
AL
70
AZ
67
AR
67
CA
73
CO
69
CT 75
DE 73
FL
71
GA
70
ID
67
IL
67
IN
68
IA
71
KS
68
KY
70
LA
70
ME
75
MD 73
MA
76
MN
73
MS
64
MO
69
MT
65
NE
68
NV
62
NH
75
NJ 68
NM
63
NY
70
NC
71
ND
67
OH
68
OK
64
OR
72
PA
70
RI 75
SC
72
SD
69
TN
70
TX
62
UT
69
VT
71
VA
70
WA
72
WV
68
WI
74
WY
60
DC 74
HI
73
AK
62
MI
74
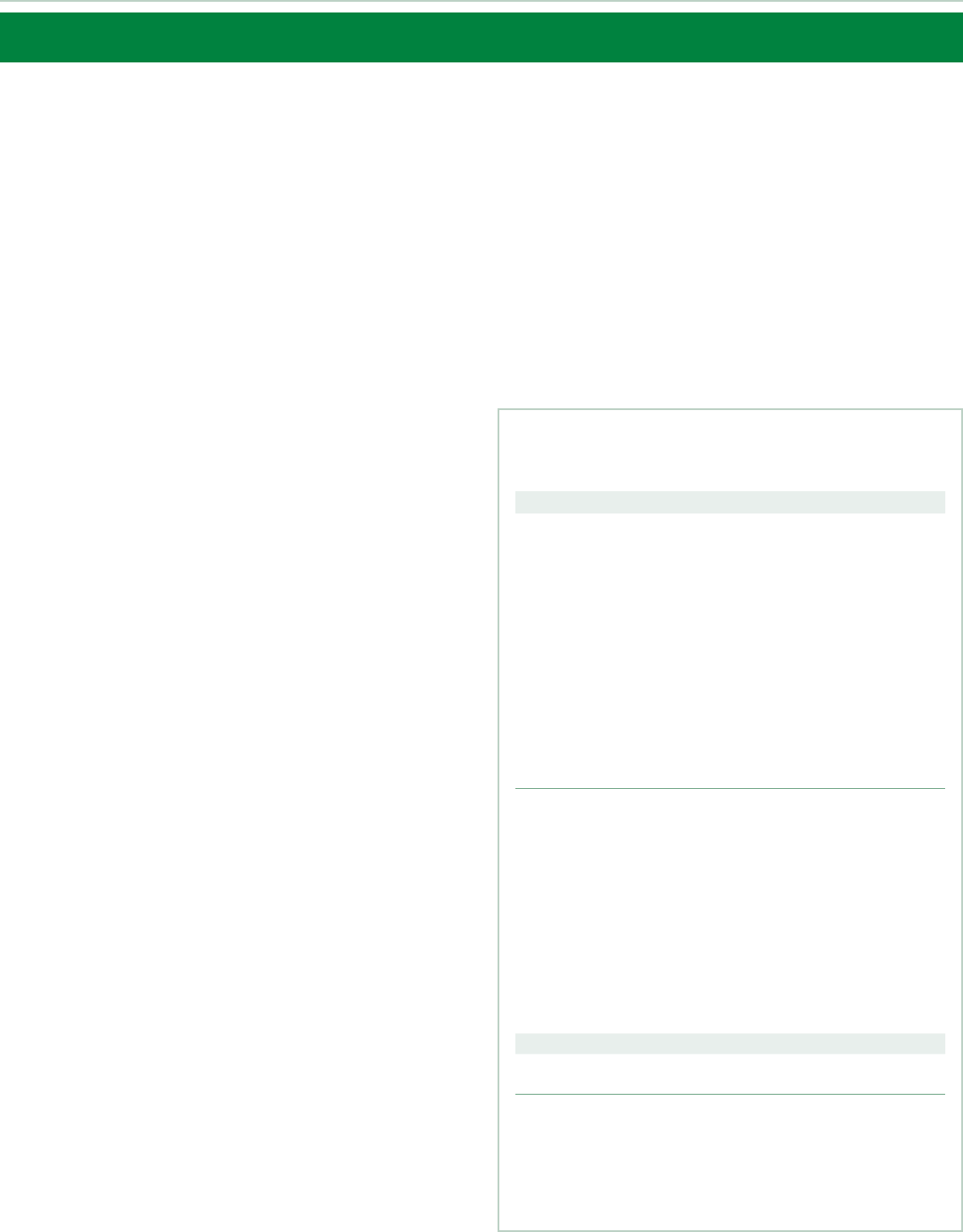
*Blood stool test, sigmoidoscopy, or colonoscopy in the past 1, 5, and 10 years, respectively.
Note: Estimates are age adjusted to the 2000 US standard population and do not distinguish between examinations for screening and diagnosis.
Source: Behavioral Risk Factors Surveillance System, 2018. See Sources of Statistics (page 32) for complete citation and more information.
Colorectal Cancer Screening Test Use* (%), Adults 50 Years and Older by State, 2018
PR
58
58% to 64%
65% to 69%
70% to 72%
73% to 76%
Colorectal Cancer
Facts & Figures 2020-2022
(page 32)

Contents
Colorectal Cancer Basic Facts 1
Figure 1. Anatomy of the Gastrointestinal System 1
Figure 2. Stages of Colorectal Cancer Growth 2
Colorectal Cancer Occurrence 3
Table 1. Estimated Number of Colorectal Cancer Cases
and Deaths in the US in 2020 by Age 3
Figure 3. Colorectal Cancer Incidence (2012-2016)
and Mortality (2013-2017) Rates by Subsite and Sex, US 4
Figure 4. Age-specific Colorectal Cancer Incidence Rates,
US, 2012-2016 4
Figure 5. Colorectal Cancer Incidence (2012-2016) and
Mortality (2013-2017) Rates by Race/Ethnicity and Sex, US 5
Figure 6. Trends in Colorectal Cancer Incidence (1975-2016)
and Mortality (1930-2017) Rates by Sex, US 6
Figure 7. Trends in Colorectal Cancer Incidence (1995-2016)
and Mortality (1970-2017) Rates by Age and Sex, US 7
Figure 8. Trends in Colorectal Cancer Incidence (1975-2016)
and Mortality (1970-2017) Rates by Race, US 8
Figure 9. Colorectal Cancer Incidence (2012-2016) and
Mortality (2013-2017) Rates by State, US 9
Table 2. Colorectal Cancer Incidence (2012-2016) and
Mortality (2013-2017) Rates by Race/Ethnicity and State, US 10
Figure 10. Colorectal Cancer Five-year Survival (%)
by Age and Race/Ethnicity, 2009-2015 11
Figure 11. Colorectal Cancer Stage Distribution (%) by Age
and Race/Ethnicity, 2012-2016 12
Colorectal Cancer Risk Factors 13
Table 3. Relative Risks for Established Colorectal Cancer
Risk Factors 13
Colorectal Cancer Screening 18
Table 4. Characteristics of Recommended Colorectal Cancer
Screening Tests 20
Table 5. Colorectal Cancer Screening (%), Adults 45 Years
and Older, US, 2018 23
Figure 12. Colorectal Cancer Screening (%), Adults 50 Years
and Older by State, 2018 24
Table 6. Colorectal Cancer Screening (%), Adults 50 Years
and Older by State, 2018 25
Colorectal Cancer Treatment 26
What Is the American Cancer Society Doing
about Colorectal Cancer? 30
Sources of Statistics 32
References 33
Global Headquarters: American Cancer Society Inc.
250 Williams Street, NW, Atlanta, GA 30303-1002
404-320-3333
©2020, American Cancer Society, Inc. All rights reserved,
including the right to reproduce this publication or
portions thereof in any form.
For permission, email the American Cancer Society
Legal department at permissionsrequests@cancer.org.
This publication attempts to summarize current scientific information about colorectal cancer.
Except when specified, it does not represent the official policy of the American Cancer Society.
Suggested citation: American Cancer Society. Colorectal Cancer Facts & Figures 2020-2022.
Atlanta: American Cancer Society; 2020.

Colorectal Cancer Facts & Figures 2020-2022 1
Colorectal Cancer
Basic Facts
What is colorectal cancer?
Cancer is a disease characterized by the unchecked
division of abnormal cells. When this type of growth
occurs in the colon or rectum, it is called colorectal
cancer (CRC). The colon and rectum (colorectum), along
with the anus, make up the large intestine, the final
segment of the gastrointestinal (GI) system. The large
intestine is sometimes called the large bowel, which is
why CRC is sometimes referred to as bowel cancer. The
function of the large intestine is to absorb water and
electrolytes from food matter and eliminate feces. As
depicted in
Figure 1
, the first part of the large intestine is
the colon, a muscular tube about 1.5 meters (5 feet) long
and 5 centimeters (2 inches) in diameter that is divided
into 4 sections:
• The ascending colon begins with the cecum (a pouch
where undigested food is received from the small
intestine) and extends upward on the right side of the
abdomen.
• The transverse colon crosses the body from right to
left, and is referred to collectively with the ascending
colon as the proximal, or right, colon.
• The descending colon descends on the left side.
• The sigmoid colon, named for its “S” shape, is the final
portion of the colon and is referred to collectively
with the descending colon as the distal, or left, colon.
Waste passes from the sigmoid colon into the rectum –
the final 15 centimeters (6 inches) of the large intestine –
and is then expelled through the anus (2-3 centimeters or
1 inch). Despite their anatomic proximity, cancers in the
anus are classified separately from those in the rectum
because they usually originate from different cell types,
and thus have different characteristics.
However, tumors within the colorectum also vary in their
molecular, biological, and clinical features, and in their
association with risk factors.
1, 2
For example, physical
inactivity is associated with increased risk of cancer in
the colon, but not in the rectum. In addition, patients are
more likely to be diagnosed with tumors in the proximal
colon if they are older (versus younger), black (versus
white), or female (versus male).
3, 4
What is a colorectal polyp?
CRC almost always begins as a polyp, which is a
noncancerous growth that develops in the mucosal layer
(inner lining) of the colon or rectum. Polyps are common,
detected in about half (including serrated polyps) of
average-risk individuals 50 years of age or older undergoing
colonoscopy, with higher prevalence in older age groups
and among men compared to women.
5
However, fewer
than 10% of polyps are estimated to progress to invasive
cancer,
6, 7
a process that usually occurs slowly over 10 to
20 years and is more likely as polyps increase in size.
8-10
Polyps are classified based on their growth pattern as
adenomatous (i.e., adenoma), which is the most common
cancer precursor, or serrated, so-called because of its
saw-toothed appearance under a microscope.
11
Serrated
Figure 1. Anatomy of the Gastrointestinal System
Esophagus
Stomach
Transverse
colon
Descending
colon
Sigmoid
colon
Ascending
colon
Anus
Liver
Small
intestine
Gallbladder
Rectum
Cecum
Appendix
©2017, American Cancer Society, Inc., Surveillance Research

2 Colorectal Cancer Facts & Figures 2020-2022
polyps are further subdivided based on biological
characteristics into sessile serrated polyps (SSPs),
traditional serrated adenomas (TSAs), and hyperplastic
polyps (HPs). Similar to adenomas, SSPs, TSAs, and large
HPs are associated with an increased risk for CRC. SSPs are
the most difficult to detect during colonoscopy because they
are usually flat, covered with a mucous cap, and colored like
the surrounding tissue. These features likely contribute to
their role as precursors for a large proportion of cancers
diagnosed prior to the next recommended colonoscopy
(interval or post colonoscopy cancers).
12
What are the stages of
colorectal cancer?
Once a polyp progresses to cancer, it can grow into the
wall of the colon or rectum where it may invade blood or
lymph vessels that carry away cellular waste and fluid
(
Figure 2
). Cancer cells typically spread first into nearby
lymph nodes, which are bean-shaped structures that help
fight infections. They can also be carried via blood vessels
to other organs and tissues, such as the liver or lungs,
13
or
be shed directly into the peritoneum (membrane lining
the abdomen).
14
The spread of cancer cells to parts of the
body distant from where the tumor started is called
metastasis.
The extent to which cancer has spread at the time of
diagnosis is described as its stage.
Staging is essential for determining
treatment choices and assessing
prognosis (prediction of disease
outcome). The two most common cancer
staging systems are the American Joint
Committee on Cancer (AJCC) tumor,
node, and metastasis (TNM) system,
typically used in clinical settings, and
the Surveillance, Epidemiology, and End
Results (SEER) summary staging system,
used for descriptive and statistical
analysis of tumor registry data. In this
document, we will describe CRC stages
using the SEER summary staging
system:
• In situ: Cancers that have not yet begun to invade the
wall of the colon or rectum; these preinvasive lesions
are not included in the cancer statistics provided in
this report
• Local: Cancers that have grown into the wall of the
colon or rectum, but have not extended through the
wall into nearby tissues
• Regional: Cancers that have spread through the wall
of the colon or rectum and have invaded nearby
tissue, or that have spread to nearby lymph nodes
• Distant: Cancers that have spread to other parts of
the body, such as the liver or lung
What are the symptoms of
colorectal cancer?
Early CRC often has no symptoms, which is one of the
reasons screening is so important. As a tumor grows, it
may bleed or block the intestine. The most common
symptoms are:
• Bleeding from the rectum
• Blood in the stool or in the toilet after having a
bowel movement
• Dark or black stools
Figure 2. Stages of Colorectal Cancer Growth
©2005, Terese Winslow
U.S. Govt. has certain rights

Colorectal Cancer Facts & Figures 2020-2022 3
• A change in bowel habits or the shape of the stool
(e.g., more narrow than usual)
• Cramping, pain, or discomfort in the lower abdomen
• An urge to have a bowel movement when the bowel
is empty
• Constipation or diarrhea that lasts for more than a
few days
• Decreased appetite
• Unintentional weight loss
In some cases, blood loss from the cancer leads to anemia
(low number of red blood cells), causing symptoms such
as weakness, excessive fatigue, and sometimes shortness
of breath. Timely evaluation of symptoms consistent with
CRC is essential for all individuals, regardless of age, given
the increasing incidence in young adults (see page 6).
Colorectal Cancer Occurrence
How many new cases and deaths are
estimated to occur in 2020?
In 2020, there will be an estimated 104,610 new cases of
colon cancer and 43,340 cases of rectal cancer diagnosed
in the US (
Table 1
). Although the majority of CRCs are in
adults ages 50 and older, 17,930 (12%) will be diagnosed in
individuals younger than age 50, the equivalent of 49 new
cases per day.
An estimated 53,200 people will die from CRC in 2020,
including 3,640 men and women younger than age 50.
Unfortunately, reliable statistics on deaths from colon
and rectal cancers separately are not available because
almost 40% of deaths from rectal cancer are misclassified
as colon cancer on death certificates.
15
The high level of
misclassification is partly attributed to the misconception
among some that the terms colon cancer and colorectal
cancer are synonymous because of the widespread use of
“colon cancer” to refer to both colon and rectal cancers in
educational messaging. To help mitigate the issue and be
more explicitly inclusive of rectal cancer patients, several
organizations have publicly ended this practice.
16
The
ability to study these deaths separately is increasingly
important given the steep rise in rectal cancer incidence
among younger adults.
17
How many people who have been
diagnosed with colorectal cancer are
alive today?
As of January 1, 2019, there were 776,120 men and 768,650
women alive in the US with a history of CRC.
18
About
one-third (35%) of these individuals were diagnosed
within the preceding 5 years, and more than half (56%)
were ages 65-84 years. Some of these people were cancer-
free, while others still had evidence of cancer and may
have been undergoing treatment.
What is the risk of developing
colorectal cancer?
Approximately 4.4% of men (1 in 23) and 4.1% of women
(1 in 25) will be diagnosed with CRC in their lifetime.
19
Lifetime risk is similar in men and women despite higher
incidence rates in men because women have longer life
expectancy. In addition to sex, age and race/ethnicity
also have a large influence on risk.
Table 1. Estimated Number of Colorectal Cancer Cases
and Deaths in the US in 2020 by Age
Cases Deaths*
Age Colorectum Colon Rectum Colorectum
0-49 years 17,93 0 11,5 40 6,390 3,640
50-64 years 50,010 32,290 17,720 13,380
65+ years 80,010 60,780 19,230 36,180
All ages 147,95 0 104,610 43,340 53,200
Estimates are rounded to the nearest 10 and exclude in situ carcinoma.
*Deaths for colon and rectal cancers are combined because a large number of
rectal cancer deaths are misclassified as colon.
©2020, American Cancer Society, Inc., Surveillance Research

4 Colorectal Cancer Facts & Figures 2020-2022
Sex
CRC incidence rates are 30% higher in men than in
women, with a larger disparity for rectal cancer (60%
higher) than for colon cancer (20% higher;
Figure 3
). As
expected, women also have a lower prevalence of both
adenomas overall and of advanced adenomas.
20, 21
However, among individuals 50 and older, women are
more likely than men to develop adenomas in the proximal
colon,
20
which are less efficiently detected through
screening.
22
Gender disparities likely reflect differences in
exposures to risk factors (e.g., cigarette smoking) and sex
hormones, as well as complex interactions between these
influences.
23
Notably, CRC incidence rates in men and
women younger than 45 years are comparable.
Age
Like most types of cancer, the risk of CRC increases with
age. For every subsequent 5-year age group, the incidence
rate approximately doubles until age 50, and thereafter
increases by about 30% (
Figure 4
). The exception is ages
50-54 years versus ages 55-59 years, for which there is only
a 15% difference (60 versus 68 per 100,000, respectively),
partly because the natural age-associated influence on
risk is disrupted by first-time CRC screening in the
younger age group. The screening effect is magnified in
current rates by single year of age (
Figure 4
), which are
actually higher in individuals ages 50-51 years than in
those ages 52-55 years. This phenomenon is absent in
incidence rates during the 1970s, prior to the uptake of
screening.
Source: Main figure: NAACCR, 2019. Inset: Surveillance, Epidemiology, and End Results (SEER) Program, 2019.
©2020, American Cancer Society, Inc., Surveillance Research
Rate per 100,000 population
Figure 4. Age-specific Colorectal Cancer Incidence Rates, US, 2012-2016
0
50
100
150
200
250
300
85+ years
80-84 years
75-79 years
70-74 years
65-69 years
60-64 years
55-59 years
50-54 years
45-49 years
40-44 years
35-39 years
30-34 years
25-29 years
20-24 years
15-19 years
10-14 years
5-9 years
0
10
20
30
40
50
60
70
80
59 years
58 years
57 years
56 years
55 years
54 years
53 years
52 years
51 years
50 years
0.1 0.3
0.9 1.5
3.0
5.7
10.5
19.0
33.1
59.5
68.4
90.2
121.4
153.0
197.5
237.9
258.8
Rates are ag
e adjusted to the 2000 US standard population. *Mortality rates by
anatomic subsite are not available because a large number of rectal cancer
deaths are misclassified as colon.
Sources: Incidence – North American Association of Central Cancer Registries
(NAACCR), 2019. Mortality – National Center for Health Statistics (NCHS), 2019.
©2020, American Cancer Society, Inc., Surveillance Research
Figure 3. Colorectal Cancer Incidence (2012-2016) and
Mortality (2013-2017) Rates by Subsite and Sex, US
Rate per 100,000 population
38.7
27.6
11.2
13.9
14.1
16.6
34.0
25.3
8.7
11.7
44.4
30.3
Sexes combined
FemaleMale
Incidence Mortality*
0
5
10
15
20
25
30
35
40
45
50
ColorectumRectumColonColorectum

Colorectal Cancer Facts & Figures 2020-2022 5
The median age at CRC diagnosis is 66 years in men and
69 years in women, but is younger for rectal cancer (age
62 and 63, respectively) than for colon cancer (age 67 and
71, respectively).
24
CRC patients overall are increasingly
younger, shifting from a median age of 72 years for
diagnoses in the early 2000s to 66 years today.
25
This is
because incidence is increasing in younger adults and
declining in older age groups.
17
Race/ethnicity
Among broadly defined racial and ethnic groups, CRC
incidence and mortality are highest in non-Hispanic
blacks (hereafter, blacks), followed closely by American
Indians and Alaska Natives (AIANs), and lowest in Asians/
Pacific Islanders (APIs;
Figure 5
). During 2012-2016, CRC
incidence rates in blacks were about 20% higher than
those in non-Hispanic whites (NHWs) and 50% higher
than those in APIs. The disparity for mortality is twice
that for incidence; CRC death rates in blacks are almost
40% higher than those in NHWs and double those in APIs.
Reasons for racial/ethnic disparities in CRC are complex,
but largely reflect differences in risk factor prevalence
and health care access, both of which are related to
socioeconomic status.
26
In 2018, the median family
income was $41,361 among blacks compared to $70,642
among NHWs, with 21% and 8%, respectively, living in
poverty.
27
People with the lowest socioeconomic status
are 40% more likely to be diagnosed with CRC than those
with the highest socioeconomic status.
28
Close to half
(44%) of this disparity is attributed to differences in the
prevalence of risk factors associated with CRC (e.g.,
smoking, obesity)
29
and a similar proportion is due to
differences in CRC screening.
30
After controlling for
differences in risk factors, black individuals are no more
likely than whites to develop adenomas or CRC, but are
less likely to receive timely follow-up of a positive screening
test and/or high-quality colonoscopy.
31, 32
Higher CRC
mortality among blacks may also reflect a larger
proportion of tumors in the proximal colon.
3
Importantly, the broad racial and ethnic groups to which
cancer statistics are generally limited mask striking
differences within these heterogeneous populations. For
example, although CRC incidence in API men overall is
25% lower than in NHW men, rates in Japanese men are
23% higher.
33
Even more alarming is the burden among
Alaska Natives, who have the highest CRC incidence (89
per 100,000) and mortality (40 per 100,000) rates in the
US, double those in blacks (46 and 19, respectively). CRC
AI: American Indian, excluding Alaska; AN: Alaska Native. Rates are age adjusted to the 2000 US standard population. *Statistics based on data from Purchased/Referred Care
Delivery Area (PRCDA) counties. AI/AN incidence rates exclude data from Kansas and Minnesota. Incidence rates for Alaska Native men and women are not statistically
significantly different.
Source: Incidence – NAACCR, 2019. Mortality – NCHS, 2019.
©2020, American Cancer Society, Inc., Surveillance Research
Rate per 100,000 population
Figure 5. Colorectal Cancer Incidence (2012-2016) and Mortality (2013-2017) Rates by Race/Ethnicity and Sex, US
Non-Hispanic White Hispanic/Latino Asian/Pacific IslanderNon-Hispanic Black
American Indian/Alaska Native*
45.7
43.3
38.6
34.1
30.0
53.8
48.5
44.0
40.9
35.3
39.9
39.1
33.9
28.7
25.7
19.0
15.8
13.8
11.1
9.5
23.8
19.4
16.3
14.1
11.4
15.6
13.0
11.7
8.7
8.1
0
10
20
30
40
50
60
WomenMenSexes combinedWomenMenSexes combined
0
20
40
60
80
100
WomenMenSexes
combined
AN
AI
89.0
40.7
85 .1
92.9
46.4
36.1
0
10
20
30
40
50
WomenMenSexes
combined
AN
AI
39.6
14.5
44.8
36.1
18.0
11. 8
MortalityIncidence

6 Colorectal Cancer Facts & Figures 2020-2022
has been the most commonly diagnosed cancer in Alaska
Natives since the early 1970s for reasons that are
unknown, but may include a higher prevalence of CRC
risk factors, such as a diet high in animal fat and low in
fruits and vegetables, vitamin D deficiency, smoking,
obesity, and diabetes.
34, 35
In addition, Alaska Natives,
particularly rural residents, have a high prevalence of
Helicobacter pylori (H. pylori),
36
a bacteria associated with
inflammation and cancer of the stomach that may also be
associated with CRC risk.
37, 38
Despite a disproportionately
high burden of advanced adenomas among Alaska
Natives,
39
the availability of endoscopic services in much
of Alaska is inadequate.
40, 41
A recent study found that
Alaska had the lowest county-level CRC screening
prevalence in the nation.
42
In addition, the primary mode
of screening at Indian Health Service facilities is stool
testing, which has a limited capacity for cancer prevention
and requires timely follow-up with colonoscopy for
positive tests. Notably, AIANs are the only racial and
ethnic group for which CRC mortality rates are not
declining (see page 8).
How has colorectal cancer occurrence
changed over time?
Incidence
Despite higher incidence in men than in women, trends
over time are very similar by sex (
Figure 6
). CRC incidence
rates increased from 1975 through the mid-1980s, but
since have generally decreased. The decline prior to 2000
is attributed equally to changing patterns in risk factors
(e.g., reductions in smoking) and the uptake of CRC
screening.
43
However, the accelerated decline that began
during the late 2000s is thought to predominantly reflect
widespread uptake of CRC screening with colonoscopy,
which increased among adults ≥50 years of age from 20%
in 2000 to 61% in 2018.
44
There is about a decade of lag
time between the detection and removal of precancerous
polyps through screening and its reflection on CRC
incidence rates.
9, 45
Notably, however, declines in CRC
incidence have decelerated in the most recent 5 data
years (2012-2016), perhaps reflecting a slowing in first-
time screening,
46
changing risk factors exposures, such
as obesity, or a combination thereof.
Age-specific incidence trends
CRC trends overall reflect the majority of cases that occur
in older age groups, masking trends in young adults. CRC
incidence rates have been increasing since the mid-1980s
in adults ages 20-39 years and since the mid-1990s in adults
ages 40-54 years, with younger age groups experiencing
the steepest increase.
17
This pattern is called a birth cohort
effect because generations of individuals with higher
incidence carry the elevated risk with them as they age.
Indeed, after decades of decline, incidence rates have also
begun to increase in ages 50-64 years. During the most
recent five data years (2012-2016), incidence rates increased
by 2.2% annually in individuals younger than 50 years
and by 1% annually in those ages 50-64 years, a sharp
contrast to declines of 3.3% per year in adults ages 65
and older (
Figure 7
). Although a similar incidence pattern
Rates are age adjusted to the 2000 US standard population. Incidence rates are
adjusted for delays in reporting and exclude appendix. Due to changes in
International Classification of Diseases (ICD) coding, numerator information for
mortality has changed over time.
Source: Incidence – Surveillance, Epidemiology, and End Results (SEER) Program,
2019. Mortality – US Mortality Volumes 1930 to 1959, US; Mortality Data
1960-2017, NCHS, 2019.
© 2020, American Cancer Society, Inc., Surveillance Research
Rate per 100,000 population
Figure 6. Trends in Colorectal Cancer Incidence
(1975-2016) and Mortality (1930-2017) Rates by Sex, US
Female mortality
Female incidence
Male incidence
0
10
20
30
40
50
60
70
80
90
201020001990198019701960195019401930
Male mortality
Year of diagnosis/death

Colorectal Cancer Facts & Figures 2020-2022 7
has been reported in many other high-income countries,
47
reasons for the increasing trend in younger age groups
are unknown. It may reflect changes in established risk
factors, such as a more sedentary lifestyle and/or
unfavorable dietary patterns, or other exposures whose
association with CRC risk is yet unknown.
Rates are age adjusted to the 2000 US standard population. Incidence rates are adjusted for reporting delays and exclude appendix.
Source: Incidence – NAACCR, 2019. Mortality – NCHS, 2019.
©2020, American Cancer Society, Inc., Surveillance Research
Rate per 100,000 population
Figure 7. Trends in Colorectal Cancer Incidence (1995-2016) and Mortality (1970-2017) Rates by Age and Sex, US
Ages 0-49
Incidence Mortality
Rate per 100,000 population
Ages 50-64
Rate per 100,000 population
Ages 65+
Male
Female
Male
Female
Rate per 100,000 population
Ages 0-49
Rate per 100,000 population
Ages 50-64
Rate per 100,000 population
Ages 65+
Male
Female
Male
0
2
4
6
8
10
20152010200520001995
0.0
0.5
1.0
1.5
2.0
2.5
3.0
2015201020052000199519901985198019751970
0
20
40
60
80
100
120
20152010200520001995
0
10
20
30
40
50
2015201020052000199519901985198019751970
0
50
100
150
200
250
300
350
400
450
20152010200520001995
0
50
100
150
200
250
2015201020052000199519901985198019751970
Male
Female
Female
Male
Female
Year of deathYear of diagnosis

8 Colorectal Cancer Facts & Figures 2020-2022
Racial/ethnic incidence trends
Historical cancer incidence data in the US are available
only for the categories white, black, and other race. CRC
incidence was similar in whites and blacks until the
mid-1980s, when rates began declining in whites while
remaining stable in blacks (
Figure 8
). These trends created
a widening racial gap until the mid-2000s and likely
reflect a combination of earlier access to and more rapid
uptake of CRC screening tests among whites, as well as
changing patterns in the prevalence of CRC risk factors.
48
Since the mid-2000s, CRC incidence rates decreased by
about 1%-3% per year in all broadly defined racial/ethnic
groups, although the pace appears to be slowing in recent
years.
24
Notably, the steepest increase in early-onset CRC
is among NHWs and AIANs.
49
As a result, incidence rates
in NHWs ages 20-49 years are now equivalent to those in
blacks (14.1 per 100,000 during 2015-2016), despite being
40% higher in blacks during 1995-1996.
50
Mortality
CRC death rates have been decreasing since 1947 in
women, but only since 1980 in men (
Figure 6
). This
inconsistency likely reflects sex differences in incidence
trends because of variable patterns in CRC risk factors,
although population-based incidence data are not
available prior to 1975. Trends over the past three
decades are very similar by sex. Declines in mortality
through 2000 are attributed to improvements in
treatment (12%), changing patterns in CRC risk factors
(35%), and screening (53%).
43
However, screening likely
played an even larger role in more recent trends given its
steep increase since 2000.
52
Rapid declines in CRC death
rates of about 3% per year from 2002 to 2012 slowed to 2%
per year from 2012 to 2017.
Age-specific mortality trends
Like incidence, CRC mortality trends vary by age (
Figure
7
). Among older adults, decades of rapid declines have
slowed, from 1% annually during 2004-2013 to 0.6%
during 2013-2017 in those ages 50-64 years and from
3.3% to 2.6%, respectively, in those ages 65 and older. In
contrast, CRC death rates have increased in individuals
younger than 50 years of age by 1.3% per year since 2004.
Racial/ethnic mortality trends
CRC death rates in whites began a slow decline in the
early 1970s that accelerated over time. In contrast, death
rates in blacks increased from the early 1970s until 1990,
then decreased sluggishly during the 1990s before
matching the decline in whites in the early 2000s (
Figure 8
).
As a result of these divergent trends, although CRC death
rates in blacks were 10% lower than those in whites in the
early 1970s, they were almost 50% higher in 2005. The
widening racial disparity was largely driven by trends
for distant-stage disease, which declined in whites while
remaining stable in blacks through the mid-2000s.
53
About
half of the racial disparity in mortality is attributed to a
combination of less screening and lower stage-specific
survival rates among blacks.
30
Since the early 2000s, CRC
death rates have declined consistently by 1.8% per year
in Hispanics and APIs and by 2.8% per year in blacks;
however, rates were stable in AIANs during this time,
and in whites declines slowed from 2.5% per year during
Rates are age adjusted to the 2000 US standard population. Incidence rates are
adjusted for reporting delays and exclude appendix. White and black race are not
mutually exclusive from Hispanic ethnicity.
Source: Incidence – SEER program, 2019. Mortality – NCHS, 2019.
©2020, American Cancer Society, Inc., Surveillance Research
Rate per 100,000 population
Figure 8. Trends in Colorectal Cancer Incidence
(1975-2016) and Mortality (1970-2017) Rates by Race, US
Incidence, blacks
Mortality, blacks
Mortality, whites
Mortality, Hispanics
Incidence, whites
Incidence, Hispanics
0
10
20
30
40
50
60
70
80
2015201020052000199519901985198019751970
Year of diagnosis/death

Colorectal Cancer Facts & Figures 2020-2022 9
2005-2012 to 1.6% per year during 2012-2017. As a result,
the black-white gap has slowly begun to narrow.
How does colorectal cancer
occurrence vary by state?
The geographic pattern of CRC has changed dramatically
over the past several decades. In contrast to the 1970s
and 1980s, when the burden was highest across the
Northeast and lowest in the South,
54
today it is highest in
parts of the South, Midwest, and Appalachia and lowest
in the West and Northeast. Current incidence rates range
from 49 (per 100,000) in Kentucky to 30 in Utah, while
death rates range from 18 in Mississippi and West Virginia
to 11 in Connecticut and Utah (
Figure 9
). This shift is
consistent with the racial and socioeconomic crossover in
disease burden that occurred during the latter half of the
20th century because of changes in dietary and smoking
patterns, as well as differences in access to early detection
and high-quality treatment.
55
For example, CRC mortality
among residents of poor counties was 20% lower than
that among residents of affluent counties in the early
1970s, but is currently 30% to 40% higher.
54, 56
Geographic
patterns are generally similar for blacks and whites,
particularly for mortality, highlighting the importance of
socioeconomic status over race in cancer disparities.
57
Table 2
shows state-level incidence and death rates by
race/ethnicity. Consistent with overall incidence, rates in
NHWs and blacks are lowest in the West and highest in
the South and Midwest. However, among Hispanics there
is no clear pattern, perhaps reflecting geographic
heterogeneity within this population in terms of place of
birth and duration of residence, both of which influence
CRC risk. Although data for AIANs are too sparse to
provide by state, a recent study found that incidence
rates for those living in Alaska (approximately 95 per
100,000) were more than two-fold higher than those
living in the East and Southwest regions (30 to 40 per
100,000) of the US during 2010-2015.
58
Factors that may
contribute to this disparity include differences in diet
and the prevalence of obesity and smoking, as well as
access to medical services, including screening. Among
some more isolated groups (e.g., Alaska Natives), genetic
differences may also play a role. (See page 5 and page 6
for more information about CRC in Alaska Natives.)
Figure 9. Colorectal Cancer Incidence (2012-2016) and Mortality (2013-2017) Rates by State, US
AL
AZ
AR
CA
CO
CT
DE
FL
GA
ID
IL
IN
IA
KS
KY
LA
ME
MD
MA
MI
MN
MS
MO
MT
NE
NV
NH
NJ
NM
NY
NC
ND
OH
OK
OR
PA
RI
SC
SD
TN
TX
UT
VT
VA
WA
WV
WI
WY
DC
HI
AK
Incidence
AL
AZ
AR
CA
CO
CT
DE
FL
GA
ID
IL
IN
IA
KS
KY
LA
ME
MD
MA
MI
MN
MS
MO
MT
NE
NV
NH
NJ
NM
NY
NC
ND
OH
OK
OR
PA
RI
SC
SD
TN
TX
UT
VT
VA
WA
WV
WI
WY
DC
HI PRPR
AK
Mortality
Nevada and the District of Columbia did not meet NAACCR high-quality incidence data standards for one or more years during 2012-2016. Incidence rates for the District of
Columbia are based on data years 2012-2014. Rates are age adjusted to the 2000 standard population.
Sources: Incidence – NAACCR, 2019. Mortality – NCHS, 2019.
©2020, American Cancer Society, Inc. Surveillance Research
29.7- 35.6
35.7 - 38.9
39.0 - 44.0
44.1 - 49.2
Rate per 100,000
11.0- 12.5
12.6 - 14.1
14.2 - 15.9
16.0 - 18.3
Data unavailable
Rate per 100,000

10 Colorectal Cancer Facts & Figures 2020-2022
Table 2. Colorectal Cancer Incidence (2012-2016) and Mortality (2013-2017) Rates* by Race/Ethnicity and State, US
State
Incidence Mortality
Men Women Men Women
Non-
Hispanic
white
Non-
Hispanic
black Hispanic
Non-
Hispanic
white
Non-
Hispanic
black Hispanic
Non-
Hispanic
white
Non-
Hispanic
black Hispanic
Non-
Hispanic
white
Non-
Hispanic
black Hispanic
Alabama 49.4 58.9 27.6 36.3 44.6 25.5 18.5 26.4 † 12.0 17.7 †
Alaska 37.0 † † 33.1 † † 13.3 † † 11.5 † †
Arizona 37.8 33.5 41.9 29.2 33.1 26.2 15.3 18.2 15.3 10.9 16.4 8.8
Arkansas 50.1 58.2 29.4 36.5 45.8 32.0 19.4 26.0 † 13.0 19.5 †
California 40.4 48.5 38.4 32.4 39.4 27.7 14.9 21.9 13.9 11.7 16.0 8.8
Colorado 35.5 48.8 44.7 29.5 34.6 33.5 13.4 19.5 16.8 10.4 11.5 11.3
Connecticut 40.8 46.1 49.4 31.5 36.1 32.9 13.0 16.7 12.8 9.5 10.9 7.1
Delaware 42.8 51.0 34.9 32.2 38.4 42.8 17.5 17.1 † 10.2 15.7 †
Dist. Of Columbia
‡,§
29.2 61.7 † 27. 8 44.6 † 7.9 26.9 † 7.3 17. 8 †
Florida 41.3 48.9 43.5 31.3 36.7 31.6 15.5 20.6 14.6 10.9 14.0 9.6
Georgia 47.8 57.3 37.3 34.5 41.4 30.9 17.6 25.7 10.4 11.5 15.1 5.6
Hawaii 42.2 44.5 46.5 37.3 † 42.5 12.3 † 19.7 13.0 † †
Idaho 39.4 † 31.4 32.3 † 24.0 15.4 † 11.9 11.4 † †
Illinois 50.3 64.4 37.5 36.8 45.9 28.5 17.5 29.1 12.4 12.4 19.0 6.8
Indiana 48.7 52.6 35.7 38.0 41.4 31.1 18.0 24.4 10.5 12.9 17.0 6.3
Iowa 50.5 57.8 36.2 39.7 37.5 19.1 17. 3 18.0 † 12.7 16.2 †
Kansas 45.2 56.6 44.8 34.9 38.5 24.7 17.8 25.3 16.8 12.2 16.4 8.9
Kentucky 57. 8 59.4 32.8 42.4 45.0 21.5 20.2 24.6 † 13.9 16.7 †
Louisiana 51.6 65.8 28.9 36.9 47. 8 22.3 18.5 28.5 † 13.0 18.2 †
Maine 41.9 † † 33.8 † † 14.7 † † 11. 4 † †
Maryland 40.0 47.8 28.4 33.1 35.6 22.3 15.4 22.5 7.5 11.5 13.9 5.2
Massachusetts 39.6 44.6 33.1 31.6 33.4 23.2 14.1 16.3 8.5 10.5 11.4 7.5
Michigan 40.7 55.3 36.1 32.4 40.8 25.3 15.8 23.6 11.6 11.5 17.0 9.4
Minnesota 42.1 47.9 33.6 33.4 40.0 43.5 14.3 13.2 † 10.7 13.2 12.6
Mississippi 52.9 70.4 † 37.8 48.9 † 20.2 30.5 † 13.9 18.0 †
Missouri 47.6 56.6 29.8 35.1 41.8 23.7 17.3 26.1 † 12.0 16.1 †
Montana 42.1 † 63.0 32.2 † † 15.5 † † 10.6 † †
Nebraska 49.0 70.8 36.9 37.5 38.5 33.9 17.5 27.8 † 12.5 20.7 †
Nevada
‡
42.3 47.1 35.2 33.5 33.3 25.5 19.9 30.4 13.6 14.9 17.0 9.1
New Hampshire 42.2 † † 33.2 † † 14.1 † † 11.8 † †
New Jersey 48.1 54.1 43.8 36.9 41.5 32.9 17.1 24.2 12.4 12.4 14.5 8.1
New Mexico 33.7 32.0 42.5 27. 8 32.3 30.8 14.7 † 18.8 10.5 † 12.1
New York 44.8 50.7 43.6 34.8 36.6 29.1 15.3 18.2 13.6 11.3 13.7 8.2
North Carolina 41.7 51.6 27.8 32.0 36.3 24.2 15.3 23.2 6.4 10.6 14.8 6.0
North Dakota 51.9 † † 36.8 † † 16.5 † † 11.0 † †
Ohio 47.1 48.1 33.0 36.2 37.3 21.1 18.2 23.2 7.4 13.0 15.8 7.3
Oklahoma 46.8 54.6 37.3 35.2 40.6 33.0 20.3 28.4 14.1 13.7 15.6 6.7
Oregon 38.6 40.3 35.8 30.6 31.4 29.0 15.3 21.0 11. 2 11.6 † 6.2
Pennsylvania 48.5 52.7 40.3 36.0 41.3 26.9 17.6 23.4 13.5 12.3 15.4 9.0
Rhode Island 38.5 35.7 35.3 31.4 25.2 23.0 14.9 † † 11.5 † †
South Carolina 42.5 54.5 29.0 32.4 37.3 30.4 16.0 24.8 † 11.1 14.9 †
South Dakota 46.4 † † 36.2 † † 19.5 † † 12.5 † †
Tennessee 45.7 56.9 21.4 35.2 41.4 17.4 17.7 28.3 † 12.5 18.0 †
Texas 44.5 56.4 46.0 32.1 40.9 28.0 17.2 26.6 17.2 11.4 16.3 8.9
Utah 32.9 58.7 38.7 25.6 † 32.2 12.7 † 12.5 9.6 † 9.1
Vermont 37.3 † † 33.2 † † 16.4 † † 13.9 † †
Virginia 39.2 49.4 25.5 31.3 38.2 24.0 15.8 24.4 9.1 10.9 15.2 6.3
Washington 39.2 42.6 36.0 32.5 33.8 26.1 14.7 17.1 9.5 10.9 13.3 6.5
West Virginia 52.0 50.1 † 41.5 43.6 † 20.4 30.6 † 15.8 15.8 †
Wisconsin 41.5 64.0 28.9 31.9 43.7 25.6 15.0 24.7 11.7 11.0 16.9 6.8
Wyoming 36.9 † 41.7 28.6 † 32.6 14.1 † † 10.0 † †
US 44.0 53.8 40.8 33.9 39.9 28.7 16.3 23.8 14.1 11.7 15.6 8.7
*Rates are per 100,000 and age adjusted to the 2000 US standard population. †Statistics not displayed due to fewer than 25 cases or deaths. ‡Incidence data for these
states are not included in US combined incidence rates because data did not meet inclusion standards for all years during 2012-2016 according to the North American
Association of Central Cancer Registries (NAACCR). §Rates are based on cases diagnosed during 2012-2014.
Sources: Incidence – NAACCR, 2019. Mortality – NCHS, 2019.
©2020, American Cancer Society, Inc., Surveillance Research

Colorectal Cancer Facts & Figures 2020-2022 11
Colorectal cancer survival
The relative survival rate for CRC is 64% at 5 years
following diagnosis and 58% at 10 years.
59
The most
important predictor of CRC survival is stage at diagnosis.
The 5-year survival rate is 90% for the 39% of patients
diagnosed with localized-stage disease, but declines to
71% and 14% for those diagnosed with regional and distant
stages, respectively (
Figure 10
and
Figure 11
). Rectal cancer
is diagnosed at a localized stage slightly more often than
colon cancer, 41% versus 38%, likely due to the earlier
appearance of symptoms and partly explaining the higher
overall 5-year relative survival (67% versus 63%). Factors
associated with advanced-stage CRC diagnosis include
low socioeconomic status, black race, and young age.
60, 61
Factors associated with CRC survival in addition to stage
include age at diagnosis, the presence of other illnesses,
and other tumor and patient characteristics, such as
race/ethnicity and socioeconomic status.
62
For reasons
that are not explained by tumor differences or other
known factors, women are slightly more likely than men
to survive after a CRC diagnosis.
63
There is some evidence
that patients with tumors located in the proximal colon
have lower survival rates than those with tumors in the
distal colon,
64
but this association may be confined to
distant-stage diagnoses.
65
Age
Although CRC patients younger than age 50 have higher
5-year relative survival rates than their older counterparts
for every stage of diagnosis (
Figure 10
), overall survival
among patients younger than age 50 (68%) is similar to
that in ages 50-64 years (69%) because of a later stage at
diagnosis. Approximately 26% of CRCs are diagnosed
at a distant stage among patients younger than age 50,
compared to 23% in ages 50-64 years and 19% among
those ages 65 and older (
Figure 11
). Despite having the
highest proportion of early-stage diagnoses, however,
individuals ages 65 and older have the lowest overall 5-year
relative survival (61%) because their stage advantage is
outweighed by age-related disadvantages, such as
additional health issues.
*Cause-specific survival rates are the probability of not dying from colorectal cancer within 5 years of diagnosis. Rates are based on cases diagnosed from 2009 to 2015, all
followed through 2016. Rates for American Indians/Alaska Natives are based on small case numbers, particularly for distant-stage disease.
Source: SEER Program, 2019.
©2020, American Cancer Society, Inc., Surveillance Research
Figure 10. Colorectal Cancer Five-year Survival (%) by Age and Race/Ethnicity, 2009-2015
0-49 years
50-64 years 65+ years All ages
Non-Hispanic white
Non-Hispanic black
Asian and Pacific Islander
American Indian/Alaska Native
Hispanic
0
10
20
30
40
50
60
70
80
90
100
DistantRegionalLocalAll stages
0
10
20
30
40
50
60
70
80
90
100
DistantRegionalLocalAll stages
Percent
68
69
61
64
94
87
90
78
76
66
71
21
16
10
14
66
60
68
63
65
90
89
92
91
72
73
71
15
12
16
17
16
67 67
89
94

12 Colorectal Cancer Facts & Figures 2020-2022
Race/ethnicity
Outcomes among racial/ethnic minorities are described in
terms of cause-specific survival because life expectancy
data for minority groups are inadequate to calculate
relative survival. The highest CRC survival rates are for
APIs (68%) and the lowest are for blacks (60%;
Figure 10
),
one-quarter of whom are diagnosed with distant-stage
disease (
Figure 11
). As described earlier, disparities in CRC
outcomes are largely driven by socioeconomic inequalities
that result in differences in access to early detection and
receipt of timely, high-quality treatment.
61, 66
Access to care
is directly related to stage at diagnosis, which plays the
largest role in racial/ethnic survival disparities.
67
Notably,
when CRC is diagnosed at localized stage, 5-year survival
is relatively similar (89%-92%) across racial/ethnic groups.
A recent nationwide study found that more than one-
half of the black-white survival disparity is explained by
differences in insurance status and one-quarter is due to
differences in tumor characteristics (e.g., grade, location).
3
There is also compelling evidence that black patients are
less likely to receive prompt follow-up after an abnormal
CRC screening test
32
and appropriate surgery, adjuvant
chemotherapy, and radiation treatments.
3, 68-70
Although a
recent study found no evidence of treatment delays in an
equal-access health system,
71
equal cancer treatment does
not eliminate the racial survival disparity.
72, 73
Thus, equity
in care across the cancer continuum, from prevention
to early detection to clinical-trial participation and
individualized treatment, is necessary to eliminate these
disparities.
74
Changes over time
The 5-year relative survival rate for CRC has increased
moderately from 50% in the mid-1970s to 64% during
2009-2015.
24
However, recent advances in the treatment
of metastatic disease, including improved surgical
methods and the development of targeted therapies,
75-77
have rapidly extended survival for these patients. For
example, the 2-year relative survival rate for distant-
stage disease increased from 21% for patients diagnosed
during the mid-1990s to 37% for those diagnosed during
2009-2015, with a larger jump for rectal cancer (22% to 41%)
than for colon cancer (21% to 36%). Although progress is
evident across race and age,
78
gains are most prominent
among white and non-elderly patients.
79
*Cause-specific survival rates are the probability of not dying from colorectal cancer within 5 years of diagnosis. Rates are based on cases diagnosed from 2009 to 2015, all
followed through 2016. Rates for American Indians/Alaska Natives are based on small case numbers, particularly for distant-stage disease.
Source: SEER Program, 2019.
©2020, American Cancer Society, Inc., Surveillance Research
Figure 10. Colorectal Cancer Five-year Survival (%) by Age and Race/Ethnicity, 2009-2015
0-49 years
50-64 years 65+ years All ages
Non-Hispanic white
Non-Hispanic black
Asian and Pacific Islander
American Indian/Alaska Native
Hispanic
0
10
20
30
40
50
60
70
80
90
100
DistantRegionalLocalAll stages
0
10
20
30
40
50
60
70
80
90
100
DistantRegionalLocalAll stages
Percent
68
69
61
64
94
87
90
78
76
66
71
21
16
10
14
66
60
68
63
65
90
89
92
91
72
73
71
15
12
16
17
16
67 67
89
94
*Cause-specific survival rates are the probability of not dying from colorectal cancer within 5 years of diagnosis. Rates are based on cases diagnosed from 2009 to 2015, all
followed through 2016. Rates for American Indians/Alaska Natives are based on small case numbers, particularly for distant-stage disease.
Source: SEER Program, 2019.
©2020, American Cancer Society, Inc., Surveillance Research
Figure 10. Colorectal Cancer Five-year Survival (%) by Age and Race/Ethnicity, 2009-2015
0-49 years
50-64 years 65+ years All ages
Non-Hispanic white
Non-Hispanic black
Asian and Pacific Islander
American Indian/Alaska Native
Hispanic
0
10
20
30
40
50
60
70
80
90
100
DistantRegionalLocalAll stages
0
10
20
30
40
50
60
70
80
90
100
DistantRegionalLocalAll stages
Percent
68
69
61
64
94
87
90
78
76
66
71
21
16
10
14
66
60
68
63
65
90
89
92
91
72
73
71
15
12
16
17
16
67 67
89
94
Source: NAACCR, 2019.
©2020, American Cancer Society, Inc., Surveillance Research
Figure 11. Colorectal Cancer Stage Distribution (%) by Age and Race/Ethnicity, 2012-2016
0-49 years 50-64 years 65+ years All ages Non-Hispanic white
Non-Hispanic black
Asian and Pacific Islander
American Indian/Alaska Native
Hispanic
0
5
10
15
20
25
30
35
40
UnstagedDistantRegionalLocal
0
5
10
15
20
25
30
35
40
UnstagedDistantRegionalLocal
Percent
31
37 37 37
38
35 35
26
23
19
21
5
6
9
7
37
35
37
34
35 35
32
37
36
20 20
21
7
8
7
9
8
25
23
34
34
Colorectal Cancer Facts & Figures 2020-2022 13
Colorectal Cancer Risk Factors
In the United States, more than half (55%) of all CRCs are
attributable to lifestyle factors, including an unhealthy diet,
insufficient physical activity, high alcohol consumption,
and smoking.
80
These behaviors are traditionally associated
with high-income countries, where CRC rates are highest.
On a global scale, increasing CRC incidence is considered
a marker of economic transition.
81
Importantly, however,
numerous studies have shown that people with healthy
lifestyle behaviors have a 27% to 52% lower risk of CRC
compared to those without these behaviors.
82
Nonmodifiable factors that increase risk are related to
heredity and medical history, including a personal or
family history of CRC or adenomas (precancerous polyps)
and a personal history of long-term chronic inflammatory
bowel disease. Most people at increased risk because of a
medical or family history should begin CRC screening
before age 45. (For more information on CRC screening
guidelines, please see page 30.) The following sections
present current knowledge about factors associated with
CRC risk.
Heredity and family history
Up to 30% of CRC patients have a family history of the
disease, making this one of the most important and
actionable risk factors.
83-85
People with a first-degree
relative (parent, sibling, or child) who has been diagnosed
with CRC have 2 to 4 times the risk of developing the
disease compared to people without this family history,
with higher risk for diagnosis before age 50 and/or multiple
affected relatives (
Table 3
).
84
However, a history of CRC
among more distant relatives also increases risk,
86
as
does a family history (first- or second-degree relatives)
of adenomas.
87
Much of the CRC clustered in families is
thought to reflect interactions between lifestyle factors
and the cumulative effect of relatively common genetic
variations that increase disease risk, referred to as high
prevalence/low penetrance mutations.
88
Identification of families with a history of CRC, especially
high-burden families with undiagnosed genetic syndromes
(i.e., low prevalence/high penetrance mutations, described
below), offers substantial opportunity to lessen cancer
incidence and mortality through increased surveillance
with colonoscopy. However, patient family history in
medical records continues to be incomplete. One study
found that less than half of primary care physicians
documented information about family members other
than first-degree relatives, and age at cancer diagnosis
was rarely collected.
89
Another study found that only
22% of CRC patient medical records had family history
information sufficient to identify individuals who should
be referred for genetic counseling and/or testing.
90
Table 3. Relative Risks for Established Colorectal
Cancer Risk Factors
Relative risk*
Factors that increase risk:
Heredity and medical history
Family history
84
CRC
1 or more first-degree relatives 2.2
1 or more first-degree relatives diagnosed
before age 50
3.6
2 or more first-degree relatives 4.0
1 or more second-degree relatives 1.7
Adenoma
1 or more first-degree relatives 2.0
Inflammatory bowel disease
115
1.7
Type 2 diabetes
124
Male 1.4
Female 1.2†
Modifiable factors
Heavy alcohol (daily average >3 drinks)
195
1.3
Obesity (body mass index ≥30 kg/m
2
)
146
1.3
Colon, male 1.5
Colon, female 1.1
Rectum, male 1.3
Rectum, female 1.0†
1.1
1.2
Red meat (100 g/day)
166
P
rocessed meat (50 g/day)
166
Smoking
190
Current vs. never 1.5
Former vs. never 1.2
Factors that decrease risk:
Physical activity
138
0.7
Dairy (400 g/day)
166
0.9
*Relative risk compares the risk of disease among people with a particular
“exposure” to the risk among people without that exposure. Relative risk for
dietary factors compares the highest with the lowest consumption. If the
relative risk is more than 1.0, then risk is higher among exposed than
unexposed persons. Relative risks less than 1.0 indicate a protective effect.
†Relative risk was not statistically significant.
©2020, American Cancer Society, Inc., Surveillance Research
14 Colorectal Cancer Facts & Figures 2020-2022
Hereditary syndromes
A recent study found that 5% of CRC patients have an
inherited gene mutation (germline mutation) associated
with a known high-risk hereditary condition, and an
additional 5% have mutations associated with moderately
increased risk.
91
Lynch syndrome
The most common hereditary risk factor for CRC is Lynch
syndrome, which accounts for about 3% of all CRCs.
91
People with Lynch syndrome are also at increased risk
for many other cancers, including endometrial, ovarian,
small intestine, stomach, urinary bladder, and female
breast.
92
These individuals have a mutation in certain
genes that hinders the cell’s ability to correct errors
introduced during DNA replication. These mistakes
result in additional mutations that can ultimately lead to
cancer,
93
the likelihood of which is dependent on which
gene is affected. Among the 80% of Lynch syndrome
patients with high-risk gene (MLH1 or MSH2) mutations,
19% to 25% will develop CRC by age 50 and 40% will
develop the disease by age 70.
94
The median age at CRC
diagnosis among Lynch syndrome patients is 61 years of
age,
95
and 8% of CRCs that occur in adults younger than
age 50 are caused by Lynch syndrome.
96
Although an estimated 1.2 million Americans (1 in 279)
have Lynch syndrome,
97
the vast majority are undiagnosed
because identification is dependent on a cancer diagnosis.
However, there is increasing recognition of the need for a
more proactive approach because rigorous colonoscopy
surveillance leads to early-stage diagnosis and high
survival in Lynch syndrome patients.
98
Numerous
organizations, including the National Comprehensive
Cancer Network and American Society for Clinical
Oncology, recommend testing for Lynch snydrome in
all patients with colorectal or endometrial cancer.
99, 100
Although implementation of universal testing has been
slow in the community hospital setting,
101
most major
public and private insurers cover the screening.
102
Polyposis syndromes
Polyposis syndromes are another type of hereditary
condition associated with increased CRC risk, the most
common of which is familial adenomatous polyposis
(FAP), which accounts for about 1% of all CRCs.
91
FAP is
characterized by the development of up to thousands of
colorectal polyps in the second and third decade of life. It
is typically caused by a mutation in the adenomatous
polyposis coli (APC) gene, which normally prevents
uncontrolled cell growth and division.
103
These mutations
are usually inherited, but occur spontaneously in 10% to
25% of affected people so there is not always a family
history of the condition.
104
Disease severity ranges from
severe (classic FAP) to mild (attenuated FAP), with the
latter associated with later age at onset and fewer polyps
(<100), but still high lifetime CRC risk.
105
Surgery is the
standard method of cancer prevention for people with
FAP once adenoma development is beyond the control of
colonoscopy. MUTYH-associated polyposis (MAP) is a
more recently recognized syndrome with large variability
in clinical features, but in which patients typically
develop a similar number of polyps as those with
attenuated FAP.
103
Other colorectal polyposis syndromes
include Peutz-Jeghers syndrome, juvenile polyposis
syndrome, and serrated polyposis syndrome.
106
BRCA1 and BRCA2
Approximately 1% of CRC patients have heritable
mutations in the breast cancer susceptibility genes
BRCA1 and/or BRCA2,
91
which are among the most
well-studied cancer predisposing genes. A gene panel
study of CRC patients younger than age 50 also found a
1% prevalence.
96
In addition to breast cancer, these
mutations confer increased risk for cancers of the ovary,
prostate, and pancreas.
107
Although their influence on
CRC risk is not well studied, a recent review reported an
association limited to BRCA1 mutation carriers, who
have about a 50% increased risk of the disease compared
to individuals without the mutation.
108
Personal medical history
People with a personal history of CRC are more likely to
develop a subsequent cancer in the colon or rectum,
especially when the initial diagnosis was at a young
age;
109
however, only 2% of patients will develop a second
primary CRC.
110
A history of adenomatous polyps also
increases CRC risk, especially multiple or large polyps.
111
Colorectal Cancer Facts & Figures 2020-2022 15
CRC risk is also increased among individuals with a
history of other cancer types because of the carcinogenic
effects of some treatments. Examples include childhood
cancer survivors, especially those who received pelvic or
abdominal or total-body radiotherapy, or certain drugs
(e.g., cisplatin, procarbazine);
112
men treated with
radiotherapy for prostate cancer;
113
and men treated with
platinum-containing chemotherapy for testicular cancer.
114
Chronic inflammatory bowel disease
Chronic inflammatory bowel disease (IBD) is a lifelong
condition, usually diagnosed in early adulthood, in which
the gastrointestinal tract is inflamed over a long period
of time. People with IBD have almost double the risk of
developing CRC compared to people in the general
population.
115
The most common forms of IBD are
ulcerative colitis and Crohn disease. Cancer risk
increases with the extent, duration, and severity of
disease,
115, 116
but has decreased over time, likely due to
the increased use of medications to control inflammation
and screening surveillance to detect premalignant
lesions.
117
Although the efficacy of anti-inflammatory
drugs for limiting IBD-related cancer occurrence
remains unclear, two recent meta-analyses reported
reduced CRC risk of 33% to 50% among individuals with
ulcerative colitis, but no effect for those with Crohn
disease.
118, 119
CRC patients with IBD are about 15 years
younger than those without IBD and 70% more likely to
die from their cancer after accounting for age and stage
at diagnosis.
120
IBD has been diagnosed in an estimated
3.1 million Americans and is most common among
non-Hispanic whites, women, and those with the least
education.
121
Although surveillance data in the US are
sparse, prevalence appears to have increased in recent
years.
122
Diabetes
People who have type 2 (adult onset) diabetes have a
slightly increased risk of CRC that appears stronger in
men than in women.
123, 124
The association between type 2
diabetes and CRC remains even after accounting for
shared risk factors (physical activity, body mass index,
and waist circumference).
125
Although some studies
suggest that metformin, a drug commonly used to lower
blood glucose levels in diabetic patients, independently
reduces CRC incidence,
126-130
a randomized controlled
trial found no association.
131
CRC patients with diabetes
are no more likely to die from their cancer than those
without diabetes, despite higher rates of cancer
recurrence, as well as mortality from other causes.
132
The prevalence of Americans with a history of diabetes
has more than doubled over the past two decades.
133
Although type 2 diabetes is rare among children and
adolescents (ages 0-19 years), incidence rates increased
by 7% per year between 2002 and 2012, from 9.0 cases per
100,000 in 2002-2003 to 12.5 in 2011-2012.
134
According to
the Centers for Disease Control and Prevention, 30.3
million people (9.4% of the population) were diabetic in
2017, including 7.2 million who were undiagnosed and
one-quarter of whom were 65 years of age and older.
135
H. pylori
Results from earlier studies evaluating the link between
infection with H. pylori, a bacteria strongly associated
with excess stomach cancer risk, and CRC occurrence
were inconsistent.
136
However, this may be because the
association is confined to specific subtypes of the
bacterium. A recent large study found that increased CRC
risk is limited to individuals with a history of infection
with particular H. pylori strains, and that this association
is strongest among black Americans.
137
Modifiable risk factors
Physical inactivity
Physical activity is strongly associated with a reduced risk
of colon cancer, but not rectal cancer. Studies consistently
show that the most physically active people have about a
25% lower risk of developing both proximal and distal
colon tumors than the least active people.
138, 139
Being
physically active from a young age may further lower
risk.
140
Likewise, people who are the most sedentary (e.g.,
spend the most hours watching TV) have a 25% to 50%
increased risk of colon cancer compared to those who are
least sedentary.
141
However, sedentary people who become
active later in life may reduce their risk.
142
Additionally,
people who were more physically active before a CRC
diagnosis are less likely to die from the disease than those
who were less active.
143
Based on these findings, as well as
16 Colorectal Cancer Facts & Figures 2020-2022
the numerous other health benefits of regular physical
activity, the American Cancer Society and the Centers for
Disease Control and Prevention recommend that adults
engage in at least 150 to 300 minutes of moderate-intensity
activity or 75 to 150 minutes of vigorous-intensity activity
each week (or a combination of these), preferably spread
throughout the week, and limit time spent sedentary in
activities like watching television.
Overweight and obesity
Excess body weight increases the risk of CRC, even
among those who are physically active.
144, 145
Compared to
people who are normal weight, obese men have about a
50% higher risk of colon cancer and a 25% higher risk of
rectal cancer, whereas obese women have about a 10%
increased risk of colon cancer and no increased risk of
rectal cancer.
146
Excess risk is also associated with higher
abdominal fat, measured by waist circumference or
waist-to-hip ratio, and fat stored within the abdominal
cavity, independent of body mass index and waist
circumference.
147
Thus, abdominal fat specifically may be
more important than overall body weight in influencing
CRC risk.
148
The timing of exposure may also be a factor,
with studies suggesting a stronger influence for excess
body weight during adolescence and young adulthood
among women, but later in life for men.
149
Higher body
weight, even within the normal range, appears to increase
risk of early-onset CRC (before age 50), at least among
women.
150
In addition, high body mass index measured
prior to diagnosis reduces the likelihood of CRC
survival.
147, 151
Excess body weight can have a negative
impact on the proper functioning of many biochemical
processes in the body (metabolic health), and studies
indicate that poor metabolic health may be related to
CRC incidence and survival independent of obesity.
152-154
Diet
Differences in CRC incidence globally, as well as the
relatively rapid changes in risk among immigrant
populations in the United States, have long suggested
that diet is linked to CRC occurrence.
155
Dietary patterns
likely influence risk both indirectly, through excess
calories and obesity, and directly through specific dietary
elements. For example, diet has a large influence on the
composition of the gut microbiome, which is the trillions
of microorganisms, including the 1,000+ different strains
of bacteria, that inhabit the large intestine. High levels of
specific bacteria in the microbiome are associated with
CRC risk.
156, 157
The microbiome is a very active area of
research because it is thought to play a dual role in both
preventing and promoting CRC and many other diseases
through its influence on immune response and
inflammation.
158-162
Diets with greater amounts of certain
foods, such as refined carbohydrates, processed sugar, and
red meat, have a higher potential to increase inflammation
and are associated with increased CRC risk.
163
However, the direct role of specific food items in cancer
occurrence is extremely challenging to study for many
reasons, including 1) difficulty defining and measuring
intake, such as challenges in the accuracy of self-reported
food questionnaires; 2) differences in the sources of
dietary constituents (e.g., cereal grains, fruits, and
vegetables all contribute to fiber intake); 3) the strong
link between dietary patterns and other health behaviors;
and 4) a constantly changing food supply. The following
is a summary of current scientific evidence for dietary
elements linked to CRC:
Dairy/Calcium: Most studies find that calcium
consumption from dairy foods and/or supplements is
associated with a decreased risk of developing adenomas
and CRC,
164-166
although the mechanism remains unclear.
Adequate calcium intake (approximately 700-1,000 mg/
day) seems to confer protection, with limited additional
benefit for higher consumption.
164
The relationship
appears to require years of follow-up to observe;
167
be
confined to cancers in the distal colon/rectum and
particular molecular subtypes;
168, 169
and perhaps be
moderated by other dietary factors.
164, 170
Whole grains/Fiber: Although it is highly plausible that
dietary fiber decreases risk of CRC for many reasons,
including less exposure to carcinogens because of higher
stool volume and faster transit time, study results,
including those from randomized controlled trials,
remain inconclusive and protective associations are
weak.
164
The evidence for whole grains specifically is
stronger than for overall fiber; two recent meta-analyses
found that CRC risk was decreased by about 5% for every
30 grams/day of whole-grain intake.
166, 171
Importantly, the
Colorectal Cancer Facts & Figures 2020-2022 17
overall health benefit of a diet high in whole grains is
clear,
172
and the American Cancer Society and the World
Cancer Research Fund both advocate a diet high in plant
foods, including whole grains, fruits, and vegetables for
the prevention of cancer and other diseases.
173, 174
Folate: Folate intake, consumed through diet or
supplements, appears to have a complex relationship
with CRC risk, potentially promoting growth of
preexisting tumors, while inhibiting formation of new
tumors in healthy tissue.
164
There has been speculation
that increased folate levels among Americans as a result
of mandatory fortification of enriched flour and cereals
in 1998 were responsible for the unexplained uptick in
CRC incidence rates in the late 1990s (
Figure 6
).
175
However, this hypothesis is not supported by an analysis
of data from randomized controlled trials that found no
association between five years of folic acid supplementation
and CRC risk.
176
Additional prospective studies conducted
post-fortification found that the highest level of folate
intake was associated with reduced risk of CRC.
177
Fruits and vegetables: Results from numerous studies
specifically evaluating the association between fruit and
vegetable intake and CRC risk are inconsistent.
164
Two
recent meta-analyses found no relationship for fruit and
a possible slightly reduced risk for the highest versus
lowest vegetable consumption.
166, 171
Any protective effect
appears to be for moderate compared to low consumption,
with high consumption providing little additional
benefit.
178, 179
Red and processed meat: Consumption of red and/or
processed meat increases the risk of CRC, with a stronger
association for colon cancer than rectal cancer and for
processed meat than red meat.
166, 180
A recent synthesis of
evidence for the World Cancer Research Fund found that
the risk of CRC is increased by 18% for every 50 grams/day
of processed meat (approximately 2 slices of lunchmeat)
and by 12% for every 100 grams/day of red meat
(marginally significant).
166
In 2015, the International
Agency for Research on Cancer classified processed meat
as “carcinogenic to humans” and red meat as “probably
carcinogenic to humans,” largely based on the evidence
related to CRC risk.
181
The reasons for this association
remain unclear, but may be related to the constituents of
meat and/or to carcinogens (cancer-causing substances)
that form during high-temperature cooking, curing, and/
or smoking.
182
Although there is concern about rising
consumption of processed foods overall, intake of
processed meat appears to have remained stable over
the past two decades.
183
Vitamin D: Higher blood levels of vitamin D may be
associated with lower risk of CRC, although research
findings remain inconsistent.
164
Clinical trials have not
found an association between daily supplementation
with vitamin D and risk of adenomas
167
or CRC.
184
However, a recent study of pooled data from 17 cohort
studies indicated that higher blood levels of vitamin D
(25[OH]D up to 100 nmol/L) were associated with
reduced CRC risk among women, and deficiency was
associated with a 37% increased risk.
185
Forthcoming
data from additional clinical trials evaluating the effect
of vitamin D supplementation on cancer prevention may
help clarify this association,
186, 187
although study design
modifications may be necessary to reconcile the current
controversy.
188
Smoking
In November 2009, the International Agency for Research
on Cancer reported that there is sufficient evidence to
conclude that tobacco smoking causes CRC.
189
In the US,
approximately 12% of CRCs are attributed to cigarette
current or former smoking, with CRC risk in current
smokers about 50% higher than that in never smokers.
80, 190
Most studies find differences in the association by
anatomic and molecular subtypes of CRC.
2, 191, 192
Smoking
is also associated with lower CRC-specific survival,
particularly for current smokers.
193, 194
Alcohol
An estimated 13% of CRCs in the US are attributed to
alcohol consumption.
80
Although there is strong evidence
that heavy consumption increases risk, the magnitude of
excess risk and the association with smaller quantities is
less certain. A recent meta-analysis reported that light-
to-moderate alcohol consumption (up to two drinks per
day) was associated with a slightly lower (8%) risk than
no consumption/occasional consumption, whereas very
heavy drinking (more than 3 drinks per day) was

18 Colorectal Cancer Facts & Figures 2020-2022
associated with a 25% higher risk.
195
However, other studies
find excess risk with just one drink per day, rising to 44%
for the heaviest drinking.
166, 196
The association appears
stronger in men, especially for heavy consumption,
perhaps because women are less likely to drink heavily
and/or because of hormone-related differences in alcohol
metabolism.
Medications
Nonsteroidal anti-inflammatory drugs
There is extensive evidence that long-term regular use of
aspirin and other nonsteroidal anti-inflammatory drugs
(NSAIDs) lowers risk of CRC.
197-199
The reduction in risk
appears to be stronger among individuals younger than
age 70 and without excess body weight.
200
Aspirin users
who do develop CRC appear to have less aggressive
tumors and better survival compared to non-aspirin
users,
201, 202
although the survival benefit may be limited
to certain tumor subtypes.
203, 204
The American Cancer
Society has not conducted a formal evidence review, but
currently does not recommend the use of NSAIDs for
cancer prevention in the general population because of
the potential side effects, namely serious gastrointestinal
bleeding. However, the US Preventive Services Task Force
currently recommends daily low-dose aspirin for the
prevention of cardiovascular disease and CRC for certain
individuals in their 50s who are at increased risk for
cardiovascular disease; the evidence for individuals in
their 60s is less convincing.
205
Decisions about aspirin use
should be made after discussion with a health care
provider. Visit
uspreventiveservicestaskforce.org
for more
information about their recommendation.
Hormones
The evidence regarding the association between steroid
hormones, both endogenous (naturally occurring within the
body) and exogenous (e.g., hormone replacement therapy
and oral contraceptives), and CRC is inconsistent.
206
Some
studies have found that higher natural levels of estrogen
among postmenopausal women are associated with
reduced CRC risk,
207
while others have found no
association.
208
Reduced risk associated with hormone
replacement therapy appears to be confined to use of
combined estrogen and progesterone formulations.
209, 210
Recent studies do not support an association between
oral contraceptive use and CRC risk.
2, 211, 212
Antibiotics
Emerging evidence suggests that oral antibiotic use may
be associated with increased risk of CRC.
213, 214
Antibiotics
might influence risk by disrupting the critical balance of
the gut microbiome. For more information on the
microbiome, see Diet on (page 16).
Other drugs
Oral bisphosphonates, which are used to treat and
prevent osteoporosis, may reduce CRC risk.
215, 216
Colorectal Cancer Screening
The typically slow course of growth from precancerous
polyp to invasive cancer to advanced-stage disease
provides a unique opportunity for the prevention and
early detection of CRC.
8
Screening can prevent cancer
through the detection and removal of precancerous
growths and detect the disease at an early stage, when
treatment is usually more successful. As a result,
screening reduces CRC mortality both by decreasing
incidence and increasing survival.
The 2018 American Cancer Society CRC screening
guideline recommends that adults ages 45 years and
older undergo regular screening with a high-sensitivity
stool-based test or visual examination (described below),
depending on patient preference and test availability.
217
As part of the screening process, all positive results on
non-colonoscopy screening tests should be followed up
with a timely colonoscopy because delays in follow-up of
abnormal results increase the risk of advanced CRC and
CRC death.
218, 219
The age to initiate CRC screening was
Colorectal Cancer Facts & Figures 2020-2022 19
lowered from 50 to 45 years because incidence rates are
increasing in younger populations, and modeling studies
demonstrated that the balance of benefit to harm was
more favorable for beginning screening at age 45 than
at 50.
220, 221
Although health insurance coverage for
screening those at average risk before age 50 remains
variable, the American Cancer Society is working
aggressively to educate insurers, lawmakers, and other
stakeholders about the evidence in support of screening
those ages 45-49 years and the importance of expanding
coverage for this group. Screening before age 45 is
recommended for those at an increased risk of CRC
because of family history or certain medical conditions
(see page 13), with age to initiate and rescreening intervals
dependent on individual circumstances. Everyone should
have a conversation with their health care provider about
CRC screening that includes information about cancer
family history well before age 45.
221
Visit
cancer.org/cancer/
colon-rectal-cancer/early-detection/acs-recommendations
for
more information, including specific guidelines for
screening individuals at increased or high risk.
Recommended options for colorectal
cancer screening
There are several recommended methods for CRC
screening, including both visual examinations, which are
performed at a health care facility, and high-sensitivity
stool-based tests, which are collected at home (
Table 4
). All
tests have a comparable ability to improve life expectancy
when performed at the appropriate time intervals and
with the recommended follow-up.
222
Patients should be
given information about the benefits and limitations of
each screening test, and choose one based on their health,
medical history, and preferences with advice from a health
care professional as needed. A growing body of evidence
demonstrates that offering patients different test
options substantially increases adherence to screening
recommendations.
223
As a result, and because one-third
of eligible adults are not up to date with CRC screening,
including half of those ages 50-54 years, the American
Cancer Society and the US Preventive Services Task Force
guidelines do not emphasize any one test and stress that
all recommended tests can help save lives.
217, 224
Visual examinations
Visual tests allow doctors to see the lining of the colon and
rectum through an endoscope or on radiological images.
Colonoscopy
Colonoscopy is the most commonly used CRC screening
test in the US. This procedure, which is usually performed
by a gastroenterologist (a doctor who specializes in the
digestive system) or surgeon, allows for direct visual
examination of the entire colon and rectum. It can be used
as a singular screening test, or may be performed as a
follow-up to abnormal results from stool and other visual
tests to complete the screening process. Colonoscopy has
the longest rescreening interval of all test options, 10
years for average-risk individuals with normal results.
Before undergoing a colonoscopy, patients are instructed
to take special laxative agents to cleanse the colorectum
completely so the intestinal lining can be thoroughly
examined. During the exam, the colon is inflated with
either air or carbon dioxide. Then a long, slender
instrument called a colonoscope is inserted into the anus
and moved slowly through the rectum to the cecum
(beginning of the colon). The colonoscope has a light and
small video camera on the end to allow for the detection
and removal of most polyps with a wire loop or electric
current. Sedation is usually provided during examinations
in the US, although it is used less frequently in some
European countries (e.g., Norway and Poland).
225
While data are not yet available from randomized
controlled trials evaluating the effectiveness of
colonoscopy,
226
results from several trials of flexible
sigmoidoscopy, a similar test discussed in the next
section, provide indirect support for the benefits of
colonoscopy. In addition, observational studies suggest
that colonoscopy can help reduce CRC incidence by about
40% and mortality by about 60%.
227-229
Like all screening tests, colonoscopy has limitations and
potential harms. For example, it can lead to unnecessary
procedures, such as the removal of small polyps that
would not have progressed to cancer.
230
A recent study
found that although >90% of polyps can be safely

20 Colorectal Cancer Facts & Figures 2020-2022
removed during colonoscopy, elective surgery to remove
nonmalignant polyps, which has a higher risk of harms,
increased by more than 50% from 2000 to 2014.
231
Other
limitations of colonoscopy include a higher risk of
complications compared to other screening tests, such
as bowel tears and bleeding, especially when a polyp is
removed or patients are older.
230, 231
Although these side
effects are rare, serious bleeding occurs in 1 to 2 of every
1,000 colonoscopies.
225, 232, 233
In addition, colonoscopy
sometimes misses adenomas, especially those that are
located in the proximal colon; those that occur in high-risk
patients; and those that are flat (sessile adenomas), from
which 20% to 30% of CRCs are thought to originate.
226, 234
The quality of colonoscopy, which is variable in the US, is
also associated with missed lesions, which sometimes
progress to CRC before the next scheduled exam (i.e.,
Table 4. Characteristics of Recommended Colorectal Cancer Screening Tests
Benefits
Performance
& Complexity* Limitations
Test Time
Interval
Visual Examinations
Colonoscopy • Examines entire colon
• Can biopsy and remove
polyps
• Can diagnose other
diseases
• Required for abnormal results
from all other tests
Performance:
Highest
Complexity:
Highest
• Full bowel cleansing
• Can be expensive
• Sedation usually needed, necessitating a
chaperone to return home
• Patient may miss a day of work.
• Highest risk of bowel tears or infections
compared with other tests
10 years
†
Computed
tomographic
colonography
(CTC)
• Examines entire colon
• Fairly quick
• Few complications
• No sedation needed
• Noninvasive
Performance:
High (for large polyps)
Complexity:
Intermediate
• Full bowel cleansing
• Cannot remove polyps or perform biopsies
• Exposure to low-dose radiation
• Colonoscopy necessary if positive
• Not covered by all insurance plans
5 years
Flexible
sigmoidoscopy
• Fairly quick
• Few complications
• Minimal bowel preparation
• Does not require sedation or
a specialist
Performance:
High for rectum & lower
one-third of the colon
Complexity:
Intermediate
• Partial bowel cleansing
• Views only one-third of colon
• Cannot remove large polyps
• Small risk of infection or bowel tear
• Slightly more effective when combined with
annual fecal occult blood testing
• Colonoscopy necessary if positive
• Limited availability
5 years
Stool Tests (Low-sensitivity stool tests, such as single-sample FOBT done in the doctor’s office or toilet bowl tests, are not recommended.)
Fecal immuno-
chemical test
(FIT)
• No bowel cleansing or
sedation
• Performed at home
• Low cost
• Noninvasive
Performance:
Intermediate for cancer
Complexity:
Low
• Requires multiple stool samples
• Will miss most polyps
• May produce false-positive test results
• Slightly more effective when combined with a
flexible sigmoidoscopy every five years
• Colonoscopy necessary if positive
Annual
High-sensitivity
guaiac-based
fecal occult
blood test
(gFOBT)
• No bowel cleansing or
sedation
• Performed at home
• Low cost
• Noninvasive
Performance:
Intermediate for cancer
Complexity:
Low
• Requires multiple stool samples
• Will miss most polyps
• May produce false-positive test results
• Pre-test dietary limitations
• Slightly more effective when combined with a
flexible sigmoidoscopy every five years
• Colonoscopy necessary if positive
Annual
Multitargeted
stool DNA test
(Cologuard
®
)
• No bowel cleansing or
sedation
• Performed at home
• Requires only a single stool
sample
• Noninvasive
Performance:
Intermediate for cancer
Complexity:
Low
• Will miss most polyps
• More false-positive results than other tests
• Higher cost than gFOBT and FIT
• Colonoscopy necessary if positive
3 years, per
manufacturer’s
recommendation
*Complexity involves patient preparation, inconvenience, facilities and equipment needed, and patient discomfort. †For average-risk individuals, e.g., does not apply to
those who have a history of adenoma.
Colorectal Cancer Facts & Figures 2020-2022 21
interval cancer).
235, 236
Low-quality colonoscopy (measured
as low adenoma detection rate) is associated with a
higher likelihood of interval CRC and CRC death.
236
Flexible sigmoidoscopy
Sigmoidoscopy was a common screening test before
2000, but current availability is limited because it has
mostly been replaced by colonoscopy (see page 23 for
current prevalence of sigmoidoscopy and other screening
tests). These tests are very similar except colonoscopy
can examine the entire colon whereas sigmoidoscopy can
only visualize the rectum and distal one-third of the
colon, and must be repeated more often (
Table 4
). Simple
bowel cleansing, usually with enemas, is sufficient to
prepare the colon, and the procedure is often performed
without sedation in a general health care practitioner’s
office. If there is a polyp or tumor present, the patient
should be referred for a colonoscopy so that the entire
colon can be examined.
Recent analysis of data from randomized controlled
trials with up to 17 years of follow-up shows that
sigmoidoscopy is associated with about a 20%-25%
reduction in CRC incidence and a 25%-30% reduction in
CRC mortality, with greater reductions in men than
women.
237-239
Computed tomographic colonography (CTC)
Also referred to as virtual colonoscopy, CTC is an
imaging procedure that provides 2- or 3-dimensional
views of the entire colon and rectum with the use of a
special x-ray machine linked to a computer.
230
Although a
full bowel cleansing is necessary for a successful
examination, sedation is not required. A small, flexible
tube is inserted into the rectum in order to allow carbon
dioxide, or sometimes air, to inflate the colon; then the
patient passes through the CT scanner, which creates
multiple images of the interior of the colon. CTC is less
invasive than colonoscopy or sigmoidoscopy and
typically takes approximately 10 to 15 minutes to
complete.
240
Patients with adenomas larger than 5
millimeters or other abnormal results are referred for
colonoscopy, optimally on the same day in order to
alleviate the necessity of a second bowel preparation.
Studies have shown that the performance of CTC is similar
to colonoscopy for the detection of invasive cancer and
advanced adenomas, but has lower sensitivity for smaller
adenomas.
241
Potential harms include cumulative
radiation exposure from regular examinations, and
unnecessary tests and/or treatment due to incidental
benign findings outside the colorectum. There is less
evidence on the benefits and harms of this test compared
to others because it is relatively new and remains
uncommon.
224
This may be because it is not covered by
Medicare and commercial insurance coverage is variable;
in 2019, 37 states mandated that commercial plans cover
this test.
242
Stool tests
Most cancerous tumors and some large adenomas bleed
intermittently into the intestine. This blood, which may
not be visible, can be detected in stool with special tests.
Modeling studies suggest that annual screening with
high-sensitivity stool tests and timely follow-up of
abnormal results will result in a reduction in mortality
similar to that achieved by colonoscopy over a lifetime of
screening.
243
Except for the multitargeted stool DNA test,
which is recommended every 3 years, stool tests should
be repeated annually. However, adherence to yearly
testing and timely follow-up with a colonoscopy after a
positive test remains a challenge, especially in low-
resource settings where stool tests are more common.
244-247
Guaiac-based fecal occult blood test (gFOBT)
These tests use a chemical reaction to detect blood in
the stool. Bleeding from cancers or adenomas may be
sporadic or undetectable, so accurate results require
annual testing of samples from 3 consecutive bowel
movements. Patients are typically instructed to avoid
nonsteroidal anti-inflammatory drugs and red meat for
3 days prior to the test because they can lead to a positive
test result when no cancer is present (false positive);
gFOBT detects blood from any source, including meat in
the diet. Vitamin C and large amounts of citrus juices
should also be avoided because they can lead to a negative
test result when cancer is present (false negative). Only
high-sensitivity gFOBT are recommended for CRC
screening.
22 Colorectal Cancer Facts & Figures 2020-2022
Data from a large clinical trial indicated that the regular
use of FOBT reduced the risk of CRC death by 32% after
30 years of follow-up.
248
FOBT has also been shown to
decrease CRC incidence by 20% by detecting large
precancerous adenomas.
249
Fecal immunochemical test (FIT)
The FIT (also sometimes referred to as the
immunochemical FOBT, or iFOBT) uses antibodies
against hemoglobin to specifically detect human blood
in the stool and is about twice as likely as most gFOBT
products to detect both advanced adenomas and
cancer.
250, 251
Many individuals prefer FIT over gFOBT
because of its convenience, lack of dietary restrictions,
and collection of fewer stool samples.
252
Multitargeted stool DNA (Cologuard®)
This test is referred to as “multitargeted” because it not
only detects blood in the stool, but also multiple genetic
mutations in the DNA of cells that are shed into the stool
by large adenomas and CRC. Cologuard® has been shown
to detect cancer and precancerous lesions more often
than FIT, but also results in more false-positive tests,
which can lead to unnecessary colonoscopies.
253
However,
because it is a relatively new test, data are still accumulating
on performance characteristics in community settings.
Although it is recognized as an acceptable screening
option by the American Cancer Society and the US
Preventive Services Task Force
224
and is covered by
Medicare, some private insurance companies may not
cover this test. Patient navigation services, which include
phone calls and reminder letters in multiple languages to
support test completion, are embedded in the cost of the
test, although the services do not extend to colonoscopy
follow-up of abnormal results.
254
Non-recommended tests for colorectal
cancer screening
There are several tests for CRC screening that are not
recommended by the American Cancer Society or other
organizations because of poorer performance. These
include in-office stool tests, in which a single-stool
sample is collected during a digital rectal exam and
placed on an FOBT card, and “toilet bowl tests,” which
are over-the-counter guaiac-based tests that are often
promoted as a type of FOBT. Despite recommendations
against in-office FOBT, some primary care physicians
continue to offer the test.
255
Toilet bowl tests have not
been evaluated in the types of rigorous clinical studies
done on the guaiac-based FOBT and FIT.
Double-contrast barium enema, also called barium
enema with air contrast, is a test that takes an x-ray of
the colon after barium sulfate is introduced. This test is
no longer recommended because it has lower sensitivity
for detecting CRC than other tests.
There are also emerging technologies that are not
currently recommended for CRC screening because there
was insufficient data on their performance compared to
other recommended options at the time the guidelines
were issued. These include blood-based tests that
measure circulating genetic abnormalities associated
with colorectal adenomas and cancer, and capsule
endoscopy, in which the patient undergoes bowel
cleansing and swallows a pill-sized device containing
tiny encapsulated cameras that transmit images of the
colon and rectum to a recording device.
Use of colorectal cancer screening
According to the National Health Interview Survey
(NHIS), CRC screening in accordance with guidelines
increased rapidly among adults ages 50 and older from
2000 (38%) to 2010 (59%), but more slowly in the past
decade, reaching 66% in 2018 (
Table 5
).
44
The most recent
NHIS data collected in 2018 contain a mix of respondents
surveyed before and after the release of the American
Cancer Society CRC screening guideline in mid-2018.
Approximately 56% of those ≥45 years of age and 21% of
those ages 45-49 years reported being up to date with
CRC screening in 2018.
Among adults ages 50 and older in 2018:
• 61% reported having a colonoscopy in the past 10
years, and 3% and 1% reported having a sigmoidoscopy
or CT colonography, respectively, in the past 5 years.
• Approximately 11% reported a recent stool test; 9%
reported an FIT or FOBT in the past year and 3%
reported stool DNA testing in the past 3 years.
44

Colorectal Cancer Facts & Figures 2020-2022 23
• Screening was lowest among ages 50-54 years (48%);
Asian Americans (55%); individuals with less than a
high school education (52%); the uninsured (30%);
and recent (<10 years) immigrants (26%).
The prevalence of CRC screening also varies substantially
among US states and territories (see cover). According to
data from the 2018 Behavioral Risk Factor Surveillance
System (BRFSS):
256
Table 5. Colorectal Cancer Screening (%), Adults 45 Years and Older, US, 2018
Stool test* Colonoscopy† Up to date‡
≥50 years ≥50 years ≥50 years 50-75 years
Overall 11 61 66 67
Gender
Males 12 62 67 67
Females 10 60 64 66
Age (years)
50-64 10 56 61 62
50-54 9 42 48 –
55-64 10 63 68 –
65+ 12 66 71 77
75+ 10 60 63 –
Race/ethnicity
White 10 63 68 69
Black 12 60 65 66
Hispanic 15 52 59 59
American Indian/Alaska Native 12 53 59 56
Asian 15 47 55 58
Sexual orientation
Gay/Lesbian 18 68 76 76
Straight 11 61 66 67
Bisexual 25 49 58 §
Education
Less than high school 11 46 52 53
High school diploma 10 57 62 63
Some college 11 62 68 68
College graduate 11 68 73 73
Immigration status
Born in US 10 63 68 69
Born in US territory § 76 80 84
In US fewer than 10 years § 20 26 30
In US 10+ years 14 49 56 58
Income level
<100% FPL 12 49 55 57
100 to <200% FPL 12 48 55 57
≥200% FPL 11 65 70 70
Insurance status
Uninsured 5 26 30 30
Private 9 60 65 65
Medicare or Medicare & Medicaid 14 61 67 73
Private & Medicare 11 71 74 80
Medicaid or Other state plan 14 44 53 54
FPL: federal poverty level. *Fecal occult blood test (FOBT) OR fecal immunochemical test (FIT) in the past 1 year OR stool DNA (sDNA) test in the past 3 years. †In the
past 10 years. ‡For ages ≥45 and ≥50 years: FOBT/FIT, sigmoidoscopy, colonoscopy, computed tomographic colonography (CTC), orsDNA test in the past 1, 5, 10, 5 and 3
years, respectively. For ages 50-75 years: FOBT/FIT, sigmoidoscopy, colonoscopy, CTC, orsDNA test in the past 1, 5, 10, 5 and 3 years, respectively, OR sigmoidoscopy in
past 10 years with FOBT/FIT in past 1 year. §Estimate not shown due to instability. Note: Estimates do not distinguish between examinations for screening and diagnosis.
All estimates except for age and insurance status are age adjusted to the 2000 US standard population.
Source: National Health Interview Survey, 2018.
©2020, American Cancer Society, Inc., Surveillance Research

24 Colorectal Cancer Facts & Figures 2020-2022
• Screening utilization ranged from 58% in Puerto Rico
and 60% in Wyoming to 76% in Massachusetts (
Figure
12
and
Table 6
).
• In all states, screening prevalence is substantially
lower in people ages 50-64 years than in those age 65
and older, with the largest absolute difference in
Puerto Rico (22%) and Florida, Mississippi, and
Oklahoma (all 19%).
Strategies to overcome screening barriers
Screening utilization for CRC remains lower than that
for breast and cervical cancers despite the large body
of evidence supporting its effectiveness for reducing
cancer incidence and mortality.
257
Use of CRC screening
is influenced by numerous individual, provider, health
system, and community factors, as well as public policy.
Barriers to screening include no usual source of care,
inadequate insurance coverage, lack of provider
recommendation, logistical factors (e.g., transportation,
scheduling, and language), fear, and lack of knowledge.
258-263
These barriers are more prevalent among people with
fewer financial resources, lower educational attainment,
and among racial/ethnic minorities, resulting in
disparities in screening prevalence and outcomes.
264
Interventions to help overcome these barriers include
increasing individual patient awareness (e.g., education and
reminders), ease of access (e.g., providing transportation,
reducing out-of-pocket expenses, mailed FIT kits, patient
navigators), provider delivery (e.g., provider reminders,
assessment, and feedback), and community demand
(e.g., media campaigns).
265
Multi-component interventions
are recommended because they are more effective at
increasing CRC screening utilization than a single
approach.
265, 266
Additionally, adherence to CRC screening
guidelines increases when patients are offered a variety
of tests.
222, 223, 267, 268
Importantly, however, the effectiveness
of screening is compromised without timely follow-up of
abnormal results. Follow-up of colonoscopy among adults
with a positive stool test may be increased through the
use of patient navigators and provider-level interventions,
such as physician reminders and performance data,
although evidence for effective strategies remains sparse.
269
Figure 12. Colorectal Cancer Screening* (%), Adults
50 Years and Older by State, 2018
Wyoming
Nevada
Texas
Alaska
New Mexico
Oklahoma
Mississippi
Montana
Arkansas
Illinois
Idaho
North Dakota
Arizona
New Jersey
Kansas
Indiana
West Virginia
Nebraska
Ohio
South Dakota
Colorado
Missouri
Utah
Tennessee
Georgia
Virginia
Pennsylvania
Alabama
Kentucky
New York
Louisiana
Florida
Iowa
Vermont
North Carolina
South Carolina
Washington
Oregon
Maryland
Hawaii
Delaware
Minnesota
California
District of Columbia
Michigan
Wisconsin
Connecticut
New Hampshire
Rhode Island
Maine
Massachusetts
Percent
*Blood stool test, sigmoidoscopy, or colonoscopy in the past 1, 5, and 10
years, respectively. Note: Estimates are age adjusted to the 2000 US standard
population and do not distinguish between examinations for screening and
diagnosis.
Source: Behavioral Risk Factors Surveillance System, 2018. See Sources of
Statistics (p. 32) for complete citation and more information.
©2020, American Cancer Society, Surveillance Research
50 60 70 80 90 100

Colorectal Cancer Facts & Figures 2020-2022 25
Table 6. Colorectal Cancer Screening* (%), Adults 50 Years and Older by State, 2018
All races
Non-Hispanic
white
Non-Hispanic
black
≥50 years 50 to 64 years ≥65 years 50 to 75 years ≥50 years ≥50 years
United States (median)
70 63 75 69 71 71
Range
60-76 50-72 66-82 58-77 61-80 63-84
Alabama
70 63 76 70 71 67
Alaska
62 52 70 60 62 †
Arizona
67 59 76 66 69 75
Arkansas
67 58 74 66 67 69
California
73 64 82 72 80 77
Colorado
69 62 74 69 71 76
Connecticut
75 71 78 75 76 76
Delaware
73 67 78 72 75 71
District of Columbia
74 69 78 74 77 73
Florida
71 61 80 69 74 67
Georgia
70 61 78 68 71 71
Hawaii
73 69 75 75 78 †
Idaho
67 59 72 66 68 †
Illinois
67 61 70 67 67 74
Indiana
68 61 73 68 69 67
Iowa
71 66 74 71 71 84
Kansas
68 60 74 67 69 66
Kentucky
70 63 76 69 70 70
Louisiana
70 64 76 69 71 70
Maine
75 69 79 75 76 †
Maryland
73 67 78 73 73 77
Massachusetts
76 72 78 77 77 82
Michigan
74 69 77 74 75 71
Minnesota
73 68 77 73 75 66
Mississippi
64 54 73 62 64 65
Missouri
69 62 75 69 69 71
Montana
65 56 71 64 65 †
Nebraska
68 62 72 68 70 67
Nevada
62 52 69 60 67 67
New Hampshire
75 70 78 75 75 †
New Jersey
68 59 75 67 69 76
New Mexico
63 55 66 64 66 †
New York
70 65 75 70 72 70
North Carolina
71 64 77 71 73 69
North Dakota
67 61 72 67 68 †
Ohio
68 61 75 67 69 68
Oklahoma
64 54 73 62 65 68
Oregon
72 66 77 72 72 †
Pennsylvania
70 66 72 72 71 68
Rhode Island
75 70 79 76 77 75
South Carolina
72 62 80 70 72 71
South Dakota
69 63 74 69 70 †
Tennessee
70 60 77 69 71 63
Texas
62 53 71 60 68 68
Utah
69 63 73 70 72 †
Vermont
71 65 72 71 71 †
Virginia
70 63 75 70 70 72
Washington
72 65 77 72 73 71
West Virginia
68 61 74 67 69 66
Wisconsin
74 69 77 75 75 82
Wyoming
60 50 67 58 61 †
Puerto Rico 58 48 70 55 † †
*Blood stool test, sigmoidoscopy, or colonoscopy in the past 1, 5, and 10 years, respectively. †Estimate not presented due to instability. Note: Estimates are age adjusted
to the 2000 US standard population and do not distinguish between examinations for screening and diagnosis. Puerto Rico not included in ranges or medians.
Source: Behavioral Risk Factor Surveillance System, 2018.
©2020, American Cancer Society, Inc., Surveillance Research

26 Colorectal Cancer Facts & Figures 2020-2022
The National Colorectal Cancer Roundtable (NCCRT), a
coalition of public, private, and voluntary organizations
and individuals established in 1997 by the American
Cancer Society and the CDC to promote CRC screening,
has produced evidence-based toolkits for policy makers,
communities, health systems, and health care providers
to help improve CRC screening uptake.
270, 271
Other efforts
include the CDC’s Colorectal Cancer Control Program
(CRCCP), which uses multicomponent interventions to
increase CRC screening among low-income, underinsured,
or uninsured individuals and certain racial and ethnic
groups, in particular. During its first year (2015-2016),
CRC screening prevalence increased by 4.4% in clinics
receiving CRCCP funds, resulting in an additional 24,100
people screened.
272
Integrated health systems have
improved CRC screening participation and reduced
CRC incidence and mortality by implementing patient
reminders and mailed FIT kits.
273
Mailed outreach FIT
programs may also be effective in community health
center settings, which historically have low CRC screening
rates and limited resources.
274
On a broader scale, provisions of the Patient Protection
and Affordable Care Act (ACA) removed some barriers to
screening. For example, CRC screening increased faster
in states that adopted the ACA provision to expand
Medicaid eligibility compared to those that did not.
275
The ACA also reduced or eliminated out-of-pocket
screening costs for those who are insured, although
loopholes remain.
276
All recommended screening options,
including colonoscopy, are covered without cost sharing
for people with Medicare insurance and most commercial
insurance plans. However, the required follow-up
colonoscopy for a positive stool test is often coded as a
diagnostic procedure, resulting in out-of-pocket costs for
patients. In addition, Medicare still imposes cost sharing
on beneficiaries who have a polyp removed during a
screening colonoscopy, undermining efforts to improve
CRC screening, particularly among low-income patients
who are at highest risk for CRC.
277
Visit
cancer.org/colonmd
for more information on programs
and resources aimed at increasing CRC screening.
Colorectal Cancer Treatment
Treatment for CRC has advanced rapidly over the past
several decades, particularly for advanced disease.
76, 278
However, it has also become increasingly clear that
outcomes vary widely based on tumor-specific molecular
features, tumor location, and patient characteristics.
279-281
Treatment decisions are made by patients with their
physicians after considering the best options available
for their tumor characteristics along with the risks and
benefits associated with each.
Colon cancer
Most people with colon cancer will have some type of
surgery to remove the tumor. Adjuvant chemotherapy
(given after surgery) may also be used. Radiation is used
less often to treat colon cancer.
Carcinoma in situ
Carcinoma in situ is malignant cancer that has not
spread beyond the layer of cells in which it began.
Surgery to remove the growth of abnormal cells may be
accomplished by polyp removal through a colonoscope
(polypectomy) or more invasive surgery. Resection of a
segment of the colon may be necessary if the tumor is too
large to be removed by local excision or if cancer cells are
found after the polyp is removed.
Localized stage
Localized stage refers to invasive cancer that has
penetrated into (but not completely through) the wall
of the colon. Surgical resection to remove the cancer,
together with a length of normal colon on either side of
the tumor and nearby lymph nodes, is the standard
treatment.
Colorectal Cancer Facts & Figures 2020-2022 27
Regional stage
Regional stage describes cancers that have grown
through the wall of the colon and/or spread to nearby
lymph nodes. If the cancer has not spread to nearby
lymph nodes, surgical resection to remove the tumor and
nearby colon and surrounding lymph nodes may be the
only treatment needed. If the cancer is likely to come back
because it has spread to other tissues or has high-risk
characteristics, chemotherapy may also be recommended.
If the cancer has spread to nearby lymph nodes, surgical
resection is usually followed by chemotherapy. Adjuvant
chemotherapy based on the drug fluorouracil (5-FU) is
typically used in patients with stage III or high-risk stage
II disease who are in otherwise good health.
282
Oxaliplatin
is often part of adjuvant chemotherapy as well.
283
However, some patients may not tolerate this regimen
given its toxicity, and there is growing appreciation for
the need to confine its use to patients who are most likely
to benefit.
76, 284, 285
Adjuvant chemotherapy for colon cancer
is as effective in patients ages 70 and older (almost half of
all patients) who are otherwise as healthy as in younger
patients, although certain drugs (e.g., oxaliplatin) may be
avoided to limit toxicity. However, studies indicate that
individuals 75 years of age and older are far less likely
than younger patients to receive this treatment.
76, 286
Distant stage
At this stage, the cancer has spread to distant organs and
tissues, such as the liver, lungs, peritoneum (lining of the
abdomen), or ovaries. When surgery is performed, the
goal is usually to relieve or prevent blockage of the colon
and to prevent other local complications. If there are only
a few metastases to the liver or lungs, surgery to remove
these, as well as the colon tumor, may improve survival.
Chemotherapy and targeted therapies may be given alone
or in combination to relieve symptoms and prolong
survival. A number of targeted therapies have been
approved in recent years by the US Food and Drug
Administration to treat metastatic CRC. Some of these
drugs inhibit new blood vessel growth to the tumor by
targeting a protein called vascular endothelial growth
factor (VEGF). Others interfere with cancer cell growth
by targeting the epidermal growth factor receptor
(EGFR) or other proteins. Genetic testing of tumors is
important because those with certain mutations (e.g.,
KRAS, NRAS, or BRAF) largely do not respond to these
drugs.
287
Immunotherapy drugs are also now approved to
treat a small portion of CRCs.
Rectal cancer
Surgery is usually the main treatment for rectal cancer,
often accompanied by chemotherapy and radiation
before and/or after surgery to reduce the risk of spread
and recurrence. The chemotherapy drugs used in the
treatment of rectal cancer are largely the same as those
used for colon cancer.
Carcinoma in situ
Treatment options include polypectomy (polyp removal),
local excision, or full-thickness rectal resection. This
resection may be carried out through the anus. No further
treatment is needed.
Localized stage
At this stage, the cancer has grown through the first layer
of the rectum into deeper layers, but has not spread
outside the rectal wall. Some small localized rectal
cancers may be treated by removal through the anus,
without an abdominal incision. For other tumors,
depending on the location, surgery may involve removal
of the cancer and some surrounding normal tissue
through one or more small abdominal incisions. For
cancers close to the anus, surgery may require removal
of the anus and the sphincter muscle, so a permanent
colostomy is needed (see next section for information
about colostomy). In most cases, no further treatment is
needed unless the tumor has high-risk features. Patients
who are not candidates for surgery may be treated with
radiation therapy.
Regional stage
At this stage, the cancer has grown through the wall of
the rectum, and may have spread into nearby tissues
and/or lymph nodes. Patients with regional-stage disease
28 Colorectal Cancer Facts & Figures 2020-2022
are increasingly treated with chemotherapy and radiation
(chemoradiation) before surgery. Some patients also
receive chemotherapy after surgery, although the potential
benefits are debated.
288-290
Distant stage
At this stage, the cancer has spread to distant organs and
tissues, such as the liver or lung. In rare cases, the cancer
can be successfully treated by removing all of the tumors
with surgery, along with other treatments. Otherwise,
palliative treatments (surgery, chemotherapy, and/or
radiation therapy) are used to relieve, delay, or prevent
symptoms and prolong life. Similar to colon cancer, a
number of targeted therapies have been approved to treat
select metastatic rectal cancers, including VEGF and
EGFR inhibitors.
Colostomy
When a section of the colon or rectum is removed during
surgery, the healthy parts can usually be reconnected,
allowing the patient to eliminate waste normally. When
reconnection is not immediately possible, the surgeon
connects the colon to an opening (stoma) that is made
in the skin of the abdomen, allowing waste to leave the
body. The surgical procedure to create an opening in the
body for the elimination of waste is called an ostomy.
When the stoma is connected to the colon it is called a
colostomy; when the stoma is connected to the small
intestine it is called an ileostomy. Usually a flat bag, held
in place by a special adhesive, fits over the stoma to
collect waste.
Most patients with CRC who require a colostomy need it
only temporarily, until the colon or rectum heals from
surgery. After healing takes place, usually in 6 to 8 weeks,
the surgeon reconnects the ends of the colon and closes
the stoma. A permanent colostomy is necessary more
often for rectal than for colon cancer patients.
A person with an ostomy learns to care for it with help
from doctors, nurses, and enterostomal therapists
(health professionals trained to care for people with
stomas). If surgery is expected to result in an ostomy, an
enterostomal therapist will often visit the patient before
surgery to explain what to expect and how to care for the
ostomy. They also provide information about lifestyle
issues, including emotional, physical, and sexual
concerns, as well as resources and support groups.
Side effects of colorectal cancer
treatment
Although many side effects that occur during cancer
treatment are temporary, some persist after treatment
has ended (long-term effects) and others do not arise
until several years later (late effects). Side effects should
be discussed with a clinician because treatment options
are often available. For example, antiemetic drugs can
prevent or lessen nausea and vomiting following
chemotherapy. To manage the long-term and late
effects of treatment, the American Cancer Society has
established guidelines to aid primary care clinicians in
delivering risk-based care to CRC survivors (see sidebar).
291
Short- and long-term effects of specific modes of CRC
treatment are briefly described in the following sections.
For more information on late and long-term effects of
cancer and its treatment, visit
cancer.org/treatment/
treatments-and-side-effects.html
.
Surgery
The time needed to heal after surgery is different for each
person. Patients often have some pain for the first few
days that can usually be controlled with medication. It
can take a few days to be able to eat normally again.
About 25% of patients experience a delay in bowel
function (postoperative ileus) because of bowel stress
caused by surgical manipulation, which may require an
extended hospital stay.
292
Patients are monitored for signs
of bleeding, infection, or other problems that require
immediate treatment.
Other side effects from surgery for CRC may include
fatigue, possibly for an extended period of time; frequent
or urgent bowel movements, diarrhea, constipation,
gas, and/or bloating, particularly among rectal cancer
patients; a temporary or permanent colostomy; and
urogenital/sexual dysfunction (e.g., erectile dysfunction
in men).

Colorectal Cancer Facts & Figures 2020-2022 29
Radiation therapy
Side effects of radiation therapy can include skin
irritation, nausea, diarrhea, rectal irritation and/or
painful inflammation, rectal bleeding, bladder
dysfunction (irritation, pain, and/or frequent urination),
fatigue, or sexual problems. Many of these side effects go
away after treatments are completed, but some, like
sexual problems and some degree of rectal and/or
bladder irritation, may be permanent. Late effects
include increased risk of bowel obstruction and fractures
in the bone at the base of the spine (the sacrum). In
addition, radiation to the pelvic area in women may
damage the ovaries, causing infertility. Fertility
counseling prior to treatment is recommended for
women for whom this is a concern (see Sexual function
and fertility, below). Radiation also increases the risk of
developing second cancers in exposed areas.
Chemotherapy
The chemotherapy drugs most often used in the
treatment of CRC are 5-fluorouracil (5-FU), capecitabine,
oxaliplatin, and irinotecan. Side effects depend on the
type and dosage of drugs, the length of treatment, and
individual patient characteristics. Some side effects are
temporary (e.g., hair loss), while others may persist after
treatment (e.g., numbness in the hands or feet). Some
patients may experience low blood cell counts because
chemotherapy can harm the blood-producing cells of the
bone marrow. This can increase the chance of infection
(due to a shortage of white blood cells), bleeding or
bruising after minor cuts or injuries (due to a shortage of
blood platelets), and fatigue or shortness of breath.
Targeted therapy
Targeted therapy is a newer class of drugs resulting from
an increased understanding of the molecular features of
cancer development. Targeted drugs for CRC (e.g., EGFR
and VEGF inhibitors) often have different but notable
side effects compared to conventional chemotherapy
drugs, such as dry skin or skin rash.
Sexual function and fertility
Many treatments for CRC directly or indirectly impact
sexual function and fertility in both male and female
patients.
293, 294
This is a particularly relevant issue for the
increasing number of affected young adults in their
reproductive years. The American Society for Clinical
Oncology clinical practice guidelines recommend that
fertility preservation be discussed with all new patients
at the time of diagnosis because efforts such as sperm
banking, embryo/oocyte cryopreservation (the freezing of
fertilized or unfertilized eggs), and ovarian transposition
(a surgical repositioning of the ovaries away from the
field of radiation) should be started far in advance of
treatment.
295
For more information, visit
cancer.org/
treatment/treatments-and-side-effects/physical-side-effects/
fertility-and-sexual-side-effects.html
.
American Cancer Society Colorectal
Cancer Posttreatment Survivorship
Care Guidelines
CRC patients have specific needs and concerns once
treatment ends. In 2015, a multidisciplinary expert
workgroup published evidence- and consensus-
based posttreatment care guidelines for clinicians to
aid in providing comprehensive, long-term care for
colorectal cancer survivors. These guidelines include
information on surveillance for cancer recurrence,
screening for new cancers, management of chronic
and late effects, and referrals for rehabilitation,
psychosocial and palliative care, or other specialty care.
Visit
cancer.org/health-care-professionals/american-
cancer-society-survivorship-guidelines/colorectal-
cancer-survivorship-care-guidelines.html
for full text of
the guidelines, as well as resources for clinicians.

30 Colorectal Cancer Facts & Figures 2020-2022
What Is the American Cancer Society Doing
about Colorectal Cancer?
Research
Colorectal cancer is an active area of scientific research;
studies span the cancer continuum from prevention and
early detection to treatment and beyond. As of August 1,
2019, the American Cancer Society was funding 78 grants
totaling more than $25 million in colorectal cancer
research. Examples of projects in which researchers in
the American Cancer Society Extramural Research
program are engaged include:
• Evaluating why certain colorectal cancers evade or
resist treatment
• Exploring new ways to prevent colorectal cancer by
manipulating gut microbiota
• Investigating whether increased consumption of
cooked dry beans, which have anti-inflammatory
and anti-cancer properties, could lower the risk of
colorectal cancer recurrence in survivors with obesity
• Understanding barriers to colonoscopy screening in
North and South Carolina
Examples of CRC research projects conducted within the
American Cancer Society Intramural Research program
include:
• Monitoring disparities in CRC screening, including
identifying medically underserved populations and
evaluating initiatives to reduce screening disparities
• Exploring the mechanisms underlying CRC
development, such as gene-environment interactions
• Analyzing disparities and emerging trends in
population-based CRC incidence and mortality rates
• Investigating factors associated with survival
following a CRC diagnosis
• Identifying the needs of CRC survivors as they
transition from active treatment and back into the
community care setting
• Developing population-based systems for monitoring
cancer patient-reported quality of life and treatment-
related side effects
Colorectal cancer screening
guidelines
Since 1980, the American Cancer Society has issued
evidence-based recommendations for CRC screening in
average-risk adults that are generally updated every 5
years. These recommendations are developed by an
independent Guideline Development Group of experts in
cancer epidemiology, primary care, and health services
research with the support of American Cancer Society
staff in the Center for Cancer Screening, the Intramural
Research program, and an ad hoc group of clinicians
with expertise in CRC. As part of the ongoing guideline
development process, American Cancer Society staff
monitor the medical and scientific literature for new
evidence that may support a change in the current
recommendations, as well as new information about
CRC screening that should be conveyed to clinicians
and target populations. The most recent update of the
American Cancer Society guideline for CRC screening
was published in 2018.
217
Strategies to reach the 80% in Every
Community nationwide goal
In 2014, the NCCRT launched the 80% by 2018 campaign
to raise CRC screening rates across the nation. Although
the nation as a whole did not achieve the 80% goal, it
was reached and even surpassed in some hospital and
community clinic settings, as well as in some health plans.
80% in Every Community is the new NCCRT campaign to
continue efforts to substantially reduce CRC as a major
public health problem by increasing colorectal screening
rates to 80% or higher in communities across the nation.
The NCCRT, established in 1997 by the American Cancer
Society and the Centers for Disease Control and
Colorectal Cancer Facts & Figures 2020-2022 31
Prevention, is a coalition of more than 100 member
organizations and individual experts dedicated to
reducing CRC incidence and mortality in the US through
coordinated leadership, strategic planning, and advocacy.
Over the past five years, more than 1,750 organizations
have committed to the shared goal of raising CRC
screening utilization. This initiative emphasizes evidence-
based screening activities that respond to individualized
needs, barriers, and motivations within a community.
Talking points, FAQs, press materials, downloadable
graphics, and more are available at
nccrt.org/80-in-every-
community
. The American Cancer Society is committed to
the 80% in Every Community goal as one of our major
initiatives and is implementing several key strategies in
support of this nationwide program, including playing a
major role as convener and leader of the effort.
Notably, our approximately 300-strong force of health
systems staff is playing a crucial role by engaging and
supporting key strategic partners – such as hospitals and
health systems, community health centers, state health
departments, corporate partners, payers, and state
and local coalitions – to encourage and support their
commitment to increasing the number of individuals
who are screened for colorectal cancer. Our staff work
with these partners to assist them in implementing
proven strategies that are known to increase CRC
screening rates, such as implementing provider and
patient reminders, helping providers assess and track
their screening rates, implementing quality screening
navigation, and using the power of the provider
recommendation. The American Cancer Society
Community Health Advocates implementing Nationwide
Grants for Empowerment and Equity (CHANGE)
program provides one avenue for health systems staff to
collaborate at the community level. CHANGE provides
both financial and technical assistance to federally
qualified health centers (FQHCs) and other community
partners to build capacity and implement interventions
to increase cancer screening rates among low income,
low education, and racially diverse populations. Since
2011, the American Cancer Society has awarded 252
grants to community-based partners to implement
evidence-based CRC interventions, reaching over one
million men and women with cancer prevention and
early detection education and outreach and providing
more than 332,000 CRC screening exams. CHANGE
grant-funded FQHCs have been found to increase
screening rates faster than nonfunded FQHCs.
Additionally, the American Cancer Society works to
unify and magnify effective communication to the public
about the value of CRC screening through multiple
channels. These activities include the development and
implementation of targeted traditional and social media
strategies to motivate unscreened consumers to get
screened. Finally, we lead by example, encouraging our own
staff and volunteers to be up to date with recommended
cancer screening tests. Through these actions, the
American Cancer Society is working to leverage the
energy of multiple and diverse partners to make history
and achieve this remarkable public health goal.
Advocacy
Our nonprofit, nonpartisan advocacy affiliate, the
American Cancer Society Cancer Action Network
SM
(ACS CAN), is involved in advocacy efforts at both the
federal and state levels that increase access to quality
CRC screening, treatment, and care for all adults. In
partnership with the American Cancer Society, the
Centers for Disease Control and Prevention (CDC), and
the National Colorectal Cancer Roundtable, as well as
over 1,750 other organizations, ACS CAN hopes to reach
the goal of achieving 80% or higher CRC screening rates
in every community. Following are some of the efforts the
American Cancer Society and ACS CAN are involved in to
help reach that goal:
• Implementing the provisions in the Patient Protection
and Affordable Care Act, more commonly referred to
as the Affordable Care Act or ACA. The reforms in
the ACA, which was signed into law in March 2010,
represent a profound structural change in how
insurance operates and how consumers and patients
use the health insurance system. ACS CAN and the
American Cancer Society have a significant impact
at the federal and state levels through our advocacy
work, which urges policy makers to implement the
law to ensure that all Americans have access to

32 Colorectal Cancer Facts & Figures 2020-2022
evidence-based prevention, early detection, and
treatment services critical to CRC patients. In
particular, ACS CAN has advocated for expansion of
Medicaid in all 50 states for those individuals up to
138% of the federal poverty level, as it was originally
intended by the ACA. This would ensure that low-
income, uninsured, and underinsured Americans
will have access to the same CRC services as those
in private and other public insurances.
• Advocating for clarification on ACA-required coverage
of CRC screening modalities as recommended by
the United States Preventive Services Task Force
(USPSTF). This includes clarifying that there should be
no cost sharing requirements for a colonoscopy that is
ordered to complete the screening process following
a positive CRC stool-based screening test (follow-up
colonoscopy), cost sharing for short interval screening
following the removal of adenomatous polyps during a
screening colonoscopy, and other ambiguous coverage
issues related to CRC screening.
• Supporting the work and maintaining funding for the
CDC’s Colorectal Cancer Control Program (CRCCP),
which currently provides funding to 30 grantees
across the US. The CRCCP’s goal is to increase
CRC screening rates in targeted populations by
implementing evidence-based, system-level
interventions through partnerships with health
systems. The program provides grants for both
population-based education and awareness campaigns
and efforts to improve access to vital CRC screening
tests and follow-up services for at-risk low-income,
uninsured, and underinsured individuals between
the ages of 50 and 75.
• Advocating for passage of the Removing Barriers to
Colorectal Cancer Screening Act of 2019, which will
ease the financial burden of people living on a fixed
income by allowing Medicare beneficiaries to receive
screenings without coinsurance, even when a polyp is
removed. This legislation would help increase
screening rates and reduce the incidence of CRC.
• Advocating for state legislation to ensure insurance
coverage in each state aligns with the American
Cancer Society’s evidence-based CRC guideline,
which recommends average-risk adults begin
screening at age 45
• Engaging governors, mayors, and state legislators to
inform them about the 80% in Every Community
initiative, urging them to help make CRC screening
a priority. Specifically, ACS CAN is urging state and
city governments to work across all sectors to increase
screening rates by eliminating cost and access barriers
to screening and by investing in or creating a state
CRC screening and control program.
Sources of Statistics
New cancer cases. The estimated number of CRC cases
in the US in 2020 was projected using a spatiotemporal
model based on incidence data from 50 states and the
District of Columbia for the years 2002 to 2016 that met
the North American Association of Central Cancer
Registries’ (NAACCR’s) high-quality data standards for
incidence. For more information on this method, please
see Zhu et al.
296
Incidence rates. Incidence rates are defined as the number
of people newly diagnosed with cancer during a given time
period per 100,000 population at risk. CRC incidence rates
for the US were calculated using case data from the
Surveillance, Epidemiology, and End Results (SEER)
Program of the National Cancer Institute, the National
Program of Cancer Registries of the Centers for Disease
Control and Prevention, and NAACCR, and population
data collected by the US Census Bureau. Incidence rates
for Alaska Natives are based on cases reported by the
Alaska Native Tumor Registry (ANTR) of the SEER
Program; rates for American Indians excluding Alaska
Natives are based on NAACCR Purchased/Referred Care
Delivery Area (PRCDA) county regions excluding the
ANTR. Incidence rates were age adjusted to the 2000 US
standard population and adjusted for delays in reporting
when possible. Trends exclude appendix.

Colorectal Cancer Facts & Figures 2020-2022 33
Estimated cancer deaths. The estimated number of CRC
deaths in the US in 2020 was calculated by fitting the
actual number of CRC deaths from 2003 through 2017 to
a statistical model that forecasts the number of deaths
three years ahead. The actual number of deaths was
obtained from the National Center for Health Statistics
(NCHS) at the Centers for Disease Control and Prevention.
For more information on this method, please see Chen
et al.
297
Mortality rates. Mortality rates, or death rates, are
defined as the number of people who die from cancer
during a given time period per 100,000 population.
Mortality rates are based on counts of cancer deaths
compiled by NCHS and population data from the US
Census Bureau. Death rates for Alaska Natives are based
on deaths occurring in the Alaska Community Health
Service Delivery Area region. Due to data limitations,
there may be a small degree of cross-contamination
between rates for American Indians and Alaska Natives
where they are presented separately. Death rates are age
adjusted to the 2000 US standard population.
Survival. Relative and cause-specific (herein referred to
as cancer-specific) survival rates were calculated using
data from the SEER registries. Relative survival rates
account for normal life expectancy by comparing overall
survival among a group of cancer patients to that of
people not diagnosed with cancer who are of the same
age, race, and sex. Cancer-specific survival is the
probability of not dying from a specific cancer (e.g.,
colorectal) within a specified time period following a
diagnosis. Cancer-specific survival was used for rates by
race and ethnicity because reliable estimates of normal
life expectancy historically have not been available by
Hispanic ethnicity or for Asians/Pacific Islanders and
American Indians/Alaska Natives.
Screening. The national prevalence of CRC screening
was estimated from the National Health Interview Survey
(NHIS) 2018 data file, obtained from NCHS, released in
2019 (
cdc.gov/nchs/nhis.htm
). The NHIS is conducted by the
US Census Bureau and is designed to provide national
prevalence estimates on health characteristics such as
cancer screening behaviors. Data are collected through
in-person interviews.
CRC screening prevalence by state was estimated from
the 2018 Behavioral Risk Factor Surveillance System
(BRFSS) public use data files, obtained from the National
Center for Chronic Disease Prevention and Health
Promotion, Centers for Disease Control and Prevention.
The BRFSS is a telephone survey designed to provide
state prevalence estimates of health behaviors and was
conducted by state health departments.
Important note about estimated cases and deaths.
The projected number of new cancer cases and deaths
for the current year are model based. For this reason,
we discourage the use of our estimates to track cancer
trends. Age-standardized incidence and mortality rates
are used to track cancer incidence and mortality trends.
References
1. Lee GH, Malietzis G, Askari A, Bernardo D, Al-Hassi HO, Clark SK.
Is right-sided colon cancer different to left-sided colorectal cancer? –
a systematic review. Eur J Surg Oncol. 2015;41(3):300-308.
2. Burón Pust A, Alison R, Blanks R, et al. Heterogeneity of colorectal
cancer risk by tumour characteristics: Large prospective study of UK
women. Int J Cancer. 2017;140(5):1082-1090.
3. Sineshaw HM, Ng K, Flanders WD, Brawley OW, Jemal A. Factors
That Contribute to Differences in Survival of Black vs White Patients
With Colorectal Cancer. Gastroenterology. 2018;154(4):906-915 e907.
4. Siegel RL, Miller KD, Fedewa SA, et al. Colorectal cancer statistics,
2017. CA Cancer J Clin. 2017;67(3):177-193.
5. Corley DA, Jensen CD, Marks AR, et al. Variation of Adenoma
Prevalence by Age, Sex, Race, and Colon Location in a Large
Population: Implications for Screening and Quality Programs. Clin
Gastroenterol Hepatol. 2013;11(2):172-180.
6. Levine JS, Ahnen DJ. Clinical practice. Adenomatous polyps of the
colon. N Engl J Med. 2006;355(24):2551-2557.
7. Risio M. The natural history of adenomas. Best Pract Res Clin
Gastroenterol. 2010;24(3):271-280.
8. Winawer SJ, Zauber AG. The advanced adenoma as the primary
target of screening. Gastrointest Endosc Clin N Am. 2002;12(1):1-9, v.
34 Colorectal Cancer Facts & Figures 2020-2022
9. Stryker SJ, Wolff BG, Culp CE, Libbe SD, Ilstrup DM, MacCarty
RL. Natural history of untreated colonic polyps. Gastroenterology.
1987;93(5):1009-1013.
10. Pickhardt PJ, Kim DH, Pooler BD, et al. Assessment of volumetric
growth rates of small colorectal polyps with CT colonography: a
longitudinal study of natural history. Lancet Oncol. 2013;14(8):711-720.
11. Øines M, Helsingen LM, Bretthauer M, Emilsson L. Epidemiology
and risk factors of colorectal polyps. Best Pract Res Clin Gastroenterol.
2017;31(4):419-424.
12. Rex DK, Ahnen DJ, Baron JA, et al. Serrated lesions of the
colorectum: review and recommendations from an expert panel. Am J
Gastroenterol. 2012;107(9):1315-1329; quiz 1314, 1330.
13. Tauriello DVF, Calon A, Lonardo E, Batlle E. Determinants of
metastatic competency in colorectal cancer. Mol Oncol. 2017;11(1):
97-119.
14. Quere P, Facy O, Manfredi S, et al. Epidemiology, Management,
and Survival of Peritoneal Carcinomatosis from Colorectal Cancer: A
Population-Based Study. Dis Colon Rectum. 2015;58(8):743-752.
15. Yin D, Morris CR, Bates JH, German RR. Effect of misclassified
underlying cause of death on survival estimates of colon and rectal
cancer. J Natl Cancer Inst. 2011;103(14):1130-1133.
16. Colon Cancer Alliance Announces Corporate Name Change
(
ccalliance.org/news/press-releases/colon-cancer-alliance-announces-corporate-
name-change
) [press release]. Washington DC 2017.
17. Siegel RL, Fedewa SA, Anderson WF, et al. Colorectal cancer
incidence patterns in the United States, 1974-2013. J Natl Cancer Inst.
2017;109(8).
18. Miller KD, Nogueira L, Mariotto AB, et al. Cancer treatment and
survivorship statistics, 2019. CA Cancer J Clin. 2019;69(5):363-385.
19. Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2020. CA Cancer J
Clin. 2020;70(1):7-34.
20. Lieberman DA, Williams JL, Holub JL, et al. Race, ethnicity,
and sex affect risk for polyps >9 mm in average-risk individuals.
Gastroenterology. 2014;147(2):351-358; quiz e314-355.
21. Ferlitsch M, Reinhart K, Pramhas S, et al. Sex-specific
prevalence of adenomas, advanced adenomas, and colorectal
cancer in individuals undergoing screening colonoscopy. JAMA.
2011;306(12):1352-1358.
22. Samadder NJ, Curtin K, Tuohy TMF, et al. Characteristics
of Missed or Interval Colorectal Cancer and Patient Survival: A
Population-Based Study. Gastroenterology. 2014;146(4):950-960.
23. Murphy G, Devesa SS, Cross AJ, Inskip PD, McGlynn KA, Cook MB.
Sex disparities in colorectal cancer incidence by anatomic subsite,
race and age. Int J Cancer. 2011;128(7):1668-1675.
24. Howlader N, Noone AM, Krapcho M, et al., eds. SEER Cancer
Statistics Review, 1975-2016. Bethesda, MD: National Cancer Institute;
2019.
25. Ries LAG, Eisner MP, Kosary CL, et al., eds. SEER Cancer Statistics
Review, 1973-1999. Bethesda, MD: National Cancer Institute; 2002.
26. Carethers JM, Doubeni CA. Causes of Socioeconomic Disparities
in Colorectal Cancer and Intervention Framework and Strategies.
Gastroenterology. 2019.
27. Semega JL, Kollar MA, Mohanty A. Income and Poverty in the
United States: 2018. In. U.S. Government Printing Office, Washington,
DC: U.S. Census Bureau; 2019.
28. Doubeni CA, Laiyemo AO, Major JM, et al. Socioeconomic status
and the risk of colorectal cancer: an analysis of more than a half
million adults in the National Institutes of Health-AARP Diet and
Health Study. Cancer. 2012;118(14):3636-3644.
29. Doubeni CA, Major JM, Laiyemo AO, et al. Contribution of
behavioral risk factors and obesity to socioeconomic differences in
colorectal cancer incidence. J Natl Cancer Inst. 2012;104(18):1353-1362.
30. Lansdorp-Vogelaar I, Kuntz KM, Knudsen AB, van Ballegooijen
M, Zauber AG, Jemal A. Contribution of screening and survival
differences to racial disparities in colorectal cancer rates. Cancer
Epidemiol Biomarkers Prev. 2012;21(5):728-736.
31. Fedewa SA, Flanders WD, Ward KC, et al. Racial and Ethnic
Disparities in Interval Colorectal Cancer Incidence: A Population-
Based Cohort Study. Ann Intern Med. 2017;166(12):857-866.
32. Laiyemo AO, Doubeni C, Pinsky PF, et al. Race and colorectal
cancer disparities: health-care utilization vs different cancer
susceptibilities. J Natl Cancer Inst. 2010;102(8):538-546.
33. Torre LA, Sauer AM, Chen MS, Jr., Kagawa-Singer M, Jemal A,
Siegel RL. Cancer statistics for Asian Americans, Native Hawaiians,
and Pacific Islanders, 2016: Converging incidence in males and
females. CA Cancer J Clin. 2016;66(3):182-202.
34. Kelly JJ, Alberts SR, Sacco F, Lanier AP. Colorectal cancer in alaska
native people, 2005-2009. Gastrointest Cancer Res. 2012;5(5):149-154.
35. Perdue DG, Haverkamp D, Perkins C, Daley CM, Provost E.
Geographic variation in colorectal cancer incidence and mortality,
age of onset, and stage at diagnosis among American Indian and
Alaska Native people, 1990-2009. Am J Public Health. 2014;104 Suppl
3:S404-414.
36. McMahon BJ, Bruce MG, Koch A, et al. The diagnosis and
treatment of Helicobacter pylori infection in Arctic regions with a
high prevalence of infection: Expert Commentary. Epidemiol Infect.
2016;144(2):225-233.
37. Sonnenberg A, Genta RM. Helicobacter pylori is a risk factor for
colonic neoplasms. Am J Gastroenterol. 2013;108(2):208-215.
38. Butt J, Varga MG, Blot WJ, et al. Serologic Response to Helicobacter
pylori Proteins Associated With Risk of Colorectal Cancer Among
Diverse Populations in the United States. Gastroenterology.
2019;156(1):175-186.e172.
39. Conway AA, Gerry JM, Sacco F, Wren SM. High Prevalence of
Adenomatous Polyps in Alaska Native People Aged 40-49 years. J Surg
Res. 2019;243:524-530.
40. Day LW, Espey DK, Madden E, Segal M, Terdiman JP. Screening
prevalence and incidence of colorectal cancer among American
Indian/Alaskan natives in the Indian Health Service. Dig Dis Sci.
2011;56(7):2104-2113.
41. Carmichael H, Cowan M, McIntyre R, Velopulos C. Disparities
in colorectal cancer mortality for rural populations in the United
States: Does screening matter? Am J Surg. 2019.
42. Berkowitz Z, Zhang X, Richards TB, Nadel M, Peipins LA, Holt J.
Multilevel Small-Area Estimation of Colorectal Cancer Screening in the
United States. Cancer Epidemiol Biomarkers Prev. 2018;27(3):245-253.
43. Edwards BK, Ward E, Kohler BA, et al. Annual report to the nation
on the status of cancer, 1975-2006, featuring colorectal cancer trends
and impact of interventions (risk factors, screening, and treatment)
to reduce future rates. Cancer. 2010;116(3):544-573.
Colorectal Cancer Facts & Figures 2020-2022 35
44. National Center for Health Statistics, Division of Health Interview
Statistics. National Health Interview Survey Public Use Data File
2018. In. Centers for Disease Control and Prevention. Hyattsville,
MD.2019.
45. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal
cancer by colonoscopic polypectomy. The National Polyp Study
Workgroup. N Engl J Med. 1993;329(27):1977-1981.
46. Legler JM, Feuer EJ, Potosky AL, Merrill RM, Kramer BS. The
role of prostate-specific antigen (PSA) testing patterns in the recent
prostate cancer incidence decline in the United States. Cancer Causes
Control. 1998;9(5):519-527.
47. Siegel RL, Torre LA, Soerjomataram I, et al. Global patterns and
trends in colorectal cancer incidence in young adults. Gut. 2019.
48. Irby K, Anderson WF, Henson DE, Devesa SS. Emerging and
widening colorectal carcinoma disparities between Blacks and
Whites in the United States (1975-2002). Cancer Epidemiol Biomarkers
Prev. 2006;15(4):792-797.
49. Siegel RL, Medhanie GA, Fedewa SA, Jemal A. State Variation in
Early-Onset Colorectal Cancer in the United States, 1995-2015. J Natl
Cancer Inst. 2019;111(10):1104-1106.
50. Surveillance, Epidemiology and End Results (SEER) Program,
SEER*Stat Database: NAACCR Incidence - CiNA Analytic File, 1995-
2016, for NHIAv2 Origin, Custom File With County, ACS Facts and
Figures projection Project, North American Association of Central
Cancer Registries. 2019.
51. Surveillance, Epidemiology, and End Results (SEER) Program
(
www.seer.cancer.gov
) SEER*Stat Database: Incidence – SEER 13 Regs
Research Data with Delay-Adjustment, Malignant Only, Nov 2018
Sub (1992-2016) <Katrina/Rita Population Adjustment> – Linked To
County Attributes – Total U.S., 1969-2017 Counties, National Cancer
Institute, DCCPS, Surveillance Research Program, Surveillance
Systems Branch, released April 2019, based on the November 2018
submission. 2019.
52. Zauber AG. The impact of screening on colorectal cancer
mortality and incidence: has it really made a difference? Dig Dis Sci.
2015;60(3):681-691.
53. Robbins AS, Siegel RL, Jemal A. Racial disparities in stage-specific
colorectal cancer mortality rates from 1985 to 2008. J Clin Oncol.
2012;30(4):401-405.
54. Siegel RL, Sahar L, Robbins A, Jemal A. Where can colorectal
cancer screening interventions have the most impact? Cancer
Epidemiol Biomarkers Prev. 2015;24(8):1151-1156.
55. Liang PS, Mayer JD, Wakefield J, Ko CW. Temporal Trends in
Geographic and Sociodemographic Disparities in Colorectal Cancer
Among Medicare Patients, 1973-2010. J Rural Health. 2016;33(4):361-
370.
56. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J
Clin. 2019;69(1):7-34.
57. Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011:
the impact of eliminating socioeconomic and racial disparities on
premature cancer deaths. CA Cancer J Clin. 2011;61(4):212-236.
58. Melkonian SC, Jim MA, Haverkamp D, et al. Disparities in Cancer
Incidence and Trends among American Indians and Alaska Natives
in the United States, 2010-2015. Cancer Epidemiol Biomarkers Prev.
2019;28(10):1604-1611.
59. Surveillance, Epidemiology, and End Results (SEER) Program
(
www.seer.cancer.gov
) SEER*Stat Database: Incidence – SEER 18 Regs
Research Data + Hurricane Katrina Impacted Louisiana Cases, Nov
2018 Sub (2000-2016) – Linked To County Attributes – Total U.S.,
1969-2017 Counties, National Cancer Institute, DCCPS, Surveillance
Research Program, Surveillance Systems Branch, released April 2019,
based on the November 2018 submission. 2019.
60. Andrew AS, Parker S, Anderson JC, et al. Risk Factors for
Diagnosis of Colorectal Cancer at a Late Stage: a Population-Based
Study. J Gen Intern Med. 2018;33(12):2100-2105.
61. Ward E, Jemal A, Cokkinides V, et al. Cancer disparities by race/
ethnicity and socioeconomic status. CA Cancer J Clin. 2004;54(2):78-93.
62. Jemal A, Ward EM, Johnson CJ, et al. Annual Report to the Nation
on the Status of Cancer, 1975-2014, Featuring Survival. J Natl Cancer
Inst. 2017;109(9).
63. Yang Y, Wang G, He J, et al. Gender differences in colorectal
cancer survival: A meta-analysis. Int J Cancer. 2017;141(10):1942-1949.
64. Petrelli F, Tomasello G, Borgonovo K, et al. Prognostic Survival
Associated With Left-Sided vs Right-Sided Colon Cancer: A Systematic
Review and Meta-analysis. JAMA Oncology. 2017;3(2):211-219.
65. Karim S, Brennan K, Nanji S, Berry SR, Booth CM. Association
Between Prognosis and Tumor Laterality in Early-Stage Colon
Cancer. JAMA Oncology. 2017;3(10):1386-1392.
66. Bach PB, Schrag D, Brawley OW, Galaznik A, Yakren S, Begg
CB. Survival of blacks and whites after a cancer diagnosis. JAMA.
2002;287(16):2106-2113.
67. Ellis L, Canchola AJ, Spiegel D, Ladabaum U, Haile R, Gomez SL.
Racial and Ethnic Disparities in Cancer Survival: The Contribution
of Tumor, Sociodemographic, Institutional, and Neighborhood
Characteristics. 2018;36(1):25-33.
68. Halpern MT, Holden DJ. Disparities in timeliness of care
for U.S. Medicare patients diagnosed with cancer. Curr Oncol.
2012;19(6):e404-e413.
69. Lai Y, Wang C, Civan JM, et al. Effects of Cancer Stage and
Treatment Differences on Racial Disparities in Survival From Colon
Cancer: A United States Population-Based Study. Gastroenterology.
2016;150(5):1135-1146.
70. Butler EN, Chawla N, Lund J, Harlan LC, Warren JL, Yabroff KR.
Patterns of colorectal cancer care in the United States and Canada: a
systematic review. J Natl Cancer Inst Monogr. 2013;2013(46):13-35.
71. Eaglehouse YL, Georg MW, Shriver CD, Zhu K. Racial
Comparisons in Timeliness of Colon Cancer Treatment in an Equal-
Access Health System. J Natl Cancer Inst. 2019.
72. Yothers G, Sargent DJ, Wolmark N, et al. Outcomes among black
patients with stage II and III colon cancer receiving chemotherapy:
an analysis of ACCENT adjuvant trials. J Natl Cancer Inst.
2011;103(20):1498-1506.
73. Haller DG, Catalano PJ, Macdonald JS, et al. Phase III study
of fluorouracil, leucovorin, and levamisole in high-risk stage II
and III colon cancer: final report of Intergroup 0089. J Clin Oncol.
2005;23(34):8671-8678.
74. Doubeni CA, Rustgi A. Racial Disparities in Colorectal Cancer
Survival: Is Elimination of Variation in Care the Cure? J Natl Cancer
Inst. 2015;107(10).
75. Kopetz S, Chang GJ, Overman MJ, et al. Improved survival in
metastatic colorectal cancer is associated with adoption of hepatic
resection and improved chemotherapy. J Clin Oncol. 2009;27(22):3677-
3683.
36 Colorectal Cancer Facts & Figures 2020-2022
76. Murphy CC, Harlan LC, Lund JL, Lynch CF, Geiger AM. Patterns of
Colorectal Cancer Care in the United States: 1990-2010. J Natl Cancer
Inst. 2015;107(10).
77. Piawah S, Venook AP. Targeted therapy for colorectal cancer
metastases: A review of current methods of molecularly targeted
therapy and the use of tumor biomarkers in the treatment of
metastatic colorectal cancer. Cancer. 2019.
78. Surveillance, Epidemiology, and End Results (SEER) Program,
SEER*Stat Database: Incidence – SEER 9 Regs Research Data, Nov
2018 Sub (1975-2016) <Katrina/Rita Population Adjustment> –
Linked To County Attributes – Total U.S., 1969-2017 Counties,
National Cancer Institute, DCCPS, Surveillance Research Program,
Surveillance Systems Branch, released April 2019. 2019.
79. Sineshaw HM, Robbins AS, Jemal A. Disparities in survival
improvement for metastatic colorectal cancer by race/ethnicity and
age in the United States. Cancer Causes Control. 2014;25(4):419-423.
80. Islami F, Goding Sauer A, Miller KD, et al. Proportion and number
of cancer cases and deaths attributable to potentially modifiable risk
factors in the United States. CA Cancer J Clin. 2018;68(1):31-54.
81. Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A,
Bray F. Global patterns and trends in colorectal cancer incidence and
mortality. Gut. 2016.
82. Kohler LN, Garcia DO, Harris RB, Oren E, Roe DJ, Jacobs
ET. Adherence to Diet and Physical Activity Cancer Prevention
Guidelines and Cancer Outcomes: A Systematic Review. Cancer
Epidemiol Biomarkers Prev. 2016;25(7):1018-1028.
83. Patel SG, Ahnen DJ. Familial colon cancer syndromes: an update
of a rapidly evolving field. Curr Gastroenterol Rep. 2012;14(5):428-438.
84. Lowery JT, Ahnen DJ, Schroy III PC, et al. Understanding
the contribution of family history to colorectal cancer risk and
its clinical implications: A state-of-the-science review. Cancer.
2016;122(17):2633-2645.
85. Jones WF, Ahnen DJ, Schroy III PC. Improving on-time colorectal
cancer screening through lead time messaging. Cancer. 2019.
86. Samadder NJ, Smith KR, Hanson H, et al. Increased Risk of
Colorectal Cancer Among Family Members of All Ages, Regardless
of Age of Index Case at Diagnosis. Clin Gastroenterol Hepatol.
2015;13(13):2305-2311 e2301-2302.
87. Tuohy TM, Rowe KG, Mineau GP, Pimentel R, Burt RW, Samadder
NJ. Risk of colorectal cancer and adenomas in the families of
patients with adenomas: a population-based study in Utah. Cancer.
2014;120(1):35-42.
88. Peters U, Hutter CM, Hsu L, et al. Meta-analysis of new
genomewide association studies of colorectal cancer risk. Hum Genet.
2012;131(2):217-234.
89. Flynn BS, Wood ME, Ashikaga T, Stockdale A, Dana GS, Naud
S. Primary care physicians’ use of family history for cancer risk
assessment. BMC Family Practice. 2010;11(1):45.
90. Wood ME, Kadlubek P, Pham TH, et al. Quality of cancer family
history and referral for genetic counseling and testing among
oncology practices: a pilot test of quality measures as part of the
American Society of Clinical Oncology Quality Oncology Practice
Initiative. J Clin Oncol. 2014;32(8):824-829.
91. Yurgelun MB, Kulke MH, Fuchs CS, et al. Cancer Susceptibility
Gene Mutations in Individuals With Colorectal Cancer. J Clin Oncol.
2017;35(10):1086-1095.
92. Win AK, Lindor NM, Young JP, et al. Risks of primary extracolonic
cancers following colorectal cancer in lynch syndrome. J Natl Cancer
Inst. 2012;104(18):1363-1372.
93. Lynch HT, Snyder CL, Shaw TG, Heinen CD, Hitchins MP.
Milestones of Lynch syndrome: 1895-2015. Nat Rev Cancer.
2015;15(3):181-194.
94. Moller P, Seppala TT, Bernstein I, et al. Cancer risk and survival
in path_MMR carriers by gene and gender up to 75 years of age:
a report from the Prospective Lynch Syndrome Database. Gut.
2018;67(7):1306-1316.
95. Hampel H, Stephens JA, Pukkala E, et al. Cancer Risk in
Hereditary Nonpolyposis Colorectal Cancer Syndrome: Later Age of
Onset. Gastroenterology. 2005;129(2):415-421.
96. Pearlman R, Frankel WL, Swanson B, et al. Prevalence and
Spectrum of Germline Cancer Susceptibility Gene Mutations
Among Patients With Early-Onset Colorectal Cancer. JAMA Oncol.
2017;3(4):464-471.
97. Win AK, Jenkins MA, Dowty JG, et al. Prevalence and Penetrance
of Major Genes and Polygenes for Colorectal Cancer. Cancer
Epidemiol Biomarkers Prev. 2017;26(3):404-412
98. Møller P, Seppälä T, Bernstein I, et al. Cancer incidence and
survival in Lynch syndrome patients receiving colonoscopic and
gynaecological surveillance: first report from the prospective Lynch
syndrome database. Gut. 2017;66(3):464-472.
99. Gupta S, Provenzale D, Llor X, et al. NCCN Guidelines Insights:
Genetic/Familial High-Risk Assessment: Colorectal, Version 2.2019. J
Natl Compr Canc Netw. 2019;17(9):1032-1041.
100. Sepulveda AR, Hamilton SR, Allegra CJ, et al. Molecular
Biomarkers for the Evaluation of Colorectal Cancer: Guideline From
the American Society for Clinical Pathology, College of American
Pathologists, Association for Molecular Pathology, and the American
Society of Clinical Oncology. J Clin Oncol. 2017;35(13):1453-1486.
101. Cohen SA, Laurino M, Bowen DJ, et al. Initiation of universal
tumor screening for Lynch syndrome in colorectal cancer patients as
a model for the implementation of genetic information into clinical
oncology practice. Cancer. 2016;122(3):393-401.
102. Green RF, Ari M, Kolor K, et al. Evaluating the role of public
health in implementation of genomics-related recommendations:
a case study of hereditary cancers using the CDC Science Impact
Framework. Genet Med. 2019;21(1):28-37.
103. Leoz ML, Carballal S, Moreira L, Ocaña T, Balaguer F. The genetic
basis of familial adenomatous polyposis and its implications for
clinical practice and risk management. Appl Clin Genet. 2015;8:95-107.
104. Aretz S, Uhlhaas S, Caspari R, et al. Frequency and parental
origin of de novo APC mutations in familial adenomatous polyposis.
Eur J Hum Genet. 2004;12(1):52-58.
105. Lynch HT, Smyrk T, McGinn T, et al. Attenuated familial
adenomatous polyposis (AFAP). A phenotypically and genotypically
distinctive variant of FAP. Cancer. 1995;76(12):2427-2433.
106. Vasen HFA, Tomlinson I, Castells A. Clinical management of
hereditary colorectal cancer syndromes. Nat Rev Gastroenterol
Hepatol. 2015;12(2):88-97.
107. Mersch J, Jackson MA, Park M, et al. Cancers associated with
BRCA1 and BRCA2 mutations other than breast and ovarian. Cancer.
2015;121(2):269-275.
108. Oh M, McBride A, Yun S, et al. BRCA1 and BRCA2 Gene
Mutations and Colorectal Cancer Risk: Systematic Review and
Metaanalysis. J Natl Cancer Inst. 2018;110(11):1178-1189.
Colorectal Cancer Facts & Figures 2020-2022 37
109. Mysliwiec PA, Cronin KA, Schatzkin A. Chapter 5: New
Malignancies Following Cancer of the Colon, Rectum, and Anus. In:
New Malignancies Among Cancer Survivors: SEER Cancer Registries,
1973-2000. Bethesda, MD: National Cancer Institute; 2006.
110. Yang L, Xiong Z, Xie QK, et al. Second primary colorectal
cancer after the initial primary colorectal cancer. BMC Cancer.
2018;18(1):931.
111. Ren J, Kirkness CS, Kim M, Asche CV, Puli S. Long-term risk of
colorectal cancer by gender after positive colonoscopy: population-
based cohort study. Curr Med Res Opin. 2016;32(8):1367-1374.
112. Teepen JC, Kok JL, van Leeuwen FE, et al. Colorectal Adenomas
and Cancers After Childhood Cancer Treatment: A DCOG-LATER
Record Linkage Study. J Natl Cancer Inst. 2018;110(7):758-767.
113. Wallis CJD, Mahar AL, Choo R, et al. Second malignancies
after radiotherapy for prostate cancer: systematic review and
metaanalysis. BMJ. 2016;352:i851.
114. Groot HJ, Lubberts S, Wit Rd, et al. Risk of Solid Cancer After
Treatment of Testicular Germ Cell Cancer in the Platinum Era. J Clin
Oncol. 2018;36(24):2504-2513.
115. Lutgens MW, van Oijen MG, van der Heijden GJ, Vleggaar FP,
Siersema PD, Oldenburg B. Declining risk of colorectal cancer in
inflammatory bowel disease: an updated meta-analysis of population-
based cohort studies. Inflamm Bowel Dis. 2013;19(4):789-799.
116. Beaugerie L, Itzkowitz SH. Cancers complicating inflammatory
bowel disease. N Engl J Med. 2015;372(15):1441-1452.
117. Castano-Milla C, Chaparro M, Gisbert JP. Systematic review with
meta-analysis: the declining risk of colorectal cancer in ulcerative
colitis. Aliment Pharmacol Ther. 2014;39(7):645-659.
118. Bonovas S, Fiorino G, Lytras T, Nikolopoulos G, Peyrin-
Biroulet L, Danese S. Systematic review with meta-analysis: use
of 5-aminosalicylates and risk of colorectal neoplasia in patients
with inflammatory bowel disease. Aliment Pharmacol Ther.
2017;45(9):1179-1192.
119. Lu MJ, Qiu XY, Mao XQ, Li XT, Zhang HJ. Systematic review with
metaanalysis: thiopurines decrease the risk of colorectal neoplasia in
patients with inflammatory bowel disease. Aliment Pharmacol Ther.
2018;47(3):318-331.
120. Jewel Samadder N, Valentine JF, Guthery S, et al. Colorectal
Cancer in Inflammatory Bowel Diseases: A Population-Based Study
in Utah. Dig Dis Sci. 2017;62(8):2126-2132.
121. Xu F, Dahlhamer JM, Zammitti EP, Wheaton AG, Croft JB.
Health-Risk Behaviors and Chronic Conditions Among Adults with
Inflammatory Bowel Disease – United States, 2015 and 2016. MMWR
Morb Mortal Wkly Rep. 2018;67(6):190-195.
122. Kappelman MD, Moore KR, Allen JK, Cook SF. Recent trends
in the prevalence of Crohn’s disease and ulcerative colitis in a
commercially insured US population. Dig Dis Sci. 2013;58(2):519-525.
123. Tsilidis KK, Kasimis JC, Lopez DS, Ntzani EE, Ioannidis JP.
Type 2 diabetes and cancer: umbrella review of meta-analyses of
observational studies. BMJ. 2015;350:g7607.
124. Ma Y, Yang W, Song M, et al. Type 2 diabetes and risk of
colorectal cancer in two large U.S. prospective cohorts. Br J Cancer.
2018;119(11):1436-1442.
125. Larsson SC, Giovannucci E, Wolk A. Diabetes and colorectal
cancer incidence in the cohort of Swedish men. Diabetes Care.
2005;28(7):1805-1807.
126. Currie CJ, Poole CD, Gale EA. The influence of glucoselowering
therapies on cancer risk in type 2 diabetes. Diabetologia.
2009;52(9):1766-1777.
127. Libby G, Donnelly LA, Donnan PT, Alessi DR, Morris AD, Evans
JM. New users of metformin are at low risk of incident cancer: a
cohort study among people with type 2 diabetes. Diabetes Care.
2009;32(9):1620-1625.
128. Lee MS, Hsu CC, Wahlqvist ML, Tsai HN, Chang YH, Huang YC.
Type 2 diabetes increases and metformin reduces total, colorectal,
liver and pancreatic cancer incidences in Taiwanese: a representative
population prospective cohort study of 800,000 individuals. BMC
Cancer. 2011;11:20.
129. Ruiter R, Visser LE, van Herk-Sukel MP, et al. Lower risk of
cancer in patients on metformin in comparison with those on
sulfonylurea derivatives: results from a large population-based
follow-up study. Diabetes Care. 2012;35(1):119-124.
130. Singh S, Singh H, Singh PP, Murad MH, Limburg PJ. Antidiabetic
medications and the risk of colorectal cancer in patients with
diabetes mellitus: a systematic review and meta-analysis. Cancer
Epidemiol Biomarkers Prev. 2013;22(12):2258-2268.
131. Home PD, Kahn SE, Jones NP, et al. Experience of malignancies
with oral glucose-lowering drugs in the randomised controlled
ADOPT (A Diabetes Outcome Progression Trial) and RECORD
(Rosiglitazone Evaluated for Cardiovascular Outcomes and
Regulation of Glycaemia in Diabetes) clinical trials. Diabetologia.
2010;53(9):1838-1845.
132. Iyengar A, Gold HT, Becker DJ. Association of diabetes with
colorectal cancer treatment and outcomes. J Clin Oncol. 2018;36(15_
suppl):e18752-e18752.
133. Geiss LS, Wang J, Cheng YJ, et al. Prevalence and incidence
trends for diagnosed diabetes among adults aged 20 to 79 years,
United States, 1980-2012. JAMA. 2014;312(12):1218-1226.
134. Mayer-Davis EJ, Dabelea D, Lawrence JM. Incidence Trends of
Type 1 and Type 2 Diabetes among Youths, 2002-2012. N Engl J Med.
2017;377(3):301.
135. Centers for Disease Control and Prevention. National Diabetes
Statistics Report, 2017. Atlanta, GA: US Department of Health and
Human Services, CDC; 2017. In.
136. Burnett-Hartman AN, Newcomb PA, Potter JD. Infectious Agents
and Colorectal Cancer: A Review of Helicobacter pylori, Streptococcus
bovis, JC Virus, and Human Papillomavirus. 2008;17(11):2970-2979.
137. Butt J, Varga MG, Blot WJ, et al. Serologic Response to
Helicobacter pylori Proteins Associated With Risk of Colorectal
Cancer Among Diverse Populations in the United States.
Gastroenterology. 2019;156(1):175-186.e172.
138. Boyle T, Keegel T, Bull F, Heyworth J, Fritschi L. Physical activity
and risks of proximal and distal colon cancers: a systematic review
and meta-analysis. J Natl Cancer Inst. 2012;104(20):1548-1561.
139. Robsahm TE, Aagnes B, Hjartaker A, Langseth H, Bray FI, Larsen
IK. Body mass index, physical activity, and colorectal cancer by
anatomical subsites: a systematic review and meta-analysis of cohort
studies. Eur J Cancer Prev. 2013;22(6):492-505.
140. Hidayat K, Zhou H-J, Shi B-M. Influence of physical activity
at a young age and lifetime physical activity on the risks of 3
obesity-related cancers: systematic review and meta-analysis of
observational studies. Nutrition Reviews. 2019.
141. Schmid D, Leitzmann MF. Television viewing and time spent
sedentary in relation to cancer risk: a meta-analysis. J Natl Cancer
Inst. 2014;106(7).
38 Colorectal Cancer Facts & Figures 2020-2022
142. Chao A, Connell CJ, Jacobs EJ, et al. Amount, type, and timing of
recreational physical activity in relation to colon and rectal cancer in
older adults: the Cancer Prevention Study II Nutrition Cohort. Cancer
Epidemiol Biomarkers Prev. 2004;13(12):2187-2195.
143. Campbell PT, Patel AV, Newton CC, Jacobs EJ, Gapstur SM.
Associations of recreational physical activity and leisure time spent
sitting with colorectal cancer survival. J Clin Oncol. 2013;31(7):876-885.
144. Larsson SC, Wolk A. Obesity and colon and rectal cancer risk: a
meta-analysis of prospective studies. Am J Clin Nutr. 2007;86(3):556-565.
145. Ortega LS, Bradbury KE, Cross AJ, Morris JS, Gunter MJ,
Murphy N. A Prospective Investigation of Body Size, Body Fat
Composition and Colorectal Cancer Risk in the UK Biobank. Sci Rep.
2017;7(1):17807.
146. Xue K, Li FF, Chen YW, Zhou YH, He J. Body mass index and
the risk of cancer in women compared with men: a meta-analysis of
prospective cohort studies. European J Cancer Prev. 2017;26(1):94-105.
147. Murphy N, Jenab M, Gunter MJ. Adiposity and gastrointestinal
cancers: epidemiology, mechanisms and future directions. Nat Rev
Gastroenterol Hepatol. 2018;15(11):659-670.
148. Aleksandrova K, Schlesinger S, Fedirko V, et al. Metabolic
Mediators of the Association Between Adult Weight Gain
and Colorectal Cancer: Data From the European Prospective
Investigation into Cancer and Nutrition (EPIC) Cohort. Am J
Epidemiol. 2017;185(9):751-764.
149. Kim H, Giovannucci EL. Sex differences in the association
of obesity and colorectal cancer risk. Cancer Causes Control.
2017;28(1):1-4.
150. Liu P-H, Wu K, Ng K, et al. Association of Obesity With Risk
of Early-Onset Colorectal Cancer Among Women. JAMA Oncology.
2019;5(1):37-44.
151. Wang N, Khankari NK, Cai H, et al. Prediagnosis body mass
index and waist-hip circumference ratio in association with
colorectal cancer survival. Int J Cancer. 2016.
152. Liang X, Margolis KL, Hendryx M, et al. Metabolic Phenotype
and Risk of Colorectal Cancer in Normal-Weight Postmenopausal
Women. Cancer Epidemiol Biomarkers Prev. 2017;26(2):155-161.
153. Myte R, Gylling B, Haggstrom J, et al. Metabolic factors and the
risk of colorectal cancer by KRAS and BRAF mutation status. Int J
Cancer. 2019;145(2):327-337.
154. Cespedes Feliciano EM, Kroenke CH, Meyerhardt JA, et al.
Metabolic Dysfunction, Obesity, and Survival Among Patients With
Early-Stage Colorectal Cancer. J Clin Oncol. 2016.
155. O’Keefe SJ. Diet, microorganisms and their metabolites, and
colon cancer. Nat Rev Gastroenterol Hepatol. 2016;13(12):691-706.
156. Kwong TNY, Wang X, Nakatsu G, et al. Association Between
Bacteremia From Specific Microbes and Subsequent Diagnosis of
Colorectal Cancer. Gastroenterology. 2018;155(2):383-390.e388.
157. Wong SH, Yu J. Gut microbiota in colorectal cancer: mechanisms
of action and clinical applications. Nat Rev Gastroenterol Hepatol
2019;16(11):690-704.
158. Tilg H, Moschen AR. Food, immunity, and the microbiome.
Gastroenterology. 2015;148(6):1107-1119.
159. Brennan CA, Garrett WS. Gut Microbiota, Inflammation, and
Colorectal Cancer. Annu Rev Microbiol. 2016;70:395-411.
160. Dejea CM, Fathi P, Craig JM, et al. Patients with familial
adenomatous polyposis harbor colonic biofilms containing
tumorigenic bacteria. Science. 2018;359(6375):592-597.
161. O’Keefe SJ, Li JV, Lahti L, et al. Fat, fibre and cancer risk in
African Americans and rural Africans. Nat Commun. 2015;6:6342.
162. Scott KP, Gratz SW, Sheridan PO, Flint HJ, Duncan SH. The
influence of diet on the gut microbiota. Pharmacol Res. 2013;69(1):52-
60.
163. Tabung FK, Liu L, Wang W, et al. Association of Dietary
Inflammatory Potential With Colorectal Cancer Risk in Men and
Women. JAMA Oncol. 2018;4(3):366-373.
164. Song M, Garrett WS, Chan AT. Nutrients, foods, and colorectal
cancer prevention. Gastroenterology. 2015;148(6):1244-1260 e1216.
165. Aune D, Lau R, Chan DS, et al. Dairy products and colorectal
cancer risk: a systematic review and meta-analysis of cohort studies.
Ann Oncol. 2012;23(1):37-45.
166. Vieira AR, Abar L, Chan DSM, et al. Foods and beverages and
colorectal cancer risk: a systematic review and meta-analysis
of cohort studies, an update of the evidence of the WCRF-AICR
Continuous Update Project. Ann Oncol. 2017;28(8):1788-1802.
167. Baron JA, Barry EL, Mott LA, et al. A Trial of Calcium and
Vitamin D for the Prevention of Colorectal Adenomas. N Engl J Med.
2015;373(16):1519-1530.
168. Keum N, Liu L, Hamada T, et al. Calcium intake and colon cancer
risk subtypes by tumor molecular characteristics. Cancer Causes
Control. 2019;30(6):637-649.
169. Keum N, Lee DH, Greenwood DC, Zhang X, Giovannucci
EL. Calcium intake and colorectal adenoma risk: dose-response
meta-analysis of prospective observational studies. Int J Cancer.
2015;136(7):1680-1687.
170. Zhao J, Giri A, Zhu X, et al. Calcium: magnesium intake ratio and
colorectal carcinogenesis, results from the prostate, lung, colorectal,
and ovarian cancer screening trial. Br J Cancer. 2019;121(9):796-804.
171. Schwingshackl L, Schwedhelm C, Hoffmann G, et al. Food groups
and risk of colorectal cancer. Int J Cancer. 2018;142(9):1748-1758.
172. Wu H, Flint AJ, Qi Q, et al. Association Between Dietary Whole
Grain Intake and Risk of Mortality: Two Large Prospective Studies in
US Men and Women. JAMA Intern Med. 2015;175(3):373-384.
173. World Cancer Research Fund/American Institute for Cancer
Research. Continuous Update Project Expert Report 2018. Diet,
nutrition, physical activity and colorectal cancer. Available at
dietandcancerreport.org
.
174. Rock CL, Thomson CA, Gansler T, et al. American Cancer Society
Guidelines on nutrition and physical activity for cancer prevention.
CA Cancer J Clin. 2019.
175. Mason JB, Dickstein A, Jacques PF, et al. A temporal association
between folic acid fortification and an increase in colorectal
cancer rates may be illuminating important biological principles: a
hypothesis. Cancer Epidemiol Biomarkers Prev. 2007;16(7):1325-1329.
176. Vollset SE, Clarke R, Lewington S, et al. Effects of folic acid
supplementation on overall and site-specific cancer incidence during
the randomised trials: meta-analyses of data on 50,000 individuals.
Lancet. 2013;381(9871):1029-1036.
177. Stevens VL, McCullough ML, Sun J, et al. High levels of folate
from supplements and fortification are not associated with increased
risk of colorectal cancer. Gastroenterology. 2011; 141(1):98-105.
178. Aune D, Lau R, Chan DS, et al. Nonlinear reduction in risk for
colorectal cancer by fruit and vegetable intake based on metaanalysis
of prospective studies. Gastroenterology. 2011;141(1):106-118.
179. Lee JE, Chan AT. Fruit, vegetables, and folate: cultivating the
evidence for cancer prevention. Gastroenterology. 2011;141(1):16-20.
Colorectal Cancer Facts & Figures 2020-2022 39
180. Chan DS, Lau R, Aune D, et al. Red and processed meat and
colorectal cancer incidence: meta-analysis of prospective studies.
PloS one. 2011;6(6):e20456.
181. Bouvard V, Loomis D, Guyton KZ, et al. Carcinogenicity
of consumption of red and processed meat. Lancet Oncol.
2015;16(16):1599-1600.
182. Kim E, Coelho D, Blachier F. Review of the association
between meat consumption and risk of colorectal cancer. Nutr Res.
2013;33(12):983-994.
183. Zeng L, Ruan M, Liu J, et al. Trends in Processed Meat,
Unprocessed Red Meat, Poultry, and Fish Consumption in the United
States, 1999-2016. J Acad Nutr Diet. 2019;119(7):1085-1098 e1012.
184. Manson JE, Cook NR, Lee IM, et al. Vitamin D Supplements
and Prevention of Cancer and Cardiovascular Disease. N Engl J Med.
2019;380(1):33-44.
185. McCullough ML, Zoltick ES, Weinstein SJ, et al. Circulating
Vitamin D and Colorectal Cancer Risk: An International Pooling
Project of 17 Cohorts. J Natl Cancer Inst. 2019;111(2):158-169.
186. Pradhan AD, Manson JE. Update on the Vitamin D and OmegA-3
trial (VITAL). J Steroid Biochem Mol Biol. 2016;155(Pt B):252-256.
187. Luttmann-Gibson H, Mora S, Camargo CA, et al. Serum
25-hydroxyvitamin D in the VITamin D and OmegA-3 TriaL (VITAL):
Clinical and demographic characteristics associated with baseline
and change with randomized vitamin D treatment. Contemp Clin
Trials. 2019:105854.
188. Chabrol T, Wion D. Randomized clinical trials of oral vitamin
D supplementation in need of a paradigm change: The vitamin D
autacoid paradigm. Med Hypotheses. 2020;134:109417.
189. Secretan B, Straif K, Baan R, et al. A review of human
carcinogens – Part E: tobacco, areca nut, alcohol, coal smoke, and
salted fish. Lancet Oncol. 2009;10(11):1033-1034.
190. Carter BD, Abnet CC, Feskanich D, et al. Smoking and mortality –
beyond established causes. N Engl J Med. 2015;372:631-640.
191. Murphy N, Ward HA, Jenab M, et al. Heterogeneity of Colorectal
Cancer Risk Factors by Anatomical Subsite in 10 European
Countries: A Multinational Cohort Study. Clin Gastroenterol Hepatol.
2019;17(7):1323-1331 e1326.
192. Limsui D, Vierkant RA, Tillmans LS, et al. Cigarette smoking and
colorectal cancer risk by molecularly defined subtypes. J Natl Cancer
Inst. 2010;102(14):1012-1022.
193. Yang B, Jacobs EJ, Gapstur SM, Stevens V, Campbell PT.
Active smoking and mortality among colorectal cancer survivors:
the Cancer Prevention Study II nutrition cohort. J Clin Oncol.
2015;33(8):885-893.
194. Ordonez-Mena JM, Walter V, Schottker B, et al. Impact of
prediagnostic smoking and smoking cessation on colorectal cancer
prognosis: a meta-analysis of individual patient data from cohorts
within the CHANCES consortium. Ann Oncol. 2018;29(2):472-483.
195. McNabb S, Harrison TA, Albanes D, et al. Meta-analysis of 16
studies of the association of alcohol with colorectal cancer. Int J
Cancer. 2020;146(3):861-873.
196. Bagnardi V, Rota M, Botteri E, et al. Alcohol consumption
and site-specific cancer risk: a comprehensive dose-response
metaanalysis. Br J Cancer. 2015;112(3):580-593.
197. Rothwell PM, Wilson M, Elwin CE, et al. Long-term effect
of aspirin on colorectal cancer incidence and mortality: 20-year
follow-up of five randomised trials. Lancet. 2010;376(9754):1741-50.
198. Cook NR, Lee IM, Zhang SM, Moorthy MV, Buring JE. Alternate-
day, low-dose aspirin and cancer risk: long-term observational
follow-up of a randomized trial. Ann Intern Med. 2013;159(2):77-85.
199. Cao Y, Nishihara R, Wu K, et al. Population-wide Impact of
Long-term Use of Aspirin and the Risk for Cancer. JAMA Oncology.
2016;2(6):762-769.
200. Rothwell PM, Cook NR, Gaziano JM, et al. Effects of aspirin on
risks of vascular events and cancer according to bodyweight and
dose: analysis of individual patient data from randomised trials.
Lancet. 2018;392(10145):387-399.
201. Amitay EL, Carr PR, Jansen L, et al. Association of Aspirin and
Nonsteroidal Anti-Inflammatory Drugs With Colorectal Cancer Risk
by Molecular Subtypes. J Natl Cancer Inst. 2019;111(5):475-483.
202. Bains SJ, Mahic M, Myklebust TA, et al. Aspirin As Secondary
Prevention in Patients With Colorectal Cancer: An Unselected
Population-Based Study. J Clin Oncol. 2016;34(21):2501-2508.
203. Hamada T, Cao Y, Qian ZR, et al. Aspirin Use and Colorectal
Cancer Survival According to Tumor CD274 (Programmed Cell Death
1 Ligand 1) Expression Status. J Clin Oncol. 2017;35(16):1836-1844.
204. Hua X, Phipps AI, Burnett-Hartman AN, et al. Timing of Aspirin
and Other Nonsteroidal Anti-Inflammatory Drug Use Among
Patients With Colorectal Cancer in Relation to Tumor Markers and
Survival. J Clin Oncol. 2017;35(24):2806-2813.
205. Chubak J, Kamineni A, Buist DSM, Anderson ML, Whitlock EP.
In: Aspirin Use for the Prevention of Colorectal Cancer: An Updated
Systematic Evidence Review for the U.S. Preventive Services Task Force.
Rockville (MD)2015.
206. Rennert G. Reproductive factors, hormones and colorectal
cancer-still unresolved. Br J Cancer. 2017;116(1):1-3.
207. Murphy N, Strickler HD, Stanczyk FZ, et al. A Prospective
Evaluation of Endogenous Sex Hormone Levels and Colorectal Cancer
Risk in Postmenopausal Women. J Natl Cancer Inst. 2015;107(10).
208. Lin JH, Zhang SM, Rexrode KM, et al. Association between
sex hormones and colorectal cancer risk in men and women. Clin
Gastroenterol Hepatol. 2013;11(4):419-424 e411.
209. Lavasani S, Chlebowski RT, Prentice RL, et al. Estrogen and
colorectal cancer incidence and mortality. Cancer. 2015;121(18):3261-
3271.
210. Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal
hormone therapy and health outcomes during the intervention and
extended poststopping phases of the Women’s Health Initiative
randomized trials. JAMA. 2013;310(13):1353-1368.
211. Charlton BM, Wu K, Zhang X, et al. Oral contraceptive use
and colorectal cancer in the Nurses’ Health Study I and II. Cancer
Epidemiol Biomarkers Prev. 2015;24(8):1214-1221.
212. Michels KA, Pfeiffer RM, Brinton LA, Trabert B. Modification
of the Associations Between Duration of Oral Contraceptive Use
and Ovarian, Endometrial, Breast, and Colorectal Cancers. JAMA
Oncology. 2018;4(4):516-521.
213. Cao Y, Wu K, Mehta R, et al. Long-term use of antibiotics and risk
of colorectal adenoma. Gut. 2018;67(4):672-678.
214. Zhang J, Haines C, Watson AJM, et al. Oral antibiotic use and risk
of colorectal cancer in the United Kingdom, 1989-2012: a matched
case-control study. Gut. 2019;68(11):1971-1978.
215. Thosani N, Thosani SN, Kumar S, et al. Reduced risk of colorectal
cancer with use of oral bisphosphonates: a systematic review and
meta-analysis. J Clin Oncol. 2013;31(5):623-630.
40 Colorectal Cancer Facts & Figures 2020-2022
216. Vogtmann E, Corley DA, Almers LM, Cardwell CR, Murray LJ,
Abnet CC. Oral bisphosphonates and colorectal cancer. Sci Rep.
2017;7:44177.
217. Wolf AMD, Fontham ETH, Church TR, et al. Colorectal cancer
screening for average-risk adults: 2018 guideline update from the
American Cancer Society. CA Cancer J Clin. 2018;68(4):250-281.
218. Corley DA, Jensen CD, Quinn VP, et al. Association Between
Time to Colonoscopy After a Positive Fecal Test Result and Risk
of Colorectal Cancer and Cancer Stage at Diagnosis. JAMA.
2017;317(16):1631-1641.
219. Doubeni CA, Fedewa SA, Levin TR, et al. Modifiable Failures in
the Colorectal Cancer Screening Process and Their Association With
Risk of Death. Gastroenterology. 2019;156(1):63-74 e66.
220. Meester RGS, Peterse EFP, Knudsen AB, et al. Optimizing
colorectal cancer screening by race and sex: Microsimulation
analysis II to inform the American Cancer Society colorectal cancer
screening guideline. Cancer. 2018;124(14):2974-2985.
221. Jones WF, Ahnen DJ, Schroy III PC. Improving on-time colorectal
cancer screening through lead time messaging. Cancer. 2019.
222. Peterse EFP, Meester RGS, Siegel RL, et al. The impact of the
rising colorectal cancer incidence in young adults on the optimal
age to start screening: Microsimulation analysis I to inform the
American Cancer Society colorectal cancer screening guideline.
Cancer. 2018;124(14):2964-2973.
223. Gupta S, Halm EA, Rockey DC, et al. Comparative Effectiveness
of Fecal Immunochemical Test Outreach, Colonoscopy Outreach,
and Usual Care for Boosting Colorectal Cancer Screening Among
the Underserved: A Randomized Clinical Trial. JAMA Intern Med.
2013;173(18):1725-32.
224. U. S. Preventive Services Task Force, Bibbins-Domingo
K, Grossman DC, et al. Screening for Colorectal Cancer: US
Preventive Services Task Force Recommendation Statement. JAMA.
2016;315(23):2564-2575.
225. Bretthauer M, Kaminski MF, Loberg M, et al. Population-Based
Colonoscopy Screening for Colorectal Cancer: A Randomized Clinical
Trial. JAMA Intern Med. 2016;176(7):894-902.
226. Lieberman D. Colorectal Cancer Screening With Colonoscopy.
JAMA Intern Med. 2016;176(7):903-904.
227. Zauber AG, Winawer SJ, O’Brien MJ, et al. Colonoscopic
polypectomy and long-term prevention of colorectal-cancer deaths.
N Engl J Med. 2012;366(8):687-696.
228. Nishihara R, Wu K, Lochhead P, et al. Long-term colorectal
cancer incidence and mortality after lower endoscopy. N Engl J Med.
2013;369(12):1095-1105.
229. Doubeni CA, Corley DA, Quinn VP, et al. Effectiveness of
screening colonoscopy in reducing the risk of death from right and
left colon cancer: a large community-based study. Gut. 2018;67(2):
291-298.
230. Levin B, Lieberman DA, McFarland B, et al. Screening and
surveillance for the early detection of colorectal cancer and
adenomatous Polyps, 2008: a joint guideline from the American
Cancer Society, the US Multi-Society Task Force on Colorectal
Cancer, and the American College of Radiology. CA Cancer J Clin.
2008;58(3):130-160.
231. Peery AF, Cools KS, Strassle PD, et al. Increasing Rates of Surgery
for Patients With Nonmalignant Colorectal Polyps in the United
States. Gastroenterology. 2018;154(5):1352-1360 e1353.
232. Ko CW, Riffle S, Michaels L, et al. Serious complications within
30 days of screening and surveillance colonoscopy are uncommon.
Clin Gastroenterol Hepatol. 2010;8(2):166-173.
233. Quintero E, Castells A, Bujanda L, et al. Colonoscopy versus fecal
immunochemical testing in colorectal-cancer screening. N Engl J
Med. 2012;366(8):697-706.
234. Zhao S, Wang S, Pan P, et al. Magnitude, Risk Factors,
and Factors Associated With Adenoma Miss Rate of Tandem
Colonoscopy: A Systematic Review and Meta-analysis.
Gastroenterology. 2019;156(6):1661-1674 e1611.
235. Meester RG, Doubeni CA, Lansdorp-Vogelaar I, et al. Variation
in Adenoma Detection Rate and the Lifetime Benefits and Cost
of Colorectal Cancer Screening: A Microsimulation Model. JAMA.
2015;313(23):2349-2358.
236. Corley DA, Jensen CD, Marks AR, et al. Adenoma detection
rate and risk of colorectal cancer and death. N Engl J Med.
2014;370(14):1298-1306.
237. Atkin W, Wooldrage K, Parkin DM, et al. Long term effects
of once-only flexible sigmoidoscopy screening after 17 years of
follow-up: the UK Flexible Sigmoidoscopy Screening randomised
controlled trial. Lancet. 2017;389(10076):1299-1311.
238. Holme O, Schoen RE, Senore C, et al. Effectiveness of flexible
sigmoidoscopy screening in men and women and different age
groups: pooled analysis of randomised trials. BMJ. 2017;356:i6673.
239. Miller EA, Pinsky PF, Schoen RE, Prorok PC, Church TR. Effect of
flexible sigmoidoscopy screening on colorectal cancer incidence and
mortality: long-term follow-up of the randomised US PLCO cancer
screening trial. Lancet Gastroenterol Hepatol. 2019;4(2):101-110.
240. Patel JD, Chang KJ. The role of virtual colonoscopy in colorectal
screening. Clin Imaging. 2016;40(2):315-320.
241. de Haan MC, van Gelder RE, Graser A, Bipat S, Stoker J.
Diagnostic value of CT-colonography as compared to colonoscopy in
an asymptomatic screening population: a meta-analysis. Eur Radiol.
2011;21(8):1747-1763.
242. American College of Radiology. Patient and Provider Groups
Tell Congress to Pass Medicare Virtual Colonoscopy Coverage. 2018;
https://www.acr.org/Media-Center/ACR-News-Releases/2018/Patient-and-Provider-
Groups-Tell-Congress-to-Pass-Medicare-Virtual-Colonoscopy-Coverage
.
243. Knudsen AB, Zauber AG, Rutter CM, et al. Estimation of Benefits,
Burden, and Harms of Colorectal Cancer Screening Strategies:
Modeling Study for the US Preventive Services Task Force. JAMA.
2016;315(23):2595-2609.
244. Gellad ZF, Stechuchak KM, Fisher DA, et al. Longitudinal
adherence to fecal occult blood testing impacts colorectal cancer
screening quality. Am J Gastroenterol. 2011;106(6):1125-1134.
245. Liss DT, Petit-Homme A, Feinglass J, Buchanan DR, Baker
DW. Adherence to repeat fecal occult blood testing in an
urban community health center network. J Community Health.
2013;38(5):829-833.
246. Bharti B, May FFP, Nodora J, et al. Diagnostic colonoscopy
completion after abnormal fecal immunochemical testing and
quality of tests used at 8 Federally Qualified Health Centers in
Southern California: Opportunities for improving screening
outcomes. Cancer. 2019.
247. Chubak J, Garcia MP, Burnett-Hartman AN, et al. Time to
Colonoscopy after Positive Fecal Blood Test in Four U.S. Health Care
Systems. Cancer Epidemiol Biomarkers Prev. 2016;25(2):344-350.
Colorectal Cancer Facts & Figures 2020-2022 41
248. Shaukat A, Mongin SJ, Geisser MS, et al. Long-term mortality
after screening for colorectal cancer. N Engl J Med. 2013;369(12):1106-
1114.
249. Mandel JS, Church TR, Bond JH, et al. The effect of fecal
occultblood screening on the incidence of colorectal cancer. N Engl J
Med. 2000;343(22):1603-1607.
250. Hassan C, Giorgi Rossi P, Camilloni L, et al. Meta-analysis:
adherence to colorectal cancer screening and the detection rate for
advanced neoplasia, according to the type of screening test. Aliment
Pharmacol Ther. 2012;36(10):929-940.
251. Robertson DJ, Lee JK, Boland CR, et al. Recommendations on
Fecal Immunochemical Testing to Screen for Colorectal Neoplasia:
A Consensus Statement by the US Multi-Society Task Force on
Colorectal Cancer. Am J Gastroenterol. 2016.
252. Tinmouth J, Lansdorp-Vogelaar I, Allison JE. Faecal
immunochemical tests versus guaiac faecal occult blood tests: what
clinicians and colorectal cancer screening programme organisers
need to know. Gut. 2015;64(8):1327-1337.
253. Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. Multitarget
stool DNA testing for colorectal-cancer screening. N Engl J Med.
2014;370(14):1287-1297.
254. Weiser E, Parks PD, Swartz RK, van Thomme J, Limburg P, BM
B. Colorectal Cancer Screening: Compliance with Multi-target Stool
DNA Testing among Medicare Beneficiaries. Digestive Disease Week;
2019; San Diego, CA.
255. Chido-Amajuoyi OG, Sharma A, Talluri R, Tami-Maury I, Shete S.
Physician-office vs home uptake of colorectal cancer screening using
FOBT/FIT among screening-eligible US adults. Cancer Med. 2019.
256. Centers for Disease Control and Prevention (CDC). Behavioral
Risk Factor Surveillance System Survey Data. 2019;
cdc.gov/brfss/
.
Accessed 09/04/2019.
257. Fedewa SA, Sauer AG, Siegel RL, Jemal A. Prevalence of Major
Risk Factors and Use of Screening Tests for Cancer in the United
States. Cancer Epidemiol Biomarkers Prev. 2015;24(4):637-652.
258. Beydoun HA, Beydoun MA. Predictors of colorectal cancer
screening behaviors among average-risk older adults in the United
States. Cancer Causes Control. 2008;19(4):339-359.
259. Guessous I, Dash C, Lapin P, Doroshenk M, Smith RA, Klabunde
CN. Colorectal cancer screening barriers and facilitators in older
persons. Prev Med. 2010;50(1-2):3-10.
260. Holden DJ, Jonas DE, Porterfield DS, Reuland D, Harris R.
Systematic review: enhancing the use and quality of colorectal
cancer screening. Ann Intern Med. 2010;152(10):668-676.
261. Doubeni CA, Laiyemo AO, Young AC, et al. Primary care,
economic barriers to health care, and use of colorectal cancer
screening tests among Medicare enrollees over time. Ann Fam Med.
2010;8(4):299-307.
262. Denberg TD, Melhado TV, Coombes JM, et al. Predictors
of nonadherence to screening colonoscopy. J Gen Intern Med.
2005;20(11):989-995.
263. Laiyemo AO, Adebogun AO, Doubeni CA, et al. Influence of
provider discussion and specific recommendation on colorectal
cancer screening uptake among U.S. adults. Prev Med. 2014;67:1-5.
264. Jerant AF, Fenton JJ, Franks P. Determinants of racial/
ethnic colorectal cancer screening disparities. Arch Intern Med.
2008;168(12):1317-1324.
265. Dougherty MK, Brenner AT, Crockett SD, et al. Evaluation of
Interventions Intended to Increase Colorectal Cancer Screening
Rates in the United States: A Systematic Review and Meta-analysis.
JAMA Intern Med. 2018;178(12):1645-1658.
266. The Community Guide. Cancer Screening: Multicomponent
Interventions – Colorectal Cancer. 2016;
https://www.thecommunityguide.
org/findings/cancer-screening-multicomponent-interventions-colorectal-cancer
.
Accessed 10/20/2019.
267. DeBourcy AC, Lichtenberger S, Felton S, Butterfield KT, Ahnen
DJ, Denberg TD. Community-based preferences for stool cards
versus colonoscopy in colorectal cancer screening. J Gen Intern Med.
2008;23(2):169-174.
268. Sequist TD, Zaslavsky AM, Marshall R, Fletcher RH, Ayanian
JZ. Patient and physician reminders to promote colorectal cancer
screening: a randomized controlled trial. Arch Intern Med.
2009;169(4):364-371.
269. Selby K, Baumgartner C, Levin TR, et al. Interventions to
Improve Follow-up of Positive Results on Fecal Blood Tests: A
Systematic Review. Ann Intern Med. 2017;167(8):565-575.
270. National Colorectal Cancer Roundtable. Tools & Resources –
80% by 2018. 2019;
http://nccrt.org/tools/80-percent-by-2018/
. Accessed
October 5, 2019.
271. Sarfaty M. How to Increase Colorectal Cancer Screening Rates
in Practice: A Primary Care Clinician’s Evidence-Based Toolbox and
Guide 2008. Eds. Peterson, K and Wender, R. Atlanta: The American
Cancer Society, the National Colorectal Cancer Roundtable, and
Thomas Jefferson University 2006, Rev 2008.
272. DeGroff A, Sharma K, Satsangi A, et al. Increasing Colorectal
Cancer Screening in Health Care Systems Using Evidence-Based
Interventions. Prev Chronic Dis. 2018;15:E100.
273. Levin TR, Corley DA, Jensen CD, et al. Effects of Organized
Colorectal Cancer Screening on Cancer Incidence and Mortality
in a Large Community-Based Population. Gastroenterology.
2018;155(5):1383-1391 e1385.
274. Coronado GD, Petrik AF, Vollmer WM, et al. Effectiveness
of a Mailed Colorectal Cancer Screening Outreach Program in
Community Health Clinics: The STOP CRC Cluster Randomized
Clinical Trial. JAMA Intern Med. 2018;178(9):1174-1181.
275. Fedewa SA, Yabroff KR, Smith RA, Goding Sauer A, Han X,
Jemal A. Changes in Breast and Colorectal Cancer Screening After
Medicaid Expansion Under the Affordable Care Act. Am J Prev Med.
2019;57(1):3-12.
276. US Department of Health and Human Services. Preventive
Services Covered Under the Affordable Care Act. 2010;
http://www.hhs.
gov/healthcare/facts/factsheets/2010/07/preventive-services-list.html
. Accessed
September 9, 2014.
277. Doubeni CA, Corley DA, Zauber AG. Colorectal Cancer Health
Disparities and the Role of US Law and Health Policy. Gastroenterology.
2016;150(5):1052-1055.
278. Kennedy RH, Francis EA, Wharton R, et al. Multicenter
randomized controlled trial of conventional versus laparoscopic
surgery for colorectal cancer within an enhanced recovery
programme: EnROL. J Clin Oncol. 2014;32(17):1804-1811.
279. Grothey A, Sargent DJ. Adjuvant Therapy for Colon Cancer: Small
Steps Toward Precision Medicine. JAMA Oncol. 2016;2(9):1133-1134.
280. Kelly KJ, Alsayadnasser M, Vaida F, et al. Does Primary Tumor
Side Matter in Patients with Metastatic Colon Cancer Treated
with Cytoreductive Surgery and Hyperthermic Intraperitoneal
Chemotherapy? Ann Surg Oncol. 2019;26(5):1421-1427.

42 Colorectal Cancer Facts & Figures 2020-2022
281. Loree JM, Pereira AAL, Lam M, et al. Classifying Colorectal
Cancer by Tumor Location Rather than Sidedness Highlights a
Continuum in Mutation Profiles and Consensus Molecular Subtypes.
Clin Cancer Res. 2018;24(5):1062-1072.
282. Sargent D, Sobrero A, Grothey A, et al. Evidence for cure by
adjuvant therapy in colon cancer: observations based on individual
patient data from 20,898 patients on 18 randomized trials. J Clin
Oncol. 2009;27(6):872-877.
283. Shah MA, Renfro LA, Allegra CJ, et al. Impact of Patient Factors
on Recurrence Risk and Time Dependency of Oxaliplatin Benefit in
Patients With Colon Cancer: Analysis From Modern-Era Adjuvant
Studies in the Adjuvant Colon Cancer End Points (ACCENT)
Database. J Clin Oncol. 2016;34(8):843-853.
284. Booth CM, Nanji S, Wei X, et al. Adjuvant Chemotherapy for
Stage II Colon Cancer: Practice Patterns and Effectiveness in the
General Population. Clin Oncol (R Coll Radiol). 2016;29(1):e29-e38.
285. Pahlman LA, Hohenberger WM, Matzel K, Sugihara K, Quirke P,
Glimelius B. Should the Benefit of Adjuvant Chemotherapy in Colon
Cancer Be Re-Evaluated? J Clin Oncol. 2016;34(12):1297-1299.
286. Abraham A, Habermann EB, Rothenberger DA, et al. Adjuvant
chemotherapy for stage III colon cancer in the oldest old: results
beyond clinical guidelines. Cancer. 2013;119(2):395-403.
287. Sveen A, Kopetz S, Lothe RA. Biomarker-guided therapy for
colorectal cancer: strength in complexity. Nat Rev Clin Oncol. 2019.
288. Bosset JF, Calais G, Mineur L, et al. Fluorouracil-based adjuvant
chemotherapy after preoperative chemoradiotherapy in rectal
cancer: long-term results of the EORTC 22921 randomised study.
Lancet Oncol. 2014;15(2):184-190.
289. Maas M, Nelemans PJ, Valentini V, et al. Adjuvant chemotherapy
in rectal cancer: defining subgroups who may benefit after
neoadjuvant chemoradiation and resection: a pooled analysis of 3,313
patients. Int J Cancer. 2015;137(1):212-220.
290. Kulaylat AS, Hollenbeak CS, Stewart DB, Sr. Adjuvant
Chemotherapy Improves Overall Survival of Rectal Cancer Patients
Treated with Neoadjuvant Chemoradiotherapy Regardless of
Pathologic Nodal Status. Ann Surg Oncol. 2016;24(5):1281-1288.
291. El-Shami K, Oeffinger KC, Erb NL, et al. American Cancer Society
Colorectal Cancer Survivorship Care Guidelines. CA Cancer J Clin.
2015;65(6):428-455.
292. Keller D, Stein SL. Facilitating return of bowel function after
colorectal surgery: alvimopan and gum chewing. Clin Colon Rectal
Surg. 2013;26(3):186-190.
293. Maiorino MI, Chiodini P, Bellastella G, Giugliano D, Esposito K.
Sexual dysfunction in women with cancer: a systematic review with
meta-analysis of studies using the Female Sexual Function Index.
Endocrine. 2016;54(2):329-341.
294. Schneider EC, Malin JL, Kahn KL, Ko CY, Adams J, Epstein AM.
Surviving colorectal cancer : patient-reported symptoms 4 years
after diagnosis. Cancer. 2007;110(9):2075-2082.
295. Oktay K, Harvey BE, Partridge AH, et al. Fertility Preservation
in Patients With Cancer: ASCO Clinical Practice Guideline Update. J
Clin Oncol. 2018;36(19):1994-2001.
296. Zhu L, Pickle LW, Ghosh K, et al. Predicting US- and state-level
cancer counts for the current calendar year: Part II: evaluation
of spatiotemporal projection methods for incidence. Cancer.
2012;118(4):1100-1109.
297. Chen HS, Portier K, Ghosh K, et al. Predicting US- and state-level
cancer counts for the current calendar year: Part I: evaluation of
temporal projection methods for mortality. Cancer. 2012;118(4):
1091-1099.
Acknowledgments
Rick Alteri; Joseph Anderson; Cammie Barnes; Durado Brooks; Lynn Butterly; Michelle DelFavero;
Carol DeSantis; Ted Gansler; Eric Jacobs; Mamta Kalidas; Marji McCullough; Michael O’Brien;
Alpa Patel; Scott Simpson; Robert Smith; Lindsey Torre; Dana Wagner; and Ann Zauber.
Colorectal Cancer Facts & Figures is a triennial publication of the American Cancer Society, Atlanta, Georgia.
For more information, contact:
Rebecca Siegel, MPH
Kimberly Miller, MPH
Ahmedin Jemal, DVM, PhD

©2020, American Cancer Society, Inc.
No. 861720
The American Cancer Society’s mission
is to save lives, celebrate lives,
and lead the fight for a world without cancer.
