

Photo page ii: Cell-to-Cell Communication.
Credit: NCATS, NIH.
Photo page vi: Enzyme Repairing DNA.
Credit: Tom Ellenberger, Washington University School of Medicine in St. Louis, and
Dave Gohara, Saint Louis University School of Medicine.
Photo page 41: Neurons.
Credit: Leterrier, NeuroCyto Lab, INP, Marseille, France.

i
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Director’s Message
To the American People,
As our nation’s biomedical research agency, the National Institutes of Health (NIH)
has been the driving force behind many of the recent innovations in science and
technology that are improving the health of all humankind. The coming years
are certain to offer many exciting new opportunities for scientic exploration—
and to pose some serious new challenges for human health. To rise to those
opportunities and challenges, it is imperative that NIH, along with all sectors of
society, work together in unprecedented ways with unprecedented speed.
Indeed, science is moving faster than ever before. To fuel this engine of discovery, NIH must continue to
support the highest caliber research throughout the country and the world, while at the same time take
vigorous steps to uphold the ethical conduct of science. NIH will further enhance the science of tomorrow
by continuing its efforts to build a next generation of researchers that better reects the rich, creative
diversity of our great nation. The increasingly complex scientic questions that our society will face in the
future will require not only diversity of scientic disciplines, but also diversity of thought, experience, and
demographics.
As a publicly funded agency, NIH has a responsibility to be a good steward of the funds entrusted
to us by the U.S. taxpayers. NIH will do this by investing efciently and effectively in a wide range of
basic, translational, clinical, and applied research, while at the same time supporting the workforce and
infrastructure required for a sustainable research enterprise. As outlined in this Strategic Plan, this approach
will enable NIH to build a solid foundation of fundamental knowledge about living systems that will serve to
accelerate research aimed at addressing our most pressing health needs.
NIH’s mission is to turn discovery into health. We thank you for your strong and steadfast support of this
crucial mission, and we look forward to your continued support as we strive to use the power of science to
create a healthier and more productive life for all.
With sincere appreciation,
Francis S. Collins
Director, National Institutes of Health


iii
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Table of Contents
Director’s Message ............................................................................................. i
NIH-Wide Strategic Plan Framework
............................................................... vii
Overview of NIH
...................................................................................................1
Mission and Goals ........................................................................................................... 1
Organization .................................................................................................................... 1
Supporting Researchers and Universities Through the Extramural
Research Program ...................................................................................................... 1
Research in Action in the NIH Intramural Research Program .................................. 2
Pioneering Clinical Research at the NIH Clinical Center ........................................... 2
NIH’s Strategy ......................................................................................................3
Objective 1: Advancing Biomedical and Behavioral Sciences ............................................ 3
Driving Foundational Science ......................................................................................... 3
Building Data Resources to Enable Research Progress ........................................... 4
Inventing Tools and Technologies to Catalyze Discovery .......................................... 6
Understanding Biological, Behavioral, and Social Determinants of
Population Health ........................................................................................................ 7
Preventing Disease and Promoting Health ..................................................................... 8
Developing New and Improved Vaccines .................................................................. 8
Addressing Risk and Burden of Disease ................................................................... 9
Harnessing Technology to Inform Decision-Making ............................................... 10
Designing Research for Everyone ............................................................................ 11
Developing and Optimizing Treatments, Interventions, and Cures ............................. 11
Giving the Right Treatment to the Right Patient at the Right Time ........................ 12
Catalyzing Cell Engineering, Bioengineering, and Regenerative Medicine ........... 13
Meeting Emerging Public Health Needs .................................................................. 14
Partnering to Advance Treatments and Cures ........................................................ 15
Objective 2: Developing, Maintaining, and Renewing Scientific Research Capacity ....... 16
Enhancing the Biomedical and Behavioral Research Workforce ................................ 16
Supporting Research Resources and Infrastructure ................................................... 18

iv
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Objective 3: Exemplifying and Promoting the Highest Level of Scientific Integrity,
Public Accountability, and Social Responsibility in the Conduct of Science .................... 20
Fostering a Culture of Good Scientific Stewardship .................................................... 21
Setting Priorities ........................................................................................................ 21
Monitoring Expenditures and Scientific Progress ................................................... 21
Making Evidence-Informed Decisions ...................................................................... 22
Assessing Programs, Processes, Outcomes, and Impact ...................................... 22
Communicating Results ........................................................................................... 23
Leveraging Partnerships ............................................................................................... 24
Federal Partnerships ................................................................................................ 24
Public-Private Partnerships ..................................................................................... 25
International Partnerships ........................................................................................ 26
Public Engagement ................................................................................................... 26
Ensuring Accountability and Confidence in Biomedical and Behavioral Sciences .... 27
Enhancing Reproducibility Through Rigorous and Transparent Research ............ 27
Improving Stewardship of Clinical Trials .................................................................. 27
Assuring Ethical and Equitable Conduct of Research Through Inclusion ............. 27
Maintaining Transparency Through Data Access and Sharing .............................. 28
Fostering a Safe and Harassment-Free Work Environment ................................... 28
Managing Risks to the Research Enterprise ........................................................... 29
Reducing Administrative Costs and Work Throughout the Grants Process .......... 30
Optimizing Operations ................................................................................................... 30
Crosscutting Themes
.......................................................................................................... 32
Improving Minority Health and Reducing Health Disparities 32
Enhancing Women’s Health ..........................................................
.......................................
................................. 33
Addressing Public Health Challenges Across the Lifespan ......................................... 33
Promoting Collaborative Science ................................................................................. 34
Leveraging Data Science for Biomedical Discovery .................................................... 34
Bold Predictions ................................................................................................35
References
.........................................................................................................37

v
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Appendix I: NIH Statutory Authority .................................................................42
Appendix II: NIH Organizational Chart
..............................................................43
Appendix III: Strategic Planning Process
.........................................................44
Appendix IV: NIH Common Fund Strategic Plan Report
..................................46
Appendix V: Acronyms
......................................................................................61
Acknowledgments
.............................................................................................64


MISSION:
To seek fundamental knowledge about the nature and behavior of living systems and the application
of that knowledge to enhance health, lengthen life, and reduce illness and disability
NIH-Wide Strategic Plan Framework
OVERVIEW OF NIH
NIH’S STRATEGY
Public Health
Challenges Across
the Lifespan
Collaborative
Science
Minority Health
and Health
Disparities
Women’s Health Data Science
Research Areas Research Capacity Research Conduct
Foundational Science
Disease Prevention and
Health Promotion
Treatments, Interventions,
and Cures
Workforce
Infrastructure and Resources
Stewardship
Partnerships
Accountability and Confidence
Management and Operations
OBJECTIVES
ORGANIZATION: 27 Institutes and Centers and the Office of the Director
• Extramural program: supporting research across the U.S. and beyond
• Intramural program: supporting research on NIH campuses
CROSSCUTTING THEMES
vii
NIH-Wide Strategic Plan for Fiscal Years 2021–2025

Figure 1. NIH Main Campus
Credit: NIH.
The James H. Shannon Building
(Building One) at the NIH main
campus in Bethesda, MD.

1
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Overview of NIH
a
For the purposes of this Strategic Plan, the term biomedical is used broadly to include biological, behavioral, and social scientic
perspectives.
Mission and Goals
At the National Institutes of Health (NIH), “Turning
Discovery into Health” is what its tens of thousands
of employees—and the hundreds of thousands of
scientists it supports—strive to accomplish every
day. As the foremost agency for funding biomedical
research
a
in the U.S., NIH’s mission is to seek funda-
mental knowledge about the nature and behavior of
living systems and to use that knowledge to enhance
health, lengthen life, and reduce illness and disability
(Figure 1).
1
To achieve this mission, NIH works to
support innovative research ultimately aimed at
protecting and improving human health; train the
biomedical research workforce and develop scientic
infrastructure; contribute to the nation’s economic
growth by expanding the biomedical knowledge
base; and promote integrity, public accountability,
and societal responsibility in scientic research. As an
operating division of the U.S. Department of Health
and Human Services (HHS), NIH is responsible for
carrying out the Department’s goal of advancing
scientic knowledge and innovation. NIH catalyzes
life-saving research breakthroughs by providing criti-
cal funding to eligible research institutions throughout
the nation and the world, and through the research
conducted in NIH laboratories.
While NIH’s primary mission is the conduct of
research, the agency is also a trusted resource for
accurate and timely biomedical information. NIH’s
biomedical information platforms are among the most
visited websites in the federal government, giving
researchers, health care professionals, and the public
highquality information and data necessary to make
informed decisions.
Organization
NIH is made up of 27 Institutes and Centers (ICs),
and the NIH Ofce of the Director (OD).
2
Each IC has
its own mission and research priorities focused on
specic diseases, body systems, life stages, or elds
of science. The NIH OD sets policy and provides
guidance, in addition to serving as a resource for
planning, managing, and coordinating the programs
and activities of all of NIH.
NIH receives its annual funding, or appropriation,
from the U.S. Congress. More than 80 percent of this
funding is passed on to researchers and research
institutions around the country—the extramural
research community—through a rigorous, competitive
process, while about 11 percent of NIH’s budget sup-
ports intramural projects conducted by scientists in
its own laboratories, which are subject to an equally
rigorous review.
3
Supporting Researchers and Universities
Through the Extramural Research Program
Every year, NIH receives more than 54,000 research
project grant applications
4
and funds almost 50,000
new and continuing grants. These grants support
more than 300,000 researchers at all career stages,
including more than 43,000 principal investigators at
approximately 2,500 universities, medical schools,
and other research institutions in every state of
the U.S. and around the world. This enterprise is
managed by NIH staff who facilitate and administer
scientic programs, consult with scientic experts to
inform priority setting, and act as agency experts for
specic scientic areas.
NIH’s funding decisions are made through a highly
competitive, rigorous dual-level peer review process
that emphasizes fairness and accountability and
prioritizes support of the best scientic ideas.
5
NIH
relies on the expertise of more than 25,000 external
reviewers annually to assess the scientic merit of
incoming grant applications in the rst stage of peer
review, which is followed by a second-level review for
mission relevance by members of national advisory
councils for ICs and the OD.
6
Final funding decisions
are made by IC Directors, taking into consideration
their IC’s research program priorities in the context of
the existing funding portfolio.
A variety of funding mechanisms—including grants,
cooperative agreements, research contracts, prize
competitions, and other less frequently used

2
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
mechanisms—are used to support NIH’s broad scien-
tic portfolio,
7
allowing maximum exibility to fund the
rapidly advancing needs of the biomedical research
community. These mechanisms are used to support
a wide range of efforts—from individual research
projects, to international consortia and networks, to
training opportunities—each of which may be tailored
to meet specic goals. For example, to create innova-
tive technologies that advance its mission and move
them toward uptake in the market, NIH supports
the Small Business Innovation Research and Small
Business Technology Transfer programs.
Research in Action in the NIH Intramural
Research Program
The NIH Intramural Research Program conducts
NIH’s in-house research and is the largest institution
committed to biomedical and behavioral research,
research training, and career development in the
world.
8
The mission of the Intramural Research
Program is to conduct distinctive, high-impact
laboratory, clinical, and population-based research;
facilitate new approaches to improve health through
prevention, diagnosis, and treatment; respond to
public health emergencies; and train the next genera-
tion of biomedical researchers. The program supports
approximately 8,000 basic, translational, and clinical
researchers at NIH research facilities located across
the U.S., including the main NIH campus in Bethesda,
Maryland; Research Triangle Park in North Carolina;
Johns Hopkins Bayview Medical Center in Baltimore,
Maryland; Frederick National Laboratory for Cancer
Research in Frederick, Maryland; Rocky Mountain
Laboratories in Hamilton, Montana; the Perinatology
Research Branch in Detroit, Michigan; and the
Phoenix Epidemiology and Clinical Research Branch
in Phoenix, Arizona. Scientists in the Intramural
Research Program include an estimated 1,200
principal investigators, 1,800 staff clinicians and
staff scientists, and 5,000 trainees. Many important
medical breakthroughs take place in the intramural
research laboratories.
Pioneering Clinical Research at the NIH
Clinical Center
The NIH Intramural Research Program includes the
NIH Clinical Center,
9
the world’s largest hospital
devoted exclusively to clinical research. The NIH
Clinical Center is designed to rapidly transition
scientic observations and laboratory discoveries
into clinical studies and bedside cures by bringing
together talented investigators and specialized
infrastructure, including unique patient cohorts, state-
of-the-art equipment, and specialized services. Since
its opening in 1953, more than half a million patients
have been active partners with NIH in medical
discovery. This partnership has resulted in a long list
of medical milestones, including the development of
chemotherapy for cancer; the development of some
of the earliest articial heart valves; the demonstration
that lithium treats depression; and the rst treatment
of HIV/AIDS with azidothymidine.
10
About 1,600 clinical research studies are in progress
at the NIH Clinical Center. Approximately half are
studies of the natural history of disease, while most
of the other studies are clinical trials, often the
rst tests of new drugs and therapies in people.
Participants come from all 50 U.S. states and around
the world. With its unique ability to assemble cohorts
of participants with rare diseases, the NIH Clinical
Center plays an important role in fostering new
multidisciplinary collaborations that study and nd
treatments for rare diseases, often revealing insights
into common diseases, as well.

3
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
NIH’s Strategy
To carry out its mission and optimize return on public investment, NIH has designed a strategic Framework
that includes three key Objectives that align with the agency’s goals. These three Objectives outline NIH’s
priorities in (1) biomedical and behavioral research areas, (2) research capacity, and (3)research conduct.
Across all of these priorities, NIH emphasizes several Crosscutting Themes—approaches that are common
to all Objectives of the Strategic Plan—including improving minority health and reducing health disparities;
enhancing women’s health; addressing public health challenges across the lifespan; promoting collaborative
science; and leveraging data science for biomedical discovery. Examples of these important crosscutting
topics are located throughout the three Objectives.
The NIH portfolio is designed with the breadth and
exibility to address current public health needs,
emerging areas of scientic opportunity, and public
health emergencies, such as the coronavirus disease
2019 (COVID-19) pandemic (Figure 2). Over the next
5 years, NIH will drive cutting-edge biomedical and
behavioral sciences forward on three interrelated
fronts—foundational science, disease prevention and
health promotion, and treatments, interventions, and
cures.
Driving Foundational Science
NIH supports a broad range of foundational scientic
research to provide the building blocks for future
diagnostics, treatments, and cures across the entire
spectrum of health, diseases, and conditions, includ-
ing those that are emerging, rare, or have yet to be
discovered.
Foundational science includes basic biological,
behavioral, and social research that generates the
knowledge of how living systems work at the molecu-
lar, cellular, organismal, behavioral, and social levels.
11
Basic research can be experimental or observational
and may involve manipulating molecules in test
tubes and cells in culture dishes, studying animal
models of disease (Figure 3), or conducting studies
to understand human health and disease processes.
Basic research also includes epidemiological studies
Advancing Biomedical and Behavioral Sciences
1
OBJECTIVE
Credit: Rocky Mountain Laboratory, NIAID, NIH.
Figure 2. COVID-19 Research
Coronavirus disease 2019 (COVID-19) is an emergent
human disease caused by a naturally arising novel corona-
virus, the severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2). This scanning electron microscope image
shows SARS-CoV-2 (round gold objects) emerging from
the surface of cells cultured in the laboratory. NIH sup-
ports research to understand SARS-CoV-2 and mitigate
the threat of COVID-19 for the health of all people by
building on existing and accelerating the development of
new research initiatives focused on five research priorities
detailed in the NIH-Wide Strategic Plan for COVID-19
Research. NIH is improving basic understanding of
SARS-CoV-2 and COVID-19 and developing the necessary
tools and approaches to better diagnose, prevent, and
treat this devastating disease. Pandemics recur, and NIH
is also considering how to enhance preparedness for the
next one.

4
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
to examine disease burden, distribution, and potential
risk and protective factors in specic populations, as
well as natural history studies that follow individuals
over time to observe early stages and progression
of a disease. NIH-supported research serves as the
world’s leading source of foundational knowledge of
relevance to both the public and private sectors of
biomedicine.
12
Much of the research process is carefully planned
and conducted, but serendipitous discoveries can
also drive progress. Because science explores the
unknown, it is not always possible to predict where
research will lead. This concept is especially true for
basic research, which integrates biology, behavior,
environment, medicine, physics, chemistry, engineer-
ing, and data science to pioneer novel technologies
capable of exploring the individual components of
life. Investments in basic science result in unexpected
breakthroughs and new elds of inquiry that could not
have been envisioned when the original experiments
were designed. For example, scientists leveraged
the discovery of the CRISPR system, a component
of the bacterial immune system that responds to
viral infection, to develop a molecular tool for editing
genes with exquisite precision. This technology
has revolutionized the ability to study genes and
holds great promise for treating numerous genetic
disorders. By investing in foundational science, NIH is
laying the groundwork for important future advances
that will improve the nation’s health.
Building Data Resources to Enable
Research Progress
NIH supports the creation of foundational data
resources that enable basic research and improve
understanding of the biological and environmental
factors that contribute to human health and disease.
NIH achieves this effort by funding investigators who
are studying and cataloging molecules that are the
basic building blocks of life—such as DNA, RNA, and
proteins—as well as researchers who are establishing
and collecting data from large cohorts of research
participants. The resulting datasets have the potential
to catalyze whole elds of research, as well as lead
to the development of new diagnostic tools and
therapies.
The 21st century opened with a crowning achieve-
ment of basic science, sequencing the human
genome—the complete collection of genetic informa-
tion within an individual. This achievement became
the foundation for the branch of science that studies
genomes across individuals to nd patterns in health
and disease and to uncover mechanisms to under-
stand how genes interact with one another and with a
person’s environment. The immense amount of data
produced by genomic studies is helping researchers
understand how the complex interactions among
different regions of the genome inuence human
development, aging, and health. One major genomic
data resource is the ENCyclopedia of DNA Elements
(ENCODE), which is aimed at identifying the function
of all parts of the human and mouse genomes and
has already been cited by thousands of research
publications.
13
The Clinical Genome (ClinGen)
Resource catalogues the physical, clinical, and
genetic characteristics of individuals to better under-
stand how small changes, or variants, in a person’s
genome are related to their health.
14
NIH will continue
to support the expansion of these databases and
improvement of the tools researchers use to generate
and analyze genomic data through the development
of new DNA-sequencing technologies and computa-
tional methods. NIH will also support new efforts to
ensure the inclusion of genomes of individuals from
Figure 3. Animal Research Models
Both people and animals have unique and important
roles as research subjects. Many medical advances that
enhance the lives of both humans and animals originate
from animal studies. NIH supports research using a wide
variety of animal models, from the familiar fruit flies,
rodents, and nonhuman primates to more unexpected
animal models, such as fish, frogs, and yeast. The
types of animals used in research are chosen for their
similarity to humans in anatomy, physiology, or genetics.
For example, zebrafish (pictured) are frequently used in
research because of their small size, rapid breeding, and
transparent bodies. Approximately 70 percent of human
genes are also found in the zebrafish, and zebrafish and
humans share many critical developmental pathways. Not
only can we learn how to prevent, treat, and cure human
diseases by studying animals, but often the treatments
developed can also be used to improve the health of
animals. In addition, NIH is acting to reduce the number
of animals needed for research by using other approach-
es, such as tissue chips.
Credit: Grimes DT, Boswell CW, Morante NF, Henkelman RM. Used with
the permission of Rebecca D. Burdine, Ph.D.

5
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
groups that have been historically underrepresented
in genomics research.
15
Harnessing the power of DNA-sequencing tech-
nologies, NIH-funded scientists have also created
fundamental datasets important to microbiome
research, or the study of the microbes—including
bacteria, viruses, and fungi—that live on and in the
human body. The average healthy adult is host to
trillions of microbes that live in the gut, in the mouth,
or on the skin, for example. The composition of the
microbiome inuences human health and response to
treatment, contributes to early development, affects
the immune system, and plays a role in metabolism.
The NIH Common Fund’s
b
Human Microbiome
Project (HMP), conducted from 2007 to 2016, was
the rst large-scale effort to map and identify the
thousands of species of microbes in the human
microbiome (Figure 4).
16
HMP generated a compre-
hensive prole of the microbiome from multiple body
sites from more than 300 healthy people and created
computational tools and resources to enable more
research. HMP also collected microbiome and human
data from three longterm cohort studies centered on
pregnancy and preterm birth, inammatory bowel
disease, and type 2 diabetes.
Ongoing studies supported by NIH are investigating
how the microbiome of pregnant women may affect
the risk of preterm birth;
17
exploring the possibility of
using complementary foods—foods given in addition
to those regularly consumed in the diet—to boost the
gut microbiome and treat childhood malnutrition;
18
understanding how benecial microbes in the mouth
protect against periodontal disease or other oral
infections;
19
and uncovering how the microbiome
inuences cancer development and response to
therapy.
20
One particularly promising area of research
is exploring the role of the microbiome in the onset
of chronic conditions involving immune system
dysfunction, such as cardiovascular disease and
inammatory diseases of the gut.
21
Studies that generate large datasets from diverse
participants provide vital fundamental research
resources. The Adolescent Brain Cognitive
Development (ABCD)
22
study is the largest long-term
study of brain development and child health in the
U.S. This study has recruited more than 11,000
children 9 to 10 years of age, who will be followed
into adulthood to explore how childhood experiences
b
For more information on the NIH Common Fund, see Appendix IV.
affect brain development and a variety of health-
related outcomes. Data collection is ongoing, and
researchers from within and outside the ABCD study
are using the data generated to conduct research on
such topics as the link between screen time and brain
structure,
23
effects of prenatal exposure to cannabis
use,
24
and the relationship between sleep and brain
structure and function.
25
Many NIH-funded projects span multiple areas of
research and include both basic and applied science.
The ambitious Brain Research through Advancing
Innovative Neurotechnologies
®
(BRAIN) Initiative aims
to answer fundamental questions about how brain
circuits work; how they become impaired in neuro-
logical, psychiatric, and substance use disorders;
and how to improve the function of these circuits to
treat brain disorders (Figure 5).
26
Components of the
BRAIN Initiative
®
include studies to record, image,
and manipulate brain circuits with the aim of develop-
ing treatments for brain disorders; development
and dissemination of informatics tools to allow
Figure 4. Human Microbiome Project
The Human Microbiome Project, which was launched by
NIH in 2007, provided the first glimpse of the microbial
diversity of healthy humans and is exploring the possible
relationships between particular human diseases and the
microbiome.
Credits: Composite image, Jonathan Bailey, NHGRI, NIH. Individual
images (Clockwise from top left), Streptococcus, Tom Schmidt; microbial
biofilm of mixed species, from human body, A. Earl, Broad Institute/
Massachusetts Institute of Technology; Bacillus, Tom Schmidt; Malassezia
lopophilis, J.H. Carr, CDC.

6
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
widespread sharing and interpretation of research
data; and efforts to discover and catalogue the
multitude of types of brain cells.
The complexity of the nearly 170 billion cells in a
human brain presents a formidable challenge to
understanding how different cell types work in brain
circuits, their role in disease, and how they might
be targeted directly by new therapies.Advances in
engineering and highthroughput methods to classify
individual cell types have enabled new opportunities
to tackle this challenge. The BRAIN Initiative
®
Cell
Census Network is developing a comprehensive
mouse brain cell atlas and applying cell type identi-
cation methods to studies of human brain tissue.
27
Scientists have begun to use these methods to deter-
mine precisely which human brain cells are affected in
a range of conditions, including Alzheimer’s disease
and related dementias, autism spectrum disorder, and
Zika virus infection.
Inventing Tools and Technologies to
Catalyze Discovery
Fundamental research includes the creation of
advanced biomedical research tools and technologies
for scientists to answer questions about biology and
human health. For example, imaging technology
has transformed science, allowing researchers to
“see” individual molecules interacting, measure brain
function, study internal tissues, visualize cell function-
ing in 3-D in real time, and locate specic molecules
in the body using chemical tags.
Certain NIH programs are initiated specically to spur
the development of new tools and technologies for
research use. The NIH Common Fund’s Single Cell
Analysis Program (SCAP) focused on developing
tools to explore the behavior of single cells, including
new ways to track cells in living multicellular organ-
isms, new imaging techniques and technologies, and
sequencing of the genome and transcriptome—the
collection of all gene readouts present in a cell.
28
Resources developed through SCAP have paved the
way for research that may lead to breakthroughs in
understanding the human body at the level of individ-
ual cells, rather than groups or populations of cells.
Such resources include the NIH Common Fund’s
Human BioMolecular Atlas Program (HuBMAP), a col-
laborative effort to develop a global open platform to
map the approximately 37 trillion cells in the human
body to understand how the relationships between
cells can affect a person’s health.
29
New technologies are yielding data in quantities
and at a level of complexity that requires increased
capacity for storage, management, and analysis.
Articial Intelligence (AI) is being used on big datasets
to augment human ability to detect patterns and
predict outcomes, thus offering signicant promise to
advance research. NIH will build a large and diverse
set of programs to foster machine learning (a subset
of AI), support the generation and management of
large-scale datasets, convene multidisciplinary teams
of researchers, and develop a set of ethical principles
for NIH-funded researchers to follow when using AI
(Figure 6).
30
Advances in data science facilitate data
processing and sharing, but concomitantly raise
concerns regarding privacy, security, ethics, and
bias. NIH is proactively engaging data and computer
scientists, engineers, clinicians, research participants,
ethicists, and the public in its plans to address future
challenges and opportunities.
Studies are beginning to demonstrate the potential AI
has for revolutionizing medical practice. For example,
NIH researchers developed a novel data-driven
approach for automated diagnosis and prognosis of
Age-related Macular Degeneration (AMD), highlighting
the potential of these systems to assist early disease
detection and enhance clinical decision-making
Figure 5. BRAIN
®
Initiative
First-place photo winner from the Brain Research through
Advancing Innovative Neurotechnologies
®
(BRAIN)
Initiative’s 2019 “Show Us Your Brains” photo and video
contest for BRAIN investigators. “Light Me Up!” is a light-
based rendering of deep brain stimulation’s electrical
excitation of neuronal fiber pathways to treat patients
who have traumatic brain injury.
Credit: Andrew Janson, Graduate Student Research Assistant, Scientific
Computing and Imaging Institute, The University of Utah.

7
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
processes.
31,32
The U.S. Food and Drug Administration
(FDA) also approved the rst automated medical
device to use AI to detect diabetic retinopathy.
33
NIH
will continue to explore and expand further uses of AI.
Understanding Biological, Behavioral, and
Social Determinants of Population Health
Building the foundation for science includes con-
structing an overall picture of how physiological,
behavioral, and social factors alone and in combi-
nation may determine human health. Conditions in
which an individual is born, lives, learns, works, and
ages combined with the behaviors that they engage
in can affect a wide range of health outcomes.
34
Understanding how these factors interact with an
individual’s biological make-up is a vital area of
research. The epigenome consists of chemical com-
pounds and proteins that can attach to DNA and turn
genes on and off. These changes in gene expression
can occur in response to social experiences (both
positive and negative) and environmental exposures
and may be passed from one generation to the
next. NIH supports research on social epigenomics,
the study of how social experiences throughout a
person’s lifetime can affect biology and health status
through changes to the epigenome. Similarly, NIH
supports research on environmental epigenomics,
which looks at how an individual’s exposure to
factors in the physical environment—such as air,
water, and soil—may also impact gene expression.
Studies designed to elucidate how social experiences
and environmental exposures—such as those experi-
enced through structural racism and lower economic
status—affect the individual epigenome among racial
and ethnic groups can provide a unique opportunity
to identify the changes that occur within and between
populations. This knowledge can be used to increase
understanding of minority health and decrease health
disparities.
Social and behavioral research is crucial to under-
standing the health and developmental effects of
using digital technology and electronic media that
have become integral parts of daily life. Findings from
the ABCD study and the NIH Intramural Research
Program have demonstrated that a signicant pro-
portion of children across a wide age range exceed
the daily limits on screen time recommended by the
American Academy of Pediatrics.
35,36
In light of the
COVID-19 pandemic, screen time has dramatically
increased for children of all ages, the effects of which
will need to be investigated. To assess how technol-
ogy and media use affect early childhood health and
development—as well as the nature of social inter-
actions among families, peers, and society—NIH will
support an initiative to study the impact of technology
and media exposure on early childhood development
and health outcomes. This effort will support coor-
dinated research projects using existing and newly
collected data, as well as determining measures for
exposure, usage, development, and health outcomes,
including neuroimaging, language development,
physical activity, and hormone levels.
Integrating different types of research to address
health needs for specic populations can improve
the health of these populations and also provide
insights into common conditions. For example, Down
syndrome is the most common genetic disease of
mild to moderate intellectual disability, occurring in
1out of every 700 babies born in the U.S. In 2018,
NIH launched the INvestigation of Co-occurring
conditions across the Lifespan to Understand Down
syndromE (INCLUDE) project, which studies con-
ditions that affect the general population and often
co-occur (i.e., are comorbid) with Down syndrome,
such as Alzheimer’s disease and related dementias,
autism, cataracts, celiac disease, cardiovascular
disease, and diabetes (Figure 7). The program
focuses on targeted, high-risk/high-reward basic
science studies on the causes of Down syndrome
comorbidities, cohort studies of individuals with
Down syndrome, and inclusion of individuals with
Down syndrome in new and existing clinical trials.
Understanding the fundamental processes underlying
human health is a key step in determining how to
promote and restore health and identify, prevent,
Figure 6. ELSI Research at NIH
The term ELSI refers to the consideration of Ethical,
Legal, and Social Implications of research, particularly
in emerging biomedical fields; ELSI has its roots in the
genomics community, but has expanded to include
other areas of NIH research. ELSI complements scien-
tific research by identifying, analyzing, and addressing
the ethical, legal, and social implications of research
as it is being conducted. NIH supports ELSI research
to facilitate the responsible integration of science into
society. Today ELSI initiatives are underway across NIH
in several areas of biomedical and behavioral research,
such as neuroscience, epidemiology, environmental
health, new and emerging technology development
and use, precision and personalized medicine, clin-
ical research and care, and special and vulnerable
population research. Key to NIH’s approach to ELSI is
collaboration with its multiple stakeholders.

8
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
and treat disease. Over
the next 5 years, NIH
will continue to invest in
fundamental research
projects that provide
new insights into basic
biological, behavioral,
and social processes
across the spectrum—
from molecules to cells to
humans to communities.
These investments will
undoubtedly lay the
groundwork for unimag-
inable breakthroughs
that will lead NIH one
step closer to improving
human health.
Preventing
Disease and
Promoting
Health
Disease prevention and health promotion are core
components of NIH’s research mission to improve
the health of all Americans. NIH research strengthens
the evidence base on which national public health
objectives and related disease prevention and health
promotion strategies are built. Prevention research
targets biological, social, and environmental factors,
individual behaviors, and health services and informs
health-related guidelines, policies, and regulations.
NIH supports a broad portfolio of research that
examines the best way to bring effective disease
prevention and health promotion strategies into
communities.
Developing New and Improved Vaccines
Vaccines provide a safe, cost-effective, and efcient
means of preventing illness, disability, and death from
infectious diseases. NIH supports a comprehensive
spectrum of immunology and infectious disease
research focused on developing improved or novel
vaccines. This includes study of pathogen–host
interactions and technological advancements in
vaccine development that have led to innovative and
exciting vaccine research strategies. For example,
NIH-supported researchers are working to identify
new platforms to deliver vaccine components and
explore how adjuvants (i.e., vaccine components that
enhance the immune
response) affect the
potency, durability, and
other aspects of vac-
cine-induced
immunity.
37
An importantremaining
need is the rapid
development of new
vaccines to mitigate
emerging infectious
disease outbreaks, such
as COVID-19, Ebola
virus disease (EVD), and
inuenza (u). NIH, in
collaboration with its
industry partner, devel-
oped an experimental
vaccine for COVID-19
in just weeks using
the genetic sequence
of SARS-CoV-2 (i.e.,
the virus that causes
COVID-19).
38
As of late 2020, the vaccine co-devel-
oped by scientists at NIH and Moderna was granted
an Emergency Use Authorization by the FDA, after
rigorously testing its safety and ability to protect
against infection. Other vaccines are still being
tested.
39
Recent outbreaks of the Ebola virus spurred
the development of multiple vaccine candidates
for EVD, including the rVSV-ZEBOV vaccine, which
through signicant federal government support was
brought to market by the private sector, licensed
in 2019, and is now widely available.
40
Preliminary
data from an outbreak in the Democratic Republic
of the Congo (DRC) has shown that this vaccine is
highly effective in preventing disease and death.
41
In
the U.S., seasonal inuenza causes 12,000–61,000
deaths annually,
42
and emerging inuenza strains
pose a pandemic risk. A key focus of the NIH
inuenza research program is developing a universal
vaccine
43
that provides robust, long-lasting protection
against multiple subtypes of inuenza (Figure 8),
eliminating the need for a seasonal u vaccine each
year and providing protection against newly emerging
strains with pandemic potential. Several u vaccine
clinical trials are being conducted, including an NIH-
sponsored trial of a universal vaccine candidate that
uses a nanoparticle technology to display portions of
the inuenza virus that are the same or very similar
among different inuenza strains.
44
Figure 7. INCLUDE Project
The INCLUDE (INvestigation of Co-occurring conditions
across the Lifespan to Understand Down syndromE)
project is an NIH-wide research initiative involving 18
Institutes and Centers that aims to understand critical
health and quality-of-life needs for individuals with
Down syndrome. Down syndrome is the most common
genetic cause of mild to moderate intellectual disability
and occurs in one out of every 700 babies born in
the U.S.
Credit: The INCLUDE Project, NIH.

9
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
In addition to furthering the development of vaccines
against specic pathogens, NIH supports the devel-
opment of technologies that enable scientists to
apply a standardized manufacturing process to devel-
op candidate vaccines against various pathogens and
create a collective database with information on their
safety. This streamlined approach can shorten the
preclinical development period from years to months
and is important for rapid response to emerging
infectious disease threats.
Addressing Risk and Burden of Disease
NIH is committed to supporting research to reduce
the impact of disease by identifying and improving
understanding of risk factors (e.g., inadequate
nutrition, low physical activity, built environment,
tobacco use, alcohol or drug misuse) and protective
factors (e.g., weight management, regular exercise,
daily tooth brushing and ossing) alone and in
combination with genetic factors. An important goal
of prevention is to alter the balance between risk and
protective factors so that protective factors outweigh
risk factors. Screening, health promotion, counsel-
ing, behavioral change, stress management, and
preventive medications are all potential strategies for
reducing individual risk. NIH investments have helped
lead to advances in screening for cardiovascular
disease, lung cancer, abnormal blood glucose, type 2
diabetes, oral cancer, and intimate partner violence,
as well as interventions to address obesity and
tobacco use in children and adolescents.
One example of NIH’s investments in risk identi-
cation is in suicide prevention (Figure 9). Suicide
remains one of the top 10 leading causes of death
in the U.S., claiming the lives of more than 48,000
people each year.
45
Although it impacts all ages
and in all parts of the country, some specic groups
are disproportionately affected, such as sexual
and gender minority (SGM) populations (especially
transgender and gender non-conforming youth)
and American Indian or Alaska Native populations
(who have the highest suicide rates of any racial or
ethnic group in the U.S.
46
). NIH-supported suicide
prevention research illustrates how improvements in
care can save lives. Universal screening for suicide
risk in emergency departments has been shown
to be effective and feasible.
47
Building on these
ndings, NIH-supported researchers are testing brief
interventions and follow-up care to prevent recurring
self-harm and related comorbidities, such as sub-
stance use disorder.
NIH-supported studies have demonstrated how long-
term, multigenerational studies of chronic diseases
can give rise to innovative prevention and intervention
strategies. For example, the Framingham Heart
Study,
48
launched in 1948, continues to inform tobac-
co cessation, nutrition, physical activity, and blood
pressure control strategies that are used all over the
world to reduce the risk of chronic disease. High
blood pressure, or hypertension, is common over
the age of 50 years and is a leading risk factor for
cardiovascular diseases like heart disease and stroke.
It may also increase the risk of dementia later in life.
Data from several NIH-funded observational studies
suggested that cardiovascular disease risk increases
when systolic blood pressure rises beyond a certain
level. NIH’s Systolic Blood Pressure Intervention Trial
(SPRINT)
49
assessed whether aggressively lowering
blood pressure can prevent these conditions. SPRINT
found that maintaining systolic blood pressure at less
than 120 mm Hg reduced the combined risk of heart
attack, heart failure, and stroke by 25 percent and
reduced the risk of death by 27 percent compared
to the standard blood pressure target at the time
(140 mm Hg).
50
These ndings helped change the
national guidelines for treating hypertension, which
now use 120 mm Hg as the standard blood pressure
target.
51
If successfully adopted into clinical practice
across the U.S., these guidelines are expected to
prevent about 107,500 deaths per year among people
at high risk for fatal cardiovascular disease.
52
Figure 8. Universal Flu Vaccine
A healthy volunteer receives an experimental universal
influenza vaccine known as H1ssF_3928 as part of
a Phase 1 clinical trial at the NIH Clinical Center in
Bethesda, Maryland. Scientists at the Vaccine Research
Center developed the vaccine.
Credit: NIAID, NIH.

10
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Harnessing Technology to Inform
Decision-Making
NIH supports the development of new or improved
interventions and technologies along with repur-
posing existing technologies to monitor and reduce
disease risk, enhance protective factors, and restore
health (Figure 10). Coupled with advances in data
science that enhance analytical capacity and speed,
these technologies and tools will help aid decision-
making by patients and providers and improve
disease prevention and health promotion strategies
at the individual, family, community, and population
health levels.
Most information used to make decisions in current
medical practice is collected at a specic moment
in time and in a clinical setting, such as taking blood
pressure, providing a limited view of an individual’s
health and disease risk. Heart rate and motion
sensors in smart watches and other wearable devices
are examples of consumer technologies that can
provide continuous feedback to help people improve
their health. These devices detect underlying signs
of illness and response to interventions, including
medications and lifestyle changes, faster than con-
ventional methods that often require weeks or months
to provide actionable feedback. NIH-supported
researchers have developed a wearable sensor made
of stretchable microelectronics that uses ultrasound
to measure blood pressure continuously, whether the
wearer is resting or active. Such devices may help
identify people at risk of stroke and heart disease by
Figure 9. Suicide Prevention
“Five action steps for helping someone in emotional pain”: Infographic.
Credit: NIMH, NIH.
Figure 10. Nanorobots for Dental Health
NIH supported a collaboration among biomedical
researchers and engineers to build microscopic
nanorobots to target, destroy, and remove dental
plaque, a harmful community of bacteria that grow on
teeth. The nanorobots, which contain an antibacterial
compound, are controlled using tiny magnets to
perform micro-scale precision cleaning, including
hard-to-reach spaces. This technology could be used
to prevent dental caries and periodontal disease, in
addition to cleaning other surfaces susceptible to
biofilms, such as metal implants and catheters or
hospital equipment.
Credit: Geelsu Hwang and Edward Steager, University of Pennsylvania.

11
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
providing patients and physicians with more frequent
and accessible information on blood pressure, includ-
ing uctuations that occur during the wide variety of
activities that people engage in every day.
53
Designing Research for Everyone
NIH prioritizes research that addresses the needs of
underserved populations to address the factors that
contribute to health disparities. NIH-wide efforts will
continue to focus on developing and testing interven-
tions to reduce health disparities, identifying key gaps
in prevention science related to health disparities,
and promoting targeted research on appropriately
tailored public health, clinical, and community pre-
ventive services in diverse settings and contexts. For
example, the NIH All of Us Research Program
54
has
been designed to reect the diversity of the U.S., with
a special focus on including participants from groups
that have been underrepresented in health research
(Figure 11).
The Collaborative Minority Health and Health
Disparities Research with Tribal Epidemiology
Centers initiative supports research on topics related
to minority health and health disparities in American
Indian or Alaska Native populations, with emphasis
on areas where there are signicant gaps in data and
knowledge. Current research projects include exam-
ining the impact of the Navajo Nation Tax on Junk
Food on health outcomes, identifying the incidence
and prevalence of arthritis and autoimmune disease
among Alaska Natives, and understanding determi-
nants of motor vehicle injuries and deaths among the
Northwest Tribes.
55
Sex and gender also inuence health and disease.
Sex refers to biological differences between females
and males, including chromosomes, sex organs,
and endogenous hormonal proles. Gender refers to
socially constructed and enacted roles and behaviors,
which occur in a historical and cultural context and
vary across societies and over time.
56
Considering
the effects of sex and gender in study design, data
collection and analysis, and dissemination of ndings
will help to inform the development of prevention
strategies and interventions for everyone.
Developing and Optimizing
Treatments, Interventions,
and Cures
Building on the solid foundation of fundamental dis-
coveries in biology, health and disease, and behavior,
as well as innovations in data science and emerging
technologies, NIH-supported scientists continue to
develop new and improved treatments and cures,
including for diseases that were considered intracta-
ble even a decade ago.
The path to a new treatment often begins not in the
clinic or community but in the laboratory, where basic
researchers rene our understanding of disease and
identify aspects of disease causation or progression
Figure 11. All of Us Research Program
The NIH All of Us Research Program is a historic effort
to collect and study data from 1 million or more people
living in the U.S. The program’s goal is better health
for all of us, and its aim is to gather data on genetics,
lifestyle, and environmental exposures. The All of Us
Research Program is unique because it is disease
agnostic, meaning that it will not focus on one disease,
risk factor, or group of people, instead enabling
researchers to evaluate multiple risk factors that are
associated with outcomes across different diseases.
This unprecedented scientific resource will enable
research on numerous diseases and conditions across
populations and the lifespan, with a special focus on
outreach to groups that have been underrepresented
in health research, to reflect the diversity of the U.S.
The All of Us Research Program has already begun to
make an early, non-finalized version of its Researcher
Workbench available, an important milestone toward
creating a publicly accessible platform to increase
research on understudied areas, including wellness and
resilience.
Credit: NIH.

12
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
that could be targeted therapeutically. Investigators
use this information to design candidate treatment
approaches using cell or tissue samples, animal
models, or computer simulations. If the candidate
approaches appear to be safe and effective in this
preclinical setting, they are moved into human trials,
where they are tested for safety and efcacy. Finally,
new and improved methods to promote the adoption
of effective and proven interventions are identied
and rened through implementation research. This
process is rarely straightforward. In fact, sometimes
the process even circles back on itself in a “virtuous
cycle,” with applied research informing new ideas in
basic research.
To illustrate, NIH-supported basic science was a
springboard for the development of a ground-breaking
new cystic brosis treatment. Cystic brosis is an
inherited disorder that causes mucus to accumulate
in the airways and digestive tract. The identication
of the CFTR gene, which is mutated in affected
individuals, along with additional discoveries over
several decades, has enabled a variety of progressively
more effective drug therapies for the disease. Recent
NIH-supported clinical trials demonstrated that a
novel triple-drug therapy could compensate for the
effects of a CFTR mutation that occurs in 90 percent
of affected individuals.
57
Now, instead of being a fatal
disease, there is promise that cystic brosis in many
individuals could soon be a chronic condition that can
be managed over a long lifetime.
NIH supports randomized controlled clinical
trials—studies conducted under “ideal” research
conditions in which participants are randomly placed
into one of two or more groups that receive different
interventions or a placebo (i.e., a treatment with
no therapeutic effect). Outcomes from each group
are then analyzed and compared. Such studies
are considered the gold standard by which clinical
researchers determine the safety and effectiveness
of interventions. NIH also supports pragmatic trials,
which are designed to evaluate interventions in
real-world settings and situations. To support and
facilitate pragmatic trials, NIH established a Health
Care Systems Research Collaboratory
58
under the
NIH Common Fund to engage with health care
delivery organizations as key research partners. The
Collaboratory disseminates best research practices,
provides education and coordination, and supports
pilot projects involving a variety of diseases and
conditions in community settings.
Giving the Right Treatment to the Right
Patient at the Right Time
Advances in molecular medicine have allowed health
professionals to move toward a precision medicine
approach for targeted treatment and prevention that
considers an individual’s genes, environment, and
lifestyle. In contrast to a one-size-ts-all approach,
in which disease treatment and prevention strategies
are developed for the average person, precision
medicine will allow doctors and researchers to predict
more accurately which treatment and prevention
strategies will work best in an individual. Unlike
research studies that focus on one disease, risk
factor, or group of people, the All of Us Research
Program is building an unprecedented scientic
resource that will enable research on numerous
diseases and conditions across populations and the
lifespan.
Patients with certain types of cancer are already
beneting from precision medicine approaches. For
example, an NIH-supported clinical trial showed that
a molecular test for the expression of 21 genes asso-
ciated with breast cancer recurrence could determine
whether patients with the most common type of
breast cancer would benet from chemotherapy in
addition to surgery.
59,60
The researchers found that
most of these women can safely avoid chemotherapy
and its toxic side effects.
The promise of precision medicine is exemplied by
the development, built on decades of research, of
new therapies that harness patients’ own immune
systems to attack their cancer. Among them are
chimeric antigen receptor (CAR) T-cell therapies
that are made by genetically engineering a patient’s
own immune cells so they will bind to specic
proteins on cancer cells and kill them. Approved
by the FDA in 2017, these biologic products have
resulted in remarkable benets to children and adults
with certain types of leukemia and lymphoma.
61
Unfortunately, some patients initially respond to these
treatments but then relapse, some patients’ cancers
do not respond at all, and the treatments can cause
serious side effects. Scientists are working to under-
stand the mechanisms underlying these challenges
and to develop additional approaches for patients.
Hundreds of clinical trials for new CAR T-cell thera-
pies are ongoing, signaling the continued promise of
this innovative new treatment for patients with cancer
and HIV/AIDS.

13
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Another area of NIH-supported research on per-
sonalized approaches to medical treatment has
been to develop articial pancreas technologies to
automatically link individualized glucose monitoring
and insulin delivery to improve the health and quality
of life of people with type 1 diabetes (Figure 12). In
the 1.6million Americans estimated to have type 1
diabetes, the immune
system destroys the
pancreatic insulin-
producing cells, leaving
the body unable to
absorb or use glucose.
Signicant progress
toward articial pancre-
as technologies—which
consist of a continuous
glucose monitor, an
insulin pump, and a
computer algorithm
that, in some cases,
can be run from the
user’s smartphone—
has been made through
extensive collaboration
among NIH ICs,
other federal agencies,
private funders, academic investigators, and industry.
In 2016, the FDA approved the rst commercial
hybrid articial pancreas device
62
and in 2019, the
FDA approved the rst interoperable system
63
that
could give patients the ability to choose the individual
components that work best for them. Studies have
shown that these technologies result in better con-
trol of blood glucose levels compared to standard
treatment, potentially lowering the risk of diabetic
complications.
64
NIH continues to support research to
develop next-generation and novel devices that are
smaller, easier to use, and available to all.
Catalyzing Cell Engineering,
Bioengineering, and Regenerative
Medicine
NIH is at the forefront of remarkable technological
advances, such as innovations in cell engineering,
bioengineering, and regenerative medicine. These
advances are not only accelerating research but
also creating the possibility of new treatments that
previous generations of clinicians could only imagine.
For example, scientists supported by the NIH BRAIN
Initiative
®65
have pioneered a new technology that
converts brain signals into audible speech—a poten-
tially life-altering breakthrough for individuals who
are unable to speak due to a stroke, injury, or other
neurological condition. Next, researchers will design
a clinical trial involving paralyzed, speech-impaired
participants to determine how to best gather brain
signal data, which can then be used to rene the
previously trained com-
puter algorithm.
Biotechnology is bringing
us closer to a cure for
AMD, a leading cause of
visual impairment among
older Americans. By 2050,
the estimated number
of people with AMD is
expected to more than
double from 2million to
5 million.
66
The discovery
of induced pluripotent
stem cells (iPSCs)—adult
cells that have been
genetically reprogrammed
to a developmental stage
such that they can be
turned into any cell type in
the body—opened the door for transformative regen-
erative medicine therapies. Researchers at NIH were
able to derive iPSCs from participants with advanced
AMD and convert them into healthy retinal tissue. The
newly developed tissue replaced damaged tissue and
prevented blindness in animal models.
67
NIH received
FDA approval to begin the rst-ever clinical trial using
replacement tissue derived from iPSCs in humans.
68
Therapeutic development for many human diseases
and conditions could become faster and more
accurate due to the expanding use of tissue chips,
or “organs-on-chips.” These devices consist of
3-D platforms that support living human tissues or
cells to model the structure and function of human
organs, such as the lung, liver, and heart. Working
closely with the pharmaceutical industry and FDA, the
Tissue Chip for Drug Screening program
69
supports
research using tissue chips to test new drugs and
predict whether they will be safe and effective in
humans. In collaboration with the International Space
Station National Laboratory (ISS-NL) and the National
Aeronautics and Space Administration (NASA), NIH
is funding nine tissue chip projects in which different
types of tissues are being sent to the ISS-NL to
determine how human tissues behave in space when
Figure 12. Artificial Pancreas
The Control-IQ artificial pancreas system was derived
from research done at the Center for Diabetes
Technology at the University of Virginia.
Credit: Tandem Diabetes Care.
14
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
exposed to reduced gravity,
70
which models aging
in an accelerated manner (Figure 13). Researchers
are also developing interconnected tissue chips that
could model the entire human body’s response to
candidate therapeutics and are being deployed to
address emerging health challenges, such as the
opioid crisis and COVID-19 pandemic. In addition,
current efforts are focused on the use of tissue chips
to inform the implementation of clinical trials.
Meeting Emerging Public Health Needs
A critical focus of the NIH mission is readiness to
address new and emerging public health needs
rapidly, comprehensively, and efciently. From the
emergence of HIV/AIDS in the 1980s to the more
recent outbreaks of infectious diseases—such as
Zika virus disease, EVD, and COVID-19—to con-
ducting research during an unfolding disaster like
the Deepwater Horizon oil spill, NIH has been at the
forefront of the global research response. NIH’s role in
combatting emerging threats involves identifying and
understanding the responsible pathogens and their
effects on the body, treating affected patients in the
NIH Clinical Center as part of research studies, and
conducting and supporting clinical trials throughout
the nation and around the world.
The NIH Clinical Center is specially equipped with
high-level respiratory isolation capabilities to handle
patients with highly infectious diseases. In addition,
the staff includes infectious disease and critical
care specialists who have received training in strict
infection control practices to prevent the spread of
potentially transmissible agents. The Special Clinical
Studies Unit is used for cutting-edge investigational
clinical studies and treatments, ranging from EVD to
universal inuenza vaccine studies to treating patients
affected by the COVID-19 pandemic.
71
NIH can also swiftly mobilize its exible infrastructure
and collaborative research partnerships to help
advance new and promising treatments, even in areas
of armed conict and tenuous security. NIH and the
Institute of Biomedical Research in the DRC conduct-
ed the Pamoja Tulinde Maisha (PALM) clinical trial,
meaning “Together Save Lives,” in Kiswahili. The pre-
liminary results were so compelling that the trial was
halted, and the results were promptly made public to
help save lives and stem the latest EVD outbreak.
72
All EVD patients in the DRC treatment centers are
now treated with one of two treatment options based
on the PALM trial results. Through this collaborative
research conducted in a region of civil unrest during
an ongoing outbreak, the U.S. and its partners have
provided the world with two new effective treatments
for an emerging disease. Additionally, this experience
demonstrated the efcacy of promising therapeutics
to treat EVD and serves as a potential guide for
conducting future clinical trials in outbreak settings.
NIH’s role in safeguarding the public health extends
beyond infectious disease. For example, at this
writing, opioid misuse and addiction continues to be
a rapidly evolving U.S. public health crisis. Although
more than 50 million Americans suffer from chronic
pain, safe non-opioid options for pain manage-
ment are unavailable.
73
In 2018, more than 46,000
Americans died of opioid overdose, making it one
of the most common causes of non-disease-related
deaths for adolescents and young adults.
74
More
than 2 million Americans live with an opioid use
disorder. To address this national crisis, NIH launched
the Helping to End Addiction Long-term
SM
(HEAL)
Initiative,
75
an aggressive, NIH-wide effort to provide
scientic solutions and offer new hope for individuals,
families, and communities affected by this devastat-
ing crisis (Figure14).
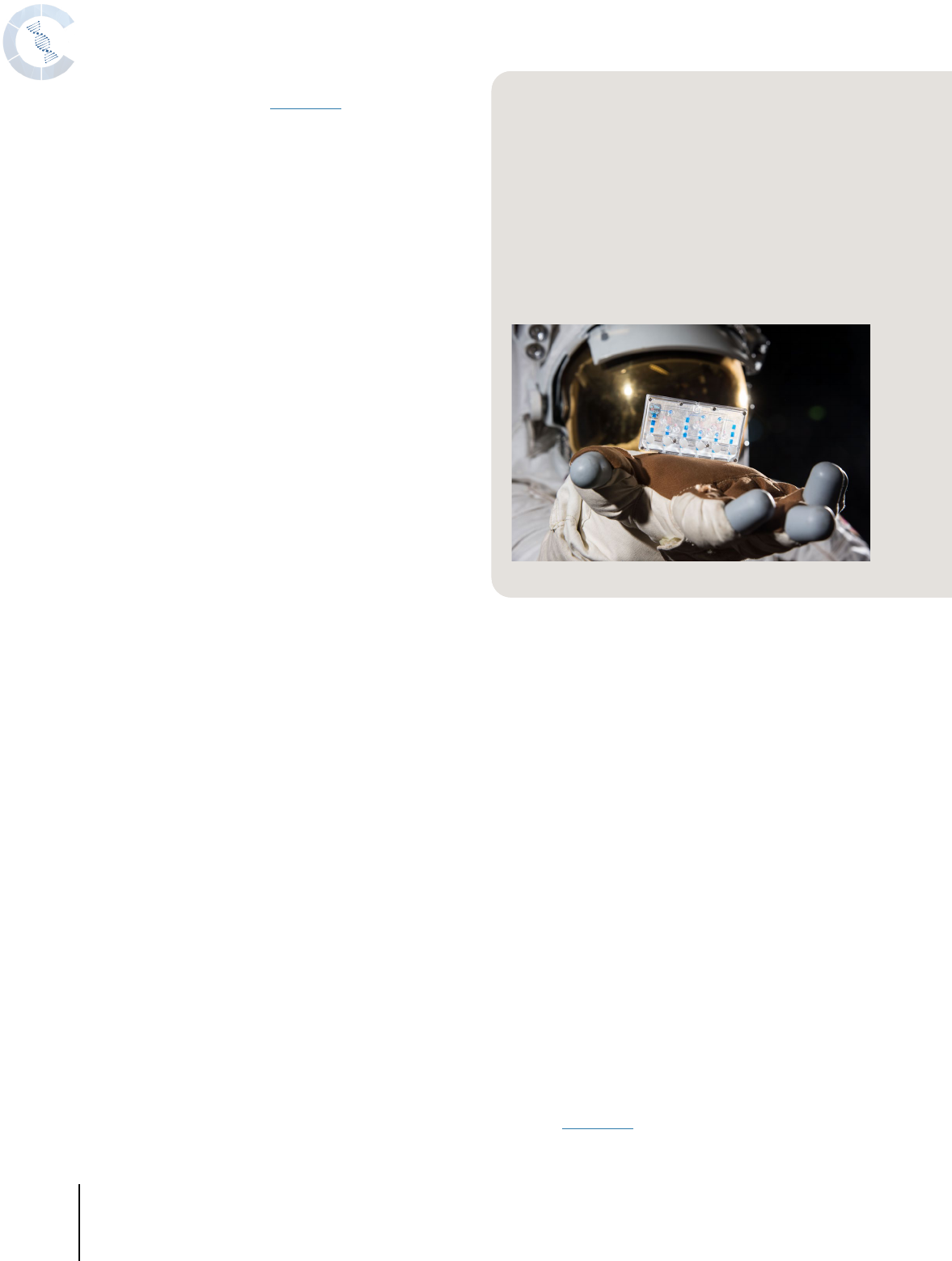
Figure 13. Tissue Chips in Space
An astronaut in a National Aeronautics and Space
Administration spacesuit is shown with a kidney tissue
chip in hand. When traveling in space, astronauts expe-
rience physiological changes normally associated with
aging, such as bone loss, muscle deterioration, and
altered immune systems. When the astronauts return to
Earth, the changes often reverse. To better understand
the relevance of the astronauts’ experience to human
health—both on the ground and in space—NIH part-
nered with the International Space Station U.S. National
Laboratory to send tissue chips, a research technology
that reflects the human body, into space.
Credit: NASA.

15
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Partnering to Advance Treatments
and Cures
Collaboration is essential to accelerating progress
in developing effective prevention and treatment
interventions, as well as ensuring that the benets of
research are available to all Americans. For example,
the Partnership for Access to Clinical Trials is a col-
laborative effort that connects health care providers
and their patients in the Washington, D.C., metropol-
itan area to NIH researchers conducting clinical trials
at the NIH Clinical Center.
76
By serving as a bridge
between research participants, their health care
providers, and NIH researchers, this program serves
as a successful model for increasing diversity in
research participation, particularly among those who
are underrepresented in clinical trials, and expanding
access to the benets of NIH research.
NIH facilitates collaboration with industry and federal
partners to advance treatment science. In 2017, in
collaboration with 12 leading biopharmaceutical
companies and advocacy organizations, NIH
launchedthe Partnership for Accelerating Cancer
Therapies,
77
a 5-year public–private research collabo-
ration, as part of Cancer Moonshot
SM
. The initial focus
of the partnership is the development, validation,
and standardization of biomarkers to better predict
response to immunotherapy—a type of biological
therapy that turns on or off the immune system
to help the body ght cancer, infection, and other
diseases.Immunotherapies have resulted in dramatic
clinical benet in certain types of cancer; however,
existing immunotherapies do not work for all patients
and are associated with substantial toxicity in some
individuals.
78
A better understanding of why immu-
notherapies work in some patients and not others is
needed to help target this treatment to the people
most likely to benet.
NIH is also transforming treatment of sickle cell dis-
ease (SCD) through collaborations (Figure 15). SCD
is a group of inherited disorders characterized by the
buildup of an abnormal protein in red blood cells.
It can cause pain, fatigue, and damage to organs
throughout the body. People of African ancestry have
the highest prevalence of SCD; it is estimated that the
disease affects up to 100,000 Americans.
79
Although
treatments are available to relieve symptoms and
extend lifespan, a bone marrow transplant is currently
the only cure for SCD.
80
Unfortunately, a transplant
is not feasible for most patients, because it requires
bone marrow from an immune-matched sibling.
In 2016, NIH established the Sickle Cell Disease
Implementation Consortium (SCDIC), the rst
Figure 14. HEAL Initiative
SM
The NIH Helping to End Addiction Long-term
SM
Initiative,
or NIH HEAL Initiative
SM
, launched in April 2018, is an
aggressive NIH-wide effort to provide scientific solutions
to the national opioid overdose crisis, including improved
treatment strategies for both pain and opioid use disorder.
Notably, a series of highly focused studies has been
launched to accelerate the development of new medica-
tions to treat all aspects of opioid use disorder, from new
formulations of existing drugs to creating new therapies
aimed at novel targets to novel devices for the treatment of
substance use disorder and pain. Working across scientific
disciplines and care settings, the NIH HEAL Initiative seeks
to match the seriousness of the crisis and offers new hope
for individuals, families, and communities affected by this
devastating crisis. In partnership with the Substance Abuse and Mental Health Services Administration (SAMHSA), in
2019 NIH launched the HEALing Communities Study to investigate how tools for preventing and treating opioid misuse
and opioid use disorder are most effective at the local level.
Credit: NIH.
Figure 15. Sickle Cell
Disease
In sickle cell disease,
red blood cells make an
abnormal protein that
causes them to take on a
sickle shape. These cells
are inflexible and can stick
to blood vessel walls,
interrupting blood flow.
Credit: Janice Haney Carr and
the CDC Public Health Image
Library.

16
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
research program to use implementation science—
the scientic study of how best to ensure the uptake
of evidence-based practice—to identify and address
barriers to quality care in SCD.
81
The SCDIC has
created a registry of more than 2,400 patients. In
2018, NIH established the Cure Sickle Cell Initiative,
an innovative collaboration among researchers in
academia and industry, clinicians, patients, and
advocates to identify and support the most promising
genetic therapies for SCD.
82
Their goal is to bring new
therapies to the point of FDA approval within the next
5–10 years.
NIH facilitates collaboration on complex scientic
questions requiring the intersection of disciplines,
methodologies, and knowledge by supporting a
variety of funding mechanisms that are focused on
collaborative or team-based work. Such opportunities
for investigator-initiated research extend from serving
as co-primary investigators on a grant award to
participating in highly complex networks of investiga-
tors and institutions charged with advancing science
in new directions. NIH looks forward to reaping the
scientic benets of continuing and expanding its
partnerships in the next 5 years.
Developing, Maintaining, and Renewing Scientific
Research Capacity
2
OBJECTIVE
NIH not only funds innovative biomedical and
behavioral research but also pursues its mission by
ensuring that the biomedical research workforce is
well trained and diverse and conducts its work within
an infrastructure that enables groundbreaking results
at a rapid pace. Over the next 5 years, NIH is poised
to enhance its support of research capacity to max-
imize the potential of the research that the agency
sustains.
Enhancing the Biomedical and
Behavioral Research Workforce
NIH recognizes that its mission will be met only
through the continued efforts of a talented and ded-
icated biomedical research workforce. The strength
of the NIH workforce depends on its sustainability
and diversity (Figure 16), which NIH supports through
both intramural and extramural focused training
programs.
Sustainability is achieved by maintaining an appro-
priate balance of researchers at different career
stages, ensuring that investigators early in their
careers are given every opportunity to excel, even
in times of limited funding. Intense competition for
funding can pose a challenge for researchers trying
to embark upon and sustain independent research
careers. NIH’s Next Generation Researchers Initiative
(NGRI) aims to enhance opportunities for early-stage
researchers by prioritizing funding of independent
research applications for investigators who are within
10 years of completing postgraduate clinical training
or their highest advanced research degree.
83
Through
this initiative, NIH has more than doubled the number
of early-stage researchers supported—from less
than 600 in 2013 to 1,316 in 2019. Moving forward,
NIH will continue to explore novel approaches to
expand pathways for funding early-stage researchers
and assess how NGRI policies affect women and
individuals from groups that are underrepresented in
biomedical and behavioral sciences.
To encourage early-stage researchers to explore new
research avenues, NIH recently created the Stephen
Figure 16. Minority Women in Science
Alma Levant Hayden was one of the first minority
women scientists in the federal government and worked
at NIH as a biochemist. Photo taken around 1952.
Credit: NIH.

17
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Ira Katz Award, in memory of the longtime director of
the National Institute of Arthritis and Musculoskeletal
and Skin Diseases. This award is designed to support
earlystage researchers who propose innovative and
unique ideas that represent a signicant change in
research direction from their past research or training
experience.
Ground-breaking, impactful biomedical and
behavioral research depends upon a diverse
workforce, composed of people trained in multiple
disciplines and from different backgrounds, who
can provide a richness of perspectives necessary to
inspire new ideas. Recognizing the need to advance
talent in muchneeded elds of study, NIH supports
training programs in a wide variety of areas, such as
bioinformatics, scientic rigor and reproducibility,
and data science. To illustrate, NIH supports
16 University-based Biomedical Informatics and Data
Science Training Programs,
84
including more than
200 Ph.D.- and postdoctoral-level researchers.
Notably, NIH also partners with high schools,
minority-serving institutions, and others to support
bioinformatics training.
Given the role that interdisciplinary approaches
and team science play in fostering innovation, NIH
has developed a number of initiatives to encourage
collaborative research. One such example is NIH’s
Building Interdisciplinary Research Careers in
Women’s Health (BIRCWH), which connects junior
and senior faculty with shared interests in interdis-
ciplinary research on women’s health.
85
Since 2000,
BIRCWH has helped more than 700 junior faculty
pursue their career goals, thereby expanding the
pipeline of women’s health researchers and beneting
the health of women.
NIH supports numerous programs designed to foster
research environments that encourage participa-
tion from a full and diverse range of talent. NIH’s
Maximizing Opportunities for Scientic and Academic
Independent Careers (MOSAIC) program
86
facilitates
the transition of promising postdoctoral researchers
from diverse backgrounds, including those from
underrepresented groups, to academic faculty
positions at institutions throughout the country. The
Native American Research Internship (NARI) program
supports diverse student researchers, including
American Indian and Alaskan Native students,
from across the country in paid summer research
internships. NARI researchers benet from cultural
and professional mentorship from American Indian or
Alaskan Native elders, community organizations, and
renowned faculty scientists.
Reective of the high priority that NIH places on
workforce diversity, the NIH Common Fund manages
several training programs targeted on diversity.
Launched in 2014, the Enhancing the Diversity of
the NIHFunded Workforce Program
87
(also called
the Diversity Program Consortium or DPC) encour-
ages the inclusion of talent across the career span.
Through integrated initiatives, DPC has supported
thousands of trainees in biomedical and behavioral
research careers by providing funding for institu-
tional infrastructure, student support, and research
mentoring. Within 4 years of launch, 1,116 students
were appointed to research-training positions through
DPC’s Building Infrastructure Leading to Diversity
(BUILD) program, with 68 percent of BUILD students
from underrepresented groups.
88
Moreover, half
of DPC member institutions (59 of 113) are either
historically Black colleges and universities or institu-
tions with a track record of training Hispanic or Latinx
students. BUILD funding enables supported scien-
tists to pursue research focused on understanding
health disparities within and across underrepresented
groups.
Plans are in place to launch the Faculty Institutional
Recruitment for Sustainable Transformation (FIRST)
initiative.
89,90
Modeled on the NIH’s Distinguished
Scholars Program,
91
FIRST aims to transform culture
at NIH-funded institutions through the recruitment
of faculty cohorts who have a demonstrated
commitment to diversity and inclusion. As it enters
Phase II of its 10-year program, the DPC will continue
to closely monitor the impact of these programs
on the careers of individuals from backgrounds
underrepresented in NIH-funded research.
NIH recognizes that women scientists often face insti-
tutional and environmental barriers that restrict their
potential to advance their careers. The NIH Working
Group on Women in Biomedical Careers aims to
identify and remove barriers to the entry, recruitment,
retention, and career development of women biomed-
ical and behavioral scientists.
92
The working group
contributed to such recommendations as extended
periods for the consideration of tenure and parental
leave, a grant program for research on causal factors
and interventions that affect the careers of women in
science and engineering, and workshops on mento-
ring women and best practices for women’s career
success. The Women of Color Committee within the

18
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
working group ensures that the unique career barriers
faced by women of color are addressed.
Public health needs extend far beyond geographical
borders. For example, deadly infectious diseases,
such as EVD and COVID-19, can spread rapidly
across international borders and continents.
Recognizing that scientic research capacity is not
equally distributed across the globe, potentially
hampering the ability to combat such challenges, NIH
develops international training programs. One such
program, the Global Infectious Disease Research
Training Program, builds infectious disease expertise
and research capacity across the world and has
prepared more than 1,200 researchers to conduct
independent and locally relevant infectious disease
research in their home countries.
93
The program
connects U.S. institutions with institutions in low- and
middle-income countries to provide degree programs,
trainings, workshops, and mentoring on topics related
to infectious diseases.
The COVID-19 pandemic has also shown the need
for local epidemiological modeling capability to
provide actionable information for policy makers to
make public health decisions during outbreaks.NIH
builds capacity for in-country analysis of COVID-19
in low- and middle-income countries by training
modelers to track and analyze the progress of the
pandemic.These activities include longstanding NIH
partners who have well-established epidemiological
and surveillance sites in Africa, South America, and
South Asia, but lack analytical capacity.
Supporting Research Resources
and Infrastructure
For the biomedical research workforce to succeed
in moving discovery forward, it requires a scientic
infrastructure that is expansive, durable, and capable
of quickly integrating state-of-the-art resources that
are available to all. To achieve this goal, NIH devel-
ops a number of programs and policies designed
to provide the biomedical research workforce with
stability and exibility, broad access to innovations
in tools and technologies, materials, and knowledge
repositories necessary for the design of impactful
research programs (Figure 17).
NIH’s support of modern technology platforms and
high-performance computing capabilities enables
innovation in scientic research in several areas,
particularly genomics, computational chemistry, and
cryo-electron microscopy imaging. Cryo-electron
microscopy is a cutting-edge technology that enables
researchers to determine the structures of biological
molecules to identify therapeutic targets for vaccines
and drugs. NIH Common Fund’s Transformative High
Resolution Cryo-Electron Microscopy program
94
aims to broaden access to cryo-electron microscopy
through the support of national service centers,
improvement of technology, and training.
NIH is also investing in the data infrastructure neces-
sary to accommodate rapid advances in biomedical
and behavioral research. Research progress has
produced an explosion of human health data that
exceeds current abilities to capture and interpret
them (Figure 18). To promote data sharing in high-
priority research areas, NIH creates a number of
different data repositories. For example, NIH has built
a data repository to maximize publication availability
and data sharing for NIH HEAL Initiative
SM
research
projects.
95
This effort promotes dissemination of new
knowledge, enhances reproducibility, and will accel-
erate the ability of researchers to build upon research
to make new discoveries. In addition, the Data and
Biospecimen Hub (DASH) is a centralized resource
that allows researchers to share and access deidenti-
ed data, and for many studies, linked biospecimens
are available to researchers.
96
Figure 17. Zebrafish Facility
At the largest zebrafish facility on NIH’s campus, Kevin
Bishop, NIH Zebrafish Core staff member, holds up a
tank of zebrafish to observe their behavior and phys-
iology. Using molecular techniques, researchers alter
the zebrafish’s genome to mimic what is seen in human
patients in the clinic.
Credit: Ernesto del Aguila III, NHGRI, NIH.

19
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Much of NIH’s efforts in resource building focuses on
providing researchers with the underlying evidence
needed to design impactful research programs.
These efforts include the development of resources
for understanding public health needs of the general
population and specic populations, resources that
will assist in providing access to patient populations,
and resources for better understanding the factors
affecting such health conditions as Alzheimer’s
disease and related dementias (Figure 19).
A widely available tool in which NIH invests to help
guide prevention and treatment efforts is the Global
Burden of Disease (GBD) enterprise.
97
GBD is the
world’s largest scientic effort to systematically
quantify health loss from all diseases, injuries, and
risk factors by age, sex, and geographic location over
time. NIH and GBD collaborated to improve the way
that disease causes and risk factors are identied.
As a result of this collaboration, NIH and the research
community can identify and track the causes and
risk factors of premature death and disability in the
U.S. over time (both historically and projecting up
to 25 years in the future). Because premature death
is often preventable, the availability of these data
not only improves understanding of the burden of
disease and key health outcomes in the U.S., but also
enhances the ability to focus on the most pressing
health challenges facing the nation.
The ability to monitor cancer in the U.S. is an import-
ant step toward determining how best to prevent and
treat cancer in specic, disproportionately affected
populations. The NIH Surveillance, Epidemiology, and
End Results (SEER)
98
Program provides information
on cancer statistics based on race, gender, and
geography to guide efforts to reduce the cancer
burden among the U.S. population. SEER currently
reects 35 percent of the U.S. population, and NIH
Figure 18. Modern Data Environments to Accelerate Research
Rapid advances in data generation and computing
power provide extraordinary potential for accelerating
biomedical research. However, researchers face technical
hurdles to accessing, sharing, and analyzing within and
across large biomedical datasets. NIH is tackling this
challenge through multiple initiatives to build modern
technology platforms, collaborative workspaces, tools,
and applications necessary for researchers to securely
find, access, share, store, and analyze data across diverse
datasets. Two examples are the Genomic Data Science
Analysis, Visualization, and Informatics Lab-space and the
Cancer Research Data Commons. These platforms enable
researchers to efficiently combine and analyze diverse
data types, which can lead to new discoveries in disease
prevention, diagnosis, and treatment. Several programs
seek to provide researchers with state-of-the-art, high-
performance computing, such as the Biowulf cluster, which
is the world’s most powerful supercomputer completely
dedicated to advancing biomedical and behavioral research.
Credit: Ernesto del Aguila III, NHGRI, NIH.
Figure 19. Alzheimer’s Disease Research
Infrastructure
More than 5.8 million Americans age 65 and older are
living with Alzheimer’s disease (AD), the most common
form of dementia. Many others younger than age 65
have developed the less common early-onset form of
AD. Still more are affected by AD-related dementias
(ADRDs). Although the underlying pathology may differ
among these conditions, their ultimate outcome is
the same: the inexorable, relentless loss of memory,
thought, and function. At present, no intervention has
been reliably proven to prevent, slow, or reverse the
effects of AD/ADRD. Under the auspices of the National
Plan to Address Alzheimer’s and Related Dementias,
NIH develops and supports a robust infrastructure for
discovery that supports activity across the full spectrum
of AD/ADRD research, including, but not limited to, the
Dominantly Inherited Alzheimer’s Network, an interna-
tional consortium of researchers who are working with
individuals from families with a rare form of the disease to
identify the sequence of brain changes before symptoms
appear; the NIH Blueprint Neurotherapeutics Network,
NIH’s preclinical/early clinical drug development program
that provides support for drug discovery and develop-
ment; and the Alzheimer’s Disease Education and Referral
Center, NIH’s primary source for consumer information on
AD/ADRD research and care.

20
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
As a steward of public resources, NIH has a respon-
sibility to uphold public trust and condence in the
agency. In addition to fostering innovative research,
NIH must endeavor to ensure that all of its operations
and the research it supports are conducted efciently,
responsibly, ethically, and with integrity. Over the next
will expand the program to cover 50 percent of the
U.S. population.
The medical advances and new technologies that
have allowed Americans to live longer and healthier
lives have not helped everyone equally. To build
capacity at institutions with a historical and cur-
rent commitment to educating underrepresented
students and providing health care in underserved
communities, NIH created the Research Centers in
Minority Institutions (RCMI) Program.
99
The goals of
RCMIs are to enhance institutional research capacity,
enable investigators to become more successful in
obtaining competitive funding, foster environments
conducive to career enhancement, promote research
on minority health and health disparities, and estab-
lish sustainable relationships with community-based
organizations.
100
NIH is also working to promote health equity in rural
populations. NIH’s Clinical and Translational Science
Awards (CTSA) Program
101,102,103
is engaging with
patients, community members, and nonprot orga-
nizations to develop and disseminate best practices
for patient-focused research in rural health.
104
Project
areas include improving access to clinical trials for
rural communities, harnessing technology to deliver
effective care, and enhancing rural community
outreach. The CTSA Program is also partnering with
other NIH ICs and federal agencies to support rural
health.
To further support rural communities, NIH is har-
nessing the Institutional Development Award (IDeA)
Program, which aims to broaden the geographic
distribution of NIH funding and to build research
capacity in states that historically have had low
levels of NIH funding. NIH is building on the research
capacity within IDeA states to help address the
medical needs of children living in rural and under-
served areas. Similarly, the Environmental inuences
on Child Health Outcomes (ECHO) Program also
leverages IDeA to expand pediatric research capacity
in the IDeA States Pediatric Clinical Trials Network.
105
Beginning in 2018, IDeA also collaborated with NIH’s
Shared Instrumentation Grant (SIG) Programs to
improve access to modern technologies for research-
ers in underresourced institutions in IDeA-eligible
states. SIG supports the acquisition of modern
scientic instruments that must be used on a shared
basis.
106
Many NIH Common Fund projects focus on devel-
oping resources that can be useful for research
communities focused on a particular topic. The NIH
Common Fund Molecular Transducers of Physical
Activity Consortium (MoTrPAC)
107,108
is building a map
of the molecular responses to exercise, both imme-
diate and over the long term. Data are being made
widely available to the entire research community so
that investigators from anywhere can use this map
to develop and test hypotheses about how exercise
improves health and ameliorates disease. The pro-
gram is scheduled to run through 2023 and released
its rst dataset through the MoTrPAC Data Hub in
2019.
Another valuable resource for the research communi-
ty includes improved understanding of the biological
and behavioral mechanisms of symptoms, which
can improve patient outcomes. The NIH Intramural
Research Program launched the Symptom Science
Center (SSC)
109
to address the need for a more
comprehensive approach to understanding the com-
plex mechanisms underlying symptoms. Increased
knowledge in this area can help develop precision
health interventions to treat patients more effectively.
Furthermore, the SSC serves as a nexus for collab-
oration among investigators from multiple ICs and
is committed to training scientists and clinicians in
symptom science.
Exemplifying and Promoting the Highest Level
of Scientific Integrity, Public Accountability, and
Social Responsibility in the Conduct of Science
3
OBJECTIVE

21
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
5 years, NIH is committed to taking additional steps
to maintain and strengthen the processes by which it
governs the conduct of science.
Fostering a Culture of Good
Scientific Stewardship
This NIH-Wide Strategic Plan positions the agency to
meet its mission by pursuing scientic opportunities
when they arise, responding to ongoing and emerging
public health needs, and addressing rare diseases.
NIH research efforts also align with and reect HHS’s
priority goals.
110
The agency promotes policies and
programs that foster and ensure a strong foundation
and culture of good scientic stewardship. As critical
research needs arise, NIH will respond by ensuring
that the scientic community has exibility to quickly
adapt to and address urgent public health issues.
Setting Priorities
Scientic priority setting at NIH encourages input from
a range of sources, including the research community;
public forums; the Advisory Committee to the NIH
Director; U.S. Congress; Administration objectives;
and consultation with advocacy groups, professional
societies, and research participants. The NIH Director
provides overall leadership to the ICs and OD ofces,
especially on efforts involving several components of
the agency. Strategic plans developed by individual
ICs and OD ofces, committees composed of repre-
sentatives from multiple ICs, and interagency working
groups describe a multitude of scientic priorities and
themes of interest to the agency.
111
NIH demonstrates effective stewardship by support-
ing the most meritorious biomedical and behavioral
research possible. The NIH peer review process
assesses research grant applications for overall
scientic and technical merit and ensures that appli-
cations receive fair, independent, expert, and timely
reviews.
112
Scientic review panels are strategically
formed to include reviewers who possess both broad
and specialized expertise and who can address
stability and recent trends in the eld. NIH makes
efforts to ensure that review panels reect diversity
in career stage, geographic region, and demographic
characteristics. NIH staff seek input from a variety
of sources to identify reviewers for panels, including
NIH program staff and advisory councils, as well
as scientic literature, meetings, and professional
organizations.
The relative merit of applications as determined
through peer review, in conjunction with input
on mission relevance from IC Advisory Councils,
informs IC Directors as they make funding decisions
that consider mission focus, portfolio balance,
scientic opportunity, emerging and ongoing public
health needs, and stakeholder priorities. Balancing
research with training and infrastructure—as well as
distribution across basic, translational, and clinical
research—are key factors taken into consideration
in maintaining a diverse portfolio. NIH also considers
the vital role of rare diseases research, through which
unique biological insights are possible. This research
is less likely to be supported by private funders than
research into more prevalent disorders.
To maintain a peer review process of the highest
caliber, NIH has developed an ongoing systematic
multimethod evaluation that will objectively assess
most peer review study sections over a 5-year
cycle.
113
The aims of the system are to keep study
sections aligned with the current state of the science,
conrm NIH is attracting applications that propose
cuttingedge science, and ensure that study sections
are functioning efciently with a balanced workload.
Additional programs, such as the Early Career
Reviewer Program,
114
help NIH refresh and diversify
its pool of reviewers, while also helping investigators
improve their grant-writing skills, develop research
evaluation capacity, and strengthen critique-writing
skills.
NIH proactively pursues scientic opportunities
through a variety of programs that promote innovative
research concepts and exploration of scientic
hypotheses that could steer science in new direc-
tions. Additionally, NIH encourages team science and
cross-disciplinary collaboration to propel research
progress. NIH will continue to look for additional ways
to capitalize on the intersection of scientic elds to
further scientic progress and improve human health.
Monitoring Expenditures and Scientific
Progress
NIH requires regular reporting from grant and contract
award recipients on research progress, spending,
and ndings. NIH staff review these reports to
ensure proper stewardship of federal funds and that
supported research is fullling all terms of the funding
agreement.

22
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Another aspect of NIH stewardship is to provide the
public with transparent and easily accessible informa-
tion about NIH research awards and allow interested
individuals to monitor NIH’s support of research.
The NIH Research Portfolio Online Reporting Tools
Expenditures and Results (NIH RePORTER)
115
tool,
for example, provides public access to information
on the grants, contracts, and intramural research
that NIH supports. Additionally, the NIH Data Book
116
provides quick access to key annual statistics, such
as application success rates, workforce and training
trends, the peer review process, and small business
awardees. NIH will continue enhancing these and
other tools in the suite of NIH RePORTER tools
117
to
better meet information and communication needs in
the coming years.
Making Evidence-Informed Decisions
NIH is committed to enhancing scientic stewardship
by optimizing approaches that generate evidence
used to inform programmatic, operational, and
policy decisions. To further these efforts, NIH has
developed several tools, available to its staff and to
the broader scientic community, that can identify
and analyze current and emerging areas of research
that will advance NIH’s mission. For example, the
iCite
118
suite of tools is a public resource that enables
users to examine validated metrics regarding the
impact of NIH-funded research articles (Figure 20).
These tools, which are informed by the judgment of
subject-matter experts, help users examine the NIH
portfolio’s productivity, balance, and priorities across
the spectrum of research—from basic to clinical and
across the diverse areas of biomedical and behavioral
research.
NIH shares common interests with many agencies
across the federal government and often coordinates
with other science agencies to promote collabo-
ration among researchers and manage research
portfolios. NIH supports Federal RePORTER,
119
a
collaborative effort among federal funders to provide
a central database for certain grant information. In
addition, NIH is partnering with the National Science
Foundation and the General Services Administration
to develop and implement computational tools to
identify overlap between grant proposals across
agencies in real-time, reducing the risk of unnec-
essarily duplicative research.
120
Collectively, these
efforts promote transparency and enable efciency
through data-driven decision-making.
Assessing Programs, Processes,
Outcomes, and Impact
The NIH Report on Approaches to Assess the Value
of Biomedical Research by NIH
121
found that a better
understanding of all aspects of NIH’s work is key
to increasing the efciency and effectiveness of the
agency. NIH uses a variety of approaches—including
monitoring, performance measurement, analysis, and
evaluation—to assess the progress and effectiveness
of its programs, policies, and operations and to
generate information for decision-making. To increase
the use of these tools, NIH is enhancing the quality
of administrative data, making it an increasingly
strategic source of information that, when coupled
with other tools, could improve the agency’s
Figure 20. Predicting Translational Progress of Research
Fundamental research can take
decades to translate into clinical
outcomes. To capture the trans-
lational potential of publications,
NIH researchers created a machine
learning model that maps papers on
a trilinear graph using three Medical
Subject Heading (MeSH) terms:
Human, Animal, and Molecular/
Cellular. Almost all NIH-funded
papers (> 96 percent) are assigned
at least one of the MeSH terms and
can be plotted somewhere on “the
triangle of biomedicine.” The graph
pictured depicts the accumulation of
fundamental, translational, and clinical research that led to cancer immunotherapy drugs like Opdivo (nivolumab). This
visualization was generated using the iCite web tool developed by NIH.
Credit: Hutchins BI, Davis MT, Meseroll RA, Santangelo GM. Predicting translational progress
in biomedical research. PLOS Biol 2019;17(10):e3000416. https://doi.org/10.1371/journal.
pbio.3000416.

23
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
effectiveness. Under HHS’s guidance, NIH will
engage in capacity- and evidence-building activities
to support the Department’s implementation of the
Foundations for Evidence-Based Policymaking Act of
2018
122
and further develop its data-driven, results-
oriented culture.
Communicating Results
NIH fosters scientic stewardship by ensuring that
the products and processes of scientic research,
such as research data and scientic publications, are
available in accord with the FAIR principles that all
research data should be ndable, accessible, interop-
erable, and reusable (Figure 21). NIH communicates
research ndings to the public in numerous ways,
including through press releases on recent scientic
advances on the NIH News & Events
123
website,
the NIH Director’s Blog,
124
and the Impact of NIH
Research pages,
125
which have examples illustrating
the downstream impact of NIH research on public
health and society. Additionally, NIH ICs and OD ofc-
es develop and disseminate a range of publicfriendly
health- and disease-specic educational materials
on a host of topics. NIH provides evidence-based
and authoritative biomedical information in highly
expeditious and proactive ways. This vital function is
especially important during public health emergen-
cies, such as infectious disease or foodborne illness
outbreaks.
Research results are also communicated through
such NIH resources as PubMed and ClinicalTrials.
gov. In 2020, NIH launched the new PubMed,
126,127
the most heavily used biomedical literature citation
database in the world, which enables the commu-
nication and discovery of scientic literature around
the world. NIH’s PubMed Central (PMC)
128
provides
public access to the full text of more than 6 million
peer-reviewed research articles (Figure 22). PMC
facilitates linking between articles and associated
data; supports discovery of these data by aggregat-
ing data citations, data availability statements, and
supplementary materials; and contains a subset of
about 3 million articles available for bulk retrieval for
text mining and other research purposes.
Reports from clinical studies are made available
through ClinicalTrials.gov, the largest public clinical
research registry and results database in the world.
This NIH resource provides patients and their
caregivers, health care providers, and researchers
with information on more than 330,000 active and
complete registered studies, including studies with
summary results, many of which are not otherwise
available through published literature. A multiyear
effort is underway to modernize ClinicalTrials.gov to
deliver an improved user experience on an updated
platform that will accommodate growth and improve
efciency.
In response to the COVID-19 pandemic, NIH part-
nered with researchers and leaders from universities
and industry to rapidly mobilize and create the
COVID-19 Open Research Dataset (CORD-19)
129
of
scholarly literature about COVID-19, SARS-CoV-2,
and other coronaviruses. CORD-19 provides
immediate, machinereadable access to the full text
of pre-print and peer-reviewed articles to assist
researchers worldwide in nding answers to high-
priority scientic questions related to the COVID-19
response. NIH also developed the COVID-19 portfolio
tool
130
as a complement to CORD-19. This tool
provides powerful search functionality and interactive
Figure 21. FAIR Principles
NIH is working to align the research that it supports
with the FAIR principles (findable, accessible, reus-
able, interoperable) to ensure that the results of NIH
investments can be leveraged by the entire research
enterprise. NIH organizes its data science efforts
around five themes: advancing data infrastructure to
increase connectivity across systems and platforms;
defining strategies to help researchers better store
and share their data; adopting and adapting data
science tools to enhance research; engaging with
stakeholder communities and enabling citizen
scientists to support the biomedical data enterprise;
and increasing the capacity of computational and
data science workers in biomedical research through
new and existing workforce programs.
Credit: Office of Data Science Strategy, NIH.

24
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
visualizations to support cutting-edge analytics of
the literature to identify gaps and opportunities in
COVID-19-related research. In addition, to assist
researchers working on the genomics of the novel
coronavirus, the COVID-19 Genome Sequence
Dataset on Registry of Open Data on Amazon Web
Services
131
is a centralized sequence repository for
strains of SARS-CoV-2.
Leveraging Partnerships
Expanding fundamental knowledge of biological
systems and applying that knowledge to the
advancement of health requires strategic partnerships
with a range of organizations, including other federal
agencies, international governments, the private
sector, and the public. These partnerships bring
enhanced coordination, critical expertise, pooled
resources, and novel stakeholder connections to
augment NIH efforts.
Federal Partnerships
NIH values collaboration with its federal partners
and partners extensively with other federal agencies.
Interagency collaborations address critical public
health needs and facilitate coordination, communica-
tion, and resource-sharing. For instance, the Tobacco
Regulatory Science Program (TRSP),
132
a partnership
between NIH and FDA, funded research on youth
tobacco use; toxins and nicotine concentration in
e-cigarettes; and the Population Assessment of
Tobacco and Health (PATH) Study, a longitudinal
examination of tobacco product use.
133
Data from
TRSP studies provide valuable evidence to inform
government-wide policymaking. Research results
from the Tobacco Centers of Regulatory Science, a
centerpiece of TRSP, will provide further insight into
who is using these products, what health outcomes
result from product use, and how to implement
interventions to target health outcomes.
134
Another key federal collaboration is the Interagency
Pain Research Coordinating Committee (IPRCC),
135
chaired by NIH with members from several agencies
within HHS, including FDA, Centers for Disease
Control and Prevention (CDC), Agency for Healthcare
Research and Quality (AHRQ), Department of Defense
(DoD), and U.S. Department of Veterans Affairs (VA).
IPRCC coordinates federal activities to enhance
pain research efforts and promote collaboration
across the government, with the ultimate goals of
advancing the fundamental understanding of pain
and improving pain-related treatment strategies. NIH
also partners with DoD and VA on the NIH-DoD-VA
Pain Management Collaboratory, which supports
the development, implementation, and testing of
cost-effective, large-scale, real-world research on
nonpharmacologic approaches for pain management
and related conditions in military and veteran health
care delivery organizations.
136
The 21st Century Cures Act established the HHS
Task Force on Research Specic to Pregnant Women
and Lactating Women (PRGLAC) to advise the HHS
Secretary regarding gaps in knowledge and research
on safe and effective therapies for pregnant women
and lactating women (Figure 23).
137
Led by NIH, other
Figure 22. PubMed Central
As a free archive of full-text biomedical and life sciences journal literature, PubMed Central is an authoritative source
of scholarly information that ensures the insights gained through biomedical discovery are made openly available to
research and clinical care communities, as well as to the public at large.
Credit: National Library of Medicine, NIH.

25
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
federal members include CDC, FDA, AHRQ, Health
Resources and Services Administration (HRSA), VA,
and HHS Ofce on Women’s Health. Non-federal
members include representatives from medical soci-
eties, nonprot organizations, and industry. More than
6 million women are pregnant in the U.S. each year,
many taking medications or dietary supplements.
PRGLAC identied the lack of scientic evidence on
the safety and efcacy of these compounds during
pregnancy or breastfeeding as a substantial knowl-
edge gap in maternal health.
Public-Private Partnerships
Public–private partnerships (PPPs) provide a mech-
anism to strategically accelerate advances and
accomplish goals that NIH cannot readily achieve by
acting alone. For example, to hasten the development
of interventions for COVID-19, NIH is leading the
Accelerating COVID-19 Therapeutic Interventions and
Vaccines (ACTIV)
138
PPP (Figure 24). PPP activities
focus on the shared goals and mandates of the
partners and leverage knowledge, skills, resources,
and services to achieve synergy. For example, NIH—
together with FDA, biopharmaceutical companies, and
nonprot organizations—launched the Accelerating
Medicines Partnership (AMP).
139
The goal of AMP is to
increase the number of new diagnostics and therapies
and reduce the time and cost of developing them.
Four AMP initiatives are underway: AMPAlzheimer’s
Disease (AMP-AD), AMP-Parkinson’s Disease (AMP-
PD), AMP-Rheumatoid Arthritis/Lupus (AMP-RA/
Lupus), and AMP-type 2 diabetes (AMP-T2D). After
successfully meeting program milestones, AMP-AD
and AMP-T2D are nalizing research plans for the next
phase of the program. New AMP initiatives have been
launched for schizophrenia
140
and are in development
for gene therapy.
To capitalize on dramatic advances in genetics, NIH
and the Bill and Melinda Gates Foundation have
expanded their cooperation toward an audacious
goal: to develop affordable, gene-based cures for
SCD and HIV within a decade. The intention is for
these cures to be made globally available, especially
in lowresource settings where people are most
affected by these conditions.
Figure 23. Research for Pregnant and
Lactating Women
The 21st Century Cures Act established the Task Force
on Research Specific to Pregnant Women and Lactating
Women (PRGLAC) to advise the Secretary of Health
and Human Services regarding gaps in knowledge and
research on safe and effective therapies for pregnant
women and lactating women. PRGLAC was tasked with
identifying these gaps and reporting its findings to the
Secretary.
Credit: NICHD, NIH.
Figure 24. ACTIV: An Unprecedented Partnership for Unprecedented Times
In April 2020, NIH launched the Accelerating COVID-19
Therapeutic Interventions and Vaccines (ACTIV) public–
private partnership to develop a coordinated research
strategy for prioritizing and speeding the clinical evaluation
of the most promising vaccines for severe acute respiratory
syndrome coronavirus 2 (SARS- CoV -2) and treatments for
coronavirus disease 2019 (COVID -19). Through ACTIV, NIH
has partnered with more than 15 biopharmaceutical com-
panies, as well as its sibling agencies and offices within
the U.S. Department of Health and Human Services, other
government agencies, the European Medicines Agency,
and representatives from academia and philanthropic
organizations. Through the ACTIV partnership, NIH is
pursuing four fast-track focus areas most ripe for oppor-
tunity: (1) developing a collaborative, streamlined forum to standardize and share evaluation methods and testing of
preclinical therapeutics and vaccines; (2) prioritizing and accelerating clinical testing of the most promising treatments
for all stages of the disease; (3) leveraging clinical trial capacity and effectiveness; and (4) accelerating the evaluation
of vaccine candidates to enable rapid authorization or approval.
Credit: NIH.

26
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
The NIH Science and Technology Research
Infrastructure for Discovery, Experimentation, and
Sustainability (STRIDES) Initiative
141
—one of many
NIH-wide efforts underway to implement the NIH
Strategic Plan for Data Science—provides NIH and
its funded researchers with cost-effectiveaccess
to state-of-the-artcloud-baseddata storage and
computational capabilities, tools, and expertise.
Through STRIDES, NIH has established PPPs with
commercial providers, such as Amazon Web Services
and Google Cloud. NIH anticipates forming additional
industry partnerships through STRIDES to broaden
access to services and tools, including training and
professional services for researchers on how to
use the latest cloud tools and technologies. These
partnerships will allow academic researchers and
industry to come together to create a data ecosystem
that maximizes the use of NIH-supported biomedical
and behavioral research data for the greatest benet
to human health.
During the next 5 years, NIH will continue to expand
partnership opportunities focused on increasing diag-
nostics and therapies for particular conditions, curing
intractable diseases, and making the vast amount of
data generated by biomedical research accessible to
as many researchers as possible.
International Partnerships
As the world grows increasingly connected, NIH
remains committed to developing and sustaining
relationships with partners around the globe. Recent
events, including the COVID-19 pandemic, have
illuminated the importance of a coordinated approach
to global health aligned with humanitarian and scien-
tic values. Geographic boundaries do not prevent
infectious disease spread, nor should they prevent
the advancement of research on such diseases. For
this reason, NIH collaborates internationally with
foreign governments and organizations.
In collaboration with the Ofce of the U.S. Global
AIDS Coordinator and Health Diplomacy, NIH sup-
ports the African Forum for Research and Education
in Health (AFREhealth)
142,143
Program and the Health-
professional Education Partnership Initiative,
144
both
of which are designed to enhance the quality, quan-
tity, retention, research engagement, and networking
of an interprofessional health workforce across Africa.
NIH also supports the Human Heredity and Health
in Africa Consortium (H3Africa) via the NIH Common
Fund.
145
This partnership includes the Wellcome Trust
and the African Academy of Sciences and seeks
to build African research capacity in the genomic
sciences and contribute to improving understanding
of health and disease in underrepresented and
underserved populations.
NIH participates in the Global Alliance for Chronic
Diseases (GACD),
146
a consortium of the world’s
largest public research funding agencies. GACD’s
mission is to reduce the burden of chronic
noncommunicable diseases (NCDs) in low- and
middle-income countries and in populations facing
conditions of vulnerability in high-income countries,
by building evidence to inform national and
internationalNCDpolicies. NIH funds GACD research
in the areas of cancer prevention, mental health, lung
disease, type 2 diabetes, hypertension, and scaling-
up evidence-based interventions.
In addition to working with international partners on
disease, NIH also supports other types of interna-
tional health initiatives. For example, the NIH Disaster
Research Response (DR2) Program, which supports
research to inform disaster and public health emer-
gency preparedness, response, and recovery, serves
as a compelling model for addressing crises. DR2
has partnered with Japan’s National Institute for
Environmental Studies and Health Canada to begin
developing similar programs in those countries.
147
Early outcomes include translation of data collection
tools to Japanese, using DR2 tools in response to
Typhoon Hagibis, collaboration on DR2 workshops
and training exercises, and international outreach.
Public Engagement
Public engagement is vital to NIH research. Patients,
research participants, disease advocacy organi-
zations, and local, state, and cultural communities
have a leading role to play in the research enterprise.
During study design, these groups can highlight
important knowledge gaps impeding community-level
programs, policies, and practices. During data
collection and analysis, they advise researchers on
the challenges of applying new knowledge in different
local and cultural contexts.
As part of its commitment to public engagement, NIH
will continue providing underrepresented groups with
equal access to research in an ethical and respon-
sible manner that protects privacy and respects
cultural sensitivities. NIH facilitated a data sharing
and use agreement between the Navajo Nation

27
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
and NIH grantees of the ECHO Program.
148
The
agreement was created to advance the Navajo Birth
Cohort Study while respecting Navajo Nation cultural
beliefs, Tribal sovereignty, and community values.
149
It is the rst Tribal data-sharing agreement for a
large-scale database as part of a nationwide research
consortium. This achievement lays the groundwork
for discussion of similar agreements with other Tribal
Nations considering participation in biomedical and
behavioral research programs.
Public engagement is also key to NIH’s maternal
health efforts. The NIH Task Force on Maternal
Mortality developed Implementing a Maternal health
and PRegnancy Outcomes Vision for Everyone
(IMPROVE), an NIH-wide research initiative. IMPROVE
was informed by input from a variety of sources,
including the public and NIH-convened meetings for
scientists and clinicians to solicit recommendations
on health disparities underlying maternal mortality,
as well as gaps and opportunities for future research.
IMPROVE will focus on women beginning in pregnan-
cy and continuing up to 1 year postpartum and will
include community-focused social and biobehavioral
research, as well as research to accelerate discovery
and advance technologies to reduce maternal health
risks.
Ensuring Accountability and
Confidence in Biomedical and
Behavioral Sciences
To foster condence in NIH-funded research and
results, NIH must ensure that both its operations
and its supported research are conducted efciently,
responsibly, ethically, and with integrity. NIH is
committed to taking steps to maintain and strengthen
the processes by which it governs the conduct of
science, continuing to be accountable for the public
funds it invests in research.
Enhancing Reproducibility Through
Rigorous and Transparent Research
Two cornerstones of scientic research are rigor in
the design and conduct of experiments and the ability
to reproduce research ndings. The application of
scientic rigor ensures robust and unbiased experi-
mental design, methodology, analysis, interpretation,
and reporting of results. When a result can be repro-
duced by multiple scientists working independently, it
validates the original result and indicates readiness to
progress to the next phase.
NIH has collaborated with scientic journal publishers
to identify shared opportunities to enhance transpar-
ency, rigor, and reproducibility in published literature.
NIH has also convened working groups and work-
shops focused on rigor, developed training modules
for the research community on good experimental
design, enhanced requirements for the content and
review of grant applications, and developed specic
funding opportunities aimed at improving rigor and
reproducibility. Moving forward, NIH will continue
working closely with researchers, publishers, and
federal partners to develop and share recommenda-
tions and best practices. Along these lines, NIH has
convened a working group of the Advisory Committee
to the Director to explore ways to enhance reproduc-
ibility and rigor in laboratory animal research.
150
Improving Stewardship of Clinical Trials
NIH invests more than $3 billion each year in clinical
trials. NIH must ensure these trials investigate
high-priority questions, do not needlessly duplicate
previous trials, recruit and maintain sufcient par-
ticipants, are completed in a timely manner, and are
likely to advance knowledge and improve health.
NIH has launched a series of efforts to enhance
accountability and transparency in clinical research,
151
as well as address challenges and shortcomings in
the design, efciency, and timeliness of reporting
clinical trial results. These efforts included dedicated
funding opportunities, Good Clinical Practice training,
a single Institutional Review Board for multisite
research policy, and an optional template that guides
investigators through the systematic development
of a comprehensive clinical protocol and required
registration and reporting of clinical trial results. In
addition, by ensuring that summaries of results of
NIH-supported clinical trials are widely and freely
available, ClinicalTrials.gov promotes transparency
and helps ensure that research ndings are contribut-
ing to the advancement of public health.
Assuring Ethical and Equitable Conduct of
Research Through Inclusion
More women and underrepresented and underserved
groups are participating in clinical research than
ever before, in large part thanks to NIH policy. NIH’s
goal is to ensure that these trends continue so that

28
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
the knowledge gained from research is applicable
to everyone affected by the disease or condition
under study (Figure 25). To this end, NIH has taken
critical steps to ensure the scientically appropriate
enrollment of women and underrepresented and
underserved groups in clinical research and is
engaged in efforts to increase inclusion of children,
older adults, pregnant and lactating women, and
individuals with disabilities as appropriate. NIH
requires researchers who propose research involving
human subjects to include plans for how participants
from these groups will be enrolled, unless there is a
scientic or ethical justication for their exclusion.
Once a grant is awarded, researchers must annually
report deidentied individual-level demographic data
so that NIH can continue to monitor inclusion.
NIH will continue its focus on challenges to recruiting
and retaining underrepresented populations in clinical
studies and will add data on the age at enrollment of
participants to the Research, Condition, and Disease
Classication (RCDC) Inclusion Statistics Report,
which allows users to view trends over time. In
addition, NIH will train researchers to include women,
underrepresented and underserved populations, and
individuals of all ages in studies as part of its efforts
to increase the diversity of study populations.
Maintaining Transparency Through Data
Access and Sharing
NIH is committed to making ndings from the
research that it funds accessible and available in a
timely manner, while also providing safeguards for
privacy, intellectual property, security, and data man-
agement. For instance, NIH-funded investigators are
expected to make the results and accomplishments
of their activities freely available within 12 months
of publication. NIH also encourages investigators to
share results prior to peer review, such as through
preprints, to speed the dissemination of their ndings
and enhance the rigor of their work through informal
peer review.
A robust culture of data sharing is critical to contin-
ued progress in science, maximizing NIH’s investment
in research, and assurance of the highest levels of
transparency and rigor. To this end, NIH will continue
to promote opportunities for data management and
sharing while allowing exibility for various data
types, sharing platforms, and strategies. Additionally,
NIH is implementing a policy requiring that all appli-
cations include data sharing and management plans
that consider input from stakeholders.
152,153
Fostering a Safe and Harassment-Free
Work Environment
NIH has an imperative to transform the culture of
science to prevent harassment (sexual, gender, and
other) and mitigate its detrimental impacts, whether
it is in the agency or anywhere NIH-funded activities
are conducted. In 2019, NIH established the Advisory
Committee to the NIH Director Working Group on
Changing the Culture to End Sexual Harassment.
154
Following this group’s recommendations, NIH is
taking actions within the agency’s authority to change
the scientic workplace to make it safer and more
welcoming (Figure 26). NIH issued several new pol-
icies, guidelines, and requirements on this topic and
communicated them widely to make expectations
clear to NIH-funded organizations and the workforce
at NIH.
155
NIH expects recipients of federal funds to have
policies and practices in place that foster a safe and
harassment-free environment.
156
For instance, NIH
must be notied if a principal investigator or other key
personnel named on an NIH grant award is unable to
Figure 25. Clinical Center Research
An NIH researcher examines a pediatric patient in the NIH
Clinical Center.
Credit: Richard Clark, NIAMS, NIH.

29
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
fulll their obligations to conduct research because
they are under investigation or have been removed
from the workplace because of sexual harassment
concerns. NIH expects recipients requesting changes
in investigator, key personnel, or recipient institution
to mention whether these requests are related to
concerns about the safety and/or work environment,
including issues related to sexual harassment or
bullying.
157
Internally, NIH has undergone a workplace
climate and harassment survey to inform policy and
practice and has expanded its human resources
program to foster civility throughout the NIH commu-
nity.
158
NIH’s efforts have led to increased scrutiny and
awareness of harassment, centralized mechanisms
for reporting harassment, and new anti-harassment
policies. NIH will continue working with its partners
and exploring policymaking options based on recom-
mendations from the Advisory Committee to the NIH
Director and ndings from internal studies to change
the scientic culture, prevent sexual harassment, and
promote a civil, safe, and respectful workplace for
everyone.
Managing Risks to the Research Enterprise
NIH is committed to proactively managing risks
that may impede the NIH mission. Such risks have
the potential to affect patient and laboratory safety,
the peer review process, laboratory animal welfare,
conict of interest disclosures, closeout of grant
awards, data security, and more. Understanding the
need to identify and manage risks, NIH incorporated
Enterprise Risk Management (ERM) capabilities into
its strategic planning, performance management, and
resource allocations (see Figure 27). Going forward,
NIH is better prepared to respond to emerging risks
that may undermine its research activities and are
inconsistent with its research values and principles.
Figure 26. NIH Harassment Does Not Work
Here Campaign
An image stating “Harassment Doesn’t Work Here”
as part of NIH’s campaign to create a safe and
civil workplace wherever NIH-funded research is
conducted.
Credit: NIH Civil Program.
Figure 27. Managing Risks to the Research Enterprise
The NIH Risk Management Program provides NIH with a
framework for systematically identifying and addressing
risks that might adversely affect NIH’s ability to fulfill its
mission. Risk management is a continuous process that
requires all NIH staff and researchers to proactively identify
and mitigate risk as part of their daily jobs. Understanding
the need to identify and manage risk, NIH has incorporated
Enterprise Risk Management (ERM) capabilities into
its strategic planning, performance management, and
resource allocations. ERM is a strategic discipline that
seeks to deliberately and proactively understand the full
spectrum of risks, including opportunities across an entire
organization, and integrates them into an enterprise-wide,
strategically aligned, and interrelated risk portfolio view. By
incorporating ERM, NIH can proactively address emerging
threats and opportunities and deliver results to the public in
a transparent and accountable manner, all in an effort to
further support NIH’s mission.
Credit: NIH Risk Management Program.

30
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
As a part of its commitment to a culture of health and
safety for people conducting NIH-funded research,
and to mitigating the effects of emergencies on the
research enterprise, the NIH Extramural Response
to Natural Disasters and Other Emergencies policy
allows NIH to provide resources and assistance to
those in the NIH community affected by public health
emergencies.
159
Under such circumstances, NIH
will provide administrative exibilities and additional
funding using a number of mechanisms to support
the continuation of research, as demonstrated during
the COVID-19 pandemic.
160
NIH and the research community have a vested
interest in mitigating any breaches of trust and
condentiality that undermine the integrity of U.S.
biomedical research, while continuing the tradition
of scientic collaboration, including international
collaboration. NIH recognizes the importance of these
collaborations to advancing its mission. However,
some researchers at NIH-funded institutions have
taken advantage of these collaborations through fail-
ing to disclose contributions of resources from foreign
organizations, diverting proprietary information to
foreign governments, and sharing condential infor-
mation obtained from NIH peer review meetings or
otherwise trying to inuence the peer review process.
NIH works with other federal agencies to take strong
actions in response to these breaches of integrity
which appear to be, at least partly, instigated by
foreign governments.
161
NIH has increased the
visibility of this issue and reminds grant recipients to
be transparent and disclose all afliations, nancial
conicts of interest, and other support (including from
foreign entities) and contacts recipient institutions
about any concerns.
162
NIH has also bolstered its
internal processes and systems and increased
awareness among its own staff.
Looking to the future, NIH will continue careful
monitoring and extensive outreach with academia,
professional societies, and federal partners to
reinforce the importance of research security and
integrity, as well as to hold people and institutions
accountable for inappropriate actions.
163
NIH will
continue to work closely with federal partners to
protect the safety, integrity, and inclusivity of U.S.
research and looks forward to continuing to work with
institutions and researchers to strengthen values that
underpin research integrity and protect the nation’s
biomedical innovations.
164
Reducing Administrative Costs and Work
Throughout the Grants Process
Reducing administrative burden increases the amount
of time that investigators can spend on research
and that administrators can spend supporting the
research enterprise. NIH works to streamline grants
policies and processes to reduce administrative
work and costs. Recent changes include automating
the issuance of certicates of condentiality that
protect participants in NIH-funded research, creating
the Application Submission System & Interface
for Submission Tracking (ASSIST) as an option for
preparing and submitting applications, developing
a tool that reduces the need to develop clinical trial
protocol text de novo, simplifying the appendix and
other material in grant applications to help during the
review process, and reducing the need for multiple
biographic proles across different systems to help
people nd information and simplify reporting and
analysis.
165
NIH will continue to work with stake-
holders to further streamline the grant application
process, while promoting rigor and fostering compli-
ance.
Optimizing Operations
NIH seeks to continually optimize operations across
an array of business, administrative, and scientic
functions, as well as to improve its physical and
technological infrastructures. Increasing coordination
and engagement throughout the agency and manag-
ing risk while fostering innovation are critical to the
stewardship of the nation’s biomedical and behavioral
research ecosystem. Over the next 5 years, NIH will
implement strategies to excel as a federal science
agency dedicated to protecting and improving public
health.
NIH will continue implementing its Optimize NIH
efforts, which were established as part of the
Reimagine HHS effort to improve performance across
the Department’s divisions. Through the Optimize NIH
initiative, the agency is focusing on administrative
areas that could be made more efcient and effective
if managed centrally, or better harmonized across
ICs and OD ofces. Using a combination of process
mapping, surveys, and focus groups, the agency will
carefully evaluate which approach or combination of
approaches would yield the greatest improvements
in each area. NIH’s optimization efforts are guided in
a data-driven and scientic manner, using teams led

31
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
by NIH experts in administrative operations with full
engagement by employees.
Examples of functional areas that have already seen
substantial improvement through Optimize NIH
include management of federal advisory committees,
employee ethics requirements, and Freedom of
Information Act (FOIA) requests. NIH has adopted
a unied system to standardize and streamline
management of FOIA requests across the agency and
has launched a public-facing portal, FOIAXpress, to
improve the FOIA requestor experience. The launch
of this portal increased information request process-
ing speed by 83 percent, decreased the backlog by
11 percent, and offered solutions that can be lever-
aged across HHS. The lessons learned through the
optimization of initial functional areas will inform NIH’s
approach to other business practice enhancements,
such as information technology security, acquisitions,
appointment of employees via a specialized hiring
mechanism, travel management, and property
management.
Optimize NIH will also continue to establish best
practices for evaluating employee workload to
improve the management of resources, inform hiring
decisions, and reduce workload inequities. Workload
harmonization across ICs and OD ofces is already
underway for scientic review, grants management,
and program management, with additional areas
identied for future improvement. NIH will also
continue to harmonize and align each IC’s strategic
plan with a common template derived from the NIH-
Wide Strategic Plan. Taken together, Optimize NIH
projects will improve organizational effectiveness and
performance and maximize the investment made by
American taxpayers.
In alignment with the Reimagine HHS and Optimize
NIH initiatives and in response to NIH community
feedback, the NIH OD launched the OD Strategic
Engagement Agenda to foster a unied and
coordinated OD, which engages seamlessly with
the ICs to advance the mission of the agency. This
data- and participant-driven initiative will solicit and
incorporate employee input through listening tours,
working groups, and an online ideation campaign
to improve communication and functionality within
the OD through coordination and engagement
with the ICs. By working toward these goals and
improving on the use of OD operating principles of
transparency, accountability, strategy, coordination,
and decisionmaking, NIH will increase the efciency
and effectiveness of collaboration across NIH.
Meeting the goal of increased efciency and effec-
tiveness of operations across the agency requires
the systematic assessment and management of
risk in NIH’s administrative and scientic programs,
processes, and procedures. NIH is committed
to integrating an ERM framework into its organi-
zational culture to help prevent surprises, avoid
operational failures, and allow quicker recovery
when the unexpected happens. For example, NIH
evaluated the extramural grant program using a
fraud risk framework to identify vulnerabilities and
develop mitigation strategies, including a staff fraud
awareness and training program, to reduce the risk
Figure 28. NIH Campuses
Aerial views and photos of various building on NIH
campuses showing a portfolio of biomedical research,
administrative, and infrastructure-supporting facili-
ties. From left to right and top to bottom: Research
Triangle Park, North Carolina; Phoenix Epidemiology
and Clinical Research Branch, Phoenix, Arizona;
Rocky Mountain Laboratories, Hamilton, Montana;
NIH Main Campus, Bethesda, Maryland; Pregnancy
and Perinatology Branch, Detroit, Michigan; National
Cancer Institute at Shady Grove, Rockville, Maryland;
NIH Animal Center, Poolesville, Maryland; Bayview
Campus, Baltimore, Maryland; and Frederick National
Laboratory for Cancer Research, Frederick, Maryland.
Credit: Office of Research Facilities Development and
Operations, NIH.

32
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Many scientic challenges and opportunities are
not unique to any one Objective in this Strategic
Plan. To emphasize this, NIH has identied ve key
Crosscutting Themes that span all aspects of NIH’s
Strategy.
Improving Minority
Health and Reducing
Health Disparities
Underserved groups—including
Black, Latinx, and Indigenous and
Native American persons, Asian
Americans and Pacic Islanders,
and other persons of color; members of religious
minorities; lesbian, gay, bisexual, transgender, and
queer (LGBTQ+) persons; persons with disabilities;
persons who live in rural areas; or persons otherwise
adversely affected by persistent poverty or inequali-
ty—have distinct health needs and often experience
disparities in health outcomes. NIH maintains that
racial and ethnic minorities, rural residents, people
with low incomes, SGM, and other populations
experiencing health disparities should be included
in all relevant research, such that there is sufcient
representation of each population to conduct relevant
analyses. Inclusivity in research generates more
broadly applicable information and improves scientic
understanding of the health and well-being of specic
population groups.
To promote health equity, NIH remains committed to
supporting a robust program of research examining
how biological, behavioral, environmental, socio-
cultural, and other factors interact with and shape
individuals’ health trajectories across the lifespan.
The science of minority health and health disparities
is founded on the principle that the social construct
of individual race and ethnicity and socioeconomic
status inuence behavior, biology, and health
outcomes in many dened and undened ways.
These individual factors interact with structural social
determinants that may promote cumulative adversity
that leads to worsened health outcomes through
biological mechanisms.
Racism and discrimination are increasingly recog-
nized as contributing to poorer health outcomes for
of fraud in the NIH extramural program and protect
public funds. By conducting risk assessments and
leveraging data collected within the ERM framework,
NIH will improve information sharing and leadership
decisionmaking and will prioritize corrective actions
for identied risks. Incorporating ERM practices into
daily operations also supports NIH in taking risks
intelligently and prudently to achieve desired mission
outcomes and enhances the agency’s transparency
and accountability to the public.
Underpinning NIH efforts to optimize its administra-
tive and scientic operations are efforts to advance
the agency’s physical and technological infrastruc-
tures. For example, many of the agency’s research
and supporting facilities were constructed more than
50 years ago and require signicant operating and
maintenance costs, repairs, and upgrades to remain
competitive in a global research environment. As
resources become available, NIH will make strategic
investments in building, expanding, and modernizing
infrastructure on all its campuses.
It is critical that NIH provide, maintain, and operate
its physical infrastructure—buildings and facilities
capable of fullling and responding to the complex,
collaborative, and changing nature of biomedical and
behavioral science (Figure 28). The conduct of sci-
entic discovery is enabled through safe and reliable
facilities that can be adapted to support research on
existing and emerging public health challenges, such
as Alzheimer’s disease and viral pandemics.NIH will
closely link its strategic research goals to the avail-
ability, suitability, and capability of existing facilities
and will plan, program, and budget for redeveloped
and new facilities using planning and space utilization
principles consistent with recognized business
practices and the National Academies of Sciences,
Engineering, and Medicine recommendations.
166
This
integration of strategic research and infrastructure
planning will enhance the oversight, prioritization, and
delivery of facilities to meet the changing scientic
needs over time.
Public Health
Challenges Across
the Lifespan
Collaborative
Science
Minority Health
and Health
Disparities
Women’s Health
Data Science
CROSSCUTTING THEMES

33
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Public Health
Challenges Across
the Lifespan
Collaborative
Science
Minority Health
and Health
Disparities
Women’s Health
Data Science
racial and ethnic minorities and other disproportion-
ately affected populations. There is also a growing
societal recognition that racism and discrimination
extend beyond the behavior of individuals and are
embedded in social, institutional, organizational, and
governmental structures, processes, procedures,
and practices that limit opportunities and resources
to segments of the population.
167
NIH understands
that health research needs to routinely incorporate
constructs and measurement of structural racism or
discrimination across multiple domains and levels of
inuence if minority health is to be optimized, health
equity achieved, and health disparities eliminated.
168
Understanding why underrepresented groups
experience specic health outcomes is at the core
of minority health science. It is essential to identify
contributing factors to minority health conditions
independent of whether a health disparity exists or
is identied. Minority health research is the scientic
investigation of distinctive health characteristics and
attributes of minority racial and/or ethnic groups that
are usually underrepresented in biomedical research
to understand health outcomes in these populations
and develop interventions to reduce disparities in
health outcomes. The NIH Minority Health and Health
Disparities Strategic Plan
169
sets the direction and
goals for NIH research in this area. Several NIH ICs
and OD ofces have core missions to address the
health of underserved and underrepresented popu-
lations and to ensure they are adequately included in
all NIH research. In addition, NIH-wide strategic plans
identify efforts specic to the needs of underrepre-
sented populations to develop synergy and facilitate
collaborations across NIH.
170,171,172
Promoting the recruitment, retention, and advance-
ment of scientists from underserved groups will also
have a signicant inuence on workforce develop-
ment and will provide opportunities for individual
scientists to achieve their full potential, thereby
improving research on minority health and reducing
health disparities.
Enhancing Women’s
Health
Women’s health is a wide-
ranging topic that goes beyond
reproductive health to address
a broader spectrum of diseases
and conditions experienced by
women throughout their lifespan. To advance science
for the health of women, the Trans-NIH Strategic
Plan for Women’s Health Research
173
established
NIH priorities across the research continuum and
emphasized the importance of interdisciplinary
partnerships. The NIH policy on Sex as a Biological
Variable,
174
along with the expanded NIH Inclusion
Policy
175
that requires investigators to report Phase
III clinical trial results by sex or gender, race, and
ethnicity to ClinicalTrials.gov,
176
will build foundational
knowledge, accelerate translational research, and
ultimately enable women to receive evidence-based
interventions specic to their needs.
Promoting the recruitment, retention, and advance-
ment of women scientists will also have a signicant
inuence on workforce development, as well as
provide opportunities for individual scientists to
achieve their full potential, thereby improving research
on the health of women.
Addressing Public
Health Challenges
Across the Lifespan
NIH supports biomedical and
behavioral research applicable to
the full spectrum of public health
challenges and needs, such as
acute and chronic diseases, persistent and emerging
infectious diseases, cancers, substance use dis-
orders, disordered eating, Alzheimer’s disease and
related dementias, the health impacts of environmen-
tal exposures, and many more.
177
NIH research must
address the prevention, treatment, and management
of public health challenges; meet new challenges
with fundamental research; and be ready to mobilize
cutting-edge science in emergent situations.
Many public health challenges affect people of
various ages and populations differently. To promote
health across the lifespan, NIH efforts include target-
ed studies of specic age groups; studies of diseases
that are unique to, or more common in, certain age
groups; longitudinal cohort studies that follow the
health outcomes of groups of individuals over long
periods of time (including across generations); and
studies that examine how early exposures, adversity,
and positive experiences affect later health outcomes.
The critical issue of maternal mortality and mor-
bidity in the U.S. is one example of a public health
challenge that requires multifaceted approaches at
different points in the lifespan. Risks include not only
complications at the time of pregnancy, birth, and
Public Health
Challenges Across
the Lifespan
Collaborative
Science
Minority Health
and Health
Disparities
Women’s Health
Data Science

34
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
postpartum, but also cumulative and intergenerational
impacts and exposures.
In addition to these programmatic approaches, NIH
policies set the expectation that all supported studies
will be designed to include children and older adults
unless there is a scientic or ethical reason to exclude
them. This policy ensures that the scientic ndings
for a given disease or condition are applicable to all
those affected.
178
Promoting Collaborative
Science
Complex public health challenges
and scientic questions require
collaborative, team-driven research
involving experts working together
across multiple scientic elds,
resulting in innovations that exceed the capacity
of a single laboratory or discipline. NIH promotes
opportunities that bring together scientists and
clinicians and recognizes patients and research
participants as partners and collaborators to generate
outcomes that address the public health challenges
that communities face. NIH partners with a wide
array of other federal agencies, and domestic and
international organizations in the public and private
sectors to leverage their respective expertise and
translate NIH research ndings into new therapies,
technologies, and evidence-based practices for
improving health. For example, efforts to accelerate
COVID-19 diagnostics, therapeutic interventions, and
vaccine development are being conducted alongside
sister agencies within HHS and representatives from
academic, nonprot, and commercial organizations.
179
Scientic progress also benets from collaboration
across NIH ICs and OD ofces. These NIH collabora-
tions occur at every level of NIH operation, resulting
in innovative scientic programs that address a wide
range of health conditions. For example, the Pediatric
Research Consortium brings together staff from
across NIH to discuss issues in pediatric research
for a range of health conditions. NIH also cultivates
strategic partnerships across HHS to strengthen the
public health ecosystem. For example, NIH plays a
key role in the Department-wide implementation and
dissemination of the HHS Secretary’s evidence-based
initiative to combat opioid use disorder.
Leveraging Data
Science for Biomedical
Discovery
An immense amount of data is
generated throughout the research
enterprise, from fundamental
experiments using cells and model
organisms to human clinical studies and communi-
ty-level epidemiological research. The exponential
growth of data has resulted from the development
of advanced biomedical technologies and computa-
tional processing unavailable a decade ago, including
advanced AI and virtual reality technologies. These
transformative changes require innovative approach-
es and business practices to address opportunities
and challenges in data science. Storing, managing,
standardizing, analyzing, sharing, and disseminating
vast amounts of data are therefore critical priorities
for NIH.
The NIHStrategic Plan for Data Science
180
provides
a roadmap for modernizing and integrating the
NIHfunded biomedical data ecosystem, which com-
prises the universe of data infrastructure, resources,
tools, and workforce. Combining existing strengths
with new strategic partnerships, NIH works to ensure
that data resources are guided by the FAIR principles
(Figure 21).
181,182
Implementing the NIH Strategic Plan
for Data Science will enhance the scientic commu-
nity’s ability to address new challenges, maximize the
value of data generated, and accelerate discoveries
that lead to better health outcomes. Woven into this
plan is NIH’s commitment to rapid, open sharing
of data and greater harmonization of data science
efforts across research domains, while respecting
participant privacy, security of sensitive data, and
Tribal sovereignty with respect to data.
Public Health
Challenges Across
the Lifespan
Collaborative
Science
Minority Health
and Health
Disparities
Women’s Health
Data Science
Public Health
Challenges Across
the Lifespan
Collaborative
Science
Minority Health
and Health
Disparities
Women’s Health
Data Science

35
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Bold Predictions
In the previous iteration of the NIH-Wide Strategic
Plan, NIH set out 14 ambitious goals, or “Bold
Predictions,” for the next 5 years. These short-term
predictions were considered aspirational goals
for biomedical and behavioral research that were
potentially within reach, but by no means guaran-
teed outcomes. The 14 Bold Predictions were not
an exhaustive list of all of the potential avenues of
success for NIH but were designed to illustrate some
of the potential achievements in a wide range of
research elds that might be possible under NIH’s
stewardship. NIH has made signicant progress on
all 14 Bold Predictions, with four being fully realized
within the ambitious 5-year timeframe. Despite the
risks associated with making short-term predictions,
it is important that NIH continue to place high hopes
on the ability for NIH-supported research to push
the boundaries of innovation faster than ever before.
Below are some of the outcomes that NIH will strive
to deliver over the next 5 years.
1. The All of Us Research Program will reach its goal of 1 million diverse participants and will have gathered the
most diverse collection of data (e.g., deep phenotypic, -omic, EHR, digital health technology) on 1 million or more
participants of any research resource in the world.
2. The regular use of genomic information will have transitioned from boutique to mainstream in all clinical settings,
making genomic testing as routine as complete blood counts.
3.
Human studies on type 1 diabetes will assess the long-term survival and function of encapsulated human islets,
as well as their efficacy in preventing or delaying the onset of complications and increasing overall survival.
4. Incorporating novel genomics findings from clinical studies on congenital heart disease will help researchers
move toward precision therapy and personalized counseling, leading to improved outcomes and longevity for
affected childr
en and adults.
5. The high burden of heart disease in communities of color and rural areas will be reduced, especially for major
outcomes, such as maternal morbidity and mortality, hypertension, and heart failure.
6. A gene therapy for muscular dystrophy will restore the function of the mutated gene and improve patient
outcomes.
7. Gene-based therapies for SCD will be evaluated and refined in large-scale clinical trials, offering a cure to the
approximately 100,000 people in the U.S. and 20 million globally who suffer severe pain and premature death
fr
om this condition.
8. First-in-human clinical trials will demonstrate the ef
ficacy of iPSC-derived products.
9. Engineered biological cells and scaffolds will be successfully used to repair and replace tissue damaged by
chronic wounds or such disorders as osteoarthritis.
10. Insight will be gained into the ultimate ability to regenerate human limbs, using emerging technologies to activate
the body’s own growth pathways and processes.
11. Research on new approaches to cervical cancer screening will lead to the development of self-sampling for
women, with the potential to substantially reduce the incidence and mortality of this disease.
12. At least one novel, non-hormonal pharmacologic treatment for endometriosis will be identified and moved to
clinical trials.
13. The number of maternal deaths per year in the U.S. will be significantly decreased, particularly among Black and
American Indian or Alaska Native women, by implementing results of research studies focusing on links between
social determinants and biological risk factors.
14. Following PRGLAC Task Force findings that almost no data exist on medications in pregnant and lactating
women, label changes will be facilitated by results of clinical trials for at least three therapeutics specific to
(1) pr
egnant women and lactating women and (2) children.
15. NIH-wide research will lead to new implementation strategies for pre-exposure prophylaxis that will significantly
reduce the number of new HIV infections and to new longacting therapies to improve viral load suppression
among people with HIV to levels that prevent transmission.

36
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
16. At least one candidate universal influenza vaccine against groups 1 and 2 with 75 percent efficacy will be
submitted to the FDA for consideration.
17. NIH-supported researchers will develop a universal coronavirus vaccine.
18. By actively engaging with underserved populations to reduce disparities for COVID-19, r
esearchers will prevent
and curb the spr
ead of COVID-19 and save lives.
19. AI will reveal molecular signatures associated with the return to health after an acute illness (e.g.,COVID-19).
20. Biomarkers will guide the choice of the most ef
fective therapy for each individual rheumatoid arthritis patient.
21. NIH-supported research will lead to the development of a clinically actionable biomarker for pr
ecision psychiatry,
using neur
oimaging and/or additional physiological and psychological biomarkers.
22. Comprehensive atlases of cell types in the mouse and human brain will provide a deeper understanding of the
circuits underlying behavior and a foundation for understanding the circuits affected in complex human brain
disorders, including depression.
23. Invasive and noninvasive human brain r
ecording and stimulation technologies will enable new paradigms for
interventions in movement disorders and neuropsychiatric diseases, as well as the development of brain-
machine interfaces for sensory and motor neural prostheses.
24. Preventive appr
oaches targeting vascular risk factors will reduce the risk for dementia and promote healthy brain
aging.
25. At least one promising lifestyle intervention to prevent Alzheimer’
s disease and related dementias will be rigor-
ously demonstrated in the next 5 years.
26. The r
ole of cellular senescence in aging and disease will be clarified and translated into interventions to improve
health.
27. Infant survival will be optimized by synthesizing milk that captures all of the components and properties of
human milk, even individualizing it to the characteristics of the infant’s mother.
28. NIH research will discover how technology exposure and media use affect developmental trajectories, health and
educational outcomes, and parent–child interactions in childhood in the post-COVID-19 era.
29. NIH research will lead to optimized treatment for infants with Neonatal Opioid Withdrawal Syndrome.
30. NIH research will identify one promising intervention to mitigate risks of altered brain development trajectories
produced by exposure to alcohol and otherdrugs among adolescents.
31. Increasing evidence of the effectiveness of nonpharmacologic treatments for pain will transform the way pain is
managed and decrease the need for opioids and other medications.
32. Effective screening based on a person’s genetics, environmental exposures, and sociobehavioral factors will
significantly decrease the 9 million lives lost each year to global air pollution by identifying those who are most
vulnerable for early intervention.
33. NIH and NASA will spearhead the development of a space-based platform that will monitor species diversity and
predict geographic areas of climate concern.
34. The number of NIH R01 awards that support principal investigators from underr
epresented racial and ethnic
gr
oups will be increased by 50 percent, and the racial funding disparities gap for NIH R01 grants will be eliminat-
ed by fiscal year 2025.
35. New forms of scientific communications, such as preprints, will accelerate clinical research and shorten the
evidence-to-practice cycle.
Bold Predictions (continued)

37
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
1 https://www.nih.gov/about-nih/what-we-do/mission-goals.
2 https://www.nih.gov/about-nih/who-we-are/organization.
3 https://www.nih.gov/about-nih/what-we-do/budget.
4 https://report.nih.gov/nihdatabook/category/10.
5 https://grants.nih.gov/grants/peer-review.htm.
6 https://grants.nih.gov/grants/peerreview22713webv2.pdf.
7 https://grants.nih.gov/funding/index.htm.
8 https://irp.nih.gov/about-us/what-is-the-irp.
9 https://irp.nih.gov/nih-clinical-center.
10 https://clinicalcenter.nih.gov/ocmr/research-discoveries.html.
11 Collins FS. NIH Basics. Science, 2012; 337:503. PMID: 22859455.
12 Moses H 3rd, et al. JAMA, 2015; 313(2):174-89. PMID: 25585329.
13 https://www.genome.gov/Funded-Programs-Projects/ENCODE-Project-ENCyclopedia-Of-DNA-Elements.
14
https://www.genome.gov/Funded-Programs-Projects/ClinGen-Clinical-Genome-Resource.
15 https://www.genome.gov/Funded-Programs-Projects/Human-Genome-Reference-Program#faq.
16 https://commonfund.nih.gov/hmp.
17
Elovitz MA, et al. Nature Communications 2019;10(1):1305. PMID 30899005.
18
Gehrig JL, et al. Science 2019;365(6449):eaau4732. PMID: 31296738.
19 Wilbert SA, et al. Cell Rep. 2020;30:4003-15.e3. PMID: 32209464.
20 https://www.cancer.gov/about-nci/budget/plan/immune-system-and-cancer.
21 Hand TW. et al. Trends Endocrinol Metab 2016;27(12):831-43. PMID: 27623245.
22
https://abcdstudy.org/about/.
23
Paulus MP, et al. Neuroimage 2019;185:140-53. PMID: 30339913.
24 Fine JD et al. JAMA Psychiatry 2019;76(7):762-4. PMID: 30916716.
25 Cheng W, et al. Mol Psychiatry, 2020. PMID: 32015467
26 https://braininitiative.nih.gov.
27
https://braininitiative.nih.gov/brain-programs/cell-census-network-biccn.
28
https://commonfund.nih.gov/singlecell.
29 https://commonfund.nih.gov/hubmap.
30 https://acd.od.nih.gov/documents/presentations/12132019AI.pdf.
31 Peng Y, et al. Ophthalmology 2019;126(4):565-75. PMID: 30471319.
32
Keenan TD, et al. Ophthalmology 2019;126(11):1533-40. PMID: 31358385.
33
https://www.fda.gov/news-events/press-announcements/fda-permits-marketing-articial-intelligence-based-de-
vice-detect-certain-diabetes-related-eye.
34 https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health.
35 Walsh JJ, et al. Lancet Child Adolesc Health 2018;2(11):783-91. PMID: 30268792.
36
Trinh MH, et al. JAMA Pediatr 2019;174(1):71-8. PMID: 31764966.
37
https://www.niaid.nih.gov/diseases-conditions/infographic-hiv-vaccine.
38 https://www.niaid.nih.gov/diseases-conditions/coronaviruses-therapeutics-vaccines.
39 https://www.nih.gov/news-events/news-releases/statement-nih-barda-fda-emergency-use-authorization-moder-
na-covid-19-vaccine.
40
Regules JA, et al. N Engl J Med 2017;376(4):330-41. PMID: 25830322.
41
https://www.who.int/csr/resources/publications/ebola/ebola-ring-vaccination-results-12-april-2019.pdf?ua=1.
42 https://www.cdc.gov/u/about/burden/index.html.
43 https://www.niaid.nih.gov/diseases-conditions/universal-inuenza-vaccine-research.
44 https://www.niaid.nih.gov/news-events/nih-begins-rst-human-trial-universal-inuenza-vaccine-candidate.
45
https://www.cdc.gov/nchs/data/nvsr/nvsr69/nvsr69-13-508.pdf.
46 https://www.cdc.gov/nchs/data/hestat/suicide/rates_1999_2017.pdf.
47
Boudreaux ED, et al. Contemp. Clin. Trials 2013;36(1):14-24. PMID: 23707435.
48 https://www.nhlbi.nih.gov/science/framingham-heart-study-fhs.
49 https://www.nhlbi.nih.gov/science/systolic-blood-pressure-intervention-trial-sprint-study.
50
SPRINT Research Group. N Engl J Med 2015;373(22):2103-16. PMID: 26551272.
51 Whelton PK, et al. Hypertension 2018;71(6):1269-324. PMID: 29133354.
52
Bress AP, et al. Circulation 2017;135(17):1617-28. PMID: 28193605.
53 Wang C,et al.Nat Biomed Eng2018;2(9):687-95. PMID: 30906648.
References

38
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
54 https://allofus.nih.gov.
55 https://grants.nih.gov/grants/guide/pa-les/PAR-17-483.html.
56 https://orwh.od.nih.gov/sex-gender.
57 https://www.nih.gov/news-events/nih-research-matters/replacing-function-impaired-cystic-brosis-protein.
58 https://commonfund.nih.gov/hcscollaboratory.
59 https://pubmed.ncbi.nlm.nih.gov/29860917/.
60 https://www.cancer.gov/news-events/press-releases/2018/tailorx-breast-cancer-chemotherapy.
61 https://pubmed.ncbi.nlm.nih.gov/29385370/.
62 https://www.fda.gov/news-events/press-announcements/fda-approves-rst-automated-insulin-delivery-de-
vice-type-1-diabetes.
63 https://www.fda.gov/news-events/press-announcements/fda-authorizes-rst-interoperable-automated-insulin-dos-
ing-controller-designed-allow-more-choices.
64 Bekiari E, et al. BMJ 2018; 361:k1310. PMID: 29669716.
65 http://www.braininitiative.nih.gov.
66 https://www.nei.nih.gov/learn-about-eye-health/resources-for-health-educators/eye-health-data-and-statistics/age-re-
lated-macular-degeneration-amd-data-and-statistics.
67 Sharma R, et al. Sci Transl Med 2019;11(475):eaat5580. PMID: 30651323.
68 https://www.nih.gov/news-events/news-releases/nih-launches-rst-us-clinical-trial-patient-derived-stem-cell-therapy-
replace-dying-cells-retina.
69 https://ncats.nih.gov/tissuechip/about/operations.
70 https://www.nih.gov/news-events/news-releases/nih-funded-tissue-chips-rocket-international-space-station.
71 https://www.niaid.nih.gov/clinical-trials/laboratory-infectious-diseases.
72 Mulangu S, et al. N Engl J Med 2019;381(24):2293-303. PMID: 31774950.
73 Dahlhamer J, et al. MMWR Morb Mortal Wkly Rep 2018;67(36):1001-6. PMID: 30212442.
74 https://www.cdc.gov/nchs/products/databriefs/db394.htm.
75 https://heal.nih.gov/.
76 https://www.niaid.nih.gov/clinical-trials/pact.
77 https://fnih.org/what-we-do/programs/partnership-for-accelerating-cancer-therapies.
78 Kennedy LB, Salama AKS. CA Cancer J Clin 2020;70(2):86-104. PMID: 31944278.
79 https://www.cdc.gov/ncbddd/sicklecell/data.html.
80 https://www.nih.gov/news-events/news-releases/nih-researchers-create-new-viral-vector-improved-gene-therapy-
sickle-cell-disease.
81 https://scdic.rti.org/.
82 https://www.nhlbi.nih.gov/science/cure-sickle-cell-initiative.
83 https://grants.nih.gov/ngri.htm.
84 https://www.nlm.nih.gov/ep/GrantTrainInstitute.html.
85 https://orwh.od.nih.gov/career-development-education/building-interdisciplinary-research-careers-wom-
ens-health-bircwh.
86 https://www.nigms.nih.gov/training/careerdev/Pages/MOSAIC.aspx.
87 https://commonfund.nih.gov/diversity.
88 https://acd.od.nih.gov/documents/presentations/06132019Diversity.pdf.
89 https://dpcpsi.nih.gov/sites/default/les/CoC_Jan_2020_1115_FIRST_program_concept_clearance.pdf.
90 https://www.sciencemag.org/news/2020/01/nih-s-new-cluster-hiring-program-aims-help-schools-attract-diverse-fac-
ulty.
91 https://diversity.nih.gov/programs-partnerships/dsp.
92 https://womeninscience.nih.gov/.
93 https://www.c.nih.gov/Programs/Pages/infectious-disease.aspx.
94 https://commonfund.nih.gov/CryoEM.
95 https://heal.nih.gov/about/public-access-data.
96 https://dash.nichd.nih.gov/.
97 https://vizhub.healthdata.org/gbd-compare/.
98 https://seer.cancer.gov/.
99 https://www.nimhd.nih.gov/programs/extramural/research-centers/rcmi/index.html.
100 https://grants.nih.gov/grants/guide/rfa-les/RFA-MD-20-006.html.
101 https://ncats.nih.gov/ctsa.
102 https://grants.nih.gov/grants/guide/notice-les/NOT-TR-19-015.html.
103 https://grants.nih.gov/grants/guide/notice-les/NOT-TR-19-016.html.
104 https://ncats.nih.gov/ctsa/projects/RuralHealth.
105 https://echochildren.org/idea-states-pediatric-clinical-trials-network.
106 https://orip.nih.gov/construction-and-instruments/s10-instrumentation-programs.
107 https://commonfund.nih.gov/moleculartransducers/overview.
108 https://motrpac-data.org/.

39
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
109 https://www.ninr.nih.gov/newsandinformation/pressreleases/press-release-symptom-science-center.
110 https://www.hhs.gov/about/strategic-plan/index.html.
111 https://report.nih.gov/reports/strategic-plans.
112 https://grants.nih.gov/grants/peer-review.htm.
113 https://public.csr.nih.gov/StudySections/CSREnquire.
114 https://public.csr.nih.gov/ForReviewers/BecomeAReviewer/ECR.
115 https://projectreporter.nih.gov/.
116 https://report.nih.gov/nihdatabook/.
117 https://report.nih.gov/.
118 https://icite.od.nih.gov/.
119 https://federalreporter.nih.gov/.
120 https://gcn.com/articles/2018/12/03/nsf-blockchain.aspx.
121 https://smrb.od.nih.gov/documents/reports/VOBR SMRB__Report_2014.pdf.
122 https://www.congress.gov/bill/115th-congress/house-bill/4174.
123 https://www.nih.gov/news-events/news-releases.
124 https://directorsblog.nih.gov/.
125 https://www.nih.gov/about-nih/what-we-do/impact-nih-research/our-stories.
126 https://pubmed.ncbi.nlm.nih.gov/.
127 https://www.nlm.nih.gov/news/NLMAnnouncesNewPubMed_202002.html.
128 https://www.ncbi.nlm.nih.gov/pmc/.
129 https://www.semanticscholar.org/cord19.
130 https://icite.od.nih.gov/covid19/search/.
131 https://registry.opendata.aws/ncbi-covid-19/.
132 https://prevention.nih.gov/tobacco-regulatory-research.
133 https://pathstudyinfo.nih.gov/landing.
134 https://prevention.nih.gov/tobacco-regulatory-research/funded-research/funded-research-tobacco-centers-regulato-
ry-science.
135 https://www.iprcc.nih.gov/.
136 http://painmanagementcollaboratory.org/.
137 https://www.nichd.nih.gov/about/advisory/PRGLAC.
138 https://www.nih.gov/research-training/medical-research-initiatives/activ.
139 https://www.nih.gov/research-training/accelerating-medicines-partnership-amp.
140 https://www.nih.gov/news-events/news-releases/nih-public-private-partnership-advance-early-interventions-schizo-
phrenia.
141 https://cloud.nih.gov/.
142 https://www.afrehealth.org/.
143 https://www.c.nih.gov/Programs/Pages/african-association-health-professions.aspx.
144 https://www.c.nih.gov/Programs/Pages/health-professional-education-partnership-initiative-hepi.aspx.
145 https://h3africa.org/.
146 https://www.c.nih.gov/Funding/Pages/collaborations-gacd.aspx.
147 https://www.niehs.nih.gov/research/programs/disaster/index.cfm.
148 https://www.nih.gov/news-events/news-releases/nih-facilitates-rst-tribal-data-sharing-agreement-navajo-nation.
149 https://echochildren.org/nih-echo-and-the-navajo-nation-make-history-with-new-data-sharing-and-use-agreement/.
150 https://www.acd.od.nih.gov/working-groups/eprar.html.
151 https://grants.nih.gov/policy/clinical-trials.htm.
152 https://www.nih.gov/about-nih/who-we-are/nih-director/statements/statement-nal-nih-policy-data-manage-
ment-sharing.
153 https://grants.nih.gov/grants/guide/notice-les/NOT-OD-21-013.html.
154 https://www.acd.od.nih.gov/working-groups/sexual-harassment.html.
155 https://www.nih.gov/anti-sexual-harassment.
156 https://grants.nih.gov/grants/policy/harassment.htm#:~:text=Anti-Sexual.
157 https://grants.nih.gov/grants/guide/notice-les/NOT-OD-20-124.html.
158 https://diversity.nih.gov/building-evidence/harassment-survey.
159 https://grants.nih.gov/policy/natural-disasters.htm.
160 https://grants.nih.gov/policy/natural-disasters/corona-virus.htm.
161 https://grants.nih.gov/policy/protecting-innovation.htm.
162 https://nexus.od.nih.gov/all/2019/07/11/clarifying-long-standing-nih-policies-on-disclosing-other-support/.
163 https://www.nih.gov/about-nih/who-we-are/nih-director/statements/statement-protecting-integrity-us-biomedical-re-
search.
164 https://nexus.od.nih.gov/all/2020/07/08/addressing-foreign-interference-and-associated-risks-to-the-integrity-of-bio-
medical-research-and-how-you-can-help/.

40
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
165 https://nexus.od.nih.gov/all/2019/08/05/linking-orcid-identiers-to-era-proles-to-streamline-application-process-
es-and-to-enhance-tracking-of-career-outcomes/.
166 https://www.nap.edu/read/25483/.
167 https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-health/interventions-resources/dis-
crimination.
168 https://www.nimhd.nih.gov/about/overview/research-framework.html.
169 https://www.nimhd.nih.gov/about/overview/strategic-plan.html.
170 https://www.nimhd.nih.gov/about/overview/strategic-plan.html.
171 https://dpcpsi.nih.gov/le/sgm-strategic-plan-2021-2025.
172 https://orwh.od.nih.gov/sites/orwh/les/docs/ORWH_Strategic_Plan_2019_02_21_19_V2_508C.pdf.
173 https://orwh.od.nih.gov/about/trans-nih-strategic-plan-womens-health-research.
174 https://grants.nih.gov/grants/guide/notice-les/NOT-OD-15-102.html.
175 https://grants.nih.gov/grants/guide/notice-les/NOT-OD-18-014.html.
176 https://clinicaltrials.gov/.
177 https://report.nih.gov/categorical_spending.aspx.
178 https://grants.nih.gov/policy/inclusion/lifespan.htm.
179 https://covid19.nih.gov/nih-strategic-response-covid-19.
180 https://datascience.nih.gov/strategicplan.
181 https://www.go-fair.org/fair-principles/.
182 Wilkinson MD, et al. Sci. Data 2016;3:19. PMID:26978244.


42
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Appendix I: NIH Statutory Authority
Begun as a one-room Laboratory of Hygiene in 1887
(renamed the Hygienic Library in 1891), the National
Institutes of Health (NIH) today is one of the world’s
foremost medical research centers. An agency of
the U.S. Department of Health and Human Services,
NIH is the federal focal point for health research. The
Statutory Authority granted to NIH generally appears
in Title IV of the Public Health Service (PHS) Act,
42 U.S.C. 281 et seq. This authority has a long
history with many revisions and additions granted
by new legislation over the years. Below are several
highlights from the legislative history of NIH.
The Ransdell Act, P.L. 71–251
On May 26, 1930, the Ransdell Act reorganized,
expanded, and redesignated the Hygienic Laboratory
of the Public Health Service as the National Institute
of Health (NIH), authorizing $750,000 for construction
of two buildings for NIH and creating a system of
fellowships.
The Public Health Service Act,
P.L. 78–410
On July 1, 1944, the PHS Act (P.L. 78—410) consol-
idated and revised existing public health legislation,
dividing the PHS into the Ofce of the Surgeon
General, the Bureau of Medical Services, the Bureau
of State Services, and NIH. The PHS Act gave NIH
the legislative basis for its postwar program, with
general authority to conduct and support research
into the diseases and impairments of man, authorized
research projects and fellowships, and made the
National Cancer Institute a division of NIH.
The National Heart Act of 1948,
P.L. 80–655
On June 16, 1948, the National Heart Act of 1948
amended the PHS Act and authorized the National
Heart Institute and changed the name of the National
Institute of Health to National Institutes of Health.
The Public Health Improvement
Act, P.L. 106–505
On November 13, 2000, the Public Health Improve-
ment Act amended the PHS Act and provided new
authorities to NIH and other PHS agencies and
placed ongoing activities or programs in statute.
The National Institutes of Health
Reform Act of 2006, P.L. 109–482
On January 15, 2007, the NIH Reform Act of 2006
afrmed the importance of NIH and its vital role in
advancing biomedical research to improve the
health of the nation. The law reinforced how NIH’s
27 Institutes and Centers, along with various other
NIH components, work together on the nation’s
largest medical research enterprise. Among its provi-
sions, the NIH Reform Act revised Title IV of the PHS
Act to create the Division of Program Coordination,
Planning, and Strategic Initiatives, to be supported by
a Common Fund.
The 21st Century Cures Act,
P.L. 114–255
On December 13, 2016, the 21st Century Cures Act
provided NIH with critical tools and resources to
advance biomedical research across the spectrum,
from foundational basic research studies to advanced
clinical trials of promising new therapies. The Cures
Act provided NIH with important new authorities that
could be employed to hasten its mission to improve
the health of Americans.

43
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Appendix II: NIH Organizational Chart
National Eye Institute National Heart, Lung,
and Blood Institute
National Institutes of Health
Office of the Director
National Human
Genome Research
Institute
National Cancer
Institute
National Institute on
Alcohol Abuse and
Alcoholism
National Institute of
Allergy and Infectious
Diseases
National Institute of
Arthritis and
Musculoskeltal and
Skin Diseases
National Institute on
Aging
Eunice Kennedy Shriver
National Institute of
Child Health and
Human Development
National Institute on
Deafness and Other
Communication
Disorders
National Institute of
Dental and Craniofacial
Research
National Institute of
Biomedical Imaging
and Bioengineering
National Institute on
Drug Abuse
National Institute of
Environmental Health
Sciences
National Institute of
General Medical
Sciences
National Institute of
Diabetes and
Digestive and Kidney
Diseases
National Institute on
Minority Health and
Health Disparities
National Institute of
Neurological
Disorders and Stroke
National Institute of
Nursing Research
National Institute of
Mental Health
John E. Fogarty
International Center
for Advanced Study in
the Health Sciences
National Center for
Advancing
Translational Sciences
National Center for
Complementary and
Integrative Health
National Library of
Medicine
Center for
Information
Technology
Center for Scientific
Review
Clinical Center

44
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Appendix III: Strategic Planning Process
The National Institutes of Health (NIH)-Wide Strategic
Plan outlines NIH’s research priorities and how these
priorities align with the agency’s mission and goals
in an evolving research landscape. It represents one
facet of NIH’s stewardship of federal dollars and
contributes to maintaining transparency and account-
ability to its many stakeholders.
Biomedical and behavioral science is progressing
rapidly. To keep pace and capitalize on scientic
advances while addressing evolving public health
needs, NIH updates the NIH-Wide Strategic Plan
every 5 years. The NIH-Wide Strategic Plan is a
living document, with each iteration building off the
foundation of the previous plan and aligning with
the agency’s near-, mid-, and long-range goals.
This latest iteration of the NIH-Wide Strategic Plan,
covering scal years 2021–2025, retains many of
the core elements of the NIH-Wide Strategic Plan
for scal years 2016–2020. However, the Strategic
Plan has been revised, updated, and expanded in
response to the many discoveries and changes in
the eld made during the past 5 years. As part of this
process, the Framework around which the Strategic
Plan is organized has also been revised.
In September 2019, NIH began updating the NIH-
Wide Strategic Plan to cover scal years 2021–2025.
The goal was to follow a process that was transpar-
ent, focused on science and good stewardship of
research, guided by evidence, and informed by NIH’s
many stakeholders.
The strategic planning process entailed four phases:
(1) pre-planning, (2) gathering internal input and
development of the Strategic Plan framework,
(3) gathering input from external stakeholders, and
(4)drafting and publishing the Strategic Plan. The
following are key activities undertaken during these
four phases.
Pre-Planning
The NIH Division of Program Coordination, Planning,
and Strategic Initiatives (DPCPSI) within the Ofce of
the Director (OD), coordinated the development of the
NIH-Wide Strategic Plan for scal years 2021–2025.
At the initiation of this process, DPCPSI developed
a timeline for the strategic planning process and
established an internal NIH-Wide Strategic Plan
Working Group, composed of staff from each Institute
and Center (IC) and OD Ofce, representing the
range of NIH’s activities and research portfolio. The
rst Working Group meeting was held at the end of
September 2019.
Gathering Internal Input and
Development of the Strategic Plan
Framework
From October to December 2019, the Working Group
met biweekly to develop the Framework for the
Strategic Plan, which outlines, at a high level, NIH’s
priorities for biomedical and behavioral research
that will be addressed over the next ve years. The
Framework of the NIH-Wide Strategic Plan for scal
years 2016-2020 was used as a starting point, and
the Framework for the new Strategic Plan evolved
over several meetings. The proposed framework was
reviewed by the IC Directors at the end of October,
the Advisory Committee to the NIH Director in
December, and the DPCPSI Council of Councils in
January 2020. The nal Framework was approved by
NIH Leadership.
In parallel with development of the Framework, ICs
and OD Ofces were asked to provide information on
biomedical and behavioral research advances that
have been made under the NIH-Wide Strategic Plan
for scal years 2016–2020 and proposed activities
that will be conducted during the next 5 years. The
Working Group reviewed the content provided and,
through an iterative process of voting and delibera-
tion, proposed for NIH Leadership’s approval the top
NIH-wide accomplishments and priorities for each
section of the Framework.
Gathering Input from External
Stakeholders
NIH recognizes that input from external stakehold-
ers—including members of the scientic and health
care communities, professional societies, advocacy
organizations, industry, other federal agencies, and

45
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
the general public—provides valuable insight to be
considered during its strategic planning process.
To solicit comments on the proposed Framework
from external stakeholders, the Working Group
developed a Request for Information (RFI) in the NIH
Guide (NOT-OD-20-064
1
) and the Federal Register
(FRN 2020-02919
2
), which was advertised broadly.
Comments were accepted online from February 12,
2020, to April 1, 2020. NIH received 160 responses
to the RFI from external stakeholders. In addition,
NIH hosted two webinars on March 9 and 16, 2020,
to provide the opportunity for stakeholders to ask
questions on the Strategic Plan development process
and comment on the Framework. A summary of RFI
responses, the webinar slides, and transcript, will
be made available on the NIH-Wide Strategic plan
webpage.
3
Drafting and Publishing the
Strategic Plan
In January 2020, the Working Group began drafting
the Strategic Plan based on the Framework and the
prioritized content approved by NIH Leadership. As
it became available from the RFI and webinars, the
Working Group reviewed public feedback on the
Framework and adjusted the draft Strategic Plan in
response to this input.
Finalizing and Publishing the
Strategic Plan
The draft Strategic Plan was nalized through an iter-
ative review process with NIH Leadership. Beginning
in July 2020, the draft Strategic Plan was reviewed
by IC and OD Ofce Directors, and subsequently by
the NIH Director and Deputy Director. It was then
reviewed by the DPCPSI Council of Councils and the
Advisory Committee to the NIH Director. Following
nal review and approval by the NIH Director and
Deputy Director, and subsequent sign off by the U.S.
Department of Health and Human Services, the nal
version of the NIH-Wide Strategic Plan for scal years
2021–2025 was posted publicly on NIH’s website and
widely disseminated to NIH stakeholders.
1 https://grants.nih.gov/grants/guide/notice-les/NOT-OD-20-064.html
2 https://www.federalregister.gov/documents/2020/02/13/2020-02919/request-for-information-r-inviting-comments-
and-suggestions-on-a-framework-for-the-nih-wide
3 https://www.nih.gov/about-nih/nih-wide-strategic-plan
Endnotes

46
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Appendix IV: NIH Common Fund Strategic
Plan Report
About the NIH Common Fund
The National Institutes of Health (NIH) Common
Fund
1
programs represent time-limited, strategic
investments in biomedical and behavioral research
(collectively referred to as biomedical research
in the remainder of this appendix) designed to
achieve high-impact goals and catalyze discovery.
Approximately 30 multidisciplinary scientic programs
are supported by the NIH Common Fund, spanning
NIH’s mission and addressing challenges and oppor-
tunities that are of high priority for NIH as a whole.
These bold scientic programs often accelerate
emerging science, enhance the biomedical research
workforce, remove research roadblocks, or support
high-risk, high-reward science. NIH Common Fund
programs frequently produce resources—such as
datasets, tools, technologies, or methods—that are
designed to spur subsequent biomedical advances
often not possible otherwise. The work supported by
the NIH Common Fund is inherently risky, but this risk
is embraced because of the potential for transfor-
mative impact in advancing science and, ultimately,
improving human health.
The origins of the NIH Common Fund lie in the NIH
Roadmap for Medical Research, which was launched
in 2004. The NIH Reform Act of 2006 created the
NIH Common Fund as a source of support for these
transformative, NIH-wide programs within the NIH
Ofce of the Director (OD). This established a novel
approach to support crosscutting, NIH-wide pro-
grams in areas of emerging scientic opportunities,
rising public health challenges, and knowledge gaps
that deserved special emphasis or would otherwise
benet from strategic planning and coordination. The
Act also mandated an emphasis on goals and mile-
stones in NIH Common Fund programs and directed
NIH to encourage participation by early-career
researchers.
The Ofce of Strategic Coordination (OSC) within
the NIH Division of Program Coordination, Planning,
and Strategic Initiatives (DPCPSI) is responsible for
managing the NIH Common Fund. OSC coordinates
teams across NIH who collectively plan, implement,
and oversee each program to ensure broad impact.
Individual awards supported through the NIH
Common Fund are administered in partnership with
NIH Institutes and Centers (ICs).
About the NIH Common Fund
Strategic Plan Report
The Public Health Service Act requires, as part of the
NIH-Wide Strategic Plan, that the NIH Director submit
a report to Congress containing a strategic plan for
funding research “that represents important areas
of emerging scientic opportunities, rising public
health challenges, or knowledge gaps that deserve
special emphasis and would benet from conducting
or supporting additional research that involves
collaboration between two or morenational research
institutesornational centers,or would otherwise
benet from strategic coordination and planning”
through the NIH Common Fund (42 U.S.C. §282a(c)
(1)(C); 282(b)(7)(A)(i)).
NIH Common Fund Program
Lifecycle
The congressional mandate to support goal- and
milestone-driven programs underlies a critical feature
of NIH Common Fund programs: Each program
establishes high-impact goals that are expected to be
achieved within a maximum of 10 years. This program
enables new needs or opportunities to be supported
as they emerge. The NIH Common Fund supports
research programs that transcend the scientic
boundaries of the individual ICs, are synergistic with
current IC-funded research, and would benet from
limited-term NIH Common Fund investment. These
programs are identied through a strategic planning
process that includes input from many stakeholders
who rst identify broad scientic areas that are prior-
ities for NIH as a whole and subsequently establish a
focused strategy for scientic initiatives that will cat-
alyze progress within that area. This process ensures
that the programs provide maximum utility to the

47
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Figure 29. Lifecycle of NIH Common Fund Programs
“Common Fund Program Lifecycle”: Infographic. Note that not all programs follow this exact timeline.
Credit: NIH Common Fund.
Program Transition
(after ~5–10 years)
Program Implementation
(~5–10 years)
Common Fund Program Lifecycle
Strategic Planning
(~15 months)
Program
Transition
*Years are approximate; Common Fund programs are supported for a maximum of 10 years.
Program
Transition
Phase 2
Strategic Planning:
Refinement
(for the second
stage of
the program)
Phase 1
Strategic Planning:
Identification
of broad
program areas
Phase 2
Strategic Planning:
Refinement
(for the first stage
of the program)
Stage 1
Program
Implementation
(Years 1–5*)
Stage 2
Program
Implementation
(Years 6–10*)
Ongoing program evaluation enables optimization throughout the lifetime of the program.
Evaluation
broad biomedical community and that they address
major roadblocks to research progress. At the com-
pletion of each program, the tools, technologies, and
data produced by the program are taken up and used
by the community at large, and the infrastructure that
the NIH Common Fund has built transitions to other
sources of support. The lifecycle of a NIH Common
Fund program is shown in Figure 29.
NIH Common Fund strategic planning is a two-phase
process. Phase 1 of strategic planning identies
broad areas that are high priorities for NIH and for
which transformational progress can be envisioned.
Phase 2 of strategic planning involves analysis
of the scientic landscape within a given eld to
identify the specic challenges and opportunities for
progress. Programmatic goals are established, with
a series of funding initiatives collectively designed to
achieve those goals. The strategic planning process
is described in more detail in the next section, “NIH
Common Fund Strategic Planning Process.”
Following strategic planning and selection of new
program areas, research projects addressing goals
and milestones identied during the planning process
are supported through a variety of funding mecha-
nisms. Awards are often implemented as partnerships
among the many scientic investigators supported by
a program and expert NIH staff, collaboratively work-
ing together to achieve dened goals. NIH Common
Fund programs are actively managed to ensure that
the output of each program is maximally useful to
the broader scientic community. Assessment of the
utility of the program to the community is emphasized
and is achieved through a variety of evaluative
processes.

48
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Figure 30. NIH Common Fund Data
Ecosystem
NIH Common Fund programs are intended to provide
resources that accelerate discovery across many differ-
ent biomedical research fields. Often these resources
include large datasets and associated digital tools
needed to mine and analyze the data. To maximize
impact, these datasets and tools must be leveraged
by researchers from different disciplines, using varying
expertise in bioinformatics and large-scale data
analysis. Additionally, these datasets must be usable
together across interoperable platforms. However,
current approaches to data storage, management,
and analysis mean that data are often not findable,
accessible, interoperable, and reusable (FAIR).
To address this challenge, the NIH Common Fund is
supporting the NIH Common Fund Data Ecosystem
(CFDE), an ongoing investment in data management
infrastructure that will support past, current, and future
NIH Common Fund datasets.
The CFDE includes several integrated efforts:
• CFDE Coordinating Center—The Coordinating
Center will manage and organize CFDE activities,
engage with participating NIH Common Fund pro-
grams, connect with user communities, support
training, develop tools and standards, and provide
technical expertise.
• Participating NIH Common Fund Data
Coordinating Centers—These Centers will work
with the CFDE Coordinating Center to understand
its program’s unique requirements for data storage
and analysis, adopt/adapt guidelines and best
practices, share resources and tools, establish
and enable use cases for cross-data analyses, and
provide training.
• Leveraging NIH-wide cloud service pro-
vider partnerships—Using the Science and
Technology Research Infrastructure for Discovery,
Experimentation, and Sustainability (STRIDES) will
ensure that data are onboarded to the cloud in a
consistent manner and provide favorable pricing
for cloud data storage and use.
Ultimately, the CFDE is intended to amplify the impact
of many NIH Common Fund programs by enabling
researchers to interrogate multiple disparate datasets
and thereby make new kinds of scientific discoveries
that were not possible before.
Evaluation is an ongoing activity throughout the
lifecycle of the program and includes both formal
and informal evaluative activities. Informal evaluation
involves convening grantees and NIH-wide teams to
review progress, discuss new challenges, and devel-
op strategies to adapt as part of routine program
management. It also involves gathering input from
external consultants and using their input, together
with internal analysis, to help guide the implementa-
tion of the program. Formal evaluations involve the
development of baseline data for new programs and
the development of multiple metrics of outcomes.
The utility of data, resources, technologies, and other
program outputs is assessed through surveys, expert
opinion, and the analysis of bibliometric data, such
as citation analyses. Challenges and opportunities to
strengthen each program are considered continuous-
ly, but this assessment is also done systematically for
every program on an annual basis. This management
process ensures that the programs stay on track
toward their stated goals while also allowing adjust-
ments to ensure that the impact of each program is
maximized.
Another ongoing activity for the NIH Common Fund
is the support of infrastructure designed to maximize
the accessibility and utility of NIH Common Fund
datasets and digital resources. To this end, the NIH
Common Fund Data Ecosystem (CFDE)
2
is working
to ensure all NIH Common Fund datasets are nd-
able, accessible, interoperable, and reusable (FAIR),
providing training for users to operate on data in a
cloud environment and ensuring that NIH Common
Fund data continue to be available after individual
programs are completed. For more information on the
CFDE, see Figure 30.
The nal stage of NIH Common Fund support
involves the transition of mature programs to other
sources of support or use within the scientic com-
munity.
Although represented as sequential activities, the
management of each program has an iterative
nature. Plans for implementation and transition are
considered early in the lifecycle but may be adapted
in response to the science. Similarly, scientic
progress may demand changes in the strategic plan,
as new opportunities or challenges are identied.
Nevertheless, early consideration of implementation
and transition ensures that program goals and
milestones are established to meet the needs
identied during strategic planning and to provide a
sustainable model for continued use by the scientic
community when NIH Common Fund support for a
program has ended.

49
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
NIH Common Fund Strategic
Planning Process
Strategic planning for the NIH Common Fund
involves the identication of NIH-wide challenges and
opportunities that meet NIH Common Fund program
criteria
3
(Figure 31). It is designed to be exible from
year to year to adapt to emerging opportunities, the
changing needs of the scientic community, and
the availability of funds. Broad topics identied in
Phase 1 are rened into well-dened programs and
initiatives in Phase 2.
Phase 1 identies broad scientic needs and
opportunities, focusing on the greatest challenges
to research discovery and translation, as well as
on the most promising emerging opportunities
to catalyze research across a variety of scientic
disciplines and disease conditions. Although specic
Phase 1 activities vary, ideas may be gathered
through meetings with external scientic experts,
solicitation of ideas from ICs, discussions with
NIH Leadership and Advisory Committees, and
engagement with the broader scientic community.
To effectively evaluate the responsiveness of the
proposed idea to NIH Common Fund criteria, as well
as the potential impact of the program, the following
questions are typically posed:
What is the greatest opportunity in biomedical
research today? How can this opportunity be
realized?
Why is now the right time for this idea (i.e., why
is this idea timely)?
What would be the goals of the program, and
what initiatives or activities are envisioned to
achieve these goals?
Generally, Phase 1 strategic planning activities gen-
erate many more ideas than can be supported. Ideas
are prioritized by the NIH Director, with input from
the OSC, DPCPSI, and Principal Deputy Directors. IC
Directors may also provide input to the NIH Director
on prioritization of concepts.A small subset of
prioritized ideas then moves into Phase 2 planning.
Phase 2 renes the prioritized set of broad ideas
identied in Phase 1 into specic, well-dened
initiatives. An NIH-wide Working Group representing
a broad range of interested scientic communities is
formed to continue the planning process and, if the
program is approved, lead program implementation.
Phase 2 strategic planning also occurs before
decisions are made to provide a second stage of
support for existing programs. OSC assesses the
progress of NIH Common Fund programs at the end
of the rst stage of funding to determine whether a
second stage of funding (up to a limit of 10 years
total) is necessary to reap maximum benet from the
program. The Phase 2 renement process includes
analysis of NIH and external scientic research
portfolios (Figure 32), solicitation of input from
subject-matter experts, and input from IC Directors.
During Phase 2 planning, the DPCPSI Council of
Councils (CoC)
4
provides input about whether the
proposed idea addresses the NIH Common Fund
criteria and, if so, whether the proposed program
initiatives are likely to achieve the program goals
and produce the highest possible impact. When the
concept for a potential new program is cleared by the
CoC, the Working Group develops a program propos-
al that clearly describes scientic needs, gaps, and
opportunities; goals and milestones of the proposed
program; description of program management;
and a budget for all years of the program. Program
proposals are presented to the NIH Director for a nal
decision about program approval.
Figure 31. NIH Common Fund Program
Criteria
Transformative: Programs must have high potential to
dramatically affect biomedical research.
Catalytic: Programs must achieve a defined set of
high-impact goals within a defined period of time.
Synergistic: Outcomes must synergistically promote
and advance individual missions of ICs to benefit
health.
Crosscutting: Program areas must cut across missions
of multiple ICs, be relevant to multiple diseases or
conditions, and require a coordinated approach
across NIH.
Unique: Programs must be something no other entity
is likely or able to do.

50
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Figure 32. Portfolio Analysis: Focusing Scope and Identifying Opportunities
Portfolio analysis occurs during Phase 2 of the strategic planning process. It is a vital part of strategic planning that
provides critical information concerning ongoing efforts in areas being considered as potential NIH Common Fund
programs. Portfolio analysis helps identify specific areas where strategic investment by the NIH Common Fund could
support unique and potentially transformative research.
The Somatic Cell Genome Editing (SCGE) program, launched in fiscal year 2018, included a robust portfolio analysis
during the planning process to identify specific activities in support of the program’s overall goal to advance therapeutic
use of precision genome editing approaches to treat or cure numerous diseases caused by genetic mutations. With the
discovery of CRISPR and similar tools that can precisely change genetic sequences, this field experienced an explosion
of interest. However, remaining gaps in research investment were holding back the translation of genome editing
approaches into the clinic, especially for rare or uncommon diseases. Information on private-sector and other govern-
ment agency investment was provided by consultation with experts, complementing the SCGE portfolio analysis that
assessed NIH investment in genome editing tools and technologies in fiscal year 2016. This analysis identified critical
gap areas, including gene editing reporter systems and in vitro models for testing efficacy and safety. Additionally, the
analysis demonstrated a pressing need to develop new genome editing tools that were less likely to produce adverse
or off-target effects. Furthermore, the analysis revealed that current investment in genome editing delivery vehicles
was highly focused on a single viral vector (adeno-associated virus, or AAV) with inherent limitations. Other delivery
systems—such as nanoparticles, alternative viruses, ribonucleoprotein complexes, and exosomes—were largely
overlooked, despite representing potentially transformative approaches to overcoming limitations associated with AAVs.
The results of this portfolio analysis, combined with expert input, identified areas of scientific opportunity that became
the basis of the SCGE program initiatives. These initiatives include (1) developing animal models for testing genome
editing tools; (2) generating assays and models to test the efficacy and safety of genome editing tools; (3) improving
genome editing delivery systems—including a wide range of delivery systems beyond AAVs—to target specific cells
and tissues; (4) expanding the number and types of genome editing complexes; and (5) distributing the knowledge and
resources developed through this program to the scientific community.
A follow-up analysis conducted in 2020 confirmed that the SCGE program is stimulating research in gap areas identified
in the baseline portfolio analysis. This analysis showed that the SCGE program is filling an important niche by support-
ing research on exploring the use of exosomes, nanoparticles, and ribonucleoproteins as delivery vehicles. The analysis
also revealed that the SCGE program is developing genome editing tools that target a wide range of tissues and organs,
including one organ system (the gastrointestinal tract) that is not targeted by any other NIH-supported genome editing
projects, as well as other several tissues or organs for which SCGE projects are the only ones using non-AAV delivery
systems for targeted delivery.
Strategic Planning Activities Since
2015
Prior to the passage of the 21
st
Century Cures Act,
5
the NIH Common Fund developed a biennial strategic
planning report. With the passage of this Act, the
NIH Common Fund Strategic Planning Report is
now included within the NIH-Wide Strategic Plan.
Described here are the strategic planning activities
that have taken place since the last NIH Common
Fund Strategic Planning Report in 2015.
6
Strategic Planning 2015–2016
In 2015, OSC held the “Innovate to Accelerate” 2-day
strategic planning workshop that brought together
more than 20 innovative thinkers representing diverse
areas of expertise to brainstorm ideas for potential
new NIH Common Fund programs beginning in scal
year 2018 or later. Following the workshop, all ideas
that emerged from the workshop were posted in an
online discussion forum, where an additional cohort
of approximately 300 selected scientic experts were
invited to view ideas, provide comments and sugges-
tions, and submit one original idea for inclusion in the
online discussion. All ideas and associated discus-
sions were considered along with ideas submitted by
IC Directors.
From these activities, two ideas were prioritized for
further planning and ultimately were launched in scal
year2018:
• Human BioMolecular Atlas Program (HuBMAP)
7
(Figure 33)—The planning process that led to
the HuBMAP program identied understanding
human physiology and disease at the level of
individual cells as a challenge that we now have
the technologies to address. Because the cell
is the fundamental unit of the human body, an
understanding of normal and disease process-
es at this level is anticipated to lead to more
specic and effective therapies. In recent years,
technologies that enable the analysis of single

51
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Figure 33. Human BioMolecular Atlas Program
The Human BioMolecular Atlas Program is a collabo-
rative effort to develop an open and global platform to
map healthy cells in the human body.
Credit: NIH Common Fund.
Figure 34. Illuminating the Druggable Genome
Program
The goal of the Illuminating the Druggable Genome
program is to compile data about the uncharacterized
proteins within the four protein classes that are most
frequently targeted by drugs.
Credit: NIH Common Fund.
cells within the context of the tissues have made
the goals of HuBMAP feasible. However, this
challenge is enormous, given that the human body
has approximately 37 trillion cells. HuBMAP is
developing an open and global platform to map
healthy cells in the human body, coordinating
with other international efforts. Capitalizing in part
upon the foundation laid by the NIH Common
Fund’s Single-Cell Analysis Program,
8
HuBMAP is
building the framework needed to construct cell
atlases, tools, and resources to understand the
function of and relationship among all the cells in
the human body. This understanding is expected
to lead to new insights into human health, growth,
development, aging, and disease.
• Transformative High Resolution Cryo-Electron
Microscopy (CryoEM)
9
—Improvements in cryoEM
technologies and new computational methods
to analyze the associated data have created a
transformative opportunity in structural biology.
With these new methods, investigators can
analyze protein structures more easily than ever
before, providing the basis for smart drug design
and fundamental biological insights. However,
the high cost of required equipment and limited
workforce procient in this technology represent
a substantial challenge. The CryoEM program
addresses this challenge. It is broadening
access to high-resolution cryoEM for biomedical
researchers by creating national service centers
and cultivating a skilled cryoEM workforce by
developing and implementing cryoEM training
materials. By expanding access and training for
cryoEM, this program aims to enable research and
accelerate development of drugs and vaccines to
combat many diseases and conditions.
In addition to launching new programs, several exist-
ing NIH Common Fund programs underwent planning
for a second stage of support that began in scal
year 2018. These programs are described below:
• Illuminating the Druggable Genome (IDG)
10
(Figure 34)—Most drugs target proteins within
four families: G protein–coupled receptors, nuclear
receptors, ion channels, and protein kinases.
However, only a small number of proteins within
each of these families are well studied, and these
proteins typically are present in many cells
throughout the body. Therefore, drugs that target
these proteins may cause widespread adverse
effects in cells and tissues that are not affected
by disease. However, the lesser known members
of these protein families may be present in fewer
tissues and thus have potential as specic drug
targets leading to fewer side effects. Technological
advances in genomics, protein characterization,
and computational methods provide an opportuni-
ty to identify and study large numbers of unknown
proteins. IDG originally launched a pilot stage in
scal year 2014 to compile data about the unchar-
acterized proteins within the four protein classes
that are most frequently targeted by drugs. In the
second stage, implementation, IDG is capitalizing
on the information gathered and technologies
developed in the pilot to further elucidate the

52
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Figure 35. Undiagnosed Diseases Network
The Undiagnosed Diseases Network is a research
study to improve the level of diagnosis of rare and
undiagnosed conditions.
Credit: NIH Common Fund.
function of uncharacterized proteins within
three key families: G protein–coupled receptors,
ion channels, and protein kinases. IDG is also
expanding the informatics tools developed in the
pilot stage and disseminating the IDG-generated
resources to the biomedical research community.
• Metabolomics
11
—Chemical reactions in the body
produce small molecules, called metabolites, that
can provide important information about diet,
environmental exposures, and drug metabolism.
The study of all of the metabolites in a given
sample, or metabolomics, therefore provides a
powerful tool for researchers and clinicians to
understand an individual’s current physiological
state and possibly to develop personalized
diagnoses and treatment approaches. The NIH
Common Fund’s Metabolomics program was
established to support broader use of metabolom-
ic analysis in basic research and in the clinic. The
rst stage of the Metabolomics program contrib-
uted to wider use of metabolomic approaches in
the biomedical research community and enhanced
researchers’ ability to conduct metabolic analyses.
In the second stage, the Metabolomics program
aims to enhance metabolomics data sharing;
develop novel tools to facilitate data analysis; and
generate standards, guidelines, and resources to
enable metabolomics research.
• Undiagnosed Diseases Network (UDN)
12
(Figure 35)—Rare diseases collectively affect
approximately 25 million Americans,
13
many of
whom face a long and frustrating process to
arrive at a diagnosis. The NIH Intramural Research
Program launched the Undiagnosed Diseases
Program (UDP) in 2008 with the goal of diagnos-
ing, understanding, and treating rare disorders.
This program leveraged revolutionary genomic
sequencing technologies to aid in the diagnosis of
rare diseases and developed a robust interdisci-
plinary approach to disease diagnosis that proved
successful. However, the overwhelming patient
need far exceeded the capacity of the UDP. In
2013, the NIH Common Fund launched UDN with
the goal of expanding the proven approach of
UDP to academic health centers across the coun-
ty, working through challenges associated with
implementing this approach in different clinical
and economic models. UDN promotes the use of
genomic data in disease diagnosis and engages
basic researchers to uncover underlying disease
mechanisms so that treatments can be identied.
UDN accepted 601 participants undiagnosed by
traditional medical practices in the rst 20 months
of operation. Of those who completed their UDN
evaluation during this time, 35 percent were given
a diagnosis. Many of these diagnoses were rare
genetic diseases, including 31 previously unknown
syndromes. In the second stage, UDN is focusing
on forming a sustainable national resource to
diagnose both rare and new diseases, advancing
laboratory and clinical research, enhancing global
coordination and collaboration among laboratory
and clinical researchers, and sharing resulting
data and approaches throughout the scientic and
clinical communities.
Strategic Planning 2016–2017
Anticipated budget limitations led to a scaled-down
strategic planning process in 2016–2017, focused on
two existing NIH Common Fund programs requesting
a second stage of support in scal year 2019:
• Diversity Program Consortium (DPC): Enhancing
the Diversity of the NIH-Funded Workforce
14
(Figure 36)—In 2012, The Advisory Committee to
the NIH Director Working Group on Diversity in the
Biomedical Research Workforce issued a report
15
acknowledging NIH’s longstanding recognition
that diversity in the biomedical research workforce
is critical to ensuring the most creative minds have
the opportunity to contribute to our research and
health goals. However, despite ongoing invest-
ment by NIH and others to increase the number of
scientists from underrepresented groups, unac-
ceptable disparities in the biomedical workforce
remain. The DPC was established to develop,
implement, assess, and disseminate innovative
and effective training and mentoring approaches
to enhance the participation and persistence of
individuals from underrepresented backgrounds

53
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Figure 36. Diversity Program Consortium
The Diversity Program Consortium was established to
develop, implement, assess, and disseminate innova-
tive and effective training and mentoring approaches to
enhance the participation and persistence of individuals
from underrepresented backgrounds in biomedical
research careers so that future programs may be more
effective at recruiting and retaining a diverse workforce.
Credit: NIH Common Fund.
in biomedical research careers so that future
programs may be more effective at recruiting
and retaining a diverse workforce. Launched
with planning grants in 2013, the rst stage of
the program had three initiatives: (1) Building
Infrastructure Leading to Diversity (BUILD), which
is developing approaches to determine the most
effective ways to engage and retain students
from diverse backgrounds in biomedical research
and to prepare students to become future con-
tributors to the NIH-funded research enterprise;
(2) the National Research Mentoring Network,
a national network of mentors and mentees
providing mentorship, professional development,
training, networking, and resources; and (3) the
Coordination and Evaluation Center, which is
coordinating and evaluating DPC activities. In
the second stage of the program, two additional
initiatives are being supported. The Sponsored
Programs Administration Development program
aims to increase the productivity of sponsored
programs ofces (or similar entities) at academic
institutions to enhance biomedical research
and research training. The DPC Dissemination
and Translation Awards (DPC DaTA) supports
non-DPC institutions to employ DPC methods
to evaluate the effectiveness of a biomedical
research training, mentoring, or research
capacity-building intervention.
• Extracellular RNA Communication (ERC)
16
—Once
thought to exist only inside cells, RNA is now
known to travel outside cells and play a role in
communication among cells throughout the body.
When the ERC program was launched in 2013,
researchers understood that RNA was exported
from cells, but fundamental questions about the
function of these extracellular RNAs (exRNAs),
how exRNAs are targeted to deliver messages to
other cells, and how exRNAs are regulated had
yet to be fully explored. Additionally, a lack of
standards, protocols, and data infrastructure was
a signicant roadblock that hindered research
progress and prevented comparison of experi-
ments between different laboratories. The ERC
program aimed to enable researchers to tackle
fundamental questions about exRNAs in a coor-
dinated way, thereby establishing new biological
paradigms and accelerating development of
exRNAs as potential therapeutics or in diagnos-
tics. The rst stage of this program catalogued
exRNA molecules found in human biouids from
more than 2,000 healthy donors; established data
standards, created a data portal, and developed
novel tools and reagents; and identied potential
exRNA biomarkers for nearly 30 diseases. In the
second stage of the program, ERC is focusing
on tool and technology development addressing
major roadblocks to understanding exRNAs,
including better understanding of the larger
complexes, like extracellular vesicles that carry
exRNAs through the body.
Strategic Planning 2017–2018
In 2017, NIH leadership identied two timely, high-
priority research areas suitable for NIH Common
Fund support. Due to the pressing public health
needs that these programs are intended to address,
both programs were planned and launched on an
accelerated timeline.
• Acute to Chronic Pain Signatures (A2CPS)
17
—As
part of NIH’s response to the growing opioid crisis,
the A2CPS program aims to further our under-
standing of the transition from acute to chronic
pain. Acute pain following injury resolves in many
patients, but for a large number of people, the
pain becomes chronic, even after the injury itself
has healed. This transition is poorly understood
and therefore prevention or treatment is difcult.
The A2CPS program is addressing this challenge

54
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Figure 37. Somatic Cell Genome Editing
Program
The Somatic Cell Genome Editing program is working
to improve the efficacy and specificity of gene editing
approaches to help reduce the burden of common and
rare diseases caused by genetic changes.
Credit: NIH Common Fund.
by developing a set of objective biomarkers (i.e.,
a “signature”) to predict susceptibility for transi-
tioning to chronic pain after an acute pain event.
The A2CPS program enhances the objectives of
the NIH Helping to End Addiction Long-term
SM
(HEAL) Initiative,
18
a transagency effort to speed
scientic solutions to end the opioid public health
crisis. A2CPS will benet the HEAL
SM
research
priority to enhance pain management. Building
upon previous efforts by the NIH Pain Consortium
and others, this program was well positioned to
rapidly launch in advance of HEAL
SM
but is now
fully coordinated with HEAL
SM
initiatives. It began
a planning stage in scal year 2019, scaling up to
implementation in scal year 2020.
• Somatic Cell Genome Editing (SCGE)
19
(Figure 37)—The development of tools and
approaches to precisely change genomic
sequences, including CRISPR, have raised the
possibility of a fundamentally new approach to
treat an enormous number of genetic diseases.
Capitalizing on the rapidly expanding eld of
precision genome editing tools, planning for the
SCGE program identied several critical areas in
need of strategic investment to accelerate devel-
opment of new genome editing–based therapies.
Signicant ongoing investments were advancing
this nascent eld but were largely focused on
ex vivo genome editing approaches, in which
cells are edited outside of the body and then
reintroduced; in vivo approaches involving editing
cells within the body were lagging behind, despite
applicability to a larger number of diseases.
Additionally, a signicant technological challenge
was targeting the editing machinery to the
appropriate cells and avoiding off-target effects.
Building upon these opportunities and challenges,
the SCGE program aims to improve the efcacy
and specicity of gene editing approaches to help
reduce the burden of common and rare diseases
caused by genetic changes. SCGE is developing
tools to perform and assess effective and safe
genome editing in nonreproductive (i.e., somatic)
cells of the body, including approaches to ensure
genome editing tools are delivered specically to
the targeted cell type within the body. By sharing
these resources with the entire research com-
munity, SCGE aims to reduce the time and cost
required to develop new therapies. An accelerated
planning process that brought together thought
leaders from academia, industry, and government
allowed this program to be quickly launched in
scal year 2018.
Additionally, discussions between NIH leadership
and IC Directors revealed enthusiasm for developing
high-priority initiatives that extend from existing NIH
Common Fund programs and leverage previous
investments. Within the CryoEM program, a new
effort was developed to increase access to cryo-
electron tomography, a related technology that
enables improved imaging of molecules within intact
cells and tissues in 3-D. Additional efforts to address
the opioid public health crisis were supported through
an expansion of the Stimulating Peripheral Activity to
Relieve Conditions (SPARC)
20
program, launching a
new initiative to generate anatomical and functional
data from neural circuits mediating visceral pain.
Strategic Planning 2018–2019
To plan for new NIH Common Fund programs for
potential launch in scal year 2021 or later, OSC host-
eda series of web-based workshops
21
with editors
from a diverse array of biomedical and behavioral
research journals. The objective of these workshops
wasto learn about new scientic trends, emerging
areas of research, and crosscutting challenges that
may contribute to planning for new NIH Common
Fund programs.Journal editors, with the exposure
to and assessment of new scientic advances, are in
a good position to understand the current scientic
landscape. One prominent theme articulated in these

55
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
workshops was the emerging opportunities presented
by integration of articial intelligence (AI) and machine
learning approaches into biomedical research.
Independently, in recognition of the opportunity and
challenges posed by AI in biomedicine, NIH orga-
nized a workshop in July 2018, Harnessing Articial
Intelligence and Machine Learning to Advance
Biomedical Research.
22
These initial discussions
contributed to additional planning activities and, ulti-
mately, a new NIH Common Fund program in AI (see
the next section, “Strategic Planning 2019–2020,” for
more details).
In addition to input gathered through the journal
editor workshops, OSC also solicited ideas from IC
Directors. From this process, three ideas emerged
that are now being pursued as potential NIH Common
Fund programs.
• Harnessing Data Science for Health Discovery
and Innovation in Africa
23
—This program will
leverage data science technologies and prior
NIH investments to develop solutions to Africa’s
most pressing public health problems through a
robust ecosystem of new partners from academic,
government, and private sectors. Extensive
mobile phone coverage in Africa provides an
opportunity to rapidly advance health care delivery
systems through mobile health applications,
point-of-care technologies, and self-management
systems. Additionally, this program leverages
and builds upon substantial investment in African
research and research training by NIH ICs, the
NIH Common Fund, and other organizations.
For example, the Data Science in Africa program
will build on and translate the resources and
expertise developed through the Human Heredity
and Health in Africa
24
program into products and
policies impacting health in Africa and around
the world. The program aims to promote sustain-
ability of the African health research enterprise
by encouraging robust partnerships with African
governmental, private, and academic partners and
will also consider ethical, legal, and social issues
for data science research and its applications
to public health in Africa. This program was
approved by the NIH Director and is anticipated to
launch in scal year 2021.
• Faculty Institutional Recruitment for Sustainable
Transformation (FIRST)
25
—Despite ongoing
investment in programs designed to enhance
the diversity of the biomedical workforce,
underrepresentation of some racial and ethnic
groups, particularly at the faculty level, remains a
persistent challenge. Many previous efforts have
focused on individuals; however, substantial evi-
dence suggests that targeting institutional culture
change is needed to achieve the desired results.
Early success of the NIH Distinguished Scholars
Program
26
and other cohort-based recruitment
programs indicates that recruitment of a critical
mass of investigators committed to diversity and
inclusion may foster the institutional changes
needed to create meaningful changes in diversity
at the faculty level. The FIRST program aims to
create cultures of inclusive excellence at NIH-
funded institutions, establishing and maintaining
scientic environments that can cultivate and
benet from a full range of talent. It will establish
a faculty cohort model for hiring, mentoring, and
professional development; integrated, institu-
tion-wide approaches to address bias, faculty
equity, mentoring, and work-life issues; and a
coordination and evaluation center to conduct
independent evaluations of program impacts. This
program was approved by the NIH Director and is
anticipated to launch in scal year 2021.
• Nutrition for Precision Health, powered by
the NIH All of Us Research Program—Current
dietary recommendations are often confusing,
sometimes contradictory, and generally do not
consider individual differences. Rapidly advancing
technologies—including high-throughput -omics
(e.g.,genomics, epigenomics, proteomics, metab-
olomics) and AI—combined with the growing
emphasis on personalized medicine approaches
present an opportunity to develop more precise
and dynamic nutritional recommendations. The
program, still in development, would aim to
understand individual responses to diet, enabling
tailored dietary recommendations to be provided
by physicians and the development of tools to
allow individuals to make more informed decisions
about healthy food choices. This program is
anticipated to launch in scal year 2021.
Strategic Planning 2019–2020
To plan for new NIH Common Fund programs to
begin in scal year 2022 or beyond, OSC used an
online crowdsourcing platform to solicit ideas from

56
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Figure 38. Artificial Intelligence for BiomedicaL Excellence Program
Following a 2018 NIH workshop on artificial intelligence (AI) and machine learning in biomedical research, the NIH
Director formed the Advisory Committee to the NIH Director (ACD) Working Group on Artificial Intelligence. This group
was charged with determining opportunities for NIH-wide efforts in AI and ways these efforts could cross biomedical
topics to positively affect diverse fields, identifying ways for NIH to build connections between the data science and
biomedical research communities, defining approaches to cross-training computer scientists and biomedical research-
ers, and identifying ethical consideration for biomedical research and AI.
This working group delivered its final recommendations in December 2019. Several of these recommendations fit well
with the criteria for NIH Common Fund programs, whereas other recommendations were within the mandate of the NIH’s
Office of Data Science Strategy. An NIH-wide working group convened and conducted planning activities to determine
how an NIH Common Fund program could effectively address the relevant recommendations, leading to development
of the Artificial Intelligence for BiomedicaL Excellence (AIBLE) program. The overall goal of this program is to generate
new biomedically relevant datasets amenable to machine learning analysis at scale, achieved through the following
initiatives:
• Support data design centers to generate rubrics of amenability to machine learning approaches that allow the
evaluation of datasets and plans to generate datasets, create infrastructure to disseminate tools, and host and
promote datasets.
• Develop software and firmware tools to accelerate AI readiness.
• Enhance existing data generation efforts to improve AI readiness.
• Generate gold-standard, multimodal human datasets that adhere to the rubrics established by the program.
• Use the rubrics to evaluate and update select existing public biomedical research data.
Because this potential program leveraged the carefully developed recommendations from the ACD working group, it is
anticipated to launch on an accelerated timeline in fiscal year 2021.
the NIH community for bold investments that could
become future NIH Common Fund programs. The
community was also encouraged to provide construc-
tive comments on ideas submitted by others, so that
each idea could benet from the collective expertise
of the NIH community. In addition to gathering ideas
through the crowdsourcing site, IC Directors were
also invited to submit ideas.
From this process, one idea focused on exploring
transposable elements and somatic mosaicism was
selected for further development. This potential
program, Somatic Mosaicism and Retrotranspositions
(SMaRt), would investigate genetic elements that
make up approximately half of the human genome
and which, in some cases, have the ability to move
within the genome and thereby create genetically
distinct cells within a single individual. This mobility
can result in genomic damage and disease, but
the extent to which this process happens and how
it is regulated is largely unknown. If approved, the
SMaRT program would aim to deliver new paradigms
concerning the regulation of these elements and how
their transposition contributes to normal biology and
disease. Pending approval, this program is anticipat-
ed to launch in scal year 2022.
In addition to the strategic planning process above,
several other NIH-wide efforts contributed to
development of new NIH Common Fund programs.
At the NIH Leadership Forum, NIH leadership and
ICDirectors identied cellular senescence as a
high-priority research area. Cellular senescence
refers to a highly stable state of cell cycle arrest in
which cells stop dividing, often in response to various
stressors, such as aging and inammation. A better
understanding of the mechanisms of cellular senes-
cence and how this process affects tissue and organ
function may lead to new approaches for addressing
the deleterious effects of aging and of numerous
diseases and conditions. If approved, this program is
planned to launch in scal year 2022.
Finally, the Advisory Committee to the NIH Director
Working Group on Articial Intelligence provided NIH-
wide recommendations
27
on how NIH could leverage
and promote AI to advance research across many
biomedical topics and have positive effects across
diverse elds. Several of these recommendations
formed the basis for a new potential NIH Common
Fund program, Articial Intelligence for BiomedicaL
Excellence (AIBLE).
28
This program aims to generate
new biomedically relevant datasets amenable to
machine learning analysis at scale. This program is
anticipated to launch in scal year 2021. For more
details, see Figure 38.

57
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Figure 39. Transition of the Human Microbiome Project
The Human Microbiome Project (HMP), supported by the NIH Common Fund from 2007 to 2016, developed numerous
research resources to enable the study of the microbial communities that live in and on the human body and the roles
these communities play in health and disease. The first stage of HMP developed DNA sequence datasets and computa-
tional tools for characterizing the microbiome in healthy adults and in people with microbiome-associated diseases. The
second stage of HMP created integrated datasets of multiple biological properties from both the microbiome and the
host over time in people with specific microbiome-associated diseases.
HMP was an extremely successful program. Some of its major accomplishments include sequencing approximately
3,000 reference bacterial genomes isolated from the human body; generating a comprehensive profile of the healthy
human microbiome; developing integrated datasets of metagenomic, transcript, protein, and metabolite profiles from
microbiome and host in multiple human cohorts; developing software and online resources to enable studies of the
microbiome; and publication of more than 700 scientific papers.
HMP helped catalyze the nascent field of microbiome research, laying the foundation for continued NIH investment
through the Institutes and Centers (ICs) after the program ended. NIH investment in microbiome research outside of
HMP has increased more than 40-fold since the inception of HMP and now spans more than 20 ICs. The Trans-NIH
Microbiome Working Group was established in 2012 to provide a forum for coordinating NIH research activities
related to the human microbiome. Ongoing access to critical HMP resources, including datasets and digital tools, will
be accomplished through the Common Fund Data Ecosystem (CFDE). Inclusion of these resources within the CFDE
ensures that the biomedical research community continues to benefit from HMP and that investment in HMP is lever-
aged for maximum possible impact.
Strategic Planning 2020–2021
OSC is currently beginning a new round of strategic
planning in 2020. Still in the early stages of develop-
ment, this round of strategic planning is intended to
leverage existing community-generated white papers
(i.e., assessments of scientic opportunities and
needs in a given scientic area). By reviewing these
thoughtful analyses from many scientic societies or
other groups, NIH may obtain well-considered input
that reects consensus views and that may reveal
overlapping challenges and opportunities affecting
multiple communities. Potential program concepts
will also be solicited from the IC Directors and may
arise from discussions involving NIH leadership,
Advisory Councils, or other entities providing input
to NIH.
Planning for Transition from NIH
Common Fund Support
NIH Common Fund programs are designed to
achieve a set of high-impact goals within a dened
time frame. At the conclusion of each program, deliv-
erables will either stimulate IC-funded research or will
transition to support by ICs or other entities that nd
the resources generated by the program useful.
Transition plans are considered early in the lifecycle of
an NIH Common Fund program, and these plans are
reconsidered throughout the lifecycle to ensure the
transition accommodates the changing needs of both
the program and the external scientic community.
A detailed description of the NIH Common Fund’s
Human Microbiome Project
29
transition is provided as
an example in Figure 39.

58
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Table 1: The NIH Common Fund Budget, Fiscal Years 2018–2021
Fiscal Year
2018 Actual
Fiscal Year
2019 Actual
Fiscal Year 2020
Actual
Fiscal Year 2021
President’s Budget
Request
a
NIH Common Fund (dollars in
millions)
$600.7 $619.2 $639.1 $596.5
NIH Common Fund
Percentage of NIH Labor/U.S.
Department of Health and
Human Services Funding
b
1.62% 1.59% 1.54% 1.54%
a
Includes March 17, 2020, budget amendment of $439.584 million for the National Institute of Allergy and Infectious Diseases.
b
Excludes mandatory funding for the Type 1 Diabetes Research program and funding appropriated through the Interior, Environment, and Related Agencies
Appropriations Act for the National Institute of Environmental Health Sciences Superfund Research Program. Includes program evaluation financing resources.
The NIH Common Fund Budget
The NIH Common Fund budget for scal years
2018–2021 is shown in Table 1. Although NIH
Common Fund programs are planned in advance, the
specic activities funded in each program depend on
the budget made available through annual appropri-
ations. As programs end, funds are freed to support
new programs and planned expansions of ongoing
programs.
The Public Health Service Act requires that the NIH
Common Fund Strategic Plan Report include an
estimate of amounts needed for (i) maximizing the
potential of the Common Fund research under 42
U.S.C. 282(b)(7)(A)(i); (ii) to be sufcient only for con-
tinuing to fund research activities previously identied
by the Division of Program Coordination, Planning,
and Strategic Initiatives; and (iii) to be necessary
to fund research described in 42 U.S.C. 282(b)(7)
(A)(i) that (1) is in addition to the research activities
described in clause (ii) and (2) for which there is the
most substantial need. See 42 U.S.C. 282a(c)(1)(C).
Budgets for ongoing NIH Common Fund programs
are planned in advance to maximize the potential of
all programs. Therefore, the amounts described in (i)
and (ii) are the same and are equal to the total budget
for all NIH Common Fund programs. In addition to the
amount for ongoing NIH Common Fund programs,
funds are available for new initiatives each year.
These new initiatives are identied by the strategic
planning principles outlined in this report, thus
ensuring they address research areas of substantial
need. Within each of the programmatic areas identi-
ed through strategic planning, the NIH peer review
process also identies specic research proposals
addressing areas of substantial need. Therefore, the
amounts described in (iii) are equal to the amount
reserved for new NIH Common Fund initiatives.
Each year, as part of the President’s Budget Request,
the NIH Common Fund describes both the amounts
estimated for each ongoing program (i and ii) and the
amounts budgeted for new initiatives (iii). Table 2
shows the estimates presented in the Fiscal Year
2021 President’s Budget Request; prior years’
Requests can be found at https://commonfund.nih.
gov/about/budgetrequests.

59
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Table 2: NIH Common Fund President’s Budget Request, Fiscal Year 2021
NIH Common Fund Program
(Dollars in Thousands)
Fiscal Year
2019 Final
Fiscal Year
2020 Enacted
Fiscal
Year 2021
President’s
Budget Request
4D Nucleome 27,997 28,860 27,485
Acute to Chronic Pain Signatures 2,094 16,636 14,648
Big Data to Knowledge (BD2K) 2,605 0 0
Enhancing the Diversity of the NIH-Funded Workforce 52,656 53,713 47,401
Extracellular RNA Communication 6,728 5,846 10,497
Gabriella Miller Kids First Pediatric Research 13,482 13,000 13,000
Genotype-Tissue Expression (GTEx) Resources 772 0 0
Global Health 15,569 11,565 9,261
Glycoscience 19,435 13,362 5,191
Health Care Systems Research Collaboratory 1,988 1,750 1,694
High-Risk Research 206,110 193,100 186,001
NIH Director’s Pioneer Award 45,446 54,265 51,293
NIH Director’s New Innovator Award Program 102,692 77,815 79,795
Transformative Research Award 35,149 38,402 34,659
NIH Director’s Early Independence Award Program 22,823 22,618 20,255
Human BioMolecular Atlas Project (HuBMAP) 15,005 27,031 31,040
Illuminating the Druggable Genome 12,970 13,390 12,971
Knockout Mouse Phenotyping Program 13,757 11,000 0
Library of Integrated Network-Based Cellular Signatures (LINCS) 9,946 87 0
Metabolomics 12,403 12,401 12,000
Molecular Transducers of Physical Activity 44,744 46,126 42,609
New Models of Data Stewardship 199 0 0
NIH Center for Regenerative Medicine (NCRM) 7,597 5,700 0
Protein Capture 1,334 0 0
Science of Behavior Change 12,674 222 0
Somatic Cell Genome Editing 33,324 38,937 44,232
S.P.A.R.C. - Stimulating Peripheral Activity to Relieve Conditions 51,559 47,268 41,883
Strengthening the Biomedical Research Workforce 56 0 0
Transformative High Resolution Cryo-Electron Microscopy (CryoEM) 14,895 51,800 36,290
Undiagnosed Diseases Network 29,207 24,401 21,683
Strategic Planning, Evaluation, and Infrastructure 10,061 22,917
21,129
Subtotal NIH Common Fund 619,166 639,111 579,017
New Initiatives in NIH Common Fund 0 0 17,450
Total NIH Common Fund 619,166 639,111 596,467

60
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
4 https://dpcpsi.nih.gov/council.
5 https://www.congress.gov/114/plaws/publ255/PLAW-114publ255.pdf.
6 https://commonfund.nih.gov/sites/default/files/2015%20Common%20Fund%20Strategic%20Planning%20Report_
final%20-%20508.pdf.
7 https://commonfund.nih.gov/HuBMAP.
8 https://commonfund.nih.gov/Singlecell.
9 https://commonfund.nih.gov/CryoEM.
10
https://commonfund.nih.gov/IDG.
11
https://commonfund.nih.gov/metabolomics.
12
https://commonfund.nih.gov/Diseases.
13
https://archives.nih.gov/asites/report/09-09-2019/report.nih.gov/nihfactsheets/ViewFactSheete790.html?c-
sid=126&key=R#R.
14
https://commonfund.nih.gov/diversity.
15
https://acd.od.nih.gov/documents/reports/DiversityBiomedicalResearchWorkforceReport.pdf.
16
https://commonfund.nih.gov/exrna.
17
https://commonfund.nih.gov/pain.
18
https://heal.nih.gov.
19
https://commonfund.nih.gov/editing.
20
https://commonfund.nih.gov/sparc.
21
https://commonfund.nih.gov/sites/default/les/Journal_Editors_Workshop_Exec_Summary_508.pdf.
22
https://datascience.nih.gov/community/2018biomedAI.
23
https://commonfund.nih.gov/AfricaData.
24
https://h3africa.org.
25
https://commonfund.nih.gov/rst.
26
https://diversity.nih.gov/programs-partnerships/dsp.
27
https://acd.od.nih.gov/documents/presentations/12132019AI.pdf.
28
https://dpcpsi.nih.gov/sites/default/files/CoC_May_2020_1.05PM_Concept_Clearance_AIBLE_Brennan_508.pdf.
29
https://commonfund.nih.gov/hmp.
Endnotes
1 https://commonfund.nih.gov.
2 https://commonfund.nih.gov/dataecosystem.
3 https://commonfund.nih.gov/sites/default/les/Initiatives_6-28-11.pdf.

61
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Appendix V: Acronyms
3-D three-dimensional
A2CPS Acute to Chronic Pain Signatures
ABCD Adolescent Brain Cognitive
Development
ACTIV Accelerating COVID-19 Therapeutic
Interventions and Vaccines
AFREhealth African Forum for Research and
Education in Health
AHRQ Agency for Healthcare Research and
Quality
AI articial intelligence
AIBLE Articial Intelligence for BiomedicaL
Excellence
AMD age-related macular degeneration
AMP Accelerating Medicines Partnership
AMP-AD AMP-Alzheimer’s Disease
AMP-PD AMP-Parkinson’s Disease
AMP-RA/
Lupus
AMP-Rheumatoid Arthritis/Lupus
AMP-T2D AMP-Type 2 Diabetes
ASSIST Application Submission System &
Interface for Submission Tracking
BIRCWH Building Interdisciplinary Research
Careers in Women’s Health
BRAIN Brain Research through Advancing
Innovative Neurotechnologies
®
BUILD Building Infrastructure Leading to
Diversity
CAR chimeric antigen receptor
CC NIH Clinical Center
CDC Centers for Disease Control and
Prevention
CFDE Common Fund Data Ecosystem
CIT Center for Information Technology
ClinGen Clinical Genome
CoC Council of Councils
CORD-19 COVID-19 Open Research Dataset
COVID-19 coronavirus disease 2019
cryoEM cryo-electron microscopy
CSR Center for Scientic Review
CTSA Clinical and Translational Science
Awards
DASH Data and Biospecimen Hub
DoD U.S. Department of Defense
DPC Diversity Program Consortium
DPC DaTA DPC Dissemination and Translation
Awards
DPCPSI Division of Program Coordination,
Planning, and Strategic Initiatives
DR2 Disaster Research Response
DRC Democratic Republic of the Congo
ECHO Environmental inuences on Child
Health Outcomes
ENCODE ENCyclopedia of DNA Elements
ERC extracellular RNA communication
ERM Enterprise Risk Management
EVD Ebola virus disease
exRNA extracellular RNA
FAIR ndable, accessible, interoperable,
and reusable
FDA U.S. Food and Drug Administration
FIC Fogarty International Center
FIRST Faculty Institutional Recruitment for
Sustainable Transformation
FOIA Freedom of Information Act
GACD Global Alliance for Chronic Diseases
GBD Global Burden of Disease
H3Africa Human Heredity and Health in Africa
Consortium

62
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
HEAL Helping to End Addiction
Long-term
SM
HHS U.S. Department of Health and
Human Services
HMP Human Microbiome Project
HRSA Health Resources and Services
Administration
HuBMAP Human BioMolecular Atlas Program
IC Institute and Center
IDeA Institutional Development Award
IDG Illuminating the Druggable Genome
IMPROVE Implementing a Maternal health and
PRegnancy Outcomes Vision for
Everyone
INCLUDE INvestigation of Co-occurring
conditions across the Lifespan to
Understand Down syndromE
IPRCC Interagency Pain Research
Coordinating Committee
iPSC induced pluripotent stem cell
ISS-NL International Space Station
U.S. National Laboratory
MOSAIC Maximizing Opportunities
for Scientic and Academic
Independent Careers
MoTrPAC Molecular Transducers of Physical
Activity Consortium
NARI Native American Research
Internship
NASA National Aeronautics and Space
Administration
NCATS National Center for Advancing
Translational Sciences
NCCIH National Center for Complementary
and Integrative Health
NCD noncommunicable diseases
NCI National Cancer Institute
NEI National Eye Institute
NGRI Next Generation Researchers
Initiative
NHGRI National Human Genome Research
Institute
NHLBI National Heart, Lung, and Blood
Institute
NIA National Institute on Aging
NIAAA National Institute on Alcohol Abuse
and Alcoholism
NIAID National Institute of Allergy and
Infectious Diseases
NIAMS National Institute of Arthritis and
Musculoskeletal and Skin Diseases
NIBIB National Institute of Biomedical
Imaging and Bioengineering
NICHD Eunice Kennedy Shriver National
Institute of Child Health and Human
Development
NIDA National Institute on Drug Abuse
NIDCD National Institute on Deafness and
Other Communication Disorders
NIDCR National Institute of Dental and
Craniofacial Research
NIDDK National Institute of Diabetes and
Digestive and Kidney Diseases
NIEHS National Institute of Environmental
Health Sciences
NIGMS National Institute of General Medical
Sciences
NIH National Institutes of Health
NIH
RePORTER
NIH Research Portfolio Online
Reporting Tools Expenditures and
Results
NIMH National Institute of Mental Health
NIMHD National Institute on Minority Health
and Health Disparities
NINDS National Institute of Neurological
Disorders and Stroke
NINR National Institute of Nursing
Research
NLM National Library of Medicine
OD NIH Ofce of the Director
OSC Ofce of Strategic Coordination
PALM
Pamoja Tulinde Maisha
PATH Population Assessment of Tobacco
and Health

63
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
PHS Public Health Service
PMC PubMed Central
PPP public–private partnership
PRGLAC Pregnant Women and Lactating
Women
RCDC Research, Condition, and Disease
Classication
RCMI Research Centers in Minority
Institutions
RFI Request for Information
SAMHSA Substance Abuse and Mental Health
Services Administration
SARS-CoV-2 severe acute respiratory syndrome
coronavirus 2
SCAP Single Cell Analysis Program
SCD sickle cell disease
SCDIC Sickle Cell Disease Implementation
Consortium
SCGE Somatic Cell Genome Editing
SEER Surveillance, Epidemiology, and End
Results
SGM sexual and gender minority
SIG Shared Instrumentation Grant
SMaRt Somatic Mosaicism and
Retrotranspositions
SPARC Stimulating Peripheral Activity to
Relieve Conditions
SPRINT Systolic Blood Pressure Intervention
Trial
SSC Symptom Science Center
STRIDES Science and Technology Research
Infrastructure for Discovery,
Experimentation, and Sustainability
TRSP Tobacco Regulatory Science
Program
UDN Undiagnosed Diseases Network
UDP Undiagnosed Diseases Program
VA U.S. Department of Veterans Affairs

64
NIH-Wide Strategic Plan for Fiscal Years 2021–2025
Acknowledgments
The NIH-Wide Strategic Plan for Fiscal Years 2021–2025 is the product of many contributors. The NIH
Director would like to thank the following stakeholders, committees, and staff for their time and effort in
helping to develop this Strategic Plan.
• We would like to thank the NIH-Wide Strategic Working Group, whose enthusiasm, knowledge, and
commitment made this document possible: Elizabeth Baden, Julie Frost Bellgowan, Michelle Bennett,
Laura Berkson, David Bochner, Laura Brockway-Lunardi, Thomas Calder, Cindy Caughman, Mindy Chai,
Stephanie Clipper, Laura Cole, Christine Cooper, Stephanie Courchesne-Schlink, Jessica Creery, Ned
Culhane, Hope Cummings, Charles Dearolf, Clarence Dukes, Deborah Duran, Yvette Edghill Spano,
Nicole Garbarini, Taylor Gilliland, Shefa Gordon, John Grason, Rebecca Hong, Cristina Kapustij, Edmund
Keane, Mary Beth Kester, David Kosub, Ira Kukic, Erica Landis, Charlene Le Fauve, Issel Anne Lim, Ryan
Mahon, Rebecca Meseroll, Wynn Meyer, Lara Miller, Kathryn Morris, Kate Nagy, Patty Newman, Sheila
Newton, Rosanna Ng, Samia Noursi, Eileen Oni, Wilma Peterman Cross, Kamilah Rashid, Reaya Reuss,
Sarah Rhodes, David Saeger, Leigh Samsel, Claire Schulkey, Paul Scott, Ching-Yi Shieh, Kelly Singel,
Tyrone Spady, Erin Spaniol, Meredith Stein, Daniel Stimson, Nathaniel Stinson, Denise Stredrick, Rachel
Sturke, Meredith D. Temple-O’Connor, Kimberly Thigpen Tart, Leslie Thompson, Valerie Virta, Marina
Volkov, Julie Wallace, Elizabeth Walsh, Bridget Williams-Simmons, Nora Wong.
• In addition, we thank those across NIH who took the time to review the Framework and draft Strategic
Plan and provide content. This includes Institute, Center, and OD Office Directors and staff.
• We would like to thank the NIH Advisory Committee to the Director and the NIH Division of Program
Coordination, Planning, and Strategic Initiatives Council of Councils for their insightful feedback on
the Framework and draft Strategic Plan.
• Finally, we are enormously appreciative of the robust input into the strategic planning process
from stakeholder communities, including members of the scientic and health care communities,
professional societies, advocacy organizations, industry, other federal agencies, and the general public.
We look forward to your continued involvement as NIH works to implement the vision outlined here.

