
Use
of
Colchicine to Treat Severe Constipation
in Developmentally Disabled Patients
Paul
S.
Frame,
MD,
Peter Dolan,
RPA,
Rakhi
Kohli,
and
Shirley
W.
Eberly, MS
Background: Patients with severe developmental disabilities often have concurrent decreased neuromuscular
tone of the gastrointestinal tract, which can lead to a weak
gag
reflex, esophageal reflux, aspiration,
and severe intractable constipation.
High
doses
of multiple laxatives are frequently needed
to
maintain
bowel
motility in these patients. Colchicine, a natural alkaloid that is primarily used for the treatment of acute
attacks of gout, causes an increase in gastrointestinal motility
by
neurogenic stimulation.
The
purpose of
this study
was
to
determine whether daily colchicine administration can improve
bowel
function and reduce
laxative use in profoundly disabled patients with severe, intractable constipation
who
currently require
large doses of multiple laxatives.
Methods:
Twelve
developmentally disabled patients
who
required three or more different laxatives to
manage their chronic constipation were selected to participate in a double-blind, crossover study.
Eleven
patients
who
completed the study received placebo treatment for 8
weeks
and colchicine treatment
for 8
weeks.
The
total number of
bowel
movements and the total number of laxatives used during each of the
two
8-week periods were compared.
Results:
Eight
of
11
patients experienced an improved
bowel
pattern while on colchicine compared with
placebo, as defined
by
an increase in total number of
bowel
movements or a decrease in total number of
rectal laxatives used.
No
clinically important complications were related to use of colchicine.
Conclusions: Colchicine appears to
be
a valuable adjunct in the management of severe intractable
constipation.
Larger,
long-term studies are needed
to
confirm these preliminary results. 0
Am
Board
Fam
Pract 1998;11:341-6.)
Constipation
is
the most common digestive com-
plaint in the United States.
In most patients
it
is
a
minor and easily managed problem. Management
of
constipation presents a difficult problem, how-
ever, in
both
the
elderly and
the
nonambulatory,
severely disabled population. Studies have shown
that
greater than
50
percent
of
patients in nursing
homes use at least one laxative daily and more than
one half
of
these laxative users took more than 60
doses
of
laxatives per month. I Death caused by in-
testinal obstruction secondary to chronic constipa-
tion has been reported in mentally and physically
handicapped patients.
2
Submitted, revised,
18
February 1998.
From Tri-County Family Medicine (PSF), Cohocton, the
Department
of
Family Medicine (PSF), and the Department
of
Biostatistics (SWE), University
of
Rochester School
of
Medicine and Dentistry, the Finger Lakes Developmental
Disabilities Services Organization (PD), and the
University
of
Rochester School
of
Medicine and Dentistry (RK), Rochester,
NY.
Address reprint requests to Paul
S.
Frame
MD,
Tri-
County Family Medicine,
25
Park
Ave,
Cohocton,
NY
14826.
This project
was
supported in part by a grant from the De-
partment
of
Family Medicine at the University
of
Rochester
School
of
Medicine and Dentistry
as
part
of
the summer re-
search fellowship program.
Constipation is frequently defined
as
having
fewer than 3 bowel movements
per
week. 1,3,4 Ex-
cessive straining during bowel movements
or
a
need for regular laxative use can also be included
in
the
definition.
The
cause
of
constipation
ap-
pears
to
be multifactor: poor dietary intake, lack
of
adequate fluids, bowel hypotonia, side effects
of
other
medications, and concomitant diseases.
Constipation
is
usually treated by eating a high-
fiber diet, increasing fluid intake, exercise, and use
oflaxatives.
Severely retarded and developmentally disabled
persons frequently have the most severe problems
with constipation, which
is
often resistant to stan-
dard modes
of
therapy.
Chronic
constipation oc-
curs in these patients for a number
of
physiologic
reasons:
(1)
they might have hypotonia and gener-
alized autonomic dysfunction, which greatly
re-
duce bowel motility;
(2)
their disabilities frequently
make them physically inactive;
(3) they might have
poor oral intake
as
a result
of
recurrent aspiration
of
gastric contents, necessitating placement
of
gas-
trostomy feeding tubes; and (4) they
might
take
other medications that aggravate constipation.
Colchicine for Constipation 341
on 29 August 2024 by guest. Protected by copyright.http://www.jabfm.org/J Am Board Fam Pract: first published as 10.3122/15572625-11-5-341 on 1 September 1998. Downloaded from

"--
The
idea for this study originated while caring
for a 34-year-old severely retarded, nonverbal,
epileptic man with diffuse hypotonia.
The
patient
had had a gastrostomy feeding tube placed because
of
recurrent aspiration and episodes
of
pneumonia.
He
had intractable constipation, which in spite
of
taking 36 doses
of
five
different laxatives per week,
receiving a high-fiber diet, and maintaining an ad-
equate fluid intake through the feeding tube peri-
odically required multiple
2-L
enemas and bisa-
codyl suppositories to get his bowels to move.
It
was noted
that
whenever the patient was
on
amoxicillin-clavulanate potassium for pulmonary
infections, his bowel function improved dramati-
cally. Diarrhea
is
a known side effect
of
this med-
ication. Amoxicillin-clavulanate potassium, how-
ever,
is
not
suitable for long-term therapy because
of
the high risk
of
developing resistant organisms.
The
beneficial effect noted with amoxicillin-clavu-
lanate potassium raised the question
of
whether
other, safer agents could be found to improve the
patient's constipation. Colchicine,
0.5
mg
three
times a day, was tried with good results.
The
pa-
tient
has had more regular bowel movements, a
decreased need for other laxatives, and
no
need for
high-volume enemas. This patient's success led to
the
hypothesis
that
colchicine could be a useful
treatment for severe refractory constipation.
Colchicine
is
an alkaloid
of
Colchicum
autumnale
(autumn crocus, meadow saffron).
It
has been used
for pain
of
articular origin since the 6th century .
AD.
It
is
currently used primarily for the treatment
of
acute attacks
of
gout,
but
it
can also be used long
term to prevent recurrent attacks
of
gout, pseudo-
gout, familial Mediterranean fever, and progres-
sion
of
amyloidosis.
The
usual dose
is
0.5
mg
to 2.0
mg
daily.5
It
is
known
to
enhance gastrointestinal
activity by neurogenic stimulation.
A literature search
of
the use
of
colchicine
to
treat constipation found only one citation.
In
a let-
ter
to
the Journal
of
the
Royal
Society
of
Medicine
in
1984, Sandyk and Gillman
6
reported the successful
use
of
colchicine to treat constipation in a patient
with Parkinson disease.
No
studies
of
the use
of
colchicine
to
treat constipation have been con-
ducted.
The
purpose
of
this study
was
to determine
whether daily colchicine administration could
im-
prove bowel function and reduce laxative use in
mentally and physically disabled patients with se-
vere, intractable constipation who currently
re-
quire large doses
of
multiple laxatives.
342
JABFP Sept.-Oct.
1998
Vol.
11
No.5
Methods
Patients were selected from the client population
of
five
state-supported individualized residential
alternative homes
(IRAs)
affiliated with the Finger
Lakes Developmental Disabilities
Services Orga-
nization (DDSO). Each IRA houses approximately
12
mentally and physically disabled patients in a
residential home and provides
24-hour
nursing
coverage.
All
of
the patients enrolled in this study
were incontinent and required diapers and person-
alized assistance with daily hygiene and feeding.
The
staff routinely recorded the number and doses
of
different laxatives used and the number
of
bowel
movements for each patient.
Study participants were selected from patients
in these homes who met the following criteria:
1.
Twenty-one years
of
age
or
older
2.
Chronic, severe constipation, defined
as
re-
quiring three
or
more different laxative agents
on
a regular basis for more than 6 months
3.
No
contraindication
to
colchicine, specifically
liver disease with a serum aspartate amino-
transferase (AST) greater than
40 mg/dL
or
re-
nal disease with a serum creatinine greater than
1.5
mg/dL
4.
Generally stable medical condition.
The
pa-
tients naturally had multiple medical
prob-
lems,
but
could
not
have been in a life-threat-
ening
situation
during
the
6
months
before
the study
or
could
not
have been expected
to
be
in
a crisis situation
in
the
6
months
after
the study
5.
Patients must weigh more than 60 pounds. Pa-
tients weighing between 60 and 99 pounds
were given colchicine and placebo at a reduced
dose twice a day instead
of
three times a day
6.
The
patient
must
have a
parent
or
legal
guardian capable
of
giving informed consent,
as
approved by the Institutional Review Board,
in accordance with the policies
of
the Finger
LakesDDSO
Twelve patients, 7 women and 5 men,
met
the
criteria and were enrolled
in the study.
Their
ages
ranged from
24
to
60 years. All patients had
pro-
found mental retardation and epilepsy. Five
of
the
12
had spastic quadriparesis.
One
patient was fed
through a gastrostomy feeding tube and the others
received a high-fiber chopped
or
pureed diet. All
of
these patients were taking
both
oral and rectal
laxatives.
Oral
laxatives were administered
on
a
routine basis, whereas rectal laxatives were given
on 29 August 2024 by guest. Protected by copyright.http://www.jabfm.org/J Am Board Fam Pract: first published as 10.3122/15572625-11-5-341 on 1 September 1998. Downloaded from

Period*
1
I
2
3
4 5 6
7 8 9
10
11
Group 1 Baseline
pt
P
P
P
Washout C C
C
C
Group 2 Baseline
c*
C
C
C
Washout P P P P
PHASE 1
PHASE 2 PHASE 3 PHASE 4
Figure
1.
Schematic
of
22-week study design, comparing colchicine with placebo for laxative effect in treatment
of
constipation in disabled patients.
"Each period represents 2
weeks.
tp
_ placebo, 2 or 3
times
per
day.
*C
- colchicine,
0.6
mg 2 or 3 times per
day.
on
an as-needed basis
if
there
were
no
bowel
movements within a defined period.
The
trial
was
a double-blind, crossover study
of
the use
of
colchicine to treat severe constipation in
profoundly disabled patients. Figure 1 schemati-
cally outlines the study design.
The
trial lasted
22
weeks and was divided into 4 phases, including 2
8-week intervention periods. Patients were dis-
tributed into two groups.
During
the 4 weeks
of
phase
1,
the laxative regimen
of
each patient was
optimized to have patients
on
as
few
different lax-
atives and laxative doses
as
possible without hav-
ing
them
experience fewer
than
3 bowel move-
ments
per
week. Patients in group 1 received
placebo either orally
or
by a gastrostomy tube for
8 weeks in phase 2 and colchicine either orally
or
by gastrostomy tube for 8 weeks in phase 4.
Group
2 patients had the reverse schedule. Phase
3 served
as
a 2-week washout period between the
two interventions.
The
consulting pharmacist
prepared
the
placebos
and
colchicine
and
randomly assigned
each patient
to
either group 1
or
2.
The
placebos
looked similar
to
the
colchicine tablets.
For
phases 2 and 4 the pharmacist prepared medica-
tion
vials
that
listed the name
of
the
patient, the
directions for taking
the
medication, and
the
dates
on
which
the
medication was
to
be
given.
Patients heavier than 99 pounds received
0.6
mg
of
colchicine three times a day and those lighter
than 99 pounds received
0.6
mg
of
colchicine two
times a
day.
The
pharmacist had
no
other
role in
the care
of
the patients and did
not
communicate
with the caretakers.
The
group assignments were
not
revealed by
the
pharmacist
to
the
investiga-
tors until the end
of
the study.
Thus,
both
the in-
vestigators and
the
caretakers were unaware
of
the treatment assignment.
Two
of
the investigators (PSF and
PD)
met
at
I
the beginning
of
the study and every 2 weeks to re-
view records
of
each patient's bowel movements.
For
ethical reasons, the protocol required that lax-
atives be adjusted so
that
patients had
at
least 3
bowel movements
per
week
but
not
more than 3
per
day.
WIthin these parameters the investigators
were free
to
adjust laxative orders.
The
study med-
ications (placebo
or
colchicine) were
not
adjusted
and the investigators were
not
aware which med-
ication the patient was receiving. All patients were
monitored clinically during the study for signs
of
colchicine toxicity, including diarrhea, vomiting,
fever, hair loss,
or
rash. A complete blood count,
12-test chemistry panel, creatinine kinase (CK),
and single stool sample for occult blood were
ob-
tained during phase 1 and after 4 weeks
of
phases 2
and
4.
The
study design and patient consents were re-
viewed and approved by
the
Institutional Review
Board
of
the Finger Lakes
DDSO.
Informed con-
sent was obtained from the parent
or
legal guard-
ian
of
each patient selected for the study in accor-
dance with the policies
of
the Finger Lakes
DDSO.
In
addition,
the
investigators obtained
permission from the patient's attending physician
for each patient to participate in the study. To pro-
vide uniformity in laxative management, the inves-
tigators ordered the patients' laxative medication
during the study.
The
number
of
different laxatives used, the
number oflaxative doses, and the number
of
bowel
movements were recorded for each patient
throughout the entire study.
The
primary compar-
isons were the total number
of
bowel movements
per 8-week treatment period and the total number
of
rectal laxatives used
per
8-week
treatment
pe-
riod.
The
differences in counts between phases 2
and 4 were calculated for each patient. A one-sam-
ple
t-test
was done
to
determine whether
the
ag-
Colchicine
for
Constipation
343
on 29 August 2024 by guest. Protected by copyright.http://www.jabfm.org/J Am Board Fam Pract: first published as 10.3122/15572625-11-5-341 on 1 September 1998. Downloaded from

Table
1.
Change
in Number of Patient's
Bowel
Movements
and Change in Amount of
Laxative
Use
While
Taking
Colchicine Compared
With
Placebo.
Study Variable 2 3
Bowel movements
on
colchicine,
No
49
54
55
Bowel movements
on
placebo,
No
31
40
44
Change in number
of
bowel movements
18
14
11
(colchicine minus placebo)
Change in dosage
of
rectal laxatives
(colchicine minus placebo)
-8
-5
-2
Change in dosage
of
oral laxatives
-37
-155
-104
(colchicine minus placebo)
gregate difference in bowel movements
was
statis-
tically significant.
Results
Twelve patients were initially enrolled.
One
pa-
tient
was
hospitalized during the study for reasons
unrelated to the trial.
His
stool counts were dis-
rupted and his study medication
was
discontinued
for a
few
days, so this patient
was
dropped from the
trial.
As
a result,
11
patients constitute the study
population.
The
results are outlined in Table
1.
Eight
of
11
patients experienced an increase in
number
of
bowel movements during the 8-week colchicine
treatment
period
as
compared with the 8-week
placebo treatment period.
We
also examined the
change in dosage
of
rectal laxatives.
We
focused
on
rectal laxative use in particular because these
laxatives, which consist mainly
of
enemas
or
sup-
positories, are
more
invasive and uncomfortable
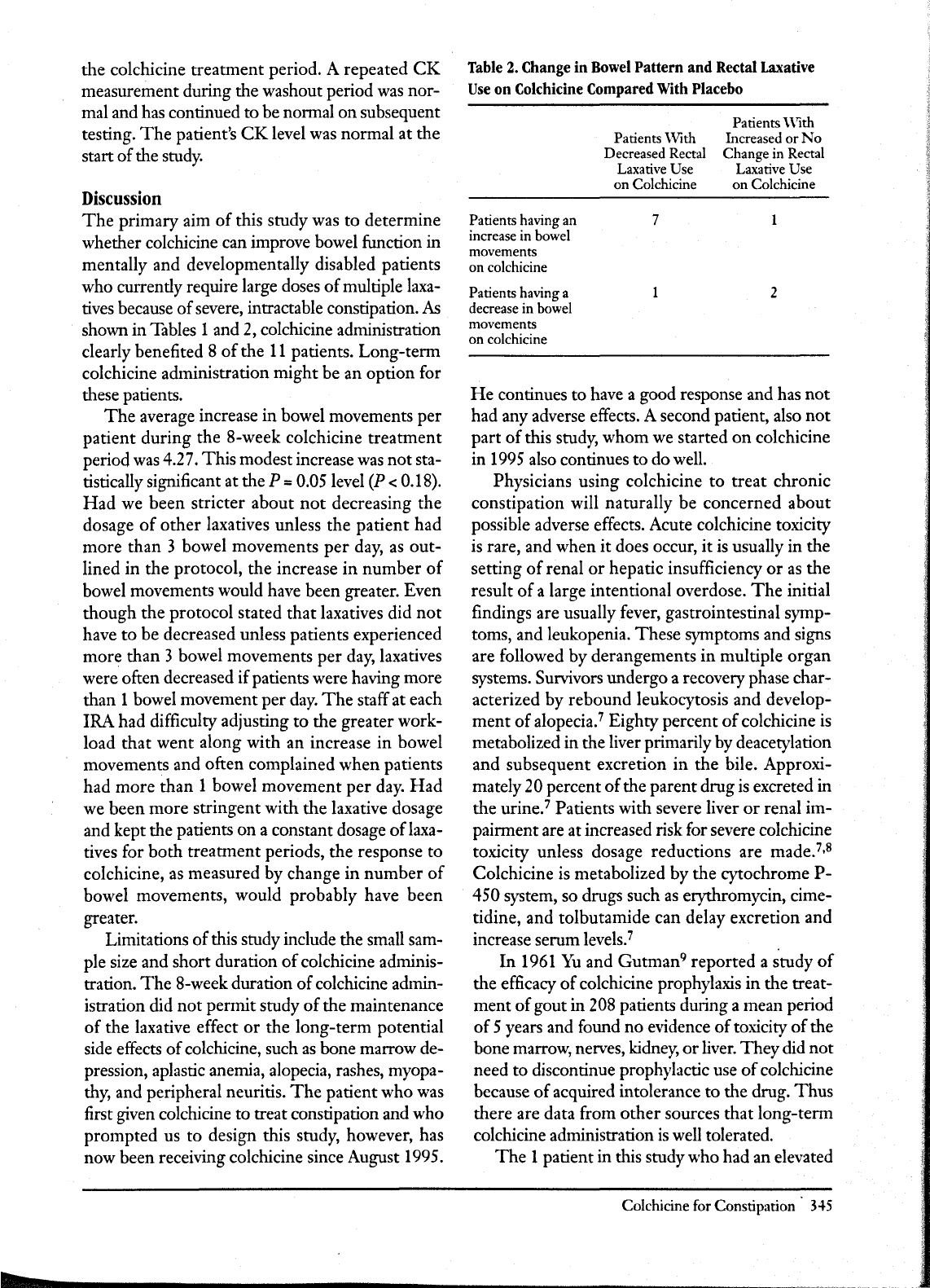
for the patient compared with oral laxatives. Table
2 describes the effect
of
colchicine treatment
on
both bowel movements and rectal laxative use for
the
11
patients. Seven
of
the 8 patients who had an
increase
in
bowel movements
on
colchicine also
required fewer rectal laxatives.
One
patient (No.
5)
experienced an increase
in
bowel movements
and an increase
in
rectal laxatives while
on
colchicine.
In
this case the increase in laxative use
was minimal.
The
patient received one more fleet
enema during the 8-week colchicine
treatment
period compared with the 8-week placebo treat-
ment period.
Two patients had a decrease in bowel move-
ments while receiving colchicine and also required
more rectal laxatives. Colchicine clearly did
not
improve the bowel pattern
of
these two patients.
One
additional patient (No.
11)
not
only had a de-
344
JABFP
Sept.-Oct.
1998
Vol.
11
No.5
Patient
4
5
6 7 8 9
10
11
32
30
41
27
35
38
35
24
22
23
34
22
32
45 45
35
10
7 7 5 3
-7
-10
-11
-6
-10
-3
-4
4 2
-5
-14
0
0
6 0
0 0
48
crease
in
bowel movements
on
colchicine,
but
also had a decrease
in
rectal laxative use. Al-
though
at
first glance this finding seems
rather
counterintuitive, during the beginning
of
phase
2,
while receiving colchicine, this patient was having
fewer than 3 bowel movements
per
week, which
prompted us to double his order
of
senna tablets.
Even with this increase he was still severely con-
stipated, which led to
our
increasing his bisacodyl
suppository order during the 7th week
of
phase
2.
This
increase in bisacodyl suppositories
was
con-
tinued throughout the washout period and phase
4, thereby resulting in a decrease in rectal laxative
use
on
colchicine compared with placebo.
More-
over,
that
patient
No.
11
's
rectal laxative dosage
was increased throughout the placebo period but
was increased only during the last 2 weeks
of
the
colchicine period
might
account for his having
more
bowel movements with placebo
than
with
colchicine.
An
aggregate comparison
of
the total number
of
bowel movements while patients were taking
colchicine compared with the total
number
of
bowel movements while taking placebo, irrespec-
tive
of
laxative dose, showed that patients experi-
enced on average 4.27 more bowel movements per
patient during the 8-week colchicine treatment pe-
riod. Although this result appears to be clinically
significant,
it
was
not
statistically significant (P =
0.18) because the sample size
was
small.
Colchicine was well tolerated by all
of
the pa-
tients.
No
problems relating to the common side
effects
of
colchicine such
as
nausea, vomiting, diar-
rhea,
or
abdominal discomfort were reported
by
the caretakers.
The
blood and stool monitoring
were all within normal limits with one exception.
One
patient (No.
11)
had an elevated
CK
level de-
tected at the end
of
phase
2,
later determined to be
on 29 August 2024 by guest. Protected by copyright.http://www.jabfm.org/J Am Board Fam Pract: first published as 10.3122/15572625-11-5-341 on 1 September 1998. Downloaded from
the colchicine treatment period. A repeated
CK
measurement during the washout period
was
nor-
mal and has continued to be normal on subsequent
testing.
The
patient's
CK
level was normal at the
start
of
the study.
Discussion
The
primary aim
of
this study was to determine
whether colchicine can improve bowel function in
mentally and developmentally disabled patients
who currently require large doses
of
multiple laxa-
tives because
of
severe, intractable constipation.
As
shown in Tables 1 and
2,
colchicine administration
clearly benefited 8
of
the
11
patients. Long-term
colchicine administration might be an option for
these patients.
The
average increase in bowel movements per
patient during the 8-week colchicine
treatment
period
was
4.27.
This
modest increase
was
not
sta-
tistically significant at the
P = 0.05 level
(P
< 0.18).
Had
we been stricter about
not
decreasing the
dosage
of
other
laxatives unless the patient had
more than 3 bowel movements
per
day,
as
out-
lined in the protocol, the increase
in
number
of
bowel movements would have been greater. Even
though the protocol stated
that
laxatives did
not
have to be decreased unless patients experienced
more than 3 bowel movements per
day,
laxatives
were often decreased
if
patients were having more
than 1 bowel movement per
day.
The
staff at each
IRA had difficulty adjusting to the greater work-
load that
went
along with an increase
in
bowel
movements and often complained when patients
had
more
than 1 bowel movement
per
day.
Had
we been more stringent with the laxative dosage
and kept the patients on a constant dosage oflaxa-
tives for
both
treatment periods, the response to
colchicine,
as
measured by change in
number
of
bowel movements, would probably have been
greater.
Limitations
of
this study include the small sam-
ple size and short duration
of
colchicine adminis-
tration.
The
8-week duration
of
colchicine admin-
istration did
not
permit study
of
the maintenance
of
the laxative effect
or
the long-term potential
side effects
of
colchicine, such
as
bone marrow de-
pression, aplastic anemia, alopecia, rashes, myopa-
thy, and peripheral neuritis.
The
patient who was
first given colchicine to treat constipation and who
prompted us to design this study, however, has
now been receiving colchicine since August 1995.
Table
2.
Change in
Bowel
Pattern and Rectal
Laxative
Use
on Colchicine Compared
With
Placebo
Patients \Vith
Decreased Rectal
Laxative
Use
on Colchicine
Patients
With
Increased
or
No
Change in Rectal
Laxative
Use
on
Colchicine
Patients having an 7
increase in bowel
movements
on colchicine
Patients having a
decrease in bowel
movements
on colchicine
2
He
continues to have a good response and has
not
had any adverse effects. A second patient, also
not
part
of
this study, whom we started
on
colchicine
in
1995
also continues to do well.
Physicians using colchicine
to
treat chronic
constipation will naturally be concerned about
possible adverse effects. Acute colchicine toxicity
is
rare, and when
it
does occur,
it
is
usually in the
setting
of
renal
or
hepatic insufficiency
or
as
the
result
of
a large intentional overdose.
The
initial
findings are usually fever, gastrointestinal symp-
toms, and leukopenia.
These
symptoms and signs
are followed by derangements
in
multiple
organ
systems. Survivors undergo a recovery phase char-
acterized by rebound leukocytosis and develop-
ment
of
alopecia.
7
Eighty percent
of
colchicine
is
metabolized in the liver primarily by deacetylation
and subsequent excretion in the bile. Approxi-
mately
20 percent
of
the parent drug
is
excreted in
the urine.
7
Patients with severe liver
or
renal im-
pairment are at increased risk for severe colchicine
toxicity unless dosage reductions are made.
7
,s
Colchicine is metabolized by the cytochrome
P-
450 system, so drugs such
as
erythromycin, cime-
tidine, and tolbutamide can delay excretion and
increase serum levels.
7
In
1961
Yu
and
Gutman
9
reported a study
of
the efficacy
of
colchicine prophylaxis in the treat-
ment
of
gout in 208 patients during a mean period
of
5 years and found no evidence
of
toxicity
of
the
bone marrow, nerves, kidney,
or
liver.
They
did
not
need to discontinue prophylactic use
of
colchicine
because
of
acquired intolerance to the drug.
Thus
there are data from
other
sources that long-term
colchicine administration
is
well tolerated.
The
1 patient in this study who had an elevated
Colchicine
for
Constipation'
H5
on 29 August 2024 by guest. Protected by copyright.http://www.jabfm.org/J Am Board Fam Pract: first published as 10.3122/15572625-11-5-341 on 1 September 1998. Downloaded from

CK
level at the end
of
the colchicine treatment
period
might
represent a case
of
colchicine-in-
duced myositis.
It
is
also possible that the abnor-
mally high
CK
value might simply be a laboratory
error, because
the
patient was asymptomatic
throughout the study and the elevated level
dropped to within the normal range
on
subse-
quent measurements.
Until there
is
more experi-
ence using long-term colchicine administration to
treat severe constipation,
it
is
certainly prudent for
clinicians to monitor patients for clinical and bio-
chemical signs
of
toxicity. Chronic colchicine ad-
ministration should be avoided in patients with
hepatic
or
renal insufficiency.
This
trial was a short-term study with a small
sample size. Nonetheless,
the
results suggest
colchicine might be a valuable treatment option
for patients who have severe, intractable constipa-
tion.
Our
intent
is
not
to promote colchicine
as
a
first-line laxative but rather to suggest its potential
as
an adjunctive form
of
therapy for difficult-to-
manage patients with decreased bowel motility.
Colchicine provides an effective alternative for pa-
tients with chronic constipation who are resistant
to standard modes
of
therapy. Future studies
should include a larger, more diverse patient popu-
lation and focus on maintenance
of
the laxative ef-
fect
as
well
as
surveillance for signs
of
toxicity.
Nursing home patients with severe bowel motility
problems might be good candidates for considera-
tion
of
colchicine therapy.
346
]ABFP
Sept.-Oct. 1998 Vol.
11
No.5
Colchicine and placebo capsules were prepared by
Thomas
Quin-
lan and Quinlan's Pharmacy, Wayland,
NY.
References
1.
Harari
D,
Gurwitz
]H,
Avorn
],
Choodnovskiy I,
Minaker KL. Constipation: assessment and manage-
ment in an institutionalized elderly population.]
Am
Geriatr Soc 1994;42:947-52.
2.
]ancar],
SpelIer C]. Fatal intestinal obstruction in
the mentalIy handicapped. ] IntelIect Disabil Res
1994;38(pt 4):413-22.
3.
Passmore
AP,
Wilson-Davies
K,
Stoker C, Scott
ME.
Chronic constipation in long stay elderly pa-
tients: a comparison
of
lactulose and a senna-fibre
combination. BM] 1993;307:769-71.
4. Lamy
Pp, Krug BH. Review oflaxative utilization in a
ski
lIed nursing facility.] Am Geriatr Soc 1978;26:
544-9.
5.
Insel
PA.
Analgesic-antipyretic and antiinflamma-
tory agents. In: Gilman AG,
RaIl
nv,
Nies
AS,
Tay-
lor
P,
editors. Goodman and Gilman's the pharma-
cological basis
of
therapeutics. 8th ed.
New
York:
McGraw-Hill, 1990.
6.
Sandyk
R,
Gillman MA. Colchicine ameliorates
constipation in Parkinson's disease. ] R
Soc Med
1984;
77:
1066.
7.
Caraco
Y,
Putterman C, Rahamimov
R,
Ben-Chetrit
E. Acute colchicine intoxication-possible role
of
erythromycin administration.] RheumatoI1992;19:
494-6.
8.
WaIl ace SL, Singer
]Z,
Duncan G], Wigley FM,
Kuncl
RW.
Renal function predicts colchicine toxic-
ity: guidelines for the prophylactic use
of
colchicine
in
gout.]
RheumatoI1991;18:264-9.
9.
Yu
TF, Gutman
AB.
Efficacy
of
colchicine prophy-
laxis
in gout.
Ann
Intern Med 1961;55:179-19.
on 29 August 2024 by guest. Protected by copyright.http://www.jabfm.org/J Am Board Fam Pract: first published as 10.3122/15572625-11-5-341 on 1 September 1998. Downloaded from
