
Features of Qualitative Data Analysis
Qualitative Data Analysis as an Art
Qualitative Compared With Quantitative
Data Analysis
Techniques of Qualitative Data Analysis
Documentation
Conceptualization, Coding, and Categorizing
Examining Relationships and Displaying Data
Authenticating Conclusions
Reflexivity
Alternatives in Qualitative Data Analysis
Ethnography
Netnography
Ethnomethodology
Conversation Analysis
Narrative Analysis
Grounded Theory
Qualitative Comparative Analysis
Case-Oriented Understanding
Visual Sociology
Mixed Methods
Combining Qualitative Methods
Combining Qualitative
and Quantitative Methods
Case Study: Juvenile Court Records
Case Study: Mental Health System
Case Study: Housing Loss in Group Homes
Computer-Assisted Qualitative Data Analysis
Ethics in Qualitative Data Analysis
Conclusions
CHAPTER10
Qualitative Data Analysis
I was at lunch standing in line and he [another male student] came up to my face and started saying stuff
and then he pushed me. I said . . . I’m cool with you, I’m your friend and then he push me again and calling
me names. I told him to stop pushing me and then he push me hard and said something about my mom.
And then he hit me, and I hit him back. After he fell I started kicking him.
—Morrill et al. (2000:521)
320

Chapter 10 Qualitative Data Analysis
321
U
nfortunately, this statement was not made by a soap opera actor but by a real student writing an
in-class essay about conflicts in which he had participated. But then you already knew that such
conflicts are common in many high schools, so perhaps it will be reassuring to know that this
statement was elicited by a team of social scientists who were studying conflicts in high schools to
better understand their origins and to inform prevention policies.
The first difference between qualitative and quantitative data analysis is that the data to be analyzed are
text, rather than numbers, at least when the analysis first begins. Does it trouble you to learn that there are no
variables and hypotheses in this qualitative analysis by Morrill et al. (2000)? This, too, is another difference
between the typical qualitative and quantitative approaches to analysis, although there are some exceptions.
In this chapter, I present the features that most qualitative data analyses share, and I will illustrate these
features with research on youth conflict and on being homeless. You will quickly learn that there is no one
way to analyze textual data. To quote Michael Quinn Patton (2002), “Qualitative analysis transforms data
into findings. No formula exists for that transformation. Guidance, yes. But no recipe. Direction can and will
be offered, but the final destination remains unique for each inquirer, known only when—and if—arrived
at” (p. 432).
I will discuss some of the different types of qualitative data analysis before focusing on computer pro-
grams for qualitative data analysis; you will see that these increasingly popular programs are blurring the
distinctions between quantitative and qualitative approaches to textual analysis.
2 Features of Qualitative Data Analysis
The distinctive features of qualitative data collection methods that you studied in Chapter 9 are also reflected
in the methods used to analyze those data. The focus on text—on qualitative data rather than on numbers—is
the most important feature of qualitative analysis. The “text” that qualitative researchers analyze is most often
transcripts of interviews or notes from participant observation sessions, but text can also refer to pictures or
other images that the researcher examines.
What can the qualitative data analyst learn from a text? Here qualitative analysts may have two different
goals. Some view analysis of a text as a way to understand what participants “really” thought, felt, or did in
some situation or at some point in time. The text becomes a way to get “behind the numbers” that are recorded
in a quantitative analysis to see the richness of real social experience. Other qualitative researchers have
adopted a hermeneutic perspective on texts—that is, a perspective that views a text as an interpretation that
can never be judged true or false. The text is only one possible interpretation among many (Patton 2002:114).
The meaning of a text, then, is negotiated among a community of interpreters, and to the extent that some
agreement is reached about meaning at a particular time and place, that meaning can only be based on con-
sensual community validation.
From a hermeneutic perspective, a researcher is constructing a “reality” with his or her interpretations
of a text provided by the subjects of research; other researchers, with different backgrounds, could come to
markedly different conclusions.
You can see in this discussion about text that qualitative and quantitative data analyses also differ in the
priority given to the prior views of the researcher and to those of the subjects of the research. Qualitative data
analysts seek to describe their textual data in ways that capture the setting or people who produced this text

Investigating the Social World
322
on their own terms rather than in terms of predefined measures and hypotheses. What this means is that
qualitative data analysis tends to be inductive—the analyst identifies important categories in the data, as
well as patterns and relationships, through a process of discovery. There are often
no predefined measures or hypotheses. Anthropologists term this an emic focus,
which means representing the setting in terms of the participants and their view-
point, rather than an etic focus, in which the setting and its participants are repre-
sented in terms that the researcher brings to the study.
Good qualitative data analyses also are distinguished by their focus on the inter-
related aspects of the setting, group, or person under investigation—the case—
rather than breaking the whole into separate parts. The whole is always understood
to be greater than the sum of its parts, and so the social context of events, thoughts, and actions becomes
essential for interpretation. Within this framework, it doesn’t really make sense to focus on two variables out
of an interacting set of influences and test the relationship between just those two.
Qualitative data analysis is an iterative and reflexive process that begins as data are being collected rather
than after data collection has ceased (Stake 1995). Next to her field notes or interview transcripts, the qualita-
tive analyst jots down ideas about the meaning of the text and how it might relate
to other issues. This process of reading through the data and interpreting them
continues throughout the project. The analyst adjusts the data collection process
itself when it begins to appear that additional concepts need to be investigated or
new relationships explored. This process is termed progressive focusing (Parlett &
Hamilton 1976).
We emphasize placing an interpreter in the field to observe the workings of the case, one who records
objectively what is happening but simultaneously examines its meaning and redirects observation to
refine or substantiate those meanings. Initial research questions may be modified or even replaced in
mid-study by the case researcher. The aim is to thoroughly understand [the case]. If early questions
are not working, if new issues become apparent, the design is changed. (Stake 1995:9)
Elijah Anderson (2003) describes the progressive focusing process in his memoir about his study of
Jelly’s Bar.
Throughout the study, I also wrote conceptual memos to myself to help sort out my findings. Usually
no more than a page long, they represented theoretical insights that emerged from my engagement
with the data in my field notes. As I gained tenable hypotheses and propositions, I began to listen and
observe selectively, focusing on those events that I thought might bring me alive to my research inter-
ests and concerns. This method of dealing with the information I was receiving amounted to a kind of
a dialogue with the data, sifting out ideas, weighing new notions against the reality with which I was
faced there on the streets and back at my desk (pp. 235–236).
Carrying out this process successfully is more likely if the analyst reviews a few basic guidelines when he
or she starts the process of analyzing qualitative data (Miller & Crabtree 1999b:142–143):
• Know yourself, your biases, and preconceptions.
• Know your question.
• Seek creative abundance. Consult others and keep looking for alternative interpretations.
Emic focus Representing a setting
with the participants’ terms and
from their viewpoint.
Etic focus Representing a setting
with the researchers’ terms and
from their viewpoint.
Progressive focusing The
process by which a qualitative
analyst interacts with the data and
gradually refines her focus.

Chapter 10 Qualitative Data Analysis
323
• Be flexible.
• Exhaust the data. Try to account for all the data in the texts, then publicly acknowledge the unex-
plained and remember the next principle.
• Celebrate anomalies. They are the windows to insight.
• Get critical feedback. The solo analyst is a great danger to self and others.
• Be explicit. Share the details with yourself, your team members, and your audiences.
Qualitative Data Analysis as an Art
If you find yourself longing for the certainty of predefined measures and deductively derived hypotheses, you
are beginning to understand the difference between setting out to analyze data quantitatively and planning to
do so with a qualitative approach in mind. Or, maybe you are now appreciating better the contrast between the
positivist and interpretivist research philosophies that I summarized in Chapter 3. When it comes right down
to it, the process of qualitative data analysis is even described by some as involving as much “art” as science—
as a “dance,” in the words of William Miller and Benjamin Crabtree (1999b) (Exhibit 10.1):
Interpretation is a complex and dynamic craft, with as much creative artistry as technical exacti-
tude, and it requires an abundance of patient plodding, fortitude, and discipline. There are many
changing rhythms; multiple steps; moments of jubilation, revelation, and exasperation. . . . The
dance of interpretation is a dance for two, but those two are often multiple and frequently changing,
and there is always an audience, even if it is not always visible. Two dancers are the interpreters and
the texts. (pp. 138–139)
Dance of Qualitative Analysis
Exhibit 10.1
Time
Organizing Style
Template Editing
Immersion/
Crystalization
I LLLRR R
RL
II
LLR

Investigating the Social World
324
Miller and Crabtree (1999b) identify three different modes of reading the text within the dance of qualita-
tive data analysis:
1. When the researcher reads the text literally, she is focused on its literal content and form, so the
text “leads” the dance.
2. When the researcher reads the text reflexively, she focuses on how her own orientation shapes her
interpretations and focus. Now, the researcher leads the dance.
3. When the researcher reads the text interpretively, she tries to construct her own interpretation of
what the text means.
Sherry Turkle’s (2011) book, Alone Together: Why We Expect More From Technology and Less From Each
Other, provides many examples of this analytic dance, although of course in the published book we are no
longer able to see that dance in terms of her original notes. She often describes what she observed in class-
rooms. Here’s an example of such a literal focus, reflecting her experience in MIT’s Media Lab at the start of the
mobile computing revolution:
In the summer of 1996, I met with seven young researchers at the MIT Media Lab who carried com-
puters and radio transmitters in their backpacks and keyboards in their pockets. . . . they called
themselves “cyborgs” and were always wirelessly connected to the Internet, always online, free from
desks and cables. (Turkle 2011:151)
Such literal reports are interspersed with interpretive comments about the meaning of her observations:
The cyborgs were a new kind of nomad, wandering in and out of the physical real. . . . The multiplicity
of worlds before them set them apart; they could be with you, but they were always somewhere else as
well. (Turkle 2011:152)
And several times in each chapter, Turkle (2011) makes reflexive comments on her own reactions:
I don’t like the feeling of always being on call. But now, with a daughter studying abroad who expects
to reach me when she wants to reach me, I am grateful to be tethered to her through the Net. . . . even
these small things allow me to identify with the cyborgs’ claims of an enhanced experience. Tethered
to the Internet, the cyborgs felt like more than they could be without it. Like most people, I experience
a pint-sized version of such pleasures. (p. 153)
In this artful way, the qualitative data analyst reports on her notes from observing or interviewing, inter-
prets those notes, and considers how she reacts to the notes. These processes emerge from reading the notes
and continue while editing the notes and deciding how to organize them, in an ongoing cycle.
Qualitative Compared With Quantitative Data Analysis
With this process in mind, let’s review the many ways in which qualitative data analysis differs from quantitative
analysis (Denzin & Lincoln 2000:8–10; Patton 2002:13–14). Each difference reflects the qualitative data analysts’
orientation to in-depth, comprehensive understanding in which the analyst is an active participant as compared
to the quantitative data analysts’ role as a dispassionate investigator of specific relations among discrete variables:
• A focus on meanings rather than on quantifiable phenomena
• Collection of many data on a few cases rather than few data on many cases

Chapter 10 Qualitative Data Analysis
325
• Study in depth and detail, without predetermined categories or directions, rather than emphasis on
analyses and categories determined in advance
• Conception of the researcher as an “instrument,” rather than as the designer of objective instruments
to measure particular variables
• Sensitivity to context rather than seeking universal generalizations
• Attention to the impact of the researcher’s and others’ values on the course of the analysis rather than
presuming the possibility of value-free inquiry
• A goal of rich descriptions of the world rather than measurement of specific variables
You’ll also want to keep in mind features of qualitative data analysis that are shared with those of quantita-
tive data analysis. Both qualitative and quantitative data analysis can involve making distinctions about textual
data. You also know that textual data can be transposed to quantitative data through a process of categorization
and counting. Some qualitative analysts also share with quantitative researchers a positivist goal of describing
better the world as it “really” is, although others have adopted a postmodern goal of trying to understand how
different people see and make sense of the world, without believing that there is any “correct” description.
2 Techniques of Qualitative Data Analysis
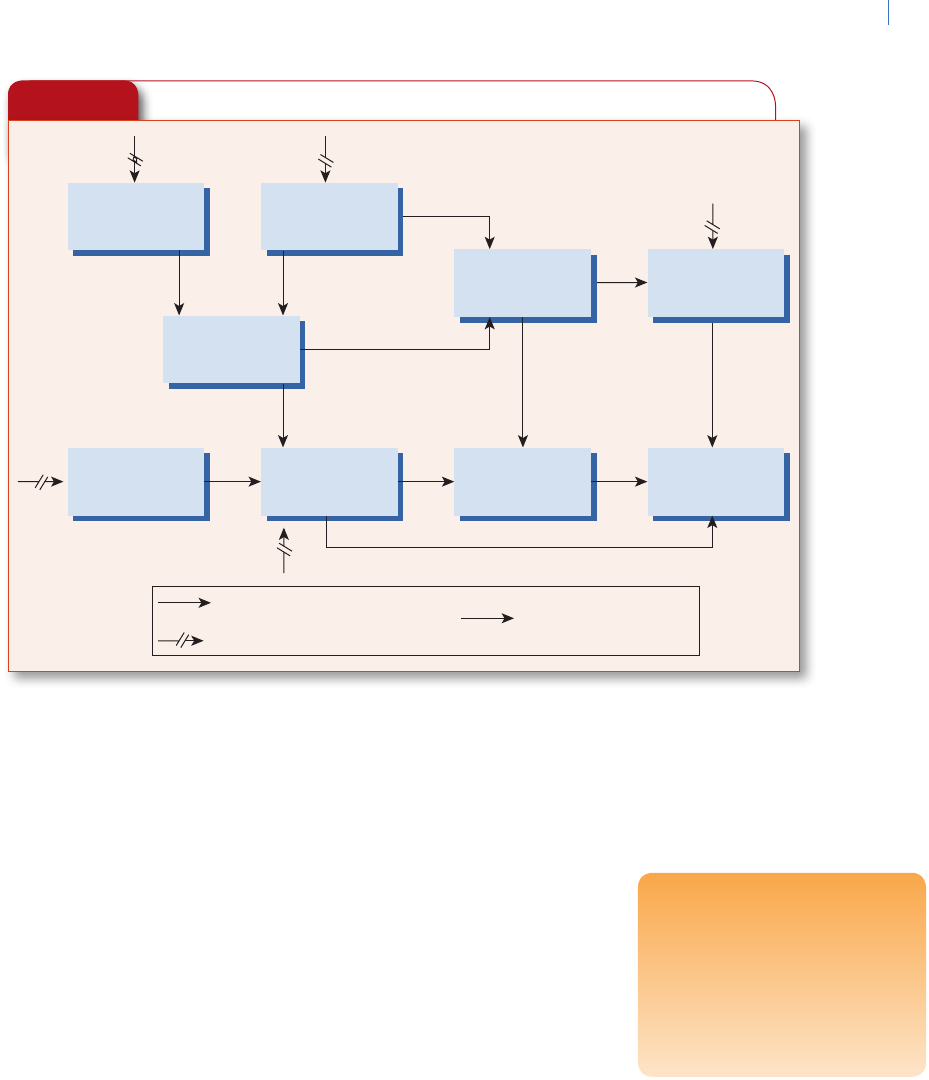
Exhibit 10.2 outlines the different techniques that are shared by most approaches to qualitative data analysis:
1. Documentation of the data and the process of data collection
2. Organization/categorization of the data into concepts
3. Connection of the data to show how one concept may influence another
4. Corroboration/legitimization, by evaluating alternative explanations, disconfirming evidence,
and searching for negative cases
5. Representing the account (reporting the findings)
The analysis of qualitative research notes begins in the field, at the time of observation, interviewing, or
both, as the researcher identifies problems and concepts that appear likely to help in understanding the situa-
tion. Simply reading the notes or transcripts is an important step in the analytic process. Researchers should
make frequent notes in the margins to identify important statements and to propose ways of coding the data:
“husband–wife conflict,” perhaps, or “tension-reduction strategy.”
An interim stage may consist of listing the concepts reflected in the notes and diagramming the relation-
ships among concepts (Maxwell 1996:78–81). In large projects, weekly team meetings are an important part of
this process. Susan Miller (1999) described this process in her study of neighborhood police officers (NPOs).
Her research team met both to go over their field notes and to resolve points of confusion, as well as to dialogue
with other skilled researchers who helped identify emerging concepts:
The fieldwork team met weekly to talk about situations that were unclear and to troubleshoot any
problems. We also made use of peer-debriefing techniques. Here, multiple colleagues, who were
familiar with qualitative data analysis but not involved in our research, participated in preliminary
analysis of our findings. (p. 233)

Investigating the Social World
326
This process continues throughout the project and should assist in refining concepts during the report-
writing phase, long after data collection has ceased. Let’s examine each of the stages of qualitative research in
more detail.
Documentation
The data for a qualitative study most often are notes jotted down in the field or during an interview—from
which the original comments, observations, and feelings are reconstructed—or text transcribed from
audiotapes. “The basic data are these observations and conversations, the actual words of people repro-
duced to the best of my ability from the field notes” (Diamond 1992:7). What to do with all this material?
Many field research projects have slowed to a halt because a novice researcher becomes overwhelmed by the
quantity of information that has been collected. A 1-hour interview can generate 20 to 25 pages of single-
spaced text (Kvale 1996:169). Analysis is less daunting, however, if the researcher maintains a disciplined
transcription schedule.
Usually, I wrote these notes immediately after spending time in the setting or the next day. Through
the exercise of writing up my field notes, with attention to “who” the speakers and actors were, I
became aware of the nature of certain social relationships and their positional arrangements within
the peer group. (Anderson 2003:235)
You can see the analysis already emerging from this simple process of taking notes.
The first formal analytical step is documentation. The various contacts, interviews, written documents,
and whatever it is that preserves a record of what happened all need to be saved and listed. Documentation
is critical to qualitative research for several reasons: It is essential for keeping track of what will be a rapidly
growing volume of notes, tapes, and documents; it provides a way of developing and outlining the analytic
process; and it encourages ongoing conceptualizing and strategizing about the text.
Miles and Huberman (1994:53) provide a good example of a contact summary form that was used to keep
track of observational sessions in a qualitative study of a new school curriculum (Exhibit 10.3).
Exhibit 10.2
Flow Model of Qualitative Data Analysis Components
Data collection period
DATA REDUCTION
DATA DISPLAYS
Anticipatory During
During
During
Post
Post
Post
CONCLUSION DRAWING/VERIFICATION
ANALYSIS

Chapter 10 Qualitative Data Analysis
327
Exhibit 10.3
Example of a Contact Summary Form
Contact type: ___________ Site: Tindale
Visit _____ X______ Contact date: 11/28-29/79
Phone ________________ Today’s date: 12/28/79
(with whom) Written by: BLT
1. What were the main issues or themes that struck you in this contact?
Interplay between highly prescriptive, “teacher-proof” curriculum that is top-down imposed and the actual
writing of the curriculum by the teachers themselves.
Split between the “watchdogs” (administrators) and the “house masters” (dept. chairs & teachers) vis à vis
job foci.
District curric, coord’r as decision maker re school’s acceptance of research relationship.
2. Summarize the information you got (or failed to get) on each of the target questions you had for this
contact.
Question Information
History of dev. of innov’n teachers Conceptualized by Curric., Coord’r, English Chairman &
Assoc. Chairman; written by teachers in summer; revised
by following summer with field testing data
School’s org’l structure Principal & admin’rs responsible for discipline; dept chairs
are educ’l leaders
Demographics emphasis Racial conflicts in late 60’s; 60% black stud. pop.; heavy on
discipline & on keeping out non-district students slipping in
from Chicago
Teachers’ response to innov’n Rigid, structured, etc. at first; now, they say they like it/
NEEDS EXPLORATION
Research access Very good; only restriction: teachers not required to
cooperate
3. Anything else that struck you as salient, interesting, illuminating or important in this contact?
Thoroughness of the innov’n’s development and training.
Its embeddedness in the district’s curriculum, as planned and executed by the district curriculum
coordinator.
The initial resistance to its high prescriptiveness (as reported by users) as contrasted with their current
acceptance and approval of it (again, as reported by users).
4. What new (or remaining) target questions do you have in considering the next contact with this site?
How do users really perceive the innov’n? If they do indeed embrace it, what accounts for the change
from early resistance?
Nature and amount of networking among users of innov’n.
Information on “stubborn” math teachers whose ideas weren’t heard initially—who are they? Situation
particulars? Resolution?
Follow-up on English teacher Reilly’s “fall from the chairmanship.”
Follow a team through a day of rotation, planning, etc.
CONCERN: The consequences of eating school cafeteria food two days per week for the next four or
five months . . .
Stop

Investigating the Social World
328
Conceptualization, Coding, and Categorizing
Identifying and refining important concepts is a key part of the iterative process of qualitative research.
Sometimes, conceptualizing begins with a simple observation that is interpreted directly, “pulled apart,” and
then put back together more meaningfully. Robert Stake (1995) provides an example:
When Adam ran a pushbroom into the feet of the children nearby, I jumped to conclusions about his
interactions with other children: aggressive, teasing, arresting. Of course, just a few minutes earlier I
had seen him block the children climbing the steps in a similar moment of smiling bombast. So I was
aggregating, and testing my unrealized hypotheses about what kind of kid he was, not postponing my
interpreting. . . . My disposition was to keep my eyes on him. (p. 74)
The focus in this conceptualization “on the fly” is to provide a detailed description of what was observed
and a sense of why that was important.
More often, analytic insights are tested against new observations, the initial statement of problems and
concepts is refined, the researcher then collects more data, interacts with the data again, and the process
continues. Anderson (2003) recounts how his conceptualization of social stratification at Jelly’s Bar developed
over a long period of time:
I could see the social pyramid, how certain guys would group themselves and say in effect, “I’m here and
you’re there.” . . . I made sense of these crowds [initially] as the “respectables,” the “nonrespectables,”
and the “near-respectables.” . . . Inside, such non-respectables might sit on the crates, but if a respect-
able came along and wanted to sit there, the lower-status person would have to move. (pp. 225–226)
But this initial conceptualization changed with experience, as Anderson realized that the participants
themselves used other terms to differentiate social status: winehead, hoodlum, and regular (Anderson 2003:230).
What did they mean by these terms? The regulars basically valued “decency.” They associated decency with con-
ventionality but also with “working for a living,” or having a “visible means of support” (Anderson 2003:231). In
this way, Anderson progressively refined his concept as he gained experience in the setting.
Howard S. Becker (1958) provides another excellent illustration of this iterative process of conceptualiza-
tion in his study of medical students:
When we first heard medical students apply the term “crock” to patients, we made an effort to learn
precisely what they meant by it. We found, through interviewing students about cases both they and the
observer had seen, that the term referred in a derogatory way to patients with many subjective symp-
toms but no discernible physical pathology. Subsequent observations indicated that this usage was a
regular feature of student behavior and thus that we should attempt to incorporate this fact into our
model of student-patient behavior. The derogatory character of the term suggested in particular that we
investigate the reasons students disliked these patients. We found that this dislike was related to what
we discovered to be the students’ perspective on medical school: the view that they were in school to get
experience in recognizing and treating those common diseases most likely to be encountered in general
practice. “Crocks,” presumably having no disease, could furnish no such experience. We were thus led
to specify connections between the student-patient relationship and the student’s view of the purpose
of this professional education. Questions concerning the genesis of this perspective led to discoveries
about the organization of the student body and communication among students, phenomena which
we had been assigning to another [segment of the larger theoretical model being developed]. Since
“crocks” were also disliked because they gave the student no opportunity to assume medical responsi-
bility, we were able to connect this aspect of the student-patient relationship with still another tentative
model of the value system and hierarchical organization of the school, in which medical responsibility
plays an important role. (p. 658)

Chapter 10 Qualitative Data Analysis
329
Exhibit 10.4
Example of Checklist Matrix
Presence of Supporting Conditions
Condition For Users For Administrators
Commitment Strong—“wanted to make it work.” Weak at building level.
Prime movers in central office
committed; others not.
Understanding “Basic” (“felt I could do it, but I just
wasn’t sure how.”) for teacher.
Absent for aide (“didn’t understand
how we were going to get all this.”)
Absent at building level and among
staff.
Basic for 2 prime movers (“got
all the help we needed from
developer.”)
Absent for other central office staff.
Materials Inadequate: ordered late, puzzling
(“different from anything I ever
used”), discarded.
NA
Front-end training “Sketchy” for teacher (“it all happened
so quickly”); no demo class.
None for aide (“totally unprepared. I
had to learn along with the children.”)
Prime movers in central office had
training at developer site; none for
others.
Skills Weak-adequate for teacher.
“None” for aide.
One prime mover (Robeson) skilled
in substance; others unskilled.
Ongoing inservice None, except for monthly committee
meeting; no substitute funds.
None
Planning,
coordination time
None: both users on other tasks
during day; lab tightly scheduled, no
free time.
None
Provisions for
debugging
None systematized; spontaneous
work done by users during summer.
None
School admin.
support
Adequate NA
Central admin.
support
Very strong on part of prime movers. Building admin. only acting on basis
of central office commitment.
Relevant prior
experience
Strong and useful in both cases:
had done individualized instruction,
worked with low achievers. But aide
had no diagnostic experience.
Present and useful in central office,
esp. Robeson (specialist).
This excerpt shows how the researcher first was alerted to a concept by observations in the field, then
refined his understanding of this concept by investigating its meaning. By observing the concept’s frequency
of use, he came to realize its importance. Then he incorporated the concept into an explanatory model of
student-patient relationships.
A well-designed chart, or matrix, can facilitate the coding and categorization process. Exhibit 10.4 shows
an example of a coding form designed by Miles and Huberman (1994:93–95) to represent the extent to which

Investigating the Social World
330
teachers and teachers’ aides (“users”) and administrators at a school gave evidence
of various supporting conditions that indicate preparedness for a new reading pro-
gram. The matrix condenses data into simple categories, reflects further analysis of
the data to identify degree of support, and provides a multidimensional summary
that will facilitate subsequent, more intensive analysis. Direct quotes still impart
some of the flavor of the original text.
Examining Relationships and Displaying Data
Examining relationships is the centerpiece of the analytic process, because it allows the researcher to move
from simple description of the people and settings to explanations of why things happened as they did with
those people in that setting. The process of examining relationships can be captured in a matrix that shows
how different concepts are connected, or perhaps what causes are linked with what effects.
Exhibit 10.5 displays a matrix used to capture the
relationship between the extent to which stakeholders in
a new program had something important at stake in the
program and the researcher’s estimate of their favorability
toward the program. Each cell of the matrix was to be filled
in with a summary of an illustrative case study. In other
matrix analyses, quotes might be included in the cells to
represent the opinions of these different stakeholders, or
the number of cases of each type might appear in the cells.
The possibilities are almost endless. Keeping this approach
in mind will generate many fruitful ideas for structuring a
qualitative data analysis.
The simple relationships that are identified with a
matrix like that shown in Exhibit 10.5 can be examined
and then extended to create a more complex causal model.
Such a model represents the multiple relationships among the constructs identified in a qualitative analysis
as important for explaining some outcome. A great deal of analysis must precede the construction of such a
model, with careful attention to identification of important variables and the evidence that suggests connec-
tions between them. Exhibit 10.6 provides an example of these connections from a study of the implementa-
tion of a school program.
Authenticating Conclusions
No set standards exist for evaluating the validity, or authenticity, of conclusions in a qualitative study, but the
need to carefully consider the evidence and methods on which conclusions are based is just as great as with
other types of research. Individual items of information can be assessed in terms of at least three criteria
(Becker 1958):
1.
How credible was the informant? Were statements made by someone with whom the researcher had a
relationship of trust or by someone the researcher had just met? Did the informant have reason to lie? If the
statements do not seem to be trustworthy as indicators of actual events, can they at least be used to help under-
stand the informant’s perspective?
2.
Were statements made in response to the researcher’s questions, or were they spontaneous? Spontaneous
statements are more likely to indicate what would have been said had the researcher not been present.
Exhibit 10.5
Coding Form for Relationships:
Stakeholders’ Stakes
Favorable
Neutral or
Unknown
Antagonistic
High
Moderate
Low
Note: Construct illustrative case studies for each cell based on fieldwork.
Matrix A form on which can be
recorded systematically particular
features of multiple cases or
instances that a qualitative data
analyst needs to examine.
Chapter 10 Qualitative Data Analysis
331
Tacit knowledge In field research,
a credible sense of understanding
of social processes that reflects
the researcher’s awareness of
participants’ actions as well as
their words, and of what they fail
to state, feel deeply, and take for
granted.
3.
How does the presence or absence of the researcher or the researcher’s informant influence the actions and
statements of other group members? Reactivity to being observed can never be ruled out as a possible explana-
tion for some directly observed social phenomenon. However, if the researcher carefully compares what the
informant says goes on when the researcher is not present, what the researcher observes directly, and what
other group members say about their normal practices, the extent of reactivity can be assessed to some extent
(pp. 654–656).
A qualitative researcher’s conclusions should also be assessed by his or her abil-
ity to provide a credible explanation for some aspect of social life. That explanation
should capture group members’ tacit knowledge of the social processes that were
observed, not just their verbal statements about these processes. Tacit knowledge—
“the largely unarticulated, contextual understanding that is often manifested in
nods, silences, humor, and naughty nuances”—is reflected in participants’ actions
as well as their words and in what they fail to state but nonetheless feel deeply and
even take for granted (Altheide & Johnson 1994:492–493). These features are evi-
dent in Whyte’s (1955) analysis of Cornerville social patterns:
The corner-gang structure arises out of the habitual association of the members over a long period of
time. The nuclei of most gangs can be traced back to early boyhood. . . . Home plays a very small role in
the group activities of the corner boy. . . . The life of the corner boy proceeds along regular and narrowly
circumscribed channels. . . . Out of [social interaction within the group] arises a system of mutual obli-
gations which is fundamental to group cohesion. . . . The code of the corner boy requires him to help
his friends when he can and to refrain from doing anything to harm them. When life in the group runs
smoothly, the obligations binding members to one another are not explicitly recognized. (pp. 255–257)
Exhibit 10.6
Example of a Causal Network Model
( − )
7. Job
mobility
8. Institution-
alization
( − )
Causal influence (inverse)Causal influence (direct)
Influence of variables not shown ∗ Site-specific variable
1. External funds
(temporary)
4. Environmental
turbulence
5. Job
insecurity
3. Program
vulnerability
2. Building
endorsement
Program
isolation*
6. Influence of
innovation
advocates

Investigating the Social World
332
Comparing conclusions from a qualitative research project to those other researchers obtained while con-
ducting similar projects can also increase confidence in their authenticity. Miller’s (1999) study of NPOs found
striking parallels in the ways they defined their masculinity to processes reported in research about males in
nursing and other traditionally female jobs:
In part, male NPOs construct an exaggerated masculinity so that they are not seen as feminine as
they carry out the social-work functions of policing. Related to this is the almost defiant expression
of heterosexuality, so that the men’s sexual orientation can never truly be doubted even if their gender
roles are contested. Male patrol officers’ language—such as their use of terms like “pansy police” to
connote neighborhood police officers—served to affirm their own heterosexuality. . . . In addition,
the male officers, but not the women, deliberately wove their heterosexual status into conversations,
explicitly mentioning their female domestic partner or spouse and their children. This finding is
consistent with research conducted in the occupational field. The studies reveal that men in female-
dominated occupations, such as teachers, librarians, and pediatricians, over-reference their hetero-
sexual status to ensure that others will not think they are gay. (p. 222)
Reflexivity
Confidence in the conclusions from a field research study is also strengthened by an honest and informative
account about how the researcher interacted with subjects in the field, what problems he or she encountered,
and how these problems were or were not resolved. Such a “natural history” of the development of the evi-
dence enables others to evaluate the findings and reflects the interpretivist philosophy that guides many
qualitative researchers (see Chapter 3). Such an account is important first and foremost because of the evolv-
ing and variable nature of field research: To an important extent, the researcher “makes up” the method in
the context of a particular investigation rather than applying standard procedures that are specified before
the investigation begins.
Barrie Thorne (1993) provides a good example of this final element of the analysis:
Many of my observations concern the workings of gender categories in social life. For example, I trace
the evocation of gender in the organization of everyday interactions, and the shift from boys and
girls as loose aggregations to “the boys” and “the girls” as self-aware, gender-based groups. In writ-
ing about these processes, I discovered that different angles of vision lurk within seemingly simple
choices of language. How, for example, should one describe a group of children? A phrase like “six
girls and three boys were chasing by the tires” already assumes the relevance of gender. An alterna-
tive description of the same event—“nine fourth-graders were chasing by the tires”—emphasizes age
and downplays gender. Although I found no tidy solutions, I have tried to be thoughtful about such
choices. . . . After several months of observing at Oceanside, I realized that my field notes were pep-
pered with the words “child” and “children,” but that the children themselves rarely used the term.
“What do they call themselves?” I badgered in an entry in my field notes. The answer it turned out, is
that children use the same practices as adults. They refer to one another by using given names (“Sally,”
“Jack”) or language specific to a given context (“that guy on first base”). They rarely have occasion
to use age-generic terms. But when pressed to locate themselves in an age-based way, my informants
used “kids” rather than “children.” (pp. 8–9)
Qualitative data analysts, more often than quantitative researchers, display real sensitivity to how a social
situation or process is interpreted from a particular background and set of values and not simply based on the
situation itself (Altheide & Johnson 1994). Researchers are only human, after all, and must rely on their own

Chapter 10 Qualitative Data Analysis
333
senses and process all information through their own minds. By reporting how and why they think they did
what they did, they can help others determine whether, or how, the researchers’ perspectives influenced their
conclusions. “There should be clear ‘tracks’ indicating the attempt [to show the hand of the ethnographer] has
been made” (Altheide & Johnson 1994:493).
Anderson’s (2003) memoir about the Jelly’s Bar research illustrates the type of “tracks” that an ethnogra-
pher makes as well as how the researcher can describe those tracks. Anderson acknowledges that his tracks
began as a child:
While growing up in the segregated black community of South Bend, from an early age, I was curious
about the goings-on in the neighborhood, particularly the streets and more particularly the corner
taverns where my uncles and my dad would go to hang out and drink. . . . Hence, my selection of a
field setting was a matter of my background, intuition, reason, and a little bit of luck. (pp. 217–218)
After starting to observe at Jelly’s, Anderson’s (2003) tracks led to Herman:
After spending a couple of weeks at Jelly’s, I met Herman. I felt that our meeting marked an important
step. We would come to know each other well . . . something of an informal leader at Jelly’s. . . . We
were becoming friends. . . . He seemed to genuinely like me, and he was one person I could feel com-
fortable with. (pp. 218–219)
So we learn that Anderson’s observations were to be shaped, in part, by Herman’s perspective, but we also
find out that Anderson maintained some engagement with fellow students. This contact outside the bar helped
shape his analysis: “By relating my experiences to my fellow students, I began to develop a coherent perspec-
tive, or a ‘story’ of the place that complemented the accounts I had detailed in my accumulating field notes”
(Anderson 2003:220).
In this way, the outcome of Anderson’s analysis of qualitative data resulted, in part, from the way in which
he “played his role” as a researcher and participant, not just from the setting itself.
2 Alternatives in Qualitative Data Analysis
The qualitative data analyst can choose from many interesting alternative approaches. Of course, the research
question under investigation should shape the selection of an analytic approach, but the researcher’s prefer-
ences and experiences also will inevitably have an important influence on the method chosen. The alterna-
tive approaches I present here (ethnography, and its new online cousin, netnography); ethnomethodology;
qualitative comparative analysis; narrative analysis; conversation analysis; case-oriented understanding; and
grounded theory) give you a good sense of the different possibilities (Patton 2002).
Ethnography
Ethnography is the study of a culture or cultures that a group of people share
(Van Maanen 1995:4). As a method, it is usually meant to refer to the process of
participant observation by a single investigator who immerses himself or herself in
the group for a long period of time (often one or more years), gradually establishing
Ethnography The study of a
culture or cultures that some
group of people shares, using
participant observation over an
extended period of time.

Investigating the Social World
334
trust and experiencing the social world as do the participants (Madden 2010:16). Ethnographic research can
also be called naturalistic, because it seeks to describe and understand the natural social world as it really is,
in all its richness and detail. This goal is best achieved when an ethnographer is fluent in the local language
and spends enough time in the setting to know how people live, what they say about themselves and what they
actually do, and what they value (Armstrong 2008:55).
As you learned in Chapter 9, anthropological field research has traditionally been ethnographic, and
much sociological fieldwork shares these same characteristics. But there are no particular methodological
techniques associated with ethnography, other than just “being there.” The analytic process relies on the thor-
oughness and insight of the researcher to “tell us like it is” in the setting, as he or she experienced it.
Code of the Street, Anderson’s (1999) award-winning study of Philadelphia’s inner city, captures the flavor
of this approach:
My primary aim in this work is to render ethnographically the social and cultural dynamics of the
interpersonal violence that is currently undermining the quality of life of too many urban neighbor-
hoods. . . . How do the people of the setting perceive their situation? What assumptions do they bring
to their decision making? (pp. 10–11)
The methods of investigation are described in the book’s preface: participant observation, including
direct observation and in-depth interviews, impressionistic materials drawn from various social settings
around the city, and interviews with a wide variety of people. Like most traditional ethnographers, Anderson
(1999) describes his concern with being “as objective as possible” and using his training as other ethnogra-
phers do, “to look for and to recognize underlying assumptions, their own and those of their subjects, and to
try to override the former and uncover the latter” (p. 11).
From analysis of the data obtained in these ways, a rich description of life in the inner city emerges.
Although we often do not “hear” the residents speak, we feel the community’s pain in Anderson’s (1999)
description of “the aftermath of death”:
When a young life is cut down, almost everyone goes into mourning. The first thing that happens is
that a crowd gathers about the site of the shooting or the incident. The police then arrive, drawing
more of a crowd. Since such a death often occurs close to the victim’s house, his mother or his close
relatives and friends may be on the scene of the killing. When they arrive, the women and girls often
wail and moan, crying out their grief for all to hear, while the young men simply look on, in studied
silence. . . . Soon the ambulance arrives. (p. 138)
Anderson (1999) uses this description as a foundation on which he develops the key concepts in his analy-
sis, such as “code of the street”:
The “code of the street” is not the goal or product of any individual’s action but is the fabric of
everyday life, a vivid and pressing milieu within which all local residents must shape their personal
routines, income strategies, and orientations to schooling, as well as their mating, parenting, and
neighbor relations. (p. 326)
Anderson’s report on his Jelly’s Bar study illustrates how his ethnographic analysis deepened as he
became more socially integrated into the Jelly’s Bar group. He thus became more successful at “blend-
ing the local knowledge one has learned with what we already know sociologically about such settings”
(Anderson 2003:236):

Chapter 10 Qualitative Data Analysis
335
Netnography The use of
ethnographic methods to study
online communities. Also termed
cyberethnography and virtual
ethnography.
I engaged the denizens of the corner and wrote detailed field notes about my experiences, and from
time to time I looked for patterns and relationships in my notes. In this way, an understanding of the
setting came to me in time, especially as I participated more fully in the life of the corner and wrote my
field notes about my experiences; as my notes accumulated and as I reviewed them occasionally and
supplemented them with conceptual memos to myself, their meanings became more clear, while even
more questions emerged. (Anderson 2003:224)
A good ethnography like Anderson’s is only possible when the ethnographer learns the subtleties of expres-
sion used in a group and the multiple meanings that can be given to statements or acts (Armstrong 2008:60–62).
Good ethnographies also include some reflection by the researcher on the influence his or her own background
has had on research plans, as well as on the impact of the research in the setting (Madden 2010:22–23).
Netnography
Communities can refer not only to people in a common physical location, but also to relationships that develop
online. Online communities may be formed by persons with similar interests or backgrounds, perhaps to create
new social relationships that location or schedules did not permit, or to supplement relationships that emerge in
the course of work or school or other ongoing social activities. Like communities of people who interact face-to-
face, online communities can develop a culture and become sources of identification and attachment (Kozinets
2010:14–15). And like physical communities, researchers can study online communities through immersion
in the group for an extended period. Netnography, also termed cyberethnography and virtual ethnography
(James & Busher 2009:34–35), is the use of ethnographic methods to study online communities.
In some respects, netnography is similar to traditional ethnography. The researcher prepares to enter the
field by becoming familiar with online communities and their language and customs, formulating an explor-
atory research question about social processes or orientations in that setting, selecting an appropriate com-
munity to study. Unlike in-person ethnographies, netnographies can focus on communities whose members
are physically distant and dispersed. The selected community should be relevant
to the research question, involve frequent communication among actively engaged
members, and have a number of participants who, as a result, generate a rich body of
textual data (Kozinets 2010:89).
The netnographer’s self-introduction should be clear and friendly. Robert
Kozinets (2010:93) provides the following example written about the online discussion
space, alt.coffee:
I’ve been lurking here for a while, studying online coffee culture on alt.coffee, learning a lot, and enjoy-
ing it very much . . . I just wanted to pop out of lurker status to let you know I am here . . . I will be
wanting to quote some of the great posts that have appeared here, and I will contact the individuals
by personal e-mail who posted them to ask their permission to quote them. I also will be making the
document on coffee culture available to any interested members of the newsgroup for their perusal
and comments—to make sure I get things right.
A netnographer must keep both observational and reflective field notes, but unlike a traditional ethnogra-
pher can return to review the original data—the posted test—long after it was produced. The data can then be
coded, annotated with the researcher’s interpretations, checked against new data to evaluate the persistence of
social patterns, and used to develop a theory that is grounded in the data.
Investigating the Social World
336
Ethnomethodology A qualitative
research method focused on the
way that participants in a social
setting create and sustain a sense
of reality.
Ethnomethodology
Ethnomethodology focuses on the way that participants construct the social world in
which they live—how they “create reality”—rather than on describing the social world
itself. In fact, ethnomethodologists do not necessarily believe that we can find an objec-
tive reality; it is the way that participants come to create and sustain a sense of reality
that is of interest. In the words of Jaber F. Gubrium and James A. Holstein (1997), in
ethnomethodology, as compared with the naturalistic orientation of ethnography,
the focus shifts from the scenic features of everyday life onto the ways through which the world comes
to be experienced as real, concrete, factual, and “out there.” An interest in members’ methods of con-
stituting their world supersedes the naturalistic project of describing members’ worlds as they know
them. (p. 41)
Unlike the ethnographic analyst, who seeks to describe the social world as the participants see it, the
ethnomethodological analyst seeks to maintain some distance from that world. The ethnomethologist
views a code of conduct like that described by Anderson (2003) not as a description of a real normative
force that constrains social action, but as the way that people in the setting create a sense of order and
social structure (Gubrium & Holstein 1997:44–45). The ethnomethodologist focuses on how reality is con-
structed, not on what it is.
Sociologist Harold Garfinkel (1967) developed ethnomethodology in the 1960s and first applied it to the
study of gender. Focusing on a teenage male-to-female transsexual who he termed “Agnes,” he described her
“social achievement of gender” as
the tasks of securing and guaranteeing for herself the ascribed rights and obligations of an adult
female by the acquisition and use of skills and capacities, the efficacious display of female appear-
ances and performances, and the mobilizing of appropriate feelings and purposes. (p. 134)
News
In the
Research in the News
READERS’ ONLINE FEEDBACK CAN BE VICIOUS
After a woman published an article in an online magazine about postpartum post-traumatic
stress disorder following a traumatic delivery experience with her baby boy, the nasty com-
ments started to pour in to the area reserved for reader responses. She was told not to have
any more babies and that she would be a bad mother. In a similar incident, an uninsured
woman who had written of her inability to function after a car accident was told to “Get
a minnie mouse bandage and go to sleep.” Why do some people get so vicious on the
Internet? One social scientist suggested that it is because of the lack of face-to-face interac-
tion, which provides constant feedback about others’ feelings through body language and
gestures.
Source: Brodesser-Akner, Taffy. 2010. “E-Playgrounds Can Get Vicious (Online Feedback From
Readers).” The New York Times, April 22:E8.

Chapter 10 Qualitative Data Analysis
337
The ethnomethodological focus on how the meaning of gender and other categories are socially con-
structed leads to a concern with verbal interaction. In recent years, this concern has led ethnomethodologists
and others to develop a more formal approach, called conversation analysis.
Conversation Analysis
Conversation analysis is a specific qualitative method for analyzing the sequential organization and details of
conversation. Like ethnomethodology, from which it developed, conversation analysis focuses on how reality
is constructed, rather than on what it is. From this perspective, detailed analysis of conversational interaction
is important because conversation is “sociological bedrock”: . . .“a form of social organization through which
the work of . . . institutions such as the economy, the polity, the family, socialization, etc.” is accomplished
(Schegloff 1996:4).
. . . it is through conversation that we conduct the ordinary affairs of our lives. Our relationships with
one another, and our sense of who we are to one another is generated, manifest, maintained, and
managed in and through our conversations, whether face-to-face, on the telephone, or even by other
electronic means. (Drew 2005:74)
Three premises guide conversation analysis (Gubrium & Holstein 2000:492):
1. Interaction is sequentially organized, and talk can be analyzed in terms of the process of social
interaction rather than in terms of motives or social status.
2. Talk, as a process of social interaction, is contextually oriented—it is both shaped by interaction
and creates the social context of that interaction.
3. These processes are involved in all social interaction, so no interactive details are irrelevant to
understanding it.
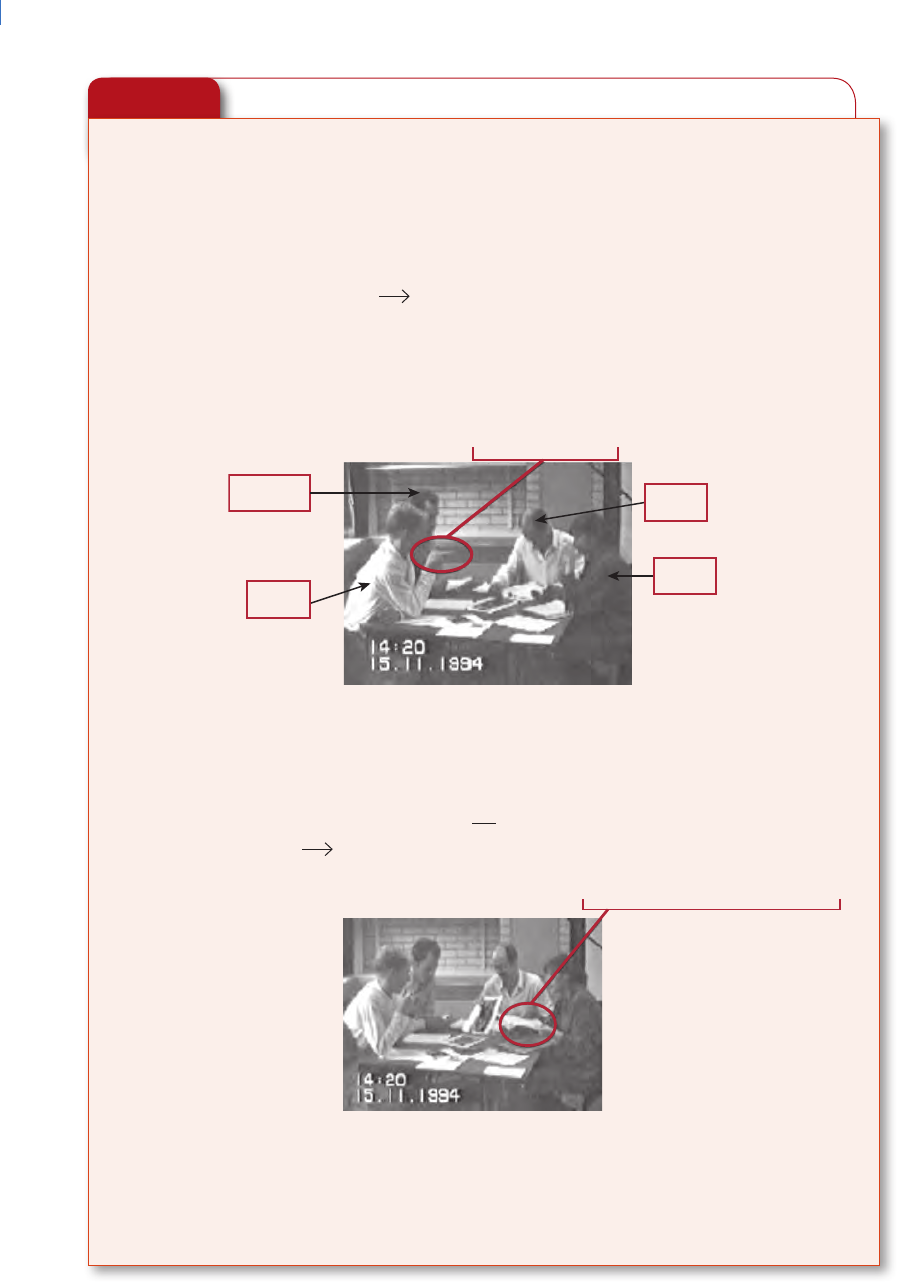
Consider these premises as you read the following excerpt from Elizabeth Stokoe’s (2006:479–480) analysis
of the relevance of gender categories to “talk-in-interaction.” The dialogue is between four first-year British psy-
chology students who must write up a description of some photographs of people (Exhibit 10.7). Stokoe incorpo-
rates stills from the video recording of the interaction into her analysis of both the talk and embodied conduct in
interaction. In typical conversation analysis style, the text is broken up into brief segments that capture shifts in
meaning, changes in the speaker, pauses, nonspeech utterances and nonverbal actions, and emphases.
Can you see how the social interaction reinforces the link of “woman” and “secretary”? Here, in part, is
how Elizabeth Stokoe (2006) analyzes this conversation:
In order to meet the task demands, one member of the group must write down their ideas. Barney’s
question at the start of the sequence, “is somebody scribing” is taken up after a reformulation: “who’s
writin’ it.” Note that, through a variety of strategies, members of the group manage their responses
such that they do not have to take on the role of scribe. At line 05, Neil’s “Oh yhe:ah.” treats Barney’s
turn as a proposal to be agreed with, rather than a request for action, and his subsequent nomina-
tion of Kay directs the role away from himself. . . . At line 08, Neil nominates Kay, his pointing gesture
working in aggregate with the talk to accomplish the action (“She wants to do it.”), whilst also attrib-
uting agency to Kay for taking up the role. A gloss [interpretation] might be “Secretaries in general are
female, you’re female, so you in particular are our secretary.” (p. 481)
Investigating the Social World
338
Exhibit 10.7
Conversation Analysis, Including Pictures
1. UT-23
01 N: D’ you reckon she’s an instructor then.
02 N: (0.2)
03 N: Of some sort,
04 B: Is somebody scribing. Who’s writin’ it. =
05 N: =Oh yhe:ah.
06 (0.8)
07 M: Well you can’t [ read my ] =
08 N: [((pointing to K)) She wants to do it.]
Barney
Neil
Kay
Mick
09 M: =writin’ once I’ve [wri:tten it.]
10 K: [.hehhhh]
11 N: We:ll secretary an’ female.
12 (0.3)
13 K: .Hh heh heh heh ((nodding, picks up pen and paper))
14 (0.4)
15 M: It’s uh::,
16 K: Yeah: I’m wearing glasses I must be the secretary.=

Chapter 10 Qualitative Data Analysis
339
Bethan Benwell and Elizabeth Stokoe (2006:61–62) used a conversation between three friends to illustrate
key concepts in conversation analysis. The text is prepared for analysis by numbering the lines, identifying the
speakers, and inserting ↑ symbols to indicate inflection and decimal numbers to indicate elapsed time.
104 Marie: ↑ Has ↑ anyone-(0.2) has anyone got any really non:
105 sweaty stuff.
106 Dawn: Dave has, but you’ll smell like a ma:n,
107 (0.9)
108 Kate: Eh [ ↑ huh heh]
109 Marie: [Right has] anyone got any ↑ fe:minine non sweaty stuff.
The gap at line 107, despite being less than a second long, is nevertheless quite a long time in conversation,
and indicates an interactional glitch or trouble. As Kate starts to laugh, Marie reformulates her request, from
“ ↑ has ↑ anyone got any really non: sweaty stuff,” to “right has anyone got any, ↑ fe:minine non sweaty stuff.”
The word really is replaced by feminine, and is produced with an audible increase in pitch and emphasis. This
replacement, together with the addition of right, displays her understanding of the problem with her previous
question. For these speakers, smelling like a man (when one is a woman) is treated as a trouble source, a laugh-
able thing and something that needs attending to and fixing. In this way, conversation analysis can uncover
meanings in interactions about which the participants are not fully aware (Antaki 2008:438).
Narrative Analysis
Narrative methods use interviews and sometimes documents or observations to “fol-
low participants down their trails” (Riessman 2008:24). Unlike conversation analysis,
which focuses attention on moment-by-moment interchange, narrative analysis seeks
to put together the “big picture” about experiences or events as the participants under-
stand them. Narrative analysis focuses on “the story itself” and seeks to preserve the
integrity of personal biographies or a series of events that cannot adequately be under-
stood in terms of their discrete elements (Riessman 2002:218). Narrative “displays the
goals and intentions of human actors; it makes individuals, cultures, societies, and
historical epochs comprehensible as wholes” (Richardson 1995:200). The coding for a narrative analysis is typi-
cally of the narratives as a whole, rather than of the different elements within them. The coding strategy revolves
around reading the stories and classifying them into general patterns.
For example, Calvin Morrill and his colleagues (2000:534) read through 254 conflict narratives written by
the ninth graders they studied and found four different types of stories:
1. Action tales, in which the author represents himself or herself and others as acting within the para-
meters of taken-for-granted assumptions about what is expected for particular roles among peers.
2. Expressive tales, in which the author focuses on strong, negative emotional responses to someone
who has wronged him or her.
3.
Moral tales, in which the author recounts explicit norms that shaped his or her behavior in the
story and influenced the behavior of others.
4.
Rational tales, in which the author represents himself or herself as a rational decision maker navi-
gating through the events of the story.
Narrative analysis A form of
qualitative analysis in which
the analyst focuses on how
respondents impose order on the
flow of experience in their lives
and thus make sense of events
and actions in which they have
participated.

Investigating the Social World
340
In addition to these dominant distinctions, Morrill et al. (2000:534–535) also distinguished the sto-
ries in terms of four stylistic dimensions: (1) plot structure (e.g., whether the story unfolds sequentially),
(2) dramatic tension (how the central conflict is represented), (3) dramatic resolution (how the central con-
flict is resolved), and (4) predominant outcomes (how the story ends). Coding reliability was checked through
a discussion between the two primary coders, who found that their classifications agreed for a large percent-
age of the stories.
The excerpt that begins this chapter exemplifies what Morrill et al. (2000) termed an action tale. Such tales
unfold in matter-of-fact tones kindled by dramatic tensions that begin with a disruption of the quotid-
ian order of everyday routines. A shove, a bump, a look . . . triggers a response . . . Authors of action
tales typically organize their plots as linear streams of events as they move briskly through the story’s
scenes . . . This story’s dramatic tension finally resolves through physical fighting, but . . . only after
an attempted conciliation. (p. 536)
You can contrast this action tale with the following narrative, which Morrill et al. (2000) classify as a moral
tale, in which the students “explicitly tell about their moral reasoning, often referring to how normative com-
mitments shape their decisionmaking” (p. 542):
I . . . got into a fight because I wasn’t allowed into the basketball game. I was being harassed by the
captains that wouldn’t pick me and also many of the players. The same type of things had happened
almost every day where they called me bad words so I decided to teach the ring leader a lesson. I’ve
never been in a fight before but I realized that sometimes you have to make a stand against the people
that constantly hurt you, especially emotionally. I hit him in the face a couple of times and I got [the]
respect I finally deserved. (pp. 545–546)
Morrill et al. (2000:553) summarize their classification of the youth narratives in a simple table that high-
lights the frequency of each type of narrative and the characteristics associated with each of them (Exhibit 10.8).
How does such an analysis contribute to our understanding of youth violence? Morrill et al. (2000) first empha-
size that their narratives “suggest that consciousness of conflict among youths—like that among adults—is not
a singular entity, but comprises a rich and diverse range of perspectives” (p. 551).
Theorizing inductively, Morrill et al. (2000:553–554) then attempt to explain why action tales were much
more common than the more adult-oriented normative, rational, or emotionally expressive tales. One pos-
sibility is Gilligan’s (1988) theory of moral development, which suggests that younger students are likely to
limit themselves to the simpler action tales that “concentrate on taken-for-granted assumptions of their peer
and wider cultures, rather than on more self-consciously reflective interpretation and evaluation” (Morrill
et al. 2000:554). More generally, Morrill et al. (2000) argue, “We can begin to think of the building blocks of
cultures as different narrative styles in which various aspects of reality are accentuated, constituted, or chal-
lenged, just as others are deemphasized or silenced” (p. 556).
In this way, Morrill et al.’s (2000) narrative analysis allowed an understanding of youth conflict to
emerge from the youths’ own stories while also informing our understanding of broader social theories
and processes.
Narrative analysis can also use documents and observations and focus more attention on how stories are
constructed, rather than on the resulting narrative (Hyvärinen 2008:452). Narrative analyst Catherine Kohler
Riessman (2008:67–73) describes the effective combination of data from documents, interviews, and field
observations to learn how members of Alcoholics Anonymous (AA) developed a group identity (Cain 1991).
Propositions that Carole Cain (1991:228) identified repeatedly in the documents enter into stories as guidelines

Chapter 10 Qualitative Data Analysis
341
for describing the progression of drinking, the desire and inability to stop, the necessity of “hitting bottom”
before the program can work, and the changes that take place in one’s life after joining AA.
Cain then found that this same narrative was expressed repeatedly in AA meetings. She only interviewed
three AA members but found that one who had been sober and in AA for many years told “his story” using this
basic narrative, while one who had been sober for only 2 years deviated from the narrative in some ways. One
interviewee did not follow this standard narrative at all as he told his story; he had attended AA only sporadi-
cally for 20 years and left soon after the interview. Cain (1991) explains,
I argue that as the AA member learns the AA story model, and learns to place the events and experi-
ences of his own life into the model, he learns to tell and to understand his own life as an AA life, and
himself as an AA alcoholic. The personal story is a cultural vehicle for identity acquisition. (p. 215)
Grounded Theory
Theory development occurs continually in qualitative data analysis (Coffey &
Atkinson 1996:23). Many qualitative researchers use a method of developing
theory during their analysis that is termed grounded theory, which involves
building up inductively a systematic theory that is grounded in, or based on, the
observations. The grounded theorist first summarizes observations into concep-
tual categories, and tests the coherence of these categories directly in the research
setting with more observations. Over time, as the researcher refines and links the
conceptual categories, a theory evolves (Glaser & Strauss 1967; Huberman & Miles 1994:436). Exhibit 10.9
diagrams the grounded theory of a chronic illness “trajectory” developed by Strauss and Corbin (1990:221).
Their notes suggested to them that conceptions of self, biography, and body are reintegrated after a process
of grieving.
Exhibit 10.8
Summary Comparison of Youth Narratives
∗
Representation of
Action Tales
(N = 144)
Moral Tales
(N = 51)
Expressive
Tales (N = 35)
Rational Tales
(N = 24)
Bases of everyday
conflict
Disruption of
everyday routines
& expectations
Normative
violation
Emotional
provocation
Goal
obstruction
Decision making Intuitive Principled
stand
Sensual Calculative
choice
Conflict handling Confrontational Ritualistic Cathartic Deliberative
Physical violence
†
In 44% (N = 67) In 27% (N = 16) In 49% (N = 20) In 29% (N = 7)
Adults in youth
conflict control
Invisible or
background
Sources of
rules
Agents of
repression
Institutions of
social control
∗
Total N = 254.
†
Percentages based on the number of stories in each category.
Grounded theory Systematic
theory developed inductively,
based on observations that are
summarized into conceptual
categories, reevaluated in the
research setting, and gradually
refined and linked to other
conceptual categories.

Investigating the Social World
342
As observation, interviewing, and reflection continue, grounded theory researchers refine their defini-
tions of problems and concepts and select indicators. They can then check the frequency and distribution of
phenomena: How many people made a particular type of comment? How often did social interaction lead to
arguments? Social system models may then be developed, which specify the relationships among different
phenomena. These models are modified as researchers gain experience in the setting. For the final analysis,
the researchers check their models carefully against their notes and make a concerted attempt to discover
negative evidence that might suggest that the model is incorrect.
Heidi Levitt, Rebecca Todd Swanger, and Jenny Butler (2008:435) used a systematic grounded method
of analysis to understand the perspective of male perpetrators of violence on female victims. Research
participants were recruited from programs the courts used in Memphis to assess and treat perpetrators
who admitted to having physically abused a female intimate partner. All program participants were of
low socioeconomic status, but in other respects Levitt and her colleagues (2008:436) sought to recruit a
diverse sample.
The researchers (Levitt et al. 2008:437–438) began the analysis of their interview transcripts by dividing
them up into “meaning units”—“segments of texts that each contain one main idea”—and labeling these
units with terms like those used by participants. They then compared these labels and combined them into
larger descriptive categories. This process continued until they had combined all the meaning units into seven
different clusters. Exhibit 10.10 gives an example of two of their clusters and the four categories of meaning
units combined within each (Levitt et al. 2008:439).
Here is how Levitt and her colleagues (2008) discuss the comments that were classified in Cluster 2,
Category 3:
Accordingly, when conflicts accumulated that could not be easily resolved, many of the men (5 of 12)
thought that ending the relationship was the only way to stop violence from recurring. (p. 440)
Exhibit 10.9
A Grounded Theory Model
TIME
REFLECTION PROCESS
Looping Process
Contextualizing Crystallization
decrystallization
recrystallization
Trajectory with Biography
Trajectory/Biography
Degrees of Contextualizing
reviews
Segmented
integrated
The BBC chain
Conceptions of self
Biography Body
Coming to Terms - takes place through confrontations
leads to integration/reintegration process - varies 0 to 100%
Time
recalls
projections
Interpreted in present
with:
chronicity
limitations
death
brought about by:
trajectory changes
biographical changes
interaction
activity/behavior
takes place through:
letting go
grieving
reconstructing
from/to:
nonacceptance
acceptance
transcendence

Chapter 10 Qualitative Data Analysis
343
I don’t deal with anybody so I don’t have any conflicts. . . . It makes me feel bad because I be lonely
sometime, but at the same time, it’s the best thing going for me right now. I’m trying to rebuild me.
I’m trying to put me on a foundation to where I can be a total leader. Like I teach my sons, “Be leaders
instead of followers.” (cited in Levitt et al. 2008:440)
Although this interviewee’s choice to isolate himself was a strategy to avoid relational dependency and
conflict, it left him without interpersonal support and it could be difficult for him to model healthy
relationships for his children. (p. 440)
With procedures such as these, the grounded theory approach develops general concepts from careful
review of text or other qualitative materials and can then suggest plausible relationships among these concepts.
Qualitative Comparative Analysis
Daniel Cress and David Snow (2000) asked a series of very specific questions about social movement outcomes
in their study of homeless social movement organizations (SMOs). They collected qualitative data from about
15 SMOs in eight cities. A content analysis of newspaper articles indicated that these cities represented a range
of outcomes, and the SMOs within them were also relatively accessible to Cress and Snow due to prior contacts.
In each of these cities, Cress and Snow used a snowball sampling strategy to identify the homeless SMOs and
the various supporters, antagonists, and significant organizational bystanders with whom they interacted.
They then gathered information from representatives of these organizations, including churches, other activ-
ist organizations, police departments, mayors’ offices, service providers, federal agencies, and, of course, the
SMOs themselves.
Exhibit 10.10
Clusters and Categories in a Grounded Theory Analysis
Clusters (endorsement) Categories (endorsement)
1. The arrest incident is a hurdle
or a test from god that I alone
have to deal with, although the
responsibility for the abuse was
not all my own. (10)
1. If alcohol or drugs had not been in the picture, we wouldn’t
have come to blows: Substance use is thought to increase
the rate of IPV (2)
2. I don’t want to get involved in conflict because I don’t want
to deal with its consequences (9)
3. Joint responsibility in conflict depends on who did more
fighting (8)
4. How women cause IPV: Being treated as a child through
nagging and being disrespected (5)
2. Passive avoidance and
withdrawal from conflict is the
best way to prevent aggression
and to please god. (10)
1. DV thought to be “cured” by passively attending classes
and learning anger management (6)
2. Religious interventions have been vague or guilt
producing, we need explicit advice and aren’t getting it (9)
3. Intimate partner violence can be stopped by cutting off
relationships, but this can be a painful experience (5)
4. Should resolve conflict to create harmony and avoid
depression—but conflict may increase as a result (10)

Investigating the Social World
344
To answer their research questions, Cress and Snow (2000) needed to operationalize each of the various
conditions that they believed might affect movement outcomes, using coding procedures that were much more
systematic than those often employed in qualitative research. For example, Cress and Snow defined “sympa-
thetic allies” operationally as
the presence of one or more city council members who were supportive of local homeless mobilization.
This was demonstrated by attending homeless SMO meetings and rallies and by taking initiatives to
city agencies on behalf of the SMO. (Seven of the 14 SMOs had such allies.) (p. 1078)
Cress and Snow (2000) also chose a structured method of analysis, qualitative comparative analysis
(QCA), to assess how the various conditions influenced SMO outcomes. This procedure identifies the com-
bination of factors that had to be present across multiple cases to produce a particular outcome (Ragin 1987).
Cress and Snow (2000) explain why QCA was appropriate for their analysis:
QCA . . . is conjunctural in its logic, examining the various ways in which specified factors interact
and combine with one another to yield particular outcomes. This increases the prospect of discerning
diversity and identifying different pathways that lead to an outcome of interest and thus makes this
mode of analysis especially applicable to situations with complex patterns of interaction among the
specified conditions. (p. 1079)
Exhibit 10.11 summarizes the results of much of Cress and Snow’s (2000) analysis. It shows that home-
less SMOs that were coded as organizationally viable used disruptive tactics, had sympathetic political allies,
and presented a coherent diagnosis and program in response to the problem they were protesting were very
likely to achieve all four valued outcomes: (1) representation, (2) resources, (3) protection of basic rights, and
(4) some form of tangible relief. Some other combinations of the conditions were associated with increased like-
lihood of achieving some valued outcomes, but most of these alternatives less frequently had positive effects.
The qualitative textual data on which the codes were based indicate how particular combinations of con-
ditions exerted their influence. For example, one set of conditions that increased the likelihood of achieving
increased protection of basic rights for homeless persons included avoiding disruptive tactics in cities that were
more responsive to the SMOs. Cress and Snow (2000) use a quote from a local SMO leader to explain this process:
We were going to set up a picket, but then we got calls from two people who were the co-chairs of the
Board of Directors. They have like 200 restaurants. And they said, “Hey, we’re not bad guys, can we
sit down and talk?” We had been set on picketing . . . Then we got to thinking, wouldn’t it be bet-
ter . . . if they co-drafted those things [rights guidelines] with us? So that’s what we asked them to do.
We had a work meeting, and we hammered out the guidelines. (p. 1089)
In Chapter 12, you will learn more about qualitative comparative analysis and see how this type of method
can be used to understand political processes.
Case-Oriented Understanding
Like many qualitative approaches, a case-oriented understanding attempts to understand a phenomenon
from the standpoint of the participants. The case-oriented understanding method reflects an interpretive
research philosophy that is not geared to identifying causes but provides a different way to explain social phe-
nomena. For example, Constance Fischer and Frederick Wertz (2002) constructed such an explanation of the
effect of being criminally victimized. They first recounted crime victims’ stories and then identified common
themes in these stories.

Chapter 10 Qualitative Data Analysis
345
Their explanation began with a description of what they termed the process of “living routinely” before
the crime: “
he/she . . . feels that the defended against crime could never happen to him/her.” “ . . . I
said, ‘nah, you’ve got to be kidding’” (pp. 288–289, emphasis in original).
In a second stage, “being disrupted,” the victim copes with the discovered crime
and fears worse outcomes: “You imagine the worst when it’s happening . . . I just
kept thinking my baby’s upstairs.” In a later stage, “reintegrating,” the victim begins
to assimilate the violation by taking some protective action: “But I clean out my
purse now since then and I leave very little of that kind of stuff in there.” (p. 289)
Finally, when the victim is “going on,” he or she reflects on the changes the crime
produced: “I don’t think it made me stronger. It made me smarter.” (p. 290)
You can see how Fischer and Wertz (2002:288–290) constructed an explanation of the effect of crime on its
victims through this analysis of the process of responding to the experience. This effort to “understand” what
happened in these cases gives us a much better sense of why things happened as they did.
2 Visual Sociology
For about 150 years, people have been creating a record of the social world with photography. This creates the
possibility of “observing” the social world through photographs and films and of interpreting the resulting
images as a “text.” You have already seen in this chapter how Elizabeth Stokoe’s conversation analysis of “gen-
der talk” (2006) was enriched by her analysis of photographs. In the previous chapter, you learned how Robert
Sampson and Stephen Raudenbush (1999) used systematic coding of videotaped observations to measure
the extent of disorder in Chicago neighborhoods. Visual sociologists and other social researchers have been
developing methods like these to learn how others “see” the social world and to create images for further study.
Continuous video recordings help researchers unravel sequences of events and identify nonverbal expressions
Exhibit 10.11
Multiple Pathways to Outcomes and Level of Impact
Pathways Outcomes Impact
1.
VIABLE
∗
DISRUPT
∗
ALLIES
∗
DIAG
∗
PROG . . . . . . . . . . . .
Representation,
Resources, Rights,
and Relief
Very strong
2.
VIABLE
∗
disrupt
∗
CITY
∗
DIAG
∗
PROG . . . . . . . . . . . . . . . . . . . . . .
Representation and
Rights
Strong
3.
VIABLE
∗
ALLIES
∗
CITY
∗
DIAG
∗
PROG . . . . . . . . . . . . . . . . . . . .
Resources and Relief Moderate
4.
viable
∗
DISRUPT
∗
allies
∗
diag
∗
PROG. . . . . . . . . . . . . . . . . . . . . . . . . . .
Relief Weak
5.
viable
∗
allies
∗
city
∗
diag
∗
PROG . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Relief Weak
6.
viable
∗
disrupt
∗
ALLIES
∗
CITY
∗
diag
∗
prog . . . . . . . . . . . . . . . . .
Resources Weak
Note: Uppercase letters indicate presence of condition and lowercase letters indicate the absence of a condition. Conditions not in the equation are considered
irrelevant. Multiplication signs (*) are read as “and.”
Case-oriented understanding An
understanding of social processes
in a group, formal organization,
community, or other collectivity
that reflects accurately the
standpoint of participants.

Investigating the Social World
346
of feelings (Heath & Luff 2008:501). As in the analysis of written text, however, the visual sociologist must be
sensitive to the way in which a photograph or film “constructs” the reality that it depicts.
An analysis by Eric Margolis (2004) of photographic representations of American Indian boarding schools
gives you an idea of the value of analysis of photographs (Exhibit 10.12). On the left is a picture taken in 1886
of Chiricahua Apaches who had just arrived at the Carlisle Indian School in Carlisle, Pennsylvania. The school
was run by a Captain Richard Pratt, who, like many Americans in that period, felt tribal societies were com-
munistic, indolent, dirty, and ignorant, while Western civilization was industrious and individualistic. So
Captain Pratt set out to acculturate American Indians to the dominant culture. The second picture shows the
result: the same group of Apaches looking like Europeans, not Native Americans—dressed in standard uni-
forms, with standard haircuts, and with more standard posture.
Many other pictures display the same type of transformation. Are these pictures each “worth a thousand
words”? They capture the ideology of the school management, but we can be less certain that they document
accurately the “before and after” status of the students.
Captain Pratt “consciously used photography to represent the boarding school mission as successful”
(Margolis 2004:79). While he clearly tried to ensure a high degree of conformity, there were accusations that
the contrasting images were exaggerated to overemphasize the change (Margolis 2004:78). Reality was being
constructed, not just depicted, in these photographs.
Darren Newbury (2005:1) cautioned the readers of his journal, Visual Studies, that “images cannot be sim-
ply taken of the world, but have to be made within it.” Photo voice is a method of using photography to engage
research participants in explaining how they have made sense of their social worlds. Rather than using images
from other sources, the researcher directing a photo voice project distributes cam-
eras to research participants and invites them to take pictures of their surroundings
or everyday activities. The participants then meet with the researcher to present
their pictures and discuss their meaning. In this way, researchers learn more about
the participants’ social worlds as they see it and react to it. The photo voice method
also engages participants as part of the research team themselves, thus enriching the
researcher’s interpretations of the social world.
Lisa Frohmann (2005) recruited 42 Latina and South Asian women from bat-
tered women’s support groups in Chicago to participate in research about the mean-
ing of violence in their lives. Frohman used photo voice methodology, so she gave each participant a camera.
After they received some preliminary instruction, Frohmann invited participants to take about five to seven
pictures weekly for 4 to 5 weeks. The photographs were to capture persons, places, and objects that represent
Exhibit 10.12
Pictures of Chiricahua Apache Children Before and After Starting
Carlisle Indian School, Carlisle, Pennsylvania, 1886
Photo voice A method in which
research participants take pictures
of their everyday surroundings
with cameras the researcher
distributes, and then meet in
a group with the researcher to
discuss the pictures’ meaning.

Chapter 10 Qualitative Data Analysis
347
the continuums of comfort-discomfort, happiness-sadness, safety-danger, security-vulnerability, serenity-
anxiety, protection-exposure, strength-weakness, and love-hate (Exhibit 10.13). Twenty-nine women then
returned to discuss the results.
With this very simple picture, one participant, Jenny, described how family violence affected her feelings:
This is the dining room table and I took this
picture because the table is empty and I feel that
although I am with my children, I feel that it is
empty because there is no family harmony, which
I think is the most important thing. (cited in
Frohmann 2005:1407)
The image and narrative represent Jenny’s concept
of family: a husband and wife who love each other
and their children. Food and eating together are
important family activities. Part of being a mother
and wife, of caring for her family, is preparing the
food. Her concept of family is fractured (Frohmann
2005:1407).
2 Mixed Methods
Different qualitative methods may be combined to take advantage of different opportunities for data collection
and to enrich understanding of social processes. Researchers may also combine qualitative with quantitative
methods in order to provide a more comprehensive analysis of different types of interrelated social processes.
These combined approaches are all termed mixed methods, but they differ in the relative emphasis given to
one or the other method and in the sequencing of their use in a research project (Cresswell 2010:57).
Combining Qualitative Methods
Qualitative researchers often combine one or more of these methods. Elif Kale-Lostuvali (2007) enriched his
research by using a combination of qualitative methodologies—including participant observation and inten-
sive interviewing—to study the citizen-state encounters after the İzmit earthquake.
One important concept that emerged from both the observations and the interviews was the distinc-
tion between a mag
ˇ
dur (sufferer) and a depremzade (son of the earthquake). This was a critical distinction,
because a mag
ˇ
dur was seen as deserving of government assistance, while a depremzade was considered to be
taking advantage of the situation for personal gain. Kale-Lostuvali (2007) drew on both interviews and partici-
pant observation to develop an understanding of this complex concept:
A prominent narrative that was told and retold in various versions all the time in the disaster area
elaborated the contrast between mag
ˇ
dur (sufferer; that is, the truly needy) and depremzades (sons of
the earthquake) on the other. The mag
ˇ
dur (sufferers) were the deserving recipients of the aid that was
Exhibit 10.13
Picture in Photo Voice Project

Investigating the Social World
348
being distributed. However, they (1) were in great pain and could not pursue what they needed; or
(2) were proud and could not speak of their need; or (3) were humble, always grateful for the little they
got, and were certainly not after material gains; or (4) were characterized by a combination of the pre-
ceding. And because of these characteristics, they had not been receiving their rightful share of the aid
and resources. In contrast, depremzades (sons of the earthquake) were people who took advantage of
the situation. (p. 755)
The qualitative research by Spencer Moore and his colleagues (2004) on the social response to Hurricane
Floyd demonstrates the interweaving of data from focus groups and from participant observation with
relief workers.
Reports of heroic acts by rescuers, innumerable accounts of “neighbors helping neighbors,” and the
comments of HWATF [task force] participants suggest that residents, stranded motorists, relief work-
ers, and rescuers worked and came together in remarkable ways during the relief and response phases
of the disaster.
Like people get along better . . . they can talk to each other. People who hadn’t talked before, they talk now,
a lot closer. That goes, not only for the neighborhood, job-wise, organization-wise, and all that. . . . [Our]
union sent some stuff for some of the families that were flooded out. (Focus Group #4) (pp. 210–211)
Combining Qualitative and Quantitative Methods
Conducting qualitative interviews can often enhance the value of a research design that uses primarily quan-
titative measurement techniques. Qualitative data can provide information about the quality of standardized
case records and quantitative survey measures, as well as offer some insight into the meaning of particular
fixed responses.
It makes sense to use official records to study the treatment of juveniles accused of illegal acts because
these records document the critical decisions to arrest, to convict, or to release (Dannefer & Schutt 1982). But
research based on official records can be only as good as the records themselves. In contrast to the controlled
interview process in a research study, there is little guarantee that officials’ acts and decisions were recorded in
a careful and unbiased manner.
Case Study: Juvenile Court Records
Interviewing officials who create the records, or
observing them while they record information,
can strengthen research based on official records.
A participant observation study of how probation
officers screened cases in two New York juvenile
court intake units shows how important such
information can be (Needleman 1981). As indicated
in Exhibit 10.14, Carolyn Needleman (1981) found
that the concepts most researchers believe they are
measuring with official records differ markedly
from the meaning attached to these records by
probation officers. Researchers assume that send-
ing a juvenile case to court indicates a more severe
disposition than retaining a case in the intake unit,
Exhibit 10.14
Researchers’ and Juvenile Court
Workers’ Discrepant Assumptions
Researcher Assumptions Intake Worker Assumptions
•
Being sent to court is a
harsher sanction than
diversion from court.
•
Screening involves
judgments about
individual juveniles.
•
Official records accurately
capture case facts.
•
Being sent to court often
results in more lenient and
less effective treatment.
•
Screening centers on the
juvenile’s social situation.
•
Records are manipulated
to achieve the desired
outcome.
Chapter 10 Qualitative Data Analysis
349
but probation officers often diverted cases from court because they thought the court would be too lenient.
Researchers assume that probation officers evaluate juveniles as individuals, but in these settings, probation
officers often based their decisions on juveniles’ current social situation (e.g., whether they were living in a
stable home), without learning anything about the individual juvenile. Perhaps most troubling for research
using case records, Needleman (1981) found that probation officers decided how to handle cases first and then
created an official record that appeared to justify their decisions.
Case Study: Mental Health System
The same observation can be made about the value of supplementing fixed-choice survey questions with more
probing, open-ended questions. For example, Renee Anspach (1991) wondered about the use of standard surveys
to study the effectiveness of mental health systems. Instead of drawing a large sample and asking a set of closed-
ended questions, Anspach used snowball sampling techniques to select some administrators, case managers,
clients, and family members in four community mental health systems, and then asked these respondents a
series of open-ended questions. When asked whether their programs were effective, the interviewees were likely
to respond in the affirmative. Their comments in response to other questions, however, pointed to many program
failings. Anspach concluded that the respondents simply wanted the interviewer (and others) to believe in the
program’s effectiveness, for several reasons: Administrators wanted to maintain funding and employee morale;
case managers wanted to ensure cooperation by talking up the program with clients and their families; and case
managers also preferred to deflect blame for problems to clients, families, or system constraints.
Case Study: Housing Loss in Group Homes
Ethnographic data complements quantitative data in my mixed-methods analysis of the value of group
and independent living options for people who are homeless and have been diagnosed with severe mental
illness. Exhibit 10.15 displays the quantitative association between lifetime substance abuse—a diagnosis
recorded on a numerical scale that was made on the basis of an interview with a clinician—and housing
Exhibit 10.15
Substance Abuse and Housing Loss in Group Homes
35
30
25
20
15
10
5
0
None Some Abuse/Dep
Percent

Investigating the Social World
350
loss—another quantitative indicator from service records (Schutt 2011:135). The ethnographic notes
recorded in the group homes reveal orientations and processes that help to explain the substance abuse-
housing loss association (Schutt 2011).
. . . the time has come where he has to decide once and for all to drink or not. . . . Tom has been feeling
“pinned to the bed” in the morning. He has enjoyed getting high with Sammy and Ben, although the
next day is always bad. . . . Since he came back from the hospital Lisandro has been acting like he is
taunting them to throw him out by not complying with rules and continuing to drink. . . . (pp. 131, 133)
In this way, my analysis of the quantitative data reveals what happened, while my analysis of the ethnographic
data helps to understand why.
2 Computer-Assisted Qualitative Data Analysis
The analysis process can be enhanced in various ways by using a computer. Programs designed for qualita-
tive data can speed up the analysis process, make it easier for researchers to experiment with different codes,
test different hypotheses about relationships, and facilitate diagrams of emerging
theories and preparation of research reports (Coffey & Atkinson 1996; Richards &
Richards 1994). The steps involved in computer-assisted qualitative data analysis
parallel those used traditionally to analyze text such as notes, documents, or inter-
view transcripts: preparation, coding, analysis, and reporting. We use three of the
most popular programs to illustrate these steps: HyperRESEARCH, QSR NVivo, and
ATLAS.ti. (A free trial version of HyperRESEARCH and tutorials can be downloaded
from the ResearchWare site, at http://www.researchware.com.)
Text preparation begins with typing or scanning text in a word processor or, with
NVivo, directly into the program’s rich text editor. NVivo will create or import a rich
text file. HyperRESEARCH requires that your text be saved as a text file (as “ASCII”
in most word processors) before you transfer it into the analysis program. HyperRESEARCH expects your text
data to be stored in separate files corresponding to each unique case, such as an interview with one subject.
These programs now allow multiple types of files, including pictures and videos as well as text. Exhibit 10.16
displays the different file types and how they are connected in the organization of a project (a “hermeneutic
unit”) with ATLAS.ti.
Coding the text involves categorizing particular text segments. This is the foundation of much qualita-
tive analysis. Each program allows you to assign a code to any segment of text (in NVivo, you drag through
the characters to select them; in HyperRESEARCH, you click on the first and last words to select text). You
can make up codes as you go through a document and also assign codes that you have already developed to
text segments. Exhibit 10.17 shows the screens that appear in HyperRESEARCH and NVivo at the coding
stage, when a particular text ms “autocode” text by identifying a word or phrase that should always receive
the same code, or, in NVivo, by coding each section identified by the style of the rich text document—for
example, each question or speaker (of course, you should check carefully the results of autocoding). Both
programs also let you examine the coded text “in context”—embedded in its place in the original document.
Computer-assisted qualitative
data analysis Uses special
computer software to assist
qualitative analyses through
creating, applying, and
refining categories; tracing
linkages between concepts; and
making comparisons between
cases and events.

Chapter 10 Qualitative Data Analysis
351
Exhibit 10.17a
HyperRESEARCH Coding Stage
Exhibit 10.16
File Types and Unit Structure in ATLAS.ti
Hermeneutic Unit
Super Codes
Families
Networks
Code Family
uses
causes
causesis a
is a
uses
uses
indicated by
indicated by
supports
PD Family
Memo Family
Codes
Quotations
Primary
documents
indicated-by
contained-in
contained-in

Investigating the Social World
352
In qualitative data analysis, coding is not a one-time-only or one-code-only procedure. Each program
allows you to be inductive and holistic in your coding: You can revise codes as you go along, assign multiple
codes to text segments, and link your own comments (“memos”) to text segments. You can work “live” with
the coded text to alter coding or create new, more subtle categories. You can also place hyperlinks to other
documents in the project or any multimedia files outside it.
Analysis focuses on reviewing cases or text segments with similar codes and examining relationships
among different codes. You may decide to combine codes into larger concepts. You may specify additional
codes to capture more fully the variation among cases. You can test hypotheses about relationships among
codes and develop more free-form models (see Exhibit 10.18). You can specify combinations of codes that
identify cases that you want to examine.
Reports from each program can include text to illustrate the cases, codes, and relationships that you specify.
You can also generate counts of code frequencies and then import these counts into a statistical program for quan-
titative analysis. However, the many types of analyses and reports that can be developed with qualitative analysis
software do not lessen the need for a careful evaluation of the quality of the data on which conclusions are based.
In reality, using a qualitative data analysis computer program is not always as straightforward as it
appears. Scott Decker and Barrik Van Winkle (1996) describe the difficulty they faced in using a computer
program to identify instances of the concept of drug sales:
The software we used is essentially a text retrieval package . . . One of the dilemmas faced in the
use of such software is whether to employ a coding scheme within the interviews or simply to leave
them as unmarked text. We chose the first alternative, embedding conceptual tags at the appropri-
ate points in the text. An example illustrates this process. One of the activities we were concerned
with was drug sales. Our first chore (after a thorough reading of all the transcripts) was to use
the software to “isolate” all of the transcript sections dealing with drug sales. One way to do this
would be to search the transcripts for every instance in which the word “drugs” was used. However,
such a strategy would have the disadvantages of providing information of too general a character
while often missing important statements about drugs. Searching on the word “drugs” would have
Exhibit 10.17b
NVivo Coding Stage

Chapter 10 Qualitative Data Analysis
353
produced a file including every time the word was used, whether it was in reference to drug sales,
drug use, or drug availability, clearly more information than we were interested in. However, such a
search would have failed to find all of the slang used to refer to drugs (“boy” for heroin, “Casper” for
crack cocaine) as well as the more common descriptions of drugs, especially rock or crack cocaine.
(pp. 53–54)
Decker and Van Winkle (1996) solved this problem by parenthetically inserting conceptual tags in the text
whenever talk of drug sales was found. This process allowed them to examine all the statements made by gang
members about a single concept (drug sales). As you can imagine, however, this still left the researchers with
many pages of transcript material to analyze.
2 Ethics in Qualitative Data Analysis
The qualitative data analyst is never far from ethical issues and dilemmas. Data collection should not begin
unless the researcher has a plan that others see as likely to produce useful knowledge. Relations developed
with research participants and other stakeholders to facilitate data collection should also be used to keep
these groups informed about research progress and findings. Research participants should be encouraged
to speak out about emerging study findings (Lincoln 2009:154–155). Throughout the analytic process, the
analyst must consider how the findings will be used and how participants in the setting will react. Miles and
Huberman (1994:293–295) suggest several specific questions that are of particular importance during the
process of data analysis:
• Privacy, confidentiality, and anonymity: “In what ways will the study intrude, come closer to people
than they want? How will information be guarded? How identifiable are the individuals and organizations
studied?” We have considered this issue already in the context of qualitative data collection, but it also must
Exhibit 10.18
A Free-Form Model in NVivo

Investigating the Social World
354
be a concern during the process of analysis. It can be difficult to present a rich description in a case study while
at the same time not identifying the setting. It can be easy for participants in the study to identify each other in
a qualitative description, even if outsiders cannot. Qualitative researchers should negotiate with participants
early in the study the approach that will be taken to protect privacy and maintain confidentiality. Selected
participants should also be asked to review reports or other products before their public release to gauge the
extent to which they feel privacy has been appropriately preserved.
• Intervention and advocacy: “What do I do when I see harmful, illegal, or wrongful behavior on the
part of others during a study? Should I speak for anyone’s interests besides my own? If so, whose interests do
I advocate?” Maintaining what is called guilty knowledge may force the researcher to suppress some parts of
the analysis so as not to disclose the wrongful behavior, but presenting “what really happened” in a report may
prevent ongoing access and violate understandings with participants.
• Research integrity and quality: “Is my study being conducted carefully, thoughtfully, and correctly in terms
of some reasonable set of standards?” Real analyses have real consequences, so you owe it to yourself and those you
study to adhere strictly to the analysis methods that you believe will produce authentic, valid conclusions.
• Ownership of data and conclusions: “Who owns my field notes and analyses: I, my organization, my
funders? And once my reports are written, who controls their diffusion?” Of course, these concerns arise in
any social research project, but the intimate involvement of the qualitative researcher with participants in
the setting studied makes conflicts of interest between different stakeholders much more difficult to resolve.
Working through the issues as they arise is essential.
• Use and misuse of results: “Do I have an obligation to help my findings be used appropriately? What
if they are used harmfully or wrongly?” It is prudent to develop understandings early in the project with all
major stakeholders that specify what actions will be taken to encourage appropriate use of project results and
to respond to what is considered misuse of these results.
Netnographers must consider additional issues:
• The challenge of online confidentiality: While a netnographer should maintain the same privacy
standards as other qualitative researchers, the retention of information on the web makes it difficult to protect
confidentiality with traditional mechanisms. Anyone reading a distinctive quote based on online text can
use a search engine to try to locate the original text. Distinctive online names intended to protect anonymity
still identify individuals who may be the target of hurtful commentary (Kozinets 2010:143–145). Some users
may think of their postings to some online community site as private (Markham 2007:274). For these reasons,
netnographers who study sensitive issues should go to great lengths to disguise the identity of the community
they have studied as well as of its participants who are quoted.
• Gaining informed consent: Since community members can disguise their identities, gaining
informed consent creates unique challenges. Men may masquerade as women and children as adults, and
yet the research should not proceed unless an effort is made to obtain informed and voluntary consent.
Netnographers must make their own identity known, state clearly their expectations for participation,
provide an explicit informed consent letter that is available as discussion participants come and go (Denzin &
Lincoln 2008:274), and attempt to identify those whose identity is not credible through inconsistencies in their
postings (Kozinets 2010:151–154).
Some indigenous peoples have established rules for outside researchers in order to preserve their own
autonomy. These rules may require collaboration with an indigenous researcher, collective approval of admis-
sion to their culture, and review of all research products prior to publication. The primary ethical commitment
is to the welfare of the community as a whole and the preservation of their culture, rather than to the rights of
individuals (Lincoln 2009:162–163).

Chapter 10 Qualitative Data Analysis
355
2 Conclusions
The variety of approaches to qualitative data analysis makes it difficult to provide a consistent set of criteria for
interpreting their quality. Norman Denzin’s (2002:362–363) “interpretive criteria” are a good place to start.
Denzin suggests that at the conclusion of their analyses, qualitative data analysts ask the following questions
about the materials they have produced. Reviewing several of them will serve as a fitting summary for your
understanding of the qualitative analysis process.
• Do they illuminate the phenomenon as lived experience? In other words, do the materials bring the set-
ting alive in terms of the people in that setting?
• Are they based on thickly contextualized materials? We should expect thick descriptions that encom-
pass the social setting studied.
• Are they historically and relationally grounded? There must be a sense of the passage of time between
events and the presence of relationships between social actors.
• Are they processual and interactional? The researcher must have described the research process and his
or her interactions within the setting.
• Do they engulf what is known about the phenomenon? This includes situating the analysis in the con-
text of prior research and also acknowledging the researcher’s own orientation on first starting the
investigation.
When an analysis of qualitative data is judged as successful in terms of these criteria, we can conclude that
the goal of authenticity has been achieved.
As a research methodologist, you should be ready to use qualitative techniques, evaluate research findings
in terms of these criteria, and mix and match specific analysis methods as required by the research problem to
be investigated and the setting in which it is to be studied.
Key Terms
Case-oriented
understanding 344
Computer-assisted qualitative
data analysis 350
Emic focus 322
Ethnography 333
Ethnomethodology 336
Etic focus 322
Grounded theory 341
Matrix 329
Narrative analysis 339
Netnography 335
Photo voice 346
Progressive
focusing 322
Qualitative comparative
analysis (QCA) 344
Tacit knowledge 331
Highlights
• Qualitative data analysts are guided by an emic focus of repre-
senting persons in the setting on their own terms, rather than by
an etic focus on the researcher’s terms.
• Case studies use thick description and other qualitative tech-
niques to provide a holistic picture of a setting or group.
• Ethnographers attempt to understand the culture of a group.

Investigating the Social World
356
• Narrative analysis attempts to understand a life or a series of
events as they unfolded, in a meaningful progression.
• Grounded theory connotes a general explanation that develops
in interaction with the data and is continually tested and refined
as data collection continues.
• Special computer software can be used for the analysis of quali-
tative, textual, and pictorial data. Users can record their notes,
categorize observations, specify links between categories, and
count occurrences.
STUDENT STUDY SITE
To assist in completing the web exercises, please access the study site at www.sagepub.com/schuttisw7e, where
you will find the web exercise with accompanying links. You’ll find other useful study materials such as self-quizzes
and e-flashcards for each chapter, along with a group of carefully selected articles from research journals that illus-
trate the major concepts and techniques presented in the book.
Discussion Questions
1. List the primary components of qualitative data analysis
strategies. Compare and contrast each of these compo-
nents with those relevant to quantitative data analysis.
What are the similarities and differences? What differ-
ences do these make?
2. Does qualitative data analysis result in trustworthy results—in
findings that achieve the goal of authenticity? Why would any-
one question its use? What would you reply to the doubters?
3. Narrative analysis provides the “large picture” of how a life
or event has unfolded, while conversation analysis focuses on
the details of verbal interchange? When is each method most
appropriate? How could one method add to another?
4. Ethnography, grounded theory, and case-oriented under-
standing each refers to aspects of data analysis that are an
inherent part of the qualitative approach. What do these
approaches have in common? How do they differ? Can you
identify elements of these three approaches in this chapter’s
examples of ethnomethodology, netnography, qualitative
comparative analysis, and narrative analysis?
Practice Exercises
1. Attend a sports game as an ethnographer. Write up your
analy sis and circulate it for criticism.
2. Write a narrative in class about your first date, car, college
course, or something else that you and your classmates agree
on. Then collect all the narratives and analyze them in a “com-
mittee of the whole.” Follow the general procedures discussed
in the example of narrative analysis in this chapter.
3. Go forth and take pictures! Conduct a photo voice project
with your classmates and write up your own review of the
group’s discussion of your pictures.
4. Review one of the articles on the book’s study site, www
.sagepub.com/schuttisw7e, that used qualitative methods.
Describe the data that were collected, and identify the steps
used in the analysis. What type of qualitative data analy-
sis was this? If it is not one of the methods presented in this
chapter, describe its similarities to and differences from one
of these methods. How confident are you in the conclusions,
given the methods of analysis used?
5. Review postings to an on-line discussion group. How could
you study this group using netnography? What challenges
would you encounter?

Chapter 10 Qualitative Data Analysis
357
Ethics Questions
1. Pictures are worth a thousand words, so to speak, but is that
1,000 words too many? Should qualitative researchers (like
yourself) feel free to take pictures of social interaction or
other behaviors anytime, anywhere? What limits should an
institutional review board place on researchers’ ability to
take pictures of others? What if the picture of the empty table
in this chapter also included the abusive family member who
is discussed? What if the picture was in a public park, rather
than in a private residence?
2. Participants in social settings often “forget” that an ethnog-
rapher is in their midst, planning to record what they say
and do, even when the ethnographer has announced his or
her role. New participants may not have heard the announce-
ment, and everyone may simply get used to the ethnographer
as if he or she was just “one of us.” What efforts should an
ethnographer take to keep people informed about their work
in the setting they are studying? Consider settings such as a
sports team, a political group, and a book group.
Web Exercises
1. The Qualitative Report is an online journal about qualitative
research. Inspect the table of contents for a recent issue at
www.nova.edu/ssss/QR/index.html. Read one of the articles
and write a brief article review.
2. Be a qualitative explorer! Go to the “Qualitative Page” website
and see what you can find that enriches your understanding
of qualitative research (www.qualitativeresearch.uga.edu/
QualPage). Be careful to avoid textual data overload.
HyperRESEARCH Exercises
1. Eight essays written by college-age women in Hesse-Biber’s
(1989) “Cinderella Study” are saved on the book’s study
site. The essays touch on how young women feel about com-
bining work and family roles. Download and install Hyper-
RESEARCH from http://www.researchware.com/ and open the
Cinderella Study (Find it at C:\ P ro gram Fi le s\HyperRESEARCH 3.0\
Documentation\Tutorials\Cinderella Study\Cinderella Study
.hs2). Look over the preliminary code categories that have
already been applied to each essay. Do you agree with the code
categories/themes already selected? What new code categories
would you add and why? Which would you delete? Why? What
are some of the common themes/codes that cut across all eight
cases concerning how young women think about what their life
will be like in 20 years?
2. Work through the tutorial on HyperRESEARCH that was
downloaded with the program. How does it seem that quali-
tative analysis software facilitates the analysis process? Does
it seem to you that it might hinder the analysis process in
some ways? Explain your answers.
Developing a Research Proposal
1. Which qualitative data analysis alternative is most appro-
priate for the qualitative data you proposed to collect
for your project (Exhibit 2.14, #18)? Using the approach,
develop a strategy for using the techniques of qualitative
data analysis to analyze your textual data.
