A business of Marsh McLennan
Act 167 (2022) Community
Engagement to Support Hospital
Transformation: Summary of
State-Level Recommendations
19 June 2024
2
© Oliver Wyman
OLIVER WYMAN EXPERTISE
Bruce H. Hamory, MD FACP
Partner & Chief Medical Officer,
Healthcare & Life Sciences
Elizabeth Southerlan
Managing Director,
Healthcare & Life Sciences
• Helps providers, health systems and countries
to redesign their delivery systems to improve
value by improving quality and reducing costs
• Has worked with many groups to improve their
operations, design appropriate physician
compensation and institute new systems of
care and management to improve performance
• Prior to joining Oliver Wyman, he was
Executive Vice President, System Chief Medical
Officer at Geisinger, and was previously
Executive Director of Penn States’ Hershey
Medical Center and COO for the campus
• Has over 50 years of experience in health care
practice, teaching, leadership, and redesign of
systems for improvement
• Has more than 15 years of experience
partnering with healthcare provider systems to
identify and deliver value from expansion
opportunities
• Provides strategic guidance to healthcare
leaders in a range of areas: corporate and
operational strategy, organizational strategic
design, health equity strategy
and operationalization, product and service
line design and launch, M&A strategy and
execution, strategic transformation,
contracting and renegotiation strategy,
and operational performance improvement
• Earned a bachelor’s degree in industrial
engineering from The Pennsylvania State
University and a master’s degree in systems
engineering and management from the
Massachusetts Institute of Technology
Irene Wei
Engagement Manager,
Healthcare & Life Sciences
DAN SHELLENBARGER
Partner,
Healthcare & Life Sciences
Danielle etzel
Senior Consultant,
Healthcare & Life Sciences
3
© Oliver Wyman
PROJECT CONTEXT
Section 2 of Act 167 (2022) requires that the GMCB, in
collaboration with the Director of Health Care Reform in the
Agency of Human Services, “develop and conduct a data-
informed, patient-focused, community-inclusive engagement
process for Vermont’s hospitals to:
- Reduce inefficiencies
- Lower costs
- Improve population health outcomes
- Reduce health inequities
- Increase access to essential services
All while maintaining sufficient capacity for emergency
management
Broad community and provider engagement in and across all
Hospital Service Areas (HSAs) in Vermont.
– a data-informed, patient-focused, community-inclusive
engagement relative to the second stream of work for Act 167
Goals: engage diverse stakeholders and ascertain their
interactions with the health system and perceived needs to
overcome any barriers to equitable access and outcomes
Current plan: conduct interviews and working sessions in 2
phases and codify qualitative and quantitative inputs to inform a
recommendation.
– Phase 1 - August through mid-November 2023
– Phase 2 - March through Sep 2024
– Timing of the phases are subject to change by mutual
agreement
Act 167 objectives Oliver Wyman’s work
4
© Oliver Wyman
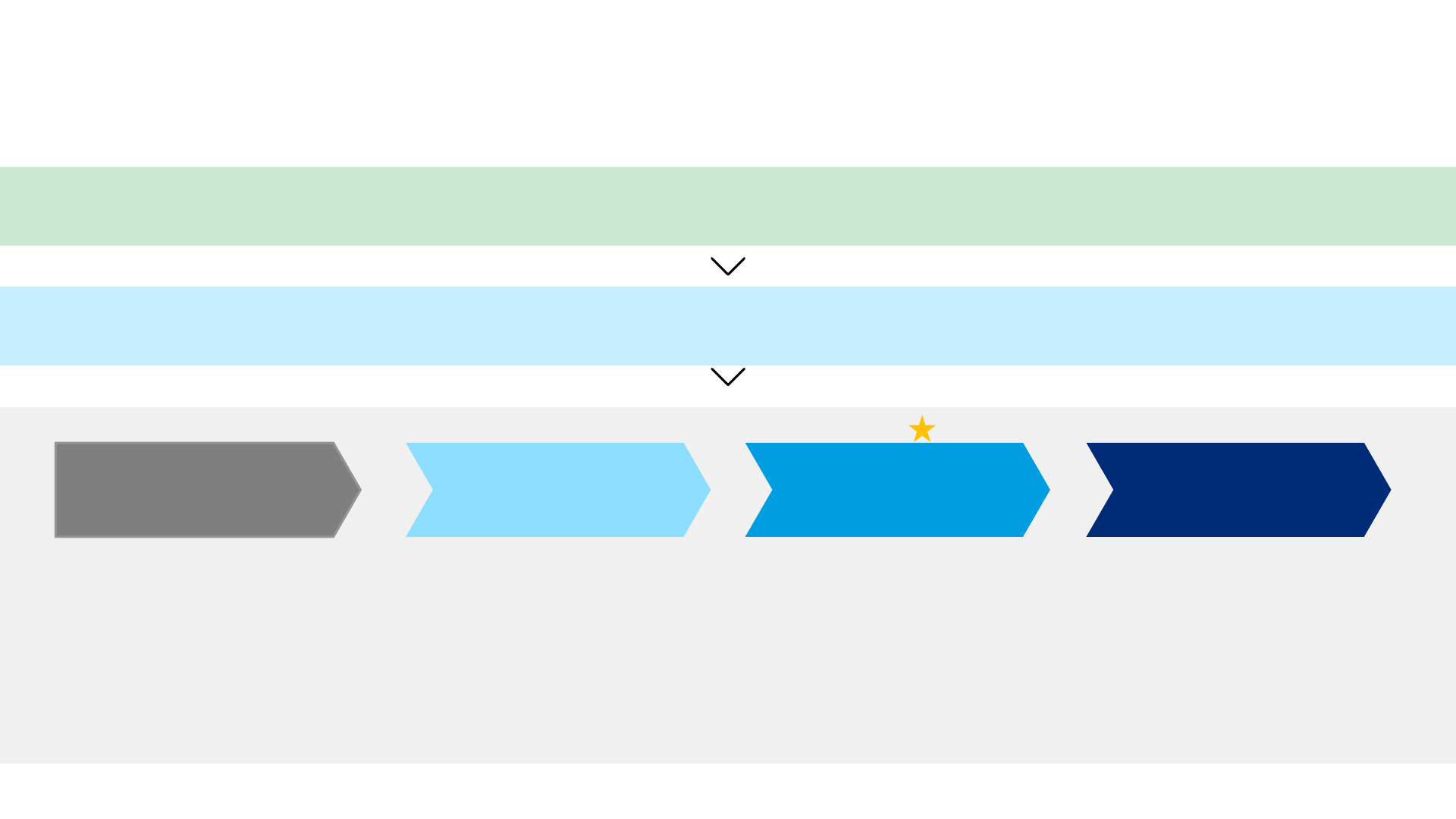
SCOPE, GOALS, AND APPROACH: IMPROVING THE VERMONT HEALTHCARE DELIVERY SYSTEM
REQUIRES INPUT FROM ACROSS THE COMMUNITY IT SERVES
Step 1. Finalize engagement
plan and interview scheduling
Identify and schedule interviews with key
stakeholders in the following groups:
• Hospital leaders
• Provider organizations
• Community leaders and members
• Diverse populations
• State of Vermont partners and Legislators
• Health related organizations
Community and provider engagement process
Step 3. Develop solution
options and vet with
community through 2
nd
round
of interviews
• Develop solutions to address current
needs and reach the desired future
state while considering Act 167 goals
– In conjunction with analytics
contractor
• Obtain stakeholder perspective
on the impact of recommendations
on hospital performance and
healthcare delivery
Step 4. Develop and deliver
final report to GMCB
• Document and socialize confirmed
current state understanding, designed
future state, and recommended steps
to achieve future state (including pros
and cons)
• Obtain stakeholder alignment
on recommendations
Step 2. Develop current state
understanding through 1
st
round of interviews
Obtain community perspective on:
• Hospital Service Area (HSA)
characteristics
• Hospital & healthcare delivery
system performance
• Community needs
• Desired health system future state
Act 167 (of 2022) requires GMCB, in collaboration with the Agency of Human Services, to develop and conduct a data-informed, patient-focused, community-inclusive engagement
process for Vermont’s hospitals to reduce inefficiencies, lower costs, improve population health outcomes, reduce health inequities, and increase access to essential services
GMCB tasked Oliver Wyman with engaging diverse healthcare stakeholders to ascertain their 1) interactions with the health system and 2) perceived needs to improve equitable
healthcare access and outcomes
Aug-Sept 2023 Sept-Nov 2023 March – July 2024 Aug – Sep 2024
We are here
5
© Oliver Wyman
Patients
Hospitals
HCPsState legislature
/ regulations
Increase
in cost
Reduced
functional
capacity
Delayed care and
compromised care
access & quality
due to long wait /
reduced access
Critical
services/
admissions
being
declined due
to lack of
IP/ER capacity
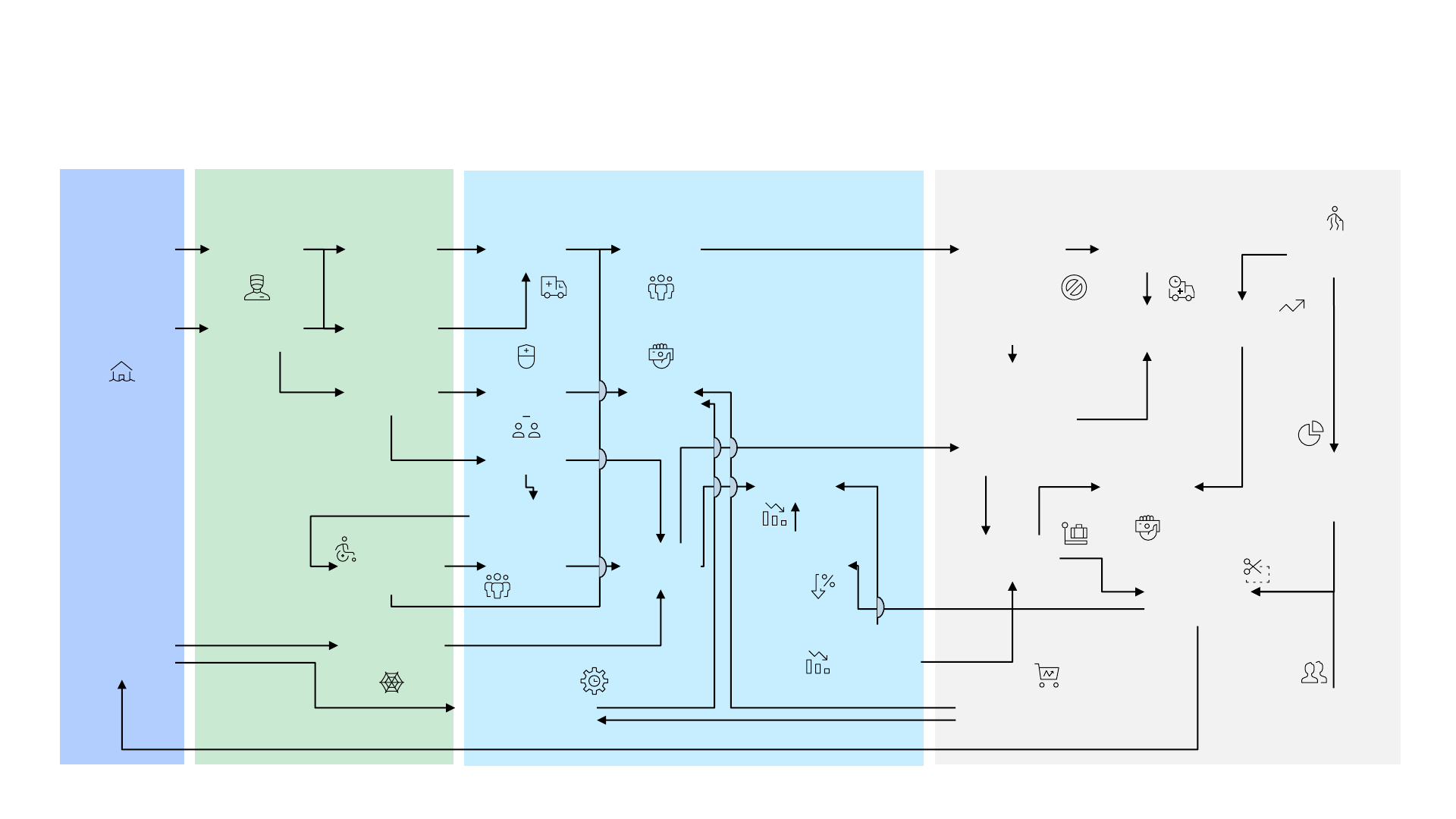
VERMONT’S HEALTHCARE CHALLENGES ARE INTER-CONNECTED AND MANY STEM FROM
IRREVERSIBLE MACRO TRENDS OUTSIDE OF THE HOSPITAL’S CONTROL
Lack
of long-term
housing
availability
Difficult to
retain HCP
Shortage
of PCPs
Shortage
of mental
health care
professionals
Shortage
of nurses
Reduction
in revenue
Patients
turn up in
ER instead
Crowding
in ER
Lack of staffed
social care facilities
Crowding
in IP
Hire travel
nurses
Difficult to
discharge
certain patients
Low CON
threshold and
long approval
process
Old equipment
are not
replaced in time
Staff
shortage
Cumbersome
licensure
requirements
Difficult to
attract HCP
Inflation and rising labor
and commodity cost
Increased
transportation
needs
Increase in
state-wide
cost
Tight hospital
reimbursement
rate
Aging
population
Shift in payer
mix – reduction
in commercial
insurance
Increase
in healthcare
demand
Long
ambulance
wait
Cost-effective
contracts cannot be
secured due to long
approval process
Reduction
in in-state
dollars to pay
for healthcare
Many go out-
of-state to
seek care
Shrinking
population
Lower
procedure
volumes and
care quality

6
© Oliver Wyman
THE SIMPLE CONCLUSION IS TO ALLEVIATE SYMPTOMS BY INCREASING FUNDING AND
HEALTHCARE PROVISION, BUT IT WOULD NOT BE AFFORDABLE NOR EFFICIENT TO DO SO
Solving for symptoms of healthcare pain points: Because…
But this requires:
❑ Higher taxation
❑ Higher commercial
insurance
❑ Increased co-pays and
deductible
...
Rural nature of Vermont and shrinking population means that,
in many parts of the state, the population size and density do
not support a hospital with full-time full-spectrum of
specialties being sustained
Vermont OOP max, deductibles, and Commercial premiums
are already high and Vermonter cannot afford to see annual
double digit growth in insurance payments. Higher taxation is
also not a viable solution as they will likely drive residents and
businesses out of state
Shrinking population (and proportionally fewer younger
people entering the medical profession). System-wide supply
of medical professionals is unlikely to increase, so increasing
demand will just increase price
And implies:
❑ Lower efficiency due to
lower population density
❑ Lower care quality due to
lack of sufficient volume to
main physician expertise
…
Easy solution
More funding to get more providers to meet access needs
Difficult to get PCP
appointments
Long ambulance waitLong wait in the ER
Long wait to get
elective procedures
Difficult to travel
to care site
…
Diverse populations
and health equity
7
© Oliver Wyman
STRATEGIC IMPERATIVES IN REDESIGNING VERMONT’S HEALTH CARE SYSTEM
Accept the new reality and adapt
Change what we can
Improve access and equity
Act fast before it’s too late and sustain consistent efforts over time
Strategic
imperatives
1
2
3
5
Ensure financial sustainability to Vermonters, the state and providers
4
in redesigning Vermont’s
healthcare system
8
© Oliver Wyman
WE NEED A DIFFERENT SOLUTION THAT FULFILS HEALTHCARE NEEDS, BUT SLIGHTLY
DIFFERENTLY FROM HOW HEALTHCARE PROVISION LOOKS TODAY
Fully embedded use of
updated and modern
information technology
Increased use of
community
-based, mobile
and alternative sites of care
Modernized and reformed
EMS
More
regional referral to
specialized centers
Complete development of
population health with
linked payment
The future healthcare in Vermont will focus on early identification and treatment of illness
and patient being able to obtain care at
the most appropriate level
9
© Oliver Wyman
SUMMARY OF HIGH-LEVEL STATE-WIDE RECOMMENDATIONS
Improve transportation
– For community members to and from acute and urgent appointments and from the ED
– For patients with appropriate means of transport between facilities (EMS and other types of transportation)
Build housing
– For the unhoused and under-housed
– For special group needs
– For people recruited to work in Vermont
Enlarge workforce and improve utilization
Administrative simplification
– Align AHS agencies with HSA boundaries and meet regularly with hospitals and providers
– Fully computerize and integrate AHS services
Improve access to appropriate levels of care in each community
– Reconfigure provider resources to better meet community need and achieve financial stability

10
© Oliver Wyman
HOUSING, PROFESSIONAL EMT, CAPACITY FOR SOCIAL CARE, AND TRANSLATION SERVICES
NEED KEY EARLY ACTION FOCUS TO ENSURE A SOLID FOUNDATION FOR OTHER INITIATIVES
Training
Affordable & Equitable Access to Healthcare
Work
force
Transportation Provider infrastructure
Payment
Productivity
• EMR optimization
• Adequate support staff
Funding
Housing
Licensure
Availability of
appropriate
transportation
• EMS
• Non-emergent
Viability
• Financial
• Operational
Affordability
Professional EMTs
Regionalized EMS
Modernized facility
Coordinated planning between providers and state
agencies
Capacity for home
health, long-term
care, and community-
based MH & SUD
Choice of most
appropriate care site
Transparency of cost
of care
Translation services
Early action priorities
Key area to optimize
Key pillars
Goal
Key components
missing
11
© Oliver Wyman
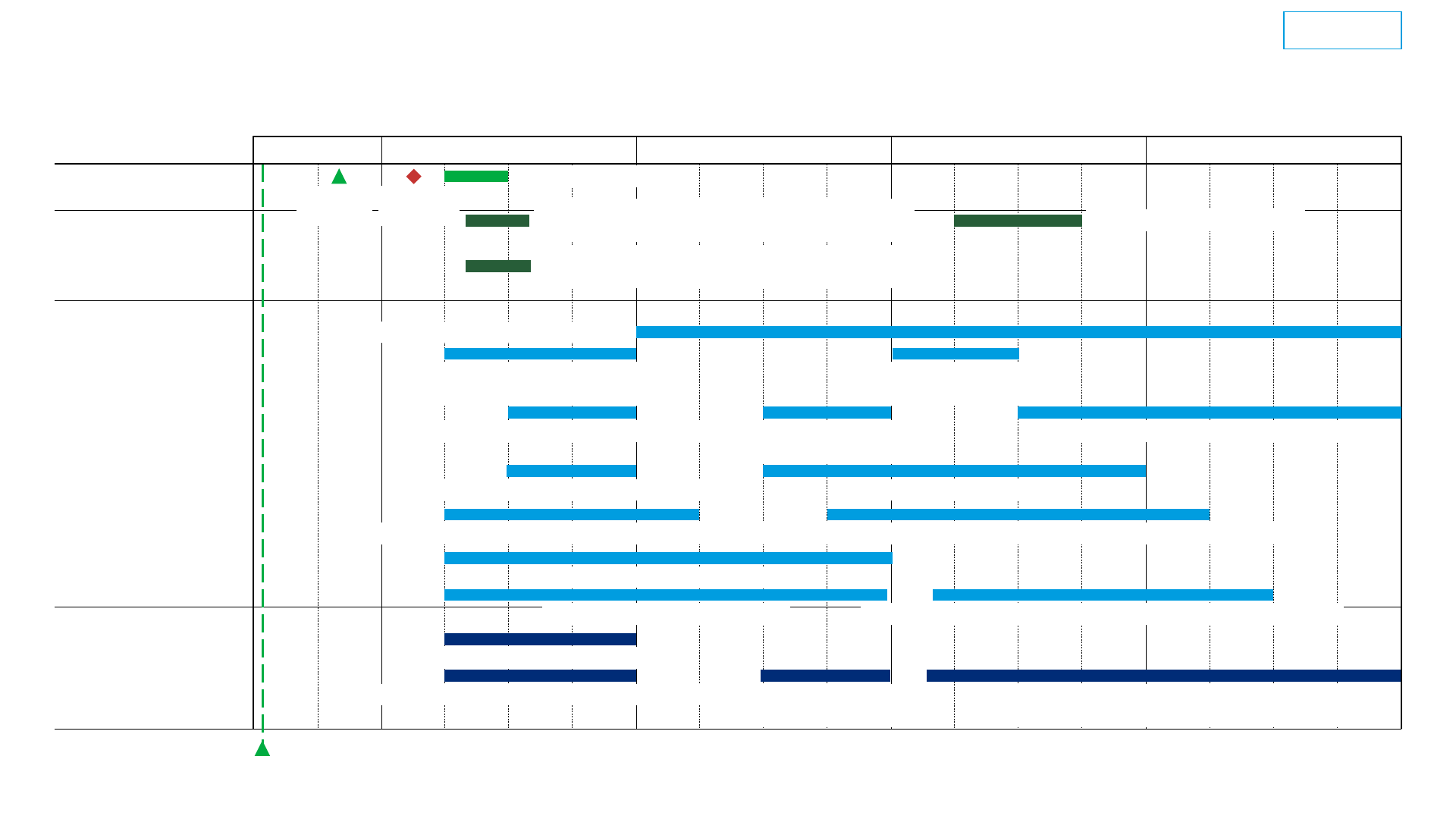
THE RUNWAY TO CHANGE WILL TAKE AT LEAST 4-5 YEARS TO COMPLETE
Illustrative action timeline, assuming positive decision to change according to current recommendation
2024 2025 2026 2027 2028
Improve VITL clinical data access
Improve rural internet coverage
Embed upgraded EMR system in each provider office’s workflow
Enhance local training programs and increase workforce pathways
Hospital actions
Revise licensure for MH professionals, pharmacists, APRN
DHMC and UVM to codify clinic notes
State-facilitated regionalization discussions
IT infrastructure
Hospital-specific
transformation plan
Conduct transformation (e.g. EMR integration,
workforce re-allocation, embed referral SOP etc)
Funding alignment
Activity
Conduct EMS transformationAlign 2026 budget plan to coordinated services
Service re-alignment
Enhance non-clinic non-hospital care provisionRealign healthcare services
to HSA boundaries
Devise AHS service-coordination plan
Reimbursement re-design
Implement primary care
incentive change for FY27
Devise and test primary care /
hospital incentive alignment model
Housing
We are here
Build low income and group housing
Licensure & training
State agency actions
Devise action plan
Approve increased care capacity and funding
for Mental Health, Long-term Care and Telehealth
Legislative actions
Obtain federal waiver (if any)
Change plan
Report
publication
Decision to
transform
Approve zoning/environmental regulation change
and funding for EMS transformation
Illustrative
12
© Oliver Wyman
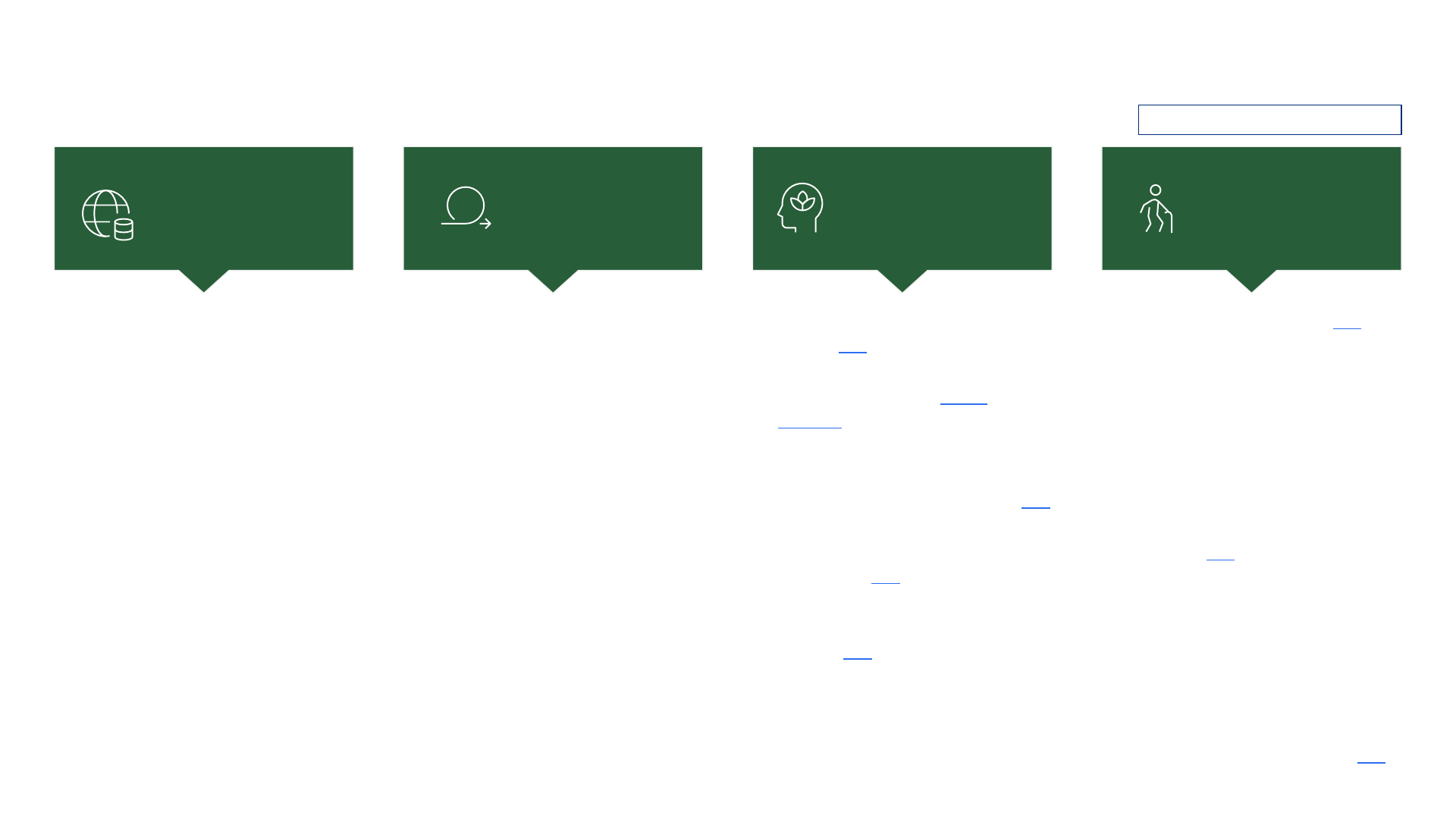
✓ Improved master patient index
✓ 5-year strategic plan
❑ ‘Unified data space’ data
aggregator
❑ Provider single sign-on
❑ Co-develop use case with providers
❑ Provider ‘self-help’ data analysis
tool
❑ Collaborate with payers to obtain
pharmacy data
❑ Modernize integrating enrolment
eligibility (legislative effort, 5-year
runway)
✓ Joined social work compact
(effective upon passing)
✓ Joined counselling and PSYPACT
(effective 1 July upon approval)
✓ Allowed bachelor-level mental
health professionals to obtain
license in VT
✓ In 2020, approved short-term
prescription extension by
pharmacist (until consultation, up
to 5 days, one time only)
❑ Act 117 to review MH licensure in
VT to streamline and further
remove barriers to licensure (study
due Dec’24)
✓ Age Strong Vermont Plan (link)
✓ SNF bed board (from March’24)
✓ 3 Adult Services Division complex
care nurses to help with care
coordination
✓ Nursing facility retrospective rate
adjustments
✓ Rate review for residential care,
assisted living, home health, and
adult day (link)
✓ Root cause analysis for hospital
case managers to address complex
discharges
❑ Further expedite new application
process for long-term care
Medicaid eligibility process
❑ Reduce minimum occupancy
threshold on nursing homes (link)
❑ Seek to bring iCare to Vermont
MANY INITIATIVES ARE UNDERWAY TO TACKLE THE SYSTEM-WIDE CHALLENGES
Medical data
infrastructure
improvement
Licensure
streamlining
Mental health /
substance use
support
Elderly care
support
Select initiatives only, non-exhaustive
✓ Mobile crisis response (since
Jan’24, link)
✓ New psychiatric residential
treatment facilities (youth,
forensic)
✓ Centralized dispatch from 988
✓ 6 new delivery system projects,
funded by $100k by OneCare (link)
✓ $1 million, one-year CCBH
Planning Grant (extended to
March’25) (link)
✓ DMH Vision 2030 on MH
integration across the healthcare
setting (link)
❑ DMH global referral checklist
❑ Seek alternative to hospital-based
administration of court ordered
medication
Key: ✓ Completed ❑ Ongoing

13
© Oliver Wyman
HOWEVER, DEEPER STRUCTURAL CHANGES NEED TO BE ACTIONED NOW TO AVOID
DEVASTATING FINANCIAL DIPS
Deeper structural
reform
Momentum of current efforts needs to
be scaled up to deliver structural reforms
in addition to patch solutions
Support local
change
Local health organizations will need
support in transitioning to new
operational models
Expedited
action
Vermont must act now with urgency to
complete structural changes in the next
5 years. Hospital systems and the state
will see deep financial deficits if no
structural reform is achieved by then
14
© Oliver Wyman
NEXT STEP: GMCB BOARD MEETING ON HEALTH SYSTEM RECOMMENDATIONS AND
COMMUNITY MEETINGS IN JULY
GMCB Board meeting on
health system
recommendations
Monday, 8 July 2024
10:00am – 12:00pm
14 in-person community
meetings
9 July 2024 – 1 Aug 2024
See GMCB website for details
1
1. https://gmcboard.vermont.gov/Act-167-Community-Meetings
Virtual community
meeting (state-wide)
5 Aug 2024
6:00pm - 7:30pm
1
