
Enhancing Motivation for Change in
Substance Use Disorder Treatment
TI
TREATMENT I
P
MPROVEMENT
35
PROTOCOL
UPDATED 2019
This page intentionally left blank

This page intentionally left blank

TIP 35
Contents
Foreword ................................................................. viii
Executive Summary .......................................................... ix
TIP Development Participants ..................................................xv
Publication Information...................................................... xxi
Chapter 1—A New Look at Motivation .......................................1
Motivation and Behavior Change ..............................................4
Changing Perspectives on Addiction and Treatment...............................6
TTM of the SOC ...........................................................13
Conclusion................................................................16
Chapter 2—Motivational Counseling and Brief Intervention...................17
Elements of Eective Motivational Counseling Approaches........................17
Motivational Counseling and theSOC .........................................23
Special Applications of Motivational Interventions ...............................26
Brief Motivational Interventions ..............................................30
Screening, Brief Intervention, and Referral to Treatment ..........................32
Conclusion................................................................33
Chapter 3—Motivational Interviewing as a Counseling Style ..................35
Introduction to MI .........................................................35
What Is New in MI .........................................................37
Ambivalence ..............................................................38
Core Skills of MI: OARS......................................................41
Four Processes of MI........................................................48
Benets of MI in Treating SUDs...............................................63
Conclusion............................................................... 64
Chapter 4—From Precontemplation to Contemplation: Building Readiness .....65
Develop Rapport and Build Trust .............................................66
Raise Doubts and Concerns About the Client’s Substance Use......................71
Treatment ..............................................................77
Conclusion................................................................81
Understand Special Motivational Counseling Considerations for Clients Mandated to
Chapter 5—From Contemplation to Preparation: Increasing Commitment......83
Normalize and ResolveAmbivalence ......................................... 84
Help Tip the Decisional Balance Toward Change ................................87
Conclusion................................................................93
v

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Chapter 6—From Preparation to Action: Initiating Change ....................95
Explore Client Change Goals .................................................96
Develop a Change Plan .....................................................99
Support the Client’s Action Steps ............................................107
Evaluate the Change Plan ..................................................108
Conclusion...............................................................108
Chapter 7—From Action to Maintenance: Stabilizing Change.................109
Stabilize Client Change.....................................................110
Support the Client’s Lifestyle Changes ........................................117
Help the Client Reenter the Change Cycle .....................................120
Conclusion...............................................................124
Chapter 8—Integrating Motivational Approaches in SUD Treatment Settings .125
Adaptations of Motivational Counseling Approaches ............................126
Workforce Development ...................................................131
Conclusion...............................................................135
Appendix A—Bibliography....................................................137
Appendix B—Screening and Assessment Instruments..............................149
1. U.S. Alcohol Use Disorders Identication Test (AUDIT) .........................150
2. Drug Abuse Screening Test (DAST-10) ......................................152
3. Drinker Inventory of Consequences (DrInC) (Lifetime) .........................154
4. What I Want From Treatment (2.0). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .157
5. Readiness to Change Questionnaire (Treatment Version) (RCQ-TV) (Revised) ......160
6. Stages of Change Readiness and Treatment Eagerness Scale–Alcohol
(SOCRATES 8A) .........................................................162
7. Stages of Change Readiness and Treatment Eagerness Scale–Drug (SOCRATES 8D) .164
8. University of Rhode Island Change Assessment (URICA) Scale...................168
9. Alcohol and Drug Consequences Questionnaire (ADCQ) .......................171
10. Alcohol Decisional Balance Scale .........................................173
11. Drug Use Decisional Balance Scale ........................................175
12. Brief Situational Condence Questionnaire (BSCQ)...........................177
13. Alcohol Abstinence Self-Ecacy Scale (AASES) ..............................179
14. Motivational Interviewing Knowledge Test .................................181
Appendix C—Resources ......................................................186
Motivational Interviewing and Motivational Enhancement Therapy................186
Stages of Change .........................................................186
Training and Supervision ...................................................186
Substance Abuse and Mental Health Services Administration .....................187
vi

TIP 35
Exhibits
Exhibit 1.1. Models of Addiction .................................................7
Exhibit 1.2. Examples of Natural Changes ........................................13
Exhibit 1.3. The Five Stages in the SOC in the TTM .................................14
Exhibit 2.1. The Drinker’s Pyramid Feedback ......................................19
Exhibit 2.2. Catalysts for Change ...............................................24
Exhibit 2.3. Counselor Focus in the SOC ..........................................25
Exhibit 2.4. RESPECT: A Mnemonic for Cultural Responsiveness ......................27
Exhibit 3.1. A Comparison of Original and Updated Versions of MI....................37
Exhibit 3.2. Misconceptions and Clarications About MI ............................38
Exhibit 3.3. Examples of Change Talk and Sustain Talk..............................40
Exhibit 3.4. Closed and Open Questions .........................................41
Exhibit 3.5. Gordon’s 12 Roadblocks to Active Listening ........................... 44
Exhibit 3.6. Types of Reective Listening Responses ................................46
Exhibit 3.7. Components in a Sample Agenda Map ................................51
Exhibit 3.8. Examples of Open Questions to Evoke Change Talk Using DARN ...........53
Exhibit 3.9. The Importance Ruler ..............................................54
Exhibit 3.10. The Condence Ruler ..............................................60
Exhibit 4.1. Counseling Strategies for Precontemplation.............................66
Exhibit 4.2. Styles of Expression in the Precontemplation Stage: The5Rs ..............69
Exhibit 4.3. An Opening Dialog With a Client Who Has Been Mandated to Treatment....79
Exhibit 5.1. Counseling Strategies for Contemplation .............................. 84
Exhibit 5.2. The Motivational Interviewing (MI) Hill of Ambivalence ..................85
Exhibit 5.3. Decisional Balance Sheet for Substance Use ............................88
Exhibit 5.4. Other Issues in Decisional Balance ....................................89
Exhibit 5.5. Recapitulation Summary ............................................92
Exhibit 6.1. Counseling Strategies for Preparation and Action ........................96
Exhibit 6.2. When Treatment Goals Dier ........................................98
Exhibit 6.3. Change Plan Worksheet............................................101
Exhibit 6.4. Mapping a Path for Change When There Are Multiple Options ...........104
Exhibit 7.1. Counseling Strategies for Action and Relapse...........................110
Exhibit 7.2. Options for Responding to a Missed Appointment ......................114
Exhibit 7.3. Triggers and Coping Strategies ......................................116
Exhibit 7.4. A Menu of Coping Strategies........................................117
Exhibit 7.5. Susan’s Story: A Client Lacking Social Support ..........................119
Exhibit 7.6. Marlatt’s RPC Process ..............................................121
Exhibit 8.1. Blending the Spirit of MI With CBT ...................................130
vii

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
Foreword
The Substance Abuse and Mental Health Services Administration (SAMHSA) is the U.S. Department of
Health and Human Services agency that leads public health efforts to reduce the impact of substance
abuse and mental illness on America’s communities. An important component of SAMHSA’s work is
focused on dissemination of evidence-based practices and providing training and technical assistance to
healthcare practitioners on implementation of these best practices.
The Treatment Improvement Protocol (TIP) series contributes to SAMHSA’s mission by providing science-
based, best-practice guidance to the behavioral health field. TIPs reflect careful consideration of all
relevant clinical and health service research, demonstrated experience, and implementation requirements.
Select nonfederal clinical researchers, service providers, program administrators, and patient advocates
comprising each TIP’s consensus panel discuss these factors, offering input on the TIP’s specific topics in
their areas of expertise to reach consensus on best practices. Field reviewers then assess draft content and
the TIP is finalized.
The talent, dedication, and hard work that TIP panelists and reviewers bring to this highly participatory
process have helped bridge the gap between the promise of research and the needs of practicing
clinicians and administrators to serve, in the most scientifically sound and effective ways, people in need of
care and treatment of mental and substance use disorders. My sincere thanks to all who have contributed
their time and expertise to the development of this TIP. It is my hope that clinicians will find it useful and
informative to their work.
Elinore F. McCance-Katz, M.D., Ph.D.
Assistant Secretary for Mental Health and Substance Use
U.S. Department of Health and Human Services
Substance Abuse and Mental Health Services Administration
viii

TIP 35
Executive Summary
Motivation for change is a key component in addressing substance misuse. This Treatment Improvement
Protocol (TIP) reflects a fundamental rethinking of the concept of motivation as a dynamic process, not a
static client trait. Motivation relates to the probability that a person will enter into, continue, and adhere to
a specific change strategy.
Although much progress has been made in identifying people who misuse substances and who have
substance use disorders (SUDs) as well as in using science-informed interventions such as motivational
counseling approaches to treat them, the United States still faces many SUD challenges. For example, the
National Survey on Drug Use and Health (Substance Abuse and Mental Health Services Administration,
2018) reports that, in 2017, approximately:
•
140.6 million Americans ages 12 and older currently consumed alcohol, 66.6 million reported
at least 1 episode of past-month binge drinking (defined as 5 or more drinks on the same
occasion on at least 1 day in the past 30 days for men and 4 or more drinks on the same
occasion on at least 1 day in the past 30 days for women), and 16.7 million drank heavily in
the previous month (defined as binge drinking on 5 or more days in the past 30 days).
•
30.5 million people ages 12 and older had used illicit drugs in the past month.
•
11.4 million people ages 12 and older misused opioids (defined as prescription pain reliever
misuse or heroin use) in the past year.
•
8.5 million adults ages 18 and older (3.4 percent of all adults) had both a mental disorder and
at least 1 past-year SUD.
•
18.2 million people who needed SUD treatment did not receive specialty treatment.
•
One in three people who perceived a need for substance use treatment did not receive it
because they lacked healthcare coverage and could not afford treatment.
•
Two in five people who perceived a need for addiction treatment did not receive it because
they were not ready to stop using substances.
Millions of people in the United States with SUDs are not receiving treatment. Many are not seeking
treatment because their motivation to change their substance use behaviors is low.
The motivation-enhancing approaches and strategies
this TIP describes can increase participation and
retention in SUD treatment and positive treatment
outcomes, including:
•
Reductions in alcohol and drug use.
•
Higher abstinence rates.
•
Successful referrals to treatment.
This TIP shows how SUD treatment counselors can influence positive behavior change by developing
a therapeutic relationship that respects and builds on the client’s autonomy. Through motivational
enhancement, counselors become partners in the client’s change process.
The TIP also describes different motivational interventions counselors can apply to all the stages in the
Stages of Change (SOC) model related to substance misuse and recovery from addiction.
A consensus panel developed this TIP’s content based on a review of the literature and on panel members’
extensive experience in the field of addiction treatment. Other professionals also generously contributed
their time and commitment to this project.
ix

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Intended Audience
The primary audiences for this TIP are:
•
Drug and alcohol treatment service providers.
•
Mental health service providers, such as
psychologists, licensed clinical social workers,
and psychiatric/mental health nurses.
•
Peer recovery support specialists.
•
Behavioral health program managers, directors,
and administrators.
•
Clinical supervisors.
•
Healthcare providers, such as primary care
physicians, nurse practitioners, general/family
medicine practitioners, registered nurses,
internal medicine specialists, and others who
may need to enhance motivation to address
substance misuse in their patients.
Secondary audiences include prevention
specialists, educators, and policymakers for SUD
treatment and related services.
Overall Key Messages
Motivation is key to substance use behavior
change. Counselors can support clients’ movement
toward positive changes in their substance use
by identifying and enhancing motivation that
alreadyexists.
Motivational approaches are based on the
principles of person-centered counseling.
Counselors’ use of empathy, not authority and
power, is key to enhancing clients’ motivation to
change. Clients are experts in their own recovery
from SUDs. Counselors should engage them in
collaborative partnerships.
Ambivalence about change is normal.
Resistance to change is an expression of
ambivalence about change, not a client trait
or characteristic. Confrontational approaches
increase client resistance and discord in the
counseling relationship. Motivational approaches
explore ambivalence in a nonjudgmental and
compassionate way.
The Transtheoretical Model (TTM) of the SOC
approach is an overarching framework that helps
counselors tailor specific counseling strategies
to different stages. Motivational counseling
strategies should be tailored to clients’ level of
motivation to change their substance use behaviors
at each of the five stages of the SOC:
•
Precontemplation
•
Contemplation
•
Preparation
•
Action
•
Maintenance
Effective motivational counseling approaches
can be brief. A growing body of evidence
indicates that early and brief interventions
demonstrate positive treatment outcomes in a
wide variety of settings including specialty SUD
treatment programs, primary care offices, and
emergency departments. Brief interventions
emphasize reducing the health-related risk
of a person’s substance use and decreasing
consumption as an important treatment outcome.
Motivational interviewing (MI) and other
motivational counseling approaches like
motivational enhancement therapy are effective
ways to enhance motivation throughout the
SOC. Motivational counseling approaches are
based on person-centered counseling principles
that focus on helping clients resolve ambivalence
about changing their substance use and other
health-risk behaviors.
MI is the most widely researched and
disseminated motivational counseling
approach in SUD treatment. The spirit of MI
(i.e., partnership, acceptance, compassion,
and evocation) is the foundation of the core
counseling skills required for enhancing clients’
motivation to change. The core counseling skills
of MI are described in the acronym OARS (Open
questions, Affirmations, Reflective listening,
andSummarization).
Counselor empathy, as expressed through
reflective listening, is fundamental to MI. Use
of empathy, rather than power and authoritative
approaches, is critical for helping clients achieve
and maintain lasting behavior change.
x

TIP 35
Adaptations of MI enhance the implementation
and integration of motivational interventions
into standard treatment methods. Training,
ongoing supervision, and coaching of counselors
are essential for workforce development and
integration of motivational counseling approaches
into SUD treatment.
Content Overview
Chapter 1—A New Look at Motivation
This chapter lays the groundwork for
understanding treatment concepts discussed
later in the TIP. It is an overview of the nature of
motivation and its link to changing substance
use behaviors. The chapter describes changing
perspectives on addiction and addiction treatment
in the United States and uses the TTM of the
SOC approach as an overarching framework to
understand how people change their substance
use behaviors.
In Chapter 1, readers will learn that:
•
Motivation is essential to substance use
behavior change. It is multidimensional,
dynamic, and fluctuating; can be enhanced; and
is influenced by the counselor’s style.
•
Benefits of using motivational counseling
approaches include clients’ enhancing
motivation to change, preparing them to enter
treatment, engaging and retaining clients in
treatment, increasing their participation and
involvement in treatment, improving their
treatment outcomes, and encouraging a rapid
return to treatment if they start misusing
substances again.
•
New perspectives on addiction treatment
include focusing on clients’ strengths
instead of deficits, offering person-centered
treatment, shifting away from labeling clients,
using empathy, focusing on early and brief
interventions, recognizing that there is a range
of severity of substance misuse, accepting risk
reduction as a legitimate treatment goal, and
providing access to integrated care.
•
People go through stages in the SOC approach;
this concept is known as the TTM of change.
•
The stages in the SOC model are:
-
Precontemplation, in which people are not
considering change.
-
Contemplation, in which people are
considering change but are unsure how
tochange.
-
Preparation, in which people have identified
a change goal and are forming a plan
tochange.
-
Action, in which people are taking steps
tochange.
-
Maintenance, in which people have met
their change goal and the behavior change
isstable.
Chapter 2—Motivational Counseling and
Brief Intervention
This chapter is an overview of motivational
counseling approaches, including screening, brief
intervention, and referral to treatment (SBIRT).
It describes elements of effective motivational
counseling approaches, including FRAMES
(Feedback, Responsibility, Advice, Menu of
options, Empathy, and Self-efficacy), decisional
balancing, discrepancy development, flexible
pacing, and maintenance of contact with clients.
The chapter describes counselors’ focus in each
stage of the SOC model. It addresses special
applications of motivational counseling with
clients from diverse cultures and with clients who
have co-occurring substance use and mental
disorders (CODs).
In Chapter 2, readers will learn that:
•
Each stage in the SOC approach has
predominant experiential and behavioral
catalysts for client change on which counselors
should focus.
•
Counselors should adopt the principles of
cultural responsiveness and adapt motivational
interventions to those principles when treating
clients from diverse backgrounds.
•
Even mild substance misuse can impede
functioning in people with CODs, including
co-occurring severe mental illness. Counselors
can adapt motivational interventions for
these clients.
xi

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
•
Brief motivational interventions, including SBIRT,
are effective in specialty SUD treatment facilities
and opportunistic settings (e.g., primary care
offices, emergency departments).
•
Brief interventions emphasize risk reduction
and referral to specialty addiction treatment
ifneeded.
Chapter 3—Motivational Interviewing as
a Counseling Style
This chapter provides an overview of the spirit of
MI, the principles of person-centered counseling,
the core counseling skills of MI (i.e. asking open
questions, affirming, reflective listening, and
summarizing), and the four processes of MI (i.e.,
engaging, focusing, evoking, and planning). It
describes what’s new in MI and dispels many
misconceptions about MI. The chapter discusses
the components that counselors use to help clients
resolve ambivalence and move toward positive
substance use behavior change.
In Chapter 3, readers will learn that:
•
Ambivalence about substance use and change is
normal and a motivational barrier to substance
use behavior change, if not explored.
•
The spirit of MI embodies the principles of
person-centered counseling and is the basis of
an empathetic, supportive counseling style.
•
Sustain talk is essentially statements the client
makes for not changing (i.e., maintaining the
status quo), and change talk is statements
the client makes in favor of change. The key
to helping the client move in the direction
toward changing substance use behaviors
is to evoke change talk and soften or lessen
the impact of sustain talk on the client’s
decision-makingprocess.
•
The acronym OARS describes the core skills
ofMI:
-
Asking Open questions
-
Affirming the client’s strengths
-
Using Reflective listening
-
Summarizing client statements
•
Reflective listening is fundamental to person-
centered counseling in general and MI in
particular and is essential for expressing
empathy.
•
The four processes in MI (i.e., engaging,
focusing, evoking, and planning) provide an
overarching framework for employing the core
skills in conversations with a client.
•
The benefits of MI include its broad applicability
to diverse medical and behavioral health
problems and its capacity to complement
other counseling approaches and to mobilize
clientresources.
Chapter 4—From Precontemplation to
Contemplation: Building Readiness
This chapter discusses strategies counselors
can use to help clients raise doubt and concern
about their substance use and move toward
contemplating the possibility of change. It
emphasizes the importance of assessing clients’
readiness to change, providing personalized
feedback to them about the effects and risks
of substance misuse, involving their significant
others in counseling to raise concern about
clients’ substance use behaviors, and addressing
special considerations for treating clients who are
mandated to treatment.
In Chapter 4, readers will learn that:
•
A client in the Precontemplation stage is
unconcerned about substance use or is not
considering change.
•
The counselor’s focus in Precontemplation is
to establish a strong counseling alliance and
raise the client’s doubts and concerns about
substance use.
•
Key strategies in this stage include eliciting the
client’s perception of the problem, exploring
the events that led to entering treatment, and
identifying the client’s style of Precontemplation.
•
Providing personalized feedback on assessment
results and involving significant others in
counseling sessions are key strategies for
raising concern and moving the client toward
contemplating change.
•
Special considerations in motivational
counseling approaches for clients mandated
to treatment include acknowledging client
ambivalence and emphasizing personal choice
and responsibility.
xii

TIP 35
Chapter 5—From Contemplation to
Preparation: Increasing Commitment
This chapter describes strategies to increase
clients’ commitment to change by normalizing
and resolving ambivalence and enhancing their
decision-making capabilities. It emphasizes
decisional balancing and exploring clients’ self-
efficacy as important to moving clients toward
preparing to change substance use behaviors.
Summarizing change talk and exploring the
client’s understanding of change prepare clients to
take action.
In Chapter 5, readers will learn that:
•
In the Contemplation stage, the client
acknowledges concerns about substance use
and is considering the possibility of change.
•
The counselor’s focus in Contemplation is to
normalize and resolve client ambivalence and
help the client tip the decisional balance toward
changing substance use behaviors.
•
Key motivational counseling strategies for
resolving ambivalence include reassuring the
client that ambivalence about change is normal;
evoking DARN (Desire, Ability, Reasons, and
Need) change talk; and summarizing the
client’sconcerns.
•
To reinforce movement toward change, the
counselor reinforces the client’s understanding
of the change process, reintroduces
personalized feedback, explores client self-
efficacy, and summarizes client change talk.
•
The counselor encourages the client to
strengthen his or her commitment to change by
taking small steps, going public, and envisioning
life after changing substance use behaviors.
Chapter 6—From Preparation to Action:
Initiating Change
This chapter describes the process of helping
clients identify and clarify change goals. It also
focuses on how and when to develop change
plans with clients and suggests ways to ensure that
plans are accessible, acceptable, and appropriate
for clients.
In Chapter 6, readers will learn that:
•
In the Preparation stage, the client is committed
and planning to make a change but is unsure of
what to do next. In the Action stage, the client
is actively taking steps to change but has not
reached stable recovery.
•
In Preparation, the counselor focuses on helping
the client explore change goals and develop a
change plan. In Action, the counselor focuses on
supporting client action steps and helping the
client evaluate what is working and not working
in the change plan.
•
The client who is committed to change and who
believes change is possible is prepared for the
Action stage.
•
Sobriety sampling, tapering down, and trial
moderation are goal-sampling strategies
that may be helpful to the client who is not
committed to abstinence as a change goal.
•
Creating a change plan is an interactive process
between the counselor and client. The client
should determine and drive change goals.
•
Identifying and helping the client reduce
barriers to the Action stage are important to the
change-planning process.
•
Counselors can support client action by
reinforcing client commitment and continuing
to evoke and reflect CAT (i.e., Commitment,
Activation, and Taking steps) change talk in
ongoing conversations.
Chapter 7—From Action to Maintenance:
Stabilizing Change
This chapter addresses ways in which motivational
strategies can be used effectively to help clients
maintain the gains they have made by stabilizing
change, supporting lifestyle changes, managing
setbacks during the Maintenance stage, and
helping them reenter the cycle of change if
they relapse or return to substance misuse. It
emphasizes creating a coping plan to reduce the
risk of recurrence in high-risk situations, identifying
new behaviors that reinforce change, and
establishing relapse prevention strategies.
In Chapter 7, readers will learn that:
•
During the Maintenance stage, the client has
achieved the initial change goals and is working
toward maintaining those changes.
xiii

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
•
In Maintenance, the counselor focuses on
helping the client stabilize change and supports
the client’s lifestyle changes.
•
During a relapse, the client returns to
substance misuse and temporarily exits
the change cycle. The counselor focuses
on helping the client reenter the cycle of
change and providing relapse prevention
counseling in accordance with the principles of
person-centeredcounseling.
•
Maintenance of substance use behavior change
in the SOC model must address the issue of
relapse. Relapse should be reconceptualized
as a return to or recurrence of substance use
behaviors and viewed as a common occurrence.
•
Relapse prevention counseling is a cognitive–
behavioral therapy (CBT) method, but the
counselor can use motivational counseling
strategies to engage the client in the process
and help the client resolve ambivalence about
learning and practicing new coping skills.
•
Strategies to help a client reenter the change
cycle after a recurrence include affirming
the client’s willingness to reconsider positive
change, exploring reoccurrence as a learning
opportunity, helping the client find alternative
coping strategies, and maintaining supportive
contact with the client.
Chapter 8—Integrating Motivational
Approaches in SUD Treatment Settings
This chapter discusses some of the adaptations
of motivational counseling approaches applicable
to SUD treatment programs and workforce
development issues that treatment programs
should address to fully integrate and sustain
motivational counseling approaches. It emphasizes
blending MI with other counseling approaches.
It also explores ways in which ongoing training,
supervision, and coaching are essential to
successful workforce development and integration.
In Chapter 8, readers will learn that:
•
Integrating motivational counseling approaches
into a treatment program requires a broad
integration of the philosophy and underlying
spirit of MI throughout the organization.
•
Adapted motivational interventions may be
more cost effective, accessible to clients,
and easily integrated into existing treatment
approaches than expected and may ease some
workload demands on counselors.
•
Technology adaptations, including motivational
counseling and brief interventions over the
phone or via text messaging, are effective,
cost effective, and adaptable to different
clientpopulations.
•
MI is effective when blended with
other counseling approaches including
group counseling, the motivational
interviewing assessment, CBT, and recovery
managementcheckups.
•
The key to workforce development is to train
all clinical and support staffs in the spirit of
MI so that the entire program’s philosophy is
aligned with person-centered principles, like
emphasizing client autonomy and choice.
•
Program administrators should assess the
organization’s philosophy and where it is
in the SOC model before implementing a
trainingprogram.
•
Training counseling staff in MI takes more than
a 1- or 2-day workshop. Maintenance of skills
requires ongoing training and supervision.
•
Supervision and coaching in MI should be
competency based. These activities require
directly observing the counselor’s skill level and
using coding instruments to assess counselor
fidelity. Supervision should be performed in the
spirit of MI.
•
Administrators need to balance training,
supervision, and strategies to enhance
counselor fidelity to MI with costs, while
partnering with counseling staff to integrate a
motivational counseling approach throughout
theorganization.
xiv

TIP 35
TIP Development Participants
Consensus Panel
Each Treatment Improvement Protocol’s (TIP)
consensus panel is a group of primarily nonfederal
addiction-focused clinical, research, administrative,
and recovery support experts with deep
knowledge of the TIP’s topic. With the Substance
Abuse and Mental Health Services Administration’s
Knowledge Application Program team, members
of the consensus panel develop each TIP via a
consensus-driven, collaborative process that blends
evidence-based, best, and promising practices
with the panel members’ expertise and combined
wealth of experience.
Chair
William R. Miller, Ph.D.
Regents Professor of Psychology and Psychiatry
Director of Research
Center on Alcoholism, Substance Abuse, and
Addictions
Department of Psychology
University of New Mexico
Albuquerque, New Mexico
Workgroup Leaders
Edward Bernstein, M.D., F.A.C.E.P.
Associate Professor and Academic Affairs
Vice Chairman
Boston University School of Medicine
Boston, Massachusetts
Suzanne M. Colby, Ph.D.
Assistant Professor of Psychiatry and Human
Behavior
Center for Alcohol and Addiction Studies
Brown University
Providence, Rhode Island
Carlo C. DiClemente, Ph.D.
Department of Psychology
University of Maryland, Baltimore County
Baltimore, Maryland
Robert J. Meyers, M.A.
Center on Alcoholism, Substance Abuse, and
Addictions
University of New Mexico
Albuquerque, New Mexico
Maxine L. Stitzer, Ph.D.
Professor of Psychiatry and Behavioral Biology
Johns Hopkins University School of Medicine
Baltimore, Maryland
Allen Zweben, D.S.W.
Director and Associate Professor of Social Work
Center for Addiction and Behavioral Health
Research
University of Wisconsin at Milwaukee
Milwaukee, Wisconsin
Panelists
Ray Daw
Executive Director
Northwest New Mexico Fighting Back, Inc.
Gallup, New Mexico
Jeffrey M. Georgi, M.Div., C.S.A.C., C.G.P.
Program Coordinator
Duke Alcoholism and Addictions Program
Clinical Associate
Department of Psychiatry and Behavioral Science
Duke University Medical Center
Durham, North Carolina
Cheryl Grills, Ph.D.
Department of Psychology
Loyola Marymount University
Los Angeles, California
xv

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
Rosalyn Harris-Offutt, C.R.N.A., L.P.C., A.D.S.
UNA Psychological Associates
Greensboro, North Carolina
Don M. Hashimoto, Psy.D.
Clinical Director
Ohana Counseling Services, Inc.
Hilo, Hawaii
Dwight McCall, Ph.D.
Evaluation Manager
Substance Abuse Services
Virginia Department of Mental Health, Mental
Retardation and Substance Abuse Services
Richmond, Virginia
Jeanne Obert, M.F.C.C., M.S.M.
Director of Clinical Services
Matrix Center
Los Angeles, California
Carole Janis Otero, M.A., L.P.C.C.
Director
Albuquerque Metropolitan Central Intake
Albuquerque, New Mexico
Roger A. Roffman, D.S.W.
Innovative Programs Research Group
School of Social Work
Seattle, Washington
Linda C. Sobell, Ph.D.
Professor
NOVA Southeastern University
Fort Lauderdale, Florida
The information given indicates participants’ affiliations
at the time of their participation in this TIP’s original
development and may no longer reflect their current
affiliations.
Field Reviewers, Resource Panel, and
Editorial Advisory Board
Field reviewers represent each TIP’s intended
target audiences. They work in addiction, mental
health, primary care, and adjacent fields. Their
direct front-line experience related to the TIP’s
topic allows them to provide valuable input on a
TIP’s relevance, utility, accuracy, and accessibility.
Additional advisors to this TIP include members of
a resource panel and an editorial advisory board.
Field Reviewers
Noel Brankenhoff, L.M.F.T., L.C.D.P.
Child and Family Services
Middletown, Rhode Island
Rodolfo Briseno, L.C.D.C.
Coordinator for Cultural/Special Populations and
Youth Treatment Program Services
Program Initiatives Texas Commission on Alcohol
and Drug Abuse
Austin, Texas
Richard L. Brown, M.D., M.P.H.
Associate Professor
Department of Family Medicine
University of Wisconsin School of Medicine
Madison, Wisconsin
Michael Burke
Senior Substance Abuse Specialist
Student Health
Rutgers University
New Brunswick, New Jersey
Kate Carey, Ph.D.
Associate Professor
Department of Psychology
Syracuse University
Syracuse, New York
Anthony J. Cellucci, Ph.D.
Director of Idaho State University Clinic
Associate Professor of Psychology
Idaho State University
Pocatello, Idaho
xvi

TIP 35
Gerard Connors, Ph.D.
Research Institute on Alcoholism
Buffalo, New York
John Cunningham, Ph.D.
Scientist
Addiction Research Foundation Division
Centre for Addiction and Mental Health
Toronto, Ontario
Janie Dargan, M.S.W.
Senior Policy Analyst
Office of National Drug Control Policy/Executive
Office of the President
Washington, D.C.
George De Leon, Ph.D.
Center for Therapeutic Community Research
New York, New York
Nereida Diaz-Rodriguez, L.L.M., J.D.
Project Director
Director to the Master in Health Science in
Substance Abuse
Centro de Entudion on Adiccion (Altos Salud
Mental)
Edif. Hosp. Regional de Bayamon
Santa Juanita, Bayamon, Puerto Rico
Thomas Diklich
Portsmouth CSR
Portsmouth, Virginia
Chris Dunn, Ph.D., M.A.C., C.D.C.
Psychologist
Psychiatry and Behavioral Science
University of Washington
Seattle, Washington
Madeline Dupree, L.P.C.
Harrisonburg-Rockingham CSB
Harrisonburg, Virginia
Gary L. Fisher, Ph.D.
Nevada Addiction Technology Transfer Center
College of Education
University of Nevada at Reno
Reno, Nevada
Cynthia Flackus, M.S.W., L.I.C.S.W.
Therapist
Camp Share Renewal Center
Walker, Minnesota
Stephen T. Higgins, Ph.D.
Professor
Departments of Psychiatry and Psychology
University of Vermont
Burlington, Vermont
Col. Kenneth J. Hoffman, M.D., M.P.H., M.C.F.S.
Preventive Medicine Consultant
HHC 18th Medical Command
Seoul, South Korea
James Robert Holden, M.A.
Program Director
Partners in Drug Abuse Rehabilitation Counseling
Washington, D.C.
Ron Jackson, M.S.W.
Executive Director
Evergreen Treatment Services
Seattle, Washington
Linda Kaplan
Executive Director
National Association of Alcoholism and Drug
Abuse Counselors
Arlington, Virginia
Matthew Kelly, Ph.D.
Clinical Director
Robert Wood Johnson Foundation
Northwest Mexico Fighting Back, Inc.
Gallup, New Mexico
Karen Kelly-Woodall, M.S., M.A.C., N.C.A.C. II
Criminal Justice Coordinator
Cork Institute
Morehouse School of Medicine
Atlanta, Georgia
Richard Laban, Ph.D.
Laban’s Training
Harrisburg, Pennsylvania
xvii

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
Lauren Lawendowski, Ph.D.
Acting Project Director
Center on Alcoholism, Substance Abuse, and
Addiction
University of New Mexico
Albuquerque, New Mexico
Bruce R. Lorenz, N.C.A.C. II
Director
Thresholds, Inc.
Dover, Delaware
Russell P. MacPherson, Ph.D., C.A.P., C.A.P.P.,
C.C.P., D.A.C., D.V.C.
President
RPM Addiction Prevention Training
Deland, Florida
George Medzerian, Ph.D.
Pensacola, Florida
Lisa A. Melchior, Ph.D.
Vice President
The Measurement Group
Culver City, California
Paul Nagy, M.S., C.S.A.C.
Director
Duke Alcoholism and Addictions Program
Duke University Medical Center
Durham, North Carolina
Tracy A. O’Leary, Ph.D.
Clinical Supervisor
Assistant Project Coordinator
Center for Alcohol and Addiction Studies
Brown University
Providence, Rhode Island
Gwen M. Olitsky, M.S.
CEO
The Self-Help Institute for Training and Therapy
Lansdale, Pennsylvania
Michele A. Packard, Ph.D.
Executive Director
SAGE Institute Training and Consulting
Boulder, Colorado
Michael Pantalon, Ph.D.
Yale School of Medicine
New Haven, Connecticut
Joe Pereira, L.I.C.S.W., C.A.S.
Recovery Strategies
Medford, Massachusetts
Harold Perl, Ph.D.
Public Health Analyst
Division of Clinical and Prevention Research
National Institute on Alcohol Abuse and Alcoholism
Bethesda, Maryland
Raul G. Rodriguez, M.D.
Medical Director
La Hacienda Treatment Center
Hunt, Texas
Richard T. Suchinsky, M.D.
Associate Director for Addictive Disorders and
Psychiatric Rehabilitation
Mental Health and Behavioral Sciences Services
Department of Veterans Affairs
Washington, D.C.
Suzan Swanton, M.S.W.
Clinical Director
R.E.A.C.H. Mobile Home Services
Baltimore, Maryland
Michael J. Taleff, Ph.D., C.A.C., M.A.C.,
N.C.A.C.II
Assistant Professor and Coordinator
Graduate Programs in Chemical Dependency
Department of Counselor Education
Counseling Psychology and Rehabilitation Services
Pennsylvania State University
University Park, Pennsylvania
Nola C. Veazie, Ph.D., L.P.C., C.A.D.A.C.
Superintendent
Medical Services Department
United States Air Force
Family Therapist/Drug and Alcohol Counselor
Veazie Family Therapy
Santa Maria, California
xviii

TIP 35
Mary Velasquez, Ph.D.
Psychology Department
University of Houston
Houston, Texas
Christopher Wagner, Ph.D.
Division of Substance Abuse Medicine
Virginia Commonwealth University
Richmond, Virginia
Resource Panel
Peter J. Cohen, M.D., J.D.
Adjunct Professor of Law
Georgetown University Law Center
Washington, D.C.
Frances Cotter, M.A., M.P.H.
Senior Public Health Advisor
Office of Managed Care
Center for Substance Abuse Treatment
Substance Abuse and Mental Health Services
Administration
Rockville, Maryland
Dorynne Czechowicz, M.D.
Associate Director
Division of Clinical and Services Research
Treatment Research Branch
National Institute on Drug Abuse
Bethesda, Maryland
James G. (Gil) Hill
Director
Office of Substance Abuse
American Psychological Association
Washington, D.C.
Linda Kaplan
Executive Director
National Association of Alcoholism and Drug
Abuse Counselors
Arlington, Virginia
Pedro Morales, J.D.
Director
Equal Employment Civil Rights
Substance Abuse and Mental Health Services
Administration
Rockville, Maryland
Harold I. Perl, Ph.D.
Public Health Analyst
Division of Clinical and Prevention Research
National Institute on Alcohol Abuse and Alcoholism
Bethesda, Maryland
Barbara J. Silver, Ph.D.
Center for Mental Health Services
Substance Abuse and Mental Health Services
Administration
Rockville, Maryland
Lucretia Vigil
Policy Advisor
National Coalition of Hispanic Health and Human
Services Organization
Washington, D.C.
Editorial Advisory Board
Karen Allen, Ph.D., R.N., C.A.R.N.
Professor and Chair
Department of Nursing
Andrews University
Berrien Springs, Michigan
Richard L. Brown, M.D., M.P.H.
Associate Professor
Department of Family Medicine
University of Wisconsin School of Medicine
Madison, Wisconsin
Dorynne Czechowicz, M.D.
Associate Director
Medical/Professional Affairs
Treatment Research Branch
Division of Clinical and Services Research
National Institute on Drug Abuse
Rockville, Maryland
xix

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
Linda S. Foley, M.A.
Former Director
Project for Addiction Counselor Training
National Association of State Alcohol and Drug
Abuse Directors
Washington, D.C.
Wayde A. Glover, M.I.S., N.C.A.C. II
Director
Commonwealth Addictions Consultants and
Trainers
Richmond, Virginia
Pedro J. Greer, M.D.
Assistant Dean for Homeless Education
University of Miami School of Medicine
Miami, Florida
Thomas W. Hester, M.D.
Former State Director
Substance Abuse Services
Division of Mental Health, Mental Retardation and
Substance Abuse
Georgia Department of Human Resources
Atlanta, Georgia
James G. (Gil) Hill, Ph.D.
Director
Office of Substance Abuse
American Psychological Association
Washington, D.C.
Douglas B. Kamerow, M.D., M.P.H.
Director
Office of the Forum for Quality and Effectiveness in
Health Care
Agency for Healthcare Research and Quality
Rockville, Maryland
Stephen W. Long
Director
Office of Policy Analysis
National Institute on Alcohol Abuse and Alcoholism
Rockville, Maryland
Richard A. Rawson, Ph.D.
Executive Director
Matrix Center and Matrix Institute on Addiction
Deputy Director
UCLA Addiction Medicine Services
Los Angeles, California
Ellen A. Renz, Ph.D.
Former Vice President of Clinical Systems
MEDCO Behavioral Care Corporation
Kamuela, Hawaii
Richard K. Ries, M.D.
Director and Associate Professor
Outpatient Mental Health Services and Dual
Disorder Programs
Harborview Medical Center
Seattle, Washington
Sidney H. Schnoll, M.D., Ph.D.
Chairman
Division of Substance Abuse Medicine
Medical College of Virginia
Richmond, Virginia
xx

TIP 35
Publication Information
Acknowledgements
This publication was prepared under contract
numbers 270-95-0013, 270-14-0445, 270-19-0538,
and 283-17-4901 by the Knowledge Application
Program (KAP) for the Center for Substance
Abuse Treatment, Substance Abuse and Mental
Health Services Administration (SAMHSA). Sandra
Clunies, M.S., I.C.A.D.C., served as the Contracting
Officer’s Representative (COR) for initial Treatment
Improvement Protocol (TIP) development. Suzanne
Wise served as the COR; Candi Byrne as the
Alternate COR; and Reed Forman, M.S.W., as the
Project Champion for the TIP update.
Disclaimer
The views, opinions, and content expressed herein
are the views of the consensus panel members and
do not necessarily reflect the official position of
SAMHSA. No official support of or endorsement by
SAMHSA for these opinions or for the instruments
or resources described is intended or should be
inferred. The guidelines presented should not be
considered substitutes for individualized client care
and treatment decisions.
Public Domain Notice
All materials appearing in this publication
except those taken directly from copyrighted
sources are in the public domain and may be
reproduced or copied without permission from
SAMHSA or the authors. Citation of the source is
appreciated. However, this publication may not
be reproduced or distributed for a fee without
the specific, written authorization of the Office of
Communications, SAMHSA.
Electronic Access and Copies of
Publication
This publication may be ordered or downloaded
from SAMHSA’s Publications and Digital Products
webpage at https://store.samhsa.gov. Or, please
call SAMHSA at 1-877-SAMHSA-7 (1-877-726-
4727) (English and Español).
Recommended Citation
Substance Abuse and Mental Health Services
Administration. Enhancing Motivation for
Change in Substance Use Disorder Treatment.
Treatment Improvement Protocol (TIP) Series No.
35. SAMHSA Publication No. PEP19-02-01-003.
Rockville, MD: Substance Abuse and Mental Health
Services Administration, 2019.
Originating Oce
Quality Improvement and Workforce Development
Branch, Division of Services Improvement, Center
for Substance Abuse Treatment, Substance Abuse
and Mental Health Services Administration, 5600
Fishers Lane, Rockville, MD 20857.
Nondiscrimination Notice
SAMHSA complies with applicable federal civil
rights laws and does not discriminate on the basis
of race, color, national origin, age, disability, or
sex. SAMHSA cumple con las leyes federales
de derechos civiles aplicables y no discrimina
por motivos de raza, color, nacionalidad, edad,
discapacidad, o sexo.
SAMHSA Publication No. PEP19-02-01-003
First printed 1999
Updated 2019
xxi
This page intentionally left blank

Chapter 1—A New Look at Motivation
Motivation to initiate and persist in change fluctuates over time
regardless of the person’s stage of readiness. From the client’s
perspective, a decision is just the beginning of change.”
—Miller & Rollnick, 2013, p. 293
TIP 35
ENHANCING MOTIVATION FOR CHANGE IN
SUBSTANCE USE DISORDER TREATMENT
KEY MESSAGES
•
Motivation is the key to substance use
behavior change.
• Counselor use of empathy, not authority
and power, is essential to enhancing client
motivation to change.
• The Transtheoretical Model (TTM) of the
Stages of Change (SOC) approach is a useful
overarching framework that can help you
tailor specific counseling strategies to the
different stages.
Why do people change? How is motivation linked
to substance use behavior change? How can you
help clients enhance their motivation to engage in
substance use disorder (SUD) treatment and initiate
recovery? This Treatment Improvement Protocol
(TIP) will answer these and other important
questions. Using the TTM of behavioral change as
a foundation, Chapter 1 lays the groundwork for
answering such questions. It offers an overview of
the nature of motivation and its link to changing
substance use behaviors. It also addresses the shift
away from abstinence-only addiction treatment
perspectives toward client-centered approaches
that enhance motivation and reduce risk.
In the past three decades, the addiction treatment
field has focused on discovering and applying
science-informed practices that help people with
SUDs enhance their motivation to stop or reduce
alcohol, drug, and nicotine use. Research and
clinical literature have explored how to help clients
sustain behavior change in ongoing recovery.
Such recovery support helps prevent or lessen the
social, mental, and health problems that result
from a recurrence of substance use or a relapse to
previous levels of substance misuse.
This TIP examines motivational enhancement
and substance use behavior change using two
science-informed approaches (DiClemente, Corno,
Graydon, Wiprovnick, & Knobloch, 2017):
1. Motivational interviewing (MI), which is a
respectful counseling style that focuses on
helping clients resolve ambivalence about
and enhance motivation to change health-risk
behaviors, including substance misuse
2. The TTM of the SOC, which provides an
overarching framework for motivational
counseling approaches throughout all phases of
addiction treatment
1

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
KEY TERMS
Addiction*: The most severe form of SUD, associated with compulsive or uncontrolled use of one or
more substances. Addiction is a chronic brain disease that has the potential for both recurrence (relapse)
andrecovery.
Alcohol misuse: The use of alcohol in any harmful way, including use that constitutes alcohol use
disorder(AUD).
Alcohol use disorder: Per the American Psychiatric Association’s (APA) Diagnostic and Statistical Manual
of Mental Disorders, Fifth Edition (DSM-5; APA, 2013), a diagnosis applicable to a person who uses
alcohol and experiences at least 2 of the 11 symptoms in a 12-month period. Key aspects of AUD include
loss of control, continued use despite adverse consequences, tolerance, and withdrawal. AUD covers a
range of severity and replaces what DSM-IV, termed “alcohol abuse” and “alcohol dependence” (APA,
1994).
Health-risk behavior: Any behavior (e.g., tobacco or alcohol use, unsafe sexual practices, nonadherence
to prescribed medication regimens) that increases the risk of disease or injury.
Recovery*: A process of change through which individuals improve their health and wellness, live a
self-directed life, and strive to reach their full potential. Even individuals with severe and chronic SUDs can,
with help, overcome their disorder and regain health and social function. This is called remission. When
those positive changes and values become part of a voluntarily adopted lifestyle, that is called “being in
recovery.” Although abstinence from all substance misuse is a cardinal feature of a recovery lifestyle, it is
not the only healthy, pro-social feature.
Recurrence: An instance of substance use that occurs after a period of abstinence. Where possible,
this TIP uses the terms “recurrence” or “return to substance use” instead of “relapse,” which can have
negative connotations (see entry below).
Relapse*: A return to substance use after a significant period of abstinence.
Substance*: A psychoactive compound with the potential to cause health and social problems, including
SUDs (and their most severe manifestation, addiction). The table at the end of this exhibit lists common
examples of such substances.
Substance misuse*: The use of any substance in a manner, situation, amount, or frequency that can cause
harm to users or to those around them. For some substances or individuals, any use would constitute
misuse (e.g., underage drinking, injection drug use).
Substance use*: The use—even one time—of any of the substances listed in the table at the end of
this exhibit.
Substance use disorder*: A medical illness caused by repeated misuse of a substance or substances.
According to DSM-5 (APA, 2013), SUDs are characterized by clinically significant impairments in health,
social function, and impaired control over substance use and are diagnosed through assessing cognitive,
behavioral, and psychological symptoms. SUDs range from mild to severe and from temporary to chronic.
They typically develop gradually over time with repeated misuse, leading to changes in brain circuits
governing incentive salience (the ability of substance-associated cues to trigger substance seeking),
reward, stress, and executive functions like decision making and self-control. Multiple factors influence
whether and how rapidly a person will develop an SUD. These factors include the substance itself; the
genetic vulnerability of the user; and the amount, frequency, and duration of the misuse. A severe SUD is
commonly called an addiction.
Chapter 1 2

TIP 35
Chapter 1—A New Look at Motivation
Substance Category Representative Examples
Alcohol
•
Beer
•
Wine
•
Malt liquor
•
Distilled spirits
Illicit Drugs
•
Cocaine, including crack
•
Heroin
•
Hallucinogens, including LSD, PCP, ecstasy, peyote, mescaline, psilocybin
•
Methamphetamines, including crystal meth
•
Marijuana, including hashish*
•
Synthetic drugs, including K2, Spice, and "bath salts"**
•
Prescription-type medications that are used for nonmedical purposes
−
Pain Relievers - Synthetic, semi-synthetic, and non-synthetic opioid
medications, including fentanyl, codeine, oxycodone, hydrocodone, and
tramadol products
−
Tranquilizers, including benzodiazepines, meprobamate products, and
muscle relaxants
−
Stimulants and Methamphetamine, including amphetamine,
dextroamphetamine, and phentermine products; mazindol products;
and methylphenidate or dexmethylphenidate products
−
Sedatives, including temazepam, flurazepam, or triazolam and
anybarbiturates
Over-the-Counter
Drugs and Other
Substances
•
Cough and cold medicines**
•
Inhalants, including amyl nitrite, cleaning fluids, gasoline and lighter gases,
anesthetics, solvents, spray paint, nitrous oxide
*As of June 2016, 25 states and the District of Columbia have legalized medical marijuana use, for states
have legalized retail marijuana sales, and the District of Columbia has legalized personal use and
home cultivation (both medical and recreational). It should be noted that none of the permitted uses
under state laws alter the status of marijuana and its constituent compounds as illicit drugs under
Schedule I of the federal Controlled Substances Act. See the section on Marijuana: A Changing Legal and
Research Environment in the Facing Addiction in America: The Surgeon General’s Report on Alcohol,
Drugs, and Health (Office of the Surgeon General, 2016). The report is available online (https://addiction.
surgeongeneral.gov/sites/default/files/surgeon-generals-report.pdf).
The definitions of all terms marked with an asterisk correspond closely to those in the Surgeon
General’sReport.
** These substances are not included in NSDUH and are not discussed in the Surgeon General's Report.
However, important facts about these drugs are included in Appendix D - Important Facts About Alcohol
and Drugs
Chapter 1 3

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Motivation and Behavior Change
Motivation is a critical element of behavior
change (Flannery, 2017) that predicts client
abstinence and reductions in substance use
(DiClemente et al., 2017). You cannot give clients
motivation, but you can help them identify their
reasons and need for change and facilitate
planning for change. Successful SUD treatment
approaches acknowledge motivation as a
multidimensional, fluid state during which people
make difficult changes to health-risk behaviors,
like substance misuse.
The Nature of Motivation
The following factors define motivation and its
ability to help people change health-risk behaviors.
•
Motivation is a key to substance use behavior
change. Change, like motivation, is a complex
construct with evolving meanings. One
framework for understanding motivation and
how it relates to behavior changes is the self-
determination theory (SDT). SDT suggests that
people inherently want to engage in activities
that meet their need for autonomy, competency
(i.e., self-efficacy), and relatedness (i.e., having
close personal relationships) (Deci & Ryan, 2012;
Flannery, 2017). SDT describes two kinds of
motivation:
- Intrinsic motivation (e.g., desires, needs,
values, goals)
- Extrinsic motivation (e.g., social influences,
external rewards, consequences)
•
MI is a counseling approach that is consistent
with SDT and emphasizes enhancing internal
motivation to change. In the SDT framework,
providing a supportive relational context that
promotes client autonomy and competence
enhances intrinsic motivation, helps clients
internalize extrinsic motivational rewards, and
supports behavior change (Flannery, 2017;
Kwasnicka, Dombrowski, White, & Sniehotta,
2016; Moyers, 2014).
•
Contingency management is a counseling
strategy that can reinforce extrinsic
motivation. It uses external motivators or
reinforcers (e.g., expectation of a reward or
negative consequence) to enhance behavior
change (Sayegh, Huey, Zara, & Jhaveri, 2017).
•
Motivation helps people resolve their
ambivalence about making difficult lifestyle
changes. Helping clients strengthen their own
motivation increases the likelihood that they
will commit to a specific behavioral change plan
(Miller & Rollnick, 2013). Research supports the
importance of SDT-based client motivation in
positive addiction treatment outcomes (Wild,
Yuan, Rush, & Urbanoski, 2016). Motivation and
readiness to change are consistently associated
with increased help seeking, treatment
adherence and completion, and positive SUD
treatment outcomes (Miller & Moyers, 2015).
•
Motivation is multidimensional. Motivation
includes clients’ internal desires, needs, and
values. It also includes external pressures,
demands, and reinforcers (positive and negative)
that influence clients and their perceptions
about the risks and benefits of engaging in
substance use behaviors. Two components of
motivation predict good treatment outcomes
(Miller & Moyers, 2015):
-
The importance clients associate
withchanges
-
Their confidence in their ability to
makechanges
•
Motivation is dynamic and fluctuates.
Motivation is a dynamic process that responds
to interpersonal influences, including feedback
and an awareness of different available choices
(Miller & Rollnick, 2013). Motivation is a strong
predictor of addiction treatment outcomes
(Miller & Moyers, 2015). Motivation can fluctuate
over different stages of the SOC and varies
in intensity. It can decrease when the client
feels doubt or ambivalence about change and
increase when reasons for change and specific
goals become clear. In this sense, motivation
can be an ambivalent state or a resolute
commitment to act—or not to act.
Chapter 1 4

TIP 35
Chapter 1—A New Look at Motivation
•
Motivation is influenced by social interactions.
An individual’s motivation to change can be
positively influenced by supportive family and
friends as well as community support and
negatively influenced by lack of social support,
negative social support (e.g., a social network of
friends and associates who misuse alcohol), and
negative public perception of SUDs.
•
Your task is to elicit and enhance motivation.
Although change is the responsibility of
clients and many people change substance
use behaviors on their own without formal
treatment (Kelly, Bergman, Hoeppner, Vilsaint,
& White, 2017), you can enhance clients’
motivation for positive change at each stage
of the SOC process. Your task is not to teach,
instruct, or give unsolicited advice. Your role
is to help clients recognize when a substance
use behavior is inconsistent with their values
or stated goals, regard positive change to
be in their best interest, feel competent to
change, develop a plan for change, begin
taking action, and continue using strategies that
lessen the risk of a return to substance misuse
(Miller & Rollnick, 2013). Finally, you should
be sensitive and responsive to cultural factors
that may influence client motivation. For more
information about enhancing cultural awareness
and responsiveness, see TIP 59: Improving
Cultural Competence (Substance Abuse
and Mental Health Services Administration
[SAMHSA], 2014a).
•
Motivation can be enhanced. Motivation is
a part of the human experience. No one is
totally unmotivated (Miller & Rollnick, 2013).
Motivation is accessible and can be enhanced at
many points in the change process. Historically,
in addiction treatment it was thought that
clients had to “hit bottom” or experience
terrible, irreparable consequences of their
substance misuse to become ready to change.
Research now shows that counselors can help
clients identify and explore their desire, ability,
reasons, and need to change substance use
behaviors; this effort enhances motivation and
facilitates movement toward change (Miller &
Rollnick,2013).
•
Motivation is influenced by the counselor’s
style. The way you interact with clients impacts
how they respond and whether treatment is
successful. Counselor interpersonal skills are
associated with better treatment outcomes.
In particular, an empathetic counselor style
predicts increased retention in treatment and
reduced substance use across a wide range of
clinical settings and types of clients (Moyers
& Miller, 2013). The most desirable attributes
for the counselor mirror those recommended
in the general psychology literature and
include nonpossessive warmth, genuineness,
respect, affirmation, and empathy. In contrast,
an argumentative or confrontational style of
counselor interaction with clients, such as
challenging client defenses and arguing, tends
to be counterproductive and is associated with
poorer outcomes for clients, particularly when
counselors are less skilled (Polcin, Mulia, &
Jones, 2012; Roman & Peters, 2016).
COUNSELOR NOTE: ARE YOU
READY, WILLING, AND ABLE?
Motivation is captured, in part, in the popular
phrase that a person is ready, willing, and able
to change:
• “Ability” refers to the extent to which a person
has the necessary skills, resources, and
confidence to make a change.
• “Willingness” is linked to the importance a
person places on changing—how much a
change is wanted or desired. However, even
willingness and ability are not always enough.
• “Ready” represents a final step in which
a person finally decides to change a
particular behavior.
Your task is to help the client become ready,
willing, and able to change.
Chapter 1 5

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Why Enhance Motivation?
Although much progress has been made in
identifying people who misuse substances and
who have SUD and in using science-informed
interventions such as motivational counseling
approaches to treat them, the United States is still
facing many SUD challenges. For example, the
National Survey on Drug Use and Health (SAMHSA,
2018) reports that, in 2017, approximately:
•
140.6 million Americans ages 12 and older
currently consumed alcohol, 66.6 million
engaged in past-month binge drinking (defined
as 5 or more drinks on the same occasion on at
least 1 day in the past 30 days for men and 4 or
more drinks on the same occasion on at least
1 day in the past 30 days for women), and 16.7
million drank heavily in the past month (defined
as binge drinking on 5 or more days in the past
30 days).
•
30.5 million people ages 12 and older had past-
month illicit drug use.
•
11.4 million people misused opioids (defined as
prescription pain reliever misuse or heroin use)
in the past year.
•
8.5 million adults ages 18 and older (3.4 percent
of all adults) had both a mental disorder and at
least one past-year SUD.
•
18.2 million people who needed SUD treatment
did not receive specialty treatment.
•
One-third of people who perceived a need for
addiction treatment did not receive it because
they lacked health insurance and could not pay
for services.
Enhancing motivation can improve addiction
treatment outcomes. In the United States, millions
of people with SUDs are not receiving treatment.
Many do not seek treatment because their
motivation to change their substance use behaviors
is low. Motivational counseling approaches are
associated with greater participation in treatment
and positive treatment outcomes. Such outcomes
include increased motivation to change; reductions
in consumption of alcohol, tobacco, cannabis,
and other substances; increased abstinence rates;
higher client confidence in ability to change
behaviors; and greater treatment engagement
(Copeland, McNamara, Kelson, & Simpson, 2015;
DiClemente et al., 2017; Lundahl et al., 2013;
Smedslund et al., 2011).
The benefits of motivational enhancement
approaches include:
•
Enhancing motivation to change.
•
Preparing clients to enter treatment.
•
Engaging and retaining clients in treatment.
•
Increasing participation and involvement.
•
Improving treatment outcomes.
•
Encouraging rapid return to treatment if clients
return to substance misuse.
Changing Perspectives on
Addiction and Treatment
Historically, in the United States, different views
about the nature of addiction and its causes
have influenced the development of treatment
approaches. For example, after the passage of
the Harrison Narcotics Act in 1914, it was illegal
for physicians to treat people with drug addiction.
The only options for people with alcohol or drug
use disorders were inebriate homes and asylums.
The underlying assumption pervading these early
treatment approaches was that alcohol and drug
addiction was either a moral failing or a pernicious
disease (White, 2014).
By the 1920s, compassionate treatment of opioid
addiction was available in medical clinics. At
the same time, equally passionate support for
the temperance movement, with its focus on
drunkenness as a moral failing and abstinence as
the only cure, was gaining momentum.
The development of the modern SUD treatment
system dates only from the late 1950s. Even
“modern” addiction treatment has not always
acknowledged counselors’ capacity to support
client motivation. Historically, motivation was
considered a static client trait; the client either
had it or did not have it, and there was nothing a
counselor could do to influence it.
This view of motivation as static led to blaming
clients for tension or discord in therapeutic
Chapter 1 6

TIP 35Chapter 1—A New Look at Motivation
relationships. Clients who disagreed with
diagnoses, did not adhere to treatment plans, or
refused to accept labels like “alcoholic” or “drug
addict” were seen as difficult or resistant (Miller &
Rollnick, 2013).
EXHIBIT 1.1. Models of Addiction
SUD treatment has since evolved in response
to new technologies, research, and theories of
addiction with associated counseling approaches.
Exhibit 1.1 summarizes some models of addiction
that have influenced treatment methods in the
United States (DiClemente, 2018).
MODEL UNDERLYING ASSUMPTIONS TREATMENT APPROACHES
Moral/legal Addiction is a set of behaviors
that violates religious, moral, or
legalcodes.
Abstinence and use of willpower
External control through hospitalization
orincarceration
Psychological Addiction results from deficits in
learning, emotional dysfunction,
orpsychopathology.
Cognitive, behavioral, psychoanalytic, or
psychodynamic psychotherapies
Sociocultural Addiction results from socialization
and sociocultural factors.
Contributing factors include
socioeconomic status, cultural
Focus on building new social and
family relationships, developing social
competency and skills, and working within a
client’sculture
and ethnic beliefs, availability of
substances, laws and penalties
regulating substance use, norms
and rules of families and other
social groups, parental and
peer expectations, modeling of
acceptable behaviors, and the
presence or absence of reinforcers.
Spiritual Addiction is a spiritual disease.
Recovery is predicated on a
recognition of the limitations of the
self and a desire to achieve health
through a connection with that
which transcends the individual.
Integrating 12-Step recovery principles or
other culturally based spiritual practices (e.g.,
American Indian Wellbriety principles) into
addiction treatment
Linking clients to 12-Step, faith- and spiritual-
based recovery, and other support groups
Medical Addiction is a chronic,
progressivedisease.
Genetic predisposition and
neurochemical brain changes are
primary etiological factors.
Medical and behavioral interventions
including pharmacotherapy, education, and
behavioral change advice and monitoring
Integrated Addiction is a chronic disease that Integrated treatment with a recovery focus
treatment is best treated by collaborative
and comprehensive approaches
that address biopsychosocial and
spiritual components.
across treatment settings
Chapter 1 7

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Earlier Perspectives
Although the field is evolving toward a more
comprehensive understanding of SUD, earlier
views of addiction still persist in parts of the
U.S. addiction treatment system. For example,
the psychological model of addiction treatment
gave rise, in part, to the idea of an “addictive
personality” and that psychological defenses (e.g.,
denial) need to be confronted. Remnants of earlier
perspectives of addiction and their associated
treatment approaches, which are not supported by
research, include:
•
An addictive personality leads to SUDs.
Although it is commonly believed that people
with SUDs possess similar personality traits
that make treatment difficult, no distinctive
personality traits have been found to predict
that an individual will develop an SUD
(Amodeo, 2015). The tendencies of an addictive
personality most often cited are denial,
projection, poor insight, and poor self-esteem.
This idea is a deficit-based concept that can lead
to counselors and clients viewing addiction as a
fixed part of an underlying personality disorder
and therefore difficult to treat (Amodeo, 2015).
•
Rationalization and denial are characteristics
of addiction. Another leftover from earlier
psychological perspectives on addiction is that
people with SUDs have strong psychological
defenses, such as denial and rationalization,
which lead to challenging behaviors like
evasiveness, manipulation, and resistance
(Connors, DiClemente, Velasquez, & Donovan,
2013). The clinical and research literature does
not support the belief that people with SUDs
have more or stronger defenses than other
clients (Connors et al., 2013).
•
Resistance is a characteristic of “unmotivated”
clients in addiction treatment (Connors et al.,
2013). When clients are labeled as manipulative
or resistant, given no voice in selecting
treatment goals, or directed authoritatively
to do or not to do something, the result is a
predictable response of resistance or reactivity
to the counselor’s directives (Beutler, Harwood,
Michelson, Song, & Holman, 2011). Viewing
resistance—along with rationalization and
denial—as characteristic of addiction and
making efforts to weaken these defenses
actually strengthens them. This paradox seemed
to confirm the idea that resistance and denial
were essential components of addiction and
traits of clients.
•
Confrontation of psychological defenses and
substance misuse behaviors is an effective
counseling approach. Historically, the idea
that resistance and denial are characteristic of
addiction led to the use of confrontation as a
way to aggressively break down these defenses
(White & Miller, 2007). However, adversarial
confrontation is one of the least effective
methods for helping clients change substance
use behaviors, can paradoxically reduce
motivation for beneficial change, and often
contributes to poor outcomes (Bertholet, Palfai,
Gaume, Daeppen, & Saitz, 2013; Moos, 2012;
Moyers & Miller, 2013; Romano & Peters, 2016).
Yet there is a constructive type of confrontation.
This kind of confrontation must be done
within the context of a trusting and respectful
relationship and is delivered it in a supportive
way that also elicits hope for change (Polcin et
al.,2012).
Chapter 1 8

TIP 35
Chapter 1—A New Look at Motivation
EXPERT COMMENT: A BRIEF HISTORY OF CONFRONTATION IN ADDICTION
TREATMENT
For many reasons, the U.S. treatment field fell into some rather aggressive, argumentative, “denial-
busting” methods for confronting people with alcohol and drug problems. This perspective was guided,
in part, by the belief that substance misuse links to a particular personality pattern characterized by such
rigid defense mechanisms as denial and rationalization. In this perspective, the counselor must take
responsibility for impressing reality on clients, who cannot see it on their own. Such confrontation found
its way into the popular Minnesota model of treatment and into Synanon (a drug treatment community
known for group sessions in which participants verbally attacked each other) and other similar
therapeutic community programs.
After the 1970s, the treatment field began to move away from such methods. The Hazelden Foundation
officially renounced the “tear them down to build them up” approach in 1985, expressing regret that
such confrontational approaches had become associated with the Minnesota model. Psychological
studies have found no consistent pattern of personality or defense mechanisms associated with SUDs.
Clinical studies have linked worse outcomes to more confrontational counselors, groups, and programs
(Miller & Wilbourne, 2002; Moos, 2012; Romano & Peters, 2016). Instead, successful outcomes (Moyers,
Houck, Rice, Longabaugh, & Miller, 2016) generally have been associated with counselors showing high
levels of empathy as defined by Carl Rogers (1980). The Johnson Institute now emphasizes a supportive,
compassionate style for conducting family interventions.
I was at first surprised when counselors attending my MI workshops and watching me demonstrate the
style observed, “In a different way, you’re very confrontational.” This comes up in almost every training
now. Some call it “gentle confrontation.” This got me thinking about what confrontation really means.
The linguistic roots of the verb “to confront” mean “to come face-to-face.” When you think about it that
way, confrontation is precisely what we are trying to accomplish: to allow our clients to come face-to-
face with a difficult and often threatening reality, to “let it in” rather than “block it out,” and to allow this
reality to change them. That makes confrontation a goal of counseling rather than a particular style
ortechnique.
Once you see this—namely, that opening to new information, face-to-face, is a goal of counseling—then
the question becomes, “What is the best way to achieve that goal?” Strong evidence suggests that
direct, forceful, aggressive approaches are perhaps the least effective way to help people consider new
information and change their perceptions. Such confrontation increases the very phenomenon it is
supposed to overcome—defensiveness—and decreases clients’ likelihood of change (Miller, Benefield,
& Tonigan, 1993; Miller & Wilbourne, 2002; Moos, 2012; Romano & Peters, 2016). It is also inappropriate in
many cultures. Getting in a client’s face may work for some, but for most, it is exactly the opposite of what
is needed—to come face-to-face with painful reality and to change.
William R. Miller, Ph.D., Consensus Panel Chair
Chapter 1 9

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
A New Perspective
As the addiction treatment field has matured,
it has tried to integrate conflicting theories and
approaches and to incorporate research findings
into a comprehensive model. The following
sections address recent changes in addiction
treatment with important implications for applying
motivational methods.
Focus on client strengths
Historically the treatment field has focused on the
deficits and limitations of clients. Today, greater
emphasis is placed on identifying, enhancing,
and using clients’ strengths, abilities, and
competencies. This trend parallels the principles
of motivational counseling, which affirm clients,
emphasize personal autonomy, support and
strengthen self-efficacy, and reinforce that change
is possible (see Chapter 4). The responsibility for
recovery rests with clients, and the judgmental
tone, which is a remnant of the moral model of
addiction, is eliminated.
Individualized and person-
centeredtreatment
In the past, clients frequently received standardized
treatment, no matter what their problems or SUD
severity. Today, treatment is increasingly based
on clients’ individual needs, which are carefully
and comprehensively assessed at intake. Positive
outcomes such as higher levels of engagement in
psychosocial treatments, decreased alcohol use,
and improved quality of life are associated with
person-centered care and a focus on individualized
treatment (Barrio & Gual, 2016; Bray et al., 2017;
Jackson et al., 2014). In this perspective, clients
have choices about desirable, suitable treatment
options—they are not prescribed treatment.
Motivational approaches emphasize choice by
eliciting personal goals from clients and involving
them in selecting the type of treatment needed or
desired from a menu of options.
A shi away from labeling
Historically, a diagnosis or disease defined the
client and became a dehumanizing attribute of
the individual. Today, individuals with asthma or a
psychosis are seldom referred to as “the asthmatic”
or “the psychotic.” Similarly, in the addiction
treatment arena, there is a trend to avoid labeling
clients with SUDs as “addicts” or “alcoholics.”
Using a motivational style will help you avoid
labeling clients, especially those who may not
agree with the diagnosis or do not see a particular
behavior as problematic. Person-first language
(e.g., a person with an SUD) is the new standard; it
reduces stigma, helps clients disentangle addiction
from identity, and eliminates the judgmental
tone left over from the moral model of addiction
(SAMHSA, Center for the Application of Prevention
Technologies, 2017).
Therapeutic partnerships for change
In the past, especially in the medical model,
the client passively received treatment. Today,
treatment usually entails a partnership in which
you and the client agree on treatment goals
and together develop strategies to meet those
goals. The client is seen as an active participant in
treatment planning. Using motivational strategies
fosters a therapeutic alliance with the client and
elicits goals and change strategies from the
client. The client has ultimate responsibility for
makingchanges.
Use of empathy, not authority and power
Historically, addiction treatment providers were
placed in the position of an authority with the
power to recommend client termination for rule
infractions, penalties for positive urine drug
screens, or promotion to a higher phase of
treatment for successfully following direction.
Research now demonstrates that counselors
who operate from a more authority-driven way
of relating to clients, such as confronting or
being overly directive, are less effective than
counselors who employ empathy, understanding,
and support with clients (Martin & Rehm, 2012).
This style of counseling is a particularly poor match
for clients who are angry or reactive to counselor
direction (Beutler et al., 2011). Positive treatment
outcomes, including decreased substance use,
abstinence, and increased treatment retention,
are associated with high levels of counselor
empathy, good interpersonal skills, and a strong
therapeutic alliance (Miller & Moyers, 2015; Moyers
& Miller,2013).
Chapter 1 10

TIP 35
Chapter 1—A New Look at Motivation
Focus on early and brief interventions
In the past, addiction treatment consisted of
detoxification, inpatient rehabilitation, long-term
rehabilitation in residential settings, and aftercare.
When care was standardized, most programs
had not only a routine protocol of services but
also a fixed length of stay. Twenty-eight days
was considered the proper length of time for
successful inpatient (usually hospital-based) care in
the popular Minnesota model of SUD treatment.
Residential facilities and outpatient clinics also
had standard courses of treatment. These services
were geared to clients with chronic, severe SUDs.
Addiction treatment was viewed as a discrete event
instead of a range of services over a continuum of
care as the treatment provided for other chronic
diseases like heart disease (Miller, Forehimes, &
Zweben, 2011).
Recently, with the shift to a continuum of care
model, a variety of treatment programs have
been established to intervene earlier with those
whose drinking or drug use is causing social,
financial, or legal problems or increases their risk
of health-related harms. These early intervention
efforts range from educational programs (e.g.,
sentencing review or reduction for people
apprehended for driving while intoxicated who
participate in such programs) to brief interventions
in opportunistic settings such as general hospital
units, emergency departments (EDs), clinics, and
doctors’ offices that use motivational strategies
to offer personalized feedback, point out the risks
of substance use and misuse, suggest behavior
change, and make referrals to formal treatment
programs when necessary.
Early and brief interventions demonstrate
positive outcomes such as reductions in alcohol
consumption and drug use, reductions in alcohol
misuse, decreases in tobacco and cannabis use,
lower mortality rates, reductions in alcohol-related
injuries, and decreases in ED return visits (Barata
et al., 2017; Blow et al., 2017; DiClemente et
al., 2017; McQueen, Howe, Allan, Mains, &
Hardy,2011).
Recognition of a continuum of
substancemisuse
Formerly, substance misuse was viewed as a
progressive condition that, if left untreated, would
inevitably lead to full-blown dependence and,
likely, early death. Today, the addiction treatment
field recognizes that substance misuse exists
along a continuum from misuse to an SUD that
meets the diagnostic criteria in DSM-5 (APA, 2013).
Not all SUDs increase in severity. Many individuals
never progress beyond substance use that poses a
health risk, and others cycle back and forth through
periods of abstinence, substance misuse, and
meeting criteria for SUD.
Recovery from SUDs is seen as a
multidimensional process along a continuum
(Office of the Surgeon General, 2016) that differs
among people and changes over time within
the individual. Motivational strategies can be
effectively applied to a person throughout the
addiction process. The crucial variable is not the
severity of the substance use pattern but the
client’s readiness for change.
Recognition of multiple SUDs
Counselors have come to recognize not only that
SUDs vary in intensity but also that most involve
more than one substance. Formerly, alcohol
and drug treatment programs were completely
separated by ideology and policy, even though
most individuals with SUDs also drink heavily and
many people who misuse alcohol also experiment
with other substances, including prescribed
medications that can be substituted for alcohol
or that alleviate withdrawal symptoms. Although
many treatment programs specialize in serving
particular types of clients for whom their treatment
approaches are appropriate (e.g., methadone
maintenance programs for clients with opioid use
disorder [OUD]), most now also treat other SUDs,
substance use, and psychological problems or at
least identify these and make referrals as necessary.
Some evidence shows that motivational counseling
approaches (including individual and group MI
and brief interventions) demonstrate positive
Chapter 1 11

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
outcomes for clients who misuse alcohol and other
substances (Klimas et al., 2014). Motivational
counseling approaches with this client population
should involve engaging clients and prioritizing
their change goals.
Acceptance of new treatment goals
In the past, addiction treatment, at least for clients
having trouble with alcohol, was considered
successful only if the client became abstinent
and never returned to substance use following
discharge. The focus of treatment was almost
entirely to have the client stop using and to start
understanding the nature of addiction. Today,
treatment goals include a broad range of
biopsychosocial measures, such as improved
health and psychosocial functioning, improved
employment stability, and reduction in crime. In
addition, recent efforts have focused on trauma-
informed care and treating co-occurring disorders
in an integrated treatment setting, where client
concerns are addressed simultaneously with
SUDs. For more information on treating clients
with trauma and co-occurring disorders, see TIP
57: Trauma-Informed Care in Behavioral Health
Services (SAMHSA, 2014b) and TIP 42: Substance
Abuse Treatment for Persons With Co-Occurring
Disorders (SAMHSA, 2013), respectively.
Focus on risk reduction
The field has expanded the definition of positive
treatment outcomes to include intermediate
goals of risk reduction. The goal of risk reduction
is to decrease clients’ risks for alcohol- and drug-
related health risks, legal involvement, sexual
behavior that can lead to sexually transmitted
diseases, social and financial problems, ED visits,
hospitalization and rehospitalization, and relapse
of substance use and mental disorders. Risk-
reduction interventions include medication-assisted
treatment for AUD and OUD and reduction in
substance use as an intermediate step toward
abstinence for clients who are not ready or willing
to commit to full abstinence. Risk-reduction
strategies can be an important goal in early
treatment and have demonstrated effectiveness
in reducing substance-use–related consequences
(Office of the Surgeon General, 2016).
Integration of addiction, behavioral health,
and healthcare services
Historically, the SUD treatment system was isolated
from mainstream health care by different funding
streams, health insurance restrictions, and lack of
awareness and training among healthcare providers
on recognizing, screening, assessing, and treating
addiction as a chronic illness. Today, a concerted
effort is under way to integrate addiction
treatment with other behavioral health and
primary care services to build a comprehensive
healthcare delivery system. Key findings of Facing
Addiction in America: The Surgeon General’s
Report on Alcohol, Drugs, and Health (Office of the
Surgeon General, 2016) include the following:
•
The separation of SUD treatment from
mainstream healthcare services has created
obstacles to successful treatment and
carecoordination.
•
SUDs are medical conditions. Integration helps
address health disparities, reduces healthcare
costs, and improves general health outcomes.
•
Many people with SUDs do not seek specialty
addiction treatment but often enter the
healthcare system through general medical
settings. This is an important but neglected
opportunity to screen for substance misuse
and provide brief interventions or referrals to
specialty care.
Motivational enhancement strategies delivered
in all settings can support client engagement in
treatment and improve substance use outcomes,
whether in EDs, primary care offices, office-based
opioid treatment programs, criminal justice
settings, social service programs, or specialized
addiction treatment programs. Screening, brief
intervention, and referral to treatment (SBIRT),
which includes motivational enhancement
strategies, is an early intervention approach that
can be a bridge from medical settings to specialty
SUD treatment in an integrated healthcare system
(McCance-Katz & Satterfeld, 2012). Chapter 2
provides detailed information on SBIRT.
Chapter 1 12

TIP 35Chapter 1—A New Look at Motivation
TTM of the SOC
In developing a new understanding of motivation,
substantial addiction research has focused on
the determinants and mechanisms of change. By
understanding better how people change without
professional assistance, researchers and counselors
have become better able to develop and apply
interventions to facilitate changes in clients’
substance use behaviors.
Natural Change
Many adults in the United States resolve an
alcohol or drug use problem without assistance
(Kelly et al., 2017). This is called “natural recovery.”
Recovery from SUDs can happen with limited
treatment or participation in mutual-aid support
groups such as Alcoholics Anonymous and
Narcotics Anonymous. As many as 45 percent of
participants in the National Prevalence Survey
resolved their substance use problems through
participation in mutual-aid support programs (Kelly
et al., 2017).
Behavior change is a process that occurs over time;
it is not an outcome of any one treatment episode
(Miller et al., 2011). Everyone must make decisions
about important life changes, such as marriage or
divorce or buying a house. Sometimes, individuals
consult a counselor or other specialist to help with
these ordinary decisions, but usually people decide
on such changes without professional assistance.
Natural change related to substance use also
entails decisions to increase, decrease, or stop
substance use. Some decisions are responses to
critical life events, others reflect different kinds of
external pressures, and still others are motivated
by personal values.
Exhibit 1.2 illustrates two kinds of natural change.
Natural changes related to substance use can go
in either direction. In response to an impending
divorce, for example, one individual may begin to
drink heavily whereas another may reduce or stop
using alcohol. Recognizing the processes involved
in natural recovery and self-directed change
illustrates how changes related to substance use
behaviors can be precipitated and stimulated by
enhancing motivation.
EXHIBIT 1.2. Examples of Natural Changes
COMMON NATURAL CHANGES NATURAL CHANGES IN SUBSTANCE USE
•
Going to college
•
Getting married
•
Getting divorced
•
Changing jobs
•
Joining the Army
•
Taking a vacation
•
Moving
•
Buying a home
•
Having a baby
•
Retiring
•
Stopping drinking after an automobile accident
•
Reducing alcohol use after college
•
Stopping substance use before pregnancy
•
Increasing alcohol use during stressful periods
•
Decreasing cigarette use after a price increase
•
Quitting cannabis use before looking for employment
•
Refraining from drinking with some friends
•
Reducing consumption following a physician’s advice
Chapter 1 13

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
SOC
Prochaska and DiClemente (1984) theorized that
the change process is a journey through stages
in which people typically think about behavior
change, initiate behavior change, and maintain
new behaviors. This model emerged from an
examination of 18 psychological and behavioral
theories about how change occurs, including
components that compose a biopsychosocial
framework for understanding addiction. In this
sense, the model is “transtheoretical” (Prochaska
& DiClemente, 1984). This model has come to be
known as the TTM of the SOC. TTM is not the only
SOC model, but it is the most widely researched
(Connors et al., 2013).
SOC is not a specific counseling method but a
framework that can help you tailor specific coun-
seling strategies to clients in different stages.
Although results are mixed regarding its useful-
ness, in the past 30 years, TTM has demonstrated
effectiveness in predicting positive addiction
treatment outcomes and has shown value as an
overarching theoretical framework for counseling
(Harrell, Trenz, Scherer, Martins, & Latimer, 2013;
Norcross, Krebs, & Prochaska, 2011). Exhibit 1.3
displays the relationship among the five stages (i.e.,
Precontemplation, Contemplation, Preparation,
Action, and Maintenance) in the SOC approach in
the original TTM.
EXHIBIT 1.3. The Five Stages in the SOC in the TTM
Source: DiClemente, 2018.
Chapter 1 14

TIP 35
Chapter 1—A New Look at Motivation
The associated features of the SOC approach are
(Connors et al., 2013):
•
Precontemplation: People who use substances
are not considering change and do not intend to
change in the foreseeable future. They may be
partly or completely unaware that a problem exists,
that they have to make changes, and that they
may need help to change. Alternatively, they may
be unwilling or too discouraged to change their
behavior. Individuals in this stage often are not
convinced that their pattern of use is problematic.
•
Contemplation: As these individuals become
aware that a problem exists, they begin to
perceive that there may be cause for concern and
reasons to change. Typically, they are ambivalent,
simultaneously seeing reasons to change and
reasons not to change. Individuals in this stage are
still using substances, but they are considering
the possibility of stopping or cutting back in the
near future. At this point, they may seek relevant
information, reevaluate their substance use
behavior, or seek help to support the possibility of
changing. They typically weigh the positive and
negative aspects of making a change. It is not
uncommon for individuals to remain in this stage
for extended periods, often for years, vacillating
between wanting and not wanting to change.
•
Preparation: When individuals perceive that the
envisioned advantages of change and adverse
consequences of substance use outweigh the
benefits of maintaining the status quo, the
decisional balance tips in favor of change. Once
initiation of change occurs, individuals enter
the Preparation stage and strengthen their
commitment. Preparation entails more specific
planning for change, such as making choices about
whether treatment is needed and, if so, what kind.
Preparation also entails examining clients’ self-
efficacy or confidence in their ability to change.
Individuals in the Preparation stage are still using
substances, but typically they intend to stop using
very soon. They may already be making small
changes, like cutting down on their substance use.
They begin to set goals for themselves and make
commitments to stop using, even telling close
associates or significant others about their plans.
•
Action: Here, individuals choose a strategy for
change and begin to pursue it. Clients are actively
engaged in changing substance use behaviors.
They are making lifestyle changes and may face
challenging situations (e.g., temptations to use,
physiological effects of withdrawal). Clients may
begin to reevaluate their self-image as they move
from substance misuse to nonuse or safe use.
Clients are committed to the change process and
are willing to follow suggested change strategies.
•
Maintenance: This stage entails efforts to sustain
gains made during the Action stage and to prevent
recurrence. Extra precautions may be necessary
to keep from reverting to health-risk behaviors.
Individuals learn to identify situations that may
trigger a return to substance use and develop
coping skills to manage such situations. During
Maintenance, clients are building a new lifestyle
that no longer includes the old substance use
behaviors.
Most people who misuse substances progress
through the stages in a circular or spiral pattern,
not a linear one. Individuals typically move back
and forth between the stages and cycle through
the stages at different rates, as shown in the
bidirectional arrows in Exhibit 1.3. As clients
progress through the stages, they often have
setbacks. However, most people do not typically
return to the Precontemplation stage to start over
again (Connors et al., 2013) and are unlikely to
move from Precontemplation back to Maintenance.
This movement through the stages can vary in
relation to different behaviors or treatment goals.
For example, a client might be in the Action
stage with regard to quitting drinking but be
in Precontemplation regarding his or her use
ofcannabis.
Relapse or recurrence of substance misuse is
a common part of the process as people cycle
through the different stages (note the circular
movement of Relapse & Recycle in Exhibit 1.3).
Although clients might return to substance misuse
during any of the stages, relapse is most often
discussed as a setback during the Maintenance
stage (Connors et al., 2013). In this model,
recurrence is viewed as a normal (not pathological)
event because many clients cycle through different
stages several times before achieving stable
change. Recurrence is not considered a failure
Chapter 1 15
TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
but rather a learning opportunity. Remember that
each time clients have a setback, they are learning
from the experience and applying whatever
skills or knowledge they have gained to move
forward in the process with greater understanding
andawareness.
COUNSELOR NOTE: MAKING
DECISIONS
People make decisions about important life
changes by weighing potential gains and losses
associated with making a choice (Janis & Mann,
1977). Weighing the pros and cons of continuing
to use substances or changing substance use
behaviors is a key counseling strategy in the
SOC model. During Contemplation, pros and
cons tend to balance or cancel each other out.
In Preparation, pros for changing substance use
behavior outweigh cons. When the decisional
balance tips toward commitment to change,
clients are ready to take action.
Conclusion
Recent understanding of the key role motivation
plays in addiction treatment has led to the
development of clinical interventions to increase
client motivation to change their substance use
behaviors (DiClemente et al., 2017). Linking this
new view of motivation, the strategies found to
enhance it, and the SOC model, along with an
understanding of what causes change, creates an
effective motivational approach to helping clients
with substance misuse and SUDs. This approach
encourages clients to progress at their own pace
toward deciding about, planning, making, and
sustaining positive behavioral change.
In this treatment approach, motivation for change
is seen as a dynamic state that you can help the
client enhance. Motivational enhancement has
evolved, and various myths about clients and
what constitutes effective counseling have been
dispelled. The notion of the addictive personality
has lost credence, and a confrontational style has
been discarded or significantly modified. Other
factors in contemporary counseling practices have
encouraged the development and implementation
of motivational interventions, which are
client centered and focus on client strengths.
Counseling relationships are more likely to rely
on empathy rather than authority and involve
the client in all aspects of the treatment process.
Less-intensive treatments have also become
increasinglycommon.
Motivation is what propels people with SUDs
to make changes in their lives. It guides clients
through several stages of the SOC that are
typical of people thinking about, initiating, and
maintaining new behaviors. The remainder of this
TIP examines how motivational interventions, when
applied to SUD treatment, can help clients move
from not even considering changing their behavior
to being ready, willing, and able to do so.
Chapter 1 16

Chapter 2—Motivational Counseling and
Brief Intervention
The prevalent clinical focus on denial and motivation as client traits was
misguided. Indeed, client motivation clearly was a dynamic process responding
to a variety of interpersonal influences including advice, feedback, goal setting,
contingencies, and perceived choice among alternatives."
—Miller & Rollnick, 2013, p. 374
KEY MESSAGES
TIP 35
ENHANCING MOTIVATION FOR CHANGE IN
SUBSTANCE USE DISORDER TREATMENT
•
Personalized feedback about a client’s use
of substances relative to others and level
of health-related risk can enhance client
motivation to change substance use behaviors.
• Counselor focus and motivational counseling
strategies should be tailored to the client’s
stage in the Stage of Change (SOC) model.
• Effective motivational counseling approaches
can be brief and include a brief intervention
(BI) and brief treatment (BT) or comprehensive
and include screening, brief intervention, and
referral to treatment (SBIRT).
Chapter 2 examines science-informed elements
of motivational approaches that are effective in
treating substance use disorders (SUDs). Any
clinical strategy that enhances client motivation
for change is a motivational intervention. Such
interventions can include counseling, assessment,
and feedback. They can occur over multiple
sessions or during one BI, and they can be used
in specialty SUD treatment settings or in other
healthcare settings. Chapter 2 also highlights what
you should focus on in each stage of the SOC
approach and discusses how to adapt motivational
interventions to be culturally responsive and
suitable for clients with co-occurring substance use
and mental disorders (CODs).
Elements of Eective Motivational
Counseling Approaches
Motivational counseling strategies have been used
in a wide variety of settings and with diverse client
populations to increase motivation to change
substance use behaviors. The following elements
are important parts of motivational counseling:
•
FRAMES approach
•
Decisional balancing
•
Developing discrepancy between personal goals
and current behavior
•
Flexible pacing
•
Maintaining contact with clients
FRAMES Approach
Miller and Sanchez (1994) identified six common
elements of effective motivational counseling,
which are summarized by the acronym FRAMES:
•
Feedback on personal risk relative to population
norms is given to clients after substance use
assessment.
•
Responsibility for change is placed with the
client.
•
Advice about changing the client’s substance
use is given by the counselor nonjudgmentally.
•
Menu of options and treatment alternatives is
offered to the client.
•
Empathetic counseling style (i.e., warmth,
respect, an understanding) is demonstrated and
emphasized by the counselor.
•
Self-efficacy is supported by the counselor to
encourage client change.
17

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Since FRAMES was developed, research and
clinical experience have expanded and refined
elements of this motivational counseling approach.
FRAMES is often incorporated into SBIRT
interventions. It has also been combined with other
interventions and tested in diverse settings and
cultural contexts (Aldridge, Linford, & Bray, 2017;
Manuel et al., 2015; Satre, Manuel, Larios, Steiger,
& Satterfield, 2015).
Feedback
Give personalized feedback to clients about
their substance use; feedback presented in this
way is effective in reducing substance misuse
and other health-risk behaviors (Davis, Houck,
Rowell, Benson, & Smith, 2015; DiClemente,
Corno, Graydon, Wiprovnick, & Knoblach, 2017;
Field et al., 2014; Kahler et al., 2018; McDevitt-
Murphy et al., 2014; Walker et al., 2017). This type
of feedback usually compares a client’s scores
or ratings on standard screening or assessment
instruments with normative data from a general
population or treatment groups. Feedback should
address cultural differences and norms related to
substance misuse. For example, a review of the
research on adaptations of BI found that providing
feedback specifically related to cultural and social
aspects of drinking to Latino clients reduced
drinking among these clients to a greater degree
than standard feedback (Manuel et al., 2015; Satre
et al., 2015).
COUNSELOR NOTE: MOTIVATIONAL
ENHANCEMENT THERAPY
Presenting and discussing assessment results can
enhance client motivation to change health-risk
behaviors. Providing personalized feedback is
sometimes enough to move clients from the
Precontemplation stage to Contemplation without
additional counseling and guidance.
Structure a feedback session thoughtfully. Establish
rapport before giving a client his or her score.
Strategies to focus the conversation before offering
feedback include the following:
•
Express appreciation for the client’s efforts in
providing the information.
•
Ask whether the client had any difficulties with
answering questions or filling out forms. Explore
specific questions that might need clarification.
•
Make clear that you may need the client’s help
to interpret the findings accurately.
•
Encourage questions: “I’ll be giving you lots
of information. Please stop me if you have a
question or don’t understand something. We
have plenty of time today or in the next session,
if needed.”
•
Stress that the instruments provides objective
data. Give some background, if appropriate,
about how the tests are standardized for all
populations and how widely they are used.
When you provide feedback,
show the client his or her score
on any screening or assessment
instrument and explain what
the score means. Exhibit 2.1
is a sample feedback handout
to share with a client after
completing the Alcohol Use
Disorders Identification Test
(AUDIT). Appendix B presents
the U.S AUDIT questionnaire
and scoring instructions.
Motivational enhancement therapy (MET) is an early offshoot of
the “drinker’s check-up,” which gave feedback nonjudgmentally
to clients about their drinking. MET is a brief motivational
counseling approach that provides personalized, neutral,
motivational interviewing (MI)-style feedback to clients.
Counselors elicit clients’ understanding of feedback, followed
by reflections and listening for signs that clients are considering
behavioral changes based on the feedback (Miller & Rollnick,
2013). Research on MET shows moderate to strong support for
reductions in substance use versus no intervention (DiClemente
et al., 2017; Lenz, Rosenbaum, & Sheperis, 2016).
Chapter 2 18

TIP 35
Chapter 2—Motivational Counseling and Brief Intervention
EXHIBIT 2.1. The Drinker’s Pyramid Feedback
The AUDIT questionnaire was developed by the World Health Organization to assess alcohol consumption,
drinking behaviors, and alcohol-related problems. Your AUDIT score shows the level of health-related risks
and other problems associated with your drinking. Higher scores can reflect more serious alcohol-related
problems. AUD refers to an alcohol use disorder as defined by the American Psychiatric Association (2013).
Your score indicates ______________________________________________________________________
Check here if applicable _____
Your response to AUDIT Question 3 indicates that
you have experienced episodes of binge drinking
(e.g., 5 drinks for men and 4 drinks for women
consumed within 2 hours on a single occasion).
The immediate risks of intoxication or binge
drinkinginclude:
•
Motor crashes or other serious accidents.
•
Falls and other physical injuries.
•
Intimate partner violence.
•
Depressed mood.
•
Suicidal or homicidal thoughts or behavior.
•
Unintended firearm injuries.
•
Alcohol poisoning.
•
Assaults and sexual assaults.
•
Unprotected sex (leading to sexually transmitted
diseases and unintended pregnancy).
•
Child abuse and neglect.
•
Property and other crime.
•
Fires.
Check here if applicable ______
Your responses to AUDIT Questions 1 (frequency)
and 2 (number of drinks consumed) indicate that
you are drinking more than the recommended
limits (no more than 3 drinks on a single day and 7
drinks per week for all women and for men older
than 65; no more than 4 drinks on a single day and
14 drinks per week for men ages 65 and younger).
Long-term risks of alcohol misuse use include:
•
Gastric distress.
•
Hypertension.
•
Cardiovascular disease.
•
Permanent liver damage.
•
Cancer.
•
Pancreatitis.
•
Diabetes.
•
Chronic depression.
•
Neurologic damage.
•
Fetal alcohol spectrum disorders in newborns
(which include physical, behavioral, and
learningdisabilities).
Sources: Babor, Higgins-Biddle, & Robaina, 2016; Venner, Sánchez, Garcia, Williams, & Sussman, 2018.
Chapter 2 19

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Use a motivational style to present the
information. Do not pressure clients to accept a
diagnosis or offer unsolicited opinions about the
meaning of results. Instead, preface explanations
with statements like, “I don’t know whether this will
concern you, but …” or “I don’t know what you’ll
make of this result, but….” Let clients form their
own conclusions, but help them by asking, “What
do you make of this?” or “What do you think
about this?” Focus the conversation on clients’
understanding of the feedback.
Strategies for presenting personalized feedback to
clients include:
•
Asking about the client’s initial reaction to the
tests (e.g., “Sometimes people learn surprising
things when they complete an assessment. What
were your reactions to the questionnaire?”).
•
Providing a handout or using visual aids
that show the client’s scores on screening
instruments, normative data, and risks and
consequences of his or her level of substance
use (see Exhibit 2.1 above). Written materials
should be provided in the client’s first language.
•
Offering information in a neutral,
nonjudgmental, and respectful way.
•
Using easy-to-understand and culturally
appropriate language.
•
Providing small chunks of information.
•
Using open questions to explore the client’s
understanding of the information.
•
Using reflective listening and an empathetic
counseling style that emphasizes the client’s
perspective on feedback and how it may have
affected the client’s readiness to change.
•
Summarizing results, including risks and
problems that have emerged, the client’s
reactions, and any change talk the feedback has
prompted, then asking the client to add to or
correct the summary.
•
Providing a written summary to the client.
Clients’ responses to feedback differ. One may
be alarmed to find that she drinks much more
in a given week than comparable peers but be
unconcerned about potential health risks of
drinking. Another may be concerned about his
potential health risks at this level of drinking. The
key to using feedback to enhance motivation is to
continue to explore the client’s understanding of
the information and what it may suggest about
possible behavior change. Personalized feedback
is applicable to other health-risk behaviors issues,
such as tobacco use (Steinberg, Williams, Stahl,
Budsock, & Cooperman, 2015).
Responsibility
Use a motivational approach to encourage clients
to actively participate in the change process
by reinforcing personal autonomy. Individuals
have the choice of continuing their behavior or
changing it. Remind clients that it is up to them
to make choices about whether they will change
their substance use behaviors or enter treatment.
Reinforcing personal autonomy is aligned with the
self-determination theory discussed in Chapter 1
(Deci & Ryan, 2012; Flannery, 2017).
Strategies for emphasizing client responsibility
include the following:
•
Ask clients’ permission to talk about their
substance use; invite them to consider the
information you are presenting. If clients have
choices, they feel less need to oppose or dismiss
your ideas.
•
State clearly that you will not ask clients to do
anything they are unwilling to do. Let them
know that it is up to them to make choices
about behavior change.
•
Determine a common agenda for each session.
•
Agree on treatment goals that are acceptable
toclients.
When clients realize they are responsible for the
change process, they feel empowered and more
invested in it. This results in better treatment
outcomes (Deci & Ryan, 2012).
Advice
Practice the act of giving advice; this simple
act can promote positive behavioral change.
BI that includes advice delivered in the MET/
MI counseling style can be effective in changing
substance use behaviors such as drinking, drug
use, and tobacco use (DiClemente et al., 2017;
Steinberg et al., 2015). As with feedback, the
Chapter 2 20

TIP 35
Chapter 2—Motivational Counseling and Brief Intervention
manner in which you advise clients influences how
or whether the client will use your advice. It is
better not to tell people what to do; suggestions
yield better results. A motivational approach to
offering advice may be either directive (making a
suggestion) or educational (providing information).
Educational advice should be based on credible
scientific evidence, such as safe drinking limits
recommended by the National Institute on
Alcohol Abuse and Alcoholism or facts that
relate to the client’s conditions (e.g., blood
alcohol concentration levels at the time of an
automobile crash).
EXPERT COMMENT: A REALISTIC
MODEL OF CHANGEADVICE TO
CLIENTS
Throughout the treatment process, clients
should have permission to talk about their
problems with substance use. During these
dialogs, I often point out some of the realities of
the recovery process:
•
Most change does not occur overnight.
•
Change is best viewed as a gradual process
with occasional setbacks, much like hiking up
a bumpy hill.
•
Difficulties and setbacks can be reframed as
learning experiences, not failures.
Linda C. Sobell, Ph.D., Consensus Panel Member
Strategies for offering advice include the following:
•
Ask permission to offer suggestions or provide
information. For example, “Would you like
to hear about safe drinking limits?” or “Can
I tell you what tolerance to alcohol is?” Such
questions provide a nondirective opportunity to
share your knowledge about substance use in a
respectful manner.
•
Ask what the client thinks about your
suggestions or information.
•
Ask for clarification if the client makes a specific
request, rather than give advice immediately.
•
Offer simple suggestions that match the
client’s level of understanding and readiness,
the urgency of the situation, and his or her
culture. In some cultures, a directive approach
is required to convey the importance of advice
or situations; in others, a directive style is
considered rude and intrusive.
This style of giving advice requires patience.
The timing of any advice is important, relying on
your ability to hear what clients are requesting
and willing to receive. Chapter 3 provides more
information about the structured format used in MI
for offering clients feedback or giving advice.
EXPERT COMMENT: THE PIES
APPROACH
In World War I, military psychiatrists first realized
that motivational interventions, done at the right
time, could return many stressed soldiers to
duty. To remember this method, they used the
acronym PIES:
•
Proximity: Provide treatment near the place of
duty; don’t evacuate to a hospital.
•
Immediacy: Intervene and treat at the first
sign of the problem.
•
Expectancy: Expect the intervention to be
successful and return the person to duty.
•
Simplicity: Listen, offer empathy, and show
understanding; this simple approach
worksbest.
Highlight that the person’s reactions are
normal; it is the situation that is abnormal. The
person will recover with rest and nourishment.
No prolonged or complex therapy is needed
for most cases. In the context of World War I,
evacuation to higher levels of care was reserved
for the low percentage of individuals who did
not respond to this straightforward approach.
Kenneth J. Hoffman, M.D., Field Reviewer
Chapter 2 21

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Menu of options
Offer choices to facilitate treatment initiation
and engagement. These choices have been
shown to enhance the therapeutic alliance,
decrease dropout rates, and improve outcomes
(Van Horn et al., 2015). Clients are more likely to
adhere to a specific change strategy if they can
choose from a menu of options. Giving clients
choices for treatment goals and types of available
service increases their motivation to participate
in treatment.
Strategies for offering a menu of options include
the following:
•
Provide accurate information on each option
and potential implications for choosing
that option.
•
Elicit from clients which options they think would
work or what has worked for them in the past.
•
Brainstorm alternative options if none offered
are acceptable to clients.
Providing a menu of options is consistent with
the motivational principle of supporting client
autonomy and responsibility. Clients feel more
empowered when they take responsibility for
their choices. Your role is to enhance their ability
to make informed choices. When clients make
independent decisions, they are likely to be more
committed to them. This concept is examined
more fully in Chapter 6.
Empathic counseling style
Use an empathic counseling style by showing
active interest in understanding clients’
perspectives (Miller & Rollnick, 2013). Counselors
who show high levels of empathy are curious,
spend time exploring clients’ ideas about their
substance use, show an active interest in what
clients are saying, and often encourage clients to
elaborate on more than just the content of their
story (Miller & Rollnick, 2013). Counselor empathy
is a moderately strong predictor of client treatment
outcomes (Elliot, Bohart, Watson, & Murphy, 2018).
As explained in Chapter 3, reflective listening
effectively communicates empathy. The client
does most of the talking when a counselor uses an
empathic style. It is your responsibility to create a
safe environment that encourages a free flow of
communication with the client. An empathic style
appears easy to adopt, but it requires training
and significant effort on your part. This counseling
style can be particularly effective with clients in the
Precontemplation stage.
Self-ecacy
Help clients build self-efficacy by being
supportive, identifying their strengths, reviewing
past successes, and expressing optimism and
confidence in their ability to change (Kaden &
Litt, 2011). To succeed in changing, clients must
believe they can undertake specific tasks in a
specific situation (Bandura, 1977). In addiction
treatment, self-efficacy usually refers to clients’
ability to identify high-risk situations that trigger
their urge to drink or use drugs and to develop
coping skills to manage that urge and not return
to substance use. Considerable evidence points
to self-efficacy as an important factor in addiction
treatment outcomes (Kadden & Litt, 2011; Kuerbis,
Armeli, Muench, & Morgenstern, 2013; Litt &
Kadden, 2015; Morgenstern et al., 2016).
Ask clients to identify how they have successfully
coped with problems in the past: “How did you get
from where you were to where you are now?” or
“How have you resisted the urge to use in stressful
situations?” Once you identify strengths, you can
help clients build on past successes. Affirm small
steps and reinforce any positive changes. Self-
efficacy is discussed again in Chapters 3, 5, and 7.
Decisional Balancing
Explore with the client the benefits and
drawbacks of change (Janis & Mann, 1977).
Individuals naturally explore the pros and cons of
any major life choice, such as changing jobs or
getting married. In SUD recovery, the client weighs
the pros and cons of changing versus not changing
substance use behaviors. You assist this process
by asking the client to articulate the positive and
negative aspects of using substances. This process
is usually called decisional balancing and is further
described in Chapter 5.
Exploring the pros and cons of substance use
behaviors can tip the scales toward a decision for
positive change. The actual number of reasons
Chapter 2 22

TIP 35
Chapter 2—Motivational Counseling and Brief Intervention
a client lists on each side of a decisional balance
sheet is not as important as the weight—or
personal value—of each. For example, a 20-year-
old who smokes cigarettes may put less weight
on getting lung cancer than an older adult, but he
may be very concerned that his diminished lung
capacity interferes with playing basketball.
Developing Discrepancy
To enhance motivation for change, help clients
recognize any discrepancy or gap between
their future goals and their current behavior.
You might clarify this discrepancy by asking,
“How does drinking fit or not fit with your goal
of improving your family relationships?” When
individuals see that present actions conflict with
important personal goals, such as good health, job
success, or close personal relationships, change is
more likely to occur (Miller & Rollnick, 2013). This
concept is expanded in Chapter 3.
Flexible Pacing
Assess the client’s readiness for change; resist
your urges to go faster than the client’s pace.
Every client moves through the SOC at his or
her own pace. Some will cycle back and forth
numerous times between stages. Others need
time to resolve their ambivalence about current
substance use before making a change. A few are
ready to get started and take action immediately.
Knowing where a client has been and is now in the
SOC helps you facilitate the change process at the
right pace. Be aware of any discrepancies between
where you want the client to be and where he or
she actually is in the SOC. For example, if a client
is still in the Contemplation stage, your suggestion
to take steps that are in the Action stage can
creatediscord.
Flexible pacing requires you to meet clients at
their level and allow them as much or as little
time as they need to address the essential tasks
of each stage in the SOC. For example, with some
clients, you may have to schedule frequent sessions
at the beginning of treatment and fewer later. In
other cases, clients might need a break from the
intensity of treatment to focus on specific aspect of
recovery. If you push clients at a faster pace than
they are ready to take, the treatment alliance may
break down.
Maintaining Contact With Clients
Employ simple activities to enhance continuity
of contact between you and the client. Such
activities may include personal handwritten
letters, telephone calls, texts, or emails. Use these
simple motivation-enhancing interventions to
encourage clients to return for another counseling
session, return to treatment following a missed
appointment, and stay involved in treatment.
Activities that foster consistent, ongoing contact
with clients strengthen the therapeutic alliance.
The treatment alliance is widely recognized as a
significant factor in treatment outcomes in most
treatment methods including addiction counseling
(Brorson, Arnevik, Rand-Hendriksen, & Duckert,
2013). Low alliance predicts higher risk of clients
dropping out of treatment (Brorson et al., 2013).
Make sure you and your clients follow all agency
policies and ethical guidelines for making contact
outside of sessions or after discharge. For more
information on using technology to maintain
contact with clients, see Treatment Improvement
Protocol (TIP) 60: Using Technology-Based
Therapeutic Tools in Behavioral Health Services
(Substance Abuse and Mental Health Services
Administration [SAMHSA], 2015b).
Motivational Counseling and
theSOC
People considering major changes in their lives,
such as adopting an alcohol- or drug-free lifestyle,
go through different change processes. Your job
as a counselor is to match your treatment focus
and counseling strategies with these processes
throughout the SOC.
Catalysts for Change
Understand how catalysts for change operate.
This will help you use motivational counseling
strategies that support and enhance changes
clients are contemplating. Prochaska (1979)
identified common personal growth processes
linked to different behavioral counseling
approaches. These processes or catalysts for
change have been further developed and applied
to the SOC model (Connors, DiClemente,
Chapter 2 23

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
Velasquez, & Donovan, 2013). Catalysts are experiential or behavioral (Exhibit 2.2). Experiential catalysts
are linked more frequently with early SOC phases and behavioral catalysts with later SOC phases.
EXHIBIT 2.2. Catalysts for Change
TYPE SPECIFIC CLIENT CHANGE PROCESSES SOC
Experiential
Consciousness raising: Gains new awareness and
understanding of substance use behavior.
Precontemplation/
Contemplation
Emotional arousal: Is motivated to contemplate change after
an important emotional reaction to current substance use
behavior or the need to change.
Precontemplation/
Contemplation
Environmental reevaluation: Evaluates pros and cons of
current substance use behavior and its effects on others and the
community.
Precontemplation/
Contemplation
Self-reevaluation: Explores the current substance use behavior
and the possibility of change in relation to own values.
Contemplation
Social liberation: Recognizes and increases available positive
socialsupports.
Contemplation/
Preparation
Behavioral
Counterconditioning: Begins to recognize the links between
internal and external cues to use substances and experiments
with substituting more healthful behaviors and activities in
response to those cues.
Preparation/Action
Helping relationships: Seeks and cultivates relationships
that offer support, acceptance, and reinforcement for positive
behavioral change.
Preparation/Action/
Maintenance
Self-liberation: Begins to believe in ability to make choices/
to change. Develops enhanced self-efficacy and commits to
changing substance usebehaviors.
Preparation/Action/
Maintenance
Stimulus control: Avoids stimuli and cues that could trigger
substanceuse.
Action
Reinforcement management: Begins to self-reward positive
behavioral changes and eliminates reinforcements for
substance use.
Action/Maintenance
Chapter 2 24

TIP 35
Chapter 2—Motivational Counseling and Brief Intervention
Counselor Focus in the SOC
Use motivational supports that match the client’s
SOC. If you try to use strategies appropriate to a
stage other than the one the client is in, the client
might drop out or not follow through on treatment
goals. For example, if a client in Contemplation
is ambivalent about changing substance use
behaviors and you argue for change or jump
into the Preparation stage, the client is likely to
become reactive.
Examples of how to tailor motivation support
to the client’s stage in the SOC include helping
the client:
•
In Precontemplation consider change by
increasing awareness of behavior change.
•
In Contemplation resolve ambivalence by
helping him or her choose positive change over
the current situation.
•
In Preparation identify potential change
strategies and choose the most appropriate one
for the circumstances.
•
In Action carry out and follow through with the
change strategies.
•
In Maintenance develop new skills to maintain
recovery and a lifestyle without substance
misuse. If misuse resumes, help the client
recover as fast as possible; support reentering
the change cycle.
Exhibit 2.3 depicts the overarching counseling
focus in each stage. Chapters 4 through 7 examine
specific counseling strategies for each stage.
EXHIBIT 2.3. Counselor Focus in the SOC
Source: DiClemente, 2018.
Chapter 2 25

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Special Applications of
Motivational Interventions
The principles underlying motivational counseling
approaches have been applied across cultures, to
different types of problems, in various treatment
settings, and with many different populations
(Miller & Rollnick, 2013). The research literature
suggests that motivational interventions (i.e.,
MI, MET, and BI) are associated with successful
outcomes including adherence to and retention
in SUD treatment; reduction in or abstinence from
alcohol, cannabis, illicit drugs, and tobacco use;
and reductions in substance misuse consequences
and related problems (DiClemente et al., 2017).
Motivational interventions have demonstrated
efficacy across ages (i.e., adolescents, young
adults, and older adults), genders, and racial and
ethnic groups (Lenz et al., 2016).
Special applications of motivational approaches
have been successfully employed as stand-alone
or add-on interventions for people with diabetes,
chronic pain, cardiovascular disease, HIV, CODs,
eating disorders, and opioid use disorder, as well
as for pregnant women who drink or use illicit
drugs (Alperstein & Sharpe, 2016; Barnes & Ivezaj,
2015; Dillard, Zuniga, & Holstad, 2017; Ekong
& Kavookjian, 2016; Hunt, Siegfried, Morley,
Sitharthan, & Cleary, 2013,: Ingersoll, Ceperich,
Hettema, Farrell-Carnahan, & Penberthy, 2013;
Lee, Choi, Yum, Yu, & Chair, 2016; Moore, Flamez,
& Szirony, 2017; Mumba, Findlay, & Snow, 2018;
Osterman, Lewis, & Winhusen, 2017; Soderlund,
2017; Vella-Zarb, Mills, Westra, Carter, & Keating,
2014). The universality of motivational intervention
concepts permits broad application and offers
great potential to reach diverse clients with many
types of problems and in many settings.
Cultural Responsiveness
Clients in treatment for SUDs differ in ethnic,
racial, and cultural backgrounds. Research and
experience suggest that the change process is
similar across different populations. The principles
and mechanisms of enhancing motivation to
change seem to be broadly applicable. For
example, one study found that MI was one of two
evidence-based treatments endorsed as culturally
appropriate by a majority of surveyed SUD
treatment programs serving American Indian and
Alaska Native (AI/AN) clients (Novins, Croy, Moore,
& Rieckmann, 2016).
Processes for engaging do differ
across cultures, but listening lies
at the heart of nearly all of them.
Good listening crosses cultures as
well. It stretches the imagination
to think of people who don’t
appreciate being welcomed,
heard, understood, affirmed,
and recognized as autonomous
human beings. In our experience
these are universally valued.”
—Miller & Rollnick, 2013, p. 349
There may be important differences among
populations and cultural contexts regarding
expression of motivation for change and the
importance of critical life events. Get familiar with
the populations with whom you expect to establish
treatment relationships, be open to listening to and
learning from clients about their cultures and their
own theories of change, and adapt motivational
counseling approaches in consideration of specific
cultural norms (Ewing, Wray, Mead, & Adams,
2012). For example, a manual for adapting MI
for use in treating AI/AN populations includes a
spiritual component that uses a prayer to describe
MI and several spiritual ceremonies to explain MI
(Venner, Feldstein, & Tafoya, 2006).
MI’s core elements, including its emphasis on
collaboration, evoking clients’ perspectives, and
honoring clients’ autonomy, align well culturally
with African Americans (Harley, 2017; Montgomery,
Robinson, Seaman, & Haeny, 2017). However, some
African American women may be less comfortable
with a purely client-centered approach (Ewing et
al., 2012). Viable approaches to adapting MI for
African Americans include training peers to deliver
MI, incorporating moderate amounts of advice,
and implementing MI approaches in community
settings such as a local church (Harley, 2017).
Chapter 2 26

TIP 35Chapter 2—Motivational Counseling and Brief Intervention
Because motivational strategies emphasize the
client’s responsibility to voice personal goals and
values as well as to select among options for
change, you should respond in a nonjudgmental
way to cultural differences. Cultural differences
might be reflected in the value of health, the
meaning of time, the meaning of alcohol or
drug use, or responsibilities to community and
family. Try to understand the client’s perspective
rather than impose mainstream values or make
quick judgments. This requires knowledge of
the influences that promote or sustain substance
use and enhance motivation to change among
different populations. Motivation-enhancing
strategies should be congruent with a client’s
cultural and social principles, standards, and
expectations. Exhibit 2.4 provides a mnemonic to
help you remember the basic principles of cultural
responsiveness.
EXHIBIT 2.4. RESPECT: A Mnemonic for Cultural Responsiveness
Respect Understand how respect is shown in different cultures and
demonstrate it through verbal and nonverbal communication.
Explanatory model Explore the client’s understanding about his or her substance use
and any cultural beliefs or attitudes about substance misuse and
how people change.
Sociocultural context Recognize how class, gender, race, ethnicity, sexual or gender
identity, age, socioeconomic status, and other personal
characteristics that might affect treatment.
Power Acknowledge the power differential between the counselor and
the client.
Empathy Express empathy in ways that communicate that you are
genuinely interested in the client’s perspective and concerns.
Concerns and fears Elicit client concerns about seeking help and entering treatment.
Trust/therapeutic
alliance
Recognize that trust must be earned, and demonstrate actions
that enhance the therapeutic relationship.
Source: SAMHSA, 2014a.
Chapter 2 27

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
EXPERT COMMENT: CULTURAL RESPONSIVENESS
In my practice with persons who have different worldviews, I’ve made a number of observations on the
ways in which culture influences the change process. I try to pay attention to cultural effects on a person’s
style of receiving and processing information, making decisions, pacing, and being ready to act. The
more clients are assimilated into the surrounding culture, the more likely they are to process information,
respond, and make choices that are congruent with mainstream beliefs and styles. The responsibility for
being aware of different cultural value systems lies with the provider, not the client being treated.
More specifically, the manner in which a person communicates, verbally and nonverbally, is often directly
related to culture. One young American Indian stated on initial contact that he “might not be able to
come back because his shoes were too tight.” This was his way of saying he had no money.
However, ethnicity doesn’t always determine the culture or values one chooses to live by. For example,
White Americans may adopt Eastern worldviews and value systems. Furthermore, an advanced education
doesn’t necessarily indicate one’s degree of assimilation or acculturation. Asian Americans or African
Americans who are well educated may choose to live according to their traditional cultural value system
and process information for change accordingly.
Culture is a powerful contributor to defining one’s identity. Not having a healthy ethnic sense of self
affects all stages of the change process. To have a strong sense of self, you have to be powerful in the
areas of being, knowing, doing, and having. Racially and ethnically diverse individuals who have been
raised in environments that isolate them from their own cultures may not have accurate information
about their ethnicity and may not develop a healthy ethnic sense of self.
I believe counselors who use MET need to know different cultural value systems and be culturally
sensitive. If in doubt of the client’s beliefs, explore them with the client. Acknowledging and honoring
differing cultural worldviews greatly influence both motivational style and therapeutic outcome.
Rosalyn Harris-Offutt, Consensus Panel Member
Understand not just how a client’s cultural values
encourage change, but how they may present
barriers to change. Some clients identify strongly
with cultural or religious traditions and work hard
to gain respect from elders or group leaders.
Others find membership or participation in
such groups unhelpful. Some cultures support
involvement of family members in counseling;
others find this disrespectful.
Know what personal and material resources are
available to clients, and be sensitive to issues of
poverty, social isolation, historical trauma, and
recent losses. Recognize that access to financial
and social resources is an important part of the
motivation for and process of change. Poverty
and lack of resources make change more difficult.
It is hard to affirm self-efficacy and stimulate
hope and optimism in clients who lack material
resources and have experienced discrimination.
You can firmly acknowledge the facts of the
situation yet still enhance hope and motivation
to change by affirming clients’ strengths and
capacity for endurance and growth despite difficult
circumstances. For more information on cultural
issues in treatment, see TIP 59: Improving Cultural
Competence (SAMHSA, 2014a).
Chapter 2 28

TIP 35
Chapter 2—Motivational Counseling and Brief Intervention
Adults With COD
Substance use and mental disorders often co-occur.
According to 2017 data from the National Survey
on Drug Use and Health (SAMHSA, 2018), 46.6
million adults ages 18 and older (19 percent of
all U.S. adults) had any mental illness during the
previous year, including 11.2 million (4.5 percent of
all adults) with serious mental illness (SMI). Of this
46.6 million, 18 percent also had an SUD versus
only 5 percent of adults without any mental illness
in the past year. Of the 11.2 million adults with an
SMI in the previous year, almost 28 percent also
had a co-occurring SUD.
Even low levels of substance misuse can have a
serious impact on the functioning of people with
SMI (Hunt et al., 2013). For example, AUD often
co-occurs with major depressive disorder (MDD),
which results in greater disease burdens than
either disorder separately (Riper et al., 2014).
MI and MI combined with cognitive–behavioral
therapy produce positive treatment outcomes,
such as reductions in alcohol consumption,
cannabis use, alcohol misuse, and depression and
other psychiatric symptoms like anxiety (Baker
et al., 2014; Baker, Thornton, Hiles, Hides, &
Lubman, 2012; Riper et al., 2014; Satre, Delucchi,
Lichtmacher, Sterling, & Weisner, 2013; Satre,
Leibowitz, et al., 2016).
Having any mental disorder increases the risk
of substance misuse. As indicated in TIP 42:
Substance Abuse Treatment for Persons With
Co-Occurring Disorders (SAMHSA, 2013), clients
with mental illness or COD may find it harder to
engage and remain in treatment. Motivational
interventions that engage and retain clients in
treatment, increase motivation to adhere to
treatment interventions, and reduce substance
use are a good fit for these clients. A meta-
analysis of randomized controlled treatment studies
of people with SMI and substance misuse found
that, although MI was not any more effective,
in general, than other psychosocial treatments,
clients who participated in an MI group reported to
their first aftercare appointment significantly more
often than clients in other treatment interventions
and these clients had greater alcohol abstinence
rates (Hunt et al., 2013). Another meta-analysis
found that MI-based interventions emphasizing
adherence to treatment significantly improved
adherence and psychiatric symptoms (Wong-
Anuchit, Chantamit-O-Pas, Schneider, & Mills,
2018). Dual Diagnosis MI (DDMI), a modified
version of MI for adults with CODs, can effectively
increase task-specific motivation and adherence
to cognitive training interventions (Fiszdon, Kurtz,
Choi, Bell, & Martino,2015).
COUNSELOR NOTE: DUAL
DIAGNOSIS MOTIVATIONAL
INTERVIEWING
DDMI is a two-session intervention for substance
misuse in clients with psychotic disorders
(Fiszdon et al., 2015). It includes accommodations
for cognitive impairments such as:
•
Asking questions and reflecting in simple
terms.
•
Repeating information and summarizing
session content frequently.
•
Providing more structure to sessions.
•
Being sensitive to emotional material.
•
Using simple, concrete examples.
•
Presenting information using visual aids and
written materials.
•
Restating information frequently.
•
Going at a slower pace.
•
Allowing pauses so clients can process
questions, reflections, and information.
Motivational interventions for SMI and co-occurring
SUDs should be modified to take into account
potential cognitive impairment and focused on
specific tasks that lead to the accomplishment
of treatment goals, as defined by each client.
For more information, see TIP 42: Substance
Abuse Treatment for Persons With Co-Occurring
Disorders (SAMHSA, 2013).
Chapter 2 29

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
EXPERT COMMENT: MI FOR ADULTS WITH COD
I became interested in MI when my team and I were trying to improve the rate of attendance at aftercare
appointments for clients with COD discharged from our psychiatric units. So, my team and I decided to
investigate MI’s effectiveness with clients with COD. We randomly assigned half of our clients to standard
treatment, in which they received standard inpatient psychiatric care, including standard discharge
planning where the team would encourage and explain the importance of aftercare. The other half were
assigned to standard treatment but also received a motivational assessment, feedback on the results at
admission, and a 1-hour MI just before discharge.
We found that clients in the MI group attended their first outpatient appointment at a rate that was
two and a half times greater than the standard treatment group. MI with virtually no modification, was
effective, particularly for clients with very low motivation. This could have been because these clients
were more verbal about their ambivalence than others and because we viewed MI as a perfect way to
resolve ambivalence. Another thing we learned was that asking clients about why they would not attend
aftercare had surprise value and greatly enhanced the rapport between therapist and client. It appeared
to let clients know that we were not only going to tell them about the importance of aftercare, but that
we were actually willing to discuss their ambivalence about it.
Clients were also surprised when we did not directly counter their reasons for not going to aftercare. For
example, if a client said, “I’m better now, I don’t need aftercare,” we would not say, “But to stay well, you
need to continue your treatment.” Instead, we used open end questions (e.g., “What do you think helped
you get better?” or “Tell me more about that”) or amplified reflection (e.g., “So, you’re saying you probably
won’t need any other treatment ever again” or, for more fragile clients, “It’s hard for you to imagine
a reason why you might continue to need treatment”). When clients offered specific disadvantages
of pursuing aftercare, such as loss of time from work or negative reactions from family, we similarly
responded with open end questions and reflective listening (e.g., “It sounds like your job is very important
to you and that you wouldn’t want anything to get in the way of that”). Frequently such questions and
reflections would lead a client to counter his or her own statements. It turned out that client could sell
themselves on the idea of aftercare better than we ever could, and MI gave us the perfect method for
facilitating this process. What was most important, however, was what we did not do—namely, argue with
the client or even attempt to therapeutically dispute his or her (sometimes) illogical ideas about aftercare.
Instead, we waited for kernels of motivation and simply shaped them along until the client finally heard
himself or herself arguing in favor of seeking further services.
Michael V. Pantalon, Ph.D., Field Reviewer
Brief Motivational Interventions
A growing trend worldwide is to view substance
misuse in a much broader context than
diagnosable SUDs. The recognition that people
who misuse substances make up a much larger
group—and pose a serious and costly public
health threat—than the smaller number of people
needing specialized addiction treatment is not
always reflected in the organization and availability
of treatment services. As part of a movement
toward early identification of alcohol misuse
and the development of effective and low-cost
methods to ameliorate this widespread problem, BI
strategies, which include motivational components,
are widely disseminated in the United States and
other countries (Joseph & Basu, 2016).
The impetus to expand the use of BI is a
responseto:
Chapter 2 30

TIP 35
Chapter 2—Motivational Counseling and Brief Intervention
•
The need for a broader base of treatment and
prevention components to serve all segments of
the population that have minimal to severe use
and misuse patterns.
•
The need for cost-effective interventions that
satisfy cost-containment policies in an era
of managed health care (Babor, Del Boca, &
Bray,2017).
•
A growing body of research findings that
consistently demonstrate the efficacy of BI
relative to no intervention (DiClemente et
al.,2017).
four sessions and typically lasts from 5 to 30
minutes (Mattoo, Prasad, & Gosh, 2018). Even
single-session interventions incorporating MET/
MI modalities have demonstrated effectiveness
in reducing substance use behaviors (Samson
& Tanner-Smith, 2015). BI for individuals who
use substances are applied most often outside
specialty addiction treatment settings (in what are
often referred to as opportunistic settings), where
clients are not seeking help for an SUD but have
come, for example, to seek medical attention or
treatment for a mental disorder (Mattoo et al.,
2018). In these situations, people seeking services
are routinely screened for substance misuse or
asked about their substance use patterns. Those
found to be misusing substances or who have
related problems receive a specific BI.
BI is a structured, person-centered counseling
approach that can be delivered by trained health
and behavioral health professionals in one to
EXPERT COMMENT: BI IN THE EMERGENCY DEPARTMENT
When I apply an MI style in my practice of emergency medicine, I experience considerable professional
satisfaction. Honestly, it’s a struggle to let go of the need to be the expert in charge. It helps to recognize
that the person I’m talking with in these medical encounters is also an expert—an expert in her own
lifestyle, needs, and choices.
After learning about the FRAMES principles in 1987, I tried them once or twice, and they worked, so I tried
them again and again. This is not to say that I don’t fall back to old ways and sometimes ask someone,
“Do you want to go to detox?” But more often than not, I try to ask permission to discuss each individual’s
substance use. I ask clients to help me understand what they enjoy about using substances and then
what they enjoy less about it. Clients often tell me they like to get high because it helps them relax and
forget their problems and it’s a part of their social life. But they say they don’t like getting sick from
drugs. They don’t like their family avoiding them or having car crashes. I listen attentively and reflect back
what I understood each person to have said, summarize, and ask, “Where does this leave you?” I also
inquire about how ready they are to change their substance use on a scale of 1 to 10. If someone is low
on the scale, I inquire about what it will take to move forward. If someone is high on the scale, indicating
readiness to change, I ask what this person thinks would work to change his or her substance use.
If a client expresses interest in treatment, I explore pros and cons of different choices. An emergency
department (ED) specialist in SUDs then works with the person to find placement in a program and, if
needed, provides a transportation voucher. This systematic approach, which incorporates MI principles, is
helpful to me in our hectic practice setting. It’s not only ethically sound, based as it is on respect for the
individual’s autonomy, but it’s less time consuming and frustrating. Each person does the work for himself
or herself by naming the problem and identifying possible solutions. My role is to facilitate that process.
Ed Bernstein, M.D., Consensus Panel Member
Chapter 2 31

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
The purpose of a BI is usually to counsel
individuals, using a motivational approach, about
substance misuse patterns; increase awareness
about the negative effects of substance misuse;
and advise them to limit or stop their use
altogether, depending on the circumstances
(Nunes, Richmond, Marzano, Swenson, & Lockhart,
2017). If the initial intervention does not result in
substantial improvement, the provider can make
a referral for specialized SUD treatment. A BI
also can explore the pros and cons of entering
treatment and present a menu of options for
treatment, as well as facilitate contact with the
treatment system. There are several BI models, but
FRAMES is the dominant BI method for substance
misuse (Mattoo et al., 2018).
BI strategies have been used effectively in SUD
treatment settings where people seek assistance
but are placed on waiting lists, as a motivational
prelude to engagement and participation in
more intensive treatment, and as a first attempt
to facilitate behavior change. A series of BI
can constitute BT, an approach that applies
motivational and other treatment methods
(e.g., cognitive–behavioral therapy) for a limited
timeframe, making the modality particularly
effective for clients who want to abstain from,
instead of reduce, alcohol or drug use (Barbosa et
al., 2017). Research has found that BT may be more
effective than BI in reducing illicit drug use patterns
(Aldridge, Dowd, & Bray, 2017).
Screening, Brief Intervention, and
Referral to Treatment
A specific BI called SBIRT, which adds screening
and referral components, has been implemented
widely in the United States in diverse settings,
including EDs, primary care offices, and
community-based health clinics, through a
SAMHSA multisite initiative (Babor et al., 2017). It is
the largest SBIRT dissemination effort in the United
States (Aldridge, Linford, & Bray, 2017). SBIRT was
specifically developed for nonspecialized treatment
settings. It has demonstrated effectiveness in
primary care offices, EDs, and general inpatient
medical units in reducing substance use and misuse
among adolescents, young adults, and adults, as
well as in increasing participation in follow-up care
(Barata et al., 2017; DiClemente et al., 2017; Kohler
& Hoffman, 2015; McQueen, Howe, Allan, Mains,
& Hardy, 2015; Merchant, Romanoff, Zhang, Liu,
& Baird, 2017; Timko, Kong, Vittorio, & Cucciare,
2016; Woolard et al., 2013).
People often seek treatment for medical concerns
that may be related to or impacted by substance
misuse but are not specifically seeking help for
substance use problems. Screening has become
an integral component of BI in these opportunistic
settings (Mattoo et al., 2018). The results of the
screening determine whether the person seeking
services is offered a BI such as FRAMES or is
referred to specialized addiction treatment when
the person meets the criteria for moderate or
severe SUD. From a public health perspective,
SBIRT is seen as both a prevention and a treatment
strategy. Although, research results about the
effectiveness of SBIRT for illicit drug use are mixed
(Hingson & Compton, 2014), recent outcome
data from a SAMHSA initiative demonstrate its
effectiveness to lower alcohol consumption,
alcohol misuse, and illicit drug use (Aldridge,
Linford, & Bray, 2017). Other studies found that
initiation of buprenorphine treatment in the ED
significantly increased clients’ engagement in
specialty addiction treatment and decreased illicit
drug use (Bernstein & D’Onofrio, 2017) and that
motivational interventions in ED and public health
settings reduced overdose risk behaviors and
nonmedical use of opioids (Bohnert et al., 2016;
Coffin et al., 2017).
In addition, a growing body of evidence supports
the use of SBIRT with adolescents, young adults,
adults, and older adults, as well as ethnically and
culturally diverse populations, particularly with
careful selection of screening tools and tailoring
the BI and referrals to each client’s needs (Appiah-
Brempong, Okyere, Owusu-Addo, & Cross, 2014;
Gelberg et al., 2017; Manuel et al., 2015; Satre
et al., 2015; Schonfeld et al., 2010; Tanner-Smith
& Lipsey, 2015). For information about an SBIRT
initiative for older adults (the BRITE Project), see
the upcoming TIP on Treating Addiction in Older
Adults (SAMHSA, planned).
Chapter 2 32

TIP 35Chapter 2—Motivational Counseling and Brief Intervention
Conclusion
Motivational interventions can be used in BI, in BT,
and throughout the SOC process. Some strategies,
like screening and FRAMES, are more applicable
to BI methods whereas others, like developing
discrepancy and decisional balancing, are more
useful in specialized addiction counseling settings
where clients receive longer and more intensive
treatment. What is common in all motivational
interventions, no matter the treatment setting or
the client population, is the focus on engaging
clients, building trust through empathetic listening,
and demonstrating respect for clients’ autonomy
and cultural customs and perspectives.
Chapter 2 33
This page intentionally left blank

Chapter 3—Motivational Interviewing as a
Counseling Style
Motivational interviewing is a person-centered counseling style for
addressing the common problem of ambivalence about change.”
—Miller & Rollnick, 2013, p. 21
KEY MESSAGES
TIP 35
ENHANCING MOTIVATION FOR CHANGE IN
SUBSTANCE USE DISORDER TREATMENT
•
The spirit of motivational interviewing (MI)
is the foundation of the counseling skills
required for enhancing clients’ motivation
tochange.
• Ambivalence about change is normal;
resolving clients’ ambivalence about
substance use is a key MI focus.
• Resistance to change is an expression of
ambivalence about change, not a client trait
or characteristic.
• Reflective listening is fundamental to the four
MI process (i.e., engaging, focusing, evoking,
and planning) and core counseling strategies.
Chapter 3 explores specific MI strategies you can
use to help clients who misuse substances or who
have substance use disorders (SUDs) strengthen
their motivation and commitment to change their
substance use behaviors. This chapter examines
what’s new in MI, the spirit of MI, the concept of
ambivalence, core counseling skills, and the four
processes of MI, as well as the effectiveness of MI
in treating SUDs.
Introduction to MI
MI is a counseling style based on the
followingassumptions:
•
Ambivalence about substance use and change is
normal and is an important motivational barrier
to substance use behavior change.
•
Ambivalence can be resolved by exploring the
client’s intrinsic motivations and values.
•
Your alliance with the client is a collaborative
partnership to which you each bring
important expertise.
•
An empathic, supportive counseling style
provides conditions under which change
can occur.
You can use MI to effectively reduce or eliminate
client substance use and other health-risk
behaviors in many settings and across genders,
ages, races, and ethnicities (DiClemente, Corno,
Graydon, Wiprovnick, & Knoblach, 2017; Dillard,
Zuniga, & Holstad, 2017; Lundahl et al., 2013).
Analysis of more than 200 randomized clinical trials
found significant efficacy of MI in the treatment of
SUDs (Miller & Rollnick, 2014).
The MI counseling style helps clients resolve
ambivalence that keeps them from reaching
personal goals. MI builds on Carl Rogers’ (1965)
humanistic theories about people’s capacity for
exercising free choice and self-determination.
Rogers identified the sufficient conditions for client
change, which are now called “common factors”
of therapy, including counselor empathy (Miller &
Moyers, 2017).
As a counselor, your main goals in MI are to
express empathy and elicit clients’ reasons
for and commitment to changing substance
use behaviors (Miller & Rollnick, 2013). MI
is particularly helpful when clients are in the
Precontemplation and Contemplation stages of
the Stages of Change (SOC), when readiness to
change is low, but it can also be useful throughout
the change cycle.
35

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
The Spirit of MI
Use an MI counseling style to support
partnership with clients. Collaborative counselor–
client relationships are the essence of MI, without
which MI counseling techniques are ineffective.
Counselor MI spirit is associated with positive
client engagement behaviors (e.g., self-disclosure,
cooperation) (Romano & Peters, 2016) and positive
client outcomes in health-related behaviors (e.g.,
exercise, medication adherence) similar to those
in addiction treatment (Copeland, McNamara,
Kelson, & Simpson, 2015).
The spirit of MI (Miller & Rollnick, 2013) comprises
the following elements:
•
Partnership refers to an active collaboration
between you and the client. A client is more
willing to express concerns when you are
empathetic and show genuine curiosity about
the client’s perspective. In this partnership,
you are influential, but the client drives
theconversation.
•
Acceptance refers to your respect for and
approval of the client. This doesn’t mean
agreeing with everything the client says but is a
demonstration of your intention to understand
the client’s point of view and concerns. In the
context of MI, there are four components
of acceptance:
-
Absolute worth: Prizing the inherent worth
and potential of the client
-
Accurate empathy: An active interest in, and
an effort to understand, the client’s internal
perspective reflected by your genuine
curiosity and reflective listening
- Autonomy support: Honoring and
respecting a client’s right to and capacity for
self-direction
- Affirmation: Acknowledging the client’s
values and strengths
•
Compassion refers to your active promotion
of the client’s welfare and prioritization of
clientneeds.
•
Evocation elicits and explores motivations,
values, strengths, and resources the client
already has.
To remember the four elements, use the acronym
PACE (Stinson & Clark, 2017). The specific
counseling strategies you use in your counseling
approach should emphasize one or more of
theseelements.
Principles of Person-Centered Counseling
MI reflects a longstanding tradition of humanistic
counseling and the person-centered approach of
Carl Rogers. It is theoretically linked to his theory
of the “critical conditions for change,” which states
that clients change when they are engaged in a
therapeutic relationship in which the counselor
is genuine and warm, expresses unconditional
positive regard, and displays accurate empathy
(Rogers, 1965).
MI adds another dimension in your efforts to
provide person-centered counseling. In MI, the
counselor follows the principles of person-centered
counseling but also guides the conversation toward
a specific, client-driven change goal. MI is more
directive than purely person-centered counseling; it
is guided by the following broad person-centered
counseling principles (Miller & Rollnick, 2013):
•
SUD treatment services exist to help recipients.
The needs of the client take precedence over
the counselor’s or organization’s needs or goals.
•
The client engages in a process of self-change.
You facilitate the client’s natural process
ofchange.
•
The client is the expert in his or her own life and
has knowledge of what works and what doesn’t.
•
As the counselor, you do not make
changehappen.
•
People have their own motivation, strengths,
and resources. Counselors help activate
thoseresources.
•
You are not responsible for coming up with
all the good ideas about change, and you
probably don’t have the best ideas for any
particularclient.
•
Change requires a partnership and
“collaboration of expertise.”
•
You must understand the client’s perspectives
on his or her problems and need to change.
Chapter 3 36

TIP 35
Chapter 3—Motivational Interviewing as a Counseling Style
•
The counseling relationship is not a power
struggle. Conversations about change should
not become debates. Avoid arguing with or
trying to persuade the client that your position
is correct.
•
Motivation for change is evoked from, not given
to, the client.
•
People make their own decisions about taking
action. It is not a change goal until the client
says so.
•
The spirit of MI and client-centered counseling
principles foster a sound therapeutic alliance.
Research on person-centered counseling
approaches consistent with MI in treating alcohol
use disorder (AUD) found that several sessions
improved client outcomes, including readiness to
change and reductions in alcohol use (Barrio &
Gual, 2016).
What Is New in MI
Much has changed in MI since Miller and Rollnick’s
original (1991) and updated (2002) work. Exhibit
3.1 summarizes important changes to MI based on
decades of research and clinical experience.
EXHIBIT 3.1. A Comparison of Original and Updated Versions of MI
ORIGINAL VERSION UPDATED VERSION
Four principles as the basis for the MI approach:
Four processes as the basis for the MI approach:
1. Express empathy: Demonstrate empathy
1. Engaging is the relational foundation.
through reflective listening.
2. Focusing identifies agenda and change goals.
2. Develop discrepancy: Guide conversations
3. Evoking uses MI core skills and strategies for
to highlight the difference between clients’
moving toward a specific change goal.
goals or values and their current behavior.
4. Planning is the bridge to behavior change.
3. Roll with resistance: Avoid arguing against
the status quo or arguing for change.
The four processes replace Phase I and II stages in
4. Support self-efficacy: Support clients’
the original version of MI. Core skills and strategies
beliefs that change is possible.
of MI include asking open questions, affirming,
using reflective listening, and summarizing; all are
Although these general principles are still
integrated into the four processes. The original four
helpful, the new emphasis in MI is on evoking
principles have been folded into the four processes
change talk and commitment to change as
as reflective listening or strategic responses to move
primary principles.
conversations along.
Resistance is a characteristic of the client. Resistance is an expression of sustain talk and
the status quo side of ambivalence, arising out of
counselor–client discord.
Rolling with resistance Strategies to lessen sustain talk and counselor–client
discord
Self-motivating statements Change talk
Decisional balancing is a strategy to help
clients move in one direction toward changing
a behavior.
Decisional balancing is used to help clients
make a decision without favoring a specific
direction of change. It may be useful as a way
to assess client readiness to change but also
may increase ambivalence for clients who are
contemplatingchange.
Source: Miller & Rollnick, 1991, 2002, 2013; Miller & Rose, 2013.
Chapter 3 37

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Exhibit 3.2 presents common misconceptions about MI and provides clarification of MI’s underlying
theoretical assumptions and counseling approach, which are described in the rest of this chapter.
EXHIBIT 3.2. Misconceptions and Clarifications About MI
MISCONCEPTION CLARIFICATION
MI is a form of
MI shares many principles of the humanistic, person-centered approach
nondirective,
pioneered by Rogers, but it is not Rogerian therapy. Characteristics that
Rogerian therapy.
differentiate MI from Rogerian therapy include clearly identified target behaviors
and change goals and differential evoking and strengthening of clients’
motivation for changing target behavior. Unlike Rogerian therapy, MI has a
strategic component that emphasizes helping clients move toward a specific
behavioral change goal.
MI is a counseling
technique.
Although there are specific MI counseling strategies, MI is not a counseling
technique. It is a style of being with people that uses specific clinical skills to foster
motivation to change.
MI is a “school”
of counseling or
psychotherapy.
Some psychological theories underlie the spirit and style of MI, but it was
not meant to be a theory of change with a comprehensive set of associated
clinicalskills.
MI and the SOC
MI and the SOC were developed around the same time, and people confuse the
approach are the
two approaches. MI is not the SOC. MI is not an essential part of the SOC and
same.
vice versa. They are compatible and complementary. MI is also compatible with
counseling approaches like cognitive–behavioral therapy (CBT).
MI always uses
Assessment feedback delivered in the MI style was an adaptation of MI that
assessment
became motivational enhancement therapy (MET). Although personalized
feedback.
feedback may be helpful to enhance motivation with clients who are on the lower
end of the readiness to change spectrum, it is not a necessary part of MI.
Counselors can
You cannot manufacture motivation that is not already in clients. MI does not
motivate clients to
motive clients to change or to move toward a predetermined treatment goal. It is
change.
a collaborative partnership between you and clients to discover their motivation
to change. It respects client autonomy and self-determination about goals for
behavior change.
Sources: Miller & Rollnick, 2013, 2014; Moyers, 2014.
Ambivalence
A key concept in MI is ambivalence. It is normal
for people to feels two ways about making an
important change in their lives. Frequently, client
ambivalence is a roadblock to change, not a
lack of knowledge or skills about how to change
(Forman & Moyers, 2019). Individuals with SUDs
are often aware of the risks associated with their
substance use but continue to use substances
anyway. They may need to stop using substances,
but they continue to use. The tension between
these feelings is ambivalence.
Ambivalence about changing substance use
behaviors is natural. As clients move from
Precontemplation to Contemplation, their
feelings of conflict about change increase. This
Chapter 3 38

TIP 35
Chapter 3—Motivational Interviewing as a Counseling Style
tension may help move people toward change,
but often the tension of ambivalence leads
people to avoid thinking about the problem.
They may tell themselves things aren’t so bad
(Miller & Rollnick, 2013). View ambivalence
not as denial or resistance, but as a normal
experience in the change process. If you interpret
ambivalence as denial or resistance, you are likely
to evoke discord between you and clients, which
iscounterproductive.
Sustain Talk and Change Talk
Recognizing sustain talk and change talk
in clients will help you better explore and
address their ambivalence. Sustain talk consists
of client statements that support not changing
a health-risk behavior, like substance misuse.
Change talk consists of client statements that
favor change (Miller & Rollnick, 2013). Sustain
talk and change talk are expressions of both sides
of ambivalence about change. Over time, MI
has evolved in its understanding of what keeps
clients stuck in ambivalence about change and
what supports clients to move in the direction of
changing substance use behaviors. Client stuck
in ambivalence will engage in a lot of sustain talk,
whereas clients who are more ready to change
will engage in more change talk with stronger
statements supporting change.
Greater frequency of client sustain talk in sessions
is linked to poorer substance use treatment
outcomes (Lindqvist, Forsberg, Enebrink,
Andersson, & Rosendahl, 2017; Magill et al., 2014;
Rodriguez, Walters, Houck, Ortiz, & Taxman, 2017).
Conversely, MI-consistent counselor behavior
focused on eliciting and reflecting change talk,
more client change talk compared with sustain talk,
and stronger commitment change talk are linked to
better substance use outcomes (Barnett, Moyers,
et al., 2014; Borsari et al., 2018; Houck, Manuel, &
Moyers, 2018; Magill et al., 2014, 2018; Romano &
Peters, 2016). Counselor empathy is also linked to
eliciting client change talk (Pace et al., 2017).
In MI, your main goal
is to evoke change talk
and minimize evoking or
reinforcing sustain talk in
counseling sessions.
Another development in MI is the delineation
of different kinds of change talk. The acronym
for change talk in MI is DARN-CAT (Miller &
Rollnick,2013):
•
Desire to change: This is expressed in
statements about wanting something different—
“I want to find an Alcoholics Anonymous (AA)
meeting” or “I hope to start going to AA.”
•
Ability to change: This is expressed in
statements about self-perception of capability—
“I could start going to AA.”
•
Reasons to change: This is expressed as
arguments for change—“I’d probably learn
more about recovery if I went to AA” or “Going
to AA would help me feel more supported.”
•
Need to change: This is expressed in client
statements about importance or urgency—“I
have to stop drinking” or “I need to find a way
to get my drinking under control.”
•
Commitment: This is expressed as a promise to
change—“I swear I will go to an AA meeting
this year” or “I guarantee that I will start AA by
next month.”
•
Activation: This is expressed in statements
showing movement toward action—“I’m ready
to go to my first AA meeting.”
•
Taking steps: This is expressed in statements
indicating that the client has already done
something to change—“I went to an AA
meeting” or “I avoided a party where friends
would be doing drugs.”
Chapter 3 39

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Exhibit 3.3 depicts examples of change talk and sustain talk that correspond to DARN-CAT.
EXHIBIT 3.3. Examples of Change Talk and Sustain Talk
TYPE OF STATEMENT EXAMPLES OF CHANGE TALK EXAMPLES OF SUSTAIN TALK
Desire “I want to cut down on my drinking.” “I love how cocaine makes me feel.”
Ability “I could cut back to 1 drink with dinner
on weekends.”
“I can manage my life just fine without
giving up the drug.”
Reasons “I’ll miss less time at work if I cut down.” “Getting high helps me feel energized.”
Need “I have to cut down. My doctor told me
that the amount I am drinking puts my
health at risk.”
“I need to get high to keep me going
every day.”
Commitment “I promise to cut back this weekend.” “I am going to keep snorting cocaine.”
Activation “I am ready to do something about
the drinking.”
“I am not ready to give up the cocaine.”
Taking steps “I only had one drink with dinner
on Saturday.”
“I am still snorting cocaine every day.”
Source: Miller & Rollnick, 2013.
To make the best use of clients’ change talk and
sustain talk that arise in sessions, remember to:
•
Recognize client expressions of change talk but
don’t worry about differentiating various kinds
of change talk during a counseling session.
•
Use reflective listening to reinforce and help
clients elaborate on change talk.
•
Use DARN-CAT in conversations with clients.
•
Recognize sustain talk and use MI strategies
to lessen the impact of sustain talk on clients’
readiness to change (see discussion of
responding to change talk and sustain talk in the
next section).
•
Be aware that both sides of ambivalence
(change talk and sustain talk) will be present in
your conversations with clients.
A New Look at Resistance
Understanding the role of resistance and
how to respond to it can help you maintain
good counselor-client rapport. Resistance in
SUD treatment has historically been considered
a problem centered in the client. As MI has
developed over the years, its understanding of
resistance has changed. Instead of emphasizing
resistance as a pathological defense mechanism, MI
views resistance as a normal part of ambivalence
and a client’s reaction to the counselor’s approach
in the moment (Miller & Rollnick, 2013).
A client may express resistance in sustain talk
that favors the “no change” side of ambivalence.
The way you respond to sustain talk can
contribute to the client becoming firmly planted
in the status quo or help the client move toward
contemplating change. For example, the client’s
show of ambivalence about change and your
arguments for change can create discord in your
therapeuticrelationship.
Client sustain talk is often evoked by discord in
the counseling relationship (Miller & Rollnick,
2013). Resistance is a two-way street. If discord
arises in conversation, change direction or
listen more carefully. This is an opportunity
to respond in a new, perhaps surprising, way
and to take advantage of the situation without
being confrontational. This new way of looking
at resistance is consistent with the principles of
person-centered counseling described at the
beginning of the chapter.
Chapter 3 40

TIP 35
Chapter 3—Motivational Interviewing as a Counseling Style
Core Skills of MI: OARS
To remember the core counseling skills of MI, use
the acronym OARS (Miller & Rollnick, 2013):
•
Asking Open questions
•
Affirming
•
Reflective listening
•
Summarizing
These core skills are consistent with the principles
of person-centered counseling and can be used
throughout your work with clients. If you use these
skills, you will more likely have greater success
in engaging clients and less incidence of discord
within the counselor–client relationship. These core
skills are described below.
Asking Open Questions
Use open questions to invite clients to tell
their story rather than closed questions, which
merely elicit brief information. Open questions
are questions that invite clients to reflect before
answering and encourage them to elaborate.
Asking open questions helps you understand their
point of view. Open questions facilitate a dialog
and do not require any particular response from
you. They encourage clients to do most of the
talking and keep the conversation moving forward.
Closed questions evoke yes/no or short answers
and sometimes make clients feel as if they have to
come up with the right answer. One type of open
question is actually a statement that begins with
“Tell me about” or “Tell me more about.” The “Tell
me about” statement invites clients to tell a story
and serves as an open question.
Exhibit 3.4 provides examples of closed and open questions. As you read these examples, imagine you are
a client and notice the difference in how you might receive and respond to each kind of question.
EXHIBIT 3.4. Closed and Open Questions
CLOSED QUESTIONS OPEN QUESTIONS
“So you are here because you are concerned about your
use of alcohol, correct?”
“What is it that brings you here today?”
“How many children do you have?” “Tell me about your family.”
“Do you agree that it would be a good idea for you to go
through detoxification?”
“What do you think about the possibility of
going through detoxification?”
“On a typical day, how much marijuana do you smoke?” “Tell me about your marijuana use on a typical
day.”
“Did your doctor tell you to quit smoking?” “What did your doctor tell you about the
health risks of smoking?”
“How has your drug use been this week compared with
last week: more, less, or about the same?”
“What has your drug use been like during the
past week?”
“Do you think you use amphetamines too often?” “In what ways are you concerned about your
use of amphetamines?”
“How long ago did you have your last drink?” “Tell me about the last time you drank.”
“Are you sure that your probation officer told you that it’s
only cocaine he is concerned about in your urine screens?”
“Tell me more about the conditions of your
probation.”
“When do you plan to quit drinking?” “What do you think you want to do about your
drinking?”
Chapter 3 41

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
There may be times when you must ask closed
questions, for example, to gather information for
a screening or assessment. However, if you use
open questions—“Tell me about the last time you
used methamphetamines”—you will often get the
information you need and enhance the process
of engagement. During assessment, avoid the
question-and-answer trap, which can decrease
rapport, become an obstacle to counselor–client
engagement, and stall conversations.
MI involves maintaining a balance between
asking questions and reflective listening (Miller &
Rollnick, 2013). Ask one open question, and follow
it with two or more reflective listening responses.
Arming
Affirming is a way to express your genuine
appreciation and positive regard for clients
(Miller & Rollnick, 2013). Affirming clients supports
and promotes self-efficacy. By affirming, you are
saying, “I see you, what you say matters, and I
want to understand what you think and feel” (Miller
& Rollnick, 2013). Affirming can boost clients’
confidence about taking action. Using affirmations
in conversations with clients consistently predicts
positive client outcomes (Romano & Peters, 2016).
When affirming:
•
Emphasize client strengths, past successes,
and efforts to take steps, however small, to
accomplish change goals.
•
Do not confuse this type of feedback with
praise, which can sometimes be a roadblock to
effective listening (Gordon, 1970; see Exhibit 3.5
below in the section “Reflective Listening”).
•
Frame your affirming statements with “you”
instead of “I.” For example, instead of saying
“I am proud of you,” which focuses more on
you than on the client, try “You have worked
really hard to get to where you are now in your
life,” which demonstrates your appreciation, but
keeps the focus on the client (Miller & Rollnick,
2013).
•
Use statements such as (Miller & Rollnick, 2013):
-
“You took a big step in coming here today.”
-
“You got discouraged last week but
kept going to your AA meetings. You
arepersistent.”
-
“Although things didn’t turn out the way you
hoped, you tried really hard, and that means
a lot.”
-
“That’s a good idea for how you can avoid
situations where you might be tempted
todrink.”
There may be ethnic, cultural, and even personal
differences in how people respond to affirming
statements. Be aware of verbal and nonverbal
cues about how the client is reacting and be
open to checking out the client’s reaction with an
open question—“How was that for you to hear?”
Strategies for forming affirmations that account
for cultural and personal differences include
(Rosengren, 2018):
•
Focusing on specific behaviors to affirm.
•
Avoiding using “I.”
•
Emphasizing descriptions instead of evaluations.
•
Emphasizing positive developments instead of
continuing problems.
•
Affirming interesting qualities and strengths
ofclients.
•
Holding an awareness of client strengths instead
of deficits as you formulate affirmations.
Reective Listening
Reflective listening is the key component of
expressing empathy. Reflective listening is
fundamental to person-centered counseling in
general and MI in particular (Miller & Rollnick,
2013). Reflective listening (Miller & Rollnick, 2013):
•
Communicates respect for and acceptance
ofclients.
•
Establishes trust and invites clients to explore
their own perceptions, values, and feelings.
•
Encourages a nonjudgmental,
collaborativerelationship.
•
Allows you to be supportive without agreeing
with specific client statements.
Chapter 3 42

TIP 35
Chapter 3—Motivational Interviewing as a Counseling Style
Reflective listening builds collaboration and a
safe and open environment that is conducive to
examining issues and eliciting the client’s reasons
for change. It is both an expression of empathy
and a way to selectively reinforce change talk
(Romano & Peters, 2016). Reflective listening
demonstrates that you are genuinely interested
in understanding the client’s unique perspective,
feelings, and values. Expressions of counselor
empathy predict better substance use outcomes
(Moyers, Houck, Rice, Longabaugh, & Miller, 2016).
Your attitude should be one of acceptance but not
necessarily approval or agreement, recognizing
that ambivalence about change is normal.
Consider ethnic and cultural differences
when expressing empathy through reflective
listening. These differences influence how
both you and the client interpret verbal and
nonverbalcommunications.
EXPERT COMMENT: EXPRESSING EMPATHY WITH AFRICAN
AMERICAN CLIENTS
One way I empathize with African American clients is, first and foremost, to be a genuine person
(not just a counselor). Clients may begin the relationship asking questions about you the person,
not the professional, in an attempt to locate you in the world. It’s as if clients’ internal dialog says,
“As you try to understand me, by what pathways, perspectives, life experiences, and values are you
coming to that understanding of me?”
Typical questions my African American clients have asked me are:
•
“Are you Christian?”
•
“Where are you from?”
•
“What part of town do you live in?”
•
“Who are your folks?”
•
“Are you married?”
All of these are reasonable questions that work to establish a real, not contrived, relationship with
the counselor. As part of a democratic partnership, clients have a right and, in some instances, a
cultural expectation to know about the helper.
On another level, many African Americans are very spiritual people. This spirituality is expressed
and practiced in ways that supersede religious affiliations. Young people pat their chests and say,
“I feel you,” as a way to describe this sense of empathy. Understanding and working with this can
enhance the counselor’s expression of empathy. In other words, the therapeutic counselor‒client
alliance can be deepened, permitting another level of empathic connection that some might
call an intuitive understanding and others might call a spiritual connection to each client. What
emerges is a therapeutic alliance—a spiritual connection—that goes beyond what mere words
can say. The more counselors express that side of themselves, whether they call it intuition or
spirituality, the more intense the empathic connection the African American client will feel.
Cheryl Grills, Ph.D., Consensus Panel Member
Chapter 3 43

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
EXPERT COMMENT: EXPRESSING EMPATHY WITH AMERICAN
INDIANNATIVE AMERICAN CLIENTS
For many traditional American Indian groups, expressing empathy begins with the
introduction. Native Americans generally expect the counselor to be aware of and practice
the culturally accepted norms for introducing oneself and showing respect. For example,
during the first meeting, the person often is expected to say his or her name, clan relationship
or ethnic origin, and place of origin. Physical contact is kept to a minimum, except for a brief
handshake, which may be no more than a soft touch of the palms.
Ray Daw, Consensus Panel Member
Reflective listening is not as easy as it sounds. It is
not simply a matter of being quiet while the client
is speaking. Reflective listening requires you to
make a mental hypothesis about the underlying
meaning or feeling of client statements and then
reflect that back to the client with your best
guess about his or her meaning or feeling (Miller
& Rollnick, 2013). Gordon (1970) called this “active
listening” and identified 12 kinds of responses that
people often give to others that are not active
listening and can actually derail a conversation.
Exhibit 3.5 describes these roadblocks to listening.
EXHIBIT 3.5. Gordon’s 12 Roadblocks to Active Listening
1. Ordering, directing,
orcommanding
Direction is given with a voice of authority. The speaker may be in
a position of power (e.g., parent, employer, counselor) or the words
may simply be phrased and spoken in a way that communicates
that the speaker is the expert.
2. Warning, cautioning, or
threatening
These statements carry an overt or covert threat of negative
consequences. For example, “If you don’t stop drinking, you are
going to die.”
3. Giving advice, making
suggestions, or providing
solutions prematurely or
whenunsolicited
The message recommends a course of action based on your
knowledge and personal experience. These recommendations often
begin with phrases like “What I would do is.”
4. Persuading with logic,
arguing, or lecturing
The underlying assumption of these messages is that the client
has not reasoned through the problem adequately and needs
help to do so. Trying to persuade the client that your position is
correct will most likely evoke a reaction and the client taking the
oppositeposition.
5. Moralizing, preaching, or
telling people what they
should do
These statements contain such words as “should” or “ought,” which
imply or directly convey negative judgment.
6. Judging, criticizing,
disagreeing, or blaming
These messages imply that something is wrong with the client or
with what the client has said. Even simple disagreement may be
interpreted as critical.
Continued on next page
Chapter 3 44

TIP 35
Chapter 3—Motivational Interviewing as a Counseling Style
Continued
7. Agreeing, approving,
or praising
Praise or approval can be an obstacle if the message sanctions
or implies agreement with whatever the client has said or if the
praise is given too often or in general terms, like “great job.” This
can lessen the impact on the person or simply disrupt the flow of
theconversation.
8. Shaming, ridiculing, or
labeling
These statements express disapproval and intent to correct a
specific behavior or attitude. They can damage self-esteem and
cause major disruptions in the counseling alliance.
9. Interpreting or analyzing You may be tempted to impose your own interpretations on a
client’s statement and to find some hidden, analytical meaning.
Interpretive statements might imply you know what the client’s
“real” problem is and puts you in a one-up position.
10. Reassuring, sympathizing,
orconsoling
Counselors often want to console the client. It is human nature to
want to reassure someone who is in pain; however, sympathy is not
the same as empathy. Such reassurance can interrupt the flow of
communication and interfere with careful listening.
11. Questioning or probing Do not mistake questioning for good listening. Although you
may ask questions to learn more about the client, the underlying
message is that you might find the right answer to all the
client’s problems if enough questions are asked. In fact, intensive
questioning can disrupt communication, and sometimes the client
feels as if he or she is being interrogated.
12. Withdrawing, distracting,
humoring, or changing
the subject
Although shifting the focus or using humor may be helpful at times,
it can also be a distraction and disrupt the communication.
Source: Gordon, 1970.
If you engage in any of these 12 activities,
you are talking and not listening. However well
intentioned, these roadblocks to listening shift
the focus of the conversation from the client to
the counselor. They are not consistent with the
principles of person-centered counseling.
Types of reective listening
In MI, there are several kinds of reflective
listening responses that range from simple (i.e.,
repeating or rephrasing a client statement) to
complex (i.e., using different words to reflect
the underlying meaning or feeling of a client
statement). Simple reflections engage clients and
let them know that you’re genuinely interested
in understanding their perspective. Complex
reflections invite clients to deepen their self-
exploration (Miller & Rollnick, 2013). In MI, there
are special complex reflections that you can use
in specific counseling situations, like using a
double-sided reflection when clients are expressing
ambivalence about changing a substance use
behavior. Exhibit 3.6 provides examples of simple
and complex reflective listening responses to client
statements about substance use.
Chapter 3 45

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
EXHIBIT 3.6. Types of Reflective Listening Responses
TYPE CLIENT STATEMENT
COUNSELOR
RESPONSE
PURPOSE
SPECIAL
CONSIDERATIONS
Simple
Repeat “My wife is nagging
me about my
drinking.”
“Your wife is nagging
you about your
drinking.”
Builds rapport.
Expresses empathy.
Avoid mimicking.
Rephrase “My wife is nagging
me about my
drinking.”
“Your wife is pressuring
you about your
drinking.”
Expresses empathy.
Highlights selected
meaning or feeling.
Move the
conversation along,
but more slowly than
complex reflections.
Complex
Feeling “I’d like to quit
smoking marijuana
so that the second-
hand pot smoke
won’t worsen my
daughter’s asthma.”
“You’re afraid that your
daughter’s asthma
will get worse if you
continue smoking
marijuana.”
Highlights selected
feeling.
Highlights
discrepancy
between values
and current
behavior.
Selectively reinforce
change talk.
Avoid reinforcing
sustain talk.
Meaning “I’d like to quit
smoking marijuana
because I read that
second-hand pot
smoke can make
asthma worse and
I don’t want that
to happen to my
daughter.”
“You want to protect
your daughter from
the possibility that her
asthma will get worse if
you continue smoking
marijuana.”
Highlights selected
meaning.
Highlights
discrepancy
between values
and current
behavior.
Selectively reinforce
change talk.
Avoid reinforcing
sustain talk.
Double- “I know I should give
“Giving up drinking
Resolves
Use “and” to join two
sided up drinking, but I
can’t imagine life
without it.”
would be hard, and you
recognize that it’s time
to stop.”
ambivalence.
Acknowledges
sustain talk and
emphasizes change
talk.
reflections.
Start with sustain
talk reflection and
end with change talk
reflection.
Amplified “I think my cocaine
use is just not a
problem for me.”
“There are absolutely no
negative consequences
of using cocaine.”
Intensifies sustain
talk to evoke
change talk.
Use sparingly.
Avoid getting stuck in
sustain talk.
Source: Miller & Rollnick, 2013.
Chapter 3 46

TIP 35
Chapter 3—Motivational Interviewing as a Counseling Style
Forming complex reections
careful reflective listening builds a strong
therapeutic alliance and facilitates the client’s self-
exploration—two essential components of person-
centered counseling (Miller & Rollnick, 2013).
The key to expressing accurate empathy through
reflective listening is your ability to shift gears
from being an expert who gives advice to being
an individual supporting the client’s autonomy
and expertise in making decisions about changing
substance use behaviors (Moyers, 2014).
Simple reflections are fairly straightforward. You
simply repeat or paraphrase what the client said.
Complex reflections are more challenging. A
statement could have many meanings. The first
step in making a complex reflection of meaning
or feelings is to make a hypothesis in your mind
about what the client is trying to say (Miller &
Rollnick,2013).
Use these steps to form a mental hypothesis
about meaning or feelings:
1. If the client says, “I drink because I am lonely,”
think about the possible meanings of “lonely.”
Perhaps the client is saying, “I lost my spouse”
or “It is hard for me to make friends” or “I
can’t think of anything to say when I am with
myfamily.”
2. Consider the larger conversational context. Has
the client noted not having much of a social life?
3. Make your best guess about the meaning of the
client’s statement.
4. Offer a reflective listening response—“You drink
because it is hard for you to make friends.”
5. Wait for the client’s response. The client will
tell you either verbally or nonverbally if your
guess is correct. If the client continues to talk
and expands on the initial statement, you are
ontarget.
6. Be open to being wrong. If you are, use client
feedback to make another hypothesis about the
client’s meaning.
Remember that reflective listening is about
refraining from making assumptions about the
underlying message of client statements, making
a hypothesis about the meaning or feeling of the
statement, and then checking out your hypothesis
by offering a reflective statement and listening
carefully to the client’s response (Miller & Rollnick,
2013). Reflective listening is basic to all of four MI
processes. Follow open questions with at least
one reflective listening response—but preferably
two or three responses—before asking another
question. A higher ratio of reflections to questions
consistently predicts positive client outcomes
(Romano & Peters, 2016). It takes practice to
become skillful, but the effort is worth it because
Summarizing
Summarizing is a form of reflective listening that
distills the essence of several client statements
and reflects them back to him or her. It is not
simply a collection of statements. You intentionally
select statements that may have particular
meaning for the client and present them in a
summary that paints a fuller picture of the client’s
experience than simply using reflections (Miller &
Rollnick,2013).
There are several types of summarization in MI
(Miller & Rollnick, 2013):
•
Collecting summary: Recalls a series of related
client statements, creating a narrative to
reflect on.
•
Linking summary: Reflects a client statement;
links it to an earlier statement.
•
Transitional summary: Wraps up a
conversation or task; moves the client along the
change process.
•
Ambivalence summary: Gathers client
statements of sustain talk and change talk
during a session. This summary should
acknowledge sustain talk but reinforce and
highlight change talk.
•
Recapitulation summary: Gathers all of the
change talk of many conversations. It is useful
during the transition from one stage to the next
when making a change plan.
At the end of a summary, ask the client whether
you left anything out. This opportunity lets the
client correct or add more to the summary and
often leads to further discussion. Summarizing
encourages client self-reflection.
Chapter 3 47

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Summaries reinforce key statements of
movement toward change. Clients hear change
talk once when they make a statement, twice
when the counselor reflects it, and again when
the counselor summarizes the discussion.
Four Processes of MI
MI has moved away from the idea of phases
of change to overlapping processes that more
accurately describe how MI works in clinical
practice. This change is a shift away from a linear,
rigid model of change to a circular, fluid model
of change within the context of the counseling
relationship. This section reviews these MI
processes, summarizes counseling strategies
appropriate for each process, and integrates the
four principles of MI from previous versions.
Engaging
Engaging clients is the first step in all counseling
approaches. Specific counseling strategies or
techniques will not be effective if you and the client
haven’t established a strong working relationship.
MI is no exception to this. Miller and Rollnick
(2013) define engaging in MI “as the process of
establishing a mutually trusting and respectful
helping relationship” (p. 40). Research supports
the link between your ability to develop this kind
of helping relationship and positive treatment
outcomes such as reduced drinking (Moyers et al.,
2016; Romano & Peters, 2016).
Opening strategies
Opening strategies promote engagement in MI
by emphasizing OARS in the following ways:
•
Ask open questions instead of closed questions.
•
Offer affirmations of client self-efficacy, hope,
and confidence in the client’s ability to change.
•
Emphasize reflective listening.
•
Summarize to reinforce that you are
listening and genuinely interested in the
client’sperspective.
•
Determine the client’s readiness to change or
and specific stage in the SOC (see Chapters 1
and 2).
•
Avoid prematurely focusing on taking action.
•
Try not to identify the client’s treatment
goals until you have sufficiently explored the
client’s readiness. Then you can address the
client’sambivalence.
These opening strategies ensure support for the
client and help the client explore ambivalence in
a safe setting. In the following initial conversation,
the counselor uses OARS to establish rapport and
address the client’s drinking through reflective
listening and asking open questions:
•
Counselor: Jerry, thanks for coming in.
(Affirmation) What brings you here today?
(Open question)
•
Client: My wife thinks I drink too much. She says
that’s why we argue all the time. She also thinks
that my drinking is ruining my health.
•
Counselor: So your wife has some
concerns about your drinking interfering
with your relationship and harming your
health.(Reflection)
•
Client: Yeah, she worries a lot.
•
Counselor: You wife worries a lot about the
drinking. (Reflection) What concerns you about
it? (Open question)
•
Client: I’m not sure I’m concerned about it, but I
do wonder sometimes if I’m drinking too much.
•
Counselor: You are wondering about the
drinking. (Reflection) Too much for…? (Open
question that invites the client to complete
the sentence)
•
Client: For my own good, I guess. I mean it’s
not like it’s really serious, but sometimes when I
wake up in the morning, I feel really awful, and I
can’t think straight most of the morning.
•
Counselor: It messes up your thinking, your
concentration. (Reflection)
•
Client: Yeah, and sometimes I have trouble
remembering things.
•
Counselor: And you wonder if these problems
are related to drinking too much. (Reflection)
•
Client: Well, I know it is sometimes.
•
Counselor: You’re certain that sometimes
drinking too much hurts you. (Reflection) Tell
me what it’s like to lose concentration and have
trouble remembering. (Open question in the
form of a statement)
Chapter 3 48

TIP 35
Chapter 3—Motivational Interviewing as a Counseling Style
•
Client: It’s kind of scary. I am way too young to
have trouble with my memory. And now that
I think about it, that’s what usually causes the
arguments with my wife. She’ll ask me to pick
up something from the store and when I forget
to stop on my way home from work, she starts
yelling at me.
•
Counselor: You’re scared that drinking is
starting to have some negative effects on
what’s important to you like your ability to think
clearly and good communication with your wife.
(Reflection)
•
Client: Yeah. But I don’t think I’m an alcoholic
oranything.
•
Counselor: You don’t think you’re that bad off,
but you do wonder if maybe you’re overdoing it
and hurting yourself and your relationship with
your wife. (Reflection)
•
Client: Yeah.
•
Counselor: You know, Jerry, it takes courage to
come talk to a stranger about something that’s
scary to talk about. (Affirmation) What do you
think? (Open question)
•
Client: I never thought of it like that. I guess
it is important to figure out what to do about
mydrinking.
•
Counselor: So, Jerry, let’s take a minute
to review where we are today. Your wife is
concerned about how much you drink. You
have been having trouble concentrating and
remembering things and are wondering if that
has to do with how much you are drinking.
You are now thinking that you need to figure
out what to do about the drinking. Did I miss
anything? (Summary)
Avoiding traps
Identify and avoid traps to help preserve client
engagement. The above conversation shows
use of core MI skills to engage the client and
help him feel heard, understood, and respected
while moving the conversation toward change.
The counselor avoids common traps that
increasedisengagement.
Common traps to avoid include the following
(Miller & Rollnick, 2013):
•
The Expert Trap: People often see a
professional, like primary care physician or nurse
practitioner, to get answers to questions and
to help them make important decisions. But
relying on another person (even a professional)
to have all the answers is contrary to the spirit
of MI and the principles of person-centered
care. Both you and the client have expertise.
You have knowledge and skills in listening and
interviewing; the client has knowledge based on
his or her life experience. In your conversations
with a client, remember that you do not have
to have all the answers, and trust that the client
has knowledge about what is important to him
or her, what needs to change, and what steps
need to be taken to make those changes. Avoid
falling into the expert trap by:
-
Refraining from acting on the “righting
reflex,” the natural impulse to jump into
action and direct the client toward a specific
change. Such a directive style is likely to
produce sustain talk and discord in the
counseling relationship.
-
Not arguing with the client. If you try to
prove a point, the client predictably takes the
opposite side. Arguments with the client can
rapidly degenerate into a power struggle and
do not enhance motivation for change.
Chapter 3 49

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
•
The Labeling Trap: Diagnoses and labels like
“alcoholic” or “addict” can evoke shame in
clients. There is no evidence that forcing a
client to accept a label is helpful; in fact,
it usually evokes discord in the counseling
relationship. In the conversation above, the
counselor didn’t argue with Jerry about whether
he is an “alcoholic.” If the counselor had
done so, the outcome would likely have been
different:
- Client: But I don’t think I’m an alcoholic
oranything.
- Counselor: Well, based on what you’ve told
me, I think we should do a comprehensive
assessment to determine whether or not
youare.
- Client: Wait a minute. That’s not what I
came for. I don’t think counseling is going to
helpme.
•
The Question-and-Answer Trap: When your
focus is on getting information from a client,
particularly during an assessment, you and
the client can easily fall into the question-and-
answer trap. This can feel like an interrogation
rather than a conversation. In addition, a
pattern of asking closed questions and giving
short answers sets you up in the expert role,
and the client becomes a passive recipient of
the treatment intervention instead of an active
partner in the process. Remember to ask open
questions, and follow them with reflective
listening responses to avoid the question-and-
answer trap.
•
The Premature Focus Trap: You can fall into this
trap when you focus on an agenda for change
before the client is ready—for example, jumping
into solving problems before developing a
strong working alliance. When you focus on an
issue that is important to you (e.g., admission to
an inpatient treatment program) but not to the
client, discord will occur. Remember that your
approach should match where the client is with
regard to his or her readiness to change.
•
The Blaming Trap: Clients often enter treatment
focused on who is to blame for their substance
use problem. They may feel guarded and
defensive, expecting you to judge them harshly
as family, friends, coworkers, or others may
have. Avoid the blame trap by immediately
reassuring clients that you are uninterested in
blaming anyone and that your role is to listen to
what troubles them.
Focusing
Once you have engaged the client, the next step
in MI is to find a direction for the conversation
and the counseling process as a whole. This is
called focusing in MI. With the client, you develop
a mutually agreed-on agenda that promotes
change and then identify a specific target behavior
to discuss. Without a clear focus, conversations
about change can be unwieldy and unproductive
(Miller & Rollnick, 2013).
Deciding on an agenda
MI is essentially a conversation you and the
client have about change. The direction of the
conversation is influenced by the client, the
counselor, and the clinical setting (Miller & Rollnick,
2013). For example, a client walking through the
door of an outpatient SUD treatment program
understand that his or her use of alcohol and other
drugs will be on the agenda.
Clients, however, may be mandated to treatment
and may not see their substance use as a problem,
or they may have multiple issues (e.g., child care,
relational, financial, legal problems) that interfere
with recovery and that need to be addressed.
When clients bring multiple problems to the table
or are confused or uncertain about the direction
of the conversation, you can engage in agenda
mapping, which is a process consistent with MI
that helps you and clients decide on the counseling
focus. Exhibit 3.7 displays the components in an
agenda map.
Chapter 3 50

TIP 35
Chapter 3—Motivational Interviewing as a Counseling Style
EXHIBIT 3.7. Components in a Sample Agenda Map
Source: Miller & Rollnick, 2013.
To engage in agenda mapping (Miller & Rollnick, 2013):
•
Have an empty agenda map handout handy, or draw 8 to 10 empty circles or shapes on a
blankpaper.
•
Present the empty agenda map or the sheet of paper to the client by saying, “I know you were
referred here to address [name the problem, such as drinking], but you may have other concerns
you want to discuss. I’d like to take a few minutes and write down things you may want to talk
about. That way, we’ll have a map we can look at to see whether we’re headed in the right
direction. How does that sound?”
•
Write a different concern or issue in each circle. Leave two or three circles blank so that you can
add a new client concern or suggest a topic that may be important to discuss. If you suggest
a topic, frame it in a way that asks permission and leaves the choice to the client: “You’ve
mentioned a few different concerns that are important to discuss. Would it be okay to also talk
about [name the problem, such as drug use] because that’s why you were referred to treatment?”
•
Ask the client what the most pressing concern is: “You’ve mentioned several things you’d like to
talk about. (Summarize) Where would you like to start?”
•
Leave time to guide the client back to the substance use concern if not discussed during
thesession.
•
Keep the map as a visual record, and refer back to it with the client as a reminder of the focus
and direction of the counseling process. Add and delete topics as needed.
•
Remember to use OARS throughout this process to move the conversation along.
Chapter 3 51

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Identifying a target behavior
Once you and the client agree on a general
direction, focus on a specific behavior the client
is ready to discuss. Change talk links to a specific
behavior change target (Miller & Rollnick, 2010);
you can’t evoke change talk until you identify a
target behavior. For example, if the client is ready
to discuss drinking, guide the conversation toward
details specific to that concern. A sample of such a
conversation follows:
•
Counselor: Marla, you said you’d like to talk
about your drinking. It would help if you’d give
me a sense of what your specific concerns are
about drinking. (Open question in the form of
astatement)
•
Client: Well, after work I go home to my
apartment and I am so tired; I don’t want to
do anything but watch TV, microwave a meal,
and drink till I fall asleep. Then I wake up with
a big hangover in the morning and have a hard
time getting to work on time. My supervisor has
given me a warning.
•
Counselor: You’re worried that the amount
you drink affects your sleep and ability to get
to work on time. (Reflection) What do you
think you’d like to change about the drinking?
(Openquestion)
•
Client: I think I need to stop drinking completely
for a while, so I can get into a healthy
sleeppattern.
•
Counselor: So I’d like to put stop drinking
for a while on the map, is that okay? [Asks
permission. Pauses. Waits for permission.] Let’s
focus our conversations on that goal.
Notice that this client is already expressing
change talk about her alcohol use. By narrowing
the focus from drinking as a general concern to
stopping drinking as a possible target behavior, the
counselor moved into the MI process of evoking.
Evoking
Evoking elicits client motivations for change.
It shapes conversations in ways that encourage
clients, not counselors, to argue for change.
Evoking is the core of MI and differentiates it
from other counseling methods (Miller & Rollnick,
2013). The following sections explore evoking
change talk, responding to change talk and sustain
talk, developing discrepancy, evoking hope and
confidence to support self-efficacy, recognizing
signs of readiness to change, and asking
keyquestions.
Evoking change talk
Engaging the client in the process of change is the
fundamental task of MI. Rather than identifying
the problem and promoting ways to solve it, your
task is to help clients recognize that their use of
substances may be contributing to their distress
and that they have a choice about how to move
forward in life in ways that enhance their health and
well-being. One signal that clients’ ambivalence
about change is decreasing is when they start to
express change talk.
The first step to evoking change talk is to ask
open questions. There are seven kinds of change
talk, reflected in the DARN acronym. DARN
questions can help you generate open questions
that evoke change talk. Exhibit 3.8 provides
examples of open questions that elicit change talk
in preparation for taking steps to change.
Chapter 3 52
TIP 35Chapter 3—Motivational Interviewing as a Counseling Style
EXHIBIT 3.8. Examples of Open Questions to Evoke Change Talk
Using DARN
Desire “How would you like for things to change?”
“What do you hope our work together will accomplish?”
“What don’t you like about how things are now?”
“What don’t you like about the effects of drinking or drug use?”
“What do you wish for your relationship with __________?”
“How do you want your life to be different a year from now?”
“What are you looking for from this program?”
Ability “If you decided to quit drinking, how could you do it?”
“What do you think you might be able to change?”
“What ideas do you have for how you could _________?”
“What encourages you that you could change if you decided to?”
“How confident are you that you could _________ if you made up your mind?”
“Of the different options you’ve considered, what seems most possible?”
“How likely are you to be able to __________?”
Reasons “What are some of the reasons you have for making this change?”
“Why would you want to stop or cut back on your use of _____________?”
“What’s the downside of the way things are now?”
“What might be the good things about quitting _____________?”
“What would make it worthwhile for you to _____________?”
“What might be some of the advantages of _____________?”
“What might be the three best reasons for _____________?”
Need “What needs to happen?”
“How important is it for you to __________?”
“What makes you think that you might need to make a change?”
“How serious or urgent does this feel to you?”
“What do you think has to change?”
Source: Miller & Rollnick, 2013. Motivational Interviewing: Helping People Change (3rd ed.), pp. 171‒173.
Adapted with permission from Guilford Press.
Chapter 3 53

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Other strategies for evoking change talk (Miller & Rollnick, 2013) include:
•
Eliciting importance of change. Ask an open question that elicits “Need” change talk (Exhibit 3.8):
“How important is it for you to [name the change in the target behavior, such as cutting back on
drinking]?” You can also use scaling questions such as those in the Importance Ruler in Exhibit 3.9 to
help the client explore change talk about need more fully.
EXHIBIT 3.9. The Importance Ruler
Not Important Extremely Important
•
Initial question: “On a scale of 0 to 10, how important is it for you to change [name the target
behavior, like how much the client drinks] if you decided to?”
•
Follow-up question 1: “How are you at a [fill in the number on the scale] instead of a [choose a lower
number on the scale]?” When you use a lower number, you are inviting the client to reflect on how he
or she is already considering change. If you use a higher number, it will likely evoke sustain talk (Miller
& Rollnick, 2013). Notice the difference in the following examples:
Lower number
- Counselor: You mention that you are at a 6 on the importance of quitting drinking. How are you at
a 6 instead of a 3?
- Client: I’m realizing that drinking causes more problems in my life now than when I was younger.
Higher number
- Counselor: You mention that you are at a 6 on the importance of quitting drinking. How are you at
a 6 instead of a 9?
- Client: Well, I am just not ready to quit right this second.
In the higher number example, the counselor evokes sustain talk, but it is still useful information and
can be the beginning of a deep conversation about the client’s readiness to change.
•
Follow-up question 2: “What would help move from a [fll in the number on the scale] to a [choose a
slightly higher number on the scale]?” This question invites the client to reflect on reasons to increase
readiness to change.
•
Exploring extremes. Ask the client to identify
the extremes of the problem; this enhances his
or her motivation. For example: “What concerns
you the most about [name the target behavior,
like using cocaine]?”
•
Looking back. To point out discrepancies and
evoke change talk, ask the client about what
it was like before experiencing substance use
problems, and compare that response with what
it is like now. For example: “What was it like
before you started using heroin?”
•
Looking forward. Ask the client to envision
what he or she would like for the future. This
can elicit change talk and identify goals to
work toward. For example: “If you decided to
[describe the change in target behavior, such as
quit smoking], how do you think your life would
be different a month, a year, or 5 years from
now?”
Chapter 3 54

TIP 35
Chapter 3—Motivational Interviewing as a Counseling Style
Reinforce change talk by reflecting it back verbally,
nodding, or making approving facial expressions
and affirming statements. Encourage the client to
continue exploring the possibility of change by
asking for elaboration, explicit examples, or details
about remaining concerns. Questions that begin
with “What else” effectively invite elaboration.
Your task is to evoke change talk and selectively
reinforce it via reflective listening. The amount
of change talk versus sustain talk is linked to
client behavior change and positive substance
use outcomes (Houck et al., 2018; Lindqvist et al.,
2017; Magill et al., 2014).
Responding to change talk and sustain talk
Your focus should be on evoking change talk and
minimizing sustain talk. Sustain talk expresses the
side of ambivalence that favors continuing one’s
pattern of substance use. Don’t argue with the
client’s sustain talk, and don’t try to persuade the
client to take the change side of ambivalence.
There are many ways to respond to sustain talk
that acknowledge it without getting stuck in it.
You can use (Miller & Rollnick, 2013):
•
Simple reflections. Acknowledge sustain talk
with a simple reflective listening response.
This validates what the client has said and
sometimes elicits change talk. Give the client an
opportunity to respond before moving on.
- Client: I don’t plan to quit drinking
anytimesoon.
- Counselor: You don’t think that abstinence
would work for you right now.
•
Amplified reflections. Accurately reflect the
client’s statement but with emphasis (and
without sarcasm). An amplified reflection
overstates the client’s point of view, which
can nudge the client to take the other side of
ambivalence (i.e., change talk).
- Client: But I can’t quit smoking pot. All my
friends smoke pot.
- Counselor: So you really can’t quit because
you’d be too different from your friends.
•
Double-sided reflections. A double-sided
reflection acknowledges sustain talk, then
pairs it with change talk either in the same
client statement or in a previous statement.
It acknowledges the client’s ambivalence yet
selectively reinforces change talk. Use “and” to
join the two statements and make change talk
the second statement (see Counselor Response
in Exhibit 3.6).
- Client: I know I should quit smoking now that
I am pregnant. But I tried to go cold turkey
before, and it was just too hard.
- Counselor: You’re worried that you won’t be
able to quit all at once, and you want your
baby to be born healthy.
•
Agreements with a twist. A subtle strategy is
to agree, but with a slight twist or change of
direction that moves the discussion forward.
The twist should be said without emphasis
orsarcasm.
- Client: I can’t imagine what I would do if I
stopped drinking. It’s part of who I am. How
could I go to the bar and hang out with
myfriends?
- Counselor: You just wouldn’t be you without
drinking. You have to keep drinking no
matter how it effects your health.
•
Reframing. Reframing acknowledges the
client’s experience yet suggests alternative
meanings. It invites the client to consider a
different perspective (Barnett, Spruijt-Metz, et
al., 2014). Reframing is also a way to refocus the
conversation from emphasizing sustain talk to
eliciting change talk (Barnett, Spruijt-Metz, et
al., 2014).
- Client: My husband always nags me about
my drinking and calls me an alcoholic. It
bugs me.
- Counselor: Although your husband expresses
it in a way that frustrates you, he really cares
and is concerned about the drinking.
Chapter 3 55

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
• A shift in focus. Defuse discord and tension by
shifting the conversational focus.
- Client: The way you’re talking, you think I’m
an alcoholic, don’t you?
- Counselor: Labels aren’t important to me.
What I care about is how to best help you.
• Emphasis on personal autonomy. Emphasizing
that people have choices (even if all the choices
have a downside) reinforces personal autonomy
and opens up the possibility for clients to choose
change instead of the status quo. When you
make these statements, remember to use a
neutral, nonjudgmental tone, without sarcasm. A
dismissive tone can evoke strong reactions from
the client.
- Client: I am really not interested in giving up
drinking completely.
- Counselor: It’s really up to you. No one can
make that decision for you.
All of these strategies have one thing in
common: They are delivered in the spirit of MI.
Developing discrepancy: A values
conversation
Developing discrepancy has been a key element
of MI since its inception. It was originally one of
the four principles of MI. In the current version,
exploring the discrepancy between clients’ values
and their substance use behavior has been folded
into the evoking process. When clients recognize
discrepancies in their values, goals, and hopes for
the future, their motivation to change increases.
Your task is to help clients focus on how their
behavior conflicts with their values and goals.
The focus is on intrinsic motivation. MI doesn’t
work if you focus only on how clients’ substance
use behavior is in conflict with external pressure
(e.g., family, an employer, the court) (Miller &
Rollnick, 2013).
To facilitate discrepancy, have a values conversation
to explore what is important to the client (e.g.,
good heath, positive relationships with family,
being a responsible member of the community,
preventing another hospitalization, staying out
of jail), then highlight the conflict the client feels
between his or her substance use behaviors and
those values. Client experience of discrepancy
between values and substance use behavior is
related to better client outcomes (Apodaca &
Longabaugh, 2009).
This process can raise uncomfortable feelings
like guilt or shame. Frame the conversation
by conveying acceptance, compassion, and
affirmation. The paradox of acceptance is that
it helps people tolerate more discrepancy and,
instead of avoiding that tension, propels them
toward change (Miller & Rollnick, 2013). However,
too much discrepancy may overwhelm the client
and cause him or her to think change is not
possible (Miller & Rollnick, 2013).
To help a client perceive discrepancy, you can
use what is sometimes termed the “Columbo
approach.” Initially developed by Kanfer & Schefft
(1988), this approach remains a staple of MI and
is particularly useful with a client who is in the
Chapter 3 56

TIP 35Chapter 3—Motivational Interviewing as a Counseling Style
Precontemplation stage and needs to be in charge clarification of the client’s problem but appears
of the conversation. Essentially, the counselor unable to perceive any solution.
expresses understanding and continuously seeks
EXPERT COMMENT: THE COLUMBO APPROACH
Sometimes I use what I refer to as the Columbo approach to develop discrepancy with clients. In the
old Columbo television series, Peter Falk played a detective named Columbo who had a sense of what
had really occurred but used a somewhat bumbling, unassuming, Socratic style of querying his prime
suspect, strategically posing questions and making reflections to piece together a picture of what really
happened. As the pieces began to fall into place, the object of Columbo’s investigation would often reveal
the real story.
The counselor plays the role of a detective who is trying to solve a mystery but is having a difficult time
because the clues don’t add up. The “Columbo counselor” engages the client in solving the mystery:
Example #1: “Hmm. Help me figure this out. You’ve told me that keeping custody of your daughter
and being a good parent are the most important things to you now. How does your heroin use fit in
withthat?”
Example #2: “So, sometimes when you drink during the week, you can’t get out of bed to get to work.
Last month, you missed 5 days. But you enjoy your work, and doing well in your job is very important
toyou.”
In both cases, the counselor expresses confusion, which allows the client to take over and explain how
these conflicting desires fit together.
The value of the Columbo approach is that it forces the client, rather than the counselor, to grapple with
discrepancies and attempt to resolve them. This approach reinforces the notion that the client is the
expert on his or her behavior and values. The client is truly the only one who can resolve the discrepancy.
If the counselor attempts to do this instead of the client, the counselor risks making the wrong
interpretation, rushing to the client to conclusions rather than listening to the client’s perspective, and,
perhaps most important, making the client a passive rather than an active participant in the process.
Cheryl Grills, Ph.D., Consensus Panel Member
Chapter 3 57

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
In addition to providing personalized feedback
(as discussed in Chapter 2), you can facilitate
discrepancy by (Miller & Rollnick, 2013):
•
Identifying personal values. For clients to
feel discrepancy between their values and
actions, they need to recognize what those
values are. Some clients may have only a vague
understanding of their values or goals. A tool to
help you and clients explore values is the Values
Card Sort.
- Print different values like “Achievement—to
have important accomplishments” (Miller &
Rollnick, 2013, p. 80) on individual cards.
- Invite clients to sort the cards into piles by
importance; those that are most important
are place in one pile, and those that are least
important are in another pile.
- Ask clients to pick up to 10 cards from
the most important pile; converse about
eachone.
- Use OARS to facilitate the conversations.
- Pay attention to statements about
discrepancy between these important values
and clients’ substance use behaviors, and
reinforce these statements.
- A downloadable, public domain version of
the Value Card Sort activity is available online
(www.motivationalinterviewing.org/sites/
default/files/valuescardsort_0.pdf).
•
Providing information. Avoid being the expert
and treating clients as passive recipients
when giving information about the negative
physical, emotional, mental, social, or spiritual
effects or consequences of substance misuse.
Instead, engage the client in a process of
mutual exchange. This process is called Elicit-
Provide-Elicit (EPE) and has three steps (Miller &
Rollnick, 2013):
- Elicit readiness or interest in the
information. Don’t assume that clients are
interested in hearing the information you
want to offer; start by asking permission. For
example: “Would it be okay if I shared some
information with you about the health risks of
using heroin?” Don’t assume that clients lack
this knowledge. Ask what they already know
about the risks of using heroin. For example:
“What would you most like to know about
the health risks of heroin use?”
- Provide information neutrally (i.e., without
judgement). Prioritize what clients have
said they would most like to know. Fill in
knowledge gaps. Present the information
clearly and in small chunks. Too much
information can overwhelm clients. Invite
them to ask more questions about the
information you’re providing.
- Elicit clients’ understanding of the
information. Don’t assume that you know
how clients will react to the information you
have provided. Ask questions:
•
“So, what do you make of
thisinformation?”
•
“What do you think about that?"
•
“How does this information impact
the way you might be thinking about
[name the substance use behavior, such
asdrinking]?"
- Allow clients plenty of time to consider and
reflect on the information you presented.
Invite them to ask questions for clarification.
Follow clients’ responses to your open
questions with reflective listening statements
that emphasize change talk whenever you
hear it. EPE is an MI strategy to facilitate
identifying discrepancy and is an effective
and respectful way to give advice to clients
about behavior change strategies during
the planning process.
Chapter 3 58

TIP 35
Chapter 3—Motivational Interviewing as a Counseling Style
•
Exploring others’ concerns. Another way to
build discrepancy is to explore the clients’
understanding of the concerns other people
have expressed about their substance use. This
differs from focusing on the external pressure
that a family member, an employer, or the
criminal justice system may be putting on clients
to reduce or abstain from substance use. The
purpose is to invite clients to explore the impact
of substance use behaviors on the people with
whom they are emotionally connected in a
nonthreatening way. Approach this conversation
from a place of genuine curiosity and even a
bit of confusion (Miller & Rollnick, 2013). Here
is a brief example of what this conversation
might look like using an open question about
a significant other’s concern, where reflecting
sustain talk actually has the effect of eliciting
change talk:
- Counselor: You mentioned that your husband
is concerned about your drinking. What do
you think concerns him? (Open question)
- Client: He worries about everything. The
other day, he got really upset because I
drove a block home from a friend’s house
after a party. He shouldn’t worry so much.
(Sustain talk)
- Counselor: He’s worried that you could
crash and hurt yourself or someone else or
get arrested for driving under the influence.
But you think his concern is overblown.
(Complex reflection)
- Client: I can see he may have a point. I really
shouldn’t drive after drinking. (Change talk)
Evoking hope and condence to support
self-ecacy
Many clients do not have a well-developed sense
of self-efficacy. They find it hard to believe that
they can begin or maintain behavior change.
Improving self-efficacy requires eliciting
confidence, hope, and optimism that change, in
general, is possible and that clients, specifically,
can change. This positive impact on self-efficacy
may be one of the ways MI promotes behavior
change (Chariyeva et al., 2013).
One of the most consistent predictors of positive
client behavior change is “ability” change talk
(Romano & Peters, 2016). Unless a client believes
change is possible, the perceived discrepancy
between desire for change and feelings of
hopelessness about accomplishing change is likely
to result in continued sustain talk and no change.
When clients express confidence in their ability to
change, they are more likely to engage in behavior
change (Romano & Peters, 2016).
COUNSELOR NOTE: SELF
EFFICACY
Self-efficacy is a person’s confidence in his
or her ability to change a behavior (Miller &
Rollnick, 2013), such as a behavior that risks one’s
health. Research has found that MI is effective
in enhancing a client’s self-efficacy and positive
outcomes including treatment completion,
lower substance use at the end of treatment,
greater desire to quit cannabis use, and
reductions in risky sexual behavior for someone
with HIV (Caviness et al., 2013; Chariyeva et al.,
2013; Dufett, & Ward, 2015; Moore, Flamez,, &
Szirony, 2017).
Because self-efficacy is a critical component of
behavior change, it is crucial that you also believe
in clients’ capacity to reach their goals. You can
help clients strengthen hope and confidence
in MI by evoking confidence talk. Here are two
strategies for evoking confidence talk (Miller &
Rollnick,2013):
•
Use the Confidence Ruler (Exhibit 3.10) and
scaling questions to assess clients’ confidence
level and evoke confidence talk.
Chapter 3 59

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
EXHIBIT 3.10. The Confidence Ruler
Not Confident Extremely Confident
•
Initial question: “On a scale of 0 to 10, how confident are you that you could change [name the target
behavior, like stop drinking] if you decided to?”
•
Follow-up questions:
- “How are you at a [fill in the number on the scale] instead of a [choose a lower number on the
scale]?” Using a lower number helps clients reflect on how far they’ve come on the confidence
scale. Using a higher number with this question may discourage clients, which can elicit sustain
talk. If that should happen, use strategies discussed previously for responding to sustain talk.
- “What would help you get from a [fill in the number on the scale] to a [choose a slightly
higher number on the scale]?” This open question invites clients to reflect on strategies to
build confidence. Don’t jump to a much higher number, which can overwhelm clients and
lowerconfidence.
Whatever the client’s response to these scaling questions, use it as an opportunity to begin a
conversation about his or her confidence or perceived ability to move forward in the change process.
•
Ask open questions that evoke client strengths
and abilities. Follow the open questions
with reflective listening responses. Here are
some examples of open questions that elicit
confidence talk:
- “Knowing yourself as well as you do, how
do you think you could [name the target
behavior change, like cutting back on
smoking marijuana]?”
- “How have you made difficult changes in
thepast?”
- “How could you apply what you learned then
to this situation?”
- “What gives you confidence that you could
[name the target behavior change, like
stopping cocaine use]?”
In addition, you can help enhance clients’ hope
and confidence about change by:
•
Exploring clients’ strengths and brainstorming
how to apply those strengths to the
currentsituation.
•
Giving information via EPE about the efficacy
of treatment to increase clients’ sense of
self-efficacy.
•
Discussing what worked and didn’t work in
previous treatment episodes and offering
change options based on what worked before.
•
Describing how people in similar situations
have successfully changed their behavior. Other
clients in treatment can serve as role models and
offer encouragement.
•
Offering some cognitive tools, like the AA
slogan “One day at a time” or “Keep it simple”
to break down an overwhelming task into
smaller changes that may be more manageable.
•
Educating clients about the biology of addiction
and the medical effects of substance use to
alleviate shame and instill hope that recovery
ispossible.
Chapter 3 60

TIP 35
Chapter 3—Motivational Interviewing as a Counseling Style
Engaging, focusing, and evoking set the stage
for mobilizing action to change. During these MI
processes, your task is to evoke DARN change talk.
This moves the client along toward taking action to
change substance use behaviors. At this point, your
task is to evoke and respond to CAT change talk.
Recognizing signs of readiness to change
As you evoke and respond to DARN change talk,
you will begin to observe these signs of readiness
to change in the client’s statements (Miller &
Rollnick, 2013):
•
Increased change talk: As DARN change talk
increases, commitment and activation change
talk begin to be expressed. The client may
show optimism about change and an intention
tochange.
•
Decreased sustain talk: As change talk
increases, sustain talk decreases. When change
talk overtakes sustain talk, it is a sign that the
client is moving toward change.
•
Resolve: The client seems more relaxed.
The client talks less about the problem, and
sometimes expresses a sense of resolution.
•
Questions about change: The client asks what
to do about the problem, how people change if
they want to, and so forth. For example: “What
do people do to get off pain pills?”
•
Envisioning: The client begins to talk about life
after a change, anticipate difficulties, or discuss
the advantages of change. Envisioning requires
imagining something different—not necessarily
how to get to that something different, but
simply imagining how things could be different.
•
Taking steps: The client begins to experiment
with small steps toward change (e.g., going to
an AA meeting, going without drinking for a few
days, reading a self-help book). Affirming small
change steps helps the client build self-efficacy
and confidence.
When you notice these signs of readiness to
change, it is a good time to offer the client a
recapitulation summary in which you restate his or
her change talk and minimize reflections of sustain
talk. The recapitulation summary is a good way
to transition into asking key questions (Miller &
Rollnick, 2013).
Asking key questions
To help a client move from preparing to
mobilizing for change, ask key questions (Miller &
Rollnick, 2013):
•
“What do you think you will do about your
drinking?”
•
“After reviewing the situation, what’s the next
step for you?”
•
“What do you want to do about your drug use?”
•
“What can you do about your smoking?”
•
“Where do you go from here?”
•
“What you might do next?”
When the client responds with change talk (e.g.,
“I intend to stop using heroin”), you can move
forward to the planning process. If the client
responds with sustain talk (e.g., “It would be too
hard for me to quit using heroin right now”), you
should go back to the evoking process. Remember
that change is not a linear process for most people.
Do not jump into the planning process if the
client expresses enough sustain talk to indicate
not being ready to take the next step. The
ambivalence about taking the next step may be
uncertainty about giving up the substance use
behavior or a lack of confidence about being able
to make the change.
Planning
Your task in the process is to help the client
develop a change plan that is acceptable,
accessible, and appropriate. Once a client decides
to change a substance use behavior, he or she
may already have ideas about how to make that
change. For example, a client may have previously
stopped smoking cannabis and already knows what
worked in the past. Your task is to simply reinforce
the client’s plan.
Don’t assume that all clients need a structured
method to develop a change plan. Many people
can make significant lifestyle changes and initiate
recovery from SUDs without formal assistance
(Kelly, Bergman, Hoeppner, Vilsaint, & White,
2017). For clients who need help developing
a change plan, remember to continue using
MI techniques and OARS to move the process
Chapter 3 61

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
from why change and what to change to how to
change (Miller & Rollnick, 2013). A change plan is
like a treatment plan but broader (e.g., going to
an addiction treatment program may be part of a
change plan), and the client, rather than you or the
treatment program, is the driver of the planning
process (Miller & Rollnick, 2013).
Identifying a change goal
Part of planning is working with the client to
identify or clarify a change goal. At this point,
the client may have identified a change goal. For
example, when you ask a key question such as
“What do you want to do about the drinking?” the
client might say, “I want to cut back to two drinks a
day on weekends.” In this situation, the focus shifts
to developing a plan with specific steps the client
might take to reach the change goal. If the client is
vague about a change goal and says, “I really need
to do something about my drinking,” the first step
is to help the client clarify the change goal.
Here is an example of a dialog that helps the client
get more specific:
•
Counselor: You are committed to making some
changes to your drinking. (Reflection) What
would that look like? (Open question)
•
Client: Well, I tried to cut back to one drink a
day, but all I could think about was going to the
bar and getting drunk. I cut back for 2 days but
did end up back at the bar, and then it just got
worse from there. At this point, I don’t think I
can just cut back.
•
Counselor: You made a good-faith effort to
control the drinking and learned a lot from that
experiment. (Affirmation) You now think that
cutting back is probably not a good strategy for
you. (Reflection)
•
Client: Yeah. It’s time to quit. But I’m not sure I
can do that on my own.
•
Counselor: You’re ready to quit drinking
completely and realize that you could
use some help with making that kind of
change.(Reflection)
•
Client: Yeah. It’s time to give it up.
•
Counselor: Let’s review the conversation,
(Summarization) and then talk about next steps.
The counselor uses OARS to help the client clarify
the change goal. The counselor also hears that the
client lacks confidence that he or she can achieve
the change goal and reinforces the client’s desire
for some help in making the change. The next step
with this client is to develop a change plan.
Developing a change plan
Begin with the change goal identified by the
client; then, explore specific steps the client
can take to achieve it. In the planning process,
use OARS and pay attention to CAT change
talk. As you proceed, carefully note the shift
from change talk that is more general to change
talk that is specific to the change plan (Miller &
Rollnick, 2013). (See Chapter 6 for information on a
developing a change plan.) Some evidence shows
that change talk is related to the completion of a
change plan (Roman & Peters, 2016).
Here are some strategies for helping clients
develop a change plan (Miller & Rollnick, 2013):
•
Confirm the change goal. Make sure that
you and the client agree on what substance
use behavior the client wants to change and
what the ultimate goal is (i.e., to cut back or to
abstain). This goal might change as the client
takes steps to achieve it. For example, a client
who tries to cut back on cannabis use may
find that that it is not a workable plan and may
decide to abstain completely.
•
Elicit the client’s ideas about how to change.
There may be many different pathways to
achieve the desired goal. For example, a client
whose goal is to stop drinking may go to AA or
SMART Recovery meetings for support, get a
prescription for naltrexone (a medication that
reduces craving and the pleasurable effects
of alcohol [Substance Abuse and Mental
Health Services Administration & National
Institute on Alcohol Abuse and Alcoholism,
2015]) from a primary care provider, enter an
intensive outpatient treatment program, or
try some combination of these. Before you
jump in with your ideas, elicit the client’s ideas
about strategies to make the change. Explore
pros and cons of the client’s ideas; determine
which appeals to the client most and is most
appropriate for this client.
Chapter 3 62

TIP 35
Chapter 3—Motivational Interviewing as a Counseling Style
•
Offer a menu of options. Use the EPE process
(see the section “Developing discrepancy: A
values conversation” above) to ask permission
to offer suggestions about accessible treatment
options, provide information about those
options, and elicit the client’s understanding of
options and which ones seem acceptable.
•
Summarize the change plan. Once you and
the client have a clear plan, summarize the plan
and the specific steps or pathways the client
has identified. Listen for CAT change talk, and
reinforce it through reflective listening.
•
Explore obstacles. Once the client applies
the change plan to his or her life, there will
inevitably be setbacks. Try to anticipate
potential obstacles and how the client might
respond to them before the client takes steps
to implement the plan. Then reevaluate the
change plan, and help the client tweak it using
the information about what did and didn’t work
from prior attempts.
Strengthening Commitment to Change
The planning process is just the beginning of
change. Clients must commit to the plan and
show that commitment by taking action. There is
some evidence that client commitment change
talk is associated with positive AUD outcomes
(Romano & Peters, 2016). One study found that
counselor efforts to elicit client commitment to
change alcohol use is associated with reduced
alcohol consumption and increased abstinence for
clients in outpatient treatment (Magill, Stout, &
Apodoaca, 2013).
Usually, people express an intention to make a
change before they make a firm commitment to
taking action. You can evoke the client’s intention
to take action by asking open questions: “What
are you willing to do this week?” or “What specific
steps of the change plan are you ready to take?”
(Miller & Rollnick, 2013). Remember that the client
may have an end goal (e.g., to quit drinking) and
intermediate action steps to achieving that goal
(e.g., filling a naltrexone prescription, going to an
AA meeting).
Once the client has expressed an intention to
change, elicit commitment change talk. Try asking
an open question that invites the client to explore
his or her commitment more clearly: “What
would help you strengthen your commitment to
__________________ [name the step or ultimate
goal for change, for example, getting that
prescription from your doctor for naltrexone]?”
(Miller & Rollnick, 2013).
Other strategies to strengthen commitment to
action steps and change goals include (Miller &
Rollnick, 2013):
•
Exploring any ambivalence clients have
about change goals or specific elements of
changeplans.
•
Reinforcing CAT change talk through
reflectivelistening.
•
Inviting clients to state their commitment to
their significant others.
•
Asking clients to self-monitor by recording
progress toward change goals (e.g., with a
drinking log).
•
Exploring, with clients’ consent, whether
supportive significant others can help with
medication adherence or other activities
that reinforce commitment (e.g., getting to
AAmeetings).
The change plan process lends itself to using
other counseling methods like CBT and MET.
For example, you can encourage clients to
monitor their thoughts and feelings in high-risk
situations where they are more likely to return to
substance use or misuse. Chapter 7 provides more
information on relapse prevention. No matter
what counseling strategies you use, keep to the
spirit of MI by working with clients and honoring
and respecting their right to and capacity for
self-direction.
Benets of MI in Treating SUDs
The number of research studies on MI has doubled
about every 3 years from 1999 to 2013 (Miller &
Rollnick, 2013). Many studies were randomized
clinical trials reflecting a range of clinical
populations, types of problems, provider settings,
types of SUDs, and co-occurring substance use
and mental disorders (Smedslund et al., 2011).
Although some studies report mixed results, the
overall scientific evidence suggests that MI is
Chapter 3 63

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
associated with small to strong (and significant)
effects for positive substance use behavioral
outcomes compared with no treatment. MI is
as effective as other counseling approaches
(DiClemente et al., 2017). A research review
found strong, significant support for MI and
combined MI/MET in client outcomes for alcohol,
tobacco, and cannabis and some support for its
use in treating cocaine and combined illicit drug
use disorders (DiClemente et al., 2017). Positive
outcomes included reduced alcohol, tobacco, and
cannabis use; fewer alcohol-related problems;
and improved client engagement and retention
(DiClemente et al., 2017). MI and combined MI/
MET were effective with adolescents, young adults,
college students, adults, and pregnant women.
•
Broad dissemination. MI has been
disseminated throughout the United States
andinternationally.
Counselor adherence to MI skills is important
for producing client outcomes (Apodaca et al.,
2016; Magill et al., 2013). For instance, using
open questions, simple and complex reflective
listening responses, and affirmations is associated
with change talk (Apodaca et al., 2016; Romano
& Peters, 2016). Open questions and reflective
listening responses can elicit sustain talk when
counselors explore ambivalence with clients
(Apodaca et al., 2016). However, growing evidence
suggests that the amount and strength of client
change talk versus sustain talk in counseling
sessions are key components of MI associated with
behavior change (Gaume et al., 2016; Houck et al.,
2018; Lindqvist et al., 2017; Magill et al., 2014).
Other benefits of MI include (Miller &
Rollnick,2013):
•
Cost effectiveness. MI can be delivered in
brief interventions like SBIRT (screening, brief
intervention, and referral to treatment) and
FRAMES (Feedback, Responsibility, Advice,
Menu of options, Empathy, and Self-efficacy,
see Chapter 2), which makes it cost effective.
In addition, including significant others in MI
interventions is also cost effective (Shepard et
al., 2016).
•
Ease of use. MI has been adapted and
integrated into many settings, including
primary care facilities, emergency departments,
behavioral health centers, and criminal justice
and social service agencies. It is useful anywhere
that focuses on helping people manage
substance misuse and SUDs.
•
Applicability to diverse health and behavioral
health problems. Beyond substance use
behaviors, MI has demonstrated benefits across
a wide range of behavior change goals.
•
Effectiveness. Positive effects from MI
counseling occur across a range of real-life
clinical settings.
•
Ability to complement other treatment
approaches. MI fits well with other counseling
approaches, such as CBT. It can enhance client
motivation to engage in specialized addiction
treatment services and stay in and adhere
totreatment.
•
Ease of adoption by a range of providers.
MI can be implemented by primary care
and behavioral health professionals, peer
providers, criminal justice personnel, and various
other professionals.
•
Role in mobilizing client resources. MI is based
on person-centered counseling principles. It
focuses on mobilizing the client’s own resources
for change. It is consistent with the healthcare
model of helping people learn to self-manage
chronic illnesses like diabetes and heart disease.
Conclusion
MI is a directed, person-centered counseling
style that is effective in helping clients change
their substance use behaviors. When delivered
in the spirit of MI, the core skills of asking open
questions, affirming, using reflective listening,
and summarizing enhance client motivation
and readiness to change. Counselor empathy,
shown through reflective listening and evoking
change talk, is another important element of MI’s
effectiveness and is associated with positive client
outcomes. MI has been adapted for use in brief
interventions and across a wide range of clinical
settings and client populations. It is compatible
with other counseling models and theories of
change, including CBT and the SOC.
Chapter 3 64

Chapter 4—From Precontemplation to
Contemplation: Building Readiness
The task for individuals in Precontemplation is to become conscious of and
concerned about the current pattern of behavior and/or interested in a new
behavior. From a change perspective, it is more important to recognize an
individual’s current views on change and address her or his reasons for not
wanting to change than it is to understand how the status quo came to be.”
—DiClemente, 2018, p. 29
KEY MESSAGES
TIP 35
ENHANCING MOTIVATION FOR CHANGE IN
SUBSTANCE USE DISORDER TREATMENT
•
In the Precontemplation stage, clients do
not recognize that they have a problem with
substance use or they recognize the problem
but are not ready to change their substance
use behaviors.
• Counselors should be nonjudgmental about
clients’ low motivation to change and instead
focus on building a strong working alliance.
• A key strategy to helping clients move from
the Precontemplation stage to contemplating
change is to raise their level of concern and
awareness of the risk associated with their
current substance use behaviors.
• Involving family members and significant
others (SOs) can increase clients’ concern
about substance use.
Chapter 4 discusses strategies you can use to
help clients raise doubt and concern about
their substance use and related health, social,
emotional, mental, financial, and legal problems.
It highlights areas of focus and key counseling
strategies that will help clients move from the
Precontemplation stage to Contemplation. This
chapter also addresses issues that may arise for
clients mandated to treatment.
In the Stages of Change (SOC) model, clients who
are unconcerned about their current substance
use or may be concerned but aren’t considering
change are in Precontemplation. They may remain
there or in the early Contemplation stage for years,
rarely or possibly never thinking about change.
You can take advantage of many opportunities
and scenarios to help someone who is misusing
substances start on a journey toward change—to
move from Precontemplation to Contemplation.
A client in Precontemplation is often moved to
enter the cycle of change by extrinsic sources of
motivation. The following situations might lead a
person who is misusing a substance to treatment:
•
A college coach refers an athlete for treatment
after he tests positive for cocaine use.
•
A wife worries about her husband’s drinking
and insists she’ll file for divorce unless he
getstreatment.
•
A tenant is displaced from a federal housing
project because of his substance use.
•
A driver is referred for treatment by the court
for driving while intoxicated.
•
A woman tests positive for substances during a
prenatal visit to a public health clinic.
•
An employer sends an employee whose job
performance has declined to the company’s
employee assistance program, and the
employee is subsequently referred for substance
use treatment.
•
A physician in an emergency department treats
a driver involved in a serious automobile crash
and discovers alcohol in his system.
65

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
•
A family physician screens a patient for alcohol
use disorder (AUD) and suggests treatment
based on the patient’s high score on the Alcohol
Use Disorders Identification Test.
•
A mother whose children were taken into
custody by Child Protective Services because
of neglect learns that she cannot get them
back until she stops using substances and
seekstreatment.
In each situation, someone with an important
relationship to the person misusing substances
stated his or her concerns about the person’s
substance misuse and its negative effects. The
response to these concerns depends, in part,
on the person’s perception of the circumstances
as well as the way feedback about substance
misuse is presented. An individual will be better
motivated to abstain from or moderate his or her
substance use if these concerned others offer
relevant information in a supportive and empathic
manner rather than in a judgmental, dismissive, or
confrontational way.
Exhibit 4.1 presents counseling strategies for
Precontemplation.
EXHIBIT 4.1. Counseling Strategies for Precontemplation
CLIENT MOTIVATION COUNSELOR FOCUS COUNSELING STRATEGIES
•
The client is not
•
Develop rapport and build
•
Elicit the client’s perceptions of the problem.
concerned about trust to establish a strong
•
Explore the events that led to
substance use or counseling alliance.
enteringtreatment.
lacks awareness
•
Raise doubts and
•
Assess the client’s stage in the SOC and
about any problems.
concerns about the client’s
readiness to change.
•
The client is not yet
substanceuse.
•
Commend the client for coming
considering change
•
Understand special
totreatment.
or is unwilling or
motivational counseling
•
Agree on a direction.
unable to change.
•
The client is often
considerations for clients
mandated to treatment.
•
Provide information about the effects and
risks of substance misuse.
pressured by others
to seek help.
•
Evoke concern about the client’s
substance use.
•
Provide personalized feedback on
assessment findings.
•
Involve SOs in treatment to raise concern
about the client’s substance use.
•
Express concern, and leave the door open.
Develop Rapport and Build Trust
Before you raise the topic of change with people
who are not thinking about it, establish rapport
and trust. The challenge is to create a safe and
supportive environment in which clients can feel
comfortable about engaging in authentic dialog.
As clients become more engaged in counseling,
their defensiveness and reluctance to change
decreases (Prochaska, Norcross, & DiClemente,
2013). Some motivational strategies for
establishing rapport in initial conversations about
behavior change include:
•
Asking the client for permission to address the
topic of changing substance use behaviors; this
shows respect for the client’s autonomy.
•
Telling the client something about how you
or your program operates and how you and
the client could work together. State how
long sessions will last and what you expect to
accomplish both now and over a specified time.
Try not to overwhelm the new client with all the
program’s rules and regulations. Specify what
assessments or other formal arrangements will
be needed, if appropriate.
Chapter 4 66

TIP 35
Chapter 4—From Precontemplation to Contemplation: Building Readiness
•
Raising confidentiality issues up front. You
must inform the client which information will
be kept private, which can be released with
permission, and which must be sent back to a
referringagency.
•
Explaining that you will not tell the client what
to do or how and whether to change. Rather,
you will be asking the client to do most of the
talking—giving him or her perspective about
what is happening while inviting the client to
share his or her own perspective. You can also
invite comments about what the client expects
or hopes to achieve.
• Asking the client to tell you why he or she has
come to treatment, mentioning what
you know about the reasons, and asking for
the client’s version or elaboration (Miller &
Rollnick, 2013). If the client seems particularly
hesitant or defensive, one strategy is to choose a
topic of interest to the client that can be linked
to substance use. (For more information about
setting an agenda, see Chapter 3.) Such
information might be provided by the referral
source or can be learned by asking whether the
client is dealing with any stressful situations, such
as illness, marital discord, or extremely heavy
workload. This can lead naturally to questions
such as “How does your use of alcohol fit into
this?” or “How does your use of heroin affect
your health?”
• Avoiding referring to the client’s “problem” or
“substance misuse,” because this may
not reflect the client’s perspective about
substance use (Miller & Rollnick, 2013). You are
trying to understand the context in which
substances are used and the client’s readiness to
change. As mentioned previously, labels can
raise a person’s defenses.
• Aligning your counseling approach to the
client’s current stage in the SOC. For example,
move to strategies more appropriate to a later
stage in the SOC if you discover that the client is
already contemplating or committed to change.
(For more information on the later stages in the
SOC, see Chapters 5 and 6.)
COUNSELOR NOTE: AGENCY
POLICY ABOUT CLIENT
INTOXICATION
In your first session, discuss your agency’s
policy on having conversations with clients
who are intoxicated. Be transparent about
the policy and what actions you will take if the
client comes to a session intoxicated. Coming
to treatment intoxicated on alcohol or drugs
impairs ability to participate in treatment,
whether it is for an initial counseling session,
assessment, or individual or group treatment
(Miller, Forechimes, & Zweben, 2011).
Many programs administer breathalyzer tests
for alcohol or urinalysis for drugs and reschedule
counseling sessions if substances are detected
at a specified level or if a client appears to
be under the influence (Miller et al., 2011). If
you determine that a client is intoxicated, ask
the client in a nonjudgmental way to leave.
Reschedule the appointment, and help the
client get home safely (Miller et al., 2011).
Elicit the Client’s Perception of the
Problem
To engage clients, invite them to explain their
understanding of the problem. Be direct, but
remain nonjudgmental. You might say, “Can you
tell me a bit about what brings you here today?”
or “I’d like to understand your perspective on
why you’re here. Can we start there?” Asking
these open questions invites clients to tell you
their story and shows your genuine interest in
theirperspective.
Explore the Events That Led to Entering
Treatment
Explore what brought the client to treatment,
starting by recognizing his or her emotional
state. The emotional state in which the client
comes to treatment is an important part of the
context in which counseling begins. A client
referred to treatment will exhibit a range of
Chapter 4 67

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
emotions associated with the experiences that
led to counseling—for example, an arrest, a
confrontation with a spouse or employer, or a
health crisis. People may enter treatment feeling
shaken, angry, withdrawn, ashamed, terrified, or
relieved and are often experiencing a combination
of feelings. Strong emotions can become
obstacles to change if you do not acknowledge
them through reflective listening.
Your initial conversation with clients should focus
on their recent experience. For example, an
athlete is likely to be concerned about his or her
continued participation in sports, as well as athletic
performance; an employee may want to keep his or
her job; and a driver is probably worried about the
possibility of losing his or her license, going to jail,
or injuring someone. A pregnant woman wants a
healthy child; a mother may want to regain custody
of her children; and a concerned husband needs
specific guidance on encouraging his spouse to
enter treatment.
Many people with substance use problems seek
treatment in response to external pressure from
family, friends, employers, healthcare providers,
or the legal system (Connors, DiClemente,
Velasquez, & Donovan, 2013). A client sometimes
blames the referring source or someone else for
pressuring him or her into treatment and report
that the referring provider simply doesn’t view
the situation accurately. Start with these external
sources of motivation as a way to raise the
client’s awareness about the impact of his or
her substance use on others. For example, if the
client’s wife has insisted he start treatment and the
client denies any problem, you might ask, “What
kind of things seem to bother her?” or “What do
you think makes her believe there is a problem
associated with your drinking?” If the wife’s
perceptions are inconsistent with the client’s, you
might suggest that the wife come to treatment so
that you can explore their different perspectives.
Similarly, you may have to review and confirm
a referring agency’s account or the physical
evidence forwarded by a healthcare provider to
help you introduce alternative viewpoints to the
client in nonthreatening ways. If the client thinks
a probation officer is the problem, you can ask,
“Why do you think your probation officer believes
you have a problem?” This lets the client express
the problem from the perspective of the referring
party and can raise awareness. Use reflective
listening responses to let the client know you are
listening. Avoid agreeing or disagreeing with the
client’s position.
Assess the Client’s SOC and Readiness
toChange
When you first meet the client, determine his
or her readiness to change and where he or she
is in the SOC; this determines what counseling
strategies are likely to work. It is tempting to
assume that the client with obvious signs of a
substance use disorder (SUD) must already be
contemplating or ready for change. However, such
assumptions may be wrong. The new client could
be at any point on the severity continuum (from
substance misuse to severe SUD), could have few
or many associated health or social problems,
and could be at any stage of readiness to change.
The strategies you use to engage clients in initial
conversations about change should be guided
by your assessment of the client’s motivation
and readiness.
The Importance and Condence Rulers
The simplest way to assess the client’s readiness
to change is to use the Importance Ruler and
the Confidence Ruler described in Chapter 3
(see Exhibit 3.9 and Exhibit 3.10, respectively).
The Importance Ruler indicates how important
it is for the client to make a change right now.
The Confidence Ruler indicates a client’s sense
of self-efficacy about making a change right
now. Together, they indicate how ready the
client is to change target behaviors. Clients in
Precontemplation will typically be at the lower end
of the rulers, generally between 0 and 3.
Keep in mind that these numerical assessments
are neither fixed nor always linear. The client
moves forward or backward across stages or
jumps from one part of the continuum to another,
in either direction and at various times. Your role
is to facilitate movement in the direction of
positivechange.
Chapter 4 68

TIP 35Chapter 4—From Precontemplation to Contemplation: Building Readiness
Identication of the client’s style
ofPrecontemplation
ambivalence about changing substance use
behaviors. Exhibit 4.2 describes different styles
of expressions of ambivalence about change
during the Precontemplation stage (known as
the 5 Rs) and counseling strategies aligned
with these different expressions of sustain talk
duringPrecontemplation.
You should tailor your counseling approach
to the ways in which the client talks about
being in Precontemplation. Clients will present
with different expressions of sustain talk (see
Chapter 3), which is the status quo side of
EXHIBIT 4.2. Styles of Expression in the Precontemplation Stage:
The5Rs
Individuals with addictive behaviors who are not yet contemplating change usually express sustain
talk in one or more of five different ways. Identifying each client’s style of expression helps determine
the counseling approach to follow.
Reveling Clients are still focused on good experiences about substance use and
have not necessarily experienced many substance-use–related negative
consequences. Providing objective, nonjudgmental feedback about their
substance use and associated health risks or other negative consequences can
raise doubt about their ability to avoid negative effects of substance use on
their lives.
Reluctance Clients lack knowledge about the dimensions of the problem or the personal
impact it can have to think change is necessary. They often respond to
nonjudgmental feedback about how substance use is affecting their lives.
They also respond to reassurance that they will be able to function without the
addictive behavior.
Rebellion Clients are afraid of losing control over their lives and have a large investment
in their substance of choice. Your challenge is to help them make more
positive choices for themselves rather than rebel against what they view as
pressure to change. Emphasizing personal choice and responsibility can work
well with them.
Resignation Clients may feel hopeless, helpless, and overwhelmed by the energy required
to change. They probably have been in treatment many times before or have
tried repeatedly with little success to quit on their own. These clients must
regain hope and optimism about their capacity for change. Explore with
them specific barriers to change and successful change attempts with other
behaviors. Offer information about how treatment has helped many people
who thought they couldn’t change, and link them to others in recovery who
can provide additional hope and support.
Rationalization Clients think they have all the answers and that substance use may be a
problem for others but not for them. Using double-sided reflection (see
Chapter 3), rather than arguing for change, seems the most effective strategy
for clients expressing rationalizations. Acknowledge what these clients say,
but point out any reservations they may have expressed earlier about current
substance use.
Source: DiClemente, 2018.
Chapter 4 69

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Readiness assessment instruments
Use assessment tools to help determine the
client’s readiness to change and place in the
SOC. These instruments can give overall scores
that correspond to levels of readiness to change.
You may find it useful to explore client responses
to specific questions to raise awareness of his
or her substance use and what may be getting in
the way of making a change. Several assessment
tools widely used in clinical and research settings
are discussed briefly below and presented in full in
Appendix B:
•
The University of Rhode Island Change
Assessment Scale (URICA) was originally
developed to measure a client’s change stage
in psychotherapy (McConnaughy, Prochaska, &
Velicer, 1983) in terms of four stages of the SOC:
Precontemplation, Contemplation, Action, and
Maintenance. It has been adapted for addiction
treatment and is the most common way of
measuring the client’s stage of change in clinical
settings (Connors et al., 2013).
- The scale has 32 items—8 items for each
of the 4 stage-specific subscales. A client
rates items on a 5-point scale from 1 (strong
disagreement) to 5 (strong agreement). The
instrument covers a range of concerns and
asks clients general questions about the
client’s “problem.” URICA subscales have
good internal consistency and validity for
SUDs (Field, Adinoff, Harris, Ball, & Carroll,
2009).
- To use this tool, the client is asked to identify
a specific “problem” (e.g., cocaine use) and
then fills out the form keeping the specific
problem in mind. There may be more than
one “problem” for which the client is seeking
help, so you may want to have the client fill
out the instrument more than once. You can
use the URICA to track a client’s movement
through the SOC by asking the client to fill it
out periodically.
•
The Stages of Change Readiness and
Treatment Eagerness Scale (SOCRATES)
measures readiness to change. The original
SOCRATES was a 32-item questionnaire that
used a 5-point scale ranging from 5 (strongly
agree) to 1 (strongly disagree). A 19-item
version was developed for clinical use and
is a self-administered paper-and-pencil
questionnaire (Miller & Tonigan, 1996). The
SOCRATES 8A is for alcohol use, and the
SOCRATES 8D is for drug use. The items on
the short version assess the recognition of the
problem, ambivalence, and efforts to take steps.
SOCRATES provides clients with feedback
about their scores as a starting point for
discussion. Changes in scores over time can
help you learn the impact of an intervention on
problem recognition, ambivalence, and progress
on making changes.
•
The Readiness To Change Questionnaire was
developed to help healthcare providers who
are not addiction treatment specialists assess
the stage of change of clients misusing alcohol
(Rollnick, Heather, Gold, & Hall, 1992). The 12
items, which were adapted from the URICA, are
associated with 3 stages—Precontemplation,
Contemplation, and Action—and reflect typical
attitudes of clients in each readiness level.
For example, a person not yet contemplating
change would likely give a positive response
to the statement “It’s a waste of time thinking
about my drinking because I do not have a
problem,” whereas a person already taking
action would probably agree with the statement
“I am actively working on my drinking problem.”
Another individual already contemplating
change would likely agree with the item
“Sometimes I think I should quit or cut down on
my drinking.” A 5-point scale is used for rating
responses, from 5 (strongly agree) to 1 (strongly
disagree).
Commend the Client for Coming
toTreatment
Offering clients affirmations over responsible
behaviors, like entering treatment, can increase
their confidence that change is possible. Clients
referred for treatment may feel they have little
control in the process. Some will expect to be
criticized or blamed; some will expect you to cure
them; and still others will hope that counseling
can solve all their problems without too much
effort. Whatever their expectations, affirm their
Chapter 4 70

TIP 35
Chapter 4—From Precontemplation to Contemplation: Building Readiness
courage for coming to treatment by saying things
like, “It took you a lot of effort to get here. You
are determined to figure out what’s going on and
how you can change things.” For example, you
can praise a client’s decision to come to treatment
rather than risk losing custody of her child by
saying, “You must care very much about your
child.” Such affirmations are supportive and remind
clients that they are capable of making good
choices that match their values.
Agree on a Direction
In helping clients who are not yet thinking
seriously of changing, plan your strategies
carefully and work with them to find an
acceptable pathway. Some clients will agree
on one option but not on another. It may be
appropriate to give advice based on your own
experience and concern. However, always ask
permission to offer advice and make sure that
clients want to hear what you have to say.
Asking permission demonstrates respect for client
autonomy and is consistent with person-centered
counseling principles and the spirit of MI (as
discussed in Chapter 3). For example: “I’d like to
tell you about what we could do here. Would that
be all right?”
Whenever you express a different viewpoint from
that of the client, do so in a way that is supportive,
not authoritative or confrontational. The client
still has the choice of whether to accept your
advice and to agree to a plan. It is not necessary
at the beginning of the process to agree on
treatment goals; however, you can use motivational
strategies, like the agenda mapping discussed
in Chapter 3, to agree on how to proceed in the
current conversation.
Throughout the process of establishing rapport
and building trust, use the OARS (asking Open
questions, Affirming, Reflective listening, and
Summarizing) approach and person-centered
counseling principles (described in Chapter 3)
to create a sense of safety and respect for the
client, as well as a genuine interest in the client’s
perspective and well-being. Emphasizing personal
autonomy will go a long way toward showing
the client that you are not pressuring him or her
to change.
Raise Doubts and Concerns About
the Client’s Substance Use
Once you have engaged the client and developed
rapport, use the following strategies to increase
the client’s readiness to change and move closer
to Contemplation.
Provide Information About the Eects
and Risks of Substance Misuse
Psychoeducational programs can increase clients’
ambivalence about substance misuse and related
problems and move them toward contemplation
of change (Yeh, Tung, Horng, & Sung, 2017). Be
sure to:
•
Provide basic information about substance
use early in the treatment process if clients
have not been exposed to drug and alcohol
educationbefore.
•
Use the motivational strategy of Elicit-Provide-
Elicit (EPE, described in Chapter 3) to engage
clients in a joint discussion rather than lecture
them (Miller & Rollnick, 2013).
•
Ask permission, for example, “Would it be okay
to tell you a bit about the effects of ________?”
or ask them to describe what they know about
the effects or risks of the substances used.
•
Talk about what happens to any user of the
substance rather than referring just to the client.
•
State what experts have found, not what you
think happens.
•
Provide small chunks of information then elicit
the client’s understanding. For example, “What
do you make of all this?”
•
Describe the addiction process in biological
terms. Understanding facts about addiction can
increase hope as well as readiness to change.
For example, “When you first start using
substances, it provides a pleasurable sensation.
As you keep using substances, your mind begins
to believe that you need these substances in
the same way you need life-sustaining things
like food—that you need them to survive. You’re
not stronger than this process, but you can be
smarter, and you can regain your independence
from substances.”
Chapter 4 71

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
EXPERT COMMENT: LIVER TRANSPLANTATIONPRECONTEMPLATION TO
CONTEMPLATION
The client in Precontemplation can appear in surprising medical settings. It is not uncommon for me to
find myself sitting across from a client with end-stage liver disease being evaluated for a liver transplant.
From a medical perspective, the cause of the client’s liver disease appears to be alcoholic hepatitis, which
led to cirrhosis. A variety of laboratory and other information further supports a history of years of alcohol
misuse. The diagnosis of AUD is not only supported by the medical information but also is made clear
when the person’s family indicates years of alcohol misuse despite intensely negative consequences, such
as being charged with driving while intoxicated and marital stress related to the drinking. Yet, despite
what might seem to be an overwhelming amount of evidence, the client himself, for a variety of dynamic
and motivational reasons, cannot see himself as having a problem with alcohol. The client may feel guilty
that he caused his liver damage and think he doesn’t deserve this life-saving intervention. Or he may be
fearful that if he examines his alcohol use too closely and shares his history, he may not be considered
for transplantation at all. He may even have already been told that if he is actively drinking, he will not be
listed for transplantation.
It is important for me as a counselor not to be surprised or judgmental about the client not wanting to
see his problematic relationship with alcohol. The simple fact is that he has never connected his health
problems with his use of alcohol. To confront the client with the overwhelming evidence about his
problem drinking only makes him more defensive, reinforces his denial, and strengthens his feelings of
guilt and shame.
During assessment, I take every opportunity to connect with the client’s history and current situation
without excessive self-disclosure. Being particularly sensitive to what the client needs and what he fears, I
will help support the therapeutic alliance by asking him to share the positive side of his alcohol and drug
use, thus acknowledging that, from his perspective, his use serves a purpose.
In a situation such as this, it is not uncommon for me, after completing a thorough assessment, to provide
the client with a medical perspective on alcohol dependence. I will talk about changes in brain chemistry,
reward systems, issues of tolerance, genetic factors, and different chemical responses to alcohol, as
well as other biological processes that support addictive disease, depending on the client’s educational
background and medical understanding. I may go into great detail. If the client has fewer years of
education, I will compare addiction to other, more familiar diseases, such as diabetes. As the client
asks questions, he sees a new picture of addictive disease and sees himself in that picture. By tailoring
the presentation to each client and encouraging questions throughout, I provide him and his family, if
present, with important information about the biological factors supporting alcohol dependence. This
knowledge often leads to self-diagnosis.
This psychoeducational reframing gives the client a different view on his relationship with alcohol,
taking away some of the guilt and shame that was based on him thinking of the disease as a moral
failing. The very act of self-diagnosis is a movement from Precontemplation to Contemplation. It can be
accomplished by a simple cognitive reframe within the context of a thorough and caring assessment
completed in a professional, yet genuinely compassionate manner.
Jeffrey M. Georgi, M.Div., Consensus Panel Member
Chapter 4 72

TIP 35
Chapter 4—From Precontemplation to Contemplation: Building Readiness
Similarly, people who have driven under the
influence of alcohol may be surprised to learn
how few drinks are needed to meet the definition
of legal intoxication and how drinking at these
levels affects their responses. Women hoping to
have children may not understand how substances
can diminish fertility and potentially harm the
fetus even before they know they are pregnant.
Clients may not realize how alcohol interacts with
other medications they are taking for depression
orhypertension.
COUNSELOR NOTE: USE
MOTIVATIONAL LANGUAGE IN
WRITTEN MATERIALS
Remember that the effective strategies for
increasing motivation in face-to-face contacts
also apply to written language. Brochures, fliers,
educational materials, and advertisements can
help a client think differently about change.
However, judgmental language like “abuse” or
“denial” is just as off-putting in writing as it is
when spoken in counseling sessions. You should
provide all written material in plain language
with motivation in mind. If your brochure
starts with a long list of rules, the client may be
scared away rather than encouraged to begin
treatment. Review written materials from the
viewpoint of the client, and keep in mind your
role as a partner in a change process for which
the client must take ultimate responsibility.
Evoke Concern About the Client’s
Substance Use
You can help move clients from Precontemplation
to Contemplation by raising doubts about
the harmlessness of their substance use and
concerns about their substance use behaviors.
As clients move beyond the Precontemplation
stage and become aware of or acknowledge
some problems in relation to their substance use,
change becomes increasingly possible. Such clients
become more aware of conflict and feel greater
ambivalence (Miller & Rollnick, 2013).
One way to raise concern in the client is to
explore the “positive” and “less-positive”
aspects of his or her substance use. For example:
•
Start with the client’s views on possible
“benefits” of alcohol or drugs and move to
less-beneficial aspects rather than simply ask
about bad things or problems associated with
substance use.
•
Do not focus only on negative aspects of
substance use because the client could end up
defending his or her substance use while you
push for unwanted change.
•
Avoid spending too much time exploring the
“good” things about substance use that may
reinforce sustain talk. Higher levels of client
sustain talk is associated with lower motivation
to change and negative treatment outcomes
(Lindqvist, Forsberg, Enebrink, Andersson, &
Rosendahl, 2017; Magill et al., 2014).
•
Be aware that the client may not be ready to
accept he or she has experienced any harmful
effects of substance use. By showing that you
understand why the client “values” alcohol or
drug experiences, you help the client become
more open to accepting possible problems. For
example, you might ask, “Help me understand
what you like about your drinking. What do
you enjoy about it?” Then ask, “What do
you like less about drinking?” The client who
cannot recognize any things that he or she
“likes less” about substance use is probably
not ready to consider change and may need
moreinformation.
•
After this exploration, summarize the
interchange in personal language so that the
client can clearly hear any ambivalence that
isdeveloping.
As mentioned in Chapter 3, you can use
double-sided reflections to respond to client
ambivalence and sustain talk (Miller & Rollnick,
2013). For example, you can say, “So, drinking
helps you relax. Yet, you say you sometimes resent
all the money you are spending, and it’s hard for
you to get to work on time, especially Monday
mornings.” Chapter 5 provides additional guidance
on working with ambivalence.
Chapter 4 73

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
You can also move clients toward the
Contemplation stage by having them consider
the many ways in which substance use can affect
life experiences. For example, you might ask,
“How is your substance use affecting your studies?
How is your drinking affecting your family life?”
As you explore the effects of substance use in the
individual’s life, use balanced reflective listening:
“Help me understand. You’ve been saying you see
no need to change, and you are concerned about
losing your family. I don’t see how this fits together.
I’m wondering if this is confusing for you, too.”
Provide Personalized Feedback on
Assessment Findings
Another effective strategy for raising doubt and
concern is to provide clients with personalized
feedback about assessment findings. As
mentioned in Chapter 2, giving personalized
feedback about clients’ substance use is effective
(Davis, Houck, Rowell, Benson, & Smith, 2015;
DiClemente, Corno, Graydon, Wiprovnick, &
Knoblach, 2017; Field et al., 2014; Kahler et al.,
2018; McDevitt-Murphy et al.; 2014; Miller et al.,
2013; Walker et al., 2017). In brief interventions,
the feedback is usually short and focused on
screening results. In specialty addiction treatment
settings, feedback can focus on results of a
comprehensive assessment, which often includes:
•
Substance use patterns and history.
•
Diagnostic and Statistical Manual of Mental
Disorders, Fifth Edition, diagnostic criteria
for SUDs.
•
General functioning and links between
substance use and lowered functioning.
•
Health and biomedical effects including sleep
disorders, HIV, and diabetes.
•
Neuropsychological effects of long-term
substance use.
•
Family history of mental disorders and
SUDs, which put clients at risk for SUDs
and co-occurring substance use and mental
disorders(CODs).
•
CODs and effects of substance use on
mentalillness.
•
Functional analysis of substance use triggers.
Provide clients with personalized feedback on
the risks associated with their own substance
use and how their consumption compares with
others of the same culture, age, or gender.
When clients hear about assessment results and
understand the risks and consequences, many
recognize the gap between where they are and
where their values lie.
To make findings from an assessment a useful
part of the counseling process, make sure the
client understands the value of such information
and believes the results will be helpful. If
possible, schedule formal assessments after the
client has had at least one session with you or use a
motivational interviewing (MI) assessment strategy
that involves having a brief MI conversation before
and after the assessment (see Chapter 8 for more
information). This approach will help establish
rapport, determine the client’s readiness for
change, and measure his or her potential response
to personalized feedback.
Start a standard assessment by explaining
what types of tests or questionnaires will be
administered and what information these
tools will reveal. Estimate how long the process
usually takes, and give any other necessary
instructions. Make sure the client is comfortable
with the assessment format (e.g., have self-
administered tests available in the client’s first
language, do a face-to-face interview instead of
a self-administered assessment if the client has
cognitive challenges).
Chapter 4 74

TIP 35
Chapter 4—From Precontemplation to Contemplation: Building Readiness
COUNSELOR NOTE: DESCRIPTION OF A TYPICAL DAY
An informal way to engage clients, build rapport as part of an assessment, and encourage clients to talk
about substance use patterns in a nonjudgmental framework is to ask them to describe a typical day
(Rollnick, Miller, & Butler, 2008). This approach can help you understand the context of clients’ substance
use. For example, it may reveal how much of each day is spent trying to get drugs and how little time is
left to spend with loved ones. By asking about both behaviors and feelings, you can learn much about
what substance use means to clients and how difficult or simple it may be to give it up. This strategy
invites clients to tell a story; that story provides important details about clients’ substance use patterns
and related negative effects.
•
Start by asking permission. “It would help me to understand how [name the substance use behavior,
such as drinking or smoking cannabis] fits into to your life. Would it be okay if we spend a few minutes
going through a typical day from beginning to end? Let’s start from the time you get up in the morning.”
•
Be curious.
•
Avoid the use of the word “problem” (unless the client uses it) in relation to substance use, otherwise
you might create discord (Rosengren, 2018).
•
Follow the client through the sequence of events for an entire day, focusing on both behaviors and
feelings. Keep asking, “What happens when… ?”
•
Ask questions carefully and slowly. Do not add your own thoughts about why certain events transpired.
•
Let the client use his or her own words.
•
Ask for clarification only if you do not understand a term the client uses or if some information
ismissing.
Once the client completes the assessment,
review findings with the client. Present
personalized feedback to the client in a way that is
likely to increase his or her awareness and develop
discrepancy between the client’s substance use
and values. Appendix C provides a link to the
Motivational Enhancement Therapy Manual,
which includes an example of a personal feedback
report to include in a comprehensive assessment.
You should adapt this report for the specific
kinds of assessment information you gather at
yourprogram.
When providing extensive feedback about
assessment results, divide it into small chunks,
and use the EPE approach, otherwise, the client
might feel overwhelmed. You may only need to
provide one or two pieces of feedback to raise
doubts and concerns and to move the client
toward Contemplation.
Involve Signicant Others
Including people with whom the client has a
close relationship can make treatment more
effective. Many people who misuse substances
or who have SUDs respond to motivation from
spouses and SOs to enter treatment (Connors
et al., 2013). An SO is typically a parent, spouse,
live-in partner, or other family member but can be
any person with a close personal relationship to
theclient.
Supportive SOs can help clients become
intrinsically rather than just extrinsically motivated
for behavior change (Bourke, Magill, & Apodaca,
2016). Including supportive SOs is cost effective
and can foster positive client outcomes, including
increased client change talk; increased client
commitment to change; and reduced substance
use, alcohol consumption, and alcohol-related
consequences (Apodaca, Magill, Longabaugh,
Jackson, & Monti, 2013; Bourke et al., 2016; Monti
et al., 2014; Shepard et al., 2016; Smeerdijk et
al.,2015).
Chapter 4 75

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
SOs can encourage clients to use their inner
resources to identify, implement, and sustain
actions leading to a lifestyle free from substance
misuse. They can be important in increasing clients’
readiness to change by addressing substance use
in the following ways:
•
Reminding clients about the importance of
family, their relationship to an SO in their lives,
or both
•
Providing helpful feedback to clients about the
negative effects of their substance use behavior
•
Encouraging clients to change substance
usebehaviors
•
Alerting clients to social and individual coping
resources that support recovery
•
Providing positive reinforcement for using
social/coping resources to change substance use
EXPERT COMMENT: INVOLVING AN SO IN THE CHANGE PROCESS
I have found that actively involving an SO, such as a spouse, relative, or friend, in motivational counseling
can affect a client’s commitment to change. The SO provides helpful input for clients who are ambivalent
about changing addictive behaviors. SO feedback can raise the client’s awareness of the negative effects
of substance use. The SO can also offer needed support in sustaining the client’s commitment to change.
Before involving the SO, I determine whether the SO has a positive relationship with the client and a
genuine investment in affecting the change process. SOs with strong ties to the client and an interest in
helping the client change substance use can help support change; those who lack these qualities can
make this process more difficult. Before involving the SO, I assess the interactions between the client and
the SO. I am particularly interested in learning whether the client’s motivational statements are supported
by the SO.
Following this brief assessment, I use many different commitment-enhancing strategies with the SO to
help him or her affect the motivational process. I try to ask questions that will help the SO feel optimistic
about the client’s ability to change. For example, I may ask the SO the following questions:
•
“Have you noticed what efforts Jack has made to change his drinking?”
•
“What has been most helpful to you in helping Jack deal with the drinking?”
•
“What is different now that leads you to feel better about Jack’s ability to change?”
Through techniques such as eliciting change talk from clients, SOs can help the change process.
Allen Zweben, D.S.W., Consensus Panel Member
Before involving an SO in the client’s treatment:
•
Ask the client for permission to contact the SO.
•
Describe the benefits of SO support.
•
Review confidentiality concerns.
•
If the client agrees, obtain the necessary
writtenreleases.
Some strategies for engaging an SO in an initial
meeting with you and the client include the
following:
•
Use MI strategies to engage the SO in the
counseling process (Belmontes, 2018).
•
Praise the SO for his or her willingness to
participate in the client’s efforts to change.
•
Offer conversation guidelines (e.g., use “I”
statements, don’t use language that blames
orshames).
Chapter 4 76

TIP 35
Chapter 4—From Precontemplation to Contemplation: Building Readiness
•
Define the SO’s role (e.g., offering emotional/
instrumental support, giving helpful feedback,
reinforcing positive reasons for change, working
with client to change substance use behavior).
•
Be optimistic about how the SO’s support and
nonjudgmental feedback can be an important
factor in increasing the client’s motivation
tochange.
•
Invite the SO to be on the client’s team that
is working to reduce the impact of substance
misuse on the couple or family.
•
Provide brief instructions to the SO on how to
ask open questions, use reflective listening,
and support client change talk (Smeerdijk et
al.,2015).
•
Invite the SO to identify the family’s values and
how the substance use behavior might not fit
with those values (Belmontes, 2018).
•
Reinforce positive comments made by the
SO about the client’s current change efforts.
Refocus the conversation if the feedback from
the SO is negative or reinforces the client’s
sustain talk.
•
Use EPE to give the SO information on support
services (e.g., Al-Anon, family peer support
providers, individual counseling) that will
help focus on his or her own recovery while
supporting the client.
•
If the SO cannot be supportive and
nonconfrontational or has substance misuse or
behavioral health concerns that interfere with his
or her ability to participate fully and supportively
in the client’s treatment, consider limiting
the SO’s role to mainly information sharing.
Refer the SO to SUD treatment or behavioral
health services and a recovery support group
(e.g., Al-Anon).
•
If the SO cannot attend counseling sessions
with the client, invite the SO to the session
figuratively by evoking and reinforcing client
change talk associated with the significance
of family and friends in the client’s motivation
to change (Sarpavaara, 2015). For example,
you might ask, “You have mentioned that your
relationship with your daughter is very important
to you. How would not drinking, impact the
quality of your relationship?”
For more information on families and SUD
treatment, see Treatment Improvement Protocol
(TIP) 39: Substance Abuse Treatment and Family
Therapy (Substance Abuse and Mental Health
Services Administration, 2015a).
Express Concern, and Leave the
DoorOpen
In the initial engagement and assessment phase,
if the client remains in Precontemplation and you
cannot mutually agree on treatment goals, express
concern about the client’s substance misuse and
leave the door open for the client to return to
treatment any time. Do this by:
•
Summarizing your concern based on screening
or assessment results or feedback from SOs.
•
Presenting feedback in a factual,
nonjudgmental way.
•
Reminding the client that you respect his or her
decision, even if data suggest a different choice.
•
Emphasize personal choice to maintain
rapport with clients in Precontemplation.
•
Making sure the client has your contact
information and appropriate crisis or emergency
contact information before ending the session.
•
Asking the client’s permission for you or
someone at your program to contact him or her
by phone in a month to check in briefly. If the
client says yes, follow up. This is an opportunity
to assess the situation and encourage the client
to return to treatment if desired.
Understand Special Motivational
Counseling Considerations for
Clients Mandated to Treatment
An increasing number of clients are mandated to
treatment (i.e., ordered to attend) by an employer,
an employee assistance program, or the criminal
justice system. In such cases, failure to enter and
remain in treatment may result in punishment
or negative consequences (e.g., job loss,
revocation of probation or parole, prosecution,
imprisonment), often for a specified time or until
satisfactorycompletion.
Chapter 4 77

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Your challenge is to engage clients who are
mandated to the treatment process. Although
many of these clients are at the Precontemplation
stage, the temptation is to use Action stage
interventions immediately that are not compatible
with the client’s motivation level. This can be
counterproductive. Clients arrive with strong
emotions because of the referral process and the
consequences they will face if they do not succeed
in changing a pattern of use they may not believe
is problematic.
In addition, evidence shows that clients mandated
to treatment tend to engage in a great deal of
sustain talk, which is consistent with being in the
Precontemplation stage and predicts negative
substance use treatment outcomes (Apodaca et al.,
2014; Moyers, Houck, Glynn, Hallgren, & Manuel,
2017). An important motivational strategy with
these clients is to lessen or “soften” sustain talk
before trying to evoke change talk (Moyers et al.,
2017). (See Chapter 3 for strategies for responding
to sustain talk that you can apply to clients who are
mandated to treatment.)
Despite these obstacles, clients mandated to
treatment have similar treatment outcomes as
those who attend treatment voluntarily (Kiluk
et al., 2015). If you use motivational counseling
strategies appropriate to their stage in the SOC,
they may become invested in the change process
and benefit from the opportunity to consider the
consequences of use and the possibility of change.
You may have to spend your first session
“decontaminating” the referral process. Some
counselors say explicitly, “I’m sorry you came
through the door this way.” Important principles to
keep in mind are to:
•
Honor the client’s anger and sense
ofpowerlessness.
•
Avoid assumptions about the type of
treatmentneeded.
•
Make it clear that you will help the client explore
what he or she perceives is needed and useful
from your time together.
When working with clients who are mandated
to treatment, you are required to establish what
information will be shared with the referring
agency. In addition, you should:
•
Formalize the release of information with clients
and the agency through a written consent for
release of information that adheres to federal
confidentiality regulations.
•
Inform clients about what information (e.g.,
attendance, urine test results, treatment
participation) will be released, and get their
consent to share this information.
•
Be sure clients understand which choices they
have about the information to be released
and which choices are not yours or theirs to
make (e.g., information related to child abuse
orneglect).
•
Take into account the role of the clients’
attorneys (if any) in releasing information.
•
Clearly delineate different levels of permission.
•
Be clear with clients about consequences they
may experience from the referring agency if
they do not participate in treatment as required.
Motivational strategies to help maintain a
collaborative working alliance with clients while
presenting such consequences (Stinson & Clark,
2017) include:
- Acknowledge clients’ ambivalence about
participating in counseling.
-
Differentiate your role from the authority of
the referring agency (e.g., “I am here to help
you make some decisions about how you
might want to change, not to pressure you
tochange”).
-
Describe the consequences of not
participating in treatment in a neutral,
nonjudgmental tone.
-
Avoid siding with clients or the referring
agency about the fairness of possible
consequences and punishments. Take a
neutral stance.
-
Emphasize personal choice/responsibility
(e.g., “It’s up to you whether you participate
in treatment”).
Exhibit 4.3 provides an example of an initial
conversation with a client who has been required
to attend counseling as a condition of parole.
Chapter 4 78

TIP 35Chapter 4—From Precontemplation to Contemplation: Building Readiness
EXHIBIT 4.3. An Opening Dialog With a Client Who Has Been Mandated
to Treatment
This dialog illustrates the first meeting between a counselor and a client who is required to attend
group counseling as a condition of parole. The counselor is seeking ways to affirm the client, to find
incentives that matter to the client, to support the client in achieving his most important personal
goals, and to help the client regain control by choosing to engage in treatment with an open mind.
The setting is an outpatient treatment program that accepts private and court-ordered referrals to a
counseling group for people who use substances. The program uses a cognitive–behavioral approach.
The primary interventional tool is rational behavior training. This is the first session between the
counselor and the court-ordered probation client.
Counselor: Good morning. My name is Jeff. You must be Paul.
Client: Yep.
Counselor: Come on in, and sit wherever you’re comfortable. I got some information from your
probation officer, but what would really help me is to hear from you, Paul, a bit more about what’s
going on in your life, and how we might help. (Open question in the form of a statement)
Client: The biggest thing is this 4-year sentence hanging over me and this crap I have to do to stay
out of prison.
Counselor: Well, again, Paul, it sounds like you’re busy and you have a lot of pressures. (Reflection) But
I wonder if there’s something the program offers that you could use.
Client: What I need from you is to get that blasted probation officer off my back.
Counselor: I’m not exactly sure what you mean, Paul.
Client: What I mean is that, I’m already running all over the place to give urine samples and meet all
the other conditions of probation, and now the court says I’ve got to do this treatment program to
stay out of jail.
Counselor: I’m still a little confused. What is it that I can do that might help? (Open question)
Client: You can tell my probation officer I don’t need to be here and that she should stay out of
mybusiness.
Counselor: I may be wrong, Paul, but as I understand it, that’s not an option for either one of us. I
want to support you so that you don’t conflict with your probation officer. For you and her to be in an
angry relationship seems a recipe for disaster. I get the sense from listening to you that you’re really
committed to yourself and to your family. (Affirmation) The last thing you want to do is to wind up in
prison facing that 4-year sentence.
Client: You got that straight.
Counselor: So, it seems to me you’ve made some good choices so far. (Reframe)
Client: What do you mean?
Continued on next page
Chapter 4 79

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
Continued
Counselor: Well, you could have just blown this whole appointment off, but you didn't. You made a
series of choices that make it clear to me that you’re committed to your family, yourself, your business,
and for that matter your freedom. I can respect that commitment and would like to support you in
honoring the choices you’ve already made. (Affirmation and emphasizing personal autonomy)
Client: Does that mean I’m not going to have to come to these classes?
Counselor: No, I don’t have the power to make that kind of decision. However, you and I can work
together to figure out how you might use this course to benefit you. (Partnership)
Client: I can’t imagine getting anything out of sitting around with a bunch of drunks, talking about
our feelings, and whining about all the bad things going on in our lives.
Counselor: You just don’t seem like a whiner to me. And in any case, that’s not what this group is
about. What we really do is give people the opportunity to learn new skills and apply those skills in
their daily lives to make their lives more enjoyable and meaningful. What you’ve already shown me
today is that you can use some of those skills to support even further the good choices that you’ve
already made. (Affirmation)
Client: That’s just a bunch of shrink talk. I already told you, all I need is to get my probation officer off
my back and live my life the way I want to live it.
Counselor: Completing this program is going to help you do that. I think from what you’ve already
demonstrated that you’ll do well in the group. I believe you can learn something that you can use
in your daily life and perhaps teach some of the other people in the group as well. I am certainly
willing to work with you to help you accomplish your goal in terms of meeting the requirements of
probation. My suggestion is that you take it one group at a time and see how it goes. All I would ask of
you is what, in a sense, you have already demonstrated, and that is the willingness to keep your mind
open and keep your goals for life clearly in front of you. I see that you’re committed to your family,
you’re committed to yourself, and you’re committed to your freedom. I want to support all three of
those goals. (Affirmation)
Client: Well, I guess I can do this group thing, at least for now. I’m still not sure what I’m going to get
from sitting around with a bunch of other guys, telling stories, but I’m willing to give it a try.
Counselor: That sounds reasonable and like another good choice to me, Paul. (Affirmation) Let me
give you a handbook that will tell you a little bit more about the group, and I’ll see you tomorrow
night at 6:30 at this office for our first group. It’s been nice to meet you. I look forward to getting to
know you better.
Client: I'll see you tomorrow night. You know, this wasn’t as bad as I thought it would be.
Jeffrey M. Georgi, M.Div., Consensus Panel Member
Chapter 4 80

TIP 35Chapter 4—From Precontemplation to Contemplation: Building Readiness
Although this counseling scenario relies primarily
on cognitive–behavioral therapy strategies, the
counselor engages the client in the spirit of MI
by emphasizing partnership and acceptance of
the client. The counselor also uses affirmations
and maintains a nonjudgmental, neutral tone
throughout the conversation, emphasizing the
client’s autonomy and values. This approach is
consistent with an effective way to engage a client
in Precontemplation who has been mandated
to treatment.
Conclusion
The first step in working with clients in the
Precontemplation stage of the SOC is to develop
rapport and establish a counseling alliance. The
next step is to assess their readiness to change,
then help them begin to develop an awareness
that their use of substances is linked to problems in
their lives. Motivational counseling strategies from
motivational enhancement therapy (e.g., providing
personalized feedback about assessment results)
and MI (e.g., using reflective listening to engage,
emphasizing personal choice and responsibility,
exploring discrepancy) are suited to helping clients
move from Precontemplation to Contemplation.
Chapter 4 81
This page intentionally left blank

Chapter 5—From Contemplation to
Preparation: Increasing Commitment
The reasons for change need to be important and
substantive enough to move the individual into
deciding to make the effort to change. The task
for individuals in Contemplation is to resolve their
decisional balance consideration in favor of change.
The decision to change marks the transition out of
the Contemplation stage and into Preparation.”
—DiClemente, 2018, p. 29
KEY MESSAGES
TIP 35
ENHANCING MOTIVATION FOR CHANGE IN
SUBSTANCE USE DISORDER TREATMENT
•
Clients in Contemplation begin to recognize
concerns about substance use but are
ambivalent about change.
• You can use motivational counseling
strategies to help clients resolve ambivalence
aboutchange.
• When using a decisional balance (DB)
strategy, you briefly reflect clients’ reasons for
continuing substance use (i.e., sustain talk)
but emphasize clients’ reasons for change (i.e.,
change talk).
• Motivational counseling strategies to enhance
commitment to change move clients closer
to the Preparation stage and taking steps
tochange.
Chapter 5 describes strategies to increase
clients’ commitment to change by normalizing
and resolving ambivalence about change and
enhancing clients’ decision-making capabilities.
Central to most strategies is the process of evoking
and exploring reasons to change through asking
open question and reflective listening. The chapter
begins with a discussion of ambivalence, extrinsic
(external) and intrinsic (internal) motivation,
and ways to help clients connect with internal
motivators to enhance decision making and their
commitment to change. It then focuses on DB
strategies—ways to explore the costs and benefits
of change and clients’ values about changing
substance use behaviors. Chapter 5 also addresses
the importance of self-efficacy in clients’ decisions
to change and provides strategies for enhancing
commitment to change once clients decide to
change. Exhibit 5.1 presents counseling strategies
for Contemplation.
83

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
EXHIBIT 5.1. Counseling Strategies for Contemplation
CLIENT MOTIVATION COUNSELOR FOCUS COUNSELING STRATEGIES
•
The client acknowledges
•
Normalize and resolve
•
Shift focus from extrinsic to intrinsic
concerns and is considering client’s ambivalence motivation.
the possibility of change about change.
•
Summarize client concerns.
but is ambivalent and
•
Help the client tip
•
Assess where the client is on the decisional
uncertain.
the DB scales toward
scale.
•
The client begins to reflect
change.
•
Explore pros/cons of substance use and
on his or her substance
behavior change.
use behavior and considers
•
Reexplore values in relation to change.
choices and options for
change.
•
Emphasize personal choice and
responsibility.
•
Explore client’s understanding of change
and expectations of treatment.
•
Reintroduce feedback.
•
Explore self-efficacy.
•
Summarize change talk.
•
Enhance commitment to change.
Normalize and
ResolveAmbivalence
You must be prepared to address ambivalence to
help clients move through the Stages of Change
(SOC) process. Ambivalence is a normal part of
any change process. Ambivalence is uncomfortable
because it involves conflicting motivations about
change (Miller & Rollnick, 2013). For example,
a client may enjoy drinking because it relaxes
him or her but may feel guilty about losing a job
because of drinking and putting his or her family in
financial risk. Clients often have conflicting feelings
and motivations (Miller & Rollnick, 2013). During
Contemplation, ambivalence is strong. As you
help clients move toward Preparation and Action,
ambivalence lessens. Miller and Rollnick (2013)
use the metaphor of a hill of ambivalence wherein
clients move up the hill during Precontemplation/
Contemplation and then journey down the hill
through the resolution of ambivalence, which
moves them into Preparation and Action (Exhibit
5.2). Chapter 2 provides a thorough description
of DARN CAT (Desire, Ability, Reasons, Need,
Commitment Activation, Taking steps) change talk.
Chapter 5 84

TIP 35
Chapter 5—From Contemplation to Preparation: Increasing Commitment
EXHIBIT 5.2. The Motivational Interviewing (MI) Hill of Ambivalence
Source: Miller & Rollnick, 2013. Motivational Interviewing: Helping People Change (3rd ed.), p. 164. Adapted with
permission from Guilford Press.
The two key motivational strategies you can use
to resolve ambivalence in Contemplation are:
1. Normalizing ambivalence. As they move closer
to a decision to change, clients often feel
increasing conflict and doubt about whether
they can or want to change. Reassure clients
that conflicting feelings, uncertainties,
and reservations are common. Normalize
ambivalence by explaining that many clients
experience similar strong ambivalence at
this stage, even when they believe they have
resolved their mixed feelings and are nearing
a decision. Clients need to understand that
many people go back and forth between
wanting to maintain the status quo and wanting
to change and yet have been able to stay on
track by continuing to explore and discuss their
ambivalence.
2. Evoking DARN change talk. DARN refers to
clients’ desire, ability, reasons, and need to
change. During Contemplation, help clients
move up the hill of ambivalence and guide them
toward Preparation by evoking and reflecting
DARN change talk. Use open questions: “How
would you like things to change so you don’t
feel scared when you can’t remember what
happened after drinking the night before?”
Exhibit 3.8 in Chapter 3 offers more examples of
open questions that evoke DARN change talk.
Use reflective listening responses to highlight
the change talk. Remember that the goal is
to guide clients to make the arguments for
change (Miller & Rollnick, 2013). The key is to
avoid jumping too quickly into evoking CAT
(i.e., commitment, activation, and taking steps)
change talk, solving problems in response to
ambivalence, or making a plan of action. The
client has to climb up the hill of ambivalence
before easing down the other side.
Chapter 5 85

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Shi the Focus From Extrinsic to Intrinsic
Motivation
To help clients prepare for change, explore the
range of both extrinsic and intrinsic motivators
that have brought them to this point. Many
clients move through the Contemplation stage
acknowledging only the extrinsic motivators that
push them to change and that brought them to
treatment. External motivators may pressure clients
into treatment, including a spouse, employer,
healthcare provider, family member, friend, or the
child welfare or criminal justice system. Extrinsic
motivators can help bring clients into and stay in
treatment, but intrinsic motivators are important
for significant, long-lasting change (Flannery,
2017; Kwasnicka, Dombrowski, White, & Sniehotta,
2016; Mahmoodabad, Tonekaboni, Farmanbar,
Fallahzadeh, & Kamalikhah, 2017).
You can help clients develop intrinsic
motivation by assisting them in recognizing the
discrepancies between “where they are” and
“where they want to be”:
•
Invite clients to explore their life goals and
values, which can strengthen internal motivation.
In searching for answers, clients often reevaluate
past mistakes and activities that were self-
destructive or harmful to others.
•
Encourage this exploration through asking open
questions about client goals: “Where would
you like to be in 5 years?” and “How does your
substance use fit or not fit with your goals?”
•
Highlight clients’ recognition of discrepancies
between the current situation and their hopes
for the future through reflective listening.
Awareness of discrepancy often evokes
desire change talk, an essential source of
intrinsicmotivation.
Sometimes, intrinsic motivation emerges from role
conflicts and family or community expectations. For
example, a single mother who lost her job because
of substance use may have a strong motivation
to get and keep another job to provide for her
children. For other clients, substance misuse has
cut their cultural or community ties. For example,
they stop going to church or neglect culturally
affirmed roles, such as helping others or serving
as role models for young people. A desire to
reconnect with cultural traditions as a source of
identity and strength can be a powerful motivator
for some clients, as can the desire to regain others’
respect. Positive change also leads to improved
self-image and self-esteem.
EXPERT COMMENT: LINKING
FAMILY, COMMUNITY, AND
CULTURAL VALUES TO A DESIRE
FOR CHANGE
Working with a group of Latino men in the
Southwest who were mandated into treatment
as a condition of parole and had spent most
of their lives in prisons, we found that as these
men aged, they seemed to tire of criminal life.
In counseling, some expressed concerns about
losing touch with their families and culture, and
many reported a desire to serve as male role
models for their sons and nephews. They all
wanted to restore their own sense of pride and
self-worth in the small community where many
of their families had lived for generations.
Newly trained in MI, we recognized a large,
untapped source of self-motivation in a
population that we had long before decided did
not want help. We had to change our previous
beliefs about this population as not wanting
treatment to seeing these men as requesting
help and support to maintain themselves
outside the prison system and in the community.
Carole Janis Otero, M.A., Consensus Panel Member
Helping clients shift from extrinsic to intrinsic
motivation helps them move from contemplating
change to deciding to act. Start with clients’
current situations, and find a natural link between
existing external motivators and intrinsic ones that
they may not be aware of or find easy to describe.
Through compassionate and respectful exploration,
you may discover untapped intrinsic motivation.
Chapter 5 86

TIP 35
Chapter 5—From Contemplation to Preparation: Increasing Commitment
Along with MI techniques presented in Chapter
3, use these strategies to identify and strengthen
intrinsic motivation:
•
Show genuine curiosity about clients. Show
interest in their lives at the first meeting and
over time. Because clients’ desire to change is
rarely limited to substance use, they may find it
easier to talk about changing other behaviors.
Most clients have concerns about several areas
of their lives and wish to reconnect with their
community, improve their finances, find work,
or fall in love. Many are highly functional and
productive in some aspects of their lives and
take great pride in special skills, knowledge, or
other abilities they do not want to lose.
•
Do not wait for clients to talk spontaneously
about their substance use. Show interest,
and ask how their substance use affects these
aspects of their lives. Even with clients who
do not acknowledge any problems, question
them about their lives to show concern and
strengthen the counseling alliance.
•
Reframe clients’ negative statements about
external pressure to get treatment. For
example, help clients reframe anger expressed
toward their spouse who has pressured them to
enter treatment as seeing their spouse as caring
and invested in the marriage.
•
Identify and strengthen intrinsic motivation
of clients who have been mandated to
treatment. Emphasize personal choice and
responsibility with these clients. Help clients
understand that they can freely choose
to change because doing so makes good
sense and is desirable, not because negative
consequences will happen if they choose not
tochange.
Summarize Client Concerns
As you evoke DARN change talk and explore
intrinsic and extrinsic motivations, you gather
important information for helping the client
resolve ambivalence about change. You have a
working knowledge, and perhaps even a written
list, of issues and areas about which the client
has conflicting feelings and which are important
intrinsic motivators for changing substance use
behaviors. A first step in helping the client
to weigh the pros and cons of change is to
organize the list of concerns and present them
to the client in a careful summary that expresses
empathy, develops discrepancy, and shifts the
balance toward change. Because you should reach
agreement on these issues, the summary should
end by asking whether the client agrees that these
are his or her concerns about the substance use.
You might ask, “Is this accurate?” or “Did I leave
anything out?”
Help Tip the Decisional Balance
Toward Change
For any decision, most people naturally weigh costs
and benefits of the potential action. In behavioral
change, these considerations are called “decisional
balancing.” This is a process of appraising or
evaluating the “good” aspects of substance use—
the reasons not to change (expressed through
sustain talk)—and the “less-good” aspects—the
reasons to change (expressed through change
talk). DB originated with Janis and Mann (1977) as
a motivational counseling strategy. It is used widely
in substance use disorder (SUD) treatment to
explore benefits and costs of continued substance
use and of changing substance use behaviors.
Research on DB in SUD treatment has shown that
DB is associated with increased motivation to
change in diverse client populations and favorable
client outcomes (Elliot & Carey, 2013; Foster &
Neighbors, 2013; Hennessy, Tanner-Smith, &
Steinka-Fry, 2015).
Motivation to reduce or stop substance use
increases when the costs of use outweigh the
benefits and when the pros of changing substance
use outweigh the cons (Connors, DiClemente,
Velasquez, & Donovan, 2013). Your task is to help
clients recognize and weigh negative aspects of
substance use to tip the scale in favor of change.
Assess Where the Client Is on the
Decisional Scale
Start by getting a sense of where the client is
with regard to the decision-making process. The
Alcohol Decisional Balance Scale and the Drug
Use Decisional Balance Scale in Appendix B are
validated instruments that ask clients to rate, on
a scale of 1 to 5, the importance of statements
Chapter 5 87
TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
like “Having to lie to others about my drinking
bothers me” in making a decision about changing
substance use behaviors (Prochaska et al., 1994).
The scores give you and the client a sense of where
the client is with regard to reporting more pros
versus more cons for continued substance use. You
can also explore specific items on the measure on
which the client scores high (e.g., “Some people
close to me are disappointed in me because of my
drug use”) as a way to build discrepancy between
the client’s values and substance use, thus evoking
change talk.
Explore the Pros and Cons of Substance
Use and Behavior Change
Weighing benefits and costs of substance use and
change is at the heart of DB work. To accomplish
this, invite the client to write out a list of
positives and negatives of substance use and
changing substance use behaviors. This can be
a homework assignment that is discussed at the
next session, or the list can be generated during a
session. Putting the items on paper makes it seem
more “real” to the client and can help structure
the conversation. You can generate a list of the
pros and cons of substance use and a list of pros
and cons of changing substance use behaviors
separately or use a grid like the one in Exhibit 5.3.
EXHIBIT 5.3. Decisional Balance
Sheet for Substance Use
Reasons to Continue
Reasons to
Substance Use
Change Substance
(StatusQuo)
Use(Change)
Positives of Negatives of
substanceuse substanceuse
Negatives of changing Positives of changing
substance use substance use
Source: Connors et al., 2013.
Presenting to clients a long list of reasons to
change and a short list of reasons not to change
may finally upset the balance and tip the scale
toward change. However, the opposite (i.e., a
long list of reasons not to change and a short life
of reason to change) can show how much work
remains and can be used to prevent premature
decision making.
Recognize that many clients find that one or two
reasons to change counterbalance the weight
of many reasons not to change and vice versa.
Therefore, it is not just the number of reasons to
change or not change but the strength of each
reason that matters. Explore the relative strength
of each motivational factor, and highlight the
weight clients place on each change factor.
Reasons for and against continuing substance use,
or for and against aspects of change, are highly
individual. Factors that shift the balance toward
positive change for one person may barely matter
to another. Also, the value or weight given to a
particular item in this inventory of pros and cons is
likely to change over time.
Whether or not you use a written worksheet,
always listen carefully when clients express
ambivalence. Both sides of ambivalence,
expressed through sustain talk and change talk,
are present in clients at the same time (Miller &
Rollnick, 2013). You may hear both in a single
client statement—for example, “I get so energized
when I snort cocaine, but it’s so expensive. I’m not
sure how I’ll pay the bills this month.” Although
discussing with clients what they like about
drinking or using drugs may establish rapport,
increasing expressions of sustain talk is associated
with negative client outcomes (Foster, Neighbors,
& Pai, 2015; Houck & Moyers, 2015; Lindqvist,
Forsberg, Enebrink, Andersson, & Rosendahl,
2017; Magill et al., 2014).
In DB, explore both sides of ambivalence, but
avoid reinforcing sustain talk, which can be
counterproductive (Krigel et al., 2017; Lindqvist
et al., 2017; Miller & Rose, 2013). Once a client
decides to change a substance use behavior, a
DB exercise on the pros and cons of change may
increase commitment to change (Miller & Rose,
2013). Carefully consider your own intention
and the client’s stage in the SOC before using a
structured DB that explores both sides of client
ambivalence equally.
Chapter 5 88

TIP 35Chapter 5—From Contemplation to Preparation: Increasing Commitment
Exhibit 5.4 describes other issues that may arise as clients explore pros and cons of change.
EXHIBIT 5.4. Other Issues in Decisional Balance
Loss and grief Giving up a way of life can be as intense as the loss of a close friend. Many clients
need time for grieving. They have to acknowledge and mourn this loss before
they are ready to build a strong attachment to recovery. Pushing them to change
too fast can weaken determination. Patience and empathy are reassuring at
thistime.
Reservations or Serious reservations about change can be a signal that you and clients have
reluctance
different views. As clients move into the Preparation stage, they may become
defensive if pushed to commit to change before they are ready or if their goals
conflict with yours. They may express this reluctance in behaviors rather than
words. For example, some will miss appointments, sending a message that they
need more time and want to slow the process. Continue to explore ambivalence
with these clients, and reassess where they are in the change process.
Premature deci- DB exercises give you a sense of whether clients are ready for change. If clients’
sion making
description of pros and cons is unclear, they may express goals for change that
are unrealistic or reflect a lack of understanding of their abilities and resources.
Clients may say what they think you want to hear. Clients who are not ready to
decide to change will let you know. Allowing clients to set themselves up for
failure can result in them stopping the change process altogether or losing trust
in you. Delay the commitment process, and return to Contemplation.
Keeping pace Some clients enter treatment after they have stopped using substances on
their own. Others stop substance use the day they call the program for the first
appointment. They have already made a commitment to stop. If you try to elicit
these clients’ concerns or conduct DB exercises, you might evoke sustain talk
unnecessarily and miss an important opportunity to provide the encouragement,
incentives, and skills needed to help action-oriented and action-ready individuals
make progress. Move with these clients immediately to create a change plan and
enter the Action stage, but be alert for ambivalence that may remain or develop.
Free choice Clients may begin using drugs or alcohol out of rebelliousness toward their
family or society. Substance use may be an expression of continued freedom—
freedom from the demands of others to act or live in a certain way. You may
hear clients say that they cannot change because they do not want to lose their
freedom. Because this belief is tied to some clients’ early-forged identities, it
may be a strong factor in their list of reasons not to change. However, as clients
age, they may be more willing to explore whether “freedom to rebel” is actually
freedom or its opposite. If you address this issue, you can reframe the rebellion
as reflection of a limitation of choices (i.e., the person must do the opposite of
what is expected). As clients age, they may be more open to making a choice
that represents real freedom—the freedom not to rebel but to do what they
trulychoose.
Chapter 5 89

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Reexplore Values in Relation to Change
Use DB exercises as opportunities to help
clients explore and articulate their values and
to connect these values with positive change.
Clients’ values influence their reasons for and
against change. For example, an adolescent
involved in drug dealing with a neighborhood
gang may say that leaving the gang is not possible
because of his loyalty to the other members.
Loyalty and belonging are important values to
him. Relate them to other groups that inspire
similar allegiance, such as a sports team or
scouting—organizations that create a sense of
belonging and reflect his core values. A young
woman with a family history of hard work and
academic achievement may wish to return to those
values by finishing high school and becoming
financiallyindependent.
Hearing themselves articulate their core values
helps clients increase their commitment to positive
change. If they can frame the process of change
within the larger context of values shared with their
family, community, and culture, they may find it
easier to contemplate change.
Emphasize Personal Choice and
Responsibility
In a motivational approach to counseling, you
don’t “give” a client a choice. The choice is not
yours to give; rather, it is the client’s to make.
Your task is to help the client make choices that
are in his or her best interest and that align with his
or her values and goals. Consistently emphasize
the client’s responsibility and freedom of choice.
The client should be used to hearing you make
statements such as:
•
“It’s up to you to decide what to do about this.”
•
“No one can decide this for you.”
•
“No one can change your drug use for you. Only
you can.”
•
“You can decide to go on drinking or
tochange.”
Explore the Client’s Understanding of
Change and Expectations of Treatment
In working toward a decision, understand
what change means to clients and what their
expectations of treatment are. Some clients
believe that quitting or cutting down means
changing their entire life—moving from their
neighborhood or cutting ties with all their
friends, even their family. Some believe they
have to change everything overnight. This can be
overwhelming. Tell clients who have never been
in treatment before about the level of motivation
and openness required to get the most from their
treatment experience (Raylu & Kaur, 2012).
In exploring these meanings and expectations with
the client, you will get a sense of which actions the
client might consider and which he or she will not.
For example, a client might state that she could
never move from her neighborhood, a well-known
drug market, because her family is there. Another
says he will not consider anything but cutting
down on his drinking. A third client may just as
strongly state that total abstinence and a stay in a
therapeutic community are the only options, as all
others have failed.
By exploring treatment expectations with clients,
you introduce information about the benefits
of treatment and can begin a discussion about
available options. When clients’ expectations
about treatment match what actually happens and
they have positive expectations about treatment,
they have better outcomes (Kuusisto, Knuuttila, &
Saarnio, 2011). It is never too soon to elicit clients’
expectations about treatment through reflective
listening. Show that you understand their concerns,
and provide accurate information about your
treatment program and the benefits of treatment
using motivational strategies like Elicit-Provide-
Elicit (described in Chapter 3).
Chapter 5 90

TIP 35
Chapter 5—From Contemplation to Preparation: Increasing Commitment
Reintroduce Feedback
Use personalized feedback after assessments
to motivate clients. Continue to use assessment
results to influence clients’ decisional
considerations. Objective medical, social, and
neuropsychological feedback prompts many clients
to contemplate change. Reviewing assessment
information can refocus clients on the need for
change. Reintroducing objective assessment data
reminds clients of earlier insights into the need
forchange.
For example, a client may be intrinsically motivated
to stop alcohol misuse because of health concerns
yet feel overwhelmed by fear that quitting is
impossible. Reintroducing feedback from the
medical assessment about the risk of serious liver
damage or a family history of heart disease could
add significant additional weight to the DB and tip
the balance in the direction of change.
Explore Self-Ecacy
By listening for self-efficacy statements from
clients, you can discover what they feel they
can and cannot do. Self-efficacy is a critical
determinant of behavior change—it is the belief
that they can act in a certain way or perform a
particular task. Even clients who admit to having
a serious problem are not likely to move toward
positive change unless they have some hope of
success. Self-efficacy can be thought of as hope
or optimism, but clients do not have to have an
overall optimistic view to believe a certain behavior
can be changed.
Statements about self-efficacy could include
thefollowing:
•
“I can’t do that.”
•
“That is beyond my powers.”
•
“That would be easy.”
•
“I think I can manage that.”
Self-efficacy is not a global measure, like self-
esteem. Rather, it is behavior specific. Underlying
any discussion of self-efficacy is the question
“Efficacy to perform what specific behavior?” There
are five categories of self-efficacy related to SUDs
(DiClemente, Carbonari, Montgomery, & Hughes,
1994: Glozah, Adu, & Komesuor, 2015):
•
Coping self-efficacy is dealing successfully with
situations that tempt one to use substances,
such as by being assertive with friends or talking
with someone when upset rather than using
thesubstance.
•
Treatment behavior self-efficacy involves the
client’s ability to perform behaviors related
to treatment, such as self-monitoring or
stimuluscontrol.
•
Recovery self-efficacy is the ability to recover
from a recurrence of the addictive behavior.
•
Control self-efficacy is confidence in one’s
ability to control behavior in risky situations.
•
Abstinence self-efficacy is confidence in one’s
ability to abstain despite cues or triggers to use.
Explore clients’ sense of self-efficacy as they
move toward Preparation. This may help you
determine more specifically whether self-efficacy
is a potential support or obstacle to change.
Remember, you can enhance client self-efficacy by
using the Confidence Ruler (see Exhibit 3.10) and
eliciting confidence talk (see the section “Evoking
hope and confidence to support self-efficacy”
inChapter 3).
Summarize Change Talk
As the client transitions from Contemplation to
Preparation, you will notice that the client has
moved to the top of the MI Hill of Ambivalence
(see Exhibit 5.2 above) and is expressing less
sustain talk and more change talk. This is a
good time to offer a recapitulation summary, as
described in Exhibit 5.5.
Chapter 5 91

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
EXHIBIT 5.5. Recapitulation Summary
At the end of DB exercises, you may sense that the client is ready to commit to change. At this point, you
should summarize the client’s current situation as reflected in your interactions thus far. The purpose of
the summary is to draw together as many reasons for change as possible while pointing out the client’s
reluctance or ambivalence. Your summary should include as many of the following elements as possible:
•
A summary of the client’s own perceptions of the problem
•
A summary of the client’s ambivalence, including what remains positive or attractive about
substance use
•
A review of objective evidence you have regarding the presence of risks and problems
•
Your assessment of the client’s situation, particularly when it aligns with the client’s own concerns
•
A summary of the client’s change talk, emphasizing desire, ability, reasons, and need to change
Remember to recognize the client’s sustain talk (i.e., reasons for staying with the status quo), but
emphasize client change talk to tip the balance in favor of change.
Enhance Commitment to Change
You should still reinforce the client’s commitment
to change even after the client has decided
to change and has begun to set goals. You
should expect client indecision at any point in
the change process. Additional strategies that
enhance commitment at this point include asking
key questions, taking small steps, going public,
and envisioning.
Asking key questions
After the summary, ask a key question—for
example, “What do you think you will do now?”
(see the section “Asking key questions” in Chapter
3)—to help the client move over the top of the
MI Hill of Ambivalence toward Preparation. Key
questions will elicit CAT change talk. One of
the main signs that the client is intending and
committed to taking steps is an increase in CAT
change talk (Miller & Rollnick, 2013). The client is
making statements of commitment (e.g., “I will
call the treatment facility to set up an intake”),
activation (e.g., “I am willing to stop smoking
marijuana for a month), and taking steps (e.g., “I
looked up the schedule for Narcotics Anonymous
meetings on its website”) (Miller & Rollnick, 2013).
Reinforce CAT change talk through reflective
listening and summarizing.
Taking small steps
You have asked the client key questions such as
“What’s next?” and have presented options to
emphasize the client’s choice to change and to
select areas of focus. Remind the client that he or
she has choices and can control the change process
to reinforce commitment. Reassure the client who
is overwhelmed by thinking of change that he or
she can set the pace and begin with small steps.
Some clients respond well to stories of others who
made large, seemingly impossible life changes one
step at a time. Don’t underestimate the value of
such stories and models in enhancing motivation.
Going public
Sharing a commitment to change with at least
one other person besides the counselor can keep
clients accountable. Telling a significant other
about one’s desire to change usually enhances
commitment to change. “Going public” can be a
critical step for a client who may not have been
ready to tell others until this point. Alcoholics
Anonymous (AA) has applied the clinical wisdom
of public commitment to change through use of
the “white chip.” An attendee at an AA meeting
who has an intention to quit drinking can pick
up a white chip. The white chip is also called a
Beginner’s Chip or Surrender Chip and is a public
acknowledgment of the person’s intention to
startrecovery.
Chapter 5 92

TIP 35Chapter 5—From Contemplation to Preparation: Increasing Commitment
Envisioning
Conclusion
Helping clients visualize their life after change
can be a powerful motivator and an effective
means of strengthening their commitment.
In addition, stories about how others have
successfully achieved their goals can be excellent
motivators. An exercise for envisioning change is
to ask clients to picture themselves after a year
has passed, during which time they have made
the changes they desire in the areas of their lives
most hurt by their substance use. Some clients
may find it valuable to write a letter to themselves
that is dated in the future and describes what
life will be like at that point. The letter can have
the tone of a vacation postcard (“Wishing you
were here!”). Others will be more comfortable
describing these scenes to you. Chapter 3
provides more information MI strategies to
strengthencommitment.
To help clients move from Contemplation to
Preparation, explore and resolve ambivalence
about change. Help clients climb the MI Hill of
Ambivalence and journey down the other side
toward commitment and change. DB exercises
can help clients explore ambivalence, clarify
reasons to change, and identify barriers to change
(e.g., reasons to continue substance use). When
tipping the balance in favor of change, emphasize
reflections of change talk, minimize the focus
on sustain talk, and use motivational strategies
to enhance commitment and facilitate clients’
movement into Preparation.
Chapter 5 93
This page intentionally left blank

Chapter 6—From Preparation to Action:
Initiating Change
The Preparation stage of change entails developing a plan of action and
creating the commitment needed to implement that plan. Decisions do
not translate automatically into action. To change a behavior, one needs
to focus attention on breaking the old pattern and creating a new one.
Planning is the activity that organizes the environment and develops the
strategies for making change.”
—DiClemente, 2018, pp. 29‒30
KEY MESSAGES
TIP 35
ENHANCING MOTIVATION FOR CHANGE IN
SUBSTANCE USE DISORDER TREATMENT
•
During the Preparation stage, clients are
considering possible paths toward changing
substance use behaviors and beginning to
take small steps to reach the final change goal.
• You can support clients’ movement from
Preparation to Action by exploring client
change goals and helping them develop a
change plan.
• You can maintain a client-centered focus
by eliciting clients’ change goals and not
imposing goals on them.
Chapter 6 describes the process of identifying and
clarifying change goals. It also focuses on how and
when to develop a change plan with the client and
suggests ways to ensure a sound plan by offering
the client a menu of options, contracting for
change, identifying and lowering barriers to action,
and enlisting social support. This chapter also
describes your tasks while the client moves into the
Action stage, like helping the client initiate the plan
and evaluating the effectiveness of the plan.
In earlier stages of the Stages of Change (SOC)
approach, you use motivational strategies to
increase clients’ readiness. In Preparation, you
use motivational strategies to strengthen clients’
commitment and help them make a firm decision
to change. Clients who commit to change and
believe change is possible are prepared for the
Action stage. Clients who are actively taking steps
to change substance use behaviors have better
long-term outcomes after treatment than clients
who have not reached this stage of the SOC
(Heather & McCambridge, 2013).
Your task is to help clients set clear goals for
change in preparation for developing a change
plan. Changing any longstanding behavior requires
preparation and planning. Clients must see change
as being in their best interest before they can move
into the Action stage. Developing a change plan
that is accessible, acceptable, and appropriate
for each client is key. The negative consequences
of ignoring the Preparation stage can be a brief
course of action followed by rapid return to
substance use. By the end of the Preparation stage,
clients should have a plan for change that guides
them into the Action stage.
95

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Exhibit 6.1 presents counseling strategies for Preparation and Action.
EXHIBIT 6.1. Counseling Strategies for Preparation and Action
SOC CLIENT MOTIVATION COUNSELOR
FOCUS
COUNSELING STRATEGIES
Preparation The client is
committed and
planning to make a
change in the near
future but is still
considering what
to do.
•
Explore client
change goals.
•
Develop a
change plan.
•
Clarify the client’s own goals.
•
Sample goals; encourage experimenting.
•
Elicit change strategies from the client.
•
Offer a menu of change options.
•
Negotiate a behavioral contract.
•
Explore and lower barriers to action.
•
Enlist social support.
Action The client actively
takes steps to
change but is not
yet stable.
•
Support the
client’s action
steps.
•
Evaluate the
change plan.
•
Help the client determine which change
strategies are working and which are not.
•
Change the strategies as needed.
Explore Client Change Goals
Once the client has decided to make a positive
change and the commitment is clear, goals should
be set. Setting goals is part of the exploring and
envisioning activities in the early and middle parts
of the Preparation stage. Having summarized and
reviewed the client’s decisional considerations,
you should now be prepared to ask about ways in
which the client might want to address some of the
reasons to change listed on the positive side of the
decisional balance sheet. The process of talking
about and setting goals strengthens commitment
to change.
Clarify the Client’s Goals
Help the client set goals that are as realistic
and specific as possible and that address the
concerns he or she described earlier about
substance use. The client may set goals in multiple
areas, not just substance use. He or she may work
toward goals such as regaining custody of children,
getting a job, becoming financially independent,
leaving an abusive relationship, and returning to
school. The client who sets several goals may need
help deciding which to focus on first.
Early on, goals should be short term,
measurable, and realistic so that clients can
begin measuring success and feeling good about
themselves as well as hopeful about the change.
If goals seem unreachable to you, discuss your
concerns. Use OARS (Open questions, Affirmations,
Reflective listening, and Summarization) to help
clients clarify their goals, decide on which goal to
focus first, and identify steps to achieving their
goals. For example, if one goal is to get a job, you
can start with an open question: “What do you
think is the first step toward meeting this goal?”
The goal is the vision, and the steps are the specific
tasks that clients perform to meet the goal.
Setting goals is a joint process. The counselor
and client work together, moving from general
ideas and visions to specific goals. Seeing how the
client sets goals and the types of goals he or she
sets provides information on the client’s sense of
self-efficacy, level of commitment, and readiness
for change. The more hopeful a client feels about
the future, the more likely he or she is to achieve
treatment goals.
Chapter 6 96

TIP 35Chapter 6—From Preparation to Action: Initiating Change
Make identifying and clarifying treatment goals
a client-driven process. Doing so is consistent
with the principles of person-centered counseling
and the spirit of motivational interviewing (MI). It is
up to the client to decide what actions to take or
treatment options to seek to address a substance
use problem. Matching the client to the preferred
substance use disorder (SUD) treatment options
can help reduce alcohol consumption and improve
drug-related outcomes (Friedrichs, Spies, Härter,
& Buchholz, 2016). In a systematic review, brief
motivational alcohol interventions for adolescents
had significantly larger effects on alcohol
consumption if they included goal-setting exercises
(Tanner-Smith & Lipsey, 2015).
Your task is to help clients identify their
preferred change goals and to enhance their
decision making by teaching them about their
treatment options. (See Chapter 3 for more
information about and strategies for identifying
change goals using MI.)
Remember that the client’s preferred treatment
goals may not match what you prefer. A client
might choose a course of action with which you do
not agree or that is not in line with the treatment
agency’s policies. A decision to reduce but not
completely stop substance use, for example, may
go against the agency’s policy of zero tolerance
for illicit substance use. Exhibit 6.2 offers some
strategies for addressing these types of situations.
Chapter 6 97

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
EXHIBIT 6.2. When Treatment Goals Differ
What do you do when the client’s goals differ from yours or those of your agency? This issue
arises in all behavioral health services but especially in a motivational approach, where you listen
reflectively to a client and actively involve him or her in decision making. As you elicit goals for
change and treatment, a client may not choose goals that you think are right for him or her.
Before exploring different ways of handling this common situation, try to clarify how the client’s
goals and your own (or your agency’s goals) do not match. For a client, goals are by definition
the objectives he or she is motivated (ready, willing, and able) to work toward. If the client is not
motivated to work toward it, it is not a goal. You or your agency, however, may have specific plans
or hopes for the client. You cannot push your hopes and plans onto the client. This situation
can become an ethical problem if you focus too much on trying to get a client to change in the
direction of your or the agency’s goals (Miller & Rollnick, 2013).
What are your clinical options when goals differ? You can choose from the following strategies:
•
Negotiate (i.e., figure out how to work out the differences)
- Rework the agenda and be open about your concerns as well as your hopes for the client
(Miller & Rollnick, 2013).
- Find goals on which you and the client can agree, and work together on those.
- Start with areas in which the client is motivated to change. Women with alcohol or drug use
disorders, for example, often come to treatment with a wide range of other problems, many
of which they see as more pressing than making a change in substance use.
-
Start with the problems that the client feels are most urgent, and then address substance
use when its relationship to other problems becomes obvious.
•
Approximate (i.e., try to find an agreed-on goal that is similar)
- Even if a client is not willing to accept your recommendations, consider the possibility of
agreeing on a goal that is still a step in the right direction. Your hope, for example, might be
that the client would eventually become free from all psychoactive substance use. The client,
however, is most concerned about cocaine and is not ready to talk about changing cannabis,
tobacco, or alcohol use.
- Rather than dismiss the client for not accepting a goal of immediate abstinence from all
substances, focus on stopping cocaine use, and then consider next steps.
•
Refer
- If you can’t help the client with treatment goals even after trying to negotiate or
approximate, refer the client to another provider or program.
- Work within state licensing and professional ethical codes to avoid suddenly ending
treatment.
- Offer a menu of options, and take an active role in linking the client to other treatment and
community-based services.
- Be open in a nonjudgmental and neutral way about the fact that you cannot help the client
with his or her treatment goal (Moyers & Houck, 2011).
Chapter 6 98

TIP 35
Chapter 6—From Preparation to Action: Initiating Change
Sample Goals and Encourage
Experimenting
You may need to help some clients sample or try
out their goals before getting them to commit
to long-term change. For instance, some clients
benefit from experimenting with abstinence or
cutting down their substance use for a short
period. The following approaches to goal sampling
may be helpful for clients who are not committed
to abstinence as a change goal:
•
Sobriety sampling. This trial period of
abstinence is commonly used with clients who
(Boston Center for Treatment Development and
Training [BCTDT], 2016):
- Are not interested in abstinence as a
treatment goal.
- Express significant need or desire to
address misuse but are not ready to commit
toabstinence.
- Have had many past unsuccessful attempts at
moderate use.
A successful trial of sobriety sampling can
enhance clients’ commitment to a goal of
abstinence. Even a 2-to-3–week period of
abstinence before treatment can lead to positive
client outcomes, including reductions in alcohol
misuse (Gueorguieva et al., 2014). However,
longer periods of trial abstinence may give
clients more of an opportunity to experience
the benefits of abstinence, like clearer thinking,
a better ability to recognize substance use
triggers, and more time to experience the
positive feeling of living without substance use
(BCTDT, 2016).
•
Tapering down. This approach has been
widely used with people who smoke to reduce
physical dependence and cravings before the
quit date and is an option for some substances
like alcohol or cannabis. This approach consists
of setting increasingly lower daily and weekly
limits on use of the substance while working
toward a long-range goal of abstinence.
The client keeps careful daily records of
consumption and schedules sessions with the
counselor as needed. Tapering off opioids,
benzodiazepines, or multiple substances
should be done under medical supervision.
•
Trial moderation. Trial moderation (i.e., clients
try to reduce substance use with careful
monitoring) may be the only acceptable goal
for some clients who are in Precontemplation.
Don’t assume that clients will fail at moderation;
however, if the moderation experiment fails
after a reasonable effort, try to get clients to
reconsider abstinence as a change goal. Clients
can gain insight into their ability to reduce
their substance use, and many will ultimately
decide to abstain if they cannot reduce their
use without negative consequences. Research
indicates that clients whose goal is moderation
have larger social networks of people who drink
daily (Gueorguieva et al., 2014). Therefore, you
should address clients’ drinking social network
as a potential barrier to moderation as a
long-term goal.
Develop a Change Plan
Your final step in readying the client to act
is to work with him or her in creating a plan
for change. (Chapter 3 provides a summary of
MI-specific strategies for developing a change
plan.) Think of a change plan as a roadmap for
the client to reach his or her change goals. A solid
plan for change enhances the client’s self-efficacy
and provides an opportunity to consider potential
barriers and the likely outcomes of each change
strategy. As mentioned in Chapter 3, some clients
need no structured change plan.
Use these strategies to work with clients to
create a sound change plan:
•
Elicit change strategies from the client.
•
Offer a menu of change options.
•
Negotiate a behavioral contract.
•
Explore and lower barriers to action.
•
Enlist social support.
Chapter 6 99

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Elicit Change Strategies From the Client
Work with clients to develop a change plan by
eliciting their own ideas about what will work
for them. This approach is a particularly helpful
if clients have made past attempts to address
substance use behaviors or have been in treatment
before. For example, you might begin with a
reflection of commitment talk and follow with
an open question: “You clearly think that giving
up cocaine is the best thing for you right now.
What steps do you think you can take to reach
thisgoal?”
Help clients create plans to match their concerns
and goals. Plans will differ among clients:
•
The plan can be very general or very specific
and can be short term or long term.
•
Some clients can commit only to a very limited
plan, like going home, thinking about change,
and returning on a specific date to talk further.
Even a small, short-term plan like this can
include specific steps for helping clients avoid
high-risk situations as well as identifying specific
coping strategies.
•
Some plans are very simple, such as stating only
that clients will enter outpatient treatment and
attend an Alcoholics Anonymous (AA) meeting
every day.
•
Other plans include details (e.g., transportation
to treatment, new ways to spend weekends).
•
Many plans include specific steps to overcome
anticipated barriers to success (Exhibit 6.3).
Some plans lay out a sequence of steps. For
example, working mothers with children who
must enter inpatient treatment may develop a
sequenced plan for arranging for child care.
100 Chapter 6

TIP 35Chapter 6—From Preparation to Action: Initiating Change
EXHIBIT 6.3. Change Plan Worksheet
The most important reasons I want to make this change are:
My main goals for myself in making this change are:
I plan to do these things to reach my goals:
Specific action When?
The first steps I plan to take in changing are:
Other people could help me in changing in these ways:
Person Possible ways he or she can help
These are some possible obstacles to change and ways I could handle them:
Possible obstacles to change How to respond
I will know that my plan is working when I see these results:
Source: Miller & Rollnick, 2002. Motivational Interviewing: Preparing People for Change (2nd ed). Adapted with
permission from Guildford Press.
Chapter 6 101

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Create a change plan using a joint process in
which you and the client work together. One of
your most important tasks is to ensure that the plan
is realistic and can be carried out. When the client
offers a plan that seems unrealistic, too ambitious,
or not ambitious enough, use shared decision
making to rework the plan. The following areas are
often part of such discussions:
•
Intensity and amount of help needed.
Encourage participation in community-based
recovery support groups (e.g., AA, Narcotics
Anonymous [NA], SMART Recovery, Women
for Sobriety), enrolling in intensive outpatient
treatment (IOP), or entering a 2-year
therapeutic community.
•
Timeframe. Choose a short-term rather than a
long-term plan and a start date for the plan.
•
Available social support. Discuss who will be
involved in treatment (e.g., family, Women
for Sobriety members, community members),
where it will take place (e.g., at home, in the
community), and when it will occur (e.g., after
work, weekends, twice a week).
•
The order of subgoals and strategies or steps
in the plan. For example:
1. Stop dealing marijuana.
2. Stop smoking marijuana.
3. Call friends or family to tell them about
the plan.
4. Visit friends or family who know about
the plan.
5. Learn relaxation techniques.
6. Use relaxation techniques when feeling
stressed at work.
•
Ways to address multiple problems.
Consider legal, financial, and health problems,
among others.
Clients may ask you for information and advice
about specific steps to add to the plan. You should:
•
Ask permission to offer advice.
•
Use the Elicit-Provide-Elicit (EPE) approach to
keep the client in the center of the conversation
(see the section “Developing discrepancy: A
values conversation” in Chapter 3).
•
Provide accurate and specific facts, and always
ask whether they understand them.
•
Elicit responses to such information by asking,
“What do you think about this?”
The last step in EPE is key to completing the
information exchange between you and the client.
How specific should you be when clients ask
what you think they should do? Providing your
best advice is an important part of your role. It
is also appropriate to share your own views and
opinions, although it is helpful to “soften” your
statements and give clients permission to disagree.
For example, you might soften your suggestion by
saying, “This may or may not work for you, but a
lot of people find it helpful to go to NA meetings
to meet others who are trying to stay away
from cocaine.” Other techniques of MI, such as
developing discrepancy, empathizing, and avoiding
arguments, also are useful during this process.
The Change Plan Worksheet in Exhibit 6.3 helps
clients focus their attention on the details of the
plan, increase commitment to change, enlist social
support, and troubleshoot potential roadblocks
tochange.
Use the Importance and Confidence Rulers in
Exhibit 3.9 and Exhibit 3.10 to determine the
client’s readiness and self-efficacy about each
change goal. These tools can help you and the
client determine which goals to address first and
which strategies to begin with. Ideally, the top goal
will be one with higher ratings on both importance
and confidence. If the client rates one goal as high
in importance and low in confidence, focus on
exploring self-efficacy and evoking confidence talk
to prepare the client for taking action.
Oer a Menu of Change Options
Enhance clients’ motivation to take action by
offering them a variety of treatment choices.
Choices can be about treatment options or about
other types of services. For example, clients who
will not go to AA meetings might be willing to
go to a Rational Recovery, SMART Recovery,
or Women for Sobriety group; clients who will
not consider abstinence might be willing to
102 Chapter 6

TIP 35
Chapter 6—From Preparation to Action: Initiating Change
decrease their consumption. Encourage clients
to learn about their options and make informed
choices to enhance their commitment to the
changeplan.
EXPERT COMMENT: TREATMENT
OPTIONS AND RESOURCES
In our alcohol treatment program, I found that
having lists of both community resources and
diverse treatment modules helps counselors
and case managers engage clients, offer
individualized programming, and meet clients’
multiple needs. The following are some options
we offer our clients:
Treatment Module Options
•
Values clarification/decision making
•
Social-skills training (e.g., assertiveness,
communication)
•
Anxiety management/relaxation
•
Anger management
•
Marital and family therapy
•
Adjunctive medication (i.e., disulfiram,
naltrexone, or acamprosate)
•
Problem-solving groups
•
Intensive group therapy
Community Treatment Resources
•
Halfway houses
•
Support groups (e.g., AA, NA, Rational Recovery,
SMART Recovery, Women for Sobriety)
•
Social services (e.g., child care, vocational
rehabilitation, food, shelter)
•
Medical care
•
Transportation
•
Legal services
•
Psychiatric services
•
Academic and technical schools
Carlo C. DiClemente, Ph.D., Consensus Panel Member
Know your community’s treatment facilities and
resources. This helps you provide clients with
suitable options and makes you an invaluable
resource for clients. Offer clients information on:
•
Specific contact people.
•
Program graduates.
•
Typical space availability.
•
Funding issues.
•
Eligibility criteria.
•
Program rules and characteristics.
•
Community resources in other service areas,
such as:
- Food banks
-
Job training programs
- Special programs for clients with co-occurring
medical and mental disorders
-
Safe shelters for clients experiencing intimate
partner violence
In addition, knowledge about clients’ resources,
insurance coverage, job situation, parenting
responsibilities, and other factors is crucial in
considering options. Initial assessment information
also helps establish treatment options and
priorities.
When discussing treatment options with clients,
be sure to:
•
Provide basic information in simple language
about levels, intensities, and appropriateness
ofcare.
•
Avoid professional jargon and technical terms
for treatment types or philosophies.
•
Limit options to several that are appropriate,
and describe these, one at a time, in
language that is understandable and matches
clients’concerns.
•
Describe the purpose of a particular treatment,
how it works, and what clients can expect.
•
Ask clients to wait to make a decision about
treatment until they understand all the options.
•
Ask clients if they have questions, and ask their
opinions about how to handle each option.
Chapter 6 103

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
•
Review the concept of the SOC; note that
it is common for people to go through the
stages several times as they move closer to
maintaining substance use behavior change and
stable recovery.
•
Remind clients that not completing a treatment
program and returning to substance use are not
failures, but opportunities to reevaluate which
change strategies are working or not working.
•
Point out that, with all the options, they are
certain to find some form of treatment that
willwork.
•
Reassure clients that you are willing to work with
them until they find the right choice.
Exhibit 6.4 provides a change-planning strategy for
situations with many possible change options.
EXHIBIT 6.4. Mapping a Path for Change When There Are Multiple
Options
•
Confirm the change goal. If there are action steps to meet the change goal, decide which step to take
first. For example, the client’s goal might be to stop drinking completely. Some action steps might
include talking with a healthcare provider about medication, going to an AA meeting, and telling a
spouse about the decision. Which step does the client think is most important?
•
Make a list of the change options available to the client (e.g., inpatient treatment, community-based
recovery support groups, IOP treatment, a sober living house or therapeutic community, medication-
assisted treatment).
•
Elicit the client’s feelings, preferences, or both on the best way to proceed. For example, ask, “Here
are the different options we have discussed that might work for you. Which one do you like the most?”
You can also discuss the pros and cons of different options (i.e., perform a decisional balance).
•
Summarize the plan and strengthen commitment. Summarize the action steps and change goal, then
evoke and reflect CAT (Commitment, Activation, and Taking steps) change talk.
•
Troubleshoot. Explore barriers to taking steps; raise any concerns about how realistic the plan is. Avoid
the expert trap (see Chapter 3), and elicit the client’s own ideas about how to manage barriers to change.
Carlo C. DiClemente, Ph.D., Consensus Panel Member
Negotiate a Behavioral Contract
Develop a written or oral contract to help clients
start working on their change plans. A contract is
a formal agreement between two parties. Clients
may choose to make a signed statement at the
bottom of the Change Plan Worksheet or may
prefer a separate document. Be sure to:
•
Explain that others have found contracts useful
at this stage, and invite them to try writing one.
•
Avoid writing contracts for clients. Composing
and signing it is a small but important
ritual of “going public” that can enhance
commitment (Connors, DiClemente, Velasquez,
& Donovan,2013).
•
Encourage clients to use their own words.
•
Be flexible. With some clients, a handshake
is a good substitute for a written contract,
particularly with clients who have challenges
with reading and writing or whose first language
is not English.
Establishing a contract raises issues for discussion
about the client’s reasons for change. What
parties does the contract involve? Some
contracts include the counselor as a party in the
contract, specifying the counselor’s functions and
responsibilities. Other clients regard the contract as
a promise to themselves, to a spouse, or to other
familymembers.
104 Chapter 6

TIP 35
Chapter 6—From Preparation to Action: Initiating Change
Contracts are often used in treatment programs
that employ behavioral techniques, such as
contingency management (CM). For many
counselors, contracts mean contingencies (i.e.,
rewards and consequences), and programs often
build contingencies into the structure of their
programs. For example, in many methadone
maintenance programs, take-home medications are
contingent on substance-free urinalyses. Rewards
or incentives have been shown to be highly
effective external reinforcers. For instance, CM
rewards are effective in reducing use and misuse of
a range of substances including alcohol, tobacco,
cannabis, and stimulants, as well as polysubstance
use (Aisncough, McNeill, Strang, Calder, & Brose,
2017; Litt, Kadden, & Petry, 2013; Sayegh, Huey,
Zara, & Jhaveri, 2017).
Clients may decide to include contingencies,
especially rewards or positive incentives, in the
contract. Rewards can:
•
Be highly individual.
•
Include enjoyable activities, favorite foods,
desired objects, or rituals and ceremonies, all
of which can be powerful objective markers of
change and reinforcers of commitment.
•
Be tied to length of abstinence, quit-date
anniversaries, or achievement of subgoals.
For instance:
-
A client may plan an afternoon at a baseball
game with her son to celebrate a month of
abstinence.
-
One client might go out to dinner with
friends after attending his 50th AA meeting.
-
Another client may light a candle at church.
-
Still another client might hike to the top of a
nearby mountain to mark an improvement in
energy and health.
Explore and Lower Barriers to Action
One category in the Change Plan Worksheet
in Exhibit 6.3 addresses possible obstacles to
change and ways to handle them. Identifying
barriers to action is an important part of the
change plan. Potential roadblocks to taking action
on change goals might include:
•
A lack of non-substance–using social supports.
•
Unsupportive family members.
•
Co-occurring medical or mental disorders.
•
Distressing side effects from medication-assisted
treatment or psychiatric medications.
•
Physical cravings or withdrawal symptoms.
•
Legal issues, money-related problems, or both.
•
Lack of child care.
•
Transportation issues.
•
A lack of cultural responsiveness of some
agencies, programs, or services.
Clients can predict some barriers better than
you can, so allow them to identify and discuss
possible problems. Specifically:
•
Do not try to predict everything that could
go wrong.
•
Focus on events or situations that are likely to
be problematic.
•
Build alternatives and solutions into the plan.
•
Before offering advice, explore clients’ ideas
about how they might handle issues as
theyarise.
•
Explore the ways clients may have overcome
these or similar barriers in the past. This is a way
to open a conversation about their strengths
and coping skills.
Some problems are evident immediately. For
instance, a highly motivated client may plan to
attend an IOP treatment program 50 miles away
3 times a week, even though this requires bus
and train rides and late-night travel. Explore the
pros and cons of this part of the change plan with
the client, and brainstorm alternative solutions,
like finding a program closer to home or a family
member, case manager, peer support specialist,
or program volunteer who can drive the client
to the program. Remember, the change plan
should include strategies that are accessible,
acceptable, and appropriate for each client.
You may need to refer clients to another
treatment program or other services following
initial consultation or evaluation, but this too
is another common barrier to action. When you
refer clients:
Chapter 6 105

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
•
Ensure they have information about how to get
to the program, whom and when to telephone,
and what to expect on the call (e.g., what type
of personal information may be requested).
•
Give them any “insider information” you have
about the program or provider, which can
reduce clients’ anxiety and makes the process
easier. For example, you may know that the
receptionist at the program is a friendly person
or that many people get lost by entering the
building on the wrong side or that a nearby
diner serves good food.
•
Use active linkage and referral interventions,
which enhance client engagement and retention
in SUD treatment and ancillary services and
improve outcomes (Rapp, Van Den Noortgate,
Broekaert, & Vanderplasschen, 2014). Strategies
for active referral procedures include:
-
Helping the client make the telephone call
to set up the intake appointment at the
chosen program. Some clients may want
to make the phone call from your office;
others might wish to call from home and
call you later to tell you that they made an
appointment. Some clients prefer to think
things over first and make the call from your
office at the next session.
-
Following up with clients and the program,
if possible and with client permission, to
ensure that clients are connected to the new
service.
- Offering a “warm handoff,” if possible,
which involves introducing clients to the new
provider.
- Linking clients to a case manager, peer
recovery support specialist, program
alumnus, or community-based recovery
support group volunteer to act as a liaison
and actively engage clients in treatment
programs; social, legal, or employment
services; or community-based recovery
support programs.
Enlist Social Support
Help clients enlist social support and build or
enhance social networks that support recovery
from SUDs. Positive social support for substance
use behavior change is an important factor in
clients’ initiating and sustaining behavior change
(Black & Chung, 2014; Fergie et al., 2018; Rhoades
et al., 2018).
As a counselor, you are a central support for
clients, but you cannot provide all the support
they need. In general, a supportive person is
someone who will listen and not be judgmental.
This supportive person should have a helpful
and encouraging attitude toward clients. Ideally,
this person does not use or misuse substances
and understands the processes of addiction and
change. The Change Plan Worksheet (Exhibit 6.3)
includes space for listing supportive individuals
and describing how they can help. As discussed in
Chapter 4, concerned significant others can offer
support by learning some MI skills (e.g., offering
simple reflective listening responses, becoming
effective partners in change).
Encourage clients to include social support
strategies in their change plans. These include:
•
Engaging in activities with friends that don’t
involve substance use. Social support often
entails participating in non-substance use
activities, so close friends with whom clients
have a history of shared interests other than
substance use are good candidates for this
helpful role. Members of social groups who
drink and use drugs are not likely to offer the
support clients need in recovery.
•
Repairing or resuming connections with
supportive family members and significant
others. Clients can find supportive people
among their family members and close
friends as well as in faith-based and spiritual
organizations, recreational centers, and
community volunteer organizations. To make
these connections, encourage clients to explore
and discuss a time in their lives before substance
use became a central focus. Ask them what gave
meaning to their lives at that time.
106 Chapter 6

TIP 35
Chapter 6—From Preparation to Action: Initiating Change
•
Participating in AA or other recovery support
groups. Recovery groups provide clients with
social support for behavior change, positive
role models of recovery, recovering friendship
networks, and hope that recovery is possible.
Research confirms that participation in AA
is associated with positive alcohol-related,
psychological, and social outcomes (Humphreys,
Blodgett, & Wagner, 2014).
•
Connecting with addiction-focused peer
support. Peer recovery support specialists
can be recovery role models and an important
source of social support for clients. Client
participation in peer recovery support services
with a peer specialist leads to positive
social support and improved substance use
outcomes, including decreased alcohol use and
hospitalizations as well as better adherence
to treatment goals after discharge (Bassuk,
Hanson, Greene, Richard, & Laudet, 2016).
Oxford Houses and similar sober living housing
options have built-in social support systems.
•
Connecting clients with a case manager.
For some clients, especially those with
chronic medical or serious mental illness, case
management teams provide a sense of safety,
structure, and support. A case manager can also
actively link clients to community-based social
services, federal and state financial assistance,
and other ancillary services that support clients’
recovery efforts.
When helping clients enlist social support, be
particularly alert for clients who have limited
social skills or social networks. Some clients may
have to learn social skills and ways to structure
leisure time. Add social skill-building steps into the
change plan. Some clients may not be connected
to any social network that is not organized around
substance use. Furthermore, addiction may have
so narrowed their focus to the point where they
have trouble recalling activities that once held
their interest or appealed to them. However, most
people have unfulfilled desires to pursue an activity
at some time in their lives. Ask about these wishes.
One client may want to learn ballroom dancing,
another to learn a martial art, or still another to
take a creative writing class. Planning for change
can be a particularly productive time for clients to
reconnect with this desire to find fulfilling activities,
and seeking such activities provides opportunities
for making new friends.
Clients with a carefully drafted change plan,
knowledge of both high-risk situations and
potential barriers to getting started, and a group
of supportive friends, family members, or recovery
supports should be fully prepared and ready to
move into the Action stage.
Support the Client’s Action Steps
DiClemente (2018) describes four main tasks for
client in the Action stage of the SOC:
1. Breaking free of the addiction using the
strategies in the change plan
2. Continuing commitment to change and
establishing a new pattern of behavior
3. Managing internal/external barriers to change
(e.g., physical cravings, lack of positive social
support)
4. Revising and refining the change plan
Your role is to continue using motivational
counseling approaches to support the client
in completing these tasks and moving into the
Maintenance stage and stable recovery. To
support clients in breaking free of substance use
behaviors:
•
Encourage clients to set a specific start date
for each behavior change (e.g., a smoking
quit date, date to enter an inpatient addiction
treatment program). Setting a start date
increases commitment.
•
Help clients create rituals that symbolize them
leaving old behaviors behind. For example,
some clients may make a ritual of burning
or disposing of substance paraphernalia,
cigarettes, beer mugs, or liquor. Support
clients in creating personally meaningful
rituals. As mentioned previously, picking up a
chip at an AA meeting is a ritual that supports
clients’ action steps toward abstinence and a
newlifestyle.
Chapter 6 107

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
To reinforce clients’ commitment to change:
•
Continue to evoke and reflect CAT change talk
in your ongoing conversations with clients.
•
Use reflective listening, summaries,
andaffirmations.
•
Manage barriers to change by identifying those
barriers (as described above in the section
“Explore and Lower Barriers to Action”),
working with clients to brainstorm personally
relevant strategies for lowering or reducing the
impact of those barriers, and offering a menu
of treatment options. For example, if a client
experiences intense alcohol or drug cravings,
you might explore the possibility of referring
the client to a medical provider for a medication
evaluation, encouraging participation in a
mindfulness meditation group, or both.
•
Evaluate, revise, and refine the change plan as
the final step in the Action stage.
Evaluate the Change Plan
Your goal of this stage of the change cycle is
to help the client sustain successful actions
for a long enough time that he or she gains
stability and moves into Maintenance (Connors
et al., 2013). It is not likely that you and the client
will be able to predict all of the issues that will
come up as the client initiates the change plan.
The client’s circumstances likely will change (e.g.,
a spouse might file for divorce), unanticipated
issues arise (e.g., the client’s drug-using social
network might put pressure on the client to
return to drug use), and change strategies may
not turn out to work well for the client (e.g., the
client loses his or her driver’s license and has to
find alternative transportation to NA meetings).
These unanticipated issues can become a barrier
to sustaining change plan actions and may require
revisions to the change plan (Connors et al., 2013).
Your task is to work with the client at each
encounter to evaluate the change plan and revise
it as necessary. Ask the client, “What’s working?”
and “What’s not working?” Miller and Rollnick
(2013) suggest that counselors think about this
process as “flexible revisiting.” The same strategies
used in the planning process of MI apply to revising
the change plan, including confirming the change
goal, eliciting the client’s ideas about how to
change, offering a menu of options, summarizing
the change plan, and exploring obstacles (see
Chapter 3). Some strategies for change may need
to be removed, whereas others can be adjusted.
For example, one client’s goal is to quit drinking,
and her action steps include attending three AA
meetings a week, including one women’s meeting.
The client stops going to the women’s meeting
because one of the regular attendees is a coworker
who likes to gossip, and the client is afraid that the
coworker will break her anonymity at work. Your
first step is to identify the issue, and then elicit the
client’s ideas about what else might work for her.
Open questions to start this process if a change
strategy is not working include (Miller &
Rollnick, 2013):
• "What now?"
• "What else might work?"
• "What’s your next step?"
Avoid jumping in too quickly with your own ideas.
Adjusting a change plan, like creating the initial
change plan, is a joint process between you and
the client; the client’s own ideas and resources are
key (Miller & Rollnick, 2013). Finally, summarize the
new change strategy and explore how the client
might respond to any new obstacles that might
come up while initiating the revised change plan
(Miller & Rollnick, 2013).
Conclusion
As clients move from contemplating change into
preparing for change, your task is to continue to
reinforce clients’ commitment to change and take
action. You can support clients to take this next
step by working together to develop a change
plan, imagining possible barriers to change that
might occur, and enlisting social support for taking
action. Change plans are client driven and based
on clients’ own goals. Continue to use motivational
counseling strategies to help clients identify and
clarify their change goals, develop a change
plan, and refine and revise the change plan as
needed. Your role is to help clients sustain their
goals for change, gain stability, and move into the
Maintenance stage of the SOC.
108 Chapter 6

Chapter 7—From Action to Maintenance:
Stabilizing Change
To become habitual, the new behavior must become integrated into
the individual’s lifestyle. This is the task of the Maintenance stage of
change. During this stage, the new behavior pattern becomes automatic,
requiring less thought or effort to sustain it…. However, even during
Maintenance there is an ever-present danger of reverting to the old
pattern. In fact, the new behavior becomes fully maintained only when
there is little or no energy or effort needed to continue it and the
individual can terminate the cycle of change.”
—DiClemente, 2018, p. 31
KEY MESSAGES
TIP 35
ENHANCING MOTIVATION FOR CHANGE IN
SUBSTANCE USE DISORDER TREATMENT
•
In the Maintenance stage of the Stages of Change (SOC) model, clients
work toward stabilizing the substance use behavioral changes they
have made.
• You can support clients in the Maintenance stage by helping them stay
motivated, identify triggers that might lead to a return to substance
misuse, and develop a plan for coping with situational triggers when
they arise.
• Relapse prevention counseling (RPC) using a motivational counseling
style can prevent a return to substance misuse and help clients reenter
the cycle of change quickly if they do return to substance use.
Maintaining change is often more challenging than
taking one’s first steps toward change. Chapter
7 addresses ways that you can use motivational
strategies to help clients maintain their success in
recovering from substance use disorders (SUDs).
It presents strategies for stabilizing change,
supporting lifestyle changes, managing setbacks
during Maintenance, and helping clients reenter
the cycle of change if a relapse or a return to
substance misuse occurs.
Using a motivational counseling style with clients in
the Precontemplation through Preparation stages
helps them move toward initiating behavioral
change. Yet when clients do take action, they
face the reality of stopping or reducing substance
use. This obstacle is more difficult than just
contemplating action. Once clients have decided
to take action, they are on the downslope of the
Motivational Interviewing (MI) Hill of Ambivalence
presented in Exhibit 5.2.
109

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
EXHIBIT 7.1. Counseling Strategies for Action and Relapse
SOC CLIENT MOTIVATION COUNSELOR FOCUS COUNSELING STRATEGIES
Maintenance The client has
achieved initial goals,
such as abstinence,
reduced substance
use behaviors, or
entering treatment,
and is now working to
maintain these goals.
•
Stabilize
clientchange.
•
Support the client’s
lifestyle changes.
•
Engage and retain the client in
SUD treatment.
•
Create a coping plan.
•
Identify new behaviors that
reinforce change.
•
Identify recovery capital (RC).
•
Reinforce family and social support.
Relapse and
Recycle
The client returns to
substance misuse and
temporarily exits the
change cycle.
Help the client
reenter the change
cycle.
•
Provide RPC.
•
Reenter the cycle of change.
Stabilize Client Change
One of the key change goals for many clients
is entry into a specialized addiction treatment
program. Options include outpatient, intensive
outpatient, inpatient, and short- or long-term
residential treatment; methadone maintenance
treatment; and office-based opioid treatment.
Making the decision to enter treatment is an action
step. To maintain that behavior change, you
should engage and retain clients in treatment.
Unfortunately, many clients enter and stop
treatment before they achieve their other change
goals. Engaging and retaining clients in treatment
are important strategies for stabilizing substance
use behavior change. Other stabilization strategies
include identifying high-risk situations and triggers
for substance use, creating a coping plan, and
helping clients practice and use new coping skills.
Engage and Retain Clients in
SUDTreatment
You play an important role in preventing clients
from stopping or dropping out of treatment
before completion—a major concern for SUD
treatment providers. A consistent predictor of
positive client outcomes across SUD treatment
services is treatment completion (Brorson, Arnevik,
Rand-Hendriksen, & Duckert, 2013). Longer lengths
of stay in treatment are consistent indicators of
reliable behavior change and positive treatment
outcomes (Running Bear, Beals, Novins, & Manson,
2017; Jason, Salina, & Ram, 2016; Turner &
Deanne, 2016).
Causes of stopping treatment early vary:
•
For some clients, dropping out, missing
appointments, or nonadherence with other
aspects of the treatment program are clear
messages of disappointment, hopelessness, or
changes of heart.
•
Some clients drop out of treatment because
their treatment or behavior change goals
don’t match those of the counselor or
program (Connors, DiClemente, Velasquez, &
Donovan,2013).
•
Strong evidence shows that low treatment
alliance is linked to client dropout in SUD
treatment (Brorson et al., 2013).
110 Chapter 7

TIP 35
Chapter 7—From Action to Maintenance: Stabilizing Change
•
Clients with co-occurring substance use and
mental disorders (CODs) and those with
cognitive problems are especially likely to
end treatment early (Running Bear et al., 2017;
Brorson et al., 2013; Krawczyk et al., 2017;
Teeson et al., 2015). For more information about
engaging clients with CODs, see Treatment
Improvement Protocol (TIP) 42: Substance
Abuse Treatment for Persons With Co-Occurring
Disorders (Substance Abuse and Mental Health
Services Administration [SAMHSA], 2013).
•
For others, dropping out may mean they have
successfully changed their substance use
behaviors on their own (Connors et al., 2013).
•
Perhaps the strongest predictor of dropout
in SUD treatment is addiction severity at
treatment entry. For example, one study of
men and women in treatment for posttraumatic
stress disorder found that a diagnosis of
both an alcohol use disorder (AUD) and a
drug use disorder strongly predicted higher
dropout rates, drug use severity predicted
worse adherence to treatment, and drug use
severity or a lifetime diagnosis of an alcohol or
drug use disorder predicted worse treatment
outcomes (Bedard-Gilligan, Garcia, Zoellner, &
Feeny2018).
MI and motivational enhancement therapy are
effective in improving treatment adherence
to and retention in SUD treatment for certain
substances (e.g., cocaine), especially for clients
who enter treatment with low motivation to change
(DiClemente, Corno, Graydon, Wiprovnick, &
Knoblach, 2017). Motivational-based strategies
that increase client engagement and retention
in SUD treatment and reduce client dropout are
addressed below.
Build a strong counseling alliance
As noted in Chapters 3 and 4, your counseling
style is an important element for establishing
rapport and building a trusting relationship
with clients. MI strategies appropriate during the
engaging process (see Chapter 3) help you connect
with and understand clients’ unique perspectives
and personal values. For example, empathy, as
expressed through reflective listening, is key
in developing rapport with clients and predicts
positive treatment alliance and client outcomes
(Anderson, Crowley, Himawan, Holmberg, &
Uhlin, 2016; Miller & Moyers, 2015; Moyers, 2014;
Moyers, Houck, Rice, Longabaugh, & Miller, 2016).
To help clients confide in you, make them feel
comfortable and safe within the treatment
setting. Clients’ natural reactions may depend
on such factors as their gender, age, race,
ethnicity, sexual or gender identity, and previous
experience. For example, some ethnic or racial
groups may be hesitant to enter treatment based
on negative life experiences, discrimination, or
problems encountered with earlier episodes of
treatment. Initially, for these clients and others who
have been marginalized or experienced trauma,
safety in the treatment setting is a particularly
important issue. (See the section “Special
Applications of Motivational Interventions” in
Chapter 2 for culturally responsive ways to engage
clients in treatment.) You should also consider
gender differences regarding the importance
of establishing a strong counseling alliance.
For example, one study found that women
who received intensive MI over nine sessions
(versus a single session) showed significantly
higher counseling alliance and better alcohol use
outcomes than men did (Korcha, Polcin, Evans,
Bond, & Galloway, 2015).
Inform clients about program rules and
expectations
Clients must become acquainted with you and the
treatment program. To accomplish this:
•
Tell clients explicitly what treatment involves,
what is expected of them, and what rules they
must follow. If clients have not been prepared
by a referring source, review exactly what will
happen in treatment to eliminate and confusion.
•
Use language clients understand.
•
Encourage questions, and provide clarification
of anything that seems confusing.
•
Explain what information must be reported
to a referring agency that has mandated the
treatment, including what it means to consent
to release of information. This discussion is part
of the regular informed consent process that
should happen when clients enter treatment.
Chapter 7 111

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Address client expectations about treatment
One of the first things you should discuss with
new clients is their expectations about the
treatment process. Ask clients about their past
treatment experiences and what they think the
current treatment experience will be like. Clients
who are in SUD treatment for the first time
do not know much about what the counseling
process entails and tend to underestimate the
level of motivation, personal commitment, and
responsibility required to take action to change
(Raylu & Kaur, 2012). This suggests that clients
without previous SUD treatment experience
benefit from discussions about treatment
expectations and the importance of being open
to the counseling process (Raylu & Kaur, 2012).
Ask clients for permission to explore their
treatment expectations. Ask for elaboration
on their initial impressions as well as their
expectations, hopes, and fears. Some common
client fears about treatment are that:
•
The counselor will be confrontational and force
treatment goals on them.
•
Treatment will take too long and require the
client to give up too much.
•
The rules are too strict, and clients will be
discharged for the smallest mistake.
•
Medication will not be prescribed for painful
withdrawal symptoms.
•
The program does not understand women,
members of different ethnic/racial groups,
or people who use certain substances or
combinations of substances.
•
A spouse or other family member will be
required to participate.
Many clients have negative expectations based
on previous treatment. A motivational approach
can help you understand their concerns, which is
especially important for clients who feel forced into
treatment by someone else (e.g., by an employer,
the court, a spouse). When clients have unrealistic
expectations, like believing the treatment program
will get their driver’s license reinstated or restore
a marriage, be open and honest about what the
program can and cannot do. Use OARS (Open
questions, Affirmations, Reflective listening, and
Summarization) to explore negative expectations
about treatment and the client’s hopes about
what treatment can accomplish.
Explore and resolve barriers to
completingtreatment
Work with clients to brainstorm and explore
solutions to common issues. As treatment
progresses, clients may experience barriers
that slow their success and could result in them
stopping treatment early. Sometimes clients do
not feel ready to participate or suddenly rethink
their decision to enter treatment. Rethinking
participation in treatment is a sign that clients
may have returned to the Contemplation stage.
If this is the case, reengage the client using the
motivational strategies discussed in Chapter 5.
If clients are clearly not ready to participate in
specialized treatment, leave the door open for
them to return at another time, and provide a
menu of options for referral to other services.
During treatment, clients may have negative
reactions or embarrassing moments when they:
•
Share with you more than they had planned
to share.
•
Experience intense or overwhelming emotions.
•
Realize the mismatch in information they have
given you.
•
Realize how they have hurt others or their
own futures.
You can deal with these difficult reactions by:
•
Anticipating and discussing such problems
before they occur.
•
Letting clients know that these reactions are a
normal part of the recovery process.
•
Working with clients to develop a plan to handle
these difficult reactions.
•
Exploring previous treatment, including their
reasons for leaving early and how to better
match current treatment to their needs.
112 Chapter 7

TIP 35
Chapter 7—From Action to Maintenance: Stabilizing Change
If this is the client’s first treatment experience,
get his or her ideas about what might be a
roadblock to completing treatment:
•
Start with an affirmation, and ask an
openquestion:
•
“It took a lot of determination and effort for you
to be here. Good for you! Sometimes things
come up during counseling sessions that are
difficult and might make you wonder if staying
in treatment is worth the effort. That’s normal.
What are some things you can imagine that
might make it challenging for you to follow
through with your commitment to completing
the program?”
•
Follow with reflective listening responses.
•
Ask the client for ideas about strategies to deal
with ambivalence about staying in treatment.
•
Be culturally aware as you help the client
manage or try to prevent common difficulties.
Increase congruence between intrinsic and
extrinsic motivation
Exploring with clients their internal and external
reasons for entering and staying in treatment
can help reduce their chances of early dropout.
Self-determination theory proposes that intrinsic
(internal) motivation may have a stronger impact
on maintaining behavior change than extrinsic
(external) motivation, which may be more effective
in helping clients initiate behavior change. A
meta-analysis of MI (which emphasizes increasing
internal motivation) and contingency management
(which emphasizes external motivators) found that
both approaches were effective in reducing use of
a wide variety of substances (Sayegh, Huey, Zara,
& Jhaveri, 2017). The analysis also found evidence
to suggest that extrinsically focused counseling
strategies produced short-term treatment effects,
whereas intrinsically focused counseling strategies
produced long-term treatment effects.
Help clients increase congruence, or agreement,
between internal and external motivations. You can
explore external motivations clients may view as
forced or unwanted and reframe them as positive
reasons that align with their internal reasons for
staying in treatment to increase congruence.
Explore client nonadherence
Clients’ nonadherence to treatment is often a sign
that they are unhappy with the counseling process.
For example, clients may miss appointments, arrive
late, fail to complete required forms, or remain
silent when asked to participate. Any occurrence of
such behavior provides an opportunity to discuss
the reasons for the behavior and learn from it.
Often clients are expressing their ambivalence
and are not ready to make a change. Explore the
behavior in a nonjudgmental, problem-solving
manner that helps you discover whether the
behavior was intentional or whether a reasonable
explanation for the behavior exists. For example,
clients might be late as a sign of “rebelling”
against what they think will be a stressful session,
or it could simply be that their car broke down.
As with all motivational strategies, you need to
draw out clients’ views of and thoughts about
the event. Generally, if you can get clients to
voice their frustrations, they will come up with the
answers themselves. Asking a question such as
“What do you think is getting in the way of being
here on time?” is likely to open a dialog. Respond
with reflective listening, open questions that evoke
change talk, and affirmations. For example, you
might ask, “How does being late fit or not fit with
your goal of getting the most out of this treatment
experience?” Remember to praise the client for
simply getting to the session.
Missed appointments or not showing up for
scheduled activities require a more proactive
approach. Some strategies for responding to
missed appointments are listed in Exhibit 7.2
(nextpage).
Chapter 7 113

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
EXHIBIT 7.2. Options for
Responding to a Missed
Appointment
•
Place a telephone call.
•
Send a text message.
•
Write an email.
•
Mail a personal letter.
•
Contact preapproved relatives or significant or
concerned others.
•
Pay the client a personal visit (if appropriate for
your role and agency policy).
•
Contact the referral source.
As part of the informed consent process, find out
from clients which contact methods they prefer,
discuss confidentiality and security issues (e.g.,
protection of clients’ personal health information,
agency policies regarding email and texting),
and obtain appropriate releases to contact other
individuals or organizations.
Reach out and follow up
You might need to reach out to the client
following certain events, such as a wedding,
birth of a child, traumatic injury or illness, or
several missed appointments. Doing so shows
your personal concern and genuine interest
in protecting the counseling relationship and
enhancing the recovery process. As mentioned
previously, explore the client’s preferred
methods for you to reach out if he or she misses
appointments or drops out of treatment. Make sure
to get written consent to contact relatives, friends,
or others. In addition, you should be aware of and
abide by the client’s cultural rules and values about
having contact outside the SUD setting.
If clients complete their initial treatment
goals and end treatment, follow up with
them periodically. Setbacks, particularly
with maintenance of substance use behavior
change, often occurs between 3 and 6 months
after treatment, and you should plan regular
follow-up sessions with clients to reinforce and
support maintenance of treatment gains (Miller,
Forcehimes, & Zweben, 2011).
Create a Coping Plan
To help clients move fully into Maintenance, help
them stabilize actual change in their substance
use behavior. Support clients’ stabilization by
helping them develop a coping plan that lists
strategies for managing thoughts, urges, and
impulses to drink or use drugs. This planning
process includes:
•
Assessing and enhancing self-efficacy.
•
Identifying high-risk situations that trigger the
impulse to drink or use drugs.
•
Identifying coping strategies to manage
high-risk situations.
•
Helping clients practice and use effective
coping skills.
Assess and enhance self-ecacy
Help clients improve their self-efficacy. Self-
efficacy is important for changing substance use
behaviors as well as sustaining those changes.
There is a strong relationship between client
self-efficacy and SUD treatment outcomes across
a variety of substances (e.g., alcohol, cannabis,
cocaine) and different counseling approaches.
There is also evidence that a strong counseling
alliance helps clients enhance self-efficacy and
increase positive treatment outcomes for alcohol
use (Kadden & Litt, 2011).
Clients may have high self-efficacy in some
situations and low self-efficacy in others. Several
validated tools can help assess clients’ level of
self-efficacy or confidence in how well they would
cope with the temptation to use substances in
high-risk situations. Scores provide feedback about
clients’ self-efficacy for a specific behavior over a
range of high-risk situations. Some computerized
versions of these instruments generate charts that
present clients’ scores in an easy-to-understand
way. Descriptions of the Situational Confidence
Questionnaire (SCQ)/Brief SCQ (BSCQ) and the
Alcohol Abstinence Self-Efficacy Scale (AASES),
three of the most widely used instruments, follow:
114 Chapter 7

TIP 35
Chapter 7—From Action to Maintenance: Stabilizing Change
•
The SCQ and BSCQ have been used with
people who misuse alcohol. The 100-item SCQ
asks clients to identify their level of confidence
in resisting drinking in 8 circumstances (Breslin,
Sobell, Sobell, & Agrawal, 2000):
-
-
Unpleasant emotions
Physical discomfort
- Testing personal control over substance use
- Urges and temptations to drink
- Pleasant times with others
- Conflicts with others
- Pleasant emotions
-
Social pressure to drink
•
Clients are asked to imagine themselves in each
situation and rate their confidence on a 6-point
scale, ranging from not at all confident (a rating
of 0) to totally confident (a rating of 6), that they
can resist the urge to drink heavily. The BSCQ
is a shortened 8-question form that asks clients
to rate these circumstances using a scale of 0%
to 100%, with 0% indicating not at all confident
and 100% indicating totally confident. The
BSCQ and its scoring instruments are available
in Appendix B.
•
The AASES measures an individual’s self-
efficacy in abstaining from alcohol (DiClemente,
Carbonari, Montgomery, & Hughes, 1994).
Although similar to the SCQ/BSCQ, the AASES
focuses on clients’ confidence in their ability
to abstain from drinking across 20 different
situations. The AASES consists of 20 items and
can be used to assess both the temptation to
drink and the confidence to abstain. The AASES
and its scoring instructions are available in
Appendix B.
By using these tools, clients can better
understand the high-risk situations in which they
have low self-efficacy. This information can be
helpful in setting realistic goals and developing
an individualized coping plan. Clients who
rank many situations as high risk (i.e., low self-
efficacy) may need to identify and develop new
copingstrategies.
•
Expressing confidence in the client’s ability
to change.
•
Reviewing past success with changing substance
use or other health behaviors.
•
Reviewing the client’s current strengths.
•
Using the Confidence Ruler (Exhibit 3.10) to
measure coping strategies.
•
Presenting a menu of coping strategies that
have a high likelihood of success.
Identify high-risk situations and coping
strategies
Another approach to helping clients identify
high-risk situations is to use a structured
interview that identifies the high-risk situation
(i.e., who, where, and when), external triggers (i.e.,
what), and internal triggers (i.e., thoughts, feelings,
and physical cravings) that led to substance use
in the past. Once these situations are identified,
clients explore coping strategies to manage these
triggers that have worked in the past and that
might work now and in the future. Understanding
these triggers helps clients target specific
strategies for coping with these triggers.
Strategies for conducting the interview include
the following:
•
Let the client know the purpose of the
interview, and ask permission to conduct it.
For example, you might say, “It can be helpful
to explore some of the situations when you
drank or used drugs in the past and what led
to your decision to use in those situations.
Sometimes those can be thoughts or feelings
or the situation itself. We sometimes call what
led to substance use internal and external
triggers. Once we know what has ‘triggered’
your drinking or drug use in the past, we can
brainstorm ways to cope with those triggers
now, instead of drinking or using. Is that okay?”
•
Draw a four-column table on a piece of paper
and label the columns High-Risk Situation,
External Triggers, Internal Triggers, and Coping
Strategies as in Exhibit 7.3.
Other strategies to enhance client self-efficacy in
Maintenance include (Miller & Rollnick, 2013):
Chapter 7 115

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
EXHIBIT 7.3. Triggers and Coping Strategies
HIGHRISK
SITUATION
WHO, WHERE,
WHEN
EXTERNAL
TRIGGERS
WHAT
INTERNAL TRIGGERS
THOUGHTS, FEELINGS, IMPULSES,
CRAVINGS
COPING STRATEGIES
Example:
“Watching a football
game with my
drinking buddies.”
Example:
“A beer
commercial
comes on.”
Example:
“My mouth waters, and I think about
how good a beer would taste.”
Example:
“I could go to the
refrigerator and get a
cold soft drink instead
of a beer.”
•
Ask an open question to start the discussion.
“Tell me about situations in which you have
been most likely to drink or use drugs in the
past, or times when you have tended to drink or
use more than expected. These might be when
you were with specific people, in specific places,
or at certain times of day, or perhaps when you
were feeling a particular way.”
•
Elicit ideas from the client about ways he or
she might have resisted temptation to use in
the past.
•
Elicit ideas from the client about strategies
he or she could use now to avoid high-risk
situation or external triggers as well as ways to
manage the internal triggers without resorting
to substance use.
•
Ask the client to elaborate on possible coping
strategies.
•
Use the Confidence Ruler (Exhibit 3.10) to
evaluate the client’s confidence in applying
these coping strategies. Evoke confidence
talk to reinforce and enhance self-efficacy
(seeChapter 3).
As you explore triggers, do not solely use reflective
listening. This technique might accidentally evoke
sustain talk from the client and decrease his or her
commitment to engaging in coping strategies.
Instead, use affirmations and reflective listening
responses to reinforce the client’s commitment
to engaging in coping strategies as an
alternative to substance use.
If the client has difficulty identifying coping
strategies:
•
Offer some ideas that others have found helpful.
•
Brainstorm with the client.
•
Offer a menu of possible coping strategies.
•
Explore with the client which options are more
likely to work as in the examples in Exhibit 7.4.
116 Chapter 7

TIP 35
Chapter 7—From Action to Maintenance: Stabilizing Change
EXHIBIT 7.4. A Menu of Coping Strategies
Coping strategies are not mutually exclusive; different ones can be used at different times. In addition,
not all are equally good; some involve getting uncomfortably close to trigger situations. Here are some
examples of a menu of strategies that might help clients in different high-risk situations.
Example #1: Client X typically uses cocaine whenever his cousin, who uses regularly, drops by the house.
Coping strategies to consider include (1) call the cousin and ask him not to come by anymore; (2) call
the cousin and ask him not to bring cocaine when he visits; (3) if there is a pattern to when the cousin
comes, plan to be out of the house at that time; or (4) if someone else lives in the house, ask him or her
to be present for the cousin’s visit.
Example #2: Client Y typically uses cocaine when she goes with a particular group of friends, one of
whom often brings drugs along. She is particularly vulnerable when they all drink alcohol. Coping
strategies to consider might include (1) go out with a different set of friends; (2) go along with this group
only for activities that do not involve drinking; (3) leave the group as soon as drinking seems imminent;
(4) tell the supplier that she is trying to stay off cocaine and would appreciate not being offered any; or
(5) ask all of her friends, or one especially close friend, to help her out by not using when she is around or
by telling the supplier to stop offering it to her.
Example #3: Client Z typically uses cocaine when feeling tired or stressed. Coping strategies might
include (1) scheduling activities to get more sleep at night, (2) scheduling activities to have 1 hour per day
of relaxation time, (3) learning and practicing specific stress reduction and relaxation techniques, or (4)
learning problem-solving techniques that can reduce stress in high-risk situations.
Use the coping strategies identified in the
structured interview to develop a written coping
plan. This could be as simple as jotting down a few
ideas for managing triggers in high-risk situations
on a file card or it could be as detailed as creating
a change plan using the Change Plan Worksheet in
Exhibit 6.3.
Help the clients practice new coping skills
Just as you would monitor and reevaluate a
change plan with clients, revisit the coping plan,
and modify it as necessary. Ask clients to rehearse
coping strategies in counseling sessions and to try
to implement those strategies in everyday life. For
example, growing evidence shows that practicing
mindfulness is an effective strategy for managing
cravings and urges to use substances (Grant et
al., 2017). If this coping strategy is new to clients,
help them develop a change plan that might
include attending a mindfulness class or group and
practicing mindfulness at home or in a counseling
session that focuses on managing cravings.
Rehearsing new skills reinforces them and helps
build self-efficacy.
Support the Client’s Lifestyle
Changes
Your task in the Maintenance stage is to support
and praise clients’ positive lifestyle and identify
behaviors that reinforce these changes. Clients
must put forth ongoing and sustained effort to
maintain their change of substance use behaviors.
As clients successfully maintain changes, they
develop a strong sense of self-efficacy. They use
less effort to cope with temptations and triggers,
and new behaviors become the norm (DiClemente,
2018). As substance use behavior change becomes
a new lifestyle, the client develops a new sense
of identity. For some, this is expressed in self-
identification as a “nonsmoker” or a “recovering
addict.” For others, the new story of identity is
about becoming an integral member of the family
or community.
Identify New Behaviors that Reinforce
Change
You should examine all areas of clients’ life for
new reinforcers, which should come from multiple
sources and be of various types. A setback in
one area can be counterbalanced by a positive
Chapter 7 117

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
reinforcer from another area. As the motivation for
positive change becomes harder to sustain, clients
need strong reasons for overcoming the challenges
they will face. Help them select positive reinforcers
that will prevail over substance use over time.
Small steps are helpful, but they cannot fill
a whole life. Abstaining from substances is a
sudden change and often leaves a large space in
clients’ lives. You can help clients fill this space by
exploring activities that will support their healthy
new identity such as:
•
Doing volunteer work links clients to the
community. Clients can fill time, decrease
isolation, and improve self-efficacy through this
prosocial activity, making positive contributions
to the community.
•
Becoming involved in 12-Step activities.
Similar to volunteering, this fills a need to be
involved with a group and contributes to a
worthwhile organization.
•
Setting goals to improve work, education,
health, and nutrition.
•
Spending more time with family, significant
others, and friends.
•
Participating in spiritual or cultural activities.
•
Learning new skills or improving old ones in
such areas as sports, art, music, and hobbies.
Identify Recovery Capital
Help clients tap into and build new sources of
positive RC and lessen the impact of negative
sources of RC as a way to support the maintenance
of change. “Recovery capital” refers to internal
and external resources a person draws on to begin
and sustain recovery. Internal resources include,
but are not limited to, values, knowledge, skills,
self-efficacy, and hope. External resources include,
but are not limited to, employment; safe housing;
financial resources; access to health care; and
social, family, spiritual, cultural, and community
supports (Granfield & Cloud, 1999). RC can be
positive (e.g., drug-free social network) or negative
(e.g., drug-using social network) (Hennesey, 2017).
Positive and negative RC interact with each other
in the recovery process and change over time
(Hennessy, 2017). RC is linked with clients’ natural
recovery resources. (See also the “Natural Change”
section in Chapter 1.)
Reinforce Family and Social Support
Family and social support are important sources
of RC. They can help clients permanently break
free from addiction and engage in a new lifestyle
(DiClemente, 2018). Family and friends who are
supportive of the clients’ recovery can be especially
helpful in stabilizing change because they can
reinforce new behavior and provide positive
incentives to continue in recovery. They can involve
clients in new social and recreational activities
and be a source of emotional and financial
support. Other types of support they provide can
be instrumental (e.g., babysitting, carpooling),
romantic, spiritual, and communal (i.e., belonging
to a particular group or community).
Identify different types of social supports that
clients have available to help determine gaps
in their support system and help them build a
larger, more diverse social network. Clients with
more severe AUD tend to have smaller, less diverse
social networks (i.e., supports other than family or
close friends) than those with no history of AUD or
less severe alcohol misuse experiences (Mowbray,
Quinn, & Cranford, 2014). More extensive social
networks in which individuals with addiction
exchange support with one another can help
individuals sustain recovery over time (Panebianco,
Gallupe, Carrington, & Colozzi, 2016). An extended
and diverse social network might comprise:
•
Family members.
•
Friends.
•
Peer support specialists.
•
Members of recovery support groups.
•
Healthcare providers.
•
Employers.
•
12-Step sponsors.
•
Spiritual advisors.
•
Members of a church or spiritual community.
•
Neighbors.
•
Members of community groups.
•
Participants in organized recreational activities.
118 Chapter 7

TIP 35
Chapter 7—From Action to Maintenance: Stabilizing Change
Use motivational counseling strategies to
explore current and potential sources of social
support and how those supports could help
clients maintain recovery and lifestyle changes.
For example, family members can act as a warning
system if they see early signs of possible relapse.
A peer recovery support specialist can link clients
to alcohol- and drug-free recreational events in the
community or other recovery support. Exhibit 7.5
describes a brief clinical scenario with a client who
lacks social support.
EXHIBIT 7.5. Susan’s Story: A Client Lacking Social Support
Client context: Susan is 41 years old and has a long history of AUD and multiple treatment
episodes. The longest period Susan has been able to maintain abstinence from alcohol has been
1 month. She has tried to participate in Alcoholics Anonymous (AA); however, she finds that most
of the meetings she can get to without a car are primarily attended by men, and she does not
feel comfortable there. Susan’s mother has been diagnosed with schizophrenia. Susan reports
that her father has been diagnosed with AUD. Her father sexually abused her for years when she
was a child. Susan is divorced and has only one friend she talks to, infrequently. Her only source
of regular support is her father.
Susan recently participated in an IOP addiction treatment program where she also attended a
Seeking Safety support group for women with histories of trauma. (For more information about
Seeking Safety, see Chapter 6 of TIP 57: Trauma-Informed Care in Behavioral Health Services
[SAMHSA, 2014b].) This is the first treatment experience in which Susan’s history of trauma has
been addressed simultaneously with her AUD. Susan completes the program and is referred to
outpatient counseling. Once she leaves the IOP treatment program, however, her only recovery
support is her outpatient counselor, Arlene.
Counseling strategies: Arlene recognizes that Susan lacks an effective social support network
that can help her maintain the progress she made in the IOP program. Arlene explores Susan’s
recent treatment experience, her prior involvement in AA, and her transportation needs. She
affirms Susan’s persistence in returning to treatment and completing the IOP program and
then elicits from Susan what she thinks was different for her this time in treatment. Susan says
that she felt safe and supported by the women in the Seeking Safety group.
Arlene works with Susan to develop a plan to re-create that experience of support now that she
is back home. The plan includes introducing Susan to a peer recovery support specialist who
can help Susan remove any barriers to becoming more engaged in community-based recovery
support services, like transportation. Arlene also suggests a menu of social support options to
Susan, including a Women for Sobriety group, a small women’s AA meeting, and an outpatient
trauma recovery support group. Finally, Arlene lets Susan know that she is available by phone
and between sessions until Susan has connected with other women who will be part of her
ongoing support network. They discuss the boundaries around between-session contact and
agree on an initial plan for weekly counseling sessions for the next 12 weeks.
Arlene sees that she can’t be Susan’s only source of recovery support. With motivational
counseling strategies, she helps Arlene build a new support network to reinforce her recovery,
maintain her long-term recovery goal of abstinence, and help her heal from trauma and
previous disruptions to her social support network.
Chapter 7 119

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Help the Client Reenter the
Change Cycle
To help clients maintain substance use behavior
change, you must address the issue of relapse.
Historically, the term “relapse” in addiction
treatment had come to mean an all-or-nothing
understanding of clients’ return to substance
use after a period of abstinence and judgment
about their lack of motivation. This TIP uses the
term “relapse” in part because the SOC model
uses the term to describe points in the recovery
process when clients leave the change cycle and
then recycle through the SOC again with more
awareness and a better understanding of how
to reach the Maintenance stage. In addition,
addiction treatment clinical research refers to
relapse prevention as a key counseling approach to
supporting clients’ ongoing recovery maintenance.
A return to substance use after a period of
abstinence does not mean a client has failed
or is no longer in recovery. The consensus
panel of this TIP seeks to reconceptualize the
recurrence of substance use after treatment as a
common aspect of recovery from SUDs based on
well-documented observations:
•
Recurrence of substance use is common.
Although relapse is not technically a stage in the
SOC, it is a normal part of change and recovery
processes.
•
The term “relapse” itself implies only two
possible outcomes—success or failure—that
do not fully describe what actually occurs.
Client outcomes are much more complex than
this. Often in the course of recovery, clients
manage to have longer and longer periods
between episodes of use, and use episodes
themselves grow shorter and less severe.
•
The assumption that abstinence equals
success and return to use equals failure
creates a self-fulfilling prophecy. It implies that
once substance use resumes, there is nothing
to lose and little that can be done. Instead, the
point is to get back on track as soon as possible.
•
Recurrence of symptoms is common to
substance use behaviors and chronic illness
ingeneral.
Part of a motivational approach in Maintenance has
to do with your perspective on a client’s return to
substance misuse and how you respond to it. You
should:
•
Avoid the expert and labeling traps
when a client returns to substance use or
substancemisuse.
•
Avoid the “righting reflex” and any temptation
to lecture, educate, blame, or judge the client
(Miller & Rollnick, 2013).
•
Explore the client’s understanding of his or her
return to substance use.
•
Use the same motivational counseling
approaches as in Precontemplation,
Contemplation, Preparation, and Action,
depending on which stage the client is in after
the recurrence.
COUNSELOR NOTE: THE RIGHTING
REFLEX
Miller and Rollnick (2013) use the term “righting
reflex” to describe the natural response to “fix”
a person’s problems from a desire to help.
This impulse can lead you to becoming overly
directive and telling a client what to do instead
of evoking the client’s own motivation and
strategies for change.
Provide Relapse Prevention Counseling
Recurrence is common in recovery; offer RPC
during Maintenance. RPC is a cognitive–behavioral
therapy (CBT) approach to identifying and
managing triggers to use, developing coping skills,
building self-efficacy, and managing setbacks.
Although this is a CBT method, you can use
motivational counseling strategies to engage
clients in the process and help them resolve
ambivalence about learning and practicing new
coping skills. (Chapter 8 provides more information
about blending motivational interviewing and CBT.)
The two major components of RPC are:
120 Chapter 7

TIP 35
Chapter 7—From Action to Maintenance: Stabilizing Change
•
Addressing the nature of the relapse
process through education and an analysis of
high-risk situations, warning signs, and other
factors that contribute to relapse, as well as
clients’strengths.
•
Providing coping-skills training. Identify and
develop clients’ coping strategies that are useful
in maintaining both cognitive and behavioral
changes that promote recovery and lessen the
likelihood of relapse. (See the section “Identify
high-risk situations and coping strategies”
above in this chapter.)
The Marlatt model (Witkiewitz & Marlatt, 2007)
is the most widely researched and implemented
RPC approach in behavioral health services. Many
of its strategies have been applied to counseling
for relapse prevention with people with SUDs
and CODs. The two key features of the Marlatt
model are:
1. Helping clients recognize and manage high-risk
situations in which they are most likely to be
tempted to immediately use substances or
engage in other risky behaviors.
2. Creating a relapse management plan that
includes positive coping strategies to lessen the
impact of a recurrence, if it happens, and avoid
a full relapse.
The two elements of a high-risk situation that
increase the client’s risk of relapse are:
•
Internal factors, which include the client’s
- Cognitive distortions.
- Intense positive and negative feelings.
- Ineffective coping responses.
- Low self-efficacy.
- Positive outcome expectancies (POEs):
positive thoughts and associations with
drinking or using drugs.
- Abstinence violation effect (AVE) such as
feelings of guilt and shame associated
with recurrence.
•
Environmental factors, which include the
client’s
-
Social influences.
- Access to substances.
-
Exposure to conditioned cues for substance
use or risk behaviors.
Exhibit 7.6 shows the dynamic process of relapse
and how RPC strategies help clients develop
effective coping mechanisms and increase self-
efficacy to decrease the probability of a relapse.
EXHIBIT 7.6. Marlatt’s RPC Process
Source: Marlett, Parks, & Witkiewitz, 2002. Adapted with permission.
Chapter 7 121

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
C-TRAPS
RPC has five components (Marlatt et al., 2002).
C-TRAPS is a handy acronym to remember them:
•
Cognitive traps
•
Temptations
•
Replacement Activities
•
Preparation for relapse
•
Strategies for coping
Cognitive traps, also known as cognitive
distortions, are the ways the mind works against
the client’s commitment to recovery and intention
to refrain from substance use. They are cognitive
early warning signs that a recurrence might be
close at hand. They include:
•
All-or-nothing thinking (e.g., “I got off my
regular eating plan today; I’m a failure, so I
might as well go all the way and eat whatever
I want tonight!”) and overt justifications (e.g.,
“My divorce was finalized today, and I really
need something to take the edge off”) for a
return to substance use.
•
Minimizing the impact of a recurrence (e.g.,
“Just one cigarette won’t push me over
theedge”).
•
Apparently irrelevant decisions or decisions
that seem unimportant but set up high-risk
situations where the likelihood of recurrence is
very high. (For example, Ginny decides to buy a
bottle of wine, just in case her friend Pam comes
over to play cards. She puts the bottle in the
liquor cabinet that she had just cleaned out with
the help of her AA sponsor, thinking she won’t
be tempted.)
Cognitive traps bring clients closer to situations
where temptation is strong and difficult to resist.
Help clients lessen the power of cognitive traps
by:
•
Teaching them how to slow down their
thinkingprocess.
•
Identifying all the steps in the process leading
up to an apparently irrelevant decision.
•
Inviting them to evaluate whether those choices
are consistent with their recovery goals.
•
Exploring possible alternative choices.
Temptations are urges or impulses closely linked
to feelings or physical cravings. To distinguish
between cravings and urges, note that cravings
are the desire and urges are the intentions to use a
substance (Witkiewitz & Marlatt, 2007). Temptation
is the attraction of the immediate, positive effects
of drinking or using drugs. These impulses can be
powerful and seem to come out of the blue. In
Alcoholics Anonymous (also known as “The Big
Book”), the authors depicted the unpredictable
lure of temptation: “Remember that we deal with
alcohol—cunning, baffling, powerful!” (Alcoholics
Anonymous, 2001, p. 10). Help clients map
out temptations and develop strategies for
responding to them.
Replacement activities reinforce clients’ lifestyle
changes through actions that support their
recovery. This involves helping clients identify
and engage in activities that provide fulfillment,
long-term satisfaction, and a substitute for
the short-term pleasure of substance use. Use
OARS to ask open questions and affirm, reflect,
and summarize clients’ ideas for replacement
activities. Brainstorming is also an effective
way to help clients discover new ideas for
replacementactivities.
Preparation for relapse includes:
•
Working with clients to anticipate and prepare
for this possibility.
•
Taking a nonjudgmental stance with clients if
they lapse.
•
Explaining to them that relapse is avoidable
but that they should be prepared for possible
setbacks and describing how to manage a return
to substance use if it occurs.
•
Reframing a recurrence as a learning
opportunity and reevaluating their
copingstrategies.
Strategies for coping are helpful ways of thinking
and acting that reduce relapse risk, enhance
self-efficacy, manage impulses and cravings, reduce
stress, and solve problems that arise in early
recovery. Elicit clients’ positive coping strategies,
and engage them in coping-skills training activities,
such as:
122 Chapter 7

TIP 35
Chapter 7—From Action to Maintenance: Stabilizing Change
•
Providing psychoeducation.
•
Teaching stress reduction and
mindfulnesspractices.
•
Brainstorming strategies with clients to avoid
high-risk situations and manage impulses
orcravings.
•
Deconstructing negative thinking patterns.
•
Sharing problem-solving skills and coping
strategies that have been helpful to others.
•
Modeling positive self-talk and
communicationskills.
•
Rehearsing how to handle high-risk situations.
•
Teaching alcohol and drug refusal skills.
•
Exchanging in nonjudgmental feedback with
other clients in RPC groups.
Relapse management strategies
If clients return to substance use, help them
avoid full relapse by teaching them to (Witkiewitz
& Marlatt, 2007):
•
Stop, look, and listen. Clients can learn how to
become aware of events as they are unfolding
and stop the process of a recurrence before it
goes further. Taking a step back from events as
an observer can help clients gain perspective
and allow them the emotional and cognitive
space to assess the situation before reacting.
The AA slogan “think…think…think” aids in
relapse prevention by providing a cognitive
reminder to stop, look, and listen before
reacting or taking action.
•
Keep calm. Staying calm is the emotional
equivalent of stop, look, and listen. Thoughts,
feelings, and behaviors are often tightly
intertwined. Sometimes, clients don’t remember
that, just because they feel anxious or have
an impulse to use substances or reengage in
risk behaviors, they don’t have to act on those
feelings or impulses. Practicing calmness and
not overreacting emotionally to a recurrence can
help clients break this pattern of impulsivity.
•
Renew their commitment to recovery. People
are often discouraged by a recurrence, which
can lower motivation and confidence about
continuing on the recovery journey. To allay
hopelessness, remind clients of previous
successes with behavior change (no matter
how “small”). Keep them looking forward by
exploring their reasons for recovery and hopes,
dreams, and goals for the future.
•
Review what led up to the recurrence. Review
the events leading up to the recurrence and do
a mini-relapse assessment taking into account
lifestyle imbalance, thoughts of immediate
gratification, urges and cravings, justifications,
apparently irrelevant decisions, and the nature
of the high-risk situation that triggered the
lapse. Review early warning signs clients may
have noticed but disregarded and explore the
cognitive traps that led to disregarding the
warning signs.
•
Make an immediate plan for recovery. Work
with clients to develop an immediate action
plan for recommitting to recovery. The plan
should include specific action steps clients can
take to avoid a full relapse that are acceptable,
accessible, and appropriate from their point
of view. Write the plan on paper or a file card.
Include client-generated strategies for handling
a recurrence, such as:
-
Call a sponsor or recovery support person.
Include specific names and phone numbers.
- Go to a recovery support meeting. Include
specific meeting times and locations.
- Engage in cognitive, emotional, physical, and
behavioral strategies for managing cravings.
- Engage in specific self-care or stress
reduction activities.
- Return to medication (if applicable).
Include adherence strategies and names
ofprescribers.
-
Call you or the treatment program to
schedule a counseling session.
Chapter 7 123

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
•
Deal with the AVE. Help clients deal with the
emotional aftereffects of recurrence, such as
guilt, shame, and the cognitive dissonance
that happens when people act in ways that do
not align with their values and recovery goals.
This cognitive and emotional disagreement
can increase the likelihood of a return to
substance use. Engage clients in exploration
with compassion and understanding; encourage
them to learn from recurrence and identify new
coping strategies.
Reenter the Cycle of Change
If clients return to substance misuse, help them
reenter the cycle as soon as possible. Most
clients do not return to the Precontemplation
stage (Connors et al., 2013). Rather, clients are
more likely to recycle back into Contemplation,
Preparation, or Action. They can use the recurrence
experience as an opportunity to identify which
strategies for the Maintenance stage worked and
which did not work. Your task is to debrief clients
about relapse and assess where they are now
in the SOC (Connors et al., 2013). If the client has
returned to Contemplation, start with resolving
ambivalence and evoking change talk. Clients who
have returned to Preparation or Action should
revisit and revise the change plan or coping plan.
Strategies for helping clients manage a return to
substance misuse include:
•
Helping them reenter the change cycle;
affirming any willingness to reconsider
positive change.
- Explore their perceptions and reactions to
resumed use.
- Use affirmations to praise them for
reengaging in the change process.
- Elicit DARN (Desire, Ability, Reasons, and
Need) change talk; reflect on the client’s
reasons to get back on track.
• Exploring the meaning of the recurrence as a
learning opportunity.
- Explore what can be learned from
the experience.
- Remind them that the experience is
a common and temporary part of the recovery
process.
- Elicit their positive experiences in recovery
and the advantages of abstinence.
- Use reflective listening.
- Avoid the question-and-answer trap.
- Explore their values, hopes, purpose, and
goals in life. Ask, “What do you want to
do now?”
• Helping clients find and continuously review
and evaluate current and alternative coping
strategies.
- Review coping strategies that have and have
not worked to maintain stated goals for
change.
- Help them identify new coping strategies.
• Maintaining supportive contact until clients exit
the change cycle for each behavior changegoal.
Conclusion
Maintaining substance use behavior change is
often more challenging for clients than taking
action toward change. Help clients stabilize and
maintain changes made in the Preparation and
Action stages by:
•
Using motivational counseling strategies to
engage and retain clients in treatment.
•
Helping them develop and practice coping
strategies for high-risk situations.
•
Reinforcing social support.
•
Helping them reenter the cycle of change
quickly if they do return to substance use.
MI strategies are useful during all stages in the
SOC and are used in conjunction with other
counseling approaches, like CBT—particularly
during the Preparation, Action, and Maintenance
stages. An important way to help clients
throughout the SOC is to continuously assess and
reassess which stage they are in the SOC and
match your counseling approach accordingly.
124 Chapter 7

Chapter 8—Integrating Motivational
Approaches in SUD Treatment Settings
From its inception MI [motivational interviewing]
has been organic, emerging, and evolving through
collaborative processes….Our decision was to focus on
promoting quality in MI practice and training….”
—Miller & Rollnick, 2013, p. 377
KEY MESSAGES
TIP 35
ENHANCING MOTIVATION FOR CHANGE IN
SUBSTANCE USE DISORDER TREATMENT
•
Motivational counseling approaches have
been widely disseminated to substance
use disorder (SUD) treatment programs.
• Adaptations of MI in group counseling, the
use of technology, and blended counseling
approaches enhance the implementation
and integration of motivational
interventions into standard treatment
methods.
• Training and ongoing supervision of
counselors are essential for workforce
development and integration of
motivational counseling approaches into
SUD treatment.
Chapter 8 discusses adaptations for using
motivational counseling approaches in group
counseling, with technology, and in blended
counseling approaches that are applicable to SUD
treatment programs. It also addresses workforce
development issues that treatment programs may
face in fully integrating and sustaining motivational
counseling approaches.
Over the past three decades, MI and motivational
counseling approaches have been widely and
successfully disseminated across the United States
and internationally to specialty SUD treatment
programs (Hall, Staiger, Simpson, Best, & Lubman,
2015). Research supports the integration of
motivational counseling strategies into treatment
as a prelude to ongoing treatment to increase
client retention and enhance participation in
treatment. Motivational counseling can increase
adherence to treatment medication and behavioral
change plans and makes achievement and
maintenance of positive substance use behavior
outcomes more likely (Miller & Rollnick, 2013).
Depending on the SUD treatment setting, different
adaptions of motivational interventions (e.g.,
individual or group counseling, blended with other
counseling approaches) may be effective both
clinically and programmatically.
Integrating motivational counseling approaches
into a treatment program requires more than
providing counseling staff with a few workshops
on MI. It requires broad integration of the
philosophy and underlying spirit of MI throughout
the organization. Just as a counselor using a
motivational approach works in partnership with
clients to help them move through the Stages of
Change (SOC) to achieve long-term behavioral
change, organizations wishing to integrate a
motivational counseling approach should work
in partnership with staff to implement program
changes. Organizations also go through a process
of change until the treatment approach becomes a
new “lifestyle.”
125

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Adaptations of Motivational
Counseling Approaches
The most common delivery of motivational
counseling approaches has been through brief or
ongoing individual counseling. For example, MI
in SUD treatment was specifically developed as a
counseling approach to be delivered in face-to-face
conversations between a counselor and a client.
Depending on the treatment program, adaptations
of motivational interventions may make treatment
more cost effective, more accessible to clients,
and easier to integrate into existing treatment
approaches, as well as ease workload demands
oncounselors.
Chapter 8 discusses the following adaptations of
motivational counseling approaches:
•
Group counseling
•
Technology adaptations (e.g., Internet-based
applications and telephone-based MI)
•
Blended counseling approaches
Group Counseling
The current context of service delivery in SUD
treatment programs places heavy emphasis on
group counseling. Many motivation-enhancing
activities can take place in group counseling that
cannot occur in individual treatment (e.g., clients
can receive feedback from peers). Because social
support is intrinsic to group treatment, clients in a
group can reinforce and help maintain each other’s
substance use behavior changes (Holstad, Diiorio,
Kelley, Resnicow, & Sharma, 2010).
However, several significant clinical issues arise
when conducting groups using MI including
(Feldstein Ewing, Walters, & Baer, 2013; Miller &
Rollnick, 2013):
•
The counselor’s ability to translate MI skills to
the group context
•
The counselor’s skill in managing
groupdynamics
•
Fewer opportunities for group members to
express change talk and receive reflective
listening responses from the counselor
•
Varying needs and experiences of
groupparticipants
•
The counselor’s ability to respond to various
participant needs (e.g., reflecting commitment
language of one participant while responding
to another participant’s ambivalence about
changing substance use behaviors)
•
Actively managing social pressures of
peer interactions, which are not present in
individual sessions
•
Responding to and managing sustain talk in a
group setting
Perhaps the most challenging aspect of group-
based MI is the possibility of group members
reinforcing each other’s sustain talk instead of
reflecting change talk (Miller & Rollnick, 2013). An
important adaptation of MI in group is to minimize
the opportunities for clients to evoke and reflect
sustain talk and maximize opportunities to evoke
and reflect change talk (Houck et al., 2015; Miller
& Rollnick, 2013). Strategies for accomplishing
thisinclude:
•
Teaching group members OARS (asking Open
question, Affirming, Reflective listening, and
Summarizing) skills (Wagner & Ingersoll, 2013).
•
Identifying the general parameters for group
interactions that are in line with the spirit of MI
(e.g., group members should support each other
without pressure to change, avoid giving advice,
focus on positives and possibilities for change)
(Miller & Rollnick, 2013).
•
Modeling MI skills in groups (Wagner &
Ingersoll, 2013).
•
Acknowledging sustain talk but emphasizing and
reinforcing change talk (D’Amico et al.,2015).
126 Chapter 8

TIP 35
Chapter 8—Integrating Motivational Approaches in SUD Treatment Settings
EXPERT COMMENT:
MOTIVATIONAL ENHANCEMENT
IN GROUP COUNSELING
Conducting motivational interventions in a group
versus individual format is more difficult, more
complex, and more challenging. Personally,
however, I find it much more rewarding. In
group counseling, particularly using motivational
techniques and strategies, clients learn through
the group. It is like a hall of mirrors; clients get
the feel of how they come across. For me, when
a client uses reflective listening with another
client or points out another client’s ambivalence,
the group is like a living, learning laboratory of
experiences practiced first in a safe environment
before being tried in the real world. In the end,
what the members have is a common goal to
reduce or stop substance misuse, and it is here
that their mutual support and peer pressure
is effective.
Linda C. Sobell, Ph.D., Consensus Panel Member
Evidence shows that, despite some challenges, MI
can be delivered successfully in a group context,
particularly when group participants hear more
change talk than sustain talk (Osilla et al., 2015).
Positive outcomes from MI in groups include
decreased alcohol use and alcohol misuse among
adolescents, greater retention in SUD treatment
after detoxification, increased retention in
methadone maintenance treatment, and adherence
to risk-reduction behaviors in women infected
with HIV (Bachiller et al., 2015; D’Amico et al.,
2015; Holstad et al., 2010; Navidian, Kermansaravi,
Tabas, & Saeedinezhad, 2016).
Integrating MI into group treatment requires
group counselors to have training and ongoing
supervision in both MI strategies and group
process. The Assessment of Motivational
Interviewing Groups—Observer Scale (AMIGOS-v
1.2) is a validated tool that assesses counselor
skills in group processes, client-centered focus,
and using MI in groups (Wagner & Ingersoll, 2017).
Appendix C provides a link to a downloadable
version of AMIGOS. This tool may be helpful for
assessing and enhancing counselor competence in
delivering MI in groups.
Technology Adaptations
Some evidence shows the effectiveness of
adaptations of MI and motivational enhancement
therapy (MET) through interactive computer
applications, Internet-based applications, and
telephone or video conferencing when used
selectively to deliver motivational interventions
(Miller & Rollnick, 2013). For example, the
“drinker’s checkup,” the original method to give
personalized feedback in MET, has been delivered
in interactive computer-based applications and has
had positive outcomes in reducing alcohol misuse
(Hester, Delaney, & Campbell, 2012).
Benefits of brief motivational interventions
delivered by interactive computer applications
include (Hester et al., 2012):
•
Ease of use.
•
Cost effectiveness.
•
Adaptability to different client populations.
•
Flexibility of design.
Although computer- or Internet-based adaptations
of motivational interventions may be useful
in providing personalized feedback to clients,
computers cannot provide empathetic listening
responses or evoke change talk. They also limit
use of brief interventions that provide feedback to
increase client engagement in treatment.
Telephone MI is the most widely used alternative
to face-to-face MI and is effective for addressing
tobacco cessation, alcohol misuse, and use of
illicit drugs (Jiang, Wu, & Gao, 2017). Telephone
counseling with, if possible, the addition of a
video component has the advantage of reaching
client populations in rural settings that do not
have access to transportation to the treatment
setting. Telephone MI approaches also have the
added benefit over computer-based interventions
of giving the counselor the opportunity to offer
interactive motivational interventions like reflective
listening, affirmations, and evoking change talk. For
Chapter 8 127

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
more information about using technology in SUD
treatment, see Treatment Improvement Protocol
(TIP) 60: Using Technology-Based Therapeutic
Tools in Behavioral Health Services (Substance
Abuse and Mental Health Services Administration
[SAMHSA], 2015b).
Blended Counseling Approaches
MI as a counseling style is compatible with a wide
range of clinical approaches that have been used
in SUD treatment including cognitive–behavioral
therapy (CBT), psychoeducation, medication-
assisted treatment, and case management
approaches (Miller & Rollnick, 2013). When
thinking about ways to integrate MI into current
treatment approach, treatment staff should address
some open questions like, “How does MI fit with
what we already do?” and “At what points in our
treatment approach are we most concerned about
engaging clients in treatment, helping clients
resolve ambivalence about change, and retaining
clients in treatment?” (Miller & Rollnick, 2013).
Three examples of blending MI with other SUD
counseling approaches supported by research are
motivational interviewing assessment (MIA), CBT,
and recovery management checkup (RMC).
MIA
The National Institute on Drug Abuse Clinical
Trials Network, in cooperation with SAMHSA,
developed a protocol to incorporate MI into a
one-session assessment intake to improve client
engagement in SUD treatment programs (Carroll et
al., 2006). This blended approach to the standard
initial assessment in SUD treatment sandwiches
a standard assessment between a brief MI
counseling segment at the beginning and end of
the session (Martino et al., 2006).
A challenge of doing a standard assessment with
clients just entering treatment is that counselors
and clients tend to fall into the question-and-
answer trap (see Chapter 3). Counselors ask
closed questions to elicit information needed
for the assessment, and clients answer with yes,
no, or short-answer responses. This pattern
of interaction sets up an expectation that the
counselor is the expert and the client is a passive
recipient of services. It can become an obstacle
to client engagement (Miller & Rollnick, 2013).
MIA incorporates MI into typical SUD treatment
program intake/assessment processes and
facilitates client engagement while addressing
the organization’s need to collect assessment
information for treatment planning and to comply
with licensing and insurance requirements.
Research supports MIA as a method to blend MI
with standard assessment approaches. An initial
study found that clients who participated in the
MIA-blended protocol were significantly more
likely than clients who participated in the standard
assessment to be enrolled in the program after 1
month (Martino et al., 2006). A more recent study
found that incorporating MI into the initial intake
and assessment processes (whether standard MI or
MIA) promoted client retention (e.g., 70 percent
remained in treatment after 4 weeks) and enhanced
treatment outcomes (e.g., a 50 percent increase
in days abstinent) (Martino et al., 2016). This same
study found that supervision of counselors in both
groups (standard MI and MIA) improved counselor
performance of MI, but the counselors who
received supervision in MIA showed significantly
greater improvements in MI competency, although
training and supervision in MIA was more costly.
A link to a manual for training and supervising
counselors in MIA, Motivational Interviewing
Assessment: Supervisor Tools for Enhancing
Proficiency Manual, is available for download at no
cost in Appendix C (Martino et al., 2006). Another
study found that the addition of motivational
feedback to a standard assessment enhanced SUD
treatment entry for a group of veterans with co-
occurring disorders (Lozano, Larowe, Smith, Tuerk,
& Roitzsch, 2013).
MI and CBT
Perhaps the most widely adopted counseling
approach used in SUD treatment is CBT. CBT
focuses on helping clients change thoughts (e.g.,
drinking is the only way to relax) and behaviors
(e.g., drinking to intoxication) that interfere with
everyday functioning. CBT strategies include
helping clients identify and manage triggers for
substance use and practicing new behaviors that
reinforce abstinence. CBT is also an evidence-
based approach that is widely used to treat mental
disorders (e.g., anxiety, depression, posttraumatic
stress disorder) that often co-occur with SUDs.
128 Chapter 8

TIP 35
Chapter 8—Integrating Motivational Approaches in SUD Treatment Settings
However, some CBT providers have acknowledged
difficulties with initial client engagement, low
motivation, and nonadherence to CBT practices,
such as completing out-of-session assignments
(Arkowitz, Miller, & Rollnick, 2015). Integrating
MI strategies to address ambivalence and
enhance motivation of clients with co-occurring
disorders can improve client adherence to CBT
treatmentcomponents.
Strategies for blending MI and CBT include
(Copeland, Gates, & Pokorski, 2017; Miller &
Rollnick, 2013; Naar-King, Safren, & Miller, 2017):
•
Engaging in a brief motivational conversation
before a client moves into a CBT-focused
component of treatment (e.g., a relapse
prevention group).
•
Alternating between MI and CBT, depending on
the goals of each session.
•
Using MI when the clinical focus is on
engaging, focusing, evoking, and emphasizing
the more directive style of CBT during the
planningprocess.
•
Shifting to MI during CBT interventions when
counselor–client discord or client ambivalence
about a specific change goal arises.
•
Using the spirit of MI as a framework
and interactional style in which to use
CBTstrategies.
Integrating MI into CBT approaches that the SUD
treatment program already supports can enhance
client motivation to engage in CBT and improve
long-term maintenance of behavior change
(Naar-King et al., 2017). Blending MI and CBT
may actually create a more powerful approach for
behavioral change in SUD treatment than either
approach alone (Copeland et al., 2017; Naar-King
et al., 2017). For example, a review of psychosocial
interventions for cannabis use disorder found
that the most consistent evidence for reducing
cannabis use among a variety of interventions was
a combination of CBT and MET (Gates, Sabioni,
Copeland, Foll, & Gowing, 2016). Other research
that evaluated studies on the integrated approach
of CBT and MI found a clinically significant effect
in treatment outcomes for co-occurring alcohol
use disorder (AUD) and major depressive disorder
compared with treatment as usual (Riper et
al.,2014).
At times, CBT may require counselors to take
on the role of a teacher or guide who is more
directive, but counselors’ overall stance should
remain that of an empathetic partner–consultant
instead of an expert. For example, in one study,
counselors using CBT who explored and connected
with clients in treatment for AUD were more
successful in evoking discussions about behavior
change than counselors who emphasized teaching
clients behavior-change skills (Magill et al., 2016).
Counselors’ most important goal is to develop a
relationship of mutual trust and respect with the
client. They should view the client as the expert in
his or her own recovery. Exhibit 8.1 provides a brief
clinical scenario that depicts a counselor blending
the spirit of MI with CBT relapse prevention
strategies (see Chapter 7) in a counseling approach
with a military veteran.
Chapter 8 129

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
EXHIBIT 8.1. Blending the Spirit of MI With CBT
Jordan is 40 years old. He has been married for 12 years and has two young children. He served in the military and did
two tours in Iraq. After discharge, he was arrested twice for driving under the influence and was mandated to alcohol and
drug counseling. He was also referred for a psychiatric evaluation and was diagnosed with posttraumatic stress disorder.
Dan is a licensed clinical social worker in a co-occurring services program at a comprehensive behavioral health services
program and has been seeing Jordan for 6 months for outpatient counseling. Initially, Jordan was angry about having to
go to counseling and Dan’s suggestion to try Alcoholics Anonymous (AA) as part of a recovery plan; however, Jordan has
been attending AA meetings and asked another veteran to be his sponsor.
Jordan has returned to heavy drinking on three occasions in the past 6 months. His relapse risk is that he stops going
to meetings and stops calling his sponsor. Then he finds himself at a local sports bar, thinking that he’ll just watch the
game (an apparently irrelevant decision), but he ends up getting drunk. Jordan now speaks highly of AA and has been
working the 12 Steps with his sponsor. He tells Dan, “I am doing everything my sponsor tells me to do and am committed
to my recovery now. I know that if I follow his suggestions and work the program, I will be okay. I just don’t understand
why I keep slipping.”
Dan has established a good rapport with Jordan. He has done a relapse risk assessment, provided information to Jordan
about the relapse process, and given Jordan homework to track high-risk situations and the coping strategies he uses to
manage them. Jordan seems to respond well to Dan’s directive approach but continues to return to drinking. Dan shifts
gears in the current session and decides to explore Jordan’s understanding of his pattern of disengagement from AA and
his sponsor instead of cautioning him again about his behavioral pattern leading up to a return to drinking.
Dan: I’m wondering what you make of this pattern: not going to meetings, not calling your sponsor just before you have
a slip. If you could name that pattern, what would you call it? (Open question)
Jordan: I guess I would call it my version of “Stinkin’ Thinkin’.” I work so hard at trying to do the right thing in my recovery,
but then I start to think that I am not getting anywhere, you know? I’m not drinking, but I don’t feel any better, so I feel
like a failure and get tired of trying. It’s like I need to take a break from recovery.
Dan: So, you work hard to do the right thing in recovery and really want to feel better, but sometimes you feel
discouraged and think you need to take a break. (Reflection)
Jordan: Yeah. That describes where I am right now.
Dan: I am curious about that. Would you say you are taking a break from recovery or taking a break from the program?
[Reframe in the form of a question that leaves open the possibility for the client to reject the new perspective]
Jordan: Gee, I never thought about it that way. I guess I’m still working on my recovery, even if I don’t talk to my sponsor.
Like the other day, I started to feel like I wanted to go to the bar to watch the game, but I remembered what you and I
had talked about last time—that this is a warning flag, and that I could do something different. So, instead of going to the
bar, I asked one of my sober friends over, and we watched the game at my house. We didn’t talk about the program; we
just watched the game.
Dan: You really worked that one out for yourself and didn’t let “Stinkin’ Thinkin’” take over. Good for you. (Affirmation)
At the end of the session, Dan summarizes Jordan’s successful approach to “doing something different” and asks Jordan
how their conversation was for him. Jordan responds that it was very helpful that Dan didn’t lecture him, but rather
asked him what he thought. This helped him realize for himself that he is still working on his recovery, even if he doesn’t
call his sponsor or go to a meeting. Jordan also mentioned that now he doesn’t feel like he is failing at recovery, so he
thinks he will get back to his AA program.
130 Chapter 8

TIP 35
Chapter 8—Integrating Motivational Approaches in SUD Treatment Settings
MI and RMC
RMC is a fairly new addiction treatment approach
that uses motivational strategies; it is modeled
after approaches used for staying connected to
people with chronic medical illnesses like diabetes.
RMC is a proactive strategy for monitoring a
client’s progress in recovery after intensive SUD
treatment and for intervening quickly if the client
returns to substance use. RMC involves regular
telephone calls (more frequently at first, then less
frequently) to the client to find out how he or she is
coping with recovery.
RMC incorporates MI strategies to enhance
motivation to return to treatment if needed.
Counselors or peer recovery support specialists
can perform RMC. Telephone-based motivational
interventions are efficacious in treating and
preventing substance use behaviors (Jiang
et al., 2017). RMC is an effective method of
monitoring clients’ progress in recovery in the
Action and Maintenance stages and intervening
quickly to reengage clients into treatment
after a substance use recurrence. It is linked to
improved long-term substance use outcomes
and increased participation in SUD treatment and
recovery support services (Dennis & Scott, 2012;
Dennis, Scott, & Laudet, 2014; Scott, Dennis, &
Lurigio, 2017).
Workforce Development
MI is not only a counseling style but a
conversational style that emphasizes guiding,
rather than directing, clients toward changing
substance use behaviors (Miller & Rollnick, 2013).
Depending on the type of treatment program,
an organization might provide aspects of MI
training to only a few counselors, the entire clinical
staff, or all staff, including support staff and
peer providers. As increasingly more programs,
including certified community behavioral health
clinics (SAMHSA, 2016), adopt a client-centered
treatment philosophy and MI as an evidence-based
treatment, organizations should train all staff in
the spirit of MI. This means all personnel—from
the first person the client encounters walking
through the door to the staff working in the billing
department—understand the importance of client
autonomy and choice, listening, and guiding
instead of lecturing or directing in creating a
welcoming environment and engaging clients in
the treatment process (Miller & Rollnick, 2013).
MI is a complex skill, like
playing a musical instrument.
Watching others play the piano
or attending a 2-day workshop is
not likely in itself to turn one into
a competent pianist.”
—Linda C. Sobell, Ph.D., Consensus
Panel Member
MI has been widely disseminated as an evidence-
based treatment, yet dissemination is not the
same as implementation. Counselors lose their MI
skills after a workshop if there is no supervision or
coaching after training (Hall et al., 2015; Schwalbe,
Oh, & Zweben, 2014). The key to workforce
development of clinical staff in MI is to move
beyond 1- or 2-day workshops and integrate
ongoing training, supervision, and coaching of
clinical staff to maintain fidelity to MI-consistent
counseling techniques.
Another factor in whether a treatment program
implements a motivational counseling approach
is how closely the organization’s mission and
philosophy are aligned with the principles of
motivational counseling. Counselors are more
likely to adopt an MI counseling style when the
organization’s philosophy is aligned with MI
principles (Ager et al., 2010).
Training
MI is an integrated and comprehensive set of
listening and interviewing skills (Miller & Rollnick,
2013). For counselors to learn these skills and
consistently integrate them into everyday practice,
staff training and learning tasks should include
(Miller & Rollnick, 2013):
•
Understanding the spirt of MI.
•
Developing skill in OARS.
•
Identifying change goals.
Chapter 8 131

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
•
Exchanging information (i.e., Elicit-Provide-Elicit
[EPE]) and giving advice skillfully.
•
Recognizing change talk and sustain talk.
•
Evoking change talk.
•
Strengthening change talk.
•
Responding skillfully to sustain talk and
counselor-client discord.
•
Developing hope and confidence.
•
Negotiating a change plan.
•
Strengthening commitment.
•
Integrating MI with other
counselingapproaches.
These learning tasks apply to training counselors
in any motivational counseling approach, including
brief interventions that use FRAMES (Feedback,
Responsibility, Advice, Menu of options, Empathy,
and Self-efficacy) and MET, where the counselor
gives personalized feedback and advice. Some
tasks are foundational, like learning reflective
listening, and are best learned through face-to-
face, interactive training experiences. Other tasks,
like recognizing change talk and sustain talk, can
be learned through reading material, like coded
transcripts of counselor-client interactions (Miller &
Rollnick, 2013).
An initial workshop that covers the foundational
components of MI (e.g., understanding the spirit of
MI, OARS, recognizing and responding to change
talk and sustain talk) may be a good beginning.
This workshop should include both knowledge
exchange and interactive skill-building exercises.
A meta-analysis of MI training found that training
produces medium-to-large-sized effects in MI
proficiency both before and after training and
medium-sized effects in MI proficiency compared
with controls (de Roten, Zimmermann, Ortega,
& Despland, 2013). Furthermore, an initial 12-to-
15-hour workshop of MI training that included
didactic, face-to-face instruction, and interactive
exercises increased counselor skills as did more
enhanced workshops that used video, web-based,
or computer technology (Schwalbe et al., 2014).
For an initial workshop, a simple format may be
appropriate and potentially more cost effective
than complex formats.
Ongoing training is the key to learning and
sustaining motivational counseling skills if skills
learned during training are not practiced. MI
counselor skills introduced in training can erode
after only 3 months if they are not used and
practiced (Schwalbe et al., 2014). Spreading out
training activities over a 6-month period and
increasing the practice training hours to 5 or more
hours increase counselor skill level and enhance
skill retention (Schwalbe et al., 2014). Ongoing
training in MI should be integrated into SUD
treatment over 24 months as part of professional
development to ensure counselor competency
(Hall et al., 2015).
There are multiple ways to train staff, and the path
an organization chooses is based on many factors.
Before implementing MI training, an organization
should consider the following questions when
developing a strategic plan:
•
Assessing organizational philosophy and
theSOC
- Is a person-centered approach to
service delivery a key component of the
organization’s mission statement and
philosophy?
- Is MI a new counseling approach for the
organization or will MI be blended with
current treatment approaches?
- At what stage of the SOC is staff with regard
to integrating a new approach?
- What kind of preparation is needed to
implement a training program?
•
Assessing staff needs
- Does support staff need an introduction to
the spirit of MI?
- Which counseling staff members have already
been trained and are using MI skills in their
counseling approach? Which staff need a
foundational workshop?
- Which clinical supervisors have been trained
in MI and demonstrate skill competence?
132 Chapter 8

TIP 35
Chapter 8—Integrating Motivational Approaches in SUD Treatment Settings
•
Tailoring a training program to meet
staffneeds
- How will the organization assess current
counselor skill level in MI and tailor the
training to different counselor skill levels?
- Which would be most effective for
theprogram:
•
Sending all counseling staff to a series of
trainings provided by outside experts?
•
Training one or two clinical supervisors
to provide in-house training and ongoing
supervision of staff?
•
Bringing an outside expert into the
organization to provide training?
•
A combination of outside and
in-housetraining?
- What strategies will the organization use
to balance effective training, supervision,
and professional development given
costconsiderations?
In developing the training plan, the organization
should consider integrating a new counseling
approach into the SUD treatment program
a long-term project that needs buy-in by the
entireorganization.
COUNSELOR NOTE: IMPLEMENTATION OF MET IN SUD TREATMENT
SERVICES IN THE VETERANS HEALTH ADMINISTRATION
In 2011, the Veterans Health Administration (VHA) implemented a national initiative to provide evidence-based MET
counseling to veterans with SUDs. VHA developed a competency-based training program (Drapkin et al., 2016) that
consisted of an initial 3.5-day training on MI plus assessment feedback, followed by 6 months of consultation with
experienced MI training consultants (TCs). TCs provided ongoing supervision and coaching based on direct observation
of counseling sessions using audio recordings. Training materials were adapted to address the specific needs of veterans.
The VHA model of implementation was based on research in the training and supervision of clinical staff in MI to
enhance implementation and fidelity.
Implementation of this competency-based model of training and supervision was enhanced by encouraging training
participants to actively engage with the VHA MET community by becoming TCs and “MET champions,” who provided
information and consultation on how local VHA facilities could best disseminate and implement MET into their SUD
treatment approach. TCs participate in monthly national conference calls with other TCs covering advanced MET
topics. This model combines the use of outside trainers with in-house workforce development of new trainers and MET
champions to create learning communities that sustain the use of MET in VHA facilities.
Supervision and Coaching
Training counselors in MI is the first step in
integrating this approach into SUD treatment
programs. Maintenance of skills and staying up
to date with new developments in any counseling
approach require ongoing supervision.
Supervision in MI should be competency based.
This means supervision should address counselors’
knowledge and proficiency in MI skills (e.g.,
the spirit of MI, OARS, EPE, recognizing and
responding to change talk and sustain talk, evoking
change talk, negotiating a change plan) needed to
practice effectively. Competency-based supervision
of MI includes directly observing counselor
sessions, using feedback to monitor counselor
proficiency, and coaching to help counselors
continue developing their knowledge and skills
(Martino et al., 2016). One study on competency-
based supervision in MI found that anywhere
from 4 to 20 supervision sessions were needed
for doctoral-level interns to reach MI competency
benchmarks (Schumaker et al., 2018).
Competency-based supervision requires direct
observation of counselors, not simply a counselor’s
self-report or subjective evaluation. Direct
observation is one of the most effective ways
of building and monitoring counselor skills and
can include use of video or audio taping sessions,
live observation of counseling sessions in person
Chapter 8 133

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
or via one-way mirrors, or both (SAMHSA, 2009).
For more information on competency-based
supervision, see TIP 52: Clinical Supervision and
Professional Development of the Substance Abuse
Counselor (SAMHSA, 2009).
The program should get permission from clients
before engaging in direct observation. Written
consent forms should include the nature and
purpose of the direct observation, a description
of how clients’ privacy and confidentiality will be
maintained, and what will happen to any video
or audio recordings after supervision or research
is completed. Program should refer to in-house
policies and state licensing board and professional
ethics code requirements for the use of video
and audio recordings for clinical supervision
orresearch.
In addition to being competency based, MI
supervision should be performed in the spirit of
MI. Clinical supervisors should reach a level of skill
in using MI to be able to:
•
Describe the underlying theoretical foundations
of MI.
•
Explore and resolve counselor ambivalence
about learning and integrating MI
intotreatment.
•
Teach counselors MI skills.
•
Model the spirit of MI and its skills in individual
and group supervision sessions.
•
Give respectful and nonjudgmental feedback to
counselors to support self-efficacy and enhance
professional development.
Coaching counselors in MI involves coding a
recorded or live observation session for consistent
(e.g., OARS responses) and inconsistent (e.g.,
giving unsolicited advice, confrontation) MI
responses and using this information to provide
feedback to the counselor (Miller & Rollnick, 2013).
Because listening to and coding a full session are
labor intensive, coaches can code brief sections of
a session and produce reliable ratings of counselor
fidelity to MI (Caperton, Atkins, & Imel, 2018). Two
coding systems for MI have been widely used in
research and clinical practice to evaluate counselor
fidelity to MI (Miller & Rollnick, 2013):
•
MI Integrity (MITI) focuses on counselor
responses and provides global ratings and
specific counts of MI-consistent responses. The
most recent version of MITI (MITI 4) has added
global ratings and greater accuracy in assessing
counselor support for client autonomy and
the use of persuasion when giving information
and advice (Moyers, Manuel, & Ernst, 2014).
The MITI 4 is a reliable way to assess counselor
fidelity to MI in both its relational and its
technical components (Moyers, Houck, Rice,
Longbaugh, & Miller, 2016). Appendix C
provides a link to the MITI 4 manual.
•
MI Skills Code (MISC) counts both counselor
and client responses (e.g., change talk, sustain
talk) (Miller, Moyers, Ernst, & Amrhein, 2008).
MISC is a reliable way to monitor counselor
fidelity to MI and can provide an accurate
measure of the ratio of client change talk to
sustain talk (Lord et al.,2014). The MISC can
provide not only feedback to counselors about
their use of MI skills but also information
about the effects of MI on counselor–client
interactions. Appendix C provides a link to the
MISC manual.
A positive aspect of using coding systems to assess
counselor fidelity to MI is that they provide reliable
and accurate measures of counselor skill level. A
less-positive aspect of using coding systems is
that they require considerable training and quality
assurance checks to establish and maintain the
reliability of the coach who is doing the coding
(Miller & Rollnick, 2013). In addition, counselors
may be ambivalent about recording client sessions
and having a supervisor, who is responsible for
performance evaluations, code the counselor’s
speech. Potential solutions to consider include:
•
Addressing counselor ambivalence in
supervision about having sessions coded.
•
Creating small learning communities in the
organization where counselors, case managers,
and peer providers can learn and practice
coding snippets of actual sessions or uncoded
audio, video, or written transcripts with one
another. Appendix C provides links to uncoded
transcripts, audio, and video examples of MI
counseling sessions.
134 Chapter 8

TIP 35
Chapter 8—Integrating Motivational Approaches in SUD Treatment Settings
•
Sending audio sessions or short excerpts to
an outside coder who can perform the coding
and return written feedback for supervisors to
discuss with counselors.
•
Encouraging counselors to listen to their
own recorded sessions and use a simplified
method of counting their use of OARS, their
inconsistent responses (e.g., giving advice
without permission), change talk and sustain
talk prompts, and client expressions of change
talk and sustain talk (Miller & Rollnick, 2013).
Counselors can then review their “self-coding”
with their supervisors.
Whichever strategies the SUD organization
employs to enhance counselor fidelity to and
proficiency in delivering MI, the organization
will need to balance cost considerations with
effective training, supervision, and professional
development. Administrators and supervisors
should partner with counseling staff to move the
organization along the SOC toward integrating
motivational approaches into SUD treatment.
Conclusion
Many different motivational approaches have
been discussed in this TIP including MI; MET;
motivational interventions in the SOC; brief
interventions; screening, brief intervention, and
referral for treatment; and blending MI with other
counseling methods. A growing body of evidence
demonstrates that motivational interventions
can enhance client motivation and improve SUD
treatment outcomes. Integrating MI and other
motivational approaches into SUD treatment
settings requires the entire organization to adopt
a client-centered philosophy and administrative
support for ongoing training and supervision of
counselors. Motivational counseling approaches
are respectful and culturally responsive methods
for helping people break free from addiction
and adopt new lifestyles that are consistent with
the values of good health, well-being, and being
integral member of the community.
Chapter 8 135
This page intentionally left blank

TIP 35
Appendix A—Bibliography
Appendix A—Bibliography
Ager, R., Roahen-Harrison, S., Toriello, P. J., Kissinger,
P., Morse, P., Morse, E., … Rice, J. (2010). Predictors
of adopting motivational enhancement therapy.
Research on Social Work Practice, 21(1), 65–76.
doi:10.1177/1049731509353170
Ainscough, T. S., McNeill, A., Strang, J., Calder, R., & Brose,
L. S. (2017). Contingency management interventions for
non-prescribed drug use during treatment for opiate
addiction: A systematic review and meta-analysis. Drug
and Alcohol Dependence, 178, 318–339.
Alcoholics Anonymous. (2001). Alcoholics Anonymous:
The story of how many thousands of men and women
have recovered from alcoholism (4th ed.). New York, NY:
Alcoholics Anonymous World Services.
Aldridge, A., Dowd, W., & Bray, J. (2017). The relative
impact of brief treatment versus brief intervention in
primary health-care screening programs for substance use
disorders. Addiction, 112, 54–64. doi:10.1111/add.13653
Aldridge, A., Linford, R., & Bray, J. (2017). Substance
use outcomes of patients served by a large U.S.
implementation of screening, brief intervention and
referral to treatment (SBIRT). Addiction, 112, 43–53.
Alperstein, D., & Sharpe, L. (2016). The efficacy of
motivational interviewing in adults with chronic pain: A
meta-analysis and systematic review. Journal of Pain,
17(4), 393-403. doi:10.1016/j.jpain.2015.10.021
American Psychiatric Association. (2013). Diagnostic
and statistical manual of mental disorders (5th ed.).
Washington, DC: Author.
American Psychiatric Association. (1994). Diagnostic
and statistical manual of mental disorders (4th ed.).
Washington, DC: Author.
Amodeo, M. (2015). The addictive personality. Substance
Use and Misuse, 50(8-9), 1031–1036. doi:10.3109/108260
84.2015.1007646
Anderson, T., Crowley, M. E., Himawan, L., Holmberg, J. K.,
& Uhlin, B. D. (2016). Therapist facilitative interpersonal
skills and training status: A randomized clinical trial on
alliance and outcome. Psychotherapy Research, 26(5),
511–529. doi:10.1080/10503307.2015.1049671
Apodaca, T. R., Borsari, B., Jackson, K. M., Magill, M.,
Longabaugh, R., Mastroleo, N. R., & Barnett, N. P. (2014).
Sustain talk predicts poorer outcomes among mandated
college student drinkers receiving a brief motivational
intervention. Psychology of Addictive Behaviors, 28(3),
631–638. doi:10.1037/a0037296
Apodaca, T. R., Jackson, K. M., Borsari, B., Magill, M.,
Longabaugh, R., Mastroleo, N. R., & Barnett, N. P. (2016).
Which individual therapist behaviors elicit client change
talk and sustain talk in motivational interviewing? Journal
of Substance Abuse Treatment, 61, 60-65. doi:10.1016/j.
jsat.2015.09.001
Apodaca, T. R., & Longabaugh, R. (2009). Mechanisms
of change in motivational interviewing: A review and
preliminary evaluation of the evidence. Addiction,104(5),
705–715. doi:10.1111/j.1360-0443.2009.02527.x
Apodaca, T. R., Magill, M., Longabaugh, R., Jackson, K.
M., & Monti, P. M. (2013). Effect of a significant other on
client change talk in motivational interviewing. Journal
of Consulting and Clinical Psychology,81(1), 35–46.
doi:10.1037/a0030881
Appiah-Brempong, E., Okyere, P., Owusu-Addo, E., &
Cross, R. (2014). Motivational interviewing interventions
and alcohol abuse among college students: A systematic
review. American Journal of Health Promotion, 29(1).
doi:10.4278/ajhp.130502-lit-222
Arkowitz, H., Miller, W. R., & Rollnick, S. (2015). Motivational
interviewing in the treatment of psychological problems
(2nd ed.). New York, NY: Guilford Publications.
Babor, T. F., Del Boca, F. D., & Bray, J. W. (2017). Screening,
brief intervention and referral to treatment: Implications
of SAMHSA’s SBIRT initiative for substance abuse policy
and practice. Addiction, 112, 110–117. doi:10.1111/
add.13675
Babor, T. F., Higgins-Biddle, J. C., & Robaina, K. (2016).
USAUDIT: The Alcohol Use Disorders Identification Test,
Adapted for use in the United States: A guide for primary
care practitioners. Retrieved from www.ct.gov/dmhas/lib/
dmhas/publications/USAUDIT-2017.pdf
Babor, T. F., Higgins-Biddle, J. C., Saunders, J. B., &
Monteiro, M. G. (2001). The Alcohol Use Disorders
Identification Test: Guidelines for use in primary care (2nd
ed.). Geneva, Switzerland: World Health Organization.
Bachiller, D., Grau-López, L., Barral, C., Daigre, C.,
Alberich, C., Rodríguez-Cintas, L., … Roncero C.
(2015). Motivational interviewing group at inpatient
detoxification: Its influence in maintaining abstinence and
treatment retention after discharge. Adicciones, 27(2),
109–118.
Baker, A. L., Kavanagh, D. J., Kay-Lambkin, F. J., Hunt, S. A.,
Lewin, T. J., Carr, V. J., & McElduff, P. (2014). Randomized
controlled trial of MICBT for co-existing alcohol misuse
and depression: Outcomes to 36–months. Journal of
Substance Abuse Treatment, 46(3), 281–290.
Appendix A 137

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Baker, A. L., Thornton, L. K., Hiles, S., Hides, L., & Lubman,
D. I. (2012). Psychological interventions for alcohol misuse
among people with co-occurring depression or anxiety
disorders: A systematic review. Journal of Affective
Disorders, 139(3), 217–229. doi:10.1016/j.jad.2011.08.004
Bandura, A. (1977). Self-efficacy: Toward a unifying theory
of behavioral change. Psychological Review, 84, 191–215.
Barata, I. A., Shandro, J. R., Montgomery, M., Polansky, R.,
Sachs, C. J., Duber, H. C., … Macias-Konstantopoulos, W.
(2017). Effectiveness of SBIRT for alcohol use disorders in
the emergency department: A systematic review. Western
Journal of Emergency Medicine, 18(6), 1143–1152.
Barbosa, C., Cowell, A., Dowd, W., Landwehr, J., Aldridge,
A., & Bray, J. (2017). The cost-effectiveness of brief
intervention versus brief treatment of screening, brief
intervention and referral to treatment (SBIRT) in the
United States. Addiction, 112, 73–81. doi:10.1111/
add.13658
Barnes, R. D., & Ivezaj, V. (2015). A systematic review of
motivational interviewing for weight loss among adults
in primary care. Obesity Reviews, 16(4), 304–318.
doi:10.1111/obr.12264
Barnett, E., Moyers, T. B., Sussman, S., Smith, C., Rohrbach,
L. A., Sun, P., & Spruijt-Metz, D. (2014). From counselor
skill to decreased marijuana use: Does change talk
matter? Journal of Substance Abuse Treatment, 46,
498–505.
Barnett, E., Spruijt-Metz, D., Moyers, T. B., Smith,
C., Rohrbach, L. A., Sun, P., & Sussman, S. (2014).
Bidirectional relationships between client and counselor
speech: The importance of reframing. Psychology of
Addictive Behaviors, 28(4), 1212–1219. doi:10.1037/
a0036227
Barrio, P., & Gual, A. (2016). Patient-centered care
interventions for the management of alcohol use
disorders: A systematic review of randomized controlled
trials. Patient Preference and Adherence, 10, 1823–1845.
doi:10.2147/PPA.S109641
Bassuk, E. L., Hanson, J., Greene, R. N., Richard, M., &
Laudet, A. (2016). Peer-delivered recovery support
services for addictions in the United States: A systematic
review. Journal of Substance Abuse Treatment, 63, 1–9.
doi:10.1016/j.jsat.2016.01.003
Bedard-Gilligan, M., Garcia, N., Zoellner, L. A., & Feeny,
N. C. (2018). Alcohol, cannabis, and other drug
use: Engagement and outcome in PTSD treatment.
Psychology of Addictive Behaviors, 32(3), 277–288.
Belmontes, K. C. (2018). When family gets in the
way of recovery. Family Journal, 26(1), 99–104.
doi:10.1177/1066480717753013
Bernstein, S. L., & D’Onofrio, G. (2017). Screening,
treatment initiation, and referral for substance use
disorders. Addiction Science and Clinical Practice, 12(1).
doi:10.1186/s13722-017-0083-z
Bertholet, N., Palfai, T., Gaume, J., Daeppen, J., & Saitz,
R. (2013). Do brief alcohol motivational interventions
work like we think they do? Alcoholism: Clinical and
Experimental Research, 38(3), 853–859. doi:10.1111/
acer.12274
Beutler, L. E., Harwood, T. M., Michelson, A., Song, A., &
Holman, J. (2011). Resistance/reactance level. Journal of
Clinical Psychology, 67(2), 133–142.
Black, J. J., & Chung, T. (2014). Mechanisms of change in
adolescent substance use treatment: How does treatment
work? Substance Abuse, 35(4), 344–351.
Blow, F. C., Walton, M. A., Bohnert, A. S., Ignacio, R. V.,
Chermack, S., Cunningham, R. M., … Barry, K. L. (2017).
A randomized controlled trial of brief interventions to
reduce drug use among adults in a low-income urban
emergency department: The HealthiER You study.
Addiction, 112(8), 1395–1405. doi:10.1111/add.13773
Bohnert, A. S. B., Bonar, E. E., Cunningham, R., Greenwald,
M. K., Thomas, L., Chermack, S., … Walton, M. (2016). A
pilot randomized clinical trial of an intervention to reduce
overdose risk behaviors among emergency department
patients at risk for prescription drug overdose. Drug and
Alcohol Dependence, 163, 40–47.
Borsari, B., Apodaca, T. R., Jackson, K. M., Fernandez,
A., Mastroleo, N. R., Magill, M., … Carey, K. B. (2018).
Trajectories of in-session change language in brief
motivational interventions with mandated college
students. Journal of Consulting and Clinical Psychology,
86(2), 158–168. doi:10.1037/ccp0000255
Boston Center for Treatment Development and Training.
(2016). Module 10: Sobriety sampling. Retrieved from
www.mass.gov/files/documents/2016/07/ty/bt-manual-
module10.pdf
Bourke, E., Magill, M., & Apodaca, T. R. (2016). The
in-session and long-term role of a significant other
in motivational enhancement therapy for alcohol use
disorders. Journal of Substance Abuse Treatment, 64,
35–43. doi:10.1016/j.jsat.2016.01.008
Bray, J. W., Aden, B., Eggman, A. A., Hellerstein, L.,
Wittenberg, E., Nosyk, B., … Schackman, B. R. (2017).
Quality of life as an outcome of opioid use disorder
treatment: A systematic review. Journal of Substance
Abuse Treatment, 76, 88–93.
Breslin, F. C., Sobell, L. C., Sobell, M. B., & Agrawal, S.
(2000). A comparison of a brief and long version of
the Situational Confidence Questionnaire. Behaviour
Research and Therapy, 38(12), 1211–1220.
Brorson, H. H., Arnevik, E. A., Rand-Hendriksen, K., &
Duckert, F. (2013). Drop-out from addiction treatment:
A systematic review of risk factors. Clinical Psychology
Review, 33(8), 1010–1024. doi:10.1016/j.cpr.2013.07.007
Caperton, D. D., Atkins, D. C., & Imel, Z. E. (2018). Rating
motivational interviewing fidelity from thin slices.
Psychology of Addictive Behaviors, 32(4), 434–441.
doi:10.1037/adb0000359
138 Appendix A

TIP 35Appendix A—Bibliography
Carey, K. B., Leontieva, L., Dimmock, J., Maisto, S. A., &
Batki, S. L. (2007). Adapting motivational interventions
for comorbid schizophrenia and alcohol use disorders.
Clinical Psychology, 14(1), 39–57.
Carroll, K. M., Ball, S. A., Nich, C., Martino, S., Frankforter,
T. L., Farentinos, C., … Woody, G. E. (2006). Motivational
interviewing to improve treatment engagement and
outcome in individuals seeking treatment for substance
abuse: A multisite effectiveness study. Drug and Alcohol
Dependence, 81, 301–312.
Caviness, C. M., Hagerty, C. E., Anderson, B. J., Dios, M. A.,
Hayaki, J., Herman, D., & Stein, M. D. (2013). Self-efficacy
and motivation to quit marijuana use among young
women. American Journal on Addictions, 22(4), 373–380.
doi:10.1111/j.1521-0391.2013.12030
Chariyeva, Z., Golin, C. E., Earp, J. A., Maman, S.,
Suchindran, C., & Zimmer, C. (2013). The role of
self-efficacy and motivation to explain the effect of
motivational interviewing time on changes in risky sexual
behavior among people living with HIV: A mediation
analysis. AIDS and Behavior, 17(2), 813–823. doi:10.1007/
s10461-011-0115-8
Coffin, P. O., Santos, G.-M., Matheson, T., Behar, E.,
Rowe, C., Rubin, T., … Vittinghoff, E. (2017). Behavioral
intervention to reduce opioid overdose among high-risk
persons with opioid use disorder: A pilot randomized
controlled trial. PLOS One, 12(10), 1–15. Retrieved from
www.ncbi.nlm.nih.gov/pubmed/29049282
Connors, G. J., DiClemente, C. C., Velasquez, M. M., &
Donovan, D. M. (2013). Substance abuse treatment
and the stages of change: Selecting and planning
interventions. New York, NY: Guilford Press.
Copeland, J., Gates, P., & Pokorski, I. (2017). A narrative
review of psychological cannabis use treatments with and
without pharmaceutical adjunct. Current Pharmaceutical
Design, 22(42), 6397–6408. doi:10.2174/1381612822666
160831094811
Copeland, L., McNamara, R., Kelson, M., & Simpson,
S. (2015). Mechanisms of change within motivational
interviewing in relation to health behaviors outcomes:
A systematic review. Patient Education and Counseling,
98(4), 401–411. doi:10.1016/j.pec.2014.11.022
Cunningham, J. A., Sobell, L. C., Gavin, D. R., Sobell, M. B.,
& Breslin, F. C. (1997). Assessing motivation for change:
Preliminary development and evaluation of a scale
measuring the costs and benefits of changing alcohol
or drug use. Psychology of Addictive Behaviors, 11(2),
107–114.
D’Amico, E. J., Houck, J. M., Hunter, S. B., Miles, J. N.,
Osilla, K. C., & Ewing, B. A. (2015). Group motivational
interviewing for adolescents: Change talk and alcohol and
marijuana outcomes. Journal of Consulting and Clinical
Psychology, 83(1), 68–80. doi:10.1037/a0038155
Davis, J. P., Houck, J. M., Rowell, L. N., Benson, J. G., &
Smith, D. C. (2015). Brief motivational interviewing and
normative feedback for adolescents: Change language
and alcohol use outcomes. Journal of Substance Abuse
Treatment, 65, 66–73.
Deci, E. L., & Ryan, R. M. (2012). Overview of self-
determination theory: An organismic dialectical
perspective. In E. Deci & R. M. Ryan (Eds.), Handbook
of self-determination research (pp. 3–38). Rochester, NY:
University of Rochester Press.
Dennis, M. L., & Scott, C. K. (2012). Four-year outcomes
from the Early Re-Intervention (ERI) experiment using
Recovery Management Checkups (RMCs). Drug and
Alcohol Dependence, 121(1–2), 10–17. doi:10.1016/j.
drugalcdep.2011.07.026
Dennis, M. L., Scott, C. K., & Laudet, A. (2014). Beyond
bricks and mortar: Recent research on substance use
disorder recovery management. Current Psychiatry
Reports, 16(4). doi:10.1007/s11920-014-0442-3
de Roten, Y., Zimmermann, G., Ortega, D., & Despland,
J.-N. (2013). Meta-analysis of the effects of MI training
on clinicians’ behavior. Journal of Substance Abuse
Treatment, 45(2), 155–162. Retrieved from www.ncbi.nlm.
nih.gov/pubmed/23537923
DiClemente, C. C. (2018). Addiction and change: How
addictions develop and addicted people recover (2nd
ed.). Guilford, NY: Guilford Publications.
DiClemente, C. C., Carbonari, J. P., Montgomery, R. P.
G., & Hughes, S. O. (1994). The Alcohol Abstinence
Self-Efficacy Scale. Journal of Studies on Alcohol, 55(2),
141–148.
DiClemente, C. C., Corno, C. M., Graydon, M. M.,
Wiprovnick, A. E., & Knoblach, D. J. (2017). Motivational
interviewing, enhancement, and brief interventions over
the last decade: A review of reviews of efficacy and
effectiveness. Psychology of Addictive Behaviors, 31(8),
862–887. doi:10.1037/adb0000318
Dillard, P. K., Zuniga, J. A., & Holstad, M. M. (2017).
An integrative review of the efficacy of motivational
interviewing in HIV management. Patient Education
and Counseling, 100(4), 636–646. doi:10.1016/j.
pec.2016.10.029
Drapkin, M. L., Wilbourne, P., Manuel, J. K., Baer, J.,
Karlin, B., & Raffa, S. (2016). National dissemination of
motivation enhancement therapy in the Veterans Health
Administration: Training program design and initial
outcomes. Journal of Substance Abuse Treatment, 65,
83–87. doi:10.1016/j.jsat.2016.02.002
Dufett, I., & Ward, C. I. (2015). Can a motivational-
interviewing-based outpatient substance abuse treatment
achieve success? A theory-based evaluation. African
Journal of Drug and Alcohol Studies, 14(1), 1–12.
Appendix A 139

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Ekong, G., & Kavookjian, J. (2016). Motivational
interviewing and outcomes in adults with type 2 diabetes:
A systematic review. Patient Education and Counseling,
99(6), 944–952. doi:10.1016/j.pec.2015.11.022
Elliott, J. C., & Carey, K. B. (2013). Pros and cons:
Prospective predictors of marijuana use on a college
campus. Psychology of Addictive Behaviors, 27(1),
230–235. doi:10.1037/a0029835
Elliott, R., Bohart, A. C., Watson, J. C., & Murphy, D. (2018).
Therapist empathy and client outcome: An updated
meta-analysis. Psychotherapy, 55(4), 399–410. Retrieved
from www.researchgate.net/publication/324562138_
Therapist_Empathy_and_Client_Outcome_An_Updated_
Meta-Analysis
Ewing, S. W., Wray, A. M., Mead, H. K., & Adams, S. K.
(2012). Two approaches to tailoring treatment for cultural
minority adolescents. Journal of Substance Abuse
Treatment, 43(2), 190–203. doi:10.1016/j.jsat.2011.12.005
Feldstein Ewing, S. W., Walters, S., & Baer, J. C. (2013).
Motivational interviewing groups for adolescents and
emerging adults. In C. C. Wagner & K. S. Ingersoll (Eds.),
Motivational interviewing in groups (pp. 387–406). New
York, NY: Guilford Press.
Fergie, L., Campbell, K. A., Coleman-Haynes, T., Ussher, M.,
Cooper, S., & Coleman, T. (2018). Identifying effective
behavior change techniques for alcohol and illicit
substance use during pregnancy: A systematic review.
Annals of Behavioral Medicine. doi:10.1093/abm/kay085
Field, C. A., Adinoff, B., Harris, T. R., Ball, S. A., & Carroll, K.
M. (2009). Construct, concurrent and predictive validity
of the URICA: Data from two multi-site clinical trials. Drug
and Alcohol Dependence, 101(1–2), 115–123.
Field, C., Walters, S., Marti, C. N., Jun, J., Foreman, M., &
Brown, C. (2014). A multisite randomized controlled trial
of brief intervention to reduce drinking in the trauma care
setting. Annals of Surgery, 259(5), 873–880. doi:10.1097/
sla.0000000000000339
Fiszdon, J. M., Kurtz, M. M., Choi, J., Bell, M. D., & Martino,
S. (2015). Motivational interviewing to increase cognitive
rehabilitation adherence in schizophrenia. Schizophrenia
Bulletin, 42(2), 327–334.
Flannery, M. (2017). Self-determination theory: Intrinsic
motivation and behavioral change. Oncology Nursing
Forum, 44(2), 155–156. Retrieved from www.ncbi.nlm.nih.
gov/pubmed/28222078
Forman, D. P., & Moyers, T. B. (2019). With odds of a
single session, motivational interviewing is a good bet.
Psychotherapy. doi:10.1037/pst0000199
Foster, D., & Neighbors, C. (2013). A review of decisional
balance research and directions for brief alcohol
intervention among college students. OA Alcohol, 1(1).
doi:10.13172/2053-0285-1-1-575
Foster, D. W., Neighbors, C., & Pai, A. (2015). Decisional
balance: Alcohol decisional balance intervention for heavy
drinking undergraduates. Substance Use and Misuse,
50(13), 1717–1727.
Friedrichs, A., Spies, M., Härter, M., & Buchholz, A. (2016).
Patient preferences and shared decision making in the
treatment of substance use disorders: A systematic
review of the literature. PLOS One, 11(1). doi:10.1371/
journal.pone.0145817
Gates, P. J., Sabioni, P., Copeland, J., Foll, B. L., & Gowing,
L. (2016). Psychosocial interventions for cannabis use
disorder. Cochrane Database of Systematic Reviews.
doi:10.1002/14651858.cd005336.pub4
Gaume, J., Magill, M., Mastroleo, N. R., Longabaugh,
R., Bertholet, N., Gmel, G., & Daeppen, J. (2016).
Change talk during brief motivational intervention
with young adult males: Strength matters. Journal of
Substance Abuse Treatment, 65, 58–65. doi:10.1016/j.
jsat.2016.01.005
Gelberg, L., Andersen, R., Vahidi, M., Rico, M., Baumeister,
S., & Leake, B. (2017). A multi-component brief
intervention for risky drug use among Latino patients of
a federally qualified health center in East Los Angeles:
A randomized controlled trial of the quit using drugs
intervention trial (quit) brief intervention. Drug and
Alcohol Dependence,171. Retrieved from https://
eurekamag.com/research/064/949/064949750.php
Glozah, F. N., Adu, N. A., & Komesuor, J. (2015). Assessing
alcohol abstinence self-efficacy in undergraduate
students: Psychometric evaluation of the alcohol
abstinence self-efficacy scale. Health and Quality of Life
Outcomes, 13(1). doi:10.1186/s12955-015-0387-1
Gordon, T. (1970). Parent effectiveness training: The nolose
program for raising responsible children. New York, NY:
Wyden.
Granfield, R., & Cloud, W. (1999). Coming clean:
Overcoming addiction without treatment. New York, NY:
New York University Press.
Grant, S., Colaiaco, B., Motala, A., Shanman, R., Booth,
M., Sorbero, M., & Hempel, S. (2017). Mindfulness-
based relapse prevention for substance use disorders:
A systematic review and meta-analysis. Journal of
Addiction Medicine, 11(5), 386–396. doi:10.1097/
adm.0000000000000338
Gueorguieva, R., Wu, R., O’Connor, P. G., Weisner, C.,
Fucito, L. M., Hoffmann, S., … O’Malley, S. S. (2014).
Predictors of abstinence from heavy drinking during
treatment in COMBINE and external validation in
PREDICT. Alcoholism: Clinical and Experimental Research,
38(10), 2647–2656.
Hall, K., Staiger, P. K., Simpson, A., Best, D., & Lubman, D. I.
(2015). After 30 years of dissemination, have we achieved
sustained practice change in motivational interviewing?
Addiction, 111(7), 1144–1150. doi:10.1111/add.13014
140 Appendix A

TIP 35Appendix A—Bibliography
Harley, D. A. (2017). Motivational interviewing and
motivational enhancement therapy: Cultural implications
in addiction intervention for African Americans. SciFed
Journal of Addiction and Therapy, 1(1). doi:10.23959/
sfjat-1000005
Harrell, P. T., Trenz, R., Scherer, M., Martins, S., & Latimer,
W. (2013). A latent class approach to treatment readiness
corresponds to a transtheoretical (“Stages of Change”)
model. Journal of Substance Abuse Treatment, 45(3),
249–256. doi:10.1016/j.jsat.2013.04.004
Hausotter, W. (2006). Motivational interviewing assessment:
Supervisory tools for enhancing proficiency. Salem, OR:
Northwest Frontier Addiction Technology Transfer Center,
Oregon Health and Science University. Retrieved from
www.motivationalinterviewing.org/sites/default/files/
mia-step.pdf
Heather, N., & Honekopp, J. (2008). A revised edition of the
readiness to change questionnaire (treatment version).
Addiction Research and Theory, 16(5), 421–433.
Heather, N., & McCambridge, J. (2013). Post-treatment
stage of change predicts 12-month outcome of treatment
for alcohol problems. Alcohol and Alcoholism, 48(3),
329–336. doi:10.1093/alcalc/agt006
Hennessy, E. A. (2017). Recovery capital: A systematic
review of the literature. Addiction Research and Theory,
25(5), 349–360. doi:10.1080/16066359.2017.1297990
Hennessy, E. A., Tanner-Smith, E. E., & Steinka-Fry, K. T.
(2015). Do brief alcohol interventions reduce tobacco
use among adolescents and young adults? A systematic
review and meta-analysis. Journal of Behavioral Medicine,
38(6), 899–911.
Hester, R. K., Delaney, H. D., & Campbell, W. (2012). The
college drinker’s check-up: Outcomes of two randomized
clinical trials of a computer-delivered intervention.
Psychology of Addictive Behaviors, 26(1), 1–12.
Hingson, R., & Compton, W. M. (2014). Screening and brief
intervention and referral to treatment for drug use in
primary care: Back to the drawing board. JAMA, 312(5),
488. doi:10.1001/jama.2014.7863
Holstad, M. M., Diiorio, C., Kelley, M. E., Resnicow, K., &
Sharma, S. (2010). Group motivational interviewing to
promote adherence to antiretroviral medications and risk
reduction behaviors in HIV infected women. AIDS and
Behavior, 15(5), 885–896. doi:10.1007/s10461-010-9865-y
Houck, J. M., Hunter, S. B., Benson, J. G., Cochrum, L.
L., Rowell, L. N., & Damico, E. J. (2015). Temporal
variation in facilitator and client behavior during
group motivational interviewing sessions. Psychology
of Addictive Behaviors, 29(4), 941–949. doi:10.1037/
adb0000107
Houck, J. M., Manuel, J. K., & Moyers, T. B. (2018).
Short- and long-term effects of within-session client
speech on drinking Outcomes in the COMBINE study.
Journal of Studies on Alcohol and Drugs, 79(2), 217–222.
doi:10.15288/jsad.2018.79.217
Houck, J. M., & Moyers, T. B. (2015). Within-session
communication patterns predict alcohol treatment
outcomes. Drug and Alcohol Dependence, 157, 205–209.
doi:10.1016/j.drugalcdep.2015.10.025
Humphreys, K., Blodgett, J. C., & Wagner, T. H. (2014).
Estimating the efficacy of Alcoholics Anonymous without
self-selection bias: An instrumental variables re-analysis
of randomized clinical trials. Alcoholism: Clinical and
Experimental Research, 38(11), 2688–2694. doi:10.1111/
acer.12557
Hunt, G. E., Siegfried, N., Morley, K., Sitharthan, T., &
Cleary, M. (2013). Psychosocial interventions for people
with both severe mental illness and substance misuse.
Cochrane Database of Systematic Reviews, 10. Art. No.:
CD001088. doi:10.1002/14651858.CD001088.pub3
Ingersoll, K. S., Ceperich, S. D., Hettema, J. E., Farrell-
Carnahan, L., & Penberthy, J. K. (2013). Preconceptional
motivational interviewing interventions to reduce alcohol-
exposed pregnancy risk. Journal of Substance Abuse
Treatment, 44(4), 407–416. doi:10.1016/j.jsat.2012.10.001
Jackson, L. A., Buxton, J. A., Dingwell, J., Dykeman, M.,
Gahagan, J., Gallant, K., … Davison, C. (2014). Improving
psychosocial health and employment outcomes for
individuals receiving methadone treatment: A realist
synthesis of what makes interventions work. BMC
Psychology, 2(1), 26. doi:10.1186/s40359-014-0026-3
Janis, L. L., & Mann, L. (1977). Decision making:
A psychological analysis of conflict, choice, and
commitment. London, England: Cassel and Collier
Macmillan.
Jason, L. A., Salina, D., & Ram, D. (2016). Oxford recovery
housing: Length of stay correlated with improved
outcomes for women previously involved with the criminal
justice system. Substance Abuse, 37(1), 248–254. doi:10.1
080/08897077.2015.1037946
Jiang, S., Wu, L., & Gao, X. (2017). Beyond face-to-face
individual counseling: A systematic review on alternative
modes of motivational interviewing in substance abuse
treatment and prevention. Addictive Behaviors, 73,
216–235
Joseph, J., & Basu, D. (2016). Efficacy of brief interventions
in reducing hazardous or harmful alcohol use in middle-
income countries: Systematic review of randomized
controlled trials. Alcohol and Alcoholism, 52(1), 56–64.
doi:10.1093/alcalc/agw054
Kadden, R. M., & Litt, M. D. (2011). The role of self-efficacy
in the treatment of substance use disorders. Addictive
Behaviors, 36(12), 1120–1126.
Kahler, C. W., Pantalone, D. W., Mastroleo, N. R., Liu,
T., Bove, G., Ramratnam, B., … Mayer, K. J. (2018).
Motivational interviewing with personalized feedback to
reduce alcohol use in HIV-infected men who have sex with
men: A randomized controlled trial. Journal of Consulting
and Clinical Psychology, 86(8), 645–656.
Appendix A 141

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Kanfer, F. H., & Schefft, B. K. (1988). Guiding the process of
therapeutic change. Champaign, IL: Research Press.
Kelly, J. F., Bergman, B. G., Hoeppner, B., Vilsaint, C., &
White, W. L. (2017). Prevalence and pathways of recovery
from drug and alcohol problems in the United States
population: Implications for practice, research, and policy.
Drug and Alcohol Dependence, 181, 162–169.
Kiluk, B. D., Serafini, K., Malin-Mayor, B., Babuscio, T.
A., Nich, C., & Carroll, K. M. (2015). Prompted to
treatment by the criminal justice system: Relationships
with treatment retention and outcome among cocaine
users. American Journal on Addictions, 24(3), 225–232.
doi:10.1111/ajad.12208
Klimas, J., Field, C., Cullen, W., O’Gorman, C., Glynn,
L., Keenan, E., … Dunne, C. (2014). Psychosocial
interventions to reduce alcohol consumption in
concurrent problem alcohol and illicit drug users:
Cochrane Review. Drug and Alcohol Dependence, 140.
doi:10.1016/j.drugalcdep.2014.02.305
Kohler, S., & Hofmann, A. (2015). Can motivational
interviewing in emergency care reduce alcohol
consumption in young people? A systematic review and
meta-analysis. Alcohol and Alcoholism, 50(2), 107–117.
doi:10.1093/alcalc/agu098
Korcha, R. A., Polcin, D. L., Evans, K., Bond, J. C., &
Galloway, G. P. (2015). Intensive motivational interviewing
for women with alcohol problems. Counselor (Deerfield
Beach), 16(3), 62–69.
Krawczyk, N., Feder, K. A., Saloner, B., Crum, R. M.,
Kealhofer, M., & Mojtabai, R. (2017). The association of
psychiatric comorbidity with treatment completion among
clients admitted to substance use treatment programs in
a U.S. national sample. Drug and Alcohol Dependence,
175, 157–163. doi:10.1016/j.drugalcdep.2017.02.006
Krigel, S. W., Grobe, J. E., Goggin, K., Harris, K. J., Moreno,
J. L., & Catley, D. (2017). Motivational interviewing and
the decisional balance procedure for cessation induction
in smokers not intending to quit. Addictive Behaviors, 64,
171–178. doi:10.1016/j.addbeh.2016.08.036
Kuerbis, A., Armeli, S., Muench, F., & Morgenstern, J.
(2013). Motivation and self-efficacy in the context of
moderated drinking: Global self-report and ecological
momentary assessment. Psychology of Addictive
Behaviors, 27(4), 934–943. doi:10.1037/a0031194
Kuusisto, K., Knuuttila, V., & Saarnio, P. (2011). Clients' self-
efficacy and outcome expectations. Addictive Disorders
and Their Treatment, 10(4), 157–168. doi:10.1097/
adt.0b013e31820dd4ec
Kwasnicka, D., Dombrowski, S. U., White, M., & Sniehotta,
F. (2016). Theoretical explanations for maintenance of
behaviour change: A systematic review of behaviour
theories. Health Psychology Review, 10(3), 277–296. doi:1
0.1080/17437199.2016.1151372
Lee, W. W., Choi, K., Yum, R. W., Yu, D. S., & Chair, S.
(2016). Effectiveness of motivational interviewing on
lifestyle modification and health outcomes of clients
at risk or diagnosed with cardiovascular diseases: A
systematic review. International Journal of Nursing
Studies, 53, 331–341. doi:10.1016/j.ijnurstu.2015.09.010
Lenz, A. S., Rosenbaum, L., & Sheperis, D. (2016). Meta-
analysis of randomized controlled trials of motivational
enhancement therapy for reducing substance use. Journal
of Addictions and Offender Counseling, 37(2), 66–86.
doi:10.1002/jaoc.12017
Lindqvist, H., Forsberg, L., Enebrink, P., Andersson, G., &
Rosendahl, I. (2017). Relational skills and client language
predict outcome in smoking cessation treatment.
Substance Use and Misuse, 52(1), 33–42. doi:10.1080/108
26084.2016.1212892
Litt, M. D., & Kadden, R. M. (2015). Willpower versus
“skillpower”: Examining how self-efficacy works in
treatment for marijuana dependence. Psychology of
Addictive Behaviors, 29(3), 532–540. doi:10.1037/
adb0000085
Litt, M. D., Kadden, R. M., & Petry, N. M. (2013). Behavioral
treatment for marijuana dependence: Randomized trial of
contingency management and self-efficacy enhancement.
Addictive Behaviors, 38(3), 1764–1775. doi:10.1016/j.
addbeh.2012.08.011
Lord, S. P., Can, D., Yi, M., Marin, R., Dunn, C. W., Imel,
Z. E., … Atkins, D. C. (2014). Advancing methods for
reliably assessing motivational interviewing fidelity using
the motivational interviewing skills code. Journal of
Substance Abuse Treatment, 49, 50–57.
Lozano, B. E., Larowe, S. D., Smith, J. P., Tuerk, P.,
& Roitzsch, J. (2013). Brief motivational feedback
may enhance treatment entry in veterans with
comorbid substance use and psychiatric disorders.
American Journal on Addictions, 22(2), 132–135.
doi:10.1111/j.1521-0391.2013.00315.x
Lundahl, B., Moleni, T., Burke, B. L., Butters, R., Tollefson,
D., Butler, C., & Rollnick, S. (2013). Motivational
interviewing in medical care settings: A systematic review
and meta-analysis of randomized controlled trials. Patient
Education and Counseling, 93(2), 157–168. doi:10.1016/j.
pec.2013.07.012
Magill, M., Apodaca, T. R., Borsari, B., Gaume, J., Hoadley,
A., Gordon, R. E. F., … Moyers, T. (2018). A meta-analysis
of motivational interviewing process: Technical, relational,
and conditional process models of change. Journal of
Consulting and Clinical Psychology, 86(2), 140–157.
Magill, M., Gaume, J., Apodaca, T. R., Walthers, J.,
Mastroleo, N. R., Borsari, B., & Longabaugh, R. (2014).
The technical hypothesis of motivational interviewing:
A meta-analysis of MI’s key causal model. Journal of
Consulting and Clinical Psychology, 82(6), 973–983.
142 Appendix A

TIP 35Appendix A—Bibliography
Magill, M., Stout, R. L., & Apodaca, T. R. (2013). Therapist
focus on ambivalence and commitment: A longitudinal
analysis of motivational interviewing treatment
ingredients. Psychology of Addictive Behaviors, 27(3),
754–762. doi:10.1037/a0029639
Magill, M., Walthers, J., Mastroleo, N. R., Gaume, J.,
Longabaugh, R., & Apodaca, T. R. (2016). Therapist and
client discussions of drinking and coping: A sequential
analysis of therapy dialogues in three evidence-based
alcohol use disorder treatments. Addiction, 111(6), 1011-
1020. doi:10.1111/add.13313
Mahmoodabad, S. S., Tonekaboni, N. R., Farmanbar, R.,
Fallahzadeh, H., & Kamalikhah, T. (2017). The effect of
motivational interviewing-based intervention using self-
determination theory on promotion of physical activity
among women in reproductive age: A randomized
clinical trial. Electronic Physician, 9(5), 4461-4472.
doi:10.19082/4461
Manuel, J. K., Satre, D. D., Tsoh, J., Moreno-John, G.,
Ramos, J. S., McCance-Katz, E. F., & Satterfield, J. M.
(2015). Adapting screening, brief intervention, and
referral to treatment for alcohol and drugs to culturally
diverse clinical populations. Journal of Addiction
Medicine, 1. doi:10.1097/adm.0000000000000150
Marlatt, G., A., Parks, G. A., & Witkiewitz, K. (2002).
Clinical guidelines for implementing relapse prevention
therapy: A guideline developed for behavioral health
recovery management project. Chicago, IL: University
of Chicago. Retrieved from www.researchgate.net/
publication/235326763_Clinical_Guidelines_for_
Implementing_RelapsePrevention_Therapy_A_Guideline_
Developed_for_the_Behavioral_Health_Recovery_
Management_Project
Martin, G. W., & Rehm, J. (2012). The effectiveness of
psychosocial modalities in the treatment of alcohol
problems in adults: A review of the evidence.
Canadian Journal of Psychiatry, 57(6), 350–358.
doi:10.1177/070674371205700604
Martino, S., Ball, S. A., Gallon, S. L., Hall, D., Garcia, M.,
Ceperich, S., … Hausotter, W. (2006). Motivational
interviewing assessment: Supervisory tools for enhancing
proficiency. Salem, OR: Northwest Frontier Addiction
Technology Transfer Center, Oregon Health and Science
University. Retrieved from www.motivationalinterviewing.
org/sites/default/files/mia-step.pdf
Martino, S., Paris, M., Añez, L., Nich, C., Canning-Ball, M.,
Hunkele, K., … Carroll, K. M. (2016). The effectiveness
and cost of clinical supervision for motivational
interviewing: A randomized controlled trial. Journal of
Substance Abuse Treatment, 68, 11–23.
Mattoo, S. K., Prasad, S., & Ghosh, A. (2018). Brief
intervention in substance use disorders. Indian Journal of
Psychiatry, 60(Suppl 4), S466–S472.
McCance-Katz, E. F., & Satterfield, J. (2012). SBIRT: A key to
integrate prevention and treatment of substance abuse
in primary care. American Journal on Addictions, 21(2),
176–177. doi:10.1111/j.1521-0391.2011.00213.x
McConnaughy, E. A., Prochaska, J. O., & Velicer,
W. F.(1983). Stages of change in psychotherapy:
Measurement and sample profiles. Psychotherapy:
Theory, Research and Practice, 20, 368–375.
McDevitt-Murphy, M. E., Murphy, J. G., Williams, J. L.,
Monahan, C. J., Bracken-Minor, K. L., & Fields, J. A.
(2014). Randomized controlled trial of two brief alcohol
interventions for OEF/OIF veterans. Journal of Consulting
and Clinical Psychology, 82(4), 562–568. doi:10.1037/
a0036714
McQueen, J., Howe, T. E., Allan, L., Mains, D., & Hardy,
V. (2011). Brief interventions for heavy alcohol users
admitted to general hospital wards. Cochrane Database
of Systematic Reviews, (8).
McQueen, J. M., Howe, T. E., Ballinger, C., & Godwin, J.
(2015). Effectiveness of alcohol brief intervention in a
general hospital: A randomized controlled trial. Journal
of Studies on Alcohol and Drugs, 76(6), 838–844.
doi:10.15288/jsad.2015.76.838
Merchant, R. C., Romanoff, J., Zhang, Z., Liu, T., & Baird,
J. R. (2017). Impact of a brief intervention on reducing
alcohol use and increasing alcohol treatment services
utilization among alcohol- and drug-using adult
emergency department patients. Alcohol, 65, 71–80.
doi:10.1016/j.alcohol.2017.07.003
Miller, M. B., Leffingwell, T., Claborn, K., Meier, E., Walters,
S., & Neighbors, C. (2013). Personalized feedback
interventions for college alcohol misuse: An update of
Walters & Neighbors (2005). Psychology of Addictive
Behaviors, 27(4), 909–920.
Miller, W. R., Benefield, R. G., & Tonigan, J. S. (1993).
Enhancing motivation for change in problem drinking: A
controlled comparison of two therapist styles. Journal of
Consulting and Clinical Psychology, 61(3), 455–461.
Miller, W. R., & Brown, J. M. (1994). What I want from
treatment (2.0). Retrieved from https://casaa.unm.edu/
inst/What%20I%20Want%20From%20Treatment.pdf
Miller, W. R., Forcehimes, A. A., & Zweben, A. (2011).
Treating addiction: A guide for professionals. New York,
NY: Guilford Press.
Miller, W. R., & Moyers, T. B. (2017). Motivational
interviewing and the clinical science of Carl Rogers.
Journal of Consulting and Clinical Psychology, 85(8),
757–766. doi:10.1037/ccp0000179
Miller, W. R., & Moyers, T. B. (2015). The forest and
the trees: Relational and specific factors in addiction
treatment. Addiction, 110(3), 401–413.
Appendix A 143

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
Miller, W. R., Moyers, T. B., Ernst, D. B., & Amrhein, P. C.
(2008). Manual for the Motivational Interviewing Code
(version 2.1). Albuquerque, NM: Center on Alcoholism,
Substance Abuse, and Addictions, University of New
Mexico. Retrieved from https://casaa.unm.edu/download/
misc.pdf
Miller, W. R., & Rollnick, S. (2014). The effectiveness and
ineffectiveness of complex behavioral interventions:
Impact of treatment fidelity. Contemporary Clinical Trials,
37(2), 234–241. doi:10.1016/j.cct.2014.01.005
Miller, W. R., & Rollnick, S. (2013). Motivational interviewing:
Helping people change (3rd ed.). New York, NY: Guilford
Press.
Miller, W. R., & Rollnick, S. (2010). Looking forward to MI-3:
A work in progress [PowerPoint slides]. Retrieved from
http://motivationalinterviewing.org/sites/default/files/
Forum_2010_Plenary_Bill.ppt
Miller, W. R., & Rollnick, S. (2002). Motivational interviewing:
Preparing people for change (2nd ed.). New York, NY:
Guilford Press.
Miller, W. R., & Rollnick, S. (1991). Motivational interviewing:
Preparing people to change addictive behavior. New
York, NY: Guilford Press.
Miller, W. R., & Rose, G. S. (2013). Motivational interviewing
and decisional balance: Contrasting responses to client
ambivalence. Behavioural and Cognitive Psychotherapy,
43(02), 129–141. doi:10.1017/s1352465813000878
Miller, W. R., & Sanchez, V. C. (1994). Motivating young
adults for treatment and lifestyle change. In G. Howard
& Nathan (Eds.), Alcohol use and misuse by young adults
(pp. 55–82). Notre Dame, IN: University of Notre Dame
Press.
Miller, W. R., & Tonigan, J. S. (1996). Assessing drinkers’
motivation for change: The Stages of Change Readiness
and Treatment Eagerness Scale (SOCRATES). Psychology
of Addictive Behaviors, 10(2), 81–89.
Miller, W. R., Tonigan, J. S., & Longabaugh, R. (1995).
The Drinker Inventory of Consequences (DrInC): An
instrument for assessing adverse consequences of alcohol
abuse, Test manual (vol. 4). Project MATCH Monograph
Series. Rockville, MD: National Institute on Alcohol Abuse
and Alcoholism. Retrieved from https://pubs.niaaa.nih.
gov/publications/projectmatch/match04.pdf
Miller, W. R., & Wilbourne, P. L. (2002). Mesa Grande: A
methodological analysis of clinical trials of treatments
for alcohol use disorders. Addiction, 97(3), 265–277.
doi:10.1046/j.1360-0443.2002.00019.x
Montgomery, L., Robinson, C., Seaman, E. L., & Haeny,
A. M. (2017). A scoping review and meta-analysis
of psychosocial and pharmacological treatments for
cannabis and tobacco use among African Americans.
Psychology of Addictive Behaviors, 31(8), 922–943. www.
ncbi.nlm.nih.gov/pubmed/29199844
Monti, P. M., Colby, S. M., Mastroleo, N. R., Barnett,
N. P., Gwaltney, C. J., Apodaca, T. R., … Cioffi, W. G.
(2014). Individual versus significant-other-enhanced brief
motivational intervention for alcohol in emergency care.
Journal of Consulting and Clinical Psychology, 82(6),
936–948. doi:10.1037/a0037658
Moore, M., Flamez, B., & Szirony, G. M. (2017). Motivational
interviewing and dual diagnosis clients: Enhancing self-
efficacy and treatment completion. Journal of Substance
Use, 23(3), 247–253. doi:10.1080/14659891.2017.13888
56
Moos, R. H. (2012). Iatrogenic effects of psychosocial
interventions: Treatment, life context, and personal
risk factors. Substance Use and Misuse, 47(13–14),
1592–1598. doi:10.3109/10826084.2012.705710
Morgenstern, J., Kuerbis, A., Houser, J., Muench, F. J.,
Shao, S., & Treloar, H. (2016). Within-person associations
between daily motivation and self-efficacy and drinking
among problem drinkers in treatment. Psychology
of Addictive Behaviors, 30(6), 630–638. doi:10.1037/
adb0000204
Mowbray, O., Quinn, A., & Cranford, J. A. (2014). Social
networks and alcohol use disorders: Findings from a
nationally representative sample. American Journal of
Drug and Alcohol Abuse, 40(3), 181–186. doi:10.3109/00
952990.2013.860984
Moyers, T. B. (2014). The relationship in motivational
interviewing. Psychotherapy, 51(3), 358–363.
Retrieved from https://www.researchgate.net/
publication/264396087_The_Relationship_in_
Motivational_Interviewing
Moyers, T. B., & Houck, J. (2011). Combining motivational
interviewing with cognitive–behavioral treatments for
substance abuse: Lessons from the COMBINE research
project. Cognitive and Behavioral Practice, 18(1), 38–45.
doi:10.1016/j.cbpra.2009.09.005
Moyers, T. B., Houck, J., Glynn, L. H., Hallgren, K. A., &
Manuel, J. K. (2017). A randomized controlled trial to
influence client language in substance use disorder
treatment. Drug and Alcohol Dependence, 172, 43–50.
doi:10.1016/j.drugalcdep.2016.11.036
Moyers, T. B., Houck, J., Rice, S. L., Longabaugh, R.,
& Miller, W. R. (2016). Therapist empathy, combined
behavioral intervention, and alcohol outcomes in the
COMBINE research project. Journal of Consulting
and Clinical Psychology, 84(3), 221–229. doi:10.1037/
ccp0000074
Moyers, T. B., Manuel, J. K., & Ernst, D. (2014). Motivational
Interviewing Treatment Integrity Coding Manual
4.1. Unpublished manual. Retrieved from https://
motivationalinterviewing.org/sites/default/files/miti4_2.
pdf
144 Appendix A

TIP 35Appendix A—Bibliography
Moyers, T. B., Martin, T., & Christopher, P. (2005).
Motivational interviewing knowledge test. Albuquerque,
NM: Center on Alcoholism, Substance Abuse, and
Addictions, University of New Mexico. Retrieved
from https://casaa.unm.edu/download/ELICIT/MI%20
Knowledge%20Test.pdf
Moyers, T. B., & Miller, W. R. (2013). Is low therapist
empathy toxic? Psychology of Addictive Behaviors, 273,
878–884. doi:10.1037/a0030274
Mumba, M. N., Findlay, L. J., & Snow, D. E. (2018).
Treatment options for opioid use disorders. Journal of
Addictions Nursing, 29(3), 221–225.
Naar-King, S., Safren, S. A., & Miller, W. R. (2017).
Motivational interviewing and CBT: Combining strategies
for maximum effectiveness. New York, NY: Guilford Press.
Navidian, A., Kermansaravi, F., Tabas, E. E., & Saeedinezhad,
F. (2016). Efficacy of group motivational interviewing
in the degree of drug craving in the addicts under the
methadone maintenance treatment (MMT) in South East
of Iran. Archives of Psychiatric Nursing, 30(2), 144–149.
doi:10.1016/j.apnu.2015.08.002
Norcross, J. C., Krebs, P. M., & Prochaska, J. O. (2011).
Stages of Change. Journal of Clinical Psychology,
67(2), 143–154. Retrieved from www.researchgate.net/
publication/49683193_Stages_of_Change
Novins, D. K., Croy, C. D., Moore, L. A., & Rieckmann, T.
(2016). Use of evidence-based treatments in substance
abuse treatment programs serving American Indian
and Alaska Native communities. Drug and Alcohol
Dependence, 161, 214–221.
Nunes, A. P., Richmond, M. K., Marzano, K., Swenson,
C. J., & Lockhart, J. (2017). Ten years of implementing
screening, brief intervention, and referral to treatment
(SBIRT): Lessons learned. Substance Abuse, 38(4),
508–512. doi:10.1080/08897077.2017.1362369
Office of the Surgeon General. (2016). Facing addiction in
America: The Surgeon General’s report on alcohol, drugs,
and health. Washington, DC: U.S. Department of Health
and Human Services. Retrieved from https://addiction.
surgeongeneral.gov/sites/default/files/surgeon-generals-
report.pdf
Osilla, K. C., Ortiz, J. A., Miles, J. N., Pedersen, E. R.,
Houck, J. M., & Damico, E. J. (2015). How group
factors affect adolescent change talk and substance use
outcomes: Implications for motivational interviewing
training. Journal of Counseling Psychology, 62(1), 79–86.
doi:10.1037/cou0000049
Osterman, R., Lewis, D., & Winhusen, T. (2017). Efficacy of
motivational enhancement therapy to decrease alcohol
and illicit-drug use in pregnant substance users reporting
baseline alcohol use. Journal of Substance Abuse
Treatment, 77, 150–155. doi:10.1016/j.jsat.2017.02.003
Pace, B. T., Dembe, A., Soma, C. S., Baldwin, S. A., Atkins,
D. C., & Imel, Z. E. (2017). A multivariate meta-analysis
of motivational interviewing process and outcome.
Psychology of Addictive Behaviors, 31(5), 524–533.
doi:10.1037/adb0000280
Panebianco, D., Gallupe, O., Carrington, P. J., & Colozzi, I.
(2016). Personal support networks, social capital, and risk
of relapse among individuals treated for substance use
issues. International Journal of Drug Policy, 27, 146–153.
doi:10.1016/j.drugpo.2015.09.009
Polcin, D. L., Mulia, N., & Jones, L. (2012). Substance users’
perspectives on helpful and unhelpful confrontation:
Implications for recovery. Journal of Psychoactive Drugs,
44(2), 144–152.
Prochaska, J. O. (1979). Systems of psychotherapy: A
transtheoretical analysis. Homewood, IL: Dorsey Press.
Prochaska, J. O., & DiClemente, C. C. (1984). The
transtheoretical approach: Crossing traditional
boundaries of therapy. Malabar, FL: R. E. Krieger.
Prochaska, J., Norcross, J., & DiClemente, C. (2013).
Applying the Stages of Change. Psychotherapy in
Australia, 19, 10–15. doi:10.1093/med:psych/9780199845
491.003.0034
Prochaska, J. O., Velicer, W. F., Rossi, J. S., Goldstein, M.
G., Marcus, B.H., Rakowski, W., … Rossi, S.R. (1994).
Stages of Change and decisional balance for 12 problem
behaviors. Health Psychology, 13, 39–46.
Rapp, R. C., Van Den Noortgate, W., Broekaert, E.,
& Vanderplasschen, W. (2014). The efficacy of case
management with persons who have substance abuse
problems: A three-level meta-analysis of outcomes.
Journal of Consulting and Clinical Psychology, 82(4),
605–618. Retrieved from www.ncbi.nlm.nih.gov/books/
NBK241643/
Raylu, N., & Kaur, I. (2012). Factors that affect treatment
expectations of outpatients with substance use problems.
International Journal of Mental Health and Addiction,
10(6), 804–817. doi:10.1007/s11469-012-9377-2
Rhoades, H., Motte-Kerr, W. L., Duan, L., Woo, D., Rice, E.,
Henwood, B., … Wenzel, S. L. (2018). Social networks
and substance use after transitioning into permanent
supportive housing. Drug and Alcohol Dependence, 191,
63–69. doi:10.1016/j.drugalcdep.2018.06.027
Riper, H., Andersson, G., Hunter, S. B., Wit, J. D., Berking,
M., & Cuijpers, P. (2014). Treatment of comorbid alcohol
use disorders and depression with cognitive-behavioural
therapy and motivational interviewing: A meta-analysis.
Addiction, 109(3), 394–406. doi:10.1111/add.12441
Rodriguez, M., Walters, S. T., Houck, J. M., Ortiz, J. A., &
Taxman, F. S. (2017). The language of change among
criminal justice clients: Counselor language, client
language, and client substance use outcomes. Journal
of Clinical Psychology, 74(4), 626–636. doi:10.1002/
jclp.22534
Appendix A 145

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
Rogers, C. R. (1980). A way of being. Boston, MA:
Houghton Mifflin.
Rogers, C. R. (1965). Client-centered therapy. New York,
NY: Houghton Mifflin.
Rollnick, S., Heather, N., Gold, R., & Hall, W. (1992).
Development of a short “readiness to change”
questionnaire for use in brief, opportunistic interventions
among excessive drinkers. British Journal of Addiction,
87, 743–754.
Rollnick, S., Miller, W. R., & Butler, C. C. (2008). Motivational
interviewing in health care: Helping patients change
behavior. New York, NY: Guilford.
Romano, M., & Peters, L. (2016). Understanding the process
of motivational interviewing: A review of the relational
and technical hypotheses. Psychotherapy Research, 26(2),
220–240. doi:10.1080/10503307.2014.954154
Rosengren, D. B. (2018). Building motivational interviewing
skills: A practitioner workbook (2nd ed.). New York, NY:
Guilford Press.
Running Bear, U. R., Beals, J., Novins, D. K., & Manson, S.
M. (2017). Alcohol detoxification completion, acceptance
of referral to substance abuse treatment, and entry
into substance abuse treatment among Alaska Native
people. Addictive Behaviors, 65, 25–32. doi:10.1016/j.
addbeh.2016.09.009
Samson, J. E., & Tanner-Smith, E. E. (2015). Single-session
alcohol interventions for heavy drinking college students:
A systematic review and meta-analysis. Journal of Studies
on Alcohol and Drugs, 76(4), 530–543.
Sarpavaara, H. (2015). Significant others in substance
abusers change talk during motivational interviewing
sessions in the Finnish Probation Service. Nordic Studies
on Alcohol and Drugs, 32(1), 91–103. doi:10.1515/
nsad-2015-0010
Satre, D. D., Delucchi, K., Lichtmacher, J., Sterling, S. A., &
Weisner, C. (2013). Motivational interviewing to reduce
hazardous drinking and drug use among depression
patients. Journal of Substance Abuse Treatment, 44(3),
323–329.
Satre, D. D., Leibowitz, A., Sterling, S. A., Lu, Y., Travis,
A., & Weisner, C. (2016). A randomized clinical trial of
motivational interviewing to reduce alcohol and drug use
among patients with depression. Journal of Consulting
and Clinical Psychology, 84(7), 571–579.
Satre, D. D., Manuel, J. K., Larios, S., Steiger, S., &
Satterfield, J. (2015). Cultural adaptation of screening,
brief intervention and referral to treatment using
motivational interviewing. Journal of Addiction Medicine,
9(5), 352–357. doi:10.1097/adm.0000000000000149
Sayegh, C. S., Huey, S. J., Zara, E. J., & Jhaveri, K. (2017).
Follow-up treatment effects of contingency management
and motivational interviewing on substance use: A
meta-analysis. Psychology of Addictive Behaviors, 31(4),
403–414. doi:10.1037/adb0000277
Schonfeld, L., King-Kallimanis, B. L., Duchene, D. M.,
Etheridge, R. L., Herrera, J. R., Barry, K. L., & Lynn, N.
(2010). Screening and brief intervention for substance
misuse among older adults: The Florida BRITE project.
American Journal of Public Health, 100(1), 108–114.
Schumacher, J. A., Williams, D. C., Burke, R. S., Epler, A.
J., Simon, P., & Coffey, S. F. (2018). Competency-based
supervision in motivational interviewing for advanced
psychology trainees: Targeting an a priori benchmark.
Training and Education in Professional Psychology, 12(3),
149–153. doi:10.1037/tep0000177
Schwalbe, C. S., Oh, H. Y., & Zweben, A. (2014). Sustaining
motivational interviewing: A meta-analysis of training
studies. Addiction, 109(8), 1287–1294. Retrieved
from https://onlinelibrary.wiley.com/doi/abs/10.1111/
add.12558
Scott, C. K., Dennis, M. L., & Lurigio, A. J. (2017).
The effects of specialized probation and recovery
management checkups (RMCs) on treatment
participation, substance use, HIV risk behaviors, and
recidivism among female offenders: Main findings
of a 3-year experiment using subject by intervention
interaction analysis. Journal of Experimental Criminology,
13(1), 53–77.
Shepard, D. S., Lwin, A. K., Barnett, N. P., Mastroleo, N.,
Colby, S. M., Gwaltney, C., & Monti, P. M. (2016). Cost-
effectiveness of motivational intervention with significant
others for patients with alcohol misuse. Addiction, 111(5),
832–839. doi:10.1111/add.13233
Skinner, H. A. (1982). The Drug Abuse Screening Test.
Addictive Behavior, 7(4), 363–371.
Smedslund, G., Berg, R. C., Hammerstrom, K. T., Steiro,
A., Leiknes, K. A., Dahl, H. M., & Karlsen, K. (2011).
Motivational interviewing for substance abuse. Cochrane
Database of Systematic Reviews, 5, CD008063
Smeerdijk, M., Keet, R., Raaij, B. V., Koeter, M., Linszen,
D., Haan, L. D., & Schippers, G. (2015). Motivational
interviewing and interaction skills training for parents
of young adults with recent-onset schizophrenia
and co-occurring cannabis use: 15-month follow-up.
Psychological Medicine, 45(13), 2839–2848. doi:10.1017/
s0033291715000793
Soderlund, P. D. (2017). Effectiveness of
motivational interviewing for improving physical
activity self-management for adults with type 2
diabetes: A review. Chronic Illness, 14(1), 54–68.
doi:10.1177/1742395317699449
Steinberg, M. L., Williams, J. M., Stahl, N. F., Budsock,
P. D., & Cooperman, N. A. (2015). An adaptation of
motivational interviewing increases quit attempts in
smokers with serious mental illness. Nicotine and Tobacco
Research, 18(3), 243–250. doi:10.1093/ntr/ntv043
Stinson, J. D., & Clark, M. D. (2017). Motivational
interviewing with offenders: Engagement, rehabilitation,
and reentry. New York, NY: Guilford Press.
146 Appendix A

TIP 35
Appendix A—Bibliography
Substance Abuse and Mental Health Services
Administration. (2019). Mental health and substance use
disorders. Retrieved from www.samhsa.gov/find-help/
disorders
Substance Abuse and Mental Health Services
Administration. (2018). Key substance use and mental
health indicators in the United States: Results from the
2017 National Survey on Drug Use and Health. HHS
Publication No. (SMA) 18-5068, NSDUH Series H-53.
Rockville, MD: Center for Behavioral Health Statistics and
Quality, Substance Abuse and Mental Health Services
Administration. Retrieved from www.samhsa.gov/data/
Substance Abuse and Mental Health Services
Administration. (2016). Criteria for the demonstration
program to improve community mental health centers
and to establish certified community behavioral health
clinics. Retrieved from Retrieved from www.samhsa.gov/
sites/default/files/programs_campaigns/ccbhc-criteria.pdf
Substance Abuse and Mental Health Services
Administration. (2015a). Substance abuse treatment
and family therapy. Treatment Improvement
Protocol (TIP) Series 39. HHS Publication No. (SMA)
15-4219. Rockville, MD: Substance Abuse and
Mental Health Services Administration. Retrieved
from https://store.samhsa.gov/product/TIP-39-
Substance-Abuse-Treatment-and-Family-Therapy/
SMA15-4219
Substance Abuse and Mental Health Services
Administration. (2015b). Using technology-based
therapeutic tools in behavioral health services.
Treatment Improvement Protocol (TIP) Series 60.
HHS Publication No. (SMA) 15-4924. Rockville,
MD: Substance Abuse and Mental Health Services
Administration. Retrieved from https://store.samhsa.
gov/product/TIP-60-Using-Technology-Based-
Therapeutic-Tools-in-Behavioral-Health-Services/
SMA15-4924
Substance Abuse and Mental Health Services
Administration. (2014a). Improving cultural competence.
Treatment Improvement Protocol (TIP) Series 59. HHS
Publication No. (SMA) 14-4849. Rockville, MD: Substance
Abuse and Mental Health Services Administration.
Retrieved from https://store.samhsa.gov/product/
TIP-59-Improving-Cultural-Competence/SMA15-4849
Substance Abuse and Mental Health Services
Administration. (2014b). Trauma-informed care in
behavioral health services. Treatment Improvement
Protocol (TIP) Series 60. HHS Publication No. (SMA)
14-4816. Rockville, MD: Substance Abuse and
Mental Health Services Administration. Retrieved
from https://store.samhsa.gov/product/TIP-57-
Trauma-Informed-Care-in-Behavioral-Health-Services/
SMA14-4816
Substance Abuse and Mental Health Services
Administration. (2013). Substance abuse treatment
for persons with co-occurring disorders. Treatment
Improvement Protocol (TIP) Series 42. HHS
Publication No. (SMA) 13-3992. Rockville, MD:
Substance Abuse and Mental Health Services
Administration. Retrieved from https://store.
samhsa.gov/product/TIP-42-Substance-Abuse-
Treatment-for-Persons-With-Co-Occurring-Disorders/
SMA13-3992
Substance Abuse and Mental Health Services
Administration. (2009). Clinical supervision and
professional development of the substance abuse
counselor. Treatment Improvement Protocol (TIP)
Series 52. HHS Publication (SMA) 14–4435. Rockville,
MD: Substance Abuse and Mental Health Services
Administration. Retrieved from https://store.samhsa.gov/
product/TIP-52-Clinical-Supervision-and-Professional-
Development-of-the-Substance-Abuse-Counselor/
SMA14-4435.html
Substance Abuse and Mental Health Services
Administration. (planned). Treating addiction in older
adults. Treatment Improvement Protocol (TIP) Series.
Rockville, MD: Substance Abuse and Mental Health
Services Administration.
Substance Abuse and Mental Health Services
Administration, Center for the Application of
Prevention Technologies. (2017). Words matter: How
language choice can reduce stigma. Retrieved from
https://facesandvoicesofrecovery.org/wp-content/
uploads/2019/06/Words-Matter-How-Language-Choice-
Can-Reduce-Stigma.pdf
Substance Abuse and Mental Health Services
Administration & National Institute on Alcohol Abuse
and Alcoholism. (2015). Medication for the treatment of
alcohol use disorder: A brief guide. HHS Publication No.
(SMA) 15-4907. Retrieved from Rockville, MD. Retrieved
from https://store.samhsa.gov/product/Medication-for-
the-Treatment-of-Alcohol-Use-Disorder-A-Brief-Guide/
SMA15-4907
Taleff, M.J. (1997). A handbook to assess and treat
resistance in chemical dependency. Dubuque, IA:
Kendall/Hunt.
Tanner-Smith, E. E., & Lipsey, M. W. (2015). Brief alcohol
interventions for adolescents and young adults:
A systematic review and meta-analysis. Journal of
Substance Abuse Treatment, 51, 1–18.
Teeson, M., Marel, C., Darke, S., Ross, J., Slade, T.,
Burns, L., … Mills, K. L. (2015). Long-term mortality,
remission, criminality and psychiatric comorbidity of
heroin dependence: 11-year findings from the Australian
Treatment Outcome Study. Addiction, 110(6), 986–983.
Appendix A 147

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Timko, C., Kong, C., Vittorio, L., & Cucciare, M. A. (2016).
Screening and brief intervention for unhealthy substance
use in patients with chronic medical conditions: A
systematic review. Journal of Clinical Nursing, 25(21–22),
3131–3143. doi:10.1111/jocn.13244
Truax, C. B., & Carkhuff, R. R. (1967). Toward effective
counseling and psychotherapy. Chicago, IL: Aldine.
Turner, B., & Deane, F. P. (2016). Length of stay as a
predictor of reliable change in psychological recovery
and well-being following residential substance abuse
treatment. Therapeutic Communities, 37(3), 112–120.
doi:10.1108/tc-09-2015-0022
Van Horn, D. H., Drapkin, M., Lynch, K. G., Rennert, L.,
Goodman, J. D., Thomas, T., … McKay, J. R. (2015).
Treatment choices and subsequent attendance by
substance-dependent patients who disengage from
intensive outpatient treatment. Addiction Research and
Theory, 23(5), 391–403.
Vella-Zarb, R. A., Mills, J. S., Westra, H. A., Carter, J.
C., & Keating, L. (2014). A randomized controlled
trial of motivational interviewing self-help versus
psychoeducation self-help for binge eating. International
Journal of Eating Disorders, 48(3), 328–332. doi:10.1002/
eat.22242
Venner, K. L., Feldstein, S. W., & Tafoya, N. (2006).
Native American motivational interviewing: Weaving
Native American and Western practices. Retrieved
from www.integration.samhsa.gov/clinical-practice/
Native_American_MI_Manual.pdf
Venner, K. L., Sánchez, V., Garcia, J., Williams, R. L., &
Sussman, A. L. (2018). Moving away from the tip of the
pyramid: Screening and brief intervention for risky alcohol
and opioid use in underserved patients. Journal of the
American Board of Family Medicine, 31(2), 243–251.
Wagner, A. J., Garbers, R., Lang, A., Borgert, A. J., &
Fisher, M. (2016). Increasing follow-up outcomes of
at-risk alcohol patients using motivational interviewing.
Journal of Trauma Nursing, 23(3), 165–168. doi:10.1097/
jtn.0000000000000200
Wagner, C. C., & Ingersoll, K. S. (2017). Development
and initial validation of the Assessment of Motivational
Interviewing Groups—Observer Scales (AMIGOS).
International Journal of Group Psychotherapy, 68(1),
69–79. doi:10.1080/00207284.2017.1315587
Wagner, C. C., & Ingersoll, K. S. (2013). Motivational
interviewing in groups. New York, NY: Guilford Press.
Walker, D. D., Walton, T. O., Neighbors, C., Kaysen,
D., Mbilinyi, L., Darnell, J., … Roffman, R. A. (2017).
Randomized trial of motivational interviewing plus
feedback for soldiers with untreated alcohol abuse.
Journal of Consulting and Clinical Psychology, 85(2),
99–110. doi:10.1037/ccp0000148
White, W. L. (2014). Slaying the dragon: The history of
addiction treatment and recovery in America (2nd ed.).
Bloomington, IL: Chestnut Health Systems/Lighthouse
Institute.
White, W., & Miller, W. (2007). The use of confrontation in
addiction treatment: History, science and time for change.
Counselor, 8(4), 12–30.
Wild, T. C., Yuan, Y., Rush, B. R., & Urbanoski, K. A. (2016).
Client engagement in legally mandated addiction
treatment: A prospective study using self-determination
theory. Journal of Substance Abuse Treatment, 69, 35–43.
doi:10.1016/j.jsat.2016.06.006
Witkiewitz, K., & Marlatt, G. A. (Eds.). (2007). Therapist’s
guide to evidence-based relapse prevention. Boston, MA:
Elsevier Academic Press.
Wong-Anuchit, C., Chantamit-O-Pas, C., Schneider, J. K.,
& Mills, A. C. (2018). Motivational interviewing–based
compliance/adherence therapy interventions to
improve psychiatric symptoms of people with severe
mental illness: Meta-analysis. Journal of the American
Psychiatric Nurses Association, 107839031876179.
doi:10.1177/1078390318761790
Woolard, R., Baird, J., Longabaugh, R., Nirenberg, T.,
Lee, C. S., Mello, M. J., & Becker, B. (2013). Project
Reduce: Reducing alcohol and marijuana misuse, Effects
of a brief intervention in the emergency department.
Addictive Behaviors, 38(3), 1732–1739. doi:10.1016/j.
addbeh.2012.09.006
Yeh, M., Tung, T., Horng, F., & Sung, S. (2017). Effectiveness
of a psychoeducational programme in enhancing
motivation to change alcohol-addictive behaviour. Journal
of Clinical Nursing, 26(21–22), 3724–3733. doi:10.1111/
jocn.13744
Yudko, E., Lozhkina, O., & Fouts, A. (2007). A
comprehensive review of the psychometric properties
of the Drug Abuse Screening Test. Journal of Substance
Abuse Treatment, 32, 189–198.
148 Appendix A

TIP 35Appendix B—Screening and Assessment Instruments
Appendix B—Screening and Assessment
Instruments
Appendix B presents the following tools:
1.
U.S. Alcohol Use Disorders Identification
Test(U.S. AUDIT)
8.
University of Rhode Island Change
Assessment (URICA) Scale
2.
3.
Drug Abuse Screening Test (DAST-10)
Drinker Inventory of Consequences
(DrInC)(Lifetime)
9.
10.
Alcohol and Drug Consequences
Questionnaire (ADCQ)
Alcohol Decisional Balance Scale
4.
What I Want From Treatment (2.0)
11.
Drug Use Decisional Balance Scale
5.
Readiness to Change Questionnaire
(Treatment Version (RCQ-TV) (Revised)
12.
Brief Situational Confidence
Questionnaire(BSCQ)
6.
Stages of Change Readiness and Treatment
Eagerness Scale–Alcohol (SOCRATES 8A)
13.
Alcohol Abstinence Self-Efficacy
Scale(AASES)
7.
Stages of Change Readiness and Treatment
Eagerness Scale–Drugs (SOCRATES 8D)
14.
Motivational Interviewing Knowledge Test
Appendix B 149

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
1. U.S. Alcohol Use Disorders Identication Test (AUDIT)
Instructions: Alcohol can affect your health and treatment. We ask all clients these questions. Your answers
will remain confidential. Circle the best answer to each question. Think about your drinking in the past
year. A drink means one beer, one small glass of wine (5 oz.), or one mixed drink containing one shot (1.5
oz.) of spirits.
1. How often do you have a drink 6. How often during the last year have you
containingalcohol? needed an alcoholic drink first thing in the
(0) Never [Skip to Questions 9 and 10] morning to get yourself going after a night of
(1)
Less than monthly heavy drinking?
(2) Monthly (0) Never
(3) Weekly (1) Less than monthly
(4) 2 to 3 times a week (2) Monthly
(5) 4 to 6 times a week (3) Weekly
(6) Daily (4) Daily or almost daily
2. How many drinks containing alcohol do you 7. How often during the last year have you had
have on a typical day when you are drinking? a feeling of guilt or remorse after drinking?
(0) 1 (0) Never
(1) 2 (1) Less than monthly
(2) 3 (2) Monthly
(3) 4 (3) Weekly
(4) 5 to 6 (4) Daily or almost daily
(5) 7 to 9
(6) 10 or more
3. How often do you have X (5 for men; 4 for 8. How often during the last year have you
women and men over age 65) or more drinks been unable to remember what happened the
on one occasion? night before because you had been drinking?
(0) Never (0) Never
(1) Less than monthly (1) Less than monthly
(2) Monthly (2) Monthly
(3) Weekly (3) Weekly
(4) 2-3 times a week (4) Daily or almost daily
(5) 4-6 times a week
(6) Daily
[Skip to Questions 9 and 10 if total score for
Questions 2 and 3 = 0]
4. How often during the last year have you 9. Have you or someone else been injured as a
found that you were not able to stop drinking result of your drinking?
once you had started? (0) No
(0) Never (2) Yes, but not in the last year
(1) Less than monthly (4) Yes, during the last year
(2) Monthly
(3) Weekly
(4) Daily or almost daily
Continued on next page
150 Appendix B

TIP 35Appendix B—Screening and Assessment Instruments
5.How often during the last year have you 10. Has a relative, friend, doctor, or another
failed to do what was normally expected from health professional expressed concern about
you because of drinking? your drinking or suggested you cut down?
(0) Never (0) No
(1) Less than monthly (2) Yes, but not in the last year
(2) Monthly (4) Yes, during the last year
(3) Weekly
(4) Daily or almost daily
Scoring
Risk Level Intervention USAUDIT Score Possible AUD (DSM-5,
ICD-10)
Zone I Feedback 0–6/7 (Women/Men) None
Zone II Feedback/brief intervention 7/8–15 (Women/Men) Mild AUD, hazardous use
Zone III Feedback/monitoring/brief
outpatient treatment
16–24 Moderate AUD,
harmfuluse
Zone IV Referral to evaluation
andtreatment
25+ Moderate/severe AUD,
alcohol dependence
Note: Questions 1 to 3 of U.S. AUDIT have been modified to reflect standard drink size in the United
States and differences for men, women, and older adults.
Source: Babor, Higgins-Biddle, & Robaina, 2016. Adapted from material in the public domain.
Appendix B 151

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
2. Drug Abuse Screening Test (DAST-10)
NAME: ____________________________________ DATE: ___________________
DRUG USE QUESTIONNAIRE (DAST-10)
The following questions concern information about your possible involvement with drugs, not including
alcoholic beverages, during the past 12 months. Carefully read each statement and decide if your answer
is "Yes" or "No." Then, circle the appropriate response beside the question.
In the statements, "drug abuse" refers to (1) the use of prescribed or over-the-counter drugs in excess of
the directions and (2) any non-medical use of drugs. The various classes of drugs may include: cannabis
(e.g., marijuana, hash), solvents, tranquillizers (e.g., Valium), barbiturates, cocaine, stimulants (e.g., speed),
hallucinogens (e.g., LSD) or narcotics (e.g.,heroin). Remember that the questions do not include alcoholic
beverages.
Please answer every question. If you have difficulty with a statement, then choose the response that is
mostly right.
Circle your
These questions refer to the past 12 months.
response
1. Have you used drugs other than those required for medical reasons? Yes No
2. Do you abuse more than one drug at a time? Yes No
3. Are you always able to stop using drugs when you want to? Yes No
4. Have you had "blackouts" or "flashbacks" as a result of drug use? Yes No
5. Do you ever feel bad or guilty about your drug use? Yes No
6. Does your spouse (or parents) ever complain about your involvement with drugs? Yes No
7. Have you neglected your family because of your drug use? Yes No
8. Have you engaged in illegal activities in order to obtain drugs? Yes No
9. Have you ever experienced withdrawal symptoms (felt sick) when you stopped Yes No
taking drugs?
10. Have you had medical problems as a result of your drug use (e.g., memory loss, Yes No
hepatitis, convulsions, bleeding, etc.)?
152 Appendix B
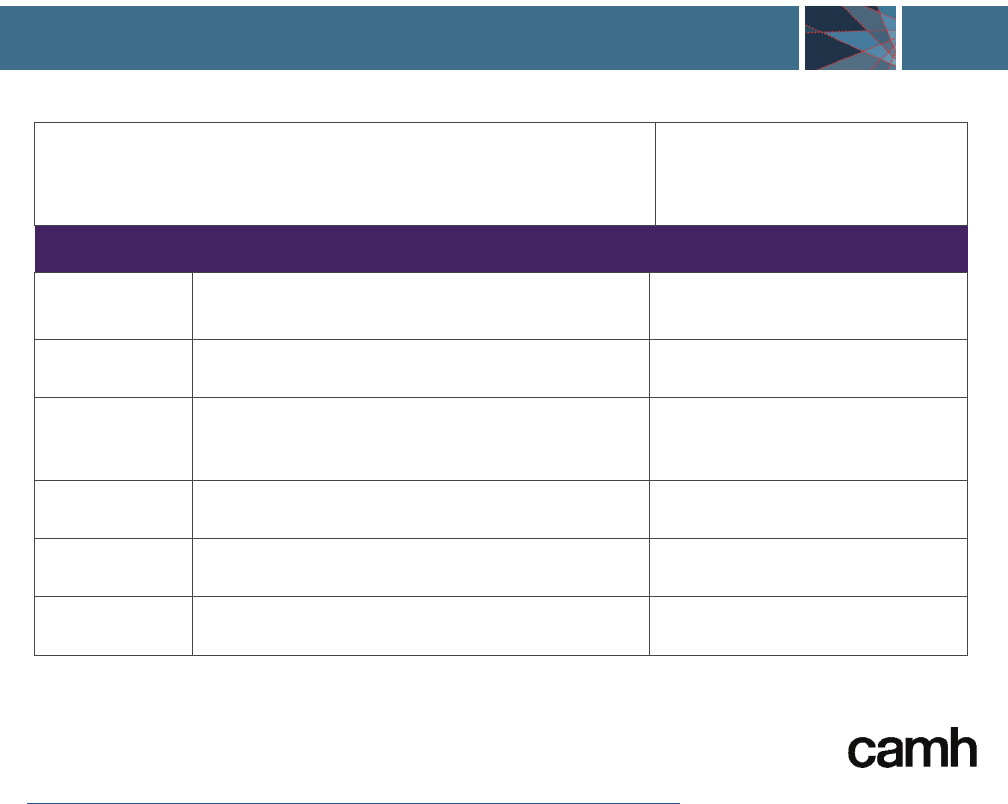
TIP 35
Appendix B—Screening and Assessment Instruments
Scoring: Score 1 point for each question answered "Yes,"
except for question 3, for which a "No" receives 1 point.
Result:
Interpretation of Score
Score Degree of Problems Related to Drug Abuse Suggested Action
0 No problem reported None at this time
1–2 Low level
Monitor, re-access at a
laterdate
3–5 Moderate level Further investigation
6–8 Substantial level Intensive assessment
9–10 Severe level Intensive assessment
5958a/03-2019/PZ074
© Copyright 1982; 2019 by the test author Dr. Harvey Skinner, York University, Toronto, Canada (harvey[email protected])
and by the Centre for Addition and Mental Health, Toronto, Canada ([email protected]).
Sources: Skinner, 1982. Adapted with permission. Available online at no cost
(http://adai.washington.edu/instruments/pdf/Drug_Abuse_Screening_Test_105.pdf).
Appendix B 153

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
3. Drinker Inventory of Consequences (DrInC) (Lifetime)
Has this EVER happened to you? Circle one answer for each item.
No Yes
1. I have had a hangover or felt bad after drinking.
0 1
2. I have felt bad about myself because of my drinking.
0 1
3. I have missed days of work or school because of my drinking.
0 1
4. My family or friends have worried or complained about my drinking.
0 1
5. I have enjoyed the taste of beer, wine, or liquor.
0 1
6. The quality of my work has suffered because of my drinking.
0 1
7. My ability to be a good parent has been harmed by my drinking.
0 1
8. After drinking, I have had trouble with sleeping, staying asleep, or nightmares.
0 1
9. I have driven a motor vehicle after having three or more drinks.
0 1
10. My drinking has caused me to use other drugs more.
0 1
11. I have been sick and vomited after drinking.
0 1
12. I have been unhappy because of my drinking.
0 1
13. Because of my drinking, I have not eaten properly.
0 1
14. I have failed to do what is expected of me because of my drinking.
0 1
15. Drinking has helped me to relax.
0 1
16. I have felt guilty or ashamed because of my drinking.
0 1
17. While drinking, I have said or done embarrassing things.
0 1
18. When drinking, my personality has changed for the worse.
0 1
19. I have taken foolish risks when I have been drinking.
0 1
20. I have gotten into trouble because of drinking.
0 1
21. While drinking or using drugs, I have said harsh or cruel things to someone.
0 1
22. When drinking, I have done impulsive things that I regretted later.
0 1
23. I have gotten into a physical fight while drinking.
0 1
Instructions: Here are a number of events that drinkers sometimes experience. Read each one carefully
and circle the number that indicates whether this has EVER happened to you (0 = No, 1 = Yes). If an item
does not apply to you, circle zero (0).
Continued on next page
154 Appendix B

TIP 35Appendix B—Screening and Assessment Instruments
24. My physical health has been harmed by my drinking.
0 1
25. Drinking has helped me to have a more positive outlook on life.
0 1
26. I have had money problems because of my drinking.
0 1
27. My marriage or love relationship has been harmed by my drinking.
0 1
28. I have smoked tobacco more when I am drinking.
0 1
29. My physical appearance has been harmed by my drinking.
0 1
30. My family has been hurt by my drinking.
0 1
31. A friendship or close relationship has been damaged by my drinking.
0 1
32. I have been overweight because of my drinking.
0 1
33. My sex life has suffered because of my drinking.
0 1
34. I have lost interest in activities and hobbies because of my drinking.
0 1
35. When drinking, my social life has been more enjoyable.
0 1
36. My spiritual or moral life has been harmed by my drinking.
0 1
37. Because of my drinking, I have not had the kind of life that I want.
0 1
38. My drinking has gotten in the way of my growth as a person.
0 1
39. My drinking has damaged my social life, popularity, or reputation.
0 1
40. I have spent too much or lost a lot of money because of my drinking.
0 1
41. I have been arrested for driving under the influence of alcohol.
0 1
42. I have had trouble with the law (other than driving while intoxicated) because
of drinking.
0 1
43. I have lost a marriage or a close love relationship because of my drinking.
0 1
44. I have been suspended/fired from or left a job or school because of drinking.
0 1
45. I drank alcohol normally, without any problems.
0 1
46. I have lost a friend because of my drinking.
0 1
47. I have had an accident while drinking or intoxicated.
0 1
48. While drinking or intoxicated, I have been physically hurt, injured, or burned.
0 1
49. While drinking or intoxicated, I have injured someone else.
0 1
50. I have broken things while drinking or intoxicated.
0 1
Appendix B 155

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
Inter-
Intra-
Impulse
Control
Physical personal
personal
Control
Social Responsibility
Scale*
1 _______
2 _______ 3 _______
4 _______
5 _______
6 _______
7 _______
8 _______
9 _______
10 _______
11 _______
12 _______
13 _______
14 _______
15 _______
16 _______
17 _______
18 _______
19 _______
20 _______
21 _______ 22 _______
23 _______
24 _______
25 _______
26 _______
27 _______
28 _______
29 _______
30 _______
31 _______ 32 _______
33 _______
34 _______
35 _______
36 _______
37 _______
38 _______
39 _______
40 _______
41 _______
42 _______
43 _______
44 _______
45 _______
46 _______
47 _______
48 _______
49 _______
50 _______
________
+
________
+
________
+
________
+
________
=
________ ________
Physical Inter- Intra- Impulse Social Total DrInC Control
personal personal Control Responsibility Score Scale*
Scoring: For each item, copy the circled number from the answer sheet next to the item number above.
Then sum each column to calculate scale totals. Sum these totals to calculate the Total DrInC Score.
* Zero scores on Control Scale items may indicate careless or dishonest responses. The Total DrInC Score reflects the overall
number of alcohol problems that have occurred during the person’s lifetime.
See the test manual for this instrument for more information about scoring and interpreting the score. It also provides the
instruments and scoring information for other versions of DrInC including one for drug use and a short version (SIP) of the
instrument for alcohol and drugs.
Source: Miller, Tonigan, & Longabaugh (1995). Adapted from material in the public domain. Available online at no cost
(https://pubs.niaaa.nih.gov/publications/projectmatch/match04.pdf).
156 Appendix B

TIP 35
Appendix B—Screening and Assessment Instruments
4. What I Want From Treatment (2.0)
Instructions: People have different ideas about what they want, need, and expect from treatment. This
questionnaire is designed to help you explain what you would like to have happen in your treatment.
Many possibilities are listed. For each one, please indicate how much you would like for this to be part
of your treatment. You can do this by circling one number (0, 1, 2, or 3) for each item. This is what the
numbersmean:
0 = No Means that you definitely do NOT want or need this from treatment.
1 = ? Means that you are UNSURE. MAYBE you want this from treatment.
2 = Yes Means that you DO want or need this from treatment.
3 = Yes! Means that you DEFINITELY want or need this from treatment.
For example: Consider item #1, which says, “I want to receive detoxification.” If you definitely do NOT
want or need to receive detoxification, you would circle 0. If you are UNSURE whether you want or need
detoxification, you would circle 1. If you DO want detoxification, you would circle 2. If you DEFINITELY
know that detoxification is an important goal for your treatment, you would circle 3.
If you have any questions about how to use this questionnaire, ask for assistance before you begin.
Do you want this from treatment?
No
0
Maybe
1
Yes
2
Yes!
3
1. I want to receive detoxification, to ease my withdrawal from
alcohol or other drugs.
0 1 2 3
2. I want to find out for sure whether I have a problem with
alcohol or other drugs.
0 1 2 3
3. I want help to stop drinking alcohol completely. 0 1 2 3
4. I want help to decrease my drinking. 0 1 2 3
5. I want help to stop using drugs (other than alcohol). 0 1 2 3
6. I want help to decrease my use of drugs (other than alcohol). 0 1 2 3
7. I want to stop using tobacco. 0 1 2 3
8. I want to decrease my use of tobacco. 0 1 2 3
9. I want help with an eating problem. 0 1 2 3
10. I want help with a gambling problem. 0 1 2 3
11. I want to take Antabuse (medication to help stop drinking). 0 1 2 3
12. I want to take Trexan (medication to help stop using heroin). 0 1 2 3
13. I want to take methadone. 0 1 2 3
14. I want to learn more about alcohol/drug problems. 0 1 2 3
15. I want to learn some skills to keep from returning to alcohol
or other drugs.
0 1 2 3
Continued on next page
Appendix B 157

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
16. I would like to learn more about 12-Step programs like
Alcoholics Anonymous (AA) or Narcotics Anonymous (NA).
0 1 2 3
17. I would like to talk about some personal problems. 0 1 2 3
18. I need to fulfill a requirement of the courts. 0 1 2 3
19. I would like help with problems in my marriage or
closerelationship.
0 1 2 3
20. I want help with some health problems. 0 1 2 3
21. I want help to decrease my stress and tension. 0 1 2 3
22. I would like to improve my health by learning more about
nutrition and exercise.
0 1 2 3
23. I want help with depression or moodiness. 0 1 2 3
24. I want to work on my spiritual growth. 0 1 2 3
25. I want to learn how to solve problems in my life. 0 1 2 3
26. I want help with angry feelings and how I express them. 0 1 2 3
27. I want to have healthier relationships. 0 1 2 3
28. I would like to discuss sexual problems. 0 1 2 3
29. I want to learn to express my feelings in a more healthy way. 0 1 2 3
30. I want to learn how to relax better. 0 1 2 3
31. I want help in overcoming boredom. 0 1 2 3
32. I want help with feelings of loneliness. 0 1 2 3
33. I want to discuss having been physically abused. 0 1 2 3
34. I want help to prevent violence at home. 0 1 2 3
35. I want to discuss having been sexually abused. 0 1 2 3
36. I want to work on having better self-esteem. 0 1 2 3
37. I want help with sleep problems. 0 1 2 3
38. I want help with legal problems. 0 1 2 3
39. I want advice about financial problems. 0 1 2 3
40. I would like help in finding a place to live. 0 1 2 3
41. I could use help in finding a job. 0 1 2 3
42. I want help in overcoming shyness. 0 1 2 3
43. Someone close to me died or left; I would like to talk about it. 0 1 2 3
44. I have thoughts about suicide, and I would like to discuss this. 0 1 2 3
45. I want help with personal fears and anxieties. 0 1 2 3
46. I want help to be a better parent. 0 1 2 3
47. I feel very confused and would like help with this. 0 1 2 3
48. I would like information about or testing for HIV/AIDS. 0 1 2 3
Continued on next page
158 Appendix B

TIP 35Appendix B—Screening and Assessment Instruments
49. I want someone to listen to me. 0 1 2 3
50. I want to learn to have fun without drugs or alcohol. 0 1 2 3
51. I want someone to tell me what to do. 0 1 2 3
52. I want help in setting goals and priorities in my life. 0 1 2 3
53. I would like to learn how to manage my time better. 0 1 2 3
54. I want help to receive SSI/disability payments. 0 1 2 3
55. I want to find enjoyable ways to spend my free time. 0 1 2 3
56. I want help in getting my child(ren) back. 0 1 2 3
57. I would like to talk about my past. 0 1 2 3
58. I need help in getting motivated to change. 0 1 2 3
59. I would like to see a female counselor. 0 1 2 3
60. I would like to see a male counselor. 0 1 2 3
61. I would like to see the counselor I had before. 0 1 2 3
62. I would like to see a doctor or nurse about medical problems. 0 1 2 3
63. I want to receive medication. 0 1 2 3
64. I would like my spouse or partner to be in treatment with me. 0 1 2 3
65. I would like to have private, individual counseling. 0 1 2 3
66. I would like to be in a group with people who are dealing with
problems similar to my own.
0 1 2 3
67. I need childcare while I am in treatment. 0 1 2 3
68. I want my treatment to be short. 0 1 2 3
69. I believe I will need to be in treatment for a long time. 0 1 2 3
Is there anything else you would like from treatment? If so, please write it here.
Source: Miller & Brown, 1994. Available online at no cost
(https://casaa.unm.edu/inst/What%20I%20Want%20From%20Treatment.pdf).
Appendix B 159

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
5. Readiness to Change Questionnaire (Treatment Version) (RCQ-TV)
(Revised)
Instructions: The following questions are designed to identify how you personally feel about your drinking
right now. Please think about your current situation and drinking habits, even if you have given up drinking
completely. Read each question below carefully, and then decide whether you agree or disagree with the
statements. Please tick the answer of your choice to each question. If you have any problems, please ask
the questionnaire administrator.
Your answers are completely private and confidential.
Key: SD = Strongly disagree; D = Disagree; U = Unsure; A = Agree; SA = Strongly agree
SD D U A SA For office use only
1. It’s a waste of time thinking about
my drinking because I do not have
aproblem.
2. I enjoy my drinking but sometimes I drink
too much.
3. There is nothing seriously wrong with
mydrinking.
4. Sometimes I think I should quit or cut
down on my drinking.
5. Anyone can talk about wanting to do
something about their drinking, but I’m
actually doing something about it.
6. I am a fairly normal drinker.
7. My drinking is a problem sometimes.
8. I am actually changing my drinking
habits right now (either cutting down
orquitting).
9. I have started to carry out a plan to cut
down or quit drinking.
10. There is nothing I really need to change
about my drinking.
11. Sometimes I wonder if my drinking is out
of control
12. I am actively working on my
drinkingproblem.
PC
C
PC
C
A
PC
C
A
A
PC
C
A
160 Appendix B

TIP 35
Appendix B—Screening and Assessment Instruments
For Office Use Only
Please enter the subject’s scores below:
Scale Scores
PC Score _______
C Score _______
A Score _______
Scoring: The scale score codes represent each of the Stages of Change:
•
Items numbered 1,3,6,10 = Precontemplation (PC)
•
Items numbered 2,4,7,11 = Contemplation (C)
•
Items numbered 5,8,9,12 = Action (A)
All items should be scored on a 5-point scale ranging from:
-2 = Strongly Disagree
-1 = Disagree
0 = Unsure
+1 = Agree
+2 = Strongly Agree
To calculate the score for each scale, simply add the item scores for the scale in question. The range of
each scale is -10 through 0 to +10. A negative scale score reflects an overall disagreement with items
measuring the stage of change, whereas a positive score represents overall agreement. The highest scale
score represents the Stage of Change Designation.
If two or more scale scores are equal, then the scale farther along the continuum of change
(Precontemplation-Contemplation-Action) represents the subject’s Stage of Change Designation. For
example, if a subject scores 6 on the Precontemplation scale, 6 on the Contemplation scale and -2 on the
Action scale, then the subject is assigned to the Contemplation stage.
If one of the five items on a scale is missing, the subject’s score for that scale should be prorated (i.e.,
multiplied by 4/3 or 1.33). If two or more items are missing, the scale score cannot be calculated. In this
case the Stage of Change Designation will be invalid.
Source: Heather & Honekopp, 2008. Adapted with permission. Source article and questionnaire are
available online at no cost (https://ndarc.med.unsw.edu.au/sites/default/files/ndarc/resources/TR.019.pdf).
Appendix B 161

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
6. Stages of Change Readiness and Treatment Eagerness Scale–Alcohol
(SOCRATES 8A)
Instructions: Please read the following statements carefully. Each one describes a way that you might (or
might not) feel about your drinking. For each statement, circle one number from 1 to 5 to indicate how
much you agree or disagree with it right now. Please circle one and only one number for every statement.
No!
Strongly
Disagree
No
Disagree
?
Undecided
or Unsure
Yes
Agree
Yes!
Strongly
Agree
1. I really want to make changes in
my drinking.
1 2 3 4 5
2. Sometimes I wonder if I am
analcoholic.
1 2 3 4 5
3. If I don’t change my drinking
soon, my problems are going to
get worse.
1 2 3 4 5
4. I have already started making
some changes in my drinking.
1 2 3 4 5
5. I was drinking too much at one
time, but I’ve managed to change
my drinking.
1 2 3 4 5
6. Sometimes I wonder if my
drinking is hurting other people.
1 2 3 4 5
7. I am a problem drinker.
1 2 3 4 5
8. I’m not just thinking about
changing my drinking, I’m already
doing something about it.
1 2 3 4 5
9. I have already changed my
drinking, and I am looking for
ways to keep from slipping back
to my old pattern.
1 2 3 4 5
10. I have serious problems
withdrinking.
1 2 3 4 5
11. Sometimes I wonder if I am in
control of my drinking.
1 2 3 4 5
Continued on next page
162 Appendix B

TIP 35Appendix B—Screening and Assessment Instruments
12. My drinking is causing a lot
ofharm.
1 2 3 4 5
13. I am actively doing things now to
cut down or stop drinking.
1 2 3 4 5
14. I want help to keep from going
back to the drinking problems
that I had before.
1 2 3 4 5
15. I know that I have a
drinkingproblem.
1 2 3 4 5
16. There are times when I wonder if
I drink too much.
1 2 3 4 5
17. I am an alcoholic.
1 2 3 4 5
18. I am working hard to change
mydrinking.
1 2 3 4 5
19. I have made some changes in my
drinking, and I want some help to
keep from going back to the way
I used to drink.
1 2 3 4 5
See the scoring and interpretation information presented in the SOCRATES 8D tool below for the
SOCRATES 8A tool presented on this page.
Appendix B 163

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
7. Stages of Change Readiness and Treatment Eagerness Scale–Drug
(SOCRATES 8D)
Instructions: Please read the following statements carefully. Each describes a way you might (or might not)
feel about your drug use. For each statement, circle one number from 1 to 5 to indicate how much you
agree or disagree with it right now. Please circle one and only one number for each statement.
No!
Strongly
Disagree
No
Disagree
?
Undecided
or Unsure
Yes
Agree
Yes!
Strongly
Agree
1. I really want to make changes in
my use of drugs.
1 2 3 4 5
2. Sometimes I wonder if I am
anaddict.
1 2 3 4 5
3. If I don’t change my drug use
soon, my problems are going to
get worse.
1 2 3 4 5
4. I have already started making
some changes in my use of drugs.
1 2 3 4 5
5. I was using drugs too much at
one time, but I’ve managed to
change that.
1 2 3 4 5
6. Sometimes I wonder if my drug
use is hurting other people.
1 2 3 4 5
7. I have a drug problem.
1 2 3 4 5
8. I’m not just thinking about
changing my drug use, I’m
already doing something about it.
1 2 3 4 5
9. I have already changed my drug
use, and I am looking for ways to
keep from slipping back to my
old pattern.
1 2 3 4 5
10. I have serious problems
withdrugs.
1 2 3 4 5
11. Sometimes I wonder if I am in
control of my drug use.
1 2 3 4 5
Continued on next page
164 Appendix B

TIP 35Appendix B—Screening and Assessment Instruments
12. My drug use is causing a lot
ofharm.
1 2 3 4 5
13. I am actively doing things now
to cut down or stop my use
ofdrugs.
1 2 3 4 5
14. I want help to keep from going
back to the drug problems that I
had before.
1 2 3 4 5
15. I know that I have a
drugproblem.
1 2 3 4 5
16. There are times when I wonder if
I use drugs too much.
1 2 3 4 5
17. I am a drug addict.
1 2 3 4 5
18. I am working hard to change my
drug use.
1 2 3 4 5
19. I have made some changes in my
drug use, and I want some help
to keep from going back to the
way I used before.
1 2 3 4 5
Appendix B 165

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
SOCRATES Scoring Form (19-Item Version 8A & 8D): Transfer the client’s answers from questionnaire:
Recognition (Re)
Ambivalence (Am)
Taking Steps (Ts)
1 _________
2 _________
4 _________
3 _________
5 _________
6 _________
7 _________
8 _________
9 _________
10 _________
11 _________
12 _________
13 _________
14 _________
15 _________
16 _________
17 _________
18 _________
19 _________
Totals:
Re: _________
Am: _________
Ts: _________
Possible Range:
7–35
4–20
8–40
SOCRATES Profile Sheet (19-Item Version 8A & 8D)
Instructions: From the SOCRATES Scoring Form above (19-Item Version) transfer the Totals to
the appropriate Raw Scores cells below. Then for each scale, CIRCLE the same value above it
to determine the decile range.
Decile Scores Recognition Ambivalence Taking Steps
90 (Very High) 19–20 39–40
80 18 37–38
70 (High) 35 17 36
60 34 16 34–35
50 (Medium) 32–33 15 33
40 31 14 31–32
30 (Low) 29–30 12–13 30
20 27–28 9–11 26–29
10 (Very Low) 7–26 4–8 8–25
Raw Scores
(from Scoring Sheet)
Re= Am= Ts=
These interpretive ranges are based on a sample of 1,726 adult men and women presenting for treatment
of alcohol problems through Project MATCH. Note that individual scores are therefore being ranked as
low, medium, or high relative to people already presenting for alcohol treatment.
166 Appendix B

TIP 35Appendix B—Screening and Assessment Instruments
Guidelines for Interpretation of SOCRATES-8A Scores: Using the SOCRATES Profile Sheet, circle the
client’s Raw Score within each of the three columns. This provides information as to whether the client’s
scores are low, average, or high relative to people already seeking treatment for alcohol problems. The
following descriptions are provided as general guidelines for interpretation of scores, but it is wise in
an individual case also to examine individual item responses for additional information. The information
should be adjusted as necessary when addressing drug problems.
Recognition High scorers directly acknowledge that they are having problems related to
their drinking, tending to express a desire for change and to perceive that
harm will continue if they do not change.
Low scorers deny that alcohol is causing them serious problems, reject
diagnostic labels such as “problem drinker” and “alcoholic,” and do not
express a desire for change.
Ambivalence High scorers say that they sometimes wonder if they are in control of their
drinking, are drinking too much, are hurting other people, and/or are
alcoholic. Thus a high score reflects ambivalence or uncertainty. A high score
here reflects some openness to reflection, as might be particularly expected in
the Contemplation stage of change.
Low scorers say that they do not wonder whether they drink too much, are
in control, are hurting others, or are alcoholic. Note that a person may score
low on ambivalence either because they “know” their drinking is causing
problems (high Recognition), or because they “know” that they do not have
drinking problems (low Recognition). Thus a low Ambivalence score should be
interpreted in relation to the Recognition score.
Taking Steps High scorers report that they are already doing things to make a positive
change in their drinking and may have experienced some success in this
regard. Change is underway, and they may want help to persist or to prevent
backsliding. A high score on this scale has been found to be predictive of
successful change.
Low scorers report that they are not currently doing things to change their
drinking, and have not made such changes recently.
Source: Miller & Tonigan, 1996. SOCRATES-8A and SOCRATES-8D are in the public domain and available online at no cost
(https://casaa.unm.edu/inst/socratesv8.pdf).
Appendix B 167

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
8. University of Rhode Island Change Assessment (URICA) Scale
Instructions: Each statement below describes how a person might feel when starting therapy or
approaching problems in his life. Please indicate the extent to which you tend to agree or disagree with
each statement. In each case, make your choice in terms of how you feel right now, not what you have
felt in the past or would like to feel. For all the statements that refer to your “problem,” answer in terms
of problems related to your drinking (or illicit drug use). The words “here” and “this place” refer to your
treatment center.
There are five possible responses to each of the items in the questionnaire:
1 = Strongly Disagree
2 = Disagree
3 = Undecided
4 = Agree
5 = Strongly Agree
Circle the number that best describes how much you agree or disagree with each statement.
Statement Strongly
Disagree
Disagree Undecided Agree Strongly
Agree
1. As far as I’m concerned, I
don’t have any problems that
needchanging.
1 2 3 4 5
2. I think I might be ready for some
self-improvement.
1 2 3 4 5
3. I am doing something about
the problems that had been
botheringme.
1 2 3 4 5
4. It might be worthwhile to work on
my problem.
1 2 3 4 5
5. I’m not the problem one. It doesn’t
make much sense for me to
consider changing.
1 2 3 4 5
6. It worries me that I might slip
back on a problem I have already
changed, so I am looking for help.
1 2 3 4 5
7. I am finally doing some work on
myproblem.
1 2 3 4 5
8. I’ve been thinking that I might want
to change something about myself.
1 2 3 4 5
Continued on next page
168 Appendix B

TIP 35Appendix B—Screening and Assessment Instruments
9. I have been successful in working
on my problem, but I’m not sure I
can keep up the effort on my own.
1 2 3 4 5
10. At times my problem is difficult, but
I’m working on it.
1 2 3 4 5
11. Trying to change is pretty much
a waste of time for me because
the problem doesn’t have to do
withme.
1 2 3 4 5
12. I’m hoping that I will be able to
understand myself better.
1 2 3 4 5
13. I guess I have faults, but there’s
nothing that I really need
tochange.
1 2 3 4 5
14. I am really working hard to change. 1 2 3 4 5
15. I have a problem, and I really think I
should work on it.
1 2 3 4 5
16. I’m not following through with what
I had already changed as well as I
had hoped, and I want to prevent a
relapse of the problem.
1 2 3 4 5
17. Even though I’m not always
successful in changing, I am at least
working on my problem.
1 2 3 4 5
18. I thought once I had resolved the
problem I would be free of it,
but sometimes I still find myself
struggling with it.
1 2 3 4 5
19. I wish I had more ideas on how to
solve my problem.
1 2 3 4 5
20. I have started working on my
problem, but I would like help.
1 2 3 4 5
21. Maybe this place will be able to
help me.
1 2 3 4 5
22. I may need a boost right now to
help me maintain the changes I’ve
already made.
1 2 3 4 5
Continued on next page
Appendix B 169

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
23. I may be part of the problem, but I
don’t really think I am.
1 2 3 4 5
24. I hope that someone will have some
good advice for me.
1 2 3 4 5
25. Anyone can talk about changing;
I’m actually doing something
aboutit.
1 2 3 4 5
26. All this talk about psychology is
boring. Why can’t people just
forget about their problems?
1 2 3 4 5
27. I’m here to prevent myself from
having a relapse of my problem.
1 2 3 4 5
28. It is frustrating, but I feel I might be
having a recurrence of a problem I
thought I had resolved.
1 2 3 4 5
29. I have worries, but so does the
next guy. Why spend time thinking
about them?
1 2 3 4 5
30. I am actively working on
myproblem.
1 2 3 4 5
31. I would rather cope with my faults
than try to change them.
1 2 3 4 5
32. After all I had done to try to change
my problem, every now and again it
comes back to haunt me.
1 2 3 4 5
Scoring
Precontemplation items 1, 5, 11, 13, 23, 26, 29, 31
Contemplation items 2, 4, 8, 12, 15, 19, 21, 24
Action items 3, 7, 10, 14, 17, 20, 25, 30
Maintenance items 6, 9, 16, 18, 22, 27, 28, 32
High scores on a SOC subscale indicate that the respondent is likely in that SOC. However, the
SOC subscales are designed to be a continuous measure, therefore, the stages are not discrete and
respondents can score high on more than one of the four stages.
Source: McConnaghy, Prochaska, & Velcier, 1983. Reprinted from material in the public domain. Available online at no cost
(https://web.uri.edu/cprc/psychotherapy-urica).
170 Appendix B
TIP 35
__________________________________________________________________________________
Appendix B—Screening and Assessment Instruments
9. Alcohol and Drug Consequences Questionnaire (ADCQ)
Instructions: There can be good and bad consequences to any change. These consequences may not be
the same for everyone. In thinking about your decision to change your alcohol or drug use, we would like
to know what consequences are important to you. This is not a test: There are no right or wrong answers.
We simply want to know what you think.
My primary problem drug is (write in name of primary drug, e.g., alcohol, cocaine)
All questions below refer to my primary drug use.
When I consider stopping or cutting down my primary drug use, the following reasons are important to
me. “IF I STOP OR CUT DOWN . . . .”
Circle the number which applies to you.
Not
Important
Slightly
Important
Moderately
Important
Very
Important
Extremely
Important
Not
Applicable
1. I will feel
betterphysically.
1 2 3 4 5 0
2. I will have
difficultyrelaxing.
1 2 3 4 5 0
3. I will change a lifestyle
Ienjoy.
1 2 3 4 5 0
4. I will have fewer
problems with my family.
1 2 3 4 5 0
5. I will feel frustrated
andanxious.
1 2 3 4 5 0
6. I will have more money
to do other things with.
1 2 3 4 5 0
7. I will be more active
andalert.
1 2 3 4 5 0
8. I will get depressed. 1 2 3 4 5 0
9. I will have fewer
problems with friends.
1 2 3 4 5 0
10. I will feel better
aboutmyself.
1 2 3 4 5 0
11. I will regain some
self-respect.
1 2 3 4 5 0
12. I will accomplish more
of the things I want to
getdone.
1 2 3 4 5 0
Continued on next page
Appendix B 171

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
13. I will have a better
relationship with
myfamily.
1 2 3 4 5 0
14. I will have difficulty
coping with
myproblems.
1 2 3 4 5 0
15. I will feel withdrawal
orcraving.
1 2 3 4 5 0
16. I will have too much time
on my hands.
1 2 3 4 5 0
17. I will have difficulty not
drinking or using drugs.
1 2 3 4 5 0
18. My health will improve. 1 2 3 4 5 0
19. I will live longer. 1 2 3 4 5 0
20. I will be more in control
of life.
1 2 3 4 5 0
21. I will feel bored. 1 2 3 4 5 0
22. I will be irritable. 1 2 3 4 5 0
23. I will be more
financiallystable.
1 2 3 4 5 0
24. I will miss the taste. 1 2 3 4 5 0
25. I will have a better
relationship with
myfriends.
1 2 3 4 5 0
26. I will feel stressed out. 1 2 3 4 5 0
27. I will save more money. 1 2 3 4 5 0
28. I will miss the feeling of
being high.
1 2 3 4 5 0
Scoring: Scale scores are derived by summing benefits and cost items, dividing by the maximum possible
subscale score, and multiplying by 100.
Benefits Score: Total the scores on items 1, 4, 6, 7, 9, 10, 11, 12, 13, 18, 19, 20, 23, 25, and 27. Divide the
total score by the maximum score of 75 (15 items X 5). Multiple by 100. Score: ________
Costs Score: Total the scores on items 2, 3, 5, 8, 14, 15, 16, 17, 21, 22, 24, 26, and 28. Divide the total
score by the maximum score of 65 (13 items X 5). Multiple by 100. Score: ________
Source: Cunningham, Sobell, Gavin, Sobell, & Breslin, 1997. Adapted with permission.
172 Appendix B

TIP 35
Appendix B—Screening and Assessment Instruments
10. Alcohol Decisional Balance Scale
Client ID#: __________________ Date: ______/______/______ Assessment Point: _____________
Instructions: The following statements may play a part in making a decision about using alcohol. We would
like to know how important each statement is to you at the present time in relation to making a decision
about your using alcohol. Please rate the level of importance to each statement on the following 5 points:
1 = Not important at all
2 = Slightly important
3 = Moderately important
4 = Very important
5 = Extremely important
Please read each statement and circle the number on the right to indicate how you rate its level of
importance as it relates to your making a decision about whether to drink at the present time.
How important is this to me? Not at All Slightly Moderately Very Extremely
1. My drinking causes problems
withothers.
1 2 3 4 5
2. I like myself better when I am drinking. 1 2 3 4 5
3. Because I continue to drink some
people think I lack the character to quit.
1 2 3 4 5
4. Drinking helps me deal with problems. 1 2 3 4 5
5. Having to lie to others about my
drinking bothers me.
1 2 3 4 5
6. Some people try to avoid me when
Idrink.
1 2 3 4 5
7. Drinking helps me to have fun
andsocialize.
1 2 3 4 5
8. Drinking interferes with my functioning
at home or/and at work.
1 2 3 4 5
9. Drinking makes me more of a
funperson.
1 2 3 4 5
10. Some people close to me are
disappointed in me because of my
drinking.
1 2 3 4 5
Continued on next page
Appendix B 173

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
11. Drinking helps me to loosen up and
express myself.
1 2 3 4 5
12. I seem to get myself into trouble
whendrinking.
1 2 3 4 5
13. I could accidentally hurt someone
because of my drinking.
1 2 3 4 5
14. Not drinking at a social gathering would
make me feel too different.
1 2 3 4 5
15. I am losing the trust and respect of my
coworkers and/or spouse because of
my drinking.
1 2 3 4 5
16. My drinking helps give me energy and
keeps me going.
1 2 3 4 5
17. I am more sure of myself when I
amdrinking.
1 2 3 4 5
I am setting a bad example for others
18.
with my drinking.
1 2 3 4 5
Without alcohol, my life would be dull
19.
and boring.
1 2 3 4 5
People seem to like me better when I
20.
amdrinking.
1 2 3 4 5
Scoring
Pros of Drinking Cons of Drinking
2, 4, 7, 9, 11, 14, 16, 17, 19, 20 1, 3, 5, 6, 8, 10, 12, 13, 15, 18
To get the average number of Pros endorsed, add up the total number of points from the items and divide
by 10.
Pros of drinking alcohol (2+4+7+9+11+14+16+17+19+20) / (10 possible items for drinking) = Sum of items
To get the average number of Cons endorsed, add up the total number of points from the items and divide
by 10.
Cons of drinking alcohol (1+3+5+6+8+10+12+13+15+18) / (10 possible items for not drinking) = Sum of
items
To calculate the difference score, subtract the Cons from the Pros. If the number is positive, the individual is
endorsing more Pros than Cons for drinking alcohol or using drugs. If the number is negative, the individual
is endorsing more Cons then Pros for drinking alcohol.
Source: Prochaska et al., 1994. Reprinted from material in the public domain. Available online at no cost
(https://habitslab.umbc.edu/files/2014/07/Alcohol-Decisional-Balance-scale.pdf).
174 Appendix B

TIP 35
Appendix B—Screening and Assessment Instruments
11. Drug Use Decisional Balance Scale
Client ID#: ___________________ Date: _____/______/______ Assessment Point: _____________
Instructions: The following statements may play a part in making a decision about using drugs. We would
like to know how important each statement is to you at the present time in relation to making a decision
about your using drugs. Please rate the level of importance to each statement on the following 5 points:
1=Not important at all
2=Slightly important
3=Moderately important
4=Very important
5=Extremely important
Please read each statement and circle the number on the right to indicate how you rate its level of
importance as it relates to your making a decision about whether to use drugs at the present time.
How important is this to me? Not at All Slightly Moderately Very Extremely
1. My drug use causes problems
withothers.
1 2 3 4 5
2. I like myself better when I am
usingdrugs.
1 2 3 4 5
3. Because I continue to use drugs some
people think I lack the character to quit.
1 2 3 4 5
4. Using drugs helps me deal
withproblems.
1 2 3 4 5
5. Having to lie to others about my drug
use bothers me.
1 2 3 4 5
6. Some people try to avoid me when I
use drugs.
1 2 3 4 5
7. Drug use helps me to have fun
andsocialize.
1 2 3 4 5
8. Drug use interferes with my functioning
at home or/and at work.
1 2 3 4 5
9. Drug use makes me more of a
funperson.
1 2 3 4 5
10. Some people close to me are
disappointed in me because of my
druguse.
1 2 3 4 5
Continued on next page
Appendix B 175
TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
11. Drug use helps me to loosen up and
express myself.
1 2 3 4 5
12. I seem to get myself into trouble when I
use drugs.
1 2 3 4 5
13. I could accidentally hurt someone
because of my drug use.
1 2 3 4 5
14. Not using drugs at a social gathering
would make me feel too different.
1 2 3 4 5
15. I am losing the trust and respect of my
coworkers and/or spouse because of
my drug use.
1 2 3 4 5
16. My drug use helps give me energy and
keeps me going.
1 2 3 4 5
17. I am more sure of myself when I am
using drugs.
1 2 3 4 5
I am setting a bad example for others
18.
with my drug use.
1 2 3 4 5
Without drugs, my life would be dull
19.
andboring.
1 2 3 4 5
People seem to like me better when I
20.
usedrugs.
1 2 3 4 5
Scoring
Pros of Using Drugs Cons of Using Drugs
2, 4, 7, 9, 11, 14, 16, 17, 19, 20 1, 3, 5, 6, 8, 10, 12, 13, 15, 18
To get the average number of Pros endorsed, add up the total number of points from the items and divide
by 10.
Pros of drug use (2+4+7+9+11+14+16+17+19+20) / (10 possible items for using drugs)= Sum of items
To get the average number of Cons endorsed, add up the total number of points from the items and
divide by 10.
Cons of drug use (1+3+5+6+8+10+12+13+15+18) / (10 possible items for not using drugs) = Sum of items
To calculate the difference score, subtract the Cons from the Pros. If the number is positive, the individual
is endorsing more Pros than Cons for using drugs. If the number is negative, the individual is endorsing
more Cons then Pros for using drugs.
Source: Prochaska et al., 1994. Reprinted from material in the public domain. Available online at no cost
(https://habitslab.umbc.edu/files/2014/07/Drug-Decisional-Balance-scale20item.pdf).
176 Appendix B
TIP 35
Appendix B—Screening and Assessment Instruments
12. Brief Situational Condence Questionnaire (BSCQ)
Name: _________________________________ Date:_________________________
Instructions: Listed below are eight types of situations in which some people experience an alcohol or
drug problem. Imagine yourself as you are right now in each of the following types of situations. Indicate
on the scale provided how confident you are right now that you will be able to resist drinking heavily or
resist the urge to use your primary drug in each situation by placing an “X” along the line, from 0% “Not at
all confident” to 100% “Totally confident.”
Right now I would be able to resist the urge to drink heavily or use my primary drug in
situations involving…
1. UNPLEASANT EMOTIONS (e.g., if I were depressed about things in general; if everything were going
badly for me).
I feel…
0% 100%
Not at all confident Totally confident
2. PHYSICAL DISCOMFORT (e.g., if I were to have trouble sleeping; if I felt jumpy and physically tense).
I feel…
0% 100%
Not at all confident Totally confident
3. PLEASANT EMOTIONS (e.g., if something good happened and I felt like celebrating; if everything were
going well).
I feel…
0% 100%
Not at all confident Totally confident
Right now I would be able to resist the urge to drink heavily or use my primary drug in situations
involving…
4. TESTING CONTROL OVER MY USE OF ALCOHOL OR DRUGS (e.g., if I were to start to believe
that alcohol or drugs were no longer a problem for me; if I felt confident that I could handle drugs or
severaldrinks).
I feel…
0% 100%
Not at all confident Totally confident
Continued on next page
Appendix B 177

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
5. URGES AND TEMPTATIONS (e.g., if I suddenly had an urge to drink or use drugs; if I were in a situation
where I had often used drugs or drank heavily).
I feel…
0% 100%
Not at all confident Totally confident
6. CONFLICT WITH OTHERS (e.g., if I had an argument with a friend; if I were not getting along well with
others at work).
I feel…
0% 100%
Not at all confident Totally confident
7. SOCIAL PRESSURE TO USE (e.g., if someone were to pressure me to “be a good sport” and drink or
use drugs with him; if I were invited to someone’s home and he offered me a drink or drugs).
I feel…
0% 100%
Not at all confident Totally confident
8. PLEASANT TIMES WITH OTHERS (e.g., if I wanted to celebrate with a friend; if I were enjoying myself at
a party and wanted to feel even better).
I feel…
0% 100%
Not at all confident Totally confident
Scoring: Each of the 8 scales produces a score from 0% to 100 %. Identify 1 to 3 situations where the client
has the lowest confidence rating for further discussion.
Instructions for presenting findings to clients are available online (www.nova.edu/gsc/forms/BSCQ%20
Instructions.pdf).
A blank self-confidence profile chart is available online (www.nova.edu/gsc/forms/BSCQ%20blank.pdf).
Source: Bresslin, Sobell, & Sobell, 2000. Adapted from material in the public domain.
178 Appendix B

TIP 35Appendix B—Screening and Assessment Instruments
13. Alcohol Abstinence Self-Ecacy Scale (AASES)
Name: _____________________________________ Date: ______/______/______
Instructions: Listed below are a number of situations that lead some people to use alcohol. We would like
to know how confident you are that you would not drink alcohol in each situation.
Circle the number that best describes your feelings of confidence not to drink alcohol in each situation
during the past week according to the following scale:
1 = Not at all confident
2 = Not very confident
3 = Moderately confident
4 = Very confident
5 = Extremely confident
Situation
Not at all Not very Moderately Very Extremely
1. When I am in agony because of
stopping or withdrawing from
alcohol use.
1 2 3 4 5
2. When I have a headache. 1 2 3 4 5
3. When I am feeling depressed. 1 2 3 4 5
4. When I am on vacation and want
torelax.
1 2 3 4 5
5. When I am concerned
aboutsomeone.
1 2 3 4 5
6. When I am worried. 1 2 3 4 5
7. When I have the urge to try just one
drink to see what happens.
1 2 3 4 5
8. When I am being offered a drink in a
social situation.
1 2 3 4 5
9. When I dream about taking a drink. 1 2 3 4 5
10. When I want to test my will power
over drinking.
1 2 3 4 5
11. When I am feeling a physical need or
craving for alcohol.
1 2 3 4 5
Confdent not to drink alcohol
Continued on next page
Appendix B 179

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
12. When I am physically tired. 1 2 3 4 5
13. When I am experiencing some
physical pain or injury.
1 2 3 4 5
14. When I feel like blowing up because
of frustration.
1 2 3 4 5
15. When I see others drinking at a bar
or a party.
1 2 3 4 5
16. When I sense everything is going
wrong for me.
1 2 3 4 5
17. When people I used to drink with
encourage me to drink.
1 2 3 4 5
18. When I am feeling angry inside. 1 2 3 4 5
19. When I experience an urge or
impulse to take a drink that catches
me unprepared.
1 2 3 4 5
20. When I am excited or celebrating
with others.
1 2 3 4 5
Scoring:
Subscale Item Number
Negative Affect 1,3,9
Social/Positive 10,11,12
Physical and Other Concerns 2,7,8
Cravings and Urges 4,5,6
To obtain a mean overall Abstinence Self-Efficacy or Temptation score, sum scores from all items and
divide by 12.
To obtain mean scores for individual subscales, sum item scores for each subscale and divide by the
number of items (3).
Source: DiClemente, Carbonari, Montgomery, & Hughes, 1994. Adapted from material in the public domain.
AASES available online at no cost
(https://habitslab.umbc.edu/files/2014/07/Alcohol-Abstinence-Self-efficacy-Scale-20item.pdf).
Drug Abstinence Self-Efficacy Scale (adapted version of AASES) available online at no cost
(https://habitslab.umbc.edu/files/2014/07/Drug-Abstinence-Self-efficacy-scale.pdf).
180 Appendix B

TIP 35Appendix B—Screening and Assessment Instruments
14. Motivational Interviewing Knowledge Test
Instructions: Choose the best answer for each of the following questions. Each question has only one
correct answer.
1.
Which of the following is NOT consistent with the MI approach to counseling?
a) rolling with resistance
b) avoiding argumentation
c) confronting denial
d) supporting self-efficacy
2.
Within the MI framework, advice may be given by a therapist to a client
a) at any time
b) when the client requests it
c) after the therapist receives permission to give it
d) never
e) both a and b
f) both b and c
3.
According to Miller and Rollnick (1991), when a therapist argues that a client’s
behavior needs to change, the client often responds by
a) accepting the need for change
b) arguing against change
c) asking for advice
d) moving to the next stage in the process of change
e) all of the above
4.
Two strategies which are usually effective for avoiding the confrontation-denial
trap are
a) giving advice and reflective listening
b) reflective listening and eliciting self-motivational statements
c) skills training and warning
d) aversive conditioning and supporting self-efficacy
5.
The MI approach is
a) completely non-directive
b) highly authoritarian
c) directive but client-centered
d) primarily educational
e) all of the above
6.
To develop discrepancy, therapists using the MI approach
a) inform clients about the harmful effects of their behavior
b) direct clients to stop the problem behavior
c) warn clients about the future consequences of their behavior
d) point out differences between the client’s own stated goals and current behavior
e) none of the above
Continued on next page
Appendix B 181

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
7.
According to Miller & Rollnick (1991), resistance is best seen as
a) a trait of difficult clients
b) a healthy assertion of independence
c) a function of a mismatch between the client’s stage of change and the therapist’s strategies
d) an indicator of poor prognosis which, if persistent, indicates that the client should be dropped
from counseling
e) none of the above
8.
Within the MI framework, ambivalence about change on the part of the client is
seen as
a) normal and useful
b) a major roadblock to change
c) pathological
d) irrelevant
9.
Which of the following therapist behaviors is NOT a roadblock to a client’s self-
expression
a) interpreting or analyzing
b) warning
c) reflecting
d) reassuring, sympathizing, or consoling
10.
Within the MI framework, individual client assessment is seen as
a) a stumbling block to change
b) an unnecessary distraction since the only effective treatment is already known
c) a vital part of determining a client’s needs
d) a dehumanizing and authoritarian exercise
11.
Which of the following is NOT an MI-consistent strategy for handling resistance?
a) simple reflection
b) amplified reflection
c) argument
d) reframe
e) emphasizing personal control
Please read this exchange between counselor and client and answer the questions
that follow:
1-C: I know I messed up. I ruined my family, my wife hates me, I got fired from my job, and now I
just feel so hopeless. I’m sad all the time, and it’s like I can’t do anything about it.
2-T: Where did you work?
3-C: Joe’s Auto. I just felt lost there all day, like I didn’t want to be there.
4-T: Did your boss know you were drinking?
5-C: Yeah, when he fired me, he told me he could smell the alcohol. God, he must really think
I’m a loser.
6-T: What you are is an addict.
7-C: I’m not addicted, OK. I just need a few beers after work to calm down.
8-T: No, you are an addict. You have to admit you are powerless over it before you can better.
Continued on next page
182 Appendix B

TIP 35Appendix B—Screening and Assessment Instruments
12.
Therapist statement #2 represents
a) a failure to express empathy
b) a failure to develop discrepancy
c) a failure to explore ambivalence
d) all of the above
e) none of the above
13.
Therapist statements #2 and #4 indicate which MI trap?
a) labeling trap
b) Q-A trap
c) expert trap
d) premature focus trap
e) blaming trap
14.
Therapist statement #6 reflects which MI trap?
a) labeling trap
b) Q-A trap
c) expert trap
d) premature focus trap
e) blaming trap
15.
Therapist statement #8 represents
a) a confrontation of denial
b) an accurate reflection
c) a failure to roll with resistance
d) both a and b
e) both a and c
For the following exchange between client and therapist, answer the questions
below:
1-T: What would you like to discuss today?
2-C: Look, the judge said I gotta come here, but I don’t think I need to be here, so don’t expect
me to cooperate with you.
3-T: You feel that things are fine.
4-C: I’m not saying that everything is perfect, but I’m not a dope fiend.
5-T: Do you feel that others see you that way?
6-C: Yeah! People at work are always on my case about it, saying I’m gonna die someday from it.
They just need to mind their business.
7-T: Sounds like they’re concerned.
8-C: Yeah, well, I guess.
16.
Therapist statement #3 is a demonstration of
a) the MI trap of labeling
b) the MI trap of premature focus
c) the MI principle of rolling with resistance
d) the MI principle of expressing empathy
e) both c and d
Continued on next page
Appendix B 183

TIP 35 Enhancing Motivation for Change in Substance Use Disorder Treatment
17.
This therapist is using which opening strategy?
a) listen reflectively
b) affirm
c) summarize
d) all of the above
18.
This therapist is using which opening strategy?
a) listen reflectively
b) affirm
c) summarize
d) all of the above
19.
The importance and confidence rulers are
a) a means of assessing client readiness
b) an intervention that is inconsistent with MI
c) used only with clients who are in the action stage of change
d) a way of rolling with resistance
20.
According to Miller and Rollnick (2002), a therapist should respond to client
change talk in all of the following ways, except by
a) elaborating on the change talk with an open question
b) reflecting the client’s change talk
c) asking the client to commit to a treatment plan
d) summarizing the client’s language
21.
The purpose of querying extreme consequences of maintaining behavior is
a) to elicit the cons of behavior change (counter change talk)
b) to warn the client about negative consequences of their behavior
c) to elicit the pros of behavior change (self-motivating statements)
d) to scare the client straight
22.
What would be the best therapist response to elicit change talk in the following situation?
T: “How confident are you on a scale of 0 to 10 that you can make this change?”
C: “About a 4.”
a) So, you’re about a 4.
b) Why are you a 4 and not a 0?
c) You’ve got some confidence, but not a lot.
d) Why are you not a 10?
184 Appendix B

TIP 35Appendix B—Screening and Assessment Instruments
Motivational Interviewing Knowledge Test Answer Key
1.
c) confronting denial
2.
f) both b and c
3.
b) arguing against change
4.
b) reflective listening and eliciting self-motivational statements
5.
c) directive but client-centered
6.
d) point out differences between the client’s own stated goals and current behavior
7.
c) a function of a mismatch between the client’s stage of change and the therapist’s strategies
8.
a) normal and useful
9.
c) reflecting
10.
c) a vital part of determining a client’s needs
11.
c) argument
12.
d) all of the above
13.
b) Q-A trap
14.
a) labeling trap
15.
e) both a and c
16.
e) both c and d
17.
a) listen reflectively
18.
c) the expert trap
19.
a) a means of assessing client readiness
20.
c) asking the client to commit to a treatment plan
21.
c) to elicit the pros of behavior change (self-motivating statements)
22.
b) Why are you a 4 and not a 0?
Source: Moyers, Martin, & Christopher, 2005. Reprinted from material in the public domain. Available online at no cost
(https://casaa.unm.edu/download/ELICIT/MI%20Knowledge%20Test.pdf).
Appendix B 185

TIP 35
Enhancing Motivation for Change in Substance Use Disorder Treatment
Appendix C—Resources
Motivational Interviewing and
Motivational Enhancement
Therapy
Motivational Interviewing Network of Trainers
(MINT) (www.motivationalinterviewing.org). This
website includes links to publications, motivational
interviewing (MI) assessment and coding resources,
and training resources and events.
Motivational Enhancement Therapy Manual
(https://casaa.unm.edu/download/met.pdf). This
manual describes the history of motivational
enhancement therapy (MET) and its use in Project
MATCH. It provides an overview of MET, its
relationship to the stages of change, the structure
of MET sessions, and a thorough review of the
assessment and personalized feedback process
used in MET.
Institute for Research, Education & Training in
Addictions Motivational Interviewing Toolkit
(https://ireta.org/resources/motivational-
interviewing-toolkit). This website provides
educational materials about MI and links to no-cost
MI resources.
Stages of Change
Health and Addictive Behaviors: Investigating
Transtheoretical Solutions Lab at the University
of Maryland, Baltimore County (https://habitslab.
umbc.edu). This website provides an overview of
the Transtheoretical Model of behavior change,
printable assessments and scoring information,
related publications, and learning tools.
Training and Supervision
Motivational Interviewing Assessment:
Supervisory Tools for Enhancing Proficiency
Manual (www.motivationalinterviewing.org/sites/
default/files/mia-step.pdf). This collection of tools
is for mentoring counselors in MI skills used in the
engagement and assessment stage of counseling
people with substance use disorders (SUDs). It
includes teaching tools, counselor self-assessment
skill summaries, MI rating guides and forms,
transcripts and ratings of sample MI interviews, and
trainer instructions.
Center on Alcoholism, Substance Abuse,
and Addictions (https://casaa.unm.edu). This
multidisciplinary research center at the University
of New Mexico provides links to alcohol and drug
assessment tools, MI coding tools and therapist
manuals, and audio files and uncoded transcripts of
counselor role plays that can be used for training.
Motivational Interviewing Resources (https://
motivationalinterviewing.org/motivational-
interviewing-resources). This MINT webpage
provides links to downloadable coding manuals
for assessing counselor fidelity to the MI spirit
and practice skills including the Manual for
the Motivational Interviewing Skill Code
(MISC) (https://casaa.unm.edu/download/
misc.pdf), the MISC 2.5 (https://casaa.unm.
edu/download/misc25.pdf), the Motivational
Interviewing Treatment Integrity Coding
Manual 4.2.1 (https://motivationalinterviewing.
org/sites/default/files/miti4_2.pdf), and the
Assessment of Motivational Interviewing
Groups—Observer Scale (AMIGOS–v 1.2) (https://
motivationalinterviewing.org/sites/default/files/
amigos_rating_form_v1.2.pdf)
186 Appendix C
TIP 35
Appendix C—Resources
Substance Abuse and Mental
Health Services Administration
Screening, Brief Intervention, and Referral to
Treatment (SBIRT) (www.samhsa.gov/sbirt). This
website has information on dissemination and
implementation of SBIRT and additional resources.
Substance Abuse and Mental Health Services
Administration-Health Resources and Services
Administration Center for Integrated Health
Solutions (www.integration.samhsa.gov). The
Center for Integrated Health Solutions promotes
development of integrated primary and behavioral
health services to better address the needs of
people with mental disorders and SUDs, whether
they are seen in specialty behavioral health or
primary care settings. This website provides
information and resources on screening tools
(www.integration.samhsa.gov/clinical-practice/
screening-tools), motivational interviewing
(www.integration.samhsa.gov/clinical-practice/
motivational-interviewing), and tobacco cessation
(www.integration.samhsa.gov/health-wellness/
wellness-strategies/tobacco-cessation-2).
Treatment Improvement Protocol (TIP) 63:
Medications for Opioid Use Disorder (https://
store.samhsa.gov/product/TIP-63-Medications-
for-Opioid-Use-Disorder-Full-Document-
Including-Executive-Summary-and-Parts-1-5-/
SMA18-5063FULLDOC). This TIP reviews the use of
the three Food and Drug Administration-approved
medications used to treat opioid use disorder—
methadone, naltrexone, and buprenorphine—and
other strategies and services to support recovery.
TIP 60: Using Technology-Based Therapeutic
Tools in Behavioral Health Services (https://store.
samhsa.gov/product/TIP-60-Using-Technology-
Based-Therapeutic-Tools-in-Behavioral-Health-
Services/SMA15-4924). This TIP provides
information on implementing technology-assisted
care. It discusses the importance of technology in
reducing access to treatment and highlights the
importance of using technology-based assessments
and interventions in behavioral health services.
TIP 59: Improving Cultural Competence (https://
store.samhsa.gov/product/TIP-59-Improving-
Cultural-Competence/SMA15-4849). This TIP
helps providers and administrators understand
the role of culture in the delivery of mental health
and substance use services. It describes cultural
competence and discusses racial, ethnic, and
cultural considerations.
TIP 57: Trauma-Informed Care in Behavioral
Health Services (https://store.samhsa.gov/product/
TIP-57-Trauma-Informed-Care-in-Behavioral-Health-
Services/SMA14-4816). This TIP helps behavioral
health professionals understand the impact of
trauma on clients. It discusses patient assessment
and treatment planning strategies. These strategies
support recovery and building a trauma-informed
care workforce.
TIP 52: Clinical Supervision and Professional
Development of the Substance Abuse Counselor
(https://store.samhsa.gov/product/TIP-52-Clinical-
Supervision-and-Professional-Development-of-
the-Substance-Abuse-Counselor/SMA14-4435.
html). This TIP presents guidelines for clinical
supervision in SUD treatment. It covers supervision
methods and models, cultural competence, ethical
and legal issues, performance monitoring, and an
implementation guide for program administrators.
TIP 42: Substance Abuse Treatment for Persons
With Co-Occurring Disorders (https://store.
samhsa.gov/product/TIP-42-Substance-Abuse-
Treatment-for-Persons-With-Co-Occurring-
Disorders/SMA13-3992). This TIP gives SUD
providers information on co-occurring mental and
substance use disorders. It discusses terminology,
assessment, and treatment strategies and models.
TIP 39: Substance Abuse Treatment and Family
Therapy (https://store.samhsa.gov/product/TIP-39-
Substance-Abuse-Treatment-and-Family-Therapy/
SMA15-4219). This TIP describes the integration
of family counseling approaches into SUD
treatment. It also discusses cultural competency,
considerations for specific populations,
policy and program issues, and guidelines for
assessingviolence.
Appendix C 187
This page intentionally left blank


