
Medical indemnity
insurance
April 2009
Medical indemnity insurance
SIXTH MONITORING REPORT
April 2009
SIXTH MONITORING REPORT
ACCC_03.09_31412

Medical indemnity insurance
Sixth monitoring report
April 2009
© Commonwealth of Australia 2009
ISBN: 978 1 921581 05 2
This work is copyright. Apart from any use permitted
by the Copyright Act 1968, no part may be
reproduced without permission of the Australian
Competition and Consumer Commission. Requests
and inquiries concerning reproduction and rights
should be addressed to the Director Publishing,
Australian Competition and Consumer Commission,
GPO Box 3131, Canberra ACT 2601.
ACCC 04/09_31412
Medical indemnity insurance report—Sixth monitoring report
iii
Contents
Abbreviations v
Glossary of terms vii
Summary xi
1 Introduction 1
1.2 Ministerial request 1
1.3 Scope of report 1
1.4 Approach to monitoring 3
1.5 Qualifications 4
1.6 Previous reports 4
1.7 Report outline 4
2 Overview of the medical indemnity industry 5
2.1 What is medical indemnity insurance? 5
2.2 Characteristics of the industry—pre 1 July 2003 7
2.3 Characteristics of the industry—post 1 July 2003 8
3 Government reforms of medical indemnity insurance 13
3.1 Medical indemnity reform by the Australian Government 13
3.2 Tort law reform 16
4 Trends in costs and premiums in medical indemnity insurance 17
4.1 Cost components of medical indemnity insurance 17
4.2 Trends in medical indemnity claims 18
4.3 Trends in other expenses 22
4.4 Trends in premiums 23
5 Actuarial justication of medical indemnity premiums 29
5.1 Qualifications 29
5.2 Assessment methodology 29
5.3 Analysis—MDO-owned insurers 32
5.4 Analysis—QBE 38
5.5 Conclusion 40
Medical indemnity insurance report—Sixth monitoring report
iv
6 Commercial justication of medical indemnity premiums 41
6.1 Qualifications 41
6.2 Assessment methodology 41
6.3 Analysis—MDO-owned insurers 43
6.4 Conclusion 56
7 Actuarial and commercial justication of medical indemnity 57
premiums within each jurisdiction
7.1 Qualifications 57
7.2 Background 57
7.3 Actuarial and commercial justification of premium 62
relativities by jurisdiction
7.4 Conclusion 64
Appendix A ACCC information request 65
Appendix B Differences with APRA reports 67
ACCC contacts 68
Medical indemnity insurance report—Sixth monitoring report
v
Abbreviations
ABS Australian Bureau of Statistics
ACCC Australian Competition and Consumer Commission
AIL Avant Insurance Limited
AMIL Australasian Medical Insurance Limited
APRA Australian Prudential Regulation Authority
ASIC Australian Securities and Investment Commission
Avant Avant Mutual Group Limited
AWE average weekly earnings
ECS exceptional claims scheme
GP general practitioner
GST goods and services tax
HCCS high cost claims scheme
HIC Health Insurance Commission
IAAust Institute of Actuaries Australia
Invivo Invivo Medical Pty Ltd
MCR minimum capital requirement
MDAN MDA National Pty Ltd
MDANI MDA National Insurance Pty Ltd
MDASA Medical Defence Association of South Australia Limited
MDAV Medical Defence Association of Victoria Limited
MDAWA Medical Defence Association of Western Australia
MDO medical defence organisation
MIA Medical Insurance Australia Pty Ltd
MIGA Medical Insurance Group Australia
MIPS Medical Indemnity Protection Society Limited
MIPSI MIPS Insurance Pty Ltd
MPSTas Medical Protection Society of Tasmania
MISS medical indemnity subsidy scheme
PIICA Professional Indemnity Insurance Company Australia Pty Limited
PSS premium support scheme
QBE QBE Insurance (Australia) Limited
QDM Queensland Doctors’ Mutual Pty Ltd
ROCS run-off cover scheme
UMP United Medical Protection Limited (as referred to in legislation)
United United Medical Protection Limited
Medical indemnity insurance report—Sixth monitoring report
vii
Glossary of terms
attachment point The level of claims payments above which reinsurance recoveries can
be claimed by the insurer.
claims expense All payments made in the year on claims arising from that and previous
notification years, as well as any adjustments to outstanding claims provisions
across the year.
claims-incurred cover This occurs when the insurer agrees to indemnify the policyholder for any valid
claims arising from incidents that occur during the coverage period, with a
claim able to be lodged at any time in the future.
claims-made cover This occurs when the insurer agrees to indemnify all claims arising from
incidents notified during the policy period, as long as the incident occurred
during the current period or any previous periods in which the policyholder
has held continuous claims-made cover with the insurer up to and including
the current period or to an earlier retroactive date. Because of the more
limited period the insurer is ‘on risk’, especially in early years. This type of
cover is typically cheaper to underwrite than claims-incurred cover.
claims frequency The ultimate number of claims expected by year of notification expressed
as a proportion of the total number of Medicare services provided in the
corresponding year.
combined ratio The sum of the loss ratio and the expense ratio showing whether the sum
of expenses (claims expenses and other expenses) is lower or higher than
premium revenue for the year.
excess of loss reinsurance When the direct insurer carries all individual losses incurred in each individual
claim up to a certain limit and the reinsurer pays the loss in excess of this
amount (known as the attachment point) for each and every claim. There may
also be an aggregate limit for all claims assumed by the reinsurer.
expense ratio The sum of all underwriting and general expenses (excluding reinsurance
expenses) as a proportion of premium revenue for the year.
incident An incident resulting in a personal injury or death that may develop into a
claim against the medical practitioner.
incurred but not Claims arising from incidents or losses that have occurred but are yet to be
reported claims reported to the insurer.
indemnified members The number of members are ‘at risk’—that is, members for whom the medical
indemnity provider may be required to pay a claim (the measure excludes
those non-indemnified members such as students and the employer-
indemnified).
long-tail class A class of insurance in which there may be a delay of many years before a
claim is reported and/or paid.
loss ratio The total claims expense in a year as a proportion of premium revenue
for that year.
Medical indemnity insurance report—Sixth monitoring report
viii
minimum capital The amount of capital that the Australian Prudential Regulation Authority
requirement requires insurers to hold as a buffer to absorb unusual or extreme shocks.
The minimum capital requirement is commensurate with an insurer’s risk
profile, but subject to a minimum of $5 million.
medical defence A not-for-profit mutual organisation created and owned by medical
organisation practitioners to provide various services, including indemnity, to members
(indemnity was only able to be offered by medical defence organisations
before 1 July 2003).
medical indemnity provider An organisation that provides liability insurance, either as an insurer or as an
authorised representative of an insurer that indemnifies medical practitioners
for financial loss arising from actions brought against them as a result of the
performance of their professional duties.
notification year The year in which the insurer is notified of a claim or an incident that may
potentially give rise to a claim.
personal injury or A claim relating to an incident that results in injury to or the death of a third
death claim party individual.
premium revenue The amount of gross written premium ‘earned’ during the period, earned
being the proportion of risk covered.
pure risk premium The amount of premium needed just to meet the cost of expected medical
indemnity claims and associated costs.
reinsurance The contract/agreement by which an insurer cedes some of its premium in
exchange for the reinsurer accepting some of the risks underwritten by that
premium. Simply put, this is insurance for an insurer.
reinsurance ratio The reinsurance expense as a proportion of premium revenue for that year.
retroactive cover Cover purchased to extend the period of incidents for which notifications are
covered. This type of cover is purchased from the medical indemnity provider
to which the medical practitioner is moving, enabling them to notify their new
provider of claims that relate to incidents that occurred before joining that
provider. Typically, this cover applies to claims-made cover.
return on net assets The emerging surplus net of tax as a percentage of the total net assets held
over the period.
run-off cover Cover purchased to extend the period for notifying an insurer of a potential
claim. This type of cover is purchased from the medical indemnity provider
from which the medical practitioner is leaving. This type of cover typically
applies to claims-made cover.
stop loss reinsurance The reinsurer is obliged to cover any part of the total annual loss burden
that exceeds an aggregate retention, where the retention is defined as a
percentage of annual premiums or a fixed sum.
ultimate claims costs All the claims costs that the insurer expects will eventually be paid for claims
arising in a given notification year.
Medical indemnity insurance report—Sixth monitoring report
ix
ultimate number of claims The total number of notifications the insurers expect will eventually become
claims and be paid.
underwriting performance A measure of the performance of the underwriting activities of an insurer,
comparing the claims expense and operating expenses of running
an insurance operation against the premiums charged to support the
insurance operation.
underwriting year The year in which an insurance policy was issued.
Medical indemnity insurance report—Sixth monitoring report
xi
Summary
Background
Medical indemnity insurance is a form of liability insurance that indemnifies medical practitioners
for financial loss arising from actions brought against them as a result of the performance of their
professional duties. Claims against medical practitioners relate to personal injury and death, and
are lodged against a medical practitioner as a result of a breach, or perceived breach, of a given
standard of care in the treatment of a patient.
Before 1 July 2003 medical indemnity protection was typically offered by medical defence
organisations that operated on a not-for-profit basis as ‘mutuals’ that were owned and operated
by members. Indemnity was offered on a discretionary basis because the MDO had no contractual
obligation to indemnify a medical practitioner.
In May 2002 the largest medical indemnity provider in Australia, United Medical Protection (United),
was placed into provisional liquidation, which resulted in a potential lack of indemnity cover for
many doctors. At the same time, medical practitioners were experiencing significant increases in
subscriptions charged across all medical indemnity providers.
The Australian Government responded to these concerns by introducing a framework of reforms
aimed at ensuring a viable and ongoing medical indemnity insurance market. The reform package
included a variety of measures, including premium subsidies, government assistance to medical
indemnity providers and medical practitioners for high-cost claims, and placing the industry within
a new regulatory framework. This meant that medical indemnity cover needed to be provided as an
insurance contract, which was only able to be provided by a licensed insurer.
ACCC’s monitoring role
In October 2002 the Australian Government announced that the Australian Competition and
Consumer Commission would monitor medical indemnity premiums on an annual basis to
assess whether they were actuarially and commercially justified. On 16 March 2005 the Australian
Government asked the ACCC to extend its monitoring to examine, to the extent possible,
the actuarial and commercial justification of premiums within each jurisdiction in more detail.
On 29 May 2006 the Australian Government asked the ACCC to continue to examine the
actuarial and commercial justification of medical indemnity premiums, including within jurisdictions,
for a further three years. The ACCC was also requested to extend its monitoring to include the
new entrant to medical indemnity insurance, Invivo, a corporate authorised representative of
QBE Insurance (Australia) Limited.
This report is the sixth and final ACCC report requested by the Australian Government arising
from this monitoring role.
Medical indemnity insurance report—Sixth monitoring report
xii
The ACCC asked the five authorised medical indemnity insurers as at 30 June 2008 to supply a
range of quantitative and qualitative information about their premium-setting arrangements, cost
structures and the impact of a number of government reforms on their operations for the current
underwriting period.
The five medical indemnity insurers as at 30 June 2008 were:
Avant Insurance Limited (AIL)•
MDA National Insurance (MDANI)•
Medical Insurance Australia Pty Ltd (MIA)•
MIPS Insurance Pty Ltd (MIPSI)•
QBE Insurance (Australia) Limited (QBE). •
This is the first report in which the ACCC has assessed the premiums of AIL. AIL began operation on
1 July 2007 after the merger of MDO parent entities Australasian Medical Insurance Limited (AMIL)
and Professional Indemnity Insurance Company Australia Pty Ltd (PIICA).
Qualifications
The ACCC analysis is based on information supplied by each of the insurers. The ACCC has
relied on information provided by insurers rather than performing an independent verification of their
information or actuarial advice. As the MDO parent entities of insurers are no longer able to sell
insurance, the ACCC has generally not examined their operations or membership pricing.
In preparing this report, it was necessary for the ACCC to maintain the confidentiality of individual
insurers’ information. Therefore, some quantitative aspects of the ACCC analysis—particularly its
assessment of individual insurers’ information—could not be disclosed in this report.
ACCC assessment methodology
The ACCC’s methodology focused on how premiums were derived by insurers from an actuarial and
commercial perspective.
The ACCC assessment of the actuarial justification of premiums considers the technical actuarial
aspects of pricing. It examines the process adopted by insurers to derive premium rates, the
approach taken to construct those premiums, the level of detail used to support pricing assumptions
and the breadth of issues taken into consideration (such as medical indemnity and tort law reforms).
The ACCC assessment of the commercial justification of premiums considers the ability of insurers
to meet their commercial obligations to key stakeholders. It assesses how premium rates were
affected by the Australian Prudential Regulation Authority’s minimum capital requirements that
insurers must have achieved to reach a fully capitalised position by 30 June 2008. The ACCC also
assesses broader commercial obligations, such as solvency targets and emerging surplus.

Medical indemnity insurance report—Sixth monitoring report
xiii
This report also provides information on the actuarial and commercial justification of premium
relativities between jurisdictions. The ACCC’s assessment of these premium relativities examines the
extent and the level of detail of the analysis to confirm or modify existing relativities, and the extent to
which insurers took into account tort law reform in setting their jurisdictional relativities. The ACCC’s
assessment of the commercial justification of premium relativities between jurisdictions compares
the actuary’s recommended relativities against the actual relativities adopted. It also examines the
quantification of cross-subsidies in the relativities.
QBE/Invivo
Following a request from the Australian Government in 2006, the ACCC began monitoring the
activities of Invivo, then a new entrant in the medical indemnity insurance market. Invivo acts as a
corporate authorised representative of QBE Insurance (Australia) Limited, which also owns half
of Invivo. Invivo has exclusive arrangements with QBE to distribute and manage professional
indemnity insurance covering medical practitioners. As an Australian Prudential Regulation
Authority-regulated insurer, QBE is, however, ultimately responsible for providing insurance cover
and services to its policyholders.
ACCC monitoring of the actuarial and commercial justification of premiums is undertaken
by assessing decisions made by medical indemnity insurers (rather than their authorised
representatives) on the setting of premiums. As indicated in the fifth medical indemnity insurance
monitoring report
1
, in monitoring Invivo the ACCC will have to consider decisions made by QBE
when setting premiums for medical indemnity insurance. In this report ‘QBE premiums’
2
refers
to premiums paid to Invivo for a QBE professional indemnity policy. Invivo, as the authorised
representative of QBE, provided information to the ACCC on QBE premiums.
Assessment of the actuarial justification of medical
indemnity premiums
The ACCC found that premiums were considered to be actuarially justified for all five insurers
operating as at 30 June 2008.
The ACCC found that the aggregate premium pool of each insurer was actuarially justified. It was
evident that insurers had made use of actuaries in premium liability assessments, pricing reports,
funding plans and financial forecasts. In each case the ACCC considered that the construction of
the recommended premium pool was soundly based and incorporated all major cost implications
for the pricing of medical indemnity insurance. All insurers determined their aggregate premium
pool having considered advice from their actuaries. However, different insurers involved actuaries at
different points in the pricing process.
1 ACCC, Medical indemnity insurance: Fifth monitoring report, April 2008; available on the ACCC website (www.accc.gov.au).
2 Unlike other medical indemnity insurers, QBE does not have a common renewal date and premiums are based on its latest
premium review. QBE’s premiums in this report are based on premiums set in 2007 for the 2008 calendar year.
Medical indemnity insurance report—Sixth monitoring report
xiv
The ACCC analysis of specialty premium rates found that most insurers conducted detailed analysis
of risk relativities between specialties or relied on previous risk relativity analysis. As in previous
monitoring reports, the ACCC found that insurers generally cited the unwinding of existing cross-
subsidisation between specialties as an objective. The ACCC noted that this was a long-term
process and that potentially not all cross-subsidies would be removed for a variety of reasons,
including commercial factors as well as data limitations. However, the ACCC still found these
rates and the relativities for income bands to be actuarially justified because the extent of cross-
subsidisation was understood and, where possible, quantified.
The ACCC analysis of the impact of government reforms on premiums includes an examination
of Australian Government medical indemnity reports (including the high cost claims scheme and
the run-off cover scheme), and federal, state and territory tort law reforms. The ACCC found that
all insurers appropriately considered HCCS and ROCS in their premium determinations and most
insurers took full account of HCCS in their reinsurance programs. One insurer that did not reflect
HCCS in its reinsurance program did so because of an unwillingness of reinsurers to fully reflect
the full benefits of the scheme in their reinsurance pricing and structure. However, this insurer took
HCCS recoveries into account when establishing their pure risk premium. All insurers took tort law
reform into account when setting their aggregate premium pools for 2008–09.
QBE/Invivo
The ACCC also conducted separate analysis on QBE’s 2008 premiums and found them to be
actuarially justified. In its analysis, the ACCC recognised that 2008 was only QBE’s third year of
underwriting medical indemnity insurance, so it had limited claims experience available. The ACCC’s
assessment included revisiting the original methodology used to set premiums, which compared
scheduled premium rates with the actuary’s recommended premium rates. It also involved assessing
the impact of specific government reforms on premiums and changes in rates based on emerging
experience and other identified issues.
Assessment of the commercial justification of medical
indemnity premiums
The ACCC found that the premiums set by medical indemnity insurers were commercially justified.
MDO-owned insurers
The net asset position of all insurers as at 30 June 2008 had improved upon their strong position as
at 30 June 2007. However, the degree to which the net asset position had improved depended on
the circumstances of individual insurers.
The ACCC notes that one insurer has scheduled future capital injections to maintain its target net
asset-to-minimum capital requirement ratio. Based on forecasts provided by the insurer, the ACCC
found that this approach is currently commercially justified.
Medical indemnity insurance report—Sixth monitoring report
xv
QBE/Invivo
The ACCC examined the commercial justification of QBE’s premiums by examining Invivo’s
financial projections and how these are consolidated within QBE’s professional indemnity insurance
business. The ACCC also examined QBE’s objectives and intentions for its medical indemnity
insurance business.
Based on this analysis, the ACCC found that QBE premiums for the 2008 underwriting year were
commercially justified.
Assessment of the actuarial and commercial justification
of medical indemnity premiums within each jurisdiction
The ACCC found that jurisdictional premium relativities were considered to be actuarially and
commercially justified for the five insurers operating as at 30 June 2008.
For the actuarial justification of premium relativities, the ACCC considered the extent of the
analysis used to determine the relativities, as well as the extent to which insurers took into account
jurisdictional variations in tort law reform. The ACCC found those insurers’ analyses continues to
be limited because of the absence of a sufficient volume of claims experience in some jurisdictions.
In the absence of this data the ACCC considered the approach used by insurers to be actuarially
justified. The lack of sufficient claims experience by jurisdiction also affected the ability of insurers to
take into account tort law reform in premium relativities.
For the commercial justification of premium relativities, the ACCC considered the extent to
which relativities recommended by actuaries were adopted in final premium rates as well as the
level of cross-subsidisation in the premium relativities. The ACCC found that in some instances
recommendations were not adopted in final premium rates because of a lack of a sufficient volume
of claims experience in some jurisdictions. The ACCC also noted that one insurer had made a
commercial decision not to change jurisdictional relativities and relied on previously undertaken
relativity analysis when setting premiums for the 2007–08 underwriting year. Consistent with previous
reports, the ACCC found that while no insurer explicitly cross-subsidised between jurisdictions,
cross-subsidies may exist because of the lack of sufficient claims experience data. The relativities
adopted were considered commercially justified.

Medical indemnity insurance report—Sixth monitoring report
xvi
Findings of previous ACCC medical indemnity insurance
monitoring reports
The ACCC’s first five medical indemnity insurance monitoring reports examined the actuarial and
commercial justification of premiums for the 2003–04, 2004–05, 2005–06, 2006–07 and 2007–08
underwriting periods.
3,4
The ACCC’s third, fourth and fifth monitoring reports also examined the
actuarial and commercial justification of premium relativities between jurisdictions for the 2005–06,
2006–07 and 2007–08 underwriting periods.
The ACCC found that the premiums levied were generally actuarially justified. In one instance, the
ACCC could not determine the actuarial justification of premiums for an insurer in the 2003–04
underwriting period. However, the premiums for this insurer were found to be justified in subsequent
periods. In addition, issues identified by the ACCC in its reports regarding the determination of the
premium pool for some insurers were generally addressed in subsequent underwriting periods.
The ACCC found that the premiums levied were commercially justified. The ACCC observed
that the insurers’ capital levels had significantly improved since 2003–04, attributable to the
transitional capital requirements set by the Australian Prudential Regulation Authority. At the end
of the transitional period for the insurers (30 June 2008), all insurers had exceeded APRA’s target
capital requirements.
Finally, the ACCC found that the jurisdictional relativities of premiums to be actuarially and
commercially justified. The ACCC has found that the insurers, to the extent possible, have attempted
to reduce cross-subsidies between jurisdictions.
Overall, the ACCC observed a significant change in the medical indemnity industry following
the government reforms. The medical indemnity industry had made a transition from providing
discretionary medical indemnity cover through MDOs to providing non-discretionary medical
indemnity insurance contracts through insurance companies regulated by APRA. The insurers are
currently in a much stronger capital position when compared to when they were established, moving
away from an objective of raising capital to maintaining capital. The medical indemnity insurers also
now actively use actuaries in the premium rating process. As outlined in this report, the ACCC has
observed decreases in real premiums as well as improvements in claims experience over the period
2003–04 to 2007–08.
The ACCC considers that the continual and active involvement of actuaries in the premium-setting
process would contribute to the actuarial and commercial justification of premiums over time.
3 The ACCC’s first monitoring report was released by the Australian Government on 23 February 2004, the second on
16 March 2005, the third on 16 February 2006, the fourth on 12 April 2007 and the fifth on 2 May 2008.
4 QBE and the former AMIL determined premiums on a calendar year basis.

Medical indemnity insurance report—Sixth monitoring report
1
1 Introduction
In May 2002 the largest medical indemnity provider in Australia, United Medical Protection (United),
was placed into provisional liquidation, which resulted in a potential lack of indemnity cover for
many doctors. At the same time, medical practitioners were experiencing significant increases
in subscriptions charged across all medical indemnity providers. In extreme cases, medical
practitioners were paying over a third of their incomes for indemnity cover, while others left the
profession or ceased high-risk procedures like obstetrics. In response to this crisis, the Australian
Government introduced a framework of reforms to ensure a viable and ongoing medical indemnity
insurance market.
The reform package included a variety of measures including premium subsidies, government
assistance to medical indemnity providers and medical practitioners for high-cost claims and placing
the industry within a new regulatory framework. The government’s reform measures are outlined in
more detail in chapter 3.
As part of the reform framework, the Australian Government announced that the Australian
Competition and Consumer Commission would monitor medical indemnity premiums to assess
whether they are actuarially and commercially justified. This report is the ACCC’s sixth and final
ACCC report requested by the Australian Government arising from this monitoring role.
1.2 Ministerial request
On 19 November 2002 the then Treasurer, the Hon. Peter Costello MP, wrote to the ACCC about
this new role and indicated that the ACCC’s monitoring role was to start on 1 January 2003 for three
years and was not a direction under the Prices Surveillance Act 1983.
5
On 29 May 2006 the then Minister for Revenue and Assistant Treasurer, the Hon. Peter Dutton MP,
wrote to the ACCC requesting that it continue examining the actuarial and commercial justification of
medical indemnity premiums, including within jurisdictions, for a further three years. The ACCC was
also requested to extend its monitoring to include the new entrant to medical indemnity insurance,
Invivo, a corporate authorised representative of QBE Insurance (Australia) Limited.
1.3 Scope of report
The ACCC’s monitoring role is limited to medical indemnity insurance written in Australia by insurers
that indemnify medical practitioners (i.e. doctors) working in the private health sector. As at 30 June
2008 there were five medical indemnity insurers:
Avant Insurance Limited (AIL)•
MDA National Insurance Pty Ltd (MDANI)•
5 The Prices Surveillance Act 1983 was repealed on 1 March 2004 when its main provisions were incorporated into Part VIIA
of the Trade Practices Act 1974. Division 5 of Part VIIA of the TPA provides for the minister to direct the ACCC to monitor
prices, costs and profits of a business or industry.

Medical indemnity insurance report—Sixth monitoring report
2
Medical Insurance Australia Pty Ltd (MIA)•
MIPS Insurance Pty Ltd (MIPSI)•
QBE Insurance (Australia) Limited (QBE). •
Medical indemnity insurance is also offered by some other commercial insurers to medical
professionals practising in the private health sector, such as hospital and ancillary staff (including
nurses and other medical staff). Medical practitioners who practise in the Australian public health
sector are generally indemnified against medical malpractice by the relevant state-based public
sector insurer for the work they perform in the public health system.
6
Unless medical practitioners
are not covered for certain procedures, they generally do not need to take out their own private
medical indemnity insurance to cover this work.
Avant Insurance
AIL began operation as a medical indemnity insurer on 1 July 2007 following the merger of the
medical defence organisation (MDO) parent entities of Australasian Medical Insurance Limited (AMIL)
and Professional Indemnity Insurance Company Australia Pty Ltd (PIICA).
In last year’s report, the ACCC assessed the actuarial and commercial justification, including within
jurisdictions, of premiums set by both AMIL and PIICA before the merger. This is the first year that
the ACCC has assessed the actuarial and commercial justification of the premiums of the merged
entity, AIL.
QBE/Invivo
Invivo, established in late 2005, is a corporate authorised representative of QBE, which also owns
half of Invivo. Invivo has exclusive arrangements with QBE to distribute and manage professional
indemnity insurance covering medical practitioners. QBE as an Australian Prudential Regulation
Authority-regulated insurer is, however, ultimately responsible for providing insurance cover and
services to policyholders.
The ACCC’s monitoring of the actuarial and commercial justification of premiums is being
undertaken by assessing decisions made by medical indemnity insurers (rather than their authorised
representatives) on the setting of premiums. The monitoring of Invivo by the ACCC, therefore,
necessitates consideration of the decisions made by QBE in setting premiums for medical
indemnity insurance.
In this report ‘QBE premiums’
7
refer to premiums paid to Invivo for a QBE professional indemnity
policy. Invivo, as the authorised representative of QBE, provided information to the ACCC on
QBE premiums.
6 Parliament of the Commonwealth of Australia, Medical Indemnity (Prudential Supervision and Product Standards) Bill 2002,
revised explanatory memorandum, p. 6.
7 Unlike other medical indemnity insurers QBE does not have a common renewal date and premiums are based on its latest
premium review. The premiums in this report are based on premiums set in 2007 for the 2008 calendar year.

Medical indemnity insurance report—Sixth monitoring report
3
1.4 Approach to monitoring
In assessing the actuarial justification of premiums, the ACCC considers the technical actuarial
aspects of pricing. It examines the process adopted by insurers to derive premium rates, the
approach taken to construct those premiums, the level of detail used to support pricing assumptions
and the breadth of issues taken into consideration. The ACCC’s assessment framework is discussed
further in chapter 5.
In assessing the commercial justification of premiums, the ACCC considers the ability of insurers to
meet their commercial obligations to key stakeholders. It assesses how premium rates were affected
by the Australian Prudential Regulation Authority’s minimum capital regulatory requirement that the
MDO-owned insurers must achieve to reach a fully capitalised position by 30 June 2008, as well as
broader commercial obligations such as solvency targets and emerging surplus levels. The ACCC’s
assessment framework is discussed further in chapter 6.
This report also provides information on the actuarial and commercial justification of premium
relativities between jurisdictions. To assess these premium relativities the ACCC examines the
extent and the level of detail of the analysis to confirm or modify existing relativities. It also looks
at the extent to which insurers took into account jurisdictional variations in tort law reform when
setting their jurisdictional relativities. In assessing the commercial justification of premium relativities
between jurisdictions, the ACCC compares the actuary’s recommended relativities against the actual
relativities adopted and examines the quantification of cross-subsidies (as well as the incorporation
of board policy) in the relativities.
The ACCC’s analysis covered the five insurers in Australia that offered insurance to private medical
practitioners as at 30 June 2008. In June 2008 the ACCC requested a range of quantitative and
qualitative information from these insurers about their premium-setting arrangements, cost structures
and the effect of various government reforms (including tort reforms) on their operations.
8
Details of
the ACCC’s information request can be found in appendix A.
This report examines premiums set by existing insurers as at 30 June 2008 for the underwriting
period from 1 July 2008 to 30 June 2009, except for AIL and QBE, which had an underwriting
period from 1 January 2008 to 31 December 2008. The ACCC has specifically not adjusted AIL’s
calendar year results to the financial year except where otherwise noted. However, QBE’s results,
where identified in this report, are provided on a financial year basis.
The ACCC engaged actuarial consultants am actuaries to provide actuarial advice in preparing
this report.
8 Invivo, as the authorised representative of QBE, provided information to the ACCC on QBE premiums.
Medical indemnity insurance report—Sixth monitoring report
4
1.5 Qualifications
The ACCC analysis is based on information supplied by each of the insurers. The ACCC has relied
on information provided by insurers rather than performing an independent verification of their
information or actuarial advice. As the MDO parent entities of insurers are no longer able to sell
insurance, the ACCC has generally not examined their operations or membership pricing. In preparing
this report, it was necessary for the ACCC to maintain the confidentiality of individual insurers’
information. Therefore, some quantitative aspects of the ACCC analysis, particularly its assessment of
individual medical indemnity insurers’ information, could not be disclosed in this report.
1.6 Previous reports
This is the sixth and final annual ACCC monitoring report requested by the Australian Government.
The five previous reports generally found that the premiums charged by medical indemnity insurers
were actuarially and commercially justified.
The third, fourth and fifth reports also made assessments regarding the actuarial and commercial
justification of premiums within each jurisdiction. These three reports found that jurisdictional premium
relativities were actuarially and commercially justified respectively for the 2005–06, 2006–07 and
2007–08 underwriting years.
1.7 Report outline
This report contains seven chapters and two appendixes.
Chapter 2 provides a brief overview of the medical indemnity insurance industry in Australia by
examining the main features of medical indemnity insurance as well as the industry structure,
concentration and regulatory arrangements.
Chapter 3 examines Australian Government reforms to medical indemnity insurance.
Chapter 4 examines historical trends in costs, premiums and the financial performance of the industry
between 1997–98 and 2007–08.
Chapter 5 presents ACCC findings on the actuarial justification of medical indemnity premiums
charged for the 2008–09 underwriting period by the five insurers operating as at 30 June 2008.
Chapter 6 presents ACCC findings on the commercial justification of medical indemnity premiums
charged for the 2008–09 underwriting period by the five insurers operating as at 30 June 2008.
Chapter 7 presents ACCC findings on the actuarial and commercial justification of medical indemnity
premiums charged in different jurisdictions for the 2008–09 underwriting period by the five insurers
operating as at 30 June 2008.
Appendix A describes the nature of the reports and other information the ACCC requested from
medical indemnity providers.
Appendix B identifies some of the methodology differences between this report and Australian
Prudential Regulation Authority’s national claims and policies database reports.

Medical indemnity insurance report—Sixth monitoring report
5
2 Overview of the medical indemnity
industry
On 1 July 2003 Australian Government legislative reforms changed the nature of the medical
indemnity insurance product offered to medical practitioners and the environment in which the
industry operates in Australia. This chapter briefly examines the nature of the medical indemnity
product and the pre-reform and post-reform characteristics of the medical indemnity industry.
Specific information about the medical indemnity legislative reforms implemented by the Australian
Government is in chapter 3.
2.1 What is medical indemnity insurance?
Insurance provides protection against the unfortunate consequence of future events by transferring
the risk of possible loss from a person or organisation (the insured) to the insurer. To gain this benefit,
the insured pays the insurer a sum of money, known as a premium, for the cost of insurance.
9
2.1.1 Liability insurance
Medical indemnity insurance is a form of liability insurance. Liability insurance is when an insurer
undertakes to indemnify the insured for losses incurred as a result of the insured becoming liable for
a breach of duty imposed by common law, contract or legislation.
Depending on the type of duty, compensation may be based on the common law principles of tort.
A tort is a wrong involving a breach of duty, such as the duty of care under the law of negligence, but
does not include a criminal wrong. Tort law aims to restore the person who suffered from the breach
of duty to the position they were in before the tort was committed—known as ‘restitution’. Therefore,
if a tort is found to be committed on one party by another party—referred to as the ‘tortfeasor’—the
tortfeasor is considered to be liable and is required to make restitution for damage suffered.
A number of different types of liability insurance exist—for example, workers compensation, motor
vehicle compulsory third party, public liability and professional indemnity. Liability insurance differs
from first party insurance, as the latter covers an insured party’s direct risks. Liability insurance covers
the risks that third parties are exposed to because of the actions of the insured.
Medical indemnity insurance is a type of professional indemnity insurance. Professional indemnity
insurance indemnifies professional people for their legal liability to their clients and others relying
on their advice and/or services.
10
With medical indemnity insurance, the professional being insured
is the medical practitioner—indemnity coverage reduces their exposure to financial losses
arising from personal injury actions brought against them as a result of the performance of their
professional duties.
9 Insurance Council of Australia, background paper no. 7 to the HIH Royal Commission, ‘A profile of the general insurance
industry’, November 2001, p. 3.
10 ibid, p. 26.

Medical indemnity insurance report—Sixth monitoring report
6
2.1.2 Medical malpractice
Malpractice insurance is another name for professional indemnity insurance, but this term has
generally been reserved for the medical professions.
11
Although medical indemnity insurance
provides protection similar to that for other professionals, the nature of medical malpractice claims
against medical practitioners will generally differ from claims against other professionals.
For example, accountants, lawyers, investment advisers and valuers are usually sued for ‘economic
loss’—that is, loss of past and/or future income resulting from advice provided. Claims against
architects and engineers are often for some physical damage leading to economic loss. They may
also involve personal injury.
Claims against medical practitioners relate to personal injury or death, and are lodged against a
medical practitioner for a breach, or perceived breach, of a given standard of care in the treatment of
a patient. This may lead to the injured party seeking compensation from the insured for general pain
and suffering, past economic loss, future economic loss, medical costs, attendant care costs and
legal costs.
These types of compensation are typically referred to as ‘heads of damage’ and are similar to claims
arising in public liability insurance in which personal injury claims represent a major portion of overall
claims costs.
2.1.3 Long-tail insurance
As with other types of liability insurance, medical indemnity insurance is often referred to as ‘long-
tail’ insurance. This means that many years may pass between the period for which cover was
provided and the date when claims are finally settled. This contrasts with most claims for damage
to motor vehicles or homes, which tend to be made in the year in which cover is provided, with final
settlement usually occurring soon after the claim is lodged.
Depending on the statute of limitations, which varies between each state and territory, medical
indemnity claims can be made years after an incident, even if the medical practitioner is no longer
practising medicine. Although tort law reforms have reduced limitation periods, this long-tail
characteristic continues to place considerable pressure on providers of such cover to be able to
identify the likely cost of future claims and build this into their pricing (premium) structures.
12
2.1.4 Types of indemnity coverage
Traditionally medical indemnity cover was provided to medical practitioners on a claims-incurred
(sometimes referred to as ‘incidents-occurring’) basis. Claims-incurred cover provides indemnity
for valid claims arising from incidents that occur during the period of cover, with a claim able to
be lodged at any time in the future.
13
Under this type of protection, the medical practitioner is
indemnified for claims arising from incidents that occurred during the period of cover, even if the
11 Insurance Council of Australia, submission to ministerial forum, Addressing the issues in professional indemnity insurance,
March 2002, p. 1.
12 Revised explanatory memorandum, Medical Indemnity (Prudential Supervision and Product Standards) Bill 2002, p. 8.
13 ibid.

Medical indemnity insurance report—Sixth monitoring report
7
claim is lodged with the insurer after the practitioner ceases to practise (because of retirement,
disablement or death) or has moved to another indemnity provider.
Since 1997 several medical indemnity providers have offered claims-made cover, in some cases
exclusively. Claims-made cover allows a medical practitioner to notify the insurer of a claim within
the terms of the current cover, for an incident that occurred within a recognised period.
14
Claims-
made cover is standard within the broader general insurance industry for professional indemnity
insurance contracts.
Claims-made cover is different to claims-incurred cover because, for the former, the incident must
have occurred and the claim must have been notified to the indemnity provider during the period of
coverage. This means that, for claims-made cover, the medical practitioner is not covered for past
incidents notified to the indemnity provider after the practitioner ceases practising medicine or moves
to another indemnity provider.
15
2.2 Characteristics of the industry—pre 1 July 2003
Before 1 July 2003 medical indemnity cover was traditionally offered by medical defence
organisations, which operated on a not-for-profit basis as ‘mutuals’ (i.e. owned and operated
by its members). Medical defence organisations (MDOs) offered indemnity protection to medical
practitioners as part of a range of services to their members.
16
Indemnity cover provided by MDOs was discretionary in that the medical practitioner had no
contractual right to be indemnified by the MDO. Rather, the MDO retained the discretion to decide
whether to provide indemnity to the medical practitioner. In practice, however, it was rare for an MDO
not to provide indemnity, except for cases of fraud, criminal activity, sexual misconduct or drug abuse.
At 30 June 2003 seven MDOs provided indemnity protection in Australia:
Medical Defence Association of South Australia Limited (MDASA)•
Medical Defence Association of Victoria Limited (MDAV)•
MDA National Pty Ltd (MDAN)•
17
Medical Indemnity Protection Society Limited (MIPS)•
Medical Protection Society of Tasmania (MPSTas)•
Queensland Doctors Mutual Pty Ltd (QDM)•
18
United Medical Protection Limited (United).•
14 Before 1 July 2003 this ‘recognised’ period related to the medical practitioner’s annual membership with the insurer.
After 1 July 2003 the recognised period relates to the policy period specified in the insurance contract issued by the medical
indemnity insurer to the medical practitioner.
15 Where a medical practitioner is indemnified on a claims-made basis, this may necessitate the purchase of what is known as
run-off or retroactive cover. Run-off cover provides the medical practitioner with indemnity coverage for claims notified to the
insurer after the end of the recognised period for incidents occurring during that period. Retroactive cover allows the insured
to notify the insurer of an incident that occurred before the current period of cover.
16 These services included legal advice for non-indemnity related situations, advice about medical practices and representations
at medical board matters, disciplinary proceedings and coronial inquests.
17 MDAN was previously known as the Medical Defence Association of Western Australia (MDAWA).
18 QDM subsequently merged with MIPS on 22 July 2004.

Medical indemnity insurance report—Sixth monitoring report
8
The above MDOs operated mainly along state lines
19
and were outside the prudential framework
regulated by the Australian Prudential Regulation Authority. Although MDOs were not insurance
companies authorised by APRA to conduct insurance business, they did have some associations
with authorised insurers. Before 1 July 2003 all MDOs operating in Australia had access to
subsidiary or ‘captive’ insurance companies, established primarily to provide reinsurance cover to
the parent MDO.
2.3 Characteristics of the industry—post 1 July 2003
These arrangements changed on 1 July 2003 when the government implemented a legislative
requirement that medical indemnity cover be provided as an insurance contract between the
medical practitioner and an insurer authorised by APRA to conduct insurance business. This meant
that MDOs were no longer able to provide indemnity protection and coverage could no longer be
discretionary. Therefore, the MDOs applied to APRA to make their captive insurers authorised to
conduct insurance business.
As at 30 June 2008, the five authorised providers of medical indemnity insurance in Australia were:
Avant Insurance Limited (AIL)—writing insurance for members of Avant Mutual Group Limited •
(Avant), which consists of members of the former United and MDAV
MIPS Insurance Limited (MIPSI)—writing insurance for members of MIPS and MPSTas (and •
previously to QDM before it merged with MIPS)
MDANI—writing insurance for members of MDAN•
Medical Insurance Australia Pty Ltd (MIA)—writing insurance for members of MDASA•
Invivo Medical Pty Ltd/QBE Insurance (Australia) Limited (QBE).•
Avant commenced operation on 1 July 2007 following the merger of United and MDAV, the parent
MDOs of Australasian Medical Insurance Limited (AMIL) and Professional Indemnity Insurance
Company Australia Pty Ltd (PIICA).
From 1 July 2007 Avant became the holding company of United, MDAV, Avant Insurance Limited
(AIL, formerly AMIL) and PIICA. From 1 October 2007 PIICA ceased to offer insurance policies and
PIICA’s insurance portfolio (i.e. its assets and liabilities relating to insurance) was transferred to AIL.
19 The first monitoring report found the following MDOs had the largest market shares in each state and territory:
• New South Wales/Australian Capital Territory—United
• Victoria—MDAV
• Queensland—United
• SouthAustralia—MDASA
• WesternAustralia—MDAN
• Tasmania—MPSTas
• NorthernTerritory—United.
However, MDOs generally had a presence in jurisdictions outside their home states.
Medical indemnity insurance report—Sixth monitoring report
9
2.3.1 Market shares
The number of indemnified members that belong to each medical indemnity provider is one
measure that can be used to determine the distribution of market shares within the industry.
Only indemnified Australian medical practitioners are included in the analysis. Total membership of
medical indemnity providers will typically be higher because of the inclusion of members who are
not medical practitioners but are health professionals (such as optometrists and dentists), or for
whom medical indemnity providers are not required to meet claims—that is, students and those
indemnified by employers.
In preparing this analysis the ACCC relied on information provided by each medical indemnity
provider. Although data on membership numbers provided by different medical indemnity providers
may not be comparable in some instances because of underlying data collection methodologies, it
nevertheless provides an indication of the general market shares of all industry participants.

Medical indemnity insurance report—Sixth monitoring report
10
Chart 2.1 shows the percentage of the total number of indemnified
20
members in Australia with each
medical indemnity provider based on the most recently available data provided for the six financial
years from 2002–03
21,22
to 2007–08.
23,24
Chart 2.1 Medical indemnity provider indemnity members, 2002–03 to 2007–08
25,26
Source: Derived from MDO-owned insurers by the ACCC.
After the merger of AMIL and PIICA, the largest medical indemnity provider is AIL, which had
approximately 52 per cent of all indemnified members in Australia in 2007–08. PIICA’s and AMIL’s
combined share of indemnified members declined during the period from 2002–03 to 2006–07,
while MIPSI’s, MDANI’s and MIA’s share of indemnified members increased.
20 Where possible, the ACCC has excluded membership numbers that relate to non-indemnified members such as students or
practitioners who are employer-indemnified.
21 Market shares for 2002–03 are based on indemnity membership of the relevant MDO. In the case of MIPSI, this incorporates
the membership of MIPS, MPSTas and QDM.
22 AIL membership numbers relate to the previous calendar year and financial year, depending on the member’s renewal
date—that is, members who have either a 1 January 2007 or 1 July 2007 renewal date have been recorded as a member
of the 2007–08 financial year.
23 The ACCC has specifically excluded QBE from its analysis of market share because its policyholder numbers were provided
on the condition of confidentiality.
24 Results may not be directly comparable to those shown in previous reports because of the revised membership data and
the exclusion of some non-medical practitioners and non-indemnified members from historical data.
25 The AIL series is the sum of AMIL’s and PIICA’s indemnified members for the period from 2002–03 to 2006–07.
26 The ACCC calculates its market share using the membership figures provided by the insurers. As such, it may not be
comparable to market share calculations from other publications.
0%
10%
20%
30%
40%
50%
60%
70%
AIL MIPSI MDANI MIA
Insurers
2002–03 2003–04 2004–05 2005–06 2006–07 2007–08

Medical indemnity insurance report—Sixth monitoring report
11
2.3.2 Transitional regulatory arrangements
Since 1 July 2003 it has been a legislative requirement that medical indemnity insurance be
provided in the form of an insurance contract between an APRA authorised insurer and the medical
practitioner.
27
This means that authorised insurers are unable to offer discretionary unlimited
indemnity protection. This change extended APRA’s prudential supervision to encompass medical
indemnity insurance because it required all medical indemnity insurers to comply with APRA’s
prudential standards that apply to general insurance.
These requirements include, among other things:
compliance with APRA’s liability valuation standards, which mandates the appointment of an •
actuary who estimates the liabilities and risk margin
having risk management systems, including pricing and underwriting control mechanisms•
holding a minimum level of capital based on an assessment of identified risks (but subject to a •
minimum of $5 million)
28
regular provision of data and reports.•
APRA established a scheme for transitional arrangements for the five MDO-owned insurers whereby
providers have up to five years from 1 July 2003 to 30 June 2008 to comply with these minimum
capital requirements (MCR). From 1 July 2008 these insurers must be fully capitalised.
29
To participate in these transitional arrangements, the five insurers were required to submit a funding
plan to APRA for approval. APRA released a series of guidelines early in 2003 that specified the
content of the funding plan and the role of actuaries and auditors in constructing these plans.
As an existing general insurer QBE does not have access to transitional arrangements because it is
already expected to comply with APRA’s capital requirements.
2.3.3 Current regulatory arrangements
Since the end of the transitional arrangements effective 1 July 2008 all medical indemnity
insurers have been subject to standard general insurance prudential standards. A new APRA
guideline was introduced (effective from 1 July 2008) that suggests medical indemnity insurers
should maintain a capital base at least 1.5 times the MCR. The target for other authorised insurers
is 1.2 times the MCR.
The Insurance Act 1973 also sets out requirements for firms seeking to exit the industry, with
guidelines for assigning liabilities, transfers and amalgamations and winding up.
27 An insurance contract forms a legally binding arrangement between the policyholder and the insurer, setting out the terms
and conditions under which indemnity is to be provided.
28 An insurer’s minimum capital requirement is determined by considering a range of risk factors that may threaten the ability of
the insurer to meet policyholder obligations. These risks fall into three broad types: insurance risk (the risk that the true value
of net insurance liabilities could be greater than the value determined under the liability valuation); investment risk (the risk
of an adverse movement in the value of an insurer’s assets and/or off-balance sheet exposures); and concentration risk (the
risk associated with an accumulation of exposures to a single catastrophic event). Sourced from APRA Prudential Standard
GPS 110, available on the APRA website (www.apra.gov.au).
29 APRA, General Insurance Prudential Practice Guides; available at www.apra.gov.au/General/General-Insurance-PPGs.cfm.

The Australian Securities and Investment Commission (ASIC) has a regulatory role in medical
indemnity insurance. It is responsible for the general administration of product standards and
disclosure requirements applying to medical indemnity insurance policies, including that:
the minimum cover limit that an insurer may offer or provide to a medical practitioner is $5 million•
a contract must provide an offer for retroactive and run-off cover for otherwise uncovered •
prior incidents.
30
ASIC also has an enforcement role in medical indemnity insurance and is responsible for ensuring
that premiums for cover contained within the terms of compulsory offers are reasonable.
30 Retroactive cover provides medical practitioners joining a new medical indemnity provider with protection against incidents
incurred before joining the provider but notified after. Run-off cover provides medical practitioners leaving practice with
protection against claims arising from previous incidents.

Medical indemnity insurance report—Sixth monitoring report
13
3 Government reforms of medical
indemnity insurance
In 2002 rising medical indemnity insurance premiums and the provisional liquidation of the
largest provider, United Medical Protection Limited (United) led to significant problems of
affordability and availability of medical indemnity insurance for private medical practitioners.
In response to these problems the Australian Government introduced a series of reforms aimed
at ensuring a viable and ongoing medical indemnity insurance market. This chapter examines
those medical indemnity reforms.
3.1 Medical indemnity reform by the
Australian Government
This chapter briefly examines the reforms programs operational as at 1 July 2008 that insurers
need to take into account when considering their price setting arrangements for the 2008–09
underwriting year (discussed in more detail in chapter 5).
These reforms include the:
exceptional claims scheme (ECS)•
run-off cover scheme (ROCS)•
UMP support payment (UMP SP)•
high cost claims scheme (HCCS)•
premium support scheme (PSS).•
More detailed information on the development of the medical indemnity reform package from
its inception to its current form is contained in the fourth ACCC medical indemnity premium
monitoring report.
31
3.1.1 Exceptional claims scheme
ECS was developed to provide protection for medical practitioners against personal liability for
private practice claims that exceed their maximum level of insurance cover.
Under ECS, the government assumes liability for 100 per cent of damages payable against a
practitioner above the individual’s insurance contract limit for claims notified after 1 January 2003,
as long as the practitioner has cover equal to or over a threshold amount. The threshold is currently
set at $20 million and is subject to review. The scheme can be activated by either a single very large
claim or an aggregate of claims that together exceed the threshold.
31 ACCC, Medical indemnity insurance: fourth monitoring report, March 2007; available on the ACCC website
(www.accc.gov.au).

Medical indemnity insurance report—Sixth monitoring report
14
ECS has no sunset clause, although it can be ended by regulation. It is anticipated that the
scheme will be reviewed from time to time in close consultation with the medical profession and
insurers to determine whether it remains necessary in light of state and/or territory tort law reform
and claims trends.
32
3.1.2 Run-off cover scheme
ROCS was developed in response to concerns within the medical profession about the capacity of
doctors to pay for run-off cover when they no longer earn an income. The scheme came into effect
on 1 July 2004.
Under ROCS, medical indemnity insurers are required to provide run-off cover for eligible doctors
(generally retired doctors over 65 years and those who are no longer earning income from private
medical practice). On becoming eligible, ROCS will cover the types of claims that were covered by a
medical practitioner’s last insurance contract. The government guarantees to pay the cost of claims
under this cover.
The scheme is funded on an ongoing basis through a charge on insurers called the run-off cover
scheme support payment, which is levied as a percentage of insurers’ medical indemnity insurance
income and is shown on doctors’ premium notices. ROCS therefore ensures that eligible doctors
receive medical indemnity cover that is secure, does not require further payment and is based on
the cover they had while they were working.
33
From 1 July 2008 this charge has been reduced from 8.5 per cent to 5.0 per cent.
34
3.1.3 High cost claims scheme
The HCCS was established to address upward pressure on medical indemnity premiums by
reducing the cost of these large claims to insurers. It does so by reimbursing insurers 50 per cent of
the cost of medical indemnity claims above a threshold amount up to the limit of the practitioner’s
cover for claims notified on or after 1 January 2003.
35
3.1.4 Premium support scheme
The PSS is an Australian Government scheme that helps eligible doctors with the costs of their
medical indemnity insurance. Eligible doctors see the benefit of the PSS through reductions in the
level of premiums charged to them by their insurer.
32 Medical Indemnity Policy Review Panel, Achieving stability and premium affordability in the Australian medical indemnity
marketplace, February 2007.
33 ibid.
34 Medical Indemnity (Run-off cover support payment) Regulations 2008, explanatory statement, available at www.austlii.edu.
au/au/legis/cth/num_reg_es/micspr2008n71o2008694.html.
35 Medical Indemnity Policy Review Panel, op. cit.

Medical indemnity insurance report—Sixth monitoring report
15
The PSS was introduced to replace the medical indemnity subsidy scheme (MISS), which provided
premium subsidies specifically to neurosurgeons, obstetricians, procedural general practitioners and
general practitioner registrars undertaking procedural training.
36,37
The PSS is designed to ensure that if a doctor’s gross medical indemnity costs exceed 7.5 per cent
of their gross private medical income, they will only pay 20c to the dollar for the cost of the premium
beyond that threshold limit.
The PSS applies to the following:
medical practitioners whose gross indemnity costs exceed 7.5 per cent of estimated income •
from private billings—the subsidy is 80 per cent of the amount by which the member’s gross
indemnity cost exceeds the base amount
procedural general practitioners in a rural area•
38
medical practitioners who have applied for and been deemed eligible for MISS—the subsidy is •
calculated as the greater of that under MISS or PSS
special category members—the subsidy is 80 per cent of the total cost to the member for the •
premium period of the member’s gross indemnity costs.
39
3.1.5 UMP support payment
The UMP support payment was introduced by the Australian Government in 2002, when
United entered provisional financial liquidation. The UMP SP provides ongoing assurance for
medical professionals who were members of UMP on 30 June 2000, in the form of indemnity for
past incidents.
To provide this assurance, the government agreed to fund most of these claims, with members of
UMP funding around one-third of the arrangement over six years through the UMP SP (formerly the
incurred but not reported levy).
The final year of the UMP SP program was 2007–08.
40
36 PSS was enacted under s. 43(1) of the Medical Indemnity Act 2002, which came into operation on 17 June 2004. MISS was
contained in the medical indemnity subsidy scheme that commenced on 20 June 2003 and applied to indemnity payments
made on or after 1 January 2003 until 30 June 2004. PSS replaced MISS from 1 January 2004.
37 The Department of Health and Ageing, Premium Support Scheme – Frequently asked questions; available at www.health.
gov.au/internet/main/publishing.nsf/Content/health-medicalindemnity-faq-pss.htm.
38 Defined as rural, remote and metropolitan areas 3 to 7 by the Department of Health and Ageing. These areas are regions
that are not capital cities or regions that contain more than 100 000 people.
The Department of Health and Ageing, Bonded medical places scheme: Information booklet; available at www.health.gov.
au/internet/main/publishing.nsf/Content/work-st-bmp-info-toc~work-st-bmp-info-rrma.
39 A special category member is a member who:
no longer practises as a doctor, or•
no longer derives a private medical income from practising as a doctor, or•
practises as a doctor only in the public sector and has a insurance contract providing indemnity cover that does not offer •
indemnity for damages awarded against a doctor (except arising from Good Samaritan acts or gratuitous advice for which
no income is received), or
has a liability in a premium period for run-off cover or retroactive cover and does not at any time have a contract of •
insurance providing medical indemnity cover with any other medical indemnity provider.
40 Sourced from the Medicare Australia website (www.medicareaustralia.gov.au).

Medical indemnity insurance report—Sixth monitoring report
16
3.2 Tort law reform
Since early 2001 tort law reforms have been introduced progressively by federal, state and
territory governments in response to concerns about the availability and affordability of public liability
and professional indemnity insurance. Many reforms deal directly with constraining the number
and size of personal injury payouts. As most medical indemnity claims are related to personal injury
cases, some of these reforms are expected to have an impact on the cost of providing medical
indemnity insurance.
The major reforms to tort law include the introduction of:
caps on damages for economic loss (i.e. loss of past and/or future income) and non-economic •
loss (i.e. compensation for pain and suffering)
minimum thresholds of impairment to access damages for non-economic loss •
settlement awards
changes in the limitation periods for personal injury cases•
increases in discount rates that apply to claims payouts.•
For more information on tort law reforms introduced by federal, state and territory governments, see
Available and affordable—improvements in liability insurance following tort law reform in Australia.
41
41 The Treasury, Available and affordable—improvements in liability insurance following tort law reform in Australia,
CanPrint Communications Pty Ltd, Canberra, December 2006; available at www.treasury.gov.au.

Medical indemnity insurance report—Sixth monitoring report
17
4 Trends in costs and premiums in
medical indemnity insurance
The Australian Government asked the Australian Competition and Consumer Commission to
monitor medical indemnity premiums to assess whether they are actuarially and commercially
justified. To do this, the ACCC requested a range of information about costs and pricing from
Medical Insurance Australia Pty Ltd (MIA), MDA National Insurance (MDANI), Avant Insurance
Limited (AIL), MIPS Insurance Pty Ltd (MIPSI) and QBE Insurance (Australia) Limited (QBE)/Invivo
as at 30 June 2008.
The ACCC used this information to determine trends in the costs associated with providing medical
indemnity insurance to 30 June 2008 and trends in premiums charged for indemnity protection.
42,43
The ACCC has not included data from QBE within the historical trend analysis of medical indemnity
insurance in this chapter. QBE is a large insurer that underwrites significant volumes of professional
indemnity insurance business other than medical indemnity
44
; therefore, it is difficult to disaggregate
QBE’s medical indemnity insurance results from its other professional indemnity business. In
addition, this is the third year that QBE has underwritten medical indemnity insurance, so it has
relatively limited claims experience in medical indemnity insurance. Information on QBE’s costs and
premiums are, however, analysed in chapters 5, 6 and 7.
4.1 Cost components of medical indemnity insurance
The ACCC examined the cost components of the medical defence organisation (MDO)-owned
insurers’ total premium pools for the six underwriting years between 2003–04 and 2008–09.
Table 4.1 shows the percentage of the actuarially recommended aggregate premium pool for each
cost category, which is presented as an average estimate based on the responses across insurers.
42 With the exception of section 4.1 and chart 4.7, all analysis contained in this chapter includes Avant results on a financial
year basis.
43 In some instances the results for this report for historical years may differ from those in previous reports because revised
data was provided by insurers.
44 The MDO-owned insurers only underwrite medical indemnity insurance, while QBE underwrites medical indemnity insurance
as well as a range of commercial and personal lines of insurance.

Medical indemnity insurance report—Sixth monitoring report
18
Table 4.1 Components of actuarially recommended aggregate premium pool,
2003–04 to 2008–09
2003–04
%
2004–05
%
2005–06
%
2006–07
%
2007–08
%
2008–09
%
Expected surplus
(a)
35 26 21 19 16 16
Net claims costs
(b)
33 36 40 45 44 45
Reinsurance expenses 17 16 14 13 14 13
Underwriting and general expenses 15 22 25 23 26 26
Total premium pool
(c)
100 100 100 100 100 100
Source: Derived from MDO-owned insurers by the ACCC.
(a) The expected surplus was typically raised for the purpose of capital accumulation. Currently it is
raised primarily for capital maintenance. This is discussed in more detail in section 5.3.5.
(b) The net cost of claims is the expected ultimate claims cost net of recoveries received or expected
to be received, including those from the Australian Government under the high cost claims scheme
(HCCS), run-off cover scheme (ROCS) or the UMP support scheme.
(c) The components of the premium pool in table 4.1 may not add to 100 in some years because
of rounding.
Note: The table represents the actuarially determined premium pool and does not include statutory third party
collections such as stamp duty, the goods and services tax (GST) or the ROCS levy.
Table 4.1 shows that for the 2008–09 underwriting year, the net cost of claims remains the largest
component of the total premium pool at 45 per cent. The expected surplus represented 16 per cent;
underwriting and general expenses, 26 per cent; and reinsurance expenses, 13 per cent.
The proportion of premium pool represented by the expected surplus has fallen over the period,
while the proportion represented by the net claims costs has risen. This is because of a decrease in
the absolute amount of surplus raised (as insurers approach their capital targets) combined with a
proportionally smaller decrease in the absolute amount expected for net claims costs. Reinsurance
expenses decreased from 17 per cent in 2003–04 to 13 per cent in 2008–09. Underwriting and
general expenses rose from 15 per cent in 2003–04 to 25 per cent in 2005–06, and have since
remained relatively constant.
4.2 Trends in medical indemnity claims
The cost of claims is the most significant driver of premiums in medical indemnity insurance.
This section examines the major cost component of medical indemnity insurance by examining
trends in the following indicators
45
:
45 For the sixth monitoring report the ACCC specifically requested that insurers provide the total number of claims (including
likely incidents as well as open and closed claims); the total amount of claims paid to date; and the actuarial outstanding
claims liability (inflated but undiscounted) as at 30 June 2008. This ensured that insurers provided information to the ACCC
on a consistent basis. Because of differing data sources, the results shown in section 4.2 may not be directly comparable
with that shown in previous monitoring reports.

Medical indemnity insurance report—Sixth monitoring report
19
ultimate claims costs by notification year—the ultimate costs of claims•
46
expected to be met by
insurers by year of notification
47
claim frequency—the ultimate number of claims expected by year of notification expressed as a •
proportion of the total number of Medicare services provided in the corresponding year
average size of claims—the ultimate expected•
48
average size of claims arising from a given
notification year that will eventually be settled.
4.2.1 Ultimate claims costs
Chart 4.1 shows the trend in ultimate claims costs
49
for claims notified between 1997–98
and 2007–08.
Chart 4.1 Ultimate claims costs by year of notification, 1997–98 to 2007–08
Source: Derived from MDO-owned insurers by the ACCC.
46 ‘Ultimate cost of claims’ refers to all claim costs an insurer reasonably expects will eventually be paid for claims arising in
that notification year. For example, an insurer may not finish paying claims arising in a notification year for several years,
so until all notifications for that year have been finalised, the ultimate cost includes all payments made for claims to date
as well as all those expected payments. Both past payments and expected payments are in nominal dollars for the years
in which they were/are expected to be made. Since ultimate claims costs and numbers are largely based on expectations,
which can change from year to year, data contained within this section may not be directly comparable with that shown in
earlier reports.
47 The notification year is the year in which an insurer is either notified of an incident occurring or, where no prior notification
has been made, when a claim is lodged with an insurer.
48 The ultimate cost of claims is based on an insurer’s past payments as well as a reasonable estimate of future expected
payments on claims not yet finalised. As this estimate of future expected payments is uncertain, the average claim size for
any given year will be an expected average size, until all claims have been settled for that notification year.
49 Calculated as total past payments and gross inflated and undiscounted outstanding claims liabilities. As a result, the
ultimate cost includes all payments in the nominal dollar values in which the insurer expects the payment to be made.
–
20
40
60
80
100
120
140
160
180
200
220
1997–98 1998–99 1999–00 2000–01 2001–02 2002–03 2003–04 2004–05 2005–06 2006–072007–08
Ultimate claims costs ($ million)
Notification year

Medical indemnity insurance report—Sixth monitoring report
20
The latest assessment of the ultimate cost of claims expected by year of notification increased
from $99 million in 1997–98 to $179 million in 2000–01, 2001–02 and 2002–03. It decreased
to $159 million in 2004–05. The ultimate cost of claims grew from $159 million in 2004–05 to
$203 million in 2007–08.
It should be noted that the recent notification years largely reflect actuarial estimates. The ultimate
claims cost changes over time as these estimates are replaced by actual experience.
4.2.2 Claims frequency
Chart 4.2 shows the ultimate number of claims expected to be met by insurers for each notification
year between 1997–98 and 2007–08, and the corresponding claims frequency for the number of
claims per million Medicare services provided.
Chart 4.2 Ultimate claim numbers and claims frequency by year of notification,
1997–98 to 2007–08
Source: Derived from MDO-owned insurers by the ACCC.
The ultimate number of claims increased by 67 per cent between 1997–98 and 2001–02 (from 1441
to 2403). The ultimate number of claims fell in 2002–03 to 2047, but generally remained around
the level experienced in 2001–02 over the next six years. The most recent actuarial estimate of the
ultimate number of claims expected for the 2007–08 notification year is 2489.
Ultimate claims numbers
Notification year
0
500
1000
1500
2000
2500
3000
3500
1997–98 1998–99 1999–00 2000–01 2001–02 2002–03 2003–042004–052005–06 2006–072007–08
0
2
4
6
8
10
12
14
Ultimate claims numbers (LHA) Claims frequency (RHA)
Number of claims per million Medicare services

Medical indemnity insurance report—Sixth monitoring report
21
The ultimate number of claims per million Medicare services increased from seven to 11 between
1997–98 and 2000–01. The claims frequency fell to nine per million Medicare services in 2002–03
and then fluctuated around this level for the next three years before falling in 2007–08 to nine claims
per million Medicare services. The fall from 2006–07 to 2007–08 represents a 10 per cent drop in
ultimate number of claims per million Medicare services.
Claims frequency has followed a largely similar trend to the ultimate number of claims. However,
between 2004–05 and 2006–07 the ultimate number of claims increased from 2360 to 2561 while
the number of claims per million Medicare services remained at approximately 10.
Chart 4.3 shows the trend in the ultimate average size of claims expected by notification year
between 1997–98 and 2007–08.
Chart 4.3 Ultimate average sizes of claims by year of notification, 1997–98 to 2007–08
Source: Derived from MDO-owned insurers by the ACCC.
The ultimate average size of claims increased from $68 801 in 1997–98 to $82 293 in 1999–00.
The spike in 2002–03 aside, the ultimate average size of claims declined to $67 740 in 2004–05.
In 2007–08 the ultimate average size of claims increased to $81 690, representing an increase of
13 per cent over 2006–07 levels. The spike in 2002–03 is attributable to the reported 15 per cent fall
in claim numbers in that year (refer to chart 4.2). The apparent increase in average size of claims in
2007–08 reflects a reduction in the estimated claims costs by actuaries for 2004–05 to 2006–07—
and hence in average claims size—rather than an increase in expected costs in 2007–08.
$–
$10 000
$20 000
$30 000
$40 000
$50 000
$60 000
$70 000
$80 000
$90 000
$100 000
1997–98 1998–99 1999–00 2000–01 2001–022002–03 2003–04 2004–05 2005–06 2006–07 2007–08
Average size
Notification year

Medical indemnity insurance report—Sixth monitoring report
22
4.3 Trends in other expenses
The ACCC examined trends in two other major categories of expenses—underwriting and general
expenses, and reinsurance expenses. The underwriting and general expenses category relates to all
expenses, other than reinsurance expenses and claims costs and related expenses. The reinsurance
expenses category refers to the amount of premium ceded to reinsurers for reinsurance during the
period. As with other costs, the ACCC has not assessed whether the level of these costs
is appropriate.
Chart 4.4 shows reinsurance expenses and underwriting and general expenses from 1999–2000
to 2007–08.
Chart 4.4 Reinsurance expenses and underwriting and general expenses,
1999–2000 to 2007–08
50
Source: Derived from MDO-owned insurers by the ACCC.
Note: Previously one insurer’s reinsurance cost as sourced from its annual report was adjusted based on
information it directly provided.
51
50 Reinsurance and underwriting expenses for the period 1999–2000 to 2007–08 is MDO-consolidated data. In previous
reports, the underwriting and general expenses of one MDO was adjusted to remove APRA-approved transfers; however,
this adjustment is not required for MDO-consolidated data. This adjustment has also been removed from historical data
in chart 4.4.
51 This insurer had previously held a reinsurance contract that included ongoing adjustment premiums for which the insurer
held reserves. As experience developed, the insurer was able to release these reinsurance premium reserves and these
releases were allocated to the reinsurance expense on the profit and loss statement. As a result of these reserve releases,
this insurer experienced a positive reinsurance expense in the three years to 2005–06, which distorted the actual reinsurance
costs experienced by the industry. The ACCC sought information on the actual reinsurance cost for each year between
2003–04 and 2005–06, excluding the impact of any release of reserves.
Underwriting and general Reinsurance
Total cost ($ million)
Financial year
1999–00 2000–01 2001–02 2002–03 2003–04 2004–05 2005–06 2006–07 2007–08
–
20
40
60
80
100
120
140

Medical indemnity insurance report—Sixth monitoring report
23
Underwriting and general expenses increased from $36 million in 1999–00 to $120 million in
2006–07. In 2007–08 underwriting and general expenses declined to $107 million. The industry
results observed in 2006–07 do not reflect individual experience; they mainly reflect abnormal
increases in expenses.
Reinsurance expenses increased from $53 million in 1999–2000 to $60 million in 2000–01, before
increasing markedly to $124 million in 2001–02.
52
Reinsurance expenses then fell significantly
to $44 million in 2002–03 and remained approximately at this level from 2003–04 and 2005–06.
Reinsurance expenses continued to fall to $41 million in 2006–07 and $37 million in 2007–08 as
some insurers retained more risk.
4.4 Trends in premiums
The ACCC examined medical indemnity premiums by examining trends in total premium revenue
53
and the average premium. The average premium is the total premium revenue earned per financial
year divided by the total number of indemnified policyholders for that year in real terms.
54
4.4.1 Total premium revenue
Chart 4.5 shows the trend in the total gross premium revenue
55
by underwriting year for 1999–2000
to 2007–08.
52 The spike in reinsurance expenses in 2001–02 was largely driven by the reinsurance arrangements of one insurer.
53 Total premium revenue as sourced from insurer’s annual reports includes revenue earned from medical indemnity insurance
policies provided to medical practitioners and, for some insurers, premium revenue from medical indemnity insurance
policies provided to other health professionals (such as optometrists and dentists).
54 Adjusted to 30 June 2008 values using the average weekly earnings index published by the Australian Bureau of Statistics
(ABS) (catalogue number 6302.0).
55 Premium revenue is earned premium—that is, the total amount of gross written premium earned during the period (‘earned’
being that proportion of risk covered by the policy that expired at the end of the reporting period).

Medical indemnity insurance report—Sixth monitoring report
24
Chart 4.5 Total gross premium revenue by underwriting year, 1999–2000 to 2007–08
Source: Derived from MDO-owned insurers by the ACCC.
Note: Excludes call revenue.
56
The total gross premium revenue rose significantly from $177 million in 1999–2000 to $310 million
in 2002–03. The total gross premium revenue fell marginally in 2003–04 to $297 million before rising
gradually to $315 million in 2006–07. In 2007–08 total gross premium declined to $306 million.
4.4.2 Average premium
Industry average premium
Chart 4.6 shows the trend in real average premium revenue (noting that it excludes stamp duty and
the run-off cover scheme) generated by medical indemnity providers from indemnified members.
This average gives an indication of the trend in real average premiums paid by medical indemnity
insurance policyholders between 1999–2000 and 2007–08.
56 Before MDOs were regulated from 1 July 2003, a ‘call’ was a request by MDOs for additional funding from members to
cover current or anticipated future shortfalls. To ease the burden on members, MDOs generally gave members the option of
taking several years to pay the amount of the call.
Total premium revenue ($ million)
Financial year
–
50
100
150
200
250
300
350
1999–00 2000–01 2001–02 2002–03 2003–042004–05 2005–06 2006–07 2007–08

Medical indemnity insurance report—Sixth monitoring report
25
Chart 4.6 Average premium—real terms, 1999–2000 to 2007–08
57
Source: Derived from MDO-owned insurers by the ACCC.
Notes: Data is shown in real terms adjusted to 30 June 2008 values using the average weekly earnings (AWE)
index published by the ABS.
Rates exclude third party statutory collections such as stamp duty and ROCS.
The real average premium increased steadily from $5263 in 1999–00 to $5816 in 2001–02, before
rising sharply in 2002–03 to $7500. The real average premium then fell gradually in each of the next
five years to 2007–08. In 2007–08 the average premium fell to $5392. This gradual decline in real
average premiums is attributable to a number of factors, including premium reductions and changes
to membership composition over time.
Medical specialty average premium
Medical practitioners who practise relatively more complex medical procedures are likely to face
a higher risk of medical negligence claims against them than those who perform less complex
procedures. The complexity of medical procedures is also a key determinant of the size of medical
negligence claims. Because levels of risk vary with specialties, so do the premiums charged by all
medical indemnity insurers for different types of specialties.
57 Results may not be directly comparable to those shown in previous reports because of revised membership data and the
exclusion of some non-medical practitioners and non-indemnified members from historical data.
Average premium rate
Financial year
1999–00 2000–01 2001–02 2002–03 2003–04 2004–05 2005–06 2006–072007–08
$–
$1000
$2000
$3000
$4000
$5000
$6000
$7000
$8000

Medical indemnity insurance report—Sixth monitoring report
26
To understand the relativities that apply between certain specialties, the ACCC obtained information
from insurers on the gross written premiums and membership for individual specialties for the
underwriting years between 2003–04 and 2008–09.
58
This information allowed the ACCC to examine
the average written premium for selected specialties across the six underwriting years to determine
the relativities between specialties as well as any changes in those relativities.
Chart 4.7 Average premium by specialty—real terms, 2003–04 to 2008–09
Source: Derived from MDO-owned insurers by the ACCC.
Notes: Data is shown in real terms adjusted to 30 June 2008 values using the AWE index published by the ABS.
Rates exclude third party statutory collections such as stamp duty, GST and ROCS.
58 The ACCC asked insurers to provide gross written premium and membership numbers as at a specific date in the 2008–09
underwriting year to allow insurers to provide the data before the end of the underwriting year. However, because the majority
of insurance is underwritten at the beginning of the underwriting year, the data should provide a reasonable estimate of the full
year’s results.
$– $10 000 $20 000 $30 000 $40 000 $50 000 $60 000
Obstetrician
Neurosurgeon
Plastic surgeon
Orthopaedic surgeon
GP—Procedural
(with cosmetic surgery)
Gynaecology
General surgeon
GP—procedural
(with obstetrics)
Anaesthetist
GP—procedural
General physician
GP—Non-procedural
2003–04 2004–05 2005–06 2006–07 2007–08 2008–09

Medical indemnity insurance report—Sixth monitoring report
27
Chart 4.7 shows that average premiums in real terms for the selected specialties varied between
$2667 for a non-procedural general practitioner (GP) to $48 910 for an obstetrician in 2008–09.
59,60
The average written premiums in 2008–09 compared to 2007–08 were generally lower across
the specialties. In real terms the average written premium decreases ranged from 3 per cent for
anaesthetists to 16 per cent for plastic surgeons. Average written premiums for the GP procedural
with obstetrics, GP procedural and general physician specialties increased by 3 per cent, 3 per cent
and 1 per cent respectively.
Chart 4.7 also shows the change in the average written premium for the selected specialties
between 2003–04 and 2008–09. In real terms the average written premium of all the selected
specialties decreased over the period; over the six-year period these decreases ranged from
9 per cent for obstetricians to 39 per cent for anaesthetists.
This analysis may be influenced by differing characteristics of the membership for each specialty.
Some specialties may include differing mixes of non-mature claims-made membership
61
, different
income levels and different jurisdictions.
62
All these factors may influence the average written
premium for reasons other than specialty relativities.
59 The analysis in chart 4.7 is not directly comparable with that shown in table 4.2 of the ACCC’s first monitoring report
because of differing methodologies. The ACCC’s first monitoring report examined the average of all mature claims-made
rates across all income bands, medical indemnity providers and jurisdictions. This analysis examines the total gross written
premium for all insurers for selected specialities divided by the total membership for all insurers for those specialties.
60 Different data sources mean that the results in chart 4.7 may not be directly comparable with those in chart 4.6.
61 Under a claims-made policy the insurer agrees to indemnify all claims arising from incidents notified during the policy period,
as long as the incident occurred during the current period or any previous periods in which the policyholder has held
continuous claims-made cover with the insurer up to, and including, the current period. As a result of the more limited period
the insurer is ‘on risk’, this product is discounted during the earlier years, until the policy becomes ‘mature’, which is typically
four to five years.
62 For example, some high-risk categories are more prevalent in jurisdictions where different legislative requirements and
historical claims experience results in a higher premium.

Medical indemnity insurance report—Sixth monitoring report
29
5 Actuarial justification of medical
indemnity premiums
This chapter presents the findings of the Australian Competition and Consumer Commission on the
actuarial justification of medical indemnity premiums charged for the 2008–09 underwriting period
63
by the five authorised providers of medical indemnity insurance to private medical practitioners as at
30 June 2008. This analysis examines the actuarial justification of premiums at an industry level by
identifying a number of issues common to medical indemnity pricing across the industry.
The ACCC’s findings regarding the actuarial justification of medical indemnity premiums charged
within each jurisdiction for 2008–09 are discussed in chapter 7.
5.1 Qualifications
The ACCC’s analysis is based on information supplied by each of the five insurers. The ACCC has
relied on the information provided by insurers rather than performing an independent verification.
As the parent entities of the four medical defence organisation-owned insurers are no longer able
to underwrite risks, the ACCC has generally not examined their operations or membership pricing.
The ACCC’s analysis examined only the premiums charged by each insurer for primary medical
indemnity insurance and specifically excluded any examination of ancillary policies, allied health care
professionals or the subscription charged by the MDO.
In preparing this report it was necessary for the ACCC to maintain the confidentiality of information
provided by individual insurers. Accordingly, some quantitative aspects of the ACCC’s analysis,
particularly its assessment of information provided by individual insurers, could not be disclosed
in this report.
5.2 Assessment methodology
5.2.1 Four MDO-owned insurers
For the four MDO-owned insurers, the ACCC review of the actuarial justification of premiums
considers the process adopted by insurers in the derivation of premium rates, the approach for
constructing those premiums, the level of detail used to support pricing assumptions, the rigour
of the analysis and the extent to which other relevant issues (such as medical indemnity and tort
reforms) have been considered in setting prices.
63 The 2008 calendar year in the case of 1 January renewal Avant Insurance Limited (AIL) members and Invivo/ QBE Insurance
(Australia) Limited (QBE) policyholders.
Medical indemnity insurance report—Sixth monitoring report
30
Specifically, the ACCC examined the following:
Ratings process—the method used by the medical indemnity insurer’s actuary to determine •
premium rates. The factors considered by the ACCC include:
the extent to which premium rates are based on sound actuarial principles and professional •
standards
the method employed by the actuary to construct the aggregate premium pool, associated •
premium relativities, the assumptions adopted and the rigour associated with setting those
assumptions
the extent to which the insurer’s board adopted the actuary’s recommended premium rates•
the degree to which the recommended actuarial premium pool details in the pricing report are •
consistent with, and supported by, other reports, such as the financial condition report and
the outstanding liability assessment.
Pure risk premium—the level of premium needed just to meet the cost of expected medical •
indemnity claims and associated costs. This can be difficult to determine accurately because
the ultimate costs associated with these claims are unlikely to be known for some years after
the premium has been set (see section 5.3.2). The estimate of pure risk premium excludes the
premium amount necessary to cover the insurer’s expenses, reinsurance expenses and any
surplus required. Factors considered include issues related to the cost structure of claims,
such as the:
adopted claims frequency assumption•
allowances for large claims•
projected rate of claims cost increases•
legal costs•
discount rate•
projected growth rate of membership numbers•
specialty mix and claims-made profile•
jurisdiction of claims.•
Expenses—the expense incurred by the insurer as a result of acquiring, writing and servicing the •
insurance business. Factors considered include assessing the appropriateness of the expected
level of costs.
Reinsurance expenses—the amount of premium ceded to reinsurers for reinsurance. Factors •
considered include:
whether the reinsurance premium is used effectively to minimise the risk exposure of the •
portfolio
the extent to which the cost of reinsurance is included in premium rates recommended •
by the actuary.
Medical indemnity insurance report—Sixth monitoring report
31
Surplus—the surplus of funds expected to emerge after the cost of claims, expenses and •
reinsurance costs are deducted from premium revenue. For insurers, these funds are typically
used to meet and maintain target capital levels and provide a contingency margin on expected
claims costs. Factors considered by the ACCC include:
assessing the capital structure of the insurer and the cost-effectiveness of how the capital •
is raised
examining the purpose for building a surplus into premiums and the appropriateness of the •
amount needed for each purpose
quantifying the effect on premiums of any allowance for the surplus.•
Recommended rates/relativities—the premium rate and/or price relativities for each classification •
used, including specialty and income band relativities. Factors considered include:
the method of derivation of relativities across classifications, including the extent of the •
analysis to confirm or modify risk classifications
quantifying cross-subsidies and incorporation of board policy in the recommended rates•
comparing the actuary’s recommended premium relativities against the actual premium rates •
charged by the insurer, with insurers being asked to explain material differences.
The analysis of jurisdictional relativities is considered separately in chapter 7.
Government reforms—the impact of measures arising from the Australian Government’s medical •
indemnity package and relevant tort law reforms introduced by the federal government and state
and territory governments on costs and premiums. The ACCC requested specific commentary
on the following government initiatives:
High cost claims scheme (HCCS)—insurers were asked to detail the degree of influence •
this scheme has had on the calculation of the required premium pool and/or recommended
premium rates and estimated claims cost reductions, as well as any allowances made for
changes in the level and cost of reinsurance and the insurer’s capital requirements.
Run-off cover scheme (ROCS)—insurers were asked to detail the degree of influence this •
scheme has had on the calculation of the required premium pool and/or recommended
premium rates and estimated claims cost reductions, as well as any allowances made for
changes in the level and cost of reinsurance and the insurer’s capital requirements.
Tort law reform—insurers were asked to detail the effect of tort reforms on the premium-•
setting arrangements. This included specific commentary by jurisdiction of the effect on costs,
premiums, assumptions and the methodology employed. When no consideration of the effect
of tort law reforms on costs and premiums was given, this was to be noted.
5.2.2 QBE Insurance (Australia) Limited
QBE’s pricing methodology differs from MDO-owned insurers that price top-down using an
aggregate premium pool combined with risk relativities based on an insured profile to determine
individual premium. QBE determines individual premiums for each specialty and jurisdiction on a
bottom-up basis. QBE’s pricing methodology is described in further detail in section 5.4.1.
Medical indemnity insurance report—Sixth monitoring report
32
Because of this, the ACCC’s assessment methodology for QBE differed from that outlined above
for the four MDO-owned insurers. The ACCC’s assessment of the actuarial justification of QBE’s
premiums examined the following:
Ratings process—the method used by QBE’s actuary to determine premium rates. Factors •
considered by the ACCC include the:
extent to which premium rates are based on sound actuarial principles and professional •
standards
method employed by the actuary to construct the individual premiums for each specialty, the •
assumptions adopted and the rigour associated with those assumptions
actuary’s inclusion of reasonable allowance for expense, reinsurance and surplus loadings in •
individual premiums
extent to which the insurer adopted the actuary’s recommended premium rates.•
Government reforms—the impact of measures arising from the Australian Government’s medical •
indemnity package and relevant tort law reforms introduced by the federal government and state
and territory governments on costs and premiums. The ACCC requested specific commentary
on the following government initiatives:
HCCS—the ACCC’s analysis examined the degree of influence this scheme has had on •
the calculation of recommended premium rates and estimated claims cost reductions, as
well as any allowances made for changes in the level and cost of reinsurance and QBE’s
capital requirements.
ROCS—the ACCC’s analysis examined the degree of influence this scheme has had on •
the calculation of recommended premium rates and estimated claims cost reductions, as
well as any allowances made for changes in the level and cost of reinsurance and QBE’s
capital requirements.
Tort law reform—the ACCC’s analysis examined the effect of tort reforms on the premium-•
setting arrangements. This included specific commentary of the effect on costs, premiums,
assumptions and the methodology employed.
Because of the differences in QBE’s pricing methodology, the actuarial justification of QBE’s
premiums is discussed separately in section 5.4.
5.3 Analysis—MDO-owned insurers
5.3.1 Ratings process
Based on the information provided by insurers, the ACCC found that the method employed in
constructing the aggregate premium pool was generally consistent across the MDO-owned insurers.
Insurers estimated the aggregate premium pool required by establishing the estimated cost of
claims, reinsurance costs, administration expenses and a margin for capital growth or maintenance.
The methodology adopted by all insurers to establish their actual premium pools was supported
by actuarial advice.

Medical indemnity insurance report—Sixth monitoring report
33
All insurers determined their aggregate premium pool having considered advice from their actuaries.
However, different insurers involved actuaries at different points in the pricing process.
On this basis the ACCC found that the ratings processes used and the aggregate premium pool
adopted by all four MDO-owned insurers were actuarially sound.
The ACCC, however, encourages the early involvement of actuaries in each stage of the
rating process.
5.3.2 Pure risk premium
The ACCC considered the pure risk premium component of the aggregate premium pool for
the 2008–09 underwriting year.
64
Pure risk premium is the basic building block for determining
the aggregate premium pool and represents the direct cost of settling claims. As shown in
table 4.1, the net claims cost represented 45 per cent of the aggregate premium pool for the
2008–09 underwriting year.
65
The ACCC found that insurers now employ similar methodologies. Insurers estimate the total losses
arising from claims notified in the year following the latest liability assessments. In some cases
explicit assumptions are made for claims frequencies and average claims costs. The projected
payments are then discounted based on an assumed pattern of payments to allow for expected
investment income. Insurers assume that the cost of claims will increase at a rate equal to or greater
than normal wage inflation.
The ACCC found that the stated approaches were all considered sound.
5.3.3 Expenses
The ACCC considered the amount of expenses incorporated into the aggregate premium pool for
the 2008–09 underwriting year. Table 4.1 shows that the expenses represented 26 per cent of the
aggregate premium pool for the 2008–09 underwriting year.
All aggregate premium pool estimates included an allowance for expenses. The proportion of
expenses to the aggregate premium pool varied between insurers; however, the ACCC has
assessed that they are actuarially justified.
One insurer experienced a large decrease in expenses following the correction of the previous year’s
calculation of expenses.
Different insurers use different service models. Some insurers provide all services to policyholders
while others outsource this to the parent MDO, which means the allocation of expenses can vary
between different insurers. Both approaches are considered reasonable and in all instances the
servicing costs were recognised and appropriate allowances for insurance company expenses were
incorporated in the aggregate premium pool.
64 The 2008 calendar year in the case of 1 January renewal AIL members.
65 The net claims costs is the expected ultimate claims cost net of recoveries received or expected to be received,
including those from the Australian Government, under the HCCS, ROCS and the UMP support scheme.

Medical indemnity insurance report—Sixth monitoring report
34
5.3.4 Reinsurance expenses
The ACCC considered the reinsurance expenses incurred by insurers to assess whether the
reinsurance program was used effectively to minimise the insurer’s risk exposure and the extent to
which the cost of reinsurance was considered in premium rates recommended by the actuary.
Table 4.1 shows that reinsurance expenses represented 13 per cent of the aggregate premium pool.
All medical indemnity insurers used reinsurance programs for the 2008–09 underwriting period to
manage the risks inherent in their portfolio. Most insurers used a combination of excess of loss and
stop-loss reinsurance to manage their risk exposure.
66
The attachment points for excess of loss
reinsurance and the aggregate retention for stop-loss reinsurance adopted by insurers varied across
the industry according to individual circumstances. All insurers factored the total cost of reinsurance
into the premiums charged to medical practitioners.
67
The ACCC acknowledges that the trade-off between the net cost of reinsurance and the level
of risk the insurer is willing to undertake is ultimately a business decision for the insurer. The ACCC
notes that, similar to last year’s report, one insurer’s reinsurance arrangements for the 2008–09
underwriting year reflected its assessment that one component of its potential reinsurance program
would have been ineffective in reducing risk given the premium being asked by the reinsurer.
The effect of this change was that the insurer has increased its potential loss in the event of
adverse claims experience; however, this increase in volatility is managed by holding a greater
amount of capital.
5.3.5 Surplus
The ACCC considered the component of each insurer’s aggregate premium pool that represented a
surplus. The surplus component is generally designed to:
build the capital needed to achieve the target level set by the Australian Prudential Regulation •
Authority (APRA)
68,69
build the additional capital needed as a result of risks underwritten in 2008–09 to maintain total •
capital at, or above, the level required by APRA
maintain a contingency (or prudential) margin over and above the actuary’s central estimate of •
the outstanding claims liability to increase the probability that the pure risk premium is adequate
to meet the cost of claims
provide a surplus (profit) to the insurer.•
66 ‘Excess of loss’ is a form of reinsurance that indemnifies a reinsured against claims in excess of an agreed amount (known
as the ‘attachment point’) and the reinsurer pays the loss in excess of this amount up to an agreed limit. In addition, there
may be an aggregate limit for all claims assumed by the reinsurer. Stop-loss reinsurance is where the reinsurer is obliged to
cover, up to a limit, any part of the total annual loss burden that exceeds an aggregate retention.
67 In some cases the reinsurance program covered risk incurred as a result of incurred but not reported claims resulting from
cover provided by the parent MDO. A portion of the reinsurance premium was then charged to the MDO.
68 As discussed in chapter 2, the change from medical indemnity being offered by discretionary mutuals to authorised insurers
from 1 July 2003 resulted in medical indemnity providers being required to maintain a minimum level of capital to support
their insurance business. In recognition of the significance of this change, APRA introduced special transition arrangements
that allowed medical indemnity providers to meet the target capital levels by 30 June 2008.
69 The ACCC understands that APRA has targeted 150 per cent minimum capital requirement as the expected level of capital
to be held by medical indemnity insurers.

Medical indemnity insurance report—Sixth monitoring report
35
Table 4.1 shows that the amount of surplus in the aggregate premium pool has decreased over the
past four underwriting years, from 35 per cent in 2003–04 to 16 per cent in 2008–09. However, it
should be noted that the actual surplus levels varied between insurers.
The decrease in the proportion of the aggregate premium pool represented by surplus reflects the
fact that insurers initially used the surplus to build capital to APRA’s target level of 150 per cent of
minimum capital requirement (MCR) and, as insurers’ capital levels passed this, their own internal
targets.
70
As a result, a significant surplus is no longer needed.
For the 2008–09 underwriting period the ACCC found that all insurers had generated sufficient
capital to satisfy APRA’s target level of 150 per cent of the MCR and no longer needed to include the
significant surplus loading built into previous years’ premiums.
Most insurers no longer include an explicit loading in their premiums for additional capital; however,
one insurer took a different approach to determine the surplus in its premium pool. Importantly, the
level of surplus was quantified by each insurer as the difference between expected collections and
the explicit premium pool components identified above.
As discussed in the last year’s report, one insurer continued to expect its aggregate premium pool to
increase its capital levels beyond its internal target levels. Smoothing premium increases over several
years has meant that in the short term this insurer will continue to generate capital at a greater
rate than required. Other mechanisms such as premium rebates were also employed for returning
surplus capital to policyholders.
The ACCC took into account the long-term pricing goals as well as the overall capital position of the
insurer when determining the actuarial justification of this insurer’s current year premiums.
No insurer explicitly included a surplus in premiums for the purpose of making a profit. While some
insurers have the ability to pay a dividend to the parent entity (the MDO), MDOs operate on a not-
for-profit-basis as ‘mutuals’ owned and operated by members and, therefore, would not have the
incentive, or the mechanism, to make and distribute any profit.
5.3.6 Recommended relativities and cross-subsidisation
The ACCC examined the premium rate relativities across the various risk specialties recommended
by the actuary to the insurer’s board.
The ACCC found that most insurers have examined premium relativities across specialties.
Insurers typically examined historical frequency and average size by specialty. The ACCC found
that cross-subsidisation between specialties was common across insurers and that in some cases
significant variance between the technical and actual relativities remained. While insurers stated
that their objective is to unwind these cross-subsidies, many indicated that this was a long-term
process and potentially not all cross-subsidies would be removed for a variety of reasons,
70 The ACCC understands that while APRA has targeted 150 per cent MCR as the expected level of capital to be held by the
four MDO-owned insurers, all insurers have set internal targets higher than this amount.

Medical indemnity insurance report—Sixth monitoring report
36
including commercial factors as well as data limitations. All insurers identified and quantified cross-
subsidies between risk specialties.
71
The ACCC also examined the premium relativities applied across broad income bands. Similar to
the analysis done for specialties, insurers generally examined these rates by comparing the risk
relativities between income bands. Cross-subsidies exist between income bands and again some
insurers indicated a desire to unwind these.
The ACCC found that, given that the premium relativities between specialties and income bands
had been examined and commented on and that cross-subsidies had been identified and, where
possible, quantified, the relativities adopted were actuarially justified.
The ACCC’s assessment of the actuarial and commercial justification of premium relativities between
jurisdictions is considered in chapter 7.
5.3.7 Government reforms
The ACCC examined the effect of the Australian Government’s medical indemnity reforms (in
particular, HCCS and the ROCS) and federal, state and territory tort law reform on costs and
premiums, which were identified as having the main impact on claims costs (and therefore
premiums). The extent to which insurers had considered these measures when determining
premiums varied across the industry.
High cost claims scheme
The HCCS was introduced to address the issue of high-cost claims for medical incidents. It was
designed to reduce the potential cost of large claims to insurers and is expected to affect premiums
in two ways: first, to reduce the pure risk premium component of premiums because the Australian
Government will pay 50 per cent of high-cost claims above a threshold amount
72
; and, second, to
reduce the amount of reinsurance needed to cover the total cost of high-cost claims. These effects
will, to some degree, be interdependent, depending on the attachment points of each insurer’s
reinsurance program.
All insurers took into account the full amount of expected HCCS recoveries in determining the pure
risk premium for the 2008–09 underwriting year. Most insurers indicated that they had factored the
full effect of the HCCS into their 2008–09 reinsurance programs. As noted in previous reports, the
rationale of the one insurer for not factoring the HCCS into the reinsurance program is as a result of
the unwillingness of the reinsurance company to factor HCCS in.
71 Cross-subsidisation between current and retired insureds has now been formalised by the introduction of ROCS, which
provides automatic free insurance cover to doctors for death, disability, maternity and retirement (doctors aged 65 or over or
who have left the workforce for three or more years). The scheme is funded by a percentage charged on the total premium
pool of medical indemnity providers, which in turn is passed on to the premiums charged to current financial medical
practitioners.
72 The threshold is currently $300 000. See the Department of Health and Ageing, viewed at www.health.gov.au/internet/main/
publishing.nsf/Content/health-medicalindemnity-faq-hccs.htm.

Medical indemnity insurance report—Sixth monitoring report
37
The ACCC view continues to be that because the rationale for not taking the HCCS fully into
account in the reinsurance program appears to be unwillingness by some reinsurers to fully
reflect the benefits of the Australian Government’s scheme, the aggregate premium pool of these
insurers is actuarially justified. Importantly, these insurers fully took HCCS recoveries into account in
establishing their pure risk premium.
Run-off cover scheme
ROCS was introduced to provide secure cover for medical practitioners who retire, die, become
permanently disabled, take maternity leave or leave the workforce for three years or more.
The scheme covers claims by these medical practitioners, with the cost funded by a charge on
current members. This scheme is expected to affect premiums by taking claims from these medical
practitioners off the insurers’ books, thereby reducing the pure risk premium. However, premiums
will increase by the amount the Australian Government charges to cover the cost of this scheme.
All insurers commented on the effect of ROCS on 2008–09 premiums. All insurers indicated that
they expected to make recoveries from ROCS on claims costs resulting from notifications received
in the 2007–08 underwriting year. Although the level of recoveries varied between insurers, none
expected recoveries of the same order as the ROCS levy imposed on final premiums.
All insurers continue to indicate they are correctly incorporating the ROCS levy into the premiums
charged to medical practitioners.
Based on this, the ACCC found that the insurers’ consideration of ROCS in determining their
premiums for the 2008–09 underwriting year was actuarially justified.
Tort law reform
The Australian Government and state and territory governments have progressively introduced tort
law reforms since early 2001 in response to problems perceived in the availability and affordability
of public liability and professional indemnity insurance.
73
Many of the reforms deal directly with
constraining the number and size of personal injury payouts. As most medical indemnity claims are
for personal injury cases, some of these reforms are expected to affect the cost of providing medical
indemnity insurance.
All insurers implicitly took tort law reform into account when setting premiums because they adopted
assumptions for average claim size and frequency based on past experience that now incorporate
these tort law reforms. Insurers generally indicated that the number of claims had decreased as
result of tort law reform.
The impact of tort law report on the average cost of claims was less clear because the reduction in
claim numbers occurred in both low-cost and high-cost claims.
73 The effect of tort law reform on costs and premiums in public liability and professional indemnity insurance is discussed in
more detail in the Australian Government publication, Available and affordable—Improvements in liability insurance following
tort law reform in Australia, December 2006, available at www.treasury.gov.au.
Medical indemnity insurance report—Sixth monitoring report
38
5.3.8 Conclusion
The ACCC found that premiums were considered to be actuarially justified for all four
MDO-owned insurers.
The ACCC examined several factors in its determination of the actuarial justification of premiums,
including assessment of the aggregate premium pool, the recommended relativities for each
classification (including specialty and income bands) and the impact of specific government reforms
on premiums.
The ACCC found that the aggregate premium pool of each insurer was actuarially justified. It was
evident that insurers had generally made use of actuaries in premium liability assessments, pricing
reports, funding plans and financial forecasts. In each case it was considered that the construction
of the recommended premium pool was soundly based and incorporated all major cost implications
for the pricing of medical indemnity insurance. All insurers determined their aggregate premium
pool having considered advice from their actuaries. However, different insurers involved actuaries at
different points in the pricing process.
The ACCC analysis of specialty premium rates found that most insurers conducted detailed analysis
on the risk relativities between specialties or relied on previous risk relativity analysis. As in previous
monitoring reports, the ACCC found that insurers generally cited the unwinding of existing cross-
subsidisation between specialties as an objective. The ACCC noted that this was a long-term
process and potentially not all cross-subsidies would be removed for a variety of reasons, including
commercial factors as well as data limitations. However, the ACCC still found these rates and the
relativities for income bands to be actuarially justified because the extent of cross-subsidisation was
understood and, where possible, quantified.
The ACCC’s analysis of the impact of government reforms on premiums includes an examination of
Australian Government medical indemnity reforms (including HCCS and ROCS) and federal, state
and territory tort law reforms. The ACCC found that all insurers appropriately considered HCCS
and ROCS in their premium determinations and most insurers took full account of HCCS in their
reinsurance programs.
Although one insurer did not reflect HCCS in its reinsurance program because of the unwillingness of
its reinsurers to fully reflect the full benefits of the scheme, the insurer fully took HCCS recoveries into
account when establishing their pure risk premium. All insurers, either implicitly or explicitly, also took
tort law reform into account in setting their aggregate premium pools for 2008–09.
5.4 Analysis—QBE
As described in section 5.3, the four MDO-owned insurers price by establishing an aggregate
premium pool and then determining risk relativities for insureds based on their jurisdiction, specialty
and income. In contrast, QBE’s pricing approach is different, with premiums established on a
bottom-up rather than a top-down approach.
This difference in approach meant that the ACCC’s analysis of QBE is separate to the four
MDO-owned insurers.
Medical indemnity insurance report—Sixth monitoring report
39
5.4.1 Ratings process
As identified in the previous reports, the method employed by QBE in constructing premiums was
based on calculating individual premiums for each specialty. The process used by QBE included
an analysis of the ultimate claims frequency and average claims size by specialty, including an
assessment of the impact of reinsurance and government reforms. Using this analysis QBE forecast
gross premiums payable to it by including the following components:
claim frequency•
average claims cost•
reinsurance costs•
expenses (including administration, brokerage and interest)•
profit.•
As a relatively new medical indemnity underwriter, QBE’s limited claims experience does not provide
a sufficient volume of claims for deriving or adjusting premium rates. However, it is being monitored
by an actuary as an input into the pricing process. Premium levels and adjustments to 2007 rates for
the 2008 calendar year were based on analysis of available market information and identified issues
considered by QBE actuaries to be likely to affect premiums. Differential premiums were applied in
each jurisdiction, also based on analysis of available industry data.
5.4.2 Government reforms
High cost claims scheme
As noted above, the HCCS is expected to reduce premiums two ways: first, by reducing the pure
risk premium component, as the Australian Government meets 50 per cent of the excess above
a threshold amount of the cost of individual large claims, and, second, by reducing the amount of
reinsurance needed to cover the total cost of high-cost claims.
QBE examined the effect of the HCCS on its pure risk premium and took into account the full
amount of expected HCCS recoveries. Further, QBE’s reinsurance program was designed to
reinsure only the risk net of the HCCS recoveries.
Run-off cover scheme
ROCS is expected to affect premiums by taking claims from medical practitioners who retire, die,
become permanently disabled, take maternity leave or permanently leave the workforce for three
years or more off the insurers’ books, thereby reducing the pure risk premium.
QBE did not explicitly take any ROCS recoveries into account when estimating its claims costs
because its pricing methodology prices risks individually.
Medical indemnity insurance report—Sixth monitoring report
40
Tort law reform
As tort law reform predominantly deals with constraining the number and size of personal injury
cases, it is expected to affect the cost of providing medical indemnity insurance because most
medical indemnity claims relate to personal injury. QBE took into account tort law reform during the
process of establishing its final average claims costs by specialty.
5.4.3 Conclusion
The ACCC found that QBE’s 2008 premiums were actuarially justified. The analysis recognised that
this is only QBE’s third year of underwriting medical indemnity insurance and therefore it has limited
available claims experience. The ACCC’s assessment included revisiting the original methodology
used to set premiums, which compared scheduled premium rates with the actuary’s recommended
premium rates. It also involved assessing the impact of specific government reforms on premiums
and changes in rates based on emerging experience and other identified issues.
5.5 Conclusion
The ACCC found that premiums were considered to be actuarially justified for the four
MDO-owned insurers.
The ACCC found that the aggregate premium pool of each MDO-owned insurer was actuarially
justified. In all cases the construction of the recommended premium pool was considered to be
soundly based and reflected consideration of detailed advice from actuaries.
The ACCC’s analysis of specialty premium rates found that all MDO-owned insurers either
conducted detailed analysis on the risk relativities between specialties or relied on recent analysis.
As in previous monitoring reports, the ACCC found that insurers generally cited the unwinding of
existing cross-subsidies between specialties as an objective, but noted that this was a long-term
process and potentially not all cross-subsidies would be removed for a variety of reasons, including
commercial factors as well as data limitations.
For most insurers, no major realignment of rates was conducted for 2008–09. However, the ACCC
still found these rates and the relativities for income bands to be actuarially justified because the
extent of cross-subsidisation was understood and, where possible, quantified.
The ACCC found that all insurers appropriately considered the HCCS and ROCS into their
premium determination and most insurers took full account of the HCCS in their reinsurance
programs. The insurer that did not reflect the HCCS in its reinsurance program did so because of
an unwillingness of reinsurers to reflect the full benefits of the scheme in their reinsurance pricing
and structure. Importantly, these insurers took the HCCS recoveries into full account when
establishing their pure risk premium. All insurers took tort law reform into account when setting
their aggregate premium pools for 2008–09.
The ACCC also conducted separate analysis of QBE’s premiums and found them to be
actuarially justified.

Medical indemnity insurance report—Sixth monitoring report
41
6 Commercial justification of medical
indemnity premiums
This chapter presents Australian Competition and Consumer Commission (ACCC) findings on the
commercial justification of medical indemnity premiums charged for the 2008–09 underwriting period
by insurers to private medical practitioners.
74
The ACCC analysis examines the commercial justification of premiums at an industry level by
identifying a number of issues common to medical indemnity pricing across the industry.
The ACCC findings regarding the commercial justification of medical indemnity premiums charged
within each jurisdiction for 2008–09 are discussed in chapter 7.
6.1 Qualifications
The ACCC analysis is based on information supplied by each of the insurers. The ACCC has relied
on information provided by insurers rather than performing an independent verification. As the
medical defence organisation parent entities of insurers are no longer able to sell insurance, the
ACCC has generally not examined their operations or membership pricing. For the MDO-owned
insurers this analysis, to the extent possible, only examined the premiums charged by each insurer
for primary medical indemnity insurance and specifically excluded any examination of ancillary
policies or the subscription charged by the MDO.
In preparing this report it was necessary for the ACCC to maintain the confidentiality of information
provided by individual insurers. Accordingly, some quantitative aspects of the ACCC analysis,
particularly relating to its assessment of an individual insurer’s information, could not be disclosed
in this report.
6.2 Assessment methodology
The ACCC’s assessment of the commercial justification of premiums considers whether each
insurer’s current premiums and pricing strategies would be sustainable in a viable and ongoing
commercial market.
Fiscally responsible insurers examine the financial impact of pricing decisions on their operations
by preparing business plans that describe how they intend to manage their business. They also
prepare detailed corporate plans on the financial effect (including on the income statement and
balance sheet) of the business plan on their overall corporate strategies. This type of analysis
74 On 1 July 2007 Avant Insurance Limited began operating as a medical indemnity insurer as the result of the merger of the
parent-MDO entities Australasian Medical Insurance Limited and Professional Indemnity Insurance Company Australia Pty
Limited. In previous reports, the commercial justification of AMIL and PIICA was assessed separately. This report is the first
to assess the commercial justification of AIL.

Medical indemnity insurance report—Sixth monitoring report
42
is necessary to ensure that insurers remain capital-compliant with the targeted capital level following
the end of the transition period.
75
The sixth medical indemnity premium monitoring report coincides with the end of Australian
Prudential Regulation Authority’s transitional arrangements. Medical indemnity providers are now
required to meet APRA’s minimum capital requirements.
In examining the commercial justification of premiums, the ACCC compared for the
MDO-owned insurers:
The financial projections contained in their initial funding plans as provided to APRA to make •
use of the transition period for building the capital to APRA-targeted capital (referred to as
‘2002–03 projections’).
The revised financial projections prepared in 2003–04, 2004–05, 2005–06, 2006–07 and •
2007–08 (referred to respectively as ‘2003–04 projections’, ‘2004–05 projections’, ‘2005–06
projections’, ‘2006–07 projections’ and ‘2007–08 projections’). These projections are typically
updated each year to take into account more recent data and developments.
76
The actual financial position as at 30 June 2004, 30 June 2005, 30 June 2006, 30 June 2007 •
and 30 June 2008 based on data provided by APRA (referred to as ‘actual results’).
77
Comparing these sets of data allows the ACCC to examine how insurers’ financial position
forecasts have changed over the six years and whether forecasts for 2008–09 were based on
insurers’ recent experiences.
78
The ACCC examined several key indicators in making its assessment of the commercial justification
of premiums, including:
solvency•
79
—the current and forecast net asset position of insurers to assess levels of solvency
emerging surplus—the emerging and forecast levels of surplus loading in premium and whether •
this was sufficient to achieve the insurers’ targeted solvency and capital requirements
minimum capital requirement coverage and capital targets—current and forecast levels of MCR •
coverage to examine whether capital targets would be met
return on net assets—current and forecast return on net assets•
underwriting performance—the emerging and forecast underwriting performance in terms of the •
loss, expense, reinsurance and combined ratios (defined in section 6.3.5).
75 The Australian Prudential Regulation Authority established a scheme for transitional arrangements whereby providers had
up to five years from 1 July 2003 to 30 June 2008 to comply with these minimum capital requirements. APRA required all
medical indemnity providers intending to use the transitional period to build the required minimum capital to provide it with a
funding plan indicating how this capital was going to be raised over the transitional period.
76 These revised projections were updated at different times depending on the insurer. The ACCC endeavoured to use the
most recent projections up to 30 June of each year.
77 The 30 June 2008 values are derived from quarterly data provided by APRA. The 30 June 2004, 30 June 2005, 30 June
2006 and 30 June 2007 values are derived from annual data provided by APRA.
78 Some historical figures have been restated to better reflect the experience of the insurance companies.
79 Solvency is a measure of whether an insurance company has sufficient assets (capital, surplus, reserves and so on) to meet
its liabilities (the cost of claims and all other expenses) as they fall due.

Medical indemnity insurance report—Sixth monitoring report
43
The ACCC’s ability to report on the commercial justification of QBE’s premiums for the 2008–09
underwriting year was limited because of data constraints surrounding the company. This is
because QBE:
has limited historical information specific to medical indemnity insurance•
is a large insurer that underwrites significant volumes of professional indemnity insurance •
business other than medical indemnity
80
and, therefore, it is difficult to disaggregate QBE’s
medical indemnity insurance results from its other professional indemnity business.
The ACCC has not included QBE’s data in the industry analysis contained in chapter 6;
however, it has separately examined the commercial justification of QBE’s premiums by examining
Invivo’s financial projections and how these are consolidated within QBE’s professional indemnity
insurance business.
6.3 Analysis—MDO-owned insurers
6.3.1 Solvency targets
The ACCC assessed insurers’ actual solvency level as at 30 June 2004 to 30 June 2008 and
compared these against the projections of solvency based on the six projection years between
2002–03 and 2007–08. This is shown in chart 6.1.
Chart 6.1 Net assets: actual results, 30 June 2004 to 30 June 2008; and projections,
2002–03 to 2007–08
80 The MDO-owned insurers only underwrite medical indemnity insurance, whereas QBE underwrites medical indemnity
insurance as well as a range of commercial and personal lines of insurance.
Net assets ($ million)
–
100
200
300
400
500
600
700
800
2002–03 projections 2003–04 projections 2004–05 projections 2005–06 projections
2006–07 projections 2007–08 projections Actual results
Financial year
2003–04
2004–05 2005–06 2006–07 2007–08 2008–09 2009–10 2010–11 2011–12
Source: Derived from MDO-owned insurers by the ACCC.

Medical indemnity insurance report—Sixth monitoring report
44
Chart 6.1 shows that the 2003–04 projections originally forecast that the net assets of the
medicalindemnity industry would increase from $186 million to $390 million between 30 June 2004
and 30 June 2008. These forecast positions improved in later projections. The 2007–08 projections
forecast the net asset position to grow from $577 million at 30 June 2008 to $707 million at
30 June 2012.
As at 30 June 2008 the industry is in a strong solvency position, with total assets exceeding
total liabilities by $619 million. This represents an improvement on the actual result observed at
30 June 2007 of $529 million.
While the actual net asset position of all insurers steadily improved from $251 million in 2003–04 to
$619 million in 2007–08, the degree to which net assets improved for individual insurers depended
on their circumstances.
6.3.2 Emerging surplus
The ACCC assessed the actual emerging surplus as at 30 June 2008 and compared this to the
emerging surplus forecast in the projection years between 2002–03 and 2007–08. This is shown in
chart 6.2.
Chart 6.2 Emerging surplus: actual position, 2003–04 to 2007–08; and projections,
2002–03 to 2007–08
Source: Derived from MDO-owned insurers by the ACCC.
2002–03 projections 2003–04 projections 2004–05 projections 2005–06 projections
2006–07 projections 2007–08 projections Actual results
Emerging surplus ($ million)
Financial year
2003–04
2004–05 2005–06 2006–07 2007–08 2008–09 2009–10 2010–11 2011–12
–
20
40
60
80
100
120
140
160
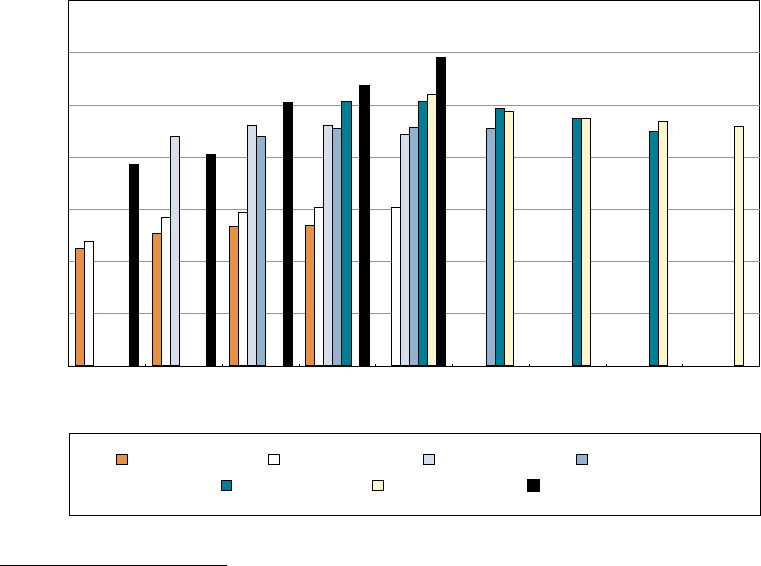
Medical indemnity insurance report—Sixth monitoring report
45
The chart shows that the 2003–04 projections forecast that the level of emerging surplus would
decrease from $86 million in 2003–04 to $49 million in 2007–08. A declining emerging surplus is
also reflected in all six projection sets for 2007–08. The 2007–08 projections show that the industry
is expecting emerging surplus to reduce in 2008–09 to $8 million, but to increase to approximately
$39 million in 2009–10, 2010–11 and 2011–12. Surpluses are now considered to be at a level
generally designed to maintain target capital goals.
The medical indemnity industry recorded a surplus of $25 million in 2007–08. The decline in
emerging surplus compared with forecast emerging surplus is because of higher than anticipated
expenses for some insurers as well as poor investment earnings.
6.3.3 MCR cover and capital targets
The ACCC assessed the actual financial position of MDO-owned medical indemnity insurers as at
30 June 2008 and compared this with the financial position forecast in the projection years between
2002–03 and 2007–08. The ACCC examined the net asset
81
to MCR ratio as an indicator of financial
strength, as shown in chart 6.3.
81 For the analysis in section 6.3.3, the net asset position is, where possible, based on the APRA-determined capital base of
the insurers. The APRA determined capital base is used by APRA to gauge compliance with the MCR.
2002–03 projections 2003–04 projections 2004–05 projections 2005–06 projections
2006–07 projections 2007–08 projections Actual results
Per cent
Financial year
2003–04
2004–05 2005–06 2006–07 2007–08 2008–09 2009–10 2010–11 2011–12
0
50
100
150
200
250
300
350
Chart 6.3 Net assets to MCR ratio: actual position, 2003–04 to 2007–08; and projections,
2002–03 to 2007–08
Source: Derived from MDO-owned insurers by the ACCC.

Medical indemnity insurance report—Sixth monitoring report
46
This chart shows that the 2003–04 projections forecast that the medical indemnity insurance
industry would have a net asset position of 119 per cent of MCR at 30 June 2004, rising to
151 per cent by 30 June 2008. Subsequent projections of the 30 June 2008 net assets-to-MCR
ratio show increases in levels for each updated projection. The 2007–08 projections forecast the
MCR coverage to be 260 per cent at 30 June 2008 and then to gradually decrease to 229 per cent
by 30 June 2012.
The actual net asset to MCR ratio of the medical indemnity industry at 30 June 2008 of 296 per cent
was higher than all prior projections.
As at 30 June 2008 all insurers have exceeded the original target and, from 1 July 2008, the
advisory target of 150 per cent MCR coverage required by APRA.
82
The ACCC notes that, for the 2007–08 underwriting year, one insurer scheduled to inject capital to
maintain its net assets to MCR ratio.
Capital injections from the parent entity can be an effective way to raise capital compared with
retained surplus from insurance premiums
83
; further, it may also represent a more efficient way to use
otherwise unused capital in not-for-profit organisations, such as MDOs.
84
Forecasts show that capital injections funded through a combination of subscriptions and unused
capital from the MDO allow the insurer to meet its internal target capital levels in the planning period.
The ACCC found that this approach is commercially justified.
82 APRA’s transitional arrangements enable medical indemnity providers to build capital up to APRA’s targeted capital level by
30 June 2008. Effective 1 July 2008, APRA advised in practice note GPG 100 that medical indemnity insures are expected
to maintain a capital ‘buffer’ of at least 150 per cent.
83 Raising capital through insurance premiums incurs a 10 per cent GST, stamp duty (which varies depending on the
jurisdiction) and 5 per cent run-off cover scheme (ROCS) levy (before 1 July 2008 it was 8.5 per cent). Income tax is also
charged on profit at 30 per cent.
Alternatively, subscriptions raised through the parent MDO do not incur stamp duty or the ROCS levy and, as they operate
as not-for-profit organisations, only incur income tax on investment returns.
84 MDOs are not subject to the same prudential requirements as the licensed insurer and as such have a lesser statutory
obligation to hold free capital.

Medical indemnity insurance report—Sixth monitoring report
47
6.3.4 Return on net assets
The ACCC assessed the returns of MDO-owned medical indemnity insurers relative to their net
asset position and compared these with the projection years between 2002–03 and 2007–08.
This
is shown in chart 6.4.
Chart 6.4 shows that the 2003–04 projections forecast the return on net assets to decrease from
64 per cent in 2003–04 to 13 per cent in 2007–08. A decline in the return on net assets was
reflected in all projections, aside from 2007–08. The 2007–08 projections show that return on net
assets is expected to increase from 1 per cent in 2008–09 to 6 per cent in 2011–12.
The return on net assets was projected to decrease because insurers initially raised significant
surpluses to fund capital requirements when their asset bases were low. However, once those
capital targets are achieved, the required surplus is reduced.
85
The 2007–08 projections of return on
net assets reflect the industry maturing and meeting its required capital targets.
85 This is further influenced by the fact that the net asset position of insurers increases as they approach their capital targets.
2002–03 projections 2003–04 projections 2004–05 projections 2005–06 projections
2006–07 projections 2007–08 projections Actual results
Per cent
Financial year
2003–04
2004–05 2005–06 2006–07 2007–08 2008–09 2009–10 2010–11 2011–12
0
10
20
30
40
50
60
70
Chart 6.4 Return on net assets: actual position, 2003–04 to 2007–08; and projections,
2002–03 to 2007–08
Source: Derived from MDO-owned insurers by the ACCC.

Medical indemnity insurance report—Sixth monitoring report
48
The downward trend in the actual results is consistent with the projections. The actual return on
net assets of 4 per cent in 2007–08 is lower than projected because of poorer than expected
investment returns and higher than projected expenses for some insurers.
6.3.5 Underwriting performance
The ACCC examined the underwriting performance in the following terms.
Loss ratio—the total claims expense attributable to each financial year on claims arising from that •
or previous years as a proportion of gross premium revenue.
86
Expense ratio—the sum of all underwriting and general expenses (excluding reinsurance •
expenses) as a proportion of gross premium revenue.
Reinsurance ratio—the reinsurance expense as a proportion of gross premium revenue.•
Combined ratio—the sum of the loss and the expense ratio. A combined ratio of less than •
100 per cent indicates that a company makes an underwriting surplus (i.e. premiums more than
cover the cost of claims and operating expenses). A ratio greater than 100 per cent indicates
that the company has an underwriting loss.
87
The ACCC examined gross ratios, which show industry performance before the effect of
reinsurance, to assess the underlying underwriting profitability of the insurers. Net ratios were also
examined to assess the performance of that part retained by the insurers. Any difference between
the gross and the net ratio highlights the effect of reinsurance on the insurers.
Loss ratio
Charts 6.5a and 6.5b show the gross and net loss ratios for MDO-owned insurers based on the
financial projections of insurers between 2002–03 and 2007–08. They also show the actual loss
ratios for 2003–04 to 2007–08.
86 As the loss ratio for the financial year includes any loss or surplus for previous underwriting years, this measure does not
necessary provide a good indicator of the profitability of the current underwriting year.
87 Analysis of underwriting performance may not necessarily indicate an insurer’s overall profitability because of the exclusion of
investment income.

Medical indemnity insurance report—Sixth monitoring report
49
2002–03 projections 2003–04 projections 2004–05 projections 2005–06 projections
2006–07 projections 2007–08 projections Actual results
Loss ratio (per cent)
Financial year
2003–04
2004–05 2005–06 2006–07 2007–08 2008–09 2009–10 2010–11 2011–12
0
20
40
60
80
100
120
Chart 6.5a Gross loss ratio: actual position, 2003–04 to 2007–08; and projections,
2002–03 to 2007–08
Source: Derived from MDO-owned insurers by the ACCC.

Medical indemnity insurance report—Sixth monitoring report
50
Chart 6.5b Net loss ratio: actual position, 2003–04 to 2007–08; and projections,
2002–03 to 2007–08
Source: Derived from MDO-owned insurers by the ACCC.
Charts 6.5a and 6.5b show that the 2003–04 projections forecast that the gross loss ratio would
rise from 56 per cent in 2003–04 to 73 per cent in 2007–08, and the net loss ratio would rise from
51 per cent in 2003–04 to 75 per cent in 2007–08. Subsequent projections also forecast increasing
gross and net loss ratios. The 2007–08 projections forecast that the gross loss ratio will increase
from 89 per cent in 2008–09 to 97 per cent in 2011–12, and forecast that the net loss ratio will
increase from 69 per cent in 2008–09 to 80 per cent in 2011–12.
The actual gross loss ratio in 2007–08 of 51 per cent and actual net loss ratio of 48 per cent in
2007–08 were lower than projected. This was also the case in 2003–04, 2004–05, 2005–06 and
2006–07. Actual loss ratios have been lower than projections because actual premium income is
generally higher than projections and actual claims costs are generally lower than projections.
While the actual results have been lower than the projections, the upward trend in the net loss ratio
is broadly consistent with the trend observed in all projections.
2002–03 projections 2003–04 projections 2004–05 projections 2005–06 projections
2006–07 projections 2007–08 projections Actual results
Loss ratio (per cent)
Financial year
2003–04
2004–05 2005–06 2006–072007–082008–092009–10 2010–112011–12
0
20
40
60
80
100
120

Medical indemnity insurance report—Sixth monitoring report
51
Expense ratio
Charts 6.6a and 6.6b show the gross and net expense ratios for MDO-owned insurers based on
the 2002–03 to 2007–08 financial projections of insurers. They also show the actual expense ratios
from 2003–04 to 2007–08.
88
88 The ACCC has adjusted one insurer’s actual expense ratios to remove some APRA-approved transfers.
2002–03 projections 2003–04 projections 2004–05 projections 2005–06 projections
2006–07 projections 2007–08 projections Actual results
Expense ratio (per cent)
Financial year
2003–04
2004–05 2005–06 2006–072007–082008–092009–10 2010–112011–12
0
5
10
15
20
25
30
35
40
45
Chart 6.6a Gross expense ratio: actual position, 2003–04 to 2007–08; and projections,
2002–03 to 2007–08
Source: Derived from MDO-owned insurers by the ACCC.

Medical indemnity insurance report—Sixth monitoring report
52
Charts 6.6a and 6.6b show that the 2003–04 projections forecast the gross expense ratio would
be between 18 and 20 per cent and the net expense ratio would be between 22 and 24 per cent
between 2003–04 and 2007–08. The 2004–05 and 2005–06 and 2006–07 projections forecast
an increase in the level of gross and net expense ratio compared to the 2003-04 projections. The
2007–08 projections show that the gross expense ratio is expected to decrease from 31 per cent in
2008–09 to 29 per cent in 2011–12, and the net expense ratio is expected to decrease from
37 per cent in 2008–09 to 34 per cent in 2011–12.
The actual gross expense ratio of 30 per cent and the net expense ratio of 35 per cent in 2007–08
were slightly lower than projected.
Initial expense projections understated actual expenses. Recent forecasts now more accurately
reflect actual expenses and show an upward trend continuing in the short term.
The high expense ratio experienced in 2006–07 does not reflect the individual experience of all
insurers and mainly reflected abnormal expenses incurred by some insurers.
2002–03 projections 2003–04 projections 2004–05 projections 2005–06 projections
2006–07 projections 2007–08 projections Actual results
Expense ratio (per cent)
Financial year
2003–04
2004–05 2005–06 2006–072007–082008–092009–10 2010–112011–12
0
5
10
15
20
25
30
35
40
45
Chart 6.6b Net expense ratio: actual position, 2003–04 to 2007–08; and projections,
2002–03 to 2007–08
Source: Derived from MDO-owned insurers by the ACCC.

Medical indemnity insurance report—Sixth monitoring report
53
Reinsurance ratio
Chart 6.7 shows the reinsurance ratio for MDO-owned insurers based on the 2002–03 to 2007–08
financial projections of insurers. It also shows the actual reinsurance ratio for 2003–04 to 2007–08.
The chart shows that the 2003–04 projections forecast reinsurance ratios would be between
16 and 19 per cent between 2003–04 and 2007–08. Subsequent forecasts for 2007–08 predicted
that the reinsurance ratio would remain between 15 and 18 per cent. The actual reinsurance ratio for
the industry of 13 per cent in 2007–08 is lower than projected, which mainly reflects the lower-than-
forecast reinsurance expenses experienced by some insurers.
The 2007–08 projections show that the reinsurance ratio is forecasted to remain relatively steady.
It is expected that the reinsurance ratio will increase from 15 per cent in 2008–09 to 16 per cent
in 2011–12.
2002–03 projections 2003–04 projections 2004–05 projections 2005–06 projections
2006–07 projections 2007–08 projections Actual results
Reinsurance ratio (per cent)
Financial year
2003–04
2004–05 2005–06 2006–072007–082008–092009–10 2010–112011–12
0
5
10
15
20
25
Chart 6.7 Reinsurance ratios: actual position, 2003–04 to 2007–08; and projections,
2002–03 to 2007–08
Source: Derived from MDO-owned insurers by the ACCC.

Medical indemnity insurance report—Sixth monitoring report
54
Combined ratio
Charts 6.8a and 6.8b show the gross and net combined ratios for MDO-owned insurers based on
projections from 2002–03 to 2007–08 provided by insurers. It also shows the actual combined ratios
for 2003–04 to 2007–08.
Chart 6.8a Gross combined ratio: actual position, 2003–04 to 2007–08; and projections,
2002–03 to 2007–08
2002–03 projections 2003–04 projections 2004–05 projections 2005–06 projections
2006–07 projections 2007–08 projections Actual results
Combined ratio (per cent)
Financial year
2003–04
2004–05 2005–06 2006–07 2007–08 2008–09 2009–10 2010–11 2011–12
0
20
40
60
80
100
120
140
Source: Derived from MDO-owned insurers by the ACCC.

Medical indemnity insurance report—Sixth monitoring report
55
The chart shows that the 2003–04 projections forecast that the gross combined ratio would
increase from 74 per cent in 2003–04 to 91 per cent in 2007–08, and that the net combined ratio
would increase from 73 to 97 per cent for the same period. The upward trend is also reflected in
subsequent projections. The 2007–08 projections forecast the gross combined ratio will increase
from 121 per cent in 2008–09 to 125 per cent in 2011–12, and that the net combined ratio will
increase from 106 per cent to 115 per cent for the same period.
As noted in section 6.3.2, insurers have been raising significant surpluses to fund their capital
requirements. However, this is projected to decrease as insurers’ capital bases increase,
approaching APRA or internal capital targets. Combined ratios are therefore projected to increase,
because insurers expect to generate lower levels of surplus as capital targets are reached.
The projected gross and net combined ratios from 2008–09 to 2011–12 are generally over
100 per cent. While a combined ratio greater than 100 per cent indicates that an insurer is making a
loss on its underwriting activities, it should be noted that a combined ratio exceeding 100 per cent
may still be profitable for an insurance business once investment income is taken into account.
The actual gross combined ratio was 82 per cent and net combined ratio was 83 per cent in
2007–08. These are both lower than projected.
Chart 6.8b Net combined ratio: actual position, 2003–04 to 2007–08; and projections,
2002–03 to 2007–08
2002–03 projections 2003–04 projections 2004–05 projections 2005–06 projections
2006–07 projections 2007–08 projections Actual results
Combined ratio (per cent)
Financial year
2003–04
2004–05 2005–06 2006–072007–082008–092009–10 2010–112011–12
0
20
40
60
80
100
120
140
Source: Derived from MDO-owned insurers by the ACCC.
Medical indemnity insurance report—Sixth monitoring report
56
6.3.6 QBE
As discussed in section 6.2, data limitations meant that QBE was excluded from the general industry
analysis contained within this chapter.
The ACCC examined the commercial justification of QBE’s premiums by examining Invivo’s
financial projections and how these are consolidated within QBE’s professional indemnity insurance
business. The ACCC has also examined QBE’s objectives and intentions for its medical indemnity
insurance business.
Based on this analysis, the ACCC found that QBE’s premiums for the 2008 underwriting year were
commercially justified.
6.4 Conclusion
The ACCC found that the premiums set by MDO-owned insurers are commercially justified.
The net asset position of all insurers as at 30 June 2008 was an improvement on the strong position
observed as at 30 June 2007. This is evidenced by the actual net asset position for the MDO-owned
insurers being higher than forecasted as at 30 June 2008.
Since the ACCC’s first medical indemnity premium monitoring report, MDO insurers have steadily
increased their net assets to reach their capital target levels. This was achieved through the surplus
that MDO insurers generated through their insurance business and, in some instances, capital
injections. As they increase their net assets, MDO insurers have reduced the surplus generated from
premiums. The lower levels of surpluses are reflected in reductions in the return on assets as they
have matured. As at 30 June 2008, all MDO insurers have met the 150 per cent MCR coverage as
required by APRA.
The ACCC notes that one insurer has scheduled future capital injections to maintain its target net
asset-to-MCR ratio. Based on forecasts provided by the insurer, the ACCC found that this approach
is currently commercially justified.
The ACCC also separately analysed QBE’s 2008 premiums and found them commercially justified.

Medical indemnity insurance report—Sixth monitoring report
57
7 Actuarial and commercial
justification of medical indemnity
premiums within each jurisdiction
This chapter presents findings by the Australian Competition and Consumer Commission (ACCC) on
the actuarial and commercial justification of medical indemnity premiums charged for the 2008–09
underwriting period
89
within each jurisdiction by the five authorised providers of medical indemnity
insurance to private medical practitioners as at 30 June 2008.
7.1 Qualifications
In preparing this analysis it was necessary for the ACCC to maintain confidentiality of information
provided by individual insurers. As noted in section 2.3, medical indemnity providers have largely
continued the tradition of providing insurance primarily in their home states.
90
Because of this, some
quantitative aspects of the ACCC analysis of the jurisdictional premiums could not be disclosed in
this report.
7.2 Background
7.2.1 Findings of previous ACCC monitoring reports
In its first and second monitoring reports, the ACCC’s assessment of the actuarial and commercial
justification of premiums examined the determination of the aggregate premium pool and, to a lesser
extent, the relativities applied to that pool for individual specialties, jurisdictions and income bands.
The ACCC’s third, fourth, fifth and sixth monitoring reports separately examined the actuarial and
commercial justification of jurisdictional relativities for the 2005–06, 2006–07, 2007–08 and 2008–09
underwriting periods. These reports all found that jurisdictional premium relativities were considered
actuarially and commercially justified for all monitored insurers.
For the sixth monitoring report, the ACCC has again separately examined the actuarial and
commercial justification of jurisdictional relativities.
89 The 2008 calendar year in the case of 1 January renewal Avant Insurance Limited (AIL) members and Invivo/QBE Insurance
(Australia) Limited (QBE) policyholders.
90 As noted in section 2.3, some insurers now have a large portion of their membership outside their home state. However, the
home state still generally represented the largest proportion of their membership base.
Medical indemnity insurance report—Sixth monitoring report
58
7.2.2 Pricing medical indemnity insurance by jurisdiction
To understand how jurisdictional relativities are derived and applied, it is important to understand the
overall process adopted by insurers when determining individual premiums.
The pricing process typically adopted by the four medical defence organisation (MDO)-owned
insurers involves each insurer determining the aggregate premium pool. The aggregate premium
pool typically includes:
the expected net cost of claims covered by the individual insurance policies issued in the current •
underwriting period, plus
an appropriate risk margin on the expected claims costs, which is intended to reflect the •
uncertainty in the expected claims costs, plus
expenses expected to be incurred in respected of business written in the current underwriting •
period, plus
the gross cost of reinsurance for the current underwriting period, • plus
future expenses required to administer claims arising in future years, • less
investment income earned on premiums until the date of payment of claims and expenses.•
Once an insurer has determined the aggregate premium pool, it will determine the risk relativities.
As with other types of insurance, the risk profile of the insured is an important determinant when
setting individual premium rates. Typically the higher the risk profile of the medical practitioner, the
higher the premium considered necessary to cover the cost of expected future claims.
Medical indemnity insurers typically base the risk profile of the medical practitioner for ratings
purposes according to several factors:
Medical specialty—medical practitioners who practise relatively more complex medical •
procedures are likely to face a higher risk of medical negligence claims being made against them
than ones who perform less complex procedures. The complexity of medical procedures is also
a key determinant of the size of medical negligence claims. Because of this, medical indemnity
insurers will group medical specialties together, based on their risk for rating purposes. The level
of grouping varies across medical indemnity insurers, with some recording relatively few groups
and others incorporating almost 100 specialty groups in their relativity pricing.
Income band/gross billing level—premium relativities are also determined on the basis of income/•
gross annual billings generated by the medical practitioner. Insurers regard this as a crude but
equitable way to assess the relative amounts of clinical practice undertaken and therefore the
risk the insurer is exposed to.
Jurisdiction in which a practice is located—the location of a doctor’s clinical practice also •
influences the premium relativity. This may reflect the different legislative requirements between
jurisdictions as well as the claims experience the insurer holds in different jurisdictions.
Insurers apply the jurisdictional relativities to premiums by applying a loading or a discount to
their premiums in their home jurisdiction.

Medical indemnity insurance report—Sixth monitoring report
59
In some instances, such as when insurers have a small membership in some categories, it can be
difficult to accurately determine ratings factors for medical specialities, income bands or jurisdictional
relativities because of a lack of statistically robust claims experience on which to base relativities.
One insurer is now able to rate several states based on its own claims experience.
QBE Insurance (Australia) Limited’s pricing methodology
91
differs from that outlined above for the
four MDO-owned insurers because it determines jurisdictional relativities based on available industry
data. As such, the ACCC has considered QBE’s jurisdictional premium relativities relative to industry
jurisdictional premium relativities, as opposed to preparing a separate analysis as discussed in
chapters 5 and 6.
7.2.3 Premium relativities
To obtain an understanding of the actual relativities applied between jurisdictions the ACCC
obtained information from the four MDO-owned insurers
92
on the gross written premium and
membership numbers by individual jurisdiction for the underwriting years 2003–04 to 2008–09.
93
This information allowed the ACCC to examine the average written premium in each jurisdiction
across the six underwriting years to determine the relativities between jurisdictions as well as any
changes in those relativities.
Chart 7.1 shows the average written premium of the four MDO-owned insurers by jurisdiction in
real terms across the six years.
94,95
91 QBE’s pricing methodology is described in detail in section 5.4.1.
92 The ACCC was also provided with information on QBE’s gross written premium and policyholder numbers; however, as
this data was only available for three underwriting years, it has not been incorporated in the ACCC’s historical analysis of
jurisdictional premiums.
93 The ACCC asked insurers to provide the gross written premium and membership numbers at a specific date in the
2008–09 underwriting year to allow insurers to provide data before the end of the underwriting year. However, because the
majority of insurance is written at the beginning of the underwriting year, the data should provide a reasonable estimate of
the full year’s results.
94 The ACCC prepared the average written premium analysis by jurisdiction by examining the average written premium of
each of the four MDO-owned medical indemnity providers and then averaging the result across all four. As noted in
section 2.3, some medical indemnity providers have largely continued the tradition of providing insurance primarily in their
home states. Because of this, presenting a weighted average written premium by jurisdiction may lead to results being
driven by individual insurers within their home states. The ACCC deemed the methodology adopted necessary to maintain
confidentiality of data.
95 The average written premium by jurisdiction is presented on a real basis to reflect the impact of inflation with nominal
premiums adjusted to 30 June 2008 values using the average weekly earnings index published by the Australian Bureau of
Statistics (catalogue number 6302.0).
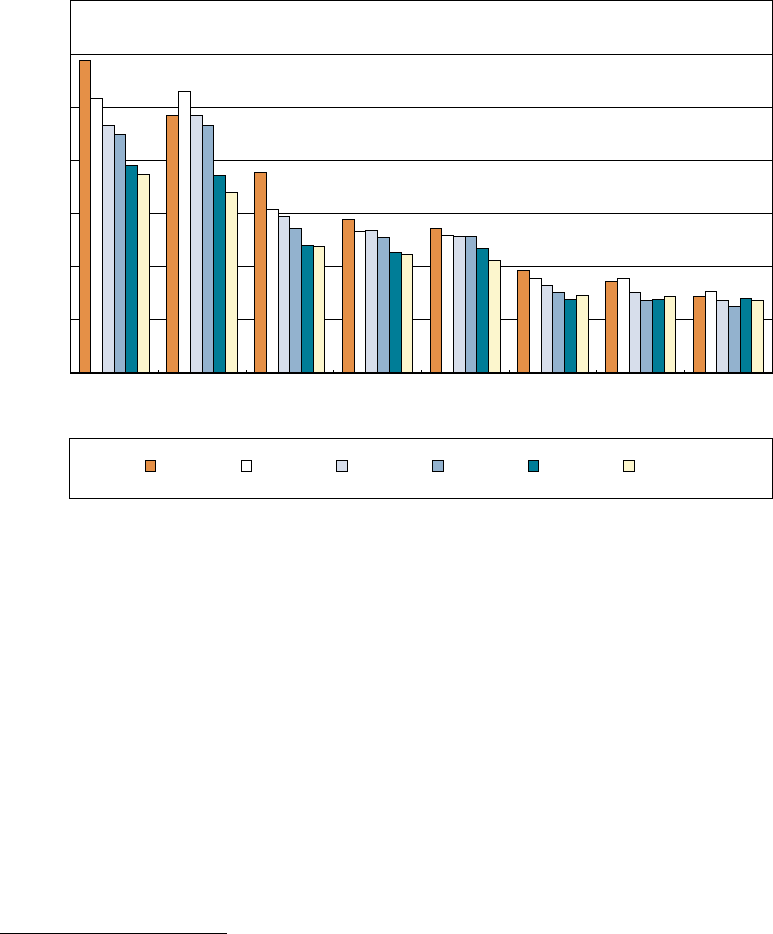
Medical indemnity insurance report—Sixth monitoring report
60
Chart 7.1 Average written premium in real terms by jurisdiction, 2003–04 to 2008–09
Source: Derived from MDO-owned insurers by the ACCC.
Chart 7.1 shows that the real average written premium in 2008–09 is highest in New South Wales
and the Australian Capital Territory and lowest in South Australia and the Northern Territory.
The chart also shows that in 2008–09 the real average written premium decreased in a majority
of jurisdictions, ranging from less than 1 per cent in the Queensland to 10 per cent in Western
Australia. The chart also shows that in 2008–09 the real average written premium increased in
Tasmania and South Australia, by 6 per cent and 4 per cent respectively.
Overall, according to chart 7.1, average premiums have decreased in 2008–09.
96
This analysis
may be influenced by differences in the medical practitioner membership between jurisdictions.
For example, some jurisdictions may have a higher proportion of low-risk specialties, which may
lead to those jurisdictions having a lower comparable average written premium. Further, some
jurisdictions may have more medical practitioners on non-mature claims-made policies
97
, resulting
in these jurisdictions having a lower comparable average written premium.
96 The jurisdictional average written premium is calculated as the total gross written premium for a particular year for a
particular jurisdiction, divided by the total membership for that jurisdiction. The national average written premium is
calculated in the same manner.
97 Under a claims-made policy the insurer agrees to indemnify all claims arising from incidents notified during the policy
period, as long as the incident occurred during the current period or any prior periods in which the policyholder has held
continuous claims-made cover with the insurer up to, and including, the current period. Because of the more limited period
the insurer is ‘on-risk’, this product is discounted during the earlier years until the policy becomes ‘mature’, which is typically
four to five years.
2003–04 2004–05 2005–06 2006–07 2007–08 2008–09
$–
$2000
$4000
$6000
$8000
$10 000
$12 000
$14 000
NSWACT QldVic.WATas.SANT

Medical indemnity insurance report—Sixth monitoring report
61
The ACCC also examined the observed jurisdictional premium relativities used by the five authorised
insurers (including QBE) for the 2008–09 underwriting year by examining the premium rates actually
set across jurisdictions. Specifically, the ACCC compared all equivalent mature claims-made
premium categories (including specialties and income bands) between the home state of each
insurer and other jurisdictions.
As noted previously, insurers apply the jurisdictional relativities to premiums by applying a loading
or discount to premiums in their home jurisdiction. As each insurer generally had a different home
jurisdiction to which other jurisdictions were compared, the ACCC compared each jurisdiction’s
premium relativity to the average premium relativities by jurisdiction across all insurers. Chart 7.2
shows the average industry observed jurisdiction relativities for all insurers (including QBE) for the
2008–09 underwriting year.
Chart 7.2 Average observed jurisdictional relativity, 2008–09
98
Source: Derived from all medical insurers (including QBE) by the ACCC.
Chart 7.2 shows that New South Wales and the Australian Capital Territory had the highest
jurisdictional premiums relative to the national average (at 24 and 20 per cent respectively), while
Tasmania has the lowest (at –16 per cent). The premiums relative to the national average for the
remaining jurisdictions ranged from between –4 per cent to –7 per cent.
98 The relative percentages refer to the premiums of a specific state relative to the national premium average.
–20
–10
0
10
20
30
NSWACT VICQLD WA NT SA TAS
Jurisdiction
Per cent

Medical indemnity insurance report—Sixth monitoring report
62
Jurisdictional premium relativities exist because, for a variety of procedural and social reasons,
the level of common law awards and settlements varies between states.
99
As claims costs is one of
the largest components of premiums, this will be a significant driver of premium differences between
jurisdictions.
Despite the different methodologies adopted in charts 7.1 and 7.2, the results are similar—New
South Wales and the Australian Capital Territory have the highest relativities while Tasmania, South
Australia and the Northern Territory have the lowest relativities. The remaining jurisdictions showed
some differences between the analyses, which may result from chart 7.1 being influenced by
different proportions of specialties and claims-made membership in each jurisdiction.
7.3 Actuarial and commercial justification of premium
relativities by jurisdiction
The ACCC examined the actuarial and commercial justification of the jurisdictional relativities applied
for the 2008–09 underwriting year by the five current insurers.
The ACCC found that most insurers who underwrote medical indemnity insurance in 2008–09
analysed whether changes should be made to jurisdictional relativities. However, most insurers
indicated that their analysis was limited by a lack of sufficient claims experience in some jurisdictions.
Partly reflecting this data issue, only two insurers that provided medical indemnity insurance in
2007–08 decided to change their existing jurisdictional relativities in the 2008–09 underwriting year.
One insurer had set interim jurisdictional premiums and another separately analysed premiums for
a specific jurisdiction.
7.3.1 Actuarial justication of jurisdictional relativities
Methodology
The ACCC examined the actuarial justification of premium relativities for the 2008–09 underwriting
year.
100
Specifically the ACCC examined the:
extent and level of detail of analysis to confirm or modify existing relativities•
extent to which insurers considered tort law reform in setting their jurisdictional relativities.•
Extent of analysis in determining jurisdictional relativities
Insurers generally adopted the same broad process for determining jurisdictional relativities, which
involved examining historical claims experience within each jurisdiction.
The extent to which this analysis was conducted varied across insurers. The majority of insurers
conducted a detailed analysis by comparing loss ratios for different jurisdictions to derive the
jurisdictional relativities for the 2008–09 underwriting year. Other insurers generally based their
analysis on reviews of detailed jurisdictional analysis prepared in previous years.
99 Institute of Actuaries Australia, submission to the Public Liability Forum, March 2002, p. 9.
100 The 2008 calendar year in the case of 1 January renewal AIL members and Invivo/QBE policyholders.

Medical indemnity insurance report—Sixth monitoring report
63
As noted in earlier ACCC monitoring reports, insurers, especially smaller insurers, generally
experienced some difficulties in accurately determining jurisdiction-based premium relativities
because of a lack of sufficient jurisdiction-based claims experience. Therefore, most insurers
made relatively simple estimates and included a flat loading or discount on premiums for medical
practitioners outside their home jurisdictions. All insurers experienced difficulties associated with a
lack of sufficient jurisdiction-based claims experience for some states and territories.
Relativities were adjusted by some insurers in some jurisdictions. These adjustments were based
on analysis of emerging claims experience.
The ACCC had previously determined that the approaches adopted by insurers to determine
jurisdictional relativities are actuarially justified given the absence of sufficient jurisdiction-based
claims experience.
Interim arrangements were introduced according to information provided by one insurer.
The approach adopted was considered reasonable with the expectation that detailed actuarial
assessments will continue.
Tort law reform
Most insurers commented on the impact of tort law reform, which has generally led to decreases in
the cost of claims. Allowance for tort law reforms is achieved through the analysis of post-tort law
reform claims experience.
7.3.2 Commercial justication of jurisdictional relativities
Methodology
The ACCC examined the commercial justification of premium relativities for the 2008–09
underwriting year.
101
Specifically the ACCC examined:
a comparison of the actuary’s recommended jurisdictional relativities with the actual relativities •
adopted, with insurers being asked to explain material differences
the quantification of cross-subsidies (as well as the incorporation of board policy) in the •
recommended relativities.
Adoption of actuarial recommendations
Insurers generally used the approved actuary when determining jurisdictional relativities.
However, the timing of the actuary’s involvement differed across insurers, with some insurers relying
on advice from their actuary to determine and recommend relativities.
Interim arrangements were a consideration for one insurer. These arrangements acted to limit the
size of any increase or decrease experienced by members moving to new premiums.
101 The 2008 calendar year in the case of 1 January renewal AIL members and Invivo/QBE policyholders.
Medical indemnity insurance report—Sixth monitoring report
64
The ACCC found that final relativities, as selected or approved by the actuary, were generally
adopted by all insurers in their final rates. The ACCC also found the interim premium relativities set
by one insurer were appropriate.
Quantication of cross-subsidies and incorporation of board policy
No insurer specifically quantified cross-subsidies between jurisdictions. However, because of a lack
of a sufficient volume of jurisdiction-based claims experience, some cross-subsidies may exist but
were not identified. As insurers continue to expand and gain greater experience in new jurisdictions,
more technical relativities can be derived and these potential cross-subsidies can be addressed.
7.4 Conclusion
The ACCC found that jurisdictional premium relativities were considered actuarially and commercially
justified for the five insurers operating as at 30 June 2008.
For the actuarial justification of premium relativities, the ACCC considered the extent of the
analysis used to determine the relativities, as well as the extent to which insurers took into account
jurisdictional variations in tort law reform. The ACCC found that insurers’ analyses were limited to an
extent because of a lack of sufficient claims experience in some jurisdictions. The ACCC has also
found that insurers have implicitly accounted for tort law reform through post-tort law reform claims
analysis. In the absence of a sufficient volume of claims data, the ACCC considered the approach
used by insurers to be actuarially justified.
For the commercial justification of premium relativities, the ACCC considered the extent to which
relativities recommended by actuaries were adopted in final premium rates as well as the level
of cross-subsidisation in the premium relativities. The ACCC found that that in some instances
recommendations were not adopted in final premium rates because of a lack of sufficient
claims experience in some jurisdictions. The ACCC also found that interim arrangements were
a consideration for one insurer. While no insurers reported explicit cross-subsidies between
jurisdictions, some cross-subsidies may exist because of the lack of a sufficient volume of claims
experience. The ACCC considers that the relativities adopted are commercially justified.

Medical indemnity insurance report—Sixth monitoring report
65
Appendix A ACCC information request
To fulfil its monitoring requirements, it was necessary for the Australian Competition and Consumer
Commission to approach medical indemnity providers directly to request relevant information.
In consultation with am actuaries, the ACCC developed a uniform information request for the four
medical defence organisation (MDO)-owned insurers to complete.
102
This appendix briefly describes the nature of the reports and information the ACCC requested
from insurers.
A.1 Actuarial pricing report
Insurers generally commissioned actuarial pricing reports for premiums to apply for the 2008–09
underwriting year. These reports provide advice to the insurer on the aggregate premium pool and,
in some cases, specialty rates. The ACCC requested a copy of this report.
As there are currently no guidelines on the content or level of detail to be contained in this report,
the ACCC outlined the scope and detail it wanted covered in these reports. Specifically, the ACCC
requested that the report include additional commentary on two areas.
First, the ACCC requested commentary on the effects (if any) of government reforms on the actuarial
assessment performed for the indemnity provider, including but not limited to:
the high cost claims scheme (HCCS)•
the run-off cover scheme (ROCS)•
tort law reform enacted in various jurisdictions.•
Second, the ACCC requested commentary on the derivation of premium relativities for each
classification factor used, including jurisdictional, speciality and income band relativities.
A.2 Actual premium rate report
The ACCC requested a report detailing the actual premiums charged for all forms of indemnity for
the 2008–09 underwriting year. If actual premium rates differed from those set out in the actuarial
pricing report, the insurer was asked to detail the reasons for these differences. This discussion was
to include all relevant commercial and regulatory factors affecting the pricing decisions made by the
indemnity provider.
As with the actuarial pricing report, the ACCC asked insurers to comment specifically on any effects
of the following government reforms on the actual premium rates being charged:
the HCCS•
the ROCS•
tort law reform enacted in various jurisdictions.•
102 The ACCC modified its information request for Invivo, which, as the authorised representative of QBE Insurance (Australia)
Limited, provided information to the ACCC on QBE premiums.

Medical indemnity insurance report—Sixth monitoring report
66
A.3 Membership, premium and claims data
The ACCC also requested the following data from insurers:
Membership data
Membership numbers by membership category, jurisdiction and income band for the 2007–08•
103
and 2008–09 underwriting years.
Premium data
Recommended individual actuarial subscription rates by membership category, jurisdiction and •
income band for the 2008–09 underwriting year.
Actual subscription rates by membership category, jurisdiction and income band for the 2008–09 •
underwriting year.
Total gross written premium by membership category and jurisdiction for the 2007–08•
104
and
2008–09 underwriting years.
Claim data
The total number of claims (including incidents likely as well as open and closed claims), the •
total amount of claims paid to date and the actuarial outstanding claims liability (inflated but
undiscounted) as at 30 June 2008.
A.4 Other information
The ACCC also requested the following information to assist in its monitoring role:
the most recent financial condition report, which is submitted to the Australian Prudential •
Regulation Authority on an annual basis and provides a comprehensive overview of the insurer’s
financial soundness
copies of financial projections prepared by the authorised insurer in 2007–08 as well as any •
updates to these projections
recent annual reports for both the insurer and the MDO group of companies•
a brief outline of any changes to the insurance policies previously offered to medical practitioners •
for the 2008–09 indemnity period.
103 While information on membership numbers was also provided by insurers for the 2007–08 underwriting year in the context
of the previous monitoring request, generally this information was provided at a specific time and may not reflect the actual
result for the full year. As such the ACCC sought revised data where this was available.
104 While information on premium rates was also provided by insurers for the 2007–08 underwriting year in the context of the
previous monitoring request, generally this information was provided at a specific time and may not reflect the actual result
for the full year. As such the ACCC sought revised data where this was available.
Medical indemnity insurance report—Sixth monitoring report
67
Appendix B Differences with APRA reports
The Australian Prudential Regulation Authority produces reports from its national claims and policies
database that cover professional indemnity and public and product liability insurance. The NCPD
reports provide an overview of professional indemnity and public and product liability insurance
based on information provided by Australian APRA-regulated general insurers.
It is not possible to directly compare information in Australian Competition and Consumer
Commission (ACCC) and NCPD reports because of differences in the methodologies used to
produce the reports. These differences include the following:
The ACCC and NCPD reports are based on different reference periods. The latest NCPD •
information is based on the 2006 calendar year while the ACCC data is generally presented on a
financial year basis.
The ACCC analysis of premiums includes data from medical defence organisation (MDO)-owned •
insurers, with the main focus on insurance for medical practitioners. The NCPD report includes
data from all insurers that underwrite medical indemnity and therefore includes insurance
premiums for other health professionals (such as optometrists and dentists) that are generally
outside the scope of the ACCC’s monitoring report.
Some of the medical indemnity premium information in the ACCC report is provided in real terms •
with data adjusted using the average weekly earnings index published by the Australian Bureau
of Statistics (catalogue number 6302.0). The NCPD data is unadjusted.
These differences will affect the size of average premium calculations in the ACCC and NCPD
reports. The trends in the data may also be affected.
Medical indemnity insurance report—Sixth monitoring report
68
ACCC contacts
Infocentre: 1300 302 502
Website: www.accc.gov.au
Callers who are deaf or have a hearing or speech impairment can contact the ACCC through the
National Relay Service: www.relayservice.com.au.
Voice-only (speak and listen) users—phone 1300 555 727 and ask for 1300 302 502.
Addresses
National office
23 Marcus Clarke Street
Canberra ACT 2601
GPO Box 3131
Canberra ACT 2601
Tel: (02) 6243 1111
Fax: (02) 6243 1199
New South Wales
Level 7, Angel Place
123 Pitt Street
Sydney NSW 2000
GPO Box 3648
Sydney NSW 2001
Tel: (02) 9230 9133
Fax: (02) 9223 1092
Victoria
Level 35, The Tower
360 Elizabeth Street
Melbourne Central
Melbourne Vic 3000
GPO Box 520
Melbourne Vic 3001
Tel: (03) 9290 1800
Fax: (03) 9663 3699
Queensland
Brisbane
Level 3, 500 Queen Street
Brisbane Qld 4000
PO Box 10048
Adelaide Street Post Office
Brisbane Qld 4000
Tel: (07) 3835 4666
Fax: (07) 3832 0372
Townsville
Level 6, 370 Central Plaza Building
Flinders Mall,
Townsville Qld 4810
PO Box 2016
Townsville Qld 4810
Tel: (07) 4729 2666
Fax: (07) 4721 1538
Western Australia
3rd floor, East Point Plaza
233 Adelaide Terrace
Perth WA 6000
PO Box 6381
East Perth WA 6892
Tel: (08) 9325 0600
Fax: (08) 9325 5976
South Australia
Level 2, 19 Grenfell Street
Adelaide SA 5001
GPO Box 922
Adelaide SA 5001
Tel: (08) 8213 3444
Fax: (08) 8410 4155
Northern Territory
Level 8, National Mutual Centre
9–11 Cavenagh St
Darwin NT 0800
GPO Box 3056
Darwin NT 0801
Tel: (08) 8946 9666
Fax: (08) 8946 9600
Tasmania
3rd floor, AMP Building
86 Collins Street
(Cnr Elizabeth and Collins streets)
Hobart Tas 7000
GPO Box 1210
Hobart Tas 7001
Tel: (03) 6215 9333
Fax: (03) 6234 7796
