International Journal of Caring Sciences May-August 2021 Volume 14| Issue 2| Page 1237
www.internationaljournalofcaringsciences.org
Original Article
Standard Precaution Practices among Doctors and Nurses in the
University College Hospital Ibadan
Akinade, Tolulope Abisola
Department of Social Work, University of Ibadan, Nigeria
Gandonu Micheal Babatunde
Department of Guidance & Counselling, Lagos State University, Nigeria
Abstract
This study examined practice of standard precautions among health workers in the University College Hospital
Ibadan. The research adopted a cross-sectional survey design using quantitative research methods.The study was
conducted within the premises of the University College Hospital (UCH), Ibadan. In this study, the reference
population included doctors and nurses in UCH, from which a representative sample size of 308 participants
was obtained. Multistage sampling technique was used to select participants for the study. Data collection was
conducted using a structured, pre-coded, self-administered questionnaire. Three hypotheses were formulated and
tested using t-test and multiple regression analysis. Majority of the HCWs reported as they ‘always’ use gloves
and gown during procedures that needs this protective equipment. But only 10.4% of them reported that they
‘always’ wore Mask and Goggle. Major reasons for low practice levels included incidents of inadequate
supplies, carelessness, discomfort with use and discomfort among patients. Further results showed that there was
no significant difference in practice of standard precautions between nurses and doctors [t(292)=-.352; p>.05].
There was also no significant difference in practice of standard precautions between respondents who reported
more positive attitude towards standard precautions and their counterparts who reported less positive attitude
towards standard precautions [t(292)=.084; p>.05]. Age (β=-.041; p>.05) and marital status (β=-.003; p>.05)
emerged as insignificant predictors of standard precautions practice, work experience (β=.103; p<.05) emerged
as a significant positive predictor of standard precautions practice among nurses and doctors in UCH. Suitable
recommendations were provided in line with the study outcomes.
Keywords: Standard precaution practice, Doctor, Nurse, University College Hospital
Introduction
Health care workers (HCWs) such as medical
doctors, nurses, laboratory staff and attendants
who work in health care settings are frequently
exposed to infectious diseases during their work.
Infections acquired in the health care setting are
major causes of anxiety for HCWs. These
infections include diseases like hepatitis B virus
(HBV), hepatitis C virus (HCV), human
immunodeficiency Virus (HIV) and other blood
borne diseases (Hosoglu et al., 2011). Globally,
it has been estimated that the annual proportions
of HCWs exposed to blood-borne pathogens
were 2.6% for HCV, 5.9% for HBV, and 0.5%
for HIV (Cutter & Jordan 2012). In Nigeria,
documented cases of HIV infection following
occupational exposure among HCWs has
continually increased to an annual average of
1000 cases since the first recorded case in 1984
(Okechukwu et al., 2012). The fact that patients’
blood and other body fluids are potentially
hazardous to HCWs, the safety of HCWs at their
work place has become a great concern for health
professionals all over the world (Izegbu, Amole
& Ajayi, 2006).
Studies have shown that HCWs are at risk of
being infected with blood borne pathogens due to
their occupational exposure to blood and other
body fluids (BBF) (Agaba et al., 2012;
Omiepirisa, 2012; Okechukwu et al., 2012;;
Prüss-Üstün et al., 2005). It has been estimated
that HCWs’ exposure to blood-borne pathogens
contributes annually to about 16,000 HCV
infections and 66,000 HBV infections among
HCWs worldwide (Prüss-Üstün et al., 2005) and
90% of these infections occurred in low-income

International Journal of Caring Sciences May-August 2021 Volume 14| Issue 2| Page 1238
www.internationaljournalofcaringsciences.org
countries (Kermode et al., 2005). In general, the
most common route of exposure is through
sharps; lancets, broken glass, needles and other
sharps instruments, while exposures from needle
stick injuries has been reported as the most
common of all (Omiepirisa, 2012). However, it
should be noted that many studies have
demonstrated that the incidence of needle stick
injuries are poorly reported globally and more so
in developing countries (Honda et al., 2011;
Bolarinwa et al., 2011; Chalya et al., 2015;
Voide et al., 2012; Amira et al., 2014). The
reasons for non-report of these incidents range
from perceived low risk of infection transmission
following exposure, to perceived lack of time
(Bolarinwa et al., 2011; Chalya et al., 2015;
Voide C et al., 2012; Amira et al., 2014).
The earliest attempt to reduce the incidence of
hospital-acquired infections among Health care
workers was in 1877, when the first
recommendation for isolation precautions was
published in the United States for patients with
known infectious diseases (Lynch, 1949; CDC,
1996). Several recommendations, guidelines and
protocols have since been published by the
Centers for Disease Control and Prevention
(CDC), the World Health Organization (WHO)
and the United States Occupational Safety and
Health Administration (OSHA); most of which
were about protection against specific diseases or
during a particular procedure. Countries adopt
recommendations and guidelines from these
bodies to develop their country-specific policies
and guidelines.
In 1983, the CDC published the Universal Blood
and Body Fluid precautions, simply called the
‘Universal Precautions’ (CDC, 1985; Farlex,
2012). These precautions were meant for patients
known to have or sSPected to have an infectious
blood-borne pathogen and were also meant to
prevent parenteral, mucous membrane and non-
intact skin exposures to blood-borne pathogens
by Health care workers (CDC, 1985). They apply
to blood, semen, vaginal secretions, deep body
fluids, body fluids with visible blood, but not to
faeces, nasal secretions, sputum, sweat, urine,
tears and vomitus; unless they contain visible
blood (CDC, 1983). In 1991, OSHA published
its Occupational Exposure to Blood-borne
Pathogen Standards, where they incorporated the
Universal Precautions and added requirements
for employers of Health care workers to provide
engineering controls, protective barriers and
devices, immunization against hepatitis for
Health care workers and training of Health care
workers on the Universal Precautions (Farlex,
2012).
However, in 1996, the CDC published new
guidelines known as the Standard Precautions
sometimes, also referred to as the ‘Safety
Precautions’ (SP) (Farlex, 2012). It includes the
Universal Precautions as well as other
recommendations for care of patients irrespective
of their diagnosis or presumed infection status.
The SP apply to blood, all body fluids, secretions
and excretions except sweat, with or without the
presence of visible blood (Garner, 1996; CDC,
2011). It includes: hand hygiene, use of personal
protective equipment (e.g., gloves, facemasks),
respiratory hygiene and cough etiquette, safe
injection practices and safe handling of
potentially contaminated equipment or surfaces
in the patient environment (CDC, 2011),
decontamination and disinfection of instruments,
maintenance of sanitary workplace and safe
waste disposal; which are the core principles of
the SP (USAID, 2000). Under each of these
principles are the recommended activities or
‘dos’ and ‘don’t’ expected of Health care
workers in order to achieve adherence to the
principles. These recommended activities are the
SP practices.
Currently the National Agency for the Control of
AIDS (NACA) in collaboration with the
Nigerian Federal Ministry of Health (FMOH) is
saddled with the responsibility of developing,
reviewing and disseminating guidelines and
policies related to safety practices among Health
care workers in health care settings in the
country (NACA, 2010). Guidelines and policies
are being periodically reviewed and disseminated
while implementation at the State and Local
Government levels are meant to be monitored by
the State and Local Government arms of the
FMOH and NACA (NACA, 2010; NACA,
2014). Some of the specific guidelines developed
to ensure optimal practise of the SP in health care
settings in Nigeria includes the following;
National policy on universal safety precaution,
Guidelines on TB infection control, TB infection
control plan, Policy and Guidelines on safety of
blood and blood products, Health care waste
management protocol, National protocol of post
exposure prophylaxis and Health workers’
injection safety guidelines (NACA, 2010).
However, no report or document was found

International Journal of Caring Sciences May-August 2021 Volume 14| Issue 2| Page 1239
www.internationaljournalofcaringsciences.org
about the efforts of the FMOH and NACA to
enforce the implementation of these guidelines
and policies at all levels.
Statement of Problem: The practice of standard
precautions is being widely promoted to protect
Health care workers from occupational exposure
to body fluids and consequent risk of infection
with blood-borne pathogens. Health care workers
are potentially exposed to blood-borne and other
infections through contact with body fluids while
performing their duties. Health care workers
frequently provide care to patients whose HBV,
HIV and hepatitis C virus (HCV) status is
unknown, and individuals may be asymptomatic
for months to years while being infectious. The
occupational health of the health care workforce
of about 35 million people globally, representing
about 12% of the working population, has been
neglected. About three million Health care
workers worldwide receive percutaneous
exposure to blood-borne pathogens each year.
These injuries may result in 15,000 HCV, 70,000
HBV and 500 HIV infections, and more than
90% of these infections occur in developing
countries. Worldwide, about 40% of HBV and
HCV infections and 2.5% of HIV infections in
Health care workers are attributable to
occupational sharps exposures, which are mainly
preventable (WHO, 2016)
The Occupational Safety and Health
Administration estimates that 5.6 million Health
care workers worldwide, who handle sharp
devices, are at risk of occupational exposure to
blood-borne pathogens. Needle stick injuries
were shown to be the commonest (75.6%)
mechanism for occupational exposure in a
Nigerian teaching hospital. These injuries are
usually under-reported for so many reasons,
which include stigma that could be associated
with an eventual infection with HIV in the
affected HCW. There is no immunization for
HIV and HCV, thus the most effective
prevention is through regular practice of the
standard precautions.
Compliance to standard precautions is low in
public secondary health facilities, especially in
resource-limited settings, thus exposing Health
care workers to the risk of infection.
Occupational safety of Health care workers is
often neglected in low-income countries in spite
of the greater risk of infection due to higher
disease prevalence, low level awareness of the
risks associated with occupational exposure to
blood, inadequate supply of personal protective
equipment (PPE), and limited organizational
support for safe practices. Blood and other body
fluids from patients are becoming increasingly
hazardous to those who provide care for them.
There is therefore a need for adequate measures
to ensure compliance to standard precautions and
reduce the risk of infection among Health care
workers.
Research Hypotheses
In line with the study objectives, the following
research hypotheses are formulated for testing.
Hi: There will be significant difference in
practice of standard precautions across health
care workers in the university college hospital
Ibadan.
Hi: Attitude towards standard precautions
will have a significant influence on practice of
standard precautions among health care workers
in the university college hospital Ibadan
Hi: Age, years of experience and marital
status will have significant joint and independent
influence on practice of standard precautions
among health care workers in the university
college hospital Ibadan
Research Methods
Design and Settings: The research adopted a
cross-sectional survey design using quantitative
research methods to examine practice of standard
precautions among health workers in the
University College Hospital Ibadan. The study
was conducted within the premises of the
University College Hospital (UCH), Ibadan. The
University College Hospital (UCH) is
strategically located in Ibadan North LGA. The
physical development of the Hospital
commenced in 1953 in its present site and was
formally commissioned after completion on 20
November 1957. The Hospital, at inception in
1957, prior to the Act of Parliament, had two
clinical Departments (Medicine and Surgery).
However, the Hospital has evolved to
accommodate about 65 Departments. The
Hospital, though a tertiary healthcare facility,
still caters for a lot of the primary and secondary
healthcare burden. The patients turn out in the
Emergency Department of the Hospital averages
6500 annually and about 150,000 new patients

International Journal of Caring Sciences May-August 2021 Volume 14| Issue 2| Page 1240
www.internationaljournalofcaringsciences.org
are seen in the various out-patient clinics every
year.
Population and Study Sample: In this study,
the reference population included doctors and
nurses in University College Hospital (UCH),
Ibadan. A representative sample size of 308
participants was obtained based on an estimated
total number of nurses and doctors in the
University College Hospital (UCH), Ibadan. The
hospital has a staff strength of over 3000 which
comprise at least 600 doctors and 1000 nurses
(Iyun, 2016). The sample size was obtained using
Slovin sample size determination formula;
n = N / (1+Ne
2
)
where; n=sample size
N=population size
e=error margin
n = 1600/(1 + 1600*.05
2
)
= 1600/5.2
=307.7
= 308 healthcare workers (doctors and nurses)
Sampling Technique: A multistage sampling
technique was used to select participants for the
study. In the first stage, a stratified random
sampling was adopted. This involved creating
limited strata made up of a minimum of 10
units/departments each within the UCH. In the
second stage simple random sampling via the
ballot technique was used to select 5
participating units/departments from each
stratum. The third stage involved the use of
purposive sampling in which nurses and doctors
from each of the participating units/departments
were selected. Factors considered included
eligibility and willingness to participate in the
study
Instrumentation: Data collection was conducted
using a structured, pre-coded, self-administered
questionnaire. Questionnaires are documents
containing questions and other items designed to
elicit information appropriate to specific research
and analysis. The questionnaire is made up of
four main sections, namely, biographical data
(section A), attitude towards standard
precautions (section B), practice of standard
precautions (section C), and factors influencing
compliance of standard precautions (section D).
The answer categories were mutually exclusive
and special instructions were provided where
necessary for easy understanding. A covering
letter also accompanied the questionnaire, which
introduced the study and its purpose to
participants and requested them to participate. It
also provided instructions on how to complete
the questionnaire. Participants were not
requested to write their name or any other form
of identity in the questionnaire in order to ensure
that their identity could not be linked with their
individual responses.
In order to measure the extent to which the
survey instruments have been able to achieve
their aims, the process of content validity will be
employed by cross examination and verification.
The knowledge gained from other investigations,
literature review, theoretical framework and
research methods was used for an initial face
validation while expert assessment from the
project supervisor provided content validatation
for the instrument. Consequently, a number of
items in the questionnaire were subject to
amendment. A pilot study was carried out among
a sample with similar charateristics to the study
population. Outcomes form the pilot study were
subjected to a split half reliability test in order to
obtain the reliability coefficient for the
instrument. Reliability coefficiants obtained were
greater than .70 and deemed adequate for the
study.
Data Collection Method: The researcher,
accompanied by research assistants, visited
participating units/departments within the
University College Hospital in Ibadan. Upon
completion of the administrative protocol, the
purpose of the study was explained to the
management of the units/department. In order to
ensure effective administration of the instrument,
a contact person (nurse/doctor) within each
unit/department was implored to distribute copies
of the questionnaire to all available colleagues
within the unit/department.
The contact persons were encouraged to ask
clarification questions. Printed instructions on
how to complete the instrument was provided on
each questionnaire, in which participants were
assured that there are no right or wrong answers
and a strict measure of confidentiality would be
ensured.
Participants were expected to fill the
questionnaires at their leisure time and return the
completed questionnaires to the contact person at
their earliest possible convenience. Data obtained
International Journal of Caring Sciences May-August 2021 Volume 14| Issue 2| Page 1241
www.internationaljournalofcaringsciences.org
from the study were input and coded into an
SPSS package for data analysis. Both descriptive
and inferential statistics were employed in the
data analysis. These included the use of
percentage frequency, t-test and multiple
regression analysis.
Results
Data was analysed using both descriptive and
inferential statistics. Percentage frequency
distribution tables, t-test and multiple regression
analysis were adopted as analytical techniques.
Results are presented in the following sections
.
Table 1: Distribution of Respondents’ Socio-Demographic Characteristics
Frequency Percent
Age
20-30years 10 3.4
31-40years 101 34.2
41-50years 117 39.7
51-60years 67 22.7
Gender
Male 107 37.3
Female 188 62.7
Marital Status
Single 107 36.3
Married 136 46.1
Divorced 34 11.5
Widowed 18 6.1
Work Experience
1-5years 52 17.6
6-10years 85 28.8
11-15years 102 34.6
16years or more 56 19.0
Designation
Nurse 179 60.7
Doctor 116 39.3
Total 295 100.0
Results from Table 1 show that majority
(74.9%) of the respondents were between
ages 31-50 years. The mean age of the
respondents was 37.6 years with a standard
deviation of 11.2. Their gender distribution
showed that 62.7% of the respondents were
female while the remaining 37.3% were
male. The disparity in gender distribution
can be alluded to the fact that nursing is a
female dominated profession. Further results
show that 36.3% of the respondents were
single while 46.1% of them were married.
the remaining were either divorced (11.5%)
or widowed (6.1%). In terms of their work
experience, 17.6% of the respondents had
work experience ranging from 1-5 years,
28.8% of the respondents had work
experience ranging from 6-10 years, 34.6%
of the respondents had work experience
ranging from 11-15 years, while 19.0% of
the respondents had work experience of 16
years or more.
From 295 HCWs only 61.5% always practice
hand washing after any direct contact with
patient, 34.4% often practice standard
precautions and the remaining 24.1% seldom
practice standard precautions. As shown in
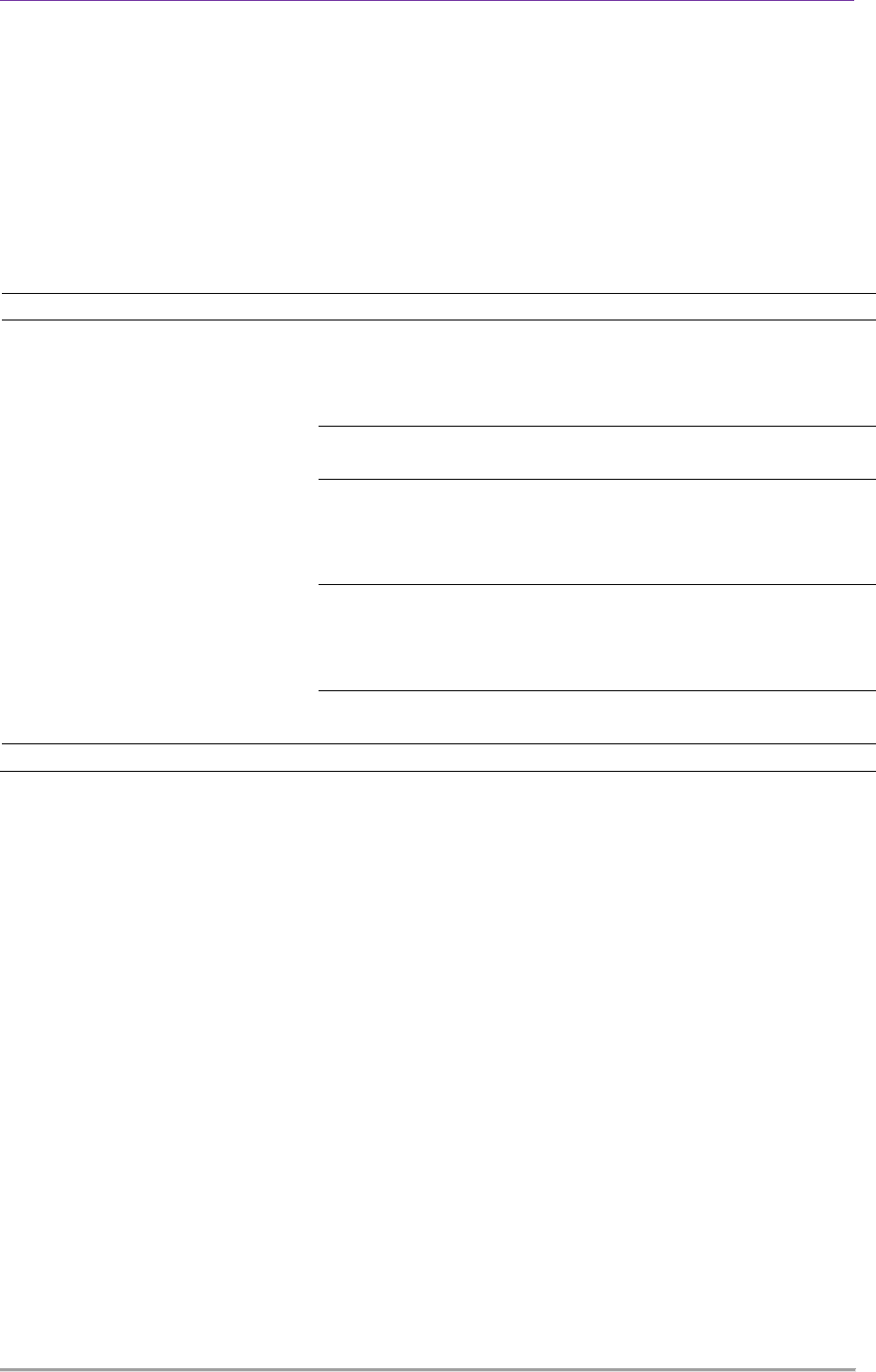
Table 4.2, majority of the HCWs reported as
they ‘always’ use gloves and gown during
procedures that needs this protective
equipment. But only 10.4% of them reported
that they ‘always’ wore Mask and Goggle.
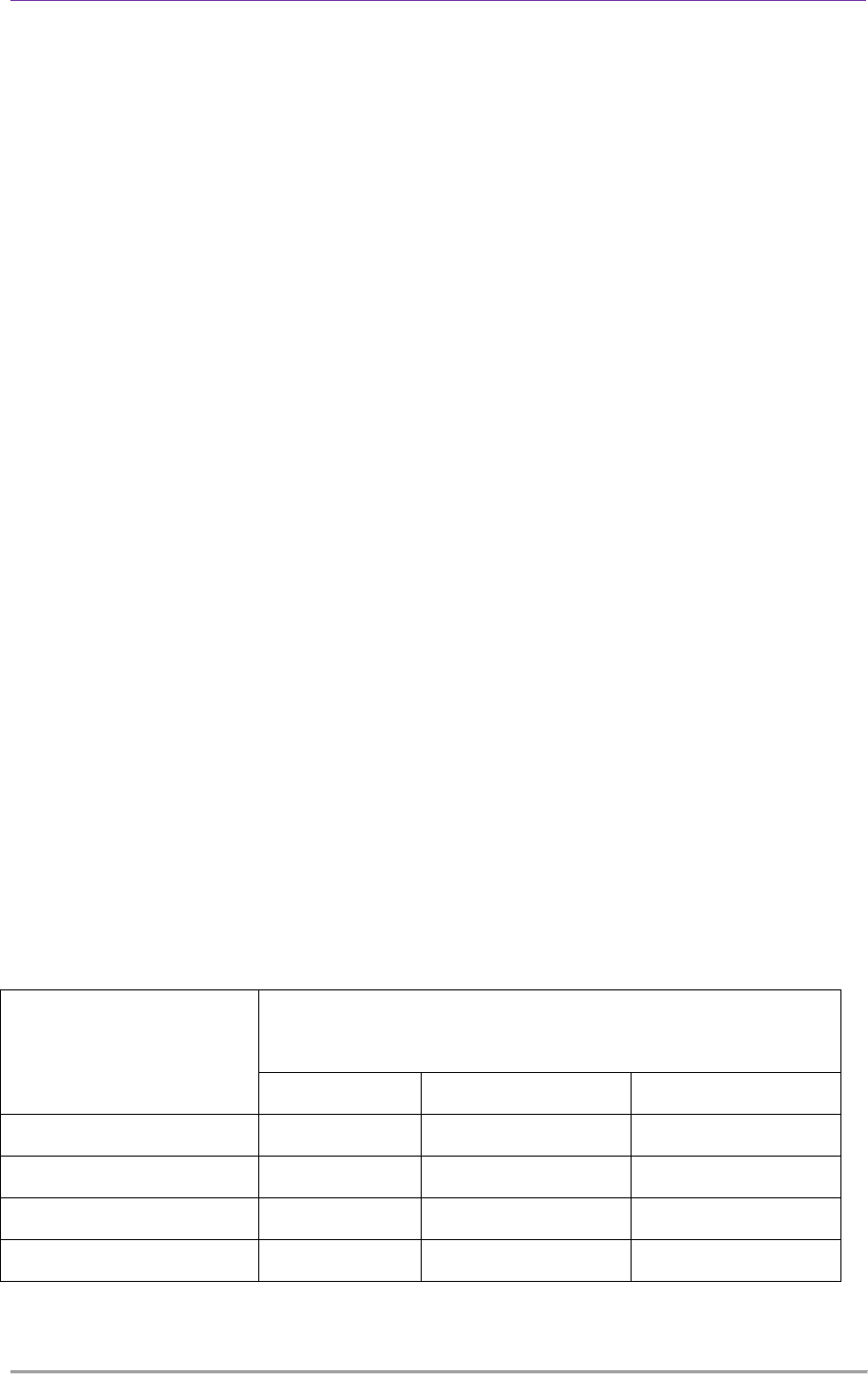
This study further assessed the major reason
for poor practice and most of 84.4% of the
respondents said that water and soap were
not available at patient care areas. As shown
in Table 3, the major reasons for poor
practice of personal protective equipment
like glove, gown and goggle, was shortage of
supply. Furthermore, 60.2% of the HCWs
International Journal of Caring Sciences May-August 2021 Volume 14| Issue 2| Page 1242
www.internationaljournalofcaringsciences.org
reported that they exposed to splash of blood
or body fluid on their mucus membrane (i.e.
eye, nose or mouth) in the last one year.
After giving injection or drawing blood from
patients 82.4% of the HCWs reported not
recapping used needles, 17.0% of them had
recapping and 0.6% of them practiced
bending needles by hand. Regarding to
exposure to sharp or needle stick injury 22.2
% of the HCWs exposed in the last one-year.
Carelessness was the major reason stated by
HCWs for recapping needles (54.1%)
Discarding used needles and other sharps in
a safety box was practiced among 79.5% of
HCWs.
Hypotheses Testing: In line with the
objectives of the study, four hypotheses were
formulated and tested using appropriate
statistical techniques. Results are presented
in the following sections
Hypothesis One: There will be significant
difference in practice of standard precautions
across health care workers in the university
college hospital Ibadan. This hypothesis was
tested using t-test for independent measures.
Results are presented in Table 4.
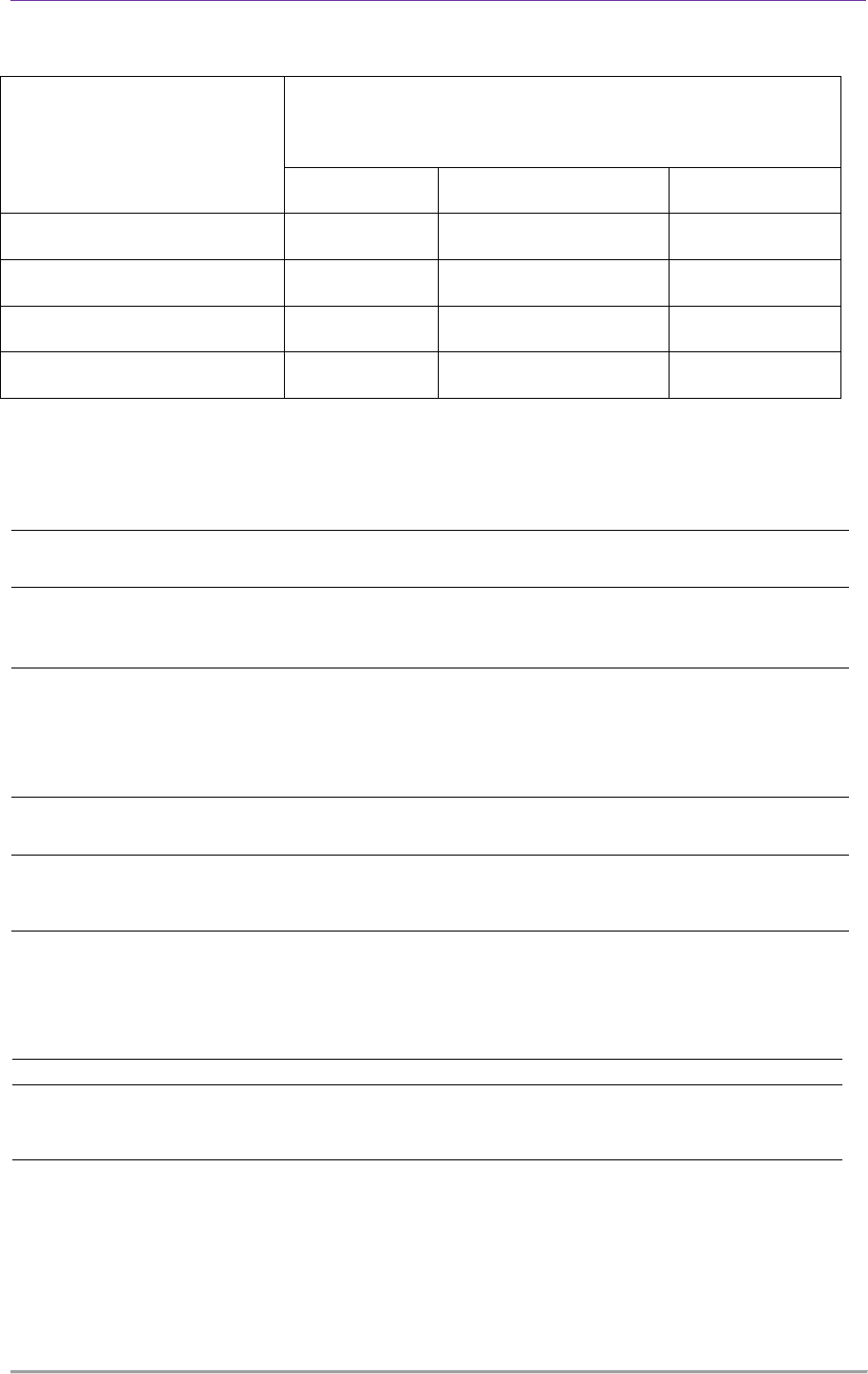
Results from Table 4.4 show that there was
no significant difference in practice of
standard precautions between nurses and
doctors [t(292)=-.352; p>.05]. The results
imply that both nurses and doctors in UCH
exhibit similar practice levels of standard
precautions. The hypothesis stated is
therefore rejected.
Hypothesis Two: Attitude towards standard
precautions will have a significant influence
on practice of standard precautions among
health care workers in the university college
hospital Ibadan. This hypothesis was tested
using t-test for independent measures.
Results are presented in Table 5.
Results from Table 5 show that there was no
significant difference in practice of standard
precautions between respondents who
reported more positive attitude towards
standard precautions and their counterparts
who reported less positive attitude towards
standard precautions [t(292)=.084; p>.05].
The results imply that attitude towards
standard precaution had no significant
influence on practice levels of standard
precaution among nurses and doctors in
UCH. The hypothesis stated is therefore
rejected.
Hypothesis Three: Age, years of experience
and marital status will have significant joint
and independent influence on practice of
standard precautions among health care
workers in the university college hospital
Ibadan. This hypothesis was tested using
multiple regression analysis. Results are
presented in Table 6
Table 2: Standard Precaution Practice
Standard Precaution
Practice
Type of Personal Protective Equipment
N=295
Glove Gown/Plastic Apron Mask and Goggle
Always 86.7 89.9 10.3
Often 11.6 6.8 20.9
Seldom 1.7 3.1 48.9
Never 0 0.1 19.9
International Journal of Caring Sciences May-August 2021 Volume 14| Issue 2| Page 1243
www.internationaljournalofcaringsciences.org
Table 3: Reasons for Poor Practice Level
Reasons for Poor Practice
Level
Type of Personal Protective Equipment
N=295
Glove Gown/Plastic Apron Mask/Goggle
Shortage of Supply 15.6 71.4 84.5
Carelessness 15.6 0 2.3
Discomfort with Use 39.1 24.5 11.6
Discomfort among Patients 29.7 6.1 1.6
Table 4: Summary of t-test showing difference in standard precaution practices
between Nurses and Doctors in UCH
Designation
N Mean Std.
Deviation
df t sig
Standard
Precaution
Practice
Nurse 179 90.1732
9.79269
292 -.352 .725
Doctor 115 90.6000
10.68513
Table 5: Summary of t-test showing influence of attitude towards standard precaution on
practice of standard precaution among nurses and doctors in UCH
Standard Precaution
Attitude
N Mean Std. Dev. df t Sig
Standard
Precaution
Practice
More positive 158
90.3861
8.74969
292 .084 .933
Less positive 136
90.2868
11.57194
Table 6: Summary of multiple regression showing influence of demographics on practice of
standard precaution among nurses and doctors in UCH
R
2
F Sig Beta t Sig.
Age
-.041 -.694 .488
Marital Status .009 .165 .920 -.003 -.050 .960
Work Experience .103 .142 .047

International Journal of Caring Sciences May-August 2021 Volume 14| Issue 2| Page 1244
www.internationaljournalofcaringsciences.org
Results from Table 6 show that age, work
experience and marital status did not have
significant joint influence on practice levels
of standard precautions among nurses and
doctors in UCH [F(3, 290)=.165; p>.05].
However, while age (β=-.041; p>.05) and
marital status (β=-.003; p>.05) emerged as
insignificant predictors of standard
precautions practice, work experience
(β=.103; p<.05) emerged as a significant
positive predictor of standard precautions
practice among nurses and doctors in UCH.
The hypothesis stated is therefore partially
accepted due to the significant influence of
work experience on standard precautions
practice.
Discussion
The first hypothesis which stated that there
will be significant difference in practice of
standard precautions across health care
workers in the university college hospital
Ibadan was not supported. The results imply
that both nurses and doctors in UCH
exhibited similar high practice levels of
standard precautions. The results may be
justified by the fact that training on standard
precautions is paramount for the profession
of nurses and doctors. Therefore, from a
professional point of view, every nurse or
doctor is expected to exhibit high practice
levels of standard precautions. Another
reason for the seemingly high levels of
standard precaution practice among the
respondents may also have emanated from
the effect of social desirability responses
from the study participants.
Supporting these findings, Arinze-Onyia,
Ndu, Aguwa, Modebe and Nwamoh (2018)
assessed the knowledge and practices of SP
among HCWs at the University of Nigeria
Teaching Hospital, Ituku-Ozalla, Enugu
State and found that those who were trained
on SP (70.8%) and PPE (69.7) were
significantly more likely to use PPEs. A
related study by Sadoh, Fawole, Sadoh,
Oladimeji & Sotiloye (2006) practice levels
of standard precautions was not comprised
by majority of the nurses and doctors. Luo et
al. (2010) investigated significant
compliance with SPs by nurses and found
that less than 5% of the 1,444 nurses did not
comply with SP. Similarly,
Maharaj et al.
(2012) that less than 7% of doctors perceived
themselves as non-compliant to the practice of
SPs. However, i
n contrast to the result
obtained in this study, Kolude, Omokhodion
& Owoaje (2004) found that practice of
standard precaution was highest among
surgical and medical residents than nurses.
The second hypothesis which stated that
attitude towards standard precautions will
have a significant influence on practice of
standard precautions among health care
workers in the university college hospital
Ibadan was not supported. The results imply
that attitude towards standard precaution had
no significant influence on practice levels of
standard precaution among nurses and
doctors in UCH. This outcome underscores
theoretical tenets that attitude does not
always predict practice. In the case of this
study, the practice of standard precautions
among majority of the respondents is more
of a professional ethic than a personal
disposition. Therefore, even though the
respondents could be grouped as having
more or less favorable disposition towards
standard precaution, their obligation to
practice these standard precautions was
unwavering.
This outcome is similar to results obtained
by Odusanya (2003) who conducted a study
on attitude and compliance with universal
precautions amongst health workers at an
emergency medical service in Lagos,
Nigeria, and found that their attitude towards
universal compliance did not translate into
safe work practices. A similar study by
Bamigboye and Adesanya (2006) it was
observed that doctor felt that the use of
safety precautions in the medical practice
could not be compromised in an era of
communicable diseases, irrespective of the
personal dispositions.
In another study Alam (2002) examined
knowledge, attitude and practices among

International Journal of Caring Sciences May-August 2021 Volume 14| Issue 2| Page 1245
www.internationaljournalofcaringsciences.org
health care workers (nurses and paramedical
staff) and found a high practice level of
standard safety precautions among them.
Efstathiou et al. (2011) explored how
hospital nurses’ shared experiences affected
by behaviour on compliance with the
practice of SPs (100%) using a focus group.
They found that fear of contracting diseases
was a more driving force towards
compliance than attitude towards safety. On
the other hand, Jawaid et al. (2009) found
that 34% of the doctors in their study often
judged the severity as a basis for strict
adherence to safety precautions; which is
indicative of a significant influence of
attitude on practice levels.
The third hypothesis which stated that age,
years of experience and marital status will
have significant joint and independent
influence on practice of standard precautions
among health care workers in the university
college hospital Ibadan was partially
accepted due to the significant influence of
work experience on standard precautions
practice. In justifying the results obtained, it
may be emphasized that medical health
workers who have more years of experience
on the job are more likely to have garnered
an accumulation of first-hand experiences or
cases that reinforce the need to adhere
strictly to all standard precautions.
Moreover, having more years of experience
on the job presents health care workers with
more opportunities for additional on-the-job
training on standard precautions and safety
measures in medical practice.
Corroborating results obtained in this study,
another study done in Ethiopia showed that,
nurses with less experience were at a higher
risk of exposure to infectious diseases and
had weak universal precautions practice
(Reda, Vandeweerd, Syre & Egata, 2009).
Similarly, Luo et al., (2010) found that
longer duration of professional experience
has been shown to be associated with
improved compliance with standard
precautions among health workers.
Abdulraheem et al. (2012) also found that
healthcare workers with ten years and above
working experience had a high level of
awareness of universal precautions than
those with below five years. Furthermore,
Abubakar et al. (2014), in their study of
nurses in Gombe state revealed that years of
experience has influence on practice of
standard precaution.
Recommendations: Based on the outcomes
of this study, health organisations must
educate their staff to increase the level of
awareness toward standard precautions, and
increase the quality of patient care.
Moreover, if the awareness of HCWs is
improved, it will hopefully reduce the
existing negative attitude toward the
implementation of standard precautions, as
the level of knowledge and compliance to
standard precautions are reciprocally related.
Looking to the future, organisations need to
involve employees in the establishment of
policies, and consider having a mandatory
program for HCWs with time allowed to
accomplish it effectively. Increasing HCWs’
awareness and acknowledgment of risk
factors in their work place, and the impact of
their poor practice on both themselves and
on patients is significant, and especially if
they do not follow the guidelines. This
change can be achieved through
communication, which is another important
aspect that impacts HCWs’ compliance.
Thus, having regular meetings with all
HCWs would reduce related practical issues,
and highlight positive perceptions that would
eventually increase and motivate HCWs to
follow the guidelines. Involving staff in the
policy process is also recommended, as
employee engagement is beneficial in
motivating staff to follow the guidelines.
However all of those factors depend mainly
on the organisation, as organisations have to
provide the protective tools for their
employees, and make sure the tools are
suitable, effective and fit for purpose,
furthermore they must be comfortable and
easy to use. Therefore, the responsibility

International Journal of Caring Sciences May-August 2021 Volume 14| Issue 2| Page 1246
www.internationaljournalofcaringsciences.org
rests not only on HCWs as employees, but
also on managers and leaders; part of their
duty is to keep updating and evaluating the
HCWs’ knowledge of standard precautions.
Hopefully, after applying these
recommendations, the HCWs’ compliance
and knowledge levels will be raised. This
will result in improved quality of patient
care.
References
Abdulraheem I, Amodu M, Saka M, Bolarinwa O and
Uthman M (2012). Knowledge, awareness and
compliance with standard precautions among
health workers in north eastern Nigeria. J
Community Med Health Edu. 2 (3): 1-5.
Adinma ED, Ezeama C, Adinma JIB, Asuzu MC.
(2009) Knowledge and practice of universal
precautions against blood borne pathogens
amongst house officers and nurses in tertiary
health institutions in Southeast Nigeria. Nigerian
Journal of Clinical Practice 12: 398–402.
Agaba P, Agaba E, Ocheke A, Daniyam C, Akanbi M,
and Okeke E (2012). Awareness and knowledge of
human immunodeficiency virus post exposure
prophylaxis among Nigerian Family Physicians:
Niger Med J. 53(3); 155–160
Amira C and Awobusuyi J (2014). Needle-stick injury
among health care workers in hemodialysis units
in Nigeria: a multi-center study. Int J Occup
Environ. 5:1-8.
Arinze-Onyia, S.U., Ndu, A.C., Aguwa, E.N.,
Modebe, I., & Nwamoh U.N. (2018) Knowledge
and practice of standard precautions by health-care
workers in a tertiary health institution in Enugu,
Nigeria. Nigerian journal of clinical practice 21
(2), 149-155
Bamigboye, AP, Adesanya, AT. (2006) Knowledge
and practice of UP among qualifying medical and
nursing students: A case of Obafemi Awolowo
University Teaching Hospitals Complex, Ile-Ife.
Research Journal of Medicine and Medical
Sciences, 1(3): 112–116.
Bolarinwa O, Asowande A and Akintimi C (2011).
Needle stick injury pattern among health care
workers in primary health care facilities in Ilorin,
Nigeria. Academic Research international. 1(3):
419-427.
Centre for Disease Control and Prevention (1983).
Acquired immunodeficiency syndrome (AIDS).
Precautions for health care workers and allied
professionals. MMWR Morb Mortal Wkly Rep.
32(34): 450-451.
Centre for Disease Control and Prevention (1985).
Recommendation for protection against viral
hepatitis. MMWR Morb Mortal Wkly Rep. 35(22):
313- 324.
Centre for Disease Control and Prevention (1996).
Guidelines for isolation precautions in hospitals.
(Online). Available:
https://wonder.cdc.gov/wonder/prevguid/p000041
9/p0000419.asp
Centre for Disease Control and Prevention (2011).
Infection control prevention plan, (Online).
Available:
http://www.cdc.gov/HAI/settings/outpatient/basic-
infection-control-prevention-plan-
2011/fundamental-of-infection-prevention.html.
Centre for Disease Control and Prevention (2013).
Infection control; Division of Oral health (online).
Available:
https://www.cdc.gov/oralhealth/infectioncontrol/fa
q/bloodborne_exposures.htm
Centre for Disease Control and Prevention (2013).
Occupational HIV transmission and prevention
among health care workers, (Online). Available:
www.cdc.gov/hiv/risk/other,occupational.html.
(Downloaded: 10/07/13 10:47pm).
Centre for Diseases Control and Prevention (1993).
HIV/AIDS surveillance report. Available:
www.cdc.gov/hiv/pdf/statistics_surveillance92pdf.
Chalya P, Seni J, Mushi M, Mirambo M, Jaka H,
Rambau P, Mabula J, Kapesa A, Ngallaba S,
Massinde A and Kalluvya S (2015). Needle-stick
injuries and splash exposures among health-care
workers at a tertiary care hospital in north-western
Tanzania. Tanzania Journal of Health Research.
17(2):1-15.
Cutter J, & Jordan S. (2012) Inter-professional
differences in compliance with standard
precautions in operating theatres: a multi-site,
mixed methods study. International Journal of
Nursing Studies 49: 953–968.
Efstathiou, Georgios & Papastavrou, Evridiki &
Raftopoulos, Vasilios & Merkouris, Anastasios.
(2011). Compliance of Cypriot nurses with
Standard Precautions to avoid exposure to
pathogens. Nursing & health sciences. 13. 53-9.
10.1111/j.1442-2018.2011.00576.x.
Honda M, Chompikul J, Rattanapan C, Wood G and
Klungboonkrong S (2011). Sharp’s injuries among
nurses in a Thai regional hospital. Prevalence and
risk factors. Intl J Occupationa Environmental
Med. 2(4): 215-223.
Hosoglu S, Akalin S, Sunbul M, Otkun M, Ozturk R.
(2011) Healthcare workers’ compliance with
universal precautions in Turkey. Medical
Hypotheses 77: 1079–1082.
Izegbu M, Amole O, Ajayi G. (2006) Attitudes,
perception and practice of workers in laboratories
in the two colleges of medicine and their teaching
hospitals in Lagos State, Nigeria as regards
universal precaution measures. Biomedical
Research 17: 49–54.
Kermode M, Jolley D, Langkham B, Thomas M and
Crofts N (2005). Occupational exposure to blood

International Journal of Caring Sciences May-August 2021 Volume 14| Issue 2| Page 1247
www.internationaljournalofcaringsciences.org
and risk of blood borne virus infection among
health care workers in rural North Indian settings.
Am J Infect Control. 33:34–41
Kolude OO, Owoaje ET, Omokhodion F. (2004)
Knowledge and compliance with UP among
doctors in a tertiary hospital. Proceedings of the
Annual General and Scientific meeting of the
West African College of Physicians. Ibadan
2004:27.
Luo Y, He G, Zhou J, Luo Y. (2010) Factors
impacting compliance with standard precautions in
nursing, China. International Journal of Infectious
Diseases 14: e1106–14.
National Agency for the Control of AIDS (2010).
National HIV/AIDS strategic plan 2010-2015.
(Online), Available:
http://www.nationalplanningcycles.org/sites/defau
lt/files/country_docs/Nigeria/hiv_plan_nigeria.pdf.
National Agency for the Control of AIDS (2014).
National HIV/AIDS Prevention plan 2014-2015.
(Online), Available:
http://sbccvch.naca.gov.ng/sites/default/files/Natio
nal%20HIV%20PrevPlan%202014- 2015(1).pdf
Omiepirisa Y (2012). Universal Precautions; A
review. The Nigerian Health Journal. 12(3); 66-
74.
Prüss-Üstün A, Rapiti E and Hutin Y (2005).
Estimation of the global burden of disease
attributable to contaminated sharps injuries among
health-care workers. Am. J. Ind. Med. 48:482-490
Reda, Alex & Vandeweerd, Jean-Michel & Syre, T.R.
& Egata, Gudina. (2008). HIV/AIDS and exposure
of healthcare workers to body fluids in Ethiopia:
attitudes toward universal precautions. The
Journal of hospital infection. 71. 163-9.
10.1016/j.jhin.2008.10.003.
Sadob, A & Fawole, Olufunmilayo & Sadoh, Wilson
& Oladimeji, AO & Sotiloye, O. (2006). Attitude
of health care workers to HIV/AIDS. African
journal of reproductive health. 10. 39-46.
10.2307/30032442.
United States Agency for International Development
(USAID) (2000). Universal precautions guidelines
for primary health care canters in Indonesia.
Universal Precautions and training project,
Indonesia.
Voide C, Darling K, Kenfak-Foguena A, Erard V,
Cavassini M and Lazor-Blanchet C (2012).
Underreporting of needlestick and sharps injuries
among healthcare workers in a Swiss University
Hospital. Swiss Med Wkly.142:w13523
WHO. 2016. Reducing Risk, Promoting Health Life.
World Health Report. Geneva.
