
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
National Health Interview Survey (NHIS)
Early Release Program
Preliminary Evaluation of the Impact of the
2019 National Health Interview Survey
Questionnaire Redesign and
Weighting Adjustments on
Early Release Program Estimates
Division of Health Interview Statistics
National Center for Health Statistics
Hyattsville, Maryland
Centers for Disease Control and Prevention
U.S. Department of Health and Human Services
Updated September 2020

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 2
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Table of Contents
Introduction ............................................................................................................................................................... 3
2019 NHIS Questionnaire Redesign ........................................................................................................................... 4
Weighting Adjustments ............................................................................................................................................. 5
NHIS Early Release Program ...................................................................................................................................... 6
Analytic Approach ..................................................................................................................................................... 8
Results ..................................................................................................................................................................... 12
Diagnosed Hypertension ................................................................................................................................... 12
Asthma Episode ................................................................................................................................................ 14
Regularly Experienced Chronic Pain ................................................................................................................. 16
Regularly Had Feelings of Worry, Nervousness, or Anxiety .............................................................................. 18
Regularly Had Feelings of Depression ............................................................................................................... 20
Disability Status ................................................................................................................................................. 22
Current Cigarette Smoking ................................................................................................................................ 24
Current Electronic Cigarette Use ...................................................................................................................... 26
Did Not Get Needed Medical Care Due to Cost ................................................................................................ 28
Did Not Take Medication as Prescribed to Save Money ................................................................................... 30
Did Not Get Needed Mental Health Care Due to Cost ..................................................................................... 32
Doctor Visit ....................................................................................................................................................... 34
Hospital Emergency Department Visit .............................................................................................................. 36
Influenza Vaccination ........................................................................................................................................ 38
Blood Pressure Check ........................................................................................................................................ 40
Health Insurance Coverage ............................................................................................................................... 41
Adults Living in Wireless-Only Households ....................................................................................................... 45
Summary .................................................................................................................................................................. 46
References ............................................................................................................................................................... 48
Suggested citation:
National Center for Health Statistics. Preliminary evaluation of the impact of the 2019 National Health Interview
Survey questionnaire redesign and weighting adjustments on Early Release Program estimates. Hyattsville,
Maryland. September 2020.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 3
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Introduction
The National Center for Health Statistics’ (NCHS) National Health Interview Survey (NHIS) provides information
on the health of the civilian noninstitutionalized population of the United States through confidential interviews
conducted in households. NHIS is the nation’s oldest ongoing household-based health survey. Since 1957, it has
provided data for analyzing health trends and tracking progress toward achieving national health objectives.
In 2019, for the first time in over 20 years, the NHIS questionnaire was redesigned to increase relevance,
enhance data quality, and minimize respondent burden. The wording of some questions and answer choices was
revised to improve quality of measurement. Some questions were dropped, and others were added, changing
the context within which some questions were asked. And some questions are now answered directly by the
adult to which they refer, rather than a family member responding on behalf of all family members. Perhaps as a
result of these changes, response rates increased and the characteristics of nonrespondents may have changed,
so a revised and updated method of adjusting sampling weights to account for nonresponse was implemented
concurrent with the questionnaire design changes.
Any differences observed between estimates for 2018 and 2019 may be due to real change in the population or
partly attributable to the 2019 NHIS questionnaire redesign and/or the updated weighting approach. This
working paper examines the effect of methods changes on the comparability of estimates over time, looking
specifically at estimates for the key indicators that are reported as part of the NHIS Early Release Program. It
examines whether the design changes appeared to impact these key estimates by comparing differences across
designs during October-December 2018 when both the prior design and a field test for the redesign were in the
field simultaneously. Moreover, it explores the impact of the updated weighting approach by examining
differences in estimates derived with the two different weighting approaches for the same data set (the
preliminary microdata files for January-December 2019). This working paper is an update to a previous version
of this report that was released on May 28, 2020; this update includes 2019 full-year Early Release estimates.
The potential impact of weighting and design effects will be further evaluated when final data become available.
This working paper is organized in the following manner. It starts with an overview of the questionnaire
redesign and how the structure of the questionnaire differs from the prior questionnaire design. Next, it briefly
describes the changes to the weighting approach. Then, it provides a description of the NHIS Early Release
Program. Following this background information, additional details are provided about the methods used to
examine whether the NHIS questionnaire redesign and updated weighting approach impacted the key estimates
from the Early Release Program. Results are then presented for each indicator and summarized at the end.
Preliminary conclusions are included in the results section regarding whether or not the 2019 NHIS
questionnaire redesign and the updated weighting approach were likely to have had an impact on each
indicator. These conclusions are based on the magnitude of the observed effect. The results of statistical
significance testing are reported and considered, but conclusions are not solely based on this testing.
When an impact of the questionnaire redesign and/or the updated weighting approach is likely, it may not be
appropriate to conclude that any observed difference or lack of difference reflects actual change or no change
over time. The conclusions presented here are preliminary and will be revisited in future NCHS reports. How the
findings of this report should be applied to specific analyses may vary depending on the objectives of that
analysis. The findings are provided to users so that they can make informed decisions about the use of the data.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 4
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
2019 NHIS Questionnaire Redesign
The content and structure of the NHIS were updated in the redesign to better meet the needs of data users.
Aims of the redesign were to improve the measurement of covered health topics, reduce respondent burden by
shortening the length of the questionnaire, harmonize overlapping content with other federal health surveys,
establish a long-term structure of ongoing and periodic topics, and incorporate advances in survey methodology
and measurement.
One “sample adult” aged 18 years or older and one “sample child” aged 17 years or younger (if any children live
in the household) are randomly selected from each household following a brief initial interview that identifies
everyone who usually lives or stays in the household. Information about the sample adult is collected from the
sample adult herself or himself unless she or he is physically or mentally unable to do so, in which case a
knowledgeable proxy can answer for the sample adult. Information about the sample child is collected from a
parent or adult who is knowledgeable about and responsible for the health care of the sample child. This
respondent may or may not also be the sample adult.
From 1997-2018, the NHIS also included a family questionnaire. Questions from the family questionnaire,
including questions on health insurance and unmet needs for medical care, were answered by a member of the
family on behalf of all members of the family. In the redesigned survey, much of the content that was collected
about the sample adult and sample child in the family section is now collected within the sample adult and
sample child questionnaires, from the sample adult or sample child’s respondent rather than another family
member. Sample adults may give different answers about themselves than would a family member responding
for them, and this could impact survey estimates.
The elimination of the family questionnaire was one part of an effort to shorten the length of the questionnaire.
In addition, questions on rare conditions or service utilization (those with less than a 2% prevalence), questions
on topics that were no longer priorities, and questions that were rarely used in analysis were dropped. A
structure of annual and rotating content was also implemented. The annual core contains the same questions
from year to year, and these questions focus on demographic characteristics, health insurance, chronic
conditions, health care access and use, health-related behaviors, and functioning and disability. The rotating
core consists of questions that will be included in the interview periodically and include expanded content on
mental health, service utilization, preventive services, health-related behaviors, injuries, and chronic pain. The
periodicity of questions in the rotating core varies by question and may be every-other year, once-every-three
years, or two-out-of-three years.
As a result of dropping questions and putting others on a rotating schedule, along with the addition of new
questions reflecting new priorities, the question order and the context of most questions (that is, the questions
that come immediately before) changed with the questionnaire redesign. These changes can affect how
subsequent questions are interpreted and responded to, and these effects could impact survey estimates.
For more details about the NHIS questionnaires, go to:
https://www.cdc.gov/nchs/nhis/data-questionnaires-
documentation.htm.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 5
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Weighting Adjustments
NHIS is a sample survey. That is, only a sample (subset) of the civilian noninstitutionalized population is selected
to participate in the survey. Additionally, not everyone selected to participate agrees to participate, which
affects the representativeness of the sample. In order to account for these two factors, sampling weights are
created. These sampling weights are used to produce representative national estimates. The weights reflect
several steps of adjustments starting with a base weight, which is inverse to the probability of selection.
Households or persons that are more likely to be selected are given lower weights so that the final estimates are
not biased by their increased likelihood of being selected.
These base weights are then adjusted for nonresponse patterns, or the different response rates among different
household and person-level subgroups. The 2019 questionnaire redesign provided an opportunity to evaluate
the adjustment approach that had been in place since 1997. At that time and continuing through 2018, the
adjustment approach was based on geography; the weights for households and persons in geographic areas
with lower response rates were increased more than for those in areas with higher response rates. That way,
final estimates were not biased by the latter group’s increased likelihood of participation. More sophisticated
methods are now available (1, 2), and based on the evaluation, the weighting process for 2019 was updated. The
updated approach for nonresponse adjustment uses multilevel regression models that consider numerous
variables that are predictive of both survey response and selected key health outcomes, the key criteria for
effective bias reduction.
Finally, the nonresponse adjusted weights are calibrated to U.S. Census Bureau population projections and
American Community Survey (ACS) one-year estimates for age, sex, race and ethnicity, educational attainment,
Census division, and Metropolitan Statistical Area status. Prior to 2019, calibration was only to age, sex, and race
and ethnicity population projections. These changes to the nonresponse adjustment approach and the
calibration methods have the potential to impact the weighted survey estimates.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 6
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
NHIS Early Release Program
Since its inception in 2001, the NHIS Early Release Program provides the public with estimates, analytic reports,
and preliminary microdata files on an expedited schedule. NHIS data users can have access to these timely
estimates, reports, and preliminary microdata files on selected key health indicators without having to wait for
the release of the final annual NCHS microdata files. Table 1 summarizes the 19 indicators that were included in
the Early Release Program prior to the 2019 NHIS questionnaire redesign and the calendar year that they were
added to the Early Release Program.
Table 1. Key indicators included in the NHIS Early Release Program prior to
the 2019 questionnaire redesign, by topic subgroup and calendar year
introduced to the Early Release Program
Indicators Calendar Year
Health Status
General health status 2001
Needing help with personal care from other persons 2002
Obesity 2001
Serious psychological distress 2003
Diagnosed diabetes 2003
Current asthma 2004
Asthma episode 2003
Health Behaviors
Excessive alcohol consumption 2001
Current smoking 2001
Leisure-time physical activity 2001
Health Care Access
Usual source of medical care 2001
Unable to obtain needed medical care due to cost 2001
Health Care Service Utilization
HIV testing 2001
Influenza vaccination 2001
Pneumococcal vaccination 2001
Health Insurance Coverage
Lack of health insurance 2001
Public health plan coverage 2002
Private health insurance coverage 2002
Telephone Ownership
Adults living in wireless-only households 2007
These estimates were released as a series of three products. On a quarterly basis, cumulative preliminary
estimates of health insurance coverage and selected key health indicators were published. On a bi-annual basis,
six-month estimates on the prevalence of adults living in households with only wireless telephone service were
published.
As part of the 2019 NHIS questionnaire redesign, the Early Release Program content was reviewed. With input
from the NCHS Board of Scientific Counselors and NCHS leadership, 18 key health indicators were selected from
the redesigned questionnaire to include in the Early Release Program in addition to the established content on
health insurance coverage and telephone ownership. Table 2 summarizes these 22 indicators and the calendar
year that they were added to the Early Release Program.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 7
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Table 2. Key indicators included in the redesigned NHIS Early Release Program, by topic
subgroup and calendar year introduced to the Early Release Program
Indicators Calendar Year
Health Status
Diagnosed hypertension in the past 12 months 2019
Asthma episode in the past 12 months 2003
Six or more workdays missed due to illness, injury or disability in the past 12 months 2019
Regularly experienced chronic pain 2019
Regularly had feelings of worry, nervousness, or anxiety 2019
Regularly had feelings of depression 2019
Disability status 2019
Health Behaviors
Current cigarette smoking 2001
Current electronic cigarette use 2019
Health Care Access
Did not get needed medical care due to cost in the past 12 months 2001
Did not take medication as prescribed to save money in the past 12 months 2019
Did not get needed mental health care due to cost in the past 12 months 2019
Health Care Service Utilization
Doctor visit in the past 12 months 2019
Hospital emergency department visit in the past 12 months 2019
Receipt of influenza vaccination in the past 12 months 2001
Blood pressure check in the past 12 months 2019
Counseled by a mental health professional in the past 12 months 2019
Dental exam or cleaning in the past 12 months 2019
Health Insurance Coverage
Lack of health insurance 2001
Public health plan coverage 2002
Private health insurance coverage 2002
Telephone Ownership
Adults living in wireless-only households 2007
Eight (42.1%) of the original 19 Early Release indicators were retained as part of the Early Release Program
(asthma episode, cigarette smoking, did not get needed medical care due to cost, influenza vaccination, lack of
health insurance, public health plan coverage, private health insurance coverage, and adults living in wireless-
only households). Fourteen new measures complemented these topics while also addressing timely and
important aspects of health and well-being, such as functioning and disability, mental health, electronic
cigarette use, and strategies used to reduce prescription drug costs. The selected measures generally reflect
current or recent health status or experiences with the health care system, may be sensitive to policy changes,
and are representative of important issues such as preventive care and cost-related barriers to care. Timely data
on the prevalence of adults living in wireless-only households is important for health survey researchers using
telephone surveys, to ensure that they adequately represent this population in their samples.
While data on each of these 22 measures were available prior to the 2019 questionnaire redesign, changes to
the wording of the questions and response options, changes to the location and context of the questions, and
changes in who answered the questions could affect the estimates and explain (at least in part) any observed
differences between 2018 and 2019. For three of these new Early Release indicators—“workdays missed”,
“dental exam or cleaning” and “counseled by a mental health professional”—the changes to both the location
and wording of the questions were so substantial that no comparison between 2018 and 2019 is recommended.
However, for the remaining 19 indicators, the changes to the location, wording, or respondent were relatively
minor. Nevertheless, for these indicators, a preliminary evaluation was conducted to assess whether the

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 8
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
questionnaire redesign, the weighting process, or both had an observable impact on the overall national
estimates.
Analytic Approach
As described earlier, the goal of this analysis is to determine how the comparability of 2018 and 2019 estimates
may have been affected by the questionnaire redesign and the change in the weighting approach. These effects
can be evaluated by examining differences among prevalence estimates that vary by questionnaire design or
weighting approach. Table 3 presents a series of five prevalence estimates (and 90% confidence intervals) for 19
Early Release indicators:
A. 2018 Production Estimates (Old Weight) – These are the official estimates for the key indicators based
on 2018 data. They were derived using the former (2018) weighting approach. Data from 25,417 sample
adults were used for these estimates.
B. 2018 Quarter 4 Production Estimates (Old Weight) – These estimates are derived in a manner similar to
the 2018 Production estimates, but they are based only on data from 4,074 sample adults that were
interviewed from October-December 2018.
C. 2018 Quarter 4 Bridge Estimates (Old Weight) – From October-December 2018, NCHS conducted a
small-scale test of the redesigned NHIS questionnaire to evaluate procedures and identify potential
problems. This test was conducted nationally; data were collected from a nationally representative
sample of 4,428 sample adults. The overlap in the data collection period of the field test with the 2018
data collection serves as a “bridge” between the two designs, and the two production periods (2018 and
2019). Estimates from this test, derived using the former (2018) weighting approach, are heretofore
referred to as bridge estimates.
D. 2019 Full-year Early Release Estimates (Old Weight) – These estimates are derived in a manner similar
to the official 2019 Early Release estimates, but they are based on application of the former (2018)
weighting approach to the data. Data from 32,391 sample adults were used for these estimates.
E. 2019 Full-year Early Release Estimates (New Weight) – These are the official estimates for the key
indicators based on Early Release data from 2019. They are derived using the updated weighting
approach. Data from 32,391 sample adults were used for these estimates.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 9
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Table 3. Key estimates (and 90% confidence intervals) for adults by time period, questionnaire design, and weighting approach
Indicator
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-
year Early
Release,
Old weight
(E)
2019 Full-
year Early
Release,
New weight
Within
2018 Q4
Difference
(C - B)
Weighting
Difference
(E - D)
Health Status
Diagnosed hypertension 27.0
(26.4 - 27.6)
27.4
(26.0 – 28.7)
25.6
(24.4 – 26.9)
26.6
(26.0- 27.1)
27.1
(26.6 - 27.7)
-1.8 0.5
Asthma episode 3.5
(3.3 - 3.8)
3.8
(3.2 - 4.5)
3.5
(3.1 - 4.0)
3.3
(3.1 - 3.6)
3.4
(3.1 - 3.6)
-0.3 0.1
Regularly experienced chronic pain 20.7
(20.2 - 21.3)
21.6
(20.3 – 22.9)
19.7
(18.6 – 20.8)
20.0
(19.5 - 20.5)
20.6
(20.1 - 21.2)
-1.9‡ 0.6
Regularly had feelings of worry, nervousness, or anxiety 8.6
(8.2 – 9.0)
9.0
(8.0 - 10.0)
11.1
(10.2 – 12.0)
10.9
(10.6 - 11.3)
11.2
(10.8 - 11.5)
2.1* 0.3
Regularly had feelings of depression 4.4
(4.2 – 4.7)
4.7
(4.1 – 5.4)
4.2
(3.7 – 4.8)
4.6
(4.4 - 4.8)
4.7
(4.5 - 5.0)
-0.5 0.1
Disability status 10.2
(9.8 - 10.6)
9.9
(9.0 - 10.8)
8.9
(8.1 - 9.7)
8.6
(8.3 - 9.0)
9.2
(8.8 - 9.6)
-1.0 0.6‡
Health Behaviors
Current cigarette smoking 13.7
(13.3 - 14.2)
13.3
(12.3 - 14.4)
12.8
(11.8 – 13.8)
13.2
(12.8 - 13.7)
14.2
(13.8 - 14.7)
-0.5 1.0**
Current electronic cigarette use 3.2
(3.0 - 3.5)
3.3
(2.7 – 3.9)
4.3
(3.7 - 5.0)
4.3
(4.0 - 4.6)
4.4
(4.1 - 4.7)
1.0‡ 0.1
Health Care Access
Did not get needed medical care due to cost 6.4
(6.1 - 6.7)
6.3
(5.6 - 7.0)
8.2
(7.2 - 9.3)
7.8
(7.5-8.2)
8.3
(8.0-8.7)
1.9* 0.5‡
Did not take medication as prescribed to save money 9.2
(8.8 - 9.7)
9.2
(8.1 - 10.3)
9.1
(8.2 - 10.2)
9.2
(8.7-9.6)
9.7
(9.2-10.1)
-0.1 0.5
Did not get needed mental health care due to cost 2.6
(2.4 - 2.9)
3.4
(2.8 - 4.0)
4.9
(4.3 - 5.6)
4.4
(4.1-4.6)
4.3
(4.1-4.6)
1.5** -0.1
Health Care Service Utilization
Doctor visit 84.3
(83.8 – 84.9)
85.2
(83.9 - 86.4)
84.2
(82.9 - 85.4)
85.2
(84.8 - 85.6)
84.9
(84.5 - 85.3)
-1.0 -0.3
Hospital emergency department visit 21.3
(20.8 – 21.9)
21.3
(20.0 - 22.6)
21.8
(20.6 - 23.0)
21.3
(20.8 - 21.7)
21.8
(21.4 - 22.3)
0.5 0.5
Influenza vaccination 44.6
(43.9 - 45.3)
44.2
(42.6 – 45.9)
45.0
(43.4 - 46.5)
47.8
(47.0 - 48.5)
46.8
(46.1 - 47.5)
0.8 -1.0
Blood pressure check 84.6
(84.1 - 85.1)
85.8
(84.6 - 87.0)
86.6
(85.4 - 87.7)
88.3
(87.9 - 88.8)
88.1
(87.6 - 88.5)
0.8 -0.2
See footnotes at end of table.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 10
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Table 3. Key estimates (and 90% confidence intervals) for adults by time period, questionnaire design, and weighting approach, cont.
Indicator
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-
year Early
Release,
Old weight
(E)
2019 Full-
year Early
Release,
New weight
Within
2018 Q4
Difference
(C - B)
Weighting
Difference
(E - D)
Health Insurance Coverage (18-64 years)
1
Lack of health insurance 13.3
(12.6 – 13.9)
14.0
(13.0 - 15.1)
13.8
(12.1 - 15.5)
13.8
(13.2 - 14.4)
14.7
(14.0 - 15.3)
-0.2 0.9‡
Public health plan coverage 19.4
(18.9 - 20.0)
18.6
(17.5 – 19.7)
17.5
(16.2 – 18.8)
19.0
(18.4 - 19.7)
20.4
(19.7 - 21.1)
-1.1 1.4*
Private health insurance coverage 68.9
(68.2 - 69.7)
68.7
(67.3 - 70.1)
71.0
(69.2 – 72.7)
69.0
(68.2 - 69.8)
66.8
(65.9 - 67.7)
2.3‡ -2.2**
Telephone Ownership
Adults living in wireless-only households 56.0
(55.2 - 56.8)
57.0
(55.5 - 58.6)
58.0
(56.5 - 59.5)
59.9
(58.9 - 60.9)
60.2
(59.2 - 61.2)
1.0 0.3
‡
p < 0.10; *p < 0.05; **p < 0.01
1
For the health insurance coverage indicators, the 2018 full-year production and 2018 quarter 4 production estimates are preliminary estimates from the National Health
Interview Survey Early Release Program, rather than final estimates. See text for further information.
SOURCES: NCHS, National Health Interview Survey, 2018, 2018 Quarter 4 Test, and 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 11
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Health policy analysts and other public health professionals are generally interested in whether there are
changes over time in the official estimates for the key indicators. That is, they will want to know whether the
2019 estimates are higher, lower, or statistically similar to the 2018 estimates. However, as noted earlier, any
differences observed between estimates for 2018 (Column A) and 2019 (Column E) may be partly attributable to
the 2019 NHIS questionnaire redesign, the updated weighting approach, or both, or they may reflect an actual
change over time. If questionnaire design effects or weighting effects are observable, it may not be appropriate
to compare the 2018 and 2019 estimates and conclude that the observed difference (or lack of difference)
reflects an actual change (or lack of change) over time. Health policy analysts are also interested in longer term
trends in addition to year-to-year changes. While design or weighting changes may affect year-to-year
comparisons, these changes may have less impact on ascertaining longer term trends.
Table 3 highlights two comparisons of interest in assessing the potential effect of the questionnaire redesign and
updated weighting approach on the official estimates. First, for each indicator, the potential effect of the
questionnaire design was examined by comparing estimates across designs during October-December 2018, a
time when both the prior design and the field test of the redesign were in the field simultaneously. That is, the
2018 Quarter 4 Production estimate (Column B) was compared to the 2018 Quarter 4 Bridge estimate (Column
C), and the statistical significance was tested. The same weighting approach was used for both data sets.
Second, for each indicator, the potential impact of the updated weighting approach was examined by comparing
estimates derived with the two different weighting approaches for the same data set. That is, the 2019 Full-year
Early Release estimate based on the old weight (Column D) was compared to the 2019 Full-year Early Release
estimate based on the new weight (Column E), and the statistical significance was tested. In this analysis, both
estimates are derived from the same questionnaire design.
Third, for each indicator, the potential impact of both the questionnaire redesign and updated weighting
approach on longer-term trends was explored by examining changes in six-month interval estimates from 2015-
2019. These line graphs, along with the information presented in Table 3, help evaluate longer-term trends
through 2019. The figures show the observed estimates for each time period and the predicted estimate if no
methodological changes had been made based on the net effect of the design and weighting changes. Note that
the predicted estimates are subject to sampling error (not shown on the figures) and will differ from what would
have been observed had no changes been made in 2019. Conclusions as to the extent of the impact of the
design and weighting changes on trends or differences between 2018 and 2019 should take this into
consideration. Detailed information on the effect of the methodologic changes is provided so readers can reach
their own conclusions as to how to interpret trends. The comparison between the January-June 2019 and July-
December 2019 estimates describes any change occurring during the calendar year. This information can be
used in conjunction with changes during the previous period to determine whether an existing increasing or
decreasing trend may have continued through 2019 in light of possible methodological impacts.
All statistical tests used a two-sided alpha level of 0.10 rather than the conventional 0.05 level to determine
statistical significance. This decision leads to identification of more significant differences and more conservative
conclusions. That is, one is more likely to conclude that questionnaire design effects and weighting effects exist
for a greater number of variables. This approach is a reasonably cautious one, suitable for this look at
preliminary data and the relatively small sample sizes available for the 2018 Quarter 4 comparisons. Readers
who wish to use an alternative approach will find the actual p-values identified in the text and footnotes for
alpha levels of 0.05 and 0.01 in the tables.
Reports from the Early Release Program for key health indicators have generally presented both unadjusted
(crude) and age-adjusted estimates in tables, but only unadjusted estimates when examining trends over time.
Similarly, the estimates and comparisons presented here are based on unadjusted estimates only.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 12
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Results
Diagnosed Hypertension
Questionnaire changes between 2018 and 2019: This indicator is based on a series of questions that ask sample
adult respondents if they have a) ever been told by a doctor or health professional that they had hypertension,
b) been told on two or more different visits that they had hypertension, c) had hypertension during the past 12
months, or d) are now taking any medication prescribed by a doctor for their high blood pressure. In 2018, there
was an additional question that asked whether any medicine was ever prescribed by a doctor for their high
blood pressure. This additional question preceded the current medication question, and the current medication
question was only asked among those that responded yes to the preceding question. The 2019 NHIS did not ask
about whether medicine was ever prescribed by a doctor but included the other four questions as in 2018.
This indicator is new to the Early Release Program and reflects sample adults who either a) had been told they
had hypertension on two or more doctor visits and had hypertension during the past 12 months, or b) had ever
had hypertension and are now taking medication for their high blood pressure.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
27.0
(26.4 - 27.6)
27.4
(26.0 – 28.7)
25.6
(24.4 – 26.9)
26.6
(26.0- 27.1)
27.1
(26.6 - 27.7)
-1.8 0.5 -1.3
Preliminary analysis:
• In 2018, the percentage of adults who had diagnosed hypertension in the past 12 months or were taking
medication to control it was 27.0%. In 2019, the full-year estimate with the new weight was 27.1% (see
Table). This difference was not statistically significant (p = 0.84).
• During the fourth quarter of 2018, the production estimate (27.4%) was 1.8 percentage points higher
than the bridge estimate (25.6%). This difference suggests a possible questionnaire design effect, but it
did not reach statistical significance (p = 0.11).
• The 2019 full-year estimate with the old weight (26.6%) was lower than, but not significantly different
from, the 2019 full-year estimate with the new weight (27.1%). This result (p = 0.28) suggests that the
weighting adjustment was unlikely to affect estimates for this indicator.
• Considered together, estimates for 2019 may have shifted downward by 1.3 percentage points due to
the methodological change. This shift may have masked an actual increase from 2018 to 2019.
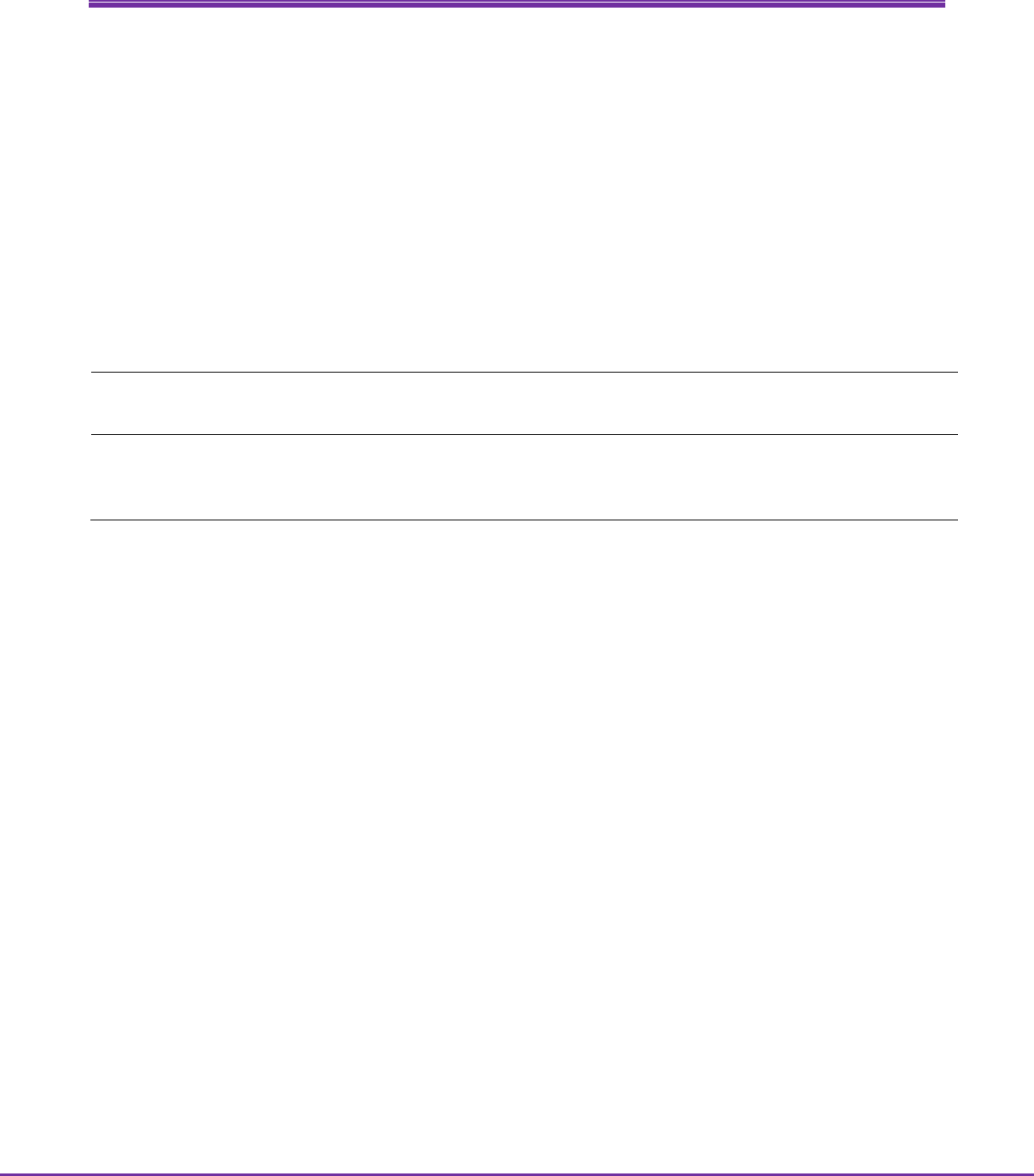
• There is no clear trend from 2015 to 2018 (see Figure). Given the potential impact of the change in the
methodology, it is not possible to determine if there was an actual increase between 2018 and 2019.
• The observed increase from January-June 2019 (26.8%) to July-December 2019 (27.5%) would be
consistent with an increase starting in 2018. However, the observed increase between the two six-
month estimates was not statistically significant (p = 0.26).

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 13
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults with diagnosed hypertension
27.1
26.1
26.6
26.9 26.9
26.1
27.2
26.9
26.8
27.5
28.1
28.8
0
5
10
15
20
25
30
35
40
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 14
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Asthma Episode
Questionnaire changes between 2018 and 2019: The two questions used for this indicator were unchanged
from 2018 to 2019. Sample adult respondents were asked, “Have you ever been told by a doctor or other health
professional that you had asthma?” If yes, they were asked “During the past 12 months, have you had an
episode of asthma or an asthma attack?”
This indicator is one of eight from the original Early Release Program and reflects sample adults who had an
asthma episode or attack in the past 12 months.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
3.5
(3.3 - 3.8)
3.8
(3.2 - 4.5)
3.5
(3.1 - 4.0)
3.3
(3.1 - 3.6)
3.4
(3.1 - 3.6)
-0.3 0.1 -0.2
Preliminary analysis:
• In 2018, the percentage of adults who had an asthma episode or attack in the past 12 months was 3.5%.
The 2019 full-year estimate with the new weight was 3.4% (see Table). This difference was not
statistically significant (p = 0.61).
• During the fourth quarter of 2018, the production and bridge estimates for this indicator were similar
(3.8% and 3.5%, respectively). This result (p = 0.53) suggests that a questionnaire design effect is
unlikely.
• The 2019 full-year estimates using the old and new weights were similar (3.3% and 3.4%, respectively).
This result (p = 0.60) suggests that the weighting adjustment did not substantially affect estimates for
this indicator.
• Considered together, estimates for 2019 may have shifted downward by 0.2 percentage points due to
the methodological change.
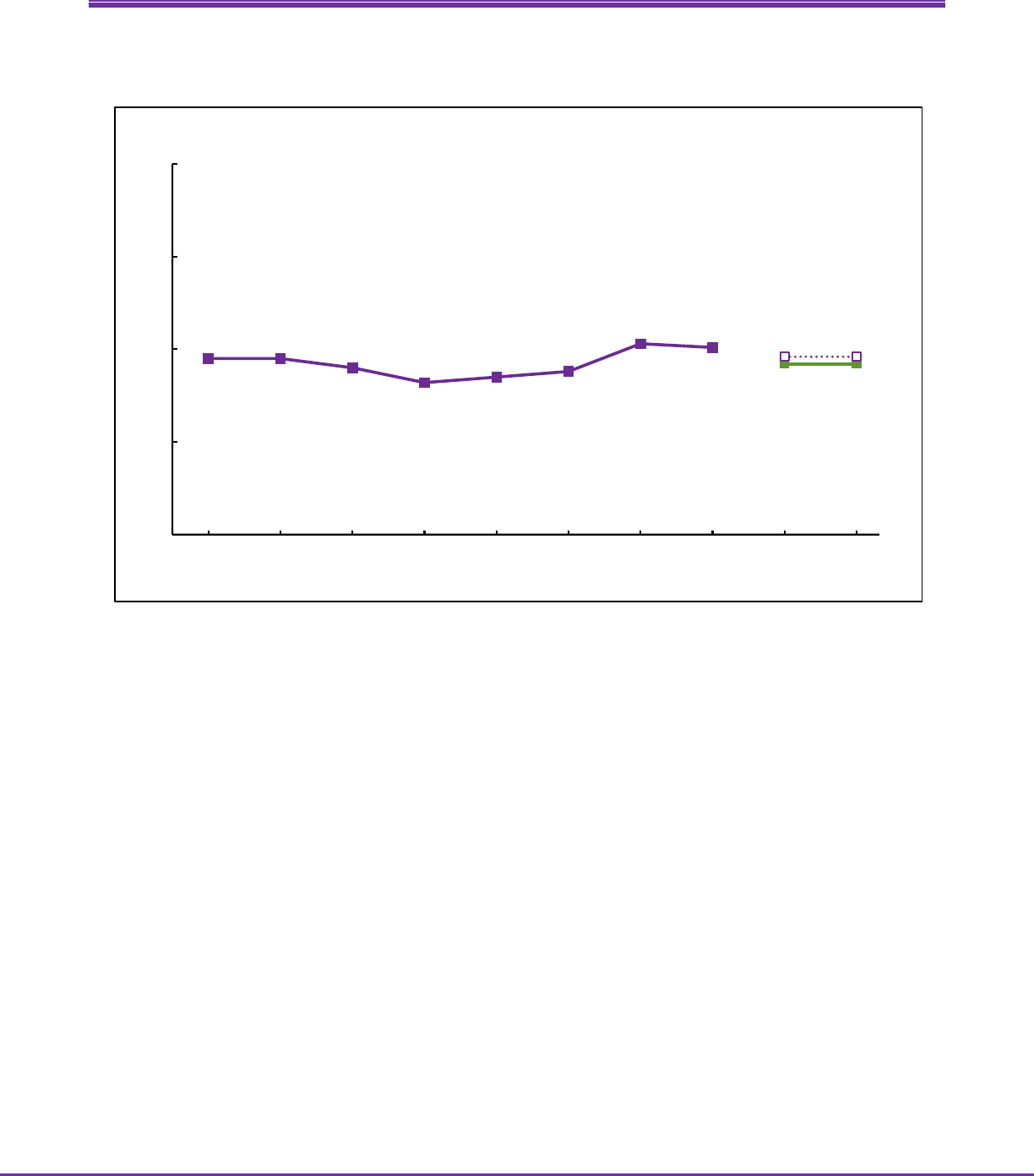
• The prevalence of an asthma episode or attack declined from 2016 through 2017. There has been no
clear trend since 2017 (see Figure).
• There was no significant change from January-June 2019 (3.4%) to July-December 2019 (3.3%, p = 0.44).
This is consistent with the absence of a trend since 2017.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 15
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults who had an asthma episode or attack in the past 12 months
4.0
3.5
4.1
3.9
3.7
3.4
3.5
3.6
3.4
3.3
3.6
3.5
0
2
4
6
8
10
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 16
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Regularly Experienced Chronic Pain
Questionnaire changes between 2018 and 2019: While the question text for this indicator was unchanged from
2018 to 2019, the context surrounding this question changed. Sample adult respondents were asked, “In the
past three months, how often did you have pain? Would you say never, some days, most days, or every day?” In
2018, this question appeared in the section entitled Adult Functioning and Disability (AFD) and was at the end of
the sample adult interview. In 2019, this question was the first in a series of questions on chronic pain, and the
chronic pain section was a little more than halfway through the sample adult interview.
This indicator is new to the Early Release Program and reflects sample adults who experienced pain either ‘every
day’ or ‘most days’.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
20.7
(20.2 - 21.3)
21.6
(20.3 – 22.9)
19.7
(18.6 – 20.8)
20.0
(19.5 - 20.5)
20.6
(20.1 - 21.2)
-1.9‡ 0.6 -1.3
Preliminary analysis:
• In 2018, the percentage of adults who regularly experienced chronic pain was 20.7%. The 2019 full-year
estimate with the new weight was 20.6% (see Table). This difference was not statistically significant (p =
0.83).
• During the fourth quarter of 2018, the production estimate (21.6%) was 1.9 percentage points higher
than the bridge estimate (19.7%). This difference was statistically significant (p = 0.07), indicating that a
questionnaire design effect is likely.
• The 2019 full-year estimate with the old weight (20.0%) was lower than, but not significantly different
from, the 2019 full-year estimate with the new weight (20.6%). This result (p = 0.18) suggests that the
weighting adjustment was unlikely to affect estimates for this indicator.
• Considered together, estimates for 2019 may have shifted downward by 1.3 percentage points due to
the methodological change. This shift may have masked an actual increase from 2018 to 2019.
• The prevalence of chronic pain increased from July-December 2016 (17.9%) through July-December
2018 (21.1%; see Figure). Given the impact of the change in methodology, it is not possible to determine
if there was an increase from July-December 2016 and into 2019.
• There was no change from January-June 2019 (20.6%) to July-December 2019 (20.6%, p = 0.99)
indicating that if there was an increasing trend starting in July-December 2016, it did not continue
through 2019.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 17
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults who regularly experienced chronic pain
19.5
19.6
19.1
17.9
18.4
18.2
20.4
21.1
20.6 20.6
21.9 21.9
0
5
10
15
20
25
30
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 18
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Regularly Had Feelings of Worry, Nervousness, or Anxiety
Questionnaire changes between 2018 and 2019: This indicator is based on responses to two questions: a) “How
often do you feel worried, nervous, or anxious? Would you say daily, weekly, monthly, a few times a year, or
never?”; and b) “Thinking about the last time you felt worried, nervous, or anxious, how would you describe the
level of these feelings? Would you say a little, a lot, or somewhere in between?” While the text of the questions
for this indicator was unchanged from 2018 to 2019, the context surrounding these questions changed. In 2018,
these questions were included in the AFD section, a section at the end of the sample adult interview. In 2019,
these questions were included at the beginning of a series of questions on mental health and towards the
middle of the sample adult interview.
This indicator is new to the Early Release Program and reflects sample adults who had feelings of worry,
nervousness, or anxiety a) daily and report the level as ‘a lot’ or ‘somewhere in between’, or b) weekly and
report the level as ‘a lot’.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
8.6
(8.2 – 9.0)
9.0
(8.0 - 10.0)
11.1
(10.2 – 12.0)
10.9
(10.6 - 11.3)
11.2
(10.8 - 11.5)
2.1* 0.3 2.4
Preliminary analysis:
• In 2018, the percentage of adults who regularly had feelings of worry, nervousness, or anxiety was 8.6%.
The 2019 full-year estimate with the new weight was 11.2% (see Table). This observed increase was
statistically significant (p < 0.001).
• During the fourth quarter of 2018, the production estimate (9.0%) was 2.1 percentage points lower than
the bridge estimate (11.1%). This difference was statistically significant (p = 0.01) indicating that a
questionnaire design effect is likely.
• The 2019 full-year estimates using the old and new weights were similar (10.9% and 11.2%,
respectively). This result (p = 0.36) suggests that the weighting adjustment did not substantially affect
estimates for this indicator.
• Considered together, estimates for 2019 may have shifted upward by 2.4 percentage points due to the
methodological change. This shift may account for the observed increase from 8.6% in 2018 to 11.2% in
2019.
• The percentage of adults who regularly had feelings of worry, nervousness, or anxiety increased from
2016 through 2017 (see Figure). There was no clear trend from July-December 2017 to July-December
2018. If the observed increase in 2019 does not indicate a real increase but reflects the methodological
effects described above, there was also no clear trend into 2019.
• There was no significant change from January-June 2019 (11.0%) to July-December 2019 (11.3%, p =
0.60). This is consistent with the absence of a trend since 2017.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 19
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults who regularly had feelings of worry, nervousness, or anxiety
7.1
7.8
7.1
7.6
7.9
8.9
8.5
8.7
11.0
11.3
8.6
8.9
0
5
10
15
20
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 20
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Regularly Had Feelings of Depression
Questionnaire changes between 2018 and 2019: This indicator is based on responses to two questions: a) “How
often do you feel depressed? Would you say daily, weekly, monthly, a few times a year, or never?”; and b)
“Thinking about the last time you felt depressed, how depressed did you feel? Would you say a little, a lot, or
somewhere in between?” While the text of the questions for this indicator was unchanged from 2018 to 2019,
the context surrounding these questions changed. In 2018, these questions were included in the AFD section, a
section at the end of the sample adult interview. In 2019, these questions were included early in a series of
questions on mental health and towards the middle of the sample adult interview. One matter of context did
not change: These questions have always followed the questions on feeling worried, nervous, or anxious.
This indicator is new to the Early Release Program and reflects sample adults who had feelings of depression a)
daily and report the level as ‘a lot’ or ‘somewhere in between’, or b) weekly and report the level as ‘a lot’.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
4.4
(4.2 – 4.7)
4.7
(4.1 – 5.4)
4.2
(3.7 – 4.8)
4.6
(4.4 - 4.8)
4.7
(4.5 - 5.0)
-0.5 0.1 -0.4
Preliminary analysis:
• In 2018, the percentage of adults who regularly had feelings of depression was 4.4%. The 2019 full-year
estimate with the new weight was 4.7% (see Table). This difference was not statistically significant (p =
0.17).
• During the fourth quarter of 2018, the production estimate (4.7%) was higher than, but not significantly
different from, the bridge estimate (4.2%). This result (p = 0.33) suggests that a questionnaire design
effect is unlikely.
• The 2019 full-year estimates using the old and new weights were similar (4.6% and 4.7%, respectively).
This result (p = 0.63) suggests that the weighting adjustment did not substantially affect estimates for
this indicator.
• Considered together, estimates for 2019 may have shifted downward by 0.4 percentage points due to
the methodological change. Though this shift was not statistically significant, it may have partially
masked an actual increase from 2018 to 2019.
• The percentage of adults who regularly had feelings of depression increased from 2016 through 2018
(see Figure). The increasing trend may have continued into 2019.
• However, there was no change from January-June 2019 (4.7%) to July-December 2019 (4.7%, p = 0.89)
indicating that if there was an increasing trend starting in 2016 it did not continue throughout calendar
year 2019.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 21
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults who regularly had feelings of depression
3.8 3.8
3.4
3.8
3.9
4.0
4.4 4.4
4.7 4.7
5.1 5.1
0
2
4
6
8
10
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019
Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 22
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Disability Status
Questionnaire changes between 2018 and 2019: While the questions regarding disability did not change
between 2018 and 2019, their location in the interview changed. Similar to the questions on chronic pain,
feelings of worry, nervousness, or anxiety, and feelings of depression, the questions that form the disability
composite variable were included in the AFD section and at the end of the sample adult interview in 2018.
Starting in 2019, these questions moved into the first half of the sample adult interview.
This indicator is new to the Early Release Program. It is defined by the reported level of difficulty (no difficulty,
some difficulty, a lot of difficulty, or cannot do at all) in six functioning domains: seeing (even if wearing glasses),
hearing (even if wearing hearing aids), mobility (walking and climbing stairs), communication (understanding or
being understood by others), cognition (remembering or concentrating), and self-care (such as washing all over
or dressing). Sample adults who responded “a lot of difficulty” or “cannot do at all” to at least one question
were considered to have a disability.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
10.2
(9.8 - 10.6)
9.9
(9.0 - 10.8)
8.9
(8.1 - 9.7)
8.6
(8.3 - 9.0)
9.2
(8.8 - 9.6)
-1.0 0.6‡ -0.4
Preliminary analysis:
• In 2018, the percentage of adults with disability was 10.2%. The 2019 full-year estimate with the new
weight was 9.2% (see Table). This observed decrease was statistically significant (p = 0.003).
• During the fourth quarter of 2018, the production estimate (9.9%) was 1.0 percentage points higher
than the bridge estimate (8.9%). This difference suggests a possible questionnaire design effect, but it
did not reach statistical significance (p = 0.16).
• The 2019 full-year estimate using the old weight (8.6%) was 0.6 percentage points lower than the 2019
full-year estimate using the new weight (9.2%). This difference was statistically significant (p = 0.05)
indicating that estimates for this indicator were likely affected by the change in the weighting approach.
• Considered together, estimates for 2019 may have shifted downward by 0.4 percentage points due to
the methodological change. This small shift due to methodological changes may account for some of the
observed decrease from 10.2% in 2018 to 9.2% in 2019.
• The percentage of adults with disability increased from July-December 2016 (8.2%) through July-
December 2018 (10.1%) (see Figure). There is no indication that this trend has continued through 2019
and there might have been a decrease between 2018 and 2019.
• There was no change from January-June 2019 (9.2%) to July-December 2019 (9.2%, p = 0.82). This could
indicate that any decrease in 2019 did not continue through the year.
Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 23
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults with disability
9.5 9.5
9.0
8.2
8.5
8.8
10.3
10.1
9.2 9.2
9.6 9.6
0
5
10
15
20
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 24
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Current Cigarette Smoking
Questionnaire changes between 2018 and 2019: The two questions used for this indicator were unchanged
from 2018 to 2019. Sample adult respondents were asked, “Have you smoked at least 100 cigarettes in your
entire life?” If yes, they were asked “Do you now smoke cigarettes every day, some days, or not at all?”
This indicator is one of eight from the original Early Release Program and reflects sample adults who smoke
cigarettes ‘every day’ or ‘some days’.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
13.7
(13.3 - 14.2)
13.3
(12.3 - 14.4)
12.8
(11.8 – 13.8)
13.2
(12.8 - 13.7)
14.2
(13.8 - 14.7)
-0.5 1.0** 0.5
Preliminary analysis:
• In 2018, the percentage of adults who were current cigarette smokers was 13.7%. The 2019 full-year
estimate with the new weight was 14.2% (see Table). This observed increase was not statistically
significant (p = 0.19).
• During the fourth quarter of 2018, the production estimate (13.3%) was higher than, but not
significantly different from, the bridge estimate (12.8%). This result (p = 0.57) suggests that a
questionnaire design effect is unlikely.
• The 2019 full-year estimate using the old weight (13.2%) was 1.0 percentage points lower than the 2019
full-year estimate using the new weight (14.2%). This difference was statistically significant (p = 0.005),
indicating that estimates for this indicator were likely affected by the change in the weighting approach.
• Considered together, estimates for 2019 may have shifted upward by 0.5 percentage points. This small
shift due to methodological changes may account for the observed increase from 13.7% in 2018 to
14.2% in 2019.
• The prevalence of current cigarette smoking declined from 2016 through 2017. There has been no clear
trend since then (see Figure). After taking the methodological changes into account, it appears that
there remains no change since July-December 2017 in the prevalence of cigarette smoking.
• There was no significant change from January-June 2019 (14.4%) to July-December 2019 (14.1%, p =
0.65). This is consistent with the absence of a trend since July-December 2017.
Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 25
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults who were current cigarette smokers
14.9
15.3
15.8
15.1
14.4
13.5
13.7 13.7
14.4
14.1
13.9
13.6
0
5
10
15
20
25
30
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 26
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Current Electronic Cigarette Use
Questionnaire changes between 2018 and 2019: The two questions used for this indicator changed slightly from
2018 to 2019 (see underlined text for additions). In 2019, sample adult respondents were asked “Have you ever
used an e-cigarette or other electronic vaping product, even just one time, in your entire life?” If yes, they were
asked “Do you now use e-cigarettes or other electronic vaping products every day, some days, or not at all?” In
2018, the question was preceded with a lengthy definition of the term ‘e-cigarettes.’ In 2019, that introduction
was not present.
This indicator is new to the Early Release Program and reflects sample adults who said that they use electronic
cigarettes ‘some days’ or ‘every day’.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
3.2
(3.0 - 3.5)
3.3
(2.7 – 3.9)
4.3
(3.7 - 5.0)
4.3
(4.0 - 4.6)
4.4
(4.1 - 4.7)
1.0‡ 0.1 1.1
Preliminary analysis:
• In 2018, the percentage of adults who were current electronic cigarette users was 3.2%. The 2019 full-
year estimate with the new weight was 4.4% (see Table). This observed increase was statistically
significant (p < 0.001).
• During the fourth quarter of 2018, the production estimate (3.3%) was 1.0 percentage points lower than
the bridge estimate (4.3%). This difference was statistically significant (p = 0.06) indicating that a
questionnaire design effect is likely.
• The 2019 full-year estimates using the old and new weights were similar (4.3% and 4.4%, respectively).
This result (p = 0.68) suggests that the weighting adjustment did not substantially affect estimates for
this indicator.
• Considered together, estimates for 2019 may have shifted upward by 1.1 percentage points due to the
methodological change. This shift due to methodological changes may account for the observed
increase from 3.2% in 2018 to 4.4% in 2019.
• The prevalence of electronic cigarette use increased from 2017 through 2018 (see Figure). Given the
impact of the change in the methodology, it is not possible to determine if there was any change
between 2018 and 2019.
• There was no change from January-June 2019 (4.4%) and July-December 2019 (4.4%, p = 0.99). This is
consistent with the conclusion that the increasing trend from 2017 to 2018 did not continue through
2019.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 27
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults who were current electronic cigarette users
3.2
3.7
3.5
2.9
2.8 2.8
2.9
3.6
4.4 4.4
3.3 3.3
0
2
4
6
8
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 28
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Did Not Get Needed Medical Care Due to Cost
Questionnaire changes between 2018 and 2019: Prior to 2019, this question was asked of the family
respondent during the family core interview. As part of the questionnaire redesign, this question is now directly
asked of the sample adult, but the question itself did not change. The sample adult is asked “During the past 12
months, was there any time when you needed medical care but did not get it because of the cost?”
This indicator is one of eight from the original Early Release Program and reflects sample adults who needed
medical care in the past 12 months but did not get it because of cost.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
6.4
(6.1 - 6.7)
6.3
(5.6 - 7.0)
8.2
(7.2 - 9.3)
7.8
(7.5-8.2)
8.3
(8.0-8.7)
1.9* 0.5‡ 2.4
Preliminary analysis:
• In 2018, the percentage of adults who did not get needed medical care due to cost in the past 12
months was 6.4%. The 2019 full-year estimate with the new weight was 8.3% (see Table). This observed
increase was statistically significant (p < 0.001).
• During the fourth quarter of 2018, the production estimate (6.3%) was 1.9 percentage points lower than
the bridge estimate (8.2%). This difference was statistically significant (p = 0.01), indicating that a
questionnaire design effect is likely.
• The 2019 full-year estimate using the old weight (7.8%) was 0.5 percentage points lower than the 2019
full-year estimate using the new weight (8.3%). This difference was statistically significant (p = 0.08);
estimates for this indicator were likely affected by the change in the weighting approach.
• Considered together, estimates for 2019 may have shifted upward by 2.4 percentage points due to the
methodological change. This shift due to methodological changes may account for the observed
increase from 6.4% in 2018 to 8.3% in 2019.
• There is no clear trend from 2015 to 2018 in the percentage of adults who did not get needed medical
care due to cost (see Figure). Given the impact of the change in methodology, it is not possible to
determine if there was an actual increase between 2018 and 2019.
• The increase from January-June 2019 (7.6%) to July-December 2019 (9.0%) was statistically significant (p
= 0.001). It is possible that 2019 is the first year of an increasing trend.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 29
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults who did not get needed medical care in the past 12 months due to cost
5.9
6.2
6.0
6.1
5.8
5.9
6.3
6.5
7.6
9.0
5.2
6.6
0
2
4
6
8
10
12
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 30
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Did Not Take Medication as Prescribed to Save Money
Questionnaire changes between 2018 and 2019: The initial question in the series of questions for this indicator
was modified slightly during the questionnaire redesign. Prior to 2019, sample adult respondents were asked
“During the past 12 months, were you prescribed medication by a doctor or other health professional?” As part
of the questionnaire redesign, sample adults were asked “At any time in the past 12 months, did you take
prescription medication?” Sample adults who answered yes were then asked the following series of yes-or-no
questions: “During the past 12 months, were any of the following true for you? 1) You skipped medication doses
to save money; 2) You took less medication to save money; 3) You delayed filling a prescription to save money.”
This indicator is new to the Early Release Program and reflects sample adults who gave an affirmative response
to at least one of these latter three questions.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
9.2
(8.8 - 9.7)
9.2
(8.1 - 10.3)
9.1
(8.2 - 10.2)
9.2
(8.7-9.6)
9.7
(9.2-10.1)
-0.1 0.5 0.4
Preliminary analysis:
• In 2018, the percentage of adults who did not take medication as prescribed to save money in the past
12 months was 9.2%. The 2019 full-year estimate with the new weight was 9.7% (see Table). This
observed increase was not statistically significant (p = 0.23).
• During the fourth quarter of 2018, the production and bridge estimates for this indicator were similar
(9.2% and 9.1%, respectively). This result suggests (p = 0.91) that a questionnaire design effect is
unlikely.
• The 2019 full-year estimate with the old weight (9.2%) was lower than, but not significantly different
from, the 2019 full-year estimate with the new weight (9.7%). This result (p = 0.24) suggests that the
weighting adjustment was unlikely to affect estimates for this indicator.
• Considered together, estimates for 2019 may have shifted upward by 0.4 percentage points due to the
methodological change. The shift due to methodological changes may account for the observed increase
from 9.2% in 2018 to 9.7% in 2019.
• There has been no clear trend in this indicator since 2015 (see Figure).
• There was no significant change from January-June 2019 (9.5%) to July-December 2019 (9.8%, p = 0.55).
This is consistent with the absence of a trend since 2015.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 31
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults who did not take medication as prescribed to save money
in the past 12 months
9.7
9.5
9.7
8.9
10.1
9.0
9.3
9.2
9.5
9.8
9.1
9.4
0
5
10
15
20
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 32
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Did Not Get Needed Mental Health Care Due to Cost
Questionnaire changes between 2018 and 2019: The question text changed slightly from 2018 to 2019. Prior to
2019, sample adult respondents were asked “During the past 12 months, was there any time when you needed
any of the following, but didn’t get it because you couldn’t afford it?” Mental health care or counseling was
included in a list, and the respondent answered yes or no to each item. Beginning in 2019, sample adult
respondents were asked specifically “During the past 12 months, was there any time when you needed
counseling or therapy from a mental health professional but did not get it because of the cost?”.
This indicator is new to the Early Release Program and reflects an affirmative response to this question.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
2.6
(2.4 - 2.9)
3.4
(2.8 - 4.0)
4.9
(4.3 - 5.6)
4.4
(4.1-4.6)
4.3
(4.1-4.6)
1.5** -0.1 1.4
Preliminary analysis:
• In 2018, the percentage of adults who did not get needed mental health care in the past 12 months due
to cost was 2.6%. The 2019 full-year estimate with the new weight was 4.3% (see Table). This observed
increase was statistically significant (p < 0.001).
• During the fourth quarter of 2018, the production estimate (3.4%) was 1.5 percentage points lower than
the bridge estimate (4.9%). This difference was statistically significant (p = 0.004) indicating that a
questionnaire design effect is likely.
• The 2019 full-year estimates using the old and new weights were similar (4.4% and 4.3%, respectively).
This result (p = 0.72) suggests that the weighting adjustment did not substantially affect estimates for
this indicator.
• Considered together, estimates for 2019 may have shifted upward by 1.4 percentage points due to the
methodological change. This shift due to methodological changes may account for most (but not all) of
the observed increase from 2.6% in 2018 to 4.3% in 2019.
• Estimates increased from July-December 2016 (1.8%) through July-December 2018 (2.9%) (see Figure).
Given the impact of the change in methodology, a small increase might have occurred between 2018
and 2019, and there may be an increasing trend in this indicator from July-December 2016 through
2019.
• The observed increase from January-June 2019 (4.2%) to July-December 2019 (4.5%) would be
consistent with an increasing trend starting in 2016. However, the observed increase was not
statistically significant (p = 0.29).

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 33
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults who did not get needed mental health care in the past 12 months
due to cost
1.8
2.0
2.1
1.8
2.0
2.2
2.4
2.9
4.2
4.5
2.8
3.1
0
2
4
6
8
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 34
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Doctor Visit
Questionnaire changes between 2018 and 2019: Both the question text and the response categories were
modified slightly between 2018 and 2019. In 2019, sample adult respondents were asked “About how long has
it been since you last saw or talked to a doctor or other health care professional about your own health?” The
underlined text was not included in the question text from 2018. The response categories changed with the
redesign, merging two response categories (6 months or less, more than 6 months but not more than 1 year
ago) into one response category in 2019 (within the past year (anytime less than 12 months ago)).
This indicator is new to the Early Release Program and reflects sample adults who had at least one doctor visit in
the past 12 months.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
84.3
(83.8 – 84.9)
85.2
(83.9 - 86.4)
84.2
(82.9 - 85.4)
85.2
(84.8 - 85.6)
84.9
(84.5 - 85.3)
-1.0 -0.3 -1.3
Preliminary analysis:
• In 2018, the percentage of adults who had at least one doctor visit in the past 12 months was 84.3%.
The 2019 full-year estimate with the new weight was 84.9% (see Table). This observed increase was not
statistically significant (p = 0.21).
• During the fourth quarter of 2018, the production estimate (85.2%) was 1.0 percentage points higher
than the bridge estimate (84.2%). This comparison suggests a possible questionnaire design effect, but it
was not statistically significant (p = 0.35).
• The 2019 full-year estimates using the old and new weights were similar (85.2% and 84.9%,
respectively). This result (p = 0.48) suggests that the weighting adjustment did not substantially affect
estimates for this indicator.
• Considered together, estimates for 2019 may have shifted downward by 1.3 percentage points due to
the methodological change. The observed increase from 2018 (84.3%) to 2019 (84.9%) may be smaller
than the true size of the actual increase. The true size of the actual increase from 2018 to 2019 may
have been masked by the methodological changes.
• There is no clear trend from 2015 to 2018 (see Figure). Given the potential impact of the change in
methodology, there might have been an actual increase between 2018 and 2019.
• There was no significant change from January-June 2019 (85.0%) to July-December 2019 (84.8%, p =
0.72). This could indicate that any increase between 2018 and 2019 did not continue through the
calendar year.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 35
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults who had at least one doctor visit in the past 12 months
84.0
83.3
83.9
85.3
85.5
84.8
84.3
84.4
85.0
84.8
86.3
86.1
0
10
20
30
40
50
60
70
80
90
100
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 36
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Hospital Emergency Department Visit
Questionnaire changes between 2018 and 2019: In 2019, sample adult respondents were asked “During the
past 12 months, how many times have you gone to a hospital emergency room about your own health?” The
underlined text was not included in the question text from 2018. In addition to this minor change to the
question text, the response options also changed. Prior to 2019, response options had to fit within
predetermined categories. Beginning in 2019, the respondent’s numerical response was entered.
This indicator is new to the Early Release Program and reflects sample adults who had at least one hospital
emergency department visit in the past 12 months.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
21.3
(20.8 – 21.9)
21.3
(20.0 - 22.6)
21.8
(20.6 - 23.0)
21.3
(20.8 - 21.7)
21.8
(21.4 - 22.3)
0.5 0.5 1.0
Preliminary analysis:
• In 2018, the percentage of adults who had at least one hospital emergency department visit in the past
12 months was 21.3%. The 2019 full-year estimate with the new weight was 21.8% (see Table). The
observed increase was not statistically significant (p = 0.29).
• During the fourth quarter of 2018, the production estimate (21.3%) was lower than, but not significantly
different from, the bridge estimate (21.8%). This result (p = 0.63) suggests that a questionnaire design
effect is unlikely.
• The 2019 full-year estimate with the old weight (21.3%) was lower than, but not significantly different
from, the 2019 full-year estimate with the new weight (21.8%). This result (p = 0.24) suggests that the
weighting adjustment did not substantially affect estimates for this indicator.
• Considered together, estimates for 2019 may have shifted upward by 1.0 percentage points due to the
methodological changes. This shift due to methodological changes may account for the observed
increase from 21.3% in 2018 to 21.8% in 2019. As a result, there may have been an actual small
decrease from 2018 to 2019 that is masked by the methodological change.
• The percentage of adults who had at least one hospital emergency department visit in the past 12
months increased from January-June 2017 (18.2%) through July-December 2018 (21.3%) (see Figure).
Given the potential impact of the change in the methodology, the increasing trend from 2017 through
2018 may not have continued into 2019.
• There was no significant change from January-June 2019 (22.0%) to July-December 2019 (21.7%, p =
0.64). This is consistent with the conclusion that the increasing trend from 2017 to 2018 did not
continue into 2019.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 37
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults who had at least one hospital emergency department visit
in the past 12 months
18.8
18.7
19.4 19.4
18.2
19.2
21.4
21.3
22.0
21.7
21.0
20.7
0
5
10
15
20
25
30
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 38
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Influenza Vaccination
Questionnaire changes between 2018 and 2019: The question text did not change between 2018 and 2019.
Sample adult respondents were asked “During the past 12 months, have you had a flu vaccination?” In 2018, this
question was preceded by questions about having a usual place of care. In 2019, this question was preceded by
questions about cancer screening.
This indicator is one of eight from the original Early Release Program and reflects sample adults who had an
influenza vaccination in the past 12 months.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
44.6
(43.9 - 45.3)
44.2
(42.6 – 45.9)
45.0
(43.4 - 46.5)
47.8
(47.0 - 48.5)
46.8
(46.1 - 47.5)
0.8 -1.0 -0.2
Preliminary analysis:
• In 2018, the percentage of adults who had an influenza vaccination in the past year was 44.6%. The 2019
full-year estimate with the new weight was 46.8% (see Table). The observed increase was statistically
significant (p < 0.001).
• During the fourth quarter of 2018, the production estimate (44.2%) was lower than, but not significantly
different from, the bridge estimate (45.0%). This result (p = 0.56) suggests that a questionnaire design
effect is unlikely.
• The 2019 full-year estimate with the old weight (47.8%) was 1.0 percentage points higher than, but not
significantly different from, the 2019 full-year estimate with the new weight (46.8%). This difference
suggests a possible weighting adjustment effect, but it did not reach statistical significance (p = 0.12).
• Considered together, estimates for 2019 may have shifted downward by 0.2 percentage points due to
the methodological change. The questionnaire design and weighting adjustment effects, if present, may
have shifted estimates in opposing directions, leading to little overall impact. The increase from 2018
(44.6%) to 2019 (46.8%) is likely to reflect actual change over time.
• This increase from 2018 to 2019 is likely a continuation of an increasing trend since July-December 2016
(see Figure).
• The observed decrease from January-June 2019 (47.2%) to July-December 2019 (46.4%) was not
statistically significant (p = 0.27) and appears to be consistent with the small decreases between
estimates for the first six months and second six months observed in other years.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 39
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Percentage of adults who had an influenza vaccination in the past year
43.9
41.3
42.5
41.9
44.5
42.3
44.8
44.4
47.2
46.4
47.4
46.6
0
10
20
30
40
50
60
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 40
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Blood Pressure Check
Questionnaire changes between 2018 and 2019: Both the question text and responses changed from 2018 to
2019. In 2018, sample adult respondents were asked “During the past 12 months, have you had your blood
pressure checked by a doctor, nurse, or other health professional?” The response was a yes or no answer. In
2019, sample adult respondents were asked “When was the last time you had your blood pressure checked by a
doctor, nurse, or other health professional?” The response categories changed from dichotomous to categorical,
and the “within the past year (anytime less than 12 months ago)” was used for this indicator.
This indicator is new to the Early Release Program and reflects sample adults who had their blood pressure
checked in the past 12 months.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
84.6
(84.1 - 85.1)
85.8
(84.6 - 87.0)
86.6
(85.4 - 87.7)
88.3
(87.9 - 88.8)
88.1
(87.6 - 88.5)
0.8 -0.2 0.6
Preliminary analysis:
• In 2018, the percentage of adults who had their blood pressure checked in the past 12 months was
84.6%. The 2019 full-year estimate with the new weight was 88.1% (see Table). The observed increase
was statistically significant (p < 0.001).
• During the fourth quarter of 2018, the production estimate (85.8%) was lower than, but not significantly
different from, the bridge estimate (86.6%). This result (p = 0.41) suggests that a questionnaire design
effect is unlikely.
• The 2019 full-year estimates using the old and new weights were similar (88.3% and 88.1%,
respectively). This result (p = 0.64) suggests that the weighting adjustment did not substantially affect
estimates for this indicator.
• Considered together, estimates for 2019 may have shifted upward by 0.6 percentage points due to the
methodological change. This small shift due to methodological changes would account for only a part of
the observed increase from 2018 (84.6%) to 2019 (88.1%). The increase is likely to reflect actual change.
• There has been no clear trend from 2015 to 2018 in the percentage of adults who had their blood
pressure checked in the past 12 months (see Figure).
• There was no change from January-June 2019 (88.1%) to July-December 2019 (88.1%, p = 0.99) (see
Figure). Any change between 2018 and 2019 did not occur throughout 2019.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 41
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Health Insurance Coverage
Questionnaire changes between 2018 and 2019: While the process for generating estimates of health insurance
coverage did not change between 2018 and 2019, the questions themselves moved from the family core to the
sample adult and sample child interviews as part of the questionnaire redesign. Prior to 2019, the questions
were answered by a family respondent who may or may not have been the sample adult or sample child
respondent. Starting in 2019, health insurance is asked directly of the sample adult for himself or herself and of
the sample child respondent on behalf of only the sample child.
These three indicators— lack of health insurance, public health plan coverage, and private health insurance
coverage—were among the eight from the original Early Release Program.
For the purposes of this working paper, analyses were limited to adults aged 18-64. In addition, the analyses
used preliminary estimates from the Early Release Program for the 2018 Production and 2018 Quarter 4
Production estimates, rather than final “official” estimates. To produce the preliminary quarterly estimates that
are included in the Early Release reports, NCHS developed a streamlined version of the usual final editing
process for health insurance data. Thus, it is more appropriate to compare the preliminary 2019 estimates to
2018 estimates that used the same streamlined editing process. The editing process for other indicators in this
working paper do not differ for preliminary and final estimates.
Percentage of adults who had their blood pressure checked in the past 12 months
83.2
82.4
83.6
85.0
85.4
85.8
84.5
84.7
88.1 88.1
87.5 87.5
0
10
20
30
40
50
60
70
80
90
100
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 42
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Lack of Health Insurance
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
13.3
(12.6 – 13.9)
14.0
(13.0 - 15.1)
13.8
(12.1 - 15.5)
13.8
(13.2 - 14.4)
14.7
(14.0 - 15.3)
-0.2 0.9‡ 0.7
• In 2018, the percentage of adults aged 18-64 who lacked health insurance at the time of interview was
13.3%. The 2019 full-year estimate with the new weight was 14.7% (see Table). The observed increase
was statistically significant (p = 0.01).
• During the fourth quarter of 2018, the production and bridge estimates for this indicator were similar
(14.0% and 13.8%, respectively). This result (p = 0.87) suggests that a questionnaire design effect is
unlikely.
• The 2019 full-year estimate using the old weight (13.8%) was 0.9 percentage points lower than the 2019
full-year estimate using the new weight (14.7%). This difference was statistically significant (p = 0.07);
estimates for this indicator were likely affected by the change in the weighting approach.
• Considered together, estimates for 2019 may have shifted upward by 0.7 percentage points due to the
methodological change. This shift due to methodological changes may account for some (but not all) of
the observed increase from 13.3% in 2018 to 14.7% in 2019.
• Even accounting for the methodological changes in 2019, the percentage of adults aged 18-64 who
lacked health insurance at the time of the interview most likely reflects an increase compared to 2018.
The trend in lack of insurance appears to be increasing since July-December 2016 (see Figure).
• The increase from January-June 2019 (13.7%) to July-December 2019 (15.6%) was statistically significant
(p = 0.003) and greater in magnitude than the increases observed in 2017 and 2018 between estimates
for the first six months and second six months of the year. This is consistent with a continuation of an
increasing trend since 2016.
Percentage of adults aged 18-64 who lacked health insurance at the time of interview
12.5
12.7
11.9
11.5
12.0
12.8
12.3
13.8
13.7
15.6
13.0
14.9
0
5
10
15
20
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Early Release estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 43
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Public Health Plan Coverage
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
19.4
(18.9 - 20.0)
18.6
(17.5 – 19.7)
17.5
(16.2 – 18.8)
19.0
(18.4 - 19.7)
20.4
(19.7 - 21.1)
-1.1 1.4* 0.3
• In 2018, the percentage of adults aged 18-64 who had public health plan coverage at the time of
interview was 19.4%. The 2019 full-year estimate with the new weight was 20.4% (see Table). The
observed increase was statistically significant (p = 0.07).
• During the fourth quarter of 2018, the production estimate (18.6%) was 1.1 percentage points higher
than the bridge estimate (17.5%). This difference suggests a possible questionnaire design effect, but it
did not reach statistical significance (p = 0.27).
• The 2019 full-year estimate using the old weight (19.0%) was 1.4 percentage points lower than the 2019
full-year estimate using the new weight (20.4%). This difference was statistically significant (p = 0.01)
indicating that estimates for this indicator were likely affected by the change in the weighting approach.
• Considered together, estimates for 2019 may have shifted upward by 0.3 percentage points due to the
methodological change. The questionnaire design and weighting adjustment effects may have shifted
estimates in opposing directions, leading to little overall impact. The increase from 2018 (19.4%) to 2019
(20.4%) is likely to reflect actual change over time.
• The percentage of adults aged 18-64 who had public health plan coverage generally declined from
January-June 2016 (21.2%) through July-December 2018 (18.6%; see Figure). This decreasing trend does
not appear to have continued into 2019. Taking the impact of the change in the methodology into
account, there might have been an increase between 2018 and 2019.
• There was no change from January-June 2019 (20.4%) to July-December 2019 (20.4%, p = 0.99). Any
change between 2018 and 2019 did not occur throughout 2019.
Percentage of adults aged 18-64 who had public health plan coverage at the time of interview
19.0
19.8
21.2
21.0
19.9
19.6
20.6
18.6
20.4 20.4
20.1 20.1
0
5
10
15
20
25
30
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Early Release estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 44
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Private Health Insurance Coverage
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
68.9
(68.2 - 69.7)
68.7
(67.3 - 70.1)
71.0
(69.2 – 72.7)
69.0
(68.2 - 69.8)
66.8
(65.9 - 67.7)
2.3‡ -2.2** 0.1
• In 2018, the percentage of adults aged 18-64 who had private health insurance coverage was 68.9%. The
2019 full-year estimate with the new weight was 66.8%. The observed decrease was statistically
significant (p = 0.002).
• During the fourth quarter of 2018, the production estimate (68.7%) was 2.3 percentage points lower
than the bridge estimate (71.0%). This difference was statistically significant (p = 0.09) indicating that a
questionnaire design effect is likely.
• The 2019 full-year estimate using the old weight (69.0%) was 2.2 percentage points higher than the
2019 full-year estimate using the new weight (66.8%). This difference was statistically significant (p =
0.002); estimates for this indicator were likely affected by the change in the weighting approach.
• Considered together, estimates for 2019 may have shifted upward by 0.1 percentage points due to the
methodological change. The questionnaire design and weighting adjustment effects shifted estimates in
opposing directions, leading to little overall impact. The decrease from 2018 (68.9%) to 2019 (66.8%) is
likely to reflect actual change over time.
• The decrease from 2018 to 2019 is a continuation of the decreasing trend since January-June 2015 (see
Figure).
• The decrease from January-June 2019 (66.7%) to July-December 2019 (65.9%) was statistically
significant (p = 0.05). This is consistent with a decreasing trend since 2015.
Percentage of adults aged 18-64 who had private health insurance coverage
at the time of interview
70.2
69.0
68.5
69.2
69.7
69.0
69.1
68.9
67.7
65.9
67.6
65.8
0
10
20
30
40
50
60
70
80
90
100
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Early Release estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 45
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Adults Living in Wireless-Only Households
Questionnaire changes between 2018 and 2019: The indicator is based on responses to questions asking
separately about landline and wireless telephone service. The question on landline service did not change
between 2018 and 2019; in both years, respondents were asked if there was “at least one phone inside your
home that is currently working and is not a cell phone.” The question on wireless service did change. In 2018,
respondents were asked whether “you or anyone in your family has a working cellular telephone.” In 2019, the
NHIS asks respondents whether they “have a working cell phone,” and if not, whether they “live with anyone
who has a working cell phone.” Moreover, these questions moved from the family core to the sample adult
interview. In 2018, these questions were answered by a family respondent who may or may not have been also
the sample adult. As part of the questionnaire redesign, these questions are now asked in the sample adult
interview. The location on the survey also changed from early in the interview to near the end of the sample
adult interview.
This indicator is one of eight from the original Early Release Program and reflects sample adults who did not
have a landline telephone in their home but did either have their own working cell phone or lived with someone
who had a working cell phone.
(A)
2018
Full-year
Production
(B)
2018
Quarter 4
Production
(C)
2018
Quarter 4
Bridge
(D)
2019 Full-year
Early Release,
Old weight
(E)
2019 Full-year
Early Release,
New weight
(F)
Within 2018
Q4 Difference
(C - B)
(G)
Weighting
Difference
(E - D)
Combined
Impact
(F + G)
56.0
(55.2 - 56.8)
57.0
(55.5 - 58.6)
58.0
(56.5 - 59.5)
59.9
(58.9 - 60.9)
60.2
(59.2 - 61.2)
1.0 0.3 1.3
Preliminary analysis:
• In 2018, the percentage of adults living in wireless-only households was 56.0%. The 2019 full-year
estimate with the new weight was 60.2%. The observed increase was statistically significant (p < 0.001).
• During the fourth quarter of 2018, the production estimate (57.0%) was 1.0 percentage points lower
than the bridge estimate (58.0%). This comparison suggests a possible questionnaire design effect, but it
was not statistically significant (p = 0.45).
• The 2019 full-year estimates using the old and new weights were similar (59.9% and 60.2%,
respectively). This result (p = 0.82) suggests that the weighting adjustment did not substantially affect
estimates for this indicator.
• Considered together, estimates for 2019 may have shifted upward by 1.3 percentage points due to the
methodological change. This shift due to methodological changes may account for some (but not all) of
the observed increase from 56.0% in 2018 to 60.2% in 2019. The increase from 2018 to 2019 is likely to
reflect actual change over time.
• The increase from 2018 to 2019 is a continuation of the increasing trend since January-June 2015 (see
Figure).
• The increase from January-June 2019 (59.2%) to July-December 2019 (61.3%) was statistically significant
(p = 0.02). This is consistent with an increasing trend since 2015.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 46
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Other categories of telephone ownership have also been evaluated for possible questionnaire design effects.
Statistically significant questionnaire design effects were observed for estimates of the prevalence of phoneless
adults and adults living in landline-only households. During the fourth quarter of 2018, the production estimates
were 1.4 and 1.6 percentage points higher, respectively, than the bridge estimates. For estimates of the
prevalence of adults living in households with both a landline and a wireless telephone, the production estimate
was 2.0 percentage points lower than the bridge estimate, but the comparison was not statistically significant (p
= 0.14). The weighting adjustment did not substantially affect estimates for any of these indicators.
When the questionnaire design and weighting effects are considered together, phoneless estimates for 2019
may have shifted downward by 1.3 percentage points due to the methodological change, landline-only
estimates may have shifted downward by 1.5 percentage points, and dual-user estimates may have shifted
upward by 1.5 percentage points.
Summary
As noted earlier, health policy analysts and other public health professionals are generally interested in whether
there are changes over time in the official estimates for the key indicators from NHIS. That is, they will want to
know whether the preliminary 2019 full-year estimates are higher, lower, or statistically similar to the 2018
estimates as well as the longer-term trend. Table 4 presents the magnitude of the 2018-to-2019 differences for
19 of the key indicators in the NHIS Early Release Program.
However, any observed difference could be affected by the 2019 NHIS questionnaire redesign, the updated
weighting approach, or both. When this occurs, it would not be appropriate to definitively conclude that any
observed difference or lack of difference reflects actual change or no change over time (short term or longer
term). The nature and magnitude of the changes need to be evaluated in light of the impact of the
methodological changes.
Percentage of adults living in wireless-only households
47.4
47.7
49.0
50.5
52.0
53.3
55.2
56.7
59.2
61.3
57.9
60.0
0
10
20
30
40
50
60
70
80
Jan-June
2015
July-Dec
2015
Jan-June
2016
July-Dec
2016
Jan-June
2017
July-Dec
2017
Jan-June
2018
July-Dec
2018
Jan-June
2019
July-Dec
2019
SOURCE: NCHS, National Health Interview Survey.
Percent
Predicted values in
the absence of
methodological
changes
Final estimates, 2015-2018
Early Release
estimates, 2019

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 47
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
In this working paper, NCHS took a preliminary look at estimates for the key indicators that are reported as part
of the NHIS Early Release Program. The extent to which the design changes impacted these key estimates was
evaluated by comparing differences for the same time period (October-December 2018) when both the prior
design and the test for the redesign were in the field simultaneously. Moreover, the impact of the updated
weighting approach was explored by examining differences in estimates derived with the two different
weighting approaches for the same data set (the preliminary microdata files for January-December 2019). A
summary of the results of these preliminary analyses is included in Table 4.
Based on this preliminary evaluation of change from 2018 to 2019, for four of 19 indicators, differences
observed between estimates for 2018 and 2019 may be partially attributable to the NHIS questionnaire
redesign: regularly experienced chronic pain; regularly had feelings of worry, nervousness, or anxiety; current
electronic cigarette use; and did not get needed mental health care due to cost.
For four of the 19 indicators, differences observed between estimates for 2018 and 2019 may be partially
attributable to the updated weighting approach: disability status; current cigarette smoking; lack of health
insurance; and public health plan coverage.
For two of the 19 indicators, differences observed between estimates for 2018 and 2019 may be partially
attributable to both the NHIS questionnaire design and the updated weighting approach: did not get needed
medical care due to cost; and private health insurance coverage.
For six out of the 19 indicators, neither the questionnaire redesign nor the updated weighting approach appears
to have an impact: asthma episode; regularly had feelings of depression; did not take medication as prescribed
to save money; hospital emergency department visit; influenza vaccination; and blood pressure check.
For an additional three indicators (diagnosed hypertension, doctor visit, and adults living wireless-only
households), neither the questionnaire redesign nor the updated weighting approach had a statistically
significant impact, but the size of the observed differences in October-December 2018 was 1.0 percentage point
or greater. The smaller sample size of the fourth-quarter estimates may have limited the ability to detect
statistically significant questionnaire design effects, even with a 0.10 alpha level. Questionnaire design effects
may have slightly (but not significantly) attenuated or enhanced the observed differences.
The NHIS Early Release Program releases quarterly and semiannual estimates for a small set of key health
indicators. The expedited processing, analysis, and dissemination is intended to provide timely tracking of trends
that may be important for programmatic and policy decisions. Some users may be less interested in the impact
of the questionnaire redesign and updated weighting approach on the level of the 2019 full-year Early Release
estimates; rather, they may be more interested in whether the shape and slope of the trend lines differ before
and after the questionnaire redesign or weighting changes. Preliminary conclusions about long-term trends
were included in this report for each of the indicators. However, to more fully examine changes in the shape and
slope of the trend lines, NCHS awaits additional estimates from 2020 and 2021. Meanwhile, within the next
year, NCHS intends to apply the updated weighting approach to estimates from 2016-2018 to further evaluate
its impact.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 48
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
References
1. Olson K. Paradata for nonresponse adjustment. The Annals of the American Academy of Political and Social
Science 645(1):142-170. 2013.
2. Valliant R, Dever JA, Kreuter F. Practical tools for designing and weighting survey samples. New York:
Springer. 2018.

Preliminary Evaluation of the Impact of 2019 NHIS Questionnaire Redesign and Weighting Adjustments Page | 49
U.S. Department of Health and Human Services ● Centers for Disease Control and Prevention ● National Center for Health Statistics
Table 4. Change in estimates from 2018 to 2019 for key indicators and summary of results from the preliminary evaluation of the
impact of the 2019 National Health Interview Survey questionnaire redesign and weighting adjustments
Indicator
2018 Full-
year
Production
2019 Full-
year Early
Release
New Weight
Percentage
point
difference
Possible
questionnaire
design effect?
Possible
weighting
effect?
Health Status
Diagnosed hypertension 27.0 27.1 0.1 Maybe No
Asthma episode 3.5 3.4 -0.1 No No
Regularly experienced chronic pain 20.7 20.6 -0.1 Yes No
Regularly had feelings of worry, nervousness, or anxiety 8.6 11.2 2.6** Yes No
Regularly had feelings of depression 4.4 4.7 0.3 No No
Disability status 10.2 9.2 -1.0** Maybe Yes
Health Behaviors
Current cigarette smoking 13.7 14.2 0.5 No Yes
Current electronic cigarette use 3.2 4.4 1.2** Yes No
Health Care Access
Did not get needed medical care due to cost 6.4 8.3 1.9** Yes Yes
Did not take medication as prescribed to save money 9.2 9.7 0.5 No No
Did not get needed mental health care due to cost 2.6 4.3 1.7** Yes No
Health Care Service Utilization
Doctor visit 84.3 84.9 0.6 Maybe No
Hospital emergency department visit 21.3 21.8 0.5 No No
Influenza vaccination 44.6 46.8 2.2
** No No
Blood pressure check 84.6 88.1 3.5** No No
Health Insurance Coverage (18-64 years)
1
Lack of health insurance 13.3 14.7 1.4* No Yes
Public health plan coverage 19.4 20.4 1.0‡ Maybe Yes
Private health insurance coverage 68.9 66.8 -2.1** Yes Yes
Telephone Ownership
Adults living in wireless-only households 56.0 60.2 4.2** Maybe No
‡
p < 0.10; *p < 0.05; **p < 0.01
NOTES: Confidence intervals for the 2018 and 2019 estimates presented in this table are available in Table 3, columns A and E. Indicators
classified as “maybe” having a questionnaire design effect are those where the difference in the October-December 2018 estimates from
the prior design and the redesign was 1.0 percentage point or greater, but the difference was not statistically significant.
1
For the health insurance coverage indicators, the 2018 full-year estimates are preliminary estimates from the National Health Interview
Survey Early Release Program, rather than final estimates. See text for further information.
SOURCE: NCHS, National Health Interview Survey, 2018 and 2019
