AACN’S VISION FOR ACADEMIC NURSING
January 2019
Executive Summary
The Vision for Nursing Education Task Force was charged to:
• Clarify preferred educational pathways and the preparation necessary to succeed in
evolving and future roles for nursing professionals;
• Evaluate the future needs of the nursing workforce; consider academic nursing’s role in
promoting population health while addressing the social determinants of health and
advancing interprofessional engagement; and
• Propose overarching and broad-based curricular recommendations for baccalaureate and
graduate nursing programs.
A comprehensive environmental scan revealed substantive trends and projected changes in
higher education, healthcare systems, characteristics of learners, technological realities related to
teaching/learning practices, competency-based education, faculty availability and mix, workforce
realities and expectations, and regulatory requirements. Using these data and evidence, the task
force crafted a vision statement designed to provide direction for nursing education to move
forward and serve as a catalyst for future work related to the AACN Essentials.
The vision statement addresses overarching academic nursing considerations and future goals
related to meeting the needs of a dynamic, global society and a diverse patient population. This
emphasis was derived from a comprehensive review of the literature and consultation with
thought leaders in nursing, health care, and higher education. The goals and suggested actions for
moving towards this vision are articulated and include in brief:
• Advance diversity and inclusion in nursing education and practice.
o Adopt holistic admissions review practices; and,
o Foster strategies for increased recruitment and retention of a diverse nursing
workforce.
• Transition to competency-based education and assessment.
o Develop consensus-derived, nationally recognized competencies; and,
o Develop valid, reliable competency-assessment methods.
• Increase collaboration between education and practice through expanded and more
formalized academic-practice partnerships.
o Adopt AACN-AONE principles for academic-practice partnerships;
o Engage around curricular design and implementation, joint faculty appointments,
preceptor and mentor sharing, joint research and scholarly projects, and joint
nursing and interprofessional education initiatives;
o Jointly design and offer short courses or learning modules; and,
o Co-create robust models for transition to basic or advanced practice.
AACN’s Vision for Academic Nursing White Paper – January 2019
2
• Increase emphasis on faculty development and career advancement.
o Faculty to demonstrate current and sustained knowledge of the AACN Essentials
as well as have documented competency in an area of practice/specialization;
o Additional study in the science of pedagogy and neuroscience of learning is
encouraged to attain faculty/master teacher status;
o Faculty hold diverse degrees and engage in robust programs of research in
education and other relevant disciplines;
o Teaching teams that include individuals with expertise in instructional and
immersive technology and other advanced learning are formed; and,
o A multidisciplinary Center for Teaching and Learning Excellence developed by
AACN, to showcase and support the development of innovative learning,
experiential, and curricular models, for both didactic, simulated and real-life
clinical learning.
• Explore and adopt opportunities for resource efficiencies.
o Assure adequate exposure to essential high risk, low volume clinical experiences
through a mix of simulated and real-life field learning;
o Develop regional consortia of nursing schools to collaborate in core and
optional/elective courses or areas of content for entry-level and advanced nursing;
o Form regional accredited learning (simulation) centers to provide access to
current and new technologies for students and practicing clinicians.
Based on the changes, goals, and possible actions as outlined, future nursing education pathways
are described. Three pathways related to entry to practice, advanced nursing study, and evolution
of current programs are referenced and include:
• Entry to practice (BSN and master’s degree entry)
o Competencies and outcomes expected of BSN entry-level graduates
o Competencies and outcomes expected of MSN entry-level graduates
o Transition to entry-level practice
• Advanced nursing study: doctoral education
o Doctoral core
o Practice doctorate
o Research-focused doctoral education
• State of current programs
o Current RN-BSN programs and dual baccalaureate/associate degree enrollment
programs
o Current MSN programs
The document is designed to address the fundamental aim of AACN to serve as a catalyst for
excellence and innovation in nursing education, research, and practice. Congruent with the
historical work of the organization, the statement is meant to highlight the contemporary impact
on academic nursing of evolving practice needs and nursing roles in the context of faculty
resources, emerging learning and technologies, and learner profiles, as we strive to educate a
highly diverse, competent, and adaptable nursing workforce.
AACN’s Vision for Academic Nursing White Paper – January 2019
3
Background
As the voice of academic nursing, the American Association of Colleges of Nursing (AACN)
serves as a catalyst for excellence and innovation in nursing education, research, and practice.
Since its inception in 1969, the organization has worked to improve the quality of nursing care
by re-envisioning traditional nursing roles, strengthening nursing education programs, and
striving to create a more highly educated nursing workforce. At a time when new models of
health care are being introduced and the roles for registered nurses (RNs) are expanding, the
need to reconsider how best to educate the nursing workforce of the future is critical.
As indispensable members of the healthcare team, nurses today are at the forefront of advancing
evidence-based solutions and leading innovation in an atmosphere of accelerating change. The
imperative to evolve is driven by the needs of students, employers, and consumers of care. Nurse
educators must be nimble enough to embrace new technology and explore fresh approaches to
teaching designed to satisfy the diverse learning needs of contemporary nursing students. Given
the growing body of evidence linking education to quality outcomes, employers increasingly
expect registered nurses to be prepared at the baccalaureate level. Increasingly, care is provided
not in hospitals, but within the community; thus, we can no longer prioritize the preparation of
nurses for roles confined to acute care settings. The scope of registered nurse practice also is
changing, with RNs expected to play a greater role in meeting the nation’s need for high quality
and accessible care. To underscore this point, the Josiah Macy Jr. Foundation
1
has emphasized
that “we simply can’t meet the primary care needs of the nation unless registered nurses are part
of the solution, and we must prepare them appropriately and then use them for this role.”
1 (p. 25)
From mounting concerns over patient safety to the growing need for primary care providers,
nurses must be supported to thrive while working on the front lines to implement solutions
needed to repair a fragmented care delivery system.
With the goal of meeting the needs of a dynamic and global society, this AACN vision for
nursing education is derived in part from a review of current trends and relevant assumptions
regarding registered nurse preparation and practice. Addressed are education pathways,
overarching curricular changes, resource needs, and learning methodologies to transform nursing
education.
These suggested actions are provided to inspire nursing education leaders to innovate and
seek opportunities to advance the nursing profession within a changing environment. As a
vision statement, this document is meant to be aspirational rather than a mandate for the
profession or schools of nursing. Further thinking and action will need to address
implementation strategies and actions to realize any or all the visionary goals.
AACN’s Vision for Academic Nursing White Paper – January 2019
4
Environmental Scan: Current State and Future Needs
The Vision for Nursing Education Task Force conducted a broad environmental scan to
summarize trends and projected changes in health care, higher education, population
demographics, learners and learning styles, the nursing workforce, nursing regulation, and
patient/populations needs. While the trends and changes described are not exhaustive, they
inform the vision being advanced.
CHANGING HIGHER EDUCATION
Higher education has been subject to shrinking federal and state funding, rising tuition, aging
infrastructure, variation in funding sources, fluctuations in available resources, and changing
demographics of enrollees.
2
Traditional higher education models, including faculty structures,
governance models, and curricula can limit flexibility and create barriers to innovation. Recent
trends—such as open access online courses, short courses that award micro-credentials or
badges, tuition models based on the number of enrollees in the course, and the growing
availability of distance learning opportunities and immersive learning technologies—are broadly
challenging traditional approaches to higher education.
The development and awarding of micro-credentials or badges by academic institutions is an
evolving trend. One study found that more than 90% of educational institutions are offering
credentials and digital badges, in part, to serve millennial students who favor badging and
certificates to traditional degrees.
3
A badge is a visual representation of an accomplishment,
achievement, or skill acquisition but not a formal degree. Digital badges have emerged as
documentation of community engagement, professional development, and accomplishments.
Badges provide recognition of incremental learning in visible ways and can support career
development.
4
Stackable credentials are another emerging practice whereby credentials such as
badges can be accumulated over time and facilitate one’s professional development along a
career trajectory.
5
Charged with educating the nursing workforce of the future, academic nursing should formulate
a proactive response to the changing landscape of higher education and the demands of
employers, prospective students, and the public. To ensure that graduates are ready for
contemporary practice requires faculty who have an awareness of evolving changes and the
understanding of the science of learning and a commitment to adapting curricula, teaching
strategies, and student learning assessment. It is paramount to inculcate graduates with the
knowledge, skills, and values for embracing change and innovation through career-long learning.
COMPETENCY-BASED EDUCATION MOVEMENT
Competency-based education has emerged in higher education and the health professions to
address criticisms of contemporary approaches to training.
6-7
Medicine has identified Entrustable
Professional Acts (EPAs) and is developing competencies for post-graduate residencies.
8-9
The
discipline of physical therapy has identified common competencies that graduates are expected
to demonstrate prior to graduation. In addition, the Physical Therapist Clinical Performance
Instrument provides a validated, standardized assessment tool that is available for programs to
AACN’s Vision for Academic Nursing White Paper – January 2019
5
document attainment of the expected competencies.
10
Dental and veterinary education also are
working to develop nationally recognized competencies that would provide a foundation for
entry into these disciplines. In nursing, competency-based education models are being developed
and studied.
11-12
However, implementation issues (such as regional accreditation requirements)
impact on faculty development and resources, and fiscal impact on the institution also have been
raised
13-16
and will need to be addressed as this transition occurs across disciplines.
CHANGING LEARNERS
Across the educational spectrum, students are calling for changes in how they are taught given
recognition of the changes in how they learn. Today’s learners are composed of Millennials
(1977-1995), Centennials (born after 1996), and Generation Z (1998-present). Baby Boomers
(1946-1964) returning to school to re-tool or pursue new career options also are a component of
today’s learners. Each cohort/group has preferences and characteristics that should guide
modification of curricular offerings and learning opportunities. For example, the literature
describes Millennials as “digital natives” who have the perceived ability to multi-task, but some
Millennials may still prefer a traditional way of learning. Centennials are the iGeneration (iGen)
who have been referred to as “digital natives on steroids.” Centennials have not known a world
without social media or the immediacy of web searches and information at their fingertips. They
generally prefer using a checklist approach and do not embrace societal conventions that view
seat time as a benchmark for higher education. Generation Z values entrepreneurship and
innovation, self-reliance, social and racial equality, and project-based learning around real-world
problems.
17-20
In addition to traditional first-time college students seeking an education and degree, second
degree learners are returning to school in greater numbers to retool their skills to better meet
workforce demands. Learners are seeking second degrees to be competitive in the workplace and
obtain marketable degrees and skills that afford them a preferred lifestyle. As such, faculty must
retool their teaching strategies to accommodate the styles of this diverse population of learners,
both first-degree students (pedagogy) as well as adults returning to school (andragogy). These
shifts in generations will require a metamorphosis of the education enterprise and the ability to
embrace the ongoing emergence of the science of learning.
CHANGING LEARNING TECHNOLOGIES
Recent advances in educational neuroscience—a term used to describe the interrelationship
between neuroscience, teaching strategies, and psychology—have resulted in new
understandings associated with how people learn. This area of science provides evidence for best
practices in teaching to include strategies that engage the learner in challenging and purposeful
learning, and where reflection on that learning is incorporated. Advances in immersive
technologies provide growing opportunities to engage the learners in their learning experiences.
The use of learning technologies is transforming higher education by blurring the boundaries
between formal and informal learning systems and offering greater opportunity for connectivity
and active engagement. The technology explosion requires faculty to have a clear understanding
of the push-pull of technology; the utility of technologies in transforming teaching-learning

AACN’s Vision for Academic Nursing White Paper – January 2019
6
experiences; and the availability, acceptability, affordability, and accessibility of technology to
enhance learning. As technologies evolve, the availability and affordability of the new learning
opportunities for all institutions and all learners must be planned. A balance is needed between
competition and collaboration among institutions considering the increased availability of
technology-driven teaching methods, the rising cost of tuition, and the proven effectiveness of
learning technologies.
A growing emphasis within the domain of learning science involves promoting active learning,
e.g., the flipped classroom movement and personalized-paced learning. Priming for classroom
learning (both actual and virtual) by creating self-study, and guided exposure to concepts and
content (knowledge) followed by teacher coaching of knowledge application in the classroom
holds much promise to enhance learning. For example, through a problem-based unfolding case
study, learners are guided through multiple steps where previous knowledge must be recalled and
applied to make clinical decisions. Adaptive learning is evolving and has significant potential to
facilitate the impact of teaching/learning. It uses computer technology (algorithms) that provide
individualized responses based on student interactions (comprehension) in real-time, making the
learning personalized. The field of adaptive learning encompasses artificial intelligence and other
curricular technologies, using knowledge domains such as cognitive science, predictive
analytics, and learning theory.
21
Access to online education and new technologies is growing. Increasingly, a design-build
approach is being used with pairing of faculty with an instructional designer to promote
innovation and effective teaching methods in the classroom. Such approaches help address
limited resources, rising education costs, and demands to expand enrollments as well as diverse
student learning styles. New models of instruction, inclusive of large class sizes, necessitate
revised strategies for team teaching, utilization of preceptors and/or teaching assistants, and
small group work, and for the testing of other advanced approaches driven by technology, such
as Artificial Intelligence /Machine Learning. These options offer opportunities for multi-pronged
approaches that facilitate student-centered learning.
22,23
CHANGING FACULTY AVAILABILITY AND MIX
The aging of the nursing faculty workforce is creating pressure to adapt new strategies to address
growing faculty shortages fueled by both increased retirements and demand. Although faculty
are delaying retirement much longer than in the past, in 2015 thirty-one percent of full-time
faculty were over 60 years of age.
24
Projections indicated that retirements between 2016-2025
would equal one third of the 2015 employed faculty workforce. On a more positive note, the
proportion of faculty age 44 or younger increased from 19% in 2006 to 24% in 2015. While the
delayed retirements may prevent hiring of less experienced faculty (potentially at lower cost),
hiring sufficient faculty with the credentials to meet program needs is the current challenge. In
2017, 55% of all nursing programs (baccalaureate, master’s, and doctoral) reported insufficient
number of faculty as one of the primary reasons for not admitting all qualified applicants.
25
In the face of evolving educational models and to meet financial challenges and faculty
shortages, the number of adjunct faculty has been steadily increasing. Widespread national
dialogues have raised questions related to the issues of the cost, purpose, and value to the
AACN’s Vision for Academic Nursing White Paper – January 2019
7
academic enterprise, and current models of tenure and promotion. To better suit the institutional
mission, many schools have instituted both clinical (or practice) and research faculty tracks for
recruitment, promotion, and tenure of faculty. Due to the differential in academic and practice
salaries, concerns have been raised about fewer nurse clinicians choosing to enter academia.
26
This challenge fuels a call for new models of faculty mix and utilization and the need to develop
robust partnerships with the practice community.
27
Growing options for practice and research
within industry and the clinical services enterprise have provided alternatives to academic
careers for nurse scholars. With the growth of the practice doctorate and the need to maintain
advanced practice licensure, new academic workload models incorporating faculty clinical
practice and enhanced academic-practice relationships are emerging.
Active engagement in practice ensures that what is taught in schools, colleges, and programs of
nursing appropriately reflects current practice; increases faculty credibility with practice; and
enhances the relevance, applicability, and implementation of research. Stronger formal and
informal collaboration between academia and practice will position nursing as a leader in
healthcare delivery.
27
CHANGING HEALTHCARE SYSTEMS
To spur broader access to an enhanced patient experience, better quality care and provider work
life, and to reduce cost, the U.S. healthcare delivery system is undergoing constant change.
Needed are adaptable, creative individuals able to work with diverse populations while being
agile to respond to the fluctuating business needs and reimbursement realities. Reimbursement
has moved from service-based payment to value-based purchasing. Integrated-care systems are
emerging that require coordination, not only across settings, but across the care and lifespan
continuum. With scientific discoveries growing exponentially (e.g., new technologies,
knowledge of genetics, treatments, and pharmacologic agents), health care is growing
increasingly complex.
In addition, the rise of personalized health care has the potential to transform the traditional
patient care experience. Precision health (frequently called precision medicine) refers to the use
of biologic markers to make accurate predictions regarding an individual’s risk for health
conditions, and/or best treatment options for existing conditions. The technologies for precision
health already exist and may lead to a significant shift in care delivery from standardized to
individualized treatments and from treating conditions to preventing conditions. This shift will
occur in conjunction with a growing emphasis on population health and the social determinants
of health. However, regulatory policy, reimbursement, and clinical adoption of available options
have been slow to change. The implementation of precision health approaches in clinical practice
requires an increased awareness and understanding of these advances by the current and future
healthcare workforce. This new approach to care requires that we reconsider what we teach,
including the knowledge, skills, and attitudes necessary to provide this individualized approach
to care.
Nurse employment settings are shifting from the most expensive venues—inpatient facilities and
emergency departments—to more primary care and community settings. Care is becoming
increasingly convenient with more mobile and technology enabled e-visits or e-encounters
AACN’s Vision for Academic Nursing White Paper – January 2019
8
available anywhere and at any time. Shifting care delivery to retail, community, or home settings
has the potential to produce cost savings, a shift in workforce distribution, and a change in
requisite skills. Healthcare systems are revising strategic goals and reorganizing services to move
more care outside of inpatient institutions. The American Hospital Association reported that
from 2008 to 2012, outpatient visits rose from 624 million to 675 million while inpatient visits
decreased from 35.7 million to 34.4 million.
28
Urgent care clinics are employing growing
numbers of advanced practice registered nurses (APRNs) to deliver services at a 72% savings
over emergency departments and project growth to 12,000 urgent care clinics by 2019.
29
The
increasing use of telehealth as well as the growth of non-hospital settings will affect the RN and
APRN nursing workforces.
Preparing graduates for the rapid advancement of technologies in practice also is a challenge.
Today’s nursing graduates are called upon to deliver quality care in increasingly technologically
enhanced settings (which include electronic health record systems used to order interventions),
document treatments, monitor patient reaction to treatments, and communicate across the care
team. Telehealth technologies are used to provide healthcare in rural (and other) areas where
health care options are limited. Technologies, including artificial intelligence and wearable
devices, are emerging rapidly to support diagnostics, patient monitoring, care delivery, and
evaluation/trending of care outcomes.
CHANGING NURSING WORKFORCE
Today’s nurses work in complex, integrated healthcare delivery systems. With patients and
families experiencing multiple transitions across care settings, nurses need to have higher level
knowledge and skills to support safe transitions and minimize fragmentation of care. Growing
demands for an increasing number of baccalaureate and higher-degree prepared nurses require
new education and professional development models, particularly new clinical education models.
Strong academic-practice partnerships are needed to co-design clinical education that is relevant
and reciprocal, ensuring that graduates are prepared to practice in the continually changing
healthcare system while solidifying nursing’s influence on efficient and effective care delivery
models. To improve healthcare outcomes and the overall health of the population, nursing
faculty will need to prepare nurses with a solid knowledge and skill set to practice across
settings, provide care to diverse populations, address the social determinants of health, and
minimize health disparities.
In 2016, the Josiah Macy Jr. Foundation brought together leaders in nursing education and
primary care to examine current education along with best practices. The result was the proposed
actionable recommendations for re-balancing nursing education and, specifically, a call to
encourage registered nurses to become leaders in primary care teams, practicing to their full
scope to improve the health of the American people.
30
The lack of primary care content in the
curricula of most nursing schools, including both didactic content and clinical experiences, was
noted; especially that nursing education continues to emphasize in-patient hospital nursing. As
most faculty are likely not prepared to teach primary care nursing, this was addressed as a need
for entry preparation and professional development. The nursing profession must partner with
others to transform our healthcare system into one that promotes the health of individuals,
families, and communities, including preventing and better managing chronic illnesses.
AACN’s Vision for Academic Nursing White Paper – January 2019
9
The Macy report must be considered in light of the 2017 report Supply and Demand Projections
of the Nursing Workforce 2014-2030,
31
which highlighted the inequitable distribution of the
nursing workforce across the United States. Although a shortage of registered nurses is a
concern, the greater problem resides with the distribution of nurses across states, particularly in
rural areas. Rural communities are greatly affected by the maldistribution of healthcare
professionals, which significantly impacts primary and acute care access. Areas with higher
proportions of low-income and minority residents, such as rural areas, tend to suffer most from
an inadequate supply of healthcare providers. The number of working RNs per capita has
remained substantively lower in rural areas than in urban areas, and the salaries of RNs who live
in rural areas remain lower than those residing in urban areas. The variables that impact the
maldistribution of the nursing workforce include lower reimbursement levels, reduced ability to
recruit and retain health professionals, higher rates of uninsured or Medicaid/Medicare patients,
and fewer rural training sites. Most future health professionals come from urban areas, as rural
students often experience educational disadvantages in terms of preparation in math and science
and development of successful academic/learning skills.
32,33
Nursing workforce demographics have changed slowly even though the United States is steadily
becoming more diverse. According to the U.S. Census Bureau, in 2016 minority groups
comprised 38.7% of the population. If this trend continues, the minority population will be the
majority by 2043. However, the nursing workforce remains predominately white with minorities
comprising 24.5% of the workforce.
34
Diversity within the nursing workforce—in terms of
race/ethnicity and gender—is desirable because it can contribute to the improvement of access
and care quality for minorities and medically underserved populations.
35
Holistic admissions
review is one strategy being used by health professional education to increase the diversity of the
professions. Holistic admissions review is defined as a flexible, individualized way of assessing
how an applicant will fare as a student and as a future professional and member of society.
36
Other health professions, particularly medicine (91%), dentistry (98%), pharmacy (78%) and
public health (78%) have adopted holistic admission processes.
37
Research findings demonstrate
that holistic admissions review practices increase diversity without decreasing workforce
preparedness and academic success of students.
38
CHANGING REGULATION OF NURSING PRACTICE
The National Council of State Boards of Nursing (NCSBN), a not-for-profit organization whose
members include the state and territorial boards of nursing, administers the national licensing
exam, the National Council Licensing Examination for Registered Nurses (NCLEX-RN
®
). The
NCLEX-RN
®
is used by all 50 states and territories as well as the Canadian provinces to license
entry-level registered nurses. The exam is based on a job analysis of newly licensed nurses
conducted every 3 years.
39
Due to the increasing complexity of decisions being made by newly
licensed nurses, NCSBN has announced that it is piloting new testing formats and assessment
items known as the next generation of NCLEX.
40
In 2002 the AACN Task Force on Education and Regulation I (TFER I) found that it was not
feasible at that time to engage in efforts to differentiate the license for baccalaureate and
associate degree nursing graduates.
41
However, evidence continues to emerge that demonstrates
AACN’s Vision for Academic Nursing White Paper – January 2019
10
that a higher mix of BSN and higher degree educated RNs in the workforce improves outcomes
of care.
42-45
In 2003, a second task force (TFER II) was charged with identifying the knowledge
and skills that would be needed by future nurses to address the many gaps in healthcare and
improve outcomes. The TFER II report, White Paper on the Role of the Clinical Nurse Leader,
delineated the education outcomes and expectations for a new master’s prepared nurse. The
AACN Board of Directors, in addition to approving the white paper, passed a motion to assume
leadership in the development of a new legal scope of practice and credential for the new
master’s prepared nursing professional, the Clinical Nurse Leader (CNL). The CNL Certification
exam was launched in 2007 and, to date, more than 6,000 master’s prepared nurses have been
credentialed through this examination. As reports increasingly show improved quality of care,
lowered costs, increased patient satisfaction, and improved care outcomes linked to this new
provider, healthcare systems continue to integrate CNLs into the nursing workforce.
46-50
Since the time of inception, regulation of advanced practice registered nurses (APRN) has varied
by state and by APRN role. In the early 1990s NCSBN began its involvement with APRN
regulation by developing model legislation for APRN licensure and core competencies. In 1995,
NCSBN began working with national APRN certifiers to ensure that examinations were suitable
for regulatory purposes.
In 2004, in response to growing variability among state boards of
nursing requirements for APRN licensure/certification, AACN and the National Organization of
Nurse Practitioner Faculties (NONPF) initiated the APRN Consensus Group and then the APRN
Joint Dialogue Group to join the work of the Consensus Group together with that of NCSBN. In
2008, the final report of the Joint Dialogue Group, Consensus Model for APRN Regulation:
Licensure, Accreditation, Certification & Education, was released and endorsed by 40 national
nursing organizations.
51
Implementation of the new regulatory model by all organizations
engaged in any aspect of the model has been ongoing since 2008. To date,16 states have fully
implemented all aspects of the model, and another 10 have implemented most of the model’s
requirements. When fully implemented across all states, the model will provide standardization
in APRN regulation for the over 488,000 credentialed APRNs in the U.S. thereby improving
mobility across states as well as increased access to APRN care.
52
Vision for the Future
The Vision for Nursing Education Task Force extensively reviewed and thoughtfully considered
the many issues explicated through the environmental scan. Built on these trends and validated
assumptions, a future vision for nursing education was developed that serves to meet the needs of
a dynamic and global society and a diverse patient population. Multiple opportunities exist for
moving nursing towards the vision for the future including identifying overarching goals for the
future and advancing preferred nursing education pathways.
OVERARCHING GOALS FOR THE FUTURE
Accelerate Diversity and Inclusion
AACN members have affirmed the need to address pervasive inequities in health care by
ensuring the preparation of nurses able to meet the needs of all individuals in an increasingly
diverse American society, including both ethnic and geographic diversity. AACN and its
member schools are committed to accelerating diversity, inclusion, and equity initiatives to
AACN’s Vision for Academic Nursing White Paper – January 2019
11
prepare the current and future nursing workforce to be reflective of the society it serves while
simultaneously fulfilling society expectations and needs.
53
Suggested actions to advance this goal
include:
• Adopt holistic admission review practices, which include attention to a student’s life
experiences and personal qualities in addition to traditional measures of academic
achievement such as grades and test scores
36, 38, 54
and support students to ensure success
in the programs.
• Foster strategies to increase recruitment and retention of the nursing workforce in all
geographic environments in consideration of the maldistribution of care providers (e.g.,
rural areas).
• Build a culture of diversity and inclusion in academic nursing.
Transition to Competency-based Education and Assessment
The current model for nursing educational experiences, both didactic and clinical, often fails to
ensure attainment of competencies. There is an inability to control available learning experiences
for each student and clinical time may avert intentionality. Hours can be logged, but there is no
assurance that all students have equitable experiences or that competencies are achieved. Moving
to a competency-based model would foster intentionality by defining competencies and
associated attributes, methods for achievement, and outcome measurement.
At the national level, consensus is growing in terms of preparing health professionals via
competency-based education (CBE).
1, 8, 11,12,55,56
Academic leaders across all disciplines are
calling for transition to programs that are predicated on mastery of competencies. In nursing,
such a move could modulate concerns of clinical preceptors and employers frustrated by the
diverse expectations of students entering clinical experiences as well as expectations of new
graduates.
There may be numerous ways to approach CBE as a multi-faceted solution to complex
challenges within higher education. Incremental steps may be needed over time, but regardless,
shifting the focus on what the learner should “know,” to what the learner must be “able to do” is
critical– and CBE is the desired framework to ensure this.
Although there may be more questions than answers at this point, evidence continues to emerge
revealing how institutions are designing and implementing time-variable CBE at the course,
program, or institutional level. While CBE has captured the attention of many in higher
education, the effectiveness and scalability must be ensured, and there are challenges to be
addressed, to include:
13-15, 57
• Considerable re-tooling of infrastructure related to prevailing institutional models, e.g.,
financial aid eligibility criteria; predictable teaching schedules and revenue expectations
based on traditional enrollment patterns; registrar practices; and traditional philosophies
about teaching and learning, along with current learning resources;
• Current strategic priorities and budget constraints;
• Current licensing requirements, certification standards, and accreditation systems.
Despite these challenges, the potential for CBE to benefit society, educational systems, learners,
and the people that we serve cannot be overlooked.
1, 58
AACN’s Vision for Academic Nursing White Paper – January 2019
12
In nursing, the transition to CBE will occur over time and will depend on the development of
nationally recognized, measurable competencies, reliable standardized assessment methods, and
support for implementation. This work will require
extensive efforts to reach consensus on competencies, assessment methods, and a plan for
implementation. Suggested actions to advance CBE include that AACN:
• Lead development of nationally recognized competencies using a consensus-based
process that engages diverse stakeholders from academia, practice, and regulation.
• Facilitate development of valid, reliable competency-assessment methods to facilitate the
valid assessment of students.
• Facilitate implementation by collaborating to align regional accreditation requirements
and evolving strategies to conserve fiscal and faculty resources.
Increase Collaboration Between Education and Practice
Expand formal academic practice partnerships. Considering the recognized need for
educational transformation that will improve the health of the public and create a workforce
matched to healthcare delivery, there is a clear need to develop expanded and new academic-
practice partnership models that go beyond what is utilized today. Envisioned are models that
include multi-school and multi-practice partnerships as well as regional coalitions. Nursing
leaders are encouraged to foster strategies that promote opportunities for relationship-based
partnerships that promote intentional cross-engagement, co-design, and commitment across
practice and education. Effective partnerships provide benefits to all engaged entities and reflect
the breadth of practice institutions, including community-based, public health, and integrated
care institutions. Such partnerships will strengthen the potential for nursing leaders to have an
influential voice in designing and implementing healthcare policy, systems, and delivery.
Stronger academic-practice partnerships are needed such that nursing faculty are engaged in the
clinical practice of the health system and clinical services are more closely connected to the
academic mission of the school of nursing.
22
To move towards this goal, exemplary actions
include:
• Adoption of the AACN-AONE principles for academic-practice partnerships by all
schools of nursing.
59
• Implementation by schools of nursing (of all classifications, geographic regions, and
missions),in partnership with practice institutions, the recommendations delineated in A
New Era for Academic Nursing.
27
• In addition to the broad, high-level goals and purposes described above, academic-
practice partnerships engage in such areas as:
o Curricular design and implementation
o Joint faculty appointments and identification and preparation of preceptors and
mentors for students and new graduates
o Development of optional transition to practice programs
o Joint participation in interdisciplinary, health-professional research teams
o Joint development of transition to practice programs; and
o Joint development of specialty education programs, which could include short
courses or learning modules (separately or within post-graduate programs focused on
specific geographical and employer needs).
AACN’s Vision for Academic Nursing White Paper – January 2019
13
Create robust transition to practice models. The complexity of health care and diversity
of practice settings is growing. Optional, accredited (by a Department of Education-recognized
entity), post-graduate transition to practice programs for both entry-level and advanced nursing
graduates offered by schools of nursing and practice entities would assist in addressing these
growing changes.
60-61
To address the variable needs of employers and nurses, particularly in
more specialized areas of practice (e.g., women’s health, care of older adults, trauma care),
schools of nursing and practice entities also could jointly offer short courses or modules
(separately or within post-graduate transition to practice programs) focused on specific areas of
practice. These learning experiences would preferably be designed to award academic credits,
promote competency enhancement, enhance potential for career advancement, and positively
influence nurses’ impact on healthcare delivery.
Increase Emphasis on Faculty Development and Career Advancement
Career-long faculty and leadership development opportunities provide for career progression as
well as growth and sustainability of the profession. This is important across an academic nursing
career in order to reflect changes in health care and higher education (e.g., new discoveries in
learning science, research, interprofessional team care and education, and healthcare and learning
technologies). Faculty providing direct or indirect applied practice learning experiences integrate
direct or indirect practice with their roles as educator and researcher.
The faculty mix based on expertise in practice, education, and research in both nursing and other
disciplines normally is shaped by the mission and needs of the institution. Discourse on how best
to prepare individuals for the faculty role transcends all health professions and other higher
education disciplines. It is desired that faculty preparing the next generation of graduates are
required to hold a terminal degree for their discipline or one closely aligned and have current
expertise related to the competencies they are teaching. As in other disciplines (e.g., engineering,
business, law), the major articulated faculty competence is practice specialization within the
discipline rather than the process of teaching. However, as expressed in the AACN document
related to the preferred professoriate profile: “The individual faculty from nursing or other
disciplines will demonstrate current and sustained competency in knowledge of the AACN
Essentials appropriate for the baccalaureate and graduate-level teaching pedagogy, interpersonal
skills, and leadership as well as competency in their area of practice/specialization.”
62
Therefore,
to become a master teacher in either the practice environment or academia, additional
preparation in the science of pedagogy is preferable to augment one’s ability to transmit the
science of the profession.
Those pursuing a graduate nursing degree and interested in an academic career could seek
additional preparation in the science of pedagogy through one or more of the following potential
options:
• Completion of elective course work during one’s graduate academic program.
• Orientation or onboarding provided by schools of nursing or the university/college
as well as mentorship for faculty new to the role.
• Coursework offered as a post-graduate badge/credential for those holding a practice
or research-focused doctorate in nursing or another aligned field of study.
A faculty mix of expertise in practice, education, and research is an asset to high quality
programs. Faculty with degrees and programs of research related to practice, education and other
AACN’s Vision for Academic Nursing White Paper – January 2019
14
areas (e.g., health policy, epidemiology, or pathophysiology) should be valued as determined by
the mission and needs of the institution. Teaching teams that include individuals with expertise
in curricular design, instructional technology and other advances in learning also are important to
address the growing complexity and diversity of health care, learners, and higher education. A
multidisciplinary Center for Teaching and Learning Excellence developed by AACN would
showcase and support the development of innovative learning experiences and curricular models,
for both didactic, simulated and real-life clinical learning.
In summary, suggested actions include:
• Faculty to demonstrate current and sustained knowledge of the AACN Essentials as
well as have documented competency in an area of practice/specialization;
• Additional study in the science of pedagogy and neuroscience of learning as
reflected in their teaching is encouraged for faculty/master teacher status;
• Faculty hold diverse degrees and engage in robust programs of research in practice,
education and other relevant disciplines;
• Teaching teams that include individuals with expertise in curriculum design,
instructional and immersive technology and other advanced learning are formed;
and,
• A multidisciplinary Center for Teaching and Learning Excellence developed by
AACN to showcase and support the development of innovative learning
experiences and curricular models, for both didactic, simulated and real-life clinical
learning.
Explore and Adopt Opportunities for Resource Efficiencies
Increasing costs and scarcity of resources in higher education and health professions education,
including the faculty shortage, are projected to grow. A shortage of qualified and experienced
faculty at each nursing school puts educational quality at risk and jeopardizes consistent student
exposure to critical knowledge and skills and guidance by expert faculty. Suggested actions to
address these changes and scarcity of resources include:
• Simulated and real-life field learning is proportioned to assure adequate exposure to
essential high-risk, low-volume clinical experiences and achieved through advancements
in technology and the development of virtual learning and assessment, including in the
affective and cognitive domains.
• Development of regional consortia of nursing schools to collaborate in providing core
and optional/elective courses or areas of content for entry-level and advanced nursing.
This is to promote high quality learning, address the faculty shortage, and better utilize
scarce resources and expertise. The consortia could be similar to the Nursing Education
Xchange (NEXus) housed at the Oregon Health & Science University or achieved
through an AACN-coordinated repository/service.
• Formation of regionally accredited learning (simulation) centers provide access to current
and new technologies for students and practicing clinicians; the centers would distribute
costs across schools offering more affordable and accessible options.
AACN’s Vision for Academic Nursing White Paper – January 2019
15
ADVANCING FUTURE NURSING EDUCATION PATHWAYS
The environmental scan presents multiple and varied challenges that will impact nursing
education. Streamlined education pathways and overarching curricular changes will move the
profession towards addressing these challenges.
Entry to Practice (Baccalaureate and Master’s Degree Entry)
In keeping with AACN’s long-time support for the Bachelor of Science in Nursing (BSN)
degree, the task force envisions that the BSN will be adopted as the minimum preparation for
registered nurse licensure and entry into the nursing profession. The degree would be conferred
by four-year colleges and universities and, where relevant, in partnership with other four-year
colleges and universities or community colleges. Models of partnerships are identified in the
Academic Progression in Nursing (APIN) final report, a Tri-Council for Nursing initiative.
63
This transition to the BSN minimum degree for entry into registered nurse practice would be
facilitated by AACN in partnership with the Tri-Council and other professional nursing
organizations.
Currently, entry-level nursing education has a major emphasis on preparing graduates for acute
care in hospitals. With the growing complexity of healthcare systems and the increasing
movement of care to the community, entry-level professional nurses need competencies in team-
based and coordinated care across a variety of venues. Consequently, the task force recommends
that entry-level professional nursing education prepare a generalist for practice across the
lifespan and continuum of care with emphasis in four areas or spheres of practice.
64
• Disease prevention/promotion of health and well-being, which includes the promotion of
physical and mental health in all patients as well as management of minor acute and
intermittent care needs of generally healthy patients;
• Chronic disease care, which includes management of chronic diseases and prevention of
negative sequela;
• Regenerative or restorative care, which includes critical/trauma care, complex acute care,
acute exacerbations of chronic conditions, and treatment of physiologically unstable
patients that generally requires care in a mega-acute care institution; and,
• Hospice/palliative/supportive care.
Competencies and Outcomes Expected of Entry-Level BSN Graduates. To prepare
graduates for the evolving healthcare system, programs will need to encompass didactic,
simulated, and clinical field learning opportunities in diverse settings, including community,
primary care, long-term care, acute care, hospice, and virtual care settings (telehealth).
Beginning competencies for patient care, care transitions and coordination, and population health
would be mastered within these four spheres of care, which are not setting-specific. For example,
a long-term care (LTC) facility may encompass all spheres of practice except, perhaps, the
regenerative (critical/trauma) sphere. Expected competencies for generalist, entry-level nursing
practice include observable and measurable competencies across the four spheres of care.
Competencies in other areas (including but not limited to professionalism, ethics, legal aspects of
practice, health policy and economics, clinical reasoning, advocacy, evidence-based practice,
population health, global health, social determinants of health, assessment, communication,
AACN’s Vision for Academic Nursing White Paper – January 2019
16
mental health, care coordination, and interprofessional team practice) are threaded and assessed
across the four spheres of care.
Substantial clinical experiences would need to be provided within appropriate areas/sites that
reflect the four spheres of care and include combinations of experiences in acute care,
ambulatory, primary care, LTC, palliative care, or other relevant settings. Also, these include
immersion (time and type) experiences for all entry-level learners encompassing one or more of
the four spheres of care near the end of the degree program. These experiences would be
designed to integrate learning into one’s clinical practice, increase care competencies, provide
continuity, and increase confidence in performing as a generalist nurse. As pre-registered nurse
licensure students, graduates from generalist bachelor’s entry degree programs will sit for the
NCLEX-RN®.
Competencies and outcomes expected of Entry-Level MSN graduates. As the
complexity of healthcare delivery and patient/population health needs continue to grow,
education preparation for the entry to professional nursing practice is expected to evolve to a
generalist master’s degree at some point in the future (some programs have already made this
transition). Similar to individuals applying to other health professions programs, generalist
master’s degree nursing programs require students to enter with a minimum of a bachelor’s
degree in another field. In addition to the entry-level professional nursing competencies and
areas of preparation (described in the previous section), master’s entry programs would provide
education for strengthened competencies in organizational and systems thinking, quality
improvement and safety, care coordination, interprofessional communication, and team-based
care and leadership. As pre-registered nurse licensure students, graduates from generalist
master’s entry-level degree programs, in addition to sitting for the NCLEX-RN
®
, would sit for a
certification exam that provides assurance of the additional competencies. This is in alignment
with the recommendation of the AACN Task Force on Education and Regulation II.
65
Eventually, it is envisioned that as entry-degree credentialing moves from a bachelor’s degree to
the masters’ degree, the RN licensure examination will completely evolve to encompass testing
of the master’s level entry competencies.
Transition to Practice. As described in the general recommendations, transition to
practice programs for baccalaureate or master’s entry nurses could be offered in any of the four
spheres: prevention/promotion of health and wellbeing, chronic disease care, regenerative
(critical/trauma) care, and hospice/palliative care. Courses in specialty areas could be offered as
stackable credentials or badges within an academic program or as part of a life-long program of
learning/career development. These would be designed and offered by schools or in conjunction
with practice partners to augment the generalist degree preparation and address identified needs
of employers and changes within the healthcare system.
Advanced Nursing Study: Doctoral Education
Nurses seeking a doctoral degree in nursing obtain their doctorate in practice or research.
Research-focused and practice-focused doctorates are terminal degrees in nursing. Individuals
holding either doctoral degree should be eligible for academic positions relevant to their degree,
background, and experience. The mix of faculty would form scholarly teams to reinforce how the
unique skill set of each degree (practice or research-focused) is critical to the development of
AACN’s Vision for Academic Nursing White Paper – January 2019
17
new knowledge and application of best evidence. Those pursuing a doctoral degree in nursing
(either research- or practice-focused) and interested in an academic career would seek additional
preparation through one of the three options for additional preparation in learning science and
pedagogy as delineated on page 13.
Doctoral Core. As advanced nursing practice degrees evolve to the practice doctorate,
the number of nurses interested in pursuing both a practice and a research degree is increasing. A
standardized core set of courses offered by all doctoral programs (practice and research-focused)
would facilitate dual degrees as well as transition from one type of program to another. An
advanced nursing (doctoral) standardized core (advanced level courses) could incorporate
advanced systems, health policy, and design thinking among other topics. An advanced nursing
(doctoral) core would allow students to easily transition from one track or degree to another as
well as standardize the expected outcomes of advanced nursing education. In addition to a
standardized doctoral core, opportunities or streamlined pathways from the research-focused
degree program to the practice doctorate program and from the practice doctorate to the research-
focused degree program increasingly will be available.
Practice Doctorate. Changes in higher education and the growing complexity of health
care have significantly impacted the entire nursing workforce, including those prepared for
advanced nursing practice. A shift to a practice doctorate from a specialty advanced practice
master’s degree is already in effect. Changes in healthcare delivery and demands for improved
outcomes and reduced costs have created burgeoning opportunities for nursing. For the future,
we envision the practice doctorate in nursing as the minimum academic degree for advanced
practice registered nurses and all other areas of advanced nursing practice, which encompass
both direct clinical care/services and systems/indirect nursing care/services.
66
After completing the advanced nursing (doctoral) core, students choose one of two broad
pathways: 1) direct point of care clinical practice or 2) systems/indirect nursing practice. Within
the pathway (whether it is a direct care or systems/indirect nursing practice focus) the student
pursues a population
51
or specialty track and masters the national competencies delineated for
that population or specialty. In either the direct or indirect pathways, practice-focused doctoral
education includes an immersion, practice experience in/with an appropriate setting/population
reflecting the track or area of advanced nursing practice. Pathway/track competence at program
completion is reflected in a relevant synthesis experience. After completing the practice
doctorate, opportunities to complete nursing or health science research-focused doctorates are
available in a streamlined path.
Research-Focused Doctoral Education. Within universities, the research-focused
doctorate is generally a PhD degree. AACN envisions that this degree remains a degree whose
structure and process are determined by the university/college in which it is embedded.
Regardless of degree designation the research-focused doctorate in nursing prepares for the
conduct of health-related knowledge generation through research. The research-focused doctoral
degree in nursing is open to those holding a minimum of a baccalaureate or higher degree in
nursing or in a related discipline. The course of study prepares individuals for the conduct of
individual and group research, as well as systems-focused research, interprofessional or nursing
practice research, and dissemination and implementation science. After completing the research-
AACN’s Vision for Academic Nursing White Paper – January 2019
18
focused degree in nursing, opportunities to complete practice-focused doctorates are available in
a streamlined path.
State of Current Programs
Current RN-BSN Programs. Given the need to move all registered nurses to
baccalaureate-level preparation at minimum, post-RN to BSN programs currently serve a
purpose. Current dual enrollment programs between community colleges and institutions
conferring the BSN represent emerging partnerships that can support the BSN as minimum
degree entry to the profession. In the best interests of the profession, any RN-BSN and dual
enrollment education should align with the baccalaureate competencies previously described.
Current Post-RN Master’s in Nursing Programs. With the shift of advanced specialty
practice to the practice doctorate degree not yet complete, some master’s degree programs still
encompass advanced specialty practice for practice at the point of care and over time will
necessitate post-APRN doctoral completion programs. However, as previously championed,
advanced nursing practice degrees will continue to evolve to the practice doctorate degree.
66
As
well, proliferating are master’s degree programs with a strong focus on indirect or systems
competencies (e.g., quality improvement and safety, health informatics, care coordination, and
leadership). These master’s degree programs are designed to complement point of care direct
practice competencies learned in becoming an RN while addressing systems competencies that
historically were addressed only at a basic level. This is in synchrony with the evolving RN role
increasingly being driven toward systems leadership and the coordination of care. Moreover,
these programs provide opportunities for nurses to advance their careers through graduate
education and assume greater accountability for care outcomes. The shift over time of these post
RN master’s degree programs to practice doctorate degrees remains to be seen but anticipated for
the future.
AACN’s Vision for Academic Nursing White Paper – January 2019
19
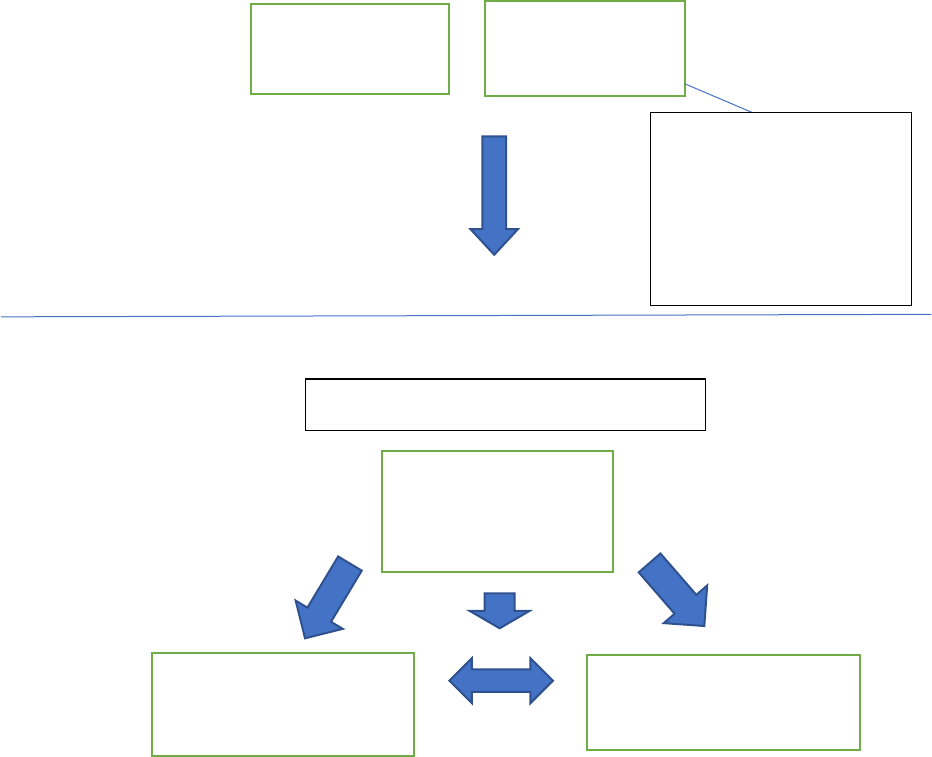
VISION FOR NURSING EDUCATION
EDUCATION PATHWAYS
Entry to the Profession
ADVANCED NURSING STUDY: Doctoral Education
BSN
Doctoral Core
Research-Focused
Doctoral Programs
Generalist MSN
In addition to NCLEX
generalist master’s
graduates sit for a
certification that
documents attainment of
the additional master’s level
competencies.
Admission to a doctoral program
Practice-Focused
(Direct and Indirect)
Doctoral Programs
Doctoral Programs
(Direct and Indirect)
AACN’s Vision for Academic Nursing White Paper – January 2019
20
Glossary
Competence - The array of abilities (knowledge, skills, and attitudes) across multiple domains or
aspects of performance in a certain context. Competence is multi-dimensional and dynamic. It
changes with time, experience, and settings.
67
Competency - An observable ability of a health professional, integrating multiple components
such as knowledge, skills, and attitudes. Since competencies are observable, they can be
measured and assessed to ensure their acquisition.
67
Competency-based Education (CBE) – An approach to preparing [clinicians] for practice that is
fundamentally oriented to a graduate’s outcome abilities and organized around competencies
derived from an analysis of societal and patient needs. It deemphasizes time-based training and
promises greater accountability, flexibility, and learner centeredness.
67
Design Thinking – An iterative process used to understand the user, challenge assumptions, and
redefine problems to identify alternative strategies and solutions that may not be apparent in
one’s initial understanding. The process is being taught around the world and across disciplines.
The process helps one systematically extract, teach, learn, and apply human-centered techniques
to solve problems in a creative way.
68
Digital Badge – a visual representation of an accomplishment, achievement, or skill acquisition –
more granular than a formal degree but helps to make incremental learning more visible.
4
Dual-Enrollment Program or Dual-Admission Program – The Dual Enrollment or Dual
Admission Model, also referred to as the Partnership Model, consists of an ADN and BSN
program collaborating to provide a simultaneous pathway for students to take courses at both
institutions. Students are concurrently enrolled in two separate programs; a degree is awarded for
both degrees (ADN from the community college and BSN from the collaborating BSN
institution.) Students may be allowed to take the licensure exam after the ADN or BSN
completion requirements, depending on the specific partnership.
69
Generalist Entry-level Master’s Degree – Entry-level or second-degree master’s program that
admits students with baccalaureate degrees in other disciplines and no previous nursing
education. The program prepares graduates for entry into the profession and awards a master’s
degree in nursing.
70
Holistic Admissions Review – Flexible, individualized way of assessing how an applicant will
fare as a student and as a future professional and member of society.
36
Patient – Includes individuals, families, groups, communities, and populations
71
Stackable Credentials - A sequence of credentials that can be accumulated over time and move
an individual along a career pathway or up a career ladder.
5
AACN’s Vision for Academic Nursing White Paper – January 2019
21
References
1. Josiah Macy Jr. Foundation. (June 2017). Achieving Competency-Based, Time-Variable
Health Professions Education Recommendations from the Macy Foundation
Conference. Accessed at
http://macyfoundation.org/docs/macy_pubs/JMF_CBTVHPE_Summary_web_JMF.pdf.
2. Chronicle of Higher Education. (2014) http://www.chronicle.com/blogs/ticker/college-
enrollments-drop-for-3rd-straight-year/91025
3. Bratcher, E. (August 2016). Can associations attract millennials with credentials?
Accessed at https://associationsnow.com/2016/08/can-associations-attract-millennials-
with-credentialing/
4. Educause (2018). Badging. Retrieved from https://www.educause.edu/badging
5. Department of Labor. (2015) (TEGL 15-10) Training and Guidance Labor Letter 15-
10. Retrieved from https://ows.doleta.gov/dmstree/tegl/tegl2k10/tegl_30-10.pdf
6. Nodine, T. R. (2016). How did we get here? A brief history of competency‐based higher
education in the United States. The Journal of Competency
‐
Based Education, 1(1), 5-11.
7. Frank J. R., Snell L. S., Cate O. T. et.al.(2010). Competency-based medical education:
Theory to practice. Medical Teacher (32), 638–645.
8. Englander, R., Cameron, T., Ballard, A. J., Dodge, J., Bull, J., & Aschenbrener, C.A.
(2013). Toward a common taxonomy of competency domains for the health professions
and competencies for physicians. Academic Medicine, 88(8), 1088-1094.
9. Hicks, P. J., Schumacher, D. J., Benson, B. J., Burke, A. E., Englander, R., Guralnick,
S., Ludwig, S., & Carraccio, C. (September 2010). The pediatrics milestones:
Conceptual framework, guiding principles, and approach to development. Journal of
Graduate Medical Education, pp 410-418.
10. Roach, K. E., Frost, J. S., Francis, N. J., Giles, S., Nordrum, J. T., & Delitto, A. (2012).
Validation of the Revised Physical Therapist Clinical Performance Instrument: Version
2006. Physical Therapy, Volume 92, 3, pp 416-428.
11. Kavanagh, J. M. & Szweda, C. (2017). A crisis in competency: The strategic and ethical
imperative to assessing new graduate nurses’ clinical reasoning. Nursing Education
Perspectives, 38(2), 57-62.
12. Litwack, K., & Brower, A. M. (2018). The University of Wisconsin-Milwaukee flexible
option for bachelor of science in nursing degree completion. Academic Medicine, 93,
3/March 2018 supplement; pp. 537-541.
13. Garrett, R. & Lurie, H. (2016). Deconstructing CBE: An assessment of institutional
activity, goals, and challenges in higher education. Eduventures. Retrieved from:
https://encoura.org/products-services/eduventures-research-and-advisory-
services/deconstructing-cbe/
14. Johnson, D. (2017). What’s keeping competency-based education out of higher
education’s mainstream? Retrieved from: https://evolllution.com/revenue-
streams/market_opportunities/whats-keeping-competency-based-education-out-of-
higher-educations-mainstream/
15. Norman, G., Norcini, J., & Bordage, G. (2014). Competency-based education:
Milestones or millstones? Journal of Graduate Medical Education, 6(1), 1-6.
16. Kogan, J. R., Whelan, A. J., Gruppen, L. D., Lingard, L. A., Teunissen, P. W., ten Cate O.
(2018). What regulatory requirements and existing structures must change if competency-based,
AACN’s Vision for Academic Nursing White Paper – January 2019
22
time-variable training is introduced into the continuum of medical education in the United
States? Academic Medicine, 93 (3)/ March 2018 Supplement; 527-531.
17. Seemiller, C., & Grace, M. (2016). Generation Z goes to college. Wiley & Sons: San
Francisco, CA.
18. Center for Generational Kinetics. (2016). Generational Breakdown: Info about all of the
generations. Retrieved from http://genhq.com/faq-info-about-generations/
19. Panopto
TM
. (2018). Are you ready to support 4 generations of learners? Retrieved from
https://www.panopto.com/blog/are-you-ready-to-support-4-generations-of-learners/.
20. Williams, A. (2015, September 20). Move Over, Millennials: Here Comes Generation
Z. Retrieved from https://www.nytimes.com/2015/09/20/fashion/move-over-millennials-
here-comes-generation-z.html.
21. Posner, A. (2017, January 11). What is Adaptive Learning Anyway? McGraw Hill
Education. Retrieved from https://www.mheducation.com/ideas/what-is-adaptive-
learning.html.
22. McMurtrie, B. (2018, August 12). How is Artificial Intelligence Changing Teaching?
The Chronical of Higher Education.
23. Marr, B. (2016, December 6). What is the difference between artificial intelligence and
machine learning? Forbes. Retrieved from
https://www.forbes.com/sites/bernardmarr/2016/12/06/what-is-the-difference-between-
artificial-intelligence-and-machine-learning/#20a6538e2742
24. Fang, D., & Kesten, K. (2017). Retirements and succession of nursing faculty in 2016-
2025. Nursing Outlook, 65:5, 633-642. doi:
https://doi.org/10.1016/j.outlook.2017.03.003
25. American Association of Colleges of Nursing. (2018). Research and Data Services.
26. Fang, D., Bednash, G. D., & Arietti, R. (2015). Identifying barriers and facilitators to
nurse faculty careers for PhD nursing students. Journal of Professional Nursing, Vol.
32, No. 3, pp 193-201
27. American Association of Colleges of Nursing. (2016). Advancing healthcare
transformation: A new era for academic nursing.
http://www.aacnnursing.org/Portals/42/AACN-New-Era-Report.pdf?ver=2017-07-06-
120430-557.
28. Vesely, R. (2014). The great migration. Hospitals & Health Networks. American
Hospital Association. Accessed at www.hhnmag.com/articles/5005-the-great-migration.
29. Rechtoris, M. (2016, March 9). 7 statistics on urgent care centers, EDs & retail clinics.
Retrieved from https://www.beckersasc.com/asc-quality-infection-control/5-statistics-
on-urgent-care-centers-emergency-departments.html.
30. Bodenheimer, T., & Mason, D. (2017). Registered Nurses: Partners in Transforming
Primary Care. Proceedings of a Conference sponsored by the Josiah Macy Jr.
Foundation in June 2016. New York: Josiah Macy Jr. Foundation, 2017. Accessed at
www.macyfoundation.org/docs/macy_pubs/Macy_Monograph_Nurses_2016_webPDF.
pdf.
31. U.S. Department of Health and Human Services, Health Resources and Services
Administration, Bureau of Health Workforce, National Center for Health Workforce.
(July 2017). Supply and Demand Projections of the Nursing Workforce: 2014-2030.
AACN’s Vision for Academic Nursing White Paper – January 2019
23
https://bhw.hrsa.gov/sites/default/files/bhw/nchwa/projections/NCHWA_HRSA_Nursin
g_Report.pdf
32. National Rural Health Association. (2012). Policy Brief: Health Care Workforce
Distribution and Shortage Issues in Rural America. Retrieved from
https://www.ruralhealthweb.org/getattachment/Advocate/Policy-
Documents/HealthCareWorkforceDistributionandShortageJanuary2012.pdf.aspx?lang=
en-US
33. Rural Health Information Hub. (2018). Rural Healthcare Information
https://www.ruralhealthinfo.org/topics/health-care-workforce#workforce.
34. U.S. Census Bureau. (2016). Quick Facts United States. Accessed March 2018 at
https://www.census.gov/quickfacts/fact/table/US/PST045216.
35. LaVeist, T. A & Pierre, G. (2014) Integrating the 3Ds-social determinants, health
disparities, and health-care workforce diversity. Public Health Reports, 2014 supplement
2, Vol. 129.
36. Association of American Medical Colleges (2014). About holistic admissions. Retrieved
from https://http://www.aamc.org/initiatives/holisticreview/about/2014 .
37. Urban Universities for Health (2014). Holistic Admissions in the Health Professions.
Retrieved from
http://urbanuniversitiesforhealth.org/media/documents/Holistic_Admissions_in_the_Hea
lth_Professions.pdf 2014.
38. Glazer, G., Clark, A., Bankston, K, Danek, J., Fair, M., & Michaels, J. (2016). Holistic
admissions in nursing: We can do this. Journal of Professional Nursing, Vol. 32, 4,
306-313.
39. NCSBN. (2018). Life Cycle of the NCLEX Test Plan. Accessed February 2018 at
https://www.ncsbn.org/The_Life_Cycle_of_the_NCLEX_Test_Plan.pdf
40. NCSBN. (2018). The Next Generation NCLEX. https://www.ncsbn.org/next-generation-
nclex.htm.
41. American Association of Colleges of Nursing (2002). Task Force on Education and
Regulation I.
42. Aiken, L. H., Clarke, S. P., Cheung, R. B., Sloane, D. M., & Silber, J.H. (2003).
Educational levels of hospital nurses and surgical patient mortality. Journal of the
American Medical Association, 290(12), 1617-1623.
43. Friese, C. R., Lake, E. T., Aiken, L. H., Silber, J. H., & Sochalski, J. (2008). Hospital
nurse practice environments and outcomes for surgical oncology patients. Health
Services Research, 43(4), 1145-1163.
44. Blegan, M. A., Goode, C. J., Park, S. H., Vaughn, T., & Spetz, J., (2013). Baccalaureate
education in nursing and patient outcomes. Journal of Nursing Administration, 43(2),
89-94.
45. Yakusheva, O., Lindrooth, R., & Weiss, M. (2014). Economic evaluation of the 80%
baccalaureate nurse workforce recommendation: A patient-level analysis. Medical Care,
52(10), 864-869.
46. Ott, K. M., Haddock, K. S., Fox, S. E., Shinn, J. K. et. al. (2009). Nursing Economics
27(6), 363-383.
47. Bender, M., Connelly, C. D., Glaser, D., Brown, C. (2012), Clinical Nurse Leader
impact on microsystem care quality. Nursing Research, October 1, 2012, 326-333.
AACN’s Vision for Academic Nursing White Paper – January 2019
24
48. Sheets, M., Bonnah, B., Kareivis, J., Abraham, P., Sweeney, M., & Strauss, J. (2012).
CNLs make a difference. Nursing2012, August 1, 2012, 54-58.
49. Bender, M. (2014). The current evidence base for the Clinical Nurse Leader: A narrative
review of the literature. Journal of Professional Nursing, 30(2), 110-123.
50. Murphy, E. A. (2014). Healthcare reform-A new role for changing times: Embracing the
Clinical Nurse Leader role–A strategic partnership to drive outcomes. Nurse Leader,
August 2014, 53-57.
51. APRN Consensus Work Group and NCSBN APRN Advisory Committee. (2008).
Consensus Model for APRN Regulation: Licensure, Accreditation, Certification &
Education. Accessed February 2018 at
http://www.aacnnursing.org/Portals/42/AcademicNursing/pdf/APRNReport.pdf?ver=20
17-05-15-111341-617.
52. Smiley R., Bauer, P., Bienemy C., Berg, J., Shireman E., Reneau K., Alexander M. The
2017 national nursing workforce survey. Journal of Nursing Regulation 9(3), S1-S88.
53. American Association of Colleges of Nursing (2017). Diversity, Inclusion, & Equity in
Academic Nursing. http://www.aacnnursing.org/News-Information/Position-Statements-
White-Papers/Diversity.
54. Glazer, G., & Bankston, K. (September 2014). Holistic admissions in the health
professions – Results of a National Study. Retrieved July 18, 2016, from
http://urbanuniversitiesforhealth.org/media/documents/holisticadmissionsinthehealthprof
essions.pdf.
55. Ring, M., Tieraona L. D., Sierpina, V., Bailey, M., Locke, A., Kogan, M., Rindfleisch, J.
A., & Saper, R. (2014). Developing and implementing core competencies for integrative
medicine fellowships. Academic Medicine 89(3), 421-428.
56. Wagner, L. M., Dolansky, M. A., & Englander, R. (2018) Entrustable professional
activities for quality and patient safety. Nursing Outlook, 66, 3, pp. 237-243.
57. American Council on Education and Blackboard (2014). The currency of higher
education: Credits and competencies. Retrieved from:
https://www.luminafoundation.org/files/resources/currency-of-he.pdf
58. Gruppen, L., Mangrulkar, R., & Kolars, J. (2012). The promise of competency-based
education in the health professions for improving global health. Human Resources for
Health. Retrieved from: https://human-resources-
health.biomedcentral.com/articles/10.1186/1478-4491-10-43
59. American Association of Colleges of Nursing and American Organization of Nurse
Executives Task Force on Academic Practice Partnerships. (2012). Guiding Principles to
Academic Practice Partnerships. http://www.aacnnursing.org/Academic-Practice-
Partnerships/The-Guiding-Principles.
60. Harper, D. C., McGuinness, T. M., & Johnson, J. (2017). Clinical residency training: Is
it essential to the Doctor of Nursing Practice for nurse practitioner preparation? Nursing
Outlook, 65(1), 50-57.
61. Rugen, K. W., Dolansky M. A., Dulay M., King S., & Harada, N. (2018). Evaluation of
veterans affairs primary care nurse practitioner residency: Achievement of
competencies. Nursing Outlook 66(1), 25-34.
62. American Association of Colleges of Nursing (2017). The Preferred Vision of the
Professoriate in Baccalaureate and Graduate Nursing Programs.
http://www.aacnnursing.org/Portals/42/News/Position-Statements/Professoriate.pdf.
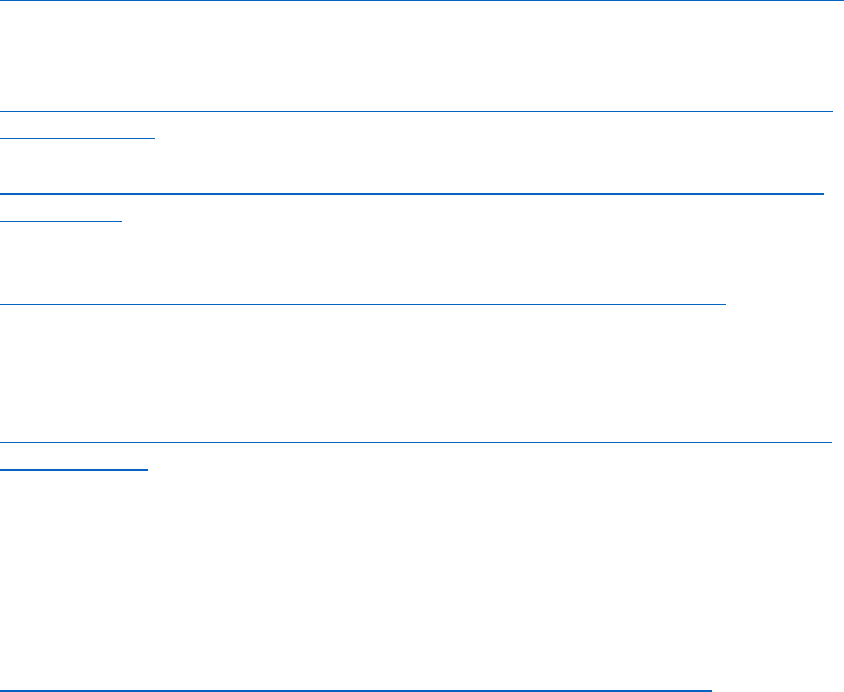
AACN’s Vision for Academic Nursing White Paper – January 2019
25
63. Farmer, P., Gerardi, T., Thompson, P., & Hoffman, B. (2018). Academic Progression in
Nursing (APIN) Final program summary and outcomes.
https://nepincollaborative.org/wp-content/uploads/2018/03/FINAL-APIN-REPORT.pdf
64. Lipstein, S. H, Kellermann, A. L., Berkowitz, B., Phillips, R., Sklar, D., Steele, G. D., &
Thibault, G. E. (September 2016). Workforce for 21st century health and health care: A
vital direction for health and health care. National Academies of Medicine.
https://nam.edu/wp-content/uploads/2016/09/Workforce-for-21st-Century-Health-and-
Health-Care.pdf
65. American Association of Colleges of Nursing (2004). Dialogue with the Board.
http://www.aacnnursing.org/Portals/42/CNL/Spring04Dialogue.pdf?ver=2017-07-31-
204147-573.
66. American Association of Colleges of Nursing. (2004). AACN Position Statement on the
Practice Doctorate in Nursing. Available at
http://www.aacnnursing.org/Portals/42/News/Position-Statements/DNP.pdf.
67. Frank J. R., Mungroo, R., Ahmad Y., Wang, M., DeRossi S., & Horsley, T. (2010).
Toward a definition of competency-based education in medicine: a systematic review of
published definitions. Medical Teacher (32) 631-637.
68. Dam R., & Siang T. (2019) What is Design Thinking and Why is it so Popular.
https://www.interaction-design.org/literature/article/what-is-design-thinking-and-why-
is-it-so-popular.
69. NEPIN. (2019). Models for Academic Progression.
https://nepincollaborative.org/models/dual-or-partnership-models/
70. American Association of Colleges of Nursing. (2017). 2016-2017 Enrollment and
Graduations in Baccalaureate and Graduate Programs in Nursing. Washington, DC:
Author.
71. American Association of Colleges of Nursing. (2008). The Essentials of Baccalaureate
Education for Professional Nursing Practice.
http://www.aacnnursing.org/Portals/42/Publications/BaccEssentials08.pdf
AACN’s Vision for Academic Nursing White Paper – January 2019
26
Task Force on AACN’s Vision for Nursing Education
Christine Pacini, PhD, Chair
Dean Consultant and Professor
University of Detroit Mercy
Mary Bishop, DNP
Associate Professor
University of West Georgia
Ginny Bowman, MSN
Director of Clinical Nursing
MD Anderson Cancer Center
Jean Giddens, PhD
Dean and Professor
Virginia Commonwealth University
Jeanne-Marie Havener, PhD
Director of Nursing
Castleton University
Cynthia McCurren, PhD
Dean, Kirkhof College of Nursing
Grand Valley State University,
Joan Shaver, PhD
Professor
University of Arizona
Joan Stanley, PhD, AACN Staff Liaison
Chief Academic Officer
Rick García, PhD. AACN Staff Liaison
Director of Nursing Education
