307
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
Introduction: The purpose of this guideline is to establish clinical practice recommendations for the pharmacologic treatment of chronic insomnia in adults,
when such treatment is clinically indicated. Unlike previous meta-analyses, which focused on broad classes of drugs, this guideline focuses on individual
drugs commonly used to treat insomnia. It includes drugs that are FDA-approved for the treatment of insomnia, as well as several drugs commonly used to
treat insomnia without an FDA indication for this condition. This guideline should be used in conjunction with other AASM guidelines on the evaluation and
treatment of chronic insomnia in adults.
Methods: The American Academy of Sleep Medicine commissioned a task force of four experts in sleep medicine. A systematic review was conducted
to identify randomized controlled trials, and the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) process was used to
assess the evidence. The task force developed recommendations and assigned strengths based on the quality of evidence, the balance of benets and
harms, and patient values and preferences. Literature reviews are provided for those pharmacologic agents for which sufcient evidence was available to
establish recommendations. The AASM Board of Directors approved the nal recommendations.
Recommendations: The following recommendations are intended as a guideline for clinicians in choosing a specic pharmacological agent for treatment
of chronic insomnia in adults, when such treatment is indicated. Under GRADE, a STRONG recommendation is one that clinicians should, under most
circumstances, follow. A WEAK recommendation reects a lower degree of certainty in the outcome and appropriateness of the patient-care strategy for
all patients, but should not be construed as an indication of ineffectiveness. GRADE recommendation strengths do not refer to the magnitude of treatment
effects in a particular patient, but rather, to the strength of evidence in published data. Downgrading the quality of evidence for these treatments is predictable
in GRADE, due to the funding source for most pharmacological clinical trials and the attendant risk of publication bias; the relatively small number of eligible
trials for each individual agent; and the observed heterogeneity in the data. The ultimate judgment regarding propriety of any specic care must be made by
the clinician in light of the individual circumstances presented by the patient, available diagnostic tools, accessible treatment options, and resources.
1. We suggest that clinicians use suvorexant as a treatment for sleep maintenance insomnia (versus no treatment) in adults. (WEAK)
2. We suggest that clinicians use eszopiclone as a treatment for sleep onset and sleep maintenance insomnia (versus no treatment) in adults. (WEAK)
3. We suggest that clinicians use zaleplon as a treatment for sleep onset insomnia (versus no treatment) in adults. (WEAK)
4. We suggest that clinicians use zolpidem as a treatment for sleep onset and sleep maintenance insomnia (versus no treatment) in adults. (WEAK)
5. We suggest that clinicians use triazolam as a treatment for sleep onset insomnia (versus no treatment) in adults. (WEAK)
6. We suggest that clinicians use temazepam as a treatment for sleep onset and sleep maintenance insomnia (versus no treatment) in adults. (WEAK)
7. We suggest that clinicians use ramelteon as a treatment for sleep onset insomnia (versus no treatment) in adults. (WEAK)
8. We suggest that clinicians use doxepin as a treatment for sleep maintenance insomnia (versus no treatment) in adults. (WEAK)
9. We suggest that clinicians not use trazodone as a treatment for sleep onset or sleep maintenance insomnia (versus no treatment) in adults. (WEAK)
10. We suggest that clinicians not use tiagabine as a treatment for sleep onset or sleep maintenance insomnia (versus no treatment) in adults. (WEAK)
11. We suggest that clinicians not use diphenhydramine as a treatment for sleep onset and sleep maintenance insomnia (versus no treatment) in adults.
(WEAK)
12. We suggest that clinicians not use melatonin as a treatment for sleep onset or sleep maintenance insomnia (versus no treatment) in adults. (WEAK)
13. We suggest that clinicians not use tryptophan as a treatment for sleep onset or sleep maintenance insomnia (versus no treatment) in adults. (WEAK)
14. We suggest that clinicians not use valerian as a treatment for sleep onset or sleep maintenance insomnia (versus no treatment) in adults. (WEAK)
Keywords: insomnia, treatment, pharmacologic, guideline
Citation: Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, Heald JL. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in
adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(2):307–349.
SPECIAL ARTICLES
Clinical Practice Guideline for the Pharmacologic Treatment of
Chronic Insomnia in Adults: An American Academy of Sleep Medicine
Clinical Practice Guideline
Michael J. Sateia, MD
1
; Daniel J. Buysse, MD
2
; Andrew D. Krystal, MD, MS
3
; David N. Neubauer, MD
4
; Jonathan L. Heald, MA
5
1
Geisel School of Medicine at Dartmouth, Hanover, NH;
2
University of Pittsburgh School of Medicine, Pittsburgh, PA;
3
University of California, San Francisco, San Francisco, CA;
4
Johns Hopkins University School of Medicine, Baltimore, MD;
5
American Academy of Sleep Medicine, Darien, IL
pii: jc-00382-16 http://dx.doi.org/10.5664/jcsm.6470

308
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
TABLE OF CONTENTS
Introduction 308
Background 309
Methodology 312
Clinical Practice Recommendations 315
Orexin receptor agonists
Suvorexant 317
Benzodiazepine receptor agonists
Eszopiclone 318
Zaleplon 321
Zolpidem 323
Benzodiazepines
Triazolam 326
Temazepam 327
Melatonin agonists
Ramelteon 329
Heterocyclics
Doxepin 331
Trazodone 332
Anticonvulsants
Tiagabine 333
Over-the-counter preparations
Diphenhydramine 334
Melatonin 335
L-tryptophan 337
Valerian 338
Literature Reviews 338
Estazolam 338
Quazepam 339
Flurazepam 340
Oxazepam 341
Quetiapine 341
Gabapentin 341
Paroxetine 341
Trimipramine 342
Discussion and Future Directions 342
INTRODUCTION
Aims
This clinical practice guideline was initiated at the request
of the Board of Directors of the American Academy of Sleep
Medicine (AASM), who also reviewed this document and
provided feedback. No formal clinical practice guidelines for
the pharmacological treatment of insomnia have previously
been issued by the AASM, despite the fact that this remains,
by far, the most common approach to therapy, after treatment
of comorbidities. Pharmacotherapy is one of two major ap-
proaches to treatment, the alternative being cognitive behav-
ioral therapies for insomnia (CBT-I), already identied as a
standard of treatment. This paper does not directly address the
relative benets of these two approaches. Rather, the conclu-
sions and recommendations regarding pharmacotherapy must
be considered within the context of specic treatment goals,
comorbidities, prior treatment responses, availability, safety,
patient preference and cost considerations. Despite the clearly
favorable benet to risk ratio of CBT-I, not all patients with an
insomnia disorder can and will derive benet from this treat-
ment alone. This failure may result from inability to access
such treatment (due to availability, cost restraints, etc.), inabil-
ity or unwillingness to participate in the therapy, or treatment
non-responsiveness. Thus, pharmacotherapy, alone or in com-
bination with CBT-I, must continue to be considered a part of
the therapeutic armamentarium, as it currently is for perhaps
25% of the population.
1
Unfortunately, many individuals use
medications or substances (e.g. over-the-counter sleep aids or
alcohol) which are not demonstrated to be effective in manag-
ing insomnia and/or have signicant potential for harm. For
the estimated 3.5% to 7% of individuals receiving prescrip-
tion medication for sleep disturbance,
2–4
signicant knowledge
gaps and anxieties about the proper usage of these agents ex-
ists among the prescribers.
This paper includes a systematic review and meta-analyses
which provides the basis of the initial AASM clinical practice
guideline for pharmacological management of insomnia. The
aims of the present analysis are: (1) to determine the efcacy
of individual prescription and non-prescription medications
for treatment of insomnia; (2) to assess the efcacy of indi-
vidual medications for specic sleep complaints (i.e. difculty
initiating sleep/difculty maintaining sleep); (3) to evaluate the
potential for adverse effects of these drugs; (4) to consider the
evidence concerning efcacy and adverse effects in delineat-
ing evidence-based guidelines for the use of pharmacotherapy
in the management of chronic insomnia; and (5) to offer rec-
ommendations for optimizing quality and uniformity of future
investigations.
This clinical practice guideline is intended to serve as one
component in an ongoing assessment of the individual patient
with insomnia. As discussed elsewhere,
5–7
a comprehensive
initial evaluation should include a detailed history of sleep
complaints, medical and psychiatric history, and medication/
substance use. These factors, together with patient preferences
and treatment availability, should be used to select specic
treatments for specic patients. This clinical practice guide-
line is not intended to help clinicians determine which patient
is appropriate for pharmacotherapy. Rather, it is intended to
provide recommendations regarding specic insomnia drugs
once the decision has been made to use pharmacotherapy. This
guideline is also not intended to recommend one drug over an-
other. Very few comparative efcacy studies have been con-
ducted among these agents. Rather, the guideline provides a
recommendation and evidence base for each individual drug.
The selection of a particular drug should rest on the evidence
summarized here, as well as additional patient-level factors,
such as the optimal pharmacokinetic prole, assessments of
benets versus harms, and past treatment history.
This guideline should be used in conjunction with other
AASM guidelines on the evaluation and treatment of chronic
insomnia. These guidelines indicate that CBT-I is a standard
of treatment and that such treatment carries a signicantly fa-
vorable benet:risk ratio. Therefore, based on these guidelines,
all patients with chronic insomnia should receive CBT-I as a
primary intervention. Medications for chronic insomnia dis-
order should be considered mainly in patients who are unable

309
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
to participate in CBT-I, who still have symptoms despite par-
ticipation in such treatments, or, in select cases, as a temporary
adjunct to CBT-I.
Clinical Guidelines and Practice Parameters
The AASM has issued several guidelines, reviews, and prac-
tice parameters related to the assessment and management of
insomnia. A 2000 review and practice parameter paper ad-
dressed the comprehensive evaluation of chronic insomnia.
5,6
Non-pharmacological management of insomnia has been
the subject of two practice parameter papers.
8–11
No formal,
evidence-based standards of practice for pharmacological
treatment of insomnia have been published, although clinical
guidelines addressing this topic have been issued by various
groups. The Standards of Practice Committee of the AASM
addressed non-prescription treatments for insomnia in a 2006
paper
12
which concluded that there is sparse or little evidence to
support use of these agents for insomnia. Preliminary but con-
icting evidence was noted for valerian and rst-generation
H
1
antagonists for short-term use. A 2005 National Institutes
of Health consensus conference
13
on manifestations and man-
agement of chronic insomnia found moderate-to-high-grade
evidence to support the efcacy of both cognitive-behavioral
therapies and benzodiazepine agonists in the short-term man-
agement of insomnia, but noted a relative paucity of data
concerning long-term usage of such treatments, despite the
chronicity of the condition. Little evidence supporting efcacy
of other widely used treatments (sedating antidepressants and
non-prescription agents) was found.
A 2008 AASM clinical guideline paper on the evaluation
and management of chronic insomnia dened psychological
and behavioral therapies as a standard of treatment (the high-
est level of recommendation at that time).
7
No specic level
of recommendation was offered for pharmacological therapies,
but the consensus recommendation was that such treatment,
when used, should be accompanied by cognitive-behavioral
therapies whenever possible. Short/intermediate acting benzo-
diazepine receptor agonists (benzodiazepines [BZDs] or newer
BZD receptor agonistic modulators [BzRAs]) or ramelteon
were recommended as rst-line pharmacotherapy. Other drugs,
such as sedating antidepressants or anticonvulsant medications
were recommended as second- or third-line agents, particu-
larly when comorbidities (e.g. mood disorder or epilepsy) are
present. Other, non-prescription drugs such as over-the counter
antihistamine sleeping aids and herbal/nutritional agents were
not recommended due to lack of demonstrated efcacy as well
as safety concerns.
A consensus statement from the British Association for
Psychopharmacology
14
assessed evidence related to chronic
insomnia, including management issues, and came to similar
conclusions. CBT interventions were recommended as rst-
line treatment. BzRAs were found effective for short-term use,
although degradation of improvement following discontinua-
tion of hypnotic was noted to be of concern. Limited evidence
and toxicity concerns were cited for other prescription and
non-prescription agents, although prolonged-release melato-
nin was recommended as a rst-line treatment for insomnia in
persons over 55 years.
In May 2016, the American College of Physicians published
its own clinical practice guideline for the management of
chronic insomnia.
15
This guideline makes two major recom-
mendations. The rst is that all patients with chronic insomnia
receive CBT-I as the initial treatment intervention. This is a
strong recommendation based on moderate quality evidence.
The second is that a shared decision-making approach be em-
ployed by clinicians in determining whether pharmacotherapy
should be employed for those patients who did not achieve
adequate response with CBT-I (weak recommendation based
on low quality evidence). The guideline notes that there was
insufcient evidence to draw conclusions regarding the overall
efcacy of pharmacotherapy in the insomnia population. More
specically, there was also insufcient evidence to determine
the efcacy of benzodiazepines, trazodone and melatonin in
the management of chronic insomnia. Studies of more recent
generation sleep aids such as BzRAs, doxepin and suvorexant
found improvement in a number of sleep outcome variable but,
as is the case with our own guideline, much of the evidence
was of low quality. Although evidence is presented for indi-
vidual drugs, there were no specic recommendations made
for single agents. Finally, there was insufcient evidence found
to determine the balance of benets versus harms.
BACKGROUND
Insomnia disorder is dened in the International Classication
of Sleep Disorders, Third Edition
16
as a complaint of trouble
initiating or maintaining sleep which is associated with day-
time consequences and is not attributable to environmental cir-
cumstances or inadequate opportunity to sleep. The disorder
is identied as chronic when it has persisted for at least three
months at a frequency of at least three times per week. When
the disorder meets the symptom criteria but has persisted for
less than three months, it is considered short-term insomnia.
Occasional, short-term insomnia affects 30% to 50% of the
population.
17
The prevalence of chronic insomnia disorder in
industrialized nations is estimated to be at least 5% to 10%.
18,19
In medically and psychiatrically ill populations, as well as in
older age groups, the prevalence is signicantly higher. Chronic
insomnia is associated with numerous adverse effects on func-
tion, health, and quality of life. Epidemiologic studies dem-
onstrate marked impairment in functional status among those
with chronic insomnia.
20,21
Increased rates of work absentee-
ism,
22
and occupational and motor vehicle accidents have also
been widely reported.
23,24
Persistent insomnia has been identi-
ed in multiple studies as a signicant risk factor for the devel-
opment of psychiatric disorders, especially mood disorder.
25,26
This condition is also associated with increased risk of relapse
for depression and alcoholism, as well as adverse effects in
chronic pain populations. More recent investigations suggest
that chronic insomnia is associated with increased risk for car-
diovascular disease. In particular, insomnia with objectively
short sleep time is a signicant risk factor for the development
of hypertension.
27,28
Chronic insomnia imposes substantial economic burdens
on society.
29–31
Estimation of the direct and indirect costs
310
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
of chronic insomnia are complicated by many confounding
variables, but virtually all analyses of these costs indicate
substantially higher economic burden for an insomnia popu-
lation. Direct cost analysis demonstrates signicantly higher
utilization of emergency and ofce health care visits as well
as greater cost for prescription drugs.
32
Likewise, indirect
costs in the form of work absenteeism, loss of productivity,
and insomnia-related accidents contribute signicantly to
the economic burden of the disorder. In the United States, a
2009 study
33
found that direct and indirect costs for insom-
nia patients were in excess of $2,000/year greater than those
of a matched non-insomnia group. Total direct and indirect
cost estimates for insomnia in the United States differ sub-
stantially due to variability in methodologies. Nevertheless,
estimates suggest direct costs of $2–16 billion per year and
indirect costs of $75–100 billion. The latter are accounted
for in large part by worker absenteeism, presenteeism (lower
productivity due to daytime impairment), and work-related
accidents.
29
General treatment measures for insomnia include the
treatment of comorbid medical and psychiatric conditions,
modifying sleep-interfering medications and substances, and
optimizing the sleep environment. Specic treatments for in-
somnia fall into two primary categories. Non-pharmacological
therapies, largely cognitive behavioral in nature, have been
the subject of numerous meta-analyses and practice guide-
lines.
10,34–37
Pharmacological therapy, including over-the-coun-
ter sleep aids and alcohol, is the most widely used treatment for
insomnia, yet no evidence-based clinical practice guidelines
have been published to date by the AASM. This paper includes
a systematic review and meta-analyses which provide the basis
of the initial AASM clinical practice guideline for pharmaco-
logical management of insomnia.
History of Hypnotic Usage
Pharmacological agents have been used for the treatment of in-
somnia throughout much of recorded history. Prior to the 20th
century, opioids, various herbal preparations, bromide salts,
and alcohol were the primary hypnotic alternatives. Through
the rst half of the 20
th
century, barbiturate and related com-
pounds became the most commonly used agents for manage-
ment of anxiety and sleep disturbance, as well as epilepsy. By
mid-century, however, the adverse side effects and lethal over-
dose potential of these agents became recognized, contributing
to curtailment of use.
The rst BZD, chlordiazepoxide, was introduced to the
United States market in 1963, followed shortly by diazepam.
Flurazepam, the rst benzodiazepine approved by the Food
and Drug Administration (FDA) as a hypnotic, became avail-
able in 1970 and rapidly supplanted the use of barbiturates
and similar compounds for treatment of insomnia. Zolpidem,
the rst United States nonbenzodiazepine, benzodiazepine
receptor agonist (non-BZD, or BzRA) hypnotic, became
available in 1992 and remains the most widely prescribed
hypnotic medication, accounting for 87.5% of all BzRA pre-
scriptions in a recent survey of hypnotic use.
38
Since 2005,
a melatonin agonist (ramelteon), a low dose form of the se-
dating tricyclic medication (doxepin), and, most recently,
an orexin receptor antagonist (suvorexant) have entered the
United States market.
Current Hypnotic Usage
Hypnotic prescribing practices have varied in recent decades
as availability of various agents and safety concerns have
evolved. Despite the development of numerous BZD hypnotic
medications of varying durations of action, the overall fre-
quency of hypnotic prescriptions for insomnia declined dur-
ing the two decades from 1970–1990, from 3.5% to 2.5%.
39
Due to apparent concerns regarding the potential for toler-
ance and dependency with BZD use, physicians increasingly
prescribed sedating antidepressants “off label,” especially
trazodone, despite the absence of efcacy studies for this or
any other sedating antidepressants for treatment of insomnia.
Survey of ofce-based physician prescribing practices for the
period 1987–1996 revealed an over 50% decline in BZD hyp-
notic prescriptions accompanied by a nearly 150% increase
in trazodone prescriptions.
40
Overall prescriptions for insom-
nia declined by about 25% during this period. A more recent
study,
38
utilizing the National Health and Nutrition Examina-
tion Survey (NHANES) data from 1999–2010, analyzed the
frequency of usage of medications commonly used for insom-
nia. This includes BZDs approved for treatment of insomnia,
BzRAs, ramelteon, trazodone, doxepin and quetiapine. The au-
thors report that just under 3% of the sample population used
one of these agents within the past month. In contrast to the
apparent trends of preceding decades, frequency of usage of
any medication commonly used for insomnia increased over
the decade, from 2.0% in the rst year sampled to 3.5% in the
nal year (2009–2010). BzRAs, predominantly zolpidem, were
most commonly prescribed (1.23% of the population), followed
by trazodone (0.97%), BZDs (0.4%), quetiapine (0.32%) and
doxepin. However, it should be noted in this and other studies
that other agents—especially BZDs not approved for insomnia,
other antidepressants, antipsychotics, and analgesics—are not
included in these data. It seems likely that the true prevalence
of medication use for sleep disturbance is higher than these
gures suggest. In fact, a subsample analysis of the NHANES
data from 2005–2008 found that approximately 19% of re-
spondents reported use of at least one pill or medication for
sleep in the past month. The 2005 National Sleep Foundation’s
(NSF) survey of sleep habits found that 7% of respondents re-
port using a prescription medication to improve sleep at least a
few nights per month.
41
Physicians and other health care providers have consistently
expressed reservations about the use of medication, particu-
larly BZDs and BzRAs, to treat insomnia. They cite concerns
regarding safety and dependency as key issues. However, they
also note a lack of awareness and/or availability of alternative
treatments.
42
Many favor an initial approach of treating asso-
ciated comorbidities and advising good sleep hygiene.
43
An
ever-increasing amount of data makes it clear that the latter
approach is very often unsuccessful, leaving providers feeling
compelled to prescribe medications. Most of those surveyed
recognize the need for additional, non-pharmacological treat-
ment for their patients, but cite a number of barriers to acquir-
ing such treatment.
44
311
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
Data concerning use of non-prescription agents for sleep
promotion are limited. The aforementioned NSF survey re-
ported that nearly one in four respondents used some form of
sleep aid “at least several times per month.” Eleven percent
stated that they used alcohol to help sleep, 9% used over-the
counter sleep aids, and 2% used melatonin.
Previous Meta-Analyses
Several meta-analyses of pharmacotherapy for insomnia have
been conducted. Nowell and colleagues
45
conducted a meta-
analysis of 22 randomized controlled trials (RCTs) of BZDs and
zolpidem for treatment of primary insomnia published from
1966 to 1996. They found moderate effect sizes (d = 0.56 to 0.71
for key sleep variables) for improvement with these agents, but
noted limitations in the duration of trials and lack of follow-up
study regarding outcome. A 2000 study commissioned by the
Canadian Medical Association
46
evaluated 45 RCTs (n = 2,672)
of BZDs for treatment of primary insomnia. This investigation
found reduction in sleep latency (non-signicant in objective
[polysomnography; PSG] assessment but signicant in subjec-
tive reports) and a somewhat larger and signicant increase in
total sleep time by both objective and subjective reports. The
authors also note an increase in adverse events with BZDs
(pooled odds ratio for any adverse event = 1.8) and call into
question the risk/benet ratio for these agents.
A comparative evaluation of the efcacy of hypnotic drugs
was conducted by the National Centre for Clinical Excellence
of the UK.
47
In summary, the analysis found little difference
among the numerous BZDs and BzRAs among the 24 studies
which directly compared more than one drug. Some small dif-
ferences were noted, such as shorter sleep latency but less total
sleep time with zaleplon when compared to zolpidem. On the
whole, major differences in adverse effects were not observed
between drugs. Meta-analyses in this report were few due to
limitations of data reporting.
Glass and colleagues
48
compared benets versus risks for
all sedative hypnotic agents in a meta-analysis of RCTs of ac-
tive agent versus placebo or other active compound in popula-
tions > 60 years of age and free of contributing comorbidities.
They reported a small effect size for improvement in sleep
quality (d = 0.14). Separate analysis of BZDs alone yielded
a somewhat more robust improvement in quality (d = 0.37).
Signicant but modest increase in total sleep time (TST) and
reduction in number of awakenings (NOA) was also found for
all sedative-hypnotics and for the BZD group alone, although
effect sizes are not reported for these variables. Cognitive
side effects were more common with sedative-hypnotics. The
authors note that, with respect to the sleep quality measures
reported for all sedative hypnotics, the number needed to
treat is 13, while the number needed to harm is 6, thereby
indicating an unfavorable risk/benet ratio for this popula-
tion. Independent analysis of this ratio for BZDs alone was
not conducted.
A 2007 meta-analysis
49
evaluated 105 RCTs of BZDs, Bz-
RAs and antidepressant medications for treatment of chronic
insomnia in the adult populations regardless of comorbidi-
ties. In summary, the analysis indicates moderate and sig-
nicant improvement in major sleep parameters with both
BZDs and BzRAs in both objective (PSG) and subjective
(sleep diary) assessments, with the exception of PSG results
for wake after sleep onset (WASO) and TST, which yielded
results just below the range of signicance. Far fewer stud-
ies were available for antidepressants. These showed signi-
cant reduction in sleep latency and a non-signicant trend
toward reduced WASO. Four studies utilizing PSG mea-
sures showed substantial improvement in TST (79.6 min)
while single subjective data set suggested reduction in TST
compared to placebo. The authors note substantial hetero-
geneity of data which was reduced in subgroup analyses by
type of drug. Between-groups comparisons showed no sig-
nicant efcacy differences between BZDs and non-BZDs.
All three groups demonstrated signicantly higher rates of
adverse events versus placebo. BZDs exhibited a higher rate
of adverse events than BzRAs.
Huedo-Medina and colleagues
50
conducted systematic re-
view and meta-analysis of data on BzRAs submitted to the
United States Food and Drug Administration from 15 studies.
They found that BzRAs produce signicant reduction of sleep
latency by both objective and subjective measures with effect
sizes of 0.36 and 0.33, respectively. Other sleep variables did
not show signicant differences but limited data reporting on
these variables precluded denitive conclusions.
Winkler and Doering
51
analyzed data from 31 randomized
controlled trials of sleep-promoting substances used for treat-
ment of primary insomnia. Studies included BZDs, BzRAs,
melatonin agonists, antidepressants and other sedating com-
pounds. Only studies which included objective (PSG) data
were considered. The meta-analysis revealed that both BZDs
and BzRAs were signicantly more effective than antide-
pressants. Both demonstrated small to moderate effect sizes
for major sleep variables. BZDs were somewhat superior to
BzRAs for subjective sleep latency (SL). No analysis of treat-
ment-emergent adverse events was reported.
Finally, Wilt and colleagues
52
conducted a systematic re-
view and meta-analyses of 35 randomized, controlled trials of
at least 4 weeks duration, and harms information from 11 long-
term observational trials. Their review found that eszopiclone,
zolpidem, and suvorexant improved short-term outcomes,
with small effect sizes and low-to-moderate strength evidence.
They also found that evidence for BZDs, melatonin agonists,
and antidepressants was insufcient or of too-low strength.
Finally, they concluded that there is insufcient evidence to
determine the comparative effectiveness or long-term efcacy
of pharmacotherapies for insomnia.
In summary, these meta-analyses suggest small to moderate
effect sizes for most major sleep outcome variables with both
BZDs and BzRAs. However, some of these analyses report
signicant increases in treatment-emergent adverse events and
raise concerns regarding their relative risk:benet ratio. Data
supporting the use of sedating antidepressants in the treatment
of insomnia are scant. Overall, the studies are limited by lack
of availability of high quality evidence and considerable vari-
ability in design and methodology across investigations. All of
these analyses addressed efcacy only for major drug groups
(e.g., BZDs, BzRAs), failing to address issues of safety or ef-
cacy for individual agents.

312
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
METHODOLOGY
Expert Task Force
In order to develop this clinical practice guideline, the AASM
commissioned a task force composed of content experts in the
eld of insomnia, an AASM Board of Directors liaison, and
AASM Science and Research Department staff members. Prior
to appointment, the content experts were required to disclose
all potential conicts of interest according to the AASM’s
policy. In accordance with the AASM’s conicts of interest
policy, task force members with a Level 1 conict were not
allowed to participate. Task force members with a Level 2
conict were required to recuse themselves from any related
discussion or writing responsibilities. All relevant conicts of
interest are listed in the Disclosures section.
PICO Questions
A PICO (Patient, Population or Prob lem, Intervention, Com-
parison, and Outcomes) question template was developed to be
the focus of this guideline:
“ In adult patients diagnosed with primary chronic insomnia,
how does [intervention] improve [outcomes], compared to
placebo?”
The PICO question template was approved by the AASM
Board of Directors. The task force identied the pharmaco-
logical interventions of interest, based on FDA approval status
and common off-label usage. Based on their expertise, the task
force developed a list of patient-oriented clinically relevant
outcomes that are indicative of whether a treatment should be
recommended for clinical practice. The task force then rated
their relative importance and selected the top six outcomes.
The following outcomes were determined to be “critical” or
“important” for clinical decision making across all interven-
tions: sleep latency, wake after sleep onset, total sleep time,
quality of sleep, number of awakenings, and sleep efciency
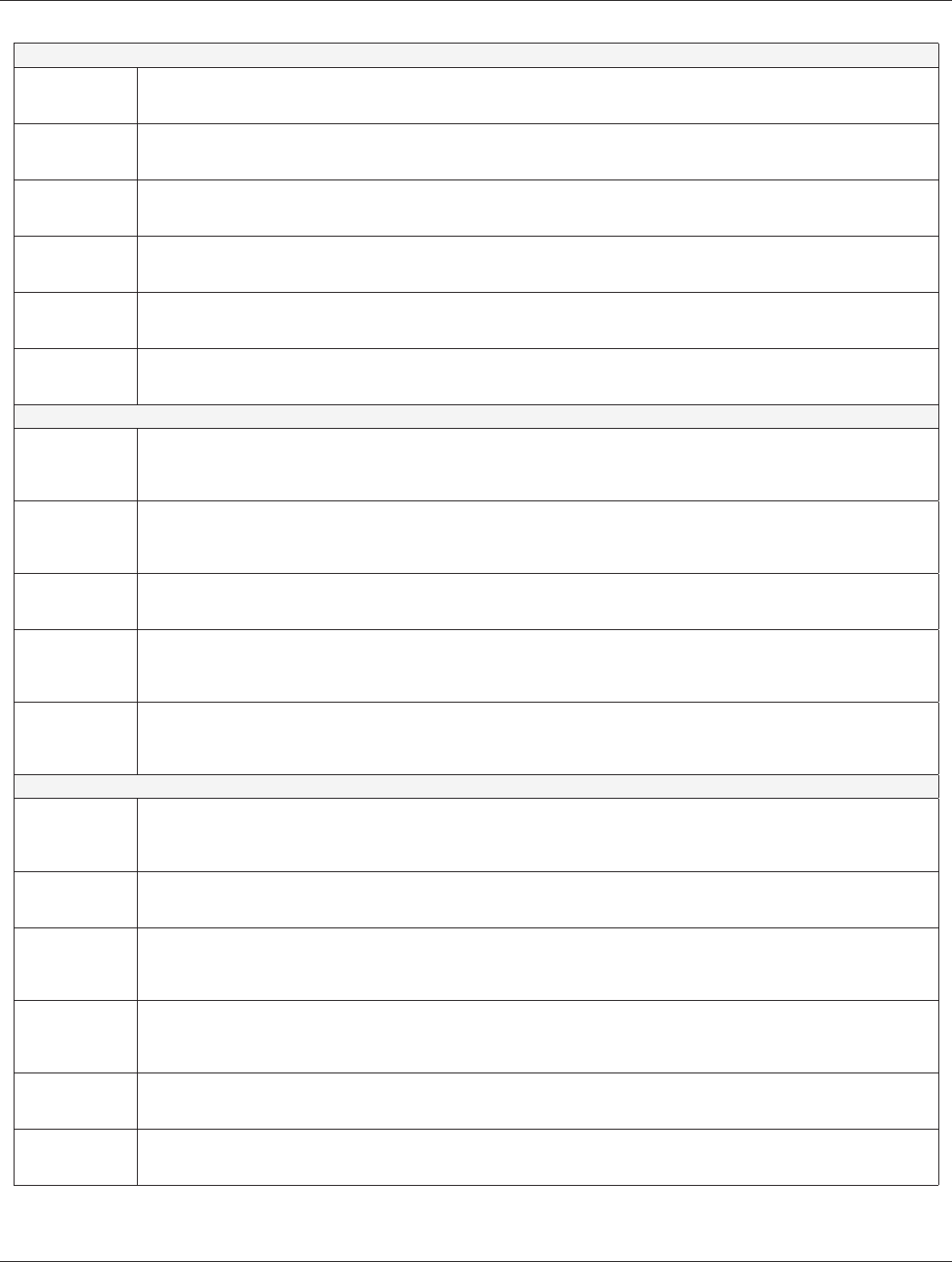
(Table 1). The task force then determined which outcomes
were “critical” for clinical decision making for each individual
intervention (Table 2). Lastly, clinical signicance thresholds,
used to determine if a change in an outcome was clinically sig-
nicant, were dened for each outcome by task force clinical
judgement, prior to statistical analysis (Table 3). These deci-
sions were made by nominal consensus of the task force, based
Table 1—PICO question parameters.
Population Intervention Comparison Outcomes
Adult patients diagnosed with
primary chronic insomnia
1. Diphenhydramine †
2. Doxepin*
3. Eszopiclone*
4. Melatonin †
5. Ramelteon*
6. Suvorexant*
7. Temazepam*
8. Tiagabine**
9. Trazodone**
10. Triazolam*
11. Tryptophan †
12. Valerian + hops †
13. Zaleplon*
14. Zolpidem*
Placebo control Sleep latency (SL)
Total sleep time (TST)
Wake after sleep onset (WASO)
Quality of sleep (QOS)
Sleep efciency (SE)
Number of awakenings (NOA)
* = FDA-approved, indicated for the treatment of insomnia. ** = FDA-approved, off-label usage for the treatment of insomnia. † = Over-the-counter
medication. Sleep latency is dened as the time to fall asleep following bedtime. PSG sleep latency may be reported as time to onset of rst epoch of
N1 (Stage 1) sleep, or, in more recent studies, as latency to persistent sleep (LPS), or time to onset of rst 10 consecutive min of sleep. Total sleep time
is dened as the total time spent in bed, minus sleep latency and wake after sleep onset. Wake after sleep onset is dened as the sum of wake times
from sleep onset to the nal awakening. Quality of sleep is a patient-reported measure, the denition of which varies by measurement tools and patient
perceptions. Sleep efciency is dened as the percentage of time spent in bed during which sleep occurs; it is calculated as (TST / time in bed) × 100.
Number of awakenings is dened as the number of awakenings after sleep onset, excluding the nal awakening.
Table 2—“Critical” outcomes by intervention.
TST SL WASO QOS
Diphenhydramine
Doxepin
Eszopiclone
Melatonin
Ramelteon
Suvorexant
Temazepam
Tiagabine
Trazodone
Triazolam
Tryptophan
Valerian-hops
Zaleplon
Zolpidem
TST = total sleep time, SL = sleep latency, WASO = wake after sleep
onset, QOS = quality of sleep.
313
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
on their expertise and familiarity with the literature and clini-
cal practice.
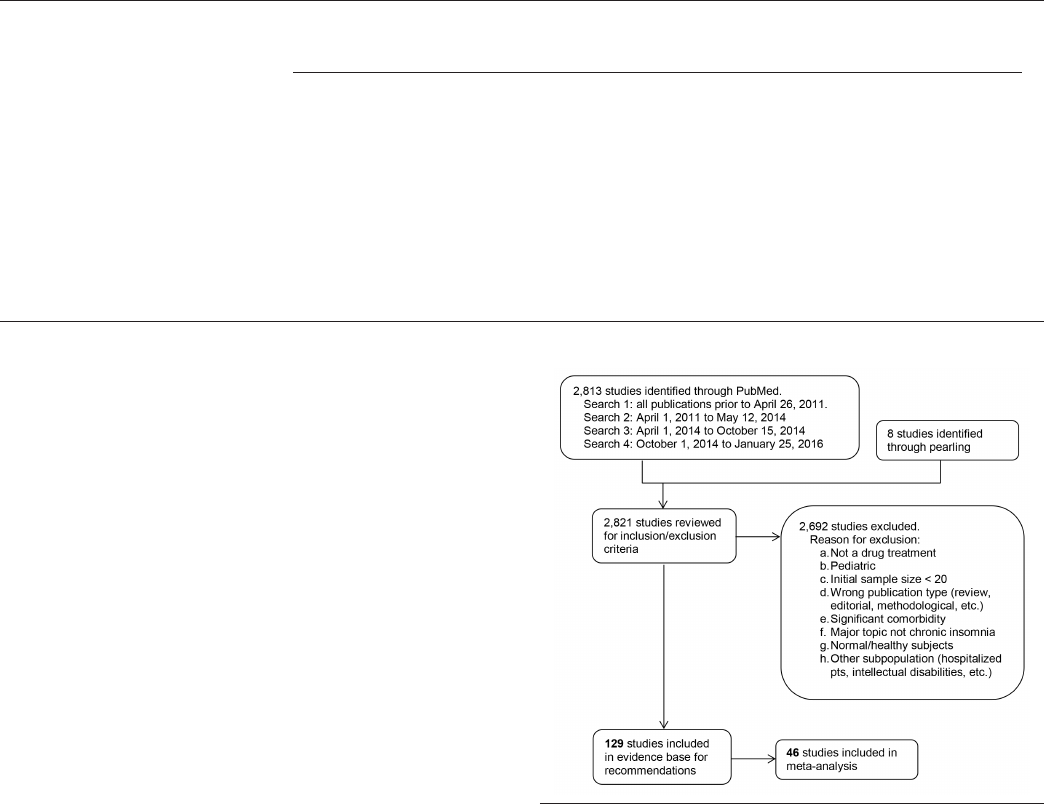
Literature Searches, Evidence Review and Data
Extraction
Multiple literature searches were performed by the AASM
research staff using the PubMed database throughout the
guideline development process (see Figure 1). Keywords and
Medical Subject Headings (MeSH) terms were:
• insomnia OR sleep initiation and maintenance disorder
NOT transient AND
• clinical trial OR randomized controlled trial
• NOT editorial, letter, comment, case reports, biography,
review
The full literature search string can be found in the supple-
mental material. Searches were performed on April 26, 2011
(search 1), May 12, 2014 (search 2), October 15, 2014 (search 3),
and January 25, 2016 (search 4). Based on their expertise and
familiarity with the insomnia literature, task force members
submitted additional relevant literature and screened reference
lists to identify articles of potential interest. This served as a
“spot check” for the literature searches to ensure that important
articles were not missed.
Abstracts from all retrieved articles were individually as-
sessed by two task force members to deter mine whether the
publication should be included or excluded from further consid-
eration in the project. Exclusion criteria can be found in Figure 1.
A total of 129 publications were approved for inclusion.
Full texts of accepted articles were reviewed and data per-
taining to GRADE
53
for the outcomes of interest were extracted
into spreadsheets by AASM staff. All data pertaining to ad-
verse events were extracted into separate spreadsheets. Arti-
cles that met inclusion criteria but did not report outcomes of
interest were rejected from the nal evidence base. If outcome
data were not presented in the format necessary for statistical
analysis (i.e., mean, standard deviation, and sample size), the
authors were contacted in an attempt to obtain the necessary
data. Finally, clinicaltrials.gov was used as a nal resource
for attempting to obtain data necessary for completing statis-
tical analyses. If the necessary data were not available from
the publication, the author, or clinicaltrials.gov, the paper was
included in the evidence base as supporting evidence, but was
not used for statistical analysis or for determining quality of
evidence. Of the 129 accepted publications, 46 were included
in the statistical and meta-analysis.
For some drugs, none of the accepted publications provided
data that could be used for statistical analysis. In these cases,
the task force did not make a recommendation, but provided a
literature review of these accepted papers instead. These pub-
lications are not included in Figure 1.
Statistical and Meta-Analysis
For outcomes of interest, data from baseline and last-treatment
time points were used for all statistical and meta-analyses.
Data from crossover trials were treated as parallel groups.
Change-from-baseline values were also used for statistical
and meta-analyses, when the change-from-baseline standard
deviation was provided or could be calculated from the pro-
vided statistic. Standardized mean difference (SMD) was used
for meta-analyses of quality of sleep (QOS) when data were
reported using variable scales. Analyses were limited to FDA-
approved doses. For adverse events, all data presented in the
accepted papers were used for statistical and meta-analysis. All
calculations and meta-analyses were performed using Review
Manager 5.3 software. Whenever possible, meta-analyses were
Figure 1—Evidence base ow diagram.
Table 3—Clinical signicance threshold.
Measurement Tool
a
Outcome Polysomnography Actigraphy Subjective
Sleep latency (SL), min 10 10 20
Total sleep time (TST), min 20 20 30
Wake after sleep onset (WASO), min 20 20 30
Quality of sleep (QOS), varies
b
Varies Varies Varies
Sleep efciency (SE), % 5 5 10
Number of awakenings (NOA), n 2 2 0.5
a
Clinical signicance was judged to be present when a specic agent led to a mean change in the outcome of this magnitude, compared to placebo.
b
For standardized mean difference (SMD), an effect size of 0.5 is considered clinically signicance (based on Cohen’s d).
314
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
performed by pooling data across studies for each outcome and
adverse event. The evidence was grouped for analysis based on
the drug, dosage, clinical outcome of interest, and methodol-
ogy used to obtain the data (e.g., data obtained by PSG were
analyzed separately from data obtained by sleep diary).
All meta-analyses were performed as per-treatment analyses
using the random effects model. For most interventions, abso-
lute effects of drug treatments are represented by the mean dif-
ference (MD) ± standard deviation (SD) of post-treatment drug
versus post-treatment placebo. Meta-analyses for adverse events
are presented as risk difference. The result of each meta-analysis
is displayed as a forest plot. Pooled results are expressed as the
total number of patients, MD and 95% condence interval (CI)
between the experimental treatment and placebo.
Interpretation of clinical signicance for outcomes of inter-
est was conducted by comparing the absolute effects of drug
treatment to the clinical signicance threshold previously de-
termined by the task force for each outcome of interest. Inter-
pretation of adverse events was based upon the risk difference
and clinical expertise of the task force.
Strength of Recommendations
The GRADE approach (Grades of Recommendation, Assess-
ment, Development and Evaluation) was used for the assess-
ment of quality of evidence. For details on how the AASM
uses GRADE to develop its clinical practice guidelines, refer
to Morgenthaler et al.
53
The task force assessed the following
three components to determine the direction and strength of
a recommendation: quality of evidence, balance of benecial
and harmful effects, and patient values and preferences.
For the determination of the quality of evidence for an inter-
vention, the task force used objective data whenever possible
(e.g., PSG). When only subjective data were available (e.g.,
sleep diaries), this evidence was used to determine the over-
all quality of evidence. The decision to use objective data as
the primary determinant of quality of evidence was based on
the preference for an objective measure of physiologic changes
for determining clinically signicant efcacy, the standard-
ization of sleep parameter measurements and reporting, and
the current requirements of PSG data for FDA approval of
hypnotic medications. The results of this assessment are pre-
sented as summary of ndings tables for each intervention (see
Tables S1–S24 in the supplemental material).
The task force developed recommendation statements con-
sistent with GRADE methodology based on the balance of the
following factors:
1. Quality of evidence. Quality of evidence was based
exclusively on the studies that could be included
in meta-analyses. The task force determined their
overall condence that the estimated effect found in
the literature was representative of the true treatment
effect that patients would see, based on the following
criteria: overall risk of bias (randomization, blinding,
allocation concealment, selective reporting, and
author disclosures); imprecision (when 95% CI cross
the clinical signicance thresholds); inconsistency (I
2
cutoff of 75%); indirectness (study population); and
risk of publication bias (funding sources). The task
force also considered the consistency of the supporting
evidence (i.e. data the met inclusion criteria, but could
not be included in the meta-analyses). However such
evidence did not impact judgments regarding the
quality of evidence or nal recommendations.
2. Benets versus harms. The task force determined if the
benecial outcomes of the intervention outweighed any
harmful side effects based on the following criteria:
meta-analysis (if applicable); analysis of any harms/
side effects reported within the accepted literature; and
the clinical expertise of the task force.
3. Patient values and preferences. The task force
determined if patient values and preferences would
be generally consistent, and if patients would use the
intervention based on the body of evidence reviewed.
These judgments were based on the clinical expertise
of the task force members and any data published on
the topic relevant to patient preferences.
Taking these major factors into consideration, and adhering to
GRADE recommendations, the task force assigned a direction
(for or against) and strength (STRONG or WEAK) for each
recommendation statement.
Additional information is provided in the form of “Remarks”
immediately following the recommendation statements, when
deemed necessary by the task force. Remarks are based on the
evidence evaluated during the systematic review, and are in-
tended to provide context for the recommendations.
Approval and Interpretation of Recommendations
A draft of the guideline was made available for public comment
for a two-week period on the AASM website. The task force took
into consideration all the comments received and made revisions
when appropriate. Based on recommendations from public com-
ments, the task force decided to include data from clinicaltrials.
gov, which allowed the development of a recommendation for the
use of suvorexant. Due to a conict of interest, Andrew Krys-
tal did not participate in the development of the suvorexant rec-
ommendation. The nal guideline was submitted to the AASM
Board of Directors who approved these recommendations.
The recommendations in this guideline dene principles of
practice that should meet the needs of most adult patients, when
pharmacologic treatment of chronic insomnia is indicated. This
guideline should not, however, be considered inclusive of all
proper methods of care or exclusive of other methods of care
reasonably used to obtain the same results. A STRONG rec-
ommendation is one that clinicians should, under most circum-
stances, always be following when pharmacological treatment
is indicated (i.e., something that might qualify as a quality
measure). A WEAK recommendation reects a lower degree
of certainty in the appropriateness of the patient-care strategy
and requires that the clinician use his/her clinical knowledge
and experience, and refer to the individual patient’s values and
preferences to determine the best course of action. The ultimate
judgment regarding propriety of any specic care must be made
by the clinician, in light of the individual circumstances pre-
sented by the patient, available diagnostic tools, accessible treat-
ment options and resources, as well as safety considerations.

315
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
of ndings tables are presented in the supplemental material. A
summary of the recommendations and GRADE determinations
is presented in Table 4. A summary of the recommendations,
“critical” outcomes, and side effects is presented in Table 5.
It is essential that the recommendations which follow be
interpreted within the appropriate context of clinical prac-
tice. Readers will note that all specic recommendations fall
within the “weak” (for or against) classication of the GRADE
system. This should not be construed to mean that no sleep-
promoting medications are clearly efcacious or indicated
in the treatment of chronic insomnia. Hypnotic medications,
along with management of comorbidities and non-pharmaco-
logical interventions such as CBT, are an important therapeutic
The AASM expects this guideline to have an impact on
professional behavior, patient outcomes, and, possibly, health
care costs. This clinical practice guideline reects the state of
knowledge at the time of publication and will be reviewed and
updated as new information becomes available.
CLINICAL PRACTICE RECOMMENDATIONS
The following clinical practice recommendations are based on
the systematic review and evaluation of evidence following the
GRADE methodology. Remarks are intended to provide con-
text for the recommendations. All meta-analyses and summary
Table 4—Summary of clinical practice recommendations and GRADE components of decision-making.
Treatment Recommendation
Direction and
Strength of
Recommendation
Quality
of
Evidence
Benets
and Harms
Assessment
Patients’ Values and Preferences
Assessment
Orexin receptor agonists
Suvorexant
This recommendation is based on trials of 10, 15/20,
and 20 mg doses of suvorexant.
We suggest that clinicians use suvorexant as a
treatment for sleep maintenance insomnia (versus no
treatment) in adults.
WEAK Low
Benets
outweigh
harms
The majority of patients would use this
treatment (over no treatment), but many
would not.
BZD receptor agonists
Eszopiclone
This recommendation is based on trials of 2 mg and
3 mg doses of eszopiclone.
We suggest that clinicians use eszopiclone as a
treatment for sleep onset and sleep maintenance
insomnia (versus no treatment) in adults.
WEAK Very low
Benets
outweigh
harms
The majority of patients would use this
treatment (over no treatment), but many
would not.
Zaleplon
This recommendation is based on trials of 10 mg
doses of zaleplon.
We suggest that clinicians use zaleplon as a
treatment for sleep onset insomnia (versus no
treatment) in adults.
WEAK Low
Benets
outweigh
harms
The majority of patients would use this
treatment (over no treatment), but many
would not.
Zolpidem
This recommendation is based on trials of 10 mg
doses of zolpidem.
We suggest that clinicians use zolpidem as a
treatment for sleep onset and sleep maintenance
insomnia (versus no treatment) in adults.
WEAK Very low
Benets
outweigh
harms
The majority of patients would use this
treatment (over no treatment), but many
would not.
Benzodiazepines
Triazolam
This recommendation is based on trials of 0.25 mg
doses of triazolam.
We suggest that clinicians use triazolam as a
treatment for sleep onset insomnia (versus no
treatment) in adults.
WEAK High
Benets
approx equal
to harms
The majority of patients would use this
treatment (over no treatment), but many
would not.
Temazepam
This recommendation is based on trials of 15 mg
doses of temazepam.
We suggest that clinicians use temazepam as a
treatment for sleep onset and sleep maintenance
insomnia (versus no treatment) in adults.
WEAK Moderate
Benets
outweigh
harms
The majority of patients would use this
treatment (over no treatment), but many
would not.
Melatonin agonists
Ramelteon
This recommendation is based on trials of 8 mg
doses of ramelteon.
We suggest that clinicians use ramelteon as a
treatment for sleep onset insomnia (versus no
treatment) in adults.
WEAK Very low
Benets
outweigh
harms
The majority of patients would use this
treatment (over no treatment), but many
would not.
Heterocyclics
Doxepin
This recommendation is based on trials of 3 mg and
6 mg doses of doxepin.
We suggest that clinicians use doxepin as a treatment
for sleep maintenance insomnia (versus no treatment)
in adults.
WEAK Low
Benets
outweigh
harms
The majority of patients would use this
treatment (over no treatment), but many
would not.
Trazodone
This recommendation is based on trials of 50 mg
doses of trazodone.
We suggest that clinicians not use trazodone as
a treatment for sleep onset or sleep maintenance
insomnia (versus no treatment) in adults.
WEAK Moderate
Harms
outweigh
benets
The majority of patients would use this
treatment (over no treatment), but many
would not.
Anticonvulsants
Tiagabine
This recommendation is based on trials of 4 mg
doses of tiagabine.
We suggest that clinicians not use tiagabine as a
treatment for sleep onset or sleep maintenance
insomnia (versus no treatment) in adults.
WEAK Very low
Harms
outweigh
benets
The majority of patients would not use
this treatment (over no treatment), but
many would.
Over-the-counter preparations
Diphenhydramine
This recommendation is based on trials of 50 mg
doses of diphenhydramine.
We suggest that clinicians not use diphenhydramine
as a treatment for sleep onset and sleep maintenance
insomnia (versus no treatment) in adults.
WEAK Low
Benets
approx equal
to harms
The majority of patients would not use
this treatment (over no treatment), but
many would.
Melatonin
This recommendation is based on trials of 2 mg
doses of melatonin.
We suggest that clinicians not use melatonin as
a treatment for sleep onset or sleep maintenance
insomnia (versus no treatment) in adults.
WEAK Very low
Benets
approx equal
to harms
The majority of patients would use this
treatment (over no treatment), but many
would not.
L-tryptophan
This recommendation is based on trials of 250 mg
doses of tryptophan.
We suggest that clinicians not use tryptophan as
a treatment for sleep onset or sleep maintenance
insomnia (versus no treatment) in adults.
WEAK High
Harms
outweigh
benets
The majority of patients would use this
treatment (over no treatment), but many
would not.
Valerian
This recommendation is based on trials of variable
dosages of valerian and valerian-hops combination.
We suggest that clinicians not use valerian as a
treatment for sleep onset or sleep maintenance
insomnia (versus no treatment) in adults.
WEAK Low
Benets
approx equal
to harms
The majority of patients would not use
this treatment (over no treatment), but
many would.
approx = approximately.
316
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
Table 5—Summary of “critical” outcomes by indication.
Recommended for Treating Sleep Onset Insomnia
Eszopiclone
Sleep latency: Mean reduction was 14 min greater, compared to placebo (95% CI: 3 to 24 min reduction); Quality of sleep*: Moderate-to-Large
a
improvement in quality of sleep, compared to placebo; Side effects: See Recommendation 2, “Harms”
This recommendation is based on trials of 2 mg and 3 mg doses of eszopiclone.
Ramelteon
Sleep latency: Mean reduction was 9 min greater, compared to placebo (95% CI: 6 to 12 min reduction); Quality of sleep*: No improvement
b
in
quality of sleep, compared to placebo; Side effects: See Recommendation 7, “Harms”
This recommendation is based on trials of 8 mg doses of ramelteon.
Temazepam
Sleep latency: Mean reduction was 37 min greater, compared to placebo (95% CI: 21 to 53 min reduction); Quality of sleep*: Small
a
improvement
in quality of sleep, compared to placebo; Side effects: See Recommendation 6, “Harms”
This recommendation is based on trials of 15 mg doses of temazepam.
Triazolam
Sleep latency*: Mean reduction was 9 min greater, compared to placebo (95% CI: 4 to 22 min reduction); Quality of sleep*: Moderate
c
improvement
in quality of sleep, compared to placebo; Side effects: See Recommendation 5, “Harms”
This recommendation is based on trials of 0.25 mg doses of triazolam.
Zaleplon
Sleep latency: Mean reduction was 10 min greater, compared to placebo (95% CI: 0 to 19 min reduction); Quality of sleep*: No improvement
b
in
quality of sleep, compared to placebo; Side effects: See Recommendation 3, “Harms”
This recommendation is based on trials of 5 mg and 10 mg doses of zaleplon.
Zolpidem
Sleep latency: Mean reduction was 5–12 min greater, compared to placebo (95% CI: 0 to 19 min reduction); Quality of sleep*: Moderate
a
improvement in quality of sleep, compared to placebo; Side effects: See Recommendation 4, “Harms”
This recommendation is based on trials of 10 mg doses of zolpidem.
Recommended for Treating Sleep Maintenance Insomnia
Doxepin
Total sleep time: Mean improvement was 26–32 min longer, compared to placebo (95% CI: 18 to 40 min improvement); Wake after sleep onset:
Mean reduction was 22–23 min greater, compared to placebo (95% CI: 14 to 30 min reduction); Quality of sleep*: Small-to-moderate
a
improvement
in quality of sleep, compared to placebo; Side effects: See Recommendation 8, “Harms”
This recommendation is based on trials of 3 mg and 6 mg doses of doxepin.
Eszopiclone
Total sleep time: Mean improvement was 28–57 min longer, compared to placebo (95% CI: 18 to 76 min improvement); Wake after sleep onset:
Mean reduction was 10–14 min greater, compared to placebo (95% CI: 2 to 18 min reduction); Quality of sleep*: Moderate-to-Large
a
improvement in
quality of sleep, compared to placebo; Side effects: See Recommendation 2, “Harms”
This recommendation is based on trials of 2 mg and 3 mg doses of eszopiclone.
Temazepam
Total sleep time: Mean improvement was 99 min longer, compared to placebo (95% CI: 63 to 135 min improvement); Wake after sleep onset: Not
reported; Quality of sleep*: Small
a
improvement in quality of sleep, compared to placebo; Side effects: See Recommendation 6, “Harms”
This recommendation is based on trials of 15 mg doses of temazepam.
Suvorexant
Total sleep time: Mean improvement was 10 min longer, compared to placebo (95% CI: 2 to 19 min improvement); Wake after sleep onset:
Mean reduction was 16–28 min greater, compared to placebo (95% CI: 7 to 43 min reduction); Quality of sleep*: Not reported; Side effects: See
Recommendation 1, “Harms”
This recommendation is based on trials of 10, 15/20, and 20 mg doses of suvorexant.
Zolpidem
Total sleep time: Mean improvement was 29 min. longer, compared to placebo (95% CI: 11 to 47 min. improvement); Wake after sleep onset: Mean
reduction was 25 min greater, compared to placebo (95% CI: 18 to 33 min reduction); Quality of sleep*: Moderate
a
improvement in quality of sleep,
compared to placebo; Side effects: See Recommendation 4, “Harms”
This recommendation is based on trials of 10 mg doses of zolpidem.
Not Recommended for Treating either Sleep Onset or Sleep Maintenance Insomnia
Diphenhydra mine
Sleep latency: Mean reduction was 8 min greater, compared to placebo (95% CI: 2 min increase to 17 min reduction); Total sleep time: Mean
improvement was 12 min longer, compared to placebo (95% CI: 13 min reduction to 38 min improvement); Quality of sleep*: No improvement
a
in
quality of sleep, compared to placebo; Side effects: See Recommendation 11, “Harms”
This recommendation is based on trials of 50 mg doses of diphenhydramine.
Melatonin
Sleep latency: Mean reduction was 9 min greater, compared to placebo (95% CI: 2 to 15 min reduction); Quality of sleep*: Small
a
improvement in
quality of sleep, compared to placebo; Side effects: See Recommendation 12, “Harms”
This recommendation is based on trials of 2 mg doses of melatonin.
Tiagabine
Total sleep time: Mean improvement was 1–7 min longer, compared to placebo (95% CI: 7 min reduction to 15 min improvement); Wake after sleep
onset: Mean reduction was 1–9 min greater, compared to placebo (95% CI: 6 min increase to 25 min reduction); Quality of sleep*: No-to-Small
a
improvement in quality of sleep, compared to placebo; Side effects: See Recommendation 10, “Harms”
This recommendation is based on trials of 4 mg doses of tiagabine.
Trazodone
Sleep latency*: Mean reduction was 10 min greater, compared to placebo (95% CI: 9 to 11 min reduction); Wake after sleep onset: Mean reduction
was 8 min greater, compared to placebo (95% CI: 7 to 9 min reduction); Quality of sleep*: No improvement
d
in quality of sleep, compared to
placebo; Side effects: See Recommendation 9, “Harms”
This recommendation is based on trials of 50 mg doses of trazodone.
L-tryptophan
Sleep latency: Not reported; Wake after sleep onset*: Mean reduction was 10 min greater, compared to placebo (95% CI: 4 to 15 min reduction);
Quality of sleep*: Small
e
improvement in quality of sleep, compared to placebo; Side effects: see Recommendation 13, “Harms”
This recommendation is based on trials of 250 mg doses of tryptophan.
Valerian
Sleep latency: Mean reduction was 9 min greater, compared to placebo (95% CI: 0 to 18 min reduction); Quality of sleep*: Not reported;
Side effects: See Recommendation 14, “Harms”
This recommendation is based on trials of variable dosages of valerian and valerian-hops combination.
Drugs are listed alphabetically. All reported measures are based on polysomnographic data, unless otherwise noted. *Based on subjective reporting.
a
Based
on Cohen’s d: 0.2 = small effect; 0.5 = moderate effect; 0.8 = large effect.
b
Based on a 7-point Likert scale (1 = excellent, 7 = very poor).
c
Based on a 4-point
scale (1 = good, 4 = poor).
d
Based on a 4-point scale (1 = excellent, 4 = poor).
e
Based on a 3-point scale (sleep quality index: 1 = low, 3 = high).

317
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
option for chronic insomnia. The strength of recommendations
within the GRADE system are driven by the degree of con-
dence in a variety of factors related to the intervention includ-
ing (1) the availability of specic data regarding efcacy; (2)
the quality of that data, and (3) other considerations such as
potential risks, impact of treatment, patient values and prefer-
ences, and perceived burden of treatment.
The existing data regarding sleep-promoting medications
imposes limits on the degree of condence as a result of sev-
eral factors. These include: (1) a high degree of variability in
the statistical information presented. Many studies, especially
older studies, do not present results that meet the criteria for
meta-analysis within GRADE and are, by necessity, excluded
from formal analysis; (2) a signicant degree of variability in
sleep outcomes within and across studies. Such variability
produces a “downgrading” of the quality of evidence within
GRADE; (3) industry sponsorship. Very few clinical trials with
adequate sample size have been sponsored by agencies outside
of industry. As a result, the quality of evidence for a vast ma-
jority of available data is downgraded due to potential publi-
cation bias associated with such sponsorship; (4) a paucity of
systematic data collection and analysis of treatment-emergent
adverse events. Absent such information, it is difcult to as-
sign a high degree of condence to estimations of benet:risk
ratio; and (5) absence of outcome data (such as functional sta-
tus or prevention of complications of chronic insomnia) that
would inform judgments regarding the impact of therapy.
The strength (or weakness) of these recommendations
speaks as much, or more, to the limitations of the data as it
does to the relative benets and risks of the treatments per se.
Clinicians must continue to exercise appropriate judgement,
based not only on the recommendations presented herein, but
also on individual patient characteristics, comorbidities, and
patient preferences in the prescribing of sleep-promoting med-
ications and general management of chronic insomnia.
Finally, the literature review, meta-analyses, and recom-
mendations are based only on FDA-approved doses. This
should not be interpreted as a recommendation for the use of
a specic dose in clinical practice. Numerous factors, includ-
ing, but not limited to, age, sex, comorbidities, and concurrent
use of other medications may affect dosage recommendations.
Clinical judgment is necessary in determining appropriate
dosage, on a patient-by-patient basis.
Orexin receptor agonists
Suvorexant for the Treatment of Chronic Insomnia
Recommendation 1: We suggest that clinicians use
suvorexant as a treatment for sleep maintenance insomnia
(versus no treatment) in adults. [WEAK]
Remarks: This recommendation is based on trials of 10,
15/20, and 20 mg doses of suvorexant.
Summary
Two RCTs
54,55
evaluated suvorexant for treatment of chronic
primary insomnia. The statistical analyses and recommen-
dation are based on data available on clinicaltrials.gov. The
overall quality of evidence was low due to imprecision and
risk of publication bias. The overall evidence for suvorexant
was weakly in favor of its effectiveness for the treatment of
sleep maintenance insomnia only. Objective reports of wake
after sleep onset (PSG) showed clinically signicant reduction
at both 10 mg and 20 mg dosages. Subjective TST data dem-
onstrated improvement, but failed to meet clinical signicance.
Objective reports (PSG) at the 10 mg and 15/20 mg dosages
showed minimal improvements in sleep latency that failed to
meet clinical signicance. However objective reports (PSG) at
20 mg dose did show clinically signicant reduction in sleep
latency, suggesting that suvorexant may improve sleep onset at
higher dosages. PSG sleep efciency (SE) results demonstrate
improvements that are near or above the level for clinical sig-
nicance. PSG number of awakenings (NOA) was not statisti-
cally signicantly reduced or increased in either study. Finally,
sleep quality ratings showed minimal change.
Adverse events were assessed in both studies. Overall fre-
quency of adverse events was not signicantly increased ver-
sus placebo. There was no evidence of daytime residual or
withdrawal symptoms. Therefore the task force judged the
overall benets to outweigh the potential harms. Based on their
clinical judgement, the task force determined that the majority
of patients would use suvorexant over no treatment.
See Tables S1–S3 in the supplemental material.
Discussion
Two RCTs
54,55
evaluated suvorexant for treatment of chronic
primary insomnia. However, data were not presented in a way
that could be used for statistical analyses; therefore the statisti-
cal analyses and recommendation are based on data available
on clinicaltrials.gov. Additional outcomes data from Herring
2012 and 2016 are discussed below as supporting evidence.
Herring 2012
55
evaluated adults 18–64 years of age with
DSM-IV primary insomnia in a randomized placebo-con-
trolled crossover study which included two 4-week trial pe-
riods. Sixty-two subjects received 10 mg suvorexant and 61
received 20 mg. Subjects underwent PSG at the end of week
4. Sleep diary data were also obtained. The primary endpoint
was sleep efciency; secondary endpoints included latency to
persistent sleep and wake after sleep onset. Inclusion criteria
were LPS > 20 min and WASO > 60 min.
Herring 2016
54
conducted two randomized placebo-con-
trolled parallel trials of 3 months each (i.e. trial 1 and trial 2).
Only data from trial 1 were available for statistical analyses.
Adults 18- to 64-years-old and adults > 65 with primary in-
somnia were included. Two-hundred fty four and 239 patients
were randomized to suvorexant 15/20 mg in the two trials, re-
spectively. The dosages of interest for this analysis were 20
mg for younger adults and 15 mg for older adults. Data for
the two dosages were pooled for analysis. Inclusion criteria
were LPS > 20 min and WASO > 60 min. Sleep diary data was
collected for all patients and a subset underwent PSG. Both
studies reported data as difference between placebo and drug
change from baseline.
Sleep latency: Herring 2012
55
found a reduction of 2.3 min
(95% CI: 13.68 min lower to 9.08 min higher) for suvorexant
318
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
10 mg when compared to placebo (not considered clinically
signicant). The quality of evidence was low due to impre-
cision and potential publication bias. At the 20 mg dosage, a
clinically signicant reduction versus placebo of 22.3 min was
reported (95% CI: 33.77 to 10.83 min lower). The quality of
evidence was MODERATE due to potential publication bias.
LPS in the rst trial of Herring 2016
54
showed reductions of
8.1 min (95% CI: 13.85 to 2.35 min lower), and failed to meet
clinical signicance. The quality of evidence was low due to
imprecision and potential publication bias. LPS in the second
trial of Herring 2016 was not available for statistical analyses.
However, published data show a reduction of 0.3 min, which
also fails to meet the clinical signicance threshold.
Subjective latency, reported as TSO in Herring 2016
54
trial 1,
showed reductions at the pooled 15/20 mg dosages (−5.2 min;
95% CI: 0.3 to 10.1 min lower) that failed to meet the clini-
cal signicance threshold. The quality of evidence was mod-
erate due to potential publication bias. Herring 2016
54
trial 2
reported reductions in TSO of 7.6 min, while TSO reported
in the Herring 2012
55
study was reduced at both dosages (−3.0
min and −4.3 min at 10 mg and 20 mg, respectively); none of
these changes met the clinical signicance threshold.
total Sleep time: Herring 2016, trial 1, reported improve-
ments in subjectively reported total sleep time of 10.6 min with
15/20 mg dosages (95% CI: 1.79 to 19.41 min higher), which
did not meet the clinical signicance threshold. The quality
of evidence for this outcome was moderate based on potential
publication bias.
PSG TST was reported only in the Herring 2012
55
inves-
tigation. At both 10 mg and 20 mg, clinically signicant im-
provement was seen versus placebo (+22.3 min and +49.9 min,
respectively).
Neither suvorexant 10 mg (+5.5 min) nor 20 mg (−1.8 min)
produced statistically or clinically signicant improvement in
subjective TST versus placebo at 4 weeks (Herring 2012). In
trial 2 of the 15/20 mg dosages (Herring 2016
54
), subjective
TST was improved (+22.1 min), although the mean change falls
below the clinical signicance threshold.
Wake after Sleep onSet: Both studies reported PSG
WASO. Herring 2012
55
found clinically signicant reduction of
WASO at both 10 mg and 20 mg (−21.4 min; 95% CI: 6.66 to
36.34 min lower; −28.1 min; 95% CI: 13.13 to 43.07 min lower,
respectively). The quality of evidence was low due to impre-
cision and potential publication bias. Herring 2016,
54
trial 1,
reported reductions of −16.6 min (95% CI: 8.33 to 24.87 min
lower) with low quality of evidence due to imprecision and po-
tential publication bias. Herring 2016
54
trial 2 reported a 31.1 min
reduction in WASO. Reductions of subjective WASO in the two
trials of 15/20 mg suvorexant in the Herring 2016
54
study did not
meet clinical signicance thresholds (−2.4 min and −7.7 min).
Quality of Sleep: Sleep quality reductions were not statis-
tically signicant in either study.
Sleep efficiency: Herring 2012
55
found PSG SE improve-
ment of +4.7% (95% CI: 0.97 to 8.43% higher) for 10 mg and
+10.4% (95% CI: 13.13 to 43.07 min lower) for 20 mg, with low
and moderate quality of evidence due to imprecision and po-
tential publication bias. These values approximate (10 mg) or
exceed (20 mg) the clinical signicance threshold of 5%.
number of aWakeningS: Number of awakenings showed
no signicant reduction in either study.
overall Quality of evidence: The overall quality of
evidence for these studies was low due to imprecision and po-
tential publication bias.
HarmS: Neither study found a signicant increase in one
or more adverse events versus placebo for suvorexant in the
10–20 mg range. Rates of serious adverse events were negli-
gible and not signicantly different between suvorexant and
placebo. Frequency of daytime somnolence was increased in
the 15/20 mg doses (Herring 2012
55
: placebo 0.4%; 20 mg 4.9%.
Herring 2016
54
: placebo = 3.4%; 15/20 mg = 5.1% [trial 1]; pla-
cebo = 3.1%; 15/20 mg = 8.4%). The degree of somnolence was
reported to be typically mild to moderate and did not often
result in discontinuation. Frequency of somnolence was noted
to increase signicantly in dose-dependent fashion at dosages
exceeding FDA-recommended levels.
Assessments of withdrawal symptoms and daytime perfor-
mance decrements did not reveal clinically signicant ndings
in either domain. There was no evidence of the emergence of
narcolepsy symptoms.
patientS’ valueS and preferenceS: The task force de-
termined that a majority of patients would likely use suvorex-
ant compared to no treatment. This assessment reects the task
force’s clinical judgment, based on suvorexant’s efcacy for
reduction of WASO and improvement in TST and SE and its
relatively benign side effect prole.
BZD receptor agonists
Eszopiclone for the Treatment of Chronic Insomnia
Recommendation 2: We suggest that clinicians use
eszopiclone as a treatment for sleep onset and sleep
maintenance insomnia (versus no treatment) in adults.
[WEAK]
Remarks: This recommendation is based on trials of 2 mg
and 3 mg doses of eszopiclone.
Summary
Six RCTs evaluated eszopiclone 2 mg for the treatment of
chronic primary insomnia.
56–61
The overall quality of evidence
was downgraded to low due to imprecision and risk of publica-
tion bias. The evidence for eszopiclone 2 mg was weakly in
favor of its efcacy for improving sleep onset disturbance and
total sleep time. Meta-analysis data from three studies which
reported objective sleep latency showed a clinically signicant
mean reduction in PSG sleep latency.
58,60,61
Four studies which
evaluated subjective total sleep time demonstrated a signicant
mean increase versus placebo.
57–59,61
Assessment of PSG SE in
319
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
two studies
58,61
and subjective sleep quality in four studies
57,59–61
revealed improvements which fell just below the threshold for
clinical signicance. Measures of reduction in wake time after
sleep onset and number of awakenings revealed trends toward
improvement which fell below the dened level of clinical sig-
nicance. Meta-analysis of adverse effects, derived from all
six studies, indicated no signicant differences versus placebo.
Six studies assessed the effects of eszopiclone 3 mg for
treatment of chronic primary insomnia.
57,60– 64
The quality of
evidence for these studies as a whole was downgraded to very
low due to signicant heterogeneity, imprecision and poten-
tial publication bias. The collective evidence for eszopiclone 3
mg was weakly in favor of efcacy for improving sleep onset,
total sleep time, sleep efciency, number of awakenings and
sleep quality. The meta-analysis data from three studies dem-
onstrated clinically signicant reduction in objective sleep la-
tency.
60–62
Four studies likewise revealed clinically signicant
increase in mean subjective total sleep time.
57,61,63,64
PSG sleep
efciency, reported in two studies
61,62
also exceeded the thresh-
old for clinically signicant improvement, as did subjective
sleep quality, which was reported in all six studies included
in meta-analysis. A trend in the direction of reduced WASO
was observed, but did not reach clinical signicance. Insuf-
cient data were available for meta-analysis of eszopiclone 3
mg adverse effects.
Overall, the benets of eszopiclone 2 mg and 3 mg were
judged to be greater than the potential harms. Based on clinical
judgment, the task force determined that the majority of well-
informed patients would use eszopiclone over no treatment.
This judgement is based on the evidence of improvement in
sleep latency, total sleep time, sleep efciency and sleep qual-
ity, coupled with its low potential for adverse events.
See Figures S1–S7, S68–S69, and Tables S4 and S5 in the
supplemental material.
Discussion
A total of nine studies were included in the meta-analyses
for eszopiclone 2 mg and 3 mg.
56–64
Three of these studies in-
cluded only older adults (> 65 years).
56,58,59
The remainder in-
cluded younger adults, typically 21–65 years of age. Inclusion
criteria for most of these studies required persistent subjective
sleep latency > 30 min and TST < 6.5 h.
57–62
Ancoli-Israel and
colleagues
56
studied 388 older adults for 12 consecutive weeks
of nightly eszopiclone 2 mg. Inclusion criteria for this study
specied TST < 6 h and WASO > 45 min. Outcome data were
patient-reported. McCall and colleagues
58
also reported on
two-week administration of 2 mg eszopiclone versus placebo
to 254 to older adults. In addition to sleep latency and TST
inclusion criteria, subjects were required to have WASO > 20
min. PSG was conducted on nights 1, 2, 13, and 14. Scharf
and colleagues
59
administered 1 and 2 mg of eszopiclone or
placebo nightly to 231 older adults for two weeks, employing
nightly patient-reported data.
Erman and colleagues
57
evaluated multiple dosages of
eszopiclone (1, 2, 2.5, and 3 mg versus placebo and an active
control (zolpidem 10 mg) in 65 adult subjects (age 21–65) who
received each intervention for two nights, followed by 3–7 day
washout, in randomized sequences. PSG was conducted for the
two nights on each treatment. The primary endpoint was la-
tency to persistent sleep, with secondary endpoints of SE and
WASO. Uchimura and colleagues
60
employed a similar cross-
over design with eszopiclone doses of 1, 2, and 3 mg, zolpidem
10 mg and placebo in 65 patients. PSG was conducted during
each two-night intervention. Primary endpoints were objective
latency to persistent sleep (LPS) and subjective SL. Zammit
and colleagues
61
examined eszopiclone 2 and 3 mg vs. placebo
for 44 consecutive nights, with PSG on nights 1, 15, 29. Patient-
reported data were collected for nights 1, 15, 29, 43, and 44.
Primary endpoint was PSG-dened LPS.
Krystal and colleagues
63
investigated six-month nightly
use of eszopiclone 3 mg versus placebo in 788 adults. Patient-
reported data were collected at weekly intervals. Similarly,
Walsh and colleagues
64
reported on nightly use of eszopiclone
3 mg in 830 adults, with weekly patient-reported data. Finally,
Boyle and colleagues,
62
in a study designed primarily to as-
sess next-day driving skill, report subjective data from a single
night of eszopiclone 3 mg versus placebo.
Sleep latency: Three studies assessed LPS as determined
by PSG for eszopiclone 2 mg.
58,60,61
The McCall investiga-
tion
58
focused exclusively on older adults and demonstrated the
greatest reduction in LPS. The mean reduction in LPS versus
placebo for the three studies (−14.87 min; CI: −5.47 to −24.27
min) exceeded the threshold for clinical signicance. The qual-
ity of evidence was LOW due to imprecision and potential pub-
lication bias.
All six trials of eszopiclone 2 mg reported subjective sleep
latency.
56–61
As noted above, three of the six included only older
adults. Mean difference from placebo fell slightly below the
clinical signicance threshold (−17.78 min; CI: −7.04 to −28.52
min). The quality of this evidence was low due to imprecision
and potential publication bias.
Three studies investigated PSG LPS with eszopiclone 3
mg.
60–62
The mean difference in LPS (−13.63 min; CI: −3.7
to −23.56 min) fell below the clinical signicance threshold.
The quality of evidence was VERY LOW due to heterogene-
ity, imprecision and potential publication bias. Subjective SL
with eszopiclone 3 mg was reported in four studies.
57,61,63,64
The
mean difference exceeded the clinical signicance threshold
(−25.00 min; CI: −13.94 to −36.07 min). The greatest reduc-
tions were reported in the extended 6-month trials of Krystal
and Walsh. Quality of evidence was low due to imprecision
and potential publication bias.
Two additional studies not included in the meta-analysis
reported subjective SL with eszopiclone 3 mg. Soares and
colleagues
65
analyzed efcacy in perimenopausal/early meno-
pausal women with sleep onset complaints. Joffe et al.
66
ex-
amined outcomes in perimenopausal/menopausal women who
exhibited hot ashes and manifested either sleep onset or main-
tenance problems. The reductions in sleep latency versus pla-
cebo for these two studies (−15.7 and −17.8 min, respectively)
were within the overall range found in the meta-analysis.
total Sleep time: Only one eszopiclone study reported
adequate objective total sleep time data. Therefore meta-anal-
ysis was not possible for this outcome at either dosage.
58
Four
320
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
studies included subjective TST for eszopiclone 2 mg.
57–59,61
The meta-analysis revealed a mean increase in TST of 27.53
min versus placebo, just below the threshold for clinical sig-
nicance of 30 min. The quality of evidence was LOW due
to imprecision and potential publication bias. The only study,
noted above, which reported objective TST (in patients > 65
years) found an increase in TST of 28.6 min greater than pla-
cebo, consistent with the subjective results.
Four studies included adequate data for subjective TST
meta-analysis for eszopiclone 3 mg.
57,61,63,64
These studies dem-
onstrate substantially greater increases in TST at this dosage
with a mean difference versus placebo of 57.1 min, exceeding
the clinical signicance threshold. The quality of evidence was
moderate, due to potential publication bias.
The two studies of eszopiclone 3 mg in perimenopausal/
early menopausal women revealed mean increases in subjec-
tive TST (versus placebo) of +66.5 min and +23.0 min.
65,66
Wake after Sleep onSet: Two studies were included in
the meta-analysis of objective WASO for eszopiclone 2 mg.
58,61
The mean reduction in WASO was 10.02 min greater than pla-
cebo, below the clinical signicance level of 20 min for PSG
data. The quality of evidence was rated as moderate due to
potential publication bias. The condence interval (−2.77 to
−17.27 min) fell below the threshold.
Five studies reported adequate data for subjective WASO
meta-analysis.
56–59,61
The mean difference versus placebo was
below the threshold for clinical signicance (−4.74 min; CI
−11.87 to +2.39 min). The quality of evidence was moderate
due to potential publication bias.
The data for PSG and patient-reported WASO with eszopi-
clone 3 mg demonstrated greater reduction of WASO than with
2 mg, but below clinical signicance levels. The two studies
including PSG WASO demonstrated a mean reduction of 14.69
min versus placebo (CI: −11.69 to −17.68 min).
61,62
Quality of
evidence was moderate (potential publication bias). Subjective
WASO for 3 mg was reported in four studies with mean reduc-
tion of 15.14 min (CI: −8.16 to −22.11 min). Quality of evidence
was low due to imprecision and potential publication bias.
Krystal and colleagues
63
published an independent sub-
group analysis of subjective WASO data from their 6-month
nightly trial of 3 mg, in order to evaluate the impact of base-
line WASO severity on outcome. They identied a positive
relationship between baseline WASO severity and degree of
improvement in WASO (as determined by eszopiclone/placebo
difference) at all time points. The two investigations of meno-
pausal women found eszopiclone-placebo mean differences for
subjective WASO of 37.3 and 14.9 min, respectively.
65,66
Quality of Sleep: The meta-analysis for sleep quality with
eszopiclone 2 mg included four studies and found a moderate
effect size of +0.47 SMD (CI: +0.32 to +0.63 SMD).
57,59–61
The
quality of evidence was moderate due to imprecision and po-
tential publication bias. Sleep quality ratings for 3 mg, based
on six studies, showed a large effect size of +0.82 SMD (CI:
+0.41 to +1.24 SMD), although quality of evidence was very
low due to imprecision, heterogeneity and potential publica-
tion bias.
57,60– 64
In addition to the studies included in meta-analysis, Soares
and colleagues
65
reported statistically signicant improvement
in quality for eszopiclone 3 mg in their study of perimeno-
pausal and postmenopausal women.
Sleep efficiency: Two studies reported PSG SE for eszopi-
clone 2 mg.
58,61
The mean improvement in SE of 4.83% fell be-
low the signicance threshold of 5%. (CI: 2.21 to +7.46%). For
the 3 mg dosage, PSG SE exceeded the clinical signicance
threshold at 5.61%.
61,62
The quality of evidence for both doses
was low due to imprecision and potential publication bias.
In studies outside the meta-analysis, Joffe
66
reported a 14.6%
improvement versus placebo in SE with 3 mg.
number of aWakeningS: The PSG NOA for 2 mg showed
an increase of 0.12 awakenings based on two studies.
58,61
Evi-
dence quality was MODERATE. Subjective NOA was based
on four studies and likewise demonstrated no clinically signi-
cant difference from placebo. Evidence quality was moderate
due to potential publication bias.
57–59,61
overall Quality of evidence: The overall quality of
evidence in the meta-analytic data from these studies was
downgraded to very low for several reasons. Substantial het-
erogeneity across studies was noted for multiple outcomes.
The data were also downgraded for imprecision, due to the
relatively large condence intervals, which cross the clinical
signicance thresholds for several outcomes. All of these stud-
ies were industry sponsored, resulting in further downgrading
of evidence due to potential publication bias. The quality of ev-
idence for individual outcomes ranged from moderate to very
low. Therefore the overall quality of evidence was very low.
HarmS: Sufcient data for meta-analysis of side effects was
available only for the 2 mg eszopiclone dosage. Five side effects
(dizziness, dry mouth, headache, somnolence and unpleasant
taste) were included. Four studies examined dizziness with 2
mg eszopiclone and found no difference from placebo.
57,58,60,61
Two studies reported adequate data for dry mouth.
58,61
A +0.06
risk difference was reported for eszopiclone. For headache,
four studies found essentially no difference between eszopi-
clone and placebo.
56,57,59,61
The same was true for next-day som-
nolence, based on ve studies.
57–61
Finally, ve studies found a
+0.07 risk difference for unpleasant taste.
56–59,61
Although meta-analysis was not possible for eszopiclone 3
mg, individual studies reported results which are consistent
with those of the 2 mg dosage. Krystal and colleagues
63
re-
ported numerically higher adverse event rates for somnolence
(eszopiclone 9.1%; placebo 2.6%), unpleasant taste (26.1%
versus 5.6%), dry mouth (6.6% versus 1.5%), and dizziness
(9.8% versus 3.1%). Boyle
62
studied braking reaction time and
other performance measures and found no difference between
eszopiclone 3 mg and placebo. Walsh
64
reported signicantly
greater frequencies of adverse events including somnolence
(eszopiclone: 8.8% versus placebo: 3.2%), unpleasant taste
(19.7% versus 1.1%) and myalgia (6.0% versus 2.9%). No dif-
ference was seen on the Benzodiazepine Withdrawal Scale
scores following discontinuation. Zammit
61
demonstrated no

321
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
impairment in digit symbol substitution at either 2 mg or 3 mg.
Joffe and colleagues
66
reported a 15.2% risk for metallic taste,
but placebo rate for this side effect was not identied. Soares
and colleagues
65
found a signicant increase in unpleasant
taste with eszopiclone (17.6% versus 0.5%). Headache fre-
quency was no different and report of dry mouth was slightly
increased for eszopiclone (4.0% to 1.4%).
In summary, the task force found that there was weak ev-
idence of efcacy in the treatment of sleep onset and main-
tenance insomnia, with limited or no consistent evidence of
adverse events in excess of placebo, with the possible excep-
tion of unpleasant taste. Therefore, benets were deemed to
marginally outweigh harms.
patientS’ valueS and preferenceS: The task force de-
termined that a majority of patients would likely use eszopi-
clone compared to no treatment. This assessment reects the
task force’s clinical judgment, based on eszopiclone’s efcacy
for sleep onset and maintenance, and its relatively benign side
effect prole.
Zaleplon for the Treatment of Chronic Insomnia
Recommendation 3: We suggest that clinicians use
zaleplon as a treatment for sleep onset insomnia (versus no
treatment) in adults. [WEAK]
Remarks: This recommendation is based on trials of 10 mg
doses of zaleplon.
Summary
Two RCTs meeting inclusion criteria investigated the use of
zaleplon 5 or 10 mg in the treatment of chronic primary in-
somnia.
67,68
One of these reported only subjective outcomes
67
,
and one reported subjective and PSG outcomes.
68
No meta-
analysis was possible for these studies, due to the manner of
reporting results. The overall quality of evidence from these
studies was downgraded to low due to imprecision and po-
tential publication bias; both studies were industry supported.
The overall evidence for zaleplon 10 mg support its efcacy
for the treatment of sleep onset insomnia. At the 10 mg dose,
one objective (PSG) study demonstrated a reduction in sleep
latency from baseline that met the criterion for clinical signi-
cance, with an approximately 9.5 min difference from placebo.
Subjective sleep latency, reported in one study, showed a non-
signicant change of −11.4 min. Subjective TST increased by
approximately 21.5 min, but the difference from placebo was
not statistically signicant. WASO was not signicantly dif-
ferent from placebo. Similarly, subjective sleep quality showed
minimal differences from placebo. The overall evidence for
zaleplon 5 mg did not support its efcacy for treatment of any
insomnia symptoms, based on self-report studies only. No
PSG studies at the 5 mg dose met inclusion criteria. Treatment-
emergent adverse events showed no signicant difference from
placebo for zaleplon 10 mg or 5 mg, and only one study sug-
gested a small increase in rebound using self-reported TST as
the outcome.
Data from three additional studies of zaleplon 5–10 mg met
our inclusion criteria but could not be included in meta-analyses
because key outcome data were presented in insufcient de-
tail.
69–71
However, the results of these three studies were con-
sistent with those of the two studies presented above, in nding
differences from placebo in subjective SOL but no signicant
differences in subjective TST or sleep quality.
Overall, the evidence for efcacy of zaleplon 10 mg is
marginal, and the evidence for harm appears equivalent to
placebo; therefore potential benets minimally outweigh po-
tential harms. The lack of evidence for efcacy of zaleplon 5
mg makes any potential benets equivalent to its minimal po-
tential harms.
Based on clinical judgment, the task force determined that
the majority of well-informed patients would use zaleplon
over no treatment. This judgement is based on the minimal
evidence of improved sleep latency across PSG and self-report
domains, coupled with a low potential for adverse events.
See Tables S6 and S7 in the supplemental material.
Discussion
Evidence from two RCTs which investigated the use of za-
leplon 5 or 10 mg in the treatment of chronic primary insomnia
was included in the main analysis of outcomes, although meta-
analysis could not be performed because data were presented
as medians, or as means with no standard deviation.
67,68,70
Subjects in each study met criteria for primary insomnia or
insomnia associated with nonpsychotic mental disorder by ei-
ther DSM-III-R or DSM-IV criteria, together with quantitative
criteria for self-reported sleep disturbance (SOL > 30 min, plus
either subjective TST < 6.5 h, WASO > 30 min, or > 3 awaken-
ings) and associated daytime complaints. Walsh 2000
68
also re-
quired PSG LPS of > 20 min on two screening nights. Patients
were 18–65 years of age
68,70
or 65 years and older.
67
Study de-
signs included randomized, double-blind, placebo run-in with
zaleplon 5–20 mg or placebo for 14–35 nights, followed by a
2–7 night placebo substitution. Walsh
68
used PSG outcomes,
whereas the other two studies used self-report only. Data for
zaleplon 20 mg were not considered here because this is not an
FDA-approved dose.
Sleep latency: One study evaluated the impact of zaleplon
10 mg versus placebo on PSG sleep latency (SL).
68
This study
showed a clinically signicant 9.5 min reduction in mean sleep
latency versus placebo (difference in median of 8.5 min) that
approached the 10 min value considered clinically signicant,
and was judged by the task force to be sufcient evidence
for making a recommendation. The CI (−0.19 to −18.80 min)
crossed the clinical signicance threshold, and therefore the
quality of evidence was downgraded for imprecision. It was
downgraded further due to the risk of publication bias since
the study was industry-funded. The resultant quality of evi-
dence is low.
Self-reported sleep latency was reported in one study,
68
which showed a reduction compared to placebo at the end of
treatment (−11.40 min; CI: −26.36 to +4.56 min), which failed
to meet the criterion for clinical signicance. Hedner
67
also
reported reductions in subjective sleep latency; however, the
results could not be subject to meta-analysis, since the mean
values were presented only in graphic form.
322
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
Additional studies not included in the primary analysis
yield similar ndings. Ancoli-Israel
69
conducted a randomized,
double-blind, multi-center study of the efcacy of zaleplon 5
and 10 mg versus placebo in older adults with DSM-IV insom-
nia, using a similar study design to Hedner,
67
with self-report
outcomes. This study reported signicant differences between
zaleplon 10 mg and placebo at both treatment weeks, and be-
tween zaleplon 5 mg and placebo at week 2 only. Elie 1999
70
reported signicant differences on placebo at weeks 1–3 of
treatment, with differences in the range of −8 to −15 min. Fry
71
reported a 28-day double-blind, placebo run-in and run-out
study of adults with DSM-III-R insomnia. Median subjective
sleep latency was signcantly different from placebo at weeks
1, 3, and 4 for zaleplon 10 mg, and at week 1 for zaleplon 5 mg.
Because mean and standard deviation data were not reported,
data from these two studies could not be formally evaluated in
our meta-analysis.
total Sleep time: The effects of zaleplon 10 mg on subjec-
tive TST were evaluated in one study.
68
Over the course of a
ve-week study, TST differed signicantly from placebo only
in week one, with a difference of 21.5 min between groups (CI:
−5.6 to +48.6 min); this difference failed to meet the criterion
for clinical signicance. Quality of the evidence was down-
graded to low due to imprecision and potential publication bias.
Objective TST was evaluated in 2 studies.
67,68
However,
meta-analysis of these studies was not possible due to the man-
ner of data reporting. These studies showed no consistent evi-
dence of a zaleplon − placebo difference at the 10 mg or 5 mg
dose of zaleplon. Mean/median differences in subjective TST
at the end of treatment were in the range of +7 to +22.4 min
in favor of zaleplon. The results of studies not included in our
formal analysis
69–71
showed very similar ndings for subjec-
tive TST, with inconsistent differences between placebo and
zaleplon 10 mg.
The effects of zaleplon 5 mg versus placebo on subjective
total sleep time were reported in one study.
67
No signicant
differences in median sleep time were found between zaleplon
5 mg and placebo across 2–4 weeks of treatment. The results of
studies not included in our formal analysis
69–71
showed similar
ndings for subjective TST, with no differences between pla-
cebo and zaleplon 5 mg.
Wake after Sleep onSet: Objective WASO was evaluated
in one study,
68
but failed to meet the criterion for clinical sig-
nicance (−2.10 min; CI: −10.23 to +6.03 min). The quality of
evidence was moderate, due to potential publication bias. Sub-
jective WASO was not reported in any of the studies.
Quality of Sleep: Subjective sleep quality, evaluated on
an ordinal 1–7 scale (1 = good, 7 = bad) was reported in one of
the formally evaluated studies for both 5 mg and 10 mg.
67
At
both dosages sleep quality improved (−0.10 points; CI: −0.27
to +0.07 points), but failed to meet the criterion for clinical
signicance. The quality of evidence for both doses was down-
graded to moderate due to potential publication bias.
In three additional studies,
69–71
subjective sleep quality dif-
fered from placebo inconsistently at either dose; the majority of
study weeks showed no difference between groups. Quality of
evidence was downgraded for publication bias. Precision and
heterogeneity could not be formally evaluated.
Sleep efficiency: Neither PSG nor subjective sleep ef-
ciency were formally evaluated in any of the studies reviewed
here.
number of aWakeningS: Number of awakenings were
evaluated in the sole PSG study.
68
However, formal evaluation
of ndings was not possible. No data were presented in the
paper, but NOA was reported not to differ between zaleplon 10
mg and placebo at any treatment week. Subjective NOA was
evaluated in the two studies formally included in our evalua-
tion but data were presented as median values and could not
be included in meta-analyses. Hedner
67
reported a difference
of uncertain clinical signicance only at week 1 and Walsh
68
reported a difference only at week 3. Data from three addi-
tional studies not included in our formal analysis
69–71
showed
no signicant differences in NOA for either zaleplon 10 mg or
zaleplon 5 mg at any study week.
overall Quality of evidence: As noted above, no meta-
analyses could be conducted on data from studies of zaleplon.
Some studies reported median data only, or mean values with
no standard deviation, for some of the key outcomes. Still other
studies presented data for key outcomes only in graphical form.
The quality of evidence was downgraded for imprecision, due
to the relatively large condence intervals which cross the clin-
ical signicance thresholds for multiple outcomes. All of these
studies were industry sponsored, resulting in further down-
grading of evidence due to potential publication bias. The qual-
ity of evidence for individual outcomes ranged from moderate
to low, therefore the overall quality of evidence was low.
HarmS: No meta-analysis was conducted on harms. Each
of the individual studies showed no signicant difference in
the overall rate of treatment-emergent adverse events between
zaleplon and placebo. Several symptoms related to the cen-
tral nervous system were more frequent numerically among
zaleplon treated patients, although these differences were not
statistically signicant due to the low overall incidence of ad-
verse events. The most common adverse events in studies of
zaleplon versus placebo included headache, asthenia, neuras-
thenia, pain, fatigue, and somnolence. There was no clear evi-
dence of dose-dependent effects.
Several of the reviewed studies reported data from double-
blind placebo runout periods. No signicant withdrawal symp-
toms were noted on the Benzodiazepine Withdrawal Symptom
Questionnaire.
70,71
The single PSG study noted no evidence
of withdrawal upon discontinuation for the 10 mg dose. Evi-
dence of discontinuation-related increases in subjective TST
were noted at the zaleplon 5 and 10 mg dose in older adults,
and for subjective SOL in older adults at the zaleplon 5 mg
dose.
67,69
A small increase in NOA of the second discontinu-
ation night was also noted with zaleplon 5 mg.
70
These dif-
ferences were small in absolute magnitude and of doubtful
clinical signicance. Other studies did not report evidence of

323
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
rebound insomnia.
71
Categorically-dened rebound insomnia
was not signicantly different for zaleplon 5 mg or zaleplon 10
mg versus placebo.
69,70
The task force found that there was weak objective evidence
of efcacy for zaleplon 10 mg in the treatment of sleep onset
insomnia that was just below criteria for clinical signicance,
and no consistent evidence for efcacy in TST. Likewise, there
was no statistical evidence of adverse events in excess of pla-
cebo, although some treatment-emergent adverse events were
numerically more prevalent in zaleplon groups. Evidence for
withdrawal effects was weak, inconsistent, and unlikely to be
clinically important. On balance, benets were deemed to mar-
ginally outweigh harms.
patientS’ valueS and preferenceS: The task force de-
termined that a majority of patients would likely use zaleplon
compared to no treatment. This assessment reects the task
force’s clinical judgment, based on zaleplon’s efcacy for sleep
onset, and its relatively benign side effect prole.
Zolpidem for the Treatment of Chronic Insomnia
Recommendation 4: We suggest that clinicians use zolpidem
as a treatment for sleep onset and sleep maintenance
insomnia (versus no treatment) in adults. [WEAK]
Remarks: This recommendation is based on trials of 10 mg
doses of zolpidem.
N.B. Although 10 mg. was the recommended starting dos-
age for adults at the time of initial approval, the FDA has
subsequently lowered the recommended starting dosage of im-
mediate-release zolpidem products to 5 mg. Further, the FDA
has recommended a reduction of starting dosage for extended-
release forms of zolpidem from 12.5 mg to 6.25 mg.
Summary
Twelve RCTs evaluated zolpidem 10 mg for the treatment of
chronic primary insomnia.
57,59,60,70,72–79
The overall quality
of evidence was downgraded to very low due to signicant
heterogeneity, imprecision, and risk of publication bias. The
evidence for zolpidem 10 mg was weakly in favor of its effec-
tiveness for improving sleep onset, sleep maintenance, sleep
quality, SE and TST. In addition, one paper evaluated the ef-
fectiveness of zolpidem extended release 6.25 mg
80
and one pa-
per assessed zolpidem extended release 12.5 mg.
81
Five studies examined the effects of zolidem 10 mg on ob-
jective sleep latency.
60,73,76,77,82
The mean reduction (vs. placebo)
for PSG-determined latency to sleep exceeded the threshold
for clinical signicance. Ten studies presented patient-reported
sleep latency data.
57,60,70,72–76,78,82
The mean reduction in subjec-
tive latency fell approximately at the signicance threshold.
Two st ud ies
73,76
reported adequate objective TST data for meta-
analysis and found that the mean improvement in TST also
exceeded the clinical signicance threshold. The same was
true for subjective TST, based on eight studies.
57,70,73–76,78,82
Two
studies
73,76
found that PSG-determined reduction in WASO was
clinically signicant. Six studies included adequate data for
meta-analysis of subjective WASO
57,72,75,76,78,82
; the mean reduc-
tion fell below the clinical signicance threshold. Six studies
evaluating sleep quality reported moderately large improve-
ment in this parameter based on SMD.
57,60,76,78,79,82
Improve-
ment in PSG SE in the four studies included also exceeded the
clinical signicance threshold.
73,76,77,82
Number of awakenings
(objective) fell below the clinical signicance threshold.
77,82
Re-
duction in subjective number of awakenings also failed to meet
the clinical signicance threshold.
The single paper reporting on extended-release zolpidem
6.25 mg
80
found moderate reduction in PSG-determined
WASO (based on only the rst 6 h of sleep) and minimal im-
provement in LPS and SE at end-treatment in an elderly popu-
lation. Overall quality of evidence from this report was LOW
due to imprecision and potential publication bias. Data from
the one study
81
on zolpidem extended-release 12.5 mg found
moderate reduction in PSG LPS. Reduction in WASO was also
moderate, while SE was not signicantly different from pla-
cebo. Overall quality of evidence was LOW due to imprecision
and potential publication bias.
Meta-analysis was conducted for amnesia, dizziness, head-
ache, nausea, somnolence and “taste perversion” (altered or
unpleasant taste) in studies employing zolpidem 10 mg. Small,
but potentially signicant increases in amnesia, dizziness and
somnolence were reported with zolpidem.
Overall, the benets of zolpidem 10 mg and extended-
release zolpidem 12.5 mg were judged to be greater than the
minimal potential harms. Benets and harms were judged to
be approximately equal for extended-release zolpidem 6.25 mg.
It was determined by clinical judgement of the task force that
the majority of well-informed patients would use zolpidem and
extended-release over no treatment. This judgement is based
on the evidence of improvement in sleep latency, total sleep
time, WASO, sleep efciency, and sleep quality, coupled with
relatively low potential for adverse events. The data for ef-
cacy of zolpidem extended-release 6.25 mg is minimal and
inconclusive at best.
See Figures S18–S27, S70–S75 and Tables S8 – S10 in the
supplemental material.
Discussion
Twelve studies were included in the meta-analysis for zolpidem
10 mg.
57,60,70,72–79,82
Dorsey and colleagues
72
studied 141 meno-
pausal or perimenopausal women who exhibited both insomnia
(TST < 6 h or WASO > 1 h) and nocturnal hot ashes or sweats.
Subjects received zolpidem 10 mg or placebo in a 4-week trial.
Outcomes included patient-reported TST, SL, WASO, and
NOA. Elie
70
investigated three dosages of zaleplon versus zol-
pidem 10 mg or placebo. The study included 615 adults with
SL > 30 min and either TST < 6.5 h or WASO > 30 min or > 3
awakenings per night. Subjects received one of three zaleplon
dosages, zolpidem 10 mg or placebo for 28 nights. Outcome
data included subjective SL, QOS, TST and NOA. Erman
57
assessed 65 adults with reported sleep-onset insomnia and
baseline PSG SL > 20 min and TST < 7 h or WASO > 20 min.
Enrollees were administered eszopiclone at 4 dosages, zolpi-
dem 10 mg and placebo in a randomized treatment sequence
of 2 nights per intervention with intervening washout. Primary
outcome was PSG-determined LPS with secondary measures
including SE, WASO and NOA. Hermann
73
administered
324
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
zolpidem 10 mg or placebo for two weeks to 21 adults with
difculty initiating or maintaining sleep. PSG was conducted
on the nal treatment night with reported outcomes including
SL, TST, SE and WASO.
Perlis
75
evaluated 199 subjects with primary insomnia
(SL > 45 min or TST < 6 h) with zolpidem 10 mg or placebo.
Subjects were instructed to take the medication 3–5 times per
week as needed over a twelve-week period. Sleep diary out-
comes included SL, TST, WASO and NOA. Jacobs
74
compared
zolpidem 10 mg, cognitive behavior therapy and placebo in 63
adults with primary sleep-onset insomnia (SL > 1 h on > 3
nights/week). Subjects received zolpidem for 28 days, followed
by taper. Primary outcome was patient-reported sleep latency
with secondary outcomes of SE and TST. Randall
76
investi-
gated the efcacy of zolpidem 10 mg (5 mg for subjects 65–70
years) over an eight-month period in 91 subjects (age 23–70
years) with screening PSG SE < 85%. Patient-reported out-
comes and PSG data at one and eight months included SL, TST,
WASO and SE. Scharf
82
evaluated 75 adults for ve weeks with
zolpidem 10 mg, 15 mg or placebo. Inclusion criteria included
SL > 30 min or TST < 6 h. Subjects underwent sleep studies on
the rst two nights of each treatment week. Primary outcomes
were dened as LPS and SE.
Staner
79
assessed the effects of three drugs, including zol-
pidem 10 mg, in a driving simulation study of 23 adults with
recurrent SL > 30 min or WASO > 60 min. Sleep quality data
was reported. Uchimura
60
compared zolpidem, eszopiclone
and placebo in a crossover design as described in the eszopi-
clone section. Walsh
78
compared the efcacy of zolpidem 10 mg
to trazodone 50 mg and placebo in 278 adults with insomnia
characterized by frequent SL > 30 min and TST 4–6 h. Sub-
jective sleep latency and TST were reported. Ware
77
assessed
rebound insomnia in zolpidem 10 mg, triazolam 0.5 mg and
placebo. Ninety-nine subjects with baseline PSG-determined
LPS > 20 min and TST 4–7 h took zolpidem 10 mg, triazolam
or placebo for 28 consecutive days. PSG LPS, SE, TST, and
WASO were evaluated.
Two studies reported on extended-release (ER) zolpidem.
Roth
81
assessed zolpidem ER 12.5 mg in 212 adults with in-
somnia who reported > 1 h WASO at least 3 nights per week.
Patients received zolpidem or placebo nightly for 3 weeks in a
parallel group design. Walsh
80
studied 205 elderly adults with
insomnia with the same inclusion criteria and design, employ-
ing a 6.25 mg dose of zolpidem ER versus placebo.
Fourteen additional studies met inclusion criteria but could
not be included in meta-analysis due to inadequate data
sets.
71,83–95
Pertinent results from these studies are noted inde-
pendently of meta-analysis results.
Sleep latency: Five studies included adequate data for PSG
SL meta-analysis.
60,73,76,77,82
The mean difference from placebo
of −11.65 min exceeded the clinical signicance threshold. The
95% CI of −4.15 to −19.15 min crossed the clinical signicance
threshold and was therefore considered imprecise. Heterogene-
ity was high. With potential publication bias as well, the qual-
ity of evidence was rated as very low.
Ten of the twelve studies used in meta-analysis reported
subjective SL.
57,60,70,72–76,78,82
The improvement in sleep latency
versus placebo was at the signicance threshold (mean differ-
ence: 19.55 min; CI: −14.2 to −24.9 min). Evidence quality was
very low due to imprecision, heterogeneity and potential pub-
lication bias.
Six additional studies assessed sleep latency outcomes with
zolpidem.
88–90,92,94,95
These studies varied signicantly with re-
gard to drug preparation, dosage, mode of administration and
methodology, rendering comparisons between them or to the
meta-analytic data difcult. Four of the six evaluated sublin-
gual zolpidem, primarily for treatment of middle-of-the-night
(MOTN) awakenings. Roth and colleagues
88
reported results
of a three-way crossover study of zolpidem sublingual 1.75 mg,
3.5 mg and placebo. Zolpidem reduced both objective (latency
to persistent sleep) and subjective latency to sleep (SL) follow-
ing MOTN awakenings (PSG: 1.75 mg: −11.2 min versus pla-
cebo; 3.5 mg: −18.4 min/subjective: 1.75 mg: −11.83 min versus
placebo; 3.5 mg: −15.23 min). Roth
89
also reported reduced sub-
jective latencies following MOTN awakenings with sublingual
zolpidem 3.5 mg over a 28-day trial. Zammit
95
administered
immediate release oral zolpidem 10 mg, zaleplon 10 mg or pla-
cebo to subjects with sleep maintenance insomnia following
induced MOTN awakenings Zolpidem reduced PSG latency to
persistent sleep following the awakenings (−30.5 min versus
placebo). Staner
90
compared the effects of sublingual zolpidem
10 mg to immediate release oral zolpidem on PSG initial sleep
latency and reported shorter latency to persistent sleep with
the sublingual preparation (−10.28 min) versus the oral prepa-
ration. Walsh
94
investigated subjective SL in an 8-week trial
of as-needed zolpidem 10 mg (3–5 times per week). For medi-
cation nights only, end treatment SL for the zolpidem 10 mg
group was 12.6 min less than the placebo group.
Walsh
80
investigated the effects zolpidem ER 6.25 mg and
found reduction of PSG LPS of 13.0 min. Roth
81
reported a
decrease in PSG LPS of 8.2 min versus placebo at end of treat-
ment with zolpidem ER 12.5 mg.
total Sleep time: Two st udies
73,76
were included in the
meta-analysis of PSG-determined TST. Mean reduction in
TST met the clinical signicance threshold at +28.91 min, how-
ever the 95% CI crossed the threshold (CI: +10.85 to +46.97
min). The quality of evidence was downgraded to LOW due
to imprecision and potential publication bias. Eight studies
reported adequate data for meta-analysis of patient-reported
TST.
57,70,73–76,78,82
The mean difference for subjective TST from
these studies exceeded the signicance threshold (+30.04 min;
CI: +15.12 to +44.96 min). Quality of evidence was low due to
imprecision and potential publication bias.
Six additional studies presented TST data which was not
sufcient to be included in the analysis.
71,83,84,88,92,95
Allain and
colleagues
83
evaluated zolpidem 10 mg administered on an as-
needed basis over a four week period. When only drug nights
were included in analysis, zolpidem produced a statistically
signicantly greater increase in subjective TST versus placebo
(+19.9 min). Cluydts
84
and Hajak
85
found no difference in sub-
jective TST with nightly versus intermittent (5/7 nights) use of
zolpidem 10 mg, both of which produced numerical improve-
ment (+11.3 and +16.9 min, respectively). In a study designed
primarily to address potential rebound insomnia following
325
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
four weeks of treatment with zaleplon, zolpidem or placebo,
Fry
71
reported substantially greater improvement in patient-
reported TST with zolpidem 10 mg versus placebo (+28.2 min).
In another study of rebound insomnia, Voshaar
92
compared
zolpidem 10 mg to temazepam 20 mg (without placebo con-
trol) administered nightly for four weeks. The two drugs pro-
duced improved TST without signicant difference between
the two. Finally, in two studies Roth
89
and Zammit
95
investi-
gated effects of zolpidem following MOTN awakenings. Roth
and colleagues compared sublingual zolpidem 1.75 mg and 3.5
mg to placebo. Both dosages produced greater TST following
awakening as compared to placebo (+14.7 min and +25.9 min,
respectively). Zammit administered zolpidem 10 mg following
MOTN awakening and reported TST after awakening 30 min
greater than placebo.
TST data were not reported in the extended-release studies.
Wake after Sleep onSet: Two studies reported adequate
data for meta-analysis of PSG WASO.
73,76
These studies yielded
a mean difference from placebo of −25.46 min (CI: −17.94 to
−32.99 min). This exceeds the threshold for clinical signi-
cance. The quality of evidence was LOW due to imprecision
and potential publication bias.
Zolpidem ER 12.5 mg reduced WASO by 20 min greater
than placebo at treatment conclusion, although this was based
on only the rst 6 h of sleep.
81
Comparison of changes from
baseline in this study, however, suggested smaller differences
between drug and placebo. Walsh,
80
using the same selective
sample of 6 h, found WASO 13.0 min less in the zolpidem ER
6.25 mg group than in the placebo group. Given the sampling
of only 6 h, it is difcult to clearly determine whether or not
these agents would fulll the criterion for clinical signicance,
which is based on an entire night of sleep.
Six studies assessed patient-reported WASO.
57,72,75,76,78,82
The
mean difference fell below the level of clinical signicance at
−13.57 min (CI: −7.30 to −19.84 min). Quality of evidence was
low due to heterogeneity and potential publication bias.
Quality of Sleep: Six studies included sleep quality
data.
57,60,76,78,79,82
The meta-analysis produced a standardized
mean difference of +0.64 (CI: +0.03 to +1.26 SMD), suggest-
ing moderate overall improvement in patient-reported sleep
quality. Quality of evidence was very low due to imprecision,
heterogeneity and potential publication bias.
Sleep efficiency: PSG sleep efciency was reported in
four studies.
73,76,77,82
The mean difference favored zolpidem
(+6.12%; CI: +4.39 to +7.85%), but did not exceed the clinical
signicance threshold. Quality of evidence was low.
In the Roth
81
study of zolpidem ER 12.5 mg, PSG SE was
3.9% better with zolpidem than placebo. Walsh
80
found a dif-
ference of 2.4% on favor of zolpidem ER 6.25 mg. Neither
value exceeds the clinical signicance threshold.
number of aWakeningS: PSG-determined number of
awakenings was reported by Scharf
82
and Ware.
77
The mean
difference from placebo was −0.95 awakenings (CI: −0.49 to
−1.41 awakenings), which fails to meet the clinical signicance
threshold. Quality of evidence was moderate. Subjective awak-
ening was reported in six studies.
70,72,73,75,78,82
Mean reduction
versus placebo was −0.31 awakenings (CI: −0.17 to −0.45
awakenings), which also fails to achieve clinical signicance.
Evidence quality was low due heterogeneity and potential pub-
lication bias.
overall Quality of evidence: The overall quality of
evidence in the meta-analytic data from these studies was
downgraded to very low for several reasons. Substantial het-
erogeneity across studies was noted for multiple outcomes.
The data were also downgraded for imprecision, due to the
relatively large condence intervals which cross the clinical
signicance thresholds for several outcomes. All of these stud-
ies were industry sponsored, resulting in further downgrading
of evidence due to potential publication bias. The quality of ev-
idence for individual outcomes ranged from moderate to very
low, therefore the overall quality of evidence was very low.
HarmS: Meta-analysis for adverse effects of zolpidem was
possible for six side effects: amnesia, dizziness, sedation,
headache, nausea, and taste perversion (altered or unpleasant
taste). Two studies
70,82
included data on amnesia and found a
minimal difference from placebo (0.03 risk difference). A
small increase in risk (0.06 risk difference) was identied for
dizziness, based on analysis of four investigations.
57,60,72,82
Risk
for headache was mildly increased in the zolpidem group (0.07
risk difference).
57,72,78
Minimal difference was observed in the
risk for nausea (0.02 risk difference),
57,82
and somnolence had a
slightly higher risk (0.04), based on six studies.
57,60,70,72,78,82
Risk
for taste perversion was low and approximately equal in both
groups.
60,70
Numerous studies have evaluated rebound insomnia after
discontinuation of zolpidem.
68,70,71,73,75,77,80,82,86,92
Some of these
studies found no evidence of rebound after varying durations
of nightly or intermittent use, for up to six months.
68,73
Other
investigations reported evidence of rebound, limited primarily
to night 1 following discontinuation.
70,71,80,81
Evaluation of daytime improvement and impairment was
limited. Dorsey
72
reported improvement in sleep-related dif-
culty with daytime function. Hajak
85
described marked
improvement in quality of life ratings with both nightly and
intermittent use. Morning alertness and performance impair-
ment were tested in several studies. Roth
81
and Walsh
80
found
no evidence of impairment on digit symbol substitution test
(DSST) or Rey auditory-verbal learning test (RAVLT) after
zolpidem modied-release 12.5 mg. Scharf
82
reported no im-
pairment on DSST or digit symbol copying. Staner
79
found
no indication of impairment in a driving simulation study
after seven consecutive nights of zolpidem 10 mg. Zammit
95
formally assessed sleepiness following administration of zol-
pidem 10 mg following MOTN awakening. Subjects showed
signicantly reduced PSG latencies versus placebo at 4, 5, and
7 h following administration. This was accompanied by im-
pairment on DSST at 4 and 5 h.
In summary, the task force found that there was weak evi-
dence of efcacy in the treatment of sleep onset and mainte-
nance insomnia, with limited evidence of mild adverse events

326
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
in excess of placebo, with the possible exception of excessive
sleepiness following administration of higher dosages (10 mg)
less than 8 h prior to awakening. Therefore, benets were
deemed to marginally outweigh harms.
patientS’ valueS and preferenceS: The task force de-
termined that a majority of patients would likely use zolpidem
compared to no treatment. This assessment reects the task
force’s clinical judgment, based on zolpidem’s efcacy for
sleep onset and maintenance, and its relatively benign side ef-
fect prole.
Benzodiazepines
Triazolam for the Treatment of Chronic Insomnia
Recommendation 5: We suggest that clinicians use
triazolam as a treatment for sleep onset insomnia (versus
no treatment) in adults. [WEAK]
Remarks: This recommendation is based on trials of 0.25
mg doses of triazolam.
Summary
Because only one study
96
contained data of sufcient quality,
meta-analysis was not performed. The quality of evidence for
this study was high. This study, consisting of patient-reported
data, showed a modest decrease in subjective SL, which fell
below the clinical signicance threshold. Two additional stud-
ies, which did not contain data suitable for meta-analysis, re-
ported statistically signicant reductions in subjective SL with
triazolam 0.25 mg versus placebo.
97,98
Roehrs
96
found an in-
crease in TST, although the mean change fell below the range
of clinical signicance. WASO was not reported, while sleep
quality showed mild to moderate reduction versus placebo.
Number of awakenings was insignicantly decreased.
No meta-analysis of harms was possible. Given the mar-
ginal evidence for efcacy in improving sleep onset, coupled
with limited evidence regarding harms, the task force judged
the harms to be approximately equal to the benets. Based on
its clinical judgement, the task force determined that, in light
of the evidence for efcacy for sleep onset and the absence of
information regarding harms, the majority of patients would
be likely to use triazolam compared to no treatment.
See Table S11 in the supplemental material.
Discussion
Roehrs
96
studied 32 adults with insomnia in a complex design
which began with 11 days in which subjects received either tri-
azolam or placebo nightly, “as needed” or every third night. This
was followed by 14 nights in which subjects chose to self-admin-
ister treatment, with placebo (week 1) or triazolam 0.25 (week 2).
Thirteen additional studies met general inclusion and exclu-
sion criteria.
97–109
These studies were highly varied in design,
many utilizing interval scales (as opposed to specic numeric
values) for reporting of sleep outcome variables. Some did not
include a placebo comparison. Many included dosages which
are higher than current recommended dosages. Therefore, only
those studies which contained pertinent data are discussed.
Bowen
100
compared triazolam 0.5 mg, urazepam 30 mg and
placebo in 120 insomnia outpatients. The two-night crossover
comparison of triazolam 0.5 mg and placebo included only 18
subjects, who completed morning sleep questionnaires. Elie
97
evaluated triazolam 0.125 mg (with upward dosage adjustment
to 0.25 mg during the study period, as indicated) versus zopi-
clone and placebo in 48 elderly (60–90 years) subjects. Subjects
received one of three interventions nightly for three weeks in
a parallel group design. Outcome variables were patient-
reported. Greenblatt
103
reported an RCT of 6 nights baseline
placebo administration followed by triazolam 0.5 mg for 7–10
nights in a total of 60 subjects with sleep onset or maintenance
insomnia. Outcome data were derived from subjective reports.
Hajak
104
treated 1,507 subjects with sleep onset or maintenance
insomnia with triazolam 0.25 mg, zopiclone or placebo. The
triazolam versus placebo comparison groups totaled 605 sub-
jects, who received drug or placebo for 28 consecutive nights
and reported sleep variables on visual analog scales.
Monti
106
assessed 24 chronic insomnia subjects with tri-
azolam 0.5 mg, zolpidem and placebo in a 27-night trial, with
PSG on nights 4/5 and 15/16 and 29/30. Reeves
98
evaluated 37
geriatric subjects (> 60 years) with triazolam 0.25 mg, uraz-
epam or placebo in a 28 day trial. The triazolam and placebo
groups included 28 subjects who completed daily sleep diaries.
Rickels
107
studied 50 subjects with sleep onset or maintenance
insomnia who received either triazolam 0.5 mg or placebo for 7
days. Outcome data were subjective ratings and interval scales.
Scharf
108
administered triazolam 0.5 mg, quazepam or placebo
to 65 chronic insomnia subjects. After placebo run-in, partici-
pants received nightly drug or placebo for 9 nights, followed by
14 nights of every-other-night administration. Outcomes were
patient reported rating scales.
Sleep latency: In the only study with adequate data for
meta-analysis, Roehrs
96
found a small reduction in subjective
SL (−9.2 min; CI: −22.3 to +3.9 min) which fell below clinical
signicance. Quality of evidence for these data was high.
Monti
106
found no signicant differences between triazolam
0.5 mg and placebo for PSG SL at any time point.
Elie
97
found larger reductions in subjective ratings of SL
for triazolam 0.125–0.25 mg versus placebo. Hajak
104
found
no signicant difference from placebo in SL “response rate”
(SL reduction of > 15 min) for triazolam 0.25 mg. In contrast,
Reeves
98
found triazolam 0.25 mg statistically superior to pla-
cebo for SL in a geriatric population on subjective ratings of
“how much [the drug] helped.” Bowen
100
found triazolam 0.5
mg to be statistically signicantly better than placebo on in-
terval ratings for reduction of sleep onset time. Greenblatt
103
reported sleep diary reductions from baseline placebo levels
of 55 min and 24 min in two separate triazolam 0.5 mg groups.
Rickels
107
reported similar subjective improvement on ratings
of sleep induction for triazolam 0.5 mg.
total Sleep time: Roehrs
96
observed a moderate increase
in subjective TST (+25.20 min; CI: −9.12 to +59.52 min). This
fell below the clinical signicance threshold of 30 min and was
not statistically different from placebo. Quality of evidence
was moderate due to imprecision.

327
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
In additional studies, Hajak
104
found no signicant differ-
ence between triazolam 0.25 mg and placebo in “percentage
of responders” for TST (dened as > 20% increase in TST).
Ratings for improvement in TST were signicantly better
for triazolam 0.25 mg than placebo in the Reeves
98
geriatric
study.
Monti
106
observed a statistically signicant increase in ob-
jective TST with triazolam 0.5 mg (+16 min versus placebo).
Bowen
100
found that triazolam 0.5 mg was signicantly pre-
ferred to placebo for sleep duration. In two separate triazolam
0.5 mg groups, Greenblatt
103
noted increases in subjective TST
of 1.02 and 0.76 h. Rickels
107
reported that triazolam 0.5 mg
was rated as signicantly superior to placebo for sleep dura-
tion. Scharf
108
noted signicantly greater subjective improve-
ment in interval ratings of TST with both daily and every other
night administration of triazolam 0.5 mg.
Wake after Sleep onSet: No studies reported data on
WASO.
Quality of Sleep: Roehrs,
96
using a 4-point scale (1 = good,
4 = poor), found small improvements in QOS ( −0.37 points; CI:
−0.66 to −0.07 points), which was not considered to be clini-
cally signicant. Quality of evidence was high.
Elie
97
found no signicant difference between triazolam
(0.125/0.25 mg) and placebo in an elderly population with
respect to QOS. Likewise, Hajak
104
reported no statistically
signicant difference between triazolam 0.25 and placebo.
Reeves
98
demonstrated signicant improvement in QOS for
triazolam 0.25 mg versus placebo in a geriatric population.
Sleep efficiency: Sleep efciency was not reported by any
study.
number of aWakeningS: Roehrs
96
reported a reduction in
NOA of 0.37 (CI: −1.7 to +0.96 awakenings), which did not
meet the clinical signicance threshold. Quality of evidence
was LOW due to signicant imprecision.
Hajak
104
noted no signicant difference from placebo in
the percentage of “responders” (reduction of NOA to < 3)
with triazolam 0.25 mg. However, Reeves
98
did nd a statisti-
cally signicant reduction at this dosage in ratings for NOAs.
Bowen
100
observed a statistically signicant reduction in sub-
jective ratings for NOA with triazolam 0.5 mg versus placebo.
Greenblatt
103
also reported reductions of 0.58 and 0.89 patient-
reported awakenings from placebo baseline in two groups ad-
ministered 0.5 mg triazolam.
overall Quality of evidence: The overall quality of
evidence for the triazolam data, based on the single study
meeting criteria for meta-analysis, was HIGH.
HarmS: Insufcient data were available for meta-analysis of
adverse events associated with triazolam 0.25 mg. Very little
systematic analysis of adverse effects is available. Hajak
104
reported that “speech disorder” was the only adverse effect,
among many, to be signicantly more frequent in the triazolam
group than in the placebo condition.
patientS’ valueS and preferenceS: The task force
determined that a majority of patients would be likely to use
triazolam compared to no treatment. This assessment reects
the task force’s clinical judgment, based on weak evidence for
triazolam’s efcacy and the absence of information regarding
harms.
Temazepam for the Treatment of Chronic Insomnia
Recommendation 6: We suggest that clinicians use
temazepam as a treatment for sleep onset and sleep
maintenance insomnia (versus no treatment) in adults.
[WEAK]
Remarks: This recommendation is based on trials of 15 mg
doses of temazepam.
Summary
Three RCTs investigated the use of temazepam in the treat-
ment of chronic primary insomnia.
110 –112
These studies pro-
vide a limited assessment of temazepam in that they included
small sample sizes of 19, 20, and 34 subjects, respectively.
The overall quality of evidence from these studies is moder-
ate. Meta-analyses for temazepam 15 mg were conducted for
SL, TST and sleep quality. Two studies
110,112
were included in
the meta-analysis of SL. These showed a reduction in subjec-
tive SL which exceeded the threshold for clinical signicance.
Meta-analysis of TST showed improvement in subjective TST
which exceed the threshold for clinical signicance. There
were insufcient data for meta-analysis of WASO. One study
of objective WASO revealed a clinically signicant reduction.
Subjective and objective SE was signicantly increased, based
on limited data from secondary studies. There was evidence
for marginal improvement in sleep quality of 0.25 standard de-
viations. This was not a clinically signicant difference from
placebo and falls below the threshold for clinical signicance.
There were minimal data on adverse effects, and the available
data do not suggest a high frequency of treatment-emergent
adverse events (TEAEs).
Meta-analysis for temazepam 30 mg was not possible for
any sleep outcomes. Data from individual studies are reported
below.
In summary, meta-analysis data are available for temaze-
pam 15 mg only. These data, coupled with data from secondary
studies not adequate for meta-analysis, demonstrate efcacy
for temazepam 15 mg in improving subjective and possibly ob-
jective sleep latency, subjective and objective TST, and objec-
tive WASO (the latter based on a single study). Temazepam 30
mg appears to have signicant efcacy for improving subjec-
tive sleep latency and TST. The data also support a clinically
signicant effect for both 15 mg and 30 mg on subjective NOA,
although data for objective NOA at 20 mg revealed no signi-
cant effect.
Given the signicant improvements in patient-reported SL
and TST, coupled with additional data derived from secondary
studies (see below), the task force judged that the benets of te-
mazepam 15 mg appear to be greater than the potential harms.
Based on its clinical judgement, the task force determined that,
in light of the evidence for efcacy and minimal evidence for

328
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
harms, the majority of well-informed patients would be likely
to use temazepam compared to no treatment.
See Figures S28–S30 and Tables S12 and S13 in the sup-
plemental material.
Discussion
Evidence from three RCTs which investigated the use of te-
mazepam in the treatment of insomnia was included in the sta-
tistical analysis.
110 –112
Glass
110
evaluated 19 subjects 70 years of age or older who
met DSM-IV diagnostic criteria for primary insomnia. Sub-
jects underwent a crossover study of two weeks of treatment
with placebo, temazepam 15 mg, or diphenhydramine 50 mg
with randomized order of administration. Sleep was assessed
using diary-derived variables. Adverse effects were recorded
and daytime impairment was systematically assessed using
the digit symbol substitution task (DSST), the manual tracking
task (MTT), and the morning-after memory impairment, using
a free-recall procedure.
Wu
112
assessed 71 patients with DSM-IV diagnosed insom-
nia who were randomized to one of four groups (CBT-I alone,
CBT-I plus pharmacotherapy with temazepam 15 mg, pharma-
cotherapy alone, or placebo). For the purpose of this analysis,
pharmacotherapy alone was compared to placebo (n = 34).
Subjects received 8 weeks of treatment. End-of-treatment PSG
and patient diary data for SL, TST and SE were compared.
Hindmarch
111
studied 20 individuals with “a history of
nighttime medication for insomnia.” No additional diagnostic
information was provided. Subjects were randomized to re-
ceive temazepam 15 and 30 mg or placebo for a single night
using a within-subjects crossover design. Outcome was as-
sessed using the Leeds Sleep Evaluation Questionnaire which
consisted of Visual Analogue Scale (VAS) ratings of “Ease of
Falling Asleep” and “Quality of Sleep.” Adverse effects were
not reported, but daytime sedation was assessed with a Choice
Reaction Time task, the Critical Flicker Fusion Test, and “Ease
of Awakening” and “Integrity of Behavior Following Wakeful-
ness” items from the Leeds scale.
Six additional studies which included temazepam-placebo
comparisons were reviewed.
92,113–117
Cuanang
113
studied 60
adult “outpatients with insomnia.” Parallel group design in-
cluded three groups: temazepam 20 mg, temazepam 10 mg
and placebo. Subjects received treatment or placebo for ve
nights. Patient-reported data including sleep quality (“better,
same or worse”), SL, and TST were collected each morning.
Fillingim
114
evaluated 75 adult patients with difculty initiat-
ing (SL > 30 min) and maintaining (> 1 awakening with dif-
culty returning to sleep) sleep and TST < 6 h. Subjects received
temazepam 30 mg, glutethimide or placebo in parallel group
design for four nights. Outcomes included patient-reported
estimates of SL, TST, NOA and QOS. Heffron
115
reported on
55 “insomnia outpatients” who received temazepam 30 mg or
placebo in parallel groups for four nights. Subjects reported
SL, TST, NOA and QOS. Tuk
116
studied 21 “primary sleep-
onset insomnia” patients in a within-patient crossover study.
Subjects received a single night of placebo and a single night
of temazepam 20 mg with one-week intervening washout. PSG
was conducted on each of the two nights. SL, TST, WASO and
SE were reported. Voshaar
92
assessed 85 individuals with
DSM-III-R primary insomnia in a within-subjects crossover
design including temazepam 20 mg, zolpidem and placebo. A
single-blind placebo period of four days was followed by 28
days of active treatment with zolpidem or temazepam. Data
are presented as means for the placebo period and active treat-
ment period for each sleep outcome. Wilson
117
conducted an
actigraphic evaluation of 38 subjects with “complaints of poor
sleep.” Subjects were randomized to one of two crossover de-
signs, each of which included two weeks of placebo and two
weeks of temazepam 20 mg. Subjective results from patient
diaries as well as actigraphic results were averaged over the
respective periods.
Sleep latency: The meta-analysis for subjective SL, based
on two studies
110,112
of temazepam 15 mg revealed a mean re-
duction of 20.06 min (CI: −1.07 to −39.05 min). Quality of evi-
dence was moderate due to imprecision.
One additional study assessed subjective SL at the 15 mg
dosage. Hindmarch
111
found no effect on the VAS scale rating
for “ease of getting to sleep.”
Three studies
114,115
evaluated the effects of temazepam 30 mg
on subjective sleep latency from patient diaries. Fillingham
114
reported a reduction of SL of 40 min versus placebo. Hef-
fron
115
found a 45 min reduction versus placebo. Hindmarch
111
reported a statistically signicant effect on a VAS for “ease of
getting to sleep” with temazepam 30 mg.
Tuk
116
found no difference between temazepam 20 mg and
placebo in PSG SL. However, it is noteworthy that in this
sample of “primary sleep onset insomnia” patients, both te-
mazepam and placebo produced a reduction from baseline
of approximately 53 min (to SL of about 24 min). Wilson
117
demonstrated a SL derived from actigraphy which was only
7 min less than that of placebo. However, of note, the end-of-
treatment SL for temazepam (by actigraphy) was only 15 min,
suggesting a possible oor effect for these results.
Three studies assessed subjective SL with temazepam 20
mg.
92,113,117
Cuanang
113
reported a reduction from baseline
which was 34.2 min greater than placebo reduction. Voshaar
92
found end-of-treatment SL for temazepam 20 mg which was 29
min less than placebo. Similarly, Wilson
117
found subjective SL
was 23 min less than placebo.
total Sleep time: Two studies
110,112
were included in the
meta-analysis for subjective TST at 15 mg. The analysis re-
vealed a mean increase in TST of 64.4 min (CI: +8.1 to +120.8
min). Quality of evidence was moderate due to imprecision.
No additional studies evaluated subjective TST at this dosage.
Wu
112
reported a PSG TST of 99.1 min greater than placebo for
15 mg.
Two st ud ies
114,115
reported subjective TST at the 30 mg dos-
age. Fillingim
114
demonstrated TST which was 53 min greater
than placebo, while Heffron
115
noted a 54.6 min greater TST
versus placebo. There were no investigations of objective TST
for this dosage.
At the 20 mg dosage, three trials
92,113,117
reported subjective
TST. Cuanang
113
found a 78 min greater TST increase from
baseline than placebo. Voshaar
92
demonstrated a 46 min greater
329
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
TST than placebo at end-of-treatment. Wilson
117
also found an
18 min greater TST with temazepam 20 mg than with placebo.
One study
117
assessed objective TST at 20 mg. Actigraphy re-
vealed a 12 min greater TST at this dosage versus placebo.
Wake after Sleep onSet: Meta-analysis for WASO was
not possible. One investigation
116
evaluated PSG WASO at the
20 mg dosage and reported WASO time which was 28.1 min
less than placebo. Of note, the subjects in this study were de-
scribed as exhibiting “sleep onset insomnia.” At the same dos-
age, subjective WASO was 15 min less than placebo.
92
This
was below the threshold for clinical signicance.
Quality of Sleep: Meta-analysis was conducted for sleep
quality ratings from two studies
110,111
for temazepam 15 mg.
The SMD was 0.25, below the range for clinical signicance.
However, it should be noted that the Hindmarch
111
study was
underpowered to detect all but extremely large effects in that it
only included 20 subjects. The quality of evidence was moder-
ate due to imprecision.
Two studies found statistically signicant improvement in
sleep quality ratings for temazepam 30 mg.
114,115
Cuanang
113
reported statistically signicant improvement for temazepam
20 mg on a quality rating comparing “better quality” to “same
or worse quality.”
Sleep efficiency: Meta-analysis was not achievable for SE
at any dosage.
At 15 mg, Wu
112
found a PSG SE which was 13.3% greater
than placebo (CI: +3.9 to +22.6%). Subjective SE was +14.1%
versus placebo (CI: +5.8 to +22.3%). The quality of evidence
for both was moderate due to imprecision. At 20 mg, Tuk
116
reported a +5.9% PSG SE versus placebo.
number of aWakeningS: No meta-analysis of NOA was
possible. One study
110
reported data for subjective NOA at the
15 mg dosage (−0.5 awakenings; CI: −1.29 to +0.29 awaken-
ings). Quality of evidence was moderate due to imprecision.
Two st ud ies
114,115
reported subjective NOA at 30 mg. They
found −1.0 and −1.24 awakenings, respectively, compared to
placebo.
Tuk
116
found no signicant reduction in PSG NOA at 20 mg.
One study
117
reported data for subjective NOA at 20 mg (−0.2
awakenings compared to placebo).
overall Quality of evidence: The overall quality of
evidence in the meta-analytic data from the two available stud-
ies was moderate for temazepam 15 mg due to imprecision.
HarmS: Limited data on adverse effects of temazepam 15
and 30 mg are available. Meta-analysis could not be performed.
Glass
110
found no notable increase in adverse effects with te-
mazepam 15 mg versus placebo and no signicant effects
were found on measures of daytime impairment. Cuanang
113
reported “no marked difference in adverse events,” although
temazepam 20 mg was associated with a modest increase in
headache, blurred vision, depression and confusion. However,
the frequency of these events was low overall. Heffron
115
found
no difference in overall frequency of adverse events but noted
that drowsiness, lethargy and vertigo were more commonly
reported with temazepam 30 mg. There is some evidence that
temazepam 30 mg is associated with daytime impairment
on tests such as the Choice Reaction Time Test and Critical
Flicker Fusion Test.
111
In summary, the task force found that there was weak evi-
dence of efcacy of temazepam in terms of therapeutic effects
on sleep onset, total sleep time, awakenings, sleep efciency,
and possibly WASO with limited or no consistent evidence of
adverse events in excess of placebo. However, there was also
limited evidence for daytime impairment with temazepam
30 mg. Over, benets were deemed to outweigh harms for te-
mazepam 15 mg.
patientS’ valueS and preferenceS: Based on its clini-
cal judgement, the task force determined that a majority of pa-
tients would be likely to use both temazepam 15 mg and 30 mg
compared to no treatment.
Melatonin agonists
Ramelteon for the Treatment of Chronic Insomnia
Recommendation 7: We suggest that clinicians use
ramelteon as a treatment for sleep onset insomnia (versus
no treatment) in adults. [WEAK]
Remarks: This recommendation is based on trials of 8 mg
doses of ramelteon.
Summary
Four RCTs investigated the use of ramelteon in the treatment
of chronic primary insomnia.
118–121
The overall quality of evi-
dence from these studies was downgraded to very low due to
substantial heterogeneity across studies, imprecision and po-
tential publication bias. The overall evidence for ramelteon 8
mg. was weakly in favor of its effectiveness for the treatment of
sleep onset disturbance only. Meta-analysis of the three stud-
ies meeting inclusion criteria that reported objective (PSG)
sleep latency demonstrated marginal reduction of sleep latency.
The analysis revealed minimal increase in PSG-determined to-
tal sleep time which fell well below the dened threshold for
clinical signicance. Measures of sleep efciency and sleep
quality showed no clinically signicant improvement. There
was no evidence of signicant difference from placebo for any
adverse events, based on available side effect data. Although
the evidence for efcacy is marginal, the benets appear to be
greater than the minimal potential harms. Based on clinical
judgment, the task force determined that the majority of well-
informed patients would use ramelteon over no treatment. This
judgement is based on the evidence of improved sleep latency,
coupled with its apparently low potential for adverse events.
See Figures S31–S38, S76 and S77 and Table S14 in the
supplemental material.
Discussion
Evidence from four RCTs which investigated the use of ramelt-
eon in the treatment of chronic primary insomnia was included
330
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
in the statistical analysis.
118–121
Subjects in all studies demon-
strated chronic primary insomnia with associated daytime
complaints. All studies required mean objective LPS of > 20
min on two nights of PSG screening. All studies except Mayer
and colleagues
119
also required mean objective WASO > 60
min. Kohsaka and colleagues
118
studied 65 chronic insomnia
patients for two nights each at ramelteon doses of 4, 8, 16, and
32 mg. Roth and colleagues
120
studied 100 older adults (age > 65
years) with chronic primary insomnia. Subjects were adminis-
tered two consecutive nights each of placebo, ramelteon 4 mg,
and ramelteon 8 mg in a three-phase crossover protocol, with
randomization of the treatment sequence and sustained wash-
out time between each two night sequence.
Zammitt
121
studied the effects of nightly ramelteon in adults
at dosages of 8 and 16 mg. PSG was conducted at baseline, and
weeks 1, 3, and 5. The Mayer paper
119
reported on six-month
nightly use of ramelteon in 451 adults with chronic insomnia
from 46 multinational sites. Two nights of PSG were conducted
in week 1 and at approximately one month intervals thereafter.
Sleep latency: The impact of 8 mg ramelteon on PSG-as-
sessed SL was evaluated in three studies.
118,120,121
Objective sleep
latency data in the study by Mayer and colleagues
119
were not
adequate for meta-analysis and therefore could not be included.
Meta-analysis of the grouped evidence demonstrated mar-
ginal improvement in this critical outcome. However, the mean
difference between the treatment and control groups was not
clinically signicant (−9.57 min; CI: −6.38 to −12.75 min). The
condence interval crossed the clinical signicance threshold,
and therefore the quality of evidence was downgraded for im-
precision. It was downgraded further for the high degree of
heterogeneity across studies (I
2
= 96%), and due to the risk of
publication bias since all these studies were funded by indus-
try. The resultant quality of evidence is very low.
Mean differences in objective sleep latency varied from −7.6
min to −13.1 min. Of note, the Roth investigation included ex-
clusively older adults and found the smallest improvement in
sleep latency. Subjective sleep latency from these investiga-
tions was comparable to objective latencies with mean differ-
ence (−11.44 min; CI: −3.31 to −19.56 min) falling below the
clinical signicance threshold.
Several additional papers which met inclusion criteria, but
did not contain data suitable for this analysis, have addressed
the efcacy and side effect prole of ramelteon.
122–126
The ob-
jective and subjective sleep latency from these results were
consistent with the meta-analysis ndings. This was likewise
the case for sub-group analysis of subjects with primary sleep
onset complaints.
124
A post-hoc analysis of the data from Zam-
mitt by Mini and colleagues
123
found a signicantly greater
percentage of ramelteon 8 mg patients with > 50% reduction in
sleep latency at week 1 (63.0% versus 39.7% for placebo), week
3 (63.0% versus 41.2%), and week 5 (65.9% versus 48.9%).
total Sleep time: All four studies included in the meta-
analysis evaluated objective total sleep time for ramelteon 8
mg.
118–121
Although small improvements in TST were observed
in some individual studies, ranging from 1.2 to 12.5 min lon-
ger, the meta-analysis reveals minimal increase (+6.58 min; CI:
+1.36 to +11.80 min) which falls well below the threshold for
clinical signicance. The quality of evidence was downgraded
to LOW due to the high degree of heterogeneity across stud-
ies, and due to the risk of publication bias since all these stud-
ies were funded by industry. Meta-analysis results of reported
subjective TST were consistent with the objective nding (+5.7
min; CI: −7.65 to +19.04 min). Additional studies not included
in meta-analysis supported these results.
122,125,126
Wake after Sleep onSet: Meta-analysis of objective WASO
from the two studies reporting adequate data
118,121
show a clini-
cally insignicant increase (+3.5 min; CI: +2.77 to +4.23 min)
in WASO for the ramelteon group, well below the signicance
threshold of 20 min. The quality of evidence was downgraded
to moderate due to potential publication bias. One study not in-
cluded in meta-analysis
122
found no difference in PSG WASO.
Zammitt and Mayer reported subjective WASO data for
meta-analysis.
119,121
The ramelteon group demonstrated a clini-
cally insignicant increase in WASO of 5.2 min (CI: −6.77 to
+17.24 min). The quality of evidence was low due to heteroge-
neity and potential publication bias. The only additional study
which assessed subjective WASO found no difference between
placebo and ramelteon 8 mg.
126
Quality of Sleep: Sleep quality ratings showed virtually
no difference from placebo in any of the studies assessed.
119 –121
Meta-analysis suggests no difference between ramelteon and pla-
cebo, with a pooled mean difference of −0.04 points (CI: −0.13 to
+0.05 points) on a 7-point Likert scale. The quality of evidence
was downgraded to low due to heterogeneity and the risk of pub-
lication bias since all these studies were funded by industry. Ad-
ditional studies which assessed subjective sleep quality found no
difference between ramelteon and placebo groups.
122,125,126
Sleep efficiency: Three studies reported sleep efciency
data included in meta-analysis.
118,120,121
Minimal improvements
in sleep efciency were reported (+1.93%; CI: +1.00 to +2.87%),
falling well below the clinically signicance threshold for ob-
jective sleep efciency of 5%. The quality of evidence was low
due to heterogeneity and potential publication bias. Additional
studies did not report sleep efciency data.
number of aWakeningS: No meta-analysis for PSG num-
ber of awakenings was conducted as only one study reported
adequate data for analysis.
119
This investigation found no clini-
cally signicant difference between ramelteon 8 mg and pla-
cebo (+0.1 awakenings; CI: +0.08 to +0.15 awakenings). The
quality of evidence was moderate due to potential publication
bias. Other studies which evaluated NOA reported no signi-
cant differences as well.
120,125,126
In summary, these studies show very weak evidence for re-
duction of sleep latency at the recommended prescribed dosage
(8 mg), with mean decrease of 9.57 min (CI: −6.38 to −12.75
min), and no consistent evidence of improvement in other ob-
jective or subjective parameters.
overall Quality of evidence: The overall quality of
evidence in the meta-analytic data from these studies was
331
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
downgraded to very low for several reasons. Substantial het-
erogeneity across studies was noted for multiple outcomes.
The data were also downgraded for imprecision, due to the rel-
atively large condence intervals, which cross the clinical sig-
nicance thresholds for multiple outcomes. All of these studies
were industry sponsored, resulting in further downgrading of
evidence due to potential publication bias. The quality of evi-
dence for individual outcomes ranged from moderate to very
low; therefore, the overall quality of evidence was very low.
HarmS: Meta-analytic data on adverse effects showed a rela-
tively low frequency of adverse effects overall and none which
were signicantly different than placebo. This analysis included
headache, nausea, upper respiratory infection and nasopharyn-
gitis. A single case of leukopenia, which was judged possibly
related to medication, was noted in the Mayer study.
119
Both
Zammitt
121
and Mayer
119
found no evidence of rebound insom-
nia or withdrawal effects following discontinuation (notably,
the Mayer et al. study was based on six months of nightly use).
The studies not included in the meta-analysis found no in-
dication of a signicant difference in adverse events between
ramelteon and placebo. Commonly reported adverse events
in these studies included fatigue, headache, dizziness and
somnolence.
Three studies assessed for next-day impairment associated
with ramelteon. Roth and colleagues reported on next-day re-
sidual pharmacological effects of ramelteon in an older adult
population.
120
Observations of DSST, immediate and delayed
recall, subjective alertness, and concentration showed no sig-
nicant residual as compared to placebo on any outcomes.
Employing the same residual effect measures, Zammitt et al.
121
reported small but statistically signicant impairment with
ramelteon 8 mg. in immediate recall at week 3 only, delayed
recall (week 1 only), level of alertness (week 5), and ability to
concentrate (week 1). Mayer
119
found no consistent evidence
of next-day impairment in alertness, recall, DSST or visual
analogue scales of mood, energy, or cognition. Overall, the
available data suggest no consistent evidence of next-day im-
pairment associated with the use of ramelteon.
In summary, the task force found that there was weak evi-
dence of efcacy in the treatment of sleep onset insomnia, with
limited or no consistent evidence of adverse events in excess
of placebo. Therefore, benets were deemed to marginally out-
weigh harms.
patientS’ valueS and preferenceS: Based on its clini-
cal judgement, the task force determined that in light of its
efcacy for sleep onset and its relatively benign side effect
prole, a majority of patients would be likely to use ramelteon
compared to no treatment.
Heterocyclics
Doxepin for the Treatment of Chronic Insomnia
Recommendation 8: We suggest that clinicians use doxepin
as a treatment for sleep maintenance insomnia (versus no
treatment) in adults. [WEAK]
Remarks: This recommendation is based on trials of 3 mg
and 6 mg doses of doxepin.
Summary
Four studies addressed the efcacy of doxepin 3 mg.
127–130
Four
studies also investigated the 6 mg dosage.
128–131
The overall
quality of evidence for both dosages was low due to poten-
tial publication bias and imprecision. The evidence suggests
minimal improvement in SL but clinically signicant im-
provements in WASO, TST and SE. The overall evidence was
graded as weakly in favor of doxepin’s efcacy in improving
sleep maintenance.
Meta-analysis shows that PSG and patient-reported SL
at 3 mg and PSG SL at 6 mg fell below the clinical signi-
cance threshold. Both PSG and subjective TST at 3 mg, as
well as PSG TST at 6 mg, were above signicance thresholds,
although subjective TST at 6 mg fell short of this criterion.
PSG data for reduction of WASO exceeded the clinical sig-
nicance threshold at both dosages, although patient diary
data for WASO at the 6 mg dosage fell below threshold, based
on two studies. The SMD in sleep quality for doxepin 3 mg
suggests moderate improvement, while the SMD for the 6 mg
dosage suggests mild improvement. The objective SE for both
dosages exceeded the clinical signicance level, while objec-
tive NOA fell short.
Meta-analysis of side effects included headache, diarrhea,
somnolence and upper respiratory infection at 3 mg, and head-
ache and somnolence at the 6 mg dose. Results suggest mild
increase in somnolence at 6 mg. Given the demonstrated im-
provements in WASO, TST and SE, with limited adverse ef-
fects, the task force judged the benets to outweigh the harms.
The clinical judgement of the task force was that the majority
of well-informed patients would use doxepin over no treatment.
This judgement is based on the evidence for clinically signi-
cant improvement in WASO, TST and SE.
See Figures S39–S53, S78–S83 and Tables S15 and S16 in
the supplemental material.
Discussion
Five studies investigated the effects of doxepin at 3 mg and/or
6 mg.
127–131
Krystal
127
conducted a 12-week RCT of nightly dox-
epin 1 and 3 mg versus placebo in 240 elderly (> 65 years) sub-
jects with predominant sleep maintenance insomnia. Subjects
were randomized to one of three treatment groups. Outcome
variables included both PSG and sleep diary data. Krystal
128
investigated doxepin 3 mg and 6 mg in a ve week trial which
included 221 adults with sleep onset and maintenance insom-
nia who were randomized to one of the two doxepin doses or
placebo. PSG data and sleep diaries were included. Roth
129
em-
ployed a crossover design with randomized assignment to one
of four treatment sequences which consisted of two nights each
of doxepin 1 mg, doxepin 3 mg, doxepin 6 mg and placebo,
with intervening washout. PSG and sleep diary data were col-
lected. The study included 67 adults who met both baseline
PSG-dened sleep onset and maintenance criteria. Scharf
130
employed the identical crossover design and dosages in 76 el-
derly insomnia subjects. Lankford
131
reported data on a four
week nightly trial of doxepin 6 mg or placebo in 254 elderly
332
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
subjects with sleep onset and sleep maintenance insomnia.
Outcome variables were patient-reported and clinician rated.
Hajak
132
also conducted a RCT of doxepin, but the dosages
(25–50 mg) were signicantly higher that FDA-approved hyp-
notic dosages. For this reason, this study was not included in
the current analysis.
Sleep latency: Four studies
127–130
reported PSG SL data
for the 3 mg dosage. The mean difference from placebo
(−2.30 min; CI: −6.22 to +1.62 min) was below the dened
signicance threshold. Evidence quality was moderate due to
potential publication bias. Likewise, patient-reported SL
127,130
did not meet clinical signicance (−9.35 min; CI: −21.89 to
+3.19 min). Quality was low due to imprecision and poten-
tial publication bias. Three studies included adequate data
for meta-analysis at the 6 mg dosage,
128–130
showing a mean
difference for objective SL of −5.29 min (CI: −1.34 to −9.25
min) with moderate quality of evidence due to publication
bias. No sleep diary data were available for meta-analysis of
SL at this dosage.
total Sleep time: Four investigations
127–130
reported PSG
data for TST at 3 mg. The analysis reveals a clinically signi-
cant increase in TST at this dosage (+26.14 min; CI: +18.49 to
+33.79 min). Quality was low due to imprecision and potential
publication bias. Subjective reports for 3 mg
127,130
were also
in the range of clinical signicance (+43.57 min; CI: +5.16 to
+81.98 min) with very low quality of evidence due to hetero-
geneity, imprecision and potential publication bias. At the 6
mg dosage, PSG-determined TST,
128–130
also met the clinical
signicance criterion (+32.27 min; CI: +24.24 to +40.30 min)
with moderate quality of evidence due to potential publication
bias. However, subjective TST at this dosage
130,131
fell short
of signicance (+18.84 min; CI: −1.65 to +39.34 min) with
LOW quality of evidence due to imprecision and potential
publication bias.
Wake after Sleep onSet: WASO was considered a key
outcome variable in all of the doxepin studies noted. The PSG
data for 3 mg doxepin showed a clinically signicant mean dif-
ference from placebo of −22.17 min (CI: −14.72 to −29.62 min),
based on four trials.
127–130
Quality of evidence was low due to
imprecision and potential publication bias. Only one study
reported subjective WASO, with a reduction of 20.0 min ver-
sus placebo. Quality of these data was low due to imprecision
and potential publication bias. At 6 mg, PSG WASO showed
a clinically signicant reduction of 23.14 min (CI: −16.36 to
−30.34 min)
128–130
with LOW quality of evidence due to impre-
cision and potential publication bias. Patient diary results did
not meet clinical signicance (−14.39 min; CI: −3.93 to −24.86
min)
130,131
with moderate quality of evidence due to potential
publication bias.
Quality of Sleep: Quality of sleep ratings for the 3 mg
dosage suggest substantial improvement (SMD: +0.57; CI:
+0.26 to 0.88 SMD) with low quality of evidence,
127,130
due to
imprecision and potential publication bias. More modest im-
provement was noted at 6 mg (SMD +0.28; CI +0.06 to 0.49
SMD)
130,131
with moderate quality of evidence due to potential
publication bias.
Sleep efficiency: PSG SE was reported in three studies
for the 3 mg dosage.
127,129,130
Evidence quality was low due to
imprecision and potential publication bias. The improvement
in SE was clinically signicant at +6.78% (CI: +4.50 to 9.07%).
SE at the 6 mg dose, based on two investigations
129,130
was also
signicantly improved (+7.06%; CI: +5.12 to 9.01%) with mod-
erate quality of evidence due to potential publication bias.
number of aWakeningS: PSG-determined NOA was
mildly increased (+0.53 awakenings; CI: −0.37 to +1.42 awak-
enings) for 3 mg
127,129,130
and the 6 mg dose (+0.44 awakenings;
CI: −0.57 to +1.44 awakenings), with moderate quality for both,
due to potential publication bias.
overall Quality of evidence: The quality of evidence
in the meta-analytic data for the majority of variables was mod-
erate to low due to industry sponsorship and, in some cases,
imprecision (due to relatively large condence intervals for
numerous variables that cross clinical signicance thresholds).
Quality was further downgraded to very low for subjective
TST at 6 mg as a result of the above factors plus heterogene-
ity of data. As a result, the overall quality of evidence for the
doxepin data is considered very low.
HarmS: Meta-analysis was available for both the 3 mg
127–129
and 6 mg
128,129,131
dosages and revealed no increase in head-
ache frequency with doxepin. Somnolence showed no sig-
nicant increase versus placebo (+0.01 risk difference) at the
3 mg level
127–129
and a small increased risk at 6 mg (+0.04
risk difference).
128,129,131
Data were also available for meta-
analysis of risk for diarrhea and upper respiratory infection.
Neither showed signicantly greater risk than placebo. With
respect to next-day residual effects, no difference was ob-
served between doxepin 3 mg or 6 mg and placebo on DSST,
Symbol Copying Test, or visual analogue scales for morning
sleepiness.
127–130
In summary, the task force found weak evidence for efcacy
in the treatment of sleep maintenance insomnia, with mini-
mal evidence of adverse events in excess of placebo. Therefore,
benets were deemed to be greater than harms.
patientS’ valueS and preferenceS: Based on its clini-
cal judgement, the task force determined that in light of the
data supporting efcacy for reducing WASO, and improving
TST, SE and sleep quality, a majority of patients would be
likely to use doxepin compared to no treatment.
Trazodone for the Treatment of Chronic Insomnia
Recommendation 9: We suggest that clinicians not
use trazodone as a treatment for sleep onset or sleep
maintenance insomnia (versus no treatment) in adults.
[WEAK]
Remarks: This recommendation is based on one trial of a 50
mg dose of trazodone.
333
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
See Table S17 in the supplemental material.
Summary
A single study
78
of trazodone 50 mg met inclusion criteria;
therefore, no meta-analysis is available. The overall qual-
ity of evidence for this study was moderate due to potential
publication bias. The patient-reported data from this study
demonstrated a modest reduction in SL which fell below the
threshold for clinical signicance. Likewise, the moderate in-
crease in TST and the small reduction in WASO did not reach
the clinical threshold criteria. Quality of sleep was insigni-
cantly improved and reduction in NOAs fell just below clinical
signicance. In summary, none of the sleep outcome variables
improved to a clinically signicant degree.
No meta-analysis of harms was possible. Given the absence of
demonstrated efcacy on numerous critical outcome variables,
coupled with limited evidence regarding harms, the task force
judged the harms to potentially outweigh the benets. Based on
its clinical judgement, the task force determined that, despite
the absence of signicant efcacy for trazodone 50 mg and the
paucity of information regarding harms, the majority of patients
would be likely to use trazodone compared to no treatment.
Discussion
Walsh
78
investigated the efcacy of trazodone 50 mg versus
zolpidem 10 mg and placebo. The nal sample for the trazo-
done and placebo groups included 187 adults with sleep on-
set insomnia. Subjects were administered either trazodone or
placebo in double-blind fashion for 14 consecutive nights. All
data were patient-reported.
Sleep latency: Subjective SL was reduced by 10.2 min (CI:
−8.95 to −11.44 min). This falls short of the clinical signicance
threshold. The quality of evidence was moderate due to poten-
tial publication bias.
total Sleep time: Sleep diary TST was increased by a clin-
ically insignicant 21.8 min (CI: +20.10 to +23.49 min). The
quality of evidence was moderate due to potential publication
bias.
Wake after Sleep onSet: Sleep diary WASO was reduced
by 7.7 min (CI: −8.89 to −6.5 min), falling below the threshold.
The quality of evidence was moderate due to potential publica-
tion bias.
Quality of Sleep: On a 4-point scale (1 = excellent,
4 = poor) sleep quality was not signicantly improved versus
placebo (−0.13 points; CI: −0.11 to −0.14 points). The quality of
evidence was moderate due to potential publication bias.
number of aWakeningS: This outcome was reduced by
0.4 (CI: −0.37 to −0.42 awakenings) compared to placebo, less
than the 0.5 subjective awakening threshold. The quality of
evidence was moderate due to potential publication bias.
overall Quality of evidence: The overall quality of
evidence for this study was moderate.
HarmS: There was no meta-analysis of harms. In the Walsh
78
paper, the trazodone group experienced signicantly more
side effects than the placebo group. Chief among these were
headache (trazodone 30%; placebo 19%) and somnolence (tra-
zodone 23%; placebo 8%). In all, 75% of trazodone subjects
reported some adverse event(s), compared to 65.4% of subjects
who received placebo.
patientS’ valueS and preferenceS: Based on its
clinical judgement, the task force determined that, despite
the absence of signicant efcacy for trazodone 50 mg and
the paucity of information regarding harms, the majority of
patients would be likely to use trazodone compared to no
treatment. This is based on the perception of trazodone as a
“safer” sleep-promoting agent by many physicians and the re-
sulting recommendations and prescribing practices of those
physicians.
Anticonvulsants
Tiagabine for the Treatment of Primary Insomnia
Recommendation 10: We suggest that clinicians not use
tiagabine as a treatment for sleep onset or sleep maintenance
insomnia (versus no treatment) in adults. [WEAK]
Remarks: This recommendation is based on trials of 4 mg
doses of tiagabine.
Summary
Three studies addressed the efcacy of tiagabine 4 mg.
133–135
The overall quality of evidence was very low due to potential
publication bias, heterogeneity, and imprecision. Meta-analy-
ses were conducted for SL (PSG and subjective), TST (PSG
and subjective), WASO (PSG and subjective), sleep quality,
SE (PSG), and NOA (PSG and subjective). These analyses
revealed that both objective and subjective measures of sleep
latency fell below the threshold for clinical signicance. Mea-
sures of TST showed minimal change (PSG) and mild to mod-
erate reduction (sleep diary). WASO data demonstrated no
clinically signicant change on either metric. Meta-analysis
of SMD for sleep quality suggested improvement which fell
below the clinical signicance threshold. Neither objective nor
subjective NOAs were reduced by clinically signicant levels,
while PSG SE was minimally reduced.
Meta-analysis of adverse effects showed no difference be-
tween tiagabine and placebo on headache or nausea. Given the
absence of demonstrated efcacy on numerous critical out-
come variables (with slight trending toward mild worsening
on some outcomes), coupled with limited evidence regarding
harms, the task force judged the harms to potentially outweigh
the benets.
It was determined by clinical judgement of the task force
that the majority of well-informed patients would not use ti-
agabine over no treatment. This judgement is based on the lack
of evidence for efcacy and the limited systematic information
regarding adverse effects.
See Figures S55–S64, S84 and S85 and Tables S18– S20 in
the supplemental material.
334
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
Discussion
Three studies were included in the meta-analyses of ti-
agabine.
133–135
Roth
133
studied 207 elderly primary insomnia
patients (65–85 years) with difculty initiating and maintain-
ing sleep who received tiagabine 2, 4, 6, or 8 mg or placebo on
two consecutive study nights with PSG recordings in a paral-
lel group design. Walsh
134
similarly evaluated 232 adults with
chronic sleep-onset and maintenance insomnia. Tiagabine 4, 6,
8, or 10 mg or placebo was administered on two consecutive
nights with PSG. Walsh
135
conducted a crossover study of 58
adults (age 35–64) with chronic sleep onset and maintenance
problems. Subjects received 4, 8, 12, and 16 mg and placebo
for two consecutive nights of sleep recording. Medication-free
washout periods between doses ranged from 5–12 nights.
Sleep latency: The meta-analysis for SL included three
studies.
133–135
PSG SL data showed a small increase in SL
(+3.65 min; CI: −8.00 to +15.31 min) with very low quality of
evidence due to heterogeneity, imprecision and potential pub-
lication bias. The subjective data
133,135
showed a moderate in-
crease in SL (+13.31 min; CI: +7.54 to 19.37 min). Quality of
evidence was moderate due to potential publication bias.
total Sleep time: Objective data for TST
133–135
demon-
strated a minimal reduction in TST (−1.21 min; CI: −7.44 to
+5.02 min) with LOW quality evidence due to heterogeneity
and potential publication bias. Patient-reported TST
133,135
was
reduced by 19.95 min (CI: −25.35 to −14.54 min) with moder-
ate quality of evidence due to potential publication bias. Nei-
ther subjective nor objective ndings met clinical signicance.
Wake after Sleep onSet: The PSG WASO analysis
133–135
revealed essentially no difference from placebo (−0.56 min; CI:
−6.77 to +5.65 min). Quality of evidence was low due to het-
erogeneity and potential publication bias. Sleep diary data
133,135
indicated a small, clinically insignicant increase (+4.29 min;
CI: −0.22 lower to +8.79 min) with moderate quality of evi-
dence due to potential publication bias.
Quality of Sleep: The meta-analysis for QOS
133,135
re-
sulted in a SMD of +0.48 (CI: −0.5 to +1.46 SMD), which falls
below the level of clinical signicance. Quality of evidence
was very low due to heterogeneity, imprecision and potential
publication bias.
Sleep efficiency: The objective sleep efciency was re-
duced (−0.53%; CI: −0.02 to −1.05%). Quality of evidence was
moderate due to potential publication bias.
number of aWakeningS: The PSG NOAs were mildly
increased (+0.5 awakenings; CI: −1.29 to +2.29 awakenings).
The subjective NOA was minimally reduced at −0.21 awaken-
ings (CI: −0.9 to +0.48 awakenings), falling below the thresh-
old for clinical signicance. Level of evidence was low for both
measures due to imprecision and potential publication bias
overall Quality of evidence: The overall quality
of evidence for the meta-analytic data was very low due to
signicant heterogeneity, imprecision and potential bias (in-
dustry sponsorship) for some critical outcomes.
HarmS: Meta-analysis was possible for two adverse effects
(headache and nausea). Neither showed any signicant dif-
ference from placebo. None of the three studies found a sig-
nicant difference from placebo on morning-after DSST or
visual analogue scales for sleepiness/alertness at the 4 mg
dose.
patientS’ valueS and preferenceS: Based on its clini-
cal judgement, the task force determined that in light of the
absence of signicant efcacy at this dose and the paucity of
information regarding harms, the majority of patients would
not be likely to use tiagabine compared to no treatment.
Over-the-counter preparations
Diphenhydramine for the Treatment of Primary
Insomnia
Recommendation 11: We suggest that clinicians not use
diphenhydramine as a treatment for sleep onset and sleep
maintenance insomnia (versus no treatment) in adults.
[WEAK]
Remarks: This recommendation is based on trials of 50 mg
doses of diphenhydramine.
Summary
Two RCTs evaluated diphenhydramine 50 mg for the treat-
ment of chronic primary insomnia.
110,136
The overall quality of
evidence was downgraded to low due to imprecision and risk
of publication bias. The overall evidence for diphenhydramine
50 mg was weakly against its effectiveness for improving
sleep onset and TST. The mean reduction in patient-reported
sleep latency versus placebo fell below the level of clinically
signicant improvement. The same studies found a small in-
crease in TST which also fell below the threshold for clinical
signicance. The single paper
136
which included PSG-deter-
mined SL and TST showed outcomes which also fell below
clinical signicance thresholds. None of the other objective
or patient-reported outcome variables reached clinical sig-
nicance thresholds. In addition, one paper meeting inclusion
criteria
137
but not including suitable data for meta-analysis
evaluated diphenhydramine 50 mg in mild to moderate in-
somnia patients.
No meta-analysis was possible for side effects. Since no
systematic data addressing harms is available, it is difcult
to make a clear determination regarding benets versus
harms. However, in light of the absence of clear benets, the
task force judged the benets and harms to be approximately
equal. It was determined by clinical judgement of the task
force that the majority of well-informed patients would not
use diphenhydramine over no treatment. This judgement is
based on the absence of evidence for clinically signicant
improvement.
See Figures S65 and S66 and Table S21 in the supplemen-
tal material.
335
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
Discussion
Two studies of diphenhydramine 50 mg included adequate
data for meta-analysis. Glass
110
studied 25 elderly subjects
(mean age = 73.9 years) with insomnia. Enrollees received
diphenhydramine, temazepam 15 mg and placebo in a cross-
over design with two weeks of nightly use for each interven-
tion, followed by washout. Primary outcomes measures were
sleep variables recorded in patient diaries. Morin
136
compared
diphenhydramine (14 nights, followed by 14 nights of pla-
cebo) to a valerian-hops preparation (28 nights) and placebo
(28 nights) in a total population of 184 adults with occasional
insomnia (2–4 nights/week with SL > 30 min or WASO > 30
min). Patients were randomly assigned to the intervention
groups and PSG and patient-reported data were collected. A
third study,
137
not included in meta-analysis, assessed mild to
moderate insomnia patients in family practice settings. Par-
ticipants received diphenhydramine 50 mg and placebo for one
week each in crossover fashion, without intervening washout.
Outcome assessment was based on patient-completed sleep
questionnaires.
Sleep latency: The single study employing PSG
136
found
a 7.89 min reduction in SL (CI: −17.40 to +1.62 min). This fell
below the signicance threshold. Quality of evidence was low
due to imprecision and potential publication bias. Two stud-
ies
110,136
met requirements for meta-analysis of subjective SL.
This revealed a mean difference from placebo of −2.47 min (CI:
−8.17 to +3.23 min). The Rickels study
137
found statistically sig-
nicant improvement in SL with diphenhydramine using a 0–4
patient-rating scale, but no specic quantitative data regarding
actual SL times were included.
total Sleep time: Morin
136
reported a PSG TST increase
of 12.37 min (CI: −13.38 to +38.12 min). This fell below the
signicance threshold of 20 min. Quality of evidence was
low due to imprecision and potential publication bias. Meta-
analysis of the two studies demonstrated a 17.86 min increase
(CI: −3.79 to + 39.51 min) in subjective TST versus placebo.
The Rickels study
137
found “statistically signicant improve-
ment” in patient-reported TST but, as noted above, it is un-
clear to what extent this represented clinically signicant
improvement.
Wake after Sleep onSet: No data pertaining to wake af-
ter sleep onset were available.
Quality of Sleep: Glass
110
found minimal difference in
sleep quality between diphenhydramine and placebo (mean
difference of +0.1 SD; CI: −0.45 to +0.65 SD). Quality of
evidence was downgraded to moderate due to potential pub-
lication bias. Rickels
137
reported statistically signicant im-
provement in sleep quality.
Sleep efficiency: The objective sleep efciency data from
the single study reporting PSG analysis
136
found no clinically
signicant improvement (+2.59%; CI: −3.25 to +8.43%). In
this same study, subjective SE also fell below the threshold
(+4.61%; CI: +1.33 to +7.88%).
number of aWakeningS: The change in subjective number
of awakenings (−0.3 awakenings; CI: −1.03 to +0.43 awaken-
ings) was not clinically signicant.
110
overall Quality of evidence: The overall quality of
evidence in the meta-analytic data from these studies was
downgraded to low for imprecision, due to condence inter-
vals which crossed the clinical signicance thresholds for sub-
jective TST, a critical outcome. These studies were industry
sponsored, resulting in further downgrading of evidence due
to potential publication bias. The quality of evidence for indi-
vidual critical outcomes ranged from moderate to low, there-
fore the overall quality of evidence was low.
HarmS: No meta-analysis of adverse effects was possible.
Neither Morin
136
nor Glass
110
found signicant differences
between diphenhydramine and placebo in adverse events.
Rickels
137
reported higher numerical rates of drowsiness, diz-
ziness, and grogginess with diphenhydramine but no statistical
analysis was conducted.
Morin
136
found no substantial rebound effects following dis-
continuation of diphenhydramine. Glass
110
noted minimal dif-
ferences between diphenhydramine and placebo in the number
of subjects experiencing rebound for at least one sleep out-
come variable. Glass
110
found no difference in morning-after
DSST or Manual Tracking Task (MTT) between interventions.
In summary, the task force found that there was weak evi-
dence demonstrating an absence of efcacy in the treatment of
sleep onset insomnia, with minimal evidence of adverse events
in excess of placebo. Therefore, benets were deemed approxi-
mately equal to harms.
patientS’ valueS and preferenceS: Based on its clini-
cal judgement, the task force determined that, in light of the
paucity of data supporting efcacy for sleep onset and mainte-
nance, a majority of patients would not be likely to use diphen-
hydramine compared to no treatment.
Melatonin for the Treatment of Primary Insomnia
Recommendation 12: We suggest that clinicians not use
melatonin as a treatment for sleep onset or sleep maintenance
insomnia (versus no treatment) in adults. [WEAK]
Remarks: This recommendation is based on trials of 2 mg
doses of melatonin.
Summary
Three studies addressed the efcacy of melatonin 2 mg.
138–140
These investigations included only older adults (> 55 years).
The overall quality of evidence was very low due to poten-
tial publication bias, heterogeneity, and imprecision. Meta-
analysis was only achievable for sleep quality. This indicated a
SMD of +0.21 (CI: −0.36 to +0.77 SMD), which was not clini-
cally signicant. The minimal overall evidence available was
weakly against melatonin’s efcacy in improving sleep onset,
maintenance, or quality.
No adequate data for meta-analysis of adverse effects was
available. Given the lack of evidence for efcacy in treating
336
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
insomnia, and the unavailability of systematic data on side ef-
fects, the task force judged the benets to be approximately
equal to harms. It was determined by the task force that the
majority of well-informed patients would use melatonin over
no treatment. This is based on its availability and the wide-
spread perception of melatonin as a benign sleep aid.
See Figure S67 and Table S22 in the supplemental material.
Discussion
Three studies included adequate data for melatonin meta-anal-
ysis.
138–140
Lemoine
138
studied 170 older adults (age > 55 years)
with primary insomnia. Subjects received either prolonged re-
lease melatonin (PRM) 2 mg or placebo nightly for 3 weeks.
Outcome data was patient-reported. Luthringer
139
similarly
studied 40 older adults (age > 55 years) who received PRM 2
mg or placebo for 3 weeks. Outcomes included both PSG and
subjective data. Finally, Wade
140
evaluated 354 patients of the
same age group with PRM 2 mg or placebo nightly for 3 weeks.
Outcome data was patient-reported.
In addition, seven trials which met inclusion criteria but
did not include adequate data for meta-analysis were identi-
ed.
141–147
These investigations employed various dosages and
combinations with other agents, rendering meaningful com-
parisons to the 2 mg RCTs impossible. Pertinent features of
these studies are included within each outcome section.
Haimov
143
conducted a randomized crossover study of el-
derly adults with insomnia consisting of one week on each of
three interventions (2 mg sustained-release melatonin, 2 mg
fast-release melatonin or placebo) with intervening washout,
followed by a 2-month extension of 1 mg slow-release melato-
nin. Data were derived from actigraphy. Zhdanova
147
evaluated
three dosages of melatonin (0.1, 0.3, and 3 mg) versus placebo in
a randomized crossover study of 30 elderly (> 50 years) adults
(15 normal sleepers and 15 insomnia subjects with reduced SE).
Subjects received each dosage or placebo for one week with
intervening washout. Wade
146
administered prolonged-release
melatonin 2 mg or placebo to adults with primary insomnia
for 3 weeks, after which the melatonin group continued for 26
weeks, while the placebo group was re-randomized to mela-
tonin or placebo (1:1). Sleep outcome variables (from sleep
diary) were analyzed according by age group as well as by
melatonin deciency status. Baskett
141
conducted a random-
ized controlled crossover study of healthy elderly with sleep
maintenance problems. Subjects received 5 mg melatonin or
placebo for four weeks with intervening washout.
Sleep latency: Meta-analysis was not possible for sleep
latency. Luthringer
139
reported a PSG SL reduction of 8.9 min
(CI: −2.35 to −15.45 min), which falls below clinical signi-
cance (prolonged release 2 mg). The quality of evidence was
low due to imprecision and potential publication bias.
In the Haimov
143
investigation, fast-release melatonin pro-
duced signicantly shorter SL than placebo at one week. At 2
months, sustained release 1 mg resulted in signicantly shorter
SL than placebo. Zhadanova
147
reported no signicant im-
provement in PSG SL at any dosage.
Wade
146
found that the melatonin decient group (includ-
ing all ages) showed no improvement with melatonin versus
placebo on SL at three weeks. However, the elder group (65–80
years) showed signicant reduction of SL with melatonin, re-
gardless of melatonin deciency status (SL: −19.1 min; pla-
cebo −1.7 min). This improvement held at 19 weeks for the
elder group (melatonin: −25.9 min; placebo: −8.3 min). Wade
145
subsequently re-analyzed these data and reported that the sig-
nicant improvement in SL held when the age range for the
“elderly” group was expanded to 55–80 years, but not lower.
Baskett
141
found no improvement in SL (as measured by sleep
diary) with melatonin 5 mg.
total Sleep time: There were inadequate data for meta-
analysis of TST. Luthringer
139
found an increase of 2.2 min ver-
sus placebo (CI: −19.13 to +23.53 min) in objective TST with
melatonin 2 mg. The quality of evidence was very low due to
signicant imprecision of the data, and potential publication
bias.
Zhdanova
147
observed no increase in objective TST at any
dosage. Wade
146
reported no improvement in patient-reported
TST in the low melatonin secretor population (regardless of
age) at 3 weeks but observed a small improvement (estimated
difference: +13.1 min) at 29 weeks. Analysis of the elderly
population revealed no signicant improvement in TST at any
point. Baskett
141
reported no improvement at the 5 mg dose as
measured by sleep diary.
Wake after Sleep onSet: No meta-analysis was possible
for WASO. Luthringer
139
found a small increase in WASO
(+8.5 min: CI: −11.75 to +28.75 min) in the prolonged release
melatonin 2 mg group. The quality of evidence was very low
due to signicant imprecision of the data, and potential publi-
cation bias.
Quality of Sleep: The meta-analysis of QOS demonstrated
a small improvement in quality of sleep (+0.21 SMD: CI: −0.36
to +0.77 SMD), which fell below the threshold for clinical sig-
nicance. The quality of evidence was very low due to hetero-
geneity, imprecision and potential publication bias.
Baskett
141
found no improvement in quality of sleep with
5 mg melatonin. Wade
146
reported no improvement with pro-
longed-release melatonin at 3 weeks and 29 weeks in the low
excretor and elderly groups.
Sleep efficiency: There were not adequate data for meta-
analysis of melatonin SE.
Haimov
143
reported small to moderate increases in acti-
graphic SE versus placebo (placebo: 77.4%; fast-release 2 mg/1
week: 78.8%; sustained release 2 mg/1 week: 80.4%; sustained
release 1 mg/2 months: 84.3%). Both of the sustained release
dosages and durations were statistically signicantly different
from placebo. Zhdanova
147
also reported signicant improve-
ment in PSG SE versus placebo in the multiple dose crossover
study (placebo: 78%; melatonin 0.1 mg: 84%; 0.3 mg 88%; 3
mg: 84%). Baskett
141
found no difference between placebo and
melatonin 5 mg for subjective SE.
number of aWakeningS: Insufcient data precluded
meta-analysis of NOA. Luthringer
139
found an increased (+1.4
337
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
awakenings; CI: −4.59 to +7.39 awakenings) NOA with mela-
tonin, as measured by PSG. The quality of evidence was very
low due to signicant imprecision of the data and potential
publication bias.
Zhdanova
147
and Baskett
141
reported no difference in NOA
between melatonin and placebo by PSG or patient diary,
respectively.
overall Quality of evidence: The overall quality of
evidence in the single outcome meta-analytic data from these
studies was downgraded to very low due to heterogeneity, im-
precision, and industry sponsorship, resulting in potential pub-
lication bias.
HarmS: Meta-analysis for adverse events was not possible. Of
the included investigations, none reported clinically signicant
differences in adverse events between melatonin and placebo
for any dosage or duration.
138–140,146
With one possible excep-
tion, no rebound or withdrawal effects were reported.
138,139,146
Haimov
143
found marginally signicant difference in SE be-
tween the active phase for two month, 1 mg sustained-release
melatonin and the withdrawal period.
In summary, the task force found that there was weak evi-
dence against clinically signicant efcacy in the treatment of
sleep onset insomnia, with little systematic evidence regarding
harms. However, mixed evidence suggests possible improve-
ment in SL in an elderly population. Therefore, benets were
deemed to be approximately equal to harms.
patientS’ valueS and preferenceS: Based on clinical
judgement, the task force determined that despite the paucity
of meta-analytic data, equivocal data regarding efcacy for
sleep-onset insomnia, and absence of data regarding sleep
maintenance, a majority of informed patients would be likely
to use melatonin compared to no treatment. As previously
noted, this is based on its availability and the widespread per-
ception of melatonin as a benign sleep aid.
L-tryptophan for the Treatment of Primary Insomnia
Recommendation 13: We suggest that clinicians not use
tryptophan as a treatment for sleep onset or sleep maintenance
insomnia (versus no treatment) in adults. [WEAK]
Remarks: This recommendation is based on trials of 250 mg
doses of tryptophan.
Summary
Only one study
148
contained adequate data, so meta-analysis
was not possible. The quality of evidence for the critical out-
comes was high. This study, consisting of patient-reported
data, showed a modest decline in TST, which was not clinically
signicant. WASO was decreased slightly, while sleep quality
was mildly increased; neither met thresholds for clinical sig-
nicance. Sleep efciency was insignicantly decreased.
No meta-analysis of harms was possible. Given the absence
of demonstrated efcacy on numerous critical outcome vari-
ables, coupled with limited evidence regarding harms, the task
force judged the harms to potentially outweigh the benets.
Based on its clinical judgement, the task force determined that,
despite the absence of signicant efcacy for tryptophan 250
mg and the absence of information regarding harms, the ma-
jority of patients would be likely to use tryptophan compared
to no treatment.
See Table S23 in the supplemental material.
Discussion
Hudson
148
investigated the effects of food source tryptophan
(250 mg), pharmacological tryptophan 250 mg, both with
carbohydrate, versus carbohydrate alone. Subjects (n = 31) re-
ceived one of the three interventions for one week. Outcome
data consisted of sleep diaries.
Two additional papers met inclusion criteria, but used much
higher dosages. Hartmann
149
compared tryptophan 1 g to seco-
barbital, urazepam, and placebo in a one week trial. Tryp-
tophan and placebo groups included 52 subjects with chronic
insomnia. Data were patient-reported. Spinweber
150
studied
20 young men with sleep onset insomnia. Following placebo
run-in, ten subjects received tryptophan 3 g and ten received
placebo for six nights, with PSG recordings nightly.
Sleep latency: The Hudson
148
study did not report sleep
latency data.
Spinweber
150
noted improvement in PSG sleep latency only
on nights 4–6 of administration (11.2 min lower than placebo
for this period). Hartmann
149
found no difference in subjective
sleep latency between tryptophan and placebo during active
treatment.
total Sleep time: Hudson
148
reported a moderate reduc-
tion in subjective TST (−20 min; CI: −31.29 to −8.7 min). The
quality of evidence was moderate due to imprecision. Other
investigations did not report TST data.
Wake after Sleep onSet: Hudson
148
noted a small reduc-
tion in subjective WASO (−9.7 min: CI −15.21 to −4.18 min),
that did not meet clinical signicance. The quality of evidence
was high.
Quality of Sleep: On a 3-point scale (1 = low, 3 = high)
sleep quality was increased (+0.3 points: CI +0.22 to +0.37
points) in the Hudson study.
148
The quality of evidence was
high. Hartmann
149
found no signicant difference between
tryptophan and placebo on a measure of “How well I slept.”
Sleep efficiency: Sleep efciency was not reported by any
study.
number of aWakeningS: NOA was not reported by any
study.
overall Quality of evidence: The overall quality of
evidence for this the critical outcomes was high.
HarmS: There was no meta-analysis of harms. None of the
papers reported systematic information regarding adverse ef-
fects associated with tryptophan.

338
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
patientS’ valueS and preferenceS: Based on clinical
judgement, the task force determined that, despite the absence
of signicant efcacy for tryptophan 250 mg and the absence
of information regarding harms, the majority of patients would
be likely to use tryptophan compared to no treatment.
Valerian for the Treatment of Primary Insomnia
Recommendation 14: We suggest that clinicians not use
valerian as a treatment for sleep onset or sleep maintenance
insomnia (versus no treatment) in adults. [WEAK]
Remarks: This recommendation is based on trials of vari-
able dosages of valerian and valerian-hops combination.
Summary
Morin
136
evaluated a combination of valerian (374 mg native
extract) and hops (83.8 native extract). The overall quality of
evidence for these data was low due to imprecision and po-
tential publication bias. PSG sleep latency was reduced to a
degree that fell below the clinical signicance threshold. Other
measures, including subjective SL, as well as PSG and patient-
reported TST and SE were improved, but did not meet clinical
signicance thresholds.
No meta-analysis of harms was possible. Given the ab-
sence of demonstrated efcacy on critical outcome variables
(with the possible exception of marginally improved PSG SL),
coupled with limited evidence regarding harms, the task force
judged the harms to be roughly equal to the benets. Based on
its clinical judgement, the task force determined that, given
the lack of efcacy for valerian (with the possible exception of
small improvements in SL) and the limited information regard-
ing harms, the majority of patients would not be likely to use
valerian compared to no treatment.
See Table S24 in the supplemental material.
Discussion
Morin
136
investigated the effects of a valerian-hops combina-
tion in dosages noted above. This combination was compared
to diphenhydramine and placebo. Subjects with mild difculty
initiating or maintaining sleep were randomized to one of the
three interventions (valerian-hops n = 59; diphenhydramine
n = 60; placebo n = 65) with nightly administration for 28 days.
A subset (valerian n = 22; placebo n = 26) underwent PSG at
baseline and at the end of weeks one and two.
One additional paper
151
met inclusion criteria, but employed
a higher dosage. Oxman conducted a randomized trial involv-
ing 405 adults of all ages with insomnia. Subjects were ran-
domized to two-week, nightly administration of valerian (3,600
mg) or placebo. Outcomes were patient-reported and captured
as ranges, therefore the data were not usable for meta-analysis.
Sleep latency: Morin
136
found a reduction in PSG SL of
9.29 min (CI: −0.27 to −18.3 min). This approached clinical
signicance. The quality of evidence was LOW due to impre-
cision and potential publication bias. Subjective SL, however,
was increased by +3.77 min (CI: −4.47 to +12.01 min), with
moderate quality of evidence due to potential publication bias.
Oxman
151
found no statistically signicant improvement in SL.
total Sleep time: In the Morin
136
study, PSG TST was in-
creased, although not to a clinically signicant degree (+10.96
min; CI: −21.67 to +43.59 min) (very low quality of evidence).
Patient-reported TST was higher (+3.12 min; CI: - 22.08 to
+28.32) with moderate quality of evidence. Oxman
151
found no
signicant improvement in subjective TST.
Wake after Sleep onSet: WASO data were not reported
in any study.
Quality of Sleep: Morin
136
did not report quality of sleep
data and Oxman
151
found no statistically signicant difference
versus placebo in the percentage of patients meeting the de-
ned sleep quality improvement criterion (valerian 28.7%; pla-
cebo 21.2%; difference +7.5% [95% CI:15.9 to 20.9%]).
Sleep efficiency: Minimal increases in objective (+0.96%;
CI: −5.02 to +6.94%) and subjective (1.85%; CI: −1.9 to +5.6%)
SE were noted by Morin.
136
Both outcomes were downgraded
due to potential publication bias, while PSG data was down-
graded further due to signicant imprecision.
number of aWakeningS: Oxman
151
observed a statistically
signicant reduction in average change scores for NOA with
valerian.
overall Quality of evidence: Quality of evidence
for all outcomes ranged from very low to moderate. The only
critical outcome for which adequate data was reported dem-
onstrated low quality evidence, therefore the overall quality of
evidence was low.
HarmS: Morin
136
observed no difference between valerian-
hops and placebo with respect to frequency of adverse events.
No serious adverse events were noted. Likewise, Oxman
151
found no increase in adverse events at the higher valerian dose
compared to placebo.
patientS’ valueS and preferenceS: Based on its clini-
cal judgement, the task force determined that, given the lack
of efcacy for valerian (with the possible exception of small
improvements in SL) and the limited information regarding
harms, the majority of patients would not be likely to use vale-
rian compared to no treatment.
LITERATURE REVIEWS
The following section contains literature reviews of drugs for
which clinical practice recommendations were not possible,
due to inadequate data for statistical analyses.
Estazolam
Summary
Three studies evaluated the efcacy of estazolam
152–154
us-
ing similar patient sleep questionnaires, but none of the data
were suitable for meta-analysis. Likewise, it was not possible
339
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
to evaluate these data with respect to the established clinical
signicance thresholds. Therefore, no recommendations re-
garding efcacy of estazolam are possible. The data suggest
statistically signicant subjective improvement versus placebo
at the 2 mg dosage for all parameters assessed.
Discussion
Cohn
152
compared estazolam 1 mg and 2 mg to urazepam and
placebo in approximately 100 adults with chronic sleep onset
and maintenance insomnia in a parallel group design. Subjects
were randomized to receive drug or placebo for seven consecu-
tive nights. Outcomes were measured by sleep questionnaires
(interval ratings and Likert scales). Dominguez
153
evaluated a
similar population of 45 adults with estazolam 2 mg, uraz-
epam or placebo for 7 nights. Sleep variables were assessed by
patient questionnaire. Scharf
154
studied 243 outpatients with
complaints of sleep onset or maintenance difculty. Subjects
were randomly assigned to one of three parallel groups: es-
tazolam 2 mg, urazepam 30 mg or placebo. Medications were
administered for 7 nights. Subjects rated sleep latency, TST,
QOS and NOA on numerical interval questionnaires.
Three studies found statistically signicant improvement
in SL on patient ratings with estazolam 2 mg. The only study
which included estazolam 1 mg reported no signicant im-
provement on SL. All three studies reported signicant im-
provement versus placebo in sleep duration at 2 mg. The 1 mg
dosage also produced signicant improvement in sleep du-
ration. Sleep quality was likewise improved at both dosages
studied, as were NOA. No studies assessed WASO or SE.
Quazepam
Summary
Seven studies evaluated the efcacy of quazepam versus pla-
cebo in randomized, controlled trials.
108,155 –160
One of these
studies
160
reported PSG ndings while the remainder relied ex-
clusively on subjective data derived from sleep questionnaires.
Data analysis varies somewhat across these studies, rendering
comparisons difcult. Only one investigation
160
met require-
ments for meta-analysis. Overall, the studies suggest efcacy
in reducing time to onset of sleep, increasing TST, and reduc-
ing NOA. The methodologies employed were not comparable
to the standard of data reporting required by GRADE and,
therefore, no specic recommendation was made. Quazepam
and its metabolites have long half-lives, raising concerns re-
garding accumulation and daytime impairment. Data regard-
ing daytime sleepiness from these studies suggests a higher
percentage of patients with somnolence in the active treatment
group versus placebo, particularly at the 30 mg dosage.
Discussion
Alden
155
evaluated 57 insomnia subjects in a 5 night, parallel
group design with quazepam 30 mg as the active drug. This
study and all additional quazepam studies reported here (with
the exception of Roth
160
) utilized patient sleep questionnaire
data consisting of numerical interval and other rating scales.
Hernandez
156
studied 36 insomnia outpatients with quazepam
15 mg and placebo in a similar ve night design. Martinez
157
assessed 41 older adults (> 65 years) with insomnia in a con-
trolled trial with quazepam 15 mg or placebo administered
over 5 consecutive nights. Mendels
158
assessed the same dos-
age in 60 adult insomnia outpatients for ve nights. O’Hair
159
reported results of a ve night trial in 60 subjects with quaz-
epam 30 mg. Scharf
108
studied quazepam 15 mg and triazolam
0.5 mg versus placebo over a ve week period. During this
time, subjects received active drug or placebo for nine con-
secutive nights, followed by 14 nights of every other night ad-
ministration. Subjects were 65 insomnia outpatients. Finally,
Roth
160
evaluated quazepam 7.5 mg and 15 mg versus placebo
in 30 older insomnia subjects (> 60 years). PSG was conducted
for two nights in the early phase of treatment (nights 1 and 2
of active treatment) and during the late phase (nights 6 and 7).
Sleep latency: Utilizing a cutoff of sleep latency < 45 min
to identify “responders,” Aden
155
reported quazepam 30 mg
to be statistically superior to placebo. O’Hair
159
demonstrated
quazepam 30 mg to be signicantly better than placebo on an
interval scale for sleep latency.
Hernandez
156
found quazepam 15 mg signicantly bet-
ter than placebo on sleep latency interval scales. Likewise,
Scharf
108
reported signicantly shorter latencies at this dos-
age on interval scales during active treatment nights in every-
other-night administration although this was apparently not
the case during the initial nightly administration. Using a 45
min sleep latency cutoff as described above,
155
Martinez
157
demonstrated a signicantly higher percentage of responders
to 15 mg in a geriatric population. Roth
160
did not report sig-
nicant differences between quazepam 7.5 mg or 15 mg and
placebo on PSG SL.
total Sleep time: Utilizing a cutoff of sleep duration > 6 h
to identify “responders,” Aden
155
reported quazepam 30 mg
to be statistically superior to placebo. O’Hair
159
demonstrated
quazepam 30 mg to be signicantly better than placebo on an
interval scale for TST.
Hernandez
156
found quazepam 15 mg to be signicantly su-
perior to placebo on sleep duration interval scales. Likewise,
Scharf
108
reported signicantly longer duration at this dosage
on interval scales during active treatment nights in every-other-
night administration, except on the initial night of administra-
tion. Using a > 6 h sleep duration cutoff as described above,
155
Martinez
157
demonstrated a signicantly higher percentage of
responders to 15 mg in a geriatric population. Roth
160
reported
improvement in PSG TST during early (treatment nights 1 and
2) and late (nights 6 and 7) with quazepam 15 mg in a geriat-
ric insomnia population. A statistically signicant effect with
quazepam 7.5 mg was seen only during nights 6 and 7.
Wake after Sleep onSet: No studies reported placebo
comparisons for WASO.
Quality of Sleep: The majority of studies of “sleep qual-
ity” with quazepam utilized a composite index for sleep qual-
ity (including questions on nightmares and overall evaluation
of the medication) which is not consistent with sleep quality
measures used in other studies; therefore these results are not
340
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
discussed. Scharf
108
reported a single measure of sleep quality
(“How would you describe your sleep”). Quazepam 15 mg was
signicantly better than placebo on active treatment nights in
both the nightly and every other night administration.
Sleep efficiency: No studies reported placebo comparison
data for SE.
number of aWakeningS: Employing a threshold for “re-
sponse” of < 2 awakenings, Aden
155
reported a signicantly
higher percentage of responders to quazepam 30 mg than pla-
cebo. O’Hair
159
also found signicantly fewer awakenings at
this dosage compared to placebo using interval scales. At the
15 mg dosage, two studies
156,157
found a signicantly greater
number of “responders” (i.e. < 2 awakenings) compared to pla-
cebo. No PSG data for NOA were reported.
adverSe effectS: Five studies reported specic data for
daytime somnolence. Aden
155
found an approximately four-
fold higher rate of somnolence at 30 mg (quazepam 16/24; pla-
cebo = 4/26). At the same dose, O’Hair
159
reported somnolence
in 12/30 quazepam and 5/30 placebo subjects. At 15 mg, Mar-
tinez
157
noted no difference in adverse events. Hernandez
156
reported somnolence in 9/30 quazepam subjects and 6/30 pla-
cebo subjects. Mendels
158
found 7/30 quazepam subjects and
4/30 placebo subjects demonstrated daytime somnolence.
Flurazepam
Summary
Sixteen studies met general inclusion and exclusion crite-
ria.
98,100,101,105,109,149,152–154,161–167
No studies contained data ad-
equate for meta-analysis. No meta-analysis of harms was
possible. These studies were highly varied in design. Of these,
three
100,101,105
included no urazepam/placebo comparison and
were excluded from discussion. All of the studies included one
or both of the standard urazepam doses: 15 mg and 30 mg.
Studies of the efcacy of urazepam had numerous method-
ological inconsistencies, including instruments for subjective
assessments of sleep outcomes that were highly variable across
these studies, which made valid comparisons across studies
impossible. Many studies incorporated interval scales with no
reports of specic values. In light of these inconsistencies, and
the related unavailability of meta-analyses, no recommenda-
tions regarding efcacy of urazepam were made. The data
for sleep onset at both the 15 mg and 30 mg dosages are mixed.
The majority of studies did report increases in TST with the 30
mg dosage, but not at 15 mg. Data for WASO are limited to two
studies, one of which (a PSG study) showed improvement at 30
mg. Sleep quality reports uniformly indicated improvement at
both dosages, while reports for NOA suggest reduction at the
30 mg dosage only.
Discussion
Cohn
152
compared urazepam 30 mg and placebo in approxi-
mately 100 adults with chronic sleep onset and maintenance
insomnia in a parallel group design. The study, with a total
n = 223, also included two dosages of estazolam, discussed
elsewhere. Subjects were randomized to receive drug or pla-
cebo for seven consecutive nights. Outcomes were measured
by sleep questionnaires (interval ratings and Likert scales).
Dominguez
153
evaluated a similar population of 45 adults with
urazepam 30 mg or placebo for 7 nights. Sleep variables were
assessed by patient questionnaire. Elie
161
studied 60 outpatient
insomnia patients using a cross-over study design in which
each patient received a single dose of ve different drugs (or
drug dosages) or placebo on one night of the week over a ve
consecutive week period. Study drugs included urazepam
15 mg, three crossover dosages of loprazolam, and placebo.
Outcomes included an index for sleep-onset based on patient
questionnaires. Elie
162
investigated efcacy of urazepam 30
mg and zopiclone versus placebo over 4 weeks. Flurazepam
and placebo groups included 12 chronic insomnia patients per
group. Subjects reported sleep outcome variables on post-sleep
numerical rating questionnaires. Hartmann
162
studied 96 adult
patients (n = 45 for urazepam and placebo groups) with vari-
ous insomnia complaints. Subjects were randomly assigned to
receive urazepam 30 mg, secobarbital, l-tryptophan, or pla-
cebo for one week of active treatment. Outcomes were assess
by sleep logs which included subjective estimates of SL, NOA,
duration of awakenings, and QOS.
Mamelak
164
investigated the effects of urazepam 30 mg
and zopiclone versus placebo in three groups of 10 insomnia
subjects per group, each of which received one of the three
treatment conditions for 12 consecutive nights. Subjective es-
timates of SL, TST and NOA were reported. Mamelak
165
stud-
ied 36 elderly patients with chronic insomnia. Patients were
randomized to urazepam 15 mg, brotizolam or placebo for
14 nights. Outcomes included patient-reported SL, NOA, TST
and wake time. Daytime performance measures were con-
ducted at the beginning of treatment and following conclusion.
Melo de Paula
166
evaluated urazepam 30 mg versus placebo
and two dosages of lormetazepam in 60 adults with sleep on-
set or maintenance problems. Subjects received one of the four
treatment conditions for two weeks. Outcome data included
subjective SL, NOA and TST.
Reeves
98
investigated the efcacy of urazepam 15 mg and
triazolam versus placebo in 61 geriatric subjects (n = 27 for
urazepam and placebo groups) with sleep onset or mainte-
nance insomnia. Subjective sleep outcomes were assessed by
interval rating questionnaires. Salkind
167
evaluated uraz-
epam 15 and 30 mg versus placebo in 30 general practice
insomnia patients. Subjects received each dose of uraz-
epam and placebo for one week in a crossover trial. Patient-
reported SL, TST and QOS were primary outcome variables.
Daytime residual effects were also reported. Scharf
154
stud-
ied 243 outpatients (n = 163 for urazepam versus placebo)
with complaints of sleep onset or maintenance difculty.
Subjects were randomly assigned to one of three parallel
groups: urazepam 30 mg, estazolam 2 mg or placebo. Treat-
ments were administered for 7 nights. Subjects rated sleep
latency, TST, QOS and NOA on numerical interval question-
naires. Sunshine
109
investigated the effects of 15 mg and 30
mg urazepam versus two dosages of triazolam and placebo
in a ve-night crossover study, with subjects receiving each
intervention for one night. Subjects were 25 inpatients who
341
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
complained of sleep onset and maintenance problems. Pa-
tients completed sleep questionnaires with interval ratings
for TST and NOA.
Kripke
163
conducted the only identied PSG study of uraz-
epam. In this study, 99 subjects with chronic insomnia were
randomized to one of four parallel groups (urazepam 15 mg,
urazepam 30 mg, midazolam or placebo). Subjects received
treatment for 14 consecutive nights, with PSG recordings on
nights 1, 2, 7, 13 and 14. Objective SL, WASO, TST, and SE
were reported.
Sleep latency: The only PSG study of 30 mg
163
found no
signicant reduction in SL versus placebo.
Five studies
152,154,164,166,167
reported statistically signicant im-
provement on subjective ratings of sleep onset for urazepam
30 mg versus placebo. Kripke
163
found improvement in patient-
reported SL for 30 mg only in the early period (nights 1 and
2) of administration. No signicant difference from placebo
was evident at end of 14-day treatment. Four reports
109,149,153,162
found no signicant subjective improvement in sleep onset
with urazepam 30 mg versus placebo.
Three studies
98,161,167
reported subjectively improved onset at
the 15 mg dosage. Kripke
163
found patient-reported improve-
ment at this dosage only on nights 1 and 2. Two investigations
demonstrated no improvement in sleep onset for urazepam 15
mg versus placebo.
total Sleep time: Eight studies
109,152–154,163,164,166,167
reported
statistically signicant improvement for urazepam 30 mg
versus placebo on various subjective scales for sleep duration.
One study
162
reported no signicant improvement in duration
at this dosage.
Two st ud ies
109,167
found signicantly improved patient-re-
ported duration at the 15 mg dosage; Kripke
163
reported sub-
jective improvement only on nights 1 and 2. Likewise, two
studies
98,165
found no signicant subjective improvement in
sleep duration for urazepam 15 mg.
Wake after Sleep onSet: Two studies reported data for
WASO. K r ipke
163
found signicantly reduced PSG WASO with
urazepam 30 mg versus placebo. Mamelak
165
reported no sig-
nicant reduction in subjective WASO with urazepam 15 mg
in an elderly insomnia population.
Quality of Sleep: Utilizing a variety of self-report scales,
six studies
98,152–154,161,167
reported improvement in sleep quality
with urazepam versus placebo. Four studies
152–154,167
found im-
provement at the 30 mg dosage and three studies
98,161,167
at the
15 mg level.
Sleep efficiency: One study
163
reported PSG sleep ef-
ciency. Flurazepam 30 mg signicantly improved sleep ef-
ciency versus placebo.
number of aWakeningS: Six studies
109,152–154,162,164
assessed
subjective NOA with urazepam 30 mg. All found signicant
reduction in NOA. Three studies
98,109,165
found no signicant
reduction in NOA with urazepam 15 mg.
adverSe effectS: Cohn
152
reported that 68% of urazepam
30 mg subjects experienced an adverse event versus 43% of
subjects receiving placebo. Approximately 50% of the uraz-
epam group reported somnolence, about twice the rate in the
placebo population. Dominguez
153
found a signicant increase
in side effects for urazepam 30 mg compared to placebo and
stated that 73% of side effects described as “undetermined”
were reports of somnolence. Elie
161
indicated that there was no
signicant difference in adverse events between urazepam 15
mg and placebo; likewise Elie
162
found no difference in rates of
somnolence for urazepam 30 mg versus placebo. Mamelak
164
found signicant performance impairment with urazepam 30
mg. Mamelak
165
reported signicantly shorter latencies to sleep
on MSLT at the beginning and end of treatment. The authors
also found signicant impairment on digit symbol substitution
and serial learning as well as a signicantly slower rate of im-
provement on reaction, response and movement time. Divided
attention was also impaired at end of treatment. Reeves
98
noted
that 6 of 13 urazepam subjects reported somnolence (versus
4/14 in the placebo group). Salkind
167
described impaired motor
performance in the urazepam 30 mg group (although not in
the 15 mg group) and a signicantly higher rate of “hangover
effect” at the higher dosage. In the cross-over design, 11 of
30 urazepam group experienced morning drowsiness/hang-
over, which was reported by only 3 of 30 subjects during the
urazepam 15 mg period and 2 of 30 while taking placebo.
Finally, Scharf
154
found AEs in 73% of the urazepam 30 mg
group versus 43% on placebo subjects. Somnolence was the
most common event, reported by 57% of urazepam subjects
and 23% of the placebo group.
Oxazepam
Götestam
168
studied the efcacy of oxazepam 25 mg vs. pla-
cebo with a crossover design in 28 patients with “insomnia.”
Subjective reports using interval ratings showed a signicant
reduction in SL and signicant improvement in QOS.
Quetiapine
One study
169
investigated the efcacy of quetiapine versus pla-
cebo control in primary insomnia. However, the study included
only 13 subjects. Numerical increase in subjective TST and de-
crease in subjective SL were found, but these differences were
not statistically signicant, possibly due to small sample size.
Gabapentin
One study
170
evaluated gabapentin for treatment of primary in-
somnia. This was an open-label investigation with 18 subjects,
variable dosages, and no placebo control. Therefore, the trial
was excluded.
Paroxetine
Two studies assessed paroxetine for treatment of primary in-
somnia. Nowell
171
reported a trial of variable dosage in 15 pa-
tients, without placebo control. As a result, this investigation
was excluded.
Reynolds
172
evaluated paroxetine 10 mg/20 mg in 27 older
adults with primary insomnia who were randomized to drug
or placebo. The two doses were pooled for statistical analysis.

342
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
PSG data showed a modest but signicant increase in SL, de-
crease in WASO and no difference in SE versus placebo. Sleep
quality was improved.
Trimipramine
Hohagen
173
studied the effects of trimipramine in 15 adults
with primary insomnia. No placebo control was included and,
as a result, the study was excluded. Riemann
174
evaluated 55
adults with primary insomnia in a placebo-controlled double
blind study. Dosage was variable (50–200 mg; mean 109.4 mg),
but pooled for analysis. No signicant difference was observed
between trimipramine and placebo for PSG TST or SL, but
SE was signicantly improved with trimipramine. Subjective
sleep quality also showed signicant improvement.
DISCUSSION AND FUTURE DIRECTIONS
Defining “Efficacy”
Assessment of the efcacy of a given agent for the treatment of
chronic insomnia is a complex and challenging task. It remains
unclear which are the most important variables for dening ef-
cacy. Older studies, particularly the majority of investigations
of benzodiazepine efcacy, utilized a variety of predominantly
subjective scales and questionnaires. These are highly diverse
and did not often include specic numerical patient estimates
for sleep outcomes. Since the advent of newer benzodiazepine
receptor agonists, more specic and uniform outcomes for both
patient-reported and objective outcomes (e.g., self-reported
and PSG sleep onset latency, wake time after sleep onset, and
total sleep time) have been employed, although continued sub-
stantial variability in data reporting has not been uncommon.
In addition to the variability in outcome measures reported,
there are a number of critical unresolved issues regarding eval-
uating the efcacy of treatments for chronic insomnia. One
is the relative importance of subjective versus objective data.
Another is whether metrics of sleep quality, whether they be
subjective or objective (e.g. analysis of the microstructure of
sleep or related physiological parameters), are perhaps more
pertinent than measures of SL, TST or WASO. An additional
issue of importance is whether efcacy is better reected by
measures of daytime alertness and cognitive, emotional, and
psychomotor function than by measures of sleep. Recent be-
havioral treatment studies in chronic insomnia have taken
yet another direction: measuring response or remission of the
insomnia syndrome as the most clinically-relevant outcome.
This approach makes sense from a patient-centered approach,
since most patients complain of “difculty” falling asleep or
staying asleep, rather than tying their complaints to any spe-
cic numerical value. Indeed, several studies have identied a
group of “non-complaining poor sleepers” whose quantitative
sleep measures are similar to those with insomnia. Examining
the insomnia syndrome is also useful because it addresses both
sleep-related and wake-related symptoms.
Absent clear answers to these questions, the present analysis
relies on conventional subjective and objective measures of
major sleep variables (sleep onset latency, total sleep time or
wake time after sleep onset). The meta-analyses conducted
yield recommendations for use of a limited number of drugs
for a limited number of specic indications (i.e. sleep onset
and/or sleep maintenance). In all cases, the recommendations
are “weak,” in that they are based on relatively limited and
low quality evidence. The majority of medications included
in these analyses are FDA-approved drugs for treating insom-
nia. This is not surprising, given that FDA approval rests on
the demonstration of statistically signicant changes in both
subjective and objective outcomes. Furthermore, FDA ap-
proval is based on standards of signicant improvement versus
placebo for one or more indications (i.e. sleep onset or sleep
maintenance insomnia). Many agents, including some which
are not FDA-approved hypnotics, have been shown in one or
more studies to be “statistically signicantly superior” to pla-
cebo for a given outcome(s), but are nonetheless not recom-
mended for treatment of chronic insomnia in this guideline. It
is important to understand the discrepancy between (1) FDA
approval and/or demonstration of “statistically signicant su-
periority” to placebo and (2) the recommendations included
in this publication. The discrepancy results from different cri-
teria employed by the FDA and individual studies, on the one
hand, and the GRADE approach to clinical guidelines, on the
other. The GRADE approach establishes evidence quality rat-
ings and clinical signicance thresholds that are not employed
in individual research studies and FDA assessment for ap-
proval. The thresholds were determined by clinical judgement
of the task force and represent best estimates of the degree of
improvement which the “typical patient” would nd signi-
cant. Although these thresholds are consistent with numerical
values that have been recommended as thresholds in contem-
porary publications, these standards entail a certain amount
of subjectivity on the part of the task force, as there are no
data which suggest absolute standards for clinical signicance.
Without question, there may be divergent opinions regarding
what constitutes clinical signicance and efcacy. Indeed, the
task force assumed that their recommendations are not abso-
lute indications of the presence or absence of clinical utility of
a given medication, but reect their best judgment based on
the available data. Each prescriber bears the responsibility for
making treatment determinations with this in mind.
Patient selection and inclusion criteria for studies are vari-
able and may substantially impact results for a given outcome
(e.g. see Krystal, 2012). Studies not requiring a minimum in-
clusion criterion for a specic outcome (e.g. inclusion thresh-
olds for SL or WASO) may be underpowered to identify
signicant change for that outcome. On the other hand, studies
with stringent PSG criteria for inclusion may not represent the
larger population of insomnia patients.
Understanding the Methodology
The recommendations of the task force were developed with
the use of GRADE, a state-of-the-art methodology for assess-
ment of clinical data. This approach has distinct strengths, as
well as certain limitations. GRADE is a rigorous, detailed, and
transparent system for evaluation of the relative strengths of
evidence for a given intervention. It incorporates several con-
siderations which may impact the quality of evidence for a
treatment approach. These factors include the heterogeneity of
343
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
data (i.e. the degree of inconsistency of results across studies),
imprecision of the data (i.e. 95% CI which cross the clinical
signicance threshold) and potential publication bias (as a re-
sult of industry sponsorship). Quality of evidence grades for
randomized clinical trials begin at HIGH and are downgraded
progressively for heterogeneity, imprecision, and/or potential
publication bias. Since the vast majority of studies in this eld
are industry sponsored, the quality of evidence for nearly all
of these studies is, therefore, reduced from HIGH to MODER-
ATE. This is to be expected for clinical trials for many drugs
(i.e. not only hypnotics), since the vast majority are industry-
sponsored FDA registration studies. The extent to which this
downgrading of evidence is warranted due to actual publica-
tion bias is unknown, but under the GRADE system we have
chosen to adopt the conservative approach and assume risk of
bias. When heterogeneity and imprecision are accounted for,
the quality of evidence for many treatments considered is LOW
or VERY LOW. These latter two factors are not uncommon,
as there is substantial variability in sleep outcome variables
across studies and condence intervals frequently overlap the
clinical thresholds for signicance.
Meta-analysis requires specic data (numerical data for a
given outcome, presented as mean and standard deviation).
Many studies, particularly older investigations, do not report
data in the required format. Some newer publications do not
report data in this format because some sleep variables, par-
ticularly sleep onset latency, are not normally distributed. In
this case, the preferred measure of central tendency is not the
mean but the median, the standard deviation may not be a valid
measure of the degree of dispersion, and the statistical analy-
ses carried out are not based on the mean and standard devia-
tion. The result of this is exclusion of substantial amounts of
data from the formal meta-analyses. While these studies are
discussed in the paper and (secondarily) considered in formu-
lation of recommendations, the inability to include such data in
meta-analysis represents a distinct limitation.
As described in the methodology section, GRADE requires
a recommendation “for” or “against” use of each treatment.
When the evidence for efcacy is clear-cut, with (1) relatively
high quality of evidence; (2) a high degree of condence that
benets clearly outweigh harms; and (3) evidence that the
effects of treatment are of substantial magnitude, without
imposition of signicant burden to the patient, a “strong” rec-
ommendation is delivered in the form of, “we recommend cli-
nicians use X for the treatment of chronic insomnia.” When
evidence for benet is less clear and the quality lower, a
“weak” recommendation is made in the form of, “We suggest
that clinicians use (or not use)…” However, it is important for
clinicians to understand that a recommendation against use,
particularly when associated with low quality evidence, is not
equivalent to a demonstration of ineffectiveness. Rather, it
is often an indication that the available evidence is simply in-
sufcient and fails to provide convincing support in favor of
usage by GRADE standards. In the case of drugs (most com-
monly older drugs) for which none of the data were reported
in a format amenable to meta-analysis, we refrain from mak-
ing any recommendation. The specic indications for use of a
hypnotic employed in this report are limited to “sleep onset”
and “sleep maintenance.” insomnia. We chose these since,
from a practical clinical consideration, these are the primary
complaints with which chronic insomnia patients present, and
for which clinicians prescribe medication. Moreover, these are
the subtypes of insomnia that were actually studied in many
investigations, consistent with FDA approval strategies and the
matching of drugs to particular types of sleep disturbance.
Hence, some medications may show substantial improve-
ment in TST or sleep quality, yet demonstrate no or insig-
nicant reduction in SL, WASO or NOA to qualify for a
recommendation in favor of use.
As described, we established thresholds for clinically sig-
nicant improvement for each objective and subjective major
sleep outcome. Nevertheless, some degree of judgment was in-
troduced in formulating nal recommendations. For example,
a medication may not have exceeded signicance thresholds
for both subjective and objective evidence but, when the to-
tality of evidence (including those investigations which could
not be included in the meta-analysis) was considered, the
task force concluded that a reasonable standard had been met.
These considerations also include the role of adverse effects in
the decisions made.
Beyond the quality of evidence for or against use of a given
drug for sleep onset or maintenance insomnia, the task force
also considered the relative benet:harm ratio and the likeli-
hood that an informed patient would use a specic agent. To a
great extent, these decisions are based on clinical judgement.
With respect to the benet:harm consideration, the data on ad-
verse events is often limited or non-existent. This may reect
the fact that treatment-emergent adverse events (TEAEs) are
typically not collected using specic assessment forms, but
rather, rely on spontaneous reporting by research participants.
In addition, the frequency of some TEAEs is so low that the re-
ported studies are underpowered to nd a difference from pla-
cebo. This also implies that the effect size for a TEAE would
be very small, and hence, it is unlikely that the clinical sig-
nicance of TEAEs has been underestimated. However, some
TEAEs are very infrequent but very serious when they do oc-
cur (e.g. sleep-related behaviors with BzRA). Clinical trials are
likely to underestimate such risks due to the limited number
of patients treated and the limited duration of treatment. As a
result of these considerations, assessment of potential harms is
largely derived from clinical experience and theoretical con-
siderations, rather than well-documented evidence. This is
clearly a limitation of the analysis and further, more systematic
investigation of adverse effects is necessary.
Prior to formulation of the specic recommendations, the
task force—based on its clinical judgement and experience—
indicated what medications well-informed patients would or
would not choose to use. These judgments do not reect the
input of actual patients, but only the task force’s judgment. In
most cases, these judgments were in agreement with recom-
mendations (i.e. an informed patient is likely to use a drug that
is recommended and not likely to use one that is not). In cer-
tain cases (e.g. melatonin), the task force considered that, given
widespread use and apparently benign side effect proles, in-
formed patients may be likely to use a specic drug even when
data do not clearly support a recommendation for use.
344
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
Clinical Application
Administration of sleep-promoting medication for chronic
insomnia is one possible component of what must be a com-
prehensive approach to evaluation and treatment of chronic
insomnia. This approach must include adequate assessment of
cause and characteristics of the disorder as well as evaluation
and treatment of contributing comorbidities. The latter may in-
clude any one or more of numerous medical, neurological and
mental disorders, as well as other primary sleep disorders.
Numerous investigations have demonstrated that hypnotic
medications are comparably efcacious to CBT-I during acute
treatment.
11,112 ,175
However, these studies also make clear that
the gains associated with CBT-I are durable following comple-
tion of treatment, whereas those associated with medication
tend to dissipate following discontinuation of the drug. The
vast majority of investigations which are included in the cur-
rent analysis address relatively short-term use (e.g. one day to
ve weeks). Some studies have shown that long-term treat-
ment with at least newer generation BzRA hypnotics can be
safe and effective under properly controlled conditions. How-
ever, chronic use should be reserved for those individuals for
whom CBT is either inaccessible or ineffective, who have been
appropriately screened for contraindications to such treatment,
who maintain long-term gains with medication, and who are
followed regularly. Patient preference must also be considered
in the determination of treatment approach.
The investigations which are included in this analysis were
focused on “primary” chronic insomnia, with the exception of
some older studies (e.g. zaleplon) which included some patients
with “mild” mental disorders, The extent to which these nd-
ings apply to chronic insomnia associated with major comor-
bidities is uncertain, although a limited number of comparative
studies suggest at least some degree of efcacy in such cases.
It should also be emphasized that the ndings presented in this
report apply only to adults. None of the agents discussed in this
report are approved for use in children and none of the nd-
ings presented apply to children or adolescents. There is very
little information concerning pharmacotherapy for childhood
insomnia. Although independent analyses of efcacy in older
adults were not conducted, examination of the ndings suggests
comparable efcacy across the adult age range. Pharmacoki-
netic and pharmacodynamic properties of many medications,
including benzodiazepine receptor agonist drugs, differ among
older and younger adults, necessitating lower starting dosages.
The limited information from these studies regarding adverse
effects in older adults does not allow meaningful conclusions
about the frequency of such events in older patients compared
to a younger population. The American Geriatric Society Beers
criteria recommend that benzodiazepines be avoided for treat-
ment of insomnia in older patients, due to risk of cognitive
impairment, falls, and motor vehicle accidents. The criteria fur-
ther recommend that newer generation benzodiazepine receptor
agonists be limited to shorter-term use (< 90 days).
The data on adverse effects derived from these clinical tri-
als, in general, do not suggest a high frequency of serious side
effects. However, the data are scant and inconsistent, suggest-
ing that caution should be applied in the assessment of rela-
tive risks associated with use of hypnotic medications. Other
reported adverse effects include—but are not limited to—de-
pendency/withdrawal, cognitive impairment, falls/fractures,
parasomnias, and driving impairment and motor vehicle ac-
cidents. Epidemiological studies have also suggested a pos-
sible link between hypnotic use and infection, depression and
overall mortality risk. These complications are observed most
frequently in older populations, who are among the most fre-
quent users of these drugs. Risks of dependency and serious
withdrawal complications are of greatest concern with true
benzodiazepine agents, particularly in the setting of escalat-
ing, long-term usage and insufcient monitoring. However,
although much concern has understandably been raised about
potential tolerance and addiction to these drugs, there is lim-
ited information regarding the true incidence of these com-
plications. The risks associated with use of these agents are
clearly increased not only in the elderly but also when they
are used in dosages in excess of those recommended, or when
combined with other psychoactive agents.
38
Given the known
sedative effects of these agents, particularly those with longer
half-lives, clinicians must be diligent in cautioning patients re-
garding potential complications related to sedation. Such com-
plications are most likely to occur with longer-acting agents
and during morning hours following bedtime administration.
Use of shorter-acting agents and the lowest effective dosage
may help to reduce sedation-related complications. Appropri-
ate patient counseling and careful monitoring will also serve
to minimize risk. Complete avoidance of these medications
should also be considered in those who may be particularly
susceptible to adverse outcomes.
Future Directions
In an attempt to develop meaningful clinical practice recom-
mendations for the use of sleep-promoting medications, it be-
came increasingly clear to the task force that this endeavor is
fraught with multiple limitations. While existing data (espe-
cially more recent data) provide a reasonable foundation for
certain recommendations contained in this study, the overall
quality of evidence is relatively low in the vast majority of
cases. For numerous drugs, there is simply insufcient evi-
dence available to draw on in determining whether or not a
compound is efcacious. Data reporting, especially that of
older studies, is highly variable and idiosyncratic. As a re-
sult, comparing data from one study to another, or conducting
meta-analyses of data, is not possible. Virtually all studies of
prescription hypnotic agents are industry-funded. While the
reasons for this are understandable, the potential for publica-
tion bias, particularly lack of publication of negative results,
compromises the quality of evidence to a signicant degree.
Moreover, the role of industry in study design and data analysis
may further compromise uniformity of data reporting.
With these limitations in mind, the task force recommends
the following for future investigations:
1. Clear denitions of inclusion and exclusion criteria;
2. Adequately powering studies to detect signicant
differences for key sleep variables;
3. Development and utilization of uniform data collection
instruments which will promote improved cross-study
analysis and comparisons;

345
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
4. Standardized statistical analysis and data presentation.
The majority of newer investigations now present
means + SD for specic PSG or sleep diary data. For
those variables that are not normally distributed, a
transformation can be sought which converts the
probability distribution to the normal distribution and
the transformed mean and SD can then be reported. An
effort to report means and SD data should be made for
all studies;
5. Although specic numerical data for individual sleep
are useful in assessing the efcacy of pharmacological
treatment for insomnia, other approaches to such
evaluation may be more clinically meaningful.
Specically, determination of the efcacy of a drug
in achieving remission of chronic insomnia disorder
has been employed in cognitive behavioral treatments
for insomnia and should be considered as a clinically
relevant outcome in pharmacological trials. This may
include not only subjective and objective outcome data
for major sleep outcomes, but also sleep quality and
daytime functional outcomes;
6. To the extent possible, encourage funding for
independent, non-industry investigation of the efcacy
and effectiveness of hypnotic medications;
7. Data for adverse events associated with hypnotic
medications are not collected and analyzed in standard
ways. This is a widespread problem common to studies
of all types of medications. Continued efforts should
be made to standardize and systematize the reporting
of adverse effects data;
8. Daytime sedation, with concomitant risk of motor
vehicle or occupational accidents, is a signicant
potential risk. Further efforts to include objective
assessments of performance impairments which may
be associated with daytime sedation is encouraged;
9. Virtually no data exists regarding the use of sleep-
promoting agents in children. Yet, such medications
are not infrequently used in this age group. As such,
studies of the efcacy and safety of sleep-promoting
medications in children and adolescents should be
required.
Summary
This analysis is, to the best of our knowledge, the most compre-
hensive assessment of efcacy of individual sleep-promoting
agents published to date. It relies heavily on rigorous evalua-
tion of the quality of evidence for efcacy, based on GRADE,
as well as determination of potential adverse effects, to the
extent possible. It is intended to serve as a useful guide for cli-
nicians in prescribing medications for the treatment of chronic
insomnia. This analysis, however, also makes it abundantly
clear that the availability and quality of the data which serve
as the foundation for such recommendations are sorely lim-
ited. The result is that many commonly used drugs, including
some which carry FDA approval for treatment of insomnia, are
not recommended. Further data are required to formulate any
reasonable conclusion regarding their efcacy or lack thereof.
As a result, clinicians must continue to exercise sound clinical
judgment, based not only on these recommendations, but also
on clinical experience, prior patient response, patient prefer-
ences, and potential adverse effects.
REFERENCES
1. 2005 Adult sleep habits and styles. National Sleep Foundation Web site.
https://sleepfoundation.org/sites/default/les/2005_summary_of_ndings.pdf.
Published 2005. Accessed June 2016.
2. Kassam A, Patten SB. Hypnotic use in a population-based sample of over
thirty-ve thousand interviewed Canadians. Popul Health Metr. 2006;4:15.
3. Kaufmann CN, Spira AP, Alexander GC, Rutkow L, Mojtabai R. Trends
in prescribing of sedative-hypnotic medications in the USA: 1993-2010.
Pharmacoepidemiol Drug Saf. 2016;25(6):637–645.
4. Ohayon MM, Caulet M, Guilleminault C. How a general population
perceives its sleep and how this relates to the complaint of insomnia. Sleep.
1997;20(9):715–723.
5. Chesson A, Jr., Hartse K, Anderson WM, et al. Practice parameters for the
evaluation of chronic insomnia. An American Academy of Sleep Medicine
report. Standards of Practice Committee of the American Academy of Sleep
Medicine. Sleep. 2000;23(2):237–241.
6. Sateia MJ, Doghramji K, Hauri PJ, Morin CM. Evaluation of chronic insomnia.
An American Academy of Sleep Medicine review. Sleep. 2000;23(2):243–308.
7. Schutte-Rodin S, Broch L, Buysse D, Dorsey C, Sateia M. Clinical guideline
for the evaluation and management of chronic insomnia in adults. J Clin Sleep
Med. 2008;4(5):487–504.
8. Chesson AL, Jr., Anderson WM, Littner M, et al. Practice parameters for the
nonpharmacologic treatment of chronic insomnia. An American Academy of
Sleep Medicine report. Standards of Practice Committee of the American
Academy of Sleep Medicine. Sleep. 1999;22(8):1128–1133.
9. Morgenthaler T, Kramer M, Alessi C, et al. Practice parameters for the
psychological and behavioral treatment of insomnia: an update. An American
Academy of Sleep Medicine report. Sleep. 2006;29(11):1415–1419.
10. Morin CM, Bootzin RR, Buysse DJ, Edinger JD, Espie CA, Lichstein KL.
Psychological and behavioral treatment of insomnia: update of the recent
evidence (1998-2004). Sleep. 2006;29(11):1398–1414.
11. Morin CM, Colecchi C, Stone J, Sood R, Brink D. Behavioral and
pharmacological therapies for late-life insomnia: a randomized controlled trial.
JAMA. 1999;281(11):991–999.
12. Meolie AL, Rosen C, Kristo D, et al. Oral nonprescription treatment for
insomnia: an evaluation of products with limited evidence. J Clin Sleep Med.
2005;1(2):173–187.
13. NIH State-of-the-Science Conference Statement on manifestations
and management of chronic insomnia in adults. NIH Consens State Sci
Statements. 2005;22(2):1–30.
14. Wilson SJ, Nutt DJ, Alford C, et al. British Association for
Psychopharmacology consensus statement on evidence-based treatment of
insomnia, parasomnias and circadian rhythm disorders. J Psychopharmacol.
2010;24(11):1577–1601.
15. Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD. Management
of chronic insomnia disorder in adults: a clinical practice guideline from the
American College of Physicians. Ann Intern Med. 2016;165(2):125–133.
16. American Academy of Sleep Medicine. International Classication of Sleep
Disorders. 3rd ed. Darien, IL: American Academy of Sleep Medicine; 2014.
17. Ellis JG, Perlis ML, Neale LF, Espie CA, Bastien CH. The natural history of
insomnia: focus on prevalence and incidence of acute insomnia. J Psychiatr
Res. 2012;46(10):1278–1285.
18. Ohayon MM. Epidemiology of insomnia: what we know and what we still need
to learn. Sleep Med Rev. 2002;6(2):97–111.
19. Ohayon MM. Observation of the natural evolution of insomnia in the american
general population cohort. Sleep Med Clin. 2009;4(1):87–92.
20. DiBonaventura M, Richard L, Kumar M, Forsythe A, Flores NM, Moline M.
The Association between Insomnia and Insomnia Treatment Side Effects on
Health Status, Work Productivity, and Healthcare Resource Use. PLoS One.
2015;10(10):e0137117.
346
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
21. Spira AP, Kaufmann CN, Kasper JD, et al. Association between insomnia
symptoms and functional status in U.S. older adults. J Gerontol B Psychol Sci
Soc Sci. 2014;69 Suppl 1:S35–S41.
22. Leigh JP. Employee and job attributes as predictors of absenteeism in a
national sample of workers: the importance of health and dangerous working
conditions. Soc Sci Med. 1991;33(2):127–137.
23. Hagg SA, Toren K, Lindberg E. Role of sleep disturbances in occupational
accidents among women. Scand J Work Environ Health. 2015;41(4):368–376.
24. Laugsand LE, Strand LB, Vatten LJ, Janszky I, Bjorngaard JH. Insomnia
symptoms and risk for unintentional fatal injuries--the HUNT Study. Sleep.
2014;37(11):1777–1786.
25. Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of
depression: a meta-analytic evaluation of longitudinal epidemiological studies.
J Affect Disord. 2011;135(1-3):10–19.
26. Breslau N, Roth T, Rosenthal L, Andreski P. Sleep disturbance and psychiatric
disorders: a longitudinal epidemiological study of young adults. Biol Psychiatry.
1996;39(6):411– 418.
27. Fernandez-Mendoza J, Vgontzas AN, Liao D, et al. Insomnia with objective
short sleep duration and incident hypertension: the Penn State Cohort.
Hypertension. 2012;60(4):929–935.
28. Bathgate CJ, Edinger JD, Wyatt JK, Krystal AD. Objective but not subjective
short sleep duration associated with increased risk for hypertension in
individuals with insomnia. Sleep. 2016;39(5):1037–1045.
29. Daley M, Morin CM, LeBlanc M, Gregoire JP, Savard J. The economic burden
of insomnia: direct and indirect costs for individuals with insomnia syndrome,
insomnia symptoms, and good sleepers. Sleep. 2009;32(1):55–64.
30. Ozminkowski RJ, Wang S, Walsh JK. The direct and indirect costs of untreated
insomnia in adults in the United States. Sleep. 2007;30(3):263–273.
31. Sivertsen B, Lallukka T, Salo P. The economic burden of insomnia
at the workplace. An opportunity and time for intervention? Sleep.
2011;34(9):1151–1152.
32. Leger D, Guilleminault C, Bader G, Levy E, Paillard M. Medical and socio-
professional impact of insomnia. Sleep. 2002;25(6):625–629.
33. Kleinman NL, Brook RA, Doan JF, Melkonian AK, Baran RW. Health
benet costs and absenteeism due to insomnia from the employer’s
perspective: a retrospective, case-control, database study. J Clin Psychiatry.
2009;70(8):1098–1104.
34. Montgomery P, Dennis J. Cognitive behavioural interventions for
sleep problems in adults aged 60+. Cochrane Database Syst Rev.
2002;(2):CD003161.
35. Trauer JM, Qian MY, Doyle JS, Rajaratnam SM, Cunnington D. Cognitive
Behavioral Therapy for Chronic Insomnia: A Systematic Review and Meta-
analysis. Ann Intern Med. 2015;163(3):191–204.
36. Wu JQ, Appleman ER, Salazar RD, Ong JC. Cognitive behavioral therapy for
insomnia comorbid with psychiatric and medical conditions: a meta-analysis.
JAMA Intern Med. 2015;175(9):1461–1472.
37. Zachariae R, Lyby MS, Ritterband LM, O’Toole MS. Efcacy of internet-
delivered cognitive-behavioral therapy for insomnia - a systematic review and
meta-analysis of randomized controlled trials. Sleep Med Rev. 2016;30:1–10.
38. Bertisch SM, Herzig SJ, Winkelman JW, Buettner C. National use of
prescription medications for insomnia: NHANES 1999-2010. Sleep.
2014;37(2):343–349.
39. Balter MB, Uhlenhuth EH. The benecial and adverse effects of hypnotics.
J Clin Psychiatry. 1991;52 Suppl:16–23.
40. Roehrs T, Roth T. ‘Hypnotic’ prescription patterns in a large managed-care
population. Sleep Med. 2004;5(5):463–466.
41. 2005 Adult Sleep Habits and Styles. National Sleep Foundation Web site.
https://sleepfoundation.org/sleep-polls-data/sleep-in-america-poll/2005-adult-
sleep-habits-and-styles. Published 2005. Accessed March 2016.
42. Cheung JM, Atternas K, Melchior M, Marshall NS, Fois RA, Saini B. Primary
health care practitioner perspectives on the management of insomnia: a pilot
study. Aust J Prim Health. 2014;20(1):103–112.
43. Pawaskar MD, Joish VN, Camacho FT, Rasu RS, Balkrishnan R. The inuence
of co-morbidities on prescribing pharmacotherapy for insomnia: evidence from
US national outpatient data 1995-2004. J Med Econ. 2008;11(1):41–56.
44. Siriwardena AN, Apekey T, Tilling M, Dyas JV, Middleton H, Orner R. General
practitioners’ preferences for managing insomnia and opportunities for
reducing hypnotic prescribing. J Eval Clin Pract. 2010;16(4):731–737.
45. Nowell PD, Mazumdar S, Buysse DJ, Dew MA, Reynolds CF, 3rd, Kupfer
DJ. Benzodiazepines and zolpidem for chronic insomnia: a meta-analysis of
treatment efcacy. JAMA. 1997;278(24):2170–2177.
46. Holbrook AM, Crowther R, Lotter A, Cheng C, King D. Meta-
analysis of benzodiazepine use in the treatment of insomnia. CMAJ.
2000;162(2):225–233.
47. Dundar Y, Dodd S, Strobl J, Boland A, Dickson R, Walley T. Comparative
efcacy of newer hypnotic drugs for the short-term management of
insomnia: a systematic review and meta-analysis. Hum Psychopharmacol.
2004;19(5):305–322.
48. Glass J, Lanctot KL, Herrmann N, Sproule BA, Busto UE. Sedative hypnotics
in older people with insomnia: meta-analysis of risks and benets. BMJ.
2005;331(7526):1169.
49. Buscemi N, Vandermeer B, Friesen C, et al. The efcacy and safety of drug
treatments for chronic insomnia in adults: a meta-analysis of RCTs. J Gen
Intern Med. 2007;22(9):1335–1350.
50. Huedo-Medina TB, Kirsch I, Middlemass J, Klonizakis M, Siriwardena AN.
Effectiveness of non-benzodiazepine hypnotics in treatment of adult insomnia:
meta-analysis of data submitted to the Food and Drug Administration. BMJ.
2012;345:e8343.
51. Winkler A, Auer C, Doering BK, Rief W. Drug treatment of primary insomnia: a
meta-analysis of polysomnographic randomized controlled trials. CNS Drugs.
2014;28(9):799–816.
52. Wilt TJ, MacDonald R, Brasure M, et al. Pharmacologic treatment of insomnia
disorder: an evidence report for a clinical practice guideline by the American
College of Physicians. Ann Intern Med. 2016;165(2):103–112.
53. Morgenthaler TI, Deriy L, Heald JL, Thomas SM. The evolution of the
AASM clinical practice guidelines: another step forward. J Clin Sleep Med.
2016;12(1):129–135.
54. Herring WJ, Connor KM, Ivgy-May N, et al. Suvorexant in patients with
insomnia: results from two 3-month randomized controlled clinical trials. Biol
Psychiatry. 2016;79(2):136–148.
55. Herring WJ, Snyder E, Budd K, et al. Orexin receptor antagonism for
treatment of insomnia: a randomized clinical trial of suvorexant. Neurology.
2012;79(23):2265–2274.
56. Ancoli-Israel S, Krystal AD, McCall WV, et al. A 12-week, randomized, double-
blind, placebo-controlled study evaluating the effect of eszopiclone 2 mg on
sleep/wake function in older adults with primary and comorbid insomnia. Sleep.
2010;33(2):225–234.
57. Erman MK, Zammit G, Rubens R, et al. A polysomnographic placebo-
controlled evaluation of the efcacy and safety of eszopiclone relative to
placebo and zolpidem in the treatment of primary insomnia. J Clin Sleep Med.
2008;4(3):229–234.
58. McCall WV, Erman M, Krystal AD, et al. A polysomnography study
of eszopiclone in elderly patients with insomnia. Curr Med Res Opin.
2006;22(9):1633–1642.
59. Scharf M, Erman M, Rosenberg R, et al. A 2-week efcacy and safety
study of eszopiclone in elderly patients with primary insomnia. Sleep.
2005;28(6):720–727.
60. Uchimura N, Kamijo A, Kuwahara H, et al. A randomized placebo-controlled
polysomnographic study of eszopiclone in Japanese patients with primary
insomnia. Sleep Med. 2012;13(10):1247–1253.
61. Zammit GK, McNabb LJ, Caron J, Amato DA, Roth T. Efcacy and safety of
eszopiclone across 6-weeks of treatment for primary insomnia. Curr Med Res
Opin. 2004;20(12):1979–1991.
62. Boyle J, Trick L, Johnsen S, Roach J, Rubens R. Next-day cognition,
psychomotor function, and driving-related skills following nighttime
administration of eszopiclone. Hum Psychopharmacol. 2008;23(5):385–397.
63. Krystal AD, Walsh JK, Laska E, et al. Sustained efcacy of eszopiclone over 6
months of nightly treatment: results of a randomized, double-blind, placebo-
controlled study in adults with chronic insomnia. Sleep. 2003;26(7):793–799.
64. Walsh JK, Krystal AD, Amato DA, et al. Nightly treatment of primary insomnia
with eszopiclone for six months: effect on sleep, quality of life, and work
limitations. Sleep. 2007;30(8):959–968.
347
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
65. Soares CN, Joffe H, Rubens R, Caron J, Roth T, Cohen L. Eszopiclone in
patients with insomnia during perimenopause and early postmenopause: a
randomized controlled trial. Obstet Gynecol. 2006;108(6):1402–1410.
66. Joffe H, Petrillo L, Viguera A, et al. Eszopiclone improves insomnia and
depressive and anxious symptoms in perimenopausal and postmenopausal
women with hot ashes: a randomized, double-blinded, placebo-controlled
crossover trial. Am J Obstet Gynecol. 2010;202(2):171.e1-e171.e111.
67. Hedner J, Yaeche R, Emilien G, Farr I, Salinas E. Zaleplon shortens subjective
sleep latency and improves subjective sleep quality in elderly patients with
insomnia. The Zaleplon Clinical Investigator Study Group. Int J Geriatr
Psychiatry. 2000;15(8):704–712.
68. Walsh JK, Vogel GW, Scharf M, et al. A ve week, polysomnographic
assessment of zaleplon 10 mg for the treatment of primary insomnia. Sleep
Med. 2000;1(1):41–49.
69. Ancoli-Israel S, Walsh JK, Mangano RM, Fujimori M. Zaleplon, A Novel
Nonbenzodiazepine Hypnotic, Effectively Treats Insomnia in Elderly Patients
Without Causing Rebound Effects. Prim Care Companion J Clin Psychiatry.
1999;1(4):114–120.
70. Elie R, Ruther E, Farr I, Emilien G, Salinas E. Sleep latency is shortened
during 4 weeks of treatment with zaleplon, a novel nonbenzodiazepine
hypnotic. Zaleplon Clinical Study Group. J Clin Psychiatry.
1999;60(8):536–544.
71. Fry J, Scharf M, Mangano R, Fujimori M. Zaleplon improves sleep without
producing rebound effects in outpatients with insomnia. Zaleplon Clinical
Study Group. Int Clin Psychopharmacol. 2000;15(3):141–152.
72. Dorsey CM, Lee KA, Scharf MB. Effect of zolpidem on sleep in
women with perimenopausal and postmenopausal insomnia: a 4-week,
randomized, multicenter, double-blind, placebo-controlled study. Clin Ther.
2004;26(10):1578–1586.
73. Herrmann WM, Kubicki ST, Boden S, Eich FX, Attali P, Coquelin JP. Pilot
controlled double-blind study of the hypnotic effects of zolpidem in patients
with chronic ‘learned’ insomnia: psychometric and polysomnographic
evaluation. J Int Med Res. 1993;21(6):306–322.
74. Jacobs GD, Pace-Schott EF, Stickgold R, Otto MW. Cognitive behavior
therapy and pharmacotherapy for insomnia: a randomized controlled trial and
direct comparison. Arch Intern Med. 2004;164(17):1888–1896.
75. Perlis ML, McCall WV, Krystal AD, Walsh JK. Long-term, non-nightly
administration of zolpidem in the treatment of patients with primary insomnia.
J Clin Psychiatry. 2004;65(8):1128–1137.
76. Randall S, Roehrs TA, Roth T. Efcacy of eight months of nightly zolpidem: a
prospective placebo-controlled study. Sleep. 2012;35(11):1551–1557.
77. Ware JC, Walsh JK, Scharf MB, Roehrs T, Roth T, Vogel GW. Minimal
rebound insomnia after treatment with 10-mg zolpidem. Clin Neuropharmacol.
1997;20(2):116–125.
78. Walsh JK, Erman M, Erwin CW, et al. Subjective hypnotic efcacy
of trazodone and zolpidem in DSMIII-R primary insomnia. Hum
Psychopharmacol. 1998;13(3)191–198.
79. Staner L, Ertle S, Boeijinga P, et al. Next-day residual effects of hypnotics
in DSM-IV primary insomnia: a driving simulator study with simultaneous
electroencephalogram monitoring. Psychopharmacology (Berl).
2005;181(4):790–798.
80. Walsh JK, Soubrane C, Roth T. Efcacy and safety of zolpidem extended
release in elderly primary insomnia patients. Am J Geriatr Psychiatry.
20 08;16(1):4 4 – 57.
81. Roth T, Soubrane C, Titeux L, Walsh JK. Efcacy and safety of zolpidem-MR:
a double-blind, placebo-controlled study in adults with primary insomnia.
Sleep Med. 2006;7(5):397–406.
82. Scharf MB, Roth T, Vogel GW, Walsh JK. A multicenter, placebo-controlled
study evaluating zolpidem in the treatment of chronic insomnia. J Clin
Psychiatry. 1994;55(5):192–199.
83. Allain H, Arbus L, Schück S, Group ZS. Efcacy and safety of zolpidem
administered ‘as needed’ in primary insomnia: results of a double-blind,
placebo-controlled study. Clin Drug Investig. 2001;21(6):391–400.
84. Cluydts R, Peeters K, de Bouyalsky I, Lavoisy J. Comparison of continuous
versus intermittent administration of zolpidem in chronic insomniacs: a double-
blind, randomized pilot study. J Int Med Res. 1998;26(1):13–24.
85. Hajak G, Cluydts R, Declerck A, et al. Continuous versus non-nightly use
of zolpidem in chronic insomnia: results of a large-scale, double-blind,
randomized, outpatient study. Int Clin Psychopharmacol. 2002;17(1):9 –17.
86. Krystal AD, Erman M, Zammit GK, Soubrane C, Roth T. Long-term efcacy
and safety of zolpidem extended-release 12.5 mg, administered 3 to 7 nights
per week for 24 weeks, in patients with chronic primary insomnia: a 6-month,
randomized, double-blind, placebo-controlled, parallel-group, multicenter
study. Sleep. 2008;31(1):79–90.
87. Maroo N, Hazra A, Das T. Efcacy and safety of a polyherbal sedative-
hypnotic formulation NSF-3 in primary insomnia in comparison to zolpidem: a
randomized controlled trial. Indian J Pharmacol. 2013;45(1):34–39.
88. Roth T, Hull SG, Lankford DA, Rosenberg R, Scharf MB. Low-dose sublingual
zolpidem tartrate is associated with dose-related improvement in sleep
onset and duration in insomnia characterized by middle-of-the-night (MOTN)
awakenings. Sleep. 2008;31(9):1277–1284.
89. Roth T, Krystal A, Steinberg FJ, Singh NN, Moline M. Novel sublingual low-
dose zolpidem tablet reduces latency to sleep onset following spontaneous
middle-of-the-night awakening in insomnia in a randomized, double-blind,
placebo-controlled, outpatient study. Sleep. 2013;36(2):189–196.
90. Staner C, Joly F, Jacquot N, et al. Sublingual zolpidem in early onset of sleep
compared to oral zolpidem: polysomnographic study in patients with primary
insomnia. Curr Med Res Opin. 2010;26(6):1423–1431.
91. Tu JH, Chung WC, Yang CY, Tzeng DS. A comparison between acupuncture
versus zolpidem in the treatment of primary insomnia. Asian J Psychiatr.
2012;5(3):231–235.
92. Voshaar RC, van Balkom AJ, Zitman FG. Zolpidem is not superior to
temazepam with respect to rebound insomnia: a controlled study. Eur
Neuropsychopharmacol. 2004;14(4):301–306.
93. Walsh JK. Zolpidem “as needed” for the treatment of primary insomnia: a
double-blind, placebo-controlled study. Sleep Med Rev. 2002;6 Suppl 1:S7–
S10; discussion S10–S11, S31–S33.
94. Walsh JK, Roth T, Randazzo A, et al. Eight weeks of non-nightly use of
zolpidem for primary insomnia. Sleep. 2000;23(8):1087–1096.
95. Zammit GK, Corser B, Doghramji K, et al. Sleep and residual sedation after
administration of zaleplon, zolpidem, and placebo during experimental middle-
of-the-night awakening. J Clin Sleep Med. 2006;2(4):417–423.
96. Roehrs T, Bonahoom A, Pedrosi B, Rosenthal L, Roth T. Treatment
regimen and hypnotic self-administration. Psychopharmacology (Berl).
2001;155(1):11–17.
97. Elie R, Frenay M, Le Morvan P, Bourgouin J. Efcacy and safety of
zopiclone and triazolam in the treatment of geriatric insomniacs. Int Clin
Psychopharmacol. 1990;5 Suppl 2:39–46.
98. Reeves RL. Comparison of triazolam, urazepam, and placebo as hypnotics in
geriatric patients with insomnia. J Clin Pharmacol. 1977;17(5-6):319–323.
99. Autret E, Maillard F, Autret A. Comparison of the clinical hypnotic effects of
zopiclone and triazolam. Eur J Clin Pharmacol. 1987;31(5):621–623.
100. Bowen AJ. Comparative efcacy of triazolam, urazepam and placebo in out-
patients insomniacs. J Int Med Res. 1978;6(4):337–342.
101. Fabre LF, Jr., Gross L, Pasigajen V, Metzler C. Multiclinic double-blind
comparison of triazolam and urazepam for seven nights in outpatients with
insomnia. J Clin Pharmacol. 1977;17(7):402–409.
102. Fleming JA, McClure DJ, Mayes C, Phillips R, Bourgouin J. A comparison of
the efcacy, safety and withdrawal effects of zopiclone and triazolam in the
treatment of insomnia. Int Clin Psychopharmacol. 1990;5 Suppl 2:29–37.
103. Greenblatt DJ, Harmatz JS, Zinny MA, Shader RI. Effect of gradual withdrawal
on the rebound sleep disorder after discontinuation of triazolam. N Engl J Med.
1987;317(12):722–728.
104. Hajak G, Clarenbach P, Fischer W, Haase W, Ruther E. Zopiclone improves
sleep quality and daytime well-being in insomniac patients: comparison
with triazolam, unitrazepam and placebo. Int Clin Psychopharmacol.
1994;9(4):251–261.
105. Leibowitz M, Sunshine A. Long-term hypnotic efcacy and safety of triazolam
and urazepam. J Clin Pharmacol. 1978;18(5-6):302–309.
106. Monti JM, Attali P, Monti D, Zipfel A, de la Giclais B, Morselli PL. Zolpidem
and rebound insomnia--a double-blind, controlled polysomnographic study in
chronic insomniac patients. Pharmacopsychiatry. 1994;27(4):166–175.
348
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
107. Rickels K, Gingrich RL, Jr., Morris RJ, et al. Triazolam in insomniac family
practice patients. Clin Pharmacol Ther. 1975;18(3):315–324.
108. Scharf MB. Feasibility of an every-other-night regimen in insomniac patients:
subjective hypnotic effectiveness of quazepam, triazolam, and placebo. J Clin
Psychiatry. 1993;54(1):33–38.
109. Sunshine A. Comparison of the hypnotic activity of triazolam, urazepam
hydrochloride, and placebo. Clin Pharmacol Ther. 1975;17(5):573–577.
110. Glass JR, Sproule BA, Herrmann N, Busto UE. Effects of 2-week treatment
with temazepam and diphenhydramine in elderly insomniacs: a randomized,
placebo-controlled trial. J Clin Psychopharmacol. 2008;28(2):182–188.
111. Hindmarch I. Effects of hypnotic and sleep-inducing drugs on objective
assessments of human psychomotor performance and subjective appraisals of
sleep and early morning behaviour. Br J Clin Pharmacol. 1979;8(1):43S–46S.
112. Wu R, Bao J, Zhang C, Deng J, Long C. Comparison of sleep condition
and sleep-related psychological activity after cognitive-behavior and
pharmacological therapy for chronic insomnia. Psychother Psychosom.
2006;75(4):220–228.
113. Cuanang JR, Limos L. Treatment of insomnia with temazepam: double-blind,
placebo-controlled evaluation. Clin Ther. 1982;4(5):402–412.
114. Fillingim JM. Double-blind evaluation of the efcacy and safety of temazepam
in outpatients with insomnia. Br J Clin Pharmacol. 1979;8(1):73S–77S.
115. Heffron WA, Roth P. Double-blind evaluation of the safety and hypnotic
efcacy of temazepam in insomniac outpatients. Br J Clin Pharmacol.
1979;8(1):69S–72S.
116. Tuk B, Oberye JJ, Pieters MS, et al. Pharmacodynamics of temazepam
in primary insomnia: assessment of the value of quantitative
electroencephalography and saccadic eye movements in predicting
improvement of sleep. Clin Pharmacol Ther. 1997;62(4):444–452.
117. Wilson SJ, Rich AS, Rich NC, Potokar J, Nutt DJ. Evaluation of actigraphy and
automated telephoned questionnaires to assess hypnotic effects in insomnia.
Int Clin Psychopharmacol. 2004;19(2):77–84.
118. Kohsaka M, Kanemura T, Taniguchi M, et al. Efcacy and tolerability
of ramelteon in a double-blind, placebo-controlled, crossover study in
Japanese patients with chronic primary insomnia. Expert Rev Neurother.
2011;11(10):1389 –1397.
119. Mayer G, Wang-Weigand S, Roth-Schechter B, Lehmann R, Staner C,
Partinen M. Efcacy and safety of 6-month nightly ramelteon administration in
adults with chronic primary insomnia. Sleep. 2009;32(3):351–360.
120. Roth T, Seiden D, Wang-Weigand S, Zhang J. A 2-night, 3-period, crossover
study of ramelteon’s efcacy and safety in older adults with chronic insomnia.
Curr Med Res Opin. 2007;23(5):1005–1014.
121. Zammit G, Erman M, Wang-Weigand S, Sainati S, Zhang J, Roth T. Evaluation
of the efcacy and safety of ramelteon in subjects with chronic insomnia.
J Clin Sleep Med. 2007;3(5):495–504.
122. Erman M, Seiden D, Zammit G, Sainati S, Zhang J. An efcacy, safety, and
dose-response study of Ramelteon in patients with chronic primary insomnia.
Sleep Med. 2006;7(1):17–24.
123. Mini L, Wang-Weigand S, Zhang J. Ramelteon 8 mg/d versus placebo in
patients with chronic insomnia: post hoc analysis of a 5-week trial using 50%
or greater reduction in latency to persistent sleep as a measure of treatment
effect. Clin Ther. 2008;30(7):1316–1323.
124. Mini LJ, Wang-Weigand S, Zhang J. Self-reported efcacy and tolerability of
ramelteon 8 mg in older adults experiencing severe sleep-onset difculty. Am
J Geriatr Pharmacother. 2007;5(3):177–184.
125. Roth T, Seiden D, Sainati S, Wang-Weigand S, Zhang J, Zee P. Effects of
ramelteon on patient-reported sleep latency in older adults with chronic
insomnia. Sleep Med. 2006;7(4):312–318.
126. Wang-Weigand S, Watissee M, Roth T. Use of a post-sleep questionnaire-
interactive voice response system (PSQ-IVRS) to evaluate the subjective
sleep effects of ramelteon in adults with chronic insomnia. Sleep Med.
2011;12(9):920–923.
127. Krystal AD, Durrence HH, Scharf M, et al. Efcacy and Safety of Doxepin 1
mg and 3 mg in a 12-week Sleep Laboratory and Outpatient Trial of Elderly
Subjects with Chronic Primary Insomnia. Sleep. 2010;33(11):1553–1561.
128. Krystal AD, Lankford A, Durrence HH, et al. Efcacy and safety of doxepin
3 and 6 mg in a 35-day sleep laboratory trial in adults with chronic primary
insomnia. Sleep. 2011;34(10):1433–1442.
129. Roth T, Rogowski R, Hull S, et al. Efcacy and safety of doxepin 1 mg, 3 mg,
and 6 mg in adults with primary insomnia. Sleep. 2007;30(11):1555–1561.
130. Scharf M, Rogowski R, Hull S, et al. Efcacy and safety of doxepin 1 mg,
3 mg, and 6 mg in elderly patients with primary insomnia: a randomized,
double-blind, placebo-controlled crossover study. J Clin Psychiatry.
2008;69(10):1557–1564.
131. Lankford A, Rogowski R, Essink B, Ludington E, Heith Durrence H, Roth T.
Efcacy and safety of doxepin 6 mg in a four-week outpatient trial of elderly
adults with chronic primary insomnia. Sleep Med. 2012;13(2):133–138.
132. Hajak G, Rodenbeck A, Voderholzer U, et al. Doxepin in the treatment of
primary insomnia: a placebo-controlled, double-blind, polysomnographic study.
J Clin Psychiatry. 2001;62(6):453–463.
133. Roth T, Wright KP, Jr., Walsh J. Effect of tiagabine on sleep in elderly subjects
with primary insomnia: a randomized, double-blind, placebo-controlled study.
Sleep. 2006;29(3):335–341.
134. Walsh JK, Perlis M, Rosenthal M, Krystal A, Jiang J, Roth T. Tiagabine
increases slow-wave sleep in a dose-dependent fashion without affecting
traditional efcacy measures in adults with primary insomnia. J Clin Sleep
Med. 2006;2(1):35 – 41.
135. Walsh JK, Zammit G, Schweitzer PK, Ondrasik J, Roth T. Tiagabine enhances
slow wave sleep and sleep maintenance in primary insomnia. Sleep Med.
2006;7(2):155–161.
136. Morin CM, Koetter U, Bastien C, Ware JC, Wooten V. Valerian-hops
combination and diphenhydramine for treating insomnia: a randomized
placebo-controlled clinical trial. Sleep. 2005;28(11):1465–1471.
137. Rickels K, Morris RJ, Newman H, Rosenfeld H, Schiller H, Weinstock R.
Diphenhydramine in insomniac family practice patients: a double-blind study.
J Clin Pharmacol. 1983;23(5-6):234–242.
138. Lemoine P, Nir T, Laudon M, Zisapel N. Prolonged-release melatonin improves
sleep quality and morning alertness in insomnia patients aged 55 years and
older and has no withdrawal effects. J Sleep Res. 2007;16(4):372–380.
139. Luthringer R, Muzet M, Zisapel N, Staner L. The effect of prolonged-release
melatonin on sleep measures and psychomotor performance in elderly
patients with insomnia. Int Clin Psychopharmacol. 2009;24(5):239–249.
140. Wade AG, Ford I, Crawford G, et al. Efcacy of prolonged release melatonin in
insomnia patients aged 55-80 years: quality of sleep and next-day alertness
outcomes. Curr Med Res Opin. 2007;23(10):2597–2605.
141. Baskett JJ, Broad JB, Wood PC, et al. Does melatonin improve sleep in older
people? A randomised crossover trial. Age Ageing. 2003;32(2):164–170.
142. Garzon C, Guerrero JM, Aramburu O, Guzman T. Effect of melatonin
administration on sleep, behavioral disorders and hypnotic drug
discontinuation in the elderly: a randomized, double-blind, placebo-controlled
study. Aging Clin Exp Res. 2009;21(1):38– 42.
143. Haimov I, Lavie P, Laudon M, Herer P, Vigder C, Zisapel N. Melatonin
replacement therapy of elderly insomniacs. Sleep. 1995;18(7):598–603.
144. Rondanelli M, Opizzi A, Monteferrario F, Antoniello N, Manni R, Klersy C. The
effect of melatonin, magnesium, and zinc on primary insomnia in long-term
care facility residents in Italy: a double-blind, placebo-controlled clinical trial.
J Am Geriatr Soc. 2011;59(1):82–90.
145. Wade AG, Crawford G, Ford I, et al. Prolonged release melatonin in the
treatment of primary insomnia: evaluation of the age cut-off for short- and
long-term response. Curr Med Res Opin. 2011;27(1):87–98.
146. Wade AG, Ford I, Crawford G, et al. Nightly treatment of primary insomnia with
prolonged release melatonin for 6 months: a randomized placebo controlled
trial on age and endogenous melatonin as predictors of efcacy and safety.
BMC Med. 2010;8:51.
147. Zhdanova IV, Wurtman RJ, Regan MM, Taylor JA, Shi JP, Leclair OU.
Melatonin treatment for age-related insomnia. J Clin Endocrinol Metab.
2001;86(10):4727–4730.
148. Hudson C, Hudson SP, Hecht T, MacKenzie J. Protein source tryptophan
versus pharmaceutical grade tryptophan as an efcacious treatment for
chronic insomnia. Nutr Neurosci. 2005;8(2):121–127.
149. Hartmann E, Lindsley JG, Spinweber C. Chronic insomnia: effects of
tryptophan, urazepam, secobarbital, and placebo. Psychopharmacology
(Berl). 1983;80(2):138–142.

349
Journal of Clinical Sleep Medicine, Vol. 13, No. 2, 2017
MJ Sateia, DJ Buysse, AD Krystal, et al. Clinical Practice Guideline: Insomnia
150. Spinweber CL. L-tryptophan administered to chronic sleep-onset insomniacs:
late-appearing reduction of sleep latency. Psychopharmacology (Berl).
1986;90(2):151–155.
151. Oxman AD, Flottorp S, Havelsrud K, et al. A televised, web-based randomised
trial of an herbal remedy (valerian) for insomnia. PLoS One. 2007;2(10):e1040.
152. Cohn JB, Wilcox CS, Bremner J, Ettinger M. Hypnotic efcacy of estazolam
compared with urazepam in outpatients with insomnia. J Clin Pharmacol.
1991;31(8):747–750.
153. Dominguez RA, Goldstein BJ, Jacobson AF, Steinbook RM. Comparative
efcacy of estazolam, urazepam, and placebo in outpatients with insomnia.
J Clin Psychiatry. 1986;47(7):362–365.
154. Scharf MB, Roth PB, Dominguez RA, Ware JC. Estazolam and urazepam: a
multicenter, placebo-controlled comparative study in outpatients with insomnia.
J Clin Pharmacol. 1990;30(5):461–467.
155. Aden GC, Thatcher C. Quazepam in the short-term treatment of insomnia in
outpatients. J Clin Psychiatry. 1983;44(12):454–456.
156. Hernandez Lara R, Del Rosal PL, Ponce MC. Short-term study of quazepam
15 milligrams in the treatment of insomnia. J Int Med Res. 1983;11(3):162–166.
157. Martinez HT, Serna CT. Short-term treatment with quazepam of insomnia in
geriatric patients. Clin Ther. 1982;5(2):174–178.
158. Mendels J, Stern S. Evaluation of the short-term treatment of insomnia in out-
patients with 15 milligrams of quazepam. J Int Med Res. 1983;11(3):155–161.
159. O’Hair DE, Winsauer HJ. Evaluation of short-term treatment with 30 mg of
quazepam in insomniac outpatients. Clin Ther. 1981;4(4):291–301.
160. Roth TG, Roehrs TA, Koshorek GL, Greenblatt DJ, Rosenthal LD.
Hypnotic effects of low doses of quazepam in older insomniacs. J Clin
Psychopharmacol. 1997;17(5):401–406.
161. Elie R, Caille G, Levasseur FA, Gareau J. Comparative hypnotic activity
of single doses of loprazolam, urazepam, and placebo. J Clin Pharmacol.
1983;23(1):32–36.
162. Elie R, Lavoie G, Bourgouin J, Le Morvan P. Zopiclone versus urazepam in
insomnia: prolonged administration and withdrawal. Int Clin Psychopharmacol.
1990;5(4):279–286.
163. Kripke DF, Hauri P, Ancoli-Israel S, Roth T. Sleep evaluation in chronic
insomniacs during 14-day use of urazepam and midazolam. J Clin
Psychopharmacol. 1990;10(4 Suppl):32S–43S.
164. Mamelak M, Buck L, Csima A, Price V, Smiley A. Effects of urazepam
and zopiclone on the performance of chronic insomniac patients: a study of
ethanol-drug interaction. Sleep. 1987;10 Suppl 1:79–87.
165. Mamelak M, Csima A, Buck L, Price V. A comparative study on the effects
of brotizolam and urazepam on sleep and performance in the elderly. J Clin
Psychopharmacol. 1989;9(4):260–267.
166. Melo de Paula AJ. Comparative study of lormetazepam and urazepam in the
treatment of insomnia. Clin Ther. 1984;6(4):500–508.
167. Salkind MR, Silverstone T. A clinical and psychometric evaluation of
urazepam. Br J Clin Pharmacol. 1975;2(3):223–226.
168. Gotestam KG, Oppoyen F, Berntzen D. Treatment of insomnia with two
benzodiazepines: a double-blind crossover study. Eur J Clin Pharmacol.
1991;41(2):137–140.
169. Tassniyom K, Paholpak S, Tassniyom S, Kiewyoo J. Quetiapine for primary
insomnia: a double blind, randomized controlled trial. J Med Assoc Thai.
2010;93(6):729–734.
170. Lo HS, Yang CM, Lo HG, Lee CY, Ting H, Tzang BS. Treatment effects of
gabapentin for primary insomnia. Clin Neuropharmacol. 2010;33(2):84–90.
171. Nowell PD, Reynolds CF, 3rd, Buysse DJ, Dew MA, Kupfer DJ.
Paroxetine in the treatment of primary insomnia: preliminary clinical and
electroencephalogram sleep data. J Clin Psychiatry. 1999;60(2):89–95.
172. Reynolds CF, 3rd, Buysse DJ, Miller MD, Pollock BG, Hall M, Mazumdar
S. Paroxetine treatment of primary insomnia in older adults. Am J Geriatr
Psychiatry. 2006;14(9):803–807.
173. Hohagen F, Montero RF, Weiss E, et al. Treatment of primary insomnia with
trimipramine: an alternative to benzodiazepine hypnotics? Eur Arch Psychiatry
Clin Neurosci. 1994;244(2):65–72.
174. Riemann D, Voderholzer U, Cohrs S, et al. Trimipramine in primary
insomnia: results of a polysomnographic double-blind controlled study.
Pharmacopsychiatry. 2002;35(5):165–174.
175. Smith MT, Perlis ML, Park A, et al. Comparative meta-analysis of
pharmacotherapy and behavior therapy for persistent insomnia. Am J
Psychiatry. 2002;159(1):5–11.
ACKNOWLEDGMENTS
The task force thanks and acknowledges the contributions of Karl Doghramji, MD,
who served as a critical reviewer of this guideline.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication September, 2016
Submitted in nal revised form September, 2016
Accepted for publication September, 2016
Address correspondence to: Michael J. Sateia, MD, Geisel School of Medicine at
Dartmouth, Hanover, NH 03755; Tel: (603) 650-7534; Fax: (603) 650-7820; Email:
research@aasmnet.org
DISCLOSURE STATEMENT
The development of this clinical practice guideline was funded by the American
Academy of Sleep Medicine. Dr. Neubauer is a member of the Board of Directors for
the National Sleep Foundation; and he has been a consultant for Purdue Pharama.
Dr. Krystal serves on a scientic advisory board for Merck, and therefore did not
participate in the development of the suvorexant recommendation; he has received
research support from the NIH, TEVA and Sunovion; and he has been a consultant
for Flamel, Atentiv, Ostuka, Neurocrine, Lundbeck, Pernix, Janssen, Jazz and
Merck. Dr. Buysse has been a consultant for Cereve, Inc, Emmi Solutions, Philips
Respironics, BeHealth; he has received research support from the NIH; and he owns
intellectual property rights in the Pittsburgh Sleep Quality Index (PSQI). Mr. Heald
is employed by the American Academy of Sleep Medicine. The other authors have
indicated no nancial conicts of interest.
Literature Search Terms:
((insomnia OR "Sleep Initiation and Maintenance Disorders"[Mesh]) AND ((clinical trial) OR (randomized controlled trial))
NOT "Editorial"[Publication Type] NOT "Letter"[Publication Type] NOT "Comment"[Publication Type] NOT "Case
Reports"[Publication Type] NOT "Biography"[Publication Type] NOT "Review"[Publication Type] NOT (transient[TI])) NOT
(animals[mh] NOT humans[mh])
Suvorexant - Summary of Findings Tables
Table S1 – Summary of Findings table for suvorexant 10 mg for the treatment of chronic insomnia
References: Herring 2012(A)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
10 mg Suvorexant vs Placebo
No of Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊝⊝
low
1,2
The mean sleep latency in the suvorexant group was
2.3 minutes lower
(13.68 lower to 9.08 higher)
175
(1 study)
A
Wake After Sleep Onset*
(PSG)
⊕⊕⊝⊝
low
2,3
The mean wake after sleep onset in the suvorexant group was
21.5 minutes lower
(36.34 to 6.66 lower)
175
(1 study)
A
Sleep Efficiency
(PSG)
⊕⊕⊝⊝
low
2,4
The mean sleep efficiency in the suvorexant group was
4.7 percent higher
(0.97 to 8.43 higher)
175
(1 study)
A
* Critical Outcome, used to determine Quality of Evidence
1
95% CI (-13.68 to 9.08) crosses the Clinical Significance Threshold (10 min)
2
Study funded by industry
3
95% CI (-36.34 to -6.66) crosses the Clinical Significance Threshold (20 min)
4
95% CI (0.97 to 8.43) crosses the Clinical Significance Threshold (5%)
Table S2 – Summary of Findings table for suvorexant 15/20 mg for the treatment of chronic insomnia
References: Herring 2016(A)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
15/20 mg Suvorexant vs Placebo
No of Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊝⊝
low
1,2
The mean sleep latency in the suvorexant group was
8.1 minutes lower
(13.85 to 2.35 lower)
423
(1 study)
A
Sleep Latency
(Subjective)
⊕⊕⊕⊝
moderate
2
The mean sleep latency in the suvorexant group was
5.2 minutes lower
(10.1 to 0.3 lower)
567
(1 study)
A
Total Sleep Time*
(Subjective)
⊕⊕⊕⊝
moderate
2
The mean total sleep time in the suvorexant group was
10.6 minutes higher
(1.79 to 19.41 higher)
567
(1 study)
A
Wake After Sleep Onset*
(PSG)
⊕⊕⊝⊝
low
2,3
The mean wake after sleep onset in the suvorexant group was
16.60 minutes lower
(24.87 to 8.33 lower)
567
(1 study)
A
* Critical Outcome, used to determine Quality of Evidence
1
95% CI (-13.85 to -2.35) crosses Clinical Significance Threshold (10 min)
2
Study funded by industry
3
95% CI (-24.87 to -8.33) crosses Clinical Significance Threshold (20 min)
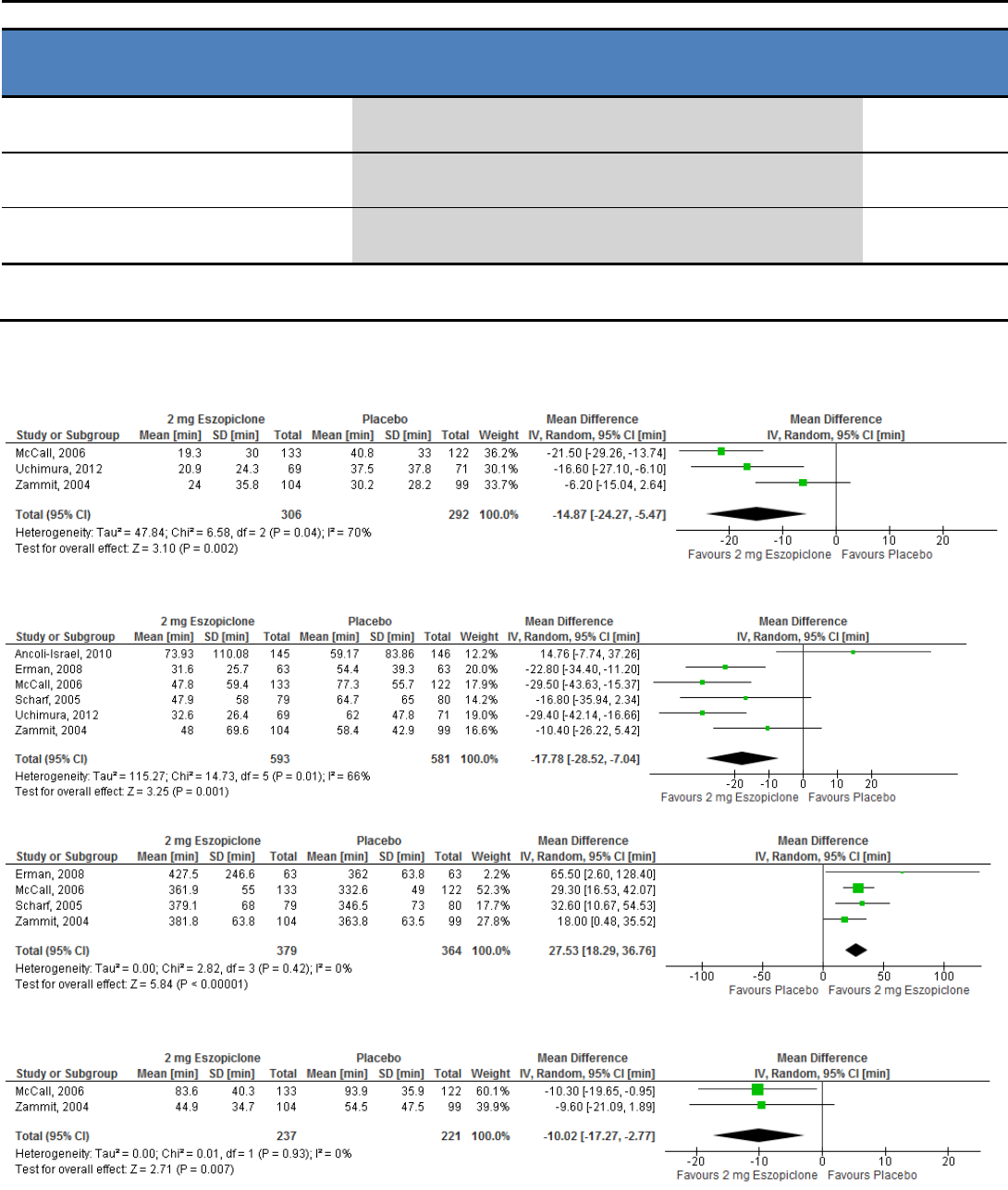
Table S3 – Summary of Findings table for suvorexant 20 mg for the treatment of chronic insomnia
References: Herring 2012(A)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
20 mg Suvorexant vs Placebo
No of Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊕⊝
moderate
2
The mean sleep latency in the suvorexant group was
22.3 minutes lower
(33.77 to 10.83 lower)
173
(1 study)
A
Wake After Sleep Onset*
(PSG)
⊕⊕⊝⊝
low
1,2
The mean wake after sleep onset in the suvorexant group was
28.1 minutes lower
(43.07 to 13.13 lower)
173
(1 study)
A
Sleep Efficiency
(PSG)
⊕⊕⊕⊝
moderate
2
The mean sleep efficiency in the suvorexant group was
10.4 percent higher
(6.65 to 14.15 higher)
173
(1 study)
A
* Critical Outcome, used to determine Quality of Evidence
1
95% CI (-43.07 to -13.13) crosses Clinical Significance Threshold (20 min)
2
Study funded by industry
Eszopiclone - Meta-Analyses and Summary of Findings Tables
Figure S1 – Meta-analysis of data for PSG-determined sleep latency in response to eszopiclone 2 mg
Figure S2 – Meta-analysis of data for subjectively-determined sleep latency in response to eszopiclone 2 mg
Figure S3 – Meta-analysis of data for subjectively-determined total sleep time in response to eszopiclone 2 mg
Figure S4 – Meta-analysis of data for PSG-determined wake after sleep onset in response to eszopiclone 2 mg
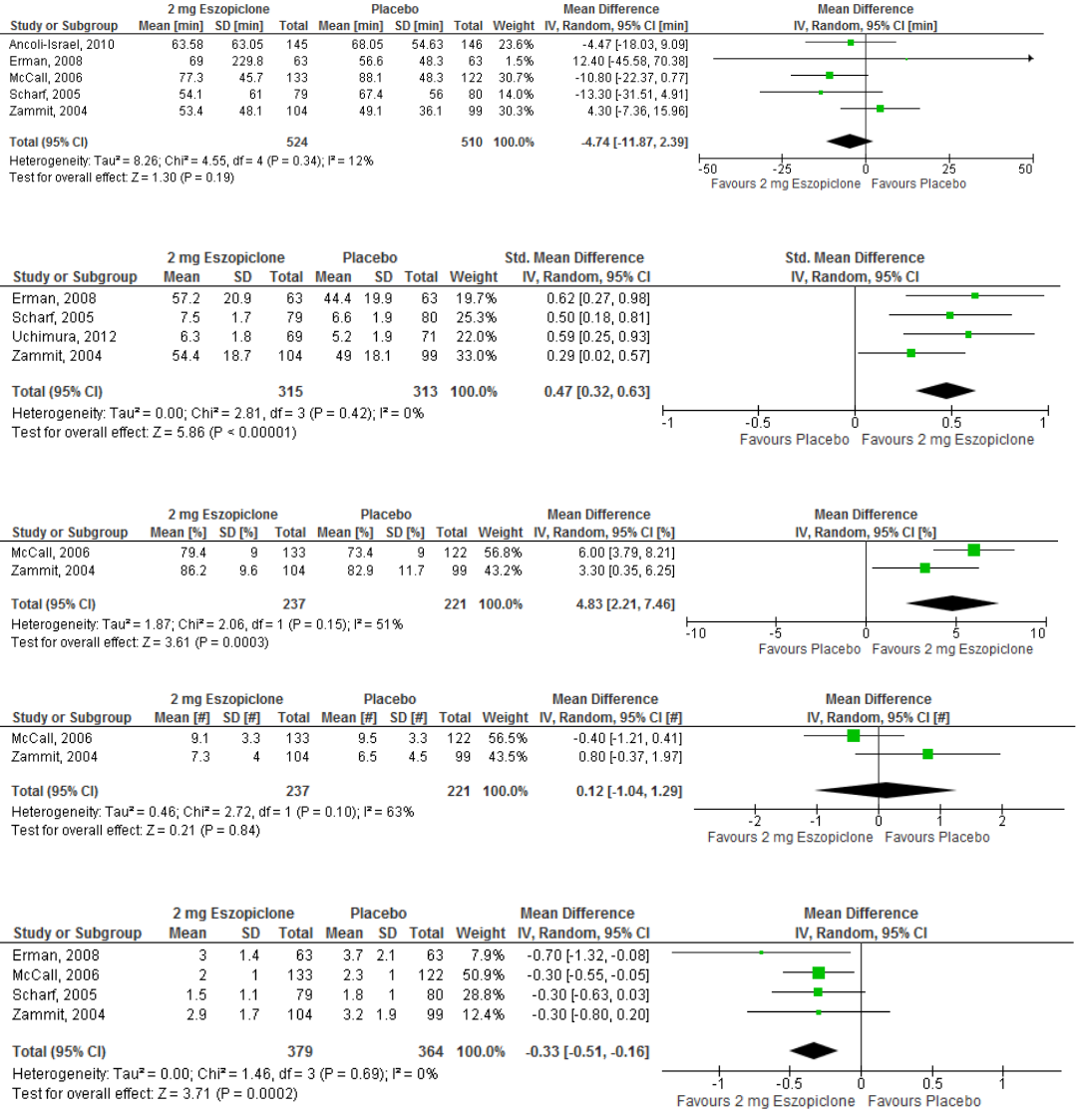
Figure S5 – Meta-analysis of data for subjectively-determined wake after sleep onset in response to eszopiclone 2 mg
Figure S6 – Meta-analysis of data for subjectively-determined quality of sleep in response to eszopiclone 2 mg
Figure S7 – Meta-analysis of data for PSG-determined sleep efficiency in response to eszopiclone 2 mg
Figure S8 – Meta-analysis of data for PSG-determined number of awakenings in response to eszopiclone 2 mg
Figure S9 – Meta-analysis of data for subjectively-determined number of awakenings in response to eszopiclone 2 mg

Figure S10– Meta-analysis of data for the occurrence of dizziness in response to eszopiclone 2 mg
Figure S11– Meta-analysis of data for the occurrence of dry mouth in response to eszopiclone 2 mg
Figure S12– Meta-analysis of data for the occurrence of headache in response to eszopiclone 2 mg
Figure S13– Meta-analysis of data for the occurrence of somnolence in response to eszopiclone 2 mg
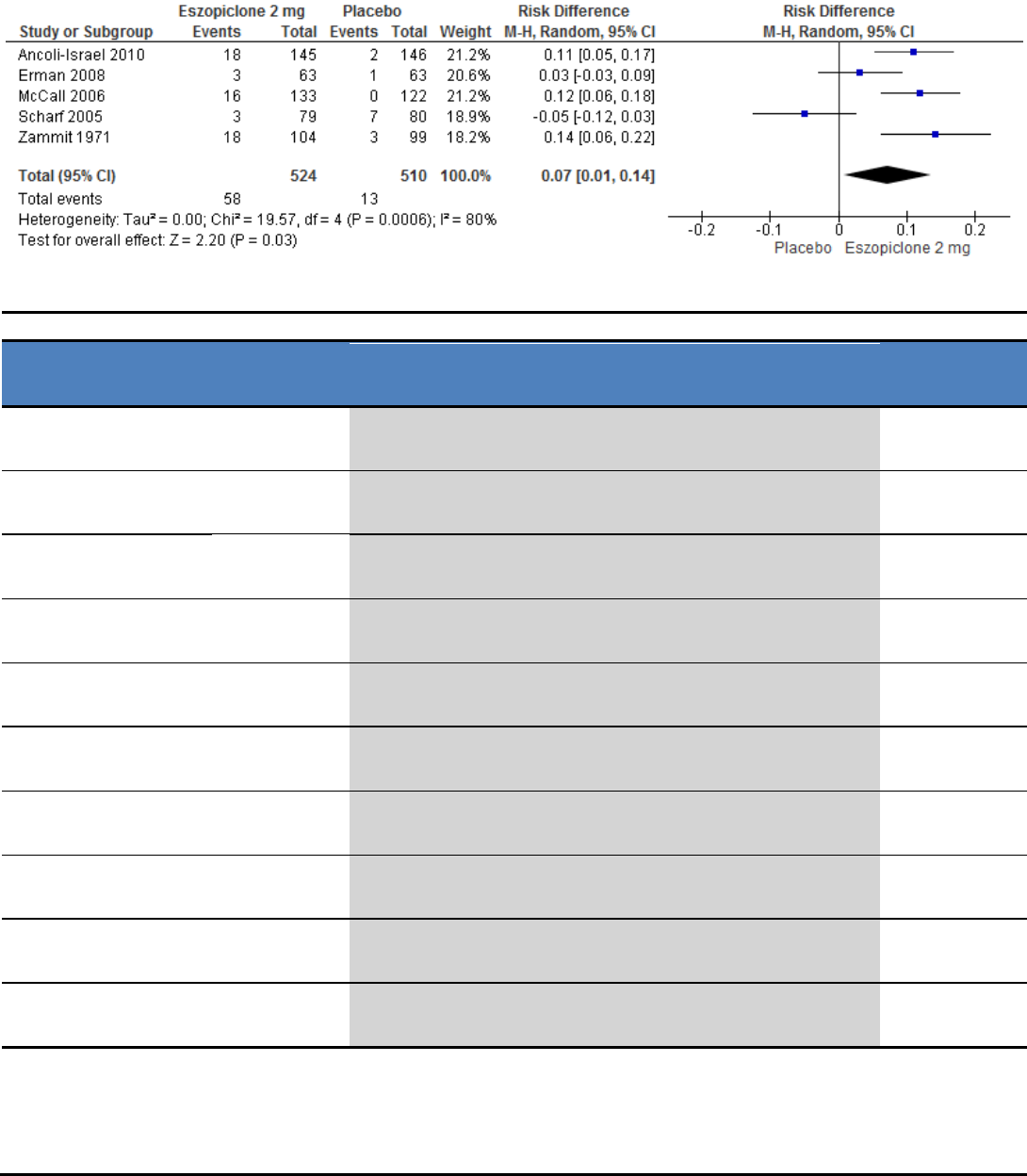
Figure S14– Meta-analysis of data for the occurrence of unpleasant taste in response to eszopiclone 2 mg
Table S4 – Summary of Findings table for eszopiclone 2 mg for the treatment of chronic insomnia
References: Ancoli-Israel 2010(A); Erman 2008(B); McCall 2006(C); Scharf 2005(D); Uchimura 2012(E); Zammit 2004(F)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
2 mg Eszopiclone vs Placebo
No of Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊝⊝
low
1,2
The mean sleep latency in the eszopiclone groups was
14.87 minutes lower
(24.27 to 5.47 lower)
598
(3 studies)
C,E,F
Sleep Latency
(Subjective)
⊕⊕⊝⊝
low
2,3
The mean sleep latency in the eszopiclone groups was
17.78 minutes lower
(28.52 to 7.04 lower)
1174
(6 studies)
A,B,C,D,E,F
Total Sleep Time*
(Subjective)
⊕⊕⊝⊝
low
2,4
The mean total sleep time in the eszopiclone groups was
27.53 minutes higher
(18.29 to 36.76 higher)
743
(4 studies)
B,C,D,F
Wake After Sleep Onset*
(PSG)
⊕⊕⊕⊝
moderate
2
The mean wake after sleep onset in the eszopiclone groups was
10.02 minutes lower
(17.27 to 2.77 lower)
458
(2 studies)
C,F
Wake After Sleep Onset
(Subjective)
⊕⊕⊕⊝
moderate
2
The mean wake after sleep onset in the eszopiclone groups was
4.74 minutes lower
(11.87 lower to 2.39 higher)
1034
(5 studies)
A,B,C,D,F
Quality of Sleep*
(Subjective)
⊕⊕⊕⊝
moderate
2,6
The mean quality of sleep in the eszopiclone groups was
0.47 standard deviations higher
(0.32 to 0.63 higher)
628
(4 studies)
B,D,E,F
Sleep Efficiency
(PSG)
⊕⊕⊝⊝
low
2,5
The mean sleep efficiency in the eszopiclone groups was
4.83 percent higher
(2.21 to 7.46 higher)
458
(2 studies)
C,F
Sleep Efficiency
(Subjective)
⊕⊕⊕⊝
moderate
2
The mean sleep efficiency in the eszopiclone groups was
0.30 percent lower
(0.79 lower to 0.19 higher)
203
(1 study)
F
Number of Awakening
(PSG)
⊕⊕⊕⊝
moderate
2
The mean number awakening in the eszopiclone groups was
0.12 awakenings higher
(1.04 lower to 1.29 higher)
458
(2 studies)
C,F
Number of Awakenings
(Subjective)
⊕⊕⊕⊝
moderate
2
The mean number of awakenings in the eszopiclone groups was
0.33 awakenings lower
(0.51 to 0.16 lower)
743
(4 studies)
B,C,D,F
* Critical Outcome, used to determine Quality of Evidence
1
95% CI (-24.27, -5.47) crosses Clinical Signficance (10 min)
2
All studies funded by industry
3
95% CI (-33.81, -6.35) crosses Clinical Signficance (20 min)
4
95% CI (18.29, 36.76) crosses Clinical Signficance (20 min)
5
95% CI (2.21, 7.46) crosses Clinical Significance (5%)
6
95% CI (0.37, 0.76) crosses Clinical Significance (SMD 0.5)
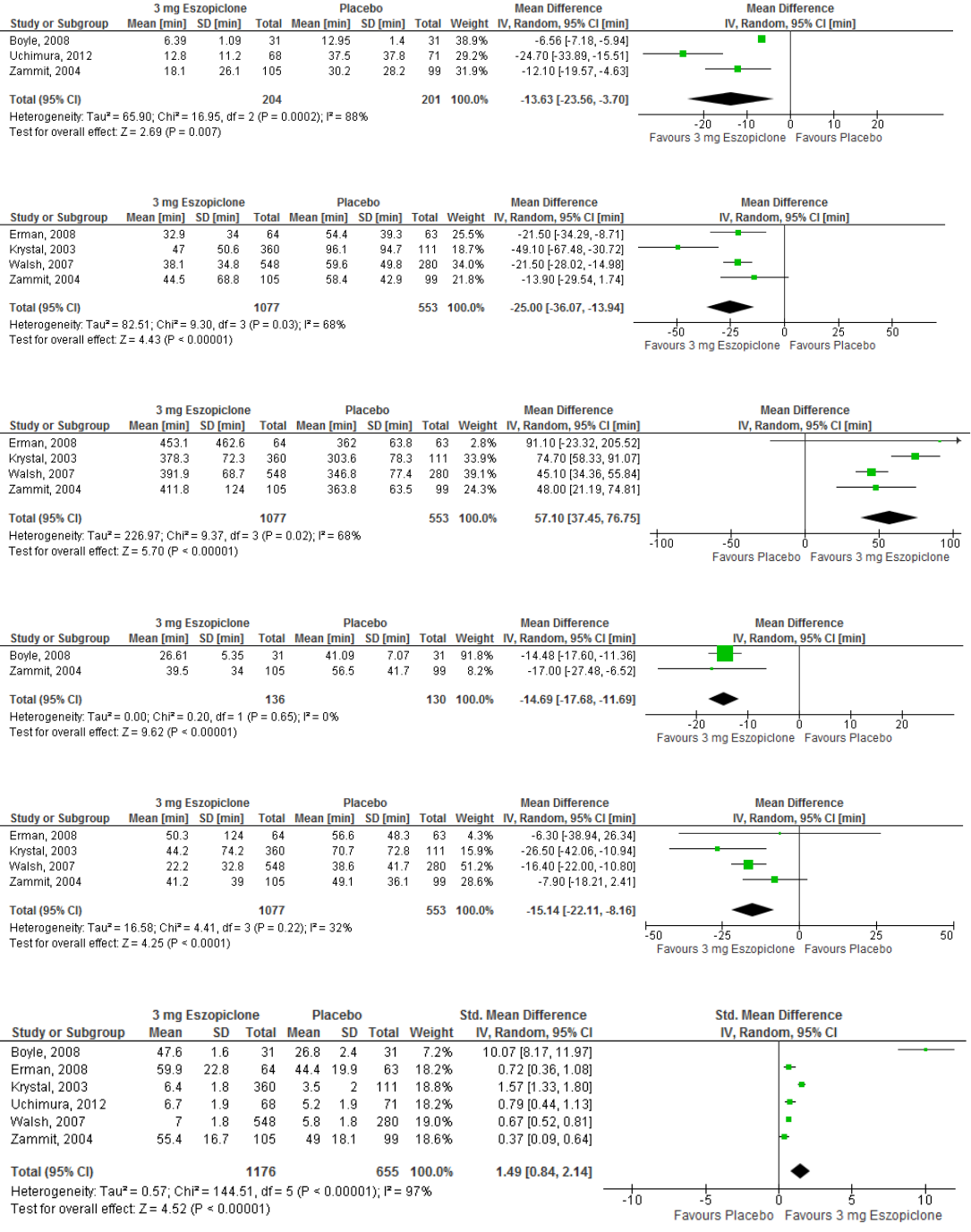
Figure S15 – Meta-analysis of data for PSG-determined sleep latency in response to eszopiclone 3 mg
Figure S16 – Meta-analysis of data for subjectively-determined sleep latency in response to eszopiclone 3 mg
Figure S17 – Meta-analysis of data for subjectively-determined total sleep time in response to eszopiclone 3 mg
Figure S18 – Meta-analysis of data for PSG-determined wake after sleep onset in response to eszopiclone 3 mg
Figure S19 – Meta-analysis of data for subjectively-determined wake after sleep onset in response to eszopiclone 3 mg
Figure S20 – Meta-analysis of data for subjectively-determined quality of sleep in response to eszopiclone 3 mg
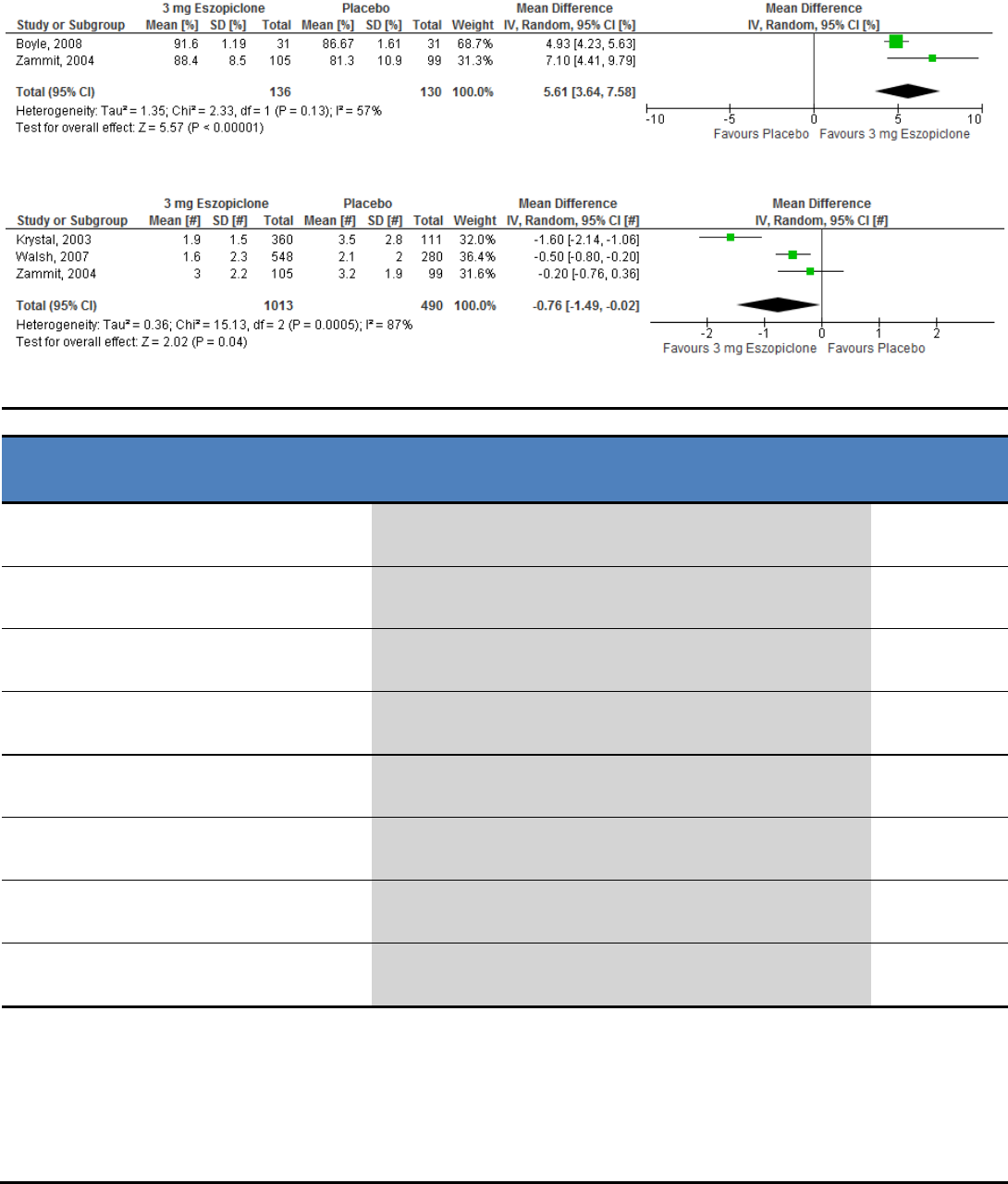
Figure S21 – Meta-analysis of data for PSG-determined sleep efficiency in response to eszopiclone 3 mg
Figure S22 – Meta-analysis of data for subjectively-determined number of awakenings in response to eszopiclone 3 mg
Table S5 – Summary of Findings table for eszopiclone 3 mg for the treatment of chronic insomnia
References: Boyle 2008(A); Erman 2008(B); Krystal 2003(C); Uchimura 2012(D); Walsh 2007(E); Zammit 2004(F)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
3 mg Eszopiclone vs Placebo
No of Participants
(studies)
Sleep Latency*
(PSG)
⊕⊝⊝⊝
very low
1,2,3
The mean sleep latency in the eszopiclone groups was
13.63 minutes lower
(23.56 to 3.7 lower)
405
(3 studies)
A,D,F
Sleep Latency
(Subjective)
⊕⊕⊝⊝
low
3,4
The mean sleep latency in the eszopiclone groups was
25.00 minutes lower
(36.07 to 13.94 lower)
1630
(4 studies)
B,C,E,F
Total Sleep Time*
(Subjective)
⊕⊕⊕⊝
moderate
3
The mean total sleep time in the eszopiclone groups was
57.10 minutes higher
(37.45 to 76.75 higher)
1630
(4 studies)
B,C,E,F
Wake After Sleep Onset*
(PSG)
⊕⊕⊕⊝
moderate
3
The mean wake after sleep onset in the eszopiclone groups was
14.69 minutes lower
(17.68 to 11.69 lower)
266
(2 studies)
A,F
Wake After Sleep Onset
(Subjective)
⊕⊕⊝⊝
low
3,5
The mean wake after sleep onset in the eszopiclone groups was
15.14 minutes lower
(22.11 to 8.16 lower)
1630
(4 studies)
B,C,E,F
Quality of Sleep*
(Subjective)
⊕⊕⊝⊝
low
3,9
The mean quality of sleep in the eszopiclone groups was
1.49
standard deviations higher
(0.
84 to 2.14 higher)
1769
(
6 studies)
A,B,C,D,E,F
Sleep Efficiency
(PSG)
⊕⊕⊝⊝
low
3,6
The mean sleep efficiency in the eszopiclone groups was
5.61 percent higher
(3.64 to 7.58 higher)
266
(2 studies)
A,F
Number of Awakenings
(Subjective)
⊕⊝⊝⊝
very low
3,6,7
The mean number awakenings in the eszopiclone groups was
0.76 awakenings lower
(1.49 to 0.02 lower)
1503
(3 studies)
C,E,F
* Critical Outcome, used to determine Quality of Evidence
1
Heterogeneity (I² = 88%) greater than allowance (75%)
2
95% CI (-23.56, -3.70) crosses Clinical Significance (10 min)
3
All studies funded by industry
4
95% CI (-36.07, -13.94) crosses Clinical Significance (20 min)
5
95% CI (-22.11, -8.16) crossess Clinical Significance (20 min)
6
Heterogeneity (I² = 87%) greater than allowance (75%)
7
95% CI (-1.49, -0.02) crosses Clinical Significance (0.5 awakenings)
8
95% CI (3.64, 7.58) crosses Clinical Significance
9
Heterogeneity (I² = 93%) greater than allowance (75%)
Zaleplon - Summary of Findings Tables
Table S6 – Summary of Findings table for zaleplon 5 mg for the treatment of chronic insomnia
References: Hedner 2000(A)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
5 mg Zaleplon vs
Placebo
No of
Participants
(studies)
Quality of Sleep*
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean quality of sleep in the zaleplon group was
0.10 points
2
lower
(0.27 lower to 0.07 higher)
277
(1 study)
A
* Critical Outcome, used to determine Quality of Evidence
1
Study funded by Industry
2
7-point scale (1=excellent, 7=extremely poor)
Table S7 – Summary of Findings table for zaleplon 10 mg for the treatment of chronic insomnia
References: Hedner 2000(A); Walsh 2000(B)
Outcomes
Quality of the evidence
(GRADE)
Absolute Difference
10 mg Zaleplon vs Placebo
No of Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊝⊝
low
1,3
The mean sleep latency in the zaleplon group was
9.50 minutes lower
(18.80 to 0.19 lower)
94
(1 study)
B
Sleep Latency
(Subjective)
⊕⊕⊝⊝
low
2,3
The mean sleep latency in the zaleplon group was
11.40 minutes lower
(27.36 lower to 4.56 higher)
92
(1 study)
B
Total Sleep Time*
(Subjective)
⊕⊕⊝⊝
low
3,4
The mean total sleep time in the zaleplon group was
21.50 minutes higher
(5.60 lower to 48.6 higher)
93
(1 study)
B
Wake After Sleep Onset
(PSG)
⊕⊕⊕⊝
moderate
3
The mean wake after sleep onset in the zaleplon group was
2.10 minutes lower
(10.23 lower to 6.03 higher)
92
(1 study)
B
Quality of Sleep*
(Subjective)
⊕⊕⊕⊝
moderate
3
The mean quality of sleep in the zaleplon group was
0.10 points
5
lower
(0.27 lower to 0.07 higher)
283
(1 study)
A
* Critical Outcome, used to determine Quality of Evidence
1
95% CI (-18.8, -0.19) crosses Clinical Significance (10 min)
2
95% CI (-27.36, 4.56) crosses Clinical Significance (20 min)
3
Study funded by Industry
4
95% CI (-5.60, 48.60) crosses Clinical Significance (30 min)
5
7-point scale (1=excellent, 7=extremely poor)
Zolpidem - Meta-Analyses and Summary of Findings Tables
Table S8 – Summary of Findings table for zolpidem 6.25 mg for the treatment of chronic insomnia
References: Walsh 2008
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
6.25 mg Zolpidem vs Placebo
No of
Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊝⊝
low
1,2
The mean sleep latency in the zolpidem group was
5.27 minutes lower
(11.47 lower to 0.93 higher)
199
(1 study)
Wake After Sleep Onset*
(PSG)
⊕⊕⊝⊝
low
1,3
The mean wake after sleep onset in the zolpidem group was
13.03 minutes
lower
(22.5 to 3.55 lower)
199
(1 study)
Sleep Efficiency
(PSG)
⊕⊕⊕⊝
moderate
1
The mean sleep efficiency in the zolpidem group was
1.60 percent higher
(1.4 lower to 4.6 higher)
199
(1 study)
* Critical Outcome, used to determine Quality of Evidence
1
Funding source not specified, author disclosures not specified.
2
95% CI (-11.47, 0.93) crosses Clinical Significance
3
95% CI (-22.5, -3.55) crosses Clinical Significance (20 min)
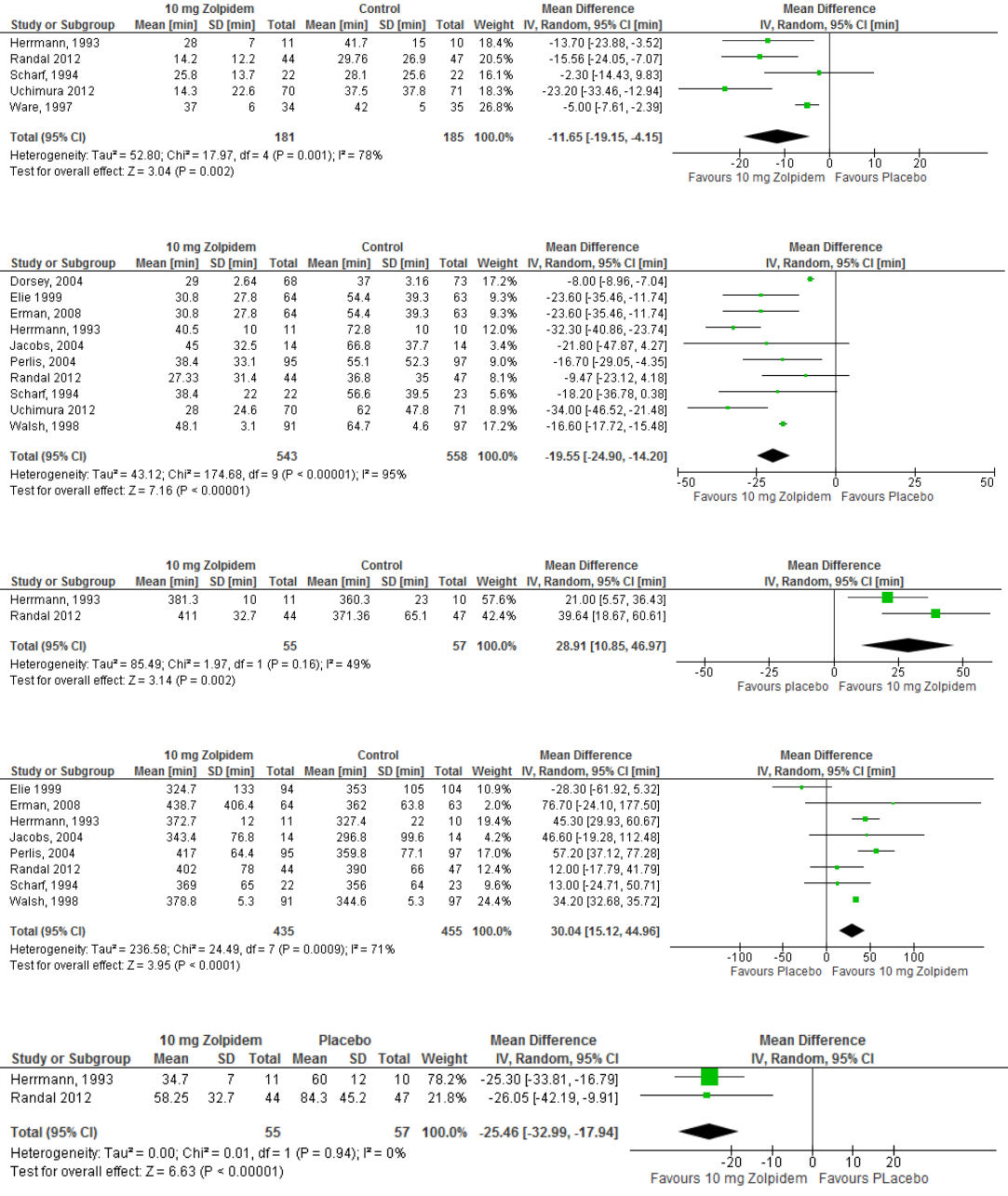
Figure S23 – Meta-analysis of data for PSG-determined sleep latency in response to zolpidem 10 mg
Figure S24 – Meta-analysis of data for subjectively-determined sleep latency in response to zolpidem 10 mg
Figure S25 – Meta-analysis of data for PSG-determined total sleep time in response to zolpidem 10 mg
Figure S26 – Meta-analysis of data for subjectively-determined total sleep time in response to zolpidem 10 mg
Figure S27 – Meta-analysis of data for PSG-determined wake after sleep onset in response to zolpidem 10 mg
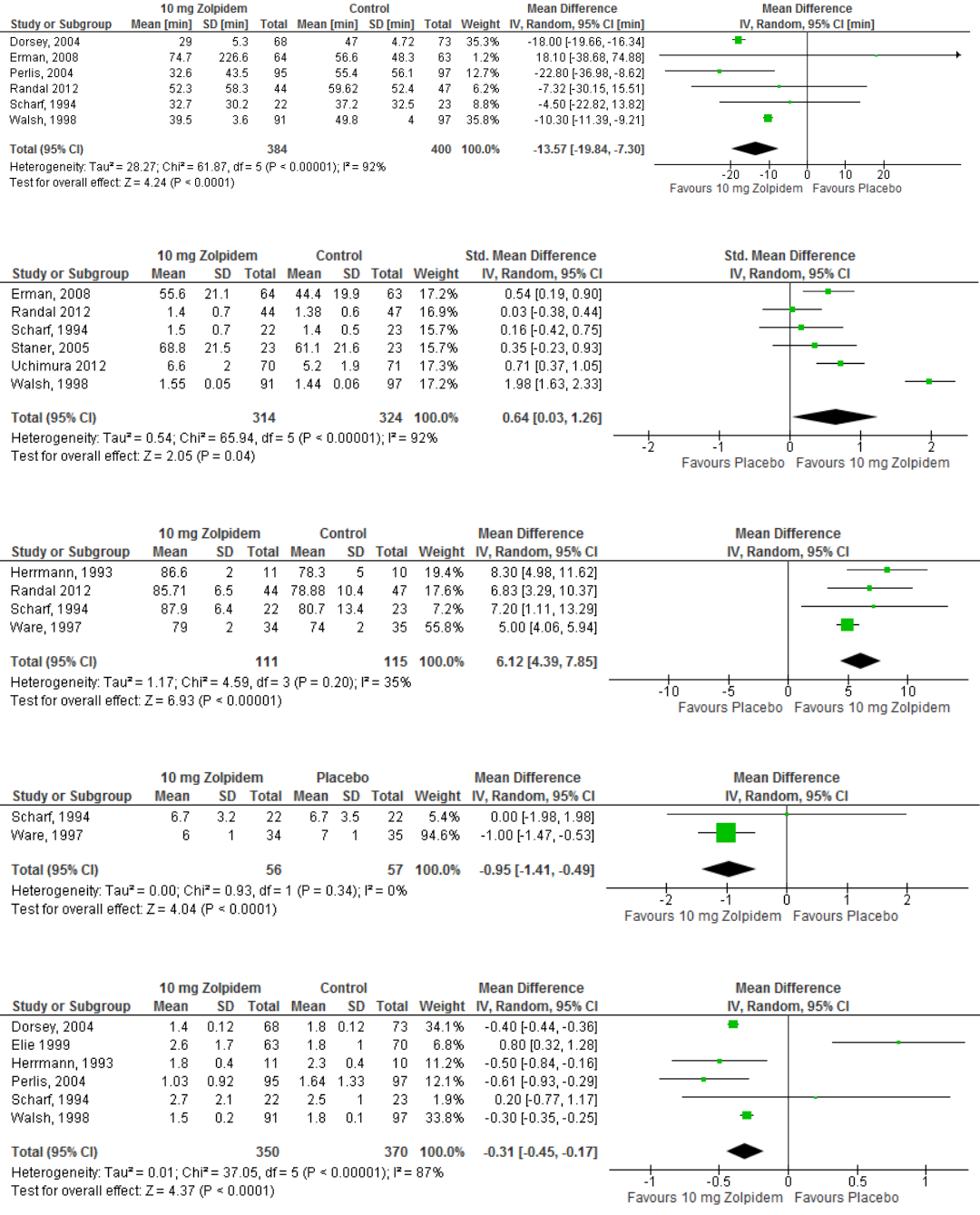
Figure S28 – Meta-analysis of data for subjectively-determined wake after sleep onset in response to zolpidem 10 mg
Figure S29 – Meta-analysis of data for subjectively-determined quality of sleep in response to zolpidem 10 mg
Figure S30 – Meta-analysis of data for PSG-determined sleep efficiency in response to zolpidem 10 mg
Figure S31 – Meta-analysis of data for PSG-determined number of awakenings in response to zolpidem 10 mg
Figure S32 – Meta-analysis of data for subjectively-determined number of awakenings in response to zolpidem 10 mg
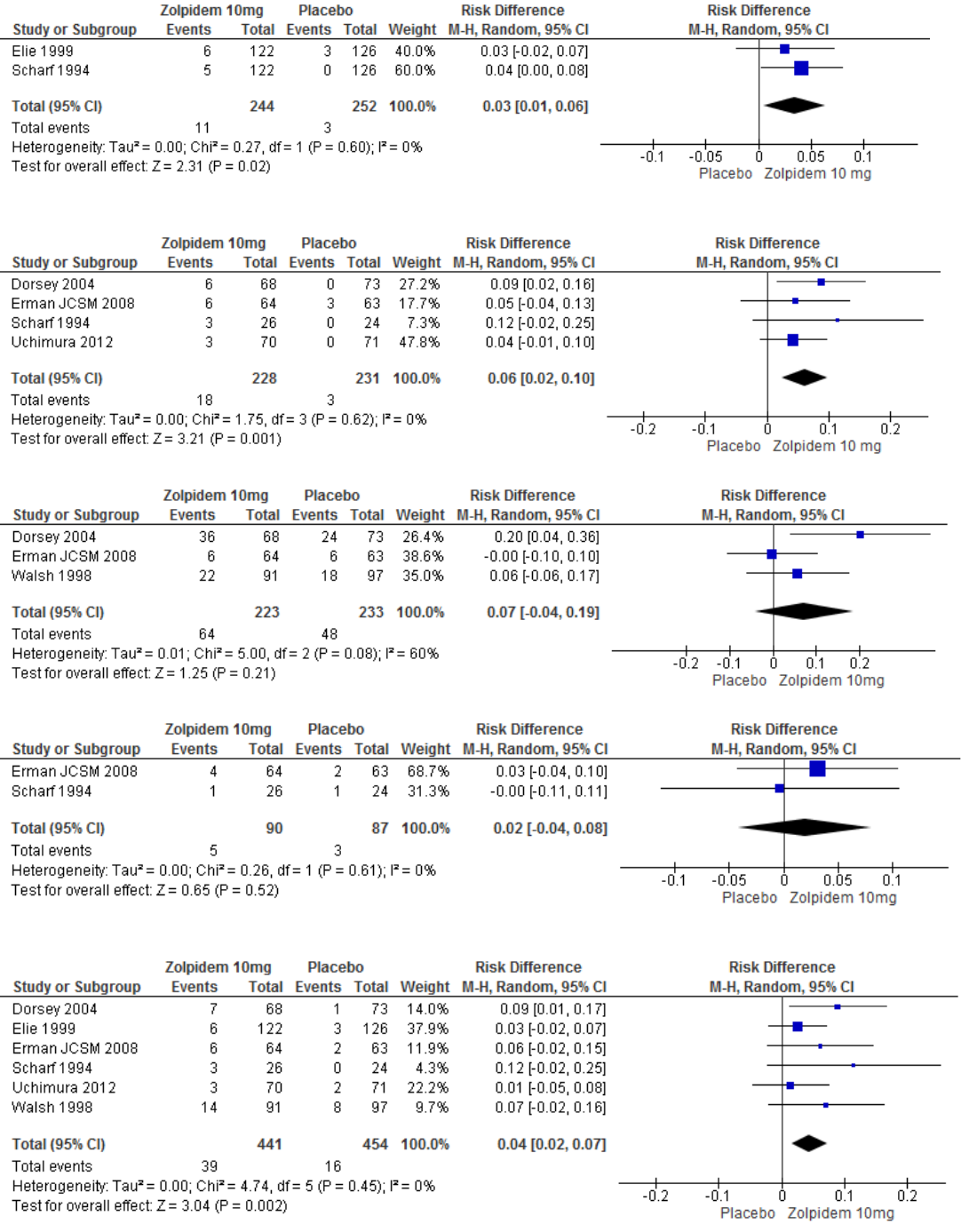
Figure S33 – Meta-analysis of data for the occurrence of amnesia in response to zolpidem 10 mg
Figure S34 – Meta-analysis of data for the occurrence of dizziness in response to zolpidem 10 mg
Figure S35 – Meta-analysis of data for the occurrence of headache in response to zolpidem 10 mg
Figure S36 – Meta-analysis of data for the occurrence of nausea in response to zolpidem 10 mg
Figure S37 – Meta-analysis of data for the occurrence of somnolence in response to zolpidem 10 mg
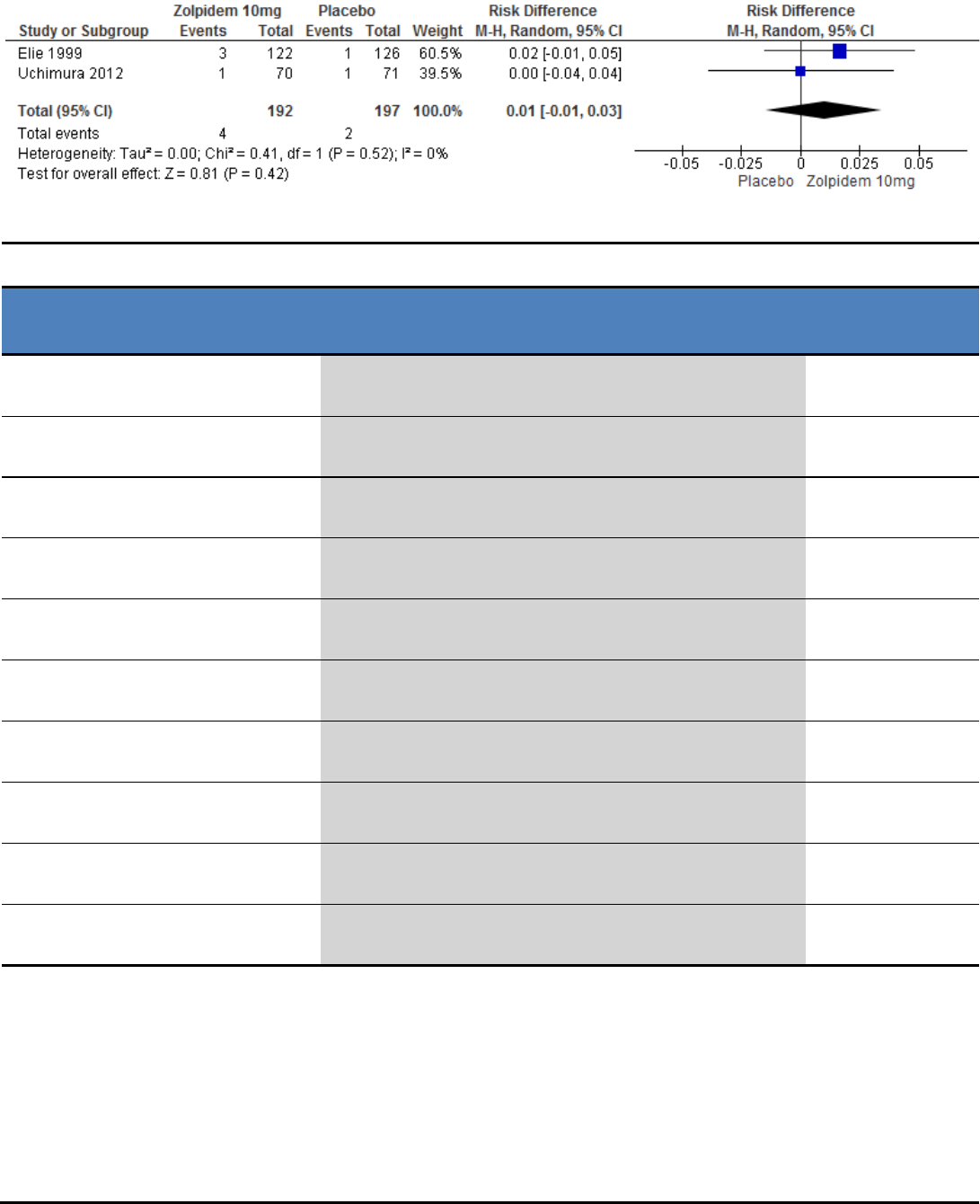
Figure S38 – Meta-analysis of data for the occurrence of taste perversion in response to zolpidem 10 mg
Table S9 – Summary of Findings table for zolpidem 10 mg for the treatment of chronic insomnia
References: Dorsey 2004(A); Elie 1999(B); Erman 2008(C); Herrmann 1993(D); Jacobs 2004(E); Perlis 2004(F); Randal 2012(G); Scharf 1994(H);
Staner 2005(I); Uchimura 2012(J); Walsh 1998(K); Ware 1997(L)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
10 mg Zolpidem vs Placebo
No of Participants
(studies)
Sleep Latency*
(PSG)
⊕⊝⊝⊝
very low
1,2,3
The mean sleep latency in the zolpidem groups was
11.65 minutes lower
(19.15 to 4.15 lower)
366
(5 studies)
D,G,H,J,L
Sleep Latency
(Subjective)
⊕⊝⊝⊝
very low
3,4,5
The mean sleep latency in the zolpidem groups was
19.55 minutes lower
(24.90 to 14.20 lower)
1101
(10 studies)
A,B,C,D,E,FG,H,J,K
Total Sleep Time*
(PSG)
⊕⊕⊝⊝
low
3,12
The mean total sleep time in the zolpidem groups was
28.91 minutes higher
(10.85 to 46.97 higher)
112
(2 studies)
D,G
Total Sleep Time*
(Subjective)
⊕⊕⊝⊝
low
3,7
The mean total sleep time in the zolpidem groups was
30.04 minutes higher
(15.12 to 44.96 higher)
890
(8 studies)
B,C,D,E,F,G,H,K
Wake After Sleep Onset*
(PSG)
⊕⊕⊝⊝
low
3,13
The mean wake after sleep onset in the zolpidem groups was
25.46 minutes lower
(32.99 to 17.94 lower)
112
(2 studies)
D,G
Wake After Sleep Onset
(Subjective)
⊕⊕⊝⊝
low
3,6
The mean wake after sleep onset in the zolpidem groups was
13.57 minutes lower
(19.84 to 7.30 lower)
784
(6 studies)
A,C,F,G,H,K
Quality of Sleep*
(Subjective)
⊕⊝⊝⊝
very low
3,10,11
The mean quality of sleep in the zolpidem groups was
0.64 standard deviations higher
(0.03 to 1.26 higher)
638
(6 studies)
C,G,H,I,J,K
Sleep Efficiency
(PSG)
⊕⊕⊝⊝
low
3,9
The mean sleep efficiency in the zolpidem groups was
6.12 percent higher
(4.39 to 7.85 higher)
226
(4 studies)
D,G,H,L
Number of Awakenings
(PSG)
⊕⊕⊕⊝
moderate
3
The mean number of awakenings in the zolpidem groups was
0.95 awakenings lower
(1.41 to 0.49 lower)
113
(2 studies)
H,L
Number of Awakenings
(Subjective)
⊕⊕⊝⊝
low
3,8
The mean number of awakenings in the zolpidem groups was
0.31 awakenings lower
(0.45 to 0.17 lower)
720
(6 studies)
A,B,D,F,H,K
* Critical Outcome, used to determine Quality of Evidence
1
Heterogeneity (I² = 78%) greater than allowance (75%)
2
95% CI (-19.15, -4.15) crosses Clinical Significance (10 min)
3
Studies funded by industry
4
Heterogeneity (I² = 95%) greater than allowance (75%)
5
95% CI (-24.90, -14.20) crosses Clinical Significance (20 min)
6
Heterogeneity (I² = 92%) greater than allowance (75%)
7
95% CI (15.12, 44.96) crosses Clinical Significance (30 min)
8
Heterogeneity (I² = 87%) greater than allowance (75%)
9
95% CI (4.39, 7.85) crosses Clinical Significance (5%)
10
Heterogeneity (I² = 92%) greater than allowance (75%)
11
95% CI (0.3, 1.26) crosses Clinical Significance (SMD 0.5)
12
95% CI (10.85, 46.97) crosses Clinical Significance (20 min)
13
95% CI (-32.99, -17.4) crosses Clinical Significance (20 min)
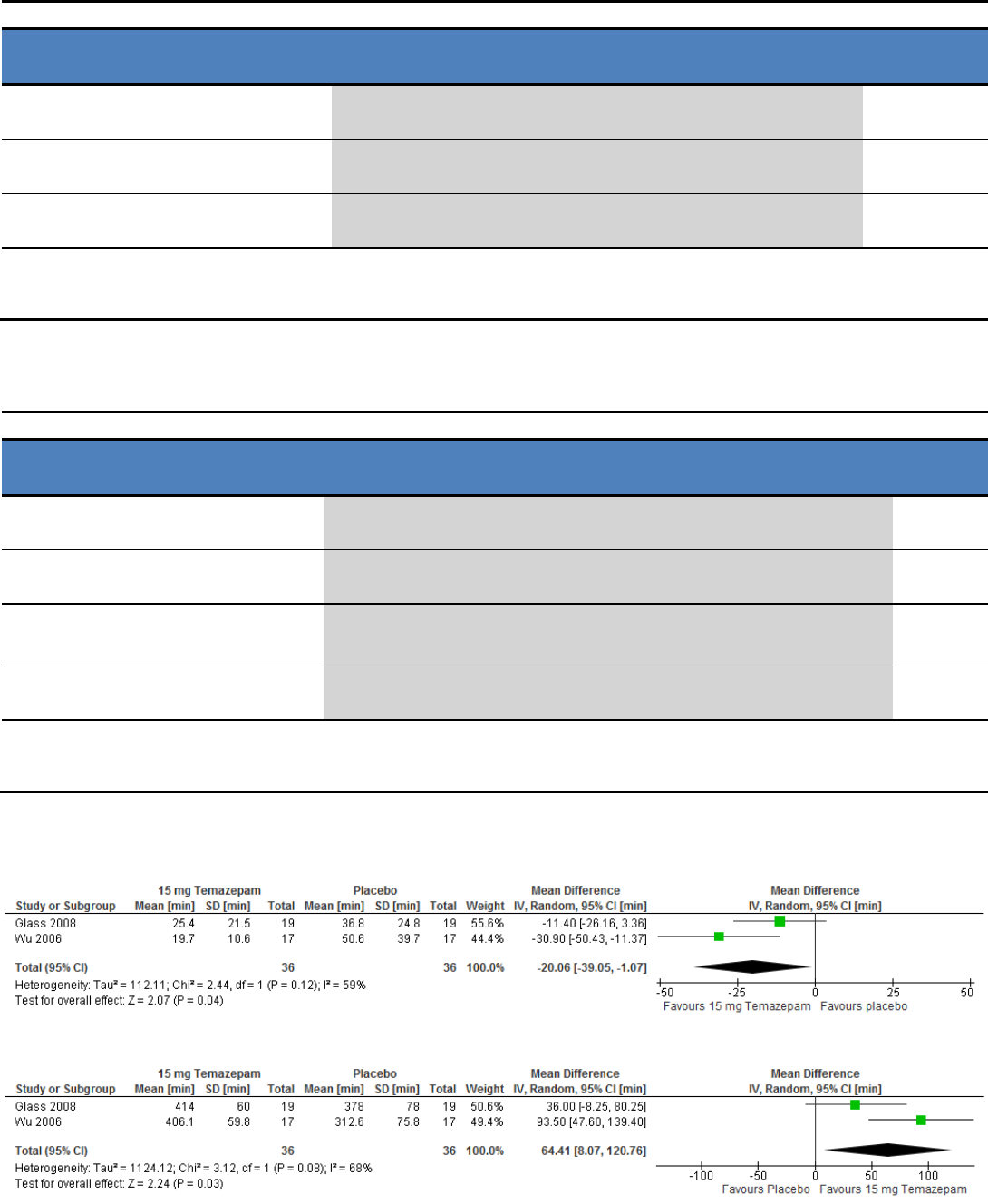
Table S10 – Summary of Findings table for zolpidem 12.5 mg for the treatment of chronic insomnia
References: Roth 2006
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
12.5 Zolpidem vs Placebo
No of
Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊝⊝
low
1,2
The mean sleep latency in the zolpidem group was
8.19 minutes lower
(15.22 to 1.15 lower)
212
(1 study)
Wake After Sleep Onset*
(PSG)
⊕⊕⊝⊝
low
1,3
The mean wake after sleep onset in the zolpidem group was
19.99 minutes lower
(27.33 to 12.64 lower)
212
(1 study)
Sleep Efficiency
(PSG)
⊕⊕⊕⊝
moderate
1
The mean sleep efficiency in the zolpidem group was
3.9 percent higher
(1.38 to 6.41 higher)
212
(1 study)
* Critical Outcome, used to determine Quality of Evidence
1
Funding source not specified, author disclosures not specified.
2
95% CI (-15.22, 1.15) crosses Clinical Significance (10 min)
3
95% CI (-27.33, -12.64) crosses Clinical Significance (20 min)
Triazolam - Summary of Findings Table
Table S11 – Summary of Findings table for triazolam 0.25 mg for the treatment of chronic insomnia
References: Roehrs 2001
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
0.25 mg Triazolam vs Placebo
No of
Participants
(studies)
Sleep Latency*
(Subjective)
⊕⊕⊕⊕
high
The mean sleep latency in the triazolam group was
9.20 minutes lower
(22.3 lower to 3.9 higher)
64
(1 study)
Total Sleep Time
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean total sleep time in the triazolam group was
25.20 minutes higher
(9.12 lower to 59.52 higher)
64
(1 study)
Quality of Sleep*
(Subjective)
⊕⊕⊕⊕
high
The mean quality of sleep in the triazolam group was
0.37 points
3
lower
(0.66 to 0.07 lower)
64
(1 study)
Number of Awakenings
(Subjective)
⊕⊕⊝⊝
low
2
The mean number of awakenings in the triazolam group was
0.37 awakenings lower
(1.7 lower to 0.96 higher)
64
(1 study)
* Critical Outcome, used to determine Quality of Evidence
1
95% CI (-9.12, 59.52) crosses Clinical Significance (30 min)
2
95% CI (-1.7, 0.96) crosses Clinical Significance (0.5 awakenings)
3
4-point scale (1=good, 4=poor)
Temazepam - Meta-Analyses and Summary of Findings Tables
Figure S39 – Meta-analysis of data for subjectively-determined sleep latency in response to temazepam 15 mg
Figure S40 – Meta-analysis of data for subjectively-determined total sleep time in response to temazepam 15 mg
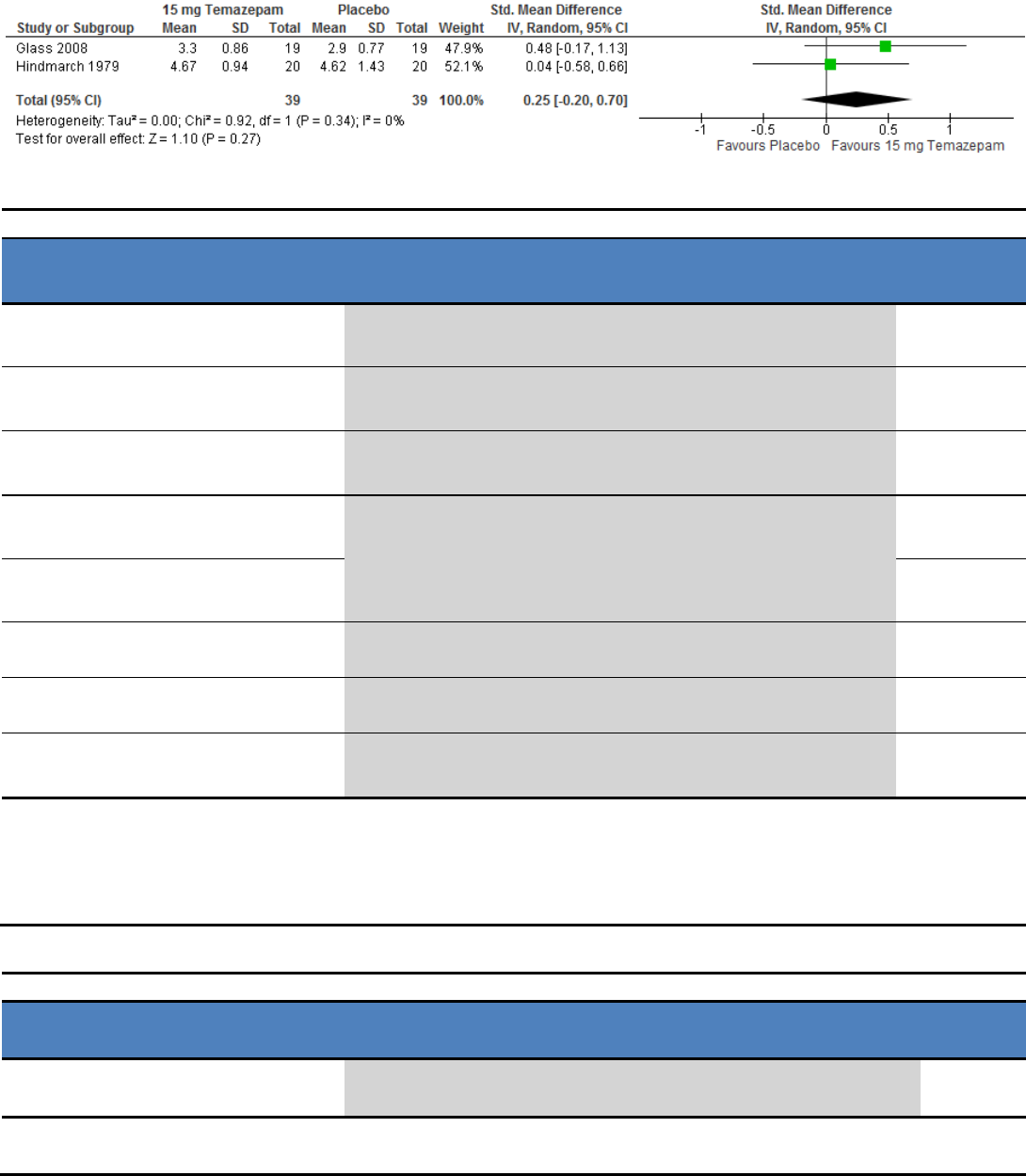
Figure S41 – Meta-analysis of data for subjectively-determined quality of sleep in response to temazepam 15 mg
Table S12 – Summary of Findings table for temazepam 15 mg for the treatment of chronic insomnia
Reference: Glass 2008(A); Hindmarch 1979(B); Wu 2006 (C)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
15 mg Temazepam vs Placebo
No of
Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊕⊕
high
The mean sleep latency in the temazepam group was
37.1 minutes lower
(52.8 to 21.31 lower)
34
(1 study)
C
Sleep Latency
(Subjective)
⊕⊕⊕⊝
moderate
2
The mean sleep latency in the temazepam group was
20.06 minutes lower
(39.05 to 1.07 lower)
72
(2 studies)
A,C
Total Sleep Time*
(PSG)
⊕⊕⊕⊕
high
The mean total sleep time in the temazepam group was
99.1 minutes higher
(63.4 to 134.7 lower)
34
(1 study)
C
Total Sleep Time
(Subjective)
⊕⊕⊕⊝
moderate
3
The mean total sleep time in the temazepam groups was
64.41 minutes higher
(8.07 to 120.76 higher)
72
(2 studies)
A,C
Quality of Sleep*
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean quality of sleep in the temazepam group was
0.25 standard deviations higher
(0.2 lower to 0.7 higher)
39
(2 studies)
A,B
Sleep Efficiency
(PSG)
⊕⊕⊕⊝
moderate
5
The mean sleep efficiency in the temazepam group was
13.3 percent higher
(3.9 to 22.6 higher)
34
(1 study)
C
Sleep Efficiency
(Subjective)
⊕⊕⊕⊝
moderate
6
The mean sleep efficiency in the temazepam group was
14.1 percent higher
(5.8 to 22.3 higher)
34
(1 study)
C
Number of Awakenings
(Subjective)
⊕⊕⊕⊝
moderate
4
The mean number of awakenings in the temazepam group was
0.5 awakenings lower
(1.29 lower to 0.29 higher)
38
(1 study)
A
* Critical Outcome, used to determine Quality of Evidence
1
95% CI (-0.2, 0.7) crosses Clinical Significance (0.5 SMD)
2
95% CI (-39.05, -1.07) crosses Clinical Significance (20 min)
3
95% CI (8.07,120.76) crosses Clinical Significance (30 min)
4
95% CI (-1.29, 0.29) crosses Clinical Significance (0.5 awakenings)
5
95% CI (3.9, 22.6) crosses Clinical Significance (5%)
6
95% CI (5.8, 22.3) crosses Clinical Significance (10%)
Table S13 – Summary of Findings table for temazepam 30 mg for the treatment of chronic insomnia
References: Hindmarch 1979
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
30 mg Temazepam vs Placebo
No of
Participants
(studies)
Quality of Sleep*
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean quality of sleep in the temazepam group was
0.69 cm
2
higher
(0.28 lower to 1.66 higher)
40
(1 study)
* Critical Outcome, used to determine Quality of Evidence
1
95% CI (-0.28, 1.66) crosses Clinical Significance (1.0 cm)
2
10 cm line analogue rating scale
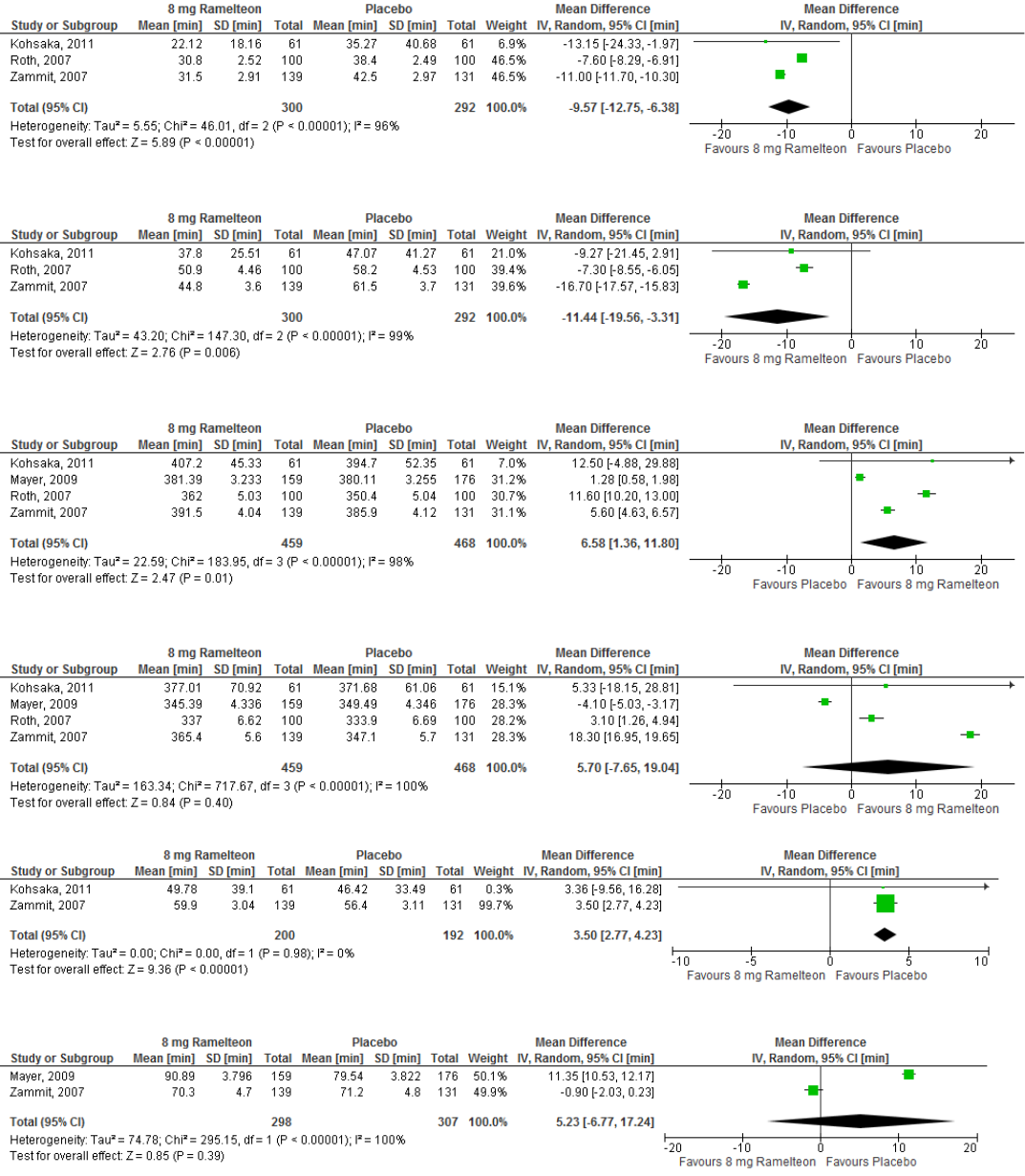
Ramelteon - Meta-Analyses and Summary of Findings Table
Figure S42 – Meta-analysis of data for PSG-determined sleep latency in response to ramelteon 8 mg
Figure S43 – Meta-analysis of data for subjectively-determined sleep latency in response to ramelteon 8 mg
Figure S44 – Meta-analysis of data for PSG-determined total sleep time in response to ramelteon 8 mg
Figure S45 – Meta-analysis of data for subjectively-determined total sleep time in response to ramelteon 8 mg
Figure S46 – Meta-analysis of data for PSG-determined wake after sleep onset in response to ramelteon 8 mg
Figure S47 – Meta-analysis of data for subjectively-determined wake after sleep onset in response to ramelteon 8 mg

Figure S48 – Meta-analysis of data for PSG-determined quality of sleep in response to ramelteon 8 mg
Figure S49 – Meta-analysis of data for PSG-determined sleep efficiency in response to ramelteon 8 mg
Figure S50 – Meta-analysis of data for the occurrence of headache in response to ramelteon 8 mg
Figure S51 – Meta-analysis of data for the occurrence of upper respiratory tract infection in response to ramelteon 8 mg
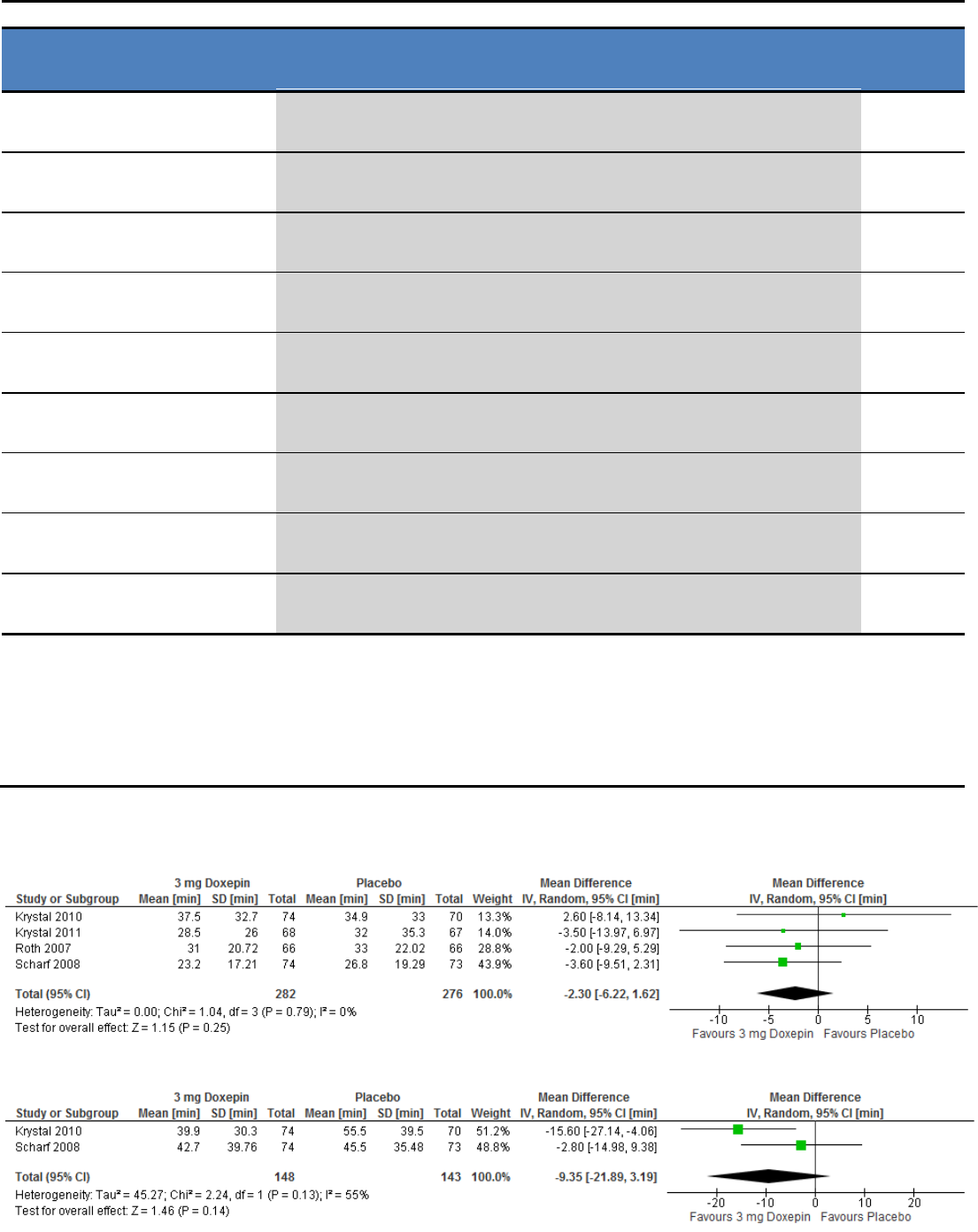
Table S14 – Summary of Findings table for ramelteon 8 mg for the treatment of chronic insomnia
References: Kohsaka 2011 (A); Mayer 2009(B); Roth 2007(C); Zammit 2007(D)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
8 mg Ramelteon vs Placebo
No of
Participants
(studies)
Sleep Latency*
(PSG)
⊕⊝⊝⊝
very low
1,2,3
The mean sleep latency in the ramelteon groups was
9.57 minutes lower
(12.75 to 6.38 lower)
592
(3 studies)
A,C,D
Sleep Latency
(Subjective)
⊕⊕⊝⊝
low
3,7,8
The mean sleep latency in the ramelteon groups was
11.44 minutes lower
(19.56 to 3.31 lower)
592
(3 studies)
A,C,D
Total Sleep Time
(PSG)
⊕⊕⊝⊝
low
1,3
The mean total sleep time in the ramelteon groups was
6.58 minutes higher
(1.36 to 11.80 higher)
927
(4 studies)
A,B,C,D
Total Sleep Time
(Subjective)
⊕⊕⊝⊝
low
3,6
The mean total sleep time in the ramelteon groups was
5.70 minutes higher
(7.65 lower to 19.04 higher)
927
(4 studies)
A,B,C,D
Wake After Sleep Onset
(PSG)
⊕⊕⊕⊝
moderate
3
The mean wake after sleep onset in the ramelteon groups was
3.50 minutes higher
(2.77 to 4.23 higher)
392
(2 study)
A,D
Wake After Sleep Onset
(Subjective)
⊕⊕⊝⊝
low
3,6
The mean wake after sleep onset in the ramelteon groups was
5.23 minutes higher
(6.77 lower to 17.24 higher)
605
(2 studies)
B,D
Quality of Sleep*
(Subjective)
⊕⊕⊝⊝
low
1,3
The mean quality of sleep in the ramelteon groups was
0.04 points lower
5
(0.13 lower to 0.05 higher)
805
(3 studies)
B,C,D
Sleep Efficiency
(PSG)
⊕⊕⊝⊝
low
3,4
The mean sleep efficiency in the ramelteon groups was
1.93 percent higher
(1.00 to 2.87 higher)
592
(3 studies)
A,C,D
Number of Awakenings
(Subjective)
⊕⊕⊕⊝
moderate
3
The mean number of awakenings in the ramelteon group was
0.12 awakenings higher
(0.08 to 0.15 higher)
335
(1 study)
B
* Critical Outcome, used to determine Quality of Evidence
1
Heterogeneity (I² = 98%) is greater than allowance (75%)
2
95% CI (-12.75, -6.38) crosses Clinical Significance (10 min)
3
All studies funded by industry
4
Heterogeneity (I² = 93%) greater than allowance (75%)
5
7-point Likert scale (1=excellent, 7=very poor)
6
Heterogeneity (I² =100%) greater than allowance (75%)
7
Heterogeneity (I² =99%) greater than allowance (75%)
8
95% CI (-21.45, 2.90) crossses Clinical Significance (20 min)
Doxepin - Meta-Analyses and Summary of Findings Tables
Figure S4952 – Meta-analysis of data for PSG-determined sleep latency in response to doxepin 3 mg
Figure S53 – Meta-analysis of data for subjectively-determined sleep latency in response to doxepin 3 mg
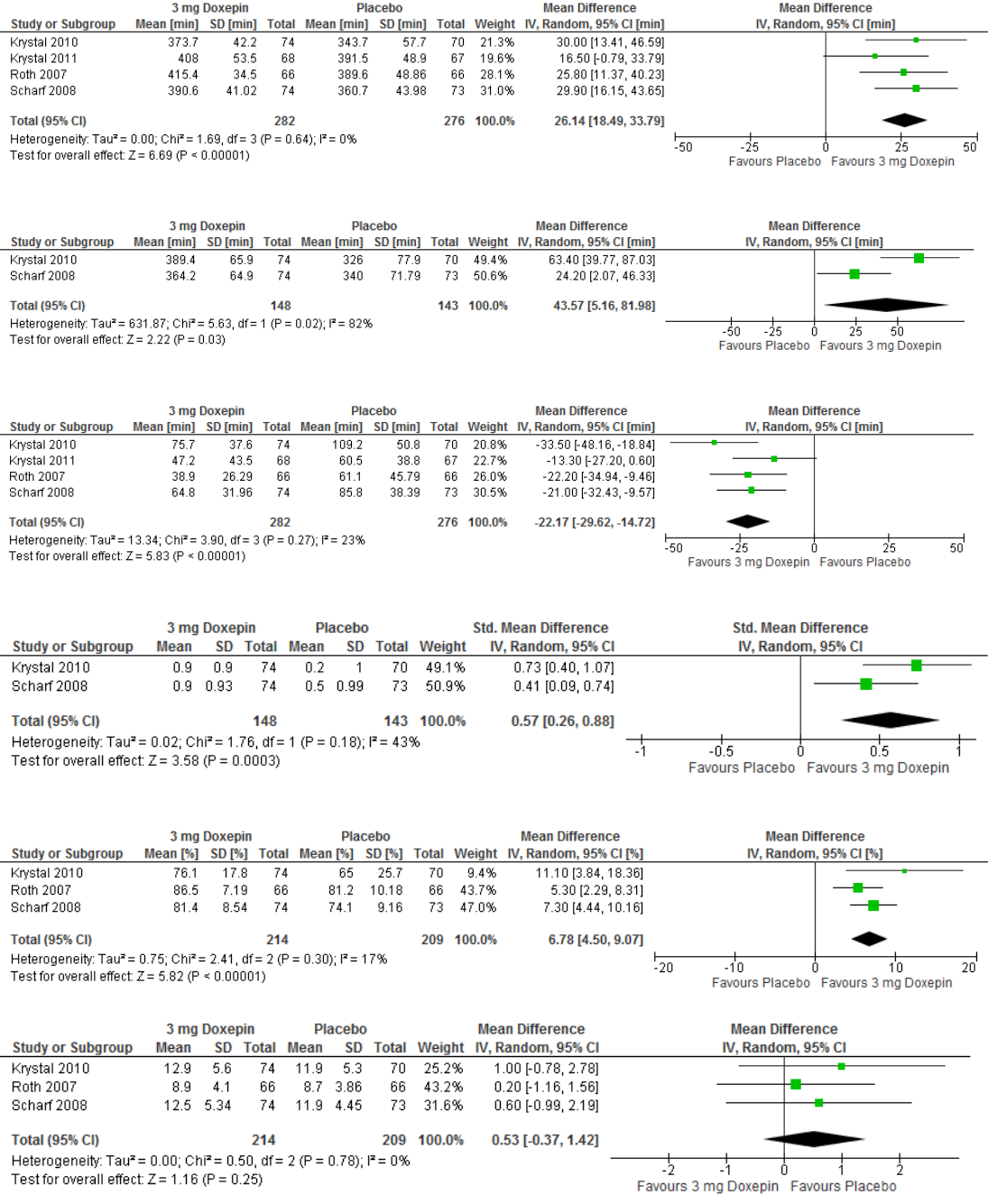
Figure S54 – Meta-analysis of data for PSG-determined total sleep time in response to doxepin 3 mg
Figure S55 – Meta-analysis of data for subjectively-determined total sleep time in response to doxepin 3 mg
Figure S56 – Meta-analysis of data for PSG-determined wake after sleep onset in response to doxepin 3 mg
Figure S57 – Meta-analysis of data for subjectively-determined quality of sleep in response to doxepin 3 mg
Figure S58 – Meta-analysis of data for PSG-determined sleep efficiency in response to doxepin 3 mg
Figure S59 – Meta-analysis of data for PSG-determined number of awakenings in response to doxepin 3 mg
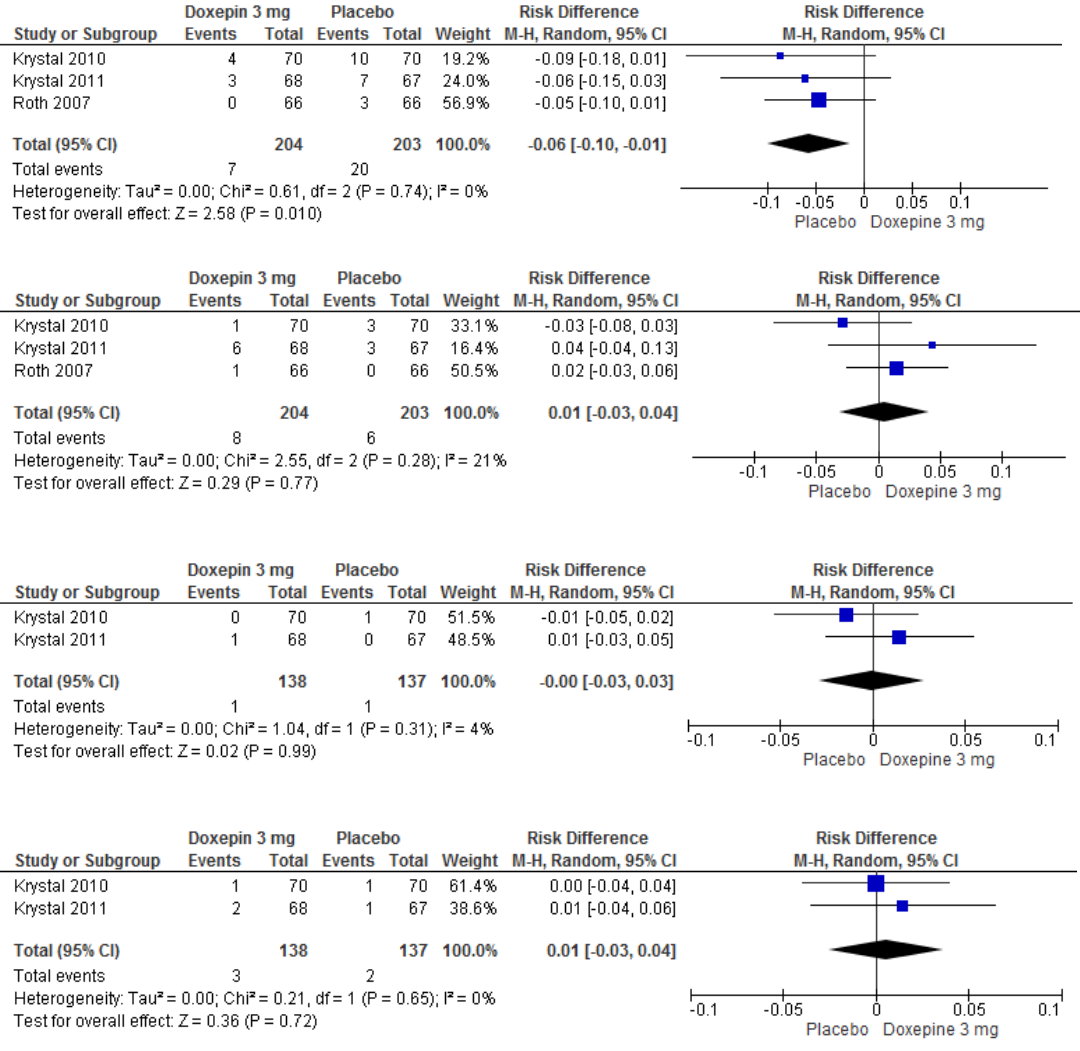
Figure S60 – Meta-analysis of data for the occurrence of headache in response to doxepin 3 mg
Figure S61 – Meta-analysis of data for the occurrence of somnolence in response to doxepin 3 mg
Figure S62 – Meta-analysis of data for the occurrence of diarrhea in response to doxepin 3 mg
Figure S63 – Meta-analysis of data for the occurrence of upper respiratory tract infection in response to doxepin 3 mg
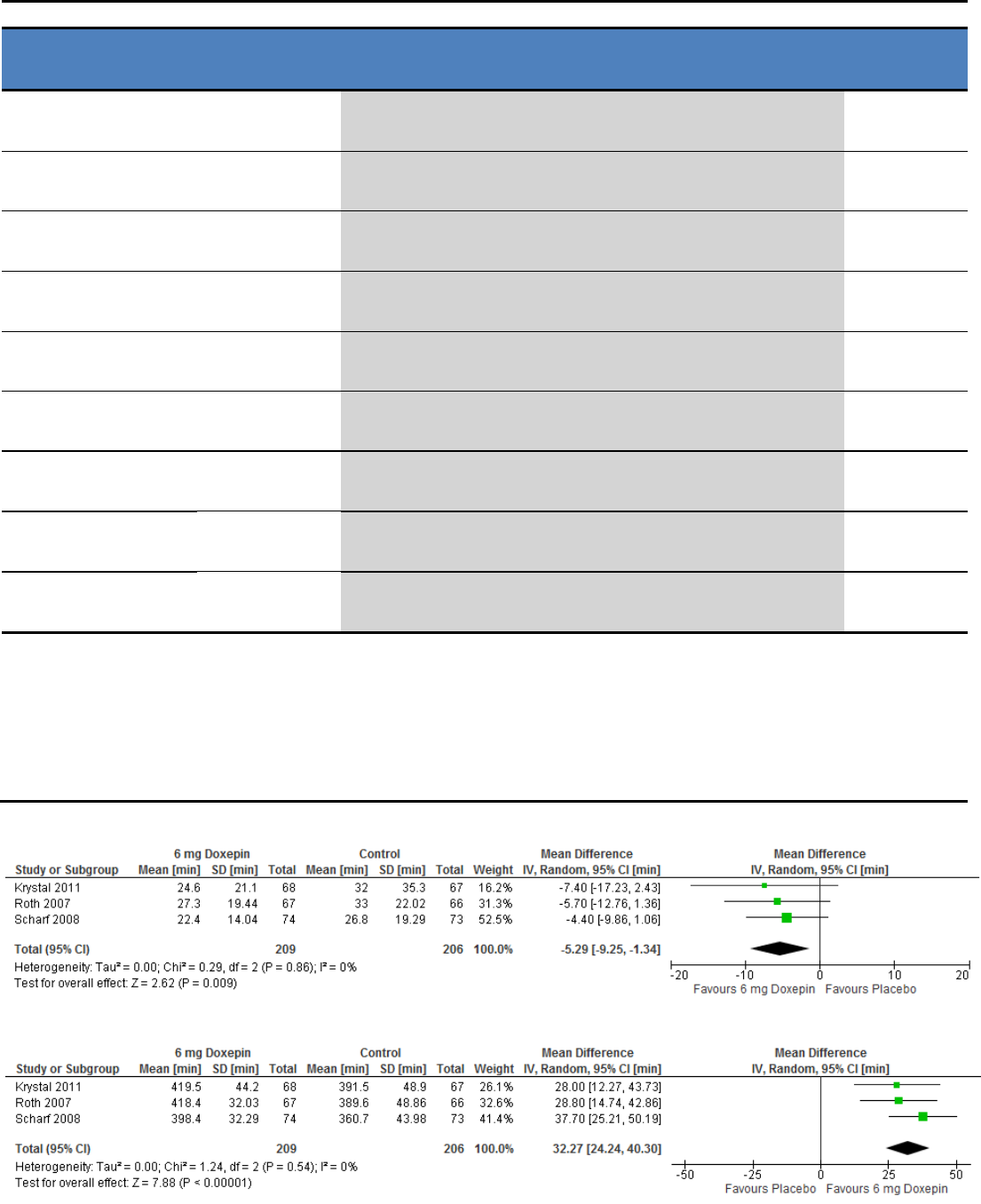
Table S15 – Summary of Findings table for doxepin 3 mg for the treatment of chronic insomnia
References: Krystal 2010(A); Krystal 2011(B); Roth 2007(C); Scharf 2008(D)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
3 mg Doxepin vs Placebo
No of
Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊕⊝
moderate
1
The mean sleep latency in the doxepin groups was
2.3 minutes lower
(6.22 lower to 1.62 higher)
558
(4 studies)
A,B,C,D
Sleep Latency
(Subjective)
⊕⊕⊝⊝
low
1,6
The mean sleep latency in the doxepin groups was
9.35 minutes lower
(21.89 lower to 3.19 higher)
291
(2 studies)
A,D
Total Sleep Time*
(PSG)
⊕⊕⊝⊝
low
1,3
The mean total sleep time in the doxepin groups was
26.14 minutes higher
(18.49 to 33.79 higher)
558
(4 studies)
A,B,C,D
Total Sleep Time
(Subjective)
⊕⊝⊝⊝
very low
1,7,8
The mean total sleep time in the doxepin groups was
43.57 minutes higher
(5.16 to 81.98 higher)
291
(2 studies)
A,D
Wake After Sleep Onset*
(PSG)
⊕⊕⊝⊝
low
1,2
The mean wake after sleep onset in the doxepin groups was
22.17 minutes lower
(29.62 to 14.72 lower)
558
(4 studies)
A,B,C,D
Wake After Sleep Onset
(Subjective)
⊕⊕⊝⊝
low
1,9
The mean wake after sleep onset in the doxepin group was
20.0 minutes lower
(39.07 to 0.92 lower)
147
(1 study)
D
Quality of Sleep*
(Subjective)
⊕⊕⊝⊝
low
1,5
The mean quality of sleep in the doxepin groups was
0.57 standard deviations higher
(0.26 to 0.88 higher)
291
(2 studies)
A,D
Sleep Efficiency
(PSG)
⊕⊕⊝⊝
low
1,4
The mean sleep efficiency in the doxepin groups was
6.78 percent higher
(4.5 to 9.07 higher)
423
(3 studies)
A,C,D
Number of Awakenings
(PSG)
⊕⊕⊕⊝
moderate
1
The mean number of awakenings in the doxepin groups was
0.53 awakenings higher
(0.37 lower to 1.42 higher)
423
(3 studies)
A,C,D
* Critical Outcome, used to determine Quality of Evidence
1
All studies funded by Industry
2
95% CI (-29.62, -14.72) crosses Clinical Significance (20 min)
3
95% CI (18.49, 33.79) crosses Clinical Significance (20 min)
4
95% CI (4.50, 9.07) crosses Clinical Significance (5%)
5
95% CI (0.26, 0.88) crosses Clinical Significance (SMD 0.5)
6
95% CI (-21.89, 3.19) crosses Clinical Significance (20 min)
7
Heterogeneity (I² = 82%) greater than allowance (75%)
8
95% CI (5.16, 81.98) crosses Clinical Significance (30 min)
9
95% CI (-39.07, -0.92) crosses Clinical Significance (30 min)
Figure S64 – Meta-analysis of data for PSG-determined sleep latency in response to doxepin 6 mg
Figure S65 – Meta-analysis of data for PSG-determined total sleep time in response to doxepin 6 mg
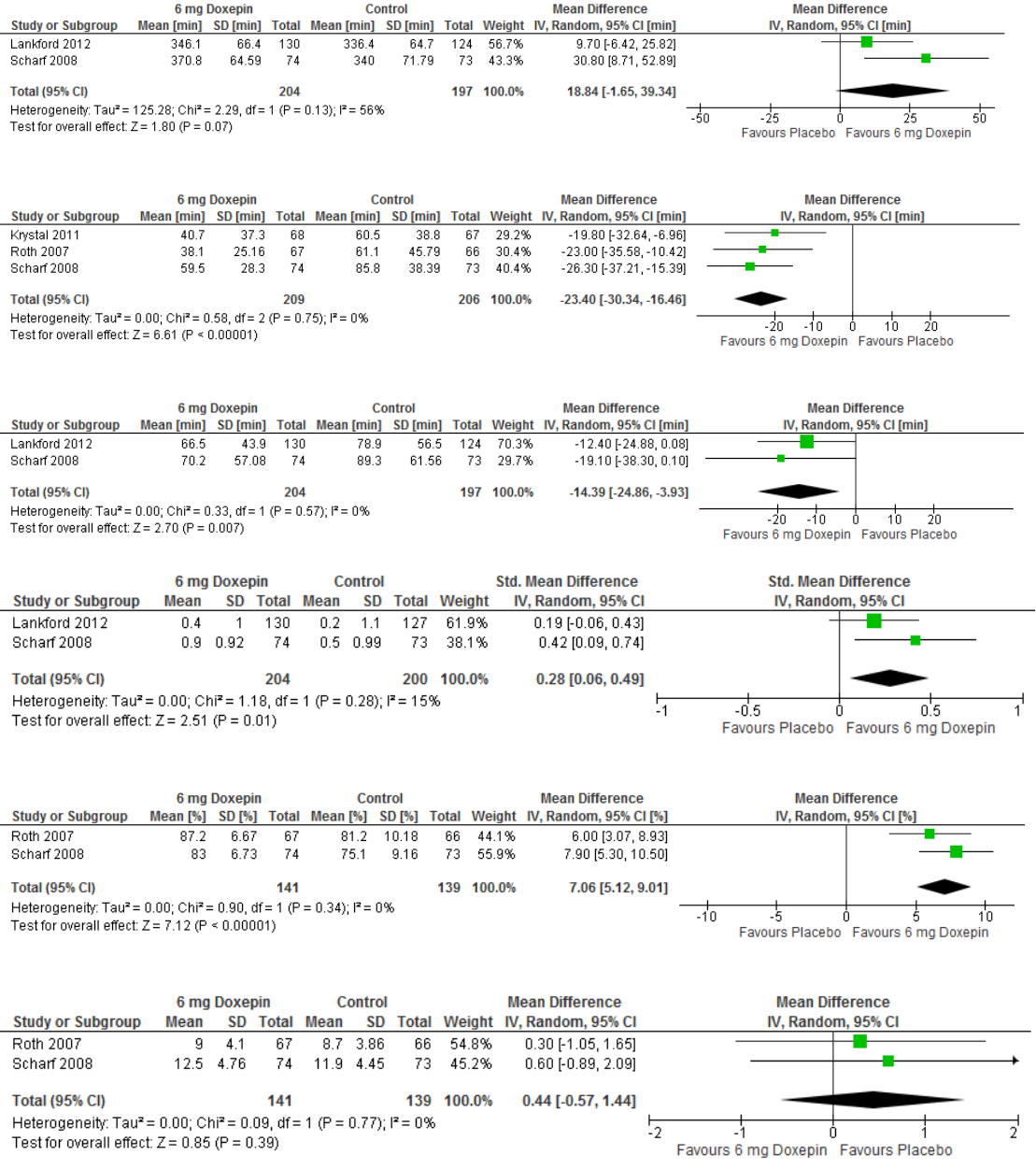
Figure S66 – Meta-analysis of data for subjectively-determined total sleep time in response to doxepin 6 mg
Figure S67 – Meta-analysis of data for PSG-determined wake after sleep onset in response to doxepin 6 mg
Figure S68 – Meta-analysis of data for subjectively-determined wake after sleep onset in response to doxepin 6 mg
Figure S69 – Meta-analysis of data for subjectively-determined quality of sleep in response to doxepin 6 mg
Figure S70 – Meta-analysis of data for PSG-determined sleep efficiency in response to doxepin 6 mg
Figure S71 – Meta-analysis of data for PSG-determined number of awakenings in response to doxepin 6 mg
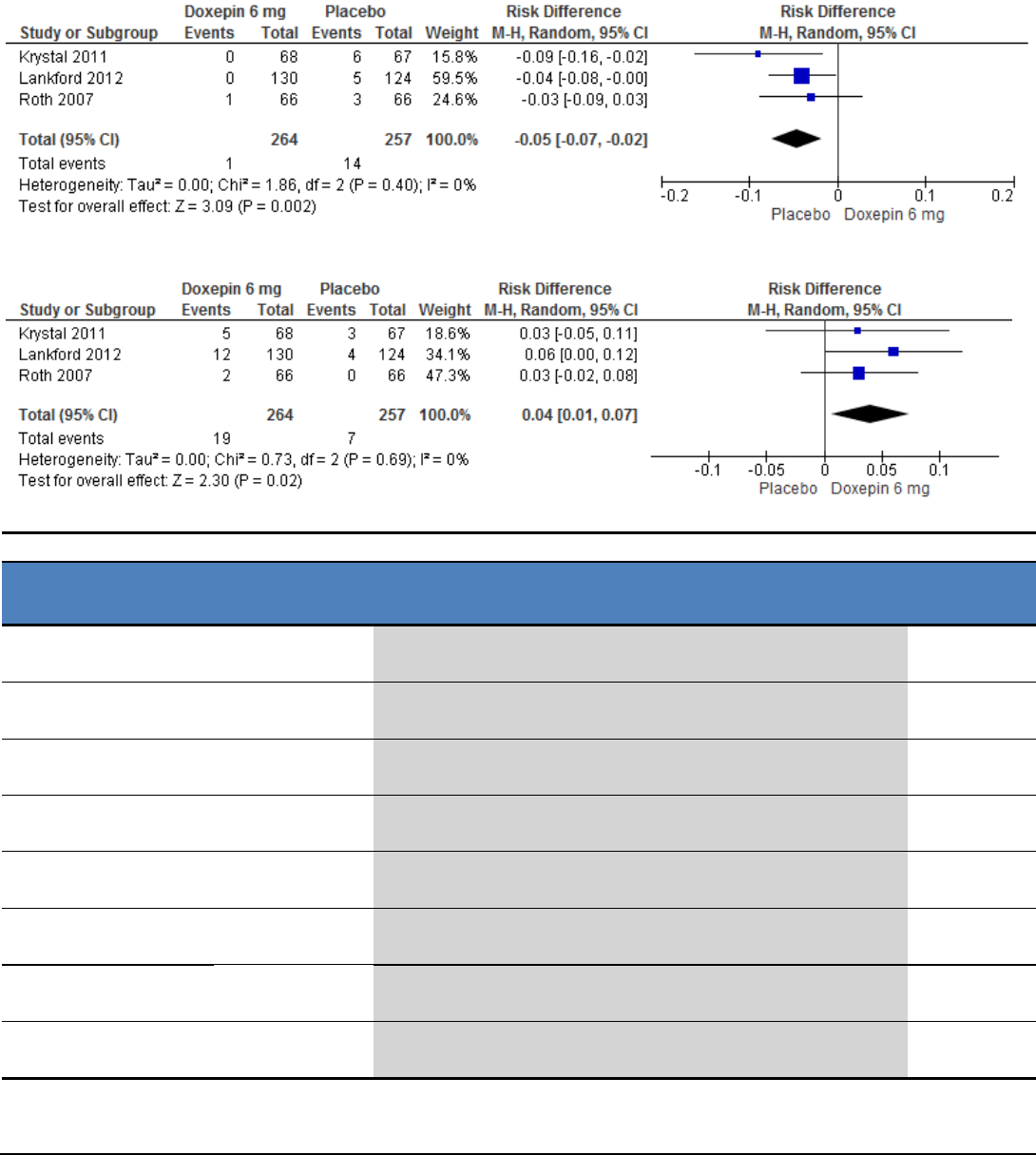
Figure S72 – Meta-analysis of data for the occurrence of headache in response to doxepin 6 mg
Figure S73 – Meta-analysis of data for the occurrence of somnolence in response to doxepin 6 mg
Table S16 – Summary of Findings table for doxepin 6 mg for the treatment of chronic insomnia
References: Krystal 2011(A); Roth 2007(B); Lankford 2012(C); Scharf 2008(D)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
6 mg Doxepin vs Placebo
No of
Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊕⊝
moderate
1
The mean sleep latency in the doxepin groups was
5.29 minutes lower
(9.25 to 1.34 lower)
415
(3 studies)
A,B,D
Total Sleep Time*
(PSG)
⊕⊕⊕⊝
moderate
1
The mean total sleep time in the doxepin groups was
32.27 minutes higher
(24.24 to 40.3 higher)
415
(3 studies)
A,B,D
Total Sleep Time
(Subjective)
⊕⊕⊝⊝
low
1,3
The mean total sleep time in the doxepin groups was
18.84 minutes higher
(1.65 lower to 39.34 higher)
401
(2 studies)
C,D
Wake After Sleep Onset*
(PSG)
⊕⊕⊝⊝
low
1,2
The mean wake after sleep onset in the doxepin groups was
23.4 minutes lower
(30.34 to 16.46 lower)
415
(3 studies)
A,B,D
Wake After Sleep Onset
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean wake after sleep onset in the doxepin groups was
14.39 minutes lower
(24.86 to 3.93 lower)
401
(2 studies)
C,D
Quality of Sleep*
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean quality of sleep in the doxepin groups was
0.28 standard deviations higher
(0.06 to 0.49 higher)
404
(2 studies)
C,D
Sleep Efficiency
(PSG)
⊕⊕⊕⊝
moderate
1
The mean sleep efficiency in the doxepin groups was
7.06 percent higher
(5.12 to 9.01 higher)
280
(2 studies)
B,D
Number of Awakenings
(PSG)
⊕⊕⊕⊝
moderate
1
The mean number of awakenings in the doxepin groups was
0.44 awakenings higher
(0.57 lower to 1.44 higher)
280
(2 studies)
B,D
* Critical Outcome, used to determine Quality of Evidence
1
All studies funded by industry
2
95% CI (-30.34, -16.46) crosses Clinical Significance (20 min)
3
95% CI (-1.65, 39.34) crosses Clinical Significance (30 min)

Trazadone - Summary of Findings Table
Table S17 – Summary of Findings table for trazodone 50 mg for the treatment of chronic insomnia
References: Walsh 1998(A)
Outcomes
Quality of the evidence
(GRADE)
Absolute Difference
50 mg Trazadone vs Placebo
No of
Participants
(studies)
Sleep Latency*
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean sleep latency in the trazadone group was
10.20 minutes lower
(11.44 to 8.95 lower)
187
(1 study)
A
Total Sleep Time*
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean total sleep time in the trazadone group was
21.80 minutes higher
(20.10 to 23.49 higher)
187
(1 study)
A
Wake After Sleep Onset*
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean wake after sleep onset in the trazadone group was
7.70 minutes lower
(8.89 to 6.5 lower)
187
(1 study)
A
Quality of Sleep*
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean quality of sleep in the trazadone group was
0.13 points
2
lower
(0.14 to 0.11 lower)
187
(1 study)
A
Number of Awakenings
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean number of awakenings in the trazadone group was
0.40 awakenings lower
(0.42 to 0.37 lower)
187
(1 study)
A
* Critical Outcome, used to determine Quality of Evidence
1
Study funded by industry
2
4-point scale (1=Excellent, 4=Poor)
Tiagabine - Meta-Analyses and Summary of Findings Tables
Figure S74 – Meta-analysis of data for PSG-determined sleep latency in response to tiagabine 4 mg
Figure S75 – Meta-analysis of data for subjectively-determined sleep latency in response to tiagabine 4 mg
Figure S76 – Meta-analysis of data for PSG-determined total sleep time in response to tiagabine 4 mg
Figure S77 – Meta-analysis of data for subjectively-determined total sleep time in response to tiagabine 4 mg
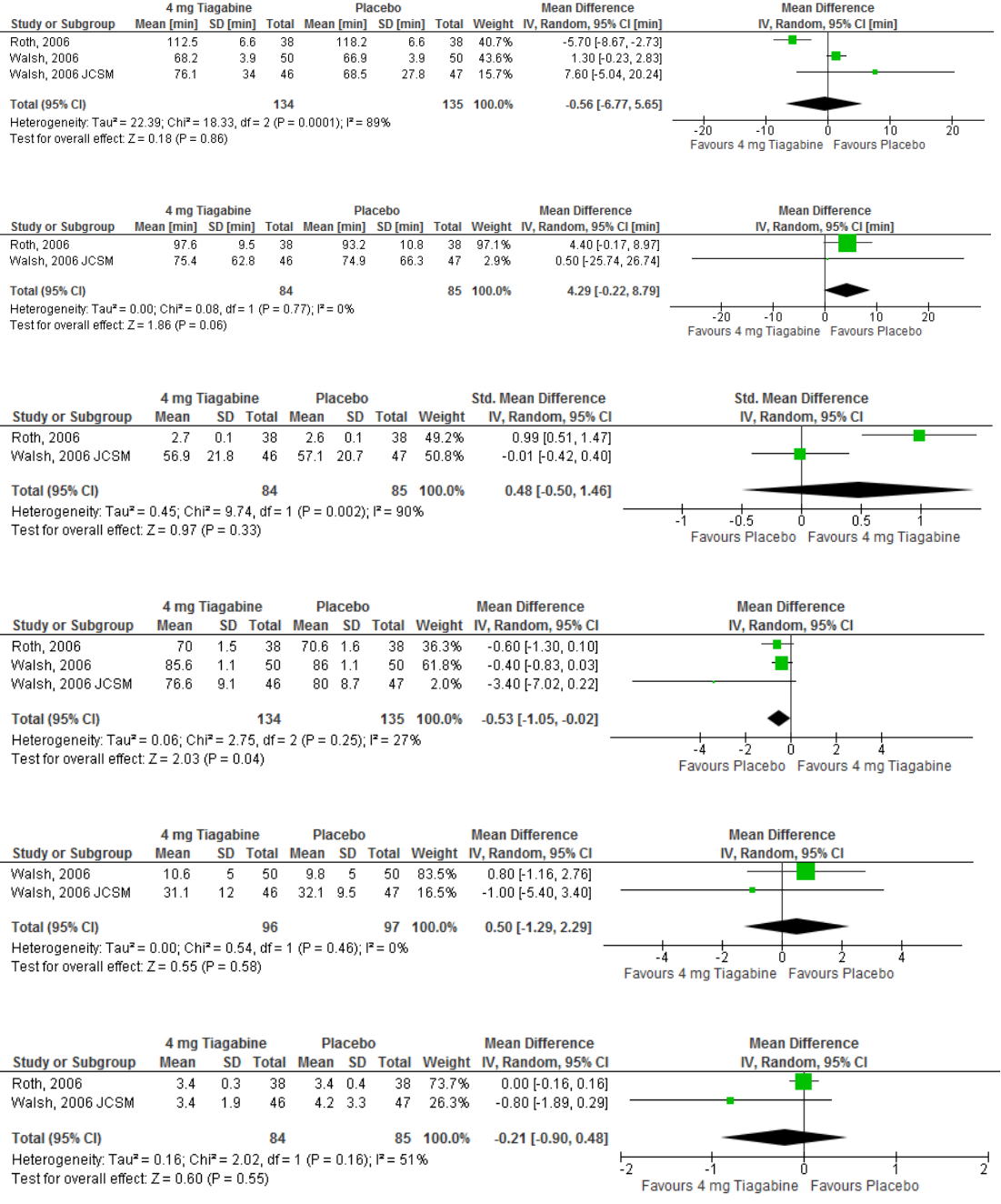
Figure S78 – Meta-analysis of data for PSG-determined wake after sleep onset in response to tiagabine 4 mg
Figure S79 – Meta-analysis of data for subjectively-determined wake after sleep onset in response to tiagabine 4 mg
Figure S80 – Meta-analysis of data for subjectively-determined quality of sleep in response to tiagabine 4 mg
Figure S81 – Meta-analysis of data for PSG-determined sleep efficiency in response to tiagabine 4 mg
Figure S82 – Meta-analysis of data for PSG-determined number of awakenings in response to tiagabine 4 mg
Figure S83 – Meta-analysis of data for subjectively-determined number of awakenings in response to tiagabine 4 mg
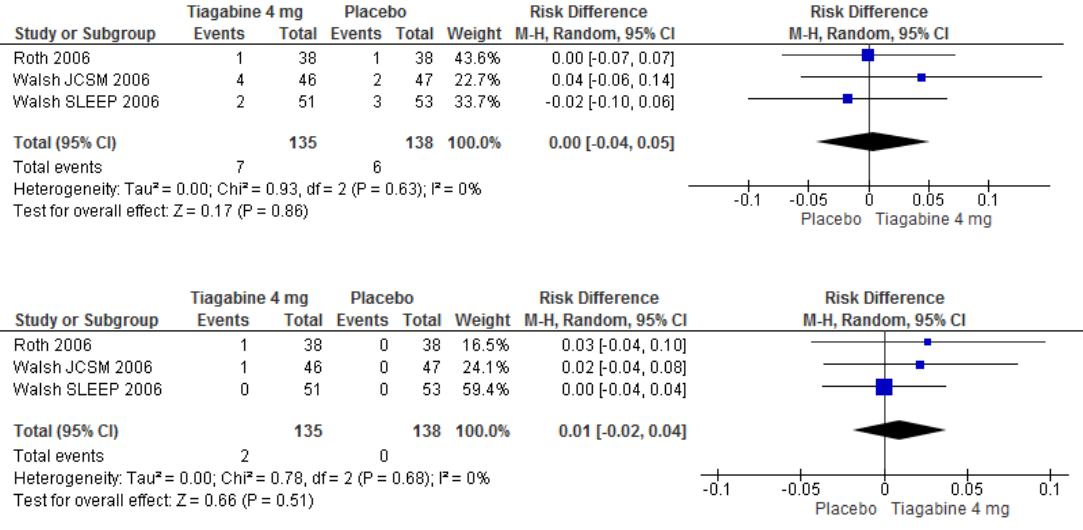
Figure S84 – Meta-analysis of data for the occurrence of headache in response to tiagabine 4 mg
Figure S85 – Meta-analysis of data for the occurrence of nausea in response to tiagabine 4 mg
Table S18 – Summary of Findings table for tiagabine 4 mg for the treatment of chronic insomnia
References: Roth 2006(A); Walsh 2006(B); Walsh 2006 JCSM(C)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
4 mg Tiagabine vs Placebo
No of Participants
(studies)
Sleep Latency
(PSG)
⊕⊝⊝⊝
very low
1,2,3
The mean sleep latency in the tiagabine groups was
3.65 minutes higher
(8 lower to 15.31 higher)
269
(3 studies)
A,B,C
Sleep Latency
(Subjective)
⊕⊕⊕⊝
moderate
3
The mean sleep latency in the tiagabine groups was
13.31 minutes higher
(7.54 to 19.07 higher)
139
(2 studies)
A,C
Total Sleep Time*
(PSG)
⊕⊕⊝⊝
low
3,5
The mean total sleep time in the tiagabine groups was
1.21 minutes lower
(7.44 lower to 5.02 higher)
269
(3 studies)
A,B,C
Total Sleep Time
(Subjective)
⊕⊕⊕⊝
moderate
3
The mean total sleep time in the tiagabine groups was
19.95 minutes lower
(25.35 to 14.54 lower)
169
(2 studies)
A,C
Wake After Sleep Onset*
(PSG)
⊕⊕⊝⊝
low
3,4
The mean wake after sleep onset in the tiagabine groups was
0.56 minutes lower
(6.77 lower to 5.65 higher)
269
(3 studies)
A,B,C
Wake After Sleep Onset
(Subjective)
⊕⊕⊕⊝
moderate
3
The mean wake after sleep onset in the tiagabine groups was
4.29 minutes higher
(0.22 lower to 8.79 higher)
169
(2 studies)
A,C
Quality of Sleep*
(Subjective)
⊕⊝⊝⊝
very low
3,7,8
The mean quality of sleep in the tiagabine groups was
0.48 standard deviations higher
(0.5 lower to 1.46 higher)
169
(2 studies)
A,C
Sleep Efficiency
(PSG)
⊕⊕⊕⊝
moderate
3
The mean sleep efficiency in the tiagabine groups was
0.53 percent lower
(1.05 to 0.02 lower)
269
(3 studies)
A,B,C
Number of Awakenings
(PSG)
⊕⊕⊝⊝
low
3,6
The mean number of awakenings in the tiagabine groups was
0.5 awakenings higher
(1.29 lower to 2.29 higher)
193
(2 studies)
B,C
Number of Awakenings
(Subjective)
⊕⊕⊝⊝
low
3,9
The mean number of awakenings in the tiagabine groups was
0.21 awakenings lower
(0.9 lower to 0.48 higher)
169
(2 studies)
A,C
* Critical Outcome, used to determine Quality of Evidence
1
Heterogeneity (I² = 99%) greater than allowance (75%)
2
95% CI (-8.0, 15.31) crosses Clinical Significance (10 min)
3
All studies funded by industry
4
Heterogeneity (I² = 89%) greater than allowance (75%)
5
Heterogeneity (I² = 85%) greater than allowance (75%)
6
95% CI (-1.29, 2.29) crosses Clinical Significance (2 awakenings)
7
Heterogeneity (I² = 90%) greater than allowance (75%)
8
95% CI (-0.50, 1.46) crosses zero standard mean difference
9
95% CI (-0.90, 0.48) crosses Clinical Significance (0.5 awakenings)
Table S19 – Summary of Findings table for tiagabine 6 mg for the treatment of chronic insomnia
References: Roth 2006(A); Walsh 2006 JCSM(B)
Outcomes
Quality of the evidence
(GRADE)
Absolute Difference
6 mg Tiagabine vs Placebo
No of Participants
(studies)
Sleep Latency
(PSG)
⊕⊕⊝⊝
low
3,7
The mean sleep latency in the tiagabine groups was
6.9 minutes higher
(2.22 to 11.58 higher)
175
(2 studies)
A,B
Sleep Latency
(Subjective)
⊕⊕⊕⊝
moderate
3
The mean sleep latency in the tiagabine groups was
5.68 minutes higher
(3.05 to 8.3 higher)
175
(2 studies)
A,B
Total Sleep Time*
(PSG)
⊕⊕⊕⊝
moderate
3
The mean total sleep time in the tiagabine groups was
7.17 minutes higher
(0.26 lower to 14.59 higher)
175
(2 studies)
A,B
Total Sleep Time
(Subjective)
⊕⊕⊕⊝
moderate
3
The mean total sleep time in the tiagabine groups was
9.65 minutes lower
(14.05 to 5.25 lower)
175
(2 studies)
A,B
Wake After Sleep Onset*
(PSG)
⊕⊝⊝⊝
very low
1,2,3
The mean wake after sleep onset in the tiagabine groups was
9.24 minutes lower
(24.78 lower to 6.3 higher)
175
(2 studies)
A,B
Wake After Sleep Onset
(Subjective)
⊕⊕⊕⊝
moderate
3
The mean wake after sleep onset in the tiagabine groups was
5.68 minutes higher
(3.05 to 8.3 higher)
175
(2 studies)
A,B
Quality of Sleep*
(Subjective)
⊕⊕⊝⊝
low
3,4
The mean quality of sleep in the tiagabine groups was
0.01 standard deviations higher
(0.28 lower to 0.31 higher)
175
(2 studies)
A,B
Sleep Efficiency
(PSG)
⊕⊕⊕⊝
moderate
3
The mean sleep efficiency in the tiagabine groups was
1.46 percent higher
(0.15 lower to 3.06 higher)
175
(2 studies)
A,B
Number of Awakenings
(Subjective)
⊕⊝⊝⊝
very low
3,5,6
The mean number of awakenings in the tiagabine groups was
0.49 awakenings lower
(1.84 lower to 0.87 higher)
175
(2 studies)
A,B
* Critical Outcome, used to determine Quality of Evidence
1
Heterogeneity (I² = 81%) crosses threshold (75%)
2
95% CI (-24.78, 6.30) crosses Clinical Significance (20 min)
3
All studies funded by industry
4
95% CI (-0.28, 0.31) crosses zero standard mean difference
5
Heterogeneity (I² = 83%) crosses threshold (75%)
6
95% CI (-1.84, 0.87) crosses Clinical Significance (0.5 awakenings)
7
95% CI (2.22, 11.58) crosses Clinical Significance (10 min)
Table S20 – Summary of Findings table for tiagabine 8 mg for the treatment of chronic insomnia
References: Roth 2006(A); Walsh 2006(B); Walsh 2006 JCSM(C)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
6 mg Tiagabine vs Placebo
No of Participants
(studies)
Sleep Latency
(PSG)
⊕⊕⊕⊝
moderate
1
The mean sleep latency in the tiagabine groups was
1.22 minutes lower
(2.66 lower to 0.22 higher)
271
(3 studies)
A,B,C
Sleep Latency
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean sleep latency in the tiagabine groups was
2.12 minutes lower
(3.48 to 0.76 lower)
171
(2 studies)
A,C
Total Sleep Time*
(PSG)
⊕⊕⊝⊝
low
1,3
The mean total sleep time in the tiagabine groups was
3.49 minutes higher
(6.43 lower to 13.42 higher)
271
(3 studies)
A,B,C
Total Sleep Time
(Subjective)
⊕⊝⊝⊝
very low
1,7,8
The mean total sleep time in the tiagabine groups was
16.09 minutes lower
(44.97 lower to 12.79 higher)
171
(2 studies)
A,C
Wake After Sleep Onset*
(PSG)
⊕⊕⊝⊝
low
1,2
The mean wake after sleep onset in the tiagabine groups was
2.42 minutes lower
(10.35 lower to 5.51 higher)
271
(3 studies)
A,B,C
Wake After Sleep Onset
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean wake after sleep onset in the tiagabine groups was
9.71 minutes higher
(5.7 to 13.72 higher)
171
(2 studies)
A,C
Quality of Sleep*
(Subjective)
⊕⊝⊝⊝
very low
1,5,6
The mean quality of sleep in the tiagabine groups was
0.37 standard deviations higher
(0.65 lower to 1.39 higher)
171
(2 studies)
A,C
Sleep Efficiency
(PSG)
⊕⊕⊝⊝
low
1,3
The mean sleep efficiency in the tiagabine groups was
0.68 percent higher
(1.41 lower to 2.76 higher)
271
(3 studies)
A,B,C
Number of Awakenings
(PSG)
⊕⊕⊝⊝
low
1,4
The mean number of awakenings in the tiagabine groups was
0.88 awakenings lower
(3.7 lower to 1.95 higher)
192
(2 studies)
B,C
Number of Awakenings
(Subjective)
⊕⊕⊝⊝
low
1,9
The mean number of awakenings in the tiagabine groups was
0.3 awakenings higher
(0.38 lower to 0.98 higher)
171
(2 studies)
A,C
* Critical Outcome, used to determine Quality of Evidence
1
All studies funded by industry
2
Heterogeneity (I² = 93%) greater than allowance (75%)
3
Heterogeneity (I² = 94%) greater than allowance (75%)
4
95% CI (-3.70, 1.95) crosses Clinical Significance (2 awakenings)
5
Heterogeneity (I² = 91%) greater than allowance (75%)
6
95% CI (-0.65, 1.39) crosses zero standard mean difference
7
Heterogeneity (I² = 89%) greater than allowance (75%)
8
95% CI (-44.97, 12.79) crosses Clinical Significance
9
95% CI (-0.38, 0.98) crosses Clinical Significance (0.5 awakenings)
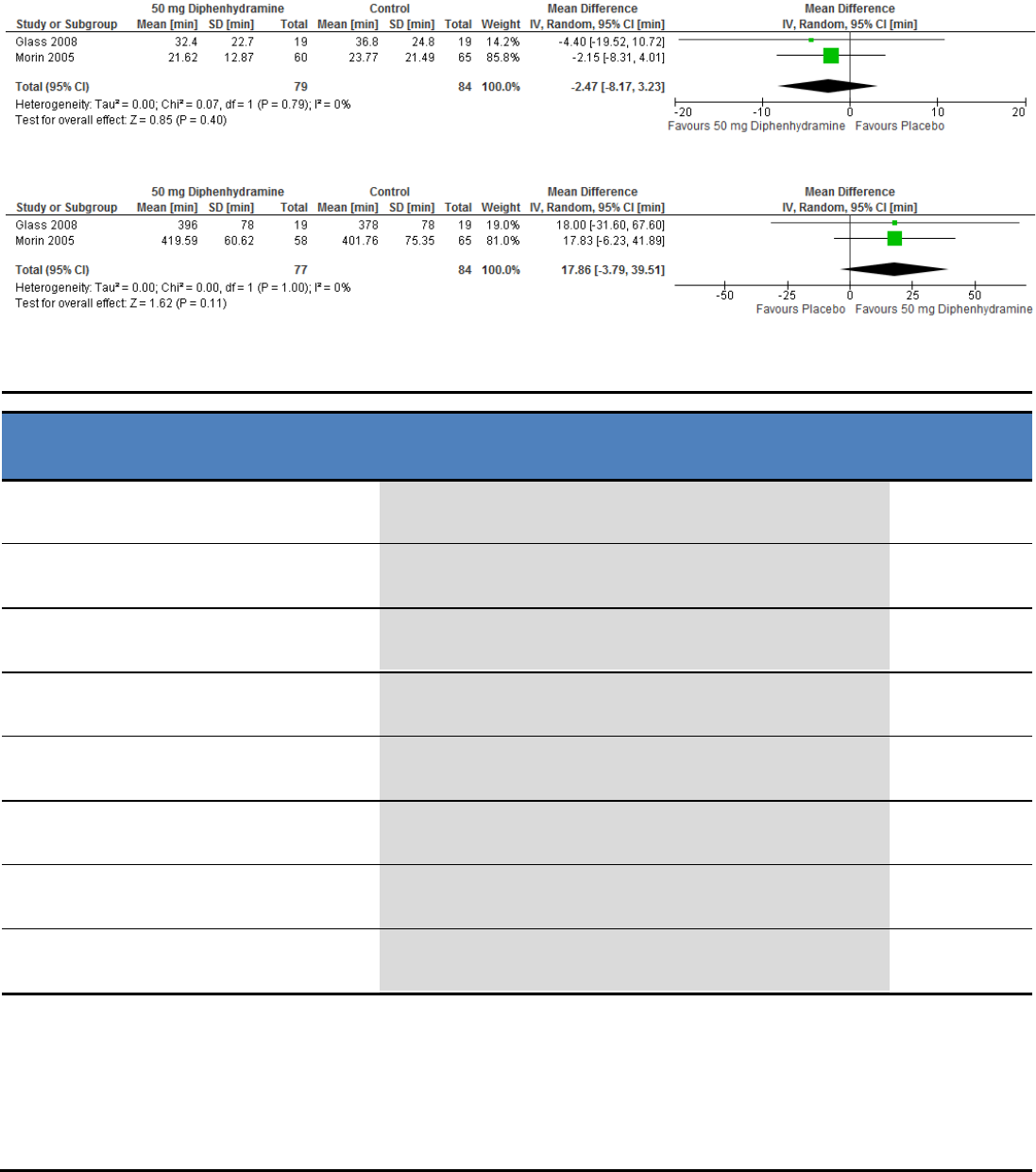
Diphenhydramine - Meta-Analyses and Summary of Findings Table
Figure S86 – Meta-analysis of data for subjectively-determined sleep latency in response to diphenhydramine 50 mg
Figure S87 – Meta-analysis of data for subjectively-determined total sleep time in response to diphenhydramine 50 mg
Table S21 – Summary of Findings table for diphenhydramine 50 mg for the treatment of chronic insomnia
References: Glass 2008(A); Morin 2005(B)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
50 mg Diphenhydramine vs Placebo
No of Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊝⊝
low
5,7
The mean sleep latency in the diphenhydramine group was
7.89 minutes lower
(17.40 lower to 1.62 higher)
52
(1 study)
A
Sleep Latency
(Subjective)
⊕⊕⊝⊝
low
1,2
The mean sleep latency in the diphenhydramine groups was
2.47 minutes lower
(8.17 lower to 3.23 higher)
163
(2 studies)
A,B
Total Sleep Time*
(PSG)
⊕⊕⊝⊝
low
5,8
The mean total sleep time in the diphenhydramine group was
12.37 minutes higher
(13.38 lower to 38.12 higher)
52
(1 study)
A
Total Sleep Time
(Subjective)
⊕⊕⊝⊝
low
1,2
The mean total sleep time in the diphenhydramine groups was
17.86 minutes higher
(3.79 lower to 39.51 higher)
161
(2 studies)
A,B
Quality of Sleep*
(Subjective)
⊕⊕⊕⊝
moderate
5
The mean quality of sleep in the diphenhydramine group was
0.1 points
9
higher
(0.45 lower to 0.65 higher)
38
(1 study)
A
Sleep Efficiency
(PSG)
⊕⊕⊝⊝
low
4,5
The mean sleep efficiency in the diphenhydramine group was
2.59 percent higher
(3.25 lower to 8.43 higher)
52
(1 study)
B
Sleep Efficiency
(Subjective)
⊕⊕⊕⊝
moderate
5
The mean sleep efficiency in the diphenhydramine group was
4.61 percent higher
(1.33 to 7.88 higher)
123
(1 study)
A
Number of Awakenings
(Subjective)
⊕⊕⊕⊝
moderate
3
The mean number of awakenings in the diphenhydramine group was
0.3 awakenings lower
(1.03 lower to 0.43 higher)
38
(1 study)
A
* Critical Outcome, used to determine Quality of Evidence
1
SL and TST 95% Ci cross Clinical Significance
2
1 of 2 studies funded by industry
3
95% CI (-1.03, 0.43) crosses Clinical Significance (0.5 awakenings)
4
95% CI (-3.25, 8.43) crosses Clinical Significance (5%)
5
Study funded by industry
6
95% CI (-0.45, 0.65) crosses zero standard mean difference
7
95% CI (-17.4, 1.62) crosses Clinical Significance (10 minutes)
8
95% CI (-13.38, 38.12) crosses Clinical Significance (20 minutes)
9
5-point scale (higher score indicates better sleep quality)
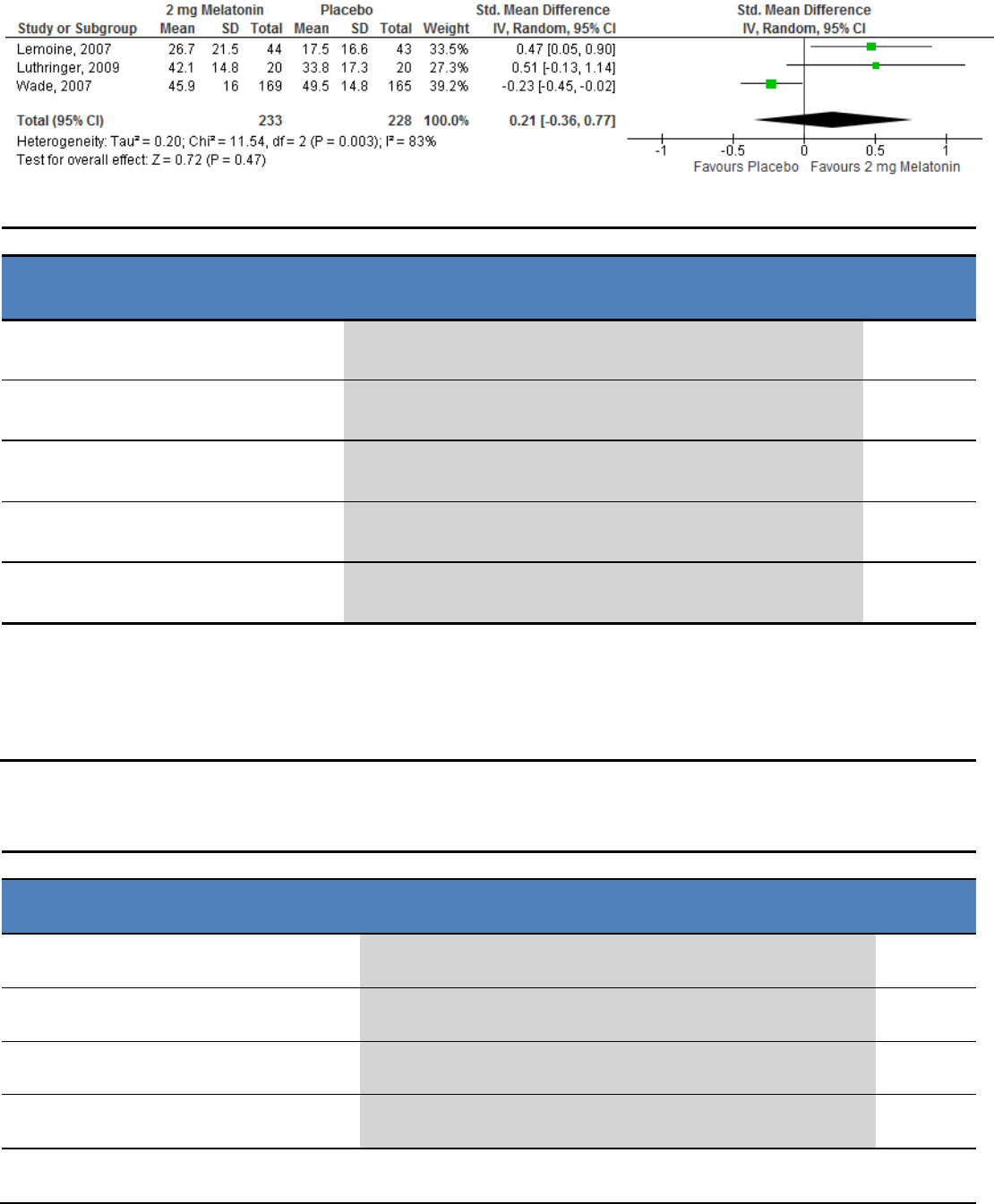
Melatonin - Meta-Analyses and Summary of Findings Tables
Figure S88 – Meta-analysis of data for subjectively-determined quality of sleep in response to melatonin 2 mg
Table S22 – Summary of Findings table for melatonin 2 mg for the treatment of chronic insomnia
References: Lemoine 2007(A); Luthringer 2009(B); Wade 2007(C)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
2 mg Melatonin vs Placebo
No of
Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊝⊝
low
3,4
The mean sleep latency in the melatonin group was
8.9 minutes lower
(15.45 to 2.35 lower)
40
(1 study)
B
Total Sleep Time
(PSG)
⊕⊝⊝⊝
very low
3,6
The mean total sleep time in the melatonin group was
2.2 minutes higher
(19.13 lower to 23.53 higher)
40
(1 study)
B
Wake After Sleep Onset
(PSG)
⊕⊕⊝⊝
low
3,5
The mean wake after sleep onset in the melatonin group was
8.5 minutes higher
(11.75 lower to 28.75 higher)
40
(1 study)
B
Quality of Sleep*
(Subjective)
⊕⊝⊝⊝
very low
1,2,3
The mean quality of sleep in the melatonin group was
0.21 standard deviations higher
(0.36 lower to 0.77 higher)
461
(3 studies)
A,B,C
Number of Awakenings
(PSG)
⊕⊝⊝⊝
very low
3,7
The mean number of awakenings in the melatonin group was
1.4 awakenings higher
(4.59 lower to 7.39 higher)
40
(1 study)
B
* Critical Outcome, used to determine Quality of Evidence
1
Heterogeneity (I² = 83%) greater than allowance (75%)
2
95% CI (-0.36, 0.77) crosses zero standard mean difference
3
All studies funded by industry
4
95% CI (-15.45, -2.35) crosses Clinical Significance (10 min)
5
95% CI (-11.75, 28.75) crosses Clinical Significance (20 min)
6
95% CI (-19.13, 23.53) crosses Clinical Significance (20 min)
7
95% CI (-4.59, 7.39) crosses Clinical Significance
L-tryptophan - Summary of Findings Table
Table S23 – Summary of Findings table for L-tryptophan 250 mg for the treatment of chronic insomnia
Reference: Hudson 2005
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
250 mg Tryptophan vs Placebo
No of
Participants
(studies)
Wake After Sleep Onset*
(Subjective)
⊕⊕⊕⊕
high
The mean wake after sleep onset in the Tryptophan groups was
9.70 minutes lower
(15.21 to 4.18 lower)
31
(1 study)
Total Sleep Time
(Subjective)
⊕⊕⊕⊝
moderate
1
The mean total sleep time in the Tryptophan groups was
20.00 minutes lower
(31.29 to 8.7 lower)
32
(1 study)
Quality of Sleep*
(Subjective)
⊕⊕⊕⊕
high
The mean quality of sleep in the Tryptophan groups was
0.30 points
2
higher
(0.22 to 0.37 higher)
32
(1 study)
Sleep Efficiency
(Subjective)
⊕⊕⊕⊕
high
The mean sleep efficiency in the Tryptophan groups was
2.20 percent lower
(4.27 to 0.12 lower)
32
(1 study)
* Critical Outcome, used to determine Quality of Evidence
1
95% CI (8.7, 31.29) crosses Clinical Significance (30 min)
2
3-point scale (Sleep Quality index: 1=low, 3=high)
Valerian - Summary of Findings Table
Table S24 – Summary of Findings table for valerian for the treatment of chronic insomnia
References: Morin 2005(A)
Outcomes
Quality of the
evidence
(GRADE)
Absolute Difference
Valerian-hops vs Placebo
No of
Participants
(studies)
Sleep Latency*
(PSG)
⊕⊕⊝⊝
low
1,2
The mean sleep latency in the Valerian-hops groups was
9.29 minutes lower
(18.3 to 0.27 lower)
48
(1 study)
A
Sleep Latency
(Subjective)
⊕⊕⊕⊝
moderate
2
The mean sleep latency in the Valerian-hops groups was
3.77 minutes higher
(4.47 lower to 12.01 higher)
124
(1 study)
A
Total Sleep Time
(PSG)
⊕⊝⊝⊝
very low
2,3
The mean total sleep time in the Valerian-hops groups was
10.96 minutes higher
(21.67 lower to 43.59 higher)
48
(1 study)
A
Total Sleep Time
(Subjective)
⊕⊕⊕⊝
moderate
2
The mean total sleep time in the Valerian-hops groups was
3.12 minutes higher
(22.08 lower to 28.32 higher)
123
(1 study)
A
Sleep Efficiency
(PSG)
⊕⊝⊝⊝
very low
2,4
The mean sleep efficiency in the Valerian-hops groups was
0.96 percent higher
(5.02 lower to 6.94 higher)
48
(1 study)
A
Sleep Efficiency
(Subjective)
⊕⊕⊕⊝
moderate
2
The mean sleep efficiency in the Valerian-hops groups was
1.85 percent higher
(1.9 lower to 5.6 higher)
123
(1 study)
A
* Critical Outcome, used to determine Quality of Evidence
1
95% CI (-18.3, -0.27) crosses Clinical Significance (10 min)
2
Study funded by industry
3
95% CI (-21.67, 43.59) crosses Clinical Significance (20 min)
4
95% CI (-5.02, 6.94) crosses Clinical Significance (5%)
