7/2392190.7
990007-000001
- 1 -
*This article,“FHA Insured Loans for Long Term Healthcare Facilities: Recent Developments
as a Popular Product Evolves to Meet Growing Needs”, Volume 23, Number 5, first appeared
in The Health Lawyer, an ABA publication, in June 2011.
*This information or any portion thereof may not be copied or disseminated in any form or by
any means or downloaded or stored in an electronic database or retrieval system without the
express written consent of the American Bar Association.
FHA INSURED LOANS FOR LONG TERM HEALTHCARE FACILITIES: RECENT
DEVELOPMENTS AS A POPULAR PRODUCT EVOLVES TO MEET GROWING
NEEDS
Andrea C. Barach, Esq.
Wendy A. Chow, Esq.
1
Bradley Arant Boult Cummings LLP, Nashville, TN
I. Introduction
The “Great Recession” continues, and the commercial financial markets remain difficult
for many borrowers. In this environment, healthcare providers have continuing challenges as
they seek financing for their facilities. The financing market can be expected to continue
difficult into 2011 and perhaps beyond. For owners of long term care facilities, one bright spot
in the financing world has been mortgage financing insured by the Federal Housing
Administration (“FHA”) under Section 232 of the National Housing Act.
2
After all, what is not
to like - long terms (35-40 years), low fixed rates, no personal recourse and no required
guaranties by high-income individuals. Even better, these loans are assumable by qualified
purchasers. Of course, nothing in life is free, and in order to enjoy these benefits, borrowers
must comply with a host of specific substantive and procedural requirements.
Within the past year,
3
the volume of Section 232 mortgage loans has grown dramatically,
and new concerns have arisen, particularly from the novel “master lease” structure for portfolio
loans, and further refinements to the treatment of accounts receivable financing.
The U.S. Department of Housing and Urban Development (“HUD”) developed and
adopted the Lean Processing program in 2008 and phased in its use during 2009. Initially, the
program began under the Office of Insured Health Care Facilities (“OIHCF”) and was processed
1
The authors gratefully acknowledge the assistance of Mr. Alex Fenner and Ms. Amanda Nichols who contributed
valuable research.
2
24 C.F.R. § 232 (2009). The National Housing Act of 1934 was adopted as part of President Roosevelt’s “New
Deal” in order to promote stability in the nation’s housing market by making mortgage credit more available to
homeowners by establishing a program of insuring mortgages made by private lenders.
3
Andrea C. Barach & Wendy A. Chow. Government Insured Financing Available for Healthcare Facilities—We’re
From the Government and We’re Here to Help—Really!, 13 Q
UINNIPIAC HEALTH L.J. 203 (2010).
7/2392190.7
990007-000001
- 2 -
out of the Seattle Multifamily Hub Office.
4
Since its adoption, and due to the increased volume
of applications, OIHCF, now known as Office of Healthcare Programs (“OHP”), has been
working to further centralize and standardize the program in order to focus more attention on the
creditworthiness of the borrower and the principals of the borrower. OHP is working toward
further standardization and modernization of the forms to be used, as well.
5
At the time of adoption, the HUD Health Systems Advisor, William Lammers, predicted
with great enthusiasm that it would become possible to close a Section 232 loan in just 30 days
from the date the application was submitted.
6
However, due to the unexpected and
unprecedented increase in application volume, despite the streamlining efforts, the processing
times have remained discouragingly long, and the average time a project application remains in
the queue has risen from four to five months to between eight to ten months.
7
With the current
economic downturn, borrowers have been turning away from the commercial financing market
and towards these insured loans in ever increasing numbers. Further increasing the volume of
applications has been the trend for larger for-profit providers to finance (or refinance) large
portfolios of projects in recent years.
8
The overwhelming success of the Lean program, and its vastly increased volume of
applications, has caused HUD to re-examine and revise some of its procedures and program
rules. This article will summarize the major provisions of these Section 232 loans and examine
some of the recent changes applicable to these popular programs for healthcare owners.
II. FHA Insured Loans For Long Term Healthcare Facilities – A Refresher on Section
232
A. Lenders and Loan Insurance Under Section 232
Section 232 of the National Housing Act
9
establishes the insured mortgage loan programs
available to owners of long term healthcare facilities, such as nursing homes, assisted living
4
U.S. Dep’t of Housing & Urban Dev., Off. of Housing, 232/223(f) LEAN Processing Training- for Lenders (2008).
5
Federal Housing Administration, HUD 2010 Annual Management Report (November 2010),
http://www.hud.gov/offices/hsg/fhafy10annualmanagementreport.pdf
(hereinafter “HUD 2010 Annual Management
Report).
6
William Lammers, Health Sys. Advisor, Office of Insured Health Care Facilities, ELA March 2007 Conference on
Financing American Hospitals Today, Section 242: Mortgage Insurance for Hospitals Overview (2007),
http://portal.hud.gov/fha/healthcare/materials/ela.pdf (hereinafter Lammers’ Presentation).
7
U.S. Department of Housing and Urban Development, HUD LEAN 232 Program Update as of November 2, 2010,
(Nov. 02, 2010), http://portal.hud.gov/hudportal/documents/huddoc?id=FHA_DOC_195.pdf.
8
In 2001 a 75 facility portfolio was approved by HUD, but there were relatively few large portfolios until fairly
recently. For example, an August 2010 closing of a 16 facility portfolio was the largest closed since 2005. Since
then, the authors are aware of several other large portfolios in the processing queue. HUD Approves Largest health-
Care Package for CFG, Inc. (Commercial), A
LLBUSINESS NEWSLETTER at 1 (June 1, 2002).; Press Release, Walker
& Dunlop, Walker & Dunlop Closes Larges HUD Healthcare Portfolio Since 2005 – Florida (August 24, 2010) on
file with author.
9
24 C.F.R. § 232 (2009).
7/2392190.7
990007-000001
- 3 -
facilities, board and care homes and certain other forms of intermediate care facilities. It does
not include acute care hospitals, as these facilities may be financed under programs authorized
under Section 242 of the National Housing Act
10
(which is beyond the scope of this article.)
All of the loans under Section 232 are made by one of the 92 private lenders currently
qualified as FHA lenders under the Multifamily Accelerated Processing Program.
11
After the
FHA lender underwrites and closes the loan in accordance with HUD procedures, the loan is
“endorsed” to HUD under the specific Section 232 program and the FHA insures the mortgage
loan. If the mortgage loan goes into default, the FHA lender can assign the loan documents to
HUD in return for HUD's payment of the insurance claim.
12
In general, FHA lenders may securitize the closed loans into pools of one or more
mortgage loans which are packaged and sold to investors as Government National Mortgage
Association (“GNMA”) Mortgage Backed Securities (or, more colloquially, “Ginnie Maes”).
Under the Ginnie Mae program, upon payment of a fee to GNMA and in reliance on and addition
to the FHA mortgage insurance, GNMA guaranties to the investors the timely payment of
principal and interest on the securities. Because investors will be purchasing the Ginnie Maes
and will want some assurance of the expected yields, the lender will provide for a period during
which prepayment is prohibited (so that the investor’s yield is guaranteed for a certain time
period) and thereafter prepayment is permitted but may carry a premium
13
. Using GNMA
multifamily mortgage backed securities allows an increased supply of mortgage credit because
funds from the capital markets are channeled into the mortgage market, and since GNMA
guaranties are backed by the full faith and credit guarantee of the U.S. Government,
14
the Ginnie
10
24 C.F.R. § 242 (2009).
11
HUD 2010 Annual Management Report, supra note 5, at pages 23-24. Lenders qualify as FHA lenders by
applying to HUD and demonstrating ability to meet HUD underwriting requirements, including successful
completion of required training programs offered by HUD.
12
It is interesting to note that § 232 loans were expressly excluded from the mortgages eligible for Partial Payment
of Claims (“PPC”). Although there is no explanation as to their exclusion, it is reasonable to assume that § 232
loans were not viewed as presenting the same risks as loans under other FHA programs. The PPC program allows
HUD to pay a portion of the unpaid principal balance to the lender and recast the remaining balance into a revised,
smaller loan that reflects a financially viable debt load for the property, with a new second priority mortgage in
favor of HUD securing the amount of the partial insurance payment. See, U.S. Department of Housing and Urban
Development, HUD Asset Management Handbook Chapter 14: Partial Payment of Claims (November 2010),
http://www.hud.gov/offices/adm/hudclips/handbooks/hsgh/4350.1/43501c14HSGH.pdf.
13
For example, a 35 year mortgage loan could be closed to prepayment for the first ten years, then starting in the
eleventh year prepayment would be permitted with a 3% premium, in the twelfth year with a 2% premium, in the
thirteenth year with a 1% premium and may be prepaid at par starting in the fourteenth year. Often the prepayment
prohibition may extend for a shorter period, with higher premiums once the loan is open to prepayment. A borrower
can negotiate these terms with its lender, but different prepayment terms will affect the interest rate charged by the
lender.
14
Mortgage Bankers Association, The Future of FHA and Ginnie Mae, (September 2010),
http://www.mbaa.org/files/ResourceCenter/FHA/TheFutureofFHAandGinnieMae.pdf
. See also Arthur Q. Frank &
James M. Manzi, GNMA Multifamily Research (May 1, 2003); Federal Reserve Bank of San Francisco, Ginnie Mae
(footnote continued on following page …)
7/2392190.7
990007-000001
- 4 -
Mae securities are more attractive to investors, which in turn results in lower interest rates. As
an alternative to the Ginnie Mae, the lender may obtain an FHA-insured pass-through
participation certificate, which offers slightly less default protection (generally 99 percent of
principal and interest at the FHA debenture rate), but this has been less popular in recent years
since the GNMA fee was reduced.
15
B. Specific Programs within Section 232
The following is a summary of the different programs available to owners of healthcare
facilities under Section 232:
16
1. Section 232
: Financing for the acquisition or construction of an eligible
healthcare project, or substantial rehabilitation of an eligible healthcare project. Substantial
rehabilitation means either (i) the cost of repairs, replacements or improvements exceeds the
greater of 15 percent of the estimated replacement cost (after completion) or (for assisted living
facilities $6,500 per unit), or (ii) two or more major building components are being substantially
replaced.
17
2. Section 232/223(f): Financing to refinance an existing mortgage
(conventional or FHA) on an eligible healthcare project that the borrower has owned (generally
for a minimum of two years). Rehabilitation costs may be included, so long as they do not
constitute “substantial rehabilitation” as in that case it would be a Section 232 loan, not a Section
232/223(f) loan.
18
3. Section 232/223(a)(7): Refinancing of an existing mortgage that has been
insured by FHA. Like the 223(f) loans, the lenders are able to use GNMA Mortgage Backed
Securities.
C. Economics of the Loan Terms.
All of the Section 232 loans are fixed interest rate loans with terms ranging between 35-
40 years.
19
The term may be shortened if three-quarters of the remaining useful life of the
(… footnote continued from previous page)
Project Loans Maintain Affordability (August, 2003),
http://www.frbsf.org/publications/community/investments/0308/article2b.html.
15
GNMA Multifamily Research, supra note 14.
16
24 CFR §§ 200(A), 242 (2010); U.S. DEPARTMENT OF URBAN HOUSING, PROGRAMS OF HUD, available at
http://www.huduser.org/resources/hudprgs/ProgOfHUD06.pdf.
17
Guide to Multifamily Accelerated Processing (MAP), CH. 3: Eligible Multifamily Mortgage Insurance Programs
§§ 4(C)(1),(2) (2002), http://www.hud.gov/offices/hsg/mfh/map/mapguide/chap03.pdf (March 15, 2002)
(hereinafter MAP GUIDE). A “unit” in an assisted living facility is a separate residential living unit for not more
than four persons per unit or per bathroom. Nursing facilities have beds rather than units, so the cost per unit is not
used for those projects.
18
Id.
19
MAP GUIDE, supra note 17, ch.3 §§ 2 (D), (E).
7/2392190.7
990007-000001
- 5 -
facility is a shorter period.
20
In most cases, the loans may be nonrecourse to the borrower,
meaning that enforcement in the event of default is limited to enforcing on the collateral, which
will be a first priority mortgage on the facility and the assets associated with the facility. As
discussed later in this article, the structures used for these loans can be quite complicated, since
the facilities are commonly subject to an operating lease, and also often have obtained working
capital financing through a pledge of accounts receivable.
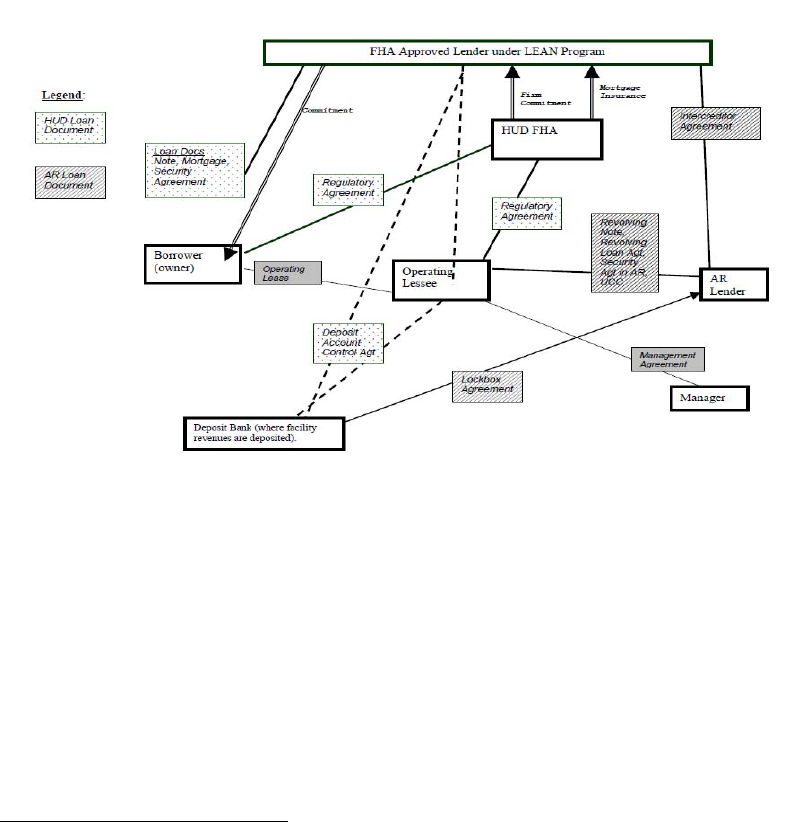
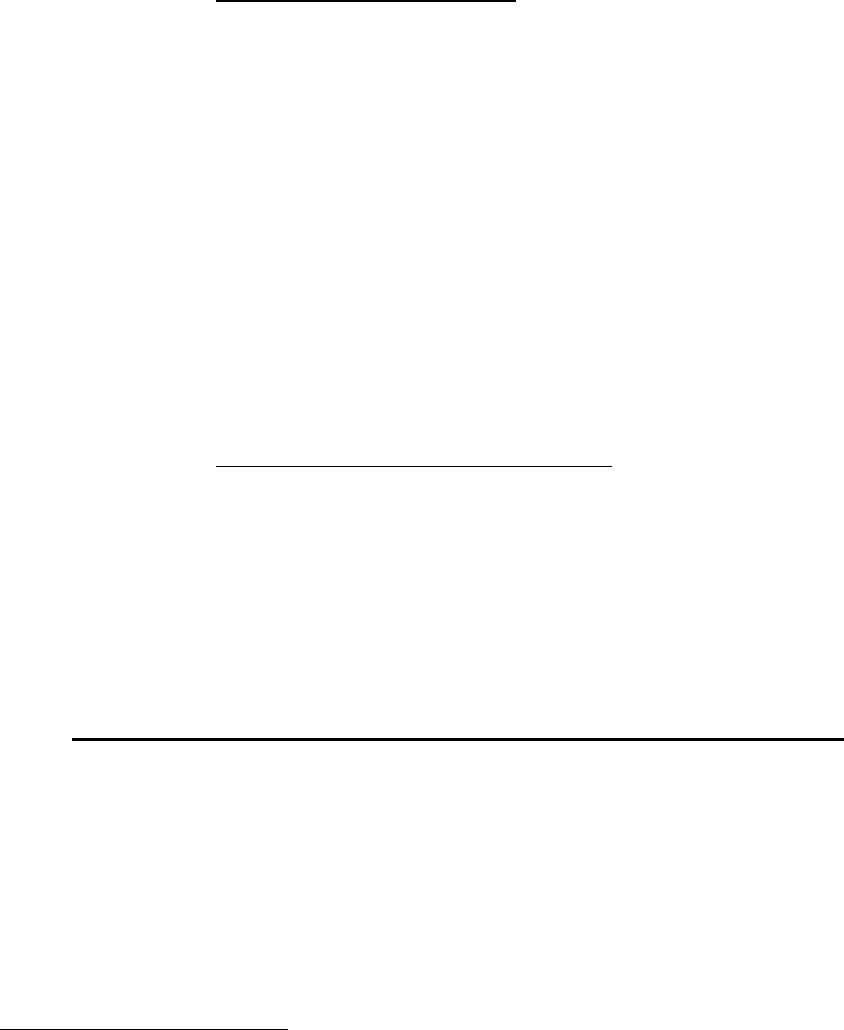
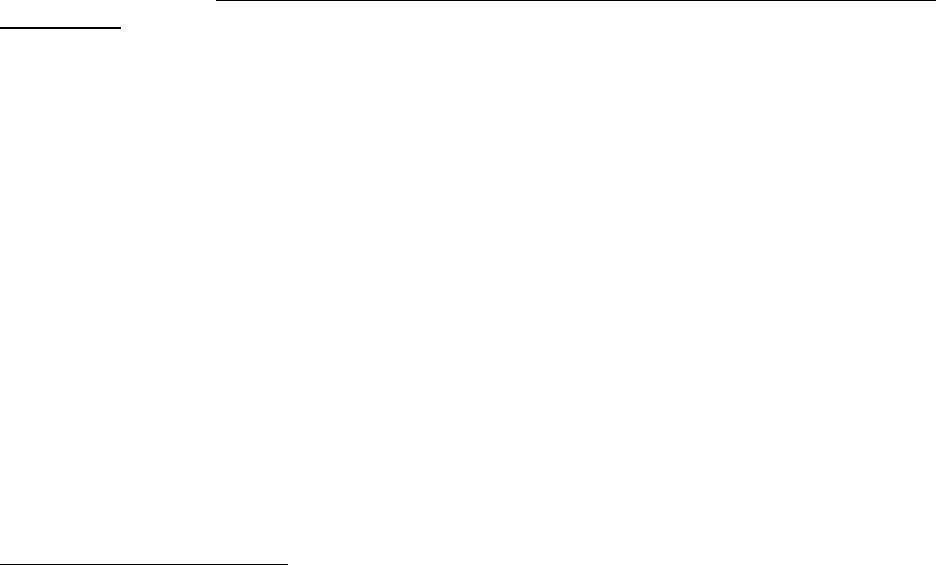
Figure 1 is a chart showing a typical structure for a Section 232 loan, including accounts
receivable financing, and shows that the structure can be quite complicated.
Figure 1.
D. Eligible Projects
Skilled nursing facilities, intermediate care facilities, board and care homes, and assisted
living facilities are “eligible projects” under Section 232.
21
In general, these facilities serve an
elderly and frail population who require some level of continuous healthcare or assistance
services, but the definition is broad enough to also include other intermediate care facilities such
as behavioral healthcare residential treatment facilities or psychiatric hospitals providing
residential care (as opposed to acute care) so long as the services are residential and are provided
under state license.
22
Eligible projects must be operated under a state license, except that in
certain states that do not license assisted living facilities, the requirement for a state license may
20
Id.
21
24 CFR § 200.3 (2010).
22
MAP GUIDE, supra note 17, ch.3 § 9 (A)(2).
7/2392190.7
990007-000001
- 6 -
be waived. In the underwriting process, if a certificate of need is required in the state in which
the facility is located, it must be submitted to the lender. If no certificate of need is required by
the state, then the underwriter will require some sort of market study in order to establish that
there is a demonstrated need for the services being provided by the facility. In addition, since
many facilities include both licensed and unlicensed (independent living) units, Section 232
loans may include facilities containing unlicensed independent living so long as the independent
living beds do not exceed 25 percent of the total beds in the facility.
23
E. Eligible Borrowers
To qualify for a Section 232 loan, a borrower must be a single asset, single purpose
entity.
24
It may be organized as a non-profit entity or a profit-motivated entity
25
, but in either
event, it may only own the single asset which is the subject matter of the Section 232 loan and its
organizational documents must limit its purposes to the ownership and operation of the single
asset.
1. Nonprofit vs. Profit-motivated Borrowers. Both nonprofit and profit
motivated entities may apply for FHA insured financing of eligible projects. Nonprofit
borrowers are entitled to higher maximum loan amounts than borrowers which are profit
motivated. This reflects the underlying assumption that a nonprofit borrower is not distributing
"profits" or surplus revenues from the facility to financially enrich its owners. If a loan is
underwritten on a nonprofit basis, the loan documents will restrict the borrower's ability to use
residual receipts remaining after payment of operating expenses and debt service for any
expenses other than repairs, improvements or enhancements to the project. For some nonprofit
borrowers which are part of larger organizations, this can prove problematic. The nonprofit
borrower may desire to use cash on hand in one facility to assist another facility within the same
nonprofit group of entities, but may not do so if the facility has been financed with a Section 232
loan as a nonprofit.
2. Leased Projects. Under Section 232, an eligible project may be leased to
an operating lessee so long as both the lease and the operating lessee are approved by HUD. The
operating lessee will hold the license from the state, be responsible for the day-to-day operation
of the facility, and receive payments for services to the patients or residents of the facility in due
course. The operating lessee may be affiliated with the mortgagor owner, or it may be an
unrelated third party, although it is quite common for the owner which obtains the Section 232
financing to lease the facility to an affiliated operating lessee for a rental amount equal to the
debt service plus real estate taxes as well as insurance and a small reserve. Operating leases
must comply with HUD requirements, including a requirement that the operating lease may not
23
MAP GUIDE, supra note 17, ch.3 § 9.
24
MAP GUIDE, supra note 17, ch.3 §2(B).
25
The term “profit-motivated” rather than “nonprofit” refers to the fact that a nonprofit facility owner may elect to
be considered as a “profit-motivated” borrower rather than being underwritten as a nonprofit borrower and being
subject to more restrictions on distribution.

7/2392190.7
990007-000001
- 7 -
be assigned without HUD prior approval, any change in bed authority requires HUD consent,
and nonprofits may only lease to other nonprofits.
26
Planning Point: Because operating lessees are not required to be single purpose, single
asset entities, sometimes several facilities may be leased to the same operating lessee. If a
facility owner owns more than one facility in the same entity and desires to refinance using
Section 232 mortgage loans, one way to meet the requirements under the Section 232 program is
to form new entities to hold each of the facilities and then have the new entities lease each
facility to the original owner, which will now be the operating lessee for all of the facilities that it
once owned outright. Depending on the state laws concerning healthcare licenses, this process
may not require full re-licensure of each of the facilities and thus may be very attractive for
certain borrowers.
3. Managed Projects. An eligible project may be managed by a management
agent (either affiliated or independent) under a separate management agreement. All agreements
must permit HUD to require the owner to terminate the management agreement (i) immediately
in the event of a default under the loan documents attributable to the management agent (ii) upon
30 days written notice for failure to comply with the provisions of the management certification;
or (iii) when HUD becomes mortgagee in possession after the loan has been endorsed to HUD by
the lender.
27
Upon any such termination, the management agent must turn over all the project’s
accounts, investments and records to the owner immediately (but in any event within 30 days),
and the owner must agree to make arrangements for acceptable alternative management of the
project. One requirement that can be troublesome in certain instances is the requirement that
there not be any “hold harmless” clause that excuses the manager from all liability for damages
and injuries.
28
4. Previous Participation Clearance – Who Must Be Disclosed? All entities
and principals of entities that expect to be a borrower, operating lessee, or manager of an eligible
project must be cleared in a process which verifies that each such entity (or its owners, directors
or officers) have not participated in other FHA insured financing which is in default.
29
In
general, the “principals” required to submit Previous Participation Certificates (also known as
HUD-2530 Forms) are, in addition to the entity itself, (i) the entity’s executive officers (defined
as the President, Vice President, Secretary, Treasurer and any other executive officers who are
directly responsible to the Board of Directors or equivalent governing board); (ii) any of its
general partners (with any ownership interest) for entities that are partnerships; (iii) for entities
that are limited partnerships, limited partners with 25 percent or more ownership interest; or (iv)
stockholders of any entity which is a corporation or LLC members for any entity which is a
limited liability company with, in either case, 10 percent or more ownership interest.
30
HUD
26
MAP GUIDE, supra note 17, ch.3 § 9(G).
27
MAP GUIDE, supra note 17, ch.10 § 6(A).
28
Id.
29
MAP GUIDE, supra note 17, ch.10 § 6.
30
MAP GUIDE, supra note 17, ch.10 § 8.3(D); See also 24 CFR § 200.215(e)(2) (2010).

7/2392190.7
990007-000001
- 8 -
strongly encourages the submission to be made using its APPS online electronic submission
format which requires obtaining enrollment credentials from HUD.
5. Regulatory Agreement. All FHA-insured loans require the borrower and
any operating lessee, and sometimes the management agent, to sign a Regulatory Agreement.
31
The Regulatory Agreement provides, in general, that the project may be used only for the
specific use stated, that the borrower must be a single asset entity, and that there may be no
discrimination in the services provided to the residents or patients. In addition, the Regulatory
Agreement provides that there must be reserves for replacement, establishes required record
keeping and accounting procedures, and provides that any transfer of the project requires the
prior consent of HUD. The Regulatory Agreement is executed by the project owner (or lessee,
as the case may be) and HUD. Any violation or event of default under the Regulatory
Agreement entitles HUD to take over the note and mortgage documents and, eventually,
foreclose on the project. The Regulatory Agreement is placed of record immediately after the
mortgage is recorded. The Regulatory Agreement will contain limitations on the use of residual
receipts (for nonprofit borrowers) or surplus funds (for profit-motivated borrowers). Nonprofit
borrowers, in particular, will be forbidden to use residual receipts for any purposes (even
purposes otherwise within the charitable purpose of the nonprofit) other than specific project
needs, without the prior consent of HUD.
F. Eligible Costs – No Equity Take-Out
The principal amount of any Section 232 loan will be limited to the total amount of
eligible costs. This is very important, because no return of equity is permitted from the proceeds
of a Section 232 loan.
32
Thus, if an owner of a facility has built up substantial equity in the
facility (which may occur if there has been substantial amortization over a number of years under
the facility's existing financing, or may occur as the result of increases in market value overall),
the Section 232 loan will be limited in amount to the proceeds necessary to repay the prior loan
and pay approved closing costs. Some lenders will make a "bridge" loan to a facility, which will
have a term of one to two years. In the initial bridge loan closing, if there is sufficient value to
support a larger loan the borrower can receive a return of equity, and then, when the bridge loan
is refinanced with a Section 232 loan, there would not be any return of equity. The period of
time between the closing of the bridge loan and its eligibility to be refinanced under Section 232
is sometimes referred to as the "seasoning period," and there are detailed requirements
concerning the length of time that a loan must be "seasoned" and the nature of debt which may
be refinanced with the proceeds of a Section 232 loan.
33
Affiliate debt, consisting of loans made
by an affiliate of the borrower to the borrower, may not be refinanced with the proceeds of a
Section 232 loan in any event. In addition, the debt that may be refinanced must be directly
31
MAP GUIDE, supra note 17, ch.3 § 2(A).
32
MAP GUIDE, supra note 17, ch.3 § 11(J).
33
U.S. Department of Housing & Urban Dev., Office of Housing, 232/223(f) LEAN Processing Training for
Lenders (2008).
7/2392190.7
990007-000001
- 9 -
related to the project, such as purchase, construction, capital improvements, working capital
associated with the project, and similar project-related expenses.
34
G. Maximum Loan Amount
The statutory maximum loan amounts range from 85 percent to 95 percent of the
appraised value of the project, subject to other limiting factors. Recently, the limits have been
reduced to reflect negative market experience in an effort to reduce future loan defaults. Under
the recent reductions, the loans will range from 75 percent to 90 percent of appraised value.
Even with the revised, lower limits, it is clear that Section 232 loans remain a very attractive
financing alternative for many long-term care facilities. The HUD underwriter will determine
the maximum loan amount in the application process. There are three criteria which will limit
the maximum amount of the loan. The test which results in the lowest amount will set the
maximum loan amount.
1. Appraisal Criterion. In the underwriting, an appraisal of the facility will
establish an appraised value. Based upon the type of facility and the type of borrower, skilled
nursing, assisted living, for profit or not-for-profit, the maximum loan amount under this test will
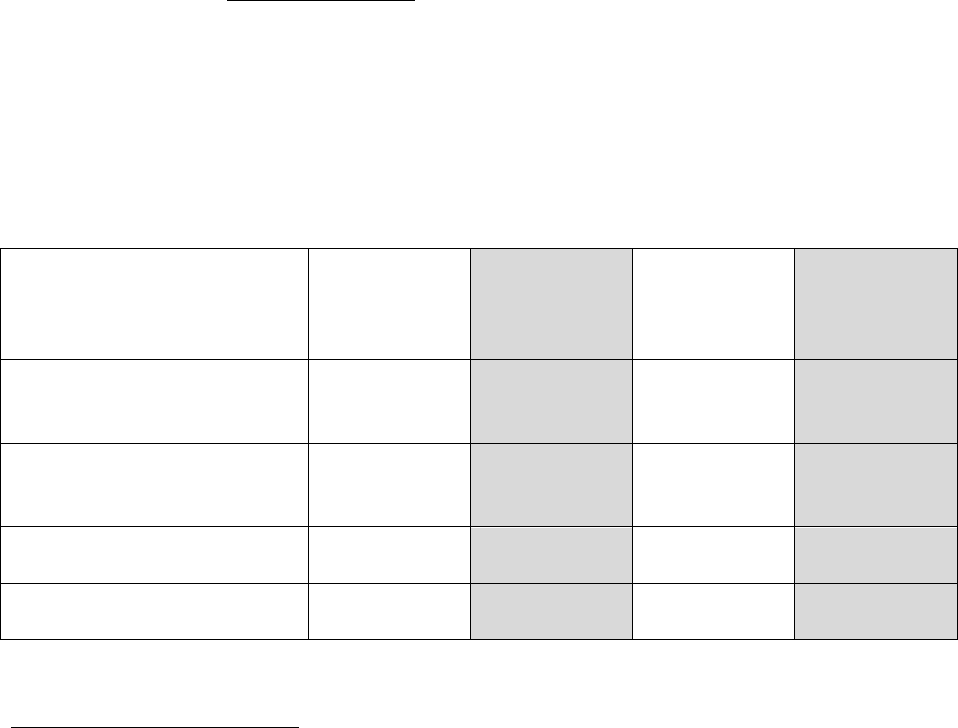
be between 75 percent and 90 percent of the appraised value. As seen in this table, HUD has
lowered the maximum amount of the loans across the board.
35
In addition, due to negative
experience in the assisted living segment of long-term care, HUD has further reduced the
maximum loan amounts for assisted living facilities. These reductions are not statutory, and in
certain cases it may be possible to apply for a loan in excess of these limits if there are suitable
mitigating factors.
Type of Entity Loan
Skilled
Nursing –
Revised
Guidelines
Skilled
Nursing
(statutory
limits)
Assisted
Living-
Revised
Guidelines
Assisted
Living
(statutory
limits)
New construction or
substantial rehab - for profit
borrowers
80 percent 90 percent 75 percent 90 percent
New construction or
substantial rehab – nonprofit
borrowers
85 percent 95 percent 80 percent 95 percent
Refinance or acquisition - for
profit borrowers
80 percent 85 percent 80 percent 85 percent
Refinance or acquisition –
nonprofit borrowers
85 percent 90 percent 85 percent 90 percent
34
Id.
35
U.S. Dep’t of Housing & Urban Dev., HUD’s LEAN 232 Program Office of Insured Health Care Facilities
(OIHCF): Update as of February 19, 2010.
7/2392190.7
990007-000001
- 10 -
This test is fairly easy to apply and in these authors' experience, is generally the limiting factor to
the size of the loan. For example, if the borrower owns a skilled nursing facility that appraises at
$10 million, and desires to refinance that facility with a Section 232 loan, if the borrower is
profit motivated, the maximum loan size, under the revised sizing rules, will be 80 percent of the
appraised value, or $8 million. If the borrower in question is non-profit, then the maximum loan
size would be 85 percent of the appraised value, or $8.5 million.
2. Eligible Costs Criterion. As discussed above, the proceeds of a Section
232 loan may be used only to pay eligible costs.
3. Debt Service Coverage Criterion
. For all projects financed under Section
232, the current guidelines require a minimum debt service coverage ratio of 1.45.
36
This
represents a tightening of requirements from the statutory requirements set forth in the MAP
Guide that requires debt service for Section 232 loan not to exceed 90 percent (for profit-
motivated mortgagors) or 95 percent (nonprofit mortgagors) of the project’s estimated net
earnings attributable to realty and nonrealty (excluding proprietary earnings) and for Section
232/223(f) loans not to exceed 85 percent of the project’s estimated net income for profit-
motivated borrowers, or 90 percent of estimated net income for nonprofit borrowers.
37
If the
project is exempt from real estate taxes, then the mortgage can exceed the debt service limit by
capitalizing the savings from any such tax abatement, so long as the tax abatement runs with the
land (not with the sponsor) and the additional mortgage amount supported by the abatement must
be amortized over the life of the abatement.
38
Since the statutory minimum debt coverage is less
strict, it is possible to submit an application with less coverage, but it would need strong
mitigating factors in order for it to be approved.
H. Secondary Financing
The Section 232 insured mortgage must be secured by a first priority mortgage or deed of
trust on the project. In addition, there are strict rules on the types of subordinate financing that is
allowed to be secured by liens subordinate to the insured mortgage. In general, the only types of
permitted secondary financing are the following:
1. Surplus Cash/Residual Receipts Note. Subordinate financing which is
payable only from residual receipts (for nonprofit borrowers) or surplus cash (for profit-
motivated borrowers) with a maturity date not earlier than the final maturity date of the Section
232 loan is permitted under certain circumstances. Any such note evidencing such a loan must
be on form FHA-2223 (“Surplus Cash Note”) or, for nonprofit borrowers, must be form FHA-
1710 (“Residual Receipts Note”).
39
These form notes are not negotiable and must be used
without any alterations. The term of the note must not be any shorter than the FHA insured
mortgage note, and repayment of principal and payment of interest is limited to surplus cash or
36
Id.
37
MAP GUIDE, supra note 17, ch. 8, § 8(A)(1)(c).
38
Id.
39
MAP GUIDE, supra note 17, ch.8 §10(A).

7/2392190.7
990007-000001
- 11 -
residual receipts (as those terms are used in the Regulatory Agreement). Unpaid interest may be
accrued, but failure to pay interest may not be an event of default.
40
The amount of the note,
must not exceed the amount that, when added to the FHA insured loan, does not exceed 92.5
percent of the fair market value of the project determined in the underwriting of the FHA insured
loan.
41
Any pledge of cash flow may not exceed 50 percent of the surplus cash or residual
receipts of the project. The note may be secured by a second priority mortgage, but only to the
extent that it is closed at the same time as the FHA insured first mortgage, and the second
mortgage may not be foreclosed at any time before the termination of the first mortgage, and
may not include any sort of cross-default provision with the first mortgage.
42
As a practical
matter, these terms are unlikely to be attractive to most commercial lenders or banks.
2. Governmental Secondary Financing
. If the secondary loan is provided by
a governmental agency or instrumentality the amount can be higher – up to 100 percent of the
difference between the FHA insured loan and the fair market value.
43
This would include
501(c)(3) tax exempt bonds issued by nonprofit organizations as well as other forms of tax
exempt financing. Even so, the other restrictions on the terms of the financing still apply. Also,
no additional subordinate financing is permitted (i.e., no third mortgages).
3. FHA Insured Supplemental Financing under Section 241. If a project
needs additional financing after the closing of the initial loan under Section 232, in certain
circumstances supplemental FHA financing secured by a second lien mortgage is available under
Section 241, which is the program under which FHA will insure supplemental loans for projects
which have already been financed with FHA insured first mortgages. The reasons for a Section
241 supplemental loan vary. Sometimes they are used to finance renovation or construction
costs (such as an expansion wing or major reconstruction) when such additional construction is
required and the original Section 232 loan remains closed to prepayment and thus cannot be
refinanced. For example, if conditions or regulatory requirements change after the original
insured loan has closed, the borrower may have an urgent need for renovation in order to
maintain regulatory compliance and it is rather difficult to obtain commercial secondary
financing due to the requirements under the Section 232 program discussed in section 1 above.
Section 241 loans are also processed under the Lean program, and in general have similar
requirements as the Section 232 requirements.
4. Accounts Receivable Financing
. In general, the FHA financing must be
secured by a first priority security interest in the accounts receivable of the project. However, as
discussed in more detail in part III(D) of this article, qualified accounts receivable financing may
be secured by priority liens in the project accounts receivable with the FHA financing to be
secured by subordinate liens in the project accounts receivable.
40
See Form FHA-2223 (2010), available at http://www.hud.gov/offices/adm/hudclips/forms/fhaforms.cfm.
41
MAP GUIDE, supra note 17, ch.8 §10(B).
42
MAP GUIDE, supra note 17, ch.8 §10(D.
43
MAP GUIDE, supra note 17, ch.8 §10(B).
7/2392190.7
990007-000001
- 12 -
I. Sale of Project, Change of Ownership, Assumption of Loan
1. TPA Process – Sale of Project. Most conventional loans include a “due-
on-sale” clause which provides that if the collateral for the loan is sold (or for any reason no
longer owned by the borrower) the entire loan is immediately due and payable. This means that
for conventionally financed projects, when the project is sold, the buyer must obtain its own new
loan, and the proceeds of the new loan will be used to pay the purchase price and allow the seller
to pay its prior loan in full. FHA insured financing may be assumed by a purchaser of the
financed facility in certain cases. The procedure for approving the transfer is called “TPA”
which stands for “Transfer of Physical Assets.” In overview, the TPA process allows HUD to
underwrite the credit of the proposed new owner of the facility, but it is substantially simpler
than obtaining the original FHA insured loan in the first place. This is because the TPA process
contains a lesser amount of facility underwriting, as the facility itself will have already been
approved when the initial loan was made. The checklist for TPA submissions includes the same
data about the new purchaser assuming the loan as would be submitted with a new application in
order to establish that the purchaser is an eligible borrower, but there are fewer requirements
concerning the facility itself, as the facility has already been determined to be an eligible
project.
44
2. Modified TPA - Changes Short of a Sale. The Regulatory Agreement and
other loan documents executed at the initial closing of a Section 232 loan will require that any
change of ownership, change of identity or change in control of the borrower, the operating
lessee or the manager requires HUD's prior written consent. The process of obtaining consent to
a change in control is called the modified TPA process. In most cases, the facility is not
changing ownership, and thus there will be no deed or other transfer document recorded. Rather,
there may be a new lessee, or a new manager. HUD processes these requests using the same
checklist of submission items that is uses for a full TPA request, except that not all of the
checklist items are applicable.
III. Recent Developments – A Magical Mystery Tour of Outstanding Hot Issues
A. Popularity of 223(a)(7) Refinancing Loans
The FHA Section 223(a)(7) program is a streamlined refinancing program that is limited
to the refinancing of multifamily properties (including healthcare facilities, under Section
232/223(a)(7)) already subject to mortgage finance insured by FHA. This is not a new program,
and is not limited to healthcare facilities. Because it allows borrowers to “reset” their interest
rates to take advantage of current low rates, it has become more popular recently for owners of
healthcare projects. This recent popularity may be a factor driving the increased volume of HUD
insured loans that has been causing processing delays.
45
The borrower can refinance at current
44
U.S. Department of Housing and Urban Development, Loan Modification (Interest Only) Checklist (2010),
http://portal.hud.gov/hudportal/documents/huddoc?id=LoanModi_Checklist.doc.
45
HUD’s LEAN 232 Program Office of Healthcare Programs Update, U.S. Department of Housing and Urban
Development (January 25, 2011). OHP acknowledges the “rapidly increasing volume” of these loans and
establishes revised processing queues.

7/2392190.7
990007-000001
- 13 -
market rates with a loan up to the original principal amount of the prior mortgage which will be
for a term co-terminus with the prior mortgage, or, based on an acceptable property inspection,
for a term equal to the original term of the prior mortgage. Naturally, this is only possible if the
prior loan has been in existence for long enough that it is past any period for which prepayment
is forbidden.
In the past, there has been less incentive for a borrower incurring the transaction costs
required to refinance under Section 223(a)(7), particularly when a refinance under Section 223(f)
allows an increased loan amount to cover repairs and renovations. However, interest rates are at
historic lows, and a Section 223(a)(7) loan may be offered at rates in the 4 percent-4.5 percent
range. If the prior Section 232 loan was at 7 percent, for example, the debt service savings
would be substantial. Also, if the prior loan has been in place for a number of years, the
amortization is sufficiently large enough that the difference between the original principal
amount and the current payoff amount will cover the closing and transactional costs. For these
reasons, the volume of (a)(7) financings has been growing.
B. LEAN Processing Revisions and Queues
The Lean processing program began in 2008, and during the 2008 fiscal year (ended
September 30, 2008) FHA insured mortgages (under Section 232) for 189 projects containing
21,679 beds for a total of $1.2 billion.
46
The volume has increased each year thereafter. During
the 2009 fiscal year (October 1, 2008 through September 30, 2009) HUD processed 271 loan
applications for healthcare facilities under Section 232 and insured mortgages for 255 projects
containing 30,155 beds for a total of $2 billion.
47
During the 2010 fiscal year, the volume of
applications rose 283 percent over the prior year, with the result that in fiscal year 2010, HUD
processed 768 applications under Section 232 and endorsed 309 loans totaling $2.6 billion
covering 35,789 beds.
48
As of October 1, 2010 there were 255 applications in the processing
queue. It may be said that the program has been a victim of its own success, as increasing
numbers of borrowers file applications to take advantage of the attractive loan terms.
The initial response to the volume increase was to establish two separate channels for
processing.
49
Initially, the so-called “Green Lane” queue was established for Section 223(a)(7)
refinancing loans so that these simpler deals could speed through the HUD process, and then the
“Green Lane” was expanded to include other Section 232 loans that presented lower risks, which
46
Mortgage Insurance for Nursing Homes, Intermediate Care, Board & Care and Assisted-Living Facilities;
Section 232 and Section 223(f), U.S. Department of Housing and Urban Development (December 30, 2009),
http://www.hud.gov/offices/hsg/mfh/progdesc/nursingalcp232.cfm.
47
U.S. Department of Housing and Urban Development, Description of HUD Programs, (February 17, 2011)
http://portal.hud.gov/hudportal/HUD?src=/federal_housing_administration/healthcare_facilities/mortgage_insurance
/about_the_office_of_healthcare_programs.
48
HUD 2010 Annual Management Report, supra note 5 at pages 23-24.
49
HUD Update as of November 2, 2010, supra note 7; Cambridge Provides $6.03 Million HUD Lean Mortgage
Loan to Refinance Crystal Pines Nursing Home in Crystal Lake, Illinois, Cambridge Realty Capital Companies
ePulse Newsletter (December 2010).

7/2392190.7
990007-000001
- 14 -
were defined to be projects which met each of the following criteria: (i) risk assessment criteria,
(ii) no regulatory waivers requested, (iii) no outstanding or unresolved underwriting issues, and
(iv) (beginning in August, 2010) all forms 2530 being filed electronically through APPS. The
remaining applications were assigned to the regular lane (perhaps the “Red Lane” is an
appropriate, though not official, moniker). The goal was to speed the simple projects through the
Green Lane, and the intent was to keep processing queues, at least in the Green Lane, down to an
acceptable wait time. However, during 2010, the great popularity of these loans meant that even
Green Lane waiting times were increasingly long.
Beginning in November 2010, and in response to the rapidly growing waiting times in
processing (from approximately four months to up to ten months in October 2010), the HUD
Office of Healthcare Programs has established five separate processing queues, and a given
application will be assigned to one of these five queues depending upon the kind of application.
These queues are:
223(f) Regular Queue – Section 232/223(f) projects (refinancings) that do not meet Green
Lane criteria
223(f) Green Lane Queue – Section 232/223(f) projects that meet Green Lane criteria and
are not part of a Large or Midsize Portfolio
223(f) Portfolio Queue – Projects that are part of a Large or Midsize Portfolio which has
been previously approved under HUD Notice H 01-03, as discussed below
Other Program Queue – Projects under Section 232 New Construction or Substantial
Rehabilitation, Section 241(a) Supplemental Loans and Section 232 Blended Rate applications.
These projects are not as common and can be more difficult to underwrite; creating a separate
queue for them was intended to speed the other queues.
223(a)(7) Queue – Projects that were financed under Section 232 in the past, and are now
being refinanced with no new proceeds or increased loan amount. As of January 2011, the
Section 223(a)(7) queue has been divided between an (a)(7) “Green Lane” for all (a)(7) loan
applications that do not propose any extension of the loan term, do not include accounts
receivable financing, and do not involve any change of entity, and with the remaining (a)(7) loan
applications to remain in the “standard” (a)(7) queue.
50
Based on the analysis performed by the OHP in October 2010, OHP believes that the
processing queues should level off at an eight to nine month level for most queues.
51
In order to
prevent large portfolios from creating “bottlenecks”, OHP has also changed the rules to require
all members of the portfolio to have complete applications before being assigned a place in the
50
U.S. Dep’t of Housing & Urban Dev., HUD’s LEAN 232 Program Office of Insured Health Care Facilities
(OIHCF): Update as .January 25, 2011.
51
U.S. Dep’t of Housing & Urban Dev., HUD’s LEAN 232 Program Office of Insured Health Care Facilities
(OIHCF): Update as of November 2, 2010.

7/2392190.7
990007-000001
- 15 -
queue.
52
Before this change, a portfolio could submit one complete application as a placeholder,
and then work on the remaining applications while the placeholder application was in the queue,
moving up the line. Delays arose because if there were application problems, or incomplete
items in the applications that were then submitted once the placeholder was at the front of the
line, processing would slow or stop while these application deficiencies were remedied.
C. Portfolios and the Master Lease Structure – New Ways to Manage Risk
1. Market Risk Issues. In the past, the FHA insured loan programs were of
most interest to the smaller companies which often own a single facility, or at most two or three
facilities. In part, this was because these smaller companies, many of which are nonprofit, have
always had more difficulty accessing the commercial financing markets due to lower
capitalization and less solid credit. However, in the past few years, the larger healthcare
companies which own and operate chains of facilities have increasingly turned to FHA insured
financing. Instead of loans for one facility at a time, or two or three, the applications have
included an entire portfolio of facilities. This trend has led HUD to review its procedures for
processing portfolio loans. Unlike commercial lenders, it is a statutory requirement that each
insured mortgage loan is made to a borrower which only owns the single project being financed.
Thus, a portfolio of projects would be financed with a group of individual mortgages to each
individual affiliate which would be closed together on parallel terms but would not otherwise
share any security or payment obligations. In recent years, HUD has realized that its mortgages
will be more secure if it develops a structure to allow the stronger facilities within a portfolio to
support the weaker ones.
There are two elements of risk that can cause a loan to go into default: (i) risk associated
with the particular borrower’s credit, and that borrower’s particular project and its operations;
and (ii) general market risk caused by the overall economy in which the project operates. The
first category of risk is the reason for detailed underwriting of any loan, with consideration to the
specific operating environment of each facility and the borrower’s credit status. To the extent
that a loan is secured by a portfolio of projects in different areas, with different operational risks,
the overall loan risk can be reduced. The second category, general market risk, is very hard to
avoid, as all operators will be facing the same global concerns of Medicare and Medicaid
regulations and rates, for example. However, two facilities in two different geographic areas
may face quite different challenges for certain matters, such as the availability of employees
willing to work at a long term care facility. For these reasons, commercial lenders often require
that a loan be secured by liens on a group of facilities rather than a single facility.
Perhaps in counterpoint, however, when a portfolio of facilities is owned by the same
organization (albeit in different affiliated entities) there is an enhanced credit risk because the
entire portfolio will be subject to an adverse credit effect on the parent entity. Thus, although in
some respects a portfolio improves the overall credit, there is also the increased risk of
concentrating the financing into a related portfolio. If HUD were to approve FHA insurance for
three separate facilities, owned by three separate borrowers, it would expect that the credit risk
52
Id.
7/2392190.7
990007-000001
- 16 -
inherent to one of these borrowers would be independent from each of the other borrowers.
However, if all three borrowers were in fact indirectly owned by the same parent company, an
adverse financial event that affected the parent company could adversely affect all three
borrowers, and thus the level of risk insured by the FHA insurance would be higher than
anticipated.
2. Traditional Portfolio Processing. Packages of loan applications for
multiple facilities owned by affiliated companies have created issues for HUD for a number of
years. HUD’s rules for underwriting portfolios of loans for facilities under affiliated ownership
were summarized in Notice H 01-03 which was issued in 2001.
53
Part of the application package
for any Section 232 loan includes a HUD Form H 01-03 which requires the borrower to set forth
all projects owned by affiliates seeking FHA insurance within an 18 month period before and
after the submission date. Use of this form allowed HUD to determine if, in fact, there was going
to be a portfolio of projects ultimately submitted, and if so, HUD could use its portfolio
processing rules for underwriting instead. It is interesting to note that even as early as 2002,
industry insiders were aware that HUD personnel were becoming concerned with the risks of
portfolio loans and realized that FHA lenders needed to pay very careful attention to ensure that
borrowers accurately disclosed their intentions for multiple facility portfolios.
54
A medium size portfolio is 11 or more properties with a total insured financing in excess
of $75 million. For medium size portfolios, in addition to the underwriting of each facility, HUD
requires a rating agency review of corporate credit to be approved by the headquarters office of
HUD. Large size portfolios are portfolios (of any number of properties) in which the total
insured financing is in excess of $250 million. For large size portfolios, in addition to the rating
agency review of corporate credit, the rating agency must perform a standardized three-part
analysis including corporate credit, site visits, and status and performance review of properties
and lines of business on all other assets held by the principals of the borrower's ownership group
which must be approved by HUD headquarters
55
.
3. New Master Lease Structure. As HUD officials realized that the existing
portfolio underwriting procedures might be insufficient to reflect the risk of a very large insured
loss if a single adverse event applied to an entire portfolio of insured loans, they sought
additional ways to mitigate risk. Although credit exposure of a portfolio of loans which were
cross-collateralized and cross-defaulted would be stronger than the traditional loan structure of
single loans to single purpose borrowers, the structure of FHA insured financing prohibits the
53
HUD Notice H 01-03, U.S. Department of Housing and Urban Development, (2001)
http://www.hud.gov/offices/adm/hudclips/notices/hsg/03hsgnotices.cfm
. HUD Notice H 01-03 requires the
submission of a Form 01-03 which discloses to HUD all projects that are expected to be submitted to HUD within a
36 month window (18 months before the application through 18 months after application) so that HUD can evaluate
the portfolio risk rather than simply looking at each project separately.
54
An Update of Legislative and Miscellaneous Federal Healthcare Matters, MORTGAGE BANKERS ASSOCIATION
BULLETIN 02/9 (Healthcare Financing Study Group Committee on Government Programs) September 24, 2002, at 2.
55
HUD Notice H 01-03 supra note 53, Section V describes the credit analysis process for medium and large size
portfolios.

7/2392190.7
990007-000001
- 17 -
sort of pooled collateral that is commonly used by commercial lenders. Therefore, HUD
officials worked with certain experienced healthcare FHA lenders to develop a new structure to
allow members of a portfolio of facilities to offer credit support to one another, while still
maintaining the statutory requirements that Section 232 loans be made only to single purpose
single asset entities. Projects proposed for financing that are affiliated by common ownership
among the owners or the operating lessee must now receive written approval from HUD, and
HUD has the right to require that they be processed under the newly created master lease
structure.
56
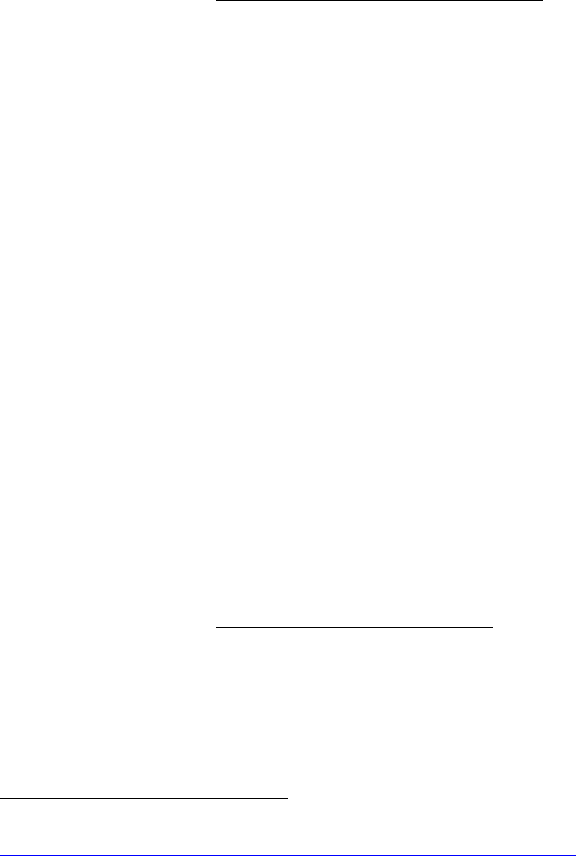
Under the master lease structure, each of the facilities in the portfolio is owned by a
separate single purpose, single asset entity. Each facility owner leases its facility to a single
master tenant. The master tenant then enters into separate subleases to a separate operating
company for each of the facilities. The operating company holds the license to the facility, is
responsible for day-to-day operation of the facility, and, as license holder, receives the payments
for services at the facility. Each of the operating lessees enters into a cross-guaranty agreement
guaranteeing to the master tenant the performance under the subleases. In general, each of the
facility owners, the master tenant, and each of the operating lessees are all affiliates under
indirect common ownership. The rents paid by the master tenant to each of the facility owners is
calculated to equal the debt service, real estate taxes and insurance allocable to that facility, plus
a small reserve. Likewise, the sub-rent paid by each operating lessee to the master tenant is a
similar amount. Since the performance by the subtenants has been guaranteed by all of the other
subtenants, however, the master tenant has the operations of all the facilities securing its receipts
of sub-rent. Therefore, as a practical matter, the operations of all of the facilities are supporting
the loans made to each facility, and this structure accomplishes the goal of improving the credit
of each facility loan. Figure 2 illustrates the structure, as applied to a three facility portfolio.
56
HUD Addendum to Operating Lease, U.S. Department of Housing and Urban Development (June 15, 2010),
portal.hud.gov/hudportal/documents/huddoc?id=FHA_DOC_85.doc.

7/2392190.7
990007-000001
- 18 -
Figure 2
4. Legal Risks of Master Lease Structure.
The master lease loan structure is
relatively new and has received mixed reviews. On the one hand, some borrowers welcome the
opportunity to create a pool of facilities to spread the risk of adverse financial consequences.
Other borrowers, however, fear that the rather complicated contractual structure in the master
lease financing may create liability risks. Borrowers fear that the contractual relationships
established by the master lease, the subleases, and the cross-guaranty could allow a plaintiff
against one facility to claim assets of the other facilities to satisfy its claim. For example, using
the structure shown on Figure 2, suppose that a tort plaintiff were to have a claim against
Subtenant 1 arising from an injury that occurred at Facility 1. Could a plaintiff somehow reach

7/2392190.7
990007-000001
- 19 -
the assets of Subtenants 2 and 3, or even Owners 2 and 3, as a result of the master lease contracts
in place?
(a) To Pierce or Not to Pierce – the Corporate Veil? The legal
argument for liability is a doctrine known as “piercing the corporate veil.” The doctrine rebuts
the general proposition that corporations are separate legal persons and holds a parent
corporation liable for the obligations of its corporate subsidiary, and holds its shareholders liable
for the subsidiary’s corporate obligations.
57
Could an enterprising plaintiff claim that because
the Master Tenant is a common parent of all three Subtenants, and because all three Subtenants
have guaranteed all three Subleases, that the separate corporate existences of all three
Subtenants, and perhaps even all three Owners, can be disregarded (thus their corporate veils
against liability are “pierced”), thus allowing the plaintiff access to the assets of all these other
entities to satisfy its claim?
Courts usually pierce the corporate veil in situations in which the corporate parent and its
subsidiaries have failed to conduct their operations as actual separate entities. Often there are
assertions of wrongful intent, with the result that a successful plaintiff may have its claims
payable both from the subsidiary and its parent, as if they were not distinct, separate legal
entities. The master lease structure, however, is rather more complicated. Referring again to
Figure 2, liability against Subtenant 1 must first reach upstream to the parent (Master Tenant)
and then back downstream to the other subsidiary entities (Subtenant 2 and Subtenant 3). While
traditional veil-piercing doctrine allows recovery against an upstream entity like a shareholder or
corporate parent, there are two derivative doctrines which allow veil-piercing in other situations.
The first doctrine, “reverse piercing” holds a corporation or subsidiary liable for the obligations
of its stockholders or parent. The second doctrine, “single business enterprise” theory,
disregards the corporate identities of an entire group of entities, treating the whole group as one
enterprise liable for the debts of all of its members.
58
Returning to the master lease structure on Figure 2, consider the application of these
doctrines. Using only the traditional veil-piercing doctrine, a plaintiff against Subtenant 1 could
recover only against two entities: Subtenant 1 and (only if successful in its piercing argument),
its parent entity (“Parent Corp”). However, by using the derivative doctrines described above,
the enterprising plaintiff could pursue other affiliated entities in one of two ways. He might
pierce to reach Parent Corp and then reverse pierce to reach a different affiliated subsidiary, such
as Subtenant 2. Or, he could ask the court to disregard all of the separate forms within a group of
subsidiaries under the single business enterprise theory. It is important to note that there is
currently no case authority that considers structures such as the master lease structure on Figure
2, and thus it is very difficult to determine if such approaches have any realistic chance of
success, or if they remain merely interesting law school hypotheticals. In practice, the
determination whether a subsidiary could fit into a “single business enterprise” group or be
accessed by reverse piercing may well depend on veil-piercing rules that differ across
jurisdictions.
57
See 18 AM. JUR. 2d Corporations §47 (2010).
58
See Green v. Champion Ins. Co., 577 So. 2d 249, 259 (La. Ct. App. 1991).
7/2392190.7
990007-000001
- 20 -
Some jurisdictions require fraud or similar abuse of the corporate form on the part of an
entity before its corporate veil can be pierced. In other jurisdictions, a sufficiently close
relationship between two entities will allow veil-piercing even absent evidence of misconduct.
Under the former rule, typical negligence actions are less likely to trigger veil-piercing.
59
A
2009 bankruptcy court discussed this distinction in detail, contrasting Colorado’s “control-and-
wrongdoing requirement” with New York’s more permissive “control-or-wrongdoing rule.”
60
(b) Specific State Law Provisions. The outcome of a claim to pierce
the corporate veil will depend on the applicable state law. While it is not practical in this article
to conduct a 50 state survey, it may be helpful to examine specific state case law precedent for
four states to illustrate the way that the doctrine is applied in different jurisdictions.
(i) Tennessee. Since 1979, the Tennessee Supreme Court has
recognized an “instrumentality rule” to determine whether a parent corporation may be held
liable for the debts of its subsidiary. In Continental Bankers Life Insurance Co. of the South v.
Bank of Alamo,
61
the Court listed a three-factor test: (1) the parent corporation, at the time of the
transaction I question, exercises complete dominion over its subsidiary, via financial control and
authority over policy and business practice to the extent that the corporate entity, as to that
transaction, had no separate mind, will or existence of its own; (2) such control must have been
used to commit fraud or wrong, to perpetuate the violation of a statutory or other positive legal
duty, or a dishonest and unjust act in contravention of third parties' rights; and (3) the aforesaid
control and breach of duty must proximately cause the injury or unjust loss complained of.
62
The Tennessee Supreme Court has recently affirmed this test.
63
Tennessee courts have never
embraced a single business enterprise theory, so plaintiffs attempting to recover against sibling
entities will rely on a two-step reverse piercing process. Even the first step—reaching the
corporate parent—will prove difficult as the Continental Bankers test requires both control and
wrongdoing. To satisfy the first prong, a plaintiff would have to trace the subsidiary’s alleged
negligence to some business decision of the parent. To satisfy the second prong, a plaintiff
would further have to show that the parent isolated its subsidiary in an attempt to avoid
responsibility for negligence to which it contributed. Even if a plaintiff succeeded against the
59
See, Town Hall Estates Whitney, Inc. v. Winters, 220 S.W.3d 71 (Tex. Ct. App. 2007) (in a suit against a nursing
home, holding that piercing the corporate veil required “something more than mere unity of financial interest,
ownership and control.”).
60
See In re Saba Enterprises, 421 B.R. 626, 648-52 (Bankr. S.D.N.Y. 2009).
61
Continental Bankers Life Ins. Co. of the South v. Bank of Alamo, 578 S.W.2d 625 (Tenn. 1979). In this case, a
borrower’s corporate subsidiary deposited $50,000 at the defendant bank, which claimed that this deposit was
intended as security for a $100,000 loan to the borrower. When the borrower defaulted on the loan, the bank refused
to allow the subsidiary to recover its deposit, and sought to pierce the corporate veil that separated the subsidiary’s
separate legal existence from that of its borrower. The court declined to pierce the corporate veil, and instead
honored the separate legal existence of the subsidiary corporation because it evinced a “mind of its own” in the
transaction and the parent company’s control was not exercised to “commit fraud, misrepresentation, or a dishonest
or unjust act on the bank.”
62
Id. at 632.
63
Gordon v. Greenview Hospital, 300 S.W.3d 635, 653 (Tenn. 2009).
7/2392190.7
990007-000001
- 21 -
veil of a corporate parent, it would still have to prevail on a reverse-piercing argument to recover
against other related entities.
Thus, while Tennessee law probably permits reverse piercing in the parent/subsidiary
context,
64
the plaintiff would still have to satisfy the Continental Bankers second prong. A
plaintiff might try to show that a parent corporation maliciously isolated a healthcare facility
operator to avoid liability, but this would be difficult to prove when the structure had been
created for an entirely different reason – namely, to qualify for FHA insured financing.
(ii) Illinois
. Illinois courts considering piercing the corporate
veil often cite Ted Harrison Oil Co. v. Dokka,
65
which lists two mandatory conditions: “for a
court to pierce the corporate veil (1) there must be such unity of interest and ownership that the
separate personalities of the corporation and the individual no longer exist; and (2) circumstances
must exist such that adherence to the fiction of a separate corporate existence would sanction a
fraud, promote injustice, or promote inequitable consequences.”
66
While the second Illinois
prong leaves room for veil-piercing based on mere control, precedent generally involves fraud or
similar wrongdoing, and Illinois has not adopted a single business enterprise theory. Courts
typically require evidence that the corporation is acting only as a “mere façade” for the
shareholders.
67
While the Tennessee rule focuses on how a corporation uses an entity under its
control, the Illinois test focuses instead on the effect of judicially recognizing “separate corporate
existence.” This distinction bears significance in theory—it might allow veil-piercing without a
finding of purposeful fraud or abuse, but successful veil-piercing attempts in Illinois still involve
purposeful wrongdoing.
68
A legitimate business purpose defense would contravene the factors
of either test that turn on a determination that the corporation is a “mere façade” for the
shareholders.
69
Thus, like Tennessee, it would appear unlikely that a plaintiff could successfully
pierce the corporate veil in the master lease situation.
(iii) Indiana. Indiana maintains a traditional veil-piercing test,
and several of its appellate courts have also endorsed a more distinctive single business
enterprise theory. The traditional test held by the Indiana Supreme Court in Aronson
70
states that
“the burden is on the party seeking to pierce the corporate veil to prove that the corporate form
was so ignored, controlled or manipulated that it was the mere instrumentality of another and that
the misuse of the corporate form would constitute a fraud or promote injustice.”
71
The court
64
Nadler v. Mountain Valley Chapel Business Trust, 2004 WL 1488544 (Tenn. Ct. App., 2004).
65
Ted Harrison Oil Co., Inc. v. Dokka, 617 N.E.2d 898 (Ill. Ct. App. 1993)
66
Id. at 901 (citing People ex rel. Scott v. Pintozzi, 277 N.E.2d 844, 851-52 (Ill. 1971).
67
Ted Harrison, 617 N.E.2d at 902; Fontana v. TLD Builders, Inc., 840 N.E.2d 767, 778.
68
See, Fontana, 840 N.E.2d at 781-82 (finding that the second mandatory prong was satisfied when defendant
corporation rapidly sold off assets to frustrate creditors).
69
Ted Harrison, 617 N.E.2d at 902; Fontana, 840 N.E.2d at 767, 778.
70
Aronson v. Price, 644 N.E.2d 864 (Ind. 1994).
71
Id. at 867.

7/2392190.7
990007-000001
- 22 -
provided a set of factors (sometimes known as the Aronson factors) relevant to both the
instrumentality and fraud prongs: (1) undercapitalization; (2) absence of corporate records; (3)
fraudulent misrepresentation by corporation shareholders or directors; (4) use of the corporation
to promote fraud, injustice or illegal activities; (5) payment by the corporation of individual
obligations; (6) commingling of assets and affairs; (7) failure to observe required corporate
formalities; or (8) other shareholder acts or conduct ignoring, controlling or manipulating the
corporate form.
72
Indiana courts have applied this test strictly against parties attempting to pierce the
corporate veil. In one case
73
the court reaffirmed the traditional test with a sharp analytical
distinction. The corporate veil could not be pierced merely to “promote substantial justice,” the
court clarified: instead, courts could only disregard the corporate form when it had been
“misuse[d] . . . to promote injustice.”
74
Thus Indiana’s traditional veil-piercing test tends to
mirror Tennessee’s standard: abuse of the corporate form will allow veil-piercing, but incidental
injustice will not. However, in some situations, plaintiffs can circumvent Indiana’s burdensome
traditional rule under a single business enterprise doctrine. In one such case,
75
the court allowed
veil-piercing even though the original plaintiff “failed to present much evidence relevant to the
Aronson factors.” When the veil-piercing inquiry concerns two “affiliated corporations” rather
than a corporation and its stockholders, the court held that one entity can be liable for the
obligations of the other if the two are “effectively one and the same corporation.”
76
Four
different factors were used: (1) whether similar corporate names were used, (2) whether there
were common officers and employees, (3) whether the corporations were operated for similar
business purposes, and (4) whether the corporations shared offices, telephone numbers and
business cards.
77
Alternatively, the court could disregard the corporate form when one
corporation conducted an operation “for the benefit of the whole enterprise.”
78
In applying this theory to the master lease structure, there tends to be more risk under
Indiana’s single business enterprise theory than from the traditional rule. The theory focuses on
three elements: (1) the actual identity of corporations, as indicated by common ownership,
directors and employees; (2) the existence of a joint enterprise, indicated by similar business
purposes and by coordinated, rather than purely self-interested, action by different entities; and
(3) presentation to the public, indicated by similar names and shared offices, telephone numbers
or business cards.
79
Cross-collateralization could increase the probability that courts perceive a
joint enterprise; the operators and owners under the master lease structure already share a
72
Id.
73
Escobedo v. BHM Health Associates, Inc., 818 N.E.2d 930 (Ind. 2004).
74
Id. at 935.
75
Smith v. McLeod Distributing, 744 N.E.2d 459, 463 (Ind. Ct. App. 2000).
76
Id. at 463-64.
77
Id. at 463.
78
Id.
79
See Oliver v. Pinnacle Homes, Inc., 769 N.E.2d 1188, 1192-93 (Ind. Ct. App. 2002).

7/2392190.7
990007-000001
- 23 -
business purpose; and Indiana courts have found single enterprises where “one corporation paid
for the obligations of the other.”
80
No court has recognized a legitimate business purposes
defense to single business enterprise piercing, although how courts would apply these doctrines
to a master lease situation is yet to be determined.
(iv) Delaware. Finally, since so many corporations are
domiciled in the State of Delaware, it would be remiss to not examine the laws of that state.
Delaware’s more established test requires fraud or wrongdoing in order to allow piercing, but a
more recent line of cases disregards this requirement. The Delaware Supreme Court issued its
seminal veil-piercing decision in 1968
81
and held that veil-piercing “may be done only in the
interest of justice, when such matters as fraud, contravention of law or contract, public wrong, or
where equitable consideration among members of the corporation require it, are involved [sic].”
Thus, even if the court assumed that a parent “wholly dominated and controlled” its subsidiary, it
could only disregard the corporate form with an additional element of fraud or injustice.
82
Cases
following this newer test require that the “corporate form cause fraud or similar injustice” before
authorizing piercing of the corporate veil.
83
A second line of cases more amenable to veil-piercing has also emerged. For example
the chancery court has indicated it would allow veil-piercing if a parent and subsidiary were
“operated as a single economic entity such that it would be inequitable . . . to uphold a legal
distinction between them.”
84
That court found that the plaintiff had raised genuine issues of
material fact on its veil-piercing claim and highlighted three relevant factors: (1) that the
defendant subsidiary had loaned its parent company money without apparent consideration; (2)
that the parent company and subsidiary maintained substantially identical boards of directors;
and (3) that officers of the parent were paid from the subsidiary’s payroll account.
85
A later
decision similarly states that “a court can pierce the corporate veil of an entity where there is
fraud or where a subsidiary is in fact a mere instrumentality or alter ego of its owner.”
86
Even when Delaware courts require no fraud or wrongdoing, they will likely accept a
legitimate business purpose defense. In Mabon, the court suggested that corporations could
avoid veil-piercing if they presented “sound business reasons” for activities that appeared to
manipulate the corporate form
87
and in Pauley, the Delaware Supreme Court refused to pierce
80
Id. at 1193.
81
Pauley Petroleum, Inc. v. Continental Oil Co., 239 A.2d 629, 633 (Del. 1968).
82
Id. at 632.
83
Wallace ex rel. Cencom Cable Income Partners II, Inc., L.P. v. Wood, 752 A.2d 1175, 1183-84 (Del. Ch. 1999);
see also Mobil Oil Corp. v. Linear Films, 718 F. Supp. 260, 268 (D. Del. 1989) (stating that to pierce the corporate
veil, “[f]raud or something like it is required.”).
84
Mabon, Nugent & Co. v. Texas American Energy Corp., 1990 WL 44267 (Del. Ct., 1990).
85
Id.
86
Geyer v. Ingersoll Publications Co., 621 A.2d 784, 793 (Del. Ch. 1992).
87
Mabon, 1990 WL 44267 at 5.
7/2392190.7
990007-000001
- 24 -
the corporate veil and found that the “separate existence” of parent and subsidiary “serve[d] a
most legitimate business purpose.”
88
Because groups of facilities should be able to demonstrate
that their structures are fragmented, at least to some extent, in order to become eligible for HUD-
backed mortgages, they should have a very convincing and viable defense under either line of
Delaware cases.
(c) Conclusions. As this discussion demonstrates, any potential
defense to veil-piercing claims should be considered under the laws of the applicable
jurisdiction. The purpose behind the master lease structure is a legitimate business purpose,
created to address particular requirements for access to financing. To the extent that HUD
requires borrowers to adopt fragmented corporate structures as a condition to being eligible for
mortgage insurance, this fragmentation clearly serves a legitimate business purpose. Companies
that qualify for FHA-insured loans benefit from lower interest rates, and can dedicate their
resulting surplus to patient care or profit. Thus, at least in the jurisdictions discussed in this
article, corporations defending fragmentation or cross-collateralization as legitimate business
decisions should be able to avoid veil-piercing liability. In all jurisdictions, whatever the
recognized doctrines, there will be a good argument that the master lease structure, required by
HUD as a precondition to access to financing, simply does not entitle a plaintiff to the “windfall”
of additional deeper pocket defendants simply by application of the arcane doctrines that were
developed in a very different atmosphere of fraudulent intent and wrongdoing.
D. Accounts Receivable Financing – Follow the Money
1. Summary of the Legal Status of Healthcare Accounts Receivable – What’s
the Big Deal?
If healthcare facilities were like apartment buildings, almost all residents or patients
would pay their rent in advance on the first day of the month, and the owner would have the
accumulated prepaid rent in its operating account, available to be used to pay debt service,
salaries, and other operating expenses. For many assisted living facilities, the scheduled monthly
fee is, in fact, routinely paid a month in advance, and the owner should have ample funds on
hand to pay its bills as they come due, assuming an acceptable occupancy level. However, in the
world of nursing homes, it is an entirely different picture. Services are provided first, and then
billed to the patient or, in almost all cases, the patient’s third party payor. For geriatric nursing
homes, this payor is predominantly Medicare or Medicaid. Then, 30, 60, or even 90 days after
the services were rendered, the submitted invoice for services is finally paid. Therefore, the
accumulated balance of accounts receivable for services rendered, billed, but not yet collected
can be a very large number, and accounts receivable become a very significant asset owned by
the operator.
Standard prudent lending practice is to require a first priority lien on all the assets of the
borrower which are used in its business. Thus, lenders require a first priority lien on the
borrower’s land, buildings, improvements, and personal property. One important element of
personal property is borrower’s accounts receivable. Liens on accounts are governed by the
88
Pauley, 239 A.2d at 633.

7/2392190.7
990007-000001
- 25 -
Uniform Commercial Code (“UCC”) (UCC Section 9-102) and may be perfected by filing a
financing statement in the office of the secretary of state of the state in which the borrower is
organized (UCC Section 9-310). HUD insured loans, like almost all other loans, require a
borrower to execute a security interest that grants a lien in all of its personal property, including
accounts, and also like almost all other loans, the lender will then file a UCC-1 Financing
Statement to perfect its lien in that personal property. For Section 232 loans to nursing homes,
the situation becomes more complex because there are special provisions concerning accounts
receivable for payments from governmental agencies, and as noted above, the majority of the
accounts receivable for a typical nursing home are Medicare and Medicaid receivables.
The statute that governs the payment of claims under Medicare Part A provides that “no
payment which may be made to a provider of services under this subchapter for any service
furnished to an individual shall be made to any other person under an assignment or power of
attorney.”
89
The provision does not apply to assignments made to government agencies or
assignments pursuant to court order, and also excludes payments made to an agent of the
provider, so long as the agent’s compensation is unconnected to the amount collected and
independent of the actual collection of payments.
90
The statute that controls the payment of claims under Medicare Part B contains similar
language. It provides that “no payment under this part for a service provided to any individual
shall…be made to anyone other than such individual or…the physician or other person who
provided the service, and including assignment to a government agency, per a court order, or to a
collection agency.”
91
Under the Medicaid program, the federal government regulates how states use federal
money to fund state plans for medical assistance. The federal Medicaid statute requires that state
plans “provide that no payment under the plan for any care or service provided to an individual
shall be made to anyone other than such individual or the person or institution providing such
care or service, under an assignment or power of attorney or otherwise.”
92
The Medicaid
provision also lists several exceptions, including assignments to government agencies and by
court order and payments to collection agencies.
93
Congress enacted the provisions prohibiting assignment of Medicare and Medicaid
payments to combat the prevalence with which entities that had bought the government
receivables would file fraudulent claims. These entities, called “factors,” would buy government
receivables at a discount from the healthcare provider, and the factors would collect the
89
42 U.S.C.A. § 1395g(c).
90
Id.
91
42 U.S.C.A. § 1395u(b) (6).
92
42 U.S.C.A. § 1396a(a) (32).
93
Id.

7/2392190.7
990007-000001
- 26 -
payments.
94
Because the factors’ profits depended on successful collection of payments, the
system lent itself to “incorrect and inflated claims” and “[s]ubstantial overpayments to many
such organizations…, one involving over a million dollars.”
95
Thus, in 1972, Congress amended
the Social Security Act to prohibit the assignment of receivables; in 1977, it further amended the
act to prohibit the transfer of receivables by power of attorney.
96
Courts have ruled that the anti-assignment provisions of the Medicare and Medicaid
statutes only prohibit assignment of the right to direct payment from the government; they do not
bar third parties from receiving Medicare and Medicaid funds.
97
Typical financing arrangements
where loans are secured by Medicare and Medicaid receivables do not violate the federal anti-
assignment provisions.
98
As long as the government can make the Medicare and Medicaid
payments directly to the provider, the provider may dispense with those payments at its own
discretion, including turning the funds over to a lender.
Courts have upheld arrangements where a healthcare provider granted a security interest
in Medicare and Medicaid receivables to a lender.
99
For example, in In re Missionary Baptist
Found. of Am.,
100
an operator of nursing homes granted a security interest in its accounts
receivable to a bank as loan collateral. The security agreement specifically stated that the
accounts receivable would include Medicare and Medicaid receivables.
101
The nursing home
operator subsequently encountered financial hardship, and the bank terminated its financing
arrangement with the borrower.
102
The bank began applying available assets, including accounts
receivable, to the loan balance.
103
After the nursing home operator filed for bankruptcy, the
bankruptcy trustee sued the bank.
104
He claimed that the bank’s loan agreements with the
nursing home operator were invalid because they allowed the bank to take a security interest in
Medicare and Medicaid receivables, despite the anti-assignment clauses in the federal statutes.
105
94
Gregory R. Salathé, Note, Reducing Health Care Costs Through Hospital Accounts Receivable Securitization, 80
V
A. L. REV. 549, 562 (1994).
95
H.R. Rep. No. 92-231 (1971), reprinted in 1972 U.S.C.C.A.N. 4989, 5090.
96
Charles E. Harrell and Mark D. Folk, Financing American Health Security: The Securitization of Healthcare
Receivables, 50 Bus. Law. 47, 56-57 (1994).
97
Lock Realty Corp. IX v. U.S. Health, LP, 2007 WL 724750 (N.D. Ind., 2007) (citing DFS Secured Healthcare
Receivables Trust v. Caregivers Great Lakes, Inc., 384 F.3d 338, 350 (7th Cir. 2004); In re E. Boston Neighborhood
Health Ctr. Corp, 242 B.R. 562, 573 (Bankr. D. Mass. 1999).
98
Credit Recovery Sys., LLC v. Hieke, 158 F.Supp.2d 689, 693 (E.D. Va. 2001).
99
See, In re Missionary Baptist Found. of Am., 796 F.2d 752 (5th Cir. 1986); Lock Realty Corp. IX v. U.S. Health
(supra note 97). In re Am. Care Corp., 69 B.R. 66 (Bankr. N.D. Ill. 1986).
100
Matter of Missionary Baptist Foundation of America, Inc., 796 F.2d at 754 (5th Cir. 1986)
101
Id. at 755.
102
Id. at 755.
103
Id.
104
Id.
105
Id. at 756.
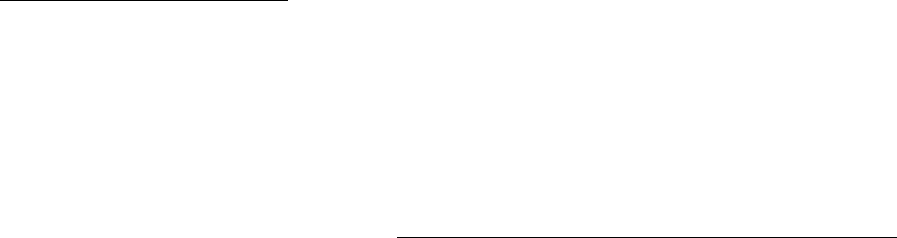
7/2392190.7
990007-000001
- 27 -
The court held that the security interest was valid.
106
First, the court reasoned that the procedure
by which the bank received the payments did not violate the Medicare and Medicaid statutes
because it did not require that the government directly pay the bank.
107
The government made
direct payment to the nursing home operator’s account at the lending bank, and the bank would
subsequently sweep that account and apply the proceeds to the loan balance.
108
Second, the
court reasoned that Congress enacted the anti-assignment statutes to combat factoring, and it did
not view the bank’s lending arrangement as comparable to a factoring arrangement.
109
While Medicare and Medicaid laws do not proscribe the assignment or creation of a
security interest in government receivables, the statutes do require direct payment to the
provider. To constitute direct payment, the government’s payment must first pass through the
control of the provider.
110
Because the payment does end up being received directly by the
provider, a lender may be concerned that the provider might divert the funds upon receipt to
other purposes rather than paying the loan. Thus, a “double lockbox” mechanism has been
developed to minimize this risk.
In the first step of the process, the Medicare and Medicaid payments owed to the provider
are paid into the provider’s deposit account.
111
Only the provider may issue instructions on this
account.
112
The lender does not have a security interest in this deposit account; however, it does
have a security interest in the deposited proceeds of the Medicare and Medicaid receivables.
113
Second, the provider instructs the bank to sweep daily the first deposit account’s funds into a
second deposit account.
114
Although the second deposit account is in the provider’s name, the
lender controls the account.
115
This control enables the lender to perfect a security interest in the
second deposit account, pursuant to the Uniform Commercial Code Section 9-312.
116
Lastly, the
lender disburses the funds in the second deposit account to pay off the provider’s obligations.
117
106
Id. at 759.
107
Id.
108
Id.
109
Id. at 758.
110
Medicare Claims Processing Manual, ch.1, § 30.2, https://www.cms.gov/manuals/downloads/clm104c01.pdf (last
visited June 18, 2010).
111
John Francis Hilson, Practicing Law Institute, Asset-Based Lending: A Practical Guide to Secured Financing, §
1:2.6, 1-20 (2010).
112
Id. at 1-21.
113
Id. at 1-21.
114
Id.
115
Id.
116
Id. at 1-20.
117
Id.

7/2392190.7
990007-000001
- 28 -
The lender can perfect its security interest in the Medicare and Medicaid receivables by
filing a financing statement with the appropriate state office.
118
The lender can perfect its
interest by filing because the Uniform Commercial Code explicitly includes healthcare insurance
receivables as a type of “account.”
119
By perfecting its security interest in the underlying
collateral, the lender also perfects its security interest in the proceeds of that collateral.
120
In a
situation with private receivables, the lender’s perfected security interest allows the lender to
assume the role of the provider if the provider defaults on the loan.
121
In this way, the lender is
able to collect payments directly from the payor—it does not have to wait for the payments to go
though the provider.
122
The Medicare and Medicaid anti-assignment statutes prevent direct payment to the
lender.
123
Thus, to ensure enforcement of the security interest, lenders use the double lockbox
mechanism to perfect their interests in the second deposit account.
124
As mentioned above,
though, at least one court has indicated that it would support court orders directing direct
payment to lenders as a means of enforcing a security interest.
125
Because of the Medicare and
Medicaid anti-assignment provisions, the lender cannot have a security interest in the provider’s
first deposit account.
126
The lender can have a security interest in the provider’s second deposit
account and can issue instructions for that account.
127
To perfect an interest in a deposit account,
the lender must have control of that deposit account.
128
The lender automatically has control
over the account if it is the bank where the deposit account is located.
129
If the lender is not the
depositary bank, the provider, the lender, and the depositary bank must have a written agreement
enabling the lender to issue instructions on the account.
130
Lastly, the lender can exercise control
over the deposit account by becoming the depositary bank’s customer with respect to that
account.
131
118
U.C.C. § 9-310(a) (2001); U.C.C. § 9-501(a) (2001).
119
U.C.C. § 9-102(2) cmt. 5(a) (2001).
120
U.C.C. § 9-315(c) (2001).
121
Kimberly Easter Zirkle, Note, Not So Perfect: The Disconnect Between Medicare and the Uniform Commercial
Code Regarding Health-Care-Insurance Receivables, 9 N.C.
BANKING INST. 373, 379-80 (2005).
122
Id.
123
Id.
124
Hilson, supra note 111, at 1-20.
125
See Lock Realty Corp. IX, 2007 WL 724750
126
Hilson, supra note 111, at 1-20.
127
Id. at 1-21.
128
U.C.C. § 9-314 (2001).
129
U.C.C. § 9-104(a) (1) (2001).
130
U.C.C. § 9-104(a) (2) (2001).
131
U.C.C. § 9-104(a) (3) (2001).

7/2392190.7
990007-000001
- 29 -
2. Accounts Receivable Financing – HUD Rules and the Realities of Third
Party Lenders.
As discussed above, the lengthy delay between the date of service and the date of
payment is a fact of life for many healthcare providers, and can be a very heavy burden on a
provider’s operations. While the provider waits for payment, it must still pay its employees,
keep the lights on, and provide meals for the residents, and all those things require money. In an
ideal world, the provider would have sufficient accumulated financial reserves to finance the
delay in payment, but in the real world, many providers seek accounts receivable financing from
lenders. There are a number of lenders which have developed programs and expertise in
healthcare accounts receivable financing, and in general these lenders use the double account
structure described above.
Until fairly recently, operating lessees of facilities with Section 232 mortgage financing
could pledge their accounts receivable freely to any working capital lender without any
requirement for HUD approval. Since the operating lessee usually holds the healthcare license
of the facility, almost all revenues of the project will initially be received by the operating lessee
as payment for services rendered, and as discussed above, the value of the accounts receivable
(representing the spread of time between the date services are provided to patients and the date
payment is received for those services) can be substantial. Allowing an operating lessee to
pledge away such a substantial project asset without lender consent seems to have been a major
omission, but recall that healthcare loans (Section 232 for long term care and Section 242 for
hospitals) represent only 2.4 percent of the total insured loan funds administered by HUD on
behalf of FHA.
132
The remaining 97.6 percent are single family residential loans and
multifamily residential loans.
133
As discussed above, residential rental properties rarely require
accounts receivable financing and so long as most tenants are paying rent in advance, as required
by their leases, the accounts receivable of an apartment project is a very small portion of the total
asset value of the project. For that reason, the traditional forms and policies for FHA insured
loans did not contain thorough provisions for accounts receivable, and in certain circumstances
(older loans on facilities subject to operating leases), allowed the asset value represented by
accounts receivable of the operating lessee to escape being pledged as collateral at all. For a
number of years, industry insiders warned that HUD was going to close the “loophole” and
require HUD consent for any such pledge by operating lessees.
134
The first change by HUD (before the Lean program was adopted) was to require a rider to
the loan documents that provided any future working capital financing would require HUD
approval and the execution of an intercreditor agreement. An intercreditor agreement is an
agreement signed by the senior and junior lenders which sets forth the priorities of the liens in
favor of each lender and provides procedures to be used by each lender in the enforcement of
such liens in the event of default (for example, usually the junior lender is barred from
132
Fiscal Year 2010 Annual Management Report, Federal Housing Administration (2010),
http://www.hud.gov/offices/hsg/fhafy10annualmanagementreport.pdf.
133
Id.
134
An Update of Legislative and Miscellaneous Federal Healthcare Matters, supra note 54 at 2.

7/2392190.7
990007-000001
- 30 -
foreclosing on its junior lien without the consent of the senior lender.) These requirements were
further explained in Notice H 08-09 which set forth HUD’s requirements to approve working
capital loans while also acknowledging their business rationales.
135
In many ways, this Notice
was a very positive step, as it demonstrated understanding of the need for accounts receivable
financing and provided fairly clear guidelines for the approval of such loans.
One of the modifications created under the Lean program, after the initial requirements
concerning intercreditor agreements, was express recognition that accounts receivable financing
was financially beneficial to many projects, under certain circumstances, and in fact could be
viewed as an asset to the viability of the project and the proposed FHA insured loan so long as
guidelines were met. HUD established procedures for the approval of accounts receivable
financing on insured facilities.
136
Under Section 232 Lean processing rules HUD has the right to
consent to any accounts receivable financing, and will generally do so as long as the financing
supports the financial viability of the project. HUD will accept accounts receivable loans to be
provided by an unrelated third party lender with experience in healthcare lending, based on a
percentage no larger than 85 percent of all accounts receivable less than 120 days old. Existing
accounts receivable financing must be described in the initial application for the loan, with a
detailed financial analysis demonstrating whether the project can support the accounts receivable
loan as well as the proposed FHA insured loan. Accounts receivable financing must be provided
from a recognized lender with experience (typically at least three years) in this type of financing
and sufficient financial controls to monitor the financial operations.
Accounts receivable financing may be provided under a single loan to more than one
facility, but only if all of the facilities are financed with FHA insured loans. There can be no
cross-collateralization between facilities, some of which are financed with FHA insured
financing and some of which are financed with non-FHA loans. There is an approved form of
intercreditor agreement that will be entered into between the FHA lender and the accounts
receivable lender, which will have a rider to it which will provide that the account receivable
lender’s interest in the accounts receivable is prior to the FHA lender’s interest. It will also
require that the accounts receivable lender receive funds in the account and disburse the monthly
payments to the FHA lender before any funds are released to the borrower. Also, advances
under the accounts receivable loan must be applied first to pay debt service to the accounts
receivable lender and second, to pay current operating expenses of the facility, before any other
payments to the borrower or its principals.
137
In one of the many other changes under Lean processing, HUD promulgated two forms
of agreements for use when there is not any separate accounts receivable financing, in order to
replicate the typical double account receivable structure used by accounts receivable lenders.
The facility first establishes an account for receipt of its governmental payer payments (Medicare
135
HUD Notice H 08-09, U.S. Department of Housing and Urban Development, (November 17, 2008),
http://www.hud.gov/offices/adm/hudclips/notices/hsg/03hsgnotices.cfm.
136
Id.
137
U.S. Dep’t of Housing & Urban Dev., Off. of Housing, 232/223(f) LEAN Processing for Section 232 Health
Care Facilities (December 2008), on file with author.

7/2392190.7
990007-000001
- 31 -
and Medicaid) with a depository bank, and that account is swept daily under the provisions of a
Deposit Account Instructions and Service Agreement among the owner, the FHA lender, and the
bank (“DAISA”). Under the DAISA, the facility owner “owns” the accounts as required for
governmental receivables, but “instructs” the bank to sweep the account on a daily basis with all
such proceeds deposited into a second account. This second account is the “lockbox” account
which receives deposits of non-governmental accounts directly, and this account is the subject of
a Deposit Account Control Agreement (“DACA”), which is also a HUD form signed by the
owner, the FHA lender, and the bank. Under the DACA, so long as there is a no default, the
funds may be used by the owner, and in general the owner will have a third account into which it
will deposit the funds released to it under the DACA and out of which it will pay its operating
expenses. Both the DAISA and the DACA must be executed by the bank in which the accounts
are held.
138
In theory, this makes sense and conforms to current lending procedures. In practice,
this can create significant difficulties. The forms are rather new, and many banks are unfamiliar
with them, so banks may be reluctant to sign them without negotiation with their legal
departments. Depending on the bank, and the legal department, this can create delay and
frustration. For example, the current HUD forms limit the bank’s liability to its negligent acts,
but bank forms generally require that the standard be “gross negligence or willful misconduct”.
While this change may be negotiated in certain situations, it needs to be addressed early in the
process. Another example is that the forms require the bank to waive its right of banker’s lien
and set off rights, and these waivers may not be acceptable to the bank. Even if the forms are
substantively similar to the bank’s form, or forms the bank has used in the past, as a practical
matter banks are accustomed to using their own printed forms, and are reluctant to start with an
unfamiliar form. The request to use a different form often results in significant delay if it must
be negotiated with the bank’s legal counsel. Thus, borrower’s counsel is well advised to request
copies of the DAISA and DACA early in the process and start working with the bank to
eliminate needless delay closer to the closing date.
In addition to the forms of DAISA and DACA, HUD is working to promulgate forms to
be used for the second priority liens that will be subordinate to a recognized and approved third
party accounts receivable lender. It is probably fair to say that these forms, as well, are still
works in progress, and HUD recognizes that there may need to be modifications based on the
particular needs of each transaction and lender.
139
The most important point for borrowers and their counsel to remember is to address the
accounts receivable documents as early as possible in the underwriting of an FHA insured loan.
Also, if possible, it is helpful for borrowers to seek their accounts receivable financing from
lenders who have experience with Section 232 loans. It may even be possible for a lender to
have on hand a form document that has been used before and approved in the past by OHP
personnel at HUD.
138
Deposit Account Control Agreement Form, U.S. Department of Housing and Urban Development,
http://portal.hud.gov/hudportal/documents/huddoc?id=DepositCAAAR(non-govt).doc
. DAISA form should be
available in the future from the same HUD portal.
139
U.S. Department of Housing and Urban Development, Office of Housing, 232/223(f) LEAN Processing Training-
for Lenders (2008).

7/2392190.7
990007-000001
- 32 -
IV. Conclusion – The Rollicking Ride Continues
As FHA insured loans become an increasingly important funding source for owners of
long term health facilities, we can expect continued “growing pains” as lengthening queues
compel new procedures and policies. Despite the great efforts being made by officers at HUD,
the volume of applications is growing faster than the expansion of processing capacity at the
OHP. Some salutary effects of the growth have taken place. The program processing protocols
have been revised in significant ways to acknowledge the realities of the underwriting of long
term care facility credit, particularly in the treatment of accounts receivable financing and the
risks of multiple facility portfolios. While some of the recent changes are still difficult for many
practitioners, and some of the newly promulgated forms have yet to be refined completely,
progress is ongoing. The financing offered under Section 232 is very important to providers, and
it is of critical importance to all of the stakeholders in the Section 232 program that these
financing vehicles remain available to the industry. For that to occur, the ultimate financial
viability of the loan programs must be preserved. For those reasons, the new developments
under these programs are important to all the parties concerned with the financial viability of the
nation’s providers of long term care to Americans.
