c. Unconsciousness for any reason ...................................................................................... 61
18.d. Eye or vision trouble except glasses ................................................................................ 61
18.e. Hay fever or allergy ....................................................................................................... 61
18.f. Asthma or lung disease .................................................................................................. 61
18.g. Heart or vascular trouble ............................................................................................... 61
18.h. High or low blood pressure ............................................................................................. 61
18.i. Stomach, liver, or intestinal trouble.................................................................................. 61
18.j. Kidney stone or blood in urine ......................................................................................... 61
18.k. Diabetes ...................................................................................................................... 61
18.l. Neurological disorders: epilepsy, seizures, stroke, paralysis, etc. ......................................... 61
18.m. Mental disorders of any sort: depression, anxiety, etc. ..................................................... 61
18.n. Substance dependence or failed a drug test ever; or substance abuse or use of illegal substance
in the last 2 years. ........................................................................................................... 62
18.o. Alcohol dependence or abuse ......................................................................................... 62
18.p. Suicide attempt ............................................................................................................ 62
18.q. Motion sickness requiring medication ............................................................................... 62
18.r. Military medical discharge .............................................................................................. 62
18.s. Medical rejection by military service ................................................................................ 62
18.t. Rejection for life or health insurance ................................................................................ 62
18.u. Admission to hospital .................................................................................................... 62
18.x. Other illness, disability, or surgery .................................................................................. 62
18.y. Medical disability benefits ............................................................................................... 62
18.v. History of (1) any arrest(s) and/or conviction(s) involving driving while intoxicated by, while
impaired by, or while under the influence of alcohol or a drug; or (2) history of any arrest(s),
and/or conviction(s), and/or administrative action(s) involving an offense(s) which resulted in the
denial, suspension, cancellation, or revocation of driving privileges or which resulted in
attendance at an educational or a rehabilitation program. ..................................................... 62
18.y. Medical Disability Benefits .............................................................................................. 63
MedXPress
User Guide
Version 5.2
April 2024
4
2 Table of Figures
Figure 1 Request an Account Button .......................................................................................... 6
Figure 2 Request an Account Submenu ...................................................................................... 7
Figure 3 Request an Account Form ............................................................................................ 7
Figure 4 Request an Account -- Privacy Act Statement ................................................................. 8
Figure 5 Account Already Exists ................................................................................................. 8
Figure 6 Account Request Result Screen ..................................................................................... 8
Figure 7 Sample Registration Confirmation Email ......................................................................... 9
Figure 8 Privacy Act Statement ............................................................................................... 10
Figure 9 Change Temporary Password Screen ........................................................................... 11
Figure 10 Password Successfully Updated ................................................................................. 11
Figure 11 Existing User Login .................................................................................................. 12
Figure 12 Existing Account – Privacy Act Statement .................................................................... 12
Figure 13 Login Confirmation Screen Header ............................................................................. 13
Figure 14 Login Confirmation Screen ........................................................................................ 13
Figure 15 Home Menu ............................................................................................................ 13
Figure 16 Account Menu ......................................................................................................... 14
Figure 17 Help Menu .............................................................................................................. 14
Figure 18 Account Maintenance - Change your Password ............................................................ 12
Figure 19 Account Maintenance - Change Answers to Security Questions ...................................... 12
Figure 20 Request to Reset Password ....................................................................................... 13
Figure 21 Request to Reset Password - Security Questions ......................................................... 13
Figure 22 - Reset Password Confirmation .................................................................................. 14
Figure 23 Password Reset Notification Email ............................................................................. 15
Figure 24 Session Timeout Message ......................................................................................... 16
Figure 25 Start New Application .............................................................................................. 16
Figure 26 Continue Application ................................................................................................ 16
Figure 27 Exam Selection Question 1 ....................................................................................... 17
Figure 28 Exam Selection Question 2 ....................................................................................... 17
Figure 29 Exam Selection Question 3 ....................................................................................... 17
Figure 30 Pilot's Bill of Rights .................................................................................................. 18
Figure 31 Step-By-Step Sections ............................................................................................. 18
Figure 32 Navigation Options .................................................................................................. 19
Figure 33 Save Application Confirmation ................................................................................... 19
Figure 34 Cancel Application ................................................................................................... 20
Figure 35 Section Error Check ................................................................................................. 20
Figure 36 Additional Instruction ............................................................................................... 21
Figure 37 Help Cursor ............................................................................................................ 21
Figure 38 General Section ...................................................................................................... 21
Figure 39 General ATC Applicants and Incumbents .................................................................... 22
Figure 40 Demographics ......................................................................................................... 23
Figure 41 Prior Certification .................................................................................................... 26
Figure 42 Medications ............................................................................................................ 28
Figure 43 - Medication Exact Match Not Found .......................................................................... 29
Figure 44 Removing Medications ............................................................................................. 29
Figure 45 Medical History ....................................................................................................... 30
Figure 46 Medical Visits .......................................................................................................... 32
Figure 47 Medical History Records ........................................................................................... 33
Figure 48 Declaration and Submissions .................................................................................... 34
Figure 49 Validate and Submit ................................................................................................ 34
Figure 50 8500-8 Step-by-Step Submit Prompt ......................................................................... 35
Figure 51 Submission Confirmation .......................................................................................... 35
Figure 52 Application Summary (Items 1 to 17b) ....................................................................... 36
MedXPress
User Guide
Version 5.2
April 2024
5
Figure 53 Application Summary (Items 18 to 20)....................................................................... 37
Figure 54 Application Summary (Continuation Page) .................................................................. 38
Figure 55 Submission Confirmation Email ................................................................................. 39
Figure 56 Submission Confirmation and Expiration Date ............................................................. 39
Figure 57 Application Imported by AME into FAA System ............................................................ 39
Figure 58 Application Status tab .............................................................................................. 40
Figure 59 No Application submitted .......................................................................................... 40
Figure 60 Submitted Status .................................................................................................... 41
Figure 61 Imported Status...................................................................................................... 42
Figure 62 Transmitted Status .................................................................................................. 43
Figure 63 In Review Status ..................................................................................................... 44
Figure 64 In Review – FAS Consultant opinion .......................................................................... 45
Figure 65 In Review - After additional info/documents are received ............................................. 46
Figure 66 My Documents and FAA Correspondence Lists ............................................................. 47
Figure 67 Action Required - Initial Info requested ...................................................................... 48
Figure 68 Action Required - Additional Info needed .................................................................... 49
Figure 69 Action Required - Partial Info received ....................................................................... 50
Figure 70 In Transmitted status for more than 60 days .............................................................. 51
Figure 71 Certificate Decision - FAA Issues Certificate, after AME deferred ................................... 52
Figure 72 Certificate Decision – AME Issues Certificate ............................................................... 53
Figure 73 Certificate Decision – AME Denial .............................................................................. 54
Figure 74 Certificate Decision – FAA Denial ............................................................................... 55
Figure 75 Certificate Decision – Final Review ............................................................................. 56

MedXPress
User Guide
Version 5.2
April 2024
6
3 Introduction
FAA MedXPress is managed by the Office of Aerospace Medicine (OAM). OAM is
responsible for a broad range of medical programs and services both the domestic and
international aviation communities. Services provided by the OAM include:
●
Medical clearance of air traffic control specialist and other FAA employees
required to meet medical standards to perform safety-sensitive duties
●
Pilot medical certification
As such, OAM has the responsibility for collecting and maintaining any information
related to the medical conditions of pilots and certain covered positions within the FAA.
All airmen, air traffic controllers (ATCs) and certain other designated FAA employees
are required to have FAA Medical Certificates or Clearance. The process of applying
for an FAA Medical Certificate or Clearance requires completion of the OMB-
approved, FAA Medical History Form 8500-8, and performance of a medical
examination of the applicant by an FAA- designated Aviation Medical Examiner
(AME). The AME is a private physician who is approved by the FAA to perform this
function.
FAA MedXPress allows applicants to complete and submit their FAA Form 8500-8 on-
line. FAA MedXPress securely transmits the completed form and makes it available to a
designated AME to review at the time of the applicant’s medical examination.
3.1 The Medical Certification Process at a Glance
●
Connect to MedXPress at https://medxpress.faa.gov
●
Request an account or login using your existing account
●
Enter medical application data on the FAA 8500-8
●
Submit your application
●
Print the summary sheet
●
Give summary sheet with confirmation number to your AME
4 Request an Account
The first step in gaining access to the electronic medical form is to create a
MedXPress account. From the FAA MedXPress Login page, click the Request an
Account button to go to the Request an Account Screen.
Figure 1 Request an Account Button
Alternatively, you can click Account / Request an Account from the Menu Bar on
the FAA MedXPress Login Screen. This will also go to the Request an Account
Screen.

MedXPress
User Guide
Version 5.2
April 2024
7
Figure 2 Request an Account Submenu
4.1 Request an Account Form
On the Request an Account Screen, you will be presented with a Request an Account Form.
Complete the Form to request an FAA MedXPress account. An email containing your initial
password and instructions for completing the Account Request process will be sent to the
email address provided.
Complete the following steps to request an FAA MedXPress Account:
1.
Enter your Last Name, First Name, and Middle Name or initial (if applicable).
2.
Enter and confirm your email address. Take care to ensure the
email address entered is accurate, as the password you will need
to access the FAA MedXPress application will be emailed to you.
3.
Select three security questions and enter an answer for each
(you will be able to change the answers at any time). Select
questions and answers that you will readily remember. You
will be required to provide the correct responses to these
questions should you ever need to make inquiries related to
your FAA MedXPress account.
Figure 3 Request an Account Form
4.
Read the ‘Privacy Act Statement’ and, if you agree and
accept the terms, check the box.

MedXPress
User Guide
Version 5.2
April 2024
8
Figure 4 Request an Account -- Privacy Act Statement
5.
Click on the Submit button. If the account is created
successfully, you will see the Account Request Result Screen.
If the email address you provided is already associated with an account, you will receive an
error message indicating the account already exists. You can reset your password from the
MedXPress Login Screen by clicking the ‘Forgot your Password?’ link.
Figure 5 Account Already Exists
4.2 Account Request Result
The Account Request Result Screen confirms your account request is received and the next
steps in the process. You will be sent an email to the account provided with a temporary
password and instructions on how to complete the process.
Click the Return to Login button to return to the MedXPress Login Screen.
Figure 6 Account Request Result Screen

MedXPress
User Guide
Version 5.2
April 2024
9
4.3 Registration Confirmation
Wait a few minutes and log in to your email account. You should receive the message
shown below soon after submitting your information.
Figure 7 Sample Registration Confirmation Email
If you do not receive the message within a reasonable amount of time you can obtain the
temporary password by contacting:
Federal Aviation Administration (FAA)
MyIT Service Center
Email: helpdesk@faa.gov
1-844-FAA-MyIT (1-844-322-6948)
To complete the registration process, you must return to the MedXPress site and log in using
the account information provided in the email sent to you. You can return to the MedXPress
site by clicking on the link provided in the email. You will be taken to the Terms of Service
Agreement and Privacy Statement screen.
Enter your email address and the password provided in the appropriate fields and click the
Login button.
4.4 Privacy Act Statement
If you have read and accept the ‘Privacy Act Statement’, select the checkbox stating this
and click on the Submit button. You will be taken to the Change Password Screen.
It is required that your temporary password be changed when entering the site for the first
time.

MedXPress
User Guide
Version 5.2
April 2024
10
Figure 8 Privacy Act Statement
Click Close to return to the MedXPress Login Screen.
4.5 Change Password
You must change your password for one of the following reasons:
●
You are logging in to MedXPress with a temporary password
●
Your password is more than 365 days old
●
This is your first login since MedXPress introduced new password guidelines
on 07/01/2020
Enter a new password of your choice.
●
Passwords are case sensitive
●
Passwords must contain between 12 and 24 characters
●
Passwords must begin with a letter
●
No character may be repeated in sequence
●
Passwords must include four types of characters:
o
English upper case letter (A through Z)
o
English lower case letter (a through z)
o
Number (0 through 9)
o
Allowable special characters ! # $ %
●
Previous passwords cannot be reused

MedXPress
User Guide
Version 5.2
April 2024
11
Figure 9 Change Temporary Password Screen
Confirm the new password and click the Change Password button. A confirmation
message will be displayed stating that your password was successfully updated.
Figure 10 Password Successfully Updated
Press OK. You will be taken to the FAA MedXPress Login page.
5 Login
Log in to the MedXPress application using your confirmed email address and password. If you
do not have an account, you can Request an Account.

MedXPress
User Guide
Version 5.2
April 2024
12
Figure 11 Existing User Login
5.1 Privacy Act Statement
Read the Privacy Act Statement and accept the terms by selecting the checkbox at the
bottom of the screen. Click on the Submit button and the Login Confirmation Screen
will display.
Figure 12 Existing Account – Privacy Act Statement
5.2 Login Confirmation
The Login Confirmation Screen verifies that you are logged into MedXPress and can
complete the FAA Form 8500-8. Your logged-in username will be displayed in the upper-
right corner of the header along with the ‘Contact Us’ and ‘Log Out’ links.

MedXPress
User Guide
Version 5.2
April 2024
13
Figure 13 Login Confirmation Screen Header
Figure 14 Login Confirmation Screen
5.3 Home
The following options are available in the Home menu bar:
●
Home – Returns you to the Login Confirmation Screen from anywhere within
the MedXPress application
Figure 15 Home Menu
5.4 Account
The following options are available in the Account menu bar:
●
My Account - Displays the My Account Screen where you can update your
personal information, email address, password, or security answers
●
Log Out (Only available after successful login)– Logs you out of MedXPress and
returns the user to the login screen

MedXPress
User Guide
Version 5.2
April 2024
14
Figure 16 Account Menu
PLEASE NOTE: Each applicant must create and use their own account. Do not
enter your application information into someone else’s MedXPress account.
5.5 Help
The following options are available in the Help menu bar:
●
FAQ - Displays a list of questions and answers commonly asked about MedXPress
●
Contact Us - Displays contact information for the FAA MyIT Service Center that helps
with MedXPress account-related issues, logging in, account lockout, and related
issues
●
User Guide - Opens the MedXPress User Guide
●
Instructions (Only available after successful login) - Opens the Instructions
for Completion of the Application Form 8500-8.
Figure 17 Help Menu
6 Account Maintenance
If you would like to update your personal information or change your password, you can select
the Account / My Account at any time from the Menu Bar.
6.1 Update Account Information
To update your account information, click in the appropriate section and change the fields.
You will receive this message below the screen title when information in any section is
successfully changed: Account Updated Successfully.

MedXPress
User Guide
Version 5.2
April 2024
12
6.1.1 Update your Personal Information
If you update your First, Middle, or Last name, the same name will be displayed on the
Form 8500-8
●
To update your Personal Information, click the field and update to the
new value. To complete the change, enter and confirm your email
address.
●
Click the Submit button.
6.1.2 Change your Password
If you change your password, you will be logged out of the application and must sign in
again.
Passwords are case sensitive. Passwords must contain between 12 and 24 characters.
Passwords must begin with a letter. No character may be repeated in sequence.
Passwords must include four types of characters: English upper case letter (A through
Z); English lower case letter (a through z); Number (0 through 9); Allowable special
characters ! # $ %. Previous passwords cannot be reused.
Figure 18 Account Maintenance - Change your Password
6.1.3 Update your Security Question Answers
Your security question answers are used to identify you when resetting your password
or contacting the Help Desk.
●
Enter the new security question answers in their appropriate fields
●
Click the Submit button
Figure 19 Account Maintenance - Change Answers to Security Questions

MedXPress
User Guide
Version 5.2
April 2024
13
6.2 Forgot Password
If you forget your password, you can request a new password by clicking on Account /
Forgot Password from the menu bar or the “Forgot Password” link on the MedXPress Login
Screen.
The following steps will walk you through the process to change your password if you forgot
or cannot log into MedXPress. At any time, you can click the Cancel button to be returned to
the MedXPress Login Screen.
Step 1: Enter your email address in the box provided and click on the Next button.
Figure 20 Request to Reset Password
Step 2: Answer the security questions in the boxes provided and click on the Next
button.
Figure 21 Request to Reset Password - Security Questions

MedXPress
User Guide
Version 5.2
April 2024
14
Step 3: Your password has been reset. A temporary password and instructions for
completing the Password Reset process will be sent to your email account.
Figure 22 - Reset Password Confirmation
6.3 Password Reset Notification
Wait a few minutes and log in to your email account. You should receive the message
shown below soon after submitting your password reset request. If you do not receive the
message within a reasonable amount of time you can obtain the temporary password by
contacting:
Federal Aviation Administration (FAA)
MyIT Service Center
Email: helpdesk@faa.gov
1-844-FAA-MyIT (1-844-322-6948)
To complete the password reset process, you must return to the MedXPress site and log in
using the account information provided in the email sent to you. You can return to the
MedXPress site by clicking on the link provided in the email. You will be taken to the
Terms of Service Agreement and Privacy Statement screen.
Enter your email address and the password provided in the appropriate fields and click the
Login button. Once you have returned to the MedXPress site you will be required to change
your password on login.

MedXPress
User Guide
Version 5.2
April 2024
15
Figure 23 Password Reset Notification Email

MedXPress
User Guide
Version 5.2
April 2024
16
6.4 Session Timeout
The MedXPress times out after 20 minutes of inactivity. If a user allows MedXPress to sit idle
for 20 minutes or more, the session will time out and the user will be directed back to the
MedXPress login screen
On the 8500-8 screen of the MedXPress, the user will receive a warning message after 15
minutes of inactivity. If the user does not click on the Continue button on the session
timeout warning message within five minutes of receiving the message, the session will
time out. Once the session times out, any update or refresh action will send the user back
to the MedXPress Login screen.
Figure 24 Session Timeout Message
7 Accessing Form 8500-8
From the Login Confirmation Screen, the user will have the option to:
●
Start New Application – Displays the exam type selection screens
●
Continue Application – If the user has previously saved an application, displays
the 8500-8 Step-by-Step
Figure 25 Start New Application
Figure 26 Continue Application
8 Exam Type Selection
The exam type selection screens display a series of questions to determine the appropriate
form 8500-8 questions to display and complete for the applicable FAA Medical Clearance or
Certification. Accurate responses are essential to proper routing and processing of your
application.
The first question asks “Why are you applying for a Medical Certificate or Clearance?”. Select

MedXPress
User Guide
Version 5.2
April 2024
17
the response that best represents the reason for your application.
●
If “Required for my employment” option is selected, Question 2 for Exam
Type Selection will be presented.
●
If “All Other” option is selected, the “Pilot's Bill of Rights” will be presented followed
by the form 8500-8.
Figure 27 Exam Selection Question 1
The second question asks “Who is your employer?”. Select the response that best describes why
you are completing the application.
●
If “Non-government”, “Contract Company to FAA/DOT”, “Government Agency other
than FAA/DOT” is selected, the Pilot's Bill of Rights will be displayed followed by the
form 8500-8.
●
If “FAA/DOT” option is selected, Exam Selection Question 3 will be displayed.
●
If “Not yet employed by the FAA. I received a tentative offer letter from the FAA to
become an Air Traffic Controller” is selected; the FAA ATC Applicant Verification
Screen will be displayed.
Figure 28 Exam Selection Question 2
The third question asks FAA employees to select the purpose of their application. Select the
response that best describes why you are completing the application.
Figure 29 Exam Selection Question 3

MedXPress
User Guide
Version 5.2
April 2024
18
9 Pilot’s Bill of Rights
Applicants for medical certification will be required to read and accept the Pilot’s Bill of Rights
Notification before being allowed to proceed to the Form 8500-8 data entry screen.
Read the Pilot’s Bill or Rights Notification and accept by selecting the checkbox at the bottom of
the screen. Click on the Submit button and the Step-By-Step Form 8500-8 will display. Click
Back to return to the Exam Type Selection screen.
Figure 30 Pilot's Bill of Rights
10 Step-by-Step Form 8500-8
The Step-By-Step Form 8500-8 is a wizard-based format that breaks the form into smaller
sections with the ability to save and quickly navigate through different sections.
The FAA Form 8500-8 is broken down into the following sections
●
General (Items 1 - 2)
●
Demographics (Items 3 - 9)
●
Prior Certification (Items 10 - 16)
●
Medication (Items 17a and 17b)
●
Medical History (Item 18)
●
Medical Visits (Item 19)
●
Declarations (Item 20)
10.1 Navigation Breadcrumb
Figure 31 Step-By-Step Sections
10.2 Navigation Buttons

MedXPress
User Guide
Version 5.2
April 2024
19
To navigate between sections, use the navigation buttons below the screen in each section.
NAVIGATION
DESCRIPTION
Previous
Moves to the previous form section
Save and Complete
Later
Validates the on-screen fields
●
Saves the form, if no validation errors are found
Displays validation failures, if found (does not save the current
content)
Cancel My
Application
Cancelling an application is the same as deleting the application, all
data previously entered is lost. There is no way to retrieve this
information once you cancel
Check for Errors
Performs a validation check on the form fields
Displays validation failures, if applicable
Next
Validates the current section fields
●
Saves the form, if no validation errors are found and moves
to the next form section
If validation errors found, displays them to the user (does not
navigate to the next section)
Figure 32 Navigation Options
10.2.1 Save and Complete Later
Click the Save and Complete Later button to save changes to your application. Be sure
to save your entries before exiting FAA MedXPress. You may save a partially completed
form and return at a later time to finish. The following message will display when you click
on the Save and Complete Later button.
Figure 33 Save Application Confirmation

MedXPress
User Guide
Version 5.2
April 2024
20
10.2.2 Cancel My Application
If you have inadvertently selected the wrong type of exam from the Exam Type Selection
page, or if you have changed your mind and do not wish to submit an application at this
time, you can cancel the application at any time prior to submitting the application by
clicking on the Cancel My Application. A message will display asking you to confirm the
cancellation.
Figure 34 Cancel Application
Cancelling an application is the same as deleting the application, all data previously
entered is lost. There is no way to retrieve this information once you cancel the
application.
Click the Yes to cancel the application return to the Login Confirmation screen. Click No to
remain on the current application.
10.2.3 Check for Errors
Click the Check for Errors button at any time to display a list of validation errors.
Data must pass validation requirements before the application can be submitted.
Validation errors will appear at the top of the Form 8500-8 data entry screen.
Figure 35 Section Error Check

MedXPress
User Guide
Version 5.2
April 2024
21
10.3 Additional Instruction
Each section will have additional instruction to help the user accurately complete the
Form 8500-8. The additional instruction text will be accessible for each item by clicking on
any item row marked with a “+”.
Figure 36 Additional Instruction
The user will also be alerted to the additional instruction when moving their mouse over
those fields the cursor will change:
Figure 37 Help Cursor
10.4 General Section (Items 1 and 2)
The General section contains:
●
Item 1 Application For
●
Item 2 Class of Medical Certificate
NOTE: These Items are not required for FAA ATC Applicants and Incumbents.
Figure 38 General Section

MedXPress
User Guide
Version 5.2
April 2024
22
10.4.1 Item 1 Application For
Radio button to select Airmen Medical Certification or Airman Medical & Student Pilot
Certificate.
NOTE: Effective April 1, 2016, this office is no longer authorized to issue
Student Certificates.
Additional Instruction:
Select Airman Medical Certificate. (Effective April 1, 2016, this office is no longer
authorized to issue Student Certificates).
10.4.2 Item 2 Class of Medical Certificate
Radio button to select 1
st
, 2
nd
, or 3
rd
Class
Additional Instruction:
Select the appropriate class of medical certificate you want to apply for: See 14 CFR
§61.23 for the requirements for medical certificates.
10.4.3 Applicant ID
For FAA ATC Applicants and Incumbents this section (Items 1 and 2) would appear as in
the screen shot below. They will be required to provide the Applicant ID the very first
time and on subsequent visit the Applicant ID will be pre-filled.
Figure 39 General ATC Applicants and Incumbents

MedXPress
User Guide
Version 5.2
April 2024
23
10.5 Demographics Section (Items 3 - 9)
The Demographics section contains:
●
Item 3 Full Name
●
Item 4 Social Security Number
●
Item 5 Address
●
Item 6 Date of Birth
●
Item 7 Color of Hair
●
Item 8 Color of Eyes
●
Item 9 Sex
Figure 40 Demographics
MedXPress
User Guide
Version 5.2
April 2024
24
10.5.1 Item 3 Full Name
●
Text box to enter Last Name
●
Text box to enter First Name
●
Text box to enter Middle Name
●
Dropdown list to select Suffix
NOTE that your last, first, and middle name is populated exactly as it appears in
the Account -> My Account screen. Edits to your name must be made on the
My Account screen.
Additional Instruction:
Enter your legal name. If your name changed for any reason since the date of your
most recent medical examination, list your current legal name in the General
Explanations Pertaining to Medical History comment box (in the Medical History
section). See 14 CFR §61.25 for the requirements for a change of name.
10.5.2 Item 4 Social Security Number
●
Text box to enter social security number
●
International/Declined to Submit (A pseudo number will be generated by the
system). Check box to decline entering a social security number and have the
system generate a pseudo number.
Additional Instruction:
Entering your SSN is optional. Enter your SSN in the box provided, or select the
International/Declined to Submit checkbox if applicable.
10.5.3 Item 5 Address
●
Text box to enter Number/Street
●
Text box to enter City
●
Dropdown list to select State
●
Text Box to enter Zip Code
●
Text box to enter Telephone
Additional Instruction:
Enter your mailing address. Enter your telephone number. See 14 CFR §61.60 for
the requirements for change of address. Do not use punctuation.
MedXPress
User Guide
Version 5.2
April 2024
25
10.5.4 Item 6 Date of Birth
●
Dropdown list to select Month
●
Dropdown list to select Day
●
Dropdown list to select Year
●
Dropdown list to select Citizenship
Additional Instruction:
Select the month, day, and year of your date of birth. Select citizenship (e.g. United
States).
10.5.5 Item 7 Color of Hair
●
Dropdown list to select Color of Hair
Additional Instruction:
Specify hair color as bald, black, blond, brown, gray, or red by selecting the
appropriate value from the drop down box.
10.5.6 Item 8 Color of Eyes
●
Dropdown list to select Color of Eyes
Additional Instruction:
Specify actual eye color as black, blue, brown, green, gray, or hazel by selecting the
appropriate value from the drop down box.
10.5.7 Item 9 Sex
●
Radio button to select Male or Female
Additional Instruction:
Indicate male or female by selecting the appropriate radio button.
10.6 Prior Certification Section (Items 10 - 16)
The Prior Certification section contains:
●
Item 10 Type of Airman Certificate(s) You Hold
●
Item 11 Occupation
●
Item 12 Employer
●
Item 13 Has Your FAA Airman Medical Certificate Ever Been Denied, Suspended,
or Revoked.
●
Item 14 Total Pilot Time (Civilian Only) To Date
●
Item 15 Total Pilot Time (Civilian Only) Past 6 Months
●
Item 16 Date of Last FAA Medical Application

MedXPress
User Guide
Version 5.2
April 2024
26
Figure 41 Prior Certification
10.6.1 Item 10 Type of Airman Certificate(s) You Hold
●
Check box to select None, Airline Transport, ATC Specialist, Commercial, Flight
Engineer, Flight Instructor, Flight Navigator, Other, Private, Recreational,
Student
●
Textbox to enter Other if checkbox is selected
Additional Instruction:
Select the boxes that apply. If you select “Other,” indicate an Airman Certificate you
hold (e.g., Aircraft dispatcher, Ground Instructor).
10.6.2 Item 11 Occupation
●
Textbox to enter Occupation
Additional Instruction:
Enter your primary means of employment (e.g., pilot, air traffic controller, flight
instructor, teacher, etc.). Enter “pilot” only if you currently work as a pilot.
MedXPress
User Guide
Version 5.2
April 2024
27
10.6.3 Item 12 Employer
●
Textbox to enter Employer
Additional Instruction:
Enter your employer’s full name. Enter “self-employed” if applicable.
10.6.4 Item 13 Has Your FAA Airman Medical Certificate Ever
Been Denied, Suspended, or Revoked?
●
Radio button to select Yes or No
●
Textbox to enter date or Calendar control to select date
Additional Instruction:
Select Yes or No. If you select Yes, enter the date your certificate was denied,
suspended, or revoked.
10.6.5 Item 14 Total Pilot Time (Civilian Only) To Date
●
Textbox to enter Total Pilot Time to Date
Additional Instruction:
Enter your total number of flight hours. The flight hours you enter can be logged or
estimated.
10.6.6 Item 15 Total Pilot Time (Civilian Only) Past 6 Months
●
Textbox to enter Total Pilot Time to Past 6 Months
Additional Instruction:
Enter your total number of flight hours in the 6-month period immediately before
the date of this application. The flight hours you enter can be logged or
estimated.
10.6.7 Item 16 Date of Last FAA Medical Application
●
Textbox to enter date or Calendar control to select date
●
Checkbox to select No Prior Application
Additional Instruction:
Select the date of your most recent FAA medical examination. If this is your first-
ever application, select "No Prior Application".

MedXPress
User Guide
Version 5.2
April 2024
28
10.7 Medication Section (Items 17a and 17b)
The Prior Certification section contains:
●
Item 17a Do You Currently Use Any Medication (Prescription or Nonprescription)?
●
Item 17b Do You Ever Use Near Vision Contact Lenses While Flying?
NOTE: Item 17b is not required for FAA ATC Applicants.
Figure 42 Medications
10.7.1 Item 17a Do You Currently Use Any Medication (Prescription
or Nonprescription)?
●
Radio button to select Yes or No
●
Textbox to enter Medication Name
●
Textbox to enter Dosage
●
Dropdown list to select Dosage Unit
●
Dropdown list to select Frequency
●
Checkbox to select Previously Reported
Additional Instruction:
1.
Select Yes or No.

MedXPress
User Guide
Version 5.2
April 2024
29
●
You are required to enter ALL prescription and nonprescription medication
you take
●
You must enter the medication name; all other fields are optional.
2.
If you selected Yes
●
Enter the name of the first medication in the Medication Name box.
●
Enter the dosage amount in the Dosage box.
●
Select a dosage unit for your medication from the Dosage Unit box.
●
Select how often you use the medication from the Frequency box.
●
Select Previously Reported if you have previously reported the medication
on an FAA medical application.
●
Click the Add button
3.
If an exact match for the medication does not appear, you will see an
error message followed by a drop-down box of possible matches.
●
If you see the correct match, select it and click the Add button again.
●
If you do not see the correct match, select Could not Locate Medication
and click the Add button again.
4.
Repeat Steps 2 and 3 for each medication.
Figure 43 - Medication Exact Match Not Found
10.7.1.1 Removing Medications
Medication information can be deleted by clicking on the “Delete” link displayed to
the right of each medication listed.
Figure 44 Removing Medications
10.8 Medical History Section (Item 18)
The Medical History section contains:
●
Item 18 Medical History - Have you ever in your life been diagnosed with, had, or
do you presently have any of the following?

MedXPress
User Guide
Version 5.2
April 2024
30
Figure 45 Medical History

MedXPress
User Guide
Version 5.2
April 2024
31
10.8.1 Item 18 Have you ever in your life been diagnosed with, had,
or do you presently have any of the following?
10.8.1.1 Part 1
●
Description of each item (a-q, u, and x)
●
See Appendix B for additional instructions for each item (a-q, u, and x)
●
Radio button to select Yes or No
●
Textbox to enter Comments (only displayed if response is Yes)
Additional Instruction:
1.
Select Yes or No for each item (a-q, u, and x)
●
Select Yes for every condition you’ve had or have been diagnosed with
now or at any time in your life.
●
Select Yes for any condition already reported on a previous FAA
medical application.
●
Do not report occasional common illnesses such as colds or sore throats.
2.
Enter comments to explain each item you marked Yes.
●
Describe the condition as required in the 8500-8 Instructions.
●
Your comment must include a description of the condition and include
the approximate date of diagnosis/occurrence.
●
Indicate whether you are taking medication (and any medication side
effects) and whether you have had any hospital visits or surgery
related to any item.
10.8.1.2 Part 2
●
Description of each item (r-t and y)
●
Radio button to select Yes or No
●
Textbox to enter Comments (only displayed if response is Yes)
Additional Instruction:
1.
Select Yes or No for each Item (r-t and y)
●
Select Yes for every item that applies to you.
●
Select Yes for any item already reported on a previous FAA
medical application.
2.
Enter Comments to explain each item you marked Yes.
●
Describe the condition as required in the 8500-8 Instructions.
●
Your comment must include a description of the situation, and include
the approximate date of occurrence.
10.8.1.3 Part 3
●
Description of each item (v-w)
●
See Appendix B for additional instructions for item v.
●
Radio button to select Yes or No
●
Textbox to enter Comments (only displayed if response is Yes)
Additional Instruction:
1.
Select Yes or No for each Item (v-w).
●
Select Yes for every item that applies to you.

MedXPress
User Guide
Version 5.2
April 2024
32
●
Select Yes for any item already reported on a previous FAA
medical application.
2.
Enter comments to explain each item you marked Yes.
●
Describe the situation as required in the 8500-8 Instructions.
●
Your comment must include: the offense, the name of the state or
other jurisdiction involved, and the date of occurrence.
10.9 Medical Visits Section (Item 19)
The Medical Visits section contains:
●
Item 19 Have you visited any health professionals within the last 3 years?
Figure 46 Medical Visits
10.9.1 Item 19 Have you visited any health professionals within
the last 3 years?
●
Radio button to select Yes or No
●
Textbox to enter date (MM/YYYY) or Calendar control to select date
●
Textbox to enter Name
●
Textbox to enter Type of Professional
●
Textbox to enter Reason

MedXPress
User Guide
Version 5.2
April 2024
33
●
Textbox to enter Number/Street
●
Textbox to enter City
●
Dropdown list to select State
●
Textbox to enter Zip Code
●
Dropdown list to select Country
Additional Instruction:
1.
Select Yes or No
●
You are required to enter ALL visits to any health professionals (such as a
physician, physician assistant, nurse practitioner, psychologist, psychiatrist,
chiropractor, clinical social worker, or substance abuse specialist, including
an EAP employer-sponsored specialist) for treatment, examination, or
medical/mental evaluation.
●
Multiple visits to one health professional for the same condition may be
aggregated on one line (you may use the most recent date in the date
field).
●
You do not need to enter routine dental and eye examinations or periodic
FAA medical examinations and visits to health professionals related to an
Authorization for Special Issuance.
2.
If you selected Yes
●
Enter the month and year in the Date of Visit box
●
Enter health professional’s name in the Name box
●
Enter the type of professional in the Type of Professional box
●
Enter the reason in the Reason box
●
Enter the health professional’s address in the address boxes
●
Click the Add button
3.
Repeat Step 2 to add all your visits to health professionals.
Figure 47 Medical History Records
10.10 Declarations Section
This section covers the Applicant’s National Driver Register and Certifying Declarations. This
is a statement certifying that all reported answers are correct and that the National Driver
Register may access information pertaining to your driving record.

MedXPress
User Guide
Version 5.2
April 2024
34
Figure 48 Declaration and Submissions
10.10.1 Item 20 Applicant's National Driver Register
and Certifying Declarations:
•
Radio button to select Yes or No
11 Validate and Submit Application
Figure 49 Validate and Submit
12 Submit My Application
If you are sure all of the information entered is correct, click the Submit My Application
button and enter your password when prompted. If there are any errors, they will be shown
after clicking Submit My Application and you will be able to correct them.

MedXPress
User Guide
Version 5.2
April 2024
35
Figure 50 8500-8 Step-by-Step Submit Prompt
***IMPORTANT*** Once you submit your application, you will not be able to make any
changes to it.
13 Application Successfully Submitted
If there are no errors, you will be taken to the Submission Confirmation Screen that tells you
your application has been successfully submitted. The screen displays your confirmation number
and gives you the option of downloading the completed application.
Figure 51 Submission Confirmation
Write down the confirmation number. If you do not wish to view the Completed Application,
click on the Logout link or Account / Log Out to exit to the MedXPress Login Screen.

MedXPress
User Guide
Version 5.2
April 2024
36
You will receive a Form 8500-8 confirmation email that will also provide your confirmation
number. If you lose your confirmation number, you can obtain it by logging back into
MedXPress and clicking on the “Form 8500-8” link that will take you to the Submission
Confirmation Screen or by contacting:
Federal Aviation Administration (FAA)
MyIT Service Center
Email: helpdesk@faa.gov
1-844-FAA-MyIT (1-844-322-6948)
14 Application Summary (Items 1 to 17b)
The application summary displays the information you entered into the Form 8500-8. It is
recommended that you print the Summary for review and take it to your exam.
Figure 52 Application Summary (Items 1 to 17b)

MedXPress
User Guide
Version 5.2
April 2024
37
15 Application Summary (Items 18 to 20)
Figure 53 Application Summary (Items 18 to 20)
16 Application Summary (Continuation Page)
The Summary also captures the Confirmation Number, Date/Time the form was submitted, and
the IP Address from which the application was submitted. The Continuation Sheet contains
comments and medication information that did not fit on the first page of the 8500-8.

MedXPress
User Guide
Version 5.2
April 2024
38
Figure 54 Application Summary (Continuation Page)
17 Application Submission Confirmation Email
You should receive the following confirmation email after you submit your application. It
displays your confirmation number. You will need this number in order for your AME to view
your application so either write the confirmation number down or print a copy of the email to
take with you.
If you lose your confirmation number, you can obtain it by logging back into MedXPress and
clicking on the “form 8500-8” link that will take you back to the saved Form 8500-8 data
entry screen with your confirmation number displayed at the top of the screen or by
contacting:
Federal Aviation Administration (FAA)
MyIT Service Center
Email: helpdesk@faa.gov
1-844-FAA-MyIT (1-844-322-6948)

MedXPress
User Guide
Version 5.2
April 2024
39
Figure 55 Submission Confirmation Email
18 Viewing Confirmation after Submission
Once you have submitted your application, you will not be able to make any changes to it. You
will see the following message when you try to access the Form 8500-8 data entry screen until
the AME imports your application.
Figure 56 Submission Confirmation and Expiration Date
After your application is imported, you will see the following message, indicating that your AME
imported the application and a new application cannot be created.
Figure 57 Application Imported by AME into FAA System

MedXPress
User Guide
Version 5.2
April 2024
40
19 Creating a New Application After Submission
Once the AME submits your application to the FAA, you will be able to create a new application
(only available after successful login).
20. Application Status
Once the MedXPress applicant has at least one application in progress then the ‘Application
Status’ tab is displayed on the top navigation. Application Status tab always displays the status
of the most recent application of the MedXPress user.
Figure 58 Application Status tab
20.1 No Application Submitted
The application status tab displays below information when the user has started filling the
application (accepted the 'Pilot's Bill of Rights Written Notification’ statement) but has not
submitted application yet.
Figure 59 No Application submitted

MedXPress
User Guide
Version 5.2
April 2024
41
20.2 Submitted
The application status displays as ‘Submitted’ when the application is submitted and is waiting
for the AME’s review.
Figure 60 Submitted Status

MedXPress
User Guide
Version 5.2
April 2024
42
20.3 Imported
The application status displays as ‘Imported’ when the AME has imported the application.
Figure 61 Imported Status

MedXPress
User Guide
Version 5.2
April 2024
43
20.4 Transmitted
The application status displays the status as ‘Transmitted’ if the AME defers the application to
the FAA for further review.
Figure 62 Transmitted Status

MedXPress
User Guide
Version 5.2
April 2024
44
20.5 In Review
The application status displays as ‘In Review’ when the FAA begins reviewing a deferred
application. The informational text will change depending on the status of the application.
Figure 63 In Review Status

MedXPress
User Guide
Version 5.2
April 2024
45
Figure 64 In Review – FAS Consultant opinion

MedXPress
User Guide
Version 5.2
April 2024
46
Figure 65 In Review - After additional info/documents are received

MedXPress
User Guide
Version 5.2
April 2024
47
Clicking ‘My Document List’ will expand a list of documentation provide in support of medical
certification. ‘FAA Correspondence List’ displays a list of correspondence sent to you by the
FAA in regard to this application.
Figure 66 My Documents and FAA Correspondence Lists
MedXPress
User Guide
Version 5.2
April 2024
48
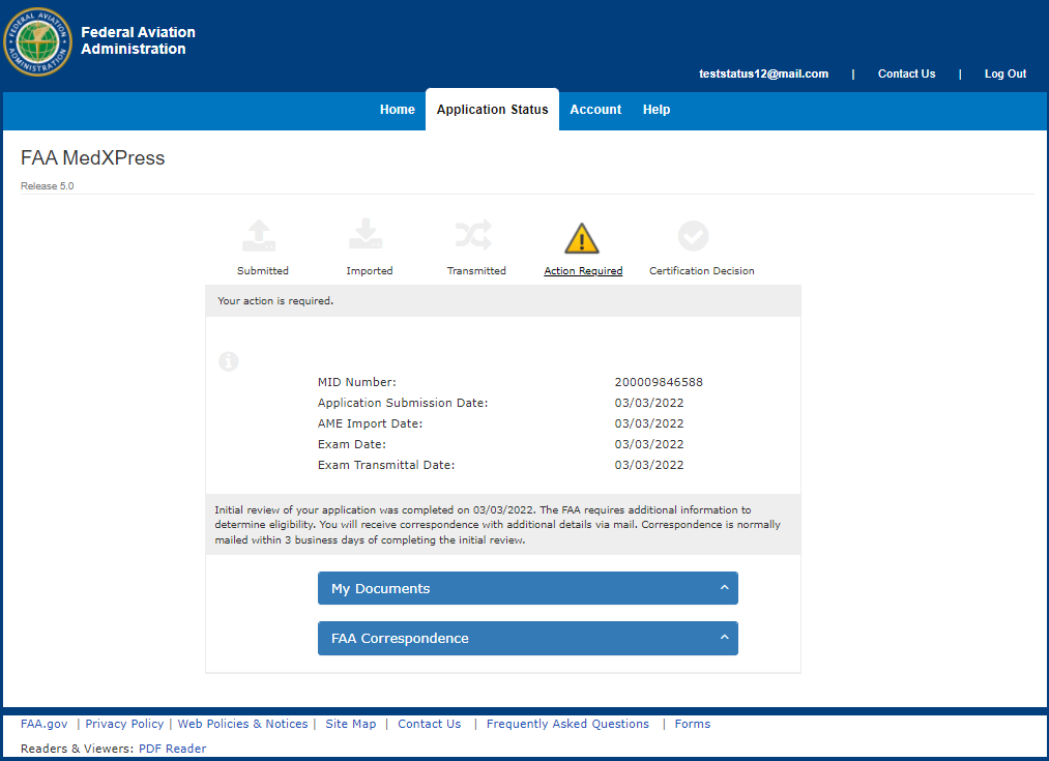
20.6 Action Required
The application status displays as ‘Action Required’ when the FAA requests more information.
The informational text will update depending on the type of request.
Figure 67 Action Required - Initial Info requested

MedXPress
User Guide
Version 5.2
April 2024
49
Figure 68 Action Required - Additional Info needed

MedXPress
User Guide
Version 5.2
April 2024
50
Figure 69 Action Required - Partial Info received

MedXPress
User Guide
Version 5.2
April 2024
51
20.7 Transmitted Status – No Activity for More Than 60 Days
The application status will display a warning if FAA review of a deferred application is not
initiated within 60 days.
Figure 70 In Transmitted status for more than 60 days

MedXPress
User Guide
Version 5.2
April 2024
52
20.8 Certificate Decision – Medical Certificate Issued
The application status displays a green checkmark and the medical certificate information
when the AME or the FAA issues a medical certificate. The informational text will vary
depending on the type of determination.
Figure 71 Certificate Decision - FAA Issues Certificate, after AME deferred

MedXPress
User Guide
Version 5.2
April 2024
53
Figure 72 Certificate Decision – AME Issues Certificate

MedXPress
User Guide
Version 5.2
April 2024
54
20.9 Certification Decision – Denial, Disqualification, Withdrawal
The application status displays a ‘STOP’ sign on the Certificate Decision when the AME denies
and/or the FAA withdraws, disqualifies, or denies medical certification.
Figure 73 Certificate Decision – AME Denial

MedXPress
User Guide
Version 5.2
April 2024
55
Figure 74 Certificate Decision – FAA Denial

MedXPress
User Guide
Version 5.2
April 2024
56
20.10 Certificate Decision - Final Review
The application status displays ‘Final Review’ when the FAA’s certification decision is being finalized.
Figure 75 Certificate Decision – Final Review
MedXPress
User Guide
Version 5.2
April 2024
4
57
Appendix A: Instructions for Completion of the Application for Airman
Medical Certificate, FAA Form 8500-8
Applicant must fill in completely numbers 1 through 20 of the application. The following
numbered instructions apply to the numbered headings on the application form that follows this
page.
NOTICE – Intentional falsification may result in federal criminal prosecution. Intentional
falsification may also result in suspension or revocation of all airman, ground instructor, and
medical certificates and ratings held by you, as well as denial of this application for medical
certification.
1.
APPLICATION FOR – Check the appropriate box.
2.
CLASS OF AIRMAN MEDICAL CERTIFICATE APPLIED FOR – Check the appropriate box
for the class of airman medical certificate for which you are making application.
3.
FULL NAME – If your name has changed for any reason, list current name on the
application and list any former name(s) in the EXPLANATIONS box of number 18 on the
application.
4.
SOCIAL SECURITY NUMBER – The social security number is optional; however, its use
as a unique identifier does eliminate mistakes.
5.
ADDRESS – Give permanent mailing address and country. Include your complete nine
digit ZIP code if known. Provide your current area code and telephone number.
6.
DATE OF BIRTH – Specify month (MM), day (DD), and year (YYYY) in numerals; e.g.,
01/31/1950. Indicate citizenship; e.g., U.S.A.
7.
COLOR OF HAIR – Specify as brown, black, blond, gray or red. If bald, so state. Do not
abbreviate.
8.
COLOR OF EYES – Specify actual eye color as brown, black, blue, hazel, gray or green.
Do not abbreviate.
9.
SEX – Indicate male or female.
10.
TYPE OF AIRMAN CERTIFICATE(S) YOU HOLD – Check applicable block(s). If “Other” is
checked, provide name of certificate.
11.
OCCUPATION – Indicate major employment. “Pilot” will be used only for those gaining
their livelihood by flying.
12.
EMPLOYER – Provide your employer’s full name. If self-employed, so state.
13.
HAS YOUR FAA AIRMAN MEDICAL CERTIFICATE EVER BEEN DENIED, SUSPENDED, OR
REVOKED – If “yes” is checked, give month and year of action in numerals.
14.
TOTAL PILOT TIME TO DATE – Give total number of civilian flight hours. Indicate
whether logged or estimated. Abbreviate as Log. or Est.
15.
TOTAL PILOT TIME PAST 6 MONTHS – Give number of civilian flight hours in the 6-
month period immediately preceding date of this application. Indicate whether logged or
estimated. Abbreviate as Log. or Est.
MedXPress
User Guide
Version 5.2
April 2024
4
58
16.
MONTH AND YEAR OF LAST FAA MEDICAL EXAMINATION – Give month and year in
numerals. If none, so state.
17.
DO YOU CURRENTLY USE ANY MEDICATION (Prescription or Nonprescription) –
a) Check “yes” or “no.” If “yes” is checked, give name of medication(s) and indicate
if the medication was listed in a previous FAA medical examination. See NOTE
below.
b) Indicate whether you use near vision contact lens(es) while flying.
18.
MEDICAL HISTORY – Each item under this heading must be checked either “yes” or
“no.” You must answer “yes” for every condition you have ever been diagnosed with, had,
or presently have and describe the condition and approximate date in the EXPLANATIONS
block.
If information has been reported on a previous application for airman medical certificate and
there has been no change in your condition, you may note “PREVIOUSLY REPORTED, NO
CHANGE” in the EXPLANATIONS box, but you must still check “yes” to the condition. Do not
report occasional common illnesses such as colds or sore throats.
“Substance dependence” is defined by any of the following: increased tolerance; withdrawal
symptoms; impaired control of use; or continued use despite damage to health or impairment
of social, personal, or occupational functioning. “Substance abuse” includes the following: use
of an illegal substance; use of a substance or substances in situations in which such use is
physically hazardous; or misuse of a substance when such misuse has impaired health or
social or occupational functioning. “Substances” include alcohol, PCP, marijuana, cocaine,
amphetamines, barbiturates, opiates, and other psychoactive chemicals.
Arrest, Conviction and/or Administrative Action History – Letter (v) of this subheading asks if
you have ever been: (1) arrested and/or convicted (which may include paying a fine, or
forfeiting bond or collateral) of an offense involving driving while intoxicated by, while
impaired by, or while under the influence of alcohol or a drug; or (2) arrested, convicted
and/or subject to an administrative action by a state or other jurisdiction for an offense for
which your license was denied, suspended, cancelled, or revoked or which resulted in
attendance at an educational or rehabilitation program. Individual traffic arrests and/or
convictions are not required to be reported if they did not involve: alcohol or a drug;
suspension, revocation, cancellation, or denial of driving privileges; or attendance at an
educational or rehabilitation program. If “yes” is checked, a description of the arrest(s),
and/or conviction(s), and/or administrative action(s) must be given in the EXPLANATIONS
box. The description must include: (1) the alcohol or drug offense for which you were arrested
and/or convicted or the type of administrative action involved (e.g., attendance at an alcohol
treatment program in lieu of conviction; license denial, suspension, cancellation, or revocation
for refusal to be tested; educational safe driving program for multiple speeding arrests and/or
convictions, etc.); (2) the name of the state or other jurisdiction involved; and (3) the date of
the arrest(s), and/or convictions and/or administrative action(s). The FAA may check state
motor vehicle driving licensing records to verify your responses. Letter (w) of this subheading
asks if you have ever had any other (nontraffic) convictions (e.g., assault, battery, public
intoxication, robbery, etc.). If so, name the charge for which you were convicted and the date
of the conviction in the EXPLANATIONS box. See NOTE below.
MedXPress
User Guide
Version 5.2
April 2024
4
59
19.
VISITS TO HEALTH PROFESSIONAL WITHIN LAST 3 YEARS – List all visits in the last 3
years to a physician, physician assistant, nurse practitioner, psychologist, clinical social
worker, or substance abuse specialist for treatment, examination, or medical/mental
evaluation. List visits for counseling only if related to a personal substance abuse or
psychiatric condition. Give date, name, address, and type of health professional consulted
and briefly state reason for consultation. Multiple visits to one health professional for the
same condition may be aggregated on one line. Routine dental, eye and FAA periodic
medical examinations and consultations with your employer-sponsored employee
assistance program (EAP) may be excluded unless the consultations were for your
substance abuse or unless the consultations resulted in referral for psychiatric evaluation
or treatment. See NOTE below.
20.
APPLICANT’S DECLARATION – Two declarations are contained under this heading. The
first authorizes the National Driver Register to release adverse driver history information,
if any, about the applicant to the FAA. The second certifies the completeness and
truthfulness of the applicant’s responses on the medical application. The declaration
section must be signed and dated by the applicant after the applicant has read it.
Appendix B: Additional Instructions (available by expanding applicable
8500-8 Items)
1.
Application For
Select Airman Medical Certificate. (Effective April 1, 2016, AAM is no longer authorized to issue
Student Pilot Certificate.)
2.
Class of Medical Certificate Applied For
Select the appropriate class of medical certificate that you want to apply for. See 14 CFR §61.23 for
the requirements for medical certificates.
3.
Full Name
Enter your legal name. If your name changed for any reason since the date of your most recent
medical examination, list your current legal name in the General Explanations Pertaining to Medical
History comment box (in the Medical History section.) See 14 CFR § 61.25 for the requirements for
change of name.
4.
Social Security Number
Entering your SSN is optional. Enter your SSN in the box provided, or select the
International/Declined to Submit checkbox if applicable.
5.
Address
Enter your mailing address. Enter your telephone number. See 14 CFR § 61.60 for the
requirements for change of address. Do not use punctuation.
6.
Date of Birth
Select the month, day, and year of your date of birth. Select citizenship (e.g. United States).
7.
Color of Hair
Specify hair color as bald, black, blond, brown, gray, or red by selecting the appropriate value from
the drop down box.
8.
Color of Eyes
Specify actual eye color as black, blue, brown, green, gray, or hazel by selecting the appropriate
value from the drop down box.
9.
Sex
Indicate male or female by selecting the appropriate radio button.
MedXPress
User Guide
Version 5.2
April 2024
4
60
10.
Type of Airman Certificate(s) You Hold
Select the boxes that apply. If you select None, that should be the only box you select. If you select
Other, indicate an Airman Certificate (not represented) that you may hold (e.g. Aircraft dispatcher,
Ground Instructor).
11.
Occupation
Enter your primary means of employment (e.g. pilot, air traffic controller, flight instructor, teacher,
etc.). Enter “pilot” only if you currently work as a pilot.
12.
Employer
Enter your employer’s full name. Enter “self-employed” if applicable.
13.
Has Your FAA Airman Medical Certificate Ever Been Denied, Suspended, or Revoked?
Select Yes or No. If you select Yes, enter the date your certificate was denied, suspended, or
revoked.
14.
Total Pilot Time (Civilian Only) to Date
Enter your total number of flight hours. The flight hours you enter can be logged or estimated.
15.
Total Pilot Time (Civilian Only) Past 6 Months
Enter your total number of flight hours in the 6-month period immediately before the date of this
application. The flight hours you enter can be logged or estimated.
16.
Date of Last FAA Medical Application
Select the date of your most recent FAA medical examination. If this is your first-ever application,
select “No Prior Application.”
17.
Medication Section (Items 17a and 17b)
17.a. Do You Currently Use Any Medication (Prescription or Nonprescription)?
1. Select Yes or No.
-You are required to enter ALL prescription and nonprescription medication you take.
-You must enter the medication name; all other fields are optional.
2. If you selected Yes
-Enter the name of the first medication in the Medication Name box.
-Enter the dosage amount in the Dosage box.
-Select a dosage unit for your medication from the Dosage Unit box.
-Select how often you use the medication from the Frequency box.
-Select Previously Reported if you have previously reported the medication on an FAA
medical application.
-Click the Add button
3. If an exact match for the medication does not appear, you will see an error message
followed by a drop-down box of possible matches.
-If you see the correct match, select it and click the Add button again.
-If you do not see the correct match, select Could not Locate Medication and click the Add
button again.
4. Repeat Steps 2 and 3 for each medication.
17.b. Do You Ever Use Near Vision Contact Lens(es) While Flying?
Do you use a contact lens in either eye for near vision? (for example: for reading or close up
work)
18.
Medical History Section (Item 18)
18.a. Frequent or severe headaches
For example: Chronic (daily or weekly) headaches, headaches that have required medical
MedXPress
User Guide
Version 5.2
April 2024
4
61
treatment, migraine headaches, cluster headaches, or headaches associated with visual or
neurological symptoms.
18.b. Dizziness or fainting spell
For example: Frequent spinning or lightheadedness; other factors associated with episodes of
dizziness or fainting, such as headache, nausea, loss of consciousness, tingling, numbness,
vertigo.
18.c. Unconsciousness for any reason
For example: Unconsciousness, no matter how short, whether explained or unexplained.
18.d. Eye or vision trouble except glasses
For example: Unusual visual experiences (halos, wavy lines, etc.), sensitivity to light, eye
injury, loss of vision, vision discomfort, eye surgery.
18.e. Hay fever or allergy
For example: Chronic or seasonal allergies controlled by allergy shots and/or medication,
nasal allergies, nasal obstruction, sinus block, sinusitis.
18.f. Asthma or lung disease
For example: Asthma attacks; use of an inhaler; COPD; chronic bronchitis; emphysema;
fistula; fungal disease; pleurisy; pneumothorax; pulmonary embolism; pulmonary fibrosis;
chest surgery; tumor(s).
18.g. Heart or vascular trouble
For example: Angina, heart pain, coronary heart disease, heart attack, myocardial infarction,
abnormal rhythm, atrial fibrillation, cardioversion, cardiac failure, congestive heart failure,
heart enlargement, cardiac decompensation, hypertrophy or dilation of the heart, pulmonary
hypertension, heart valve disease, heart valve repair or replacement, pacemaker, anti-
tachycardia device, implantable defibrillator, congenital heart disease, endocarditis, heart
inflammation, pericarditis or heart transplant.
18.h. High or low blood pressure
For example: Diagnosis of high or low blood pressure, whether treated or not; use of blood
pressure medication of any kind.
18.i. Stomach, liver, or intestinal trouble
For example: Appendicitis, bleeding ulcer, bowel obstruction, cancer, Crohn's disease, chronic
hepatitis, cirrhosis, colostomy, irritable bowel syndrome, hernia, ulcerative colitis, any
surgery.
18.j. Kidney stone or blood in urine
For example: Kidney stone, kidney cancer, kidney transplant, blood in urine, chronic recurrent
urinary tract infections, urinating frequently at night.
18.k. Diabetes
For example: Pre-diabetes, type I diabetes, or type II diabetes treated with insulin,
medication (oral or injectable), and/or diet and exercise.
18.l. Neurological disorders: epilepsy, seizures, stroke, paralysis, etc.
Also, muscle weakness, disturbance of sensation, disturbance of consciousness, loss of
coordination, head injury, concussion.
18.m. Mental disorders of any sort: depression, anxiety, etc.
Also, attention deficit disorder, attention deficit hyperactivity disorder, bipolar disorder,
obsessive compulsive disorder, panic attacks, personality disorder, post-traumatic stress
disorder, psychosis.
MedXPress
User Guide
Version 5.2
April 2024
4
62
18.n. Substance dependence or failed a drug test ever; or substance abuse or use of illegal substance
in the last 2 years.
For example: Select Yes if you have been diagnosed and/or treated in an inpatient or
outpatient setting for substance use. Select Yes if you ever had a diagnosis of substance use
disorder. Select Yes for any and all positive drug tests whether administered at the federal,
state, or local level, or by a private employer. For a detailed description of substance,
substance dependence, substance abuse, and drug and alcohol testing, refer to 14 CFR
§67.107, §67.207, and §67.307, paragraphs (a)(4) and (b).
18.o. Alcohol dependence or abuse
For example: Select Yes if you have been diagnosed and/or treated in an inpatient or
outpatient setting for misuse of alcohol. Select Yes if you ever had a diagnosis of alcohol use
disorder. Select Yes for any and all positive alcohol tests whether administered at the federal,
state, or local level, or by a private employer. For a detailed description of substance,
substance dependence, substance abuse, and drug and alcohol testing, refer to 14 CFR
§67.107, §67.207, and §67.307, paragraphs (a)(4) and (b).
18.p. Suicide attempt
For example: Thoughts of suicide, attempted suicide.
18.q. Motion sickness requiring medication
For example: Unresolved, chronic motion sickness (in flight while traveling by other
vehicle) for which you must be medicated.
18.r. Military medical discharge
No Additional Instructions
18.s. Medical rejection by military service
No Additional Instructions
18.t. Rejection for life or health insurance
No Additional Instructions
18.u. Admission to hospital
List any hospitalization(s) not already reported in the APPLICANT EXPLANATION box in
relation to items 18a-y.
18.x. Other illness, disability, or surgery
List any illness/illnesses or disability/disabilities not provided for in 18a-y..
18.y. Medical disability benefits
For example: Veterans Affairs (VA), Social Security Disability Insurance (SSDI),
workers' compensation, and any other disability benefits.
18.v. History of (1) any arrest(s) and/or conviction(s) involving driving while intoxicated by, while
impaired by, or while under the influence of alcohol or a drug; or (2) history of any arrest(s), and/or
conviction(s), and/or administrative action(s) involving an offense(s) which resulted in the denial,
suspension, cancellation, or revocation of driving privileges or which resulted in attendance at an
MedXPress
User Guide
Version 5.2
April 2024
4
63
educational or a rehabilitation program.
For purposes of this application:
"Arrest" means being detained or taken into custody by any law enforcement or
military authority for any reason related to a driving stop for suspected driving while
intoxicated by, while impaired by, or under the influence of drugs or alcohol. List, for
each arrest, the place, date, and circumstance (s) of the arrest.
"Conviction" means any judgment of guilt based on a jury, court, or military verdict, a
plea of guilty, or a plea of nolo contendere/no contest. Examples include, but are not
limited to, assault, battery, disorderly conduct, domestic violence, driving under the
influence, driving while intoxicated, murder, possession of drugs, public intoxication,
reckless driving, etc. If you answer yes, you should report all misdemeanors and
felony convictions regardless of the classification of the conviction and regardless of
whether the conviction is pending on appeal to another court. List the charge(s) for
which you were convicted, the date of the conviction, and the state, federal, military,
or foreign court in which you were convicted. If a conviction has been reversed or
vacated in a final judgment, state the date of the final judgment and the court that
issued the final judgment. If the record of a conviction has been expunged, state the
date that the record was expunged and the court that ordered the expunction.
List, for each denial, suspension, cancellation, or revocation of your driver's license or
driving privileges, the U.S. state, U.S. military base, or foreign country where the
action occurred, the specific type of action taken (for example, the driver's license was
denied, suspended, cancelled, or revoked, the date each action was taken, and the
basis for the action.) Examples of educational or rehabilitation programs include, but
are not limited to, anger management program(s), drug or alcohol treatment
program(s), safe driving course(s), etc. List the type of educational or rehabilitation
program you were required to attend as part of a criminal, civil, or military action, the
entity that required you to attend, and the date(s) and place(s) of your attendance.
18.y. Medical Disability Benefits
For example: Veterans Affairs (VA), Social Security Disability Insurance (SSDI), workers’
compensation, and any other disability benefits
19. Have you visited any health professionals within the last 3 years?
1. Select Yes or No
-You are required to enter ALL visits to any health professionals (such as physician,
physician assistant, nurse practitioner, psychologist, psychiatrist, chiropractor,
clinical social worker, or substance abuse specialist, including an EAP employer-
sponsored specialist) for treatment, examination, or medical/mental evaluation.
-Multiple visits to one health professional for the same condition may be
aggregated on one line (you may use the most recent date in the date field).
-You do not need to enter routine dental and eye examinations or periodic FAA
medical examinations and visits to health professionals related to an Authorization
for Special Issuance.
2. If you selected Yes
-Enter the month and year in the Date of Visit box
-Enter health professional’s name in the Name box
-Enter the type of professional in the Type of Professional box
-Enter the reason in the Reason box
-Enter the health professional’s address in the address boxes
-Click the Add button
3. Repeat Step 2 to add all your visits to health professionals.
MedXPress
User Guide
Version 5.2
April 2024
4
64
20. Applicant’s National Driver Register and Certifying Declarations
No Additional Instructions
