PREDECISIONAL
1
Missouri Department of Social Services
Rapid Response Review –
Assessment of Missouri Medicaid Program
FINAL REPORT
February 11, 2019
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
2
Contents
Executive Summary 3
Overview of Medicaid Program 7
The Current Program 7
Major Industry Trends Affecting the Program 11
Projected Spending Without Significant Course Corrections 13
Opportunities and Potential Initiatives 16
Acute Care Services 17
Long-Term Services and Supports 43
Pharmacy 57
Managed Care 62
Program Integrity 73
Federal Financing 79
Medicaid Management Information System (MMIS) 83
Operations 93
Implementation Considerations 110
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
3
Executive Summary
Missouri’s Medicaid program is an important safety net for Missouri’s most vulnerable
populations, providing health care and support for activities of daily living for nearly one million
Missourians. Children in low-income families comprise 63.5% of participants, while persons with
disabilities comprise the largest share (46%) of spending. In State Fiscal Year (SFY) 2018, total
spending for the program was approximately $10 billion, funded 53% by federal funds, 21% by
state general revenues, and the balance by provider taxes and other funds.
Analysis of historical trends indicates that the financial sustainability of Missouri’s Medicaid
program is currently under pressure: Medicaid spending has grown from 17% of state general
revenues in SFY2009 to 24% in SFY2018. Based on continuation of these trends, spending
could grow to 26% by SFY2023. This number could be even higher (30%) if Missouri were to
experience an economic downturn, given the potential for such a downturn to increase Medicaid
enrollment while also reducing growth in state general revenues.
Under any of the scenarios described in the pages that follow, significant changes in the
structure and performance of Missouri’s Medicaid program would be necessary to bring
Medicaid spending growth in line with projected economic growth of the state.
Opportunities for Improvement
Since October, a detailed assessment of the Missouri Medicaid program has uncovered a wide
range of opportunities for improvement, which may collectively deliver substantial reductions in
the rate of growth of Medicaid spending. These opportunities, detailed in the pages that follow,
are based on extensive interviews with state agency leaders and staff, detailed analysis of
claims- and non-claims data, review of agency operations, and benchmarking against other
states as well as Medicaid managed care organizations (MCOs) and other health insurers.
High-level summaries are provided below for each of eight programmatic and functional areas.
Further details follow in the report, including descriptions of opportunities (with supporting facts)
and potential initiatives that may be considered by the state in shaping its approach to Medicaid
transformation. Potential initiatives include possible changes to provider payment methods, care
management, and contracting with MCOs and other vendors, as well as improvements in
agency and vendor operations. A selection of potential initiatives outlined in the following pages
could collectively enable the Medicaid program to achieve significant cost savings while
maintaining or improving access to high-quality care, without broad-based cuts in provider rates,
or reductions in eligibility or covered services.
Were Missouri to effectively address the opportunities and potential initiatives outlined in this
report, total savings to the program (including federal and state share) could total up to $0.5-1.0
billion by SFY2023. This level of savings, while significant, does not represent an absolute
reduction in the size of the Medicaid program but rather a meaningful reduction in the rate of
growth of Medicaid spending, to bring it more closely in line with growth of the economy.
Implementing changes at this scale would make the program more financially sustainable under
all future financing scenarios, allowing for the state to continue to make investments to protect
the program’s essential role in serving the state’s most vulnerable populations.
Acute Care Services. Missouri spent ~$4.2 billion in SFY2018 on acute care services, including
hospital, clinic, physician, and diagnostics services, across both the managed care and non-
managed care populations. (Pharmaceutical services are discussed in a separate section).
Provider payment for acute care providers in Missouri is currently almost exclusively fee-for-
service. Fee schedules are based on historical costs; in some cases, these are adjusted each
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
4
year based on changes in operating costs. Accordingly, the payment methods used offer few
incentives for providers to contain costs. A significant proportion of Missouri Medicaid acute
care expenditures is associated with potentially avoidable exacerbations and complications
(PECs) and inefficiencies in the choice of provider, site, or treatment. In addition, Missouri
Medicaid is unique in making “add-on payments” to hospitals for services provided by Missouri
hospitals to non-Missouri residents. Potential initiatives to improve incentives and reduce costs
include adjusting rate setting methodologies, moving to value-based payment models, and
investing in the rural and safety net heath care infrastructure, including primary care and
behavioral health. In total, the gross impact of Acute Care initiatives could range anywhere from
$250 million to $500 million, depending on choices made by the state.
Long-Term Services and Supports. Missouri spent ~$2.9 billion in SFY2018 on long-term
services and supports (LTSS) for approximately 106,000 Medicaid participants accessing these
services. LTSS in Missouri consist of institutional services (e.g., nursing homes for frail elderly,
intermediate care facilities for individuals with intellectual disabilities), and home and
community-based services (both residential and non-residential) covered by the Medicaid State
Plan and nine waivers. Nursing facilities are reimbursed using a cost-based, facility-level per
diem methodology without adjustments for acuity, quality, or outcomes, and home and
community-based services (HCBS) are reimbursed on a fee-for-service basis. LTSS in Missouri
are administered by Missouri Medicaid in conjunction with the Department of Health and Senior
Services (DHSS) and the Department of Mental Health (DMH), each of which administers
HCBS waivers and conducts assessments to determine access to LTSS. The assessment
process currently in use by DHSS uses decades-old standards and, as such, may not
consistently determine institutional level of care accurately. Potential initiatives include
incorporating an acuity adjustment into the nursing home reimbursement methodology,
completing and expanding upon revisions currently underway for the state's assessment
algorithms, more directly applying assessment results in the care planning process, and
improving the consistency of the prior authorization approval process for personal care services.
In total, the gross potential impact across LTSS initiatives ranges from $90 million to $275
million, depending on choices made by the state.
Pharmacy. Missouri spent ~$1.5 billion in SFY2018 on pharmaceutical products. This spending
is inclusive of all participants as the state carves pharmacy benefits out of its MCO
arrangements. The state utilizes a preferred drug list and receives statutory and supplemental
rebates to help control costs. The basis for drug ingredient cost reimbursement was recently
updated, and Missouri is in the process of updating dispensing fees. Missouri rebate
performance is below the average for other states, potentially due to expansive grandfathering.
While the state uses a broad range of approaches to ensure appropriate utilization, there is an
opportunity to expand it to other high-cost drug classes such as oncology, hemophilia, and IVIG.
Potential initiatives include limiting grandfathering, implementing additional utilization
management, joining a purchasing consortium to increase supplemental rebate capture,
requiring NDC submission on claims for non-J-code HCPCS drugs, and applying for a value-
based contracting waiver from CMS. In total, the gross potential impact across Pharmacy
initiatives ranges from $35 million to $60 million, depending on choices made by the state.
Program Integrity. Program integrity functions within the state Medicaid agency center serve to:
prevent fraud, waste, and abuse; ensure proper participant enrollment and identify third-party
resources to pay for medical claims. Numerous divisions within the state help accomplish these
goals; however, the separation of divisions leads to siloed data and communication. Potential
initiatives include expanding adoption of best practices from the National Correct Coding
Initiative, updating certain medical and reimbursement policies to prevent improper payments,
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
5
implementing claims edits that would prevent improper billing based on Missouri’s current
policies, optimizing the state’s ability to identify and enroll participants who are eligible for
Medicare, and improving third-party liability identification. In total, Program Integrity initiatives
could deliver savings between $65 and $100 million, depending on choices made by the state.
Managed Care. Missouri's Medicaid managed care program covers primarily acute care and
professional services for non-disabled adults and children. Approximately 75% of Medicaid
participants are covered by managed care, whereas approximately 23% of Medicaid
expenditures (~$2.2 billion) flow through managed care contracts. Most pharmacy and
behavioral health services for the managed care population remain "carved out" of managed
care; the Medicaid aged, blind, and disabled (ABD) population is entirely excluded from the
current managed care program. Potential initiatives include incorporating additional adjustments
to managed care rates to remove inefficient utilization (e.g., inpatient stays that could have been
avoided with better outpatient care) from rate calculations, expanding day-one managed care
eligibility to streamline participant transitions and reduce residual fee-for-service payments,
strengthening key contract provisions and the compliance and performance management
relationship between MHD and the MCOs, and altering the scope of the managed care
program—for example, including additional services or Medicaid eligibility groups. In total, the
gross potential impact of all Managed Care-related initiatives ranges from $175 million to $300
million, depending on choices made by the state.
Federal Financing. Federal Financing focuses on identifying opportunities to optimize federal
funding for the state’s Medicaid program. Overall, Missouri has been able to capture a
significant share of the available federal funding opportunities, capturing funds across Medicaid
spending and non-Medicaid spending within DSS, DMH, and DHSS and capturing enhanced
match on select categories. However, there remain several opportunities that the state could
pursue to capture additional federal funding. These opportunities could include new waiver and
grant programs released in the SUPPORT for Patients and Communities Act, enhanced match
on substance use disorder (SUD) focused health homes, among others. In total, potential
impact from these improvements may be $10 million to $20 million, based on choices made by
the state.
Medicaid Management Information System. Missouri’s Medicaid Management Information
System (MMIS) is a set of ~70 components, partially developed within a mainframe-based
system dating from 1979. The system supports a wide range of vital activities within the
Medicaid program, but is not positioned to meet both current and future needs. Its limited
functionalities underlie several of the opportunities for improvement identified in other topical
areas. There is little alignment between program strategy and the MMIS replacement plan, and
the Information Systems (IS) group lacks the wide range of capabilities needed to ensure an
MMIS replacement trajectory that will deliver the future functionality Missouri needs. The
potential initiatives discussed in this section attempt to address these challenges.
Operations. This section analyzes the performance and operational efficiency of three
operational functions: participant managed care enrollment, claims processing, and contact
centers. These functions are currently executed through a mix of state staff and vendor
contracts. In comparison to other states, work processes often appear fragmented, process
steps seem poorly integrated and best-practice management principles are variably applied.
Potential initiatives include organizational process optimization, automation and digitization, and
improved contract management. Adoption of best practices across the different functional areas
could liberate up to 15-20% of operational resources, which could be redeployed to improve
service levels for participants and for other external and internal “customers” of the different
functions.
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
6
Implementation Considerations
The potential initiatives described in the following pages are wide-ranging, including operational
improvements to bring the program up to date with common practices among other state
Medicaid programs, as well as best practices and more transformational changes. Some of the
potential initiatives outlined represent alternative ways of achieving similar goals: in some
cases, the initiatives could reinforce one another; in other instances, they could be mutually
exclusive. Such interdependencies will be highlighted throughout.
Broadly, the state could balance two approaches to controlling spending. One approach
commonly adopted by both public programs and managed care would rely primarily on
controlling the unit prices paid for services and seeking to curb utilization through broad-based
utilization management. Such an approach could reduce costs in the short term. However, on its
own such an approach may not provide incentives to improve outcomes. As an alternative
approach, the state could seek to adopt value-based payment and care delivery models that
reward providers for quality and efficiency of the total care delivered to patients. This approach
may support more transformational changes in care delivery, with corresponding improvements
in patient outcomes and experience. However, such an approach is likely to require greater
commitment of resources and will take longer to generate impact given the need for providers to
adopt new capabilities and implement changes in clinical practices.
Aligning the growth of Medicaid expenditures with the state’s economic growth may involve a
combination of these approaches, with targeted use of utilization management and targeted
adjustments in provider rates in the near-term, combined with investments in care management
and value-based payment to support sustainable improvements in quality and efficiency. In
parallel, there may be a series of operational changes that the state could implement to bring
policies and operations up to speed with common practices, such as state-of-the-art program
integrity measures and improvements of internal administrative processes. Such changes could
generate near-term savings to offset investments in transformation changes.
Any substantial portfolio of initiatives would demand careful planning and execution, as well as
investments to support the transformation and build new capabilities. Key requirements for
effective design and implementation of Medicaid transformation include: strong and visible
executive leadership; effective stakeholder engagement; commitment to fact-based decision
making supported by robust data; upskilling of key agency staff; a well-resourced transformation
office; and modernization of the program’s technological infrastructure.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
7
Overview of Medicaid Program
In State Fiscal Year 2018, Missouri Medicaid was a $10.3 billion program, funded by state
general revenue ($2.2 billion), federal funds ($5.5 billion), and other funds ($2.6 billion).
1
The
“other funds” consisted primarily of revenue from provider taxes ($1.4 billion).
2
Since 2009, Medicaid spending has grown in proportion to the total state budget, and in
proportion to state general revenues. In 2009, Medicaid spending comprised 17% of state
general revenues; in 2018, it was 24%.
3
Without significant changes in the Missouri Medicaid
program, spending growth may continue to outpace growth in state general revenues and
could comprise 26-30% of state general revenues by 2023.
4
The following pages provide a brief introduction of the Missouri Medicaid program and a
summary of key trends in the larger U.S. healthcare context that influence program spending,
as well as state fiscal scenarios that could lead Medicaid spending to represent a greater
share of state general revenues.
THE CURRENT PROGRAM
Enrollment and Spending
Missouri Medicaid is a $10.3 billion program that covers predominantly four types of
participants: low-income children; parents of low-income children; pregnant women; and aged,
blind, or disabled (ABD) individuals.
5
Children comprise the largest eligibility group in Missouri
Medicaid, representing 63.5% of enrollees; however, persons with disabilities account for the
greatest proportion (46%) of Medicaid spending (see Exhibit 1 and Exhibit 2).
1
Missouri DSS, “TSM Expenditures History FY05 to FY18,” 2018; Missouri DSS, “Final FY18 Total State Medicaid
Expenditures,” 2018.
2
Missouri DSS: see note 1.
3
Missouri DSS: see note 1.
4
Analysis based on projections from past trends. Missouri DSS: see note 1.
5
Missouri DSS, “MO HealthNet enrollees and expenditures,” 2018, see: dss.mo.gov/mhd/general/pdf/mhdollars.pdf.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
8
EXHIBIT 1: MEDICAID ENROLLMENT & SPENDING BY ELIGIBILITY CATEGORY, SFY2018
6
EXHIBIT 2: MEDICAID ENROLLMENT & SPENDING BY TYPE OF COVERAGE, SFY2018
7
6
Missouri DSS: see note 5.
7
Missouri DSS: see note 5.
63.5%
12.3%
8.2%
16.0%
Persons with
disabilities
Seniors
46.0%
$4.3B
Enrollees by
eligibility category
27.5%
$2.6B
16.9%
$1.6B
9.6%
$0.9B
Expenditures by
eligibility category
100% = $9.4 billion
Children
Pregnant women,
custodial parents
100% = 976,779 enrollees
63.5%
22.9%
12.3%
14.2%
8.2%
62.9%
16.0%
Seniors
Persons with
disabilities
Enrollees by
eligibility category
Expenditures by
type of coverage
Children
Pregnant women,
custodial parents
Fee-for-service
population
FFS spend for
MC population
Managed care
100% = 976,779 enrollees 100% = $9.4 billion

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
9
Services for >155,000 persons with disabilities and >80,000 elderly participants (the aged, blind
and disabled [ABD] population) are provided through Medicaid fee-for-service, comprising
24.2% of enrollees but 62.9% of total program expenditures. The ABD population includes
distinctive subpopulations with different cost patterns: frail elderly, individuals with intellectual
and/or developmental disabilities, individuals with severe behavioral health issues, and others.
Non-disabled children, parents, and pregnant women comprise 75.8% of enrollees (about
650,000 in all) but 37.1% of total program costs, of which 22.9% is covered through managed
care and 14.2% (pharmacy and behavioral health) is paid through Medicaid fee-for-service.
Exhibit 3 shows one possible categorization of diagnostic groups,
8
including numbers of
participants per group, and average per member per month (PMPM) spending per main
category (institutional long-term services and supports [LTSS], home and community-based
services [HCBS], acute services).
All elderly and 40% of individuals with disabilities are dually eligible for both Medicaid and
Medicare. For these participants, Medicare pays for the acute care costs (e.g., hospitals,
physicians, drugs); Medicaid pays for long-term services and supports (e.g., home care, nursing
homes).
EXHIBIT 3: SUBPOPULATIONS WITHIN THE ABD POPULATION, SFY2018
9
8
Medical diagnosis, procedure codes and demographic information from Missouri Medicaid claims for SFY2018
were used to develop sub-segmentations of ABD population by diagnosis category. Diagnosis categories are based
on claims data only, with the exception of the frail elderly category which is based on age and participant chronicity.
9
Analysis of Missouri Medicaid claims data, SFY2016-18; participants may overlap across categories.
6.8
36.4
38.6
73.4
28.3
20.7
22.2
6.6
39
32
44
45
48
45
60
35
Institution
HCBS
LTSS
Non-LTSS
Other
Physical
disability
Sensory Deficit
Conditions
High needs BH
ID/DD
ABI
Neurodegenera-
tive Conditions
SFY 2018 average
participants, K
Average spend, $K
PMPYABD population Description
Annualized
participants, %
total
Frail elderly
35%
70%
6%
27%
37%
20%
21%
6%
298
1,156
2,863
1,264
1,750
229
1,245
1,060
Total spend, $M
▪ Do not meet criteria of any of the above
▪ Traumatic brain injury
▪ Cerebral infarction
▪ Cerebral hemorrhage
▪ Genetic syndromes with intellectual disability
▪ Congenital brain injury
▪ Developmental disability (e.g., Autism)
▪ Presence of a behavioral health diagnosis, or
utilization, with at least one mental health
condition
▪ Dementia, Parkinson’s, Alzheimer’s, ALS,
Multiple Sclerosis
▪ Blindness
▪ Hearing loss
▪ Spinal cord injury
▪ Paralysis
▪ Chronic pain / weakness
▪ Age 65+ with 2 or more chronic conditions

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
10
Financing and Budget
Missouri Medicaid is funded by state general revenue ($2.2 billion), federal funds ($5.5 billion),
and other funds ($2.6 billion).
10
The “other funds” are primarily provider taxes ($1.1 billion from
hospitals, and $0.3 billion from nursing homes and pharmacies).
11
As these taxes generate
federal matching funds (nearly two federal dollars for every dollar generated through provider
taxes
12
), they are significant to the financing of the Missouri Medicaid program. Exhibit 4 shows
the flow of funds, highlighting the hospital tax and its integration in the Medicaid funding flow.
EXHIBIT 4: MISSOURI MEDICAID FUNDS FLOW (SFY2018, USD BILLIONS)
13
Organization
Three departments jointly manage parts of the Medicaid program. The Department of Social
Services (DSS) operates MO HealthNet (MHD), which is primarily responsible for medical
expenses for eligible individuals. This includes both the fee-for-service and the managed care
populations. The Department of Mental Health (DMH) administers services for populations with
10
Missouri DSS: see note 1.
11
Missouri DSS, “Provider taxes overview,” 2018.
12
Kaiser Family Foundation (KFF), “Federal Medical Assistance Percentage (FMAP) for Medicaid and Multiplier,”
2018, see: www.kff.org/medicaid/state-indicator/federal-matching-rate-and-multiplier.
13
Office of Administration, “The Missouri budget fiscal year 2018 summary,” 2018, see:
www.oa.mo.gov/sites/default/files/FY_2018_Budget_Summary.pdf; Missouri DSS: see note 1; Missouri DSS: see
note 11; Missouri DSS, “Annual_Table 23 and 24_FY18 by Large Group PMPM,” 2018; Missouri DSS, “Payments
Assessment for SFY 14-18,” 2018.
Federal funds
Other funds
General revenue
Medicaid spend
5.5
2.2
2.6
9.4
8.8
9.4
10.3
1.1
Federal match of provider tax
2.2
State gov’t collects ~5.5%
FRA tax on provider
revenue
3
Federal gov’t
matches revenue
collected from
provider tax
27.6
Overall MO budget Medicaid Hospitals
IP/OP reimbursement
(Medicaid FFS)
2.8
IP/OP reimbursement
(all other payors)
17.9
IP/OP reimbursement
(Medicaid MC)
1.5

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
11
developmental disabilities (both intellectual and physical disabilities, as well as certain learning
disabilities), community-based health centers, psychiatric rehabilitation services, comprehensive
substance treatment and rehabilitation (CSTAR) services, and health home programs, amongst
others. The Department of Health and Senior Services (DHSS) operates the Division of Senior
and Disability Services (DSDS), which administers the HCBS benefits for adults 18 and over,
and Special Health Care Needs (SHCN), which administers the Healthy Children and Youth
benefits for persons with special health care needs up to 21 years of age. DSS is responsible
for the largest share of Medicaid spending at approximately $7.9 billion, DMH’s share is $1.5
billion, and DHSS’ share of Medicaid spending is $0.9 billion.
14
MAJOR INDUSTRY TRENDS AFFECTING THE PROGRAM
Healthcare inflation rising faster than GDP
The United States faces increasing pressure to contain its rising healthcare costs. In 2017, total
U.S. healthcare spending reached $3.5 trillion, marking a 3.9% increase from the previous year,
amounting for almost 18% of gross domestic product (GDP)
15
. U.S. health spending per person
climbed to over $10,739 in 2017, the third year that the spending has exceeded $10,000.
16
The
growth in per-person spending, or medical cost inflation, outpaces the general inflation rate (see
Exhibit 5). CMS projects spending to grow 1% faster than GDP to reach $5.7 trillion by 2026.
17
EXHIBIT 5: MEDICAL INFLATION, GENERAL INFLATION, GDP GROWTH, SFY2001-17, %
18
14
Missouri DSS: see note 1.
15
CMS, “NHE Fact Sheet,” 2017, see: www.cms.gov/research-statistics-data-and-systems/statistics-trends-and-
reports/nationalhealthexpenddata/nhe-fact-sheet.html.
16
CMS, “The National Health Expenditure Summary including share of GDP, CY 1960-2017,” 2017,
www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-
Reports/NationalHealthExpendData/NationalHealthAccountsHistorical.html.
17
The Balance, “U.S. Inflation Rate by Year from 1929 to 2020,” 2019, see: www.thebalance.com/u--inflation-rate-
history-by-year-and-forecast-3306093; The Balance, “U.S. GDP by Year Compared to Recessions and Events,”
2019, see: www.thebalance.com/us-gdp-by-year-3305543.
18
The Balance: see note 17.
9
8
6
6
6
5
4
3
3
3
3
4
5
4
3
2
2
3
4
3
2
3
2
1
1
2
2
2
3
4
4
3
2
3
2
2
3
3
2
03 09052001 1402 04 06 1007 11 20171208 13 15 16
1
2
2
2
3
7
3
0
0
-3
2
2
Medical inflation rate
General inflation rate
GDP growth rate
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
12
Costs are rising in Medicare and Medicaid, putting pressure on both federal and state budgets.
In addition, rising health care costs create challenges in the commercial market as well.
Employees’ contribution to health insurance grew almost three times faster than wages between
2010 and 2015,
19
and middle-class Americans’ healthcare spending increased 60% over the
past 30 years.
20
The growing financial burden of healthcare has been a significant factor in the
low growth in purchasing power of the middle class in the U.S. over the past two decades.
21
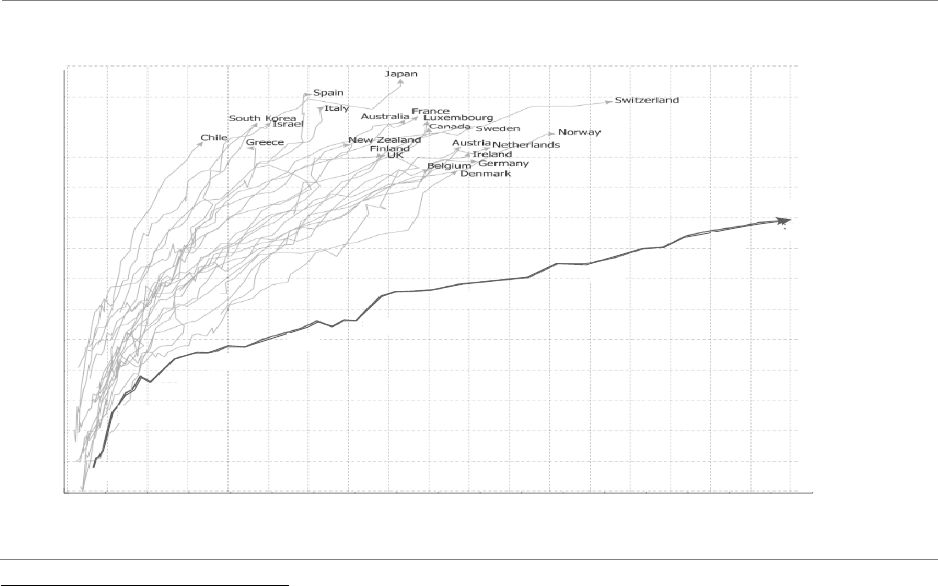
While rising health expenditures are not unique to the U.S., its spending exceeds that of other
countries even after adjusting for differences in average wealth. While outcomes of U.S.
healthcare exceed those of other countries for some catastrophic illnesses and other complex
conditions (e.g. breast and colorectal cancer), outcomes lag other countries for most chronic
conditions.
22
Chronic conditions, in particular, account for a significant portion of healthcare
spending growth, underscoring concerns that increased levels of investment in healthcare have
not translated to proportional improvements in life expectancy or quality of life (see Exhibit 6).
EXHIBIT 6: LIFE EXPECTANCY AND HEALTH EXPENDITURE ACROSS COUNTRIES
23
19
KFF, “2015 Employer Health Benefits Survey,” 2015, see: www.kff.org/health-costs/report/2015-employer-health-
benefits-survey.
20
Hamilton Project, “Where Does All the Money Go: Shifts in Household Spending Over the Past 30 Years,” 2016,
see:www.hamiltonproject.org/papers/where_does_all_the_money_go_shifts_in_household_spending_over_the_pa
st_30_y.
21
Pew Research, “For most U.S. workers, real wages have barely budged in decades,” 2018, see:
www.pewresearch.org/fact-tank/2018/08/07/for-most-us-workers-real-wages-have-barely-budged-for-decades/.
22
Peterson-Kaiser Health System Tracker, “How does health spending in the U.S. compare to other countries?”
2018, see: www.healthsystemtracker.org/chart-collection/health-spending-u-s-compare-countries;
www.kff.org/slideshow/how-does-the-quality-of-the-u-s-healthcare-system-compare-to-other-countries/.
23
Our World in Data, “Link between health spending and life expectancy: US is an outlier,” 2017, see:
ourworldindata.org/the-link-between-life-expectancy-and-health-spending-us-focus.
70
71
72
73
76
74
75
77
78
79
80
81
82
83
84
1,000$
Health expenditure
2,000$ 3,000$500$
Life expectancy
0 4,000$ 5,000$ 6,000$ 7,000$ 8,000$ 9,000$
2014
2010
2005
2000
1995
1990
1985
1980
1975
1970
USA

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
13
CMS taking steps to reduce federal spending on health care
The Centers for Medicare & Medicaid Services (CMS) have undertaken a series of initiatives to
reduce federal healthcare costs for Medicare, ranging from attempts to reduce what it pays for
drugs and outpatient visits in Medicare to limiting cost growth in Medicare Advantage plans.
24
As the federal government will pay for 50% to 78% of Medicaid costs through federal match in
2019 (65% in Missouri)
25
, federal spending on Medicaid is similarly assessed for cost reduction
opportunities: CMS has announced its intention to increase the level of scrutiny of Medicaid
waiver expenditures.
26
In addition, CMS has described its intention to increase audits of state
claims for federal matching funds and beneficiary eligibility determination, among others.
27
Public and private payors are migrating to value-based payment
There is a broad consensus that one of the key drivers of waste and inefficiency in U.S.
healthcare is the fee-for-service (FFS) payment model that characterizes most provider
payments. FFS stimulates volume rather than coordination of services, and there are no
inherent incentives to achieve optimal outcomes nor to deliver care in an efficient manner.
28
Both public and private payors are transitioning from FFS to value-based payment (VBP), using
Alternative Payment Models (APMs) to reward providers for delivering high-quality care at lower
cost. Research suggests that well-designed APMs improve the quality of care and can
meaningfully reduce the cost of care if implemented across the full spending base.
29
PROJECTED SPENDING WITHOUT SIGNIFICANT COURSE CORRECTIONS
Over the last 10 years, Medicaid spending growth has outpaced growth in state general
revenues. For example, in 2009, 17% of state general revenue funds were directed toward
Medicaid; however, in the wake of the Great Recession, Medicaid grew to 22% of state general
revenue by 2012 and, in 2018, reached 24% (see Exhibit 7). Although Medicaid enrolment has
fluctuated over this timeframe, total Medicaid spending growth has outpaced growth in state
general revenues when measured over any five-year timeframe, due to the increase in spending
per participant enrolled in the program. Notwithstanding reductions in Medicaid enrollment
observed since the beginning of SFY2019, program spending is likely to occupy a greater share
of state general revenue over the coming five years, absent changes in program performance.
In this section, we consider three scenarios as a method for gauging the level of fiscal pressure
that may arise from Medicaid spending growth. In Scenario 1, Medicaid spending as a share of
state general revenues continues to grow at a pace similar to the last five years; in Scenario 2,
24
CMS, “CMS-1695-P: Hospital Outpatient Prospective Payment- Notice of Proposed Rulemaking (NPRM),” 2019,
see: www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/Hospital-Outpatient-
Regulations-and-Notices-Items/CMS-1695-P.html; CMS, “Prior Authorization and Step Therapy for Part B Drugs in
Medicare Advantage,” 2018, see: www.cms.gov/Medicare/Health-
Plans/HealthPlansGenInfo/Downloads/MA_Step_Therapy_HPMS_Memo_8_7_2018.pdf.
25
The percentage varies by state; for Missouri the match rate in FY2019 is 65.4%.
26
CMS, “Budget Neutrality Policies for Section 1115(a) Medicaid Demonstration Projects,” 2018, see:
www.medicaid.gov/Federal-Policy-Guidance/downloads/SMD18009.pdf.
27
CMS, “CMS announces initiatives to strengthen Medicaid program integrity,” 2018, see:
www.cms.gov/newsroom/press-releases/cms-announces-initiatives-strengthen-medicaid-program-integrity.
28
Health Care Learning and Action Network, "Alternative payment model (APM) framework. Updated version 2017,"
2017, see: hcp-lan.org/workproducts/apm-refresh-whitepaper-final.pdf.
29
McKinsey, “The seven characteristics of successful alternative payment models,” 2019, see:
www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/the-seven-characteristics-of-
successful-alternative-payment-models.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
14
an economic downturn accelerates the growth of Missouri Medicaid spending while reducing the
growth of state general revenue; in Scenario 3, the trends from Scenario 1 are exacerbated by
potential changes in CMS policies that would reduce federal revenue for Missouri.
EXHIBIT 7: MEDICAID SPENDING AS PERCENT OF GENERAL REVENUE, SFY2009-23
30
Scenario 1—Continuation of Recent Trends: Spending on the program increased from 21%
of state general revenue in 2013 (36% of total state spending) to 24% (40% of total spending) in
2018.
31
In the first scenario illustrated in Exhibit 7, the assumption is that growth of both
Medicaid spending and total state spending continue at the pace observed over these past five
years. Under this scenario, total Medicaid spending would increase to $12.8 billion by 2023,
while the state’s total spending would grow to $29.2 billion (growing 2.5% annually) by 2023. In
2023, Medicaid spending would comprise 44% of the overall state spending and 26% of state
general revenues.
Scenario 2—Potential Impact of Economic Downturn: In the second scenario, a severe
economic downturn (comparable to the recession that began in 2008) affects both state general
revenues and Medicaid enrollment. Based on analyses by Moody’s, an economic downturn
occurring within the next four years could reduce total general revenue by approximately 12%
over a two-year period. This reduction in general revenue will likely coincide with an increase in
Medicaid enrollment, as individuals lose jobs and incomes fall, resulting in an estimated
increase in Medicaid spending by 1.9% in total over the course of two years.
32
These changes
could translate to Medicaid spending growing to comprise 51% of total state spending and 30%
of state general revenues in 2023.
30
Medicaid expenditures have continued to outpace economic growth. Missouri DSS: see note 1.
31
Missouri DSS: see note 1.
32
Moody’s, “Stress-Testing States,” 2017, see: www.economy.com/getlocal?q=91a42834-85af-4773-b408-
5da811028c00&app=eccafile.
24
31
27
19
25
28
26
29
18
30
0
20
21
22
23
21%
2009 22
23%
171411
20%
22%
13
28%
17%
1610
24%
12
21%
23%
15 2018 19
22%
30%
2023
Status quo
(Scenario 1)
Recession
(Scenario 2)
CMS policy changes
(Scenario 3)
19%
26%
21

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
15
Scenario 3—Potential Changes in CMS Policies: In the third scenario, no recession occurs,
but CMS policy changes could lead to reductions in federal funds for the state’s Medicaid
program and, consequently, to greater pressure on the state budget. A 3.5% drop in net federal
funds could reduce federal funding by approximately $200 million in SFY2023.
33
If the Medicaid
program’s total spending were to remain unchanged, the loss of federal funds may need to be
offset by a similar increase in funding from state general revenues. This could increase the
program’s share of state general revenues to 28% in SFY2023.
Savings needed to keep spending growth in line with State General Revenues
Under any of the scenarios described above, significant changes in the structure and
performance of Missouri’s Medicaid program would be necessary to bring Medicaid spending
growth in line with projected economic growth of the state. Following are estimates of the
reductions in Medicaid program spending that would be necessary to maintain spending at 24%
of state general revenues through SFY2023, under each of the three scenarios.
• In Scenario 1 (continuation of recent historical trends), Missouri would need to reduce the
growth rate of Medicaid spending by approximately 2 percentage points to bring it in line
with the growth of state general revenue, to maintain spending at 24% of state general
revenue. In SFY2023, this would equal approximately $735 million savings to total
Medicaid spending, or approximately $260 million savings to state general revenues.
• In Scenario 2 (occurrence of a recession similar in magnitude to that experienced 10 years
ago), it would be necessary to reduce Medicaid spending by nearly $1.7 billion, or $590
million in spending from state general revenues, to maintain spending at 24% of state
general revenues.
• In Scenario 3 (continuation of historical trends, exacerbated by CMS policy changes), it
would be necessary to reduce total program spending by approximately $1.3 billion, or
$460 million in spending from state general revenues to maintain spending at 24% of state
general revenue.
34
The funding gap implied by the above scenarios is meant to provide context for understanding
the estimated $0.5 billion to $1.0 billion in cost savings associated with the opportunities and
potential initiatives detailed in the pages that follow. Maintaining spending at 24% of state
general revenues may not necessarily represent the state’s policy objective and may not be
feasible in all future scenarios. In all scenarios, however, implementation of initiatives such as
those outlined in the pages that follow could help the Medicaid program to reduce fiscal
pressure on the state budget while maintaining or improving access to high-quality care, without
broad-based cuts in provider rates, or reductions in eligibility or covered services.
33
As outlined in the section on acute care services, existing risks to the state’s federal match revenue exist (e.g.
inpatient UPL calculations, planned federal reduction of DSH payments, DSH payments-related legal
developments, federal scrutiny of existing provider tax pooling arrangements, federal initiatives to reduce the
provider tax safe harbor, and so forth). $200 million is a low estimate of the impact of any combination of two to
three of these risks becoming reality.
34
Assumes a corresponding $120 million decrease in provider tax and $80 million decrease in other cuts to federal
funding (e.g., DSH payments). The savings would bring the percentage of Medicaid spending of state general
revenue to SFY2018 levels.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
16
Opportunities and Potential Initiatives
Without significant changes, Medicaid spending may increase from 24% of state general
revenues in SFY2018 to comprise 26% to 30% of state general revenues by SFY2023.
Significant cost savings would be necessary to bring growth of Medicaid spending in line with
the level of economic growth of the state, while preserving access to care for participants.
The Missouri Department of Social Services, MO HealthNet Division (MHD) commissioned a
rapid, in-depth independent assessment of its programs and operations to identify potential
opportunities and strategies to transform the Missouri Medicaid program, including evaluation of
which functions the Department is performing well in, what activities or practices could be
improved, and what priorities could be considered for future investment.
Overall, the Missouri Medicaid program is currently outdated in most aspects compared to other
peer states, and significant opportunities exist relative to industry best practices:
• Dollars spent in the program are not well aligned with value received from delivery system;
• Specifically, methods to pay providers lack incentives to contain costs or enhance quality;
• Approaches to utilization management; eligibility management; fraud, waste, and abuse;
and third-party liability are limited, partially due to the limitations of the MMIS (see below);
• Programs for special needs populations are fragmented;
• There is no substantial measurement nor transparency of outcomes of care; and
• Service levels to consumers and providers could also be improved, including reductions in
average wait times for handling questions, as well as increased service channels.
Leaders and staff in DSS, DMH, and DHSS are aware of these challenges and highly motivated
to modernize the program. However, the foundational operational capabilities to do so are
equally outdated, hampering opportunities for improvement: the existing technology
infrastructure (MMIS) is antiquated; data quality needed for program management is
suboptimal; and access to key management information is absent.
Detailed findings from the assessment conducted over the past several months are outlined in
the pages that follow, organized into eight project areas which collectively address sixteen
performance opportunities prioritized by DSS at the outset of this assessment. For each topical
area, potential opportunities for improvement have been identified and evaluated through
interviews with functional leaders and subject matter experts within the relevant departments,
analysis of claims- and non-claims data, review of activities and operations, assessment of
supporting infrastructure and analytics, and benchmarking against other state Medicaid
programs, Medicaid managed care organizations (MCOs), or other private health insurers.
Based on these opportunities, a wide range of potential initiatives have been outlined for further
consideration by the Department. Depending on the selection of initiatives the state chooses to
pursue, total gross savings to the program (including federal and state share) could total up to
$0.5 billion to $1.0 billion by SFY2023. These estimated savings would be net of reinvestments
in the delivery system (e.g., in primary care, rural health, and the safety net; as well as rewards
for providers that generate savings under value-based payment models) and in the Medicaid
program’s operations to improve service levels to participants and providers.
35
35
One-time investments as well as MMIS replacement investments are not included.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
17
Many of the opportunities for improvement could require changes in policies and contracts
requiring cooperation of local providers, support from the state legislature, and in some cases
federal approval. Potential initiatives outlined in this report are not meant to represent advocacy
for specific policies, nor conclusions yet reached by DSS. The state retains sole responsibility
for decision making over which of these potential improvement initiatives (or others) to pursue,
and in what form, in compliance with applicable laws, rules and regulations.
ACUTE CARE SERVICES
Missouri spent ~$4.2 billion in SFY2018 on acute care services, including hospital, clinic,
physician, and diagnostics services, across both the managed care and non-managed care
populations. Including pharmaceutical services, the total is ~$5.7 billion.
36
Hospitals are paid
through a combination of base rates and “add-on payments”, updated periodically based on
changes in hospital operating expenses. This approach offers minimal incentives for providers
to contain costs, making it an outlier among states. Uniquely, Missouri Medicaid makes add-on
payments to hospitals for services provided to non-Missouri, non-eligible residents.
Physicians and behavioral health providers are also paid per service (fee-for-service [FFS]).
Compared to other states, physicians’ reimbursement is low. Also, total spending on non-
hospital acute care services (physicians, Federally Qualified Health Centers [FQHCs], clinics,
and rural health services) is lower than other, comparable states.
The overall value of care delivered (dollars spending vs outcomes for participants) varies
significantly across counties. In general, >15% of Missouri Medicaid acute care expenditures
may be associated with potentially avoidable exacerbations and complications (PECs), which
includes costs of PECs associated with the prevention and treatment of opioid use disorder
(OUD). In addition, 5% to 10% of expenditures may be associated with inefficiencies, such as a
site of service or choice of therapy that might be more expensive without adding quality.
37
Potential initiatives to improve incentives and reduce costs range from adjusting rate setting
methodologies, moving to value-based payment models and investing in the rural and safety net
heath care infrastructure, including primary care and behavioral health. In total, the impact of the
acute care initiatives could range from $250 million to $500 million, net of potential
reinvestments in the delivery system, depending on the state’s choices.
38
To achieve the higher
end of this range, the state may need to pursue a combination of initiatives, striking the balance
between initiatives primarily focused on rates with initiatives focused on value-based payment
(VBP) and investments.
The state could build on its providers’ broad experience with Medicaid, Medicare, and
Commercial Alternative Payment Models (APMs). Missouri has significant experience with
Patient Centered Medical Homes (PCMH) and Health Homes in Medicaid, which aim to
integrate physical, behavioral, and substance use disorder (SUD) care for patients with, or at
risk of, multiple chronic conditions.
36
Pharmaceutical services are discussed in a separate section. The projected savings are not likely to overlap
between these sections.
37
Analysis of Missouri Medicaid claims data, SFY2016-18.
38
Analysis of Missouri Medicaid claims data, SFY2018; Interviews with Medicaid program staff and analysis of state
data, 2018.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
18
This section will first describe the current reimbursement methodologies and the experience
with and impact (where quantifiable) of VBP models in Missouri. Subsequently, it will highlight
the opportunities to bend the cost curve and improve the value of care for Missourians and
present an associated range of initiatives.
Current situation
This section gives an overview of Missouri’s current methodology of hospital outpatient
reimbursement, inpatient reimbursement, utilization management, out-of-state payments,
hospital tax, physician reimbursement, behavioral health reimbursement, and acute care value-
based payment initiatives.
Population served, and services provided
For Medicaid, the providers discussed in this section serve both the managed care population
(children, parents, and pregnant women) as well as those participants in the disabled population
that are not dually eligible.
39
Exhibit 8 shows the breakdown of the total Medicaid costs by
service for these populations.
EXHIBIT 8: BREAKDOWN OF ACUTE CARE COSTS BY SERVICE CATEGORY, SFY2018
40
In the managed care population, costs are driven by mental illness diagnoses (including
substance use disorders) and by perinatal care (pregnancy care, delivery, post-delivery care,
39
Dually eligible participants receive their acute care services through Medicare.
40
Analysis of Missouri Medicaid claims data, SFY2016-18; does not include beneficiaries who have no eligibility
during any given month, as well as beneficiaries who are dually eligible or have third party liability; beneficiaries
may overlap across categories.
240
Radiology
Hospital inpatient care
Office and clinic care
12
ED care
Hospital outpatient care
Specialty pharma
Ambulance and transportation
Lab and pathology
Prescription drugs
550
Ancillary services
DME and supplies
PT/OT/ST
19
55
Other locations
Other types of care
1,166
1,488
517
709
484
65
66
273
130
Hospital
and ED
Total spend = $ 5,683M
SFY2018, $M
Diagnostics
Other
Total acute care spend,
$M
Share of total
acute care
spend
Average beneficiaries,
000
Share of total
acute care
beneficiaries
Total pop = 1,173K beneficiaries
383
370
139
45
408
762
419
753
103
262
24
21
172
130
Acute care service category
2%
11%
10%
15%
4%
32%
20% 12%
12%
36%
8%
66%
26%
65%
1%
9%
1%
33%
1%
23%
0%
2%
5%
4%
9%
35%
0%
2%
Office
Pharma-
ceuticals

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
19
and newborn care) (see Exhibit 9). In the non-dual disabled population, mental illness
diagnoses drive more than one-third of the total costs, followed by cardiovascular diagnoses
(see Exhibit 10). In these exhibits, substance use disorders (including opioid use) are included
in the mental illness diagnostic category.
EXHIBIT 9: MEDICAL COSTS BY DIAGNOSIS GROUP FOR MANAGED CARE
POPULATION, SFY2018
41
41
Analysis of Missouri Medicaid claims data, SFY2016-18.
Diseases of the musculoskeletal system and connective tissue
Injury and poisoning
Diseases of the nervous system and sense organs
Diseases of the digestive system
Mental Illness
Certain conditions originating in the perinatal period
3%
Complications of pregnancy; childbirth; and the puerperium
Diseases of the respiratory system
Congenital anomalies
8%
Diseases of the circulatory system
Endocrine; nutritional; and metabolic diseases and immunity disorders
Neoplasms
Other
18%
10%
11%
6%
6%
24%
3%
4%
3%
2%
2%
MANAGED CARE POPULATION
Medical spend by diagnosis groups for adult and child claimants, SFY2018
Percent of medical spend

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
20
EXHIBIT 10: MEDICAL COSTS BY DIAGNOSIS GROUP FOR NON-DUAL DISABLED
POPULATION, SFY2018
42
Inpatient reimbursement
For inpatient (IP) care, Missouri uses a hospital-specific per diem, based on historical cost
reports up to two decades old. The base per diem is not differentiated by type of services
provided nor patient characteristics. In SFY2018, $540 million of inpatient payments were paid
to hospitals. In addition, add-on payments are made. $817 million “direct Medicaid” add-ons
compensate providers for differences between the base per diem and trended costs as
determined by more recent cost reports. In addition, direct Medicaid payments help offset
provider tax payments.
43
Other add-ons include disproportionate share hospital (DSH)
payments ($759 million) and graduate medical education (GME) payments ($139 million) (see
Exhibit 11).
The state uses a vendor to manage utilization of inpatient services. The vendor conducts six
types of reviews: prospective (pre-admission), admission (initial), continued stay review,
retrospective (post-discharge), and ongoing validation reviews. All review determinations are
made using Milliman Care Guidelines
®
and pertinent medical information received from the
attending physician or hospital regarding the patient's condition and planned services.
42
Analysis of Missouri Medicaid claims data, SFY2016-18.
43
Missouri Foundation for Health, “Briefing Book for Missouri Medicaid,” 2016, see: mffh.org/wordpress/wp-
content/uploads/2016/04/Medicaid-Financing.pdf.
Medical spend by diagnosis groups for non-dual disabled claimants, SFY2018
Percent of medical spend
4%
Diseases of the circulatory system
Diseases of the respiratory system
Diseases of the nervous system and sense organs
1%
34%
13%
Mental Illness
Diseases of the musculoskeletal system and connective tissue
Injury and poisoning
Neoplasms
Endocrine; nutritional; and metabolic diseases and immunity disorders
Diseases of the digestive system
7%
Congenital anomalies
Complications of pregnancy; childbirth; and the puerperium
Certain conditions originating in the perinatal period
Other
13%
6%
6%
7%
5%
5%
<1%
<1%
NON-DUAL DISABLED

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
21
MHD covers up to 24 hours of observation services, ordered for patients who require
significant periods of treatment or monitoring before a decision on admission is made. Only
one observation code per stay can be billed, capping the reimbursable portion to 24 hours.
Outpatient reimbursement
For outpatient (OP) FFS reimbursement, Missouri pays a percentage of charges for individual
services. The percentage is based on analysis of historical cost reports trended to the current
state fiscal year. Currently, the state is transitioning towards a Medicare-based outpatient fee
schedule model. In SFY2019, hospitals received $319 million in outpatient base rate payments.
In addition, add-on payments are made to further help offset provider taxes (these are included
in the “direct Medicaid” add-ons, see Exhibit 11).
44
The state uses a vendor to conduct prior authorizations for advanced imaging (CT/CTA,
MRI/MRA, and PET) and select cardiac procedures (cardiac nuclear medicine and cardiac
catheterization).
EXHIBIT 11: HOSPITAL REIMBURSEMENT BREAKDOWN, MEDICAID FFS, SFY2019
45
Provider tax
Like other states, Missouri taxes hospitals and uses these revenues to fund Medicaid and draw
down federal funds at the Missouri federal match rate of 65.4% (see Exhibit 4). Missouri’s
hospital tax rate is higher than most other states (greater than 5.5%).
46
Missouri compensates
44
Missouri DSS, “FRA 19-3 – 10 24 18 – FINAL,” 2019; UPL analysis, Missouri DSS, 2018-19.
45
Missouri DSS, see note 44; uses FY18 data for outpatient base rate payments.
46
KFF: see note 12.
Description and methodology
Add-on payment stream
Base reimbursement stream
540
319
817
759
OP base
IP base
139
Total FFS Medicaid hospital spend
(SFY 19), USD, millions
Graduate
Medical
Education
(GME)
payments
Direct
Medicaid
payments
Direct
Medicaid
payments
Inpatient
base rate
payments
Outpatient
base rate
payments
Dispropor-
tionate
Share
Hospital
payments
Graduate
Medical
Education
payments
▪ Per diem payments for inpatient services
▪ For a given hospital, per diems are the same regardless of diagnosis or type of care
(“single per diem”)
▪ Per diems built off cost reports from the time the hospital enrolled. They are not trended
over time, regardless of changes to patient or service mix
▪ Payments for outpatient services
▪ Rates for each hospital are calculated as a percentage of billed charges
▪ The payment percentage is based off historical cost-to-charge ratios, trended forward to
current year
▪ Outpatient rates are trended over time based on updated cost reports
▪ Payments to compensate for costs not covered by per diem (see below), including
– Compensation for FRA payments (i.e., provider tax payments)
– Payment for difference between per diem and trended costs (based on cost-reports)
▪ Decreases in inpatient base rates will increase Direct Medicaid payments to compensate
for the increased difference between per diem and trended costs
▪ Payments to compensate for costs of care to uninsured individuals, distributed proportionally
to hospitals based on total uncompensated care
▪ Payments to compensate for costs associated with offering medical education through
residency programs

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
22
hospitals for these Federal Reimbursement Allowance (FRA) payments through the FFS add-on
payments. To attempt to make the tax closer to budget neutral for hospitals, the Missouri
Hospital Association (MHA) operates a pooling mechanism (see Exhibit 12).
47
Since 2017, when managed care was implemented statewide, the state includes a portion of
add-ons (primarily to offset provider taxes) in the managed care capitation rate. Through a
Memorandum of Understanding, the MCOs and the MHA have agreed to uphold efforts to
compensate hospitals for their costs attributable to the FRA assessment.
48
EXHIBIT 12: MISSOURI HOSPITAL ASSOCIATION FRA FUNDING POOL
49
Physician reimbursement
Physicians are reimbursed through a fee schedule based on a percentage of what Medicare
pays for the same services. Once fees are set (e.g., when fees are initially calculated as a
percentage of Medicare’s rates for a certain procedure code), they are static until the state
legislature changes them. Physicians who are organized in clinics can bill the services provided
47
Missouri Hospital Association, “How the FRA funds are used,” 2014, see: web.mhanet.com/FRA%20Tutorial.pdf.
48
MHA Management Services Corporation, “MSC Health Plan MOU and Amendment,” 2017.
49
Missouri Hospital Association, “Missouri’s Hospital Provider Tax Pooling Arrangement,” 2016, see:
web.mhanet.com/article/4387/Missouri8217sHospital-Provider-Tax-Pooling-Arrangement.aspx?articlegroup=2663.
Missouri DSS: see note 1. KFF: see note 12.
FRA assessed at
~5.50% of each
provider’s adjusted
net revenue (both
IP and OP, Medicaid
and non-Medicaid)
Tax collection
and matching
Reimbursement to
hospitals
Hospitals are
compensated for FRA
payments primarily
through Direct
Medicaid add-on
payments
State paid federal
matching funds
at 65.40%
Provider
participates
in a MHA
pool?
Provider
keeps full
add-on
payment
Provider
receives more in
payments from FRA than
it pays in FRA (pool
contributor)?
Provider
transfers FRA-
funded
payments to
pool operated
by MHA
To net out the FRA paid with the payments received,
MHA reimburses providers that receive less in FRA-
funded payments than they pay (pool recipients)
After payment to pool recipients, MHA returns remaining
funds in central account to pool contributors
Pooling of FRA funds
Yes
Provider waits
for pooling
and
redistribution
of payments
Yes
No
No
MOU b/t MHA and MCOs: agreed to
uphold attempt to compensate individual
hospitals FRA-related gains and losses
for payments within Managed Care
Intention of
voluntary MHA
pooling arrangement
is participation of all
FRA paying
hospitals
FRA funds approximately 33% of the Missouri Medicaid program:
$1.2B collected from providers with additional $2.2B in federal match

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
23
through their clinics, for which reimbursement rates are generally higher than they are for
physicians.
Behavioral health reimbursement
Behavioral health services are covered by both DMH and MO HealthNet. DMH covers
Community Psychiatric Rehabilitation services, which include intake and annual evaluations,
behavioral health assessment, psychosocial rehabilitation, and day treatment for youth.
50
DMH
also covers Comprehensive Substance Treatment and Rehabilitation (CSTAR) services. MO
HealthNet covers other behavioral health services, such as various psychotherapy services
(e.g., family and group therapy, individual psychotherapy), services in a school setting, applied
behavioral analysis, and selected telehealth services, among other covered services.
51
Behavioral health services not covered by Medicaid include housing supports, drug screens,
transportation, and occupational therapy for adults. Behavioral health services are reimbursed
on a fee-for-service basis, determined by relevant information (e.g., charge information from
providers across the state, recommendations from the State Medical Consultant) and current
appropriated funds.
Value-based payment (VBP)
There is significant experience with VBP in the state, both within Medicaid and across other
payors, although many of these models are not yet fully mature or at scale. The initiatives in
Medicaid are primarily focused on PCMHs and health homes (both within the FFS and through
the managed care local community care coordination program [LCCCP]), through which
providers may receive additional payments to improve the value of the care delivered. The
impact of some initiatives can be quantified.
• Local community care coordination program (LCCCP). Missouri contracts require MCOs to
develop a LCCCP to be approved by the state in which MCOs are to develop VBP
contracts (such as ACOs, PCMHs, primary care case management programs [PCCM])
with providers. Provider participation should have reached 10% in June 2018, with 20% of
participants enrolled in the LCCCP by the end of the contract period. The program has
recently started; no results are yet available.
• Accountable care organizations (ACOs). In addition to the LCCCP initiatives, there are at
least 13 ACOs in Missouri, concentrated in St. Louis, Kansas City and Springfield, of which
11 are Medicare ACOs, and two are commercial ACOs. The six Medicare ACOs for which
the number of participants has been published jointly serve >184,000 Missourians. At least
three of these ACOs have risk-based contracts; one reported $8.9 million in earned
savings in 2017.
52
• Patient-centered medical home (PCMH). There are currently 419 NCQA accredited
PCMHs in Missouri,
53
contracting with MCOs through the LCCCP program and with
commercial plans. Fifty-three practices participate in CMS’ Medicare Comprehensive
Primary Care Plus Initiative (CPC+), in which Blue Cross Blue Shield of Kansas City and
50
MO HealthNet Community Psych Rehab Program Manual.
http://manuals.momed.com/collections/collection_cpr/print.pdf.
51
MO HealthNet Behavioral Health Services Manual. http://manuals.momed.com/collections/collection_psy/print.pdf.
52
CMS, “Shared Savings Program Accountable Care Organizations (ACO) Public-Use Files,” 2017, see:
www.cms.gov/Research-Statistics-Data-and-Systems/Downloadable-Public-Use-Files/SSPACO/index.html.
53
National Committee for Quality Assurance, “Practices,” see: reportcards.ncqa.org/#/practices/list?state=Missouri.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
24
UnitedHealth also participate; these practices receive care management fees and quality-
and efficiency bonus payments. No Missouri-specific results have been published.
• Health homes. Missouri was one of the first states to create health homes. Health homes
must meet specific quality criteria and receive a per member per month (PMPM) payment
for care management and other dedicated health home services. Primary care health
homes (PCHH) focus on patients with at least two physical chronic conditions, such as
diabetes, cardiovascular disease, or substance use disorder. As of 2017, PCHHs received
$63.72 PMPM for health home services; of the 38 PCHHs, 25 are federally qualified health
centers (FQHCs), 11 are hospital affiliated providers, and two are clinics. In 2018, 24,580
Medicaid participants were receiving care from PCHHs. According to evaluations published
by the state, PCHHs saved $98.35 PMPM, compared to baseline in 2016 (see Exhibit
13).
54
Lower actual and risk-adjusted PMPM costs for the PCHH population are partially
driven by lower inpatient costs (see Exhibit 14).
55
EXHIBIT 13: IMPACT OF PRIMARY CARE HEALTH HOMES: HOSPITAL USE, SFY2012-18
56
54
Missouri DSS, “Paving the way,” 2017, see: dss.mo.gov/mhd/cs/health-homes/pdf/pchh-paving-the-way.pptx;
Missouri DSS, “MO HealthNet PCHH Progress Report 2014-2017 FINAL 07192018,” 2018, analysis of Missouri
Medicaid claims data, SFY2016-18.
55
Analysis of Missouri Medicaid claims data, SFY2016-18.
56
Missouri DSS: see note 54.
Percentage of PCHH enrolees who had a hospitalization, %Percentage of PCHH enrollees who had an ED visit, %
87
63
41
39
23
17
12
Yr 5Yr 2 Yr 3BL Yr 6Yr 4Yr 1
58
35
24
17
14
11
8
Yr 3Yr 1 Yr 4BL Yr 2 Yr 5 Yr 6
4.7
0.5
BL Yr 1 Yr 2 Yr 6Yr 3 Yr 4 Yr 5
1.5
0.8
0.5
0.4
0.3
0.3
0.2
Yr 3BL Yr 1 Yr 2 Yr 5Yr 4 Yr 6
In total, the percentage
of high utilizers who are
admitted to the hospital
has been reduced by
86%.
The average number of
hospitalizations has
decreased by 87 % from
baseline to year six.
The impact of PCHH on ED and hospital use has been especially effective among high utilizers
There has been an 86%
decrease in ED visits for
individuals who are
considered to have high ED
or hospital utilization.
The average number of ED
visits decreased from 4.7
visits per person to less than
one visit/person by year six,
an 89% decrease.
% of high utilizers with ED visits % of high utilizers with hospital admissions
Average # of ED visits for high utilizers Average # of hospitalizations for high utilizers
43
37
32
31
31
30
28
Yr 4Yr 1BL Yr 3Yr 2 Yr 5 Yr 6
25
21
20
17
22
23
20
Yr 4Yr 3BL Yr 6Yr 1 Yr 2 Yr 5
There has been a 35%
decrease in ED use for all
PCHH enrollees from
baseline, through year 6 of
the PCHH program
There has been a 20%
decrease in hospital use
from the baseline,
through year six of the
program.
Utilization results across all PCHH enrollees
Utilization results across high utilizers

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
25
EXHIBIT 14: COMPARISON OF EXPENDITURES IN PCHH PROGRAM WITH NON-PCHH
PARTICIPANTS WITH COMPARABLE RISK-PROFILE (MANAGED CARE), SFY2018
57
Community mental health center health homes (CMHC HH) focus on patients with (serious)
mental illness and/or substance use disorder. CMHCs receive $85.23 PMPM to support the
infrastructure needed to deliver CMHC HH services; of the 28 CMHCs, 22 are clinics and six
are hospital affiliated providers (15 of these CMHCs have become certified community
behavioral health clinics [CCBHCs; see below]). As of January 2017, 24,844 participants
were enrolled in CMHC HH. An evaluation by the state concluded that in 2016, CMHC HHs
saved $284.94 PMPM compared to baseline (see Exhibit 15 for additional results).
58
To
compare participants served by CMHC HHs with participants with comparable conditions
and co-morbidities, individuals with high behavioral health needs were identified within the
CMHC HH population as well as in the non-HH population.
59
In this comparison, participants
in the non-dual disabled population show similar nominal PMPM costs but lower risk-
adjusted PMPM costs for the CMHC population. As in the PCHH analyses, these results
were driven partially by higher pharmacy costs and lower inpatient costs in the CMHC
57
Analysis of Missouri Medicaid claims data, SFY2016-18.
58
Missouri DMH, “DMH CMHC Healthcare Homes progress report,” 2016, see:
dmh.mo.gov/mentalillness/provider/docs/cmhchchprogreport16.pdf.
59
In these analyses, participants were flagged as having high behavioral health needs if they either (1) have
diagnoses of schizophrenia, bipolar disorder with psychosis, major depression w/ psychosis, attempted suicide or
self-injury, homicidal ideation, or substance use with pregnancy or one year postpartum OR (2) have one or more
behavioral health-related utilization of inpatient hospital visit, crisis unit visit, residential facility visit, rehab facility
visit, medication-assisted treatment, ED visit, or injection antipsychotics AND presence of bipolar disorder without
psychosis, major depression without psychosis, other depression, PTSD, substance use, conduct disorder,
personality disorder, psychosis, ODD, or eating disorders.
SFY2018
9%
8%
9%
10%
13%
20%
16%
13%
8%
7%
13%
34%
23%
5% 75M
1,447M
In PCHH
program
Not in PCHH
program
880
1,194
452
618
100,951
7,065
Ambulance and transportation Home and community-based
Other types of care
Ancillary services
DME and supplies
ED care
Hospital inpatient care
Hospital outpatient care
Specialty pharmaInstitutional care Treatment and evaluation at other sites
Lab and pathology
Office and clinic care
Physical, occupational, speech therapy
Radiology
Retail prescriptions
MANAGED CARE POPULATION
Spend by service category by HH enrollees, vs. comparable population
Total
members
included Breakdown of total spend
Risk-
adjusted
PMPM, $
Program
type
Actual
PMPM, $

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
26
population. This comparison could indicate that the CMHC is cost-effective, improving the
care for these patients (including utilization of needed drugs) and reducing potentially
avoidable hospital admissions (see Exhibit 16). (The results for the managed care
population, mostly children, did not show a comparable difference.)
EXHIBIT 15: IMPACT OF COMMUNITY MENTAL HEALTH CENTER HEALTH HOMES ON
HOSPITAL USE, SFY2011-2015
60
60
Missouri DMH: see note 58.
34%
28%
26%
22%
25%
45%
40%
34%
31%
31%
20
24
10
18
12
14
16
22
26
28
30
32
34
36
38
40
42
44
46
48
50
Yr 4BL Yr 1 Yr 2 Yr 3
Hospital ER
2.32
2.09
1.90
1.90
1.90
0.73
0.56
0.51
0.42
0.33
2011 14
0
12 13 2015
0.5
2.5
1.0
1.5
2.0
Avg # of ER visits/Enrollee/Year
Avg # of Hospitalizations/Enrollee/Year
Percent of enrollees with one or more hospitalization or
ER visit
Average ER and hospitalizations per enrollee per
calendar year
Average number of hospitalizations has been reduced 14%, and average emergency room visits decreased 19%

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
27
EXHIBIT 16: COMPARISON OF PARTICIPANTS WITH SEVERE BEHAVIORAL HEALTH
NEEDS IN CMHC PROGRAM WITH NON-CMHC PARTICIPANTS WITH SEVERAL
BEHAVIORAL HEALTH NEEDS (NON-DUAL DISABLED POPULATION), SFY2018
61
Certified Community Behavioral Health Clinics (CCBHC), a new initiative started in 2017,
focus on a similar patient population as CMHCs, and can also provide Health Home
services. Of the 28 CMHCs mentioned above, 14 have become CCBHCs (and one new
CCBHC has been created). As of November 2018, CCBHCs HHs served ~16,650 Medicaid
participants (largely participants who were enrolled in CMHC HHs before).
62
CCBHCs are
reimbursed using a prospective payment system, in which health home payments are
included. No results have yet been published.
– Bundled Payments. There are currently seven participating healthcare facilities in CMS’
Medicare Bundled Payment for Care Improvement (BPCI) Advanced program, which have
selected between one and 19 episodes, including sepsis, hip/knee replacement, and spinal
fusion surgery.
63
Additionally, 36 hospitals participated in CMS’ Medicare Comprehensive
Care for Joint Replacement (CJR) program in 2016-2017, earning savings of on average
~$2 million.
64
61
Excludes health home PMPM payments; analysis of Missouri Medicaid claims data, SFY2016-18.
62
Interviews with Medicaid program staff.
63
CMS, “BPCI Advanced,” 2018, see: innovation.cms.gov/initiatives/bpci-advanced/.
64
CMS, “Comprehensive Care for Joint Replacement Model,” 2018, see: innovation.cms.gov/initiatives/cjr.
SFY2018
8%
17%
25%
14%
22%
14%
8%
30%
23%
4%
591M
4% 65M5%
5%
6%
High acuity
BH
population in
CMHC
program
High acuity
BH
population
not in CMHC
program
3,449
3,379
816
1,034
1,582
14,579
Ambulance and transportation
Hospital outpatient careDME and supplies
Treatment and evaluation at other sitesED care
Ancillary services
Physical, occupational, speech therapy
Office and clinic care
Home and community-based
Hospital inpatient care
Institutional care
Lab and pathology
Other types of care
Radiology
Retail prescriptions
Specialty pharma
Spend by service category by HH enrollees, vs. comparable population
Total
members
included Total spend
Risk-
adjusted
PMPM, $
Program
type
Actual
PMPM, $
NON-DUAL DISABLED

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
28
Durable Medical Equipment
• The state follows a CMS fee schedule for most DME products (with exceptions such as
speech generation software and accessories, and certain types of hospital beds, which use
negotiated rates on a case-by-case basis). Total SFY2018 costs were $52 million, of which
27% were for respiratory DME, 27% were for bulky DME (such as wheelchairs and lift
chairs), 14% were for orthotics and prosthetics, and the remainder were for other DME
categories such as incontinence products and infusions.
65
• Utilization management techniques are in place for DME products. Prior authorization,
precertification, or meeting medical necessity criteria is required for most high-cost/high-
utilization products such as power wheelchairs and other bulky DME.
Potential opportunities for improvement
This section identifies potential opportunities to improve Missouri’s current approach to hospital
and physician reimbursement, as well as regulatory and stakeholder risks. The opportunities are
not intended to be mutually exclusive: opportunities for savings or improved outcomes may
overlap.
• The cost-based, single per diem payment method for hospital inpatient care
provides limited incentives to contain costs and improve quality. An outlier among
states, Missouri’s use of a single per diem lacks a direct connection between payments,
actual care provided, and types of patients served. This lack of incentive for efficiency is
exacerbated by the tight coupling between the reported cost of delivery and the level of the
per diem: increased costs lead to higher per diems. Most state Medicaid programs (similar
to Medicare and most commercial health insurers) currently use Diagnosis-Related Groups
(DRGs), which make a fixed payment for the entire stay in the hospital, creating cost-
containment incentives while also accounting for patient mix and severity.
66
• There is no inpatient readmissions policy. While Missouri spent $160 million on hospital
readmissions in SFY2018, it has no policies in place to address potentially avoidable
readmissions. CMS, MCOs, and other state Medicaid agencies have extensive experience
with such policies.
• The cost-based, outpatient payment method also contains limited incentives for
cost containment. Proactive outreach to avoid exacerbations of depression or
inefficiencies in diabetes care is not part of the standard fee schedule; in fact, reducing ER
visits or hospital (re-)admissions reduces revenue for providers in a FFS payment
system.
67
In addition, providers tend to have no access to data about the overall costs and
outcomes of the care they provide, making it difficult to fully mobilize to prevent potentially
avoidable complications and inefficiencies.
Most states use outpatient fee schedules that are indexed to Medicare’s fee schedule or
ambulatory payment group models.
68
Missouri has started to move towards a comparable,
65
Analysis of Missouri Medicaid claims data, SFY2016-18.
66
MACPAC, “State Medicaid Payment Policies for Inpatient Hospital Services,” 2018, see:
www.macpac.gov/publication/macpac-inpatient-hospital-ayment-landscapes.
67
Krupka, DC et al., “The Impact On Hospitals Of Reducing Surgical Complications Suggests Many Will Need
Shared Savings Programs With Payers,” 2012, Health Affairs, 31: 2571-78.
68
Such as Enhanced Ambulatory Patient Groups (EAPG) or Ambulatory Payment Classification (APC)
methodologies.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
29
Medicare-based outpatient fee schedule model, but has not yet completed that transition.
For SFY2020, the state currently estimates this transition to be budget-neutral.
69
Expansion of this approach could generate savings over time as hospitals improve
operational efficiencies. Savings could be realized more quickly depending on the
approach taken to setting prices under the new fee schedule.
• Several categories of high-cost outpatient services do not require prior
authorization. Prior authorization (PA) is limited to advanced imaging and select cardiac
procedures. Other states and MCOs incorporate measures to ensure appropriate utilization
on other OP procedures such as sleep studies, radiation therapy, and arthroscopies.
• Providing add-on payments to hospitals for non-Missouri residents served is a
unique feature of the Missouri Medicaid program. Throughout the U.S., hospitals
serving out-of-state Medicaid patients will be paid by the patient’s home state according to
that state’s Medicaid regulations. In Missouri, the state provides additional add-on
payments (estimated at approximately $177 million in SFY2019) to its hospitals for
services provided to persons eligible for Medicaid from Kansas, Illinois or elsewhere.
70
• Managed care payments to hospitals are set at a higher rate than FFS payments.
Excluding compensation for provider taxes, current MCO inpatient base payments are
approximately 30% higher than FFS per diem payments.
71
An estimated >$100 million of
MCO payments to hospitals are at rates above 120-130% of FFS payments.
72
• Variability in reimbursement levels between hospitals is significant. Excluding the
Medicaid portion of each hospital’s provider tax assessment, the difference between the
Medicaid payments hospitals received and their individual UPLs varied between <50% and
>150% of their hospital-specific UPLs in SFY2016.
73
The variation in outpatient procedure
fees is currently being reduced through the introduction of the Medicare-based outpatient
fee schedule.
• Physician reimbursement is lower than in most other states. Physicians are paid
based on a fee schedule that is historically linked to Medicare but is not regularly updated.
Reimbursement rates are less than in other states: Missouri Medicaid pays 79% of the
national average (ranked 46th); for primary care, the state pays 81% (ranked 42th).
Compared to Medicare fees, Medicaid pays 60% for overall physician services (ranked
44th) and 55% for primary care services (ranked 41th).
74
Spending on non-hospital
physician services, including Federally Qualified Health Centers (FQHCs), clinics, and rural
health services, is lower than other comparable states: In SFY2016, Missouri spent 5% of
69
Missouri DSS, “MHD – FY 19 Core exercise,” 2018.
70
Third-party analysis provided by MHD, 2018.
71
Third-party analysis provided by MHD, 2018.
72
Missouri DSS, “20181119 Medicaid Update,” 2018.
73
Missouri DSS, FY2016 UPL analyses; AHA Hospital Cost Report Files (HCRIS): CMS.Gov Case Mix Index Data;
Missouri DSS, FY2016 FRA schedule; FRA share of Medicaid revenue calculated by multiplying each hospital’s
FY2016 Medicaid revenue, the FRA tax rate (5.95% in FY2016), and the percentage of FRA payments from FFS
(91%, per the FRA schedule).
74
KFF, “Medicaid physician fees,” 2016, see: www.kff.org/state-category/medicaid-chip/medicaid-physician-fees/.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
30
total expenses on non-hospital physician services, as opposed to 9% in comparable
states.
75
• >15% of Missouri Medicaid acute care expenditures may be associated with
potentially avoidable exacerbations and complications (PECs). A PEC is any event
that negatively affects the patient and is potentially controllable by the health care delivery
system: an ER visit for an asthma exacerbation, a hospital readmission for a post-surgical
wound infection, or an emergency admission for a patient with a depression. PECs are an
inherent part of health care: a patient with bronchitis can develop a pneumonia, and post-
surgical complications will likely never be completely eradicated. But improving the
coordination and quality of care can significantly reduce the volume and costs of PECs.
76
As mentioned earlier, the current FFS reimbursement method does not reward
coordination of care or adequate care management. Likewise, preventing PECs tends to
negatively impact provider economics. Reducing such events, however, is an important
source of value for payors and patients alike: addressing PECs means reducing total costs
of care through improving outcomes for patients.
In Exhibit 17, the risk-adjusted total costs of care for the Medicaid managed care
population
77
are shown per county and mapped against the percentage of total costs that
are associated with PECs. The percentage of costs associated with PECs per county is
highly variable, ranging from <10% to >23%. (For persons with disabilities, the variability is
comparable; percentages range between 6% and 14%.)
78
Reducing PECs by 20% would
amount to ~$170 million in savings or opportunities for reinvestment.
75
FMR, 2016; comparable states are other states with enrollment in managed care of 30% or less (Alaska,
Arkansas, Alabama, Colorado, Connecticut, Idaho, Massachusetts, Montana, North Carolina, North Dakota,
Oklahoma, South Dakota, Vermont, and Wyoming).
76
De Brantes, F, A Rastogi, and M Painter, “Reducing potentially avoidable complications in patients with chronic
diseases,” 2010, Health Serv Res, 45: 1854-71.
77
Excluding dually eligible beneficiaries.
78
PECs percentages are lower for this population as a larger proportion of the spending is LTSS spending, which is
not included in PECs.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
31
EXHIBIT 17: POTENTIALLY AVOIDABLE EXACERBATIONS AND COMPLICATIONS AND
RISK ADJUSTED SPENDING BY COUNTY, MANAGED CARE POPULATION
79
There are several ways value-based payment could support reducing PECs: incentivizing high
quality, integrated primary care; rewarding a focus on high-cost patients who cycle in and out
of ERs and hospitals (for persons with disabilities, 4% of participants account for nearly one-
third of all ER visits) (see Exhibit 18); and strengthening the role of behavioral health care
throughout the care cycle (mental health and substance use are the main reasons for hospital
admissions amongst the individuals with disabilities, and – after maternal and newborn care –
the second main reason in the children and adults population). See Exhibit 19 for the
admissions for mental health diagnoses in the non-dual disabled population.
80
79
Analysis of Missouri Medicaid claims data, SFY2016-18; excludes counties <15,000 member-months. “Managed
Care Population” refers to those individuals eligible for managed care: children, parents, and pregnant women.
80
Analysis of Missouri Medicaid claims data, SFY2016-18.
7% 8% 9% 10% 11% 12% 13% 14% 15% 16% 17% 18% 19% 20% 21% 22% 23% 24% 25% 26% 27%
% Total cost associated with PECs
Better
performance
260
280
300
320
340
360
380
400
420
440
460
480
500
520
540
560
580
600
620
640
Risk adjusted
PMPM
County, bubble size
represents total $ paid
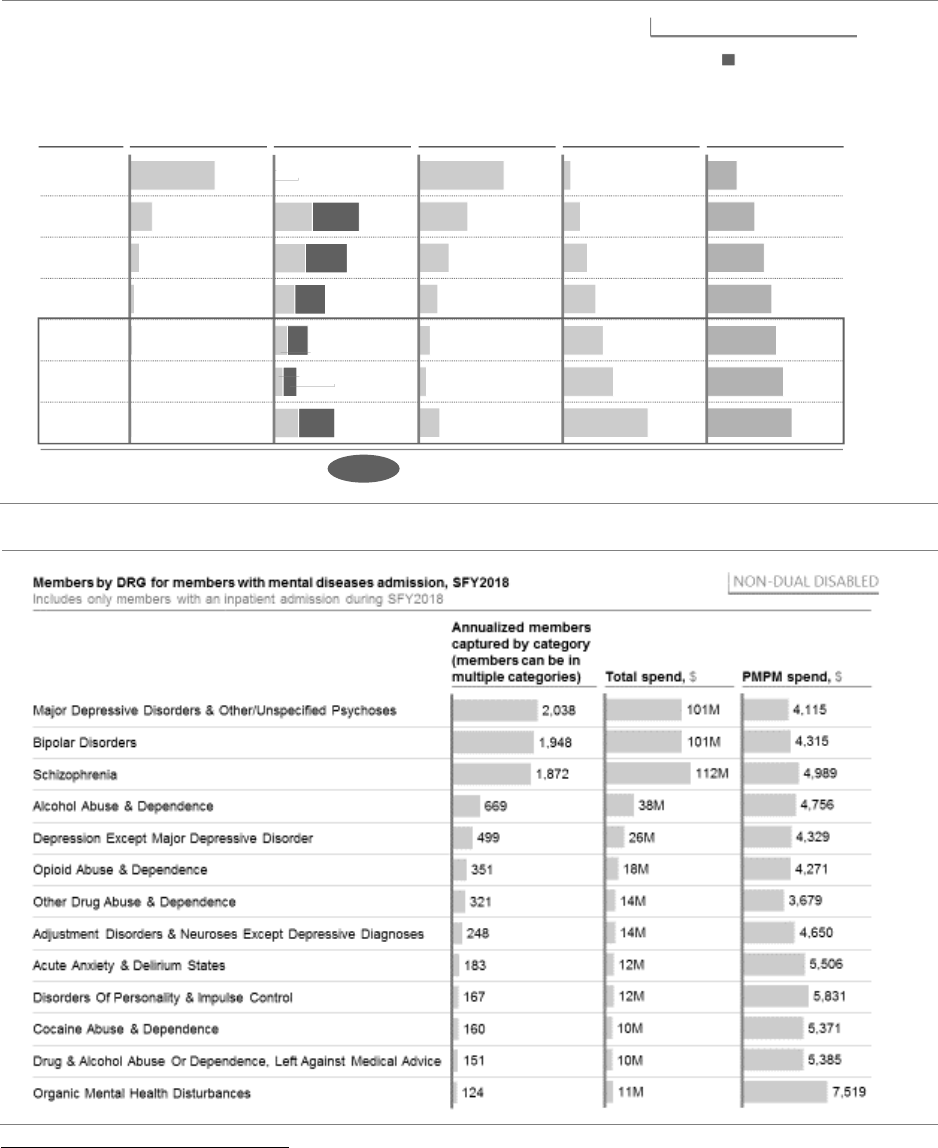
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
32
EXHIBIT 18: 4% OF MANAGED CARE PARTICIPANTS ACCOUNT FOR ALMOST ONE-
THIRD OF ED VISITS, OF WHICH >50% ARE POTENTIALLY AVOIDABLE
81
EXHIBIT 19: HOSPITAL ADMISSIONS IN THE NON-DUAL DISABLED POPULATION
82
81
Analysis of Missouri Medicaid claims data, SFY2016-18.
82
Analysis of Missouri Medicaid claims data, SFY2016-18; excludes top and bottom 2.5% of episodes by cost.
13
5 visits
4 visits
0 visit 561
1 visit
2 visits
3 visits
6+ visits
148
65
31
15
8
Members
(K)
Grand
total:
841 K 621 K
0
58
0
8973
8060
26
40
68
39
26
17
47
ED visits
(K)
SFY2018
1,150
156
256
661
406
106
285
$2,860 M
171
372
521
694
849
1,065
1,783
288
456
545
618
664
730
810
Spend PMPM ($)
ED visit
count
Risk adj spend
PMPM ($)
Total medical
spend
(M)
$299 $369
Potentially avoidable
MANAGED CARE POPULATION
58%

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
33
• 5-10% of Missouri Medicaid acute care expenditures may be associated with the
location where services are provided and the choice of diagnostics and
interventions. FFS does not incentivize efficiency considerations in making diagnostic or
therapeutic decisions, nor does it stimulate providers to select the most cost-effective
location to perform these services. Serving people in the ER is costly compared to serving
them in a doctor’s office; opting for an MRI scan where a CT scan could suffice is similarly
inefficient. The risk-adjusted variation in spending per county is ~100%, driven partially by
differences in hospital admissions that do not appear to be due to differences in overall
differences in risk score per county (see Exhibit 20 and Exhibit 21). In general, across all
payors, Missouri’s hospital utilization is high compared to that of other states (see Exhibit
22). Analyzing spending per episode of care shows similar variability in expenditures:
Exhibit 23 illustrates that perinatal care costs also vary ~100% for perinatal care between
high-volume zip codes.
83
As with PECs, some efficiencies may be unavoidable: the MRI
may simply be available faster, or the primary care practice – as an alternative to the ER –
might be closed. Yet reducing these inefficiencies tends to be feasible. Reducing these
inefficiencies by 20%, without negatively impacting the quality of care, would amount to
$55 million to $110 million in savings or opportunities for reinvestment.
84
EXHIBIT 20: RISK ADJUSTED SPENDING BY COUNTY, MANAGED CARE, SFY2018
85
83
Analysis of Missouri Medicaid claims data, SFY2016-18. Some of these admissions and costs may be due to
PECs.
84
Calculation: 20% of 5-10% of $5.7 billion (total acute care spending) = $55-110 million (rounded).
85
Analysis of Missouri Medicaid claims data, SFY2016-18; not calculated for counties with fewer than 1,000
managed care-eligible Medicaid-enrolled residents (“N/A”).
MANAGED CARE POPULATION
Total cost of care PMPM by county, SFY2018
Lowest quartile (< $326)
2nd quartile ($326 – 347)
3rd quartile ($347 – 376)
Highest quartile (> $376)
N/A
Cape
Girard-
eau
Audrain
Barry
Bates
Benton
Bolli-
nger
Boone
Butler
Callaway
Camden
Carter
Cass
Cedar
Chariton
Christian
Clay
Cole
Cooper
Craw
ford
Dade
Dallas
Dent
Franklin
Gas-
conade
Greene
Henry
Hickory
Howard
Howell
Iron
Jackson
Jasper
Jefferson
Johnson
Laclede
Lafayette
Lawr-
ence
Lincoln
Mcdonald
Madison
Maries
Miller
Mississippi
Moniteau
Mont
gomery
Morgan
New Madrid
Newton
Oregon
Osage
Ozark
Perry
Pettis
Phelps
Pike
Platte
Polk
Pulaski
Ralls
Ray
Reynolds
Ripley
St. Charles
St. Clair
Ste. Genevieve
St.
Francois
St. Louis
Saline
Scott
Shannon
Stoddard
Stone
Taney
Texas
Vernon
Warren
Washin-
gton
Wright
St. Louis City
Adair
Andrew
Atchison
Caldwell
Clark
Daviess
De
Kalb
Grundy
Harrison
Lewis
Linn
Livingston
Macon
Marion
Mercer
Nodaway
Scotland
Shelby
Sullivan
Buchanan
Web-
ster
Carroll
Douglas
Wayne
Barton
Monroe
Ran-
dolph
Gentry
Worth
Clinton
Holt
Knox
Putnam
Schuyler

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
34
EXHIBIT 21: INPATIENT ADMISSIONS BY COUNTY, MANAGED CARE, SFY2018
86
EXHIBIT 22. HOSPITAL USE COMPARED TO OTHER STATES (ALL-PAYORS)
87
86
Analysis of Missouri Medicaid claims data, SFY2016-18; not calculated for counties with fewer than 1,000
managed care-eligible Medicaid-enrolled residents (“N/A”).
87
KFF, “Hospital Outpatient Visits per 1,000 Population by Ownership Type,” 2016, see: www.kff.org/other/state-
indicator/outpatient-visits-by-ownership.
MANAGED CARE POPULATION
Inpatient admissions by county, SFY2018
Lowest quartile (<102 per 1,000)
2nd quartile (102 – 112 per 1,000)
3rd quartile (113 – 120 per 1,000)
Highest quartile (> 120 per 1,000)
N/A
Audrain
Barry
Bates
Benton
Bolli-
nger
Boone
Butler
Callaway
Camden
Cape
Girard-
eau
Carter
Cass
Cedar
Chariton
Christian
Clay
Cole
Cooper
Craw
ford
Dade
Dallas
Dent
Franklin
Gasconade
Greene
Henry
Hickory
Howard
Howell
Iron
Jackson
Jasper
Jefferson
Johnson
Laclede
Lafayette
Lawr-
ence
Lincoln
Mcdonald
Madison
Maries
Miller
Moniteau
Mont
gomery
Morgan
Newton
Oregon
Osage
Ozark
Pemiscot
Perry
Pettis
Phelps
Pike
Platte
Polk
Pulaski
Ralls
Ray
Reynolds
Ripley
St. Charles
St. Clair
St.
Francois
St. Louis
Saline
Scott
Shannon
Stoddard
Stone
Taney
Texas
Vernon
Warren
Washin-
gton
Wright
St. Louis City
Adair
Andrew
Atchison
Caldwell
Clark
Daviess
De Kalb
Grundy
Harrison
Holt
Lewis
Linn
Livingston
Macon
Marion
Mercer
Nodaway
Putnam
Schuyler
Scotland
Shelby
Sullivan
Buchanan
Web-
ster
Ran-
dolph
Ste. Genevieve
Mississippi
New Madrid
Dunklin
Carroll
Clinton
Gentry
Worth
Knox
Monroe
Barton
Douglas
Wayne
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
35
EXHIBIT 23: VARIATION IN HIGH-SPEND EPISODES: PERINATAL, SFY2018
88
• There is little to no transparency of outcomes of care in Medicaid. Available data
(e.g., external quality reviews of the MHD managed care program)
89
covers a limited range
of performance measures. There is no readily publicly accessible information about the
outcomes of care delivered per (sub)population or condition and per (groups of) provider.
This limits consumer choice, accountability, and the opportunity and incentive for provider
self-improvement.
• The incentives embedded in several existing programs can be made stronger and
aimed more explicitly at the outcomes of care that matter most to participants. There
are opportunities to build upon the success of the primary care initiatives, Accountable
Care Organizations (ACOs), bundled payments, and health homes: increasingly link
upside incentives to the outcomes of care, and tie the rewards received to the amount of
savings realized. By reducing PECs by 1 percentage point in a Missouri managed care
population, a PCMH, health home or ACO with 50,000 attributed lives could receive $1.5
million
90
in savings shared to further invest in improving their care (assuming 50% shared
savings). Sharing in the savings could also help these providers to focus even more on the
social determinants that may drive up PECs.
88
Analysis of Missouri Medicaid claims data, SFY2016-18; figures are based on total claims-based expenditure
associated with a perinatal episode triggered by live birth diagnosis and delivery procedure code. The top and
bottom 2.5% of episodes by cost were excluded in analyses of variation.
89
Behavioral Health Concepts, “2016 MO HealthNet Managed Care Program External Quality Review: Report of
Findings,” 2016, see: dss.mo.gov/mhd/mc/pdf/2016-external-quality-review-report-mohealthnet-managed-care.pdf.
90
Estimate based on a 500 PMPM average spending of which 18% is associated with PECs.
10,000
1,000
14,000
0
2,000
3,000
6,000
4,000
5,000
7,000
8,000
9,000
11,000
12,000
13,000
15,000
16,000
Each vertical bar represents a zip code
High
avg.
episode
cost ($)
Low avg.
episode
cost ($)
MANAGED CARE POPULATION
Average episode cost by member zip code for all zip codes

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
36
• There are physician shortages in many parts of the state, particularly rural areas.
80% of Missouri counties are considered physician shortage areas, and only 10% of new
physicians enter rural primary care. At 267, the state falls below the national average
physician to patient ratio of 272 physicians per 100,000 people; for primary care, the state
has 87 PCPs per 100,000 people, compared to 91.7 nationally. In rural areas, these issues
are particularly challenging: of the 101 rural counties, 99 are Primary Medical Health
Professional Shortage Area (HPSAs), 97 are Mental Health HPSAs, and 95 are Dental
HPSAs.
91
This may contribute to system inefficiencies and the incidence of PECs: these
services tend to be key to avoiding PECs and can lead to institutional care when
community care might have been preferable. Creating innovative delivery or
reimbursement models fitting the challenges of rural healthcare is difficult within the limits
of the FFS fee schedules.
92
• The financial viability of many rural and safety net providers is precarious. Some
rural and safety net providers are financially frail, with year over year negative results.
Approximately 90% of safety net hospitals and ~60% of rural hospitals had negative
margins in SFY2016.
93
Without a rural health care infrastructure that is viable and meets
local community needs, access to care for rural Missourians could be threatened. This
could in turn lead to higher downstream costs due to missed (secondary) prevention
opportunities.
In addition to the previously outlined potential opportunities, there are regulatory and
stakeholder challenges which may impact current reimbursement approaches:
• Recent changes in CMS IP Upper Payment Limit (UPL) calculations may result in inpatient
payments exceeding the UPL and thus a corresponding loss of federal funds. UPLs limit
state Medicaid FFS spending on specific provider classes (e.g., hospital inpatient) to what
Medicare would have paid for these services. For IP, both FFS base payments, out-of-
state payments, and add-on payments count against the IP UPL. FFS payments that
exceed the UPL are not eligible for federal match. CMS has recently introduced a new
template to calculate the inpatient UPL, leading to Missouri’s inpatient payments to
possibly exceed the UPL by $16 million.
94
• Missouri’s tax rate is currently within the federal safe harbor limit (6%), but regulatory
scrutiny of exact mechanisms used to compensate hospitals for tax payments could
increase. Alternatively, CMS may reduce the current 6% provider tax limit below which it
has so far allowed comparable payment arrangements in several states to e.g. 5% or even
3%.
95
• Provider tax compensation arrangements in FFS and managed care are under pressure as
hospitals that are net contributors to pooling mechanisms may opt out.
96
Under the
existing MHA pooling mechanism, participating providers who receive more in estimated
91
Association of American Medical Colleges, “2017 State Physician Workforce Data Report,” 2017, see:
members.aamc.org/eweb/upload/2017%20State%20Physician%20Workforce%20Data%20Report.pdf.
92
Missouri DHSS, “Health in Rural Missouri Biennial Report 2016-2017,” 2017, see:
health.mo.gov/living/families/ruralhealth/pdf/biennial2017.pdf.
93
AHA Hospital Cost Report Files (HCRIS); CMS.Gov Case Mix Index Data.
94
UPL calculation, Missouri DSS, January 2019.
95
KFF: see note 12.
96
MHA: see note 49.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
37
FRA-related add-on payments than their provider tax payments contribute to the pool so
that other hospitals can be compensated. If pool contributors withdraw from the voluntary
transfers, the pool would become less able to compensate pool recipients, thus
exacerbating the concern of some hospitals with the provider tax.
• In SFY2016, Medicaid made $19.7 billion in DSH payments nationally ($8.5 billion in state
funds and $11.2 billion in federal funds). A reduction of $4 billion is planned for 2020, with
the reduction increasing to $8 billion for each year from 2021 to 2025.
97
This could lead to
a substantial reduction in available federal DSH funding for the state.
• CMS may recoup parts of DSH payments made to hospitals from previous years’
allotments. Many states and hospitals have operated under the assumption that third-party
payments did not have to be included in Medicaid DSH payment calculations and audits. In
2017, however, CMS issued a final rule stating that inclusion was needed, which has since
been contested in several courts. If CMS prevails, this could lower hospital-specific DSH
limits, creating, for example, a potential risk for Missouri hospitals of $96 million from 2011
and 2012 allotments alone.
98
• Missouri’s DME rates are higher than CMS’ DME fee schedule across most product
categories. Commercial payors, MCOs, and some state Medicaid agencies set DME rates
significantly below CMS’ DME rates (between approximately 65% to 75%); Missouri’s DME
fee schedule is currently priced at over 100% of CMS’ DME rates. The variance between
current pricing and pricing at 70% of CMS’ DME rates is >$10 million.
99
Potential initiatives
The following is a wide range of potential initiatives that Missouri Medicaid may consider, either
in combination or as alternatives for improving the financial sustainability of the program. In
total, the gross impact of the hospital, physician and behavioral health reimbursement initiatives
outlined below could range from $250 million to $500 million, depending on choices made by
the state. This excludes the impact on provider tax revenues (see the section on federal
financing).
Potential initiatives to improve incentives and reduce costs include adjusting the inpatient (IP)
and outpatient (OP) base rate methodologies and the add-on payments for out-of-state patients.
Following other states, Medicare and commercial plans, Missouri could also consider
transitioning further to value-based payment models and transparency of care costs and
outcomes, which would maximize incentives for providers to deliver high-quality care while
lowering costs. Through the latter, the state could work to address the significant costs
associated with potentially avoidable exacerbations and complications (PECs) as well as other
inefficiencies. In addition, value-based payment models could facilitate investments in the rural
and safety net heath care infrastructure, including primary and behavioral health.
To achieve the higher end of the estimated impact range, the state would likely need to combine
a focus on adjusting hospital reimbursement rates and utilization management with a broader
97
MACPAC, “Disproportionate share hospital payments,” see: www.macpac.gov/subtopic/disproportionate-share-
hospital-payments.
98
Modern Healthcare, “CMS appeals Missouri court decision stopping DSH clawback,” 2018, see:
www.modernhealthcare.com/article/20180416/NEWS/180419941.
99
Analysis of Missouri Medicaid claims data, SFY2016-18; CMS, “DME18-A,” 2018, see:
www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/DMEPOSFeeSched/DMEPOS-Fee-Schedule-
Items/DME18-A.htm.
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
38
value-based payment program in which providers could share in the savings realized across the
total cost of care or in episodes of care. The state could choose its preferred balance between
these approaches, which would imply choosing between those initiatives that address similar
opportunities in different ways. The list below is intended as an outline of potential options for
the state, providing the state with the opportunity to decide on both sizing and timing of the
potential implementation of a selection of initiatives.
1. Implement an inpatient hospital readmissions policy. Inpatient hospital readmission
policies are used by commercial payors, MCOs, other state Medicaid programs, and CMS
to not only ensure appropriate utilization of services but also to improve quality. This policy
could be modeled after policies that MCOs have today and further refined by the state.
This could help ensure safe and appropriate discharge of participants and would also
provide important feedback to hospitals. Operationally, this initiative would require modest
policy and MMIS changes.
2. Expand prior authorization (PA) to additional outpatient procedures. PA policies are
likewise used by commercial and other payors. This initiative could add select categories
to the current PA list, and it could potentially make changes to the approach used in the
existing outpatient PA process. This may require additional system edits and updates to
current vendor contracts.
3. Adjust outpatient base rate methodology. Missouri could consider further anchoring
outpatient base rate payments to a percentage of Medicare fee schedule rather than a
percentage of charges across all outpatient services. This could allow Missouri to improve
alignment between payments and services provided, increase predictability of outpatient
expenditures, and be better able to compare rates both within the state and with other
states. In addition, the Medicare fee schedule evolves with changes in the science and
practice of medicine, thus ensuring the appropriateness of the payment methodology over
time. As this transition has already been set in motion, the implementation complexity of this
initiative would be limited.
4. Adjust inpatient base rate per diem methodology. To increase provider incentive for cost
containment, Missouri could adopt a stratified per diem for inpatient services, offering
different per diem rates for different types of patients (e.g., medical, surgical, maternity,
neonatal, psych). Rates could be set in one of two ways: 1) based on current payment levels
using a state-set trend factor, which would build off current price-setting methodology; or 2)
based on regional average costs for each per diem category. Both approaches would likely
improve alignment between payments and services offered, but they would not maximize
cost containment incentives given the pay-per-service setup. The second approach, basing
rates on regional average costs, may better improve alignment between payments and
services as it eliminates link to historical costs. But additional risk adjustment would likely be
necessary to capture within-region variations across hospital types (e.g., safety net hospitals
may not incur the same costs as non-safety net). While it would not be challenging to
implement the change from a regulatory respective, redesigning the per diem methodology
– including ensuring a smooth transition without disruptive impact on reimbursements of
individual hospitals – is not a well-standardized approach and is likely to be complex from a
technical and operational standpoint.
5. Consider case rate methodology for inpatient and/or outpatient services. Missouri
could move away from per diems and payments for individual outpatient services toward a
case rate-based reimbursement model. Such models employ a grouping mechanism that
varies for inpatient and outpatient services and are in use in many other states. For

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
39
outpatient, widely used grouper options are Enhanced Ambulatory Patient Groups (EAPG)
and Ambulatory Payment Classification (APC). For inpatient, the standard is Diagnosis-
Related Groups (DRG). Like the stratified per diem method above, pricing could be based
on regional average costs or historical pricing with forward-looking trend factors set by the
Medicaid program. Although payments are no longer determined at the individual service
level, this payment methodology would still be volume-focused and hence would still limit
cost containment incentives. The implementation complexity will likely be significant: in
particular, the change from single inpatient per diem payments will require a thorough
rebasing effort so that the transition is within the planned inpatient expenditures, remains
predictable, includes the needed add-ons, and does not create financial disruptions for
individual providers. In addition, the current MMIS is not currently equipped to handle case
rate-based reimbursement models. Workarounds through additional DRG grouping
applications exist, but these would have to handle all payments to hospitals.
6. Reevaluate add-on payments for out-of-state (non-MO) residents. Missouri could
reduce or eliminate the reimbursements it makes to hospitals for treating out-of-state
patients. Out-of-state payments are concentrated in a limited set of hospitals. The technical
implementation complexity of this initiative is likely to be low, but the impact on affected
providers may be significant.
7. Modify Direct Medicaid payments methodology. The Direct Medicaid payments (one
component of the add-on payments) attempt to bridge the gap between base rate payments
and the hospitals’ costs to serve the Medicaid population. The state could consider limiting
the reliance on cost reports so that reduced utilization or reductions in payments due to
other initiatives are not compensated by increased Direct Medicaid payments.
8. Apply UPL caps to individual hospitals. The state could consider applying hospital-
specific outpatient and inpatient UPL caps. Currently, consistent with federal regulations, the
state applies UPL caps to the total of payments made within the applicable service category,
but it does not apply individual hospital’s UPL caps. As the UPL in Missouri is significantly
impacted by the OOS payments, reducing them would affect the UPLs of the recipients of
OOS payments.
9. Adjust MCO hospital payments. The state could cap MCO hospital payments at a fixed
percentage of Medicaid FFS payments.
100
This initiative would require a modification of
MCO contracts.
10. Improve physician and behavioral health reimbursement. For physicians, not only has
the methodology for establishing rates (e.g., as a percentage of Medicare) not been
updated, but once set, the rates do not change. As a result, physician reimbursement is low.
It is likely that increasing reimbursement could help reduce provider shortage. Likewise,
there is a shortage of behavioral health providers. The state could consider integrating this
initiative in an overall VBP program.
11. Re-examine payment levels for financially vulnerable rural and safety net providers.
To the extent that other initiatives are undertaken that could reduce revenue to hospitals
generally, the state could consider re-examining the effects of the initiatives on financially
vulnerable rural and safety net providers in particular to determine whether adjustments in
payment levels, value-based payment structures, or other changes are necessary to
mitigate the potential for erosion of access to care.
100
Missouri DSS: see note 72.
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
40
12. Transition to value-based payments. In line with the healthcare industry trend led by other
states, Medicare, and commercial plans, Missouri could consider moving from its current
FFS payment methods to value-based payment (Alternative Payment Models, or APMs). In
VBP, providers do not miss or lose revenue by increasing efficiencies and reducing
potentially avoidable care services, as they tend to do in FFS. Rather, APMs allow providers
to be rewarded if they reduce hospital (re-)admissions and nursing home admissions. This
creates a strong business case for providers to invest in primary care, care coordination,
integration of physical and behavioral health care, and home health care. In addition, if
investing in social determinants of health creates net savings in Medicaid expenditures,
shared savings or other VBP payments can be leveraged to fund those services.
Some forms of value-based payment could be implemented without changing the
underlying architecture of the current FFS payment methods by overlaying rewards (and in
some cases penalties) on top of FFS payment streams. This would facilitate
implementation, as current administrative and billing processes, including the role of the
MMIS, would require little change. The additional analytical capabilities required for VBP
tend to be delivered by vendors, requiring limited interaction with the MMIS. With a
combination of models, building upon current, successful initiatives, Missouri could include
most Medicaid participants in VBP initiatives:
– Population-based models. Advanced Primary Care models (APCs) build on the PCMH
model but increase accountability for improved outcomes of the total attributed
population and total cost of care. Improvement in these parameters leads to higher
bonus payments and a share in the savings realized. Accountable care organizations
(ACOs) take this responsibility for the total costs and outcomes of care for a population
one step further. If the ACO manages to reduce total costs of care below a target
budget (usually based on the historical costs of care of the ACO’s population), they
receive up to 50% of the savings. ACOs can be upside-only (e.g., only savings are
shared), or they can include up- and downside risk (e.g., both potential savings and
losses are shared). As risk-based APMs reduce the payor’s risk for losses, they can
share significantly higher percentages of the realized savings (up to 100%) with the
providers. ACOs can be led by primary care organizations, hospitals, and (virtually)
integrated groups of providers, amongst others.
For specific high-need subpopulations (e.g. individuals with co-morbidity, severe mental
illness, and/or substance use disorder), the existing health home model(s) could be
leveraged to further improve outcomes.
Population-based models stimulate a focus on prevention and the management of
chronic disease and individuals with severe comorbidities: avoiding the need for
(institutional) care (including many PECs) is the most cost-efficient way to realize
savings.
– Bundled payments or episode-based models. In episode-based models, providers
assume responsibility for the costs and outcomes of a set of services to treat a certain
clinical condition or conduct a certain procedure. Like an ACO, episodes have target
budgets, and they can be upside-only or risk-based. Episode-based models stimulate
the creation of patient-centered care pathways across organizational boundaries. PECs
and the inefficient utilization of care services are addressed through care coordination.
Episodes tend to achieve impact faster as population-based models, as the
opportunities for improvement tend to be clear and specific. Several private and public
payors have combined population- and episode-based payments to create a “best-of-

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
41
both-worlds” mix of incentives for population health and high-value condition-specific
care.
– Global budgets for rural hospitals. In rural areas, the state could consider global hospital
budgets. Sixty-seven percent of Missouri counties have less than 5,000 managed care
Medicaid participants. Access to primary care physicians and hospital facilities can be
difficult, and the financial viability of many rural hospitals is under pressure. For such
hospitals, global budgets (based on the expected cost of the hospital services for an
attributed population) could create financial stability and facilitate transformation to a
care delivery model aligned with local community needs. The establishment of regional
ACOs or advanced primary care models with, for example, performance-dependent
PMPM care management fees could further help to mature these geographies’ regional
care infrastructure.
EXHIBIT 24: MEDICAID ENROLLMENT PER COUNTY, DISTRIBUTION OF BEDS,
SFY2016
101
13. Create transparency for outcomes of care. Providing transparency of outcomes for
(sub)populations and key conditions/procedures is a prerequisite of any health care
system oriented towards value. Juxtaposing these outcomes to the risk-adjusted costs of
care shines light on the performance of the healthcare delivery system and provides the
information providers, payors, participants, and policymakers require to make informed
choices and focus improvement efforts. As the collection point of all Medicaid claims
101
Analysis of Missouri Medicaid claims data, SFY2016-18.
12
24
34
38
41
44
46
48
100
50
51
53
54
56
57
58
59
60
62
63
64
65
66
67
68
69
5K or less 5 - 10K 10 – 15K 15K or more
Total members distribution by county, SFY2018
Audrain
Barry
Barton
Bates
Benton
Bolli-
nger
Boone
Butler
Callaway
Camden
Cape
Girard-
eau
Carroll
Carter
Cass
Cedar
Chariton
Christian
Clay
Cole
Cooper
Craw
ford
Dade
Dallas
Dent
Douglas
Dunklin
Franklin
Gasconade
Greene
Henry
Hickory
Howard
Howell
Iron
Jackson
Jasper
Jefferson
Johnson
Laclede
Lafayette
Lawr-
ence
Lincoln
Mcdonald
Madison
Maries
Miller
Mississippi
Moniteau
Monroe
Mont
gomery
Morgan
New Madrid
Newton
Oregon
Osage
Ozark
Pemiscot
Perry
Pettis
Phelps
Pike
Platte
Polk
Pulaski
Ralls
Randolph
Ray
Reynolds
Ripley
St. Charles
St. Clair
Ste. Genevieve
St Francois
St. Louis
Saline
Scott
Shannon
Stoddard
Stone
Taney
Texas
Vernon
Warren
Washington
Wayne
Webster
Wright
St. Louis City
Adair
Andrew
Atchison
Caldwell
Clark
Clinton
Daviess
De Kalb
Gentry
Grundy
Harrison
Holt
Knox
Lewis
Linn
Livingston
Macon
Marion
Mercer
Nodaway
Putnam
Schuyler
Scotland
Shelby
Sullivan
Worth
Buchanan
Size: Avg. # of
beds in FY16
≤100
100-200
200-400
>400
Critical access hospitals
Private hospital systems
Rural
Safety net
Academic hospitals
Other
Annualized members K
Cum.
%
Share of total members
1
(%)
St. Charles
Greene
20
32
St. Francois
Boone
Jasper
Jackson
18
140
St. Louis
Pemiscot
Clay
Jefferson
12
Buchanan
Callaway
Christian
Franklin
Butler
12
Pettis
14
24
Cass
15
Washington
13
Cape Girardeau
14
Barry
12Scott
Platte
Lincoln
Other
139
McDonald
355
17
18
50
30
24
114
14
14
14
13
13
St. Louis city
16
Grand total 1,156 K

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
42
data, the state could publish such information on the total costs and outcomes of care
per county or (group of) provider(s).
102
14. Include MCOs in a VBP program to maximize impact and align incentives for
providers across the total Medicaid population. The majority of Medicaid program
participants are enrolled in MCOs.
103
To create the volume for providers to be
sufficiently incentivized to participate, both FFS and managed care participants may
need to be included, and the APMs across MCOs and Medicaid FFS may need to be
adequately aligned. If some MCOs implement bundles and others carve out ACO
subpopulations in different ways, providers cannot (and will not be motivated to) make
the investments to change their business models. In addition, without alignment between
APM definitions, the measurement of outcomes and financial performance will likely not
be statistically feasible. Following the example of an increasing number of states,
Missouri could consider working with its MCOs to facilitate this alignment and change
MCO contracts accordingly.
15. Explore multi-payor VBP alignment. To further increase the potential impact of value-
based payment, the state could consider collaborating with non-Medicaid payors in the
state to align APMs and set collective goals. To significantly increase impact (see
previous initiative), multi-payor models are becoming increasingly widespread: CMS’
Comprehensive Primary Care models (CPC and CPC+) are an example. Two options
the state could explore are, first, alignment with the other main state government payor,
the Missouri Consolidated Health Care Plan (MCHCP).
104
Second, the state could
consider engaging with CMS to facilitate mutual alignment between the existing and
forthcoming Medicare APMs and the Missouri VBP strategy.
105
16. Update the DME fee schedule. Missouri could update its DME rates to match those of
other state Medicaid agencies and MCOs, which could potentially be supported by
competitive procurements in specific categories. Operationally, this would require a
change in the fee schedule, potential procurements, and efforts to ensure access.
102
Transparency of costs and outcomes requires a minimum number of attributed participants to allow comparisons;
individual professionals, for example, may not see sufficient participants to be meaningfully compared to others.
103
To optimally align incentives between the state, the MCOs and providers in APMs, Missouri could consider
carving in pharmacy and behavioral health for the MCO population.
104
Including MCHCP would add approximately 100,000 lives. See: http://www.mchcp.org.
105
This could be relevant for both duals (who make up a disproportionately large share of both Medicaid’s as well as
Medicare’s total spending) as well as for non-duals (where alignment between APMs would increase impact in the
same way as alignment with other payors would).

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
43
LONG-TERM SERVICES AND SUPPORTS
Certain elderly populations and others with disabilities are eligible to receive long-term services
and supports (LTSS) to assist with activities of daily living and otherwise support greater
independence. Before receiving LTSS, Medicaid-eligible individuals undergo an assessment
process, which determines eligibility but does not impact placement, type, or intensity of
services to be provided. Once individuals are deemed eligible, the services they may receive fall
into two categories: 1) institutional services and 2) home and community-based services
(HCBS, which can be split into residential and non-residential services). Nursing facilities are
reimbursed using a cost-based payment methodology without adjustments for acuity, quality of
care, or outcomes. As a result, there are minimal incentives for these facilities to provide
differentiated care to high-needs patients, or to transition lower-needs participants back to their
homes or the community. HCBS are provided through a combination of State Plan and waiver
programs; HCBS providers are not held accountable for nursing home (re-)admission rates.
Opportunities to improve quality and control costs of LTSS are primarily to be realized from
increasing the proportion of LTSS recipients that receive services at home or in the community
rather than in more costly institutional settings, and improving care planning and care
management of members regardless of their setting of care.
106
Potential initiatives include
improving utilization management, adjusting the nursing facility reimbursement methodology to
an acuity-based system, completing and expanding upon planned improvements to the
assessment algorithm and process, expanding current grant- or waiver-funded programs to
cover services that support individuals in the home or community, and shifting to value-based
payment. In total, the gross impact of the LTSS initiatives could range from $90 million to $275
million, net of potential reinvestments in the delivery system, depending on choices that the
state may make in the selection, design, and implementation of initiatives.
107
Current situation
This section gives an overview of the population receiving LTSS in Missouri, the assessment
and service authorization process, institutional services, and HCBS.
LTSS population and services
In SFY2018, approximately 106,000 individuals received LTSS in Missouri, representing 39% of
the state’s total aged, blind, and disabled (ABD) population.
108
However, spending for recipients
of LTSS, which was approximately $2.9 billion in SFY2018, represented 71% of the state’s total
spending on the ABD population. 53% of Medicaid elderly and 33% of persons with disabilities
receive LTSS (see Exhibit 25).
109
106
IBM Watson Health, “Medicaid Expenditures for Long-Term Services and Supports in FY 2016,” 2016, see:
www.medicaid.gov/medicaid/ltss/downloads/reports-and-evaluations/ltssexpenditures2016.pdf.
107
AARP, Commonwealth Fund, SCAN Foundation, “Long-Term Services & Supports State Scorecard,” 2018, see:
longtermscorecard.org/databystate/state?state=MO; IBM Watson Health: see note 106.
108
Analysis of Missouri Medicaid claims data, SFY2016-18.
109
Analysis of Missouri Medicaid claims data, SFY2016-18.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
44
EXHIBIT 25: LTSS PARTICIPANTS ~40% OF ABD POP’N, 70% OF COSTS, SFY2018
110
There exist several publicly available reports and datasets that compare performance of the
LTSS system across states. These sources reveal several insights about the current
performance of Missouri’s system. For example, Missouri is ninth in the country on the
performance of its No Wrong Door system, which is a national program to streamline access
to new LTSS options, improving the patient experience and potentially reducing cost of
care.
111
In addition, the state is near the top quartile of states when ranked by the share of
LTSS expenditures that goes towards HCBS. In SFY2018, approximately 61% were for home
and community-based services (see Exhibit 25). The national average of the HCBS proportion
of total LTSS spending was 57% in SFY2016.
In other areas, Missouri performs below the national average. For example, the state ranks
49
th
in the country in the percentage of nursing home residents that have low care needs (24%
vs. the national average of 11%), suggesting opportunities for a greater share of LTSS
recipients to be supported within the home and/or community.
112
Furthermore, Missouri ranks
42
nd
in the country in the employment rate (19% vs. the national average of 22%) for adults
with Activities of Daily Living (ADL) disabilities, relative to those without them.
110
Analysis of Missouri Medicaid claims data, SFY2016-18; Validation checks performed against Table 23 suggests
a total of 1.04 million beneficiaries after inclusion of Women's Health Services (977k not including Women’s Health
Services). There is ~12% gap in enrollment due to differences in participant accounting (e.g., exclusion of non-
claimants).
111
AARP, Commonwealth Fund, SCAN Foundation: see note 107.
112
AARP, Commonwealth Fund, SCAN Foundation: see note 107.
27%
(1.5B)
100% =
61%
(165K)
39%
(106K)
5.5B
Members
52%
(2.9B)
20%
(1.1B)
Non-LTSS
spend for
LTSS
beneficiaries
Spend
LTSS spend
Spend for
non-LTSS
beneficiaries
270K
SFY2018 LTSS beneficiaries, K, and spend, $
Breakdown of SFY2018 Medicaid participants by
eligibility type, K
Elderly (81)
Total Medicaid
members
Managed care
population
(903)
Non-ABD
population
Disabled
(189)
ABD population
1,173
270
▪ LTSS analysis is focused on 270K participants in ABD population that make up 23% of total Medicaid
enrollment
▪ Across the elderly and disabled beneficiaries, we found that individuals receiving LTSS services make up
~40% in enrollment but ~70% of total spend
Individuals
receiving
LTSS
Individuals
not
receiving
LTSS

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
45
Non-institutional services with the highest overall spending are residential services and
personal care.
113
Residential services are covered exclusively by DMH’s Comprehensive
Waiver (see “HCBS” section for additional details on this waiver). Personal care is covered by
both the State Plan and almost all the waivers. The State Plan pays for the personal care for
the majority (58%) of LTSS participants.
See Exhibit 26 for a breakdown of the LTSS spending by service category and the number of
participants receiving services in each category.
114
EXHIBIT 26: BREAKDOWN OF LTSS SPENDING BY SERVICE CATEGORY, SFY2018
115
Assessment and service authorization
Individuals can receive LTSS through either DHSS or DMH. DHSS follows different
authorization procedures for adults and for children. For adults, personal care services can be
either agency-directed (e.g., where a state agency is responsible for managing participants’
personal care, including selection and supervision of personal care assistants) or consumer-
directed (e.g., where the participants manage their own services by selecting, hiring, and
supervising their own personal care assistants). For adults, LTSS can also include institutional
care (nursing homes). DHSS uses the interRAI HC assessment (commonly used nationally) to
113
Analysis of Missouri Medicaid claims data, SFY2016-18.
114
Analysis of Missouri Medicaid claims data, SFY2016-18.
115
Analysis of Missouri Medicaid claims data, SFY2016-18; participants may overlap across categories.
Residential services 661
Targeted case management
Community services
701
Skilled nursing facility
Intermediate care
Counseling and therapy
Adult day care / day habilitation
LTSS Other
Career and financing
Personal care
Personal care
Private duty nursing
Respite care
Targeted case management
Private duty nursing
1,041
84
182
10
5
5
63
16
4
58
27
20
9
Institutional
Total spend = $ 2,886M
SFY2018
Waiver
HCBS
State plan
HCBS
Total LTSS spend, $M
Share of total
LTSS spend
Average participants, K
Share of total
LTSS pop.
Total pop =
105.2K participants
0.4
1.2
29.8
0.3
1.5
6.1
5.8
15.0
6.8
3.4
0.2
0.4
13.3
61.7
6.0
LTSS service category
24%
58%
1%
0%
0%
6%
2%
13%
1%
14%
36% 28%
6%
6%
0%
6%
0%
1%
0%
1%
23%
6%
2%
3%
1%
0%
3% 0%
0%
1%

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
46
determine need for institutional level of care. For children, personal care services – which must
be agency-directed – can be authorized through the Bureau of Special Health Care Needs and
are renewed every six months. For these children, the criterion for care is medical necessity
rather than institutional level of care needs. Meanwhile, DMH has multiple assessments and
determines which to use primarily based on the age of the individual (e.g., the MOCABI
116
for
adults; the Vineland assessment or another age-appropriate
117
substitute for children).
The department conducting the assessment then processes the results of the assessment to
determine whether the individual is eligible to receive LTSS. DHSS uses a points-based system:
individuals who receive a score of 24 points or above are eligible for institutional level of care,
which makes them eligible for LTSS offered through DHSS. On the other hand, if DMH
determines that the individual has two or more (three or more for waivers) functional limitations,
the assessor completes a Level of Care form to demonstrate the need for intermediate care
facility for individuals with intellectual disabilities (ICF/IID) level of care.
Once an individual is deemed eligible for LTSS, the departments then engage in person-
centered care planning, in which case managers work directly with individuals to determine
setting, level, and type of care to be provided. For services provided through DHSS (except for
those provided through the Independent Living Waiver), person-centered care planning is
performed by regional assessors. For the Independent Living Waiver, person-centered care
planning is provided through targeted case management (TCM) providers covered under the
waiver. For services provided through DMH, care planning is performed by TCM providers
covered by the Medicaid State Plan. The care planning process does not consistently use the
results of the assessment to inform the setting, level, or type of care authorized. Rather,
assessors are trained to use an HCBS manual (for DHSS services) or an Individual Support
Plan (ISP) guide (for DMH services) to inform what, where, and how much of each service can
be authorized, but unlike many other states, Missouri does not require that the assessor follow
these guidelines.
Institutional services
Nursing facilities are reimbursed using a cost-based per diem methodology at the facility level.
While not uncommon among states, this methodology does not take into account patient
acuity, intensity of service, quality, or outcomes in determining nursing facility payment levels.
As a result, nursing facilities are not necessarily incentivized to provide cost-efficient or
appropriate levels of care. Furthermore, the per diem rates are based on historical cost reports
that can date back over two decades; yearly incremental adjustments are determined by the
state legislature. In total, Missouri’s nursing facility payments fall well below the nursing facility
Upper Payment Limit.
118
Approximately 40% of the funds used to pay nursing facility reimbursement is derived from the
Nursing Facility Federal Reimbursement Allowance (NFFRA).
119
Like other states, Missouri
taxes nursing facilities and uses these revenues to fund Medicaid and draw down federal funds
at the Missouri federal match rate of 65.4%.
120
116
Missouri Critical Adaptive Behaviors Inventory.
117
Interviews with Medicaid program staff members.
118
UPL analysis, Missouri DSS, 2018.
119
Missouri DSS, “SFY 2014-2019 Rate by Funding Source & Cost Component – 9-28-18,” 2018.
120
KFF: see note 12.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
47
For individuals with intellectual and/or developmental disabilities, the state operates four public
ICFs/IID known as habilitation centers, which collectively house 315 participants, and contracts
with a number of private ICFs/IID, which house another 82 individuals, totaling 397 participants
in 2018 (down from 435 in 2017).
121
This number will likely continue to trend downward, as the
state plans to reduce admissions in Missouri ICFs/IID further.
HCBS
Missouri covers HCBS through a combination of State Plan and waiver programs. State Plan
services include targeted case management, personal care, and private duty nursing. For these
services, individuals who exhaust the maximum amount allowed by the State Plan may then
access additional allotment of these services through waivers, which cover care beyond what
the State Plan is able to fund. Waivers can include a broad range of services, such as personal
care and residential services. These waivers do not qualify for enhanced federal match, and
each waiver has an expiration date, at which point the state can elect to renew the waiver or
allow it to expire.
There are nine HCBS waivers, four of which are administered in coordination with DMH and five
of which are administered in coordination with DHSS. While these waivers use various rate-
setting mechanisms, they are fundamentally cost-based. Most individuals can only be on one
waiver at any given time. HCBS are split between residential and non-residential services.
Residential services, which include shared living and group home services, serve over 6,800
individuals, primarily through the DMH Comprehensive Waiver.
The set of waivers
122
includes the following (see Exhibit 27 for a summary of trends in costs
and participant count in these waivers):
• Aged and Disabled Waiver (DHSS through the Department of Senior and Disability
Services / DSDS, served 15,200 individuals in Waiver Year [WY] 2016): For individuals
age 65 years and older (or 63 and older if they have disabilities) that have impairment and
unmet needs. Services covered include homemaker and chore services, home-delivered
meals, respite, and adult day care.
• Adult Day Care Waiver (DHSS through DSDS, served 1,588 individuals in WY16): For
individuals age 18 to 63 years with impairments and unmet needs. This waiver exclusively
covers adult day care services.
• Independent Living Waiver (DHSS through DSDS, served 190 individuals in WY16): For
individuals age 18 to 64 years with cognitive and/or physical disabilities but also the ability to
self-direct. This is the only one of the nine waivers that covers targeted case management;
part of the waiver’s purpose is to serve as a continuation of State Plan targeted case
management.
123
It is also the only one of the five DHSS waivers that explicitly covers self-
directed personal care.
• Comprehensive Waiver (DMH, served 8,882 individuals in WY15): For individuals with
intellectual and/or developmental disabilities. This is the only one of the nine waivers that
121
Missouri DSS, “State Operated Habilitation Centers,” 2018.
122
DHSS waivers with < than 400 individuals served (number served in WY16): AIDS Waiver (90), Medically Fragile
Adult Waiver (166). DMH waivers with <400 individuals served (number served in WY15): MO Children with
Developmental Disabilities Waiver (320).
123
Interviews with Medicaid program staff members.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
48
covers residential services (e.g., group home, shared living, individualized supported living;
see Exhibit 28), but it also covers a range of other services, including personal care.
• Community Support Waiver (DMH, served 1,886 individuals in WY15): For individuals
with intellectual and/or developmental disabilities who already have a place to live in the
community. Given that requirement, residential services are not covered by this waiver, but it
otherwise covers the same range of services as the Comprehensive Waiver. It has an annual
per capita cost cap of $28,000.
• Partnership for Hope Waiver (DMH, served 2,614 individuals in WY15): For individuals
with intellectual and/or developmental disabilities who reside in one of 104 Missouri
counties plus St. Louis City. It covers the same set of services as the Community Support
Waiver – in addition to others, such as dental services – and it has an annual per capita
cost cap of $12,362.
EXHIBIT 27: COST PATTERNS FOR THE LARGEST LTSS WAIVERS
124
124
Missouri DHSS, “HCBS Waivers DHSS,” 2018; Missouri DMH, “HCBS Waivers DHS,” 2018.
17,378
17,067
16,343
15,280
15,200
-3% p.a.
95.5
99.9
64.8
75.4
94.2
-10% p.a.
5,749
5,518
5,846
4,936
4,266
-7% p.a.
15.4
14.7
14.4
8.9
+20% p.a.
268
187
135
152
190
14132012 201615
-8% p.a.
201615142012 13
1.7
1.8
1.7
0.5
1.6
-2% p.a.
6,772
9,147
3,839
10,716
8,772
2012 13 14 15 2016
+7% p.a.
1,333
1,543
1,522
1,588
+6% p.a.
6,673
9,338
9,640
9,703
+13% p.a.
567.2
621.6
630.8
512.7
+7% p.a.
8,126
8,442
8,461
8,503
+2% p.a.
63,091
67,193
73,461
74,190
+6% p.a.
19.2
27.0
23.1
15.6
+20% p.a.
1,406
1,504
1,560
1,886
+10% p.a.
11,087
12,741
14,817
14,338
+9% p.a.
5.8
14.0
10.1
13.3
+34% p.a.
1,314
2,009
2,373
2,614
+26% p.a.
4,445
5,023
5,589
5,372
+7% p.a.
Costs by waiver year
USD, millions
Number of individuals served by
waiver year
PMPY, USDName of the waiver
Adult Day Care
Waiver
Comprehensive
Waiver
Community Support
Waiver
Partnership for Hope
Waiver
Aged and Disabled
Waiver
Independent Living
Waiver

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
49
EXHIBIT 28: SERVICES COVERED ACROSS LTSS WAIVERS
125
While Missouri Medicaid covers a range of HCBS, the plurality of spending is for personal
care, covered by both the State Plan and every waiver except for the Adult Day Care Waiver.
Potential opportunities for improvement
This section identifies potential opportunities to improve Missouri’s current approach to LTSS.
The opportunities are not intended to be mutually exclusive: cost savings opportunities
identified in individual opportunities may overlap with those identified in others. When
compared to experiences and practices in other states, the following observations can be
made:
• The patient journey to get access to LTSS can be complex. Three state agencies
(DSS, DHSS, and DMH) play a role in the process of determining eligibility for LTSS and
planning care for LTSS recipients. As a result, while Missouri has adopted the principle of
“no wrong door” for eligibility and access to LTSS, the participant journey (see Exhibit 29)
can be complex and can vary widely depending on the participant’s condition and entry
point into the system.
125
Missouri DMH and DHSS: see note 124.
Operated by DHSS Operated by DMH
Aged and
Disabled
Independent
Living
AIDS
Medically
Fragile Adult
Adult Day Care
Comprehensive
waiver
Community
Support
MOCDD
Partnership for
Hope
Waiver
Service category
Community
services
Counseling
and therapy
Residential
services Other
1
Career and
financing
Adult day
care/day hab
Personal
care
Private duty
nursing Respite
Supplies and
technology
Targeted case
management

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
50
EXHIBIT 29: LTSS PATIENT-CENTERED PROCESS FLOW
126
• The DHSS assessment process to determine need for institutional level of care
uses decades-old standards and, as such, may not consistently determine
institutional level of care needs. DHSS is currently considering changes to the
algorithm it has used to determine nursing facility level of care. Although the state has
changed the threshold scores for determining LTSS eligibility, the algorithm has not
meaningfully changed since 1982.
127
• Assessment results are not consistently used to inform setting of care, type, or
intensity of services authorized. The care planning process currently does not
consistently use the results of the level of care assessment to inform the plan of care. As
a result, the setting of care, services, and service levels participants are authorized to
receive may not be consistent across programs or care planners, and the care provided
may not match participants’ needs.
• Personal care services are administered inconsistently depending on the channel
through which they are received. For example, utilization of consumer-directed
126
Interviews with Medicaid program staff members.
127
Missouri DSS, “Rules of Department of Health and Senior Services, Division 30-Division of Regulation and
Licensure, Chapter 81-Certification,” 2018, see: www.sos.mo.gov/cmsimages/adrules/csr/current/19csr/19c30-
81.pdf.
Patient receives
personal care
funded by State
Plan
Assess-
ment to
determine
and
Medicaid
eligibility NF
level of care
Case manager
develops person
centered care plan to
determine service
types and levels to
authorize
Institutional
/ residential
Personal
care
Other State
Plan
service
Non-PC
DMH
waiver
service
Patient receives
personal care
funded by
waiver(s)
1
▪ Patient is deemed not eligible
for LTSS services if score is
below 24 points on
assessment (i.e., below NF
level of care)
▪ If receiving DMH waiver,
patient must receive case
management; otherwise
targeted case management
provided only if necessary
▪ State Plan services that are
also covered by waivers (e.g.,
dental, PT/OT/ST for children,
applied behavioral analysis for
children with autism, DME)
require that patients exhaust
coverage from State Plan first
before seeking waiver
coverage
▪ Patients seeking just teaching
and cueing services can
receive services through DMH
waiver directly
3
4
1
2
3
4
Non-PC
DHSS
waiver
service
Service authorization Service delivery
Assessment
of patient
Targeted case
management to
determine service
types and levels to
authorize
2
Administered by DHSS
Administered by DMH
Administered by either DHSS or DMH
Potential service options

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
51
personal care services is almost two times higher than the agency-directed model.
128
Currently, so long as a given participant is eligible to receive consumer-directed care, she
may elect to choose it (e.g., participants are not allocated to one or the other). The
difference in utilization does not appear to be correlated with participant mix or participant
risk. In addition, average reimbursement rates vary depending on whether they are
provided through DMH or through DHSS; while these rates have converged in recent
years, there remain differences in rates, primarily due to funds available for each
department’s waivers.
129
• Nursing facility rates are based on historical costs, and they do not reimburse
based on patient acuity or create incentives for quality or outcomes. While there are
yearly adjustments to the per diem rates, the rates are based on cost reports from
SFY2001 (trended to SFY2005).
130
Although these per diems are intended to cover
nursing facilities’ costs, the reimbursement methodology does not necessarily reflect their
current costs. Additionally, there is little correlation between nursing facility per diem rates
and either patient acuity or facility quality (see Exhibit 30: darker bubbles represent
facilities that experience higher patient acuity on average, while bubbles on the right
represent facilities with higher Star ratings).
131
Currently, per diem rates vary from
$135.08 to $175.41 by facility, meaning the facility with the highest per diem rate receives
approximately 30% more than the facility with the lowest per diem rate.
132
Finally, per
diem rates do not incentivize facilities to discharge residents or attempt to avoid
admissions where feasible.
128
Analysis of Missouri Medicaid claims data, SFY2016-18.
129
Missouri DSS, “Adult Day Care Waiver,” 2018; Missouri DSS, “Aged and Disabled Waiver,” 2018; Missouri DSS,
“Aids Waiver,” 2018; Missouri DSS, “Community Support Waiver,” 2018; Missouri DSS, “Comprehensive Waiver,”
2018; Missouri DSS, “Independent Living Waiver,” 2018; Missouri DSS, “Medically Fragile Adult Waiver,” 2018;
Missouri DSS, “MOCDD Waiver,” 2018; Missouri DSS, “Partnership for Hope Waiver,” 2018; Missouri DSS, “Private
Duty Nursing,” 2018; Missouri DSS, “State Plan Personal Care,” 2018; Missouri DSS, “Targeted Case
Management,” 2018; interviews with Medicaid program staff members.
130
Missouri DSS, “Rules of Department of Social Services, Division 70-MO HealthNet Division, Chapter 10-Nursing
Home Program,” 2018, see: www.sos.mo.gov/CMSImages/AdRules/csr/current/13csr/13c70-10.pdf.
131
Analysis of Missouri Medicaid claims data and MDS data, 2016-18.
132
Missouri DSS, “Nursing Facility Rate List,” 2018 (updated 7/1/2018), see:
dss.mo.gov/mhd/providers/pages/nfrates.htm.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
52
EXHIBIT 30: SKILLED NURSING FACILITIES BY PER DIEM, STAR RATING, SFY2018
133
• Nursing homes have a relatively high number of low-acuity Medicaid residents. In
Missouri, 23.7% of nursing home residents have low care needs (e.g., could potentially be
adequately served through HCBS services) compared to the national median of
11.2%.
134
Diverting participants with low care needs to HCBS to reach the level of
median state performance could yield a reduction of spending of up to $90 million.
135
• Occupancy rates in nursing facilities are relatively low. With an average nursing
facility occupancy rate of 72%, Missouri ranks 43rd amongst other states, with the top 12
at occupancy rates of 88% or higher.
136
With further reductions likely, the inefficiencies
inherent to low occupancy rates will increase, and some nursing homes may not be able
to maintain their current business model.
• Additional waivers or grants could provide key services to certain subpopulations.
For example, the Money Follows the Person (MFP) program is set to expire. Extending it
or substituting it with a waiver may help ensure that individuals transferring from nursing
133
Acuity measured as average score on 10 MDS functional status questions (e.g., Section G0110) on most recent
25 days of information retained by the state. Providers with fewer than 15 data points excluded. High complexity
refers to SNFs with average ADL score of 4+; low with an average score of 2 or less; analysis of Missouri Medicaid
claims data and MDS data, 2016-18.
134
AARP, Commonwealth Fund, SCAN Foundation: see note 107.
135
IBM Watson Health: see note 106.
136
KFF, “Certified Nursing Facility Occupancy Rate,” 2016, see: www.kff.org/other/state-indicator/nursing-facility-
occupancy-rates.
146
148
140
168
158
164
176
166
154
156
170
150
162
160
152
36
144
136
138
142
High complexity Medium complexity Low complexity
Bubble size indicates total spend
Per Diem rate,
$
Star rating, number of stars
1 2 3 4 50
Some SNFs are
paid higher than
average despite
low STAR ratings,
suggesting
potential
opportunity to
redirect care to
higher quality
providers
Providers with
high quality of
care and low per
diem rates

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
53
facilities or habilitation centers have access to the resources they need to facilitate their
transitions. By shifting more people from institutional settings back to the community, this
change could result in savings of $12.5 million to $14 million.
137
Additionally, the state
could consider following through on discussions to implement a waiver that covers
children with developmental disabilities who do not require habilitative services, which
would cover the cost of care for children who do not qualify for Medicaid because of their
parents’ income. Currently, children need to be hospitalized for a certain period before
they can be considered eligible for Medicaid regardless of parental income; this may
result in children being hospitalized even if it does not suit the level of care they require.
• There may be additional opportunity to provide care for participants in less
intensive and restrictive settings even across the continuum of HCBS services.
Though a substantial amount of rebalancing from institutional to residential and other
HCBS (waiver and State Plan) services has taken place, there may be opportunity to
transition members receiving residential services in congregate care settings away from
their homes to less intensive and restrictive settings within the continuum of HCBS
services. See Exhibit 31 for a breakdown of LTSS spending based on utilization levels of
different services.
138
137
Interviews with Medicaid program staff members and analysis of state data, 2018.
138
Analysis of Missouri Medicaid claims data, SFY2016-18.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
54
EXHIBIT 31: LTSS UTILIZATION FOR LTSS ADMINISTERED BY DMH, SFY2018
139
• There are limited incentives connecting reimbursement of HCBS providers and
outcomes of care. Reimbursement of HCBS providers is not tied to their success in
keeping their clients out of nursing homes (or other forms of residential care). Likewise, as
payment is based on units of care delivered, there is no economic incentive to stimulate
participants’ independence from care. Payments to provider groups that aim to relocate
participants from nursing homes or residential care facilities to their homes could be tied
to their success rate, for example. Sharing in the savings could also help these providers
to focus even more on the social determinants that often stand in the way of successful
transition.
• There is little to no transparency of outcomes of care in LTSS. While available data
on the performance of LTSS in Missouri show mixed results, there is little or no publicly
accessible information about the outcomes of care delivered per (sub)population or
condition and per provider (or group thereof). This limits consumer choice, provider
accountability, and the information necessary for provider self-improvement.
139
Only considers population receiving services from administered by DMH; analysis of Missouri Medicaid claims
data, SFY2016-18; residential services include individual supported living, group home, and shared living services;
CRG stands for Clinical Risk Group.
4.6
<0.1
<0.1
0.4
0.4
<0.1
<0.1
0.1
2.2
0.4
6.8
0.4
0.6
4.4
<0.1
0.1
2.9
6.0
6.0
3.0
3.0
5.5
5.5
5.6
5.5
5.5
6.0
5.8
6.0
6.6
6.6
7.0
6.3
6.1
62
137
95
45
36
28
24
37
149
213
22
1
71
212
22
14
21
Waiver PCAICF
State Plan PCAA
Residential Other HCBS
Average spend by service
category, $K PMPY
Utilization
CRG risk score
Average annualized
beneficiaries, 000
ICF / IIDs
HCBS
1
(excl.
residen-
tial
services)
Residen-
tial
services
0-30 days
31-60 days
31-60 days
90+ days
61-90 days
0-30 days
Overall
11-20 hr / wk
21-40 hr / wk
41-80 hr / wk
0-10 hr / wk
Overall
81-120 hr / wk
160+ hr / wk
121-160 hr / wk
90+ days
Overall
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
55
Potential initiatives
Based on a review of Missouri’s current approach, interviews with functional leaders and subject
matter experts within the relevant departments, and analysis of other states’ activities, this
section discusses potential initiatives Missouri could consider to improve the value of LTSS in
the state, which include reducing costs and, through increasing the number of participants that
would be able to remain in their own homes and/or in the community, possibly improving
participant experience, quality, and outcomes. In total, the gross financial impact of LTSS
initiatives ranges from $90 million to $275 million, depending on choices made by the state.
1. Include an acuity adjustment in the nursing home reimbursement methodology.
Missouri could consider adding an acuity adjustment to the current per diem methodology.
By using an acuity adjustment such as a resource utilization group (RUG)-based grouper,
Missouri could categorize patients based on need and reimburse nursing facilities
accordingly, using a stratified set of per diem rates. This shift would enable allocation of
resources based on need. Additionally, it may encourage further rebalancing from
institutional care to HCBS.
2. Rationalize rates for similar HCBS services provided through different programs and
funding authorities. For services provided through multiple waivers or through a
combination of State Plan and one or more waivers (e.g., personal care services), Missouri
could consider standardizing rates independent of the funding source for the service.
Without standardization, providers may be reimbursed different amounts for care provided
to patients with similar needs and acuity levels, which may encourage them to participate
selectively in certain programs while not participating in others. This may result in access
issues in certain programs and/or geographic areas, eroding patient experience and
outcomes. DHSS has engaged an external vendor to conduct a rate study to determine the
validity of the reimbursement rates for services covered in their waivers, which may reveal
further opportunities to rationalize rates.
3. Complete and expand upon revisions currently underway to assessment algorithm
and process. The state recently announced changes to DHSS’ algorithm to assign points
using the interRAI HC assessment instrument, which represent the first major changes
since 1982. These revisions could improve the accuracy of the level of care assessment
process. The state could also consider further streamlining and strengthening the
assessment process across populations, programs, and departments (e.g., improving
capture of personal care data with review on a per-reviewer and per-physician basis,
especially in the consumer-directed program).
4. More directly employ assessment results in care planning process. In addition to
improving the assessment process as is currently planned, Missouri could consider
incorporating additional functionality into the assessment instrument. First, it could be used
to determine eligibility for services. Second, it could more closely tie results of assessment
to the care planning process. For example, DHSS has previously considered using a case
rate-based system, using a RUG-based grouper mechanism layered on top of the current
interRAI HC assessment. This could include more consistently using assessment results as
a standardized basis for setting of care determinations and the types and intensity of
services to be provided. Third, the assessment instrument could be used to determine
payment levels for care. Fourth, the assessment results could serve as an auditing
mechanism: care planners and/or providers could be flagged if they are providing a level of
care that is inconsistent with the results of the assessment.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
56
5. Improve the consistency of the approval process for personal care services. The
state could better capture personal care (PCA) PA data digitally and review it on a per
reviewer and physician level to ensure consistency in implementing assessment tools and
appeals processes. This would be especially important in the consumer-directed program,
as different PA approvers may be inconsistent in the type and degree of services they
authorize for different individuals with similar care needs.
6. Extend Money Follows the Person (MFP) through a new grant or waiver. On average,
MFP in Missouri has helped 206 individuals each year to transition back to their
communities.
140
The quality of life of individuals living at home may be much higher than it
may be for those living in an institution; in addition, the cost of a year of nursing home care
is $45,000, versus ~$8,300 for home-based care. According to experts interviewed, if the
state includes a rent subsidy for those in the MFP program, it could double the number of
transitions per year, to approximately 400 per year.
7. Implement additional waivers (e.g., waiver for children with developmental
disabilities who do not require habilitative services) or expand current waivers.
Implementing such a waiver would allow children who are ineligible for Medicaid because
of their parents’ income to receive Medicaid services without hospitalization. This would not
only allow children to receive care from the comfort of their homes, if they do not require
more intensive care, but would also potentially reduce the cost of care.
8. Missouri could consider introducing Alternative Payment Models (APMs) for LTSS
services. The main value opportunity for LTSS services is moving care from a nursing
home or residential services to care in the participant’s home where possible. The costs of
this care are generally less than half the cost of intuitional care and living at home tends to
be highly preferable.
141
Improving care planning and management for this population can
also be a significant source of value. An Accountable Care Organization model, specifically
designed for LTSS, may be one option to incentivize providers to create this value. Yet for
those providers most likely to do so – home care providers – taking on the financial
responsibility for nursing home costs is a large risk and is likely not feasible for many
smaller providers. Alternatively, such providers could be incentivized by tying a part of their
reimbursement to the key outcomes that matter to participants, such as the extent to which
they can be successful in delaying or avoiding nursing home admissions, improving self-
determination, encouraging independence at home, etc.
9. Create transparency of the outcomes of care. Providing transparency of outcomes for
(sub)populations is a prerequisite of any healthcare system oriented towards value.
Juxtaposing these outcomes to the risk-adjusted costs of care shines light on the
performance of the healthcare delivery system and provides the information providers,
payors, participants, and policymakers require to make informed choices and focused
improvement efforts. As the collection point of all Medicaid claims and assessment data,
the state could publish such information on the total costs and outcomes of care per county
per provider, or per group of providers.
140
Missouri DSS, “Money follows the person,” 2018.
141
Missouri DSS: see note 140.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
57
PHARMACY
In SFY2018, Missouri Medicaid spent ~$1.5 billion on pharmaceutical products.
142
Missouri is
one of four states that carves pharmacy out of its managed care arrangements.
143
This carve-
out gives the state complete responsibility for paying for and managing the utilization of drugs
for all participants. To ensure appropriate utilization and control spending, the state has
established a preferred drug list (PDL), which requires prior authorizations, step therapy, and
quantity limits for select drugs. Through its process of “grandfathering” treatment, Missouri does
not require participants that are established on a non-preferred drug to switch to a preferred
drug. In addition to the PDL, Missouri receives statutory and supplemental rebates from
pharmaceutical manufacturers as means of cost containment. The state uses a vendor to help it
maintain its PDL and to assist in supplemental rebate negotiations.
The state pays for retail drugs in two ways: an ingredient cost and a dispensing fee. In terms of
reimbursement for the ingredient cost, Missouri, like other state Medicaid agencies, has
converted to an average actual cost methodology. The state is in the process of revising its
dispensing fee.
Potential initiatives for Pharmacy include the elimination of grandfathering of drug selection,
implementing additional utilization management, joining a purchasing consortium to increase
supplemental rebate capture, requiring NDC submission on claims for non-J-code HCPCS
drugs, establishing a preferred specialty pharmacy, and applying for a value-based contracting
waiver from CMS. When combined, the potential impact of Pharmacy initiatives could range
from $35 million to $60 million, net of ongoing operational costs.
144
This savings opportunity is
variable and dependent on decisions that are made with respect to initiatives discussed in the
managed care and acute care services sections (e.g., including pharmacy as an MCO-covered
benefit).
Current situation
This section gives an overview of Missouri’s current pharmacy in terms of spending and
structure, reimbursement methodology, utilization management (UM) practices, clinical
guidelines and (for pharmacy) rebate capture.
Program spending and structure
In SFY2018, 25 drugs accounted for ~25% of Missouri’s $1.5 billion pharmacy spending, while
4141 drugs accounted for the other 75%. Total pharmacy costs have grown 5% over the last
three years. Treatment for attention-deficit/hyperactivity disorder (ADHD), hepatitis C,
behavioral health conditions, hemophilia, rheumatologic conditions, diabetes, asthma, growth
deficiency syndromes, and pain are the main drivers of pharmacy spending and growth (see
Exhibit 32).
145
142
Analysis of Missouri Medicaid claims data, SFY2016-18; only includes pharmaceutical products billed as
separate pharmacy claims.
143
KFF, “States Focus on Quality and Outcomes Amid Waiver Changes: Results from a 50-State Medicaid Budget
Survey for State Fiscal Years 2018 and 2019,” 2018, see: www.kff.org/report-section/states-focus-on-quality-and-
outcomes-amid-waiver-changes-pharmacy-and-opioid-strategies.
144
Analysis of Missouri Medicaid claims data, SFY2016-18; interviews with Medicaid program staff members.
145
Analysis of Missouri Medicaid claims data, SFY2016-18.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
58
EXHIBIT 32. 25 DRUGS ACCOUNT FOR ~25% OF PHARMACY SPENDING, SFY2018
146
Missouri carves pharmacy benefits out of its managed care program. Missouri’s SFY2018
spending of $1.5 billion was paid on a fee-for-service basis. All pharmacy program operations,
including utilization management, are the responsibility of MHD. Missouri also utilizes a
preferred drug list vendor. This vendor assists the state with supplemental rebate negotiation
and updating/reviewing the state’s PDL. Finally, the state has an open pharmacy network,
including an open specialty network. An open network allows participants to use any pharmacy
of their choice.
Reimbursement
Missouri uses a recently modified hierarchy method to determine reimbursement for drug
ingredient costs. Missouri reimburses covered drugs by applying a hierarchy method that
starts with National Average Drug Acquisition Cost (NADAC), followed by Missouri Maximum
Allowed Cost (MAC), and Wholesale Acquisition Cost (WAC). Missouri uses the usual and
customary (U&C) charge submitted by the provider if it is lower than the chosen price.
Reimbursement for covered drugs for 340B providers who carve-in for Medicaid was modified
by applying the following method: WAC-25% or the U&C charge submitted by the provider if it
is lower.
147
146
Analysis of Missouri Medicaid claims data, SFY2016-18.
147
Missouri DSS, “State of Missouri Pharmacy Manual,” 2019, see:
manuals.momed.com/collections/collection_pha/print.pdf.
Drugs
LATUDA
MAVYRET
INVEGA SUSTENNA
HUMIRA PEN
METHYLPHENIDATE ER
VYVANSE
PROAIR HFA
LYRICA
ADVAIR DISKUS
LANTUS SOLOSTAR
NORDITROPIN FLEXPRO
SYMBICORT
SPIRIVA
ADDERALL XR
ARIPIPRAZOLE
FLOVENT HFA
NOVOLOG FLEXPEN
SYNAGIS
OXYCONTIN
KOGENATE FS
METFORMIN HCL ER
PALIPERIDONE ER
ONFI
SUBOXONE
GENVOYA
36.0
28.9
28.8
20.7
20.6
20.6
18.9
18.4
16.6
16.5
15.9
15.0
12.8
12.6
12.2
11.9
11.7
10.8
10.4
10.1
9.7
9.1
8.8
8.5
8.5
SFY2018 Spend, ($M) SFY2017 to SFY2018 spend trend
3%
22%
16%
13%
-1%
6%
9%
-8%
-6%
18%
6%
-7%
-10%
-22%
16%
12%
-7%
-25%
110%
55%
13%
17%
39%
31%
-5%
65%
5%
-5%
-1%
-1%
-6%
-19%
-21%
14%
-1%
-24%
-2%
-6%
16%
-3%
-7%
-28%
52%
-13%
3%
13%
37%
26%
SFY2017 to SFY2018 utilization trend
New to the market in SFY2018

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
59
Missouri also has structured fees for reimbursement rates for pharmacy dispensing fees. The
state currently pays $9.55 in base dispensing fee to all pharmacy providers, and $4.82 in
enhanced dispensing fee to in-state pharmacy providers. In addition, $5.00 in preferred
generic product incentive fee is paid for each multi-source product to in-state pharmacy
providers. In addition to the retail fees, an additional $0.50 in long-term care dispensing fee is
paid per claim under specific circumstances. Outpatient physician-administered drugs are
reimbursed as a percentage of billed charges for hospital providers. These fees are under
active review with CMS.
148
Utilization management practices and clinical guidelines
Utilization management protocols are in place for a range of drug classes but lacking in some.
Prior authorization (PA), step therapy, and quantity limits are used across the PDL. However,
these UM techniques are lacking in certain drug classes (e.g., hemophilia, oncology). Newly
approved drugs are automatically placed on the PA list for the first six months after launch.
Additionally, Missouri uses an automated PA system for first-level clinical reviews. The system
can match participant diagnosis codes to approval criteria to generate automated
approvals/denials.
Rebate capture
The state collects both federal and supplemental rebates. Missouri’s SFY2018 federal and
supplement rebate capture rates were 52.4% and 3.0% of total pharmacy spending,
respectively.
149
All claims for physician administered drugs with “J” prefixed HCPCS codes are
required to be submitted with an NDC so that rebates can be captured.
The state’s PDL vendor negotiates supplemental rebates on its behalf. The state collects
supplemental rebates in various therapeutic categories such as: growth hormones, anti-virals
to treat hepatitis C, ADHD therapies, and drugs used to treat rheumatologic conditions.
The process for rebate invoicing to manufacturers is highly manual. This process involves
using different computer systems to compare claims and invoices. Additionally, it takes the
effort of multiple FTEs to convert data from one system to another, do quality checks, send
invoices to manufacturers, and review any appeals that come back from the manufacturers.
In Missouri, providers may choose to either carve-in to or carve-out of 340B. The state follows
the guidelines set forth by the Health Resources and Services Administration (HSRA). All
covered entity providers are identified as such by the state and rebates are not collected on
these drugs.
Potential opportunities for improvement
This section identifies potential opportunities to improve Missouri’s pharmacy program. When
compared to the practices of other states, the following observations can be made:
• Missouri’s expansive grandfathering practice limits the state’s ability to shift
utilization to the lowest net cost drug. While some states allow grandfathering for
specific drug classes, most require participants to follow changes to the PDL.
• For certain high-cost drug classes (such as oncology, hemophilia, and IVIG), there
are no medical necessity policies. MCOs and some state Medicaid agencies have
148
Missouri DSS, “Missouri MoHealthNet Provider Bulletin Volume 39 Number 52,” 2017, see:
dss.mo.gov/mhd/providers/pdf/bulletin39-52_2017april14.pdf.
149
Analysis of Missouri Medicaid claims data, SFY2016-18.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
60
medical policies and often use utilization management levers such as PA, step therapy,
and quantity limits to ensure appropriate utilization in these high-cost drug classes.
150
• Missouri’s rebate capture rates are below the national average. While federal rebate
capture has improved from 43.4% to 52.4% between SFY2016 and SFY2018, Missouri is
still below the weighted national average of 55.5% (see Exhibit 33) and further below the
highest-performing quartile. Additionally, the state’s SFY2018 supplemental rebate capture
rate of 3.0% also falls below the weighted national average of 3.8%.
151
These deviations
from the mean may be in part due to grandfathering practices or PDL design.
EXHIBIT 33: STATE-BY-STATE, FEDERAL REBATE CAPTURE IN SFY2016
152
• Missouri does not currently participate in any value-based contracts with
pharmaceutical manufactures. Value-based contracting is becoming more popular with
commercial and MCO players. Recently, CMS approved waivers for Oklahoma and
Michigan to negotiate value-based contracts with pharmacy manufacturers.
150
Missouri DSS: see note 147.
151
Medicaid.gov, “Expenditure Reports from MBES/CBES,” see: www.medicaid.gov/medicaid/finance/state-
expenditure-reporting/expenditure-reports/index.html; analysis of state data, 2018.
152
Medicaid.gov: see note 151.
FFS national rebate benchmarks, SFY2016
Alabama
Arkansas
Arizona
California
Colorado
Connecticut
Florida
Georgia
Iowa
Idaho
Illinois
Indiana
Kansas
Kentucky
Louisiana
Massachusetts
Maine
Michigan
Minnesota
Missouri
Mississippi
Montana
North Carolina
North
Dakota
Nebraska
New Hampshire
New Mexico
Nevada
New York
Ohio
Oklahoma
Oregon
Pennsylvania
South
Carolina
South
Dakota
Tennessee
Texas
Utah
Virginia
Vermont
Washington
Wisconsin
West
Virginia
Wyoming
Washington, DC
Delaware
Maryland
New Jersey
Rhode Island
Hawaii
Alaska
Data not available
Lowest Quartile 2nd Quartile 3rd Quartile Highest Quartile
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
61
Potential initiatives
Based on review of Missouri’s current approach, interviews with functional leaders and subject
matter experts, and analysis of other states’ activities, this section has identified six potential
initiatives Missouri could consider for improvements to its pharmacy program. These initiatives
build on the existing progress made by the state and could result in a reduction of total Medicaid
expenditures from $35 million to $60 million, depending on state choices.
1. Implement medical necessity guidelines and prior authorizations in drug classes that
do not have such policies. The state could implement new medical necessity policies for
oncology, hemophilia, IVIG, and other select high-cost physician-administered therapies.
This could not only bring Missouri in line with other states and MCOs but could also require
that participants are receiving care based on accepted clinical guidelines in the proper
clinical sequence. A vendor could be utilized to handle this process, or the process could be
done in-house.
2. Reduce grandfathering. Missouri could consider only targeted use of grandfathering for
specific drug classes (e.g., antipsychotics) based on an review of clinical need.
Operationally, some requirements would include proper notification to participants and
providers to ensure that all stakeholders are aware of pending changes and to avoid any
impact on access.
3. Join a purchasing consortium to increase supplemental rebate capture. There are
three supplemental rebate consortiums that state Medicaid programs utilize today: the
National Medicaid Pooling Initiative (NMPI), the Optimal PDL Solution (TOPS) and the
Sovereign States Drug Consortium (SSDC). Missouri would need to consider how these
consortia fit with their current approach and PDL vendor. Additionally, the state would need
to submit a State Plan Amendment to CMS.
4. Require NDC submission on claims for non-J-code HCPCS drugs. This initiative could
ensure that rebates are captured on all physician administered drugs. Operationally, some
requirements would include provider notification and modest MMIS system edits.
5. Consider whether to contract with a specialty pharmacy. The state could establish a
preferred specialty pharmacy which may provide lower prices for certain specialty drugs,
and potentially better care management and improved clinical outcomes for participants.
Before doing this, the state would need to determine whether such an approach would be
consistent with any willing provider regulations. Additionally, the state would likely have to
go through the required procurement process.
6. Apply for a value-based contracting waiver from CMS. The state could apply for a value-
based contracting waiver from CMS, which would allow the state to negotiate drug prices
with manufacturers based on clinical outcomes. CMS approval of a State Plan Amendment
would be required, as would negotiation with manufacturers to determine the optimal
drug(s), outcome(s), and pricing.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
62
MANAGED CARE
In 2017, Missouri’s managed care program for children and families was expanded statewide
under three capitated managed care organizations (MCOs).
153
The state has taken several
steps to improve the performance of the managed care program and ensure its value, and the
current managed care contracts attempt to create an environment that fosters innovation
through incentive programs and specialized care coordination programs. Nevertheless, both the
managed care contracts and rates can be improved to further increase efficiency, eliminate
ambiguity in contract language, and lay the foundation for improved MCO performance and
state-of-the-art performance management. Finally, the state could consider increasing the
scope of managed care and carving in pharmacy and behavioral health services for the current
managed care populations. The state could also consider introducing managed care for (parts
of) the ABD population or continuing to improve management of those populations outside of
the managed care program.
The total potential impact across these initiatives ranges from $175 million to $300 million, net of
recurring investments.
154
While there are opportunities to improve the performance and
efficiency of the current managed care program, the largest component of this potential impact
could be achieved through the inclusion of additional services (e.g., behavioral health,
pharmacy) and populations (e.g., ABD) in managed care. If managed care were expanded to
the ABD population, MCOs could realize savings partially through implementing similar
initiatives as described in the LTSS section above. As a result, there is natural overlap in the
potential impact of these areas; if services for the ABD population – including LTSS – are fully
carved into managed care, then the aforementioned total potential impact would overlap with
the $90 million to $275 million from the LTSS section (and eliminating any incremental savings
from it).
Current situation
Scope of managed care
The managed care program encompasses children, parents, and pregnant women, and it
excludes most pharmacy and behavioral health services
155
(see Exhibit 34). Medicaid ABD
populations are entirely excluded from the managed care program. Children in foster care or in
subsidized, post-adoption or guardianship programs are included on an opt-out basis. Total
managed care spending is ~$2.2 billion (see Exhibit 35; children, parents, and pregnant
women comprise ~67% of Medicaid enrollees but drive only 23% of the spending, excluding
FFS spending for that same population).
156
153
Analysis of state data, 2018; Missouri Foundation for Health, “Missouri Medicaid Basics,” 2017, see:
mffh.org/wordpress/wp-content/uploads/2017/03/MedicaidBasics2017.pdf.
154
Missouri DSS, “Annual Table 23 and 24 for FY18,” 2018; Analysis of state data, 2018.
155
Missouri Foundation for Health: see note 153.
156
Missouri DSS: see note 5.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
63
EXHIBIT 34: CURRENT BEHAVIORAL HEALTH COVERAGE
EXHIBIT 35: MHD ENROLLMENT, MANAGED CARE AND FEE-FOR-SERVICE SPENDING
BY ELIGIBILITY GROUP AND CATEGORY OF SERVICE, SFY2018
157
157
Missouri DSS: see note 154; “children” excludes eligibility groups associated with foster care; “foster children”
includes foster care, child welfare; estimated share of Title XIX HDN population attributable to subsidized child
FFS MC
Foster Children (Ages 0-20);
Independent Former Foster
Adolescents (Ages 21-25)
All other MC eligibility groups:
Adults (21+), Pregnant Women,
Children COA 1, CHIP Exp, CHIP
Separate
FFS
MC
FFS
FFS
FFS (under 21)
FFS
FFS
FFS
FFS
FFS
FFS
FFS
FFS
MO HealthNet Covered Benefits
Outpatient “clinic option” services
Inpatient Behavioral Health Admissions
Inpatient Admission with both Behavioral and
Physical Diagnoses
Applied Behavior Analysis for Autism Spectrum Disorder
Tobacco Cessation Counseling - psychologists,
LPCs, LCSWs
CPR (Comprehensive Psychiatric Rehab - DMH)
CSTAR (Comprehensive Substance Treatment and
Rehab - DMH)
TCM (Targeted Case Management - DMH)
Waivers
FFS FFS
MC
MC
MC
Managed care Fee-for-service
156Disabled
751M 1226M 866M 139M 32M 138M1183M
46M 114M 1076M 106M <1M 114M141M
Seniors
Rx
Behavioral
Health LTSS
Rehab &
specialty EPSDT OtherMedical
Children
368M 146M <1M 7M 62M <1M1556M
162M
Members
Thousands
590
81
94
22
34
Custodial
parents
155M 26M 6M 2M <1M <1M401M
72M
Pregnant
women
23M 5M 1M 1M 1M <1M131M
42M
Foster
children
52M 131M <1M 2M 28M <1M71M
46M
<$100M $100-500M >$500M
Expenditures, $ Millions

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
64
Managed care rate setting
Missouri’s MCO rate-setting methodology encourages efficiency, adjusts payments based on
risk, and manages non-benefit expenses. Efficiency adjustments have been implemented to
avoid payments for some avoidable emergency department (ED) and inpatient (IP) services
(e.g., low-acuity non-emergency adjustment for ED utilization that could have been diverted to
other settings, potentially preventable hospital admissions adjustment for inpatient utilization).
A risk-adjusted efficiency adjustment process is also used to address differences in claim
levels among MCOs within a region after adjusting for the underlying risk profile of each
MCO’s population. Furthermore, a general ledger review of MCO administrative costs has
been performed recently, and target MCO profit margins (i.e., underwriting gains) were
adjusted to account for lower corporate taxes in Calendar Year 2018.
Contracting, compliance, and performance management
Current managed care contracts establish minimum standards for MCO performance and
attempt to create an environment that fosters innovation. Contract provisions cover areas
including care management, utilization management, provider payment, program integrity,
provider network, grievances and appeals, among others. For care management, Missouri
requires initial screening within 90 days of enrollment, with shorter timelines for pregnant
women, children with elevated blood lead levels, and members with diseases. The current
contracts contain provisions to stimulate innovation and value in the managed care program,
through the Local Community Care Coordination Program (LCCCP) as well as member and
provider incentive programs.
The performance management regime established through current contracts relies primarily
on performance withholds, liquidated damages and sanctions. The performance withhold
program is under revision based on negotiation between MHD and the MCOs, with an
intention to use predominantly HEDIS measures going forward.
158
Liquidated damages for
contract compliance infractions cover a broad set of potential operational issues, with penalties
ranging from $100 per day for failure to submit a report to $10,000 per month for failure to
adhere to claims processing standards.
The performance management relationship between MHD and MCOs centers on ensuring
basic contract compliance and rectifying performance issues. MHD requires 24 distinct reports
from MCOs in addition to submission of encounter data and other information. To date, MHD
activities have focused on improving and validating the quality of the information submitted by
MCOs.
Potential opportunities for improvement
• The rate-setting methodology could be further strengthened. While the current
methodology employs several strong elements to ensure managed care rates account for
all reasonable, appropriate, and attainable costs, opportunities remain to further enhance
the rates. Additional efficiency adjustments are available for each of the major categories
of expenditures to remove inefficient utilization (e.g., inpatient stays that could have been
avoided with better outpatient care) from rate calculations.
159
Steps could also be taken to
simplify the rate cell structure by combining small, high-cost rate cells to reduce potential
welfare programs, and independent foster children ages 18-26; “custodial parents” excludes independent foster
children ages 18-26.
158
Interviews with Medicaid program staff members.
159
Interviews with Medicaid program staff members; analysis of state data, 2018.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
65
volatility in capitation payments. Finally, as discussed in the acute care section, the state
could consider capping MCO hospital payments at a fixed percentage of Medicaid FFS
payments, while simultaneously adapting overall MCO capitation rates accordingly.
• Day one MCO eligibility and/or passive MCO enrollment could be implemented for
additional populations. Except for foster children, new participants eligible for managed
care will remain in fee-for-service for some time before either choosing or being
automatically assigned to an MCO. States such as Ohio have adopted day one eligibility
with passive enrollment for individuals eligible for Medicaid managed care, while still
preserving a participant’s ability to actively choose or switch MCOs for a period of time.
160
In such states, individuals may be enrolled in an MCO retroactively to the first day of the
month in which Medicaid eligibility is determined. In such states, there is no fee-for-service
period before MCO enrollment occurs. This can reduce the administrative burden and
financial risk to the state and accelerate the process of availing participants to care
management and coordination.
• Operational contract provisions could be further strengthened to improve program
performance, increase efficiency and improve member and provider experience.
Timeliness standards for key processes (e.g., provider payment, prior authorization,
grievances and appeals) can be further specified. Program integrity requirements
(including fraud, waste, and abuse) can be further elaborated to define overpayments to be
investigated and clarify roles (e.g., between the state and MCOs) in preventing, detecting,
recovering and retaining overpayments. The state may also have an opportunity to revisit
provider network and network adequacy requirements, especially considering CMS’
November 8, 2018 notice of proposed rulemaking on Medicaid and CHIP managed
care.
161
• Care management requirements can be further elaborated and appropriately
enforced. The contracts do not clearly specify standards for risk stratification and
identification of participants for care management, the proportion of participants the state
expects to receive care management, case load standards for care managers, or care
management activity requirements once participants are enrolled in care management
programs. While the contracts allow MCOs to coordinate care management activities with
providers including health homes, it does not set forth a clear expectation or requirement
for them to do so. In addition, initial steps to increase healthcare value (e.g., member
incentive programs, provider incentive programs and LCCCPs) have not seen broad
uptake and MCO progress in implementing these programs and realizing their potential for
impact has been uneven.
162
• For a subset of health home enrollees, the state pays both MCOs and health homes
for care management services. Approximately 6,500 MCO members are enrolled in a
Primary Care Health Home (PCHH), and 5,500 members are enrolled in a Community
Mental Health Center Healthcare Home (CMHC HH) or Certified Community Behavioral
Health Clinic Health Home (CCBHC HH).
163
In addition to their regular payments from
160
Ohio Medical Assistance provider agreement for managed care plan. Ohio Department of Medicaid, 2018.
161
CMS, “CMS Proposes Changes to Streamline and Strengthen Medicaid and CHIP Managed Care Regulations”,
2018, see: www.cms.gov/newsroom/press-releases/cms-proposes-changes-streamline-and-strengthen-medicaid-
and-chip-managed-care-regulations.
162
Interviews with Medicaid program staff members.
163
Interviews with Medicaid program staff members.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
66
MCOs, Missouri health homes receive additional care management payments directly from
the state. Some behavioral health services provided by health home providers are carved
out of managed care, but the responsibility for care management and coordination with
other services is attributed to both the MCO and the health home.
• The state has not fully leveraged the available levers for incentivizing MCO
performance or disincentivizing MCO underperformance. Additional levers are
available to the state to create positive incentives for MCO performance on, for instance,
operational or quality metrics. At present, the auto-assignment algorithm used to assign
participants to MCOs only takes into consideration the level of MCO enrollment in each
region (subject to minimum and maximum enrollment levels for each MCO). Other states
have incorporated operational or quality metrics (e.g., encounter data submission or
provider payment operational measures; HEDIS quality measures) into the auto-
assignment algorithm to reward better performing MCOs with additional participants.
164
Pooled rewards, bonuses, or public report cards could also be considered as additional
performance management levers. Furthermore, while the MCO contracts specify a broad
set of liquidated damages or sanctions for performance infractions, the state could revisit
the structure and magnitude of these penalties to ensure their efficacy, and clearly
communicate to MCOs which areas of performance will be most closely monitored. Exhibit
36 shows the incentive and disincentive levers currently used in Missouri against a broader
set of levers observed in other states, highlighting several opportunities for new levers to
encourage MCO compliance and performance.
164
KFF, “Medicaid Reforms to Expand Coverage, Control Costs and Improve Care: Results from a 50-State
Medicaid Budget Survey for State Fiscal Years 2015 and 2016,” 2015, see: www.kff.org/medicaid/report/medicaid-
reforms-to-expand-coverage-control-costs-and-improve-care-results-from-a-50-state-medicaid-budget-survey-for-
state-fiscal-years-2015-and-2016.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
67
EXHIBIT 36: MCO COMPLIANCE AND PERFORMANCE MANAGEMENT LEVERS
165
• Reporting requirements for MCOs can be improved, reducing administrative burden
and improving the value of the information received. Current required reporting
includes seven financial data reports (e.g., unaudited and audited financial statements,
copies of administrative services contracts and management agreements), and 17
operational data reports (e.g., contact center reports, provider network reports, care
management logs).
166
The state does not appear to be fully processing the volume of
detailed data contained in these reports and providing concise, aggregated analysis and
feedback that can drive MCO performance improvement. In addition, in several cases,
ambiguity or disagreement over the type of information required, granularity, or frequency
at which it must be reported have made it difficult to yield reliable data and produce
meaningful insights. These issues have led to challenges in establishing the preconditions
for optimal performance dialogues between the state and MCOs.
• The poor quality of the encounter data limits adequate performance management.
The state’s MMIS system is not able to take in some encounters or encounter data
variables. The quality of MCO encounter data submissions is variable, in part because
encounters are being held back due to issues the MMIS system has in processing
encounters. The result is that the state has neither a complete, accurate set of encounter
data, nor a full understanding of which encounters are not being submitted. Consequently,
the state does not appear to be performing certain analyses on spending or spending
165
Based on review of approximately 15 publicly available managed care contracts across states from 2013-2018.
166
Missouri DSS, “Managed Care Contracts,” 2018, see: dss.mo.gov/business-processes/managed-care/.
Cost/
efficiency Quality Network Pharmacy
Contract
perform-
ance
Data sub-
mission
Program
integrity
APM /
innovation
Member
experienceLever
Contract dimensions
Used by MO
Use pooled rewards
Freeze enrollment
Report health
grades
Increase auto-
enrollment priority
Increase
transparency
Decrease auto-
enrollment priority
Enforce
fines/penalties
Require corrective
action plans
Offer bonuses
Use withholds
Termination
Incentives
Dis-
incentives
Build encounter
data quality and
timeliness into
auto-enrollment
algorithm
Report publicly on
how MCOs are doing
at participation in
their member and
provider incentive
programs
Offer
bonuses to
drive APM
and
innovation
Observed in other states

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
68
trends, for example, or adequately comparing performance between plans, in ways that
could be beneficial to the management of the Medicaid program, as a whole, and the
managed care program specifically.
• The performance dialogues between the state and the MCOs could be more focused
on the value of the care delivered. The amount of and reliance on detailed process
measures and the poor quality of the encounter data lead to a lack of focus on key
outcomes in the performance dialogues between the state and the MCOs. Recent
interactions between the state and MCOs have focused on improving the timeliness and
validity of information reported, rather than MCO performance on improving quality,
outcomes, and experience for the population. Performance dialogues could be advanced
to cover more substantive, outcome-, and improvement-oriented conversations. This could
be consistent with and supportive of the implementation of value-based payment programs
and reimbursement models that reward quality and outcomes as discussed elsewhere in
this document (e.g., in the Acute Care Services and LTSS sections). The state also has an
opportunity to codify the cadence and approach to performance dialogues with MCOs,
establishing its agenda and priorities for these conversations rather than reacting to MCO
priorities. Exhibit 37 provides a conceptual illustration of the evolution of the relationship
between the state and its MCOs, highlighting potential priorities for more sophisticated
levels of state/MCO collaboration.
EXHIBIT 37: EVOLUTION TOWARD MORE ADVANCED COLLABORATION WITH MCOS
Description
Maturing managed care
Strategic Sourcing
Advanced managed care
Supplier Collaboration
Shift to managed care
Transactional Sourcing
Characteristics
▪ RFPs scored on a set rubric
and awarded to MCOs with
most points
▪ Meets mandatory
requirements
▪ Ad-hoc improvement
initiatives
▪ Compliance-based
performance conversations
▪ Greater focus on quality,
outcomes and member
engagement
▪ Improved integration of care
across behavioral and
physical health
▪ Comprehensive and
deliberate sourcing strategy
▪ Fact-based, holistic
performance conversations
▪ Openness to joint innovation and
collaboration
▪ Partnership to improve care
coordination and integration
▪ Cost and investment transparency
to support shared prioritization
▪ Attention to MCO capability
development
▪ Payment for quality, value and
outcomes
▪ Performance-based partnerships
▪ Advanced analytics to improve
quality and efficiency
▪ Active management across MCO
portfolio
▪ Partner to address non-core
Medicaid policy goals
▪ Structured sourcing and
contract negotiations
▪ Effective program integrity/
performance management
▪ Management of complex
categories
▪ Established path to program-
wide payment innovation
▪ Focused on monitoring
contractual compliance
▪ Dominated by “firefighting”
on unexpected issues
▪ Basic KPIs/performance
management processes

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
69
• The scope of services covered under managed care for children, parents, and
pregnant women is narrower than that in many other states. For the managed care
population, most prescription drugs and certain behavioral health services are carved
out.
167
A significant majority of managed care states include pharmacy benefits in their
managed care contracts (though different approaches exist to managing rebates,
formularies, and preferred drug lists), and a growing number include a comprehensive set
of behavioral health services. In light of the increasing emphasis on the need to integrate
physical and behavioral health services (including substance use), many states have
decided that a coordination barrier between physical and behavioral health may hamper
the realization of optimal outcomes for patients. Carving in these services can create
additional value (in efficiency, quality, and experience) through integrated care
management across a more comprehensive continuum of services for covered
participants. In addition, moving to value-based payment may also be facilitated by carving
in these services as MCOs would otherwise have different incentives than VBP providers
in making drug or behavioral health treatment choices.
• The state could consider including (a portion of) the ABD population in managed
care. In Missouri, the Medicaid ABD populations remain in traditional (FFS) Medicaid.
While the multiple improvements to efficiency, quality of care and outcomes discussed in
the preceding sections (e.g., care management, rebalancing of the LTSS system,
reimbursement based on quality and outcomes) could be achieved through multiple
models, managed care represents one potential approach to support these efforts. A
transition to managed care could be accomplished through a Medicaid managed care
model that includes only the Medicaid benefits for dual or non-dual eligible ABD
beneficiaries and/or through one of the several available models for integrating Medicare
and Medicaid benefits. Recent guidance from CMS has signaled a renewed focus on
programs that integrate Medicare and Medicaid benefits.
168
As shown in Exhibit 38, a
majority of states now include at least part of this population in managed care.
169
This may
be due to a belief that managed care models present opportunities to improve care
management and thus improve quality, outcomes and experience for this population, while
increasing the efficiency of the program by better managing medical cost trends over time.
While the body of empirical evidence across states to support these claims remains
nascent, several studies that have focused on specific subsegments of the ABD population
(e.g., LTSS recipients or participants with high behavioral health needs) have shown
evidence of the potential for well-designed and implemented managed care programs to
improve program performance.
170
167
Missouri DSS: see note 166.
168
Medicaid.gov, “Ten Opportunities to Better Serve Individuals Dually Eligible for Medicaid and Medicare,” 2018,
see: www.medicaid.gov/federal-policy-guidance/downloads/smd18012.pdf.
169
McKinsey, “Next-generation contracting: Managed Medicaid for individuals with special or supportive care
needs,” 2016, see: healthcare.mckinsey.com/next-generation-contracting-managed-medicaid-individuals-special-or-
supportive-care-needs.
170
McKinsey: see note 169; McKinsey, “Improving care delivery to individuals with special or supportive care
needs,” 2016, see: healthcare.mckinsey.com/improving-care-delivery-individuals-special-or-supportive-care-needs.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
70
EXHIBIT 38: MANAGED CARE FOR SPECIAL OR SUPPORTIVE CARE NEEDS
171
Potential initiatives
Based on a review of Missouri’s current approach, interviews with functional leaders and subject
matter experts within the relevant departments, and analysis of other states’ activities, this
section has identified 12 potential initiatives Missouri could consider to improve managed care
in the state. The total potential impact across these initiatives ranges from $175 million to $300
million, which may include the savings from the LTSS section depending on whether the state
fully carves in services for the ABD population
1. Incorporate additional efficiency measures into the managed care rate-setting
process. Three efficiency adjustments have been put into place in the current managed
care rate-setting methodology: 1) removing claims for potentially preventable inpatient
admissions, 2) removing emergency department claims that could have been avoided, and
3) conducting an overall adjustment for risk-adjusted efficiency. These efficiency
adjustments can be continued. In addition, there are several other efficiency adjustments
available that have not yet been employed, covering spending areas such as short-stay
admissions, readmissions and maternity care (e.g., inpatient stays that could have been
avoided with better outpatient care). These additional adjustments would need to be
examined for potential overlap with the adjustments current in place (e.g., risk-adjusted
efficiency, a more broad-based adjustment, may already capture some of the value that
could be captured through new adjustments), but they have the potential to create additional
cost savings for the program.
2. Implement stop-loss provision and combine small rate cells. The current rate structure
contains several small but high-cost, potentially volatile rate cells (e.g., a rate cell for
participants in neonatal intensive care units). The state could consider implementing a stop-
loss provision and combining smaller, more volatile rate cells with larger, more stable ones.
171
McKinsey: see note 169.
BH
LTSS
BH and LTSS
BH, LTSS, and I/DD BH and I/DD I/DD and LTSS
2005
D.C.
2016
D.C.
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
71
This could increase the predictability of state outlays for managed care capitation payments
and simplify administration of the rate structure.
3. Expand day one managed care eligibility and passive enrollment to additional
populations. Day one MCO eligibility and passive enrollment could be expanded beyond
foster children to additional populations. Passive enrollment, while still allowing participants
to choose or switch MCOs as required by federal regulations, can streamline participant
transitions, increase access to care management for participants by requiring it at the time of
Medicaid enrollment, and reduce the burden on the FFS system.
4. Further specify contract provisions regarding key operational processes and
timelines. Contract requirements laying out the process and required decision timelines for
prior authorization, provider payment, and resolution of grievances and appeals could be
clarified and strengthened. In addition, program integrity language can be further elaborated
to set expectations and clarify roles between the state and MCOs for eliminating
overpayments due to fraud, waste, and abuse. These improvements to the MCO contract
could remove ambiguity and improve MCO performance and the state’s ability to monitor
and manage MCO performance against these requirements.
5. Clarify and strengthen care management requirements. The state could enhance care
management requirements by adding specificity around risk stratification and participant
identification, the proportion of participants to receive care management, case load
standards for care managers, and/or care management activity requirements for MCOs. The
state could consider further clarifying expectations for MCOs to collaborate and/or formally
delegate care management requirements to health homes or other care management
entities. This could ensure clarity of roles and prevent against payment by the state for
duplicative care management efforts by multiple parties (e.g., MCOs and health homes).
6. Clarify and strengthen incentive programs and programs intended to encourage
adoption of value-based payment. The state could engage in a focused effort to
collaborate with and manage MCOs in designing and rolling out member incentives,
provider incentives, and LCCCP programs. Depending on the choices the state makes in its
approach to value-based payment, it could incentivize or require MCOs to align or integrate
their efforts with the state’s strategy and include definitions for Alternative Payment Models
in MCO contracts and/or performance management.
7. Deploy additional levers to incentivize MCO performance on key metrics. In addition to
the revisions to the withhold program currently underway, the state can consider additional
levers such as MCO prioritization in the auto-assignment algorithm based on performance,
pooled rewards, bonuses, or public report cards. Expanding the levers in use can enable the
state to incentivize performance across a broader set of metrics covering operational
performance, quality, and healthcare value (e.g., encounter data submission,
member/provider incentive program participation, LCCP or VBP program participation, care
management). If the state were to prioritize improving data submission, it would need to
ensure that remaining obstacles in the state’s encounter data intake process are resolved.
8. Optimize financial penalties to better regulate MCO performance on key metrics. The
state could revisit the structure and magnitude of the sanctions and liquidated damages set
forth in the contract to ensure their efficacy. The state could also more clearly communicate
to MCOs which areas of performance will be most closely monitored in a given time period.
9. Streamline MCO reporting requirements and improve accuracy and timeliness of
information reported by MCOs; establish cadence for performance management

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
72
dialogues. Accuracy and timeliness of information reported by MCOs could be improved to
enable more informed, focused performance management discussions. This could include
further streamlining of MCO reporting requirements, shifting from a focus on processes to
outcomes based on collaboration between MHD and each of the MCOs. A cadence for
performance management dialogues between the state and MCOs could be established
along with clear priorities and expectations for the topics to be covered in each discussion.
10. Carve in additional services to managed care for the current managed care
population. The scope of services covered under managed care for the current managed
care population could be broadened to include pharmacy benefits and additional behavioral
health services (e.g., those under DMH-administered programs). Including these services
could enhance the MCOs’ ability to manage the overall health and total cost of care for the
managed care population as well as VBP programs, which could help improve quality,
outcomes, and participant experience while increasing program efficiency.
11. Transition to a single-MCO model with specialized capabilities for the foster care
population. The structure of the managed care program for children in foster care or in
subsidized, post-adoption, or guardianship programs could be modified to place this
population into a single MCO offering specialized capabilities, experience and expertise with
this population, potentially procured through a more tailored procurement process. This
could avoid the sometimes-fragmented nature of current services for this vulnerable
population, ensure the application of focused expertise and experience within one MCO and
optimally leverage its infrastructure to meet this population’s needs. Relying on the expertise
of one MCO may also improve the ability of the state to conform to the regulatory
requirements associated with serving this population (e.g. the management of
psychotropics).
12. Expand the scope of the managed care program to include the ABD population (in
whole, in part, or on a phase-in basis). Expanding managed care to portions of the ABD
population represents one potential approach to achieving the improvements to efficiency,
quality of care, and outcomes discussed in the preceding sections, among alternatives such
as improved state-led care management programs or meaningful adoption of alternative
payment models. Expanding managed care to this population would likely require statutory
change and could take many forms given the heterogeneity of the ABD population and the
services required by its various subpopulations. In general, MCO capabilities in serving the
ABD population – and state experience in operating managed care programs for this
population – vary widely by subsegment of the population and associated services.
Managed care programs covering the core medical, behavioral, LTSS, and pharmacy
benefits of non-dual eligible ABD participants are becoming increasingly common, as are
managed care programs focused on covering the LTSS services for dual-eligible
beneficiaries. Meanwhile, managed care programs for persons with intellectual and/or
developmental disabilities (whether residing in an institutional setting or on an HCBS waiver)
remain relatively rare. Any potential consideration of managed care for the ABD population
may take into consideration the diverse and nuanced characteristics and needs of the
various subsegments of this population. Finally, through enrolling elderly and/or dually
eligible participants with disabilities in Medicaid managed care plans, the state could take
advantage of the increased opportunities recently provided by CMS to improve integrated
care for dually eligible populations through, for example, Dual Eligible Special Needs Plans
(D-SNPs) or Medicare Advantage Medicare-Medicaid Plans (MMPs).
172
172
Medicaid.gov: see note 168.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
73
PROGRAM INTEGRITY
To maintain the functional integrity of the state’s Medicaid organization, Missouri has divisions
that prevent fraud, waste, and abuse (FWA) and ensure proper payments. Fraud, waste, and
abuse detection and prevention are largely the responsibility of Missouri Medicaid Audit and
Compliance (MMAC) and the Welfare Investigations Unit (WIU), but multiple other agencies
within DSS conduct or enable investigations or enforcement. The WIU is responsible for
preventing participant fraud, while MMAC is responsible for enrolling, auditing, investigating,
and sanctioning providers.
The Cost Recovery Unit administers cost avoidance and a recovery program to offset
expenditures for the state Medicaid agency. This unit ensures that appropriate third-party
resources (including but not limited to Medicare, commercial insurers, workers’ compensation,
probate-estate recoveries, and others) are utilized as the primary source of payment prior to the
state paying for services. Enrollment of eligible participants into Medicare is especially important
for the state as this population typically has more limitations of average daily living, poorer
health, and higher medical expenditures.
When combined, the potential initiatives could save $65 million to $100 million or more, net of
recurring investments, depending on decisions made by the state.
173
Potential initiatives include
enhancing the quality and quantity of FWA claims-based analytics, increasing coordination
between MMAC and relevant internal and external stakeholders, optimizing the identification
and enrollment of Medicare-eligible participants, and improving the implementation of certain
pre-payment edits.
Current situation
This section provides an overview of Missouri’s current FWA organizational structure and
functionality, third-party liability (TPL) identification, Medicare Buy-In, and estate recoveries.
Organizational structure and functionality
There are multiple divisions responsible for conducting investigations or performing
compliance duties within the state. These divisions include Missouri Medicaid Audit and
Compliance (MMAC), the Division of Legal Services (which includes the Welfare Investigations
Unit [WIU] and the General Assignment Unit), Family Support Division, Division of Youth
Services, Children’s Division, and the Division of Finance & Administrative Services.
Missouri handles Medicaid participant fraud through the WIU. WIU deters participant fraud,
prosecutes offenders, and collects money lost to the state because of fraud. The WIU currently
has 18 investigators.
Missouri handles provider fraud and abuse through MMAC. In SFY2018, MMAC produced
about $40 million in savings for the state.
174
MMAC is responsible for enrolling, auditing,
investigating, and sanctioning providers. MMAC is currently appropriated 76.5 FTEs, including
twenty-nine FTEs dedicated to provider audits and participant lock-in and eight investigators.
MMAC works with an analytics vendor and the CMS Unified Program Integrity Contractor to
identify opportunities to improve program integrity. Through its investigations, MMAC provides
feedback to the policy teams within MHD, another unit within DSS.
TPL identification
173
Analysis of Missouri Medicaid claims data, SFY2016-18; interviews with Medicaid program staff members.
174
Analysis of state data, 2018; interviews with Medicaid program staff members.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
74
TPL information is obtained at the time a participant is enrolled. Family Support Division (FSD)
specialists obtain TPL information primarily during the MHD eligibility determination process.
Supplementing this initial contact are data matches with both private and public entities, edits
within the claims processing system, direct inquiries to participants, non-custodial parents and
other potential liable parties. MHD uses a vendor to perform data matches between participant
claims’ data and external sources of third-party coverage.
TPL identification for participants enrolled into MCOs is the responsibility of the MCO. CMS
recommends states use one of four options to ensure that they meet the coordination/TPL
requirements: (1) exclude individuals with known sources of TPL from enrollment in MCOs; (2)
enroll individuals with known sources of TPL in MCOs, with the state retaining responsibility for
COB/TPL; (3) enroll individuals with known sources of TPL in MCOs and contractually require
that the MCO assume responsibility for COB/TPL; or (4) exclude individuals with commercial
managed care coverage from enrollment in MCOs but enroll individuals with other types of
third party coverage in the MCOs.
175
Missouri uses the third option, and as such, MCOs act as
agents for the state for coordination of benefits and third-party reimbursement in the following
circumstances: workers’ compensation, tortfeasors, motorist insurance, and liability/casualty
insurance. The state’s MCOs are required to report their identified savings and the future
capitation payments are adjusted accordingly.
Dual enrollment and Medicare Buy-In
Missouri is one of nine 209(b) states. At least one of Missouri’s income eligibility criterion is
more restrictive than the SSI program, thus making it one of nine states that are considered
209(b) states (see Exhibit 39).
176
States that elected this option may not use more restrictive
standards than those in effect in January 1, 1972, and must provide for deductions of incurred
medical expenses from income through Medicaid spenddown so that individuals may reduce
their income to the income eligibility level. As a result of being a 209(b), the participant
enrollment process is separate from the SSD/I determination.
175
Medicaid.gov, “Medicaid Third Party Liability & Coordination of Benefits,” see:
www.medicaid.gov/medicaid/eligibility/tpl-cob/index.html.
176
Social Security Administration, “SI 01715.020 List of State Medicaid Programs for the Aged, Blind and Disabled,”
2016, see: secure.ssa.gov/poms.nsf/lnx/0501715020.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
75
EXHIBIT 39: MEDICAID-SOCIAL SECURITY ELIGIBILITY AND ENROLLMENT
177
Missouri identifies Medicare leads through three main sources. As a cost-saving measure,
Medicare premiums are paid for participants of Old Age Assistance, Permanently and Totally
Disabled, Aid to the Blind, Temporary Assistance for Needy Families, Specified Low Income
Medicare Beneficiary, and Qualified Medicare Beneficiary programs who meet the criteria for
Medicare coverage. Staff verifies Medicare leads through reports produced from files sent by
CMS, the Social Security Administration, or the TPL/Medicare contractor through a data
match.
178
In addition, the state has a policy that mandates participants apply for Medicaid, and
they must also apply for Medicare.
Estate recoveries
Missouri identifies estate recoveries through data matches from various organizations. The
state uses data from the DHSS’ Vital Statistics, FSD county office staff, and cooperation of
other public and private groups. When cases are established, TPL staff verifies expenditure
documentation and assembles data for evidence. The TPL staff appears in court to testify on
behalf of the state and to explain MHD policies and procedures.
Potential opportunities for improvement
This section identifies potential opportunities to strengthen the state Medicaid agency’s program
integrity. When compared to common practices in other states, the following observations can
be made:
• Improved coordination across multiple agencies could help improve fraud, waste,
and abuse (FWA) efforts. Each division may have its own computer system, eligibility
criteria, provider and participant enrollment service authorizations, service delivery,
payments, audits, investigations, and compliance functions. In addition, divisions with
177
Social Security Administration: see note 176.
178
Missouri DSS, “Third Party Liability,” see: dss.mo.gov/mhd/general/pages/about.htm#tpl.
1634 209(b) SSI
Description
209(b)
states
1634 states
SSI States
There are three classifications for states’
eligibility and Medicaid enrollment
State by state eligibility determination classification
▪ Have at least one eligibility
criterion more restrictive than SSI
▪ Must allow for Medicaid
spenddown
▪ Eligibility determinations are the
responsibility of the state
▪ Have the same eligibility criteria as
SSI
▪ Eligibility determinations are made
by SSA
▪ Have the same eligibility criteria as
SSI
▪ Eligibility determinations can be
made by SSA or the state
▪ States may require separate
enrollment process

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
76
primary fraud and abuse functions are dependent on staff within the other divisions to
detect potential fraud or abuse situations and make a referral in an acceptable format with
supporting documentation (see Exhibit 40). However, MHD has recently established an
interdisciplinary taskforce to improve coordination of FWA activities.
EXHIBIT 40: DIVISIONS INVOLVED IN FWA EFFORTS AND ASSOCIATED CHALLENGES
• MMAC could increase collaboration with relevant clinical policy teams. A closed-loop
communication system between FWA and clinical policy teams – meaning whenever FWA
is identified, the situation is communicated to the clinical staff – could help shape
corresponding policy changes in a timely fashion. This might also require additional
capacity within the clinical policy teams.
• The analytical capacity and capability, and the range of FWA concepts tested in
Missouri could be increased in line with other Medicaid programs and commercial
plans. The internal analytics function – currently two FTEs – could benefit from additional
capacity. MMAC’s analytics vendor currently tests for between 25 to 40 program integrity
opportunity areas; this funnel could be greatly expanded using a prioritized subset of
opportunity concepts adopted by other programs.
• Ensuring access to a larger set of higher quality data could improve Program
Integrity (PI) performance. MHD current faces challenges in the quality of MCO
encounter data as well as some aspects of FFS data. Approaches to improve this data
quality are described in other parts of this document. In addition, MHD could work with
CMS to access other data sources directly (e.g., Medicare claims) that might be helpful in
PI opportunity identification.
• The state’s enrollment of dual-eligible participants into Medicare is lower than
historic state and national averages. In SFY2013, 16% of Missouri’s participants were
Children’s
Division
Division of
Finance &
Administrative
Services
MMAC
Division of
Legal
Services
Family
Support
Division
Division of
Youth
Services
DSS
Numerous divisions within DSS either conduct FWA
tasks or enable other divisions to do so
Challenges with this model
▪ Each division may use unique software and
databases for determining:
– Eligibility
– Provider and participant enrollment
– Service authorizations
– Service delivery
– Payments, audits
– Investigations
– Compliance functions
▪ Divisions with primary fraud and abuse
functions are dependent upon staff within the
other divisions to recognize a situation could
be fraud or abuse and make a referral in an
acceptable format with their supporting
documentation
▪ Ability to work with data across divisions

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
77
dually enrolled in Medicare and Medicaid, which was consistent with the national average
at the time. In SFY2018, the state’s dual-eligible enrollment as a percentage of total
participants was 14.5% (see Exhibit 41).
179
The decrease in dual enrollment appears to be
more prominent in the disabled population that is less than 65 years of age.
EXHIBIT 41: CHANGES IN DUAL ENROLLMENT AS PERCENTAGE OF TOTAL MEDICAID
ENROLLMENT
• Missouri could increase the number of sources it currently uses for TPL
identification. Other state Medicaid agencies and CMS have pharmacy claims databases
to identify primary payors. Using pharmacy claims databases typically allows states to
identify an additional cohort of participants who have TPL at a faster rate because of the
faster typical timing of pharmacy claims.
Potential Initiatives
Based on review of Missouri’s current approach, interviews with functional leaders and subject
matter experts, and analysis of other states’ activities, this section includes five potential
initiatives Missouri could consider improving program integrity. In total, the financial impact of
Program Integrity initiatives could range from $65 million to $100 million, depending on state
choices.
1. Expanding the national correct coding initiatives (NCCI) coding edits that the state
has in place. CMS developed the National Correct Coding Initiative to promote national
correct coding methodologies and to control improper coding leading to inappropriate
payment in claims. There are two broad classifications of NCCI edits: Procedure-to-
Procedure edits, which prevent improper payment when incorrect code combinations are
179
KFF, “Dual Eligibles as a Percent of Total Medicaid Beneficiaries,” 2013, see: www.kff.org/medicaid/state-
indicator/duals-as-a-of-medicaid-beneficiaries; analysis of Missouri Medicaid claims data, SFY2016-18; interviews
with Medicaid program staff members.
15.1
14.7
14.0
14.5
SFY2016SFY2015 SFY2017 SFY2018
16%
Lowest Quartile 2nd Quartile 3rd Quartile Highest Quartile
Duals as a percent of total enrollment in SFY2013
Since SFY2013, dual-enrollment has fallen
to 14.5% of the total population
US average: 16%

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
78
reported, and Medically Unlikely edits, which prevent improper payments when services are
reported with incorrect units of service. Missouri has implemented some of these edits but
has not implemented the full suite of edits. This initiative would require changes to the MMIS
system to implement the full suite of codes, among other requirements.
2. Create an experimental, investigation, and unproven (EIU) medical procedure policy
to prevent improper payments. This agency policy would identify devices or procedures
that have not been proven to be medically effective. This initiative would require the state’s
clinical staff to identify these procedures and review the procedure on annual basis.
Additionally, the initiative would require feasible changes to the MMIS system.
3. Expand the analytical funnel to identify additional improper payments that can be
prevented using claims edits and pre-pay changes or can result in recoveries. As an
example, for given procedure codes, Missouri has set billing limits that the state only
reimburses hospital observation stays for up to 24 hours. The state could ensure that the
claims system is preventing payment for procedures after the allotted 24-hour period.
Opportunities that take the form of edits would require feasible changes to the MMIS
system.
4. Optimize the state’s ability to identify and enroll participants who are currently and
may become Medicare eligible. The state could implement (either internally or through a
vendor) new claims-based technology that would allow the state to identify participants who
are currently Medicare-eligible or may become eligible. Missouri staff could then help notify
participants about this benefit. This would require medium-complexity changes to the MMIS
system and potentially a new vendor.
5. Improve TPL identification. Missouri could begin to utilize additional sources (e.g.,
pharmacy claims data) to increase TPL identification rate. To do this, the state could
contract with a vendor that would add additional sources of data.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
79
FEDERAL FINANCING
Missouri has captured a significant share of the federal funding it is eligible for, but there may be
additional opportunities to capture federal revenue through new federal programs, both through
grants and enhanced match. The state also could consider evaluating the use of inter-
governmental transfers (IGT) as an alternative or supplemental financing approach. The total
federal financing opportunity is expected to be $10 million to $20 million in grant funding and
additional enhanced match.
180
This section will describe the current state of federal financing in Missouri, observed
opportunities for improvement, and potential initiatives for the state to consider.
Current situation
Overall Medicaid spending across departments
Medicaid spend represents over 80% of the budget for DSS and approximately two-thirds of the
budget for DHSS and DMH (see Exhibit 42).
181
The largest areas of Medicaid spending include
managed care, pharmacy reimbursement, hospital and nursing facility reimbursement, physician
reimbursement, and community programs. Nearly all these funds receive some form of federal
match based on the category of spending (see Exhibit 43). Federal funds represent
approximately 65% of the total spending across top Medicaid spending categories.
EXHIBIT 42: MEDICAID SPENDING BY DEPARTMENT
180
U.S. Congress, “H.R.6- SUPPORT for Patients and Communities Act,” 2018, see: www.congress.gov/bill/115th-
congress/house-bill/6; CMS, “Maternal Opioid Misuse (MOM) Model,” 2018, see:
www.cms.gov/sites/drupal/files/2018-10/10-23-
2018%20Fact%20Sheet%20Maternal%20Opioid%20Misuse%20%28MOM%29%20Model%20%28FINAL%29.pdf;
CMS, “Integrated Care for Kids (InCK) Model,” 2018, see: www.cms.gov/newsroom/fact-sheets/integrated-care-
kids-inck-model.
181
SFY2018 available appropriations: Office of Administration, “Fiscal Year 2019 Budget Priorities,” 2019, see:
oa.mo.gov/sites/default/files/FY_2019_Budget_Summary.pdf; Medicaid spend: Missouri DSS, see note 1.
32%68%DMH 2,158
DSS 9,32485% 15%
DHSS 1,41366% 34%
Non-MedicaidMedicaid
Total Medicaid spend and department budget appropriation, SFY2018, USD, millions

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
80
EXHIBIT 43: DSS MEDICAID SPENDING
182
Unmatched spending across departments
In DSS, only a handful of narrow categories do not receive federal funds. Some examples of
these categories are Medicare buy-in, through which the state helps pay Medicare premiums
for Medicare Part A and Part B for qualified individuals; state-only assistance, which includes
social services block grants; Temporary Assistance for Needy Families (TANF) grants; and
State General Fund. In addition, DHSS and DMH have more categories of unmatched
spending, although the value of unmatched dollars is a small percentage of the total spending
across the departments. Within DHSS, there could be potential to receive additional match for
Alzheimer’s services and communicable diseases, and within DMH, opportunity exists in
autism spending, crisis intervention services (24-hour hotline and mobile outreach for
psychiatric patients, although only outreach could be eligible for match), and some emergency
room enhancements (ERE).
Other state funds
Provider taxes contribute $1.4 billion to the state Medicaid program, of which $1.1 billion is
derived from hospital taxes and $0.3 billion from nursing homes and pharmacies. The hospital
tax (>5.5%) and nursing home tax ($13.40 per patient day) rates are both high compared to
other states.
183
The use of intergovernmental transfers (IGTs) is limited.
182
Office of Administration and Missouri DSS: see note 181; Missouri DSS, “MHD-FY 18 MMIS Expenditures Final
8-13-18,” 2018; interviews with Medicaid program staff members.
183
Missouri DSS, see note 11.
Federal matching, %
Medicaid spend by department – DSS , USD, millions
108
Managed Care
Pharmacy – Medicare Part D
Pharmacy
449186
1,256
70
69
168
130
65
Nursing Facilities
Physician
Rehab & Specialty
Hospital Care
MMIS
Other
1,961
45
178
1,274
298
704
564
506
835
212
481
331
425
Premium Payments
364
328
259
280
254
State - GR FederalState - Other
64%
66%
64%
65%
65%
60%
66%
0%
69%
54%

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
81
Potential opportunities for improvement
This section identifies potential opportunities to improve Missouri’s current approach to federal
financing. The opportunities are not intended to be mutually exclusive: potential savings
identified in individual opportunities may overlap with those identified in others.
• Missouri could consider leveraging new federal programs that provide federal
funding for innovative Substance Use Disorder/Opioid Use Disorder (SUD/OUD) and
behavioral health models. A variety of new funding opportunities have recently been
made available to states, including CMMI grants for the design of alternative payment
models, guidance from CMS on additional demonstration opportunities that grant
increased flexibility in how Medicaid funds are used, and the wide-ranging funds made
available to a variety of agencies through the SUPPORT for Patients and Communities Act
(SUPPORT Act). Exhibit 44 contains a breakdown of different sources of non-federal funds
for Medicaid payments.
EXHIBIT 44: SHARE OF NON-FEDERAL FUNDS FROM DIFFERENT SOURCES
184
Potential initiatives
The state could consider several potential initiatives to improve its federal financing. The total
opportunity could be $10 million to $20 million in grant funding and additional enhanced match,
depending on decisions made by the state.
185
These initiatives address overlapping populations
and provide different types of funding (grants, enhanced match, regular match for new sets of
services). The state could consider strategically combining initiatives to maximize efficiency and
184
MACPAC, “The Impact of State Approaches to Medicaid Financing on Federal Medicaid Spending,” 2017, see:
www.macpac.gov/wp-content/uploads/2017/07/The-Impact-of-State-Approaches-to-Medicaid-Financing-on-Federal-
Medicaid-Spending.pdf.
185
U.S. Congress, CMS: see note 180.
70%
72%
80%
36%
22%
10%
9%
6%
19%
32%
16%
14%
9%
44%
42%
5%
5%
DSH payments
Managed care
payments
5%
Fee for service
Payments
4%
Total
1%
Non-DSH
supplemental
payments
State funds
Other sourcesProvider taxes and donations
Funds from local governments

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
82
generate funding to support the design, development, and implementation of the models as well
as the associated care delivery costs.
1. Access enhanced match by strengthening SUD focus in health homes. While Missouri
has exhausted the eight quarters of enhanced match for the health home program, the
SUPPORT Act allows for the creation of a new SUD-focused SPA that would cover 10
quarters of enhanced match for individuals with SUD not previously covered under a health
home. There are three groups of individuals whom the state could potentially consider as
part of a new SUD-focused SPA: (a) participants with SUD who meet the existing health
home criteria but were never successfully engaged (e.g., no payment occurred for those
participants); (b) participants with SUD who are newly eligible and meet the existing health
home criteria; and (c) participants who are not eligible under the current criteria but would be
eligible if the state created additional eligibility pathways for the SUD population (e.g.,
making receipt of MAT a qualifying factor, creating an eligibility pathway for pregnant women
with OUD). The state would need to meet reporting requirements outlined in the SUPPORT
Act (e.g., quality of care reporting, reporting of costs of individuals in health homes).
186
2. Pursue a State Plan Amendment to access federal funds for SUD services provided in
IMDs. Missouri may be able to leverage the Amendment to the IMD Exclusion to use federal
funds to pay for treatment services in residential settings that qualify as IMDs. To access the
funds, Missouri would need to design a program emphasizing quality and value. Missouri
could consider working with CMS to develop a State Plan Amendment (SPA) initiating the
program; this SPA could potentially be effective as early as October 1, 2019. As the services
currently are not provided, this initiative would be an investment which the state could
consider as part of a value-based program, for example, to reduce total cost of SUD care.
3. Apply for the Serious Mental Illness/Severe Emotional Disturbance (SMI/SED)
demonstration through a Section 1115 Waiver. The SMI/SED demonstration allows
states to use federal funds to pay for treatment services in residential settings that qualify as
IMDs for individuals with SMI/SED.
187
To access the funds, Missouri would need to design a
program emphasizing quality and value that meets budget neutrality requirements for a
Section 1115 Waiver. Missouri would be expected to achieve a statewide average length of
stay of 30 days for participants receiving care in IMDs. Additional analysis would be required
to understand the net budgetary impact of funding for SMI/SED services provided in IMDs.
4. Apply for CMMI grant funding through the Maternal Opioid Misuse (MOM) and
Integrated Care for Kids (InCK) Models. The models provide states with federal funds to
help the state fund programs to combat OUD in pregnant and postpartum Medicaid
participants and improve behavioral health care for children up to 21 years.
188
MOM
provides up to $64.5 million nationally for implementation, transition, and milestone funding
distributed across up to 12 states; InCK provides $16 million
189
. The state could consider
applying for these grants, which could be (but need not be) seen as two sides of the same
coin. The Notices of Funding Opportunity (NOFO) for both programs are expected in early
2019; applications for funding are likely to be due early in 2019 and funds awarded in late
2019.
186
U.S. Congress: see note 180.
187
U.S. DHHS, “Section 1115 Demonstration Process Improvements,” 2017, see: www.medicaid.gov/federal-policy-
guidance/downloads/cib110617.pdf.
188
CMS, see note 180.
189
CMS, see note 180.
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
83
MEDICAID MANAGEMENT INFORMATION SYSTEM (MMIS)
The current MMIS is a set of ~70 integrated components that plays a fundamental role in most
of functions of the Missouri Medicaid program. Its “core” is a 1979 mainframe system,
maintained and operated by Wipro; a set of additional components are maintained and operated
by Conduent. Three main improvement opportunities were identified. First, while the level of
spending on technology is not misaligned with the needs of a Medicaid system of Missouri’s
size, the functioning of the technology does not meet current or future needs. Its limited
functionalities and the antiquated architecture underlie several of the program’s performance
challenges identified throughout this report. Second, there is an opportunity to increase
alignment between program strategy and the Information Systems group’s (IS) strategy. The
current MMIS replacement plan does not include the specificity required to ensure that the
forthcoming modules will meet future needs. Third, the IS group lacks the range of capabilities
needed to ensure an MMIS replacement trajectory that will deliver that future functionality.
Within this context, the IS group has taken important steps, such as the creation of an outline of
a strategic plan for modular replacement and the prioritization of an Enterprise Datawarehouse
(EDW) and Business Intelligence System (BIS). However, the state could consider a concerted,
integrated effort to set up the MMIS for success. A full end-to-end plan could further define the
current roadmap for modular replacement based upon the functionalities most needed from the
perspective of the future Medicaid program, including prioritization and specified use cases. If
the state would decide to take such an approach, it could consider integrating strategic program
priorities, operating models, capabilities, governance, and environment (e.g., procurement,
FMAP) into the updated end-to-end plan.
Current situation
This section describes the MMIS, the in-flight initiatives and the plans for future improvements
and its costs.
MMIS definition
MMIS includes the Core system operated by Wipro, the Clinical Management Services &
System for Pharmacy Claims & Prior Authorization (CMSP), and the Program Integrity solution
operated by Truven. The MMIS is not managed by the Information Technology Services
Division (ITSD) of the Office of Administration but rather by MHD, with a few notable exceptions:
Financial Cycles and Federal Financial Reporting is managed by Division of Finance and
Administrative Services (DFAS), HCBS Assessment is managed by DHSS, and Provider
Enrollment and Program Integrity is managed by MMAC. The Eligibility Determination systems
(managed by Family Support Division [FSD], Division of Youth Services [DYS], and Children’s
Division [CD]) and Claims Pre-Processing and Adjudication (managed by DMH and DHSS)
were excluded from the analysis.
The “MMIS” refers to a disparate range of technologies that are integrated. The components
tend to be named for the function they support, and they can include staff or vendor staff
activities associated with the technologies. There are also components that largely consist of
(vendor) staff activities rather than technology, as when for example several components are
managed by the same vendor. This broad definition can and does cause confusion in strategic
and tactical discussions, where what “MMIS” means may vary amongst those involved.
Functional and Technical
Missouri’s MMIS consists of a collection of technologies that include ~70 components
supporting a broad range of administrative functions of the Missouri Medicaid Program. These

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
84
components are supported by three vendors. Wipro manages the core MMIS IBM mainframe-
based system, programmed in COBOL (~7 million lines of code)
190
, originally installed in 1979.
Conduent manages the as-a-service CMSP system
191
which is heavily interconnected with the
Core and supports Care Quality Solutions (inpatient certification, reporting, and provider web
tool), Prescription Delivery (clinical decisions for claims processing and clinical edits), and the
Health Information Exchange. Truven manages the current Program Integrity system
192
which
is interconnected with the Wipro system.
Some of the components are managed by a single vendor while others have shared vendor
responsibilities. Given the architecture and history of the system, many of the ‘components’ are
not partitioned, distinct subsystems but may be highly intertwined within the COBOL code. To
help the planning for future modular replacement, the Information Systems groups has classified
the existing components into the below 11 functional categories.
1. Core Claims / Encounter Processing (administered by MHD): supports core Medicaid
functions such as FFS claims processing, participant web portal, and financial management
(e.g., calculation and transmission of payments, provider specific taxes and
reimbursements, financial summaries). Wipro manages the majority of this functionality
while some components are maintained by ITSD (Medicare buy-in and premium collections
and spend down) and Conduent (participant web portal).
2. Pharmacy and Drug Rebate (administered by MHD), operated by both Conduent and Wipro.
Pharmacy, clinical adjudication, and preferred drug list are operated by Conduent. These
components include pharmacy functions such as managing participant pharmacy benefits,
maintaining and applying the drug formulary, and performing pharmacy pre-certification.
Wipro operates several functions including drug rebate processing and initial claims
validation and pricing.
3. Pharmacy Administration (administered by MHD): primarily manages the drug formulary and
setting supplemental drug rebate amounts. These services are operated primarily by
Conduent.
4. Provider Enrollment (administered by MMAC): is responsible for enrolling, screening, and
monitoring both FFS and managed care providers. It is maintained by Wipro, which
subcontracts parts of this work to LexisNexis.
5. Managed Care Enrollment Broker (administered by MHD): these components are
responsible for the enrollment of managed care participants in plans through a web portal,
associated physical mailings, auto-assignment, and a contact center. The web portal and
auto-assignment system are maintained by ITSD, while the contact centers and any
physical mailings are operated by Wipro.
6. Contact centers (administered by MHD): supports both the provider relations, participant,
and prior authorization contact centers. The provider contact center covers inquiries from
providers around program policies, claim assistance, and claim processing instructions,
while the participant contact center covers inquiries from participants about eligibility,
spenddown, and covered services. The prior authorization contact centers support prior
authorizations over the phone. The Contact centers category is operated by Wipro and
includes the phone system and contact documentation software.
190
This system is hosted by Wipro in a data center in Omaha, NE.
191
This system is hosted by Conduent in data centers in East Windsor, NJ; Sandy, UT; and Richmond, VA.
192
This system is hosted by Truven in a private cloud.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
85
7. Data, Analytics, and Reporting (administered by MHD): supports the Medicaid program’s
needs to access, analyze, and report on data stored in the MMIS. The current system is
primarily focused on providing the required outputs to Transformed Medicaid Statistical
Information System (T-MSIS)
193
federal financial reporting, and program reporting. Both
Wipro and Conduent manage various analytics and reporting components, aligned with their
business functions.
8. Program Integrity (administered by MMAC): supports the detection of potential Medicaid
fraud, waste, and abuse (FWA) through the analysis of claims data. It is currently operated
primarily by Truven Health Analytics and consists of Data Pro (which runs state-defined
algorithms to detect possible FWA and provides ad hoc reporting) and Truven Advantage
Suite (which provides dashboard reporting). Additionally, the surveillance and utilization
review components are operated by Wipro.
9. Health Information Network (administered by MHD): covers the connection of MMIS to
various Health Information Networks (HINs). The platform, maintained by Conduent, is in
place but is currently not connected to any HINs, pending contract negotiations between the
state and HIN(s).
10. Prior Authorization (administered by MHD): encompasses the automated PA system, the PA
web portal, participant case management, and the processing of various prior
authorizations. The web portal is operated exclusively by Conduent and the case
management and prior authorization processing is handled by both Wipro and Conduent,
with the exception of dental, physician, audiology, and out-of-state services, which are
handled by Wipro.
11. Ancillary / Supporting Services (administered by MHD): these include cross-cutting
components that support other components, such as printing and mailroom, help desks, and
project management. These services may be shared across functions and vendors.
Current replacement plans
CMS has issued guidance for the replacement of MMIS, outlining the criteria for which states
can be eligible for 90/10 federal match of MMIS replacement initiatives.
194
These guidelines
emphasize a modular approach to the acquisition of MMIS modules to encourage reuse,
reduce the need for customization, stimulate and expand the vendor landscape, grow adoption
of shared services, and reduce overall MMIS cost. To meet the CMS criteria, the 11 categories
outlined above are identified as the modules in which Missouri has organized the ~70
functions of its current MMIS.
As an overall business strategy for the Missouri Medicaid program is not clearly defined and
integrated with IS’ plans, the detailed three- to five-year end-to-end approach for MMIS
modular replacement (e.g., the timing and requirements for specific modules beyond currently
planned initiatives) has not yet been fully determined.
193
T-MSIS is a data set that CMS requires states to submit which includes data such as: utilization and claims data,
enhanced information on beneficiary eligibility, managed care data, and Medicaid and CHIP expenditure data, see:
www.medicaid.gov/medicaid/data-and-systems/macbis/tmsis/index.html.
194
CMS, “Mechanized Claims Processing and Information Retrieval Systems-Enhanced Funding,” 2016, see:
www.medicaid.gov/federal-policy-guidance/downloads/smd16004.pdf; CMS, “Mechanized Claims Processing and
Information Retrieval Systems – APD Requirements,” 2016, see: www.medicaid.gov/federal-policy-
guidance/downloads/smd16009.pdf; CMS, “CMS-2392-F Mechanized Claims Processing and Information Retrieval
Systems – Modularity,” 2016, see www.medicaid.gov/federal-policy-guidance/downloads/smd16010.pdf.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
86
The state has started the replacement process with two modules identified as priorities. CMS
has approved the Advance Planning Documents (IAPDs) and contracts have been awarded in
April/September 2018 for a Program Integrity solution and a Business Intelligence
Solution/Enterprise Data Warehouse (BIS/EDW). To support a Medicaid transformation effort,
providing access to MMIS data in a timely and efficient way is considered important. The
BIS/EDW, therefore, is considered a foundational module
195
. The Program Integrity solution
has been contracted to replace current functionality and facilitate incremental improvements.
Cost
Total SFY2019 projected MMIS spending is $85 million, comprised mainly by two main
contractors: Wipro and Conduent ($51 million [60%] and $17 million [20%], respectively).
196
IS
project spending is set to increase from $65 million (SFY2018) to $93 million (SFY2020)
197
,
driven primarily by net-new spending, such as Truven spending on BIS/EDW and PI (the start
of the modular replacement), a managed care pilot, T-MSIS, Health Information Network
connection, Electronic Health Records, and HCBS support. Current system costs for MMIS
and CMSP remain stable. Projected MMIS spending from SFY2018-SFY2020, by vendor, by
funding source, and by spend type is shown in Exhibit 45.
The SFY2019 weighted average federal match is 73%, up from 69% in SFY2018, and it is
projected to increase to 75% in SFY2020, driven by increased match on implementing new
MMIS modules.
198
In SFY2019, this is projected to split into 90% match for design,
development, and implementation activities (DD&I) ($20 million, or 24% of total); 75% match
for maintenance and operations activities (M&O) ($48 million, or 56% of total), and 50% match
for administrative activities ($17 million, or 20% of total). When the implementation activities
have been completed, funding for components will shift to 75/25. Overall spending on these
items is expected to decrease as the activities shift from DD&I to M&O. From SFY2018-
SFY2020, administrative costs are projected to remain stable, thus decreasing as percentage
of total cost as total cost increases.
195
Interviews with Medicaid program staff members.
196
Missouri DSS, “MHD – FY 18 MMIS Expenditures FINAL 8-13-18,” 2018; Missouri DSS, “MHD – FY 19 MMIS
Expenditures 10-31-18,” 2019.
197
Missouri DSS, “MMIS Spend Plan FY20 Compare to FY19,” 2019.
198
Missouri DSS: see note 197.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
87
EXHIBIT 45: PROJECTED MMIS SPENDING THROUGH SFY2020
Potential opportunities for improvement
This section highlights observations based on a high-level assessment of the current state.
• The current MMIS is insufficient for current and future needs, and the antiquated
mainframe technology poses a risk to the program. The limitations of the current
systems prevent Missouri Medicaid from operating at maximum efficiency. Examples
surfaced in other areas of this assessment of the Medicaid program include the following:
the MMIS system rejecting certain MCO data submissions resulting in incomplete MCO
data; incomplete encounter data limiting the effectiveness of MMAC audit reviews; difficulty
in transferring MCO encounter data into MMIS likely resulting in increased error rates;
multiple-format data entry required for pharmacy rebate information increasing rebate
processing time; challenges in eligibility determinations with MEDES data for MCOs
impacting participants’ ability to enroll; difficulty in adding new data fields to the proprietary
layout; and challenges to identifying certain eligibility categories reducing ability to correctly
identify CHIP-eligible children.
To support new initiatives coming from other topical areas, changes would be required in the
MMIS, sometimes with difficult tradeoffs. Generally, there are three categories into which
new initiatives fall.
― Narrow configuration / code changes, where system changes to support an initiative can
be directly made in the current system with minimal disruption. Examples include
additional clinical edits to allow for pharmacy policy adjustments, automation of claim
adjudication driven by lab testing diagnoses, or modifications to MCO auto-assignment
and lock-in logic to expand day-one managed care eligibility and passive enrollment.
$69.7
(75%)
$44.8
(69%)
$19.7
(31%)
$62.6
(73%)
$22.9
(25%)
$22.6
(27%)
$64.5
$85.2
$92.6
$12.7
(20%)
$0
$49.9
(77%)
$50.6
(59%)
$9.1
(11%)
$1.9
$16.7
(20%)
$8.8
(10%)
$51.2
(55%)
$17.6
(19%)
$12.7
(14%)
$11.1
(12%)
$64.5
$85.2
$92.6
$50.6
(55%)
$16.1
(25%)
$45.3
(70%)
$26.9
(29%)
$3.1
(5%)
SFY2018
$47.6
(56%)
$17.4
(20%)
$20.2
(24%)
SFY2019
$15.1
(16%)
SFY2020
$64.5
$85.2
$92.6
OtherConduentWiPro IBM / Truven
Federal State
Vendor
($M)
Funding
source
($M)
Spend type
($M)
Admin (50/50) M&O (75/25) DD&I (90/10)

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
88
― Limited workaround, where workarounds may exist separate from the system that can
be implemented to support new or updated functionality with relatively few changes
made in the current MMIS system. These workarounds range from a separate
software/service to support VBP analytics, a standalone data intake system to augment
current encounter data, to a supplemental submission flow for X12 data.
― Extensive workaround or rebuild, where a workaround is theoretically possible, but may
involve altering so much of the existing MMIS system that it is worthwhile considering
rebuilding the functionality in a modular replacement instead. Changes this intensive
include drug-level pricing for 340B drugs, DRG classification and payment processing,
and additional rate cells for MCO ABD carve-in.
The state could consider prioritizing the first two categories, as the return on investment of
making these changes is likely better than for the third category. Changes in the third
category could involve a tradeoff between a temporary, possibly costly and higher-risk
investment in the current system while the desired functionality could also be implemented
as part of a forthcoming modular replacement.
Additionally, the decades-old mainframe technology poses a risk to future Missouri Medicaid
success. It is increasingly difficult to maintain the aging core mainframe technology, as the
needed expertise and talent in the marketplace are decreasing. Depreciating technology is
supported by fewer and fewer vendors due to market trends.
Monolithic mainframe systems lead to a lack of agility to make changes in one part of the
system without risking impact to others, as it is especially difficult to fully trace the impacts of
changes in a non-modular system. Ultimately, the risk of mainframe impact inhibits the
ability to quickly make system changes. For example, to make a small update, code
changes may be required in another 50+ locations which may not be simple to edit.
Current MMIS module offerings (such as an off-the-shelf Pharmacy Benefits Management
solution) are built on more modern generations of technology or delivery models (virtualized,
containerized data centers, or cloud services), further risking interoperability between the old
MMIS and new modules.
• Lack of alignment and coordination between Information Systems (IS) and the
Medicaid program. Interviews with IS staff indicate that there is currently no structural
process to incorporate IS in strategic program decisions or to maintain adequate program
awareness of IS challenges and opportunities. In addition, the IS department’s strategic
plan does not appear to be well aligned with program strategic priorities and outcomes, as
these have not been well established, resulting in a lack of detail and prioritization of
program initiatives.
199
The lack of alignment may limit the ability of IS to create MMIS-
related procurements with specific, precise program goals.
• MHD’s IS organization does not map to the needs of a next-generation, modular
MMIS. Based on discussions with IS staff as well as expert interviews across different
states, Missouri’s IS organization appears to not be appropriately staffed and structured to
handle both the day-to-day maintenance and operation of the present MMIS as well as the
planning, implementation, and certification of a new, modular MMIS. Across four areas,
staff and interviewees noted that the IS department lacks key capabilities to support the
new requirements of a modular MMIS.
199
Interviews with Medicaid program staff members.
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
89
― Technology: Covers the capability to define a technical architecture both between and
across vendors, manage several simultaneous procurements and implementations, and
sufficiently understand business process implications on the IS group. Lack of
capabilities within the technology area can result in systems which are not built toward a
centralized architecture, interruptions in current system maintenance, and delays in the
procurement and certification processes. IS currently has one dedicated technical
resource and does not appear to have resources to cover the additional activities
currently slated for the modular replacement. Examples of positions that may provide
these capabilities include technical architects, system operations managers, and
technical managers / project managers.
― Data: Covers the capability to articulate a data governance strategy, align data
management strategy to program goals, and translate between program requirements
and data environment. Missing these capabilities can lead to issues with data quality,
management, and governance. IS does not currently have any resources dedicated to
data capabilities. Positions that could provide these capabilities might include data
architects, and data scientists / engineers.
― Contract management: Covers capabilities such as technical assessment of bid
responses, alignment between RFP/contract outcomes to program goals, and
certification of multiple modules simultaneously. Without these capabilities, contracts
may lack conciseness and precision, risking suboptimal functionality. Additionally,
certification cycle time may increase without appropriate certification resources. IS
currently does some limited contract management through OA and its project managers,
but OA does not currently have dedicated resources to compose xAPDs (PAPDs,
IAPDs, and OAPDs). Example positions that could provide these capabilities include:
contract managers, xAPD writers/budget managers, and dedicated resources for various
contracts and certification tasks.
― Vendor management and accountability: Covers capabilities such as holding vendors
accountable to contract and program outcomes/deadlines and facilitating cross-vendor
cooperation. Without these capabilities, the risk of vendors delivering suboptimal or
incompatible functionality, or failing to meet milestone deadlines, is increased, especially
as the number of vendors is likely to increase. IS currently has a limited number of
project managers but does not appear to be sufficiently resourced to support upcoming
modular replacement activities. Additional project managers and a clear governance
structure (including who is making decisions regarding areas such as infrastructure,
policy, or participant interactions) is an industry best practice without which vendors may
not be able to align to a unified vision and work cohesively.
Potential initiatives for consideration
1. Improve alignment between IS and program. Missouri could consider adopting the
following industry best practices in place in many other states.
The state could include an integrated perspective across both IS and the program in both
strategy development / planning and day-to-day operations. This would include having IS
representation at key program meetings to advise on technical implications and feasibility of
various program decisions. In this way, IS would be able to inform and advise on
implications of program decisions, introduce novel ideas, provide insights in IS-driven needs
as well as opportunities ahead of time. Additionally, it would allow IS to keep business
informed about in-flight initiatives to take into account during program decision-making.
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
90
Additionally, the state could conduct joint planning exercises to ensure that IS timelines are
in accordance with program-desired outcome delivery dates of both technical and functional
requirements. These exercises could also help IS explain the choices that the program may
have to make and the implications of those choices. These decisions, which tend to be
made by the program, will impact the delineations between modules as well as the
sequencing of module implementation. Holding these planning exercises may help tighten
the feedback loop for IS to explain the choices that the program may have to make and the
implications thereof.
Lastly, the state could consider including specific desired functional/program outcomes in
procurement documents (e.g., RFPs, vendor contracts) such that vendors are operating
against both technical specifications required by IS and functional specifications required to
drive targeted, prioritized program outcomes. The additional specificity may help ensure that
IS day-to-day tactical actions are more closely aligned.
2. Evaluate the current modular replacement strategy and define an updated strategy
informed by clear strategic direction from the program and reflecting better alignment
to the market, other states, and CMS. First, Missouri could reevaluate the structure of
modules used in the current replacement plan, realign it closer to the modules
recommended by CMS and those utilized in other states further along in their MMIS
modernizations, and map to solutions offered in marketplace. Additionally, finalized modules
may be aligned to program priorities (e.g., the decision to carve pharmacy in or out of
managed care would alter the future Pharmacy module). To create an illustrative example of
a potential module alternative, several interviews were conducted with experts both in
Medicaid and in the MMIS industry to understand the common module structures and
market offerings. In Exhibit 46, a sample alternative module option is displayed, along with
Missouri’s current module structure as well as the common marketplace modules.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
91
EXHIBIT 46: ILLUSTRATIVE EXAMPLE OF ALTERNATIVE MODULES
Next, the state could conduct further rigorous planning to help create a roadmap aligned to
program priorities with IS input on feasibility. Four sample evaluation criteria were created
that could be used to develop a heatmap of module priorities: program
priority/value/service delivery strategy (e.g., impact of module and functionality on program
priority and service delivery strategy, specific program outcomes driven by the module, and
urgency and criticality of value unlocked by module), solution availability (e.g., maturity and
competitiveness of marketplace, variety of marketplace solutions available), resources
(e.g., available resources to dedicate, potential upfront and ongoing costs), and complexity
(e.g., dependencies on upstream, downstream, other modules, or other departments and
change required).
Through a sample planning exercise conducted with IS staff, each module from the
potential alternative module option was evaluated against the sample criteria, considering
factors such as updated vendor landscape information, incompletely defined program
decisions, populations affected by module change, and ongoing procurements in other
departments. The preliminary illustrative roadmap created (shown below in Exhibit 47)
could be updated as program priorities are clarified and strategic decisions (e.g., pharmacy
carve in/out, additional managed care population carve-in) are made by the program.
Additionally, any roadmap could be validated at multiple levels and pressure-tested for
feasibility, with many dependencies (e.g., vendor responses, CMS approvals).
Core MMIS/Encounter
Prior Authorization
Pharm./Drug Rebate
Pharm. Admin
Enrollment Broker
Call Centers
Provider Enrollment
Program Integrity
BIS – EDW
Health Info Network
Ancillary Services
MO Modules
Core MMIS/Encounter
Pharmacy
Provider Management
Program Integrity
BIS – EDW
Third-Party Liability
Care Management
Prior Authorization
System Integrator
Financial Man.
Enrollment Broker
Call Centers
Health Info Network
Commercially available
vendor solutions
Core MMIS/Encounter
Prior Authorization
Pharmacy
Enrollment Broker
Member Call Center
Provider Management
Program Integrity 1
BIS – EDW
Health Info Network
Ancillary Services
Third-Party Liability
Care Management
System Integrator
Program Integrity 2
Potential Alternate
Potential Alternate Rationale
Third-Party Liability:
Consolidated standalone solutions
exist
Care Management: off-the-shelf
integrated solutions available, split
from Prior Authorization
Pharmacy: Best practice across
states to have single pharmacy
module
Call Centers: Best practice is to
have member call center
outsourced and provider call
center bundled with claims
processing or provider
management
Program Integrity 2: Next-
generation capability added in a
new module separate from
Program Integrity 1 module
System Integrator: Future
requirement due to increase in
vendor complexity
Ancillary Services: Services not
directly related to technology
which should be handled
separately

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
92
EXHIBIT 47: ILLUSTRATIVE MODULE SEQUENCING
Based on clarified program priorities and a value assessment of the current modular
replacement strategy, the state could then define their clear, updated, end-to-end strategy.
3. Strengthen IS capabilities through hiring, partnering for talent, and
retraining/upskilling. DSS could consider prioritizing upskilling IS to complement the
currently available skill sets with capabilities focused on technology, data, contract
management and vendor management and accountability. Training, hiring, or outsourcing
individual expertise are all possible routes towards this goal.
4. Optimize insourcing vs. outsourcing. Increasingly, Medicaid leaders across the country
are confronted with the need to make informed decisions about what MMIS activities to keep
in-house and what to outsource. This decision is particularly critical given that most
agencies are making greater use of managed care, implementing value-based purchasing at
scale, and/or replacing the business information system platforms they use for eligibility
determinations, claims processing, and provider management. All these changes have
significant impact on the component’s required functionalities. CMS guidance would suggest
that a best practice is to keep policy and infrastructure-related decisions in house, allowing
for additional oversight and agility. Other activities, such as handling participant interactions
may be more efficiently outsourced or delivered through a hybrid model. To make this
determination, the state could evaluate factors such as strategic priorities, existing talent,
and vendor availability.
High complexity, with
interdependencies or upstream
milestones required
Relatively standalone,
moderate criticality and
difficulty
Critical needs
or quick wins
Foundational, relatively
independent
(In-progress)
Case Management
(DMH): In-progress of
creating / releasing RFP,
TBD
▪ BIS – EDW
▪ Program Integrity 1
▪ Pharmacy / Drug Rebate:
Foundational piece with
several vendors offering
modular solutions; not
tightly integrated with Core
MMIS
▪ Health Information
Network: Federally
mandated with immediate
deadline
▪ Provider Enrollment:
Important piece with
simplified procurement
through NASPO, impacts
providers but not members
▪ System Integrator:
Necessary across new
modules
▪ Enrollment Broker:
Implementation timeline
can shift due to managed
care carve ins; affects
potentially majority of
population
▪ Third-Party Liability:
Some initiatives
dependent on TPL
▪ Call Center: Easier to
procure, but depending on
carve ins/outs, vendor may
need to interface with
several different modules /
systems
▪ Prior Authorization: Will
require business process
updates / improvements
prior to implementation;
dependent on new Core
MMIS for new PA layouts
▪ Core MMIS / Encounter
Data Processing: Long
implementation time and
vendors are essentially the
same as monolithic MMIS
providers; market does not
currently have many
modular providers
▪ Program Integrity 2: Not
technically difficult to
implement, but need BIS –
EDW and Program Integrity
1 in place prior to
implementation

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
93
OPERATIONS
The Family Support Division (FSD) and MHD are responsible for critical participant- and
provider-focused functions for the Medicaid program such as eligibility determination, participant
enrollment, provider enrollment, prior authorizations/medical management, claims processing,
and general participant and provider queries and escalations. Cross-cutting support functions,
such as contact centers and data and analytics, support these customer-focused tasks. The
functions are executed through a mix of staff and vendor contracts.
In this section, the performance and operational efficiency of three functions identified by state
staff as having relevant opportunities for improvement are discussed: managed care enrollment,
claims processing, and contact centers.
200
Compared to other states and viewed from the customer-focused functional level (the integrated
process of participant enrollment from eligibility determination to MCO enrollment, for example),
actual work processes often appear fragmented, process steps seem poorly integrated and
best-practice management principles are variably applied. Individual staff participants tend to
have deep knowledge about their own responsibilities but much less insight into the overall
processes and responsibilities therein. Perceived inefficiencies in handoffs between different
parts of the organization (such as manual rework) are often accepted as “inevitable” or
“unavoidable.” Currently, outsourced roles do not appear to be optimally integrated or managed
to ensure high performance of functions.
Potential initiatives identified, if employed, may help improve suboptimal service provided to
participants and providers, create efficiencies in deployment of scarce staff, reduce frustrations
in the workforce, and realize savings while improving vendor performance. Initiatives could
include process optimization, with redesign starting from the perspective of the client(s);
automation improvements and improved contract management. Improvements made to address
the gap with best practices across the different functional areas could lead to up to 15% to 20%
improvements in productivity. This may create staff capacity that could be redeployed for other
purposes, to improve program effectiveness and workforce satisfaction.
201
Current situation
Participant managed care enrollment
Participant enrollment processes within MHD aim to enroll children and pregnant women found
eligible by FSD into the managed care program.
202
Once a participant is found to be MCO-
eligible, the Information Technology Services Division (ITSD) passes that information to the
Enrollment Broker (EB). The information the EB sends is determined based on whether the
applicant is a “state care and custody” individual, a pregnant woman, and/or “all other”
individuals. “State care and custody” applicants are auto-assigned to a Medicaid plan. They
receive letters with this information, additional information about switching plans if they wish,
and enrollment guides. Pregnant women and all other individuals receive a welcome letter with
an enrollment form and an enrollment guide. Pregnant women also receive a health risk
assessment. If they do not decide within seven days, they are auto-assigned to an MCO. All
other MCO-eligible participants have 15 days to choose an MCO before they are auto-assigned.
200
Interviews with Medicaid program staff members.
201
Analysis of DSS data versus industry benchmarks.
202
Interviews with Medicaid program staff members; for participants not in managed care no additional enrollment is
required. Once found eligible, notices are triggered, and these participants are covered as long as they keep up to
date on any premium payments, spend downs, etc.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
94
While the majority of process steps are automated, errors with inbound data feeds and
interactions with other state agencies drive manual interventions to ensure participant
enrollment is accurate and timely. Communications with several other state agencies take place
and are coordinated by the MHD team over email and phone correspondence.
The participant enrollment function serves as a critical interface with FSD. The process consists
of four steps (see Exhibit 48). Eligibility determination is performed within FSD, and managed
care enrollment is performed as a downstream process within MHD through an enrollment
broker. The function relies heavily on upstream FSD systems for data and information feeds.
MHD receives enrollment information from five systems, with the majority of volume driven by
FSD systems. MEDES, the primary system for managed care eligibility, supplies participant
information such as age, income, pregnancy status, etc. Once automated processes have run,
any exceptions and errors are handled within MHD participant enrollment staff through manual
intervention and communication with other state agencies such as FSD.
EXHIBIT 48: PARTICIPANT ENROLLMENT WORKFLOW
The function also engages other state services: Information feeds from the Department of
Corrections, DSS, and the Children’s Division are received monthly for manual enrollment
updates. Information supplied contains data on incarceration dates, status in foster home
programs (flagged as runaway), etc.
Claims operations
Claims operations include processes from intake of claim files, prior authorizations, claim
adjudication and finalization.
203
Claims operations involve multiple stakeholders across claims
203
Interviews with Medicaid program staff members.
FSD and other
state agencies
Data provided
to MO Health
Net for MCO
enrollment
Errors are manually
adjusted to ensure
accuracy
Enrollment updated based
on information from
department of corrections,
child services, etc.
Errors require
manual processing
Enrollments
process begins
automatically
Error reconciliation
Upstream eligibility
determination
Periodic enrollment
status updates
Errors in enrollment data are
manually reconciled
FSD and other
agencies determine
eligibility
Participant status updated
based on information from
state agencies
ITSD and MMIS process
upstream enrollment data
MCO enrollment
Process
workflow
Process
description
▪ FSD, child services,
youth services and
other agencies
determine eligibility
for Medicaid
enrollment
▪ Participant
information is
passed to MO
Health Net for MCO
enrollment
▪ Eligibility data received
from state agencies is
ingested and checked
for accuracy
▪ Accurate records begin
the enrollment process
through data intake by
ITSD and MMIS
systems
▪ However, data errors
drive need for manual
reconciliation
▪ Manual adjustments are
made to erroneous data
inputs to ensure accurate
enrollments are processed
▪ Information exchange is
often over email and phone
with various agencies
▪ Participant status
changes are often
received from
department of
corrections, child
services and other
agencies
▪ Updates are reflected
through manual updates
to enrollment systems

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
95
operations, IT, and vendor resources. These operations are both largely automated and
outsourced, in line with industry best practices (see Exhibit 49).
EXHIBIT 49: CLAIMS INTAKE, ADJUDICATION, AND PAYMENT PROCESSING WORKFLOW
The claims operations function cuts across core claims operations, IT systems (MMIS), and
other adjacent processes such as prior authorization. The claim intake is largely digital with
limited need for OCR or manual intake in MMIS. The sources of manual intake include out-of-
state provider claims, some drug claims, and some DME claims. Various labor-intensive
process steps such as manual adjudication and prior authorization have been outsourced and
MHD staff focus on issue resolution with vendors and providing expertise to allow vendors to
adjudicate claims appropriately. Although the MMIS system is outdated (see previous section),
its core FFS claim processing functionality has over the years become well-aligned with
current work processes and needs. The system yields high auto adjudication rates, reducing
manual work and improving accuracy for participant and provider stakeholders.
Claims operation processes are largely outsourced: vendors are utilized across almost all
process components, including exception adjudication and medical record review.
Contact Centers
DSS manages two large clusters of contact centers. Some contact centers are outsourced; the
largest, internal FSD contact centers are composed of ~350 FTEs. FSD contact centers
handle calls related to food stamps, health care, child care, and child support for families.
Internal contact centers employ full-time state staff members, many of whom served as case
workers before the state moved away from the practice of assigning recipients case workers.
The internal center within FSD handles queries related to food stamp benefits and processing
in addition to a dedicated tier of agents who conduct interviews for food stamp and child care
Adjudication
Pre-Cert /
authorization
Payment and
communications
EDI
gateway
Claims
Accums
DB
Claim
finalized
Manual
adjudication
Auto
Adjudication
Pre-
auth
DB
Provider
payment
EOB
Phone
EDI
EMR
and
benefit
data
Pre-auth
DB
Adjustments and
reprocessing
Claims
Intake
checks
Claim payment calculated and
data synced
Provider verifies
eligibility
Patient and provider
informed of adjudication
decision
837 files
received
Claim
routed to
adjudication
platform
Intake and routing
Process
workflow
Process
description
▪ Pre-authorizations
are received
electronically or
manually
▪ Processed both
internally and by
vendors
▪ Process is largely
automated but
some manual
decision making is
required
▪ Intake includes both
receipt and preparation
of claims for
adjudication
▪ Process is largely
automated with specific
claim types such as out
of state claims triggering
manual intervention
▪ Vendors engaged for
mailroom and OCR
activities
▪ Clean claims are passed to
adjudication system for
finalization
▪ Edits built into system
appropriately adjudicate
claims as to be paid or
denied
▪ Small portion of claims are
pended requiring manual
adjudication
▪ After claim adjudication,
finalized claims are
passed to payment
processes
▪ Appropriate payments
and notifications are
triggered to both
participants and
providers

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
96
eligibility, while outsourced FSD contact centers handle MAGI-related requests. The FSD
contact centers handled 3.2 million calls in 2018.
204
The constituent health services (CHS)
contact centers are largely outsourced. Both internal and external contact centers handle
queries related to the state-run Medicaid program for participants and providers.
205
See
Exhibit 50 for a breakdown of staff members across DSS contact centers.
EXHIBIT 50: MISSOURI DSS CONTACT CENTERS BREAKDOWN
206
Incoming calls to FSD contact centers are routed to one of five tiers based on call reason.
~50% of FSD incoming calls are classified as Tier 1 (family support helpline): basic information
requests, queries about outbound communication (annual review letters) and case status
requests. ~30% of FSD incoming calls are classified as Tier 3 (food stamp interviews), which
handle mandatory food stamp interviews. The remaining ~20% of calls are routed to Tier 2, 4,
or 5 and are requests for live case-processing over the phone (e.g., for issuance of food-stamp
benefits) or MAGI hearing requests (see Exhibit 51). Wait times average ~10 minutes but can
reach over an hour for each tier.
207
204
Analysis of state data, 2018; interviews with Medicaid program staff members.
205
Interviews with Medicaid program staff members.
206
Analysis of state data, 2018.
207
Analysis of state data, 2018.
Constituent
health
services
(~100 FTEs)
Family
Support
Division
(~500 FTEs)
5
23
31
56
Technical helpdesk
28
4
Participant
services
5
7
Provider
relations
Service
authorization
38
60
In-house
Outsourced
55
107
10
Technical Helpdesk
MAGI Helpline
Tier support
desk
Eligibility
and enrollment
~350
FTE

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
97
EXHIBIT 51: OVERVIEW OF FSD CALL TYPES
208
Internal FSD contact center operations are spread across 10 contact centers located
throughout the state. These average a size of ~30-50 FTEs in each location; training, hiring
and other support functions are centralized and require staff member travel. Exhibit 52 shows
the number of staff members as well as the average handle time (AHT) per location.
208
Interviews with Medicaid program staff members; analysis of state data, 2018.
Call type
Tier 1
Tier 2
Tier 3
Tier 4
Tier 5
Description
▪ Basic questions about
applications, eligibility,
minor system changes,
and SS updates
▪ Case processing for food
stamps and MHABD
▪ Interviews for programs
including food stamps and
child support
▪ Hearing request for MAGI
▪ Case processing for
temporary assistance,
childcare, and food stamps
of specific participant
groups (e.g., disabled)
FTEs in
each tier
67
38
160
33
32
AHT Per
Tier (mins)
10.0
15.3
29.2
23.3
16.0
% of
calls
53%
11%
30%
3%
4%
Average wait
times (mins)
13.0
10.9
8.0
9.0
Max wait
times (mins)
67.0
62.2
60.9
61.5

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
98
EXHIBIT 52: FTE BREAKDOWN BY LOCATION – FSD INTERNAL CONTACT CENTERS
209
The AHT varies across locations: there is a 40% variation between the location with the
highest and lowest handle times. Workforce management practices are limited across the
centers. Each location operates for ~12 hours, leading to support ratios of one supervisor to
eight frontline agents and one manager to 45 frontline agents.
Outsourced operations deliver several key services to the Missouri Medicaid program: MHD
participant and provider communications, which handles incoming calls related to participant
and provider queries related to the Medicaid program (e.g., premiums, cost estimates); service
authorizations; and the technical helpdesk for the MHD program.
210
In addition, within FSD, the outsourced contact center specializes in MAGI enrollment and the
eligibility helpdesk, including calls related to program eligibility, enrollment of new participants
into the Medicaid program, inquires related to MAGI and case updates for the existing MAGI
programs.
Potential opportunities for improvement
This section identifies potential opportunities to improve the efficiency and outcomes of
Missouri’s operations functions.
209
Analysis of state data, 2018. ATT: average talk time. ACW: after call work (avg. time for the agent to wrap up
call-related tasks).
210
Analysis of state data, 2018.
Number of FTEs, # AHT in Tier 1, secondsLocation
62
59
53
46
42
37
32
30
28
26
Jennings
Hillsboro
Chouteau
St. Charles
Cape
Midtown
Page
St. Mary’s
Sikeston
Boone
406
478
410
490
545
538
649
593
478
392
-40%
ACWATT

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
99
Participant managed care enrollment and claims operations
• Limited KPI tracking and dashboarding: There is limited tracking of Key Performance
Indicators (KPIs) across key functions. Also, compared to best-in-class payors, contract
management could be improved in areas such as claim handle time, adjustment rate, and
timeliness of payment at a granular level.
211
• Staff members, particularly those involved in the participant enrollment process,
perform a significant number of repetitive manual tasks: Some of these tasks include
incarcerated participant disenrollment, runaway children closeouts in ITSD (while they
remain eligible), immediate enrollment of women who have just given birth, and error
reconciliation.
212
Significant manual intervention is required to ensure enrollment
information is correct and up to date.
For claims operations, the need for manual and resource intensive interventions is limited
primarily to medical record review and claims adjudication. The adjudication of complex
claims typically requires manual intervention to ensure the right amount is being paid for
relevant/appropriate services provided to participants. In some cases, this implies
requesting medical records, that may be reviewed by clinicians, to ensure that services
provided conform to existing policies. Such cases can require significant time as multiple
records are received piecemeal from providers and only a subset may be matched to the
correct claim. Even if the medical record was available, the content/document
management process is not always able to link the record with the corresponding claim.
• Upstream processes and outputs drive errors and limit scope for process
automation: Challenges with the quality of data received from upstream systems drives
manual intervention (e.g., duplicate DCNs, deceased eligibility, >9 months pregnancies).
The information received can be erroneous and needs to be manually resolved by MHD
staff.
213
Resolutions involve review of data received (e.g., re-coding a pregnant participant
as female instead of male) and communication with agencies providing data to gain
clarifications (e.g., managing multiple DCNs). Data updates for participants are often
received through email and must be manually inputted or modified within enrollment
systems including ITSD and MMIS. Several of these issues are currently being addressed
by FSD.
• Participant correspondence processes are not integrated across FSD and MHD:
Parallel communication with participants drives repeat, out-of-order, and therefore
potentially confusing communication to participants. For example, participants receive
eligibility notices and premium notifications separately from both FSD and MHD. FSD
notifications do not inform individuals that they might have to pay a premium and instead
only inform them that they are eligible for Medicaid. Subsequently, secondary premium
notifications from MHD may go unnoticed, resulting in poor response rates and potential
disenrollment.
• Staff members perform significant tasks within participant enrollment: Compared to
those at best-in-class payors, staff members perform a significant number of tasks across
processes such as managed care enrollment, disenrollment, and error correction, which in
other state Medicaid programs are often managed by vendors. Currently, therefore,
211
Interviews with Medicaid program staff members.
212
Interviews with Medicaid program staff members.
213
Interviews with Medicaid program staff members.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
100
internal staff spend much of their time performing tasks that could potentially be
outsourced instead of, for example, focusing on quality assurance of the processes.
Contact centers
• In the FSD internal contact center, current non-phone self-service options are
limited, leading to a high number of live contacts and high wait times: Limited
alternative self-service options (e.g., chat or SMS bots) are available for answering basic
questions, which creates high call volume in Tier 1. In addition, no status notification
systems are in place to inform the participants about the status of food stamp applications
or document requests, leading to requests for over-the-phone case processing and status
updates. The combination of these factors leads to high incoming call volume in Tier 1,
leading to high wait times and sub-optimal customer and staff member experience (e.g.,
waiting 60 minutes for a 1-minute answer to a question). Addressing the above
opportunities could drive a 15% to 25% reduction in incoming call volume while
significantly enhancing participant experience during the food stamp interview process.
214
In addition, the self-service options could reduce call volume in Tiers 2, 3, 4, and 5 through
notification and tracking of claims processing, scheduling hearing requests via email or
chatbots, and alerting an individual when their application is ready for interview via SMS or
email. Self-service options require thoughtful design, as suboptimal website and chat bot
design may reduce participant experience rather than improve it.
• FSD outbound communications (e.g., letters, review requests) and applications
highlight live customer support options that result in high wait times in FSD contact
centers: Many communications focus on providing customer support via phone and do not
guide participants to alternate resources such as the website or clarify the frequently asked
questions in the communication. For example, the Missouri food stamp application form
bolds the customer support number and asks a participant to call as soon as possible,
even though the participant needs to wait 24 hours after submission for the form to be
uploaded in the system.
215
In comparison, Florida food stamp application forms more
clearly explain the processing window and guide participants to resources on the web (see
Exhibit 53).
216
Missouri could adopt a combination of these approaches to improve
participant access to timely support.
214
Analysis of state data, 2018.
215
Missouri DSS, “886-0460 (9-16) Application for Food Stamp Benefits,” see:
dss.mo.gov/fsd/formsmanual/pdf/fs1.pdf.
216
Florida state government, “Access Florida Application,” 2016.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
101
EXHIBIT 53: FOOD STAMP APPLICATION EXAMPLE
217
• Customer experience is impacted due to both variability in average handle time for
calls and high wait times: In each tier, bottom-quartile agents require 1.7 times longer to
handle an average call in comparison to the top-quartile agents. For example, in Tier 3 top-
quartile agents handle an interview in ~18 minutes, while bottom-quartile agents take ~30
minutes (see Exhibit 54).
218
Top-performing agents may handle a call in ~30-40% lower
handle time compared to lower-performing agents.
219
This could indicate gaps in training
and coaching processes, which prevent delivery of a consistent experience. In addition, in
the internal contact centers, workforce management practices are not deployed to match
incoming call volume to expected staffing of agents in each tier; this likely leads to high
wait times in certain tiers during peak times (e.g., >60-minute wait time in Tier 1 on
Monday mornings). Currently, Tier 1 has 67 dedicated agents; although analysis indicates
at least 100 agents may be required to meet demand. Conversely, Tier 5 has 32 agents
although only 15 may be required to meet demand.
220
217
Missouri DSS and Florida state government: see note 215 and note 216.
218
Analysis of state data, 2018.
219
Analysis of state data, 2018.
220
Analysis of state data, 2018.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
102
EXHIBIT 54: AVERAGE HANDLE TIME VARIABILITY – FSD INTERNAL CONTACT CENTER
• In the internal contact centers, multiple locations limit the efficiency of support
functions: Many locations operate at low scale which leads to performance variability,
challenges in support services, and underutilization of facility space.
221
Several locations
have significantly lower management spans in comparison to the industry benchmark ratio
of 15 frontline agents per supervisor (see Exhibit 55).
222
Multiple locations not only lead to
higher cost to serve but also to diminished staff member experience due to reduced scale.
For example, staff members receive less training because of the need to travel to a central
location, and there is inconsistent operating experience in centers.
221
Internal contact center site observations; Interviews with Medicaid program staff members.
222
Analysis of state data, 2018.
422
1,620
Average
335
335
402
487
4th quartile
1st quartile
3rd quartile
2nd quartile
+45%
1,109
1,109
1,479
1,784
+61%
Tier 3Tier 1
AHT per agent quartile (Seconds/call, Aug- Oct 2018)

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
103
EXHIBIT 55: AGENT, SUPERVISOR, AND MANAGER STAFFING LEVELS
• Policies governing the outsourced contact center operations lead to rework for
internal state staff members: In MAGI contact center operations, policies prohibit
outsourced contact centers from submission of MAGI case updates in case of change of
coverage. This tends to lead to a case transfer to internal case processing teams, who
rework the case from the beginning, doubling work and increasing processing time, as well
as potentially frustrating customers. Currently, 38% of calls to the MAGI contact center
must be transferred for internal processing.
223
Similarly, a policy to transfer calls from
MHD reception for internal escalation as opposed to directly to the vendor leads to
disruptions in workflow for internal agents and could potentially be simplified to improve
customer and staff member experience.
• Dual operating environment of in-house and outsourced operating model: The state
currently manages both in-house and outsourced operations in its current contact center
operations. Currently, Missouri’s state in-house operations and outsourcers have similar
operating costs. The state has approximately the same set of resources dedicated to
managing in-house operations and for contracts for outsourced operations. This may lead
to a dual focus of administrative resources and limited opportunity to focus and hone
expertise in either of the skillsets.
223
Analysis of state data, 2018.
5.6
Lowest
span
(Boone)
Highest
Span
(Cape)
Average
(across all
locations)
8.8
8.3
Current Avg.
Benchmark
~15
35.0
60.0
44.4
Avg.
Benchmark
Current
~90
Number of agents per supervisor, #
Number of agents per manager, #
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
104
Potential initiatives
Based on observations and engagement of Missouri’s leaders and functional process owners,
potential initiatives spanning organizational process optimization, automation and digitization,
and sourcing optimization have been identified.
Implementation of outlined initiatives could drive opportunity for MHD across the following axes:
• Enhanced customer experience: Automation, digitization and process improvement
could drive improved experience for participants and reduce pain points.
• Improved staff utilization and satisfaction: Elimination of repetitive, manual processes
and reduction of error corrections could help staff contribute to other high value processes.
FTE capacity created could potentially be used to address limited staffing in other core
operations functions.
• Optimized vendor spending: Assessment of current vendor contracts and management
of existing work types could help reduce administrative expense and vendor performance.
Initiatives that deal with technological improvements and capabilities should likely be
considered in conjunction with the initiatives discussed in the section on MMIS.
Potential organizational process optimization initiatives
1. Develop process guides for staff member efficiency improvement and error
reduction: Currently, a limited number of job guides exist to guide staff member on best
practices for repetitive tasks. The creation of such guides could drive improved efficiency,
reduce errors, and greatly shorten time to ramp up new staff members on core manual
processes. Specifically, the enrollment process has many potential tasks that could benefit
from the creation of a guide, such as incarcerated disenrollment and error reconciliation.
Guides that provide step-by-step instructions on how to complete these tasks could be
readily created and may be greatly beneficial.
2. Develop job aides for high-volume tasks: High-volume tasks that are currently performed
through experience and on-the-job learning have the potential to be standardized and
expedited through the creation of job aids. (Job aids are basic decision trees, checklists,
planning tools that support work and activity by guiding or directing tasks at hand.) For
example, within claims operations, the team could create job aids who provide algorithmic
guides specifically for top edits and manual adjudications.
3. Implement workforce management: In contact centers, for example, shifting staff
members across tiers and optimizing staffing in each tier could achieve reduced wait time on
the phone (i.e., average speed of answer of less than 60 seconds against current average of
over 10 minutes). To achieve this reduction in wait time, potential solutions include moving
agents from Tiers 3, 4, and 5 to Tier 1 and ensuring the right shrinkage factors (e.g.,
absenteeism) are factored into the staffing model. Workforce management principles could
also improve efficiencies within claims processing by further aligning staff members to
specializations by skill level and claim type. This could improve processing times and staff
productivity.
4. Adopt performance management practices: In contact centers, the state could coach
toward behaviors that drive high talk-time and quality and reduce variability in average
handle time across each tier to achieve a ~10% to 12% reduction in average handle time in
each tier and improve customer experience. The state could adopt best-in-class

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
105
performance management practices, including defining clear agent goals and KPIs and
increasing structured coaching and uniform meeting cadence. To help define clear goals
and a holistic set of KPIs, scorecards could be updated with realistic goals against important
KPIs. (See Exhibit 56 for typical measurements that are leveraged in contact center
environments and shared across contact centers to hold individuals/teams accountable for
their role in creating a positive participant experience.) With clearer scorecards and KPIs,
coaching could become more structured and efficient, driving better customer experience
and lower wait time through reduction in average handle time.
KPIs and dashboarding could be equally essential in participant enrollment and claims
processing (see Exhibit 57 for typical KPIs). In the claims tracking process, for example,
organizational leadership could increase its effectiveness if it could have access to critical
KPIs such as auto-adjudication rate, adjustment rate, percentage of claims paid as billed,
rate of denial by denial reason code and denials overturn rate.
EXHIBIT 56: EXAMPLE BEST PRACTICE CONTACT CENTER KPIS
Key KPIs
Service/
Quality
Efficiency
Volume
Dimension
Category Metric Typical definition
▪ Resolution rate ▪ Repeat transaction rate
▪ FCR
▪ % SR requests/calls with a repeat call/SR within 24 hours
▪ % of calls resolved during the first call
▪ CSAT ▪ End-user satisfaction
▪ End-user dissatisfaction
▪ TNPS
▪ On a scale of 1-5, % of customers that have rated 4 or 5 (satisfied/
very satisfied)
▪ % of customers choosing “dis-satisfied (2)” or “very dissatisfied (1”)
▪ Promoters – Detractors
▪ Escalation & transfer
▪ Volume
▪ Escalation and transfer
rates
▪ Transactions offered
▪ % of answered calls escalated /transferred to Tier 2/ other
departments/desks
▪ Availability ▪ Attendance
▪ Schedule adherence
▪ CSR showing up for work on their scheduled day
▪ Time CSR is available / time they are scheduled to work
▪ Utilization ▪ Utilization
▪ Occupancy ratio
▪ (Talk+Hold+ACW)/ Total paid time
▪ Talk and wrap time divided by logged time
▪ Average handle time ▪ Average handle time ▪ (Talk+Hold+ACW)/ Total number of answered calls. Average
processing time for deferred transactions
▪ Transactions quality ▪ Quality score
▪ Critical accuracy score
▪ Call monitoring score(%) (average score on call
monitoring/maximum score)
▪ % of monitored calls without any fatal errors
▪ On time (for deferred
transactions)
▪ Service level
▪ Average time late
▪ % of transactions processed within targeted cycle time
▪ Average time late of transactions which are outside of targeted cycle
time.
▪ Speed of answer ▪ Service level
▪ Avg. speed of answer
▪ % of intervals that achieve the target service level
▪ Total wait time/ Total number of answered calls
▪ Abandoned rate ▪ Abandoned rate after the
IVR
▪ Abandoned rate during
the IVR
▪ Calls dropped after it reaches an CSR/Calls offered
▪ Calls dropped during IVR, before it reaches an CSR (excluding self-
serve calls)/Calls offered

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
106
EXHIBIT 57: EXAMPLE PARTICIPANT ENROLLMENT AND CLAIMS PROCESSING KPIS
5. Within the participant enrollment flow, integrate mailer and correspondence process
with FSD: The state could implement process change to integrate correspondence of
premium notices with FSD eligibility notices to drive improved response rate. This could
require a simple process change to implement the inclusion of the first premium notice in the
same envelope as the eligibility notice. This may significantly reduce non-responses to
premium notices.
6. Improve medical record matching to reduce incorrect denials in participant
enrollment: Matching medical records to appropriate claims to minimize inaccurate denials
could drive significant improvement in enrollment accuracy and reduce downstream rework.
7. Improve accumulator accuracy to help manage spend down errors: Spend down
inaccuracy drives significant billing errors and inbound inquiries. The state could consider
setting up a team to minimize spend down on out of sync scenarios, which could help
minimize errors.
8. Assess prior authorization (PA) list for high pass rate codes and optimize through
quarterly refreshes: State staff could conduct analysis to identify drivers of manual PAs
and ensure quarterly list refreshes. This could minimize manual PAs for high pass rate
codes.
9. Redesign root-cause drivers (e.g., participant communication & notification) to
reduce call volume to contact centers: The state could institute ongoing processes to
Participant
enrollment
Claims
Payor value
chain function
Metric subcategory
Average enrollment processing days
Enrollment accuracy
Specific metric
ID cards ▪ Percent of participants that received cards before effective date
Summary metrics ▪ Enrollment cost per total transaction
▪ Total enrollment transactions per FTE per year
▪ Total automated electronic transactions as a % of total member
transactions
Billing ▪ Total number of bills sent per participant
Claims type rates ▪ Total suspension rate
▪ Total claims auto-adjudication rate
▪ Total adjustment rate
▪ Denied claims rate
Speed of processing ▪ Average payment period in days
▪ Average inventory in days
Percent of claims processed within
the following days of receipts
▪ 0-14 days
▪ 15-30 days
▪ 31-60 days
▪ > 60 days
Timing of claims ▪ Claims turnaround time (TAT)
Summary metrics ▪ Suspended (manual) claims processed per FTE per year
▪ Cost per suspended (manual claim)
▪ Claims processed per claims FTE per year
▪ Cost per claims processed
Quality ▪ Dollar accuracy percent
▪ Frequency accuracy percent
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
107
address root-cause drivers currently leading to increased call volumes. There are several
near-term initiatives that could lead to the reduction of call volume. For example, the state
could consider redesigning forms and letters to guide to digital channels and highlight
additional communication resources available. This communication could provide clear and
updated guidelines on when to call the contact center after application submission. In the
case of interviews, the state could consider asking the applicants to wait 24 hours to allow
for the appropriate processing time before calling.
10. Revise policy guidance on MAGI helpdesk to avoid rework: The state could review
internal policies that currently prohibit outsourced MAGI helpdesk agents from completing
case updates in situations when a change of coverage occurs (currently, these changes
must be completed by an internal agent). Also, the state could consider updating policies to
enable MHD staff members to transfer to Wipro, when applicable, to reduce downstream
rework in internal case processing team.
Potential automation and digitization process optimization initiatives
11. Implement macros and automation to replace repetitive manual tasks: The state could
identify repetitive manual tasks and build simple macros/automation to reduce manual
intervention. Batch enrollment corrects or incarcerated participants disenrollment could be
executed automatically, for example. Implementation would require both macro
development and inbound data manipulation. Creating macros or process automation
routines that utilize database queries and pre-set algorithms to perform defined tasks such
as participant information updates or error reconciliation could significantly reduce the
manual intervention required. Engaging vendors to identify and build use cases for
automation could drive efficiency gains: in some quick-win cases, technologies like optical
character recognition (OCR) could be implemented within 6 to 12 months, while more
complex implementations (e.g., machine learning to improve auto adjudication rates) could
take 12 to 24 months.
12. Improving upstream systems to help reduce manual rework: Erroneous information
feeds drive significant rework within MHD processes. Engaging FSD leadership to drive
changes in these upstream systems (especially MEDES) could significantly reduce rework
within participant enrollment function. Improved data formats (e.g., pipe-delimited flat files
rather than email-based information) could provide basis for rapid system updates,
eliminating manual processes.
13. The state could engage inbound data stream owners to align on data feed formats:
Currently, data from various other state agencies is primarily received via email. Convening
leaders to align on unified and simple data exchange formats (some best-in-class payors
use pipe-delimited files) could allow for easy and automated intake into ITSD systems. This
could reduce manual workarounds and potential for error.
14. Invest in improvement of auto adjudication rates: The state could conduct detailed
analysis to assess current drivers of manual adjudication – such as edits, medical policies,
system issues – and inbound data issues, in addition to implementing improvements in the
claims systems to improve auto-adjudication rates. For example, the state could consider
identifying top edits that trigger manual adjudication and determining modifications to edits
that could drive claims to be auto-adjudicated. For example, if an edit requires an
assessment of a particular attachment or medical record and it is found that such claims are
paid with a high pass rate, removing that requirement could eliminate need for manual
intervention.

Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
108
15. Implement issue and project tracking system: Currently, issue and request management
is done through email. The state could consider transitioning to a ticket-based management
system that provides real time tracking, escalation paths and pan-organizational
transparency.
16. Build digital participant engagement platform: Transitioning traditional communication
channels to a digital medium for high-impact communications such as premium notices
(e.g., e-pay functions), ID cards, or explanation of benefits (EOB) delivery could drive
improved participant engagement. The state could consider investing to get ahead of
developing participant digital preference trends and drive adoption for new enrollees over a
five-year horizon.
224
Some of these participant engagement practices could help promote
self-service and reduce call volumes for the contact center and save on costs incurred due
to existing communication using traditional channels, such as printed ID cards and EOBs.
Given the proliferation of different modes of communication, it could also be helpful to
note/flag the preferred method of communication during the enrollment process.
17. Provide self-service options for Tier 1 calls to reduce live calls and wait times: The
state could consider investing in new self-service channels for the resolution of simple
issues like status of cases or food stamp eligibility through alternative channels to reduce
call volume by ~15% to 20% in Tier 1. This could ease the load and reduce the current peak
wait time for 60 minutes significantly. The state could consider potential quick wins like
website-based self-service options and SMS-based notifications and bots to provide quick
answers to simple requirement questions. Likewise, chatbots in the website could potentially
answer queries on case status and document uploads (e.g., an AI-based chat service with
limited human intervention).
Sourcing optimization initiatives
18. Evaluate engaging additional vendors: The state could consider engaging a vendor for
improved participant address management. Significant correspondence challenges stem
from dead or out-of-date addresses. Engaging vendors to conduct address reconciliation
and quality improvement is a best-in-class payor practice and can help better engage
participants. Ensuring mail is sent to correct participant addresses could also drive cost
savings by reducing rework and through postage and printing cost reduction.
In addition, the state could consider engaging vendors to maximize value added work
performed by the department’s participant enrollment team. MHD could consider the
potential to outsource enrollment correction processes and assess the current reliance on
participant enrollment team to solve routine and complex enrollment issues.
19. Define future operating model for state contact centers to balance in-house vs
outsourcing options: As part of future review of the state’s contact center operation, the
state could consider three options for future operating model for contact centers:
• Focus on operations excellence and operate contact centers internally with only
strategic outsourced vendor partners as required
• Focus on contract excellence and move to a primarily outsourced model with retention
or strategic contact center operations in-house
224
McKinsey, “Healthcare’s digital future,” 2014, see: www.mckinsey.com/industries/healthcare-systems-and-
services/our-insights/healthcares-digital-future.
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
109
• Continue blended operating model with focus on operations excellence with internal
center and focus on contract excellence for outsourced operations with adequate
resources to manage in-house operations and outsourced operations
All options could facilitate providing best-in-class contact center services to participants
and providers. In the first two options, the state could choose to dedicate its resources to
focus on either on operational excellence or contract excellence; in a blended model, the
state would likely need to ensure that appropriate resources are dedicated to each area
against a shared resourcing model with dual focus. To determine the best fit option for the
long term, the state could evaluate each of these options in view of cost, quality of service,
strategic fit, administrative priorities, and operational agility to determine the best choice
going forward.
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
110
Implementation Considerations
Without significant changes, Medicaid spending may comprise 26% to 30% of state general
revenues by 2023. To bring growth of Medicaid spending in line with the level of economic
growth of the state while preserving access for participants and avoid reducing eligibility or
coverage, significant savings would be necessary. In the preceding pages, eight programmatic
and functional areas were analyzed, and descriptions of the current state, potential opportunities
for improvement, and potential initiatives were provided.
Were Missouri to fully and effectively address the opportunities and potential initiatives outlined
in this report, total gross savings to the program (including federal and state share) could total
up to $0.5 billion to $1.0 billion by SFY2023 (net of potential reinvestments in the delivery
system and in the Medicaid program’s operations). These potential savings are not meant to
represent an absolute reduction in Medicaid program spending but rather a meaningful
reduction in the growth rate of the program to bring it in line with economic growth of the state.
In addition, many initiatives focus on reducing cost growth through improving participant
outcomes and experience. Adopting such a transformation agenda could make the program
more financially sustainable and reduce fiscal pressure that may arise in the event of a
recession or changes in federal financing.
Potential initiatives are wide-ranging, including operational improvements to bring the program
up to date with common practices among other state Medicaid programs, as well as
implementing best practices and more transformational changes. The following entails some of
the choices the state may consider in selecting the portfolio of initiatives that will comprise
Missouri’s approach to Medicaid transformation. Also outlined below is a summary of the key
requirements for implementation.
Approach to Portfolio Selection
Broadly, the state could balance two approaches to controlling spending. One approach
commonly adopted by both public programs and managed care would rely primarily on
controlling the unit prices paid for services and seeking to curb utilization through payor
decisions regarding clinical necessity. This approach could reduce costs and drive efficiency
across provider types, readily realizes savings, with limited associated technical complexity. Yet
this approach may lead to provider resistance and does not provide an incentive to improve
patient outcomes. Finally, mainly focusing on rates and volume would likely be only a temporary
solution: as one of the root causes of the problem – the underlying FFS payment mechanism –
would not be addressed, fragmentation and growth of volume may continue to exist, potentially
leading to the need for further rounds of budgetary tightening.
In the second approach, the state would seek to adopt innovative value-based payment and
care delivery models that reward providers for quality and efficiency of the total care delivered to
patients. This approach may support more transformational changes in care delivery, with
corresponding improvements in patient outcomes and experience. A key focus would be
reducing costs through improved outcomes for participants: strengthening primary care,
integrating behavioral and physical care, emphasizing independent living at home (with
community support where needed), and addressing social determinants of health. This
approach would pay for the outcomes that matter to participants rather than volume and would
stimulate the transparency of provider performance. The approach is likely to require greater
commitment of resources and longer to generate impact, given the need for providers to adopt
not only the new payment models but also to adopt new capabilities and implement changes in
clinical practices.
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
111
To align the growth of Medicaid expenditures with the state’s economic growth could require a
combination of these approaches, balancing and prioritizing shorter- with longer-term needs and
strategic goals. Regardless of the balance chosen, there is a range of “no regret,” operational
initiatives that the state may consider bringing policies and operations up to speed with common
practices, including state-of-the-art fraud, waste, and abuse (FWA) as well as third-party liability
(TPL) methodologies, targeted use of utilization management, as well as improvements in
contact centers and other internal administrative processes. Adoption of common and leading
practices in these areas will address outlier practice patterns and inefficiencies, generate near-
term savings, improve customer experience, increase workforce satisfaction and reduce
pressure on the rest of the system while longer-term, more transformational changes are being
implemented.
Any substantial portfolio of initiatives would demand careful planning and execution, and
investments to support the transformation and build new capabilities. Key requirements for
effective design and implementation of Medicaid transformation include: strong and visible
executive leadership; effective stakeholder engagement; commitment to fact-based decision
making supported by robust data; upskilling of key agency staff; a well-resourced transformation
office; and modernization of the program’s technological infrastructure.
Requirements for Implementation
Whichever approach the state adopts, any substantial portfolio of initiatives will demand careful
planning and execution, and thoughtful investments in new capabilities. Many states
underestimate the resources needed and the challenges that may be encountered in the
implementation process.
The assessment of the state’s Medicaid program revealed that the Departments responsible for
the Medicaid program are aware of many of the opportunities identified and would embrace an
ambitious transformation plan. Yet both leadership and staff are also acutely aware of the
challenges the state will face in effecting changes. While there is significant institutional
knowledge that will greatly benefit the state’s efforts, few have experience with managing large-
scale transformations. In addition, many of the potential initiatives will require technical
knowledge based on experiences outside Missouri. Finally, most initiatives will require building
upon operational processes that themselves were identified as needing improvement, as well as
outdated technology and data and analytics infrastructure.
Based on our experience, key requirements for successful implementation would include strong
executive leadership, a detailed and objective fact base, and extensive stakeholder
engagement. In parallel, significant attention to upskilling key agency staff and improving
technical abilities (ranging from MMIS functionality to data and analytics to the digitization of key
operational bottlenecks) will be necessary to ensure success and sustainability of
improvements. The following briefly describes these key requirements in turn.
Strong and visible executive leadership. Successful transformation of the Medicaid
program will require active and visible leadership from the Governor’s Office, the Medicaid
Director, and other agency leaders and senior staff across DSS, DHSS, and DMH, as well as
additional support from the Office of Administration. In most states, the Medicaid Director
would be the owner of the overall transformation and regular Steering Group meetings, which
could include other agency directors/commissioners, the Medicaid CFO, and Governor’s Office
representative(s), for example. Such a steering group could lead not only through decision-
making but also through role-modeling for senior staff, creating a sense of urgency, adopting
creative solutions to problems, and communicating a compelling change story.
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
112
The planning and execution of the individual initiatives could be grouped into workstreams
which could be owned by agency leaders or senior staff (“sponsors”) responsible for the areas
impacted by the workstream. The exact configuration of this group will be highly state-specific,
but a portfolio derived from this current assessment could require sponsor roles of the
Medicaid COO, CFO, and CIO, in addition to the Managed Care Director, the Value-Based
Payment lead, and the Program Integrity lead, among others. Not allocating sufficient time to
these roles is one of the most frequent reasons for implementation failure. In other states,
sponsors will spend 20% to 30% of their time for several years per workstream. The Medicaid
Director will likely have to commit to an on-the-ground leadership role in the transformation for
the majority of his/her time.
A well-resourced transformation office. To realize the implementation of an ambitious
portfolio of initiatives, a well-resourced transformation office (TO) has proven to be essential.
The TO commonly sits outside of the normal line organization and explicitly operates with a
with a clear – and bold – mandate of the executive leadership. The function of the TO goes
well beyond the traditional Project Management Office to help the executive leadership, the
steering group, and the workstreams to achieve their goals by fulfilling several core roles:
• Drive action, help clarify goals, balance priorities and coordinate between initiatives
• Help create and execute the initiative- and workstream specific implementation plans
• Create, maintain, report on, and further develop the fact base for initiatives per workstream
• Perform advanced data and analytics functions for the workstreams
• Support the stakeholder engagement process in its different forms
• Manage resources, timelines, internal- and external meetings and realization of the targets
• Facilitate training of agency staff
To fulfill all these roles, a TO will need sufficient resources. Successful states draw on talented
agency staff as well as on subject matter experts who may bring knowledge of best practices
from other states, payors, or industries to build the TO. The TO also requires rigorous project
management and in-depth experience with all the dimensions of the change process. The TO
should be led by a full-time, sufficiently senior member of the senior leadership with
experience in change management.
Upskilling of key agency staff. The Missouri Medicaid program benefits from agency staff
who are not only committed to the performance and sustainability of the program, but who
collectively possess significant institutional knowledge. At the same time, staff and leadership
realize that the future state (and the change process needed to get there) will require
knowledge and skills that are currently absent or in short supply. Without these new
capabilities, no change efforts can hope to be sustainable.
The more ambitious the agenda, the more critical it is that Medicaid agencies develop strong,
end-to-end talent capabilities – including the ability to attract, develop, deploy, reward, and
retain top talent. Key skills and roles that would require investment (in number of individuals
and/or level of skills) are, for example:
• Project management
• Lean or other business process redesign
• Vendor contracting
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
113
• Data and analytics
• Performance management
• Outcomes transparency
• Payment innovation
• Communication
• Technical and data architects
• Data scientists / engineers
• Technical and systems operations management
• Contract management
Best practices in other states include optimally building on existing talent, investing in training
(including on-the-job), redeployment, and re-training, as well as recruitment of new leaders
and staff. As several of the initiatives address the optimization of the Department’s own
operations, staff may become available for new organizational roles.
Detailed and objective fact base. A firm footing in data is necessary to set measurable
goals, and track progress and ROI. In addition, a solid base of objective facts is the foundation
for effective decision making. The opportunities outlined in this report are based on a breadth
of research and analysis conducted over the past three months. Going forward, detailed
design and implementation of initiatives will demand an even richer fact base to
• Determine the improvement opportunities per initiative in more detail and set goals
(including financial targets, outcomes of care, customer experience);
• Analyze options for granular initiative design decisions, ranging from the clinical criteria to
be incorporated into new medical policies for utilization management; methods for adjusting
new payment models for patient risk and severity; planning internal contact center redesign;
or rebasing reimbursement rates;
• Apply risk adjustment, set target budgets, calculate shared savings/losses, quality
outcomes and bonus payments;
• Forecast and track possible impacts on provider finances from changes in reimbursement;
• Forecast and track possible impacts of relevant initiatives on rural health and the safety net
(financial, access and quality); and
• Create transparency of care costs and outcomes (value) per subpopulation, key conditions,
regions and other relevant dimensions;
Stakeholder engagement. Each of the potential initiatives discussed in this report has the
potential to affect participants, providers, and other stakeholders, placing a premium on
transparency and proactive communication. Certain initiatives – chiefly those associated with
reimbursement, value-based payment, and possible changes in the scope of managed care –
pose more significant implications for stakeholders and therefore likely demand a collaborative
process for design and implementation of changes. Without adequate stakeholder
engagement, those impacted by the planned changes are more likely to experience change as
something happening to them rather than as something that was co-shaped by them as
partners in the change process. Also, without adequate stakeholder engagement, initiatives
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
114
may fail to be adequately grounded in the reality of care delivery and payment, and the
experience of participants.
Effective stakeholder engagement will take different forms, ranging from a statewide working
group consisting of stakeholder leaders, committees focused on specific initiatives or cross-
cutting topics (“regulatory issues,” or “APM quality measures”), a clear communication plan,
interactive web-based discussion forums, informative webinars, regional stakeholder
conferences, and training opportunities.
Experience has shown that successful stakeholder engagement starts with a shared narrative
about the need for change, and a strong fact base underpinning key decisions. Clarity of goals
is essential. Subsequently, initiatives should be fleshed out and design decisions and the
implementation plan should be discussed with stakeholders. Stakeholder engagement should
continue during the implementation itself as well as during the first year(s) of rollout, and
progress toward goals should be jointly monitored. As the implementation and go-live of
initiatives always run into unforeseen issues, obstacles, and opportunities, having the ability to
jointly address these is a great benefit.
Technology
The existing MMIS poses one of the key challenges for any substantial portfolio of initiatives the
state may want to implement. Many of the initiatives will require functionalities that the current
MMIS does not offer. If the planning and implementation does not take these limitations
sufficiently into account, these initiatives may fail to achieve their intended goals. That said, the
current state of the MMIS does not have to hamper achieving ambitious goals. Functional
limitations can be addressed in three ways:
1. Limited configuration or code changes. For many of the utilization management or pharmacy
initiatives, for example, or the further modernization of hospital outpatient FFS
reimbursement, minor changes to the existing MMIS will suffice. These can be incorporated
in the initiative’s implementation plan and – after ensuring that the combination of required
MMIS changes is feasible – executed.
2. Adding new, rapidly deployable functionalities with high program but low system impact. A
cross-cutting need for the transformation process as well as the program, as a whole, is
improved access to the claims data, improvement of data quality and the analytical
capabilities needed to generate the fact base mentioned above. This ranges from the
identification of improvement opportunities, monitoring of APM spending, risk adjustment,
calculation of shared savings, creation of reports for stakeholders to the tracking program
transformation goals. Vendors that support large-scale transformation processes in
Medicaid programs tend to be able to ingest states’ data (and potentially and quickly deploy
the analytics required. In addition, using state-of-the-art, off-the-shelf technology and agile
design, high-impact digitization of key operational bottlenecks can be achieved at limited
cost.
3. Planning the initiative as dependent on the MMIS replacement process. Some functionalities
are difficult to realize without significant program and system impact. The current MMIS, for
example, cannot support DRGs or drug-level pricing for 340B drugs, which are both
potential initiatives. Although analytical capabilities to create DRGs and identify these drugs
could be rapidly deployed, these functionalities would have to go much beyond analyses:
providers would have to be paid using DRGs and different drug payment schedules, and
existing program integrity algorithms (such as claims edits) would need to be changed. Such
cases could lead the state to delay or deprioritize the initiative or opt for an alternative
Missouri Department of Social Services PREDECISIONAL
Rapid Response Review – Assessment of Missouri Medicaid Program
115
initiative to achieve the goal (in this case, help reduce inpatient spending) with less system
impact. As highlighted in the section on MMIS, the state could reassess the MMIS
replacement strategy and module requirements in the light of the prioritized initiatives, thus
simultaneously solving some of the MMIS’ key limitations and facilitating the transformation’s
success.
□ □ □
As described, the Missouri Medicaid program faces significant fiscal pressure, assuming
continuation of historically observed increases in program spending, outpacing growth with
state general revenues, with the potential for further exacerbation based on both economic
and regulatory risks. There are opportunities for Missouri to dramatically improve the
effectiveness and efficiency of the program. The potential range of initiatives as previously
outlined are ambitious in scale and scope. Addressing these opportunities and initiatives will
require a thoughtful approach to portfolio selection and investment of significant resources.
However, with sufficient leadership and commitment to long-term change, Missouri has the
potential to dramatically improve the quality and efficiency of its Medicaid program and in so
doing protect the financial sustainability of the program for future generations.
